Behandelproblematiek en laatste ontwikkelingen in...
25
Behandelproblematiek en laatste ontwikkelingen in Hepatitis B Nationale hepatitis dag 2017 Bart Takkenberg Academisch Medisch Centrum Amsterdam
Transcript of Behandelproblematiek en laatste ontwikkelingen in...

Behandelproblematiek en laatste
ontwikkelingen in Hepatitis B
Nationale hepatitis dag 2017
Bart Takkenberg
Academisch Medisch Centrum
Amsterdam

Disclosures
• Speaker for Gore WL, Bayer, and Norgine
• Advisory board for Gilead

Behandelproblematiek

EASL HBV guidelines 2017
• Behandeling gebaseerd op:
– HBV DNA (> 20,000 IU/mL)
– ALAT (> 2xULN; ULN ~ 40 IU/mL)
– Mate van leverschade (cirrose ja/nee)

Casus 1
• De heer C, 58-jarige man, oorspronkelijk afkomstig uit China.
• Chronische hepatitis B
• ALAT 34, ASAT 28
• HBsAg positief (>150 IU/mL), HBeAg negatief
• HBV DNA 2,32x10e4 IU/mL
• Echo: Geen afwijkingen, milt 8 cm
• Fibroscan: 7,9 kPa, CAP 198 dB/m
• Vraag:
– Gaat u starten met behandelen?

Casus 1: Doel van behandeling
• Primair eindpunt:
– Verbeteren van overleving en kwaliteit van leven d.m.v:
• Voorkomen van progressie van ziekte.
• Voorkomen van HCC.
• Secundaire eindpunten:
– Voorkomen van perinatale transmissie.
– Voorkomen van hepatitis B reactivatie.
– Voorkomen en behandelen van extrahepatische HBV-
geassocieerde aandoeningen.
EASL HBV guidelines 2017

Casus 1: Wat zegt de richtlijn
• All patients with HBeAg positive or – negative chronic
hepatitis B, defined by HBV DNA > 2,000 IU/mL, ALT > ULN,
and/or at least moderate liver necroinflammation or fibrosis,
should be treated (Level I).
• Patients with HBeAg-negative chronic HBV infection and
serum HBV DNA ≥ 2,000 IU/mL who do not fullfill any of the
above teatment indications should be followed every 3
months for the first year and every 6 months thereafter (Level
III).
EASL HBV guidelines 2017

Casus 1: Risico op HCC: REACH-B
Yang HI et al, Lancet oncol 2011; 12(6)568-74
De heer C: 11 punten

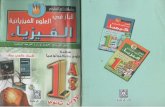
Casus 1: effect NA op HCC incidentie
Hoang et al, Medicine 2016; 95 (31): 1-7
Retrospectieve studie:
• effect antivirale therapie op
HCC incidentie.
• 3665 US en Taiwanese CHB
patiënten zonder cirrose
– 2882: ALAT< 2x ULN
– 1543: ALAT< 2x ULN en HBV
DNA > 20,000 IU/mL
• HCC risico gescoord middels
REACH-B model
ALAT < 2xULN

Casus 1: effect NUC op HCC incidentie
Hoang et al, Medicine 2016; 95 (31): 1-7
5 jaar
10 jaar

Casus 2
• De heer A, 44-jarige man, oorspronkelijk afkomstig uit Marokko.
• Chronische hepatitis B
• Nu al 6 jaar tenofovir.
• ALAT 19, ASAT 17
• HBsAg positief (87 IU/mL), HBeAg negatief
• HBV DNA: TND IU/mL
• Echo: Geen afwijkingen, milt 9 cm
• Fibroscan: 6.7 kPa, CAP 210 dB/m
• Vraag:
– Kan er gestopt worden met behandelen?

Casus 2: Wat zegt de richtlijn
• Discontinuation of NAs in selected non-cirrhotic HBeAg-
negative patients who have achieved long-term (≥ 3 years)
virological suppression under NA(s) may be considered if
close post-NA monitoring can be guaranteed (Level II-2)
EASL HBV guidelines 2017

Casus 2: respons na staken NUC
Lok et al, Hepatology 2016: 63(1);284-306
Author Year Treatment N Virological
relapse
Clinical
relapse
Fung et al 2004 LAM 27 30%
Liu et al 2011 LAM 61 50%
Hadziyannis et al 2012 ADF 33 45%
Jeng et al 2013 ENT 95 45%
Chang et al 2015 LAM 263 30%
Jun Yong Park et al 2014 - - 54%

Casus 2: respons na staken NUC
Papatheodoridis et al, Hepatology 2016: 63(5);1481-92
• In totaal 967 HBeAg negatieve patiënten.
57%
KL
IN. R
EL
AP
SE
Pa
tiën
ten
in
Viro
log
isch
e re
mis
sie

Casus 2
• De heer A, 44-jarige man, oorspronkelijk afkomstig uit Marokko.
• Chronische hepatitis B
• Nu al 6 jaar tenofovir.
• ALAT 19, ASAT 17
• HBsAg positief (87 IU/mL), HBeAg negatief
• HBV DNA TND IU/mL
• Echo: Geen afwijkingen, milt 9 cm
• Fibroscan: 6.7 kPa, CAP 210 dB/m
• Vraag:
– Is het HBsAg voorspellend?

Casus 2
• Lagere HBsAg waarden op het moment van stoppen ADF
waren voorspellend voor HBsAg verlies (39%).1
• Lagere baseline HBsAg waarden hebben grotere kans op
“sustained response”.2
1 Hadziyannis et al, Gastroentrology 2012; 143: 629-636 2 Berg et al. J. Hepatol 2017 (67) 918-924

Casus 2: HBsAg en fase van infectie
Jaroszewicz et al, J. Hepatol. 2010; 52(4): 514-22
Inactief
n=68
Actief
n=68
inactief actief
HBsAg 87 IU/mL
HBeAg negatief

Laatste ontwikkelingen….
…. en de rol van TAF

Booming: nieuwe behandelingen voor HBV
Durantel J Hep 2016
Durantel et al J. hepatol 2016

Tenofovir alafenamide (TAF)
1Chan et al. Buti et al. Lancet Gastroenterol Hepatol 2016; 1: 185-95 2Buti et al. Lancet Gastroenterol Hepatol 2016;
1: 196–206
%ALAT normalisatie
%HBV DNA NEG

TAF als nieuwe behandeling?
1Chan et al. Buti et al. Lancet Gastroenterol Hepatol 2016; 1: 185-95 2Buti et al. Lancet Gastroenterol Hepatol 2016;
1: 196–206
HBeAg POS1
botdichtheid
Creatinine
HBeAg NEG2

Wat zegt de richtlijn
EASL HBV guidelines 2017

Is tenofovir dan niet meer veilig?
Buti et al, Dig Dis Sci 2015;60:1457-64
Welke patiënten?
De novo or switch?

Conclusie
• Behandeldoel:
– Preventie van progressie
– HCC preventie.
• ± 40% HBeAg negatieve patiënten blijft inactief na staken NA.
• Op korte termijn geen nieuwe middelen.
• Plaats van TAF moet bediscussieerd worden.
– CAVE: economische belangen boven patiënt belangen!

Vragen?