




Talen
Pages
Wettelijk

Nice to have or need to have?
Unraveling Dosage of Pain Rehabilitation
Franka Waterschoot
The research project “Nice to have or need to have” was funded by:
Pijnrevalidatie - Centrum voor revalidatie UMCG
The publication of this thesis was fi nancially supported by:
University of Groningen - RUG
Graduate school for Health Research - SHARE
Centrum voor Revalidatie - Universitair Medisch Centrum Groningen (UMCG)
Pijnrevalidatie - Centrum voor revalidatie UMCG
Stichting Beatrixoord Noord - Nederland
Menzis Zorgverzekering
Cover design: Isontwerp - ‘s Hertogenbosch
Layout: Gildeprint - Enschede
Printed by: Gildeprint - Enschede
Waterschoot, Franka. Nice to have or need to have. Unraveling dosage of pain rehabilitation.
Thesis University of Groningen, the Netherlands – with references – with summary in Dutch.
ISBN: 978-90-367-8512-9 (printed version)
ISBN: 978-90-367-8513-6 (electronic version)
Copyright © 2015. F.P.C. Waterschoot.
Nice to have or need to have?
Unraveling Dosage of Pain Rehabilitation
Proefschrift
ter verkrijging van de graad van doctor aan de
Rijksuniversiteit Groningen
op gezag van de
rector magnifi cus prof. dr. E. Sterken
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
maandag 15 februari 2016 om 14.30 uur
door
Franka Petronella Catharina Waterschoot geboren op 20 juni 1978
te Hoogeloon
Promotores
Prof. dr. M.F. Reneman
Prof. dr. J.H.B. Geertzen
Prof. dr. P.U. Dijkstra
Beoordelingscommissie
Prof. dr. J.G.M. Rosmalen
Prof. dr. K.M.G. Schreurs
Prof. dr. C. van Bennekom

Paranimfen: Annemieke de Jong
Berry van Holland

Table of content
Chapter 1 General introduction. 9
Chapter 2 Dose or content? Effectiveness of pain rehabilitation programs for 19
patients with chronic low back pain: A systematic review.
Chapter 3 Course of disability reduction during a pain rehabilitation program: 43
A prospective clinical study.
Chapter 4 Dosage of pain rehabilitation programs for patients with chronic 57
musculoskeletal pain: A non- inferiority randomized controlled trial.
Chapter 5 Dosage of pain rehabilitation programs: A qualitative study from 73
patient and professionals’ perspectives.
Chapter 6 Towards a case complexity index of patients with chronic 91
non-specifi c musculoskeletal pain: A Delphi and feasibility study.
Chapter 7 General discussion. 109
Summary 123
Samenvatting 129
Dankwoord 137
Over de auteur 143
Research institute SHARE 147
Extremities, Pain and Disability (Expand) 153


R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
10 | Chapter 1
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 11
1Background of thesis
In Europe, 19% of the adult population suffers from chronic pain of moderate to severe intensity 1. Chronic pain is associated with lower quality of life, less participation in major life domains,
higher healthcare utilization, lower work productivity, and higher direct and indirect costs 1,2.
Among the many treatment options for chronic pain are multidisciplinary pain rehabilitation
programs (PRPs). There is robust evidence that PRPs are effective 3-5. They can help to improve
quality of life, improve participation in major life domains, and decrease healthcare utilization.
There is confl icting evidence on the benefi ts for work-related outcomes, however 5,6.
The positive effects are ro bust, although the average size of the effects is modest and there is a
great need for further improvements. Optimizing the outcomes of PRPs should benefi t patients
suffering from chronic pain, and the benefi ts should extend to the patients’ families, in addition
to other stakeholders such as rehabilitation centers, healthcare providers, healthcare insurers,
employers, coworkers and disability insurers (temporary and permanent). Up to now, all studies
that have aimed at optimizing outcomes of PRP have focused on content, composition and
delivery form, such as individually or multidisciplinary therapy 3-10. However, optimal PRP may
also relate to dosage of PRP. Dosage of PRP appears to be a neglected, but potentially relevant,
topic in PRP and PRP research. Dose variables can be expressed as the total duration and amount
of contact hours (Text box). Additionally, the number of healthcare professionals involved in the
program, regardless of whether an inpatient or an outpatient program is offered, and dosage per
contact hour are related to the total dosage of PRP.
There are several motives for arguing why a closer look at the dosage of PRP might be necessary:
- In clinical practice, large variations of PRP-dosage are observed, in the Netherlands as well as
internationally. There are also large variations observed in dosages that have been described
in PRP research 6,7. The rationale for dosage variations is unknown.
- Scientifi cally, a consequence of research focused on content only is that infl uence of
dosage on the effect of PRP is neglected. For example, a study concluding inferiority of PRP,
comparing multidisciplinary PRP of 100 hours with mono-disciplinary physiotherapy of 50
hours could be confounded because not only does the content differ, but also dosage does
differ. Theoretically, both content and dose variables can contribute to the effectiveness
of PRP. There is a lack of studies comparing multidisciplinary PRPs with only dosage as a
comparing variable: randomized controlled trials comparing differences in dosage between
multidisciplinary treatments with the same content have not yet been performed.
- Viewed from the process of care, optimizing the entire logistic process of PRP, from registration
to discharge, is important. It can reduce waiting lists and improve cost effectiveness,
benefi tting both patients and rehabilitation centers. To manage this process, it is necessary
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
12 | Chapter 1
to determine the total number of patients treated, as well as the in- and outfl ow of patients.
Consequently, to infl uence the outfl ow to optimize infl ow, it is necessary to determine the
offered dosage of PRP.
- Ethically, not knowing the optimal dosage of PRP, the question is raised as to whether over-
or undertreatment will occur.
- Developments in the Dutch healthcare system require more transparency regarding quality
and fi nancial sustainability of specialist medical care. This transparency will lead to a better
understanding of rationale of care, which will benefi t patients, health insurers and healthcare
providers. These developments call for comparability of treatments with regard to content,
composition, dosage, and fi nances.
Therefore, the time has come to include dose variables in the question of “what works for whom”,
and therefore to analyze dosage at the level of the individual patient related to accomplishing
their goals, and analyzing dosage related to effect from the perspective of different stakeholders
to optimize the cost-effectiveness of multidisciplinary PRPs.
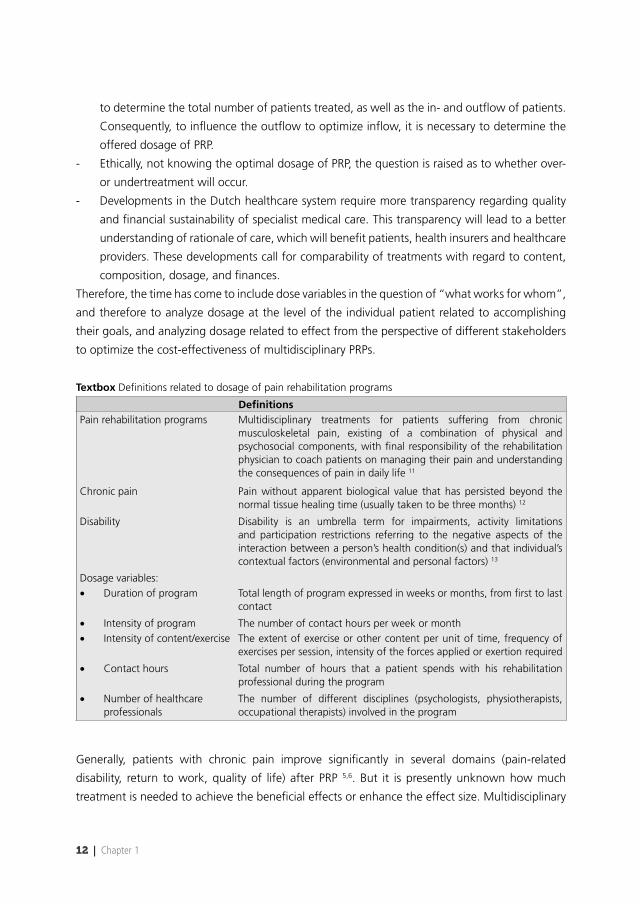
Textbox Defi nitions related to dosage of pain rehabilitation programs
Defi nitionsPain rehabilitation programs Multidisciplinary treatments for patients suffering from chronic
musculoskeletal pain, existing of a combination of physical and psychosocial components, with fi nal responsibility of the rehabilitation physician to coach patients on managing their pain and understanding the consequences of pain in daily life 11
Chronic pain Pain without apparent biological value that has persisted beyond the normal tissue healing time (usually taken to be three months) 12
Disability Disability is an umbrella term for impairments, activity limitations and participation restrictions referring to the negative aspects of the interaction between a person’s health condition(s) and that individual’s contextual factors (environmental and personal factors) 13
Dosage variables:• Duration of program Total length of program expressed in weeks or months, from fi rst to last
contact
• Intensity of program The number of contact hours per week or month• Intensity of content/exercise The extent of exercise or other content per unit of time, frequency of
exercises per session, intensity of the forces applied or exertion required
• Contact hours Total number of hours that a patient spends with his rehabilitation professional during the program
• Number of healthcare professionals
The number of different disciplines (psychologists, physiotherapists, occupational therapists) involved in the program
Generally, patients with chronic pain improve signifi cantly in several domains (pain-related
disability, return to work, quality of life) after PRP 5,6. But it is presently unknown how much
treatment is needed to achieve the benefi cial effects or enhance the effect size. Multidisciplinary
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 13
1PRPs are based on the bio-psycho-social model that aims to reduce pain-related disability. The
cognitive-behavioral components assume that patients change their pain management skills
during PRP. These behavioral changes support the reduction of pain-related disability without the
aim of pain reduction. Consequently, aiming for behavioral changes during PRP, the dosage of
PRP could be based on the dosage of other therapies that use cognitive-behavioral therapy for
chronic pain. Unfortunately, the optimum dosage of those cognitive-behavioral interventions for
patients with chronic pain is also unknown 14. In conclusion, there is currently a gap in knowledge
regarding dosage of PRP based on cognitive-behavioral principles.
In order to fi nd the optimum dosage of PRP, underlying constructs of dosage of PRP should be
explored. When unraveling this topic in pain rehabilitation research, multiple questions were
raised. Some questions are as follows:
• What is the rationale for the dosage of the present programs in today’s daily practice in
Dutch PRP?
• Is therapy needed each week or is a time-out also possible?
• Which healthcare professionals should be involved in PRP and what is their added value in
PRP?
• Which patients require higher dosage of PRP and for whom would a lower dosage be
suffi cient?
• What are reasons to stop PRP and how do these reasons relate to the desired improvements?
• How does reduction of disability occur during weeks of PRP?
• Can the dosage of PRP be reduced without a reduction in the effects?
• Should there be different dosages for patients that exhibit differences in case complexity?
Aim and research questions
The overall aim of the thesis is to acquire insight into the effects of dosage of multidisciplinary
pain rehabilitation programs for patients with chronic pain.
This overall aim is specifi ed in the following research questions:
• What is the reported dosage of treatment for patients with chronic low back pain and what
is the infl uence of dose variables on the outcome of PRPs for patients with chronic low back
pain? (Chapter 2).
• Which course does disability reduction during PRP follow and which factors infl uence this
course over time? (Chapter 3).
• Is a shorter form of PRP non-inferior to the PRP in care as usual? Do effects differ signifi cantly?
(Chapter 4).
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
14 | Chapter 1
• What are the differences and similarities in the experiences and perspectives of patients who
underwent PRP and rehabilitation professionals working in PRPs regarding dosage of PRP
between three centers in the Netherlands? (Chapter 5).
• Which factors determine case complexity of patients with CMP that are eligible for PRP?
(Chapter 6).
Outline of thesis
Since, up to now, dosage has been a neglected topic in pain research, different research methods
and perspectives have been applied in this thesis.
The systematic review and meta-analysis described in Chapter 2 aimed to analyze the infl uence
of dose variables on the outcome of PRPs. There were no studies found that primarily analyzed
the relationship between dose and effects of PRP. Therefore, this review focused on randomized
controlled trials (RCTs) aimed at assessing effectiveness of PRPs that reported dose variables of
the studied programs. The reported dose variables were used to analyze the infl uence of dose
variables on the effects.
The course of disability reduction during PRP and factors infl uencing this course were analyzed
in Chapter 3. The majority of studies analyzed pre- and post-outcomes of disability reduction.
However to acquire insight into the dosage of PRP, it is a prerequisite to analyze the course of the
primary outcome during PRP.
Chapter 4 describes the fi rst randomized controlled trial in PRP research that compared PRPs with
similar content but different dosages. The control arm was PRP performed in care as usual dosage
(8, 12, 16 or 20 weeks) and the experimental arm was PRP performed at a duration four weeks
shorter than the care as usual.
To gain in-depth information on the experiences and perspectives of patients and rehabilitation
professionals regarding dosage of PRP, a qualitative study was performed, which is described in
Chapter 5. Interviews with patients and focus group interviews with rehabilitation professionals
were conducted in three centers in the Netherlands offering PRP with differences in dosage of
PRP, while patient characteristics were similar.
From clinical practice, a relationship was hypothesized between case complexity and the required
dosage of PRP. However, little research is available regarding the interpretation of case complexity
within multidisciplinary PRP. Therefore, it was not possible to test this relationship. In Chapter

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 15
16, the operationalization of case complexity was studied using a Delphi technique among
rehabilitation professionals working in pain rehabilitation centers throughout the Netherlands.
In Chapter 7, the general discussion, all fi ndings from the previous chapters are integrated
and discussed. Implications for clinical practice and recommendations for future research are
presented.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
16 | Chapter 1
References
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287-333.
2. Lambeek LC, van Tulder MW, Swinkels IC, Koppes LL, Anema JR, van Mechelen W. The trend in total cost of back pain in the netherlands in the period 2002 to 2007. Spine (Phila Pa 1976). 2011;36(13):1050-1058.
3. Flor H, Fydrich T, Turk DC. Effi cacy of multidisciplinary pain treatment centers: A meta-analytic review. Pain. 1992;49(2):221-230.
4. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: A systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
5. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. 2015;350:h444.
6. van Geen JW, Edelaar MJ, Janssen M, van Eijk JT. The long-term effect of multidisciplinary back training: A systematic review. Spine (Phila Pa 1976). 2007;32(2):249-255.
7. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. BMJ. 2001;322(7301):1511-1516.
8. Smeets RJ, Vlaeyen JW, Hidding A, et al. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? fi rst direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7:5.
9. Dufour N, Thamsborg G, Oefeldt A, Lundsgaard C, Stender S. Treatment of chronic low back pain: A randomized, clinical trial comparing group-based multidisciplinary biopsychosocial rehabilitation and intensive individual therapist-assisted back muscle strengthening exercises. Spine (Phila Pa 1976). 2010;35(5):469-476.
10. Kainz B, Gulich M, Engel EM, Jackel WH. Comparison of three outpatient therapy forms for treatment of chronic low back pain-- fi ndings of a multicentre, cluster randomized study. Rehabilitation (Stuttg). 2006;45(2):65-77.
11. Köke A, Brouwers M, Heuts P, et al. Consensus rapport pijnrevalidatie Nederland. 2005.
12. International Association for the Study of Pain. Task Force on Taxonomy. Classifi cation of chronic pain: Descriptions of chronic pain syndromes and defi nitions of pain terms. 2nd ed. Seattle: IASP Press; 1994.
13. World HO, Organisation Mondiale de lS, World HO. How to use the ICF: A practical manual for using the international classifi cation of functioning, disability and health (ICF): Exposure draft for comment. Genf: WHO; 2013.
14. Ehde DM, Dillworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: Effi cacy, innovations, and directions for research. Am Psychol. 2014;69(2):153-166.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 17
1

FrFrFrannankakaka PP.C.CC.. WaWaW tetet rsrsrschchchoooooot,t,t, PPPieeeteteter r U.U.U. DDDijijijkskskstrtrraaa PhPhP D,D,D, NNNieieek kk HoHoHolll akakak MMMScScSc, HaHaHaititi zezeze JJJ.. dedede VVVrirr esess PPPhDhDhD, Jaannn H.H.H.B.BB. GGGeeeee rtrtr zezez nn MDMDD,, PhPhPhD,D,D, MMMiccchihhielele FFF. ReReReneneemamaannn PhPhP D.D
PaPaP ininin, 20202014141 ,1,11555555 (((1)1)1):: 1717179-9--898989..

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
20 | Chapter 2
Abstract
We sought to systematically analyze the infl uence of dose of Pain Rehabilitation Programs (PRPs)
for patients with chronic low back Pain (CLBP) on disability, work participation and quality of life
(QoL). Literature searches were performed in PUBMED, Cochrane library, Cinahl and EMBASE up
to October 2012, using MeSH terms, other relevant terms and free-text words.
Randomized controlled trials in English, Dutch and German, analyzing the effect of PRPs, were
included. One of the analyzed interventions had to be a PRP. Outcomes should be reported
regarding disability, work participation or QoL. To analyze dose, the number of contact hours
should be reported. Two reviewers independently selected titles, abstract and full text articles on
the basis of inclusion and exclusion criteria. Data were extracted and risk of bias was assessed. Effect
sizes (ES) were calculated for each intervention, and infl uence of dose variables was analyzed by a
mixed model analysis. Eighteen studies were identifi ed, reporting a wide variety of dose variables
and contents of PRPs. Analyses showed that evaluation moment, number of disciplines, type of
intervention, duration of intervention in weeks, percentage of women, and age, infl uenced the
outcomes of PRPs. The independent effect of dose variables could not be distinguished from
content because these variables were strongly associated. Because dose variables were never
studied separately or reported independently, we were not able to disentangle the relationship
between dose, content, and effects of PRPs on disability, work participation and QoL.
Keywords
Chronic low back pain, dose, effectiveness, pain rehabilitation programs
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 21
2
Introduction
Multidisciplinary pain rehabilitation programs (PRPs) are effective in improving daily functioning
of patients with chronic low back pain (CLBP) 1-3. Most studies investigating the effects of PRPs
focused on the relationship between therapy content and effect. Guidelines for managing CLBP
are based on evidence obtained from these studies 4,5. However, this evidence might be biased.
In a literature search, we could not identify any study analyzing the relationship between dose
and effect as a primary objective. Two systematic reviews 2,3 were identifi ed that analyzed dose
and effect as a secondary objective. These reviews presented confl icting conclusions on dose
effects.
In a review of Guzman et al 2, 10 randomized controlled trials (RCTs) were included reporting
on 12 PRPs. PRPs were divided into 2 categories: daily intensive programs with more than 100 h
of therapy, and once- or twice-weekly programs with less than 30 h of therapy. Based the basis
of that distinction, it appeared that multidisciplinary PRPs of more than 100 h were superior to
monodisciplinary treatment, and PRPs of less than 30 h were not. The authors concluded that
intensive multidisciplinary PRPs are superior to less intensive multidisciplinary PRPs 2. These results
have been used in guidelines and clinical practice 4,6. However, it may be debated whether the
conclusion regarding dose is valid to support its clinical implications. First, there is an absence
of knowledge about PRPs with doses between 30 to 100 h. Second, no distinction was made
within intensive and less intensive PRPs, although there was a wide variety within the groups. Less
intensive PRPs ranged from 17.5 to 30 h, while intensive PRP ranged from 100 to 280 h. Third,
the review 2 was designed to assess the effect of different PRPs on clinically relevant outcomes.
All PRPs differed not only in dose, but also in content, setting and number of disciplines involved,
which may have confounded the dose aspect of the conclusion. Additionally, the authors
discussed whether the improvements gained with intensive PRP are worth the expense.
The review of Van Geen et al. 3 also had some limitations. It assessed the long-term effect of
PRPs with different contents and doses. Ten studies were included, and a distinction was made
between 30 h of training a week or more (intensive therapy) vs less than 30 h of training a week
(low-intensive therapy). Both the intensive and low-intensive PRPs showed positive effects. The
conclusion in that review was that the dose of the intervention had no substantial infl uence on
the effectiveness of the intervention.
In summary, while many studies provide evidence for effectiveness of multidisciplinary PRP, dose
of multidisciplinary PRP to achieve these effects remains unclear. The objective of the current
study was to analyze the infl uence of dose variables on the outcome of PRPs for patients with
CLBP.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
22 | Chapter 2
Methods
Publications were retrieved by computer-aided search on PUBMED, the Cochrane library, Cinahl,
and EMBASE up to October 2012. A specifi c search was developed using MeSH terms and other
relevant terms for each database. The PubMed search is described in the Supplement. Refworks
was used to store the results of the searches and to remove duplicates.
Selection of studies
Selection criteria were applied independently by two reviewers (FW and NH). The retrieved studies
were fi rst selected by title and abstract. Doubtful cases were discussed by the reviewers and
included or excluded for full text analysis by consensus. Full-text reports of studies eligible for
inclusion were analyzed. Disagreements were resolved by consensus or when necessary by a third
reviewer (HdV).
Studies were selected on the basis of the following inclusion criteria: (1) RCTs written in English,
Dutch or German; (2) the objective was to assess effectiveness of a multidisciplinary PRP for patients
with CLBP; PRP was defi ned as a rehabilitation program on the basis of the biopsychosocial model 7 with 3 or more disciplines providing the program (with or without a medical doctor); (3) total
number of contact hours of PRP was described; (4) participants were between 18 and 65 years
with disabling nonspecifi c CLBP for at least 3 months; (5) outcome variables were described in
the domain of disability, work participation or quality of life (QoL). Studies were excluded if: (1)
the multidisciplinary PRP was given in primary care; (2) the objective was to assess effectiveness
of only a biomedical intervention; (3) the study included participants who were diagnosed with
specifi c disorders or severe comorbidities interfering with PRP, such as heart failure, rheumatoid
arthritis, or psychiatric disorders; and (4) only total duration of PRP was reported.
Data management
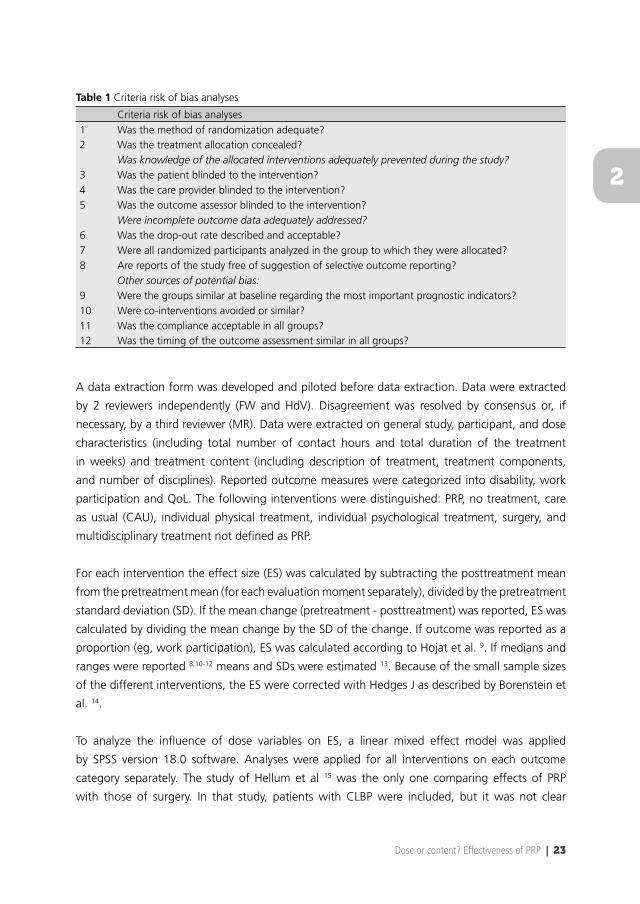
Risk of bias of included studies was assessed according to the Cochrane Back Review Group 8
by 2 reviewers independently (FW and HdV). The criteria are presented in Table 1. Each criterion
was scored as positive (Y), negative (N) or unclear (U). The total score was computed by counting
the number of criteria scored as positive. Studies with a score of 6 or higher were defi ned as
low risk of bias; a score lower than 6 was defi ned as high risk of bias. In case of unclear scores,
corresponding authors of the studies were contacted by e-mail.
Performance bias was analysed with different items of blinding. The item regarding blinding of
care providers for intervention is frequently impossible in nondrug trials. To analyze the infl uence
of lack of blinding of care providers on the judgment of methodological quality, we performed a
sensitivity analyses by excluding item 4 of the risk of bias analyses.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 23
2
Table 1 Criteria risk of bias analyses
Criteria risk of bias analyses1 Was the method of randomization adequate?2 Was the treatment allocation concealed?
Was knowledge of the allocated interventions adequately prevented during the study?3 Was the patient blinded to the intervention?4 Was the care provider blinded to the intervention?5 Was the outcome assessor blinded to the intervention?
Were incomplete outcome data adequately addressed?6 Was the drop-out rate described and acceptable?7 Were all randomized participants analyzed in the group to which they were allocated?8 Are reports of the study free of suggestion of selective outcome reporting?
Other sources of potential bias:9 Were the groups similar at baseline regarding the most important prognostic indicators?10 Were co-interventions avoided or similar?11 Was the compliance acceptable in all groups?12 Was the timing of the outcome assessment similar in all groups?
A data extraction form was developed and piloted before data extraction. Data were extracted
by 2 reviewers independently (FW and HdV). Disagreement was resolved by consensus or, if
necessary, by a third reviewer (MR). Data were extracted on general study, participant, and dose
characteristics (including total number of contact hours and total duration of the treatment
in weeks) and treatment content (including description of treatment, treatment components,
and number of disciplines). Reported outcome measures were categorized into disability, work
participation and QoL. The following interventions were distinguished: PRP, no treatment, care
as usual (CAU), individual physical treatment, individual psychological treatment, surgery, and
multidisciplinary treatment not defi ned as PRP.
For each intervention the effect size (ES) was calculated by subtracting the posttreatment mean
from the pretreatment mean (for each evaluation moment separately), divided by the pretreatment
standard deviation (SD). If the mean change (pretreatment - posttreatment) was reported, ES was
calculated by dividing the mean change by the SD of the change. If outcome was reported as a
proportion (eg, work participation), ES was calculated according to Hojat et al. 9. If medians and
ranges were reported 8,10-12 means and SDs were estimated 13. Because of the small sample sizes
of the different interventions, the ES were corrected with Hedges J as described by Borenstein et
al. 14.
To analyze the infl uence of dose variables on ES, a linear mixed effect model was applied
by SPSS version 18.0 software. Analyses were applied for all interventions on each outcome
category separately. The study of Hellum et al 15 was the only one comparing effects of PRP
with those of surgery. In that study, patients with CLBP were included, but it was not clear
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
24 | Chapter 2
whether they had a specifi c or nonspecifi c diagnosis. Because of the unique character of that
study, the analyses were done twice: with and without this study for outcome categories disability
and QoL. ES per intervention was the response variable. Predictor variables were PRP (yes/no),
number of disciplines involved in the program, number of contact hours, treatment duration in
weeks, type of intervention (no treatment, CAU, surgery, individual physical therapy [exercise],
psychological treatment, other multidisciplinary treatment, PRP), evaluation moment (in months),
age, percentage of women and risk of bias (high/low). These variables were entered one by one
into the model. The variables remained in the model if the regression coeffi cient was signifi cant
(<0.05) or the model fi t increased signifi cantly (-2log-likelihood criterion). Random intercepts
were modeled because of a better fi t of the model. Patient characteristics such as duration of pain
and work status were reported insuffi ciently to be included in the statistical model.
Because augmentation of the content of the program can lead to deployment of more disciplines
and more contact hours or total treatment duration, we assumed that content and dose variables
could be correlated. Spearman correlations were used to analyze this assumption.
Results
Results of the search
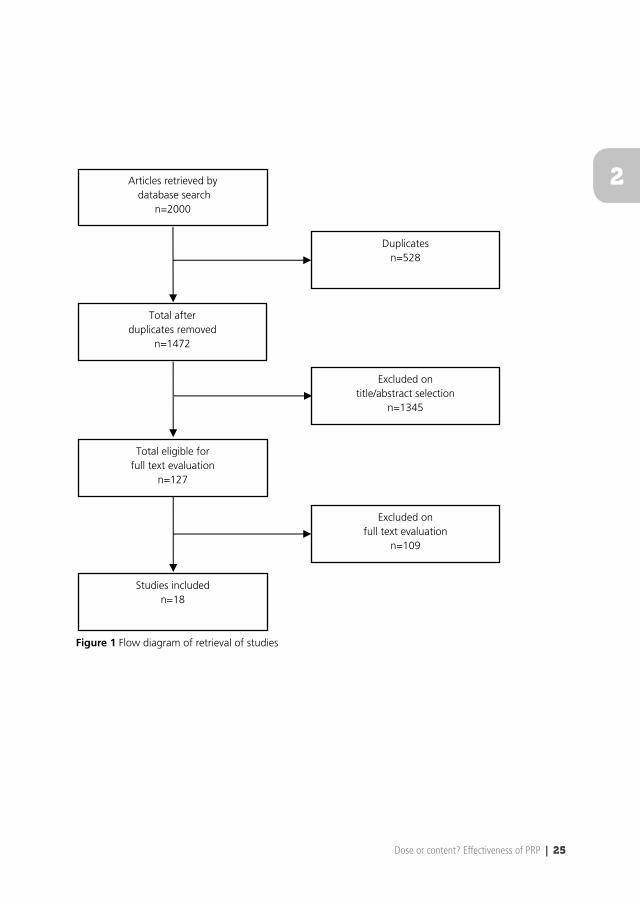
A total of 2000 records was obtained from the electronic search, and 528 duplicates were
removed. In total, 1472 articles were assessed on title and abstract, and 127 articles were eligible
for full-text assessment. Grounds for exclusion after full-text assessment were mostly because
studies were not randomized, did not fi t the defi nition of multidisciplinary PRP, or contact hours
were not described. Follow-up studies of included RCTs were not regarded as a separate study,
but follow-up data were included in the analysis. Eighteen unique studies were included for risk
of bias assessment. (Figure 1)
Assessment of risk of bias
Agreement between reviewers expressed in Cohen’s Kappa was 0.65. All disagreements between
reviewers were solved by consensus. After fi rst assessment, 12 studies were categorized as
low risk of bias (score > 6) 16. However, many items were answered with “unclear” because
information was not clearly reported in the articles. Two articles had no unclear answers 17,18. The
e-mail address of 1 author 19 could not be retrieved. The authors of 14 articles were contacted for
clarifi cation, and answers were received from 11 of the 14 authors. After clarifi cation with the
author, 16 studies 8,10-12,15,17,18,20-28 had a score of 6 or higher (low risk of bias) and 2 studies 19,29
had a lower score and therefore a high risk of bias (Table 2).
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 25
2Articles retrieved by database search
n=2000
Total after duplicates removed
n=1472
Total eligible for full text evaluation
n=127
Studies included n=18
Duplicates n=528
Excluded on title/abstract selection
n=1345
Excluded on full text evaluation
n=109
Figure 1 Flow diagram of retrieval of studies
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
26 | Chapter 2
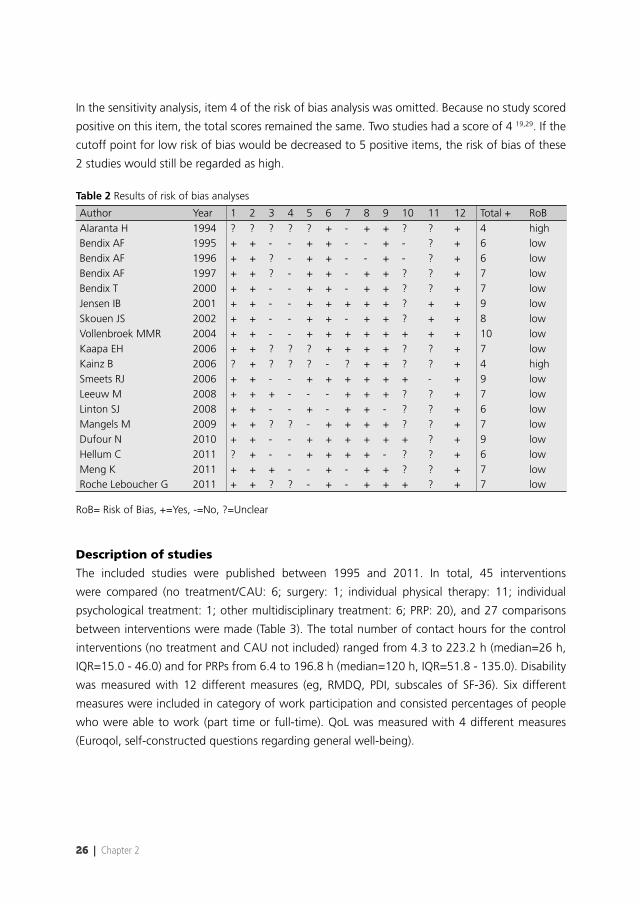
In the sensitivity analysis, item 4 of the risk of bias analysis was omitted. Because no study scored
positive on this item, the total scores remained the same. Two studies had a score of 4 19,29. If the
cutoff point for low risk of bias would be decreased to 5 positive items, the risk of bias of these
2 studies would still be regarded as high.
Table 2 Results of risk of bias analyses
Author Year 1 2 3 4 5 6 7 8 9 10 11 12 Total + RoBAlaranta H 1994 ? ? ? ? ? + - + + ? ? + 4 highBendix AF 1995 + + - - + + - - + - ? + 6 lowBendix AF 1996 + + ? - + + - - + - ? + 6 lowBendix AF 1997 + + ? - + + - + + ? ? + 7 lowBendix T 2000 + + - - + + - + + ? ? + 7 lowJensen IB 2001 + + - - + + + + + ? + + 9 lowSkouen JS 2002 + + - - + + - + + ? + + 8 lowVollenbroek MMR 2004 + + - - + + + + + + + + 10 lowKaapa EH 2006 + + ? ? ? + + + + ? ? + 7 lowKainz B 2006 ? + ? ? ? - ? + + ? ? + 4 highSmeets RJ 2006 + + - - + + + + + + - + 9 lowLeeuw M 2008 + + + - - - + + + ? ? + 7 lowLinton SJ 2008 + + - - + - + + - ? ? + 6 lowMangels M 2009 + + ? ? - + + + + ? ? + 7 lowDufour N 2010 + + - - + + + + + + ? + 9 lowHellum C 2011 ? + - - + + + + - ? ? + 6 lowMeng K 2011 + + + - - + - + + ? ? + 7 lowRoche Leboucher G 2011 + + ? ? - + - + + + ? + 7 low
RoB= Risk of Bias, +=Yes, -=No, ?=Unclear
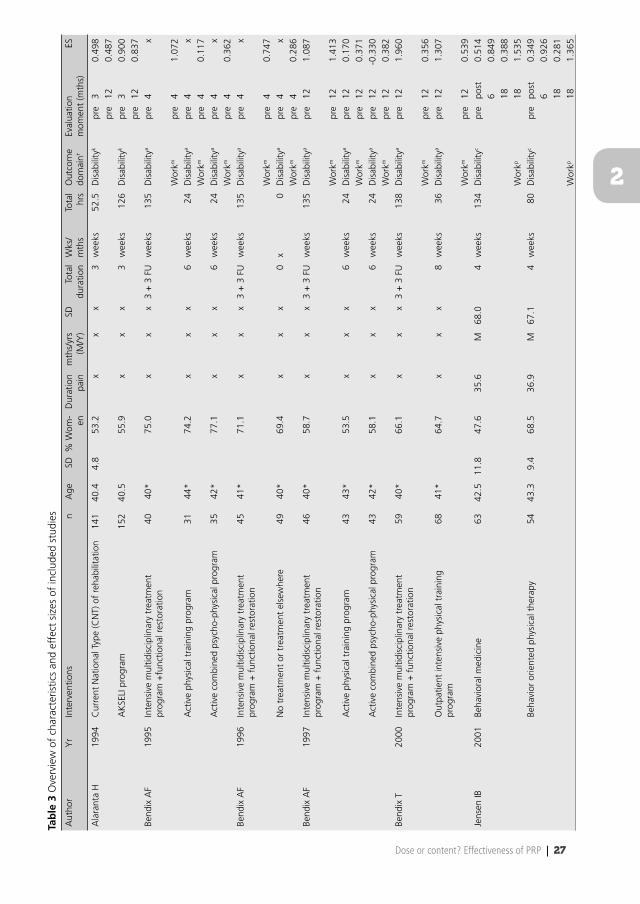
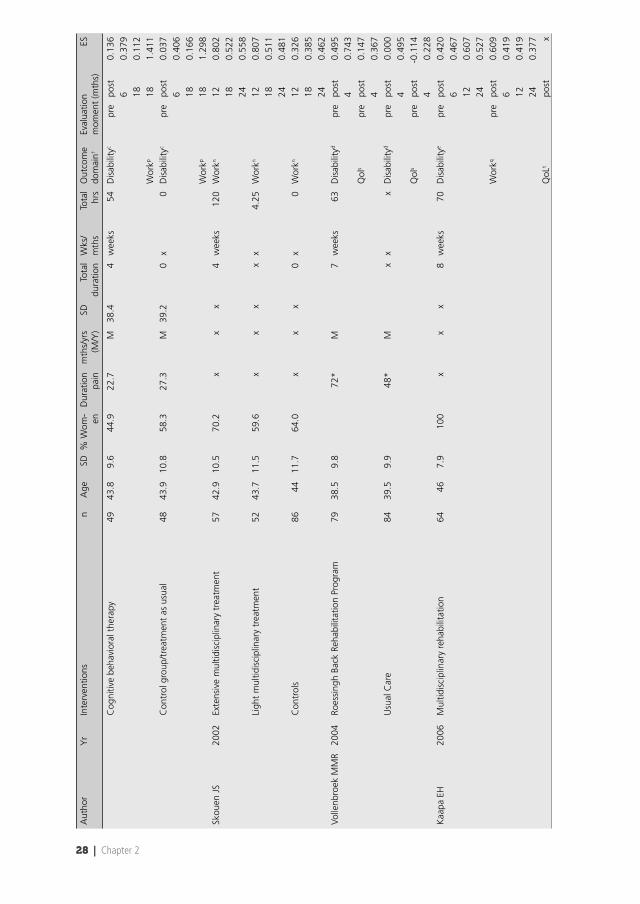
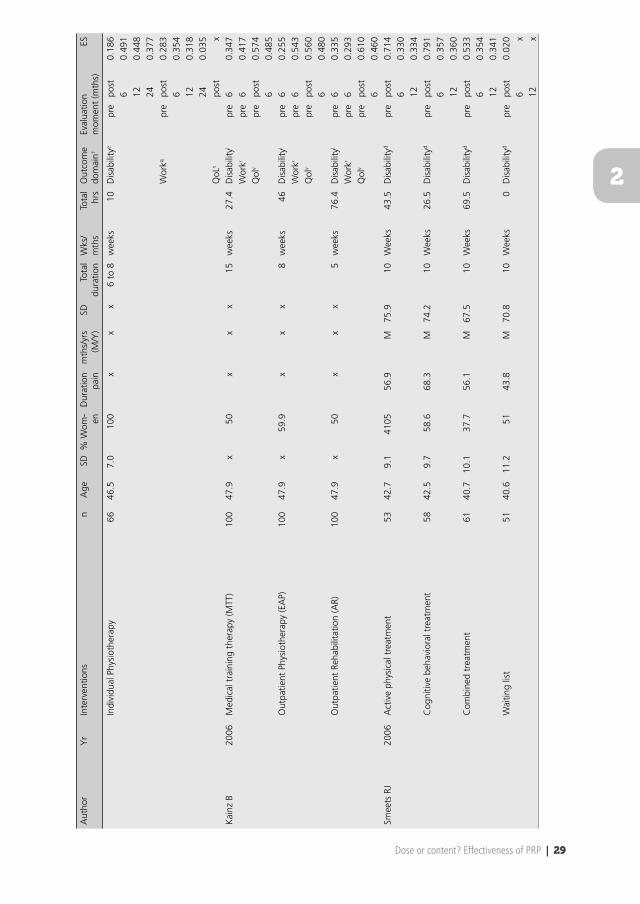
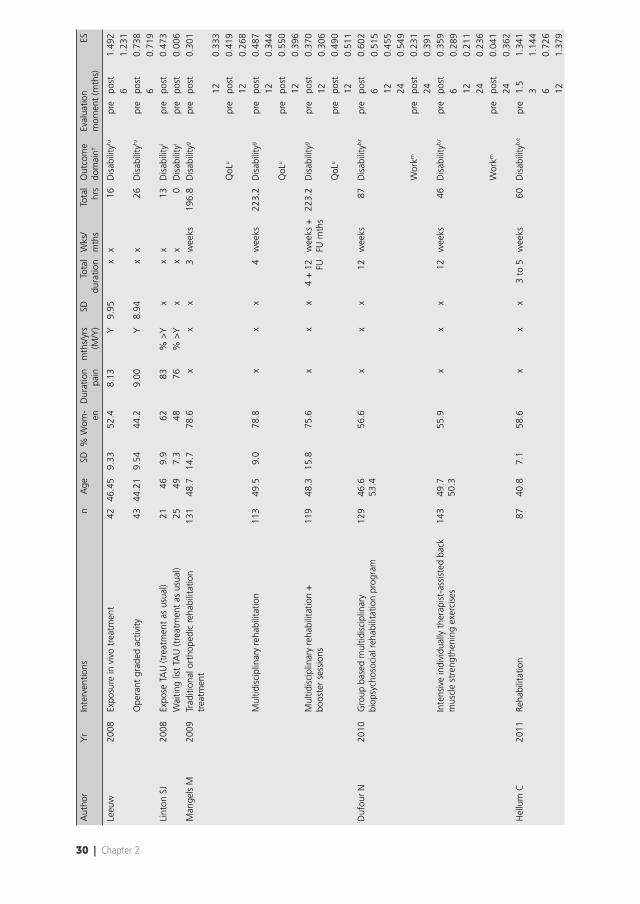
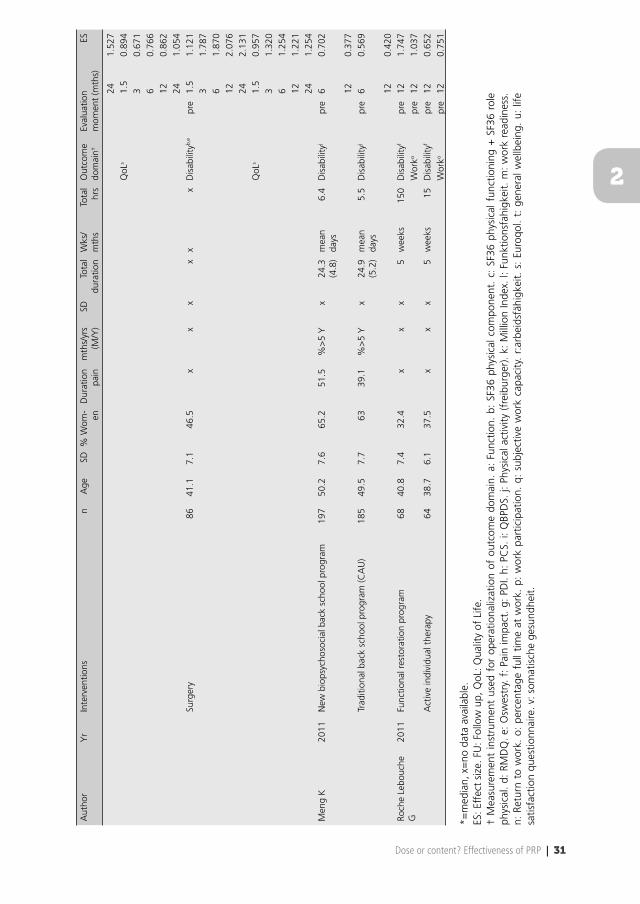
Description of studies
The included studies were published between 1995 and 2011. In total, 45 interventions
were compared (no treatment/CAU: 6; surgery: 1; individual physical therapy: 11; individual
psychological treatment: 1; other multidisciplinary treatment: 6; PRP: 20), and 27 comparisons
between interventions were made (Table 3). The total number of contact hours for the control
interventions (no treatment and CAU not included) ranged from 4.3 to 223.2 h (median=26 h,
IQR=15.0 - 46.0) and for PRPs from 6.4 to 196.8 h (median=120 h, IQR=51.8 - 135.0). Disability
was measured with 12 different measures (eg, RMDQ, PDI, subscales of SF-36). Six different
measures were included in category of work participation and consisted percentages of people
who were able to work (part time or full-time). QoL was measured with 4 different measures
(Euroqol, self-constructed questions regarding general well-being).
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 27
2
Tab
le 3
Ove
rvie
w o
f ch
arac
teris
tics
and
effe
ct s
izes
of
incl
uded
stu
dies
Aut
hor
Yr
Inte
rven
tions
nA
geSD
% W
om-
enD
urat
ion
pain
mth
s/yr
s(M
/Y)
SDTo
tal
dura
tion
Wks
/m
ths
Tota
l hr
sO
utco
me
dom
ain†
Eval
uatio
n m
omen
t (m
ths)
ES
Ala
rant
a H
1994
Cur
rent
Nat
iona
l Typ
e (C
NT)
of
reha
bilit
atio
n14
140
.44.
853
.2x
xx
3w
eeks
52.5
Dis
abili
tyk
pre
30.
498
pre
120.
487
AK
SELI
pro
gram
152
40.5
55.9
xx
x3
wee
ks12
6D
isab
ility
kpr
e3
0.90
0pr
e12
0.83
7Be
ndix
AF
1995
Inte
nsiv
e m
ultid
isci
plin
ary
trea
tmen
t pr
ogra
m +
func
tiona
l res
tora
tion
4040
*75
.0x
xx
3 +
3 F
Uw
eeks
135
Dis
abili
tya
pre
4x
Wor
kmpr
e4
1.07
2A
ctiv
e ph
ysic
al t
rain
ing
prog
ram
3144
*74
.2x
xx
6w
eeks
24D
isab
ility
apr
e4
xW
orkm
pre
40.
117
Act
ive
com
bine
d ps
ycho
-phy
sica
l pro
gram
3542
*77
.1x
xx
6w
eeks
24D
isab
ility
apr
e4
xW
orkm
pre
40.
362
Bend
ix A
F19
96In
tens
ive
mul
tidis
cipl
inar
y tr
eatm
ent
prog
ram
+ f
unct
iona
l res
tora
tion
4541
*71
.1x
xx
3 +
3 F
Uw
eeks
135
Dis
abili
tya
pre
4x
Wor
kmpr
e4
0.74
7N
o tr
eatm
ent
or t
reat
men
t el
sew
here
4940
*69
.4x
xx
0x
0D
isab
ility
apr
e4
xW
orkm
pre
40.
286
Bend
ix A
F19
97In
tens
ive
mul
tidis
cipl
inar
y tr
eatm
ent
prog
ram
+ f
unct
iona
l res
tora
tion
4640
*58
.7x
xx
3 +
3 F
Uw
eeks
135
Dis
abili
tya
pre
121.
087
Wor
kmpr
e12
1.41
3A
ctiv
e ph
ysic
al t
rain
ing
prog
ram
4343
*53
.5x
xx
6w
eeks
24D
isab
ility
apr
e12
0.17
0W
orkm
pre
120.
371
Act
ive
com
bine
d ps
ycho
-phy
sica
l pro
gram
4342
*58
.1x
xx
6w
eeks
24D
isab
ility
apr
e12
-0.3
30W
orkm
pre
120.
382
Bend
ix T
2000
Inte
nsiv
e m
ultid
isci
plin
ary
trea
tmen
t pr
ogra
m +
fun
ctio
nal r
esto
ratio
n59
40*
66.1
xx
x3
+ 3
FU
wee
ks13
8D
isab
ility
apr
e12
1.96
0
Wor
kmpr
e12
0.35
6O
utpa
tient
inte
nsiv
e ph
ysic
al t
rain
ing
prog
ram
6841
*64
.7x
xx
8w
eeks
36D
isab
ility
apr
e12
1.30
7
Wor
kmpr
e12
0.53
9Je
nsen
IB20
01Be
havi
oral
med
icin
e63
42.5
11.8
47.6
35.6
M68
.04
wee
ks13
4D
isab
ility
cpr
epo
st0.
514
60.
849
180.
388
Wor
kp18
1.53
5Be
havi
or o
rient
ed p
hysi
cal t
hera
py54
43.3
9.4
68.5
36.9
M67
.14
wee
ks80
Dis
abili
tyc
pre
post
0.34
96
0.92
618
0.28
1W
orkp
181.
365
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
28 | Chapter 2
Aut
hor
Yr
Inte
rven
tions
nA
geSD
% W
om-
enD
urat
ion
pain
mth
s/yr
s(M
/Y)
SDTo
tal
dura
tion
Wks
/m
ths
Tota
l hr
sO
utco
me
dom
ain†
Eval
uatio
n m
omen
t (m
ths)
ES
Cog
nitiv
e be
havi
oral
the
rapy
4943
.89.
644
.922
.7M
38.4
4w
eeks
54D
isab
ility
cpr
epo
st0.
136
60.
379
180.
112
Wor
kp18
1.41
1C
ontr
ol g
roup
/tre
atm
ent
as u
sual
4843
.910
.858
.327
.3M
39.2
0x
0D
isab
ility
cpr
epo
st0.
037
60.
406
180.
166
Wor
kp18
1.29
8Sk
ouen
JS
2002
Exte
nsiv
e m
ultid
isci
plin
ary
trea
tmen
t57
42.9
10.5
70.2
xx
x4
wee
ks12
0W
orkn
120.
802
180.
522
240.
558
Ligh
t m
ultid
isci
plin
ary
trea
tmen
t52
43.7
11.5
59.6
xx
xx
x4.
25W
orkn
120.
807
180.
511
240.
481
Con
trol
s86
4411
.764
.0x
xx
0x
0W
orkn
120.
326
180.
385
240.
462
Volle
nbro
ek M
MR
2004
Roes
sing
h Ba
ck R
ehab
ilita
tion
Prog
ram
7938
.59.
872
*M
7w
eeks
63D
isab
ility
dpr
epo
st0.
495
40.
743
Qol
spr
epo
st0.
147
40.
367
Usu
al C
are
8439
.59.
948
*M
xx
xD
isab
ility
dpr
epo
st0.
000
40.
495
Qol
spr
epo
st-0
.114
40.
228
Kaa
pa E
H20
06M
ultid
isci
plin
ary
reha
bilit
atio
n64
467.
910
0x
xx
8w
eeks
70D
isab
ility
epr
epo
st0.
420
60.
467
120.
607
240.
527
Wor
kqpr
epo
st0.
609
60.
419
120.
419
240.
377
QoL
tpo
stx
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 29
2
Aut
hor
Yr
Inte
rven
tions
nA
geSD
% W
om-
enD
urat
ion
pain
mth
s/yr
s(M
/Y)
SDTo
tal
dura
tion
Wks
/m
ths
Tota
l hr
sO
utco
me
dom
ain†
Eval
uatio
n m
omen
t (m
ths)
ES
Indi
vidu
al P
hysi
othe
rapy
6646
.57.
010
0x
xx
6 to
8w
eeks
10D
isab
ility
epr
epo
st0.
186
60.
491
120.
448
240.
377
Wor
kqpr
epo
st0.
283
60.
354
120.
318
240.
035
QoL
tpo
stx
Kai
nz B
2006
Med
ical
tra
inin
g th
erap
y (M
TT)
100
47.9
x50
xx
x15
wee
ks27
.4D
isab
ility
lpr
e6
0.34
7W
orkr
pre
60.
417
Qol
vpr
epo
st0.
574
60.
485
Out
patie
nt P
hysi
othe
rapy
(EA
P)10
047
.9x
59.9
xx
x8
wee
ks46
Dis
abili
tyl
pre
60.
255
Wor
krpr
e6
0.54
3Q
olv
pre
post
0.56
06
0.48
0O
utpa
tient
Reh
abili
tatio
n (A
R)10
047
.9x
50x
xx
5w
eeks
76.4
Dis
abili
tyl
pre
60.
335
Wor
krpr
e6
0.29
3Q
olv
pre
post
0.61
06
0.46
0Sm
eets
RJ
2006
Act
ive
phys
ical
tre
atm
ent
5342
.79.
141
0556
.9M
75.9
10W
eeks
43.5
Dis
abili
tyd
pre
post
0.71
46
0.33
012
0.33
4C
ogni
tive
beha
vior
al t
reat
men
t58
42.5
9.7
58.6
68.3
M74
.210
Wee
ks26
.5D
isab
ility
dpr
epo
st0.
791
60.
357
120.
360
Com
bine
d tr
eatm
ent
6140
.710
.137
.756
.1M
67.5
10W
eeks
69.5
Dis
abili
tyd
pre
post
0.53
36
0.35
412
0.34
1W
aitin
g lis
t51
40.6
11.2
5143
.8M
70.8
10W
eeks
0D
isab
ility
dpr
epo
st0.
020
6x
12x
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
30 | Chapter 2
Aut
hor
Yr
Inte
rven
tions
nA
geSD
% W
om-
enD
urat
ion
pain
mth
s/yr
s(M
/Y)
SDTo
tal
dura
tion
Wks
/m
ths
Tota
l hr
sO
utco
me
dom
ain†
Eval
uatio
n m
omen
t (m
ths)
ES
Leeu
w20
08Ex
posu
re in
viv
o tr
eatm
ent
4246
.45
9.33
52.4
8.13
Y9.
95x
x16
Dis
abili
tyh,
ipr
epo
st1.
492
61.
231
Ope
rant
gra
ded
activ
ity43
44.2
19.
5444
.29.
00Y
8.94
xx
26D
isab
ility
h,i
pre
post
0.73
86
0.71
9Li
nton
SJ
2008
Expo
se T
AU
(tre
atm
ent
as u
sual
)21
469.
962
83%
>Y
xx
x13
Dis
abili
tyi
pre
post
0.47
3W
aitin
g lis
t TA
U (t
reat
men
t as
usu
al)
2549
7.3
4876
% >
Yx
xx
0D
isab
ility
ipr
epo
st0.
006
Man
gels
M20
09Tr
aditi
onal
ort
hope
dic
reha
bilit
atio
n tr
eatm
ent
131
48.7
14.7
78.6
xx
x3
wee
ks19
6.8
Dis
abili
tyg
pre
post
0.30
1
120.
333
QoL
upr
epo
st0.
419
120.
268
Mul
tidis
cipl
inar
y re
habi
litat
ion
113
49.5
9.0
78.8
xx
x4
wee
ks22
3.2
Dis
abili
tyg
pre
post
0.48
712
0.34
4Q
oLu
pre
post
0.55
012
0.39
6M
ultid
isci
plin
ary
reha
bilit
atio
n +
bo
oste
r se
ssio
ns11
948
.315
.875
.6x
xx
4 +
12 FU
wee
ks +
FU
mth
s22
3.2
Dis
abili
tyg
pre
post
0.37
012
0.30
6Q
oLu
pre
post
0.49
012
0.51
1D
ufou
r N
2010
Gro
up b
ased
mul
tidis
cipl
inar
y bi
opsy
chos
ocia
l reh
abili
tatio
n pr
ogra
m12
946
.653
.456
.6x
xx
12w
eeks
87D
isab
ility
b,r
pre
post
0.60
26
0.51
512
0.45
524
0.54
9W
orkm
pre
post
0.23
124
0.39
1In
tens
ive
indi
vidu
ally
the
rapi
st-a
ssis
ted
back
m
uscl
e st
reng
then
ing
exer
cise
s14
349
.750
.355
.9x
xx
12w
eeks
46D
isab
ility
b,r
pre
post
0.35
96
0.28
912
0.21
124
0.23
6W
orkm
pre
post
0.04
124
0.36
2H
ellu
m C
2011
Reha
bilit
atio
n87
40.8
7.1
58.6
xx
x3
to 5
wee
ks60
Dis
abili
tyb,
epr
e1.
51.
341
31.
144
60.
726
121.
379
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 31
2
Aut
hor
Yr
Inte
rven
tions
nA
geSD
% W
om-
enD
urat
ion
pain
mth
s/yr
s(M
/Y)
SDTo
tal
dura
tion
Wks
/m
ths
Tota
l hr
sO
utco
me
dom
ain†
Eval
uatio
n m
omen
t (m
ths)
ES
241.
527
QoL
s1.
50.
894
30.
671
60.
766
120.
862
241.
054
Surg
ery
8641
.17.
146
.5x
xx
xx
xD
isab
ility
b,e
pre
1.5
1.12
13
1.78
76
1.87
012
2.07
624
2.13
1Q
oLs
1.5
0.95
73
1.32
06
1.25
412
1.22
124
1.25
4M
eng
K20
11N
ew b
iops
ycho
soci
al b
ack
scho
ol p
rogr
am19
750
.27.
665
.251
.5%
>5
Yx
24.3
(4
.8)
mea
n da
ys6.
4D
isab
ility
jpr
e6
0.70
2
120.
377
Trad
ition
al b
ack
scho
ol p
rogr
am (C
AU
)18
549
.57.
763
39.1
%>
5 Y
x24
.9
(5.2
)m
ean
days
5.5
Dis
abili
tyj
pre
60.
569
120.
420
Roch
e Le
bouc
he
G20
11Fu
nctio
nal r
esto
ratio
n pr
ogra
m68
40.8
7.4
32.4
xx
x5
wee
ks15
0D
isab
ility
fpr
e12
1.74
7W
orko
pre
121.
037
Act
ive
indi
vidu
al t
hera
py64
38.7
6.1
37.5
xx
x5
wee
ks15
Dis
abili
tyf
pre
120.
652
Wor
kopr
e12
0.75
1
*=m
edia
n, x
=no
dat
a av
aila
ble.
ES: E
ffec
t si
ze. F
U: F
ollo
w u
p, Q
oL: Q
ualit
y of
Life
.†
Mea
sure
men
t in
stru
men
t us
ed f
or o
pera
tiona
lizat
ion
of o
utco
me
dom
ain.
a:
Func
tion.
b:
SF36
phy
sica
l com
pone
nt.
c: S
F36
phys
ical
fun
ctio
ning
+ S
F36
role
ph
ysic
al.
d: R
MD
Q.
e: O
swes
try.
f:
Pain
impa
ct.
g: P
DI.
h: P
CS.
i: Q
BPD
S. j:
Phy
sica
l act
ivity
(fr
eibu
rger
). k:
Mill
ion
Inde
x. l:
Fun
ktio
nsfa
higk
eit.
m:
wor
k re
adin
ess.
n:
Ret
urn
to w
ork.
o:
perc
enta
ge f
ull t
ime
at w
ork.
p:
wor
k pa
rtic
ipat
ion.
q:
subj
ectiv
e w
ork
capa
city
. r:
arbe
idsf
ähig
keit.
s:
Euro
qol.
t: g
ener
al w
ellb
eing
. u:
life
sa
tisfa
ctio
n qu
estio
nnai
re. v
: som
atis
che
gesu
ndhe
it.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
32 | Chapter 2
ES for disability ranged from -0.33 to 2.13 (median 0.36, IQR 0.23 - 0.67) for control interventions
and from 0.31 to 1.96 (median 0.54, IQR 0.43 - 1.04) for PRPs. ES for work participation ranged
from 0.04 to 1.41 (median 0.38, IQR 0.32 - 0.54) for controls and for PRPs from 0.23 to 1.54
(median 0.54, IQR 0.38 - 0.98). QoL ranged from -0.11 to 1.32 (median 0.56, IQR 0.34 - 1.24)
for controls and from 0.15 to 1.05 (median 0.55, IQR 0.43 - 0.81) for PRPs (Table 4). In one study 15, the control intervention (surgery) was superior to PRP. That study was also responsible for the
highest ES for the control intervention for disability (2.13) and QoL (1.25).
Table 4 Ranges of ES per outcome category for PRPs and control interventions
Outcome PRP Controls PRP ControlsIncluding study of Hellum et al. Excluding study of Hellum et al.
Disability 0.306 to 1.960 -0.330 to 2.131 0.306 to 1.960 -0.330 to 1.307Work Participation 0.231 to 1.535 0.035 to 1.411 0.231 to 1.535 0.035 to 1.411Quality of life 0.147 to 1.054 -0.114 to 1.320 0.147 to 0.610 -0.114 to 0.574
ES: Effect size. PRP: Pain Rehabilitation Program.
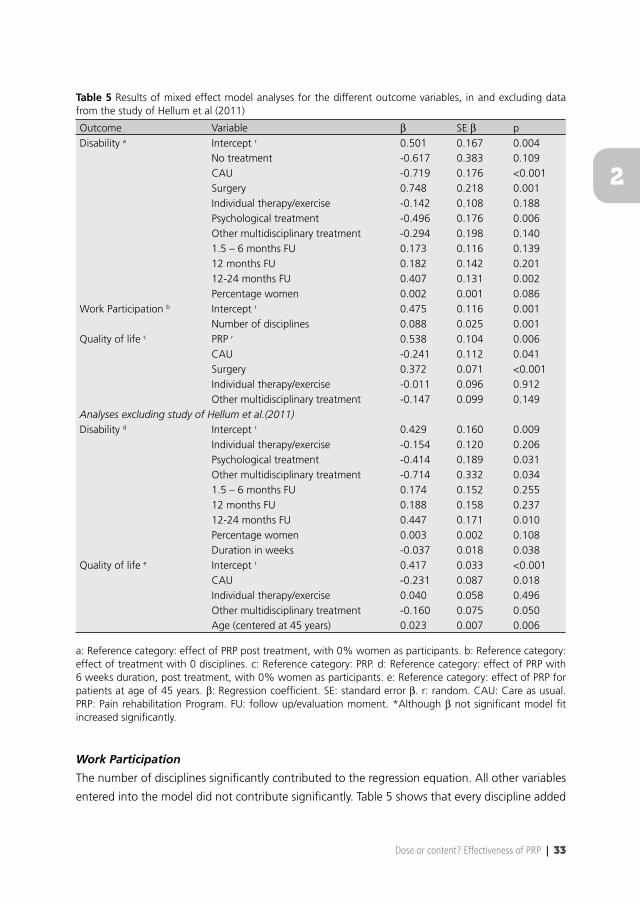
Mixed effect modeling
Disability
Type of intervention, evaluation moment, and percentage of women signifi cantly contributed to
the regression equation. In this analysis, the reference category was effect of PRP immediately
after treatment, with 0% women as participants. The negative coeffi cients indicate that control
interventions had a smaller ES than PRP (β=0.501), except surgery, which had a signifi cantly
larger ES (β=0.748), indicating that the ES of surgery was 0.501 + 0.748= 1.249. The coeffi cient
of 12 to 24 months for evaluation moment indicates that the ES is 0.407 points larger at 12 to
24 months than immediately after intervention (reference category) (Table 5). The coeffi cient
of 0.002 for percentage of women indicates that for every 1% women extra as participants,
the ES increases with 0.002. Performing the analyses without the study of Hellum et al 15, the
reference category was effect of PRP with 6 weeks’ duration after treatment, with 0% women as
participants. A signifi cant contribution of type of intervention, evaluation moment, percentage
of women, and duration in weeks was found (Table 5). All control interventions had a smaller
ES than PRP (β=0.429) ranging from -0.714 to -0.154. Evaluation moment between 12 and 24
months after the study had a regression coeffi cient of 0.447, indicating that the ES at 12 to 24
months is 0.447 larger than immediately after treatment. The coeffi cient of 0.003 for percentage
of women indicates that for every 1% women extra as participants, the ES increases by 0.003.
The coeffi cient of -0.037 for duration in weeks indicates that for each additional week above 6
weeks, the ES decreases with 0.037.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 33
2
Table 5 Results of mixed effect model analyses for the different outcome variables, in and excluding data from the study of Hellum et al (2011)
Outcome Variable β SE β pDisability a Intercept r 0.501 0.167 0.004
No treatment -0.617 0.383 0.109CAU -0.719 0.176 <0.001Surgery 0.748 0.218 0.001Individual therapy/exercise -0.142 0.108 0.188Psychological treatment -0.496 0.176 0.006Other multidisciplinary treatment -0.294 0.198 0.1401.5 – 6 months FU 0.173 0.116 0.13912 months FU 0.182 0.142 0.20112-24 months FU 0.407 0.131 0.002Percentage women 0.002 0.001 0.086
Work Participation b Intercept r 0.475 0.116 0.001Number of disciplines 0.088 0.025 0.001
Quality of life c PRP r 0.538 0.104 0.006CAU -0.241 0.112 0.041Surgery 0.372 0.071 <0.001Individual therapy/exercise -0.011 0.096 0.912Other multidisciplinary treatment -0.147 0.099 0.149
Analyses excluding study of Hellum et al.(2011)Disability d Intercept r 0.429 0.160 0.009
Individual therapy/exercise -0.154 0.120 0.206Psychological treatment -0.414 0.189 0.031Other multidisciplinary treatment -0.714 0.332 0.0341.5 – 6 months FU 0.174 0.152 0.25512 months FU 0.188 0.158 0.23712-24 months FU 0.447 0.171 0.010Percentage women 0.003 0.002 0.108Duration in weeks -0.037 0.018 0.038
Quality of life e Intercept r 0.417 0.033 <0.001CAU -0.231 0.087 0.018Individual therapy/exercise 0.040 0.058 0.496Other multidisciplinary treatment -0.160 0.075 0.050Age (centered at 45 years) 0.023 0.007 0.006
a: Reference category: effect of PRP post treatment, with 0% women as participants. b: Reference category: effect of treatment with 0 disciplines. c: Reference category: PRP. d: Reference category: effect of PRP with 6 weeks duration, post treatment, with 0% women as participants. e: Reference category: effect of PRP for patients at age of 45 years. β: Regression coeffi cient. SE: standard error β. r: random. CAU: Care as usual. PRP: Pain rehabilitation Program. FU: follow up/evaluation moment. *Although β not signifi cant model fi t increased signifi cantly.
Work Participation
The number of disciplines signifi cantly contributed to the regression equation. All other variables
entered into the model did not contribute signifi cantly. Table 5 shows that every discipline added

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
34 | Chapter 2
to the intervention, compared to the reference category of treatment with 0 disciplines, will
increase the ES with 0.088.
QoL
To predict the ES for outcome QoL, only type of intervention contributed signifi cantly to the
regression equation. Table 5 shows an effect of 0.417 for PRP (reference category). The negative
coeffi cients indicate a smaller effect for control interventions except for the intervention surgery
(β=0.372), indicating an effect for surgery of 0.538 + 0.372= 0.910. Type of intervention and
age contributed signifi cantly to the regression equation when performing the analysis without
the data of Hellum et al. 15 (Table 5). For QoL, the effect of PRP for patients at age of 45 years is
0.417; CAU and other multidisciplinary treatment for patients at age 45 years had smaller effect;
only individual therapy for patients aged 45 years showed a 0.040 (not signifi cant) larger effect
compared to PRP. Contact hours and number of disciplines were correlated (r=0.57, p<.01). The
number of disciplines involved and contact hours were larger in PRP (respectively, median 3 and
87.0) compared to other interventions (respectively, median 1 and 27.4). No other signifi cant
associations were found between contact hours, total duration of the treatment and number of
disciplines involved.
Discussion
To our knowledge, this is the fi rst systematic review analyzing the relationship between dose and
effect of multidisciplinary PRPs. Twelve out of the 18 studies were unique; they were not included
in the reviews of Guzman et al. 2 and Van Geen et al. 3. Some studies were published after these
2 reviews; other studies were not included in the current review because of different inclusion
and exclusion criteria. The current review shows a wide variety in contact hours and ES for all
interventions treating patients with CLBP. Within the interventions defi ned as multidisciplinary
PRP, substantial variation was observed in ES, contact hours, content, total duration and number
of disciplines. Analyzing the infl uence of predictor variables on effect of PRP on disability
demonstrated that the type of intervention, evaluation moment, percentage of women, and
the total duration in weeks infl uenced that effect. The number of disciplines involved infl uenced
effects on work participation, and QoL was additionally infl uenced by the type of intervention
and age of participants. PRP and surgery had the strongest effects on the outcome disability. PRP
had the strongest effect on the outcome work participation. Surgery, as described by Hellum et al. 15, was the only intervention that was superior to PRP. Surprisingly, no other studies were obtained
from the literature search comparing surgery to PRP for patients with CLBP.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 35
2
The review of Guzman et al. 2 provided evidence that intensive PRP of more than 100 h of therapy
produced greater improvements in function than PRP of less than 30 h of therapy. The current
review provides a wide variety of contact hours in PRPs, with a range of 6.4 to 196.8 h, with
larger ES than most of the control interventions. This shows that there are also PRPs producing
improvements within the range of 30 to 100 h of therapy. Therapies within this range of contact
hours were not included in the review of Guzman et al. 15,17,18,22,26. It is unknown whether these
PRPs are as effective as the PRPs of more than 100 h.
This study focused on dose aspects of treatment. The results of the analyses of this review showed
that type of intervention, evaluation moment, percentage of women, number of disciplines,
duration in weeks, and the age of the participants infl uenced the effect of interventions for
patients with CLBP. However, because contact hours and number of disciplines were interrelated
for all interventions, we are not able to draw conclusions about the relationship between
independent components and effects. In most cases, the number of disciplines involved depends
on the aim and content of the treatment. However, we demonstrated that it is currently not
possible to disentangle dose and content, which supports the importance of paying attention
to both components for analyzing the effectiveness of PRPs. Regarding the evaluation moment,
it is not clear whether the effect increases over time as a result of the intervention or as a result
of natural recovery. PRPs were on average more effective than the other interventions, but all
included studies analyzed PRPs with different doses and contents. Because studies were not
designed to investigate dose variables independently, we were not able to analyze the relationship
between dose and effects in PRP alone. Consequently, research on the effectiveness of PRPs may
have been biased because it has been focused solely on content and neglected dose of treatment.
All included studies were similar with regard to participants and study design. Subgroups were
made to analyze outcome domains and follow-up time separately. Therefore, we judged the
studies to be suffi ciently homogeneous to perform a meta-analysis. The heterogeneity of the
content of PRPs and outcomes is a strength of the study when focusing on the clinical use of the
information about dose aspects of PRPs, but is also a weakness regarding the methodological
strength of this review.
Study limitations
RCTs included in this study were aimed to analyze the effect of PRP. No RCTs were obtained
analyzing the relationship between dose and effect. Therefore, this study provides only indirect
conclusions, which is a limitation of the study. Another limitation is the statistical heterogeneity,
which was almost inevitable because of the wide variety of PRPs in terms of content, outcome
measures, dose and so on. Fortunately, more and more guidelines and recommendations 30 are
being published to encourage the homogeneity in chronic pain research. Another shortcoming

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
36 | Chapter 2
of this study is that the conclusions are based on a small sample of RCTs concerning PRPs,
resulting in a limited power. This small sample was the result of selection criteria for studies
to provide similar interventions and study designs and from the lack of consistent reporting of
dose variables. The small sample resulted in categories of evaluation moment with different
intervals and ES from different interventions, which limits the interpretability of these results.
The coeffi cients of the categories seem to indicate a much larger effect at 12 to 24 months (β=
0.460, β= 0.485) compared to the other evaluation moments. However, this category contains 12
months compared to 1 or 4.5 months interval in the other categories. An increase of ES during
the different evaluation moments exists, but it fl attens. Risk of bias was assessed with the tool
recommended by the Cochrane Back Review Group. The choice to use this risk of bias scale may
be debated because of the ongoing discussion about the blinding of patients and therapists
in nondrug trials. Although blinding is recommended to assess performance bias in RCTs 31,
patients were blinded in only 2 studies, and care providers were blinded in none of the studies 23,27. Low risk of bias was defi ned as scoring positively for 6 or more out of 12 items. Blinding of
patients and care providers covers 2 out of 12 items. Consequently, failure to blind care providers
and/or patients does not necessarily lead to a low quality rating. To fulfi ll the criteria of risk
of bias, there are methods regarding blinding of patients to interventions in nondrug trials,
such as evaluating treatment credibility, patient expectations and patient treatment preference.
Blinding of care providers is more diffi cult in nondrug trials; nevertheless, knowledge of which
intervention a patient received can infl uence treatment effects. Because of this risk of bias, the
extension of the CONSORT statement for nondrug trials suggests to report the interpretation of
the results regarding lack of or partial blinding in RCTs 32. Another option to control for lack of
blinding is measuring care providers’ allegiance and expectations towards dose and content of
the treatment protocol. To analyze the effect of the risk of bias analysis on the outcome of this
review, we performed a sensitivity analysis. Taking the item blinding of care providers out of the
risk of bias analysis would not have made a difference in the overall judgment of high or low risk
of bias, or of the fi nal conclusions of this review. Other quality assessment tools to analyze the risk
of bias are available for trials in which it is diffi cult to blind participants or therapists 33,34. Another
limitation is the language restriction. It is possible that other high-quality RCTs exist written in
other languages that could provide relevant information regarding aspects of dose.
Conclusion
This review supports the evidence that PRPs are effective and superior to most other interventions
in treating patients with CLBP on disability and work participation. Within PRPs, a wide variety of
contents and doses are observed. Dose aspects of PRPs are reported and analyzed insuffi ciently. On
the basis of the current literature, it is unknown how many hours, months, or weeks are needed
to achieve the best effects. It is also not possible to draw conclusions about the infl uences of dose
on effect, which could support the clinical decisions for dose of PRP for individual patients. To
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 37
2
further improve PRPs, there is need to report dose aspects (total duration of treatment, number of
contact hours, number of disciplines) in analyzing effects of PRPs and to study dosage (duration
and intensity) of PRPs. Additionally, qualitative studies aiming to identify relevant aspects of
dosage of PRPs could provide more insight in the importance and clinical relevance of dose.
Acknowledgement
We certify that no party having a direct interest in the results of the research supporting this
article has or will confer a benefi t on us or on any organization with which we are associated.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
38 | Chapter 2
References
1. Flor H, Fydrich T, Turk DC. Effi cacy of multidisciplinary pain treatment centers: A meta-analytic review. Pain. 1992;49(2):221-230.
2. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. BMJ. 2001;322(7301):1511-1516.
3. van Geen JW, Edelaar MJ, Janssen M, van Eijk JT. The long-term effect of multidisciplinary back training: A systematic review. Spine (Phila Pa 1976). 2007;32(2):249-255.
4. Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4. european guidelines for the management of chronic nonspecifi c low back pain. Eur Spine J. 2006;15 Suppl 2:S192-300.
5. Sanders SH, Harden RN, Vicente PJ. Evidence-based clinical practice guidelines for interdisciplinary rehabilitation of chronic nonmalignant pain syndrome patients. Pain Pract. 2005;5(4):303-315.
6. van Hooff ML, van der Merwe JD, O’Dowd J, et al. Daily functioning and self-management in patients with chronic low back pain after an intensive cognitive behavioral programme for pain management. Eur Spine J. 2010;19(9):1517-1526.
7. Waddell G. 1987 volvo award in clinical sciences. A new clinical model for the treatment of low-back pain. Spine (Phila Pa 1976). 1987;12(7):632-644.
8. Bendix AF, Bendix T, Vaegter K, Lund C, Frolund L, Holm L. Multidisciplinary intensive treatment for chronic low back pain: A randomized, prospective study. Cleve Clin J Med. 1996;63(1):62-69.
9. Hojat M, Xu G. A visitor’s guide to effect sizes: Statistical signifi cance versus practical (clinical) importance of research fi ndings. Adv Health Sci Educ Theory Pract. 2004;9(3):241-249.
10. Bendix AF, Bendix T, Lund C, Kirkbak S, Ostenfeld S. Comparison of three intensive programs for chronic low back pain patients: A prospective, randomized, observer-blinded study with one-year follow-up. Scand J Rehabil Med. 1997;29(2):81-89.
11. Bendix AF, Bendix T, Ostenfeld S, Bush E, Andersen. Active treatment programs for patients with chronic low back pain: A prospective, randomized, observer-blinded study. Eur Spine J. 1995;4(3):148-152.
12. Bendix T, Bendix A, Labriola M, Haestrup C, Ebbehoj N. Functional restoration versus outpatient physical training in chronic low back pain: A randomized comparative study. Spine (Phila Pa 1976). 2000;25(19):2494-2500.
13. Hozo SP, Djulbego. Estimating the mean and variance from the median, range, and the size of a sample. BMC Medical research methodology. 2005;5:13.
14. Borenstein M. Introduction to meta-analysis. Chichester, UK. Wiley; 2009:421.
15. Hellum C, Johnsen LG, Storheim K, et al. Surgery with disc prosthesis versus rehabilitation in patients with low back pain and degenerative disc: Two year follow-up of randomised study. BMJ. 2011;342:d2786.
16. Furlan AD, Pennick V, Bombardier C, van Tulder M, Editorial Board, Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the cochrane back review group. Spine (Phila Pa 1976). 2009;34(18):1929-1941.
17. Smeets RJ, Vlaeyen JW, Hidding A, et al. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? fi rst direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7:5.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 39
2
18. Vollenbroek-Hutten MM, Hermens HJ, Wever D, Gorter M, Rinket J, Ijzerman MJ. Differences in outcome of a multidisciplinary treatment between subgroups of chronic low back pain patients defi ned using two multiaxial assessment instruments: The multidimensional pain inventory and lumbar dynamometry. Clin Rehabil. 2004;18(5):566-579.
19. Alaranta H, Rytokoski U, Rissanen A, et al. Intensive physical and psychosocial training program for patients with chronic low back pain. A controlled clinical trial. Spine (Phila Pa 1976). 1994;19(12):1339-1349.
20. Jensen IB, Bergstrom G, Ljungquist T, Bodin L, Nygren AL. A randomized controlled component analysis of a behavioral medicine rehabilitation program for chronic spinal pain: Are the effects dependent on gender? Pain. 2001;91(1-2):65-78.
21. Skouen JS, Grasdal AL, Haldorsen EM, Ursin H. Relative cost-effectiveness of extensive and light multidisciplinary treatment programs versus treatment as usual for patients with chronic low back pain on long-term sick leave: Randomized controlled study. Spine (Phila Pa 1976). 2002;27(9):901-9; discussion 909-10.
22. Kaapa EH, Frantsi K, Sarna S, Malmivaara A. Multidisciplinary group rehabilitation versus individual physiotherapy for chronic nonspecifi c low back pain: A randomized trial. Spine (Phila Pa 1976). 2006;31(4):371-376.
23. Leeuw M, Goossens ME, van Breukelen GJ, et al. Exposure in vivo versus operant graded activity in chronic low back pain patients: Results of a randomized controlled trial. Pain. 2008;138(1):192-207.
24. Linton SJ, Boersma K, Jansson M, Overmeer T, Lindblom K, Vlaeyen JW. A randomized controlled trial of exposure in vivo for patients with spinal pain reporting fear of work-related activities. Eur J Pain. 2008;12(6):722-730.
25. Mangels M, Schwarz S, Worringen U, Holme M, Rief W. Evaluation of a behavioral-medical inpatient rehabilitation treatment including booster sessions: A randomized controlled study. Clin J Pain. 2009;25(5):356-364.
26. Dufour N, Thamsborg G, Oefeldt A, Lundsgaard C, Stender S. Treatment of chronic low back pain: A randomized, clinical trial comparing group-based multidisciplinary biopsychosocial rehabilitation and intensive individual therapist-assisted back muscle strengthening exercises. Spine (Phila Pa 1976). 2010;35(5):469-476.
27. Meng K, Seekatz B, Roband H, Worringen U, Vogel H, Faller H. Intermediate and long-term effects of a standardized back school for inpatient orthopedic rehabilitation on illness knowledge and self-management behaviors: A randomized controlled trial. Clin J Pain. 2011;27(3):248-257.
28. Roche-Leboucher G, Petit-Lemanac’h A, Bontoux L, et al. Multidisciplinary intensive functional restoration versus outpatient active physiotherapy in chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976). 2011;36(26):2235-2242.
29. Kainz B, Gulich M, Engel EM, Jackel WH. Comparison of three outpatient therapy forms for treatment of chronic low back pain-- fi ndings of a multicentre, cluster randomized study. Rehabilitation (Stuttg). 2006;45(2):65-77.
30. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1-2):9-19.
31. Higgins JP, Altman DG, Gotzsche PC, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
32. Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, CONSORT Group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann Intern Med. 2008;148(4):295-309.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
40 | Chapter 2
33. Yates SL, Morley S, Eccleston C, de C Williams AC. A scale for rating the quality of psychological trials for pain. Pain. 2005;117(3):314-325.
34. Boutron I, Moher D, Tugwell P, et al. A checklist to evaluate a report of a nonpharmacological trial (CLEAR NPT) was developed using consensus. J Clin Epidemiol. 2005;58(12):1233-1240.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dose or content? Effectiveness of PRP | 41
2

FrFrFranaankakaka PPPC CC WaWaWatetetersrsr chchchoooot,t,t PPieieeteteter r UUU DiDiD jkjkksttstraraa PPPhDhDhD,JaJaJannn HBHBHB GGGeeeeeertrtrtzezez nnn MDMDMD,, PhPhPhD,D,D, MMMicicichihihielele FFF RRenene ememanann PPPhDhDhD.
InInInt tt J JJ ReReRehahahabiibil ll ReReRes ss 20202015515, 383838 ((1)1)1): 343434-9-9-9.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
44 | Chapter 3
Abstract
The aim of this study was to analyze the course of reduction of disability during a pain rehabilitation
program (PRP) and factors infl uencing this course. A prospective cohort study was carried out. All
patients with chronic musculoskeletal pain treated in a PRP between March 2010 and December
2010 were eligible for this study. All patients were treated at a University-based rehabilitation
center and received an outpatient multidisciplinary PRP. Main outcome measures, Pain Disability
Index (PDI), and average pain measured with a numeric rating scale, were measured every 2
weeks during the PRP. To analyze the course of disability, a linear mixed-effect model was applied.
One hundred twenty-eight patients participated in the study, of which 20% dropped out during
the PRP. Initial PDI (β= 0.8), treatment week (β= -0.2), treatment week squared (β=0.03), average
pain (β= 2.3), and interaction between initial PDI and treatment week (β= -0.02) infl uenced the
course of disability during PRP. Disability reduces during the PRP. Initial PDI, treatment week,
average pain, and interaction between initial PDI and treatment week infl uence the course of
disability reduction during the PRP. These results could aid in predicting the required duration of
a PRP at the start.
Keywords
Chronic pain, disability, Pain Disability Index, Patient Care Team, Rehabilitation
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Course of disability reduction during a PRP | 45
3
Introduction
On the basis of pre and post measurements, it is known that pain rehabilitation programs (PRPs)
are effective in disability reduction in patients with chronic musculoskeletal pain (CMP) 1-7.
However, the course of disability reduction is unknown. Understanding the course of disability
reduction could aid in determining the optimum duration of PRPs. This understanding would
benefi t patients, clinicians, insurance companies and health care providers because it prevents
overtreatment or undertreatment and contributes towards better use of (public) recourses.
A wide diversity of content, composition, and duration of PRPs exist 3,4. In one systematic review,
differences in duration were unrelated to differences in outcomes 3. However, in another review
it was reported that multidisciplinary PRP of more than 100 h was superior to monodisciplinary
treatment, and that multidisciplinary PRP of less than 30 h was not superior to monodisciplinary
treatment. Although the authors focused on the content of different PRPs and the review was
designed to assess the effect of PRP, they concluded that PRPs of more than 100 h were more
effective. The conclusions of these reviews were used to establish guidelines and clinical practice 8,9. However, these conclusions were based only on pre-post assessments. To our knowledge,
no studies have analyzed the course of disability reduction during the programs to establish the
optimum duration of a PRP. In addition, it is unknown whether the improvements gained with
intensive PRPs are worth the expenses 4. Theoretically, if 90% of the improvements are observed
in the fi rst half of the PRP, it may be debated whether these 100 h or more, as proposed by
Guzman et al 4, are needed.
Because no previous research is available into this specifi c aspect of PRPs, we hypothesized that
there would be several possible courses of reduction of disability (Fig. 1). Line A assumes that the
course of disability has a steeper slope at the end of the PRP. This implies that disability decreases
most in the last part of the PRP. In contrast, line B assumes a steeper slope at the fi rst half of
the PRP. This Implies that disability decreases most in the fi rst part of the PRP. Line C implies a
linear decrease of disability, and an alternating pattern of decrease and increase during the PRP
is hypothesized in line D.
The aim of this study was to analyze the course of reduction of disability during PRP and to
analyze factors infl uencing this course.
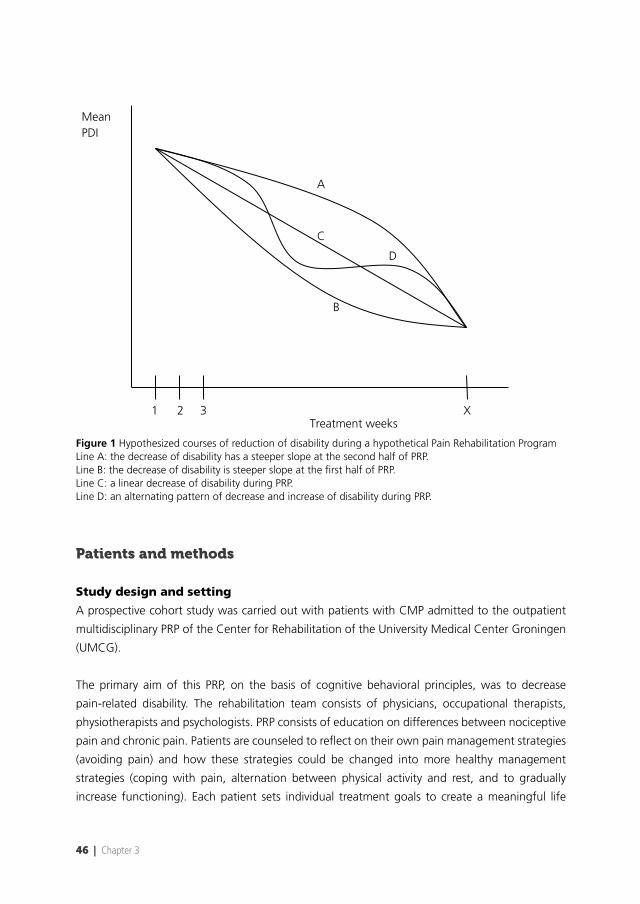
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
46 | Chapter 3
Treatment weeks
Mean PDI
1 2 3 X
A
B
C
D
Figure 1 Hypothesized courses of reduction of disability during a hypothetical Pain Rehabilitation ProgramLine A: the decrease of disability has a steeper slope at the second half of PRP. Line B: the decrease of disability is steeper slope at the fi rst half of PRP. Line C: a linear decrease of disability during PRP.Line D: an alternating pattern of decrease and increase of disability during PRP.
Patients and methods
Study design and setting
A prospective cohort study was carried out with patients with CMP admitted to the outpatient
multidisciplinary PRP of the Center for Rehabilitation of the University Medical Center Groningen
(UMCG).
The primary aim of this PRP, on the basis of cognitive behavioral principles, was to decrease
pain-related disability. The rehabilitation team consists of physicians, occupational therapists,
physiotherapists and psychologists. PRP consists of education on differences between nociceptive
pain and chronic pain. Patients are counseled to refl ect on their own pain management strategies
(avoiding pain) and how these strategies could be changed into more healthy management
strategies (coping with pain, alternation between physical activity and rest, and to gradually
increase functioning). Each patient sets individual treatment goals to create a meaningful life
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Course of disability reduction during a PRP | 47
3
despite the pain. To achieve these goals, each professional applies specifi c techniques. Physical
therapists apply exercise programs and sports activities, improve patients’ confi dence in movement,
and reduce pain related fear. Occupational therapists assess current activities and patterns in daily
living and educate patients on how these activities can be changed into healthy activity levels and
patterns. The psychologists coaches patients in understanding and dealing with the social and
emotional impact of pain in daily life, pain beliefs, and barriers for behavior change, and coach
patients on how to cope with pain. The rehabilitation physicians are responsible for the medical
diagnosis and interventions, and the overall treatment plan. During intake, the rehabilitation
team decides whether the patient can be admitted for PRP. PRP consisted of occupational therapy
sessions, 30 min, two times a week, physiotherapy sessions, 30-60 min, two times a week, and
psychology sessions, 60 min, once a week. The session frequency of occupational therapy and
physiotherapy reduced to once a week during the second half of PRP to encourage patients self
management among patients. After intake, the rehabilitation physician proposed a duration of
8, 12, 16 or 20 weeks of PRP to the patient on the bases of assessment of the complexity of the
physical, social and personal situation of the patient, motivation, and ability to change behavior.
The duration in weeks of the PRP could be adapted (increased or reduced) depending on clinical
progress. Duration could be increased when additional decrease in disability was expected by
lengthening the program. Duration was reduced when treatment goals were achieved earlier
than expected, when the patient showed continued lack of progress, or stops the treatment
because it did not match patients’ expectations or for reasons not related to the program.
Patients were included for PRP when they were 18 years or more of age, had CMP for more
than 3 months, experienced disabilities because of CMP, were not attending any other type
of treatment, were willing to participate in a PRP, and had signed an informed consent form.
Patients with severe comorbidities, interfering with PRP, such as heart failure, rheumatoid arthritis,
psychiatric disorders, and participants with an indication for surgery were not included for the
PRP. All patients treated in the PRP of the UMCG from March 2010 until December 2010 were
eligible for the study.
At baseline, patient characteristics (age, sex, marital status and employment status) were recorded.
The fi rst visit to the PRP (T1) and every uneven treatment week during the program (T2= week 3,
T3= week 5 etc), patients fi lled in the Pain Disability Index (PDI) and a numeric rating scale (NRS)
for average pain in the previous week (0 = no pain, 10= unbearable pain). The last assessment
was performed during the last visit. Patients were blinded for previous scores. If patients could
not be measured at the proposed week, they fi lled in the questionnaire the next visit.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
48 | Chapter 3
Main outcome
The PDI measures self reported disability on seven domains: family/home responsibilities,
recreation, social activity, occupation, sexual behavior, self-care, and life-support activity.
The patient scores the amount of interference in daily life because of pain for each domain
(0= no interference, 10= total interference). Total PDI is calculated by adding the scores of all
domains [range 0 (no disability) to 70 (extreme disability)]. Internal consistency for the PDI is high
(Cronbach’s α=0.86) 10. Construct validity is supported by a multiple regression analyses showing
nine variables to predict the PDI scores (R=0.74) 10. Test-retest reliability (1-week interval) is good
(intraclass correlation coeffi cient=0.91) 11. The minimal clinically important change is 8.5 point 12.
A maximum of two missing items was accepted for the PDI. If more than two items were missing,
a sum score was not calculated. When one or two items of the PDI were missing, the mean score
of the other items of that patient was calculated. The total score was calculated by replacing the
missing item by this calculated mean.
As patients provided written permission to use their clinical data and data were gathered during
care as usual, in the Netherlands, approval from a Medical Ethics Committee is not needed.
Statistical analysis
Descriptive statistics were computed for patient characteristics and outcome variables. Means
and SDs were used for PDI and pain scores. An independent sample t-test was used to compare
means of initial PDI of completers (participants who completed the program) versus noncompleters
(participants who dropped out before the program was ended). Q-Q plots were constructed
to check the assumptions of normal distribution of initial PDI scores. The duration of PRP was
categorized according to the total number of weeks that a patient received treatment. Categories
were: ≤ 8, 9 ≤ 12, 13 to ≤ 16 and ≥17 weeks. To analyze the course of disability during PRP and
factors infl uencing this course, a linear mixed-effect model was applied. A linear mixed-model
analysis corrects for autocorrelation in data, which occurs in repeated measurements over time
within individuals. All available data were taken into account in the analysis, including those of
patients with incomplete datasets 13,14. Outcomes on the PDI were entered as response variable.
Before this analysis, the change in PDI scores during PRP was assessed in a graph to check linearity
for applying the appropriate regression model. Possible predictor variables of the course were
patient characteristics (age, sex, marital status, and employment status), treatment week (=week
of measurement), duration of PRP (in categories), initial PDI score, pain characteristics (average
pain in the week before the PDI assessment, pain duration, and pain localization) and completing
PRP (yes, no). These variables were entered stepwise in the regression model. Assessment of
the graph showed that the change of PDI during PRP allowed a quadratic (treatment week x
treatment week) or cubic model (treatment week x treatment week x treatment week). These
models were explored by entering variable treatment week2 and treatment week3 in the regression
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Course of disability reduction during a PRP | 49
3
equation. Entered predictors remained in the model if the model fi t (-log-likelihood) increased
signifi cantly or if the regression coeffi cient was signifi cant. After the main effects were established
the covariance structure best applicable to the data was explored, again using the model fi t as
criterion. After determining the covariance structure, random intercept and slopes were explored
using the model fi t. Interactions between predictors were explored if main effects were signifi cant
(P≤0.05). Data were analyzed using SPSS (version 18.0; SPSS Inc., Chicago, Illinois, USA).
Results
A total of 128 patients participated in the study. Mean age of the patients was 41.7 (SD 11.8,
range 19-68) years. CMP was categorized as chronic back pain (55%), chronic neck pain
(19%) and other types of chronic pain (26%), such as widespread pain, non-specifi c pain of
lower extremities (knee, foot) etc. Patients attended PRP for an average duration of 12.5 (SD
4.0, range 3-23) weeks and received on average 38 (SD 17.1, range 5.5-89.8) contact hours.
Thirty-eight percent (n=49) of the patients received the proposed amount of treatment weeks
(range ± 1 week). Thirty-seven percent (n=47) received less (including noncompleters) and 13%
(n=17) received more than amount of treatment weeks proposed by the rehabilitation physician.
The proposed duration was not reported in 12% (n=15) of the cases. Twenty-six (20%) of the
128 patients dropped out during the PRP; they did not complete the program for lack of effect
(2%, n=2), unrealistic expectations of the program (3%, n=4), wanting additional diagnostic
procedures (2%, n=2), because they believed that the benefi ts of the program did not weigh
against efforts (3%, n=4), treatment was too demanding (3%, n=4) or other reasons (8%,
n=10). The majority of noncompleters stopped during the fi rst 8 weeks of PRP. Because of
different treatment durations and dropout, the total number of participants decreased from the
fi rst to the 27th treatment week (Fig. 2). Baseline characteristics (n= 128) are shown in Table 1.
Noncompleters and completers signifi cantly differed on age, marital status, and employment
status. The difference in duration of pain of completers versus noncompleters was not signifi cant.
The mean PDI for all patients at T1 (n = 125) was 34.2 (SD 12.0). Mean NRS average pain was 5.6
(SD 1.9). The mean initial PDI was signifi cantly (P=0.013) lower for completers compared to
noncompleters [mean difference= 6.6, confi dence interval (CI) 1.4-11.7] (Table 2).
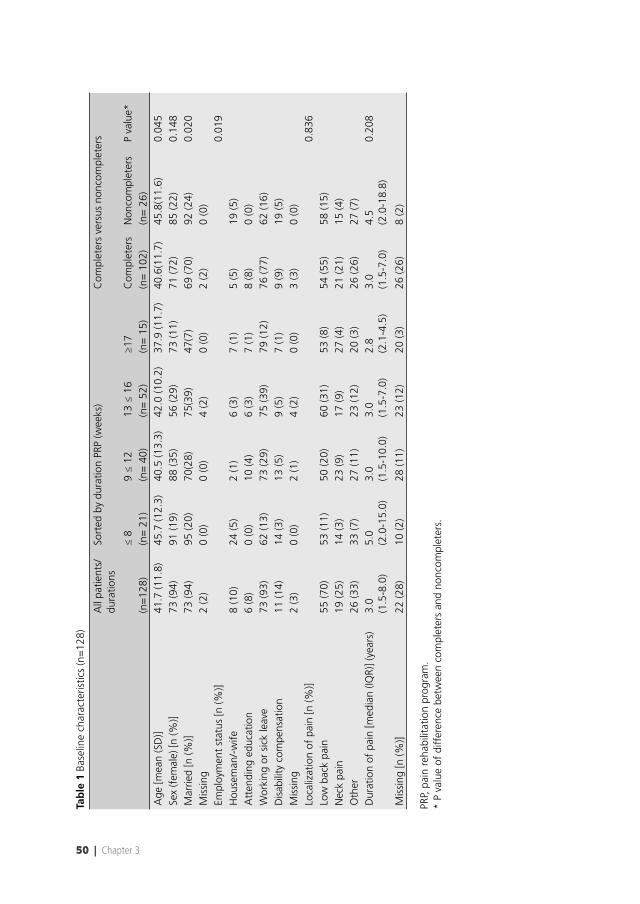
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
50 | Chapter 3
Tab
le 1
Bas
elin
e ch
arac
teris
tics
(n=
128)
All
patie
nts/
du
ratio
nsSo
rted
by
dura
tion
PRP
(wee
ks)
Com
plet
ers
vers
us n
onco
mpl
eter
s
≤ 8
9 ≤
12
13 ≤
16
≥17
Com
plet
ers
Non
com
plet
ers
P va
lue*
(n=
128)
(n=
21)
(n=
40)
(n=
52)
(n=
15)
(n=
102
)(n
= 2
6)A
ge [m
ean
(SD
)]41
.7 (1
1.8)
45.7
(12.
3)40
.5 (1
3.3)
42.0
(10.
2)37
.9 (1
1.7)
40.6
(11.
7)45
.8(1
1.6)
0.04
5Se
x (f
emal
e) [n
(%)]
73 (9
4)91
(19)
88 (3
5)56
(29)
73 (1
1)71
(72)
85 (2
2)0.
148
Mar
ried
[n (%
)]73
(94)
95 (2
0)70
(28)
75(3
9)47
(7)
69 (7
0)92
(24)
0.02
0M
issi
ng
2 (2
)0
(0)
0 (0
) 4
(2)
0 (0
)2
(2)
0 (0
)Em
ploy
men
t st
atus
[n (%
)]0.
019
Hou
sem
an/-
wife
8 (1
0)24
(5)
2 (1
)6
(3)
7 (1
)5
(5)
19 (5
)A
tten
ding
edu
catio
n6
(8)
0 (0
)10
(4)
6 (3
)7
(1)
8 (8
)0
(0)
Wor
king
or
sick
leav
e73
(93)
62 (1
3)73
(29)
75 (3
9)79
(12)
76 (7
7)62
(16)
Dis
abili
ty c
ompe
nsat
ion
11 (1
4)14
(3)
13 (5
)9
(5)
7 (1
)9
(9)
19 (5
)M
issi
ng2
(3)
0 (0
)2
(1)
4 (2
)0
(0)
3 (3
)0
(0)
Loca
lizat
ion
of p
ain
[n (%
)]0.
836
Low
bac
k pa
in55
(70)
53 (1
1)50
(20)
60 (3
1)53
(8)
54 (5
5)58
(15)
Nec
k pa
in19
(25)
14 (3
)23
(9)
17 (9
)27
(4)
21 (2
1)15
(4)
Oth
er26
(33)
33 (7
)27
(11)
23 (1
2)20
(3)
26 (2
6)27
(7)
Dur
atio
n of
pai
n [m
edia
n (IQ
R)] (
year
s)
3.0
(1.5
-8.0
)
5.0
(2.0
-15.
0)3.
0 (1
.5-1
0.0)
3.0
(1.5
-7.0
)2.
8 (2
.1-4
.5)
3.0
(1.5
-7.0
)
4.5
(2.0
-18.
8)
0.20
8
Mis
sing
[n (%
)]22
(28)
10 (2
)28
(11)
23 (1
2)20
(3)
26 (2
6)8
(2)
PRP,
pai
n re
habi
litat
ion
prog
ram
.*
P va
lue
of d
iffer
ence
bet
wee
n co
mpl
eter
s an
d no
ncom
plet
ers.
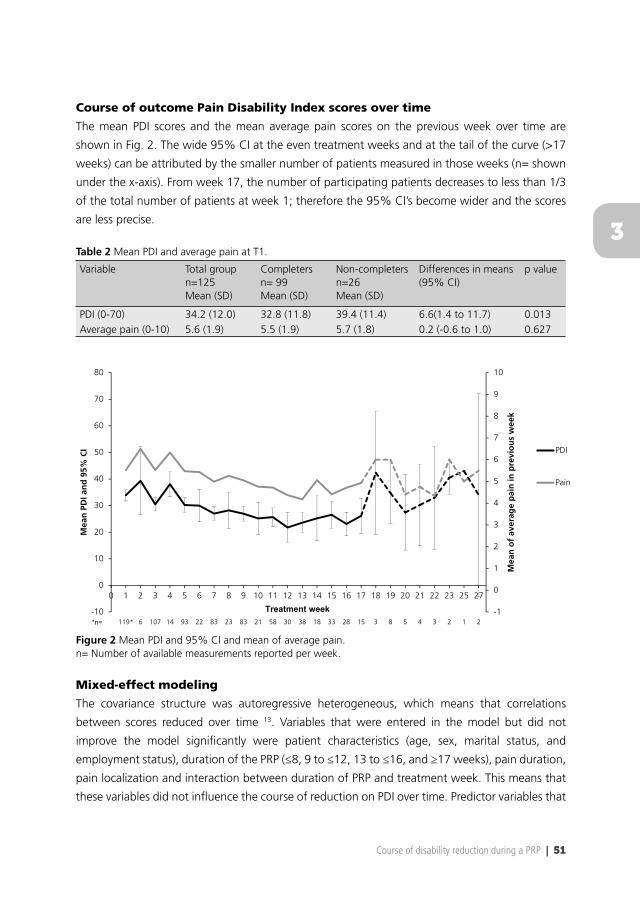
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Course of disability reduction during a PRP | 51
3
Course of outcome Pain Disability Index scores over time
The mean PDI scores and the mean average pain scores on the previous week over time are
shown in Fig. 2. The wide 95% CI at the even treatment weeks and at the tail of the curve (>17
weeks) can be attributed by the smaller number of patients measured in those weeks (n= shown
under the x-axis). From week 17, the number of participating patients decreases to less than 1/3
of the total number of patients at week 1; therefore the 95% CI’s become wider and the scores
are less precise.
Table 2 Mean PDI and average pain at T1.
Variable Total groupn=125Mean (SD)
Completersn= 99Mean (SD)
Non-completersn=26Mean (SD)
Differences in means (95% CI)
p value
PDI (0-70) 34.2 (12.0) 32.8 (11.8) 39.4 (11.4) 6.6(1.4 to 11.7) 0.013Average pain (0-10) 5.6 (1.9) 5.5 (1.9) 5.7 (1.8) 0.2 (-0.6 to 1.0) 0.627
119* 6 107 14 93 22 83 23 83 21 58 30 38 18 33 28 15 3 8 5 4 3 2 1 2-1
0
1
2
3
4
5
6
7
8
9
10
-10
0
10
20
30
40
50
60
70
80
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 25 27
Mea
n o
f av
erag
e p
ain
in p
revi
ou
s w
eek
Mea
n P
DI a
nd
95%
CI PDI
Pain
Figure 2 Mean PDI and 95% CI and mean of average pain.n= Number of available measurements reported per week.
Mixed-effect modeling
The covariance structure was autoregressive heterogeneous, which means that correlations
between scores reduced over time 13. Variables that were entered in the model but did not
improve the model signifi cantly were patient characteristics (age, sex, marital status, and
employment status), duration of the PRP (≤8, 9 to ≤12, 13 to ≤16, and ≥17 weeks), pain duration,
pain localization and interaction between duration of PRP and treatment week. This means that
these variables did not infl uence the course of reduction on PDI over time. Predictor variables that
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
52 | Chapter 3
signifi cantly infl uenced the model were treatment week, initial PDI score, average pain, and the
interaction between initial PDI and treatment week. This means that these variables did infl uence
the course. The model improved signifi cantly by allowing for each patient a random intercept
and a random slope for average pain (Table 3). Treatment week2 contributed signifi cantly toward
the regression equation, treatment week3 did not. This means that the PDI reduces according to
a quadratic model over time during PRP, and not according to a cubic model.
Table 3 Results of a linear mixed-model analysis to predict change in Pain Disability Index score during a pain rehabilitation program.
Predictor βa SE β P valueIntercept (Pb) -5.3 1.9 0.005Treatment week -0.2 0.2 0.174Initial PDI 0.8 0.05 < 0.001Average pain previous week (Pb) 2.3 0.2 < 0.001Time X Initial PDI -0.02 0.004 < 0.001Treatment week x Treatment week 0.03 0.007 < 0.001
PDI, Pain Disability Index.aβ: Regression coeffi cient.bP: random for patient.
Clinically, this means that treatment week, initial PDI score, average pain, and the interaction
between initial PDI and treatment week infl uence the course of PDI scores during PRP. The
coeffi cients of Table 3 indicate that, for instance, a patient with an initial PDI score of 40 and a
score of 6 on average pain in the fourth treatment week will have an average PDI score of 36.3 in
the fi fth treatment week of the PRP. This can be calculated using the following formula:
PDI= -5.3 + (-0.2 x treatment week) + (0.8 x initial PDI) + (2.3 x average pain) + (0.03 x treatment
week2) + [-0.02 x (initial PDI x treatment week)].
Discussion
At group level, disability reduction during PRP occurs following a quadratic model, quite similar
to the hypothesized line B in Fig. 1. Reduction in average pain in the previous week precedes
decrease of disability. The strength of this infl uence is 2.3 points on PDI per point pain reduction
(Table 3). Hence, a reduction of 1 point on average pain will decrease disability with 2.3 points.
The interaction between initial PDI and treatment weeks also infl uences the course, which means
the strength of infl uence per treatment week on PDI (β=-0.02) depends on the initial PDI: a
higher initial PDI will lead to a steeper decrease per week compared with a lower initial PDI. The
infl uence of the quadratic factor of treatment week on the course is 0.03: the effect of treatment
week on PDI (-0.2 per treatment week) is reduced by the quadratic term of treatment week
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Course of disability reduction during a PRP | 53
3
(0.03). This means that towards the end of the PRP, disability reduction per week becomes smaller
(Fig. 1, line B).
The results of this study have provided insight into the course of disability reduction over time. The
clinical relevance of this study is two-fold. First, because most of the gain in disability reduction
is obtained in the earlier weeks of PRP, the added value of additional PRP toward the end of
the program may become trivial. Second, the relevance of knowing which factors infl uence the
course of disability reduction may be that one can on average predict the duration of the PRP
if one knows the target reduction of disability. For example, if the target reduction is 8.5 PDI
points, the minimal clinically important change 12, the predicted mean duration of the PRP for an
‘average patient’, with an initial PDI of 40 and an average pain score of 6, would be 14 weeks.
This is the fi rst study in which the course of disability during a PRP was analyzed. Most studies
have focused on the effect of PRPs based on pre, post, and follow-up measurements, focused on
other types of treatments or other groups of participants 6,15,16. With this study, we have provided
a new aspect of research of PRPs: dose of PRP. Within the rehabilitation literature, there is no
robust evidence to substantiate dose aspects (duration and contact hours) of PRPs. It appears that
dose aspects have been neglected in PRP research. Generalization of the fi ndings of this study may
be challenging and calls for replication studies within and outside the Netherlands. The general
principle of the course of disability reduction might also apply to PRPs outside the Netherlands.
However, dose choices are also infl uenced by cultural factors and differences between professional
teams within and outside the Netherlands. In addition, fi nancial reimbursement will also infl uence
the choice of dose.
Study limitations
This study has some limitations. Some data were missing on PDI items. However, the effects
of these missing data were limited because the total score of PDI is used, which represents
general (average) disability. For the statistical analyses, the use of a mixed model limited the
infl uence of missing data. In clinical practice, we could not arrange a rigidly fi xed measurement
time equal for each patient. We had to deal with absence of patients and care as usual was
not ready for digitalized versions of the questionnaires to minimize missing data because of
absence. Nevertheless, all available data were used in the mixed-effect model. Because of ethical
regulations related to digital patient information safety, we could not follow up patients every
2 weeks after PRP. It is advised, however, that future studies focus on the follow up period also
because it is assumed that further progress occurs after completion of the program. Twenty
percent of the patients dropped out, but data of all patients, completers and noncompleters,
were taken into account for the mixed-model analysis. Noncompleters may be considered a
limitation from a statistical point of view. However, in daily clinical care, noncompletion is often
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
54 | Chapter 3
observed. Noncompletion has not been the subject of study. In this study, it appeared challenging
for the clinicians to estimate treatment duration before the PRP. As shown in the result section,
the actual PRP duration differed from the pretreatment estimated duration. This may be regarded
a limitation of this study because this provides variance in total treatment weeks and number
of patients per treatment duration, but it underscores the clinical need to know the course of
disability reduction and factors predicting this course that could contribute toward more rational
estimations of treatment duration.
The major strength of this study is the strong relation to clinical practice, which enhances the
external validity: measurements were performed in care as usual and the results of the mixed-
model analyses can contribute toward estimate of the duration of PRPs. Also, the heterogeneous
group strengthens the results of this study because differences in pain locations did not affect
the results and therefore the outcome is generalizable to a broader group of patients with CMP.
Conclusions regarding optimum duration of PRPs cannot be drawn. However, the results of this
study show the need for further research on the course of disability and dose aspects of PRPs.
Future research could focus on the effect of shortening a PRP on the course of disability reduction
or the course of disability after completion of a PRP. It should also focus on the added value of
additional PRP (h/weeks) to analyze at which point treatments are no longer benefi cial for the
patient or no longer cost-effective.
Conclusion
From the results of this study, we can conclude that disability reduces according to a quadratic
model during PRPs. Initial PDI, treatment week, average pain, and interaction between initial PDI
and treatment week infl uence the course of disability reduction during PRP. These data could aid
in clinical practice to predict the duration of the PRP at start. Further research investigating dose
aspects of PRPs is needed to aid in the effectiveness and cost-effectiveness of PRPs.
Acknowledgements
Many thanks are due to all the therapists of the Pain Rehabilitation Department of the Center for
Rehabilitation of the University Medical Center Groningen for collecting the data.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Course of disability reduction during a PRP | 55
3
References
1. McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: Outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27(22):2564-2573.
2. Gatchel RJ, Okifuji A. Evidence-based scientifi c data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779-793.
3. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: A systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
4. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. BMJ. 2001;322(7301):1511-1516.
5. Smeets RJ, Vlaeyen JW, Hidding A, et al. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? fi rst direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7:5.
6. Skouen JS, Grasdal AL, Haldorsen EM, Ursin H. Relative cost-effectiveness of extensive and light multidisciplinary treatment programs versus treatment as usual for patients with chronic low back pain on long-term sick leave: Randomized controlled study. Spine (Phila Pa 1976). 2002;27(9):901-9; discussion 909-910.
7. Jensen IB, Bergstrom G, Ljungquist T, Bodin L, Nygren AL. A randomized controlled component analysis of a behavioral medicine rehabilitation program for chronic spinal pain: Are the effects dependent on gender? Pain. 2001;91(1-2):65-78.
8. Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4. european guidelines for the management of chronic nonspecifi c low back pain. Eur Spine J. 2006;15 Suppl 2:S192-300.
9. van Hooff ML, van der Merwe JD, O’Dowd J, et al. Daily functioning and self-management in patients with chronic low back pain after an intensive cognitive behavioral programme for pain management. Eur Spine J. 2010;19(9):1517-1526.
10. Tait RC, Chibnall JT, Krause S. The pain disability index: Psychometric properties. Pain. 1990;40(2):171-182.
11. Gronblad M, Hupli M, Wennerstrand P, et al. Intercorrelation and test-retest reliability of the pain disability index (PDI) and the oswestry disability questionnaire (ODQ) and their correlation with pain intensity in low back pain patients. Clin J Pain. 1993;9(3):189-195.
12. Soer R, Reneman MF, Vroomen PC, Stegeman P, Coppes MH. Responsiveness and minimal clinically important change of the pain disability index in patients with chronic back pain. Spine (Phila Pa 1976). 2012;37(8):711-715.
13. Field A. Multilevel linear models. In: Discovering statistics using SPSS. 3rd ed. Los Angeles, London, New Delhi, Singapore, Washington DC: Sage; 2009:725.
14. Twisk JWR. Applied longitudinal data analysis for epidemiology: A practical guide. Cambridge etc.: Cambridge University Press; 2003:301.
15. Gross DP, Haws C, Niemelainen R. What is the rate of functional improvement during occupational rehabilitation in workers’ compensation claimants? J Occup Rehabil. 2012;22(3):292-300.
16. Rainville J, Jouve CA, Hartigan C, Martinez E, Hipona M. Comparison of short- and long-term outcomes for aggressive spine rehabilitation delivered two versus three times per week. Spine J. 2002;2(6):402-407.
FrFrFrananankakaka PPP.CCC. WaWaWatetetersrsrschchchoooooot,t,, PPieieeteteter rr U.U.U DDDijiji ksksk trtraaa PhPhPhD,D,DJoJoJohahahannnn esses GGG.MM.M.. BuBuBurgrggerererhohoof f PhPhPhD,D,D JJananan HHH.BBB. GeGeGeerere tzztzenen MMD,D,D, PPPhDhDhD,
HeHeHenrnrn icicicaaa R.RR SSchchipipphohohorsst tt PrPrPreueue pepeper r r MDMDMD,,, PhPhP D,D,D, MMMiccchihhieleel FFF. ReReR nennemamam nnn PhPhPhD.DD
SuSuSubmbmbmitittteteted dd fofoor r pupublblblicicicatatatioioonn

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
58 | Chapter 4
Abstract
Objective: To analyze effects of multidisciplinary pain rehabilitation programs with different
dosages; care as usual (CAU) versus care as usual short form (CAU-SF).
Methods: A single blinded, 2 armed, randomized controlled trial, with non-inferiority design
was performed. All patients with chronic musculoskeletal pain referred to an outpatient
multidisciplinary pain rehabilitation program were eligible for this study. Only dosage in weeks
differed between the 2 groups, content was similar. The pain disability index (PDI) was the primary
outcome measure. Four points difference on PDI was applied as non-inferiority margin. Treatment
effects within groups were expressed in standardized mean difference (SMD) and effect sizes (ES)
were calculated between groups.
Results: Both groups improved signifi cantly on PDI (CAU: -10.8, CAU-SF: -8.3). Frequent extension
of CAU-SF leads to limited contrast in dosage between groups. The 2.5 points difference on PDI
falls within the non-inferiority margin but the confi dence interval (CI) (-2.2 to 7.3) exceeded it.
SMDs of CAU and CAU-SF were 0.8 and 0.7 respectively. ES was 0.2.
Conclusions: Reduction of dosage of pain rehabilitation programs did not lead to non-inferior
mean results. Difference in means showed non-inferiority but CI exceeded both the upper and
lower border of the non-inferiority margin. The results of this trial are inconclusive.
Keywords
Dosage, Pain Rehabilitation Program, Chronic pain, Chronic musculoskeletal pain.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 59
4
Introduction
Multidisciplinary Pain Rehabilitation Programs (PRPs) are recommended for patients with chronic
low back pain (CLBP) 1. They aim to reduce disability, distress and use of health care services
by education of physical, psychological and practical techniques to improve function, work
participation and health related quality of life 2. Multidisciplinary programs are effective for
patients with chronic musculoskeletal pain (CMP) 1,3,4.
Across pain rehabilitation centres nationally and internationally, there is much diversity in content
and dosage of PRPs. Health care systems aim for the best treatments based on available evidence.
However, there is paucity of evidence about the infl uence of dose on effects of PRP. In a recent
systematic review 5, no randomized controlled trials (RCTs) were identifi ed that were designed to
analyse effects of differences in dose variables on outcome of PRPs. Additionally no studies were
identifi ed with the primary objective to analyze the association between dose and effect of PRP.
If PRPs optimal dosage is known, this may benefi t patients and could reduce direct or indirect
costs. If similar effects are achieved with a shorter program, this could lead to earlier reduction of
disability, regaining quality of life, and sooner participation in daily life, and minimize direct and
indirect costs associated with PRP. Employers could also benefi t from earlier return to work (RTW)
for patients with work productivity loss, rehabilitation centres can reduce waiting lists and overall
it can improve effi ciency of care. Additionally shorter programs are also attractive for health care
insurers and society as a result of reducing direct and indirect costs.
The aim of this study was to analyze differences in effects of PRPs with different duration: care as
usual (CAU) and PRP short form care as usual (CAU-SF) in a non-inferiority design. CAU-SF was
hypothesized to be non-inferior to CAU in an outpatient pain rehabilitation setting.
Methods
Design
The study is a single blinded, 2 armed, RCT, with a non-inferiority design. The RCT took place
at the University Medical Centre Groningen (UMCG), Department of Rehabilitation Medicine,
Centre for Rehabilitation, location Beatrixoord Haren. The Medical Ethics Committee of the
UMCG approved the study protocol [NL30094.042.11]. Trial registration: international clinical
trials registry platform of WHO, TrialID= NTR3385.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
60 | Chapter 4
Defi nitions
Because dosage variables are relatively new to the scientifi c fi eld of PRP, we have defi ned dosage
related terms for this study. Duration means the total length of PRP and is expressed in weeks.
Contact hours are the total amount of hours that a patient spends with his therapist during PRP.
Participants
All patients with CMP referred to an outpatient PRP at the Centre for Rehabilitation, UMCG,
between September 2011 and October 2013 were potential participants for this study. This
centre provides PRPs with duration of 8, 12, 16 or 20 weeks. Patients were eligible for the study
when: 1. They were admitted for a 12, 16 or 20 week PRP; 2. they had CMP for more than three
months without a specifi c pathological cause; 3. they experienced CMP induced disability; 4.
social and psychological factors were complex and were assumed to be relevant in maintaining
CMP induced disability 2; 5. they were willing to stop other treatments for CMP during PRP (except
pain medication); 6. they were 18 years or older; 7. they were motivated to participate in PRP
and 8. they were willing to participate in the study and signed informed consent. Patients were
excluded when: 1. they were referred to the 8 weeks PRP; 2. they were unable to understand
the Dutch language; 3. they had co morbidities such as heart failure, rheumatoid arthritis, or
psychiatric disorders preventing a PRP.
Interventions
Common features of CAU and CAU-SF
The objectives of CAU and CAU-SF were the same and the content was similar; both treatments
were outpatient, multidisciplinary PRPs aimed to decrease CMP related disability, optimize
participation and increase quality of life. PRP is intended to coach patients to self manage their
pain and disability. The rehabilitation team consisted of rehabilitation physicians, occupational
therapists (OTs), physiotherapists (PTs) and psychologists (PSYs). The PRP, based on cognitive
behavioural principles, consisted of pain education, for example regarding differences between
nociceptive and chronic pain. Patients were counselled to refl ect on their pain management
strategies (avoiding pain) and how these strategies could be changed into other management
strategies (pain coping, alternating physical activity and rest and gradually increasing activities).
Each patient set individual treatment goals. PTs applied exercise programs and sports activities,
to improve patients’ confi dence in movement and reduce pain-related fear, improve activity level,
and physical functioning. OTs assessed current activities and patterns in daily living and educated
patients how activities could be changed into, healthy activity levels and patterns. PSYs coached
patients in understanding and dealing with the social and emotional impact of pain in daily life,
pain beliefs, barriers for behaviour change and coached patients how to cope with pain. The
rehabilitation physicians were responsible for the medical diagnosis and interventions (if any) and
coordinated the overall treatment plan.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 61
4
After the rehabilitation physician considered patients to be eligible for PRP, they were invited for
an intake procedure, consisting of an interview by an OT, a PT and a PSY. These interviews were
aimed at admitting a patient to PRP or not, and to formulate a treatment plan. If the patient was
admitted to PRP, based on the assessments during intake, the team (rehabilitation physician, OT,
PT, PSY) determined the required duration of 8, 12, 16 or 20 weeks based on assessment of the
complexity of the physical, social and personal situation of the patient, motivation and ability to
change behaviour. The team who determined treatment duration consisted of professionals with
on average 9 years of experience in pain rehabilitation.
PRP consisted of OT sessions, 30 minutes, 2 times a week, PT sessions, 30 to 60 minutes, 2
times a week and PSY sessions, 60 minutes, once a week. The session frequency of OT and
PT reduced to once a week, the PSY sessions reduced to once every 2 weeks, based on the
frequency protocols per duration. All sessions were delivered in a individual setting. For clinical
reasons, the duration in weeks of PRP could be adapted (extended or shortened) in CAU and
in CAU-SF, depending on the progression of the patient. Duration could be extended when
additional coaching was needed to decrease in disability during the extra weeks of PRP. Duration
was shortened when treatment goals were achieved earlier than expected, when the patient
demonstrated continued lack of progress, or when the patient stopped the treatment, because it
did not match patient expectations or reasons not related to the program (for instance holidays).
Extending or shortening of the duration of PRP was based on agreement between the patient and
the PRP team and decided by the rehabilitation physician. Reasons for extending or shortening
PRP were registered.
The difference between CAU and CAU-SF was the duration (in weeks) of PRP proposed to the
patients after the randomization procedure. Differences in duration will also result in differences
in contact hours. Patients allocated to the CAU group received 12, 16 or 20 weeks of PRP as
proposed after the intake procedure. Patients allocated to the CAU-SF group received a 4 week
shortened form of PRP than proposed (which will result in approximately 10 fewer contact hours
on average). Thus patients in CAU-SF received 4 weeks less than proposed after intake. Patients
allocated to 8 weeks of PRP in CAU were excluded because the treatment team thought it would
not be feasible to offer PRP in 4 weeks with frequencies twice a week.
Outcomes
The primary outcome variable was self-reported disability assessed with the Pain Disability Index
(PDI) 6. The questionnaire consists of seven items related to work, leisure and activities of daily life
each item is scored on an 11-point scale (0 indicating no disability and 10 indicating maximum
disability). The total scale ranges from 0 to 70. The high correlation between the PDI and Oswestry
Disability Index (r=0.83) indicates good validity. Test-retest reliability is high (ICC=0.91) 7. Minimal
Clinically Important Change (MCIC) ranges from 8.5 to 9.5 points 8.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
62 | Chapter 4
The secondary outcome variable, quality of life, was measured with the Euroqol 5D-5L (EQ5D-5L;
scale range -0.329 to 1.000) 9. The EQ-5D-5L assesses 5 dimensions (mobility, self-care, usual
activities, pain/discomfort, anxiety/depression) of health on a 5 point scale: no problems, slight
problems, moderate problems, severe problems, and extreme problems. The overall health is
assessed on a 0-100 visual analogue scale of 20 cm (EQ-5D-VAS). A higher score indicates a
better overall health state. The minimally clinical important difference (MCIC) was 10.5 points for
the EQ-5D VAS and 0.03 points for the 5 dimensions of the EQ-5D-3L 10. The EQ-5D-5L version is
based on the EQ-5D-3L version. The 5L version demonstrates improved discriminatory power 11,
but the exact MCIC for this version has not been examined (yet).
Sample size
Sample size was calculated using the group sequential non-inferiority criterion. The standard
deviation (SD) on PDI scores in CAU was 11. The non-inferiority margin was calculated as 40%
of the mean change on PDI scores in CAU, which was 10 points, thus the non-inferiority margin
was set at 4 points. For group sequential non-inferiority design an alpha of 0.045 and power of
0.8 was used. Using PASS software, these data gave an estimation of 124 patients needed per
arm and 248 patients in total. Including 10% drop-outs, 276 patients should be included for the
study.
Randomization
After determination of PRP duration by the team and after obtainment of informed consent,
patients were randomized by an independent person. Patients were stratifi ed on work status
(paid work or unpaid/no work), resulting in 2 strata. For each stratum blocks of 6 were used.
Sequentially numbered, sealed, opaque envelopes were used for each stratum.
Blinding
Patients were blinded for intervention. Before inclusion, they were informed about duration
of CAU, which could be 8, 12, 16 or 20 weeks. Patients were explained that a duration was
proposed by the team based on the assessment results. Furthermore, they were informed about
the experiment of 4 weeks shortening duration. They were unaware of the treatment duration
they supposed to receive in CAU, and, therefore, they were blinded of allocation to CAU or CAU-
SF. Patients were outcome assessor for outcome measurements; they were blinded for T0 scores.
Rehabilitation physicians, OTs, PTs and PSYs could not be blinded for intervention for the 20
weeks duration because this part only exists in the CAU group. Eight week PRPs could be CAU-SF
or patients not included in the study attending 8 weeks PRP.
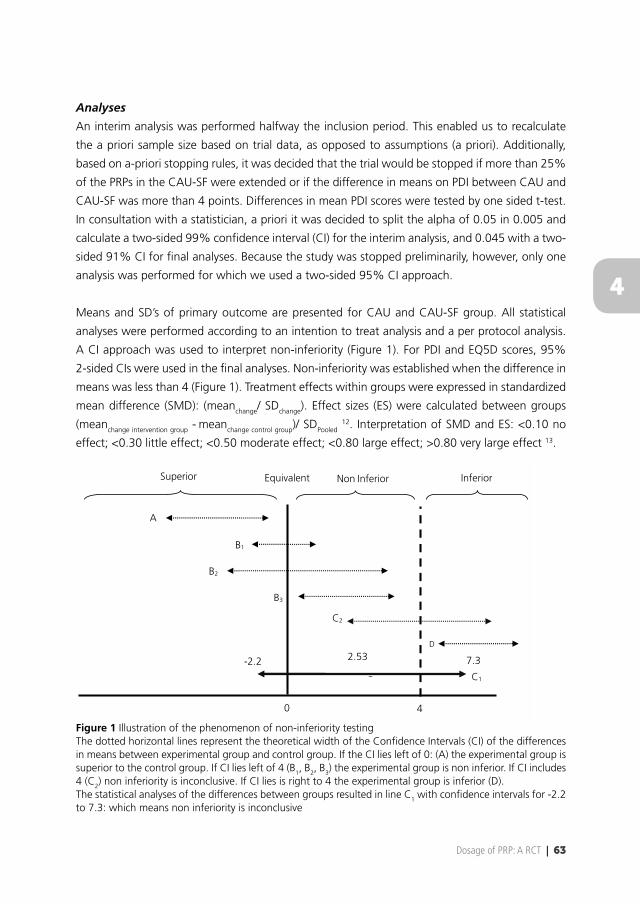
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 63
4
Analyses
An interim analysis was performed halfway the inclusion period. This enabled us to recalculate
the a priori sample size based on trial data, as opposed to assumptions (a priori). Additionally,
based on a-priori stopping rules, it was decided that the trial would be stopped if more than 25%
of the PRPs in the CAU-SF were extended or if the difference in means on PDI between CAU and
CAU-SF was more than 4 points. Differences in mean PDI scores were tested by one sided t-test.
In consultation with a statistician, a priori it was decided to split the alpha of 0.05 in 0.005 and
calculate a two-sided 99% confi dence interval (CI) for the interim analysis, and 0.045 with a two-
sided 91% CI for fi nal analyses. Because the study was stopped preliminarily, however, only one
analysis was performed for which we used a two-sided 95% CI approach.
Means and SD’s of primary outcome are presented for CAU and CAU-SF group. All statistical
analyses were performed according to an intention to treat analysis and a per protocol analysis.
A CI approach was used to interpret non-inferiority (Figure 1). For PDI and EQ5D scores, 95%
2-sided CIs were used in the fi nal analyses. Non-inferiority was established when the difference in
means was less than 4 (Figure 1). Treatment effects within groups were expressed in standardized
mean difference (SMD): (meanchange/ SDchange). Effect sizes (ES) were calculated between groups
(meanchange intervention group - meanchange control group)/ SDPooled 12. Interpretation of SMD and ES: <0.10 no
effect; <0.30 little effect; <0.50 moderate effect; <0.80 large effect; >0.80 very large effect 13.
0 4
D
C2
B3
B2
B1
A
Superior Equivalent Non Inferior Inferior
2.53 -2.2 7.3
C1
Figure 1 Illustration of the phenomenon of non-inferiority testingThe dotted horizontal lines represent the theoretical width of the Confi dence Intervals (CI) of the differences in means between experimental group and control group. If the CI lies left of 0: (A) the experimental group is superior to the control group. If CI lies left of 4 (B1, B2, B3) the experimental group is non inferior. If CI includes 4 (C2) non inferiority is inconclusive. If CI lies is right to 4 the experimental group is inferior (D). The statistical analyses of the differences between groups resulted in line C1 with confi dence intervals for -2.2 to 7.3: which means non inferiority is inconclusive
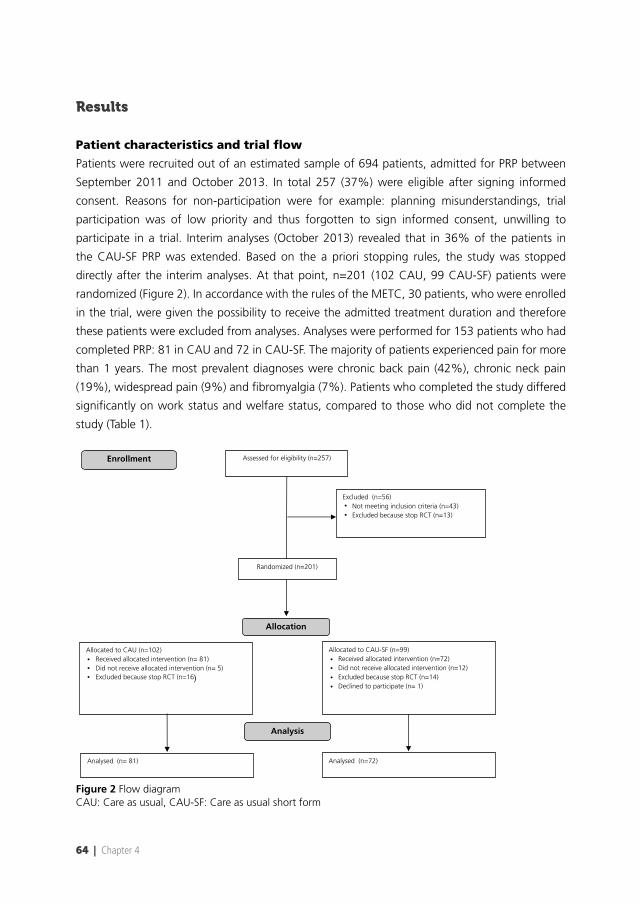
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
64 | Chapter 4
Results
Patient characteristics and trial fl ow
Patients were recruited out of an estimated sample of 694 patients, admitted for PRP between
September 2011 and October 2013. In total 257 (37%) were eligible after signing informed
consent. Reasons for non-participation were for example: planning misunderstandings, trial
participation was of low priority and thus forgotten to sign informed consent, unwilling to
participate in a trial. Interim analyses (October 2013) revealed that in 36% of the patients in
the CAU-SF PRP was extended. Based on the a priori stopping rules, the study was stopped
directly after the interim analyses. At that point, n=201 (102 CAU, 99 CAU-SF) patients were
randomized (Figure 2). In accordance with the rules of the METC, 30 patients, who were enrolled
in the trial, were given the possibility to receive the admitted treatment duration and therefore
these patients were excluded from analyses. Analyses were performed for 153 patients who had
completed PRP: 81 in CAU and 72 in CAU-SF. The majority of patients experienced pain for more
than 1 years. The most prevalent diagnoses were chronic back pain (42%), chronic neck pain
(19%), widespread pain (9%) and fi bromyalgia (7%). Patients who completed the study differed
signifi cantly on work status and welfare status, compared to those who did not complete the
study (Table 1).
Assessed for eligibility (n=257)
Excluded (n=56) Not meeting inclusion criteria (n=43) Excluded because stop RCT (n=13)
Randomized (n=201)
Analysed (n= 81) Analysed (n=72)
Allocated to CAU-SF (n=99) Received allocated intervention (n=72) Did not receive allocated intervention (n=12) Excluded because stop RCT (n=14) Declined to participate (n= 1)
Allocated to CAU (n=102) Received allocated intervention (n= 81) Did not receive allocated intervention (n= 5) Excluded because stop RCT (n=16)
Enrollment
Allocation
Analysis
••
••
•
••••
Figure 2 Flow diagramCAU: Care as usual, CAU-SF: Care as usual short form
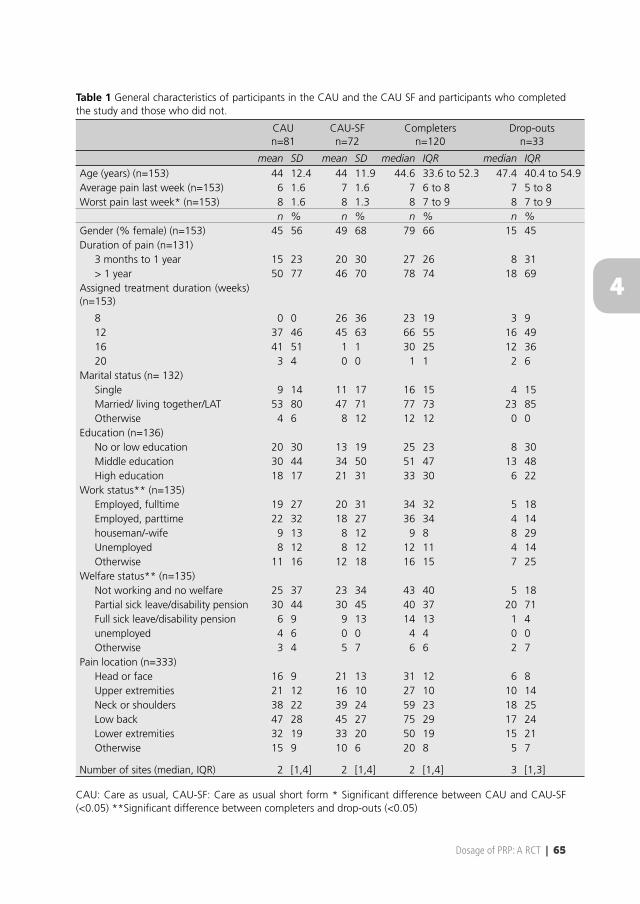
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 65
4
Table 1 General characteristics of participants in the CAU and the CAU SF and participants who completed the study and those who did not.
CAUn=81
CAU-SFn=72
Completersn=120
Drop-outsn=33
mean SD mean SD median IQR median IQRAge (years) (n=153) 44 12.4 44 11.9 44.6 33.6 to 52.3 47.4 40.4 to 54.9Average pain last week (n=153) 6 1.6 7 1.6 7 6 to 8 7 5 to 8Worst pain last week* (n=153) 8 1.6 8 1.3 8 7 to 9 8 7 to 9
n % n % n % n %Gender (% female) (n=153) 45 56 49 68 79 66 15 45Duration of pain (n=131)
3 months to 1 year 15 23 20 30 27 26 8 31> 1 year 50 77 46 70 78 74 18 69
Assigned treatment duration (weeks)(n=153)
8 0 0 26 36 23 19 3 912 37 46 45 63 66 55 16 4916 41 51 1 1 30 25 12 3620 3 4 0 0 1 1 2 6
Marital status (n= 132)Single 9 14 11 17 16 15 4 15Married/ living together/LAT 53 80 47 71 77 73 23 85Otherwise 4 6 8 12 12 12 0 0
Education (n=136)No or low education 20 30 13 19 25 23 8 30Middle education 30 44 34 50 51 47 13 48High education 18 17 21 31 33 30 6 22
Work status** (n=135)Employed, fulltime 19 27 20 31 34 32 5 18Employed, parttime 22 32 18 27 36 34 4 14houseman/-wife 9 13 8 12 9 8 8 29Unemployed 8 12 8 12 12 11 4 14Otherwise 11 16 12 18 16 15 7 25
Welfare status** (n=135)Not working and no welfare 25 37 23 34 43 40 5 18Partial sick leave/disability pension 30 44 30 45 40 37 20 71Full sick leave/disability pension 6 9 9 13 14 13 1 4unemployed 4 6 0 0 4 4 0 0Otherwise 3 4 5 7 6 6 2 7
Pain location (n=333)Head or face 16 9 21 13 31 12 6 8Upper extremities 21 12 16 10 27 10 10 14Neck or shoulders 38 22 39 24 59 23 18 25Low back 47 28 45 27 75 29 17 24Lower extremities 32 19 33 20 50 19 15 21Otherwise 15 9 10 6 20 8 5 7
Number of sites (median, IQR) 2 [1,4] 2 [1,4] 2 [1,4] 3 [1,3]
CAU: Care as usual, CAU-SF: Care as usual short form * Signifi cant difference between CAU and CAU-SF (<0.05) **Signifi cant difference between completers and drop-outs (<0.05)
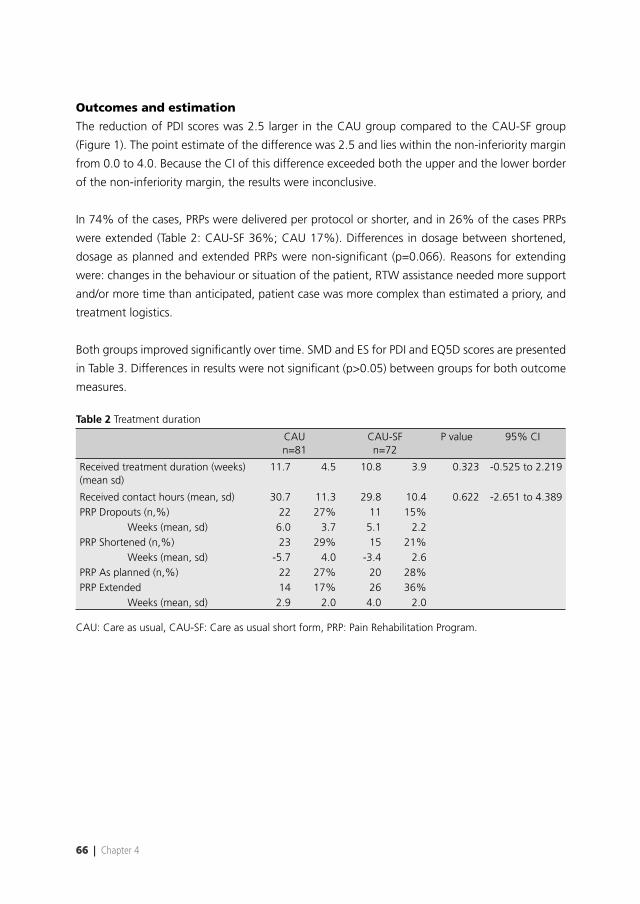
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
66 | Chapter 4
Outcomes and estimation
The reduction of PDI scores was 2.5 larger in the CAU group compared to the CAU-SF group
(Figure 1). The point estimate of the difference was 2.5 and lies within the non-inferiority margin
from 0.0 to 4.0. Because the CI of this difference exceeded both the upper and the lower border
of the non-inferiority margin, the results were inconclusive.
In 74% of the cases, PRPs were delivered per protocol or shorter, and in 26% of the cases PRPs
were extended (Table 2: CAU-SF 36%; CAU 17%). Differences in dosage between shortened,
dosage as planned and extended PRPs were non-signifi cant (p=0.066). Reasons for extending
were: changes in the behaviour or situation of the patient, RTW assistance needed more support
and/or more time than anticipated, patient case was more complex than estimated a priory, and
treatment logistics.
Both groups improved signifi cantly over time. SMD and ES for PDI and EQ5D scores are presented
in Table 3. Differences in results were not signifi cant (p>0.05) between groups for both outcome
measures.
Table 2 Treatment duration
CAUn=81
CAU-SFn=72
P value 95% CI
Received treatment duration (weeks) (mean sd)
11.7 4.5 10.8 3.9 0.323 -0.525 to 2.219
Received contact hours (mean, sd) 30.7 11.3 29.8 10.4 0.622 -2.651 to 4.389PRP Dropouts (n,%) 22 27% 11 15%
Weeks (mean, sd) 6.0 3.7 5.1 2.2PRP Shortened (n,%) 23 29% 15 21%
Weeks (mean, sd) -5.7 4.0 -3.4 2.6PRP As planned (n,%) 22 27% 20 28%PRP Extended 14 17% 26 36%
Weeks (mean, sd) 2.9 2.0 4.0 2.0
CAU: Care as usual, CAU-SF: Care as usual short form, PRP: Pain Rehabilitation Program.
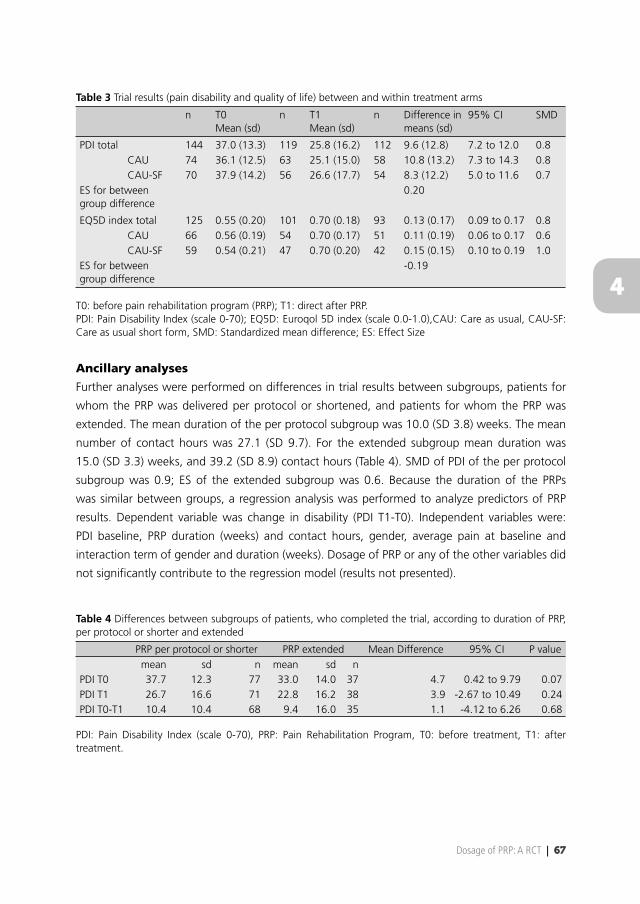
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 67
4
Table 3 Trial results (pain disability and quality of life) between and within treatment arms
n T0Mean (sd)
n T1Mean (sd)
n Difference in means (sd)
95% CI SMD
PDI total 144 37.0 (13.3) 119 25.8 (16.2) 112 9.6 (12.8) 7.2 to 12.0 0.8CAU 74 36.1 (12.5) 63 25.1 (15.0) 58 10.8 (13.2) 7.3 to 14.3 0.8CAU-SF 70 37.9 (14.2) 56 26.6 (17.7) 54 8.3 (12.2) 5.0 to 11.6 0.7
ES for between group difference
0.20
EQ5D index total 125 0.55 (0.20) 101 0.70 (0.18) 93 0.13 (0.17) 0.09 to 0.17 0.8CAU 66 0.56 (0.19) 54 0.70 (0.17) 51 0.11 (0.19) 0.06 to 0.17 0.6CAU-SF 59 0.54 (0.21) 47 0.70 (0.20) 42 0.15 (0.15) 0.10 to 0.19 1.0
ES for between group difference
-0.19
T0: before pain rehabilitation program (PRP); T1: direct after PRP.PDI: Pain Disability Index (scale 0-70); EQ5D: Euroqol 5D index (scale 0.0-1.0),CAU: Care as usual, CAU-SF: Care as usual short form, SMD: Standardized mean difference; ES: Effect Size
Ancillary analyses
Further analyses were performed on differences in trial results between subgroups, patients for
whom the PRP was delivered per protocol or shortened, and patients for whom the PRP was
extended. The mean duration of the per protocol subgroup was 10.0 (SD 3.8) weeks. The mean
number of contact hours was 27.1 (SD 9.7). For the extended subgroup mean duration was
15.0 (SD 3.3) weeks, and 39.2 (SD 8.9) contact hours (Table 4). SMD of PDI of the per protocol
subgroup was 0.9; ES of the extended subgroup was 0.6. Because the duration of the PRPs
was similar between groups, a regression analysis was performed to analyze predictors of PRP
results. Dependent variable was change in disability (PDI T1-T0). Independent variables were:
PDI baseline, PRP duration (weeks) and contact hours, gender, average pain at baseline and
interaction term of gender and duration (weeks). Dosage of PRP or any of the other variables did
not signifi cantly contribute to the regression model (results not presented).
Table 4 Differences between subgroups of patients, who completed the trial, according to duration of PRP, per protocol or shorter and extended
PRP per protocol or shorter PRP extended Mean Difference 95% CI P valuemean sd n mean sd n
PDI T0 37.7 12.3 77 33.0 14.0 37 4.7 0.42 to 9.79 0.07PDI T1 26.7 16.6 71 22.8 16.2 38 3.9 -2.67 to 10.49 0.24PDI T0-T1 10.4 10.4 68 9.4 16.0 35 1.1 -4.12 to 6.26 0.68
PDI: Pain Disability Index (scale 0-70), PRP: Pain Rehabilitation Program, T0: before treatment, T1: after treatment.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
68 | Chapter 4
Adverse events
No trial related adverse events were reported.
Discussion
The statistical analyses showed a point estimate difference between groups of 2.5 with CI from
-2.2 to 7.3, which means non-inferiority was inconclusive. Within both groups, short term ES
were moderate to large for outcome measures disability and quality of life. In a quarter of all
cases the duration of PRP could be reduced.
Because of extension of PRP in patients randomized to CAU-SF, this study was not able to detect
differences in dosage or effect. The results could imply that shortening of PRP duration may be
considered in some cases, without loss of short term results. A lower dosage may benefi t patients
and other stakeholders. However, 26% of all PRPs (36% within CAU-SF and 17% within CAU)
were extended to achieve a desired outcome. Extending (and shortening) of PRP was always
agreed upon by the patients and the PRP team, and was a result of a difference between baseline
needs and progress during PRP. At this point in time it is not possible to identify characteristics of
patients whose PRPs were extended or shortened, and thus to plan a correct dosage at the start.
This topic should be subject of further investigation. On the other hand, the results of the extended
subgroup were similar to the per protocol group, indicating that extension of treatment might
not be a solution to improve treatment outcome. Signifi cant differences between completers and
drop-outs may be hypothesized by less motivation of patients with disability compensation or
housewives to complete treatment. However, characteristics of dropouts have not been subject
of study. It is unknown whether this has systematically infl uenced the results of this study.
Because this trial is the fi rst of its kind, the results of this trial cannot be compared to other pain
rehabilitation trials with similar designs. Patient characteristics such as pain disability, pain intensity,
pain duration, gender distribution, appear similar to other PRP trials, both in the Netherlands
and internationally 5, and regular clinical secondary and tertiary rehabilitation programs in the
Netherlands. Dosage of PRP in this study was ‘midrange’ when compared to dosage reported
in other studies 14. The results of this study stress the relevance of further dosage studies in
different settings 5. One of the main challenges expressed in pain rehabilitation is the issue of
‘what works for whom’. We suggest adding another challenge: ‘how much works for whom?’
Within pain rehabilitation, this may apply to the multidisciplinary program as a whole, but also
to its components. This question may open a new line of research that may lead to major new
insights. Because dosage has been a methodological blind spot in PRP research, and dosage
variables were defi ned and interpreted differently across studies, results of previous trials may
have been biased by lack of control for dosage. If A is compared to B and A leads to superior
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 69
4
results, it is expected that A is the treatment of choice. However, theoretically, if the dose of A
was higher than B, the difference also might be explained by under dosage of B 15. Differences
in dosage could also explain differences between studies and could be reasons why some studies
were not able to detect signifi cant differences between interventions 14.
Weaknesses and strengths
Weakness of the study was that it had to be discontinued prematurely because too many PRPs
in de CAU-SF group were extended. This caused lack of contrast regarding dosage between the
CAU and CAU-SF groups, which may explain partly the inconclusiveness of the results. In addition
the small sample size caused wide CI, which also led to inconclusiveness.
Different scenario’s were considered and discussed with the team to shorten the program. CAU
was offered in programs of 8,12,16 and 20 weeks. In absence of evidence, it was decided to test
shortening of PRP with 1 step (4 weeks). This could be considered a methodological weakness
of the study, because the relative impact differed between programs (from 12 to 8 weeks: 33%
reduction, 12 to 16 week: 25% reduction, 20 to 16 weeks: 20% reduction). On the other hand,
adherence to CAU strengthens this study because it reduced the risk of allocation bias in patients
and clinicians.
Extension of treatment duration may be regarded as a limitation or even as adverse event or
program violation. However, during this study, we were obliged to adhere to the Dutch health
care regulations and the Medical Ethics Committee. As a consequence, we were not allowed
to deny health care that was deemed necessary for good patient care. Within the area of pain
rehabilitation there are no guidelines regarding dosage of PRPs. As described in the introduction,
PRPs aim to reduce disability and use of health care services. During PRP patients are coached to
self manage pain and disability. As far as we know there are no published validated measures
to assess these self management skills. Consequently, it is unclear at what point a patient will
be ready to self manage his pain and disability, and when PRP is no longer of added value.
Partly because of lack of evidence regarding dosage of PRP, choices of dosage of PRP are unclear
and arbitrary. This may result in differences in dosage between and within PRP teams. This is a
weakness of this study because, for some cases this resulted in shortening or extending of PRP
in both the CAU and CAU-SF groups. On the other hand, this is an important reason for future
research to focus on the rationale underlying dosage of PRP, including transparency of choices in
dosage of treatment. This should eventually lead to more rational dosage of PRP, including explicit
arguments on which dosage for individual patients is based. This could result in development of
validated measurements to determine dosage of PRP.
A strength of this study is the pragmatic, clinical design; including the struggle of clinical practice
regarding dosage of PRPs. This study shows results of shortening and extending PRPs. Based on
the regression analyses, which showed that dosage did not signifi cantly contribute to the model,
reducing PRP is possible and extending does not automatically lead to better results. As this
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
70 | Chapter 4
was the fi rst trial within pain rehabilitation to study dosage, we suggest replication in different
settings, and that all future trials in this fi eld clearly describe dosage issues to enable future
(meta-)analyses of trial results.
In conclusion, reduction of dosage of PRP did not lead to non-inferior mean results. Because the
CI of the mean difference exceeded both the upper and the lower border of the non-inferiority
margin, the results of this trial are inconclusive.
Acknowledgements
The authors acknowledge the participation of the patients in this study, and the clinical and
support staff of the Pain Rehabilitation Department of the Centre for Rehabilitation of the UMCG.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dosage of PRP: A RCT | 71
4
References
1. Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4. european guidelines for the management of chronic nonspecifi c low back pain. Eur Spine J. 2006;15 Suppl 2:S192-300.
2. Köke A, Brouwers M, Heuts P, et al. Consensus rapport pijnrevalidatie Nederland. 2005.
3. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: A systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
4. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst Rev. 2014;9:CD000963.
5. Waterschoot FP, Dijkstra PU, Hollak N, de Vries HJ, Geertzen JH, Reneman MF. Dose or content? effectiveness of pain rehabilitation programs for patients with chronic low back pain: A systematic review. Pain. 2014;155(1):179-189.
6. Tait RC, Chibnall JT, Krause S. The pain disability index: Psychometric properties. Pain. 1990;40(2):171-182.
7. Gronblad M, Hupli M, Wennerstrand P, et al. Intercorrelation and test-retest reliability of the pain disability index (PDI) and the oswestry disability questionnaire (ODQ) and their correlation with pain intensity in low back pain patients. Clin J Pain. 1993;9(3):189-195.
8. Soer R, Reneman MF, Vroomen PC, Stegeman P, Coppes MH. Responsiveness and minimal clinically important change of the pain disability index in patients with chronic back pain. Spine (Phila Pa 1976). 2012;37(8):711-715.
9. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new fi ve-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736.
10. Soer R, Reneman MF, Speijer BL, Coppes MH, Vroomen PC. Clinimetric properties of the EuroQol-5D in patients with chronic low back pain. Spine J. 2012;12(11):1035-1039.
11. Janssen MF, Pickard AS, Golicki D, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual Life Res. 2013;22(7):1717-1727.
12. Borenstein M. Introduction to meta-analysis. Chichester, UK. Wiley; 2009:421.
13. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988:567.
14. Smeets RJ, Vlaeyen JW, Hidding A, et al. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? fi rst direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7:5.
15. Bendix T, Bendix A, Labriola M, Haestrup C, Ebbehoj N. Functional restoration versus outpatient physical training in chronic low back pain: A randomized comparative study. Spine (Phila Pa 1976). 2000;25(19):2494-2500.

FrrFrananankakaka PPP.C.CC. . WaWaW tetersrsrschchchooooo t,t,t, EEElsslselee innneee BeBeBennnnenenen MMMscscc, HeHeHenrnrnricicaaa R.RR SSSchchchipipphohohorsrsst tt PrPrPreueuupepeper r r MDMDMD,, PhPhPhD,D,D PiiPietetetererer UUU. DiDiDijkjkkststs raaa PPPhDhDhD, JaJaJann H.H.H.B.BB. GGGeeeeeertrtzezez nnn MDMDMD, PhPhPhD,D,D, MMMiccchihihielele FFF. ReReReneneemamaann PhPhPhDDD
SuSuubmbmbmititittetted dd fofofor rr pupupublbbliciicatatatioioionnn

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
74 | Chapter 5
Abstract
There is a large variety in prescribed dosages of pain rehabilitation programs (PRP) but evidence
regarding the optimum dosage is unknown. The aim of this study was to explore perspectives
of patients and rehabilitation professionals regarding dosages (e.g. total duration, number of
contact hours) of PRP in three different rehabilitation centers in the Netherlands. A study using
an explorative qualitative research design was performed with thematic analysis. Individual semi-
structured interviews were conducted with patients undergoing PRP, and focus groups were
formed with rehabilitation professionals involved in PRP. In total, 12 patient interviews and three
focus groups with 17 rehabilitation professionals were analyzed. All patients were satisfi ed with
offered dosage. Several factors were considered important in relation to the choices in dosage of
PRP. All factors were categorized as patient-related factors, treatment-related factors and external
factors. Although dosage of PRP differed among the participating rehabilitation centers, patients
and rehabilitation professionals mentioned similar factors. In absence of evidence, differences in
choices of PRP dosage appear mainly based on historical grounds and clinical expertise.
Keywords
Pain rehabilitation programs, dosage, qualitative analysis, chronic pain.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 75
5
Introduction
Multidisciplinary Pain Rehabilitation Programs (PRPs) are recommended to treat patients with
chronic musculoskeletal pain (CMP) 1,2. These PRPs, based on the biopsychosocial model, aim to
decrease disability and optimize participation of patients with CMP. A systematic review showed
that PRPs have a moderate, but consistent, positive effect on disability and pain, compared to
usual care or physical treatment programs for patients with chronic low back pain 3. PRPs result in
better self-management of pain and disability, and a reduction in healthcare utilization in treated
patients was found, which may contribute to a decrease of direct and indirect costs over the long
term 4.
Although effective, PRPs are relatively expensive. The multidisciplinary characteristics, as well
as the high number of contact hours and total duration of PRP, provide relatively high direct
costs and travel expenses for the patients. An aspect of PRP is dosage, which includes the total
duration, the total number of contact hours, and intensity of treatment (number of contact hours
per week). Differences in the dosage of PRP may lead to differences in direct and indirect costs.
Choices for dosage and how dosage is established for an individual patient is unknown. A recent
systematic review showed that dosage of PRP has never been studied as a primary aim and the
optimum dosage of PRPs is currently unknown 5. The studies included in that review differed in
terms of dosage (total duration, from weeks to months, and regarding contact hours, from fewer
than 10 to over 100 hours) and effect.
Better understanding of dose variables could lead to better and more effi cient patient care, which
will benefi t patients, rehabilitation facilities, insurers and employers. To acquire insight into factors
related to dosage of multidisciplinary PRP, this study aimed at exploring perspectives of patients
who underwent PRP, as well as of the rehabilitation professionals working in PRPs. In addition,
this study aimed at examining the argumentations/reasons and underlying choices in dosage of
PRPs in three rehabilitation centers in the Netherlands.
Methods
A study using an exploratory qualitative design with thematic analyses was used to gain in-depth
information about the perspectives of patients and rehabilitation professionals involved in PRPs
regarding the doses of these programs. The study was performed in three rehabilitation centers in
the Netherlands. These centers were selected because of their differences in dosage, while patient
characteristics were similar 6. Individual semi-structured interviews with patients who underwent
multidisciplinary PRP, as well as focus groups with professionals working in multidisciplinary PRP,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
76 | Chapter 5
were used. The medical ethics committee of the University Medical Center of Groningen (UMCG)
granted a waiver for this study. All participants signed informed consent for participation, digital
recording and the use of data.
Participants
A purposeful sample of patients was recruited from three rehabilitation centers in the Netherlands:
Adelante in Hoensbroek (RC1), located in the south; Roessingh in Enschede (RC2), located in the
east and the Center of Rehabilitation of the UMCG (RC3), located in the north. We aimed at
including patients with varying characteristics, who completed a multidisciplinary PRP: working/
not working, differences in dosage of PRPs, males/females, and a variety of ages. PRP should
have been completed for at least two weeks. The fi rst author contacted the recruited patients via
telephone to check their willingness to participate in the study and to plan the interview. They
received written information about the purpose of the interview.
Rehabilitation professionals from the three rehabilitation centers were included for participation
in the focus groups, provided that they were working within the area of multidisciplinary PRP for
a minimum of two years, for at least 0.5 fte. We aimed to include rehabilitation professionals
from different disciplines (i.e. occupational therapist/ physiotherapist/ psychologist/ physiatrist).
These rehabilitation professionals should be involved in determining the individual dosages of the
program for the patient.
Data collection
Data were collected between May and September 2014. A total sample of 15 patients was
planned for the interviews, fi ve patients from each rehabilitation center, with the expectation
of reaching data saturation. A semi-structured interview scheme was constructed [Appendix]
for patients using open questions enabling refl ection about experiences and perceptions on
dosage of treatment received. The interview started with questions about the total duration
and intensity of PRP, followed by questions regarding personal experiences and perceptions of
treatment dosage, such as: “what did you like and dislike about the duration and intensity of the
program” and “which factors, in your opinion, infl uence dosage of PRP?”. Also patients’ opinion
regarding the relationship of dosage to return to work and personal and general costs were
asked. Face-to-face interviews were performed at the rehabilitation center where the patient was
treated. The interviews were scheduled for 60 minutes and were audio recorded. Prior to this
study, an interview was pilot tested. Patient interviews were planned prior to the focus group at
each center.
For the focus groups meetings, a minimum of fi ve rehabilitation professionals of different
disciplines per center were invited in order to achieve variation in perspectives on PRP dosage per
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 77
5
rehabilitation center. Meetings were planned for 90 to 120 minutes and were audio recorded. An
interview scheme was constructed [Appendix], aiming to gain insight into the line of reasoning
underlying dosage choices, as well as rehabilitation professionals’ perspectives on optimum
dosage of PRPs.
Measures of validity
The fi rst author (FW), who has over 10 years of experience as an occupational therapist in pain
rehabilitation, conducted all patient interviews and also led the focus group meetings in the
Adelante and Roessingh rehabilitation centers. Because she was closely acquainted with the
rehabilitation professionals at UMCG, a psychologist with experience in chronic pain treatment
but who was not involved in PRP of the UMCG led this focus group. The second author (EB)
assisted in all focus groups.
Data analysis
Interviews and focus groups were audio recorded and transcribed verbatim by the fi rst and
second authors (FW and EB). Transcripts were imported into ATLAS.ti, version 5.2, to analyze
data. Thematic analysis was considered as the appropriate approach for identifying, analyzing
and reporting factors related to dosage of PRP 7. Because of the lack of evidence regarding
dosage of rehabilitation programs, especially PRP aimed at behavior change, it was not possible
to provide a detailed theoretical framework. Initially, the fi rst and second authors (FW and EB)
conducted the inductive coding of the interviews and another independent researcher validated
the codes. All codes and quotations were re-analyzed, merged, and renamed.
Results
Participants
In total, 13 patients were interviewed and 12 interviews were analyzed. Initially, fi ve patients
per center were planned, two dropped out because of logistics problems and one was excluded
because the audio was impossible to transcribe. Seventeen rehabilitation professionals participated
in the focus groups (RC1: 5; RC2: 5; RC3: 7). Different disciplines participated: occupational
therapists (4), physiotherapists (3), movement teacher (1), psychologists (4), social workers (2)
and physiatrists (3). The characteristics of participants are described in Table 1. Data saturation
was reached for patient interviews and focus groups for rehabilitation professionals.
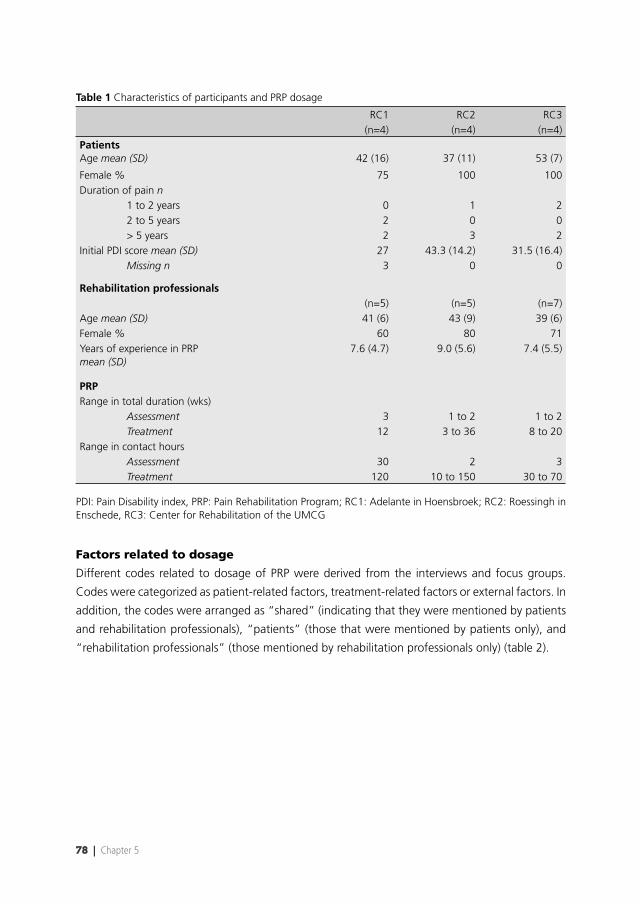
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
78 | Chapter 5
Table 1 Characteristics of participants and PRP dosage
RC1 RC2 RC3(n=4) (n=4) (n=4)
PatientsAge mean (SD) 42 (16) 37 (11) 53 (7)
Female % 75 100 100Duration of pain n
1 to 2 years 0 1 2 2 to 5 years 2 0 0 > 5 years 2 3 2
Initial PDI score mean (SD) 27 43.3 (14.2) 31.5 (16.4)Missing n 3 0 0
Rehabilitation professionals(n=5) (n=5) (n=7)
Age mean (SD) 41 (6) 43 (9) 39 (6)Female % 60 80 71Years of experience in PRP mean (SD)
7.6 (4.7) 9.0 (5.6) 7.4 (5.5)
PRP Range in total duration (wks)
Assessment 3 1 to 2 1 to 2Treatment 12 3 to 36 8 to 20
Range in contact hoursAssessment 30 2 3Treatment 120 10 to 150 30 to 70
PDI: Pain Disability index, PRP: Pain Rehabilitation Program; RC1: Adelante in Hoensbroek; RC2: Roessingh in Enschede, RC3: Center for Rehabilitation of the UMCG
Factors related to dosage
Different codes related to dosage of PRP were derived from the interviews and focus groups.
Codes were categorized as patient-related factors, treatment-related factors or external factors. In
addition, the codes were arranged as “shared” (indicating that they were mentioned by patients
and rehabilitation professionals), “patients” (those that were mentioned by patients only), and
“rehabilitation professionals” (those mentioned by rehabilitation professionals only) (table 2).
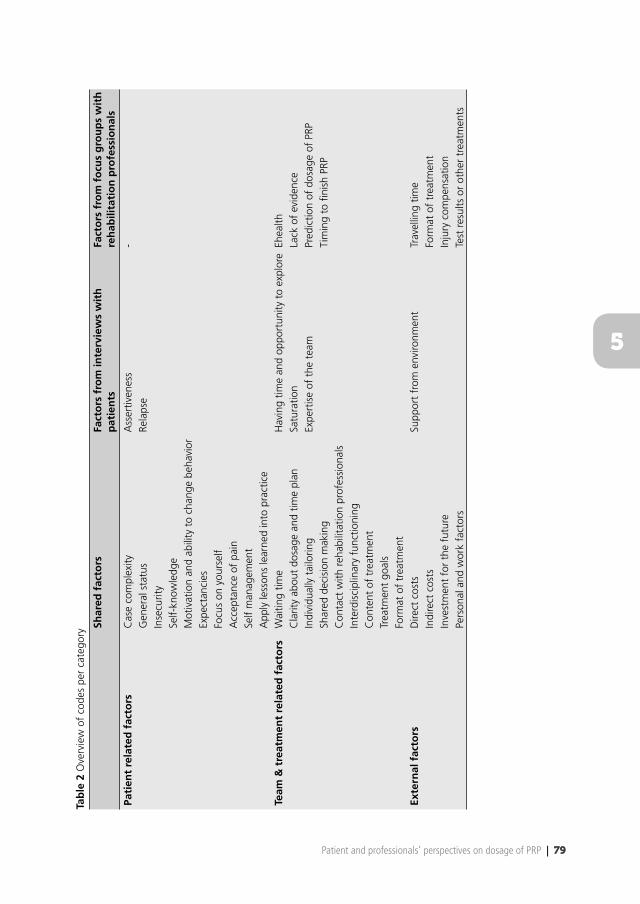
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 79
5
Tab
le 2
Ove
rvie
w o
f co
des
per
cate
gory
Shar
ed f
acto
rsFa
cto
rs f
rom
inte
rvie
ws
wit
h
pat
ien
tsFa
cto
rs f
rom
fo
cus
gro
up
s w
ith
re
hab
ilita
tio
n p
rofe
ssio
nal
s
Pati
ent
rela
ted
fac
tors
Cas
e co
mpl
exity
Ass
ertiv
enes
s-
Gen
eral
sta
tus
Rela
pse
Inse
curit
ySe
lf-kn
owle
dge
Mot
ivat
ion
and
abili
ty t
o ch
ange
beh
avio
rEx
pect
anci
es
Focu
s on
you
rsel
fA
ccep
tanc
e of
pai
nSe
lf m
anag
emen
tA
pply
less
ons
lear
ned
into
pra
ctic
eTe
am &
tre
atm
ent
rela
ted
fac
tors
Wai
ting
time
Hav
ing
time
and
oppo
rtun
ity t
o ex
plor
eEh
ealth
Cla
rity
abou
t do
sage
and
tim
e pl
anSa
tura
tion
Lack
of
evid
ence
Indi
vidu
ally
tai
lorin
gEx
pert
ise
of t
he t
eam
Pred
ictio
n of
dos
age
of P
RPSh
ared
dec
isio
n m
akin
gTi
min
g to
fi ni
sh P
RPC
onta
ct w
ith r
ehab
ilita
tion
prof
essi
onal
sIn
terd
isci
plin
ary
func
tioni
ngC
onte
nt o
f tr
eatm
ent
Trea
tmen
t go
als
Form
at o
f tr
eatm
ent
Exte
rnal
fac
tors
Dire
ct c
osts
Supp
ort
from
env
ironm
ent
Trav
ellin
g tim
eIn
dire
ct c
osts
Form
at o
f tr
eatm
ent
Inve
stm
ent
for
the
futu
reIn
jury
com
pens
atio
n Pe
rson
al a
nd w
ork
fact
ors
Test
res
ults
or
othe
r tr
eatm
ents
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
80 | Chapter 5
Patient-related factors:
Shared factors:
Both patients and rehabilitation professionals mentioned case complexity of a patient as an
important factor related to dosage of PRP as well as an important issue to take into account for
indication of dosage of PRP. Both patients and rehabilitation professionals described characteristics
that affect dosage of PRP, such as the general status (the level of physical condition or the
degree of experienced disability), as well as the degree of insecurity, self-understanding,
motivation and ability to change behavior, in addition to the expectancies patients have
regarding treatment and treatment results. (P3): “It depends on what is going on with someone.
Is he traumatized? Does he want to talk about it? Is he able to manage his problems? Does he
have some self-understanding; does he know what his problem is?”
Both patients and rehabilitation professionals mentioned that PRP requires focusing on
yourself. Patients and rehabilitation professionals involved with both high and low PRP dosages
mentioned this focus as being related to dosage. A patient (P7) who underwent semi-inpatient
PRP described: “The inpatient format of treatment was a good experience. It was quite intense,
but actually very good because you really have to focus on yourself. If I would have been at
home, I would have been distracted by all the things you have to do at home”. Focusing on
oneself and on the treatment was also mentioned by a patient (P9) as motivation for preferring
twice a week PRP instead of once a week: “Yes, two times a week, than you are really engaged
with the treatment. Treatment only once a week…. well, then a whole week is in between…”.
Rehabilitation professionals mentioned that being able or motivated to focus on oneself results
in being motivated to follow the prescribed dosage of PRP. In some cases, for example (T13) “if
a patient is overloaded”, being able to focus on oneself is a motivation for the choice of dosage
and the format of PRP, such as inpatient PRP.
Acceptance of pain is related to the content of PRP because PRP is aimed at improving function,
not reducing pain. Participants mentioned that PRP contributed to the acceptance of pain and
that patients need time to go through this process of acceptance (P4): “I think the minimum
duration of PRP should be 12 weeks. Especially because you experience a process of change in
which you need time… time to make a start, because after those 12 weeks you still need to go
on for yourself”.
If a patient is able to self-manage his pain and disabilities, participants suggest needing a lower
dosage of PRP compared to a patient that is not able to. A rehabilitation professional in a focus
group (T16) described: “Sometimes the minimum dosage of PRP is just one hour of intake. There
are patients who just need some explanation to self manage their lives again. Being able to self
manage pain is related to patient characteristics and behavior, the way people are, and whether
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 81
5
they are able to cope with their pain and disabilities themselves”. Patients also mentioned that
if they are able to learn the principles of self-management during the process of PRP, they will
ultimately need a lower dosage.
To apply lessons learned into practice, patients need time. This is a motivation of patients and
rehabilitation professionals for dose variables such as total duration of PRP. (P9) “It is a process
which requires time, 6 or 8 weeks… well, that’s quite short…. You need to be aware of things,
you have to practice, adjust and adopt”. Needing time to apply lessons learned was additionally
mentioned with regard to intensity (contact hours per week) and the reduction of intensity
of contact hours during PRP. (T13): “At the end of the program, reducing the intensity of the
program (fewer days or fewer contact hours per week), could support the process of putting the
lessons learned into practice”.
Factors from interviews with patients:
Assertiveness was mentioned by patients with regard to the ability to stand up for themselves.
This code is part of the goals and content of PRP and therefore patients mentioned this in relation
to needing a lower dose when patients are already able to stand up for themselves. However, the
code has also been reported in terms of “shared decision making” regarding dosage of PRP.
(P8) “I had to learn to set boundaries. My day was fully planned and I used to do whatever I was
told, which resulted in being exhausted at the end of the day”. Some patients reported that they
needed support during times of relapse. (P2): “Everything was going well; I also felt it that way.
However, I did not have the feeling that I was ready. I was afraid that I would relapse and that
was why I needed some sessions”.
Factors from focus groups with rehabilitation professionals:
No other patient-related factors were reported by rehabilitation professionals only.
Treatment-related factors:
Shared factors:
Waiting time before and during treatment can infl uence, in a negative or positive way, the
general status of a patient at the start of treatment, therefore having an infl uence on the dose
of PRP. One patient (P1) described how she was able to turn the negative result of the waiting
time into a positive action: ”I had to wait for a long time before start of PRP. For me personally,
it has led to an increase of pain and I became depressed. Consequently, I realized I had to do
something and I started doing things on my own”. Most patients knew the total duration of PRP
beforehand. Patients were satisfi ed with this clarity about dosage and time plan for PRP: (P4)
“I compare it with knowing when to go on holidays: the last week at work you are really into
holidays. With therapy, it is the same – you have a set goal to work on in time”. Nevertheless,
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
82 | Chapter 5
besides structured dosages providing this clarity, participants emphasized that the possibility
of individually tailoring dosage to their needs is important. The individually tailored dosage
is also related to shared decision-making. Patients and rehabilitation professionals attached
value to shared decision-making in terms of PRP dosage. Good contact between patient and
rehabilitation professionals supported therapy and therefore could reduce dosage: (P11): “You
need to have a connection with your rehabilitation professionals; otherwise you will not make
any progress”. However, too many changes in rehabilitation professionals during therapy can
impede the connection, and therefore the process, because: “you have to tell your story again
and again”. Related to this code, patients and rehabilitation professionals mentioned that good
interdisciplinary functioning of the team supported effectiveness and therefore had a positive
infl uence on PRP dosage. (P9): “I experienced that everyone knew who I was and what I needed.
Everyone had read all reports and you did not need to tell the same stories”. Both patients and
rehabilitation professionals made it clear that dosage of PRP was strongly related to the content
of treatment, treatment goals and the format of treatment (e.g. inpatient versus outpatient).
Factors from interviews with patients:
Most patients had the experience of having time and opportunity during PRP to explore
themselves and reach their goals. However, some patients also experienced this as a problem when
the frequency was reduced from fi ve days to two days per week. “Content became more intensive,
everything was put together in two days and everything had to go faster…I had to hurry….”.
Some patients denoted that towards the end of treatment, saturation of treatment content
occurred. Therefore, they suggested that retrospectively, the dosage could have been reduced.
(P2): “At a certain moment, you are done with it”. Patients stated that they trust the expertise
of the team, both with regard to the content of treatment as a prediction of dosage and when
decisions are made regarding the need to prolong or reduce PRP dosage. (P1): “I thought, well if
that is the success of the therapy, then I am going to do it that way”. Rehabilitation professionals
felt that they had to be experts in the fi eld and should offer a high PRP quality. They related this
quality and expertise to content and dosage of PRP.
Factors from focus groups with rehabilitation professionals:
Rehabilitation professionals suggested that different forms of ehealth could infl uence the
dosage of PRP in the near future. “Patients can receive home assignments by mail after intake
and before starting. Also aftercare can be supported by ehealth”. The focus groups revealed that
there was a lack of evidence for the delivered doses of PRP. (T15) “These programs have been
developed and adapted over the years based on skills acquired by the team, and developments
such as group based treatments. This provides certain components in the program. This is what
we have; we did not question ourselves if it is necessary for patients”. Additionally, with that lack
of evidence, it is hard to predict dosage of PRP and to know when the timing is right to fi nish
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 83
5
PRP: “It is a diffi cult decision, at what point a patient is ready, and to reach consensus about this
within the team and also with the patient…. “
External factors:
Shared factors:
Opinions regarding fi nancial factors were of interest to the interviewer. The majority of participants
stated that fi nancial factors should not infl uence dosage of PRP. Patients could imagine that
direct costs that patients have to pay themselves, like travel costs, could be of concern for some
patients, although they did not experience that for themselves. (P11): It is regrettable if your own
development depends on a few Euros extra per month”. Direct costs of therapy and indirect
costs, for example those related to returning to work, should not infl uence treatment because
patients saw the costs of therapy as an investment in the future: (P9): Well, I think, on the
longer term, if therapy works, you save money. It also applies for work: if my boss did not allow
me time for this therapy, I might not yet be at work for 100%”. Personal and work factors
could have a positive or negative infl uence on the opportunity to receive therapy, and therefore
could infl uence the satisfaction or choice for dosage of PRP. Some patients had to adjust their
activities at home to their therapy: (P11): “On therapy days, I did not have the energy to do things
at home. I was happy I made the choice to delegate the household tasks. The days at home I had
time to do things with my children and husband”. A rehabilitation professional mentioned that
sometimes, dosage of therapy can be adjusted to work or personal situations: “If patients are
not able to organize the required dosage of two times a week and they have strong reasons, we
sometimes decide to reduce frequency of treatment to once a week”.
Factors from interviews with patients:
Patients perceived support from environment (e.g. partner, colleagues, employer) as a positive
factor because it helped with completing the program well and spending the time needed for the
program. Lack of support could have a negative infl uence on the effects of the program because
it could interfere with the process of therapy and lead to extension of PRP.
Factors from focus groups with rehabilitation professionals:
In the focus groups, rehabilitation professionals mentioned that travel time could infl uence
the choice of the offered format of treatment, therefore infl uencing the dosage of PRP. “This
center is a center of expertise regarding pain rehabilitation, so patients come from across the
province, which makes outpatient rehabilitation not appropriate”. If the patient received injury
compensation, it sometimes can impede progression in treatment. Therefore, rehabilitation
professionals stated that in some cases, this could be a reason for not starting PRP or for stopping
it prematurely. Test results or other treatments can also infl uence the dosage of PRP: “More
often you see a sort of intermediate treatment if patients need other treatments, like EMDR

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
84 | Chapter 5
….. Or if test results are not available; waiting for these results causes delay” (EMDR is the
abbreviation for Eye Movement Desensitization and Reprocessing; trauma treatment).
Differences and similarities
Interviews and focus groups were performed in three rehabilitation centers across the Netherlands.
All centers offered multidisciplinary PRP for patients with CMP. Although dosages differed per
center, factors were similar for all centers. All patients, in general, mentioned being satisfi ed
with the received dosage, although some had suggestions for improvements related to dosage of
PRP. Rehabilitation professionals reported that they supported the choices for current dosages of
PRP; however they also had suggestions for improvements and implications for further research
in order to eliminate the lack of evidence for an optimal dosage of PRP.
Discussion
As a contribution to gather knowledge about factors related to dosage of PRP, this study provides
insight into perspectives of patients and rehabilitation professionals regarding dosage of PRP.
Several general factors were considered relevant. Overall, all codes could be summarized into
patient, treatment and external factors. Interestingly, despite differences in offered and received
dosages of PRP, these factors were similar across centers with different PRP dosages. For example,
in general, patients need clarity about dosages at the start of PRP. However, during PRP, they
would like to have the opportunity to adapt the dosage to their individual needs, in consultation
with their rehabilitation professionals. Patients and rehabilitation professionals mentioned that
different personal characteristics, such as motivation and ability to change, general status of
a patient, acceptance, and self-understanding, are related to dosage of PRP. However, similar
“ability to change” can lead to 12 weeks, divided into treatment of six weeks, fi ve times a week,
eight hours a day, and six weeks, three times a week, eight hours a day of PRP in RC1, and 12
weeks, twice a week, 2,5 hours a day of PRP in RC3. Remarkably, no explicit reasons for these
differences in choices of dosage were expressed during the focus groups.
Treatment outcome is caused by specifi c and aspecifi c factors of treatment. The content of PRP
is a specifi c factor. Outcome, defi ned as “being satisfi ed” with treatment, is an example of an
aspecifi c factor infl uencing the effect of treatment. The factors in this study regarding dosage
of treatment seemed to be linked both to specifi c and aspecifi c factors. Ehealth and evidence
regarding optimum dosage are specifi c factors which can contribute to better prediction of
dosage and more effi cient PRP. Content and format of treatment, and external factors (e.g. direct
and indirect costs, investment in future, personal and work factors, support, test results) are
specifi c factors infl uencing choices of, and satisfaction with dosage. These specifi c factors could
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 85
5
explain part of the differences in choices of the offered PRP dosage. However, the results of this
study showed that also other, more aspecifi c factors seemed to be relevant although not specifi c
related to dosage.
Some of these latter factors are similar to the common factors analyzed for explaining equivalence
of various treatment approaches 8,9. In a systematic review fi ve categories of common factors
were analyzed in psychotherapy research: patient characteristics, therapist qualities, change
processes, treatment structure and therapeutic relationships 8. Patient characteristics, such as
expectations of patients with chronic pain, are related to outcomes of pain treatment 10-12.
Rosenzweig 9 already in 1934 described the effect of therapy characteristics with the introduction
of the concept of common factors. In physical therapy care, a systematic review analyzing
patient satisfaction concluded that characteristics of the therapist and the process of care were
determinants of satisfaction of musculoskeletal physical therapy care 13. However, the association
between satisfaction and treatment outcome was inconsistent. The category of change processes
consists of, for example, the opportunity for catharsis, practice of new behaviors in a safe
environment, provision of rationale and foster insight 8. These common factors are similar to
the factors identifi ed in this study: having time and opportunity to explore, applying lessons
learned into practice, acceptance of pain, and self-management. Hush et al. 13 also described the
relationship between patient satisfaction and the process and organization of care. Timely and
effi cient treatment, adequate treatment frequency and follow up, patient involvement in decision
making and individualized care were variables of the process of care, contributing to patient
satisfaction. Variables contributing to patient satisfaction regarding the quality and effi ciency
of the organization of care were: good access to services, location, parking and approachable
support staff 13. Communication, as part of the treatment structure 8, is concluded to be an
important factor in healthcare 14. This is in line with the factors “clarity”, “shared decision-
making” and “contact with rehabilitation professionals” mentioned by patients and professionals
in this study. Communication based on patient-centered care strategies, is also associated with a
stronger therapeutic relationship 15. In addition, studies have analyzed therapeutic relationships as
important common factors that could be related to the effects of different healthcare treatments 16-18. All common factors were analyzed in different contexts of treatments and in the associations
between different variables of treatment. Remarkably, however, in this study with similar contexts
and aims of PRP, similar common factors led to different dosages of PRP. Therefore, it is a challenge
to analyze the effect of the different components of PRP on outcome.
As a result of the lack of evidence regarding dosage of PRP, as mentioned in the focus groups,
all rehabilitation centers made different choices regarding dosage. These choices were based
on different motives related to content, dosage, and composition at the time of developing
the multidisciplinary PRP. Over time, dosage was adapted because of changes in society, costs,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
86 | Chapter 5
experiences, and new insights related to content or format of therapy. At present, no evidence
can support the choices of dosage of PRP and therefore, rehabilitation professionals are not able
to rationally choose optimum dosage of PRP.
Strengths and limitations
Analyzing factors associated with dosage using a qualitative method from the perspective of
patients and rehabilitation professionals is considered a strength of this study because it is the
fi rst study providing an overview of factors related to dosage from patient and professionals’
perspectives. Taking into account three different rehabilitation centers with different dosages of
PRP and similar content across the Netherlands is a strength because this provides insight into the
differences and similarities regarding perspectives of dosage, resulting in similar factors regardless
of variety in the offered dosage. Although this study was performed in three different centers, it
focused solely on centers in the Netherlands, limiting generalization to PRPs performed in centers
in other countries. In addition, the qualitative nature of this study resulted in perspectives of
patients and rehabilitation professionals and cannot simply be generalized to all other groups
of patients and rehabilitation professionals involved in PRPs. For example, we were not able to
include more male patient participants. Although, the majority of patients in PRP are female,
more male patient participants would have improved comparability to clinical practice.
Recommendations
This study is an initial exploration of the perspectives of patients and rehabilitation professionals
regarding PRP dosage. It resulted in an overview of factors that can be used for future research
and clinical practice regarding PRP dosage. The overview can contribute to further analysis of
these factors and their relationship to dosage. Also, it can improve the awareness of these factors
related to dosage of PRP in clinical practice. The results indicate that factors other than content
and dosage of PRP were perceived as being important factors by patients and rehabilitation
professionals. Clinical practice can be improved by taking these other factors into account as
contributors to the overall success of PRP.
Conclusion
This study shows that, although dosage of PRP differed, patients and rehabilitation professionals
generally mentioned the same factors related to characteristics of patients and treatment, as well
as similar external factors. In absence of evidence, differences in choices of PRP dosage appear
mainly based on historical grounds and clinical expertise. Therefore, research is needed to guide
choices of optimum PRP dosage.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 87
5
Acknowledgements
The authors would like to thank all patients and rehabilitation professionals who participated
in the interviews and focus groups at all three rehabilitation centers. They also extend their
appreciation to Ernst Schrier for leading the focus group and Annemieke de Jong and Suzanne
Broekema for their support with data analysis.
Confl ict of interest
We certify that no party having a direct interest in the results of the research supporting this
article has or will confer a benefi t on us or on any organization with which we are associated.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
88 | Chapter 5
References
1. Turk DC. Clinical effectiveness and cost-effectiveness of treatments for patients with chronic pain. Clin J Pain. 2002;18(6):355-365.
2. Airaksinen O, Brox JI, Cedraschi C, et al. Chapter 4. European guidelines for the management of chronic nonspecifi c low back pain. Eur Spine J. 2006;15 Suppl 2:S192-300.
3. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. 2015;350:h444.
4. Lambeek LC, van Tulder MW, Swinkels IC, Koppes LL, Anema JR, van Mechelen W. The trend in total cost of back pain in the Netherlands in the period 2002 to 2007. Spine (Phila Pa 1976). 2011;36(13):1050-1058.
5. Waterschoot FP, Dijkstra PU, Hollak N, de Vries HJ, Geertzen JH, Reneman MF. Dose or content? effectiveness of pain rehabilitation programs for patients with chronic low back pain: A systematic review. Pain. 2014;155(1):179-189.
6. Preuper HR, Boonstra AM, Wever D, et al. Differences in the relationship between psychosocial distress and self-reported disability in patients with chronic low back pain in six pain rehabilitation centers in the netherlands. Spine (Phila Pa 1976). 2011;36(12):969-976.
7. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006;3(2):77-101.
8. Grencavage LM, Norcross JC. Where are the commonalities among the therapeutic common factors? Professional Psychology: Research and Practice. 1990;21(5):372-378.
9. Rosenzweig S. Some implicit common factors in diverse methods of psychotherapy. Journal of Psychotherapy Integration. 2002;12(1):5-9.
10. Kalauokalani D, Cherkin DC, Sherman KJ, Koepsell TD, Deyo RA. Lessons from a trial of acupuncture and massage for low back pain: Patient expectations and treatment effects. Spine (Phila Pa 1976). 2001;26(13):1418-1424.
11. Bhana N, Thompson L, Alchin J, Thompson B. Patient expectations for chronic pain management. J Prim Health Care. 2015;7(2):130-136.
12. Burns JW, Nielson WR, Jensen MP, Heapy A, Czlapinski R, Kerns RD. Specifi c and general therapeutic mechanisms in cognitive behavioral treatment of chronic pain. J Consult Clin Psychol. 2015;83(1):1-11.
13. Hush JM, Cameron K, Mackey M. Patient satisfaction with musculoskeletal physical therapy care: A systematic review. Phys Ther. 2011;91(1):25-36.
14. Roberts L, Bucksey SJ. Communicating with patients: What happens in practice? Phys Ther. 2007;87(5):586-594.
15. Pinto RZ, Ferreira ML, Oliveira VC, et al. Patient-centred communication is associated with positive therapeutic alliance: A systematic review. J Physiother. 2012;58(2):77-87.
16. Burns JW, Glenn B, Lofl and K, Bruehl S, Harden RN. Stages of change in readiness to adopt a self-management approach to chronic pain: The moderating role of early-treatment stage progression in predicting outcome. Pain. 2005;115(3):322-331.
17. Ferreira PH, Ferreira ML, Maher CG, Refshauge KM, Latimer J, Adams RD. The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Phys Ther. 2013;93(4):470-478.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Patient and professionals’ perspectives on dosage of PRP | 89
5
18. Degnan A, Seymour-Hyde A, Harris A, Berry K. The role of therapist attachment in alliance and outcome: A systematic literature review. Clin Psychol Psychother. 2014.

FrFrF ananankakak PP.CCC. WaWaWatetetersrsrschchchoooooot,t,t, EEElslsselele innne e BeBeBennnnnnenenen MMMsccsc,,, LuLuLucacacas ss H.HH V.VV vvananan dddereer WWWououo dedede PPPhDhDhD,HeHeHenrnn iccaaa R.R.R. SSSchchchipipiphohohorsrsrst t PrPrreueeupepep r rr MDMDMD,, PhPhPhD,D,D, MMMiccchihhielele FFF. ReeRenenemamannn PhPPhD.DD
AcAcccececeptptptededed IIntntnt JJ RRRehehehabababiliil RRReseses

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
92 | Chapter 6
Abstract
Assessment of case complexity of patients with chronic non-specifi c musculoskeletal pain (CMP)
is currently clinician based, not transparent and with low reliability. The objective of this study was
to explore case complexity and to initiate development of a Case Complexity Index (CCI).
A three-round Delphi study among clinicians involved in multidisciplinary Pain Rehabilitation
Programs was performed to identify important factors which are assumed to infl uence functioning
in patients with CMP. The 10 most important factors were used to initiate development of a CCI
with the mean ratings of importance per factor as weights. The feasibility of the CCI was tested
in a pilot study on 16 patients with CMP.
In the fi rst round, 166 factors were identifi ed; in the second round, the 10 most important factors
were selected; in the third round, relative weights of each factor were calculated, ranging from
1.75 (features of complaints) to 3.56 (psychiatric disorders) on a scale of 0 (no weight) to 4 (very
heavy weight). The assessments for the factors were mainly based on clinical examination and
reasoning. Clinicians could rate all patients using the CCI, which establish feasibility of the CCI.
Ten, mainly psychosocial factors were identifi ed, which were assumed to be most important for
assessment of case complexity of a patient with CMP. With these factors a CCI was created for
which feasibility was established. This CCI is transparent, easy to use and might provide a basis
for further developments of a structured assessment of case complexity, which may have scientifi c
and clinical relevance.
Keywords
Chronic pain, chronic non-specifi c musculoskeletal pain, multidisciplinary pain rehabilitation
program, case complexity, complexity index, Delphi technique

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 93
6
Introduction
Development of chronic non-specifi c musculoskeletal pain (CMP) is often explained with the
biopsychosocial model, because interacting factors may be involved infl uencing CMP and its
consequences 1,2. The number of factors and their relative involvement creates a highly variable
case complexity of patients with CMP.
Due to the multifactorial nature of the problem, a multidisciplinary approach is needed to treat
patients with CMP. Multidisciplinary Pain Rehabilitation Programs (PRP) are effective in improving
pain and daily functioning in patients with CMP 3, but improvement is modest. PRPs are highly
variable and optimal content and dosage are unknown 4. To analyze the clinical situation of
patients eligible for PRP, to set goals and to estimate dosage of PRP, clinicians assess the case
complexity of patients. This study defi ned case complexity as the extent to which combinations
of factors infl uence functioning of patients with CMP. It comprises both a number of factors
and their relative weight. Theoretically, a patient presenting a large number of factors that each
weigh heavily, is considered a more complex case than a patient with fewer factors that weigh
lighter. Complex cases might need different treatment and different dosage of PRP than low
complex cases. A patient presenting only one heavy weight factor could need high dosage of
mono-disciplinary therapy, but will not be considered as complex case for this study, because
there is only one factor infl uencing functioning. This patient is not eligible for PRP. Although
never investigated, for the evaluation of PRPs, case complexity could be considered as potential
moderator, because besides infl uencing content of treatment it might also infl uence dosage.
However, we are presently unable to reliably and validly assess case complexity, and therefore
unable to test relationships between case complexity and dosage of PRP.
Case complexity of patients admitted to PRPs, is currently assessed ‘intuitively’ by clinicians, partly
based on validated questionnaires. However, psychometric properties of the fi nal complexity
assessment are unknown. A standardized, transparent and psychometrically sound method
assessing case complexity specifi cally for patients with CMP is unavailable. In the Netherlands,
the Workgroup Pain Rehabilitation Netherlands (WPN) developed a four level classifi cation system
for case complexity of patients with CMP 5 (textbox 1). Patients with WPN level 3 or 4 are eligible
for PRP. While this classifi cation is considered as gold standard for the complexity assessment by
rehabilitation specialists in the Netherlands, its criteria are not described, lack transparency and
objectivity, and has moderate interrater reliability 6. Moreover, differentiation is low because levels
are very wide, and PRP content and dosage cannot be derived from this classifi cation. Thus, a
standardized, transparent and psychometrically sound method to assess case complexity will help
improve PRP scientifi cally and clinically.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
94 | Chapter 6
Textbox 1 Defi nitions of WPN levels (author’s translation)
WPN level Criteria1 Patients with pain and (imminent) limitations in activities without infl uence on (work)
participation, no or minimal psychosocial problems.
2 Patients with pain and limitations in activities and (work) participation, no or minimal psychosocial problems.
3 Patients with pain and limitations in activities and (work) participation, psychosocial problems that have moderate to severe infl uence on the (self-reported) level of functioning.
4 Patients with pain and limitations in activities and (work) participation, psychosocial problems that have very severe infl uence on the (self-reported) level of functioning.
The objectives of this study were to:
1. Explore the most important factors infl uencing case complexity of patients with CMP eligible
for PRP.
2. Initiate development of a Case Complexity Index (CCI) based on factors, deemed most
relevant by clinicians.
3. Explore means of assessment used to determine the relevance of CCI individual factors.
4. Test the CCI feasibility.
Materials and Methods
A 3-round online Delphi study was conducted among clinicians working in PRPs in the Netherlands.
Participants
Rehabilitation specialists were selected through purposive sampling and invited by email. The
rehabilitation specialists were asked to invite physiotherapists, psychologists and occupational
therapists from their rehabilitation team to participate (snowball sampling). Rehabilitation
specialists, physiotherapists, psychologists and occupational therapists who were for more than
two years substantially (0.5 FTE or more) involved in a PRP for patients with CMP were considered
experts for this Delphi study. The experts worked in rehabilitation centres spatially dispersed across
the country. For the sample size in a Delphi study there are no strict rules, but a minimum sample
size of 10-15 for a homogenous group of experts has been suggested 7. Because the sample
consisted of four different disciplines, a minimal sample size of 10 in each discipline was chosen.
First round
Objective: to determine all factors that are assumed to infl uence the case complexity of patients
eligible for multidisciplinary PRP. The experts were sent a link to an online survey. This survey
consisted of one open question in which the experts were asked to list all factors that might
infl uence case complexity.
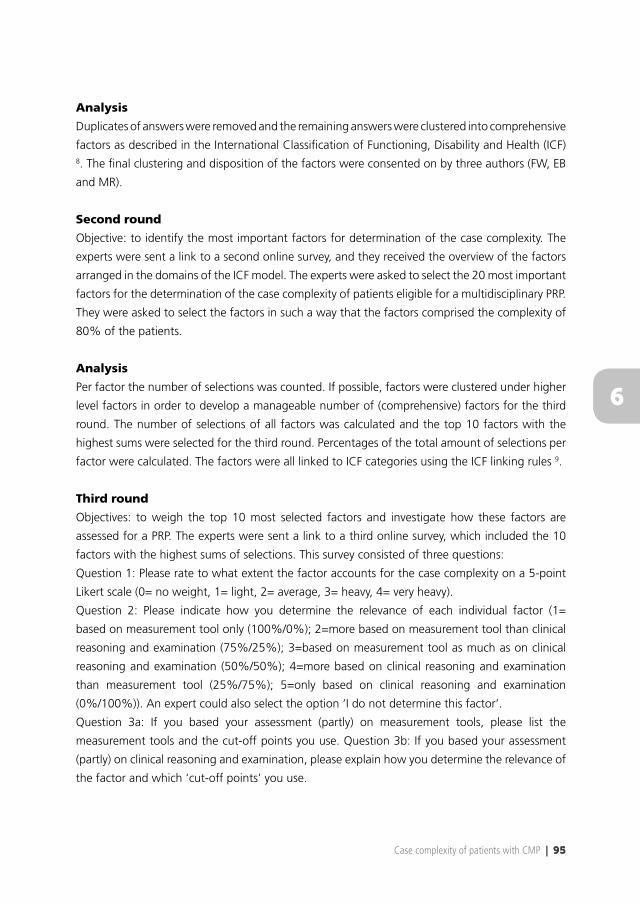
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 95
6
Analysis
Duplicates of answers were removed and the remaining answers were clustered into comprehensive
factors as described in the International Classifi cation of Functioning, Disability and Health (ICF) 8. The fi nal clustering and disposition of the factors were consented on by three authors (FW, EB
and MR).
Second round
Objective: to identify the most important factors for determination of the case complexity. The
experts were sent a link to a second online survey, and they received the overview of the factors
arranged in the domains of the ICF model. The experts were asked to select the 20 most important
factors for the determination of the case complexity of patients eligible for a multidisciplinary PRP.
They were asked to select the factors in such a way that the factors comprised the complexity of
80% of the patients.
Analysis
Per factor the number of selections was counted. If possible, factors were clustered under higher
level factors in order to develop a manageable number of (comprehensive) factors for the third
round. The number of selections of all factors was calculated and the top 10 factors with the
highest sums were selected for the third round. Percentages of the total amount of selections per
factor were calculated. The factors were all linked to ICF categories using the ICF linking rules 9.
Third round
Objectives: to weigh the top 10 most selected factors and investigate how these factors are
assessed for a PRP. The experts were sent a link to a third online survey, which included the 10
factors with the highest sums of selections. This survey consisted of three questions:
Question 1: Please rate to what extent the factor accounts for the case complexity on a 5-point
Likert scale (0= no weight, 1= light, 2= average, 3= heavy, 4= very heavy).
Question 2: Please indicate how you determine the relevance of each individual factor (1=
based on measurement tool only (100%/0%); 2=more based on measurement tool than clinical
reasoning and examination (75%/25%); 3=based on measurement tool as much as on clinical
reasoning and examination (50%/50%); 4=more based on clinical reasoning and examination
than measurement tool (25%/75%); 5=only based on clinical reasoning and examination
(0%/100%)). An expert could also select the option ‘I do not determine this factor’.
Question 3a: If you based your assessment (partly) on measurement tools, please list the
measurement tools and the cut-off points you use. Question 3b: If you based your assessment
(partly) on clinical reasoning and examination, please explain how you determine the relevance of
the factor and which ‘cut-off points’ you use.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
96 | Chapter 6
Analysis
Question 1: For each factor, the mean, standard deviation, median and interquartile range (IQR) of
the ratings were calculated. The differences between the four different disciplines were analyzed
by means of the Kruskal-Wallis test. The differences between rehabilitation specialists and the
other disciplines as one group were analyzed by means of the Mann-Whitney U test. Question
2: medians and IQRs were calculated for each factor. Question 3: measurement tools and cut-off
points were listed.
Case Complexity Index
The mean ratings of relevance (Q1, 3rd round), were used to calculate the weights. The weights
were linearly transformed to obtain a CCI on a 0-100 scale. The formula for the complexity index
was formed by calculating the sum of the products of the factors and their mean weights. The
options for the scoring of every individual factor were 0 (not present), 0.5 (partially present) or
1 (fully present), or ‘cannot determine’. The minimum score of the presence of the factors was
0, calculated by scoring every factor 0. The maximum score was 10, calculated by scoring every
factor 1. The minimum total CCI score is 0 (no presence of any factor) and the maximum score is
100 (all factors are fully present).
Feasibility
A feasibility study of the CCI was performed at the University Medical Centre Groningen, Centre
for Rehabilitation. A convenience sample of 16 consecutive patients with CMP who underwent a
clinical assessment for a PRP, was included. The rehabilitation specialists, occupational therapists,
physiotherapists and psychologists acted as assessors by fi lling in a form following the clinical
assessments. The rehabilitation specialists fi lled out the form independently from the other
member of the team. The other members of the team fi lled out the form together during team
meetings after completion of the individual assessments. The form was designed to identify the
WPN level and the presence of the 10 factors of the CCI. The defi nitions of the WPN levels were
provided for this pilot study, each WPN level was divided into three categories: ‘-‘ (light), ‘normal’
(typical) or ‘+’ (severe). For the CCI, the assessors scored every factor to what extent the factor
was present, based the clinical judgement. The options were: ‘not present’ (score 0), ‘partially
present’ (0.5), ‘fully present’ (1.0) and ‘cannot determine’. The option ‘cannot determine’ was
considered as a missing value.
Analysis
CCI was calculated for every patient. To deal with the missing values, two methods were used:
(1) Fully Conditional Specifi cation Method in SPSS to replace the missing values (imputation), and
(2) dividing the complexity index by the number of fi lled in factors (mean complexity index). The
medians, means and standard deviations of the values of the factors, complexity index and WPN
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 97
6
level were calculated. Spearman’s rho was calculated between CCI and WPN level. To investigate
the relevance of the factors without the weights, Spearman’s rho was calculated between the
unweighted CCI (sum of the values of the factors for every patient) and the WPN level. The
analyses were conducted separately for the rehabilitation specialists and treatment team. The
interrater agreement between the rehabilitation specialists and treatment team on the WPN level
and the assessment of the factors was assessed by calculating Kappa with linear weighting.
Results
Participants
A total of 52 experts participated in the Delphi study: 21 rehabilitation specialists, 12 physical
therapists, 11 occupational therapists and 8 psychologists. Round 1: 44 experts; 17 rehabilitation
specialists, 11 occupational therapists, 10 physical therapists and 6 psychologists. Round 2: 41
experts (response rate= 93.2%); 16 rehabilitation specialists, 9 occupational therapists, 9 physical
therapists and 7 psychologists. Round 3: 36 experts (response rate= 81.8%); 13 rehabilitation
specialists, 9 occupational therapists, 8 physical therapists and 6 psychologists. The experts
worked in 15 rehabilitation centres in 11 out of 12 provinces in the Netherlands. Three non-
responding experts declared that lack of time was their reason for not responding.
First round
After removal of duplicates, the experts listed a total of 166 factors that were deemed important
for the determination of the case complexity (Appendix 1).
Second round
All experts selected 20 factors which they deemed most relevant for determining the case
complexity. Three experts selected less than 20 factors, which resulted in a total of 802 selections.
The majority of unique selections were clustered into 25 (comprehensive) factors in the second
round. The top 10 most selected factors are presented in table 1. These 10 factors represent
59.1% of the total amount of selections. Appendix 2 shows the defi nitions of the 10 factors.
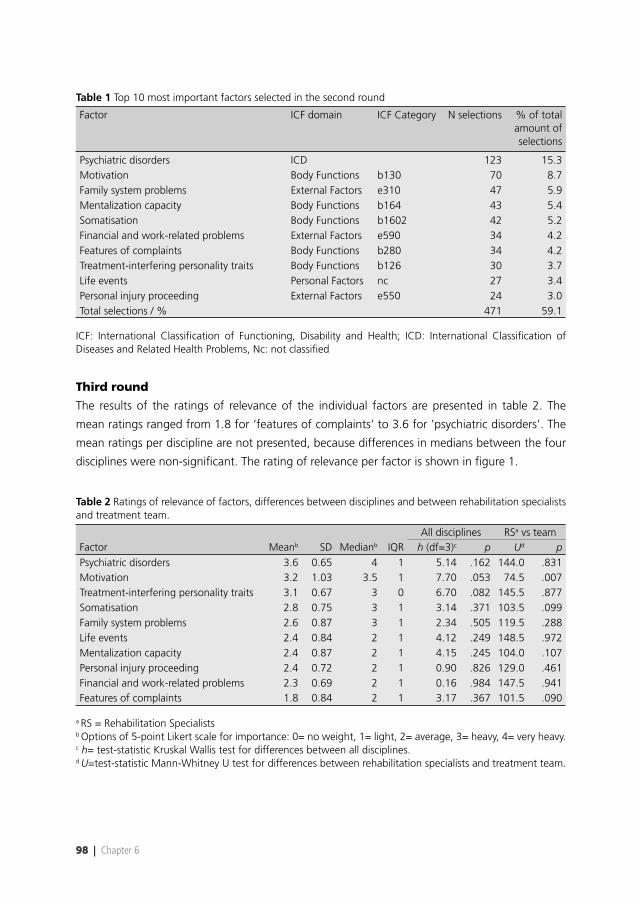
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
98 | Chapter 6
Table 1 Top 10 most important factors selected in the second round
Factor ICF domain ICF Category N selections % of total amount of selections
Psychiatric disorders ICD 123 15.3Motivation Body Functions b130 70 8.7Family system problems External Factors e310 47 5.9Mentalization capacity Body Functions b164 43 5.4Somatisation Body Functions b1602 42 5.2Financial and work-related problems External Factors e590 34 4.2Features of complaints Body Functions b280 34 4.2Treatment-interfering personality traits Body Functions b126 30 3.7Life events Personal Factors nc 27 3.4Personal injury proceeding External Factors e550 24 3.0Total selections / % 471 59.1
ICF: International Classifi cation of Functioning, Disability and Health; ICD: International Classifi cation of Diseases and Related Health Problems, Nc: not classifi ed
Third round
The results of the ratings of relevance of the individual factors are presented in table 2. The
mean ratings ranged from 1.8 for ‘features of complaints’ to 3.6 for ’psychiatric disorders’. The
mean ratings per discipline are not presented, because differences in medians between the four
disciplines were non-signifi cant. The rating of relevance per factor is shown in fi gure 1.
Table 2 Ratings of relevance of factors, differences between disciplines and between rehabilitation specialists and treatment team.
All disciplines RSa vs teamFactor Meanb SD Medianb IQR h (df=3)c p Ud pPsychiatric disorders 3.6 0.65 4 1 5.14 .162 144.0 .831Motivation 3.2 1.03 3.5 1 7.70 .053 74.5 .007Treatment-interfering personality traits 3.1 0.67 3 0 6.70 .082 145.5 .877Somatisation 2.8 0.75 3 1 3.14 .371 103.5 .099Family system problems 2.6 0.87 3 1 2.34 .505 119.5 .288Life events 2.4 0.84 2 1 4.12 .249 148.5 .972Mentalization capacity 2.4 0.87 2 1 4.15 .245 104.0 .107Personal injury proceeding 2.4 0.72 2 1 0.90 .826 129.0 .461Financial and work-related problems 2.3 0.69 2 1 0.16 .984 147.5 .941Features of complaints 1.8 0.84 2 1 3.17 .367 101.5 .090
a RS = Rehabilitation Specialistsb Options of 5-point Likert scale for importance: 0= no weight, 1= light, 2= average, 3= heavy, 4= very heavy.c h= test-statistic Kruskal Wallis test for differences between all disciplines. d U=test-statistic Mann-Whitney U test for differences between rehabilitation specialists and treatment team.
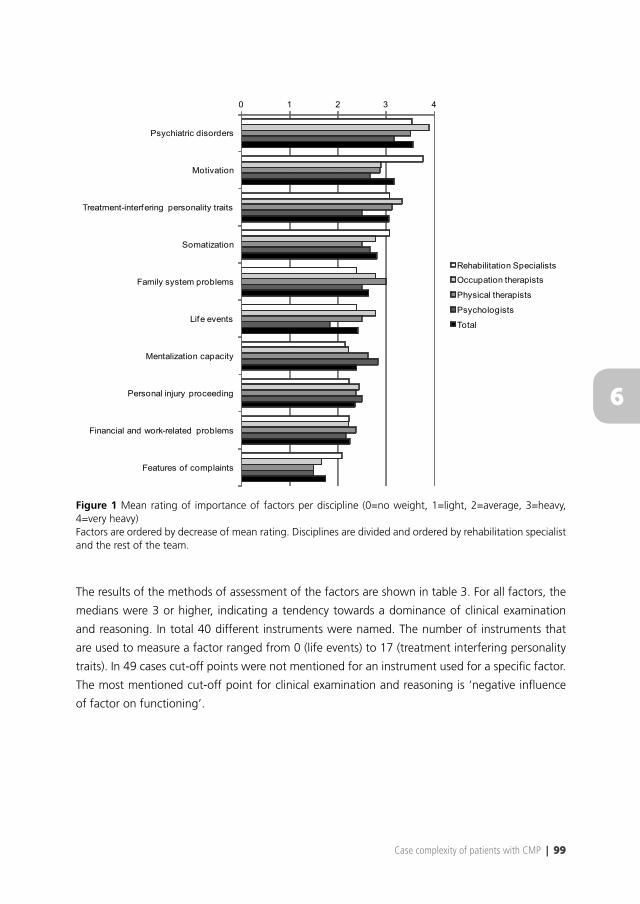
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 99
6
0 1 2 3 4
Psychiatric disorders
Motivation
Treatment-interfering personality traits
Somatization
Family system problems
Life events
Mentalization capacity
Personal injury proceeding
Financial and work-related problems
Features of complaints
Rehabilitation Specialists
Occupation therapists
Physical therapists
Psychologists
Total
Figure 1 Mean rating of importance of factors per discipline (0=no weight, 1=light, 2=average, 3=heavy, 4=very heavy)Factors are ordered by decrease of mean rating. Disciplines are divided and ordered by rehabilitation specialist and the rest of the team.
The results of the methods of assessment of the factors are shown in table 3. For all factors, the
medians were 3 or higher, indicating a tendency towards a dominance of clinical examination
and reasoning. In total 40 different instruments were named. The number of instruments that
are used to measure a factor ranged from 0 (life events) to 17 (treatment interfering personality
traits). In 49 cases cut-off points were not mentioned for an instrument used for a specifi c factor.
The most mentioned cut-off point for clinical examination and reasoning is ‘negative infl uence
of factor on functioning’.
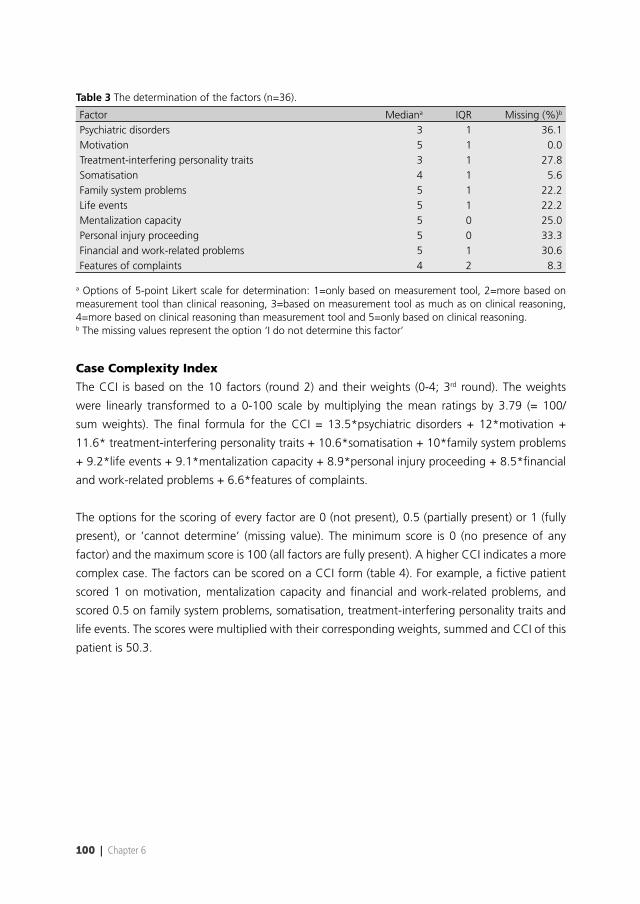
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
100 | Chapter 6
Table 3 The determination of the factors (n=36).
Factor Mediana IQR Missing (%)b
Psychiatric disorders 3 1 36.1Motivation 5 1 0.0Treatment-interfering personality traits 3 1 27.8Somatisation 4 1 5.6Family system problems 5 1 22.2Life events 5 1 22.2Mentalization capacity 5 0 25.0Personal injury proceeding 5 0 33.3Financial and work-related problems 5 1 30.6Features of complaints 4 2 8.3
a Options of 5-point Likert scale for determination: 1=only based on measurement tool, 2=more based on measurement tool than clinical reasoning, 3=based on measurement tool as much as on clinical reasoning, 4=more based on clinical reasoning than measurement tool and 5=only based on clinical reasoning. b The missing values represent the option ‘I do not determine this factor’
Case Complexity Index
The CCI is based on the 10 factors (round 2) and their weights (0-4; 3rd round). The weights
were linearly transformed to a 0-100 scale by multiplying the mean ratings by 3.79 (= 100/
sum weights). The fi nal formula for the CCI = 13.5*psychiatric disorders + 12*motivation +
11.6* treatment-interfering personality traits + 10.6*somatisation + 10*family system problems
+ 9.2*life events + 9.1*mentalization capacity + 8.9*personal injury proceeding + 8.5*fi nancial
and work-related problems + 6.6*features of complaints.
The options for the scoring of every factor are 0 (not present), 0.5 (partially present) or 1 (fully
present), or ‘cannot determine’ (missing value). The minimum score is 0 (no presence of any
factor) and the maximum score is 100 (all factors are fully present). A higher CCI indicates a more
complex case. The factors can be scored on a CCI form (table 4). For example, a fi ctive patient
scored 1 on motivation, mentalization capacity and fi nancial and work-related problems, and
scored 0.5 on family system problems, somatisation, treatment-interfering personality traits and
life events. The scores were multiplied with their corresponding weights, summed and CCI of this
patient is 50.3.
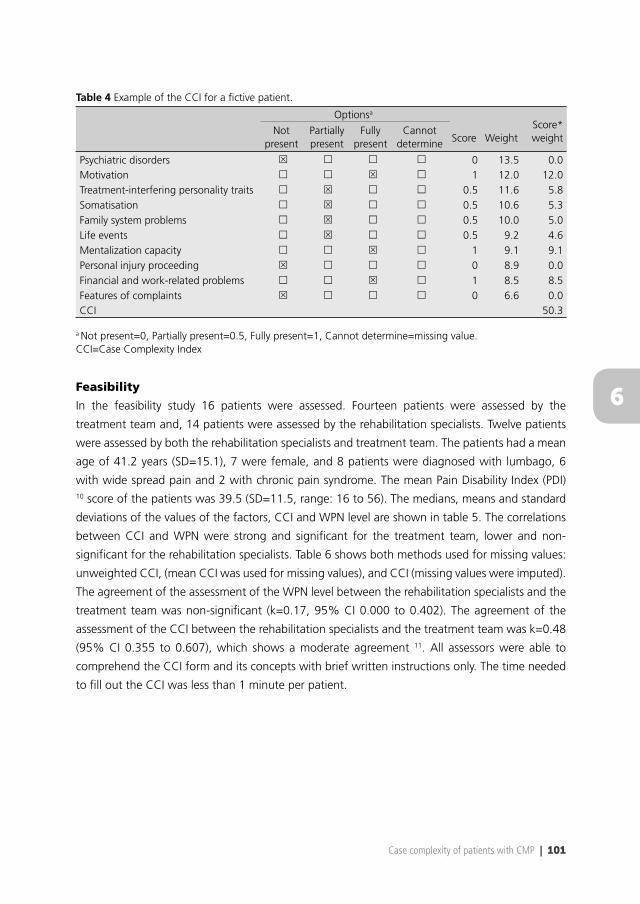
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 101
6
Table 4 Example of the CCI for a fi ctive patient.
Optionsa
Score WeightScore* weight
Not present
Partially present
Fully present
Cannot determine
Psychiatric disorders 0 13.5 0.0Motivation 1 12.0 12.0Treatment-interfering personality traits 0.5 11.6 5.8Somatisation 0.5 10.6 5.3Family system problems 0.5 10.0 5.0Life events 0.5 9.2 4.6Mentalization capacity 1 9.1 9.1Personal injury proceeding 0 8.9 0.0Financial and work-related problems 1 8.5 8.5Features of complaints 0 6.6 0.0CCI 50.3
a Not present=0, Partially present=0.5, Fully present=1, Cannot determine=missing value. CCI=Case Complexity Index
Feasibility
In the feasibility study 16 patients were assessed. Fourteen patients were assessed by the
treatment team and, 14 patients were assessed by the rehabilitation specialists. Twelve patients
were assessed by both the rehabilitation specialists and treatment team. The patients had a mean
age of 41.2 years (SD=15.1), 7 were female, and 8 patients were diagnosed with lumbago, 6
with wide spread pain and 2 with chronic pain syndrome. The mean Pain Disability Index (PDI) 10 score of the patients was 39.5 (SD=11.5, range: 16 to 56). The medians, means and standard
deviations of the values of the factors, CCI and WPN level are shown in table 5. The correlations
between CCI and WPN were strong and signifi cant for the treatment team, lower and non-
signifi cant for the rehabilitation specialists. Table 6 shows both methods used for missing values:
unweighted CCI, (mean CCI was used for missing values), and CCI (missing values were imputed).
The agreement of the assessment of the WPN level between the rehabilitation specialists and the
treatment team was non-signifi cant (k=0.17, 95% CI 0.000 to 0.402). The agreement of the
assessment of the CCI between the rehabilitation specialists and the treatment team was k=0.48
(95% CI 0.355 to 0.607), which shows a moderate agreement 11. All assessors were able to
comprehend the CCI form and its concepts with brief written instructions only. The time needed
to fi ll out the CCI was less than 1 minute per patient.
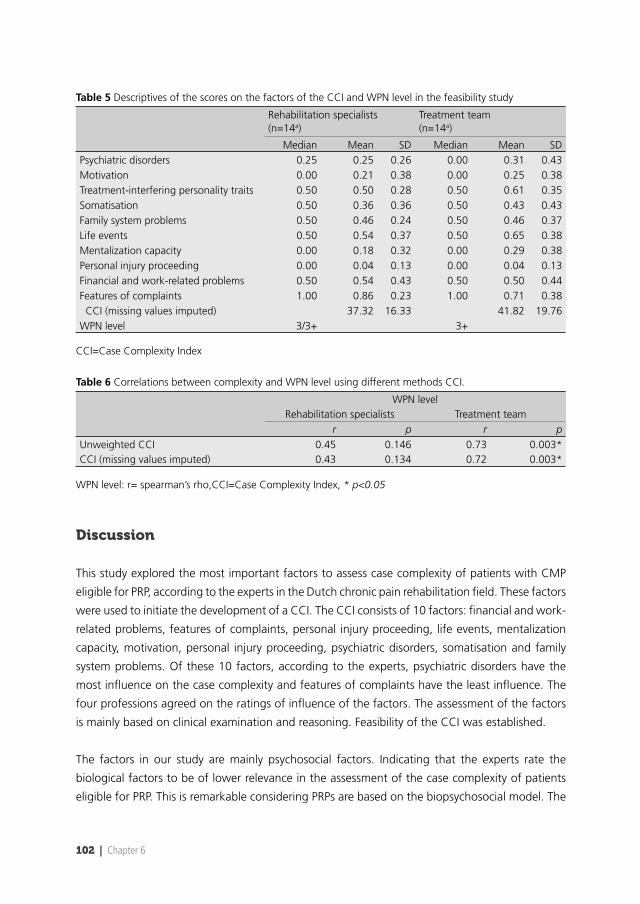
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
102 | Chapter 6
Table 5 Descriptives of the scores on the factors of the CCI and WPN level in the feasibility study
Rehabilitation specialists (n=14a)
Treatment team (n=14a)
Median Mean SD Median Mean SDPsychiatric disorders 0.25 0.25 0.26 0.00 0.31 0.43Motivation 0.00 0.21 0.38 0.00 0.25 0.38Treatment-interfering personality traits 0.50 0.50 0.28 0.50 0.61 0.35Somatisation 0.50 0.36 0.36 0.50 0.43 0.43Family system problems 0.50 0.46 0.24 0.50 0.46 0.37Life events 0.50 0.54 0.37 0.50 0.65 0.38Mentalization capacity 0.00 0.18 0.32 0.00 0.29 0.38Personal injury proceeding 0.00 0.04 0.13 0.00 0.04 0.13Financial and work-related problems 0.50 0.54 0.43 0.50 0.50 0.44Features of complaints 1.00 0.86 0.23 1.00 0.71 0.38 CCI (missing values imputed) 37.32 16.33 41.82 19.76WPN level 3/3+ 3+
CCI=Case Complexity Index
Table 6 Correlations between complexity and WPN level using different methods CCI.
WPN levelRehabilitation specialists Treatment team
r p r pUnweighted CCI 0.45 0.146 0.73 0.003*CCI (missing values imputed) 0.43 0.134 0.72 0.003*
WPN level: r= spearman’s rho,CCI=Case Complexity Index, * p<0.05
Discussion
This study explored the most important factors to assess case complexity of patients with CMP
eligible for PRP, according to the experts in the Dutch chronic pain rehabilitation fi eld. These factors
were used to initiate the development of a CCI. The CCI consists of 10 factors: fi nancial and work-
related problems, features of complaints, personal injury proceeding, life events, mentalization
capacity, motivation, personal injury proceeding, psychiatric disorders, somatisation and family
system problems. Of these 10 factors, according to the experts, psychiatric disorders have the
most infl uence on the case complexity and features of complaints have the least infl uence. The
four professions agreed on the ratings of infl uence of the factors. The assessment of the factors
is mainly based on clinical examination and reasoning. Feasibility of the CCI was established.
The factors in our study are mainly psychosocial factors. Indicating that the experts rate the
biological factors to be of lower relevance in the assessment of the case complexity of patients
eligible for PRP. This is remarkable considering PRPs are based on the biopsychosocial model. The

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 103
6
results of this study showed that there are no unambiguous measurement tools for the factors,
which is in line with a systematic review that there is a large variability in measurement tools for
predictors of outcome of multidisciplinary PRPs for patients with chronic low back pain 12. These
predictors overlapped partially with the factors in the current study.
The CCI is based on a combination of 10 factors, which is a number chosen by the authors to
construct a manageable tool. These factors account for 59.1% of the total number of selections.
Therefore, it does not capture all factors that determine case complexity, but it does contain the
most important factors as viewed by the experts. Also, the case complexity does not take the
interaction between the factors into account. The goal of this Delphi study was to gain insight
into the assessment of the case complexity based on opinions of experts and take fi rst steps to
create a new concept for the assessment of case complexity based on this insight. Therefore, the
results of this Delphi study do not represent “the truth”. It presents an expert view about factors
of case complexity, and a state of the art on how these factors are assessed in rehabilitation
practice. The experts were all from the Netherlands, which may limit generalizations to pain
rehabilitation settings in other countries.
The CCI might be a useful tool for the assessment of the case complexity of patients with CMP.
It is transparent, easy to score, takes very little time to fi ll out and provides a numeric value
to the case complexity. The complexity index can be used by the rehabilitation specialists and
other members of the treatment team. For the assessment of the treatment team, the results
of the pilot study show that the CCI is associated with the WPN level. The CCI is currently still a
rather subjective measure, just as the gold standard WPN method, because the decision on the
presence of each factor is based on clinical reasoning. However the criteria of the CCI are more
specifi c, which can provide a basis for structured assessment of case complexity and stimulation
to validate the decision on assessing each factor. Other advantages of the CCI compared to the
WPN level is the better differentiation between patients, because of its numeric value (0-100)
compared to (broad) categories and the possibility to convert the factors into treatment goals.
On the limitations side, contra-indications for the treatment were not considered. Factors may
be too dominantly present that it cannot be treated with the expertise of a typical PRP team. For
example, a patient with a dominantly present personality disorder that interferes with PRP may
not benefi t from a PRP, and may be better referred to other specialists. Also one factor can be
heavily present, needed much therapy, but need other therapy than multidisciplinary PRP. The
present CCI does not account for this.
Some other attempts to capture complexity have been described the Rehabilitation Complexity
Scale 13, the Vector Model of Complexity 14, COMPRI 15 and INTERMED 16. However none of these
methods are designed to assess case complexity specifi cally for patients with CMP. As stated 17,
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
104 | Chapter 6
there is need for more research to assess case complexity for more specialist rehabilitation
programs for individual patients within the rehabilitation process. The CCI is a more specifi c
measure, only addressing relevant factors for the clinical assessment of patients with CMP who
are eligible for a multidisciplinary PRP and includes factors derived from experts in the fi eld.
Therefore, the factors of the CCI and its score seem to be more appropriate for the use within
this specifi c setting of multidisciplinary PRP.
Our study showed that the assessment is mainly based on clinical examination and reasoning.
Also, the used cut-off points for the clinical examination and assessment are highly variable for
each factor. Because the clinical examination and reasoning will be infl uenced by the assessors’
experiences and beliefs and various implicit cut-off points are used, it is challenging to reach
consensus about the case complexity of an individual patient. In this way, the clinical examination
and reasoning of the assessor will likely infl uence the determined case complexity of a patient.
This can still be the problem with the CCI, which showed a fair interrater agreement between
the rehabilitation specialists and treatment team. However, these results are based on a small
sample size and many different assessors were involved. The defi nitions of the factors were also
not given to the assessors, which may have lead to variability in the interpretation of the factors.
A few assessors were also involved in the Delphi study and therefore had more knowledge of
the factors. These exploratory analyses were performed within the context of feasibility. Clearly,
formal studies are needed to study psychometric properties of the CCI.
The fi rst steps of the development of the CCI have been reported in this paper. However, we
realize that the present CCI is not an end-product. The contribution of each factor to the case
complexity should be tested in a sensitivity analysis. In this analysis other factors should also be
considered. To improve the CCI, it is recommended to objectify the assessment of the individual
factors. For some factors validated instruments are available and these could be incorporated
in the CCI. It might be necessary to have an extra option between ‘partially present’ and ‘fully
present’ for the scoring of the presence of the factors (e.g. similar to the ICF qualifi ers), as there
is a large gap between those options. Because the present CCI represents 59.1% of the case
complexity, the addition of an extra open factor may be considered to facilitate for the 40.9%
that are unaccounted for. Contra-indications for the treatment should be explored and added to
the CCI. The validity, reliability and the practicality of the CCI need to be tested in several settings
to ensure the generalizability within chronic pain rehabilitation. Future research is also needed to
explore the usability of the total CCI score compared to the scores and weights per factor and
analyse relationships of case complexity with dosage of PRPs.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 105
6
Acknowledgements
The authors acknowledge the participation of all experts in the Delphi study and the participation
of the rehabilitation physicians and the other team members in the feasibility study.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
106 | Chapter 6
References
1. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: Scientifi c advances and future directions. Psychol Bull. 2007;133(4):581-624.
2. Dansie EJ, Turk DC. Assessment of patients with chronic pain. Br J Anaesth. 2013;111(1):19-25.
3. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. BMJ. 2001;322(7301):1511-1516.
4. Waterschoot FP, Dijkstra PU, Hollak N, de Vries HJ, Geertzen JH, Reneman MF. Dose or content? effectiveness of pain rehabilitation programs for patients with chronic low back pain: A systematic review. Pain. 2014;155(1):179-189.
5. Köke A, Brouwers M, Heuts P, et al. Consensus rapport pijnrevalidatie Nederland. 2005.
6. Boonstra AM, Schiphorst Preuper HR, Brouwer MAH, Weerdt de M, Knol D, Köke A. Classifi catie van patiënten met chronische pijnklachten: Onderzoek naar de betrouwbaarheid van de WPN niveaus. Ned T Pijnbestrijding. 2011;30:5-10.
7. Delbecq AL, Van de Ven AH, Gustafson DH. Group techniques for program planning: A guide to nominal group and delphi processes. Glenview, Ill: Scott, Foresman; 1975:174.
8. World Health Organization. ICF: International classifi cation of functioning, disability and health. Geneva: World Health Organization; 2001:299.
9. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G. ICF linking rules: An update based on lessons learned. J Rehabil Med. 2005;37(4):212-218.
10. Tait RC, Chibnall JT, Krause S. The pain disability index: Psychometric properties. Pain. 1990;40(2):171-182.
11. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174.
12. van der Hulst M, Vollenbroek-Hutten MM, Ijzerman MJ. A systematic review of sociodemographic, physical, and psychological predictors of multidisciplinary rehabilitation-or, back school treatment outcome in patients with chronic low back pain. Spine (Phila Pa 1976). 2005;30(7):813-825.
13. Turner-Stokes L, Williams H, Siegert RJ. The rehabilitation complexity scale version 2: A clinimetric evaluation in patients with severe complex neurodisability. J Neurol Neurosurg Psychiatry. 2010;81(2):146-153.
14. Safford MM, Allison JJ, Kiefe CI. Patient complexity: More than comorbidity. the vector model of complexity. J Gen Intern Med. 2007;22 Suppl 3:382-390.
15. Huyse FJ, de Jonge P, Slaets JP, et al. COMPRI--an instrument to detect patients with complex care needs: Results from a European study. Psychosomatics. 2001;42(3):222-228.
16. de Jonge P, Huyse FJ, Slaets JP, Sollner W, Stiefel FC. Operationalization of biopsychosocial case complexity in general health care: The INTERMED project. Aust N Z J Psychiatry. 2005;39(9):795-799.
17. Wade D. Complexity, case-mix and rehabilitation: The importance of a holistic model of illness. Clin Rehabil. 2011;25(5):387-395.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Case complexity of patients with CMP | 107
6


R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
110 | Chapter 7
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion | 111
7
The main aim of this thesis was to acquire insight into aspects of dosage for multidisciplinary
Pain Rehabilitation Programs (PRPs) for patients with chronic pain. Five studies were performed.
In this concluding chapter, the main fi ndings and factors related to PRP dosage will be discussed,
followed by clinical, scientifi c and societal implications, strengths and limitations of this thesis and
recommendations for future research.
Main Findings
A systematic review and meta-analysis (Chapter 2) revealed that PRP dosage had never been studied
as a primary objective within pain rehabilitation research. Analyzing studies that investigate the
effects of PRPs and comparing the reported dose variables resulted in an overview of PRPs with
a wide variety of dosages having different outcome measures and effects on disability, quality of
life (QoL) and work participation. Evaluation moment, number of disciplines, type of intervention,
duration of intervention, percentage of women, and age infl uenced the effect of PRP. However,
because dose variables and content variables were strongly interrelated, a distinction between
these variables regarding their effects was impossible.
Chapter 3 describes a clinical study in which the course of disability reduction during PRP was
analyzed. At a group level, the course of disability reduction occurred following a quadratic time
model. This course was infl uenced by initial Pain Disability Index (PDI) scores, treatment week,
average pain, and the interaction between initial PDI scores and treatment week, resulting in, for
example, a steeper slope (faster disability reduction) for patients with higher initial PDI scores and
average pain.
Chapter 4 describes a RCT in which the effects of PRPs with similar content but different dosages
were compared. Frequent extension of the Care as Usual – Short Form (CAU-SF) program led
to exceeding predefi ned stopping rules, and the study had to be stopped prematurely. Because
of lack of power and extension of CAU-SF, differences in dosages between the control and
experimental group were too small to detect signifi cance of non-inferiority. Hence, no robust
conclusions could be drawn. Ancillary regression analysis showed that dose variables did not
contribute to the prediction model, which could be interpreted as a possibility of shortening PRP
without loss of effect.
Chapter 5 describes a study in which patient and therapists’ perceptions were explored regarding
dosages of PRP in three rehabilitation centers in the Netherlands with different dosage of PRP.
Factors that determined the dosage were related to patient, treatment and external factors. The
results showed that although PRPs differed in dosage, perceptions of factors that were important
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
112 | Chapter 7
for determining dosage were similar. Remarkably, similar factors seemed to lead to different
choices in terms of PRP dosage in different centers.
Chapter 6 describes a study in which factors related to the general status, defi ned as case
complexity of patients eligible for PRP, were explored. The 10 most important factors were listed
and weights of infl uence were explored, resulting in a case complexity index (CCI), which was
tested for feasibility in clinical practice. Our hypothesis of a possible relationship between case
complexity and dosage was consistent with the theme of “general status” from the interviews
described in Chapter 5. Patients and rehabilitation professionals mentioned a relationship between
dosage and the general status of a patient, which includes factors similar to the factors in the
CCI. Therefore, it could be assumed that the CCI could be tested in clinical practice to determine
case complexity and to relate this to the prediction of PRP dosage. The relationship between case
complexity and dosage should be tested to confi rm or reject this hypothesis.
Factors associated with PRP dosage
While these fi ve studies have not led to defi nitive conclusions about the optimum PRP dosage, it
has contributed relevant insights regarding factors related to dosage and the effects of PRP. These
can be divided into 1: factors related to the effect of PRP; 2: patient related factors; 3: PRP related
factors; 4: common therapeutic factors and, 5: external factors.
Factors related to the effect of PRP
Literature and studies performed in this thesis showed a wide variety in PRP dosage 1,2. To determine
the optimum PRP dosage, the question of “how much therapy is needed to establish the desired
effect” should be answered. However, up until now, most studies have analyzed effects of PRP
at a certain dosage by analyzing pre/post and follow-up outcomes 3-6, not knowing whether this
effect could also be reached with a lower dosage or a greater effect could be reached at a higher
dosage. Generally, studies do not explicitly target a certain effect, nor do they explicitly adjust
dosages towards this target effect. Additionally, the question arises regarding which effect should
be analyzed with respect to PRP: the effect of PRP on improving participation or the effect patients
reach at a certain moment using better self-management skills acquired from PRP. For example,
can PRP considered effective if a patient does not acquire a clinically important change on PDI,
but shows good skills to self-manage his disabilities in the future? Moreover, multidimensional
effects of multidisciplinary therapies, including psychological components, are more diffi cult to
defi ne, compared to the unidimensional effect of mono-disciplinary therapy, including mainly
physical components. Additionally, it is easier to measure “physical condition” compared to
measuring ”the ability to improve physical condition”. The current literature shows a wide variety
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion | 113
7
of outcome measures and domains addressing the effect of PRP in relation to participation, such
as disability reduction, QoL and work participation 1,2,7. However, other outcome measures related
to self-management skills should be added to assess the effect of PRP and could be used to assist
with determining the optimum dosage. Being able to self-manage pain-related disabilities would
presumably effect participation in daily life 8.Measuring self-management skills as an effect of PRP,
in addition to rehabilitation programs in general, is in line with changes in the new concepts of
health. Instead of describing health as “a state of complete physical, mental and social wellbeing
and not merely the absence of disease or infi rmity” 9, Huber et al. stated that health is “the ability
to adapt and to self-manage, in the face of social, physical and emotional challenges” 10.
Regarding the effects of PRP, it can be debated from which perspective the optimum effect
should be targeted – optimum from the perspective of the patient, from the rehabilitation
professionals or from an economic perspective. In the current system of healthcare fi nance in
the Netherlands, and in some cases, from an economic perspective, a higher PRP dosage may
provide more income for the rehabilitation provider, while from the perspective of a patient and/
or rehabilitation professional, the desired effect may have already been reached. If the optimum
dosage is defi ned from this economic perspective, overtreatment could occur. For these reasons,
more insight is needed regarding which factors are important to determine optimum PRP dosage.
Additionally, scientifi c evidence and consensus regarding target effects of PRP are needed to
improve comparability and the ability to determine optimum PRP dosage.
Patient related factors
Dosage of PRP could be related to the patients’ case complexity at the beginning and during PRP.
Chapters 2, 3, 5 and 6 showed that several patient characteristics and patient-related factors,
both physical and psychological, can, or are assumed to, infl uence the effect of PRP and the
required dosage. Taking together the fi ndings of this thesis and the questions regarding the
effects of PRP, there could be an association between the stages of change 11 and PRP dosage.
The transtheoretical model of changing behavior presumes that the readiness of change can be
described in different stages of change. During the precontemplation stage, patients believe that
chronic pain is primarily a biomedical problem and rehabilitation professionals could help relieve
the pain during PRP 12. Therefore, they are not willing to change behavior and are not motivated to
take the biopsychosocial approach offered in PRP. At the contemplation stage, patients are aware
of the biopsychosocial nature of their problem, but do not know how to manage this. Therefore
at this stage, a patient needs professionals help to manage the pain and related disabilities. In the
later stages (preparation and action stages), patients have learned how to self-manage their pain
and disabilities and they need to maintain this healthy behavior. Being able to self-manage pain-
related disabilities and to make plans for maintaining healthy behaviors will theoretically result in
less need for professional help, and therefore, less, or even no, PRP. Self-management skills will

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
114 | Chapter 7
theoretically also result in late-treatment improvements in outcomes of reduction of experienced
disability, QoL and work participation. This is in line with the results from previous studies 12,13.
A recent study 14 analyzed changes in precontemplation and action attitudes during cognitive-
behavioral therapy (CBT) for patients with chronic pain. From this study, it was concluded that
there might be an association between changes in the stages of behavior modifi cation and the
following outcome improvements. However, at present, this association has not been proven
regarding PRPs, there has been no documented association related to PRP dosage. In addition,
measuring the stage of change of a patient at a certain moment is still diffi cult and arbitrary 14.
PRP related factors
PRP itself, as well as the rehabilitation professionals involved in PRP, could infl uence dosage. PRP
is offered at a certain dosage – total duration in weeks, total number of contact hours, number
of rehabilitation professionals involved, form of intervention and physical dosage of exercise
(weight, repetition, duration, frequencies). These dosage variables differ across PRPs, nationally
and internationally. From the systematic review and the interviews conducted in Chapters 2
and 5 respectively, it can be concluded that there is a lack of scientifi c evidence regarding on
which factors the offered PRP dosage is based. Choices of dosages of PRPs included in Chapter
5 are mainly based on clinical expertise and historical grounds. Remarkably, both rehabilitation
professionals and patients are generally satisfi ed with the offered and received PRP, regardless of
the large differences in offered dosages. Patient satisfaction was studied in a systematic review
within physical therapy care 15, concluding that therapist characteristics, the process of care, and
the organization of care were consistently identifi ed factors that infl uenced satisfaction with care,
whereby treatment outcome and expectations of physical therapy were less-frequently reported
factors.
Dosage can be expressed in terms of total duration, in addition to expressing it in terms of total
number of contact hours. For example, PRP can be offered for the same number of weeks (total
duration), but with a greater or fewer total number of contact hours. These differences in the total
duration and corresponding number of contact hours per week are based on different choices
regarding the content of contact hours, the number of rehabilitation professionals, and the form
of PRP. The choice of content of contact hours, for example, is based on the assumption of what
content should be offered within the contact hours of PRP and which activities or homework should
be performed by the patient himself outside the rehabilitation center. Apparently, rehabilitation
teams have made different choices regarding offered content and related dosages based on
different assumptions and the best available evidence 1. Several studies have been performed
to analyze components of PRP, such as differences between outpatient and inpatient PRP 16 and
graded activity versus graded exposure 17. However, evidence for the optimum composition of
PRP and related optimum PRP dosages, including all components and factors, is lacking.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion | 115
7
Common factors
Common therapeutic factors 18 are described as possible explanations for equivalent effectiveness
across different treatment approaches within psychotherapy. Rosenzweig wondered whether
“the factors alleged to be operating in a given therapy are identical with the factors that
actually are operating, and whether the factors that actually are operating in several different
therapies may not have much more in common than have the factors alleged to be operating”.
Examples of common factors are reassurance, feedback, insight, success experiences, therapeutic
alliances, patient expectations, therapist expertness, and trust 19. Because of the biopsychosocial
characteristics of PRP, common factors could probably infl uence the effects and PRP dosage. The
results of the qualitative study in Chapter 5 showed that these common factors are similar but
lead to different choices in PRP dosage. However, little evidence is available regarding specifi c
and common factors and their relationship to outcomes of chronic pain treatment 14,20-22 and its
dosage.
Overall, this thesis opened a black box in pain rehabilitation research. It is the fi rst step in
unraveling the complexities of PRP dosages. Still, it is a huge challenge to answer the question of
optimum PRP dosage, taking into account the relationship of dosage and content, including all
of the above-mentioned factors. Adding the factor of dosage to what Burns 14 stated regarding
the working mechanisms for CBT, “it is not yet clear whether CBT worked for reasons specifi ed by
theory, through the inspiration of hope and the support and encouragement of a good therapist,
or a combination of factors”.
External factors
The legislation of expenses and reimbursements in healthcare could lead to differences in PRP
dosages across countries. Direct and indirect costs become more and more important. In general,
PRPs have proven cost effectiveness 23,24, but it is a challenge to balance how much treatment is
needed versus its costs. Because the effect of PRP is not strictly defi ned, costs of PRP can be the
motivation for offering a certain PRP dosage in order to ensure cost benefi ts. In 2014, the Dutch
government started, in cooperation with the Dutch Association of Physicians in Rehabilitation
Medicine, to develop a new system of fi nancing for rehabilitation medicine. Physicians across
the Netherlands described the content of rehabilitation treatment according to different therapy
components. Registering contact hours linked to these therapy components will lead to more
transparency for all rehabilitation activities performed during rehabilitation programs across the
Netherlands. Based on the combination of content and contact hours, a new fi nance system will
be implemented before 2019. The present fi nance system is only based on the number of contact
hours divided across categories, regardless of the content or effect of therapy. The adjustment
of content in terms of therapy components related to contact hours of rehabilitation programs
will probably draw attention and discussion regarding dosage of programs because of the link to
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
116 | Chapter 7
funding. Consequently, if dosages will be adapted, this will lead to more comparability of these
programs across the Netherlands.
This thesis showed that PRP dosage is associated with many implicit and un- or under-researched
factors. Therefore, it is presently diffi cult to draw robust conclusions about the optimum PRP
dosage, and further research is needed to acquire more insight into, and scientifi c evidence of,
differences and similarities between these factors and their interrelationships.
Implications
Clinical implications
In general, multidisciplinary PRPs have proven their effectiveness 1,6,7,25. However, no distinction
can be made between different PRPs. This thesis resulted in a critical look at the different aspects
of dosage, and it should encourage clinical practice and research to focus more on PRP dosage.
Implications for patients
Patients should be made aware of the different dosages. In the long term, research aimed at
optimizing PRP dosage will benefi t patients because healthcare providers will be better able to
estimate which PRP dosage is required for subgroups of patients. Eventually, patients will receive
the most effective and effi cient PRP.
Implications for therapists
Therapists involved in PRP should refl ect on the dosage of the offered program. They have to
be aware of the differences of dosage within PRPs and they should be aware of the distinction
between what is “nice to have or need to have”. Even though it seems like there is always
something to practice or teach, there is room for improvement and patients have the right to
receive the optimum care related to content and dosage of treatment. Over- or under-dosage of
treatment will not benefi t anyone. Therapists should integrate all factors related to the patients’
needs and preferences, as well as their professional experience, and they should be aware of the
infl uence of common factors, costs and the available evidence to offer optimum PRP dosage.
Implications for rehabilitation centers
Insight into PRP dosage and being able to offer optimum PRP dosage will benefi t the entire
rehabilitation process. It will benefi t the patient fl ow, and will reduce waiting lists and over- or
underdosing treatment. As a result, centers will be able to treat the maximum number of patients
suffering from chronic pain and offer cost-effective PRPs. The issue of dosage studied in this thesis,
while studied within the pain rehabilitation context, is not unique for pain rehabilitation only. The
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion | 117
7
results of this thesis can be used as an example for other rehabilitation programs. Rehabilitation
programs assist in improving health in terms of “the ability to adapt and self-manage,” and all
rehabilitation programs can use this concept to offer more cost-effective programs.
Scientifi c implications
The results of this thesis, combined with the present developments regarding costs of healthcare,
indicate that dosage of rehabilitation programs is important to include in analyzing these
programs. Dosage of PRP has been a neglected topic in pain rehabilitation research, as well
as in rehabilitation research in general. Previous studies analyzing the effect of PRPs could
be confounded, and therefore, conclusions should be interpreted with caution. A theoretical
example: a study comparing the effectiveness of physical therapy to PRP. The total duration of
both programs is 10 weeks; however, physical therapy is given two hours a week and PRP is given
10 hours a week. PRP showed superior results, but it is questionable whether the content or the
dosage is superior, or whether other common factors were responsible for differences in the
effects. More research is needed to analyze what and how much works for whom.
Societal implications
Societal implications in general
The results of this thesis contribute to the ability to optimize PRP dosage and other rehabilitation
programs in general. Obtaining evidence of optimum dosage will lead to the reduction of over-
or underdosing treatment, thereby preventing the overdosage of treatment that leads to more
“needs”. Over- or underdosing also leads to the opposite of self-management.
Implications for (work)participation
The effect of patients being able to self-manage their pain will subsequently optimize participation
in daily life. Insight into “how much works for whom” will lead to the most desirable effects at
the optimum PRP dosage for each individual. This will allow them to participate in daily life and
return to work as soon as possible.
Financial implications
Because this thesis is an initial attempt at unraveling the complexities related to PRP dosage,
at this stage, no fi nancial implications can be described since there is no solid evidence on the
dose–effect relationship.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
118 | Chapter 7
Future research
Future studies in rehabilitation research should report dosage of treatment. This will improve
transparency, comparability and generalizability of rehabilitation treatment dosages and will give
researchers the ability to analyze dose–effect relationships. Within pain rehabilitation research,
future studies should also focus on the distinction between desired effect of PRP itself to be able
to fi nish PRP and the desired long-term effect of the patient self-management skills regarding
disability, QoL and (work) participation. Dosage of PRP should be analyzed together with all
specifi c and aspecifi c factors, such as a core set of working mechanisms of effective PRPs. In the
beginning, analyzing optimum PRP dosages appeared to be diffi cult. However, this thesis has
yielded an overview of dosage-related factors. The results can be combined into new hypotheses
regarding PRP dosages. The course of disability, which is reduced over time, could be related to
the desired effect and the stages of change and needs of patients during PRP. This qualitative
study confi rmed the relationship between case complexity and dosage. The Delphi study gives
substance to case complexity with the CCI, which can be used in clinical practice in relation to the
required dosage, and can also be used to scientifi cally analyze this relation. Moreover, the RCT
provides evidence that both arms with different dosages resulted in positive effects. This coincides
with the positive experiences of the PRP at different dosages used in the qualitative study, as
well as with the overview of effect sizes in the systematic review. These insights could be further
analyzed to determine whether there is a trend towards shortening PRPs. Future research could
result in more scientifi c evidence for optimum dosage, which will lead to better insight into what
works for whom and how much therapy is needed. This will accomplish the optimum effects at
the optimum dosage, with an addition focus on cost-effectiveness in terms of direct and indirect
healthcare costs.
Strengths and limitations
The research questions from this thesis evolved out of clinical practices, resulting in strengths
and limitations since the methodological strictness is not always compatible with clinical practice.
Because the studies in this thesis were the fi rst that analyzed PRP dosage, and no evidence was
available beforehand mistakes were made. Some choices made became weaknesses. Most studies,
except the systematic review, were performed in the Netherlands within the context of the Dutch
healthcare system, which limits generalization. However, although the Dutch healthcare system
differs from the healthcare systems in other countries, PRP dosage and rehabilitation in general is
an important issue all over the world. This thesis could be used to perform similar studies within
different countries to optimize dosage of therapy in each particular country. A strength of the
thesis is the variety of methods used. Qualitative and quantitative methods were used to reveal
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion | 119
7
different factors related to PRP dosage, resulting in an overview of important factors that now
need to be analyzed in future research to unravel and improve optimum PRP dosages.
Conclusion
This thesis is the fi rst that focuses on PRP dosage. Consequently, it should be regarded as a
starting point for determining factors related to dosages and exploring optimum PRP dosages.
This thesis analyzed dosage of PRP using different research methods and acquired different
insights in aspects of dosage. Therefore, this thesis contributes to the body of research in the area
of pain rehabilitation research aimed at analyzing the effects of all components and their dosages.
Additionally, results from the studies within this thesis contribute to societal developments in
transparency, comparability and cost effectiveness of PRPs and can be a basis for others to analyze
the dosages of rehabilitation programs.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
120 | Chapter 7
References
1. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. BMJ. 2001;322(7301):1511-1516.
2. Waterschoot FP, Dijkstra PU, Hollak N, de Vries HJ, Geertzen JH, Reneman MF. Dose or content? effectiveness of pain rehabilitation programs for patients with chronic low back pain: A systematic review. Pain. 2014;155(1):179-189.
3. McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: Outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27(22):2564-2573.
4. Smeets RJ, Vlaeyen JW, Hidding A, et al. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? fi rst direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;7:5.
5. Gatchel RJ, Okifuji A. Evidence-based scientifi c data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779-793.
6. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: A systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
7. van Geen JW, Edelaar MJ, Janssen M, van Eijk JT. The long-term effect of multidisciplinary back training: A systematic review. Spine (Phila Pa 1976). 2007;32(2):249-255.
8. Jensen MP, Nielson WR, Turner JA, Romano JM, Hill ML. Changes in readiness to self-manage pain are associated with improvement in multidisciplinary pain treatment and pain coping. Pain. 2004;111(1-2):84-95.
9. WHO. http://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?ua=1&ua=1. Updated 20052015.
10. Huber M. Towards a new, dynamic concept of health. its operationalisation and use in public health and healthcare, and in evaluating health effects of food.; 2014.
11. Prochaska JO, DiClemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: Theory, Research & Practice. 1982;19(3):276-288.
12. Burns JW, Glenn B, Lofl and K, Bruehl S, Harden RN. Stages of change in readiness to adopt a self-management approach to chronic pain: The moderating role of early-treatment stage progression in predicting outcome. Pain. 2005;115(3):322-331.
13. Glenn B, Burns JW. Pain self-management in the process and outcome of multidisciplinary treatment of chronic pain: Evaluation of a stage of change model. J Behav Med. 2003;26(5):417-433.
14. Burns JW, Nielson WR, Jensen MP, Heapy A, Czlapinski R, Kerns RD. Specifi c and general therapeutic mechanisms in cognitive behavioral treatment of chronic pain. J Consult Clin Psychol. 2015;83(1):1-11.
15. Hush JM, Cameron K, Mackey M. Patient satisfaction with musculoskeletal physical therapy care: A systematic review. Phys Ther. 2011;91(1):25-36.
16. Boonstra AM, Reneman MF, Schiphorst Preuper HR, Waaksma BR, Stewart RE. Differences between patients with chronic musculoskeletal pain treated in an inpatient or an outpatient multidisciplinary rehabilitation program. Int J Rehabil Res. 2014;37(2):187-191.
17. Leeuw M, Goossens ME, van Breukelen GJ, et al. Exposure in vivo versus operant graded activity in chronic low back pain patients: Results of a randomized controlled trial. Pain. 2008;138(1):192-207.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion | 121
7
18. Rosenzweig S. Some implicit common factors in diverse methods of psychotherapy. Journal of Psychotherapy Integration. 2002;12(1):5-9.
19. Lambert MJ, Ogles BM. Common factors: Post hoc explanation or empirically based therapy approach? Psychotherapy. 2014;51(4):500-504.
20. Thorn BE, Burns JW. Common and specifi c treatment mechanisms in psychosocial pain interventions: The need for a new research agenda. Pain. 2011;152(4):705-706.
21. Jensen MP. Psychosocial approaches to pain management: An organizational framework. Pain. 2011;152(4):717-725.
22. Day MA, Jensen MP, Ehde DM, Thorn BE. Toward a theoretical model for mindfulness-based pain management. The Journal of Pain. 2014;15(7):691-703.
23. Turk DC. Clinical effectiveness and cost-effectiveness of treatments for patients with chronic pain. Clin J Pain. 2002;18(6):355-365.
24. Sletten CD, Kurklinsky S, Chinburapa V, Ghazi S. Economic analysis of a comprehensive pain rehabilitation program: A collaboration between fl orida blue and mayo clinic fl orida. Pain Med. 2015;16(5):898-904.
25. Flor H, Fydrich T, Turk DC. Effi cacy of multidisciplinary pain treatment centers: A meta-analytic review. Pain. 1992;49(2):221-230.


R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
124 | Summary
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary | 125
S
Pain rehabilitation programs (PRPs) consist of multidisciplinary treatments based on the
biopsychosocial model. It can assist people with chronic musculoskeletal pain to manage their
pain more effectively, and it can decrease pain related disabilities. Scientifi c research has shown
that pain rehabilitation has a positive effect on disabilities, work participation and quality of life.
However, there is a large amount of variation with regard to the content, form (inpatient or
outpatient, individual or in a group), duration and intensity of treatments, and the number of
disciplines involved in PRPs. In literature, very little is known about dosage of PRPs. Therefore,
the aim of the studies in this thesis was to gain insight into the effect of the different aspects of
dosage of PRPs. Various methods were used during the research and are described in the chapters
of this thesis. In this thesis, dosage of PRP has been defi ned as the total duration of treatment in
weeks, the total amount of contact hours, and the number of contact hours per week (intensity).
In Chapter 2 a systematic review is described. During the review process, no studies were found
that primarily dealt with the analysis of dosage of PRPs. Therefore, the aim of this review was
to study randomized controlled trials that analyzed the effects of PRPs. A requirement was that
these studies included dosage of treatments. The result is an overview of these studies, dosage of
the treatments that were compared and the accompanying effects sizes regarding the domains:
disabilities, work participation, and quality of life. Dosage of PRPs varied from 6.4 to 196.8
contact hours. In addition, the infl uence of dosage on the effect sizes was analyzed. A number of
variables were found to infl uence effects. Because these variables were strongly related to dosage
and it was not possible to isolate other factors, no robust conclusions could be drawn with regard
to the infl uence of dosage on the effects.
Chapter 3 presents a prospective cohort study. Its objective was to analyze the course of disability
reduction during PRP. The Pain Disability Index (PDI) was used as a measure of self-reported
disability. Many studies are aimed at the effects of PRPs and use pre- and post-treatment outcome
measures. With regard to dosage, however, the course of disability reduction during a treatment
becomes important. The duration of a program could be shortened if the desired effect could
be achieved before the end of the treatment. The analyses showed that the course of disability
reduction occurred following a quadratic model. This means that disability reduction is greater
in the beginning of the program and levels off as the treatment progresses. In addition, the
measurement moment, initial PDI score, average pain score, and interaction between the initial
PDI and measurement moment infl uenced the course of disability reduction. This means that
disability reduction is faster for a patient with higher initial PDI and average pain score than for a
patient with lower initial PDI and average pain score. The infl uence of the interaction between the
measurement moment and the initial PDI makes the reduction in PDI per measurement moment
become smaller at the end of the treatment. The results of this study can be used in clinical
practice to predict the course of PDI, and to adjust dosage to the desired effect.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
126 | Summary
The literature study, performed prior to the systematic review, resulted in no studies performed
to analyze dosage of PRPs as a primary objective. In Chapter 4 a randomized controlled trial is
described with regard to the use of different dosages of PRPs. The objective was to analyze the
effect of PRP with a lower dosage compared to the current program at the Center of Rehabilitation
UMCG. The treatment of the experimental group was 4 weeks shorter and had less contact hours
than that of the control group. The content of the programs was similar. The trial is of a non-
inferiority design. This means that the effect on the experimental group must not be worse than
the effect on the control group. The PDI was used as primary outcome measure. A non-inferiority
margin of 4 points difference was applied. Disability reduction was observed in both groups. The
difference between both groups was 2.5 points. This difference lies within the non-inferiority
margin. However, the 95 percent confi dence interval was -2.2 to 7.3. Because this interval is
outside the margin between 0 and 4 points, non-inferiority cannot be established for certain.
In the trial, treatments were often extended in the experimental group, making the contrast in
dosage between both groups too small. Based on a priori stopping rules, the trial was stopped
prematurely. Due to the lack of contrast in dosage between both groups and the wide margin
with regard to the precision of the results, the conclusion that a shorter treatment is non-inferior
cannot be drawn. Additionally, the difference in effects between the extended and non-extended
treatments was analyzed. The analyses did not show a signifi cant difference. This trial was the
fi rst to have the analysis of dosage as its primary goal. From the results, no robust conclusions can
be drawn for now. However, the results do indicate possibilities to shorten PRPs and the need for
further research into dosage of PRP.
Besides quantitative data regarding dosage of PRPs, it is of added value to gather qualitative
data. Chapter 5 presents a qualitative study with the aim of gaining insight into the perspectives
of patients and professionals concerning dosage of PRPs. Patients who had fi nished a PRP and
professionals of 3 rehabilitation centers in the Netherlands were interviewed, patients individually
and professionals in focus groups. The treatments of the 3 rehabilitation centers differed in
dosage. A total of 12 patients were interviewed, as well as a total of 17 professionals in 3
focus groups. Audio recordings were made of all interviews. These recordings were transcribed
verbatim, and the data was analyzed and arranged thematically. In general, patients were
satisfi ed with the dosage of treatment they had received. Although dosages differed, patients as
well as professionals mentioned similar factors regarding dosage. All factors were categorized as
patient-related, treatment-related, and external factors. Remarkably, the factors mentioned were
the same to a large extent despite the difference in dosage. Furthermore, in the focus groups
professionals reported that little is known about dosage in literature, and that is why, at the
moment, the choice of dosage of PRP is based on clinical expertise and historical grounds.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary | 127
S
The objective of the study described in Chapter 6 was to explore case complexity of patients
with chronic non-specifi c musculoskeletal pain (CMP). There could be a relationship between
case complexity and the required dosage of PRP. However, the case complexity of this specifi c
group was not transparent and diffi cult to measure, and that is why this relationship could not
be analyzed. Because of this, a three-round Delphi study was performed among professionals
involved in PRP in the Netherlands. These professionals were asked what they believed to be
important factors that could infl uence the functioning of patients with CMP. In the fi rst round,
a total of 166 factors were identifi ed. In the second round, the 10 most important factors were
selected. In the third round, relative weights of each of these 10 factors were calculated. A scale of
0 (no weight) to 4 (very heavy weight) was used. The 10 most important factors were: psychiatric
disorders, motivation, family system problems, mentalization capacity, somatization, fi nancial
and work related problems, features of complaints (duration, intensity), treatment-interfering
personality traits, life events, and personal injury procedures. In daily clinical practice, establishing
the infl uence of these factors on a patient’s disability is mainly based on clinical reasoning. The
10 factors were used to initiate the development of a Case Complexity Index (CCI). This index
has a minimum score of 0 and a maximum score of 100, it shows the degree of case complexity,
and is measured by establishing the presence of the 10 factors and the accompanying degree of
infl uence on case complexity. Rehabilitation physicians and professionals tested the feasibility of
the CCI on 14 patients. A reasonable similarity in CCI scores was found between the rehabilitation
physicians and professionals. This study can help to initiate the assessment of case complexity.
It may be used to gain transparency in case complexity, and to analyze the relationship between
case complexity and dosage.
In the general discussion in Chapter 7, the main fi ndings of this thesis are summarized. The factors
related to dosage of PRPs are discussed, such as factors regarding the desired effect of treatment,
patient- and PRP-related factors, and general and external factors. Clinical, scientifi c and societal
implications are described, and divided using different perspectives. Because this thesis is a fi rst
step towards scientifi c research concerning dosage of PRP, recommendations are made for future
research. The strengths and limitations of this thesis are described. The fi nal conclusion in this
chapter is that the results of this thesis offer a contribution towards: the research of PRP, making
treatments transparent and comparable, and improving cost- effectiveness.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
130 | Samenvatting
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting | 131
S
Pijnrevalidatie kan mensen met chronische pijn aan bewegingsapparaat helpen om beter te
leren omgaan met hun pijn en het kan de pijngerelateerde beperkingen verminderen. Deze
revalidatie bestaat uit multidisciplinaire behandelingen gebaseerd op het biopsychosociale model.
Wetenschappelijk onderzoek heeft aangetoond dat pijnrevalidatie een positief effect heeft op
beperkingen, participatie en kwaliteit van leven bij mensen met chronische pijn. De praktijkvariatie
in inhoud, vorm (klinisch - poliklinisch/ individueel - groepsbehandeling), duur en intensiteit van
de behandeling en het aantal disciplines betrokken bij de pijnrevalidatie, is echter groot. Er is nog
maar weinig bekend over de effecten van dosis van pijnrevalidatie op uitkomsten. Het doel van
de studies in dit proefschrift was dan ook het analyseren van dosisaspecten van pijnrevalidatie en
inzicht krijgen in de invloed van dosis op effecten van pijnrevalidatie. Dit is onderzocht middels
verschillende onderzoeksmethoden, beschreven in de hoofdstukken in dit proefschrift. Onder
dosis wordt in dit proefschrift verstaan: de totale duur van de behandeling in weken, het totale
aantal contacturen en het aantal contacturen per week (intensiteit).
In hoofdstuk 2 is een systematische review beschreven. De zoekstrategie in de wetenschappelijke
literatuur naar studies die primair gericht waren op het analyseren van de dosis van pijnrevalidatie,
leverde geen studies op. Daarom is gekozen om de review te richten op studies die de effecten
van pijnrevalidatie hebben geanalyseerd middels een gerandomiseerde gecontroleerde studie.
Een vereiste was dat de dosis van de onderzochte behandelingen was beschreven en het effect
gemeten was voor minimaal 1 van de uitkomsten ervaren beperkingen, arbeidsparticipatie en
kwaliteit van leven. Het resultaat is een overzicht van deze studies, de dosis van de behandelingen
en de bijbehorende omvang van effect voor de genoemde uitkomsten. De dosis van de
geïncludeerde pijnrevalidatiebehandelingen varieerde in contacturen van 6,4 tot 196,8 uur.
Aanvullend is de invloed van de dosis op het effect geanalyseerd. Een aantal variabelen bleek
invloed te hebben op het effect. Maar die variabelen waren onderling ook sterk verbonden.
Het was daarom niet mogelijk factoren te isoleren. Het was dan ook niet mogelijk om robuuste
conclusies te trekken met betrekking tot de invloed van de dosis op uitkomsten.
Hoofdstuk 3 is een prospectieve cohort studie met als doel het verloop van ervaren beperkingen,
gemeten met de Pain Disability Index (PDI), gedurende pijnrevalidatie te analyseren. Veel studies
onderzoeken het effect van pijnrevalidatie en meten uitkomstmaten vooraf en aan het eind van de
behandeling. Echter in relatie tot dosis is het verloop van de uitkomst gedurende de behandeling
interessant, omdat de behandeling verkort zou kunnen worden indien het effect al behaald is
voor het einde van de behandeling. Uit de studie bleek dat de ervaren beperkingen afnamen
volgens een kwadratisch tijd model: De mate van afname in ervaren beperkingen is in het begin
van de behandeling groter en naarmate de behandeling vordert, vlakt de afname af. Daarbij
bleek dat het meetmoment, de initiële score op de PDI, de gemiddeld pijnscore en de interactie
tussen initiële PDI en meetmoment invloed hadden op het verloop van de ervaren beperkingen.
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
132 | Samenvatting
Klinisch betekent deze uitkomst dat de afname van ervaren beperkingen sneller gaat voor een
patiënt met een hogere initiële score op PDI en hogere pijnscore, dan voor een patiënt met een
lagere initiële score op PDI en pijnscore. De invloed van de interactie tussen het meetmoment en
de initiële PDI maakt dat de afname van PDI per meetmoment aan het einde van de behandeling
kleiner wordt. De bevindingen uit deze studie kunnen gebruikt worden om in de klinische praktijk
het verloop van de PDI te voorspellen en de dosis op het gewenste resultaat aan te passen.
Uit de literatuurstudie voorafgaand aan de systematische review, bleek dat er geen studies
waren, die primair gericht zijn op het vergelijken van pijnrevalidatie met verschillende doses. In
hoofdstuk 4 is een gerandomiseerde gecontroleerde studie beschreven waarin pijnrevalidatie
met verschillende doses is aangeboden. Het doel was het analyseren van het effect van een
pijnrevalidatiebehandeling met een lagere dosis ten opzichte van de dosis van de huidige
behandeling van het Centrum voor Revalidatie UMCG. De behandeling van de experimentele
groep was 4 weken korter en bestond uit minder contacturen dan de controle groep. De inhoud
bleef gelijkwaardig. De studie had een non-inferiority design. Dat betekent dat het effect van
de experimentele groep niet slechter mocht zijn dan het effect van de controle groep. De
PDI was gebruikt als primaire uitkomstmaat om het effect te meten, waarbij een marge van
4 punten verschil werd toegestaan als gelijkwaardig effect. Ervaren beperkingen namen af in
beide groepen. Het verschil tussen beide groepen was gemiddeld 2,5 punten. Aangezien dit
verschil binnen de marge van 4 punten ligt, wordt dit als gelijkwaardig geïnterpreteerd. De
95% betrouwbaarheidsintervallen lagen tussen -2.2 en 7.3. Aangezien de interval buiten de
gestelde marge van 0 tot 4 punten ligt, is gelijkwaardigheid niet met zekerheid vast te stellen.
In de praktijk werden de behandelingen in de experimentele groep vaak verlengd, waardoor
het contrast in dosis tussen beide groepen te klein werd. De studie moest, vanwege vooraf
opgestelde stopregels, voortijdig worden beëindigd. Het gebrek aan contrast in dosis tussen
de groepen en de grote marge in betrouwbaarheid van de resultaten, betekent dat niet met
zekerheid geconcludeerd kan worden dat het effect van een kortere behandeling gelijkwaardig
is. Aanvullend zijn analyses gedaan om het verschil tussen effect van het al dan niet verlengen van
behandelingen te analyseren. De effecten waren signifi cant verschillend. Deze studie was de eerste
waarbij dosis als primair doel werd geanalyseerd. Uit deze resultaten kunnen nog geen robuuste
conclusies getrokken worden. De resultaten geven echter wel een indicatie voor mogelijkheden
voor het verkorten van pijnrevalidatiebehandelingen en daarmee voor de noodzaak voor verder
onderzoek naar de dosis van pijnrevalidatie.
Naast kwantitatieve gegevens omtrent de dosis van pijnrevalidatie, is het ook van toegevoegde
waarde om kwalitatieve gegevens te verzamelen. Hoofdstuk 5 beschrijft een kwalitatieve studie
met als doel het verkrijgen van inzicht in de perspectieven van de patiënten en professionals
in relatie tot de dosis van pijnrevalidatie. Patiënten die een pijnrevalidatie behandeling hadden
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting | 133
S
afgerond en professionals werkzaam binnen de pijnrevalidatie in 3 revalidatiecentra in Nederland
zijn geïnterviewd. Patiënten werden individueel geïnterviewd en professionals in een groep. De
behandelingen van de 3 deelnemende revalidatiecentra verschilden in dosis. In totaal zijn 12
patiënten geïnterviewd en zijn 17 professionals in 3 groepen geïnterviewd. Van alle interviews
waren geluidsopnamen gemaakt. Deze opnamen zijn daarna letterlijk uitgeschreven en de
data zijn geanalyseerd en thematisch geordend. Over het algemeen waren patiënten tevreden
met de verkregen dosis. Ondanks de verschillen in dosis, werden zowel door de patiënten als
door de professionals soortgelijke factoren benoemd in relatie tot de dosis. Alle factoren zijn
gecategoriseerd in factoren gerelateerd aan de patiënt, aan de behandeling en aan externe
factoren. Opmerkelijk was, dat ondanks verschillen in dosis, de genoemde factoren grotendeels
hetzelfde waren tussen centra. Verder werd in de focusgroepen met de professionals aangeven,
dat er weinig bekend is over de dosis in de literatuur, waardoor de keuze van de dosis van
pijnrevalidatie op dit moment gebaseerd is op klinische ervaringen en historische gronden.
De studie beschreven in hoofdstuk 6, is opgezet om de complexiteit van de casus van de patiënten
met chronische pijnklachten die in aanmerking komen voor pijnrevalidatie, te bestuderen. Er
zou een relatie kunnen bestaan tussen de complexiteit van de casus en de benodigde dosis
van pijnrevalidatie. “Complexiteit” van de casus bleek echter voor deze specifi eke doelgroep
niet transparant en moeilijk meetbaar, waardoor de genoemde relatie niet geanalyseerd kon
worden. Vanuit de klinische praktijk leek de complexiteit te bestaan uit invloed van verschillende
factoren. In de studie namen professionals deel die werkzaam zijn binnen de pijnrevalidatie in
heel Nederland. In 3 vragenrondes werd gevraagd welke factoren een relevante invloed kunnen
hebben op het functioneren van patiënten met chronische pijnklachten. In de eerste ronde zijn
166 factoren benoemd. In de tweede ronde is hieruit een top 10 samengesteld. In de derde
ronde zijn voor de factoren uit de top 10 de mate van invloed aangegeven op het functioneren
van patiënten met chronische pijnklachten op een schaal van 0 tot 4 (0 geen invloed en 4
erg sterk van invloed). De 10 belangrijkste factoren waren: psychiatrische problematiek, lage
motivatie, systeemproblematiek, gering mentaliserend vermogen, somatisatie, fi nanciële en
werkgerelateerde problemen, klachtkenmerken (duur, intensiteit), persoonlijkheidskenmerken
die de behandeling belemmeren, life events en letselschadeprocedure. Het vaststellen van (de
mate van invloed van) deze factoren bleek in de huidige praktijk vooral gebaseerd op klinisch
redeneren; niet op basis van uitkomsten van meetinstrumenten. De 10 factoren zijn gebruikt om
een casus complexiteitsindex (CCI) op te stellen. Deze index, geeft de mate van complexiteit weer.
De CCI wordt berekend op basis van de aanwezigheid van de 10 factoren en de bijbehorende
mate van invloed op complexiteit. De score kan variëren van 0 tot 100, waarbij een hoge score
duidt op een hoge casus complexiteit. De score kan bestaan uit aanwezigheid van meerdere
factoren of een paar factoren met een hoge mate van invloed. Het gebruik van de CCI is getest
in de huidige praktijk door revalidatieartsen en het behandelteam bij 14 patiënten. Er bleek een

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
134 | Samenvatting
redelijke overeenstemming van score van CCI tussen de revalidatieartsen en het behandelteam.
Deze studie heeft een eerste aanzet gedaan naar het meetbaar maken van de complexiteit van
de casus. De resultaten van deze studie kunnen mogelijk gebruikt worden om transparantie te
krijgen in casuscomplexiteit en om de relatie tussen complexiteit en dosis te analyseren.
In de algemene discussie in hoofdstuk 7 zijn de voornaamste resultaten van het proefschrift
beschreven. De verschillende factoren die gerelateerd zijn aan de dosis van PRP, zoals factoren
met betrekking tot het beoogde behandeleffect, patiënt en PRP gerelateerde factoren, algemene
en externe factoren, worden benoemd en bediscussieerd. De klinische, wetenschappelijke en
maatschappelijke implicaties worden vanuit verschillende perspectieven beschreven. Omdat
dit proefschrift een eerste stap is geweest om de dosis van pijnrevalidatie wetenschappelijk te
onderzoeken, zijn aanbevelingen gedaan voor vervolgonderzoek. De sterke en minder sterke
punten van het proefschrift zijn beschreven. Het hoofdstuk wordt afgesloten met de conclusie dat
de resultaten van dit proefschrift kunnen bijdragen aan onderzoek binnen de pijnrevalidatie, het
transparant en vergelijkbaar maken van keuzes ten aanzien van de dosis en op termijn mogelijk
tot het verbeteren van de kosteneffectiviteit.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting | 135
S


R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
138 | Dankwoord
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord | 139
D
In september 2009 ben ik gestart met mijn promotietraject. Een enorme uitdaging; dat was het
zeker!!! Gelukkig heb ik vaak steun ervaren van de mensen om mij heen, met wie ik vele goede,
en zeker ook de minder goede momenten heb mogen delen. Via deze weg wil ik iedereen
bedanken en een aantal mensen in het bijzonder:
Allereerst alle professionals en patiënten die deel hebben genomen aan de verschillende
onderzoeken. Zonder deelnemers, geen onderzoek. Dank voor ieders inzet en bijdrage.
Dank aan mijn promotieteam: prof. dr. JHB Geertzen, prof. dr. MF Reneman en prof. dr. PU
Dijkstra. Voor mij was dit promotieteam de perfecte combinatie. Balans tussen actie en rust;
inhoud en praktijk en de zuidelijke gezelligheid en de noordelijke stugheid. Ik dank jullie voor de
prettige samenwerking en alles wat ik van jullie heb geleerd.
Beste Jan, jij gaf mij de kans om als ergotherapeut te promoveren. De eerste jaren was jij mijn
eerste promotor. Zodra Michiel benoemd werd tot professor, werd hij eerste promotor. Stiekem
ben je, naast Michiel, ook altijd een beetje mijn eerste promotor gebleven! Dank voor al de
kritische noten, de waardevolle aanvullingen en natuurlijk de Brabantse touch!
Beste Michiel, ik weet nog dat je kort na de promotie van Remko tegen mij zei: “Wij hadden
bedacht dat jij over een aantal jaren ook wel in die aula kon gaan staan”. Het duurde bij mij
even voordat ik in de gaten had waar je het over had. Dank dat je mij deze kans hebt gegeven
en dank voor de vele steun, het inkorten en afkappen van mijn ellenlange zinnen en discussies.
Maar bovenal voor het vertrouwen dat je me gegeven hebt. Als ik even door de bomen het bos
niet meer zag, kon je me in laten zien hoe mooi het project was en wat het onderzoek allemaal
opleverde! Daardoor raakte ik, ondanks de obstakels die ik moest nemen, toch weer gemotiveerd
om positief verder te gaan.
Beste Pieter, jij kwam iets later bij de club. Wat ben ik vaak blij geweest met jouw expertise. Al die
data en al die statistische formules waar ik niets van snapte en wat jij met alle geduld uitlegde.
Samen zochten we naar de vertaalslag van de resultaten naar de betekenis voor klinische praktijk.
Dank voor je geduld, je wijze raad en de goede en gezellige gesprekken.
Het nemen van de stap om als ergotherapeut wetenschappelijk onderzoek te gaan doen en
uiteindelijk te gaan promoveren, heb ik voornamelijk te danken aan Nelleke Kombrink, Rita
Schiphorst Preuper en Michiel Reneman. Zij hebben hier een belangrijke bijdrage aan geleverd.
Nelleke, jij bent degene die mij heeft aangespoord om de wetenschappelijke kant op te gaan. Jij was
teammanager van het pijnteam en tijdens mijn jaargesprek kwamen de onderwerpen uitdaging
en wetenschap bij elkaar. Je stimuleerde me om mijzelf te oriënteren op de mogelijkheden een
wetenschappelijke studie te gaan doen. Ik ben je dankbaar voor het advies wat je me toen
gegeven hebt met dit proefschrift als resultaat!
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
140 | Dankwoord
Rita, jij stimuleerde dit ook. Je dacht mee over de mogelijkheden om te kunnen promoveren en
adviseerde mij tijdens het hele promotietraject. Jouw klinische en wetenschappelijke blik en de
daaruit voortkomende zinvolle aanvullingen en ideeën hebben de uitvoer van het hele project
goed gedaan! Dank hiervoor.
Annemieke de Jong en Berry van Holland, wat geweldig dat jullie mijn paranimfen willen zijn!
Annemieke: als collega’s in het pijnteam, als onderzoekers en zeker niet op de laatste plaats ook
als dames die graag samen een hapje gaan eten om bij te kletsen, hebben we vele gesprekken
gehad en heb ik veel aan je gehad. Dank voor alles: voor de gesprekken, adviezen en gezellige
eetafspraken!
Berry, je bent de beste kamergenoot die iemand zich kan wensen! Of het nu ging om de goede
Engelse bewoording, de lastige formules in Excel, het vieren van de successen of het uiten van
de frustraties, je had altijd een luisterend oor en was altijd behulpzaam! Heel, heel erg bedankt
daarvoor!
Alle collega’s en ex-collega’s van het pijnteam wil ik bedanken voor alle steun, acties, bijdragen,
kritische blikken, discussies, interesses en ieders luisterend oor. De revalidatieartsen Maikel, Jitze,
Rita en Wim: speciale dank voor het informeren en includeren van alle patiënten voor de RCT en
ieders bijdrage aan het onderzoek en dit proefschrift. Alle ergotherapeuten, fysiotherapeuten,
psychologen en maatschappelijk werkster bedankt! Zonder jullie inzet was het niet gelukt en
zonder jullie steun was het mij nooit gelukt om dit tot een goed einde te brengen. Speciale dank
voor mijn directe collega’s van de ergotherapie: Anne, Judith en Lucienne. Ik kon altijd bij jullie
terecht, dat waardeer ik enorm.
De secretaresses van het pijnteam en in het bijzonder Marleen Speller: dank voor alle hulp die
jullie geboden hebben gedurende het hele traject en met name tijdens de uitvoer van de RCT.
Wat kunnen jullie veel werk verzetten en ook nog overzicht houden! Dank hiervoor.
Alle coauteurs wil ik bedanken voor hun waardevolle bijdrage aan het tot stand komen van de
verschillende artikelen in dit proefschrift.
Tijdens een promotietraject kruisen vele praktische en emotionele zaken je pad. Wat was ik dan
ook altijd blij met de collega’s die dezelfde ervaringen hadden op het gebied van onderzoek doen
en promoveren. De collega-onderzoekers van het pijnteam: Remko, Haitze, Berry en de collega’s
van Oker: Sacha, Ilse, Feyuna, Christa, Ria, Anja en Ant. Dank voor alle adviezen en het delen van
jullie (persoonlijke) ervaringen en expertise.
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord | 141
D
Tenslotte wil ik mijn lieve familie en vrienden bedanken voor alle steun en belangstelling.
Er was altijd tijd en belangstelling voor mijn project.
Lieve pap, mam en Ellen, dank dat jullie er altijd voor me zijn!
Lieve Gino, jij hebt altijd geloofd en gezegd dat ik dit kon, ondanks dat ik daar zelf nog niet zo
overtuigd van was. En je had gelijk: het is gelukt! Thanx laiverd!


R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
144 | Over de auteur
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Over de auteur | 145
A
Franka Waterschoot, geboren op 20 juni 1978 te Hoogeloon, groeide op in de buurt van
Eindhoven. Na de middelbare school is ze de opleiding tot ergotherapeut gaan volgen in Heerlen,
waar ze in 2002 afstudeerde. Nadien verhuisde ze van Noord Brabant naar Groningen. Het
eerste half jaar heeft ze gewerkt als ergotherapeut in verpleegtehuis Dilgtoord in Haren en de
daarbij horende locatie de Burcht in Hoogezand. Vanaf oktober 2002 is zij gaan werken bij het
UMCG, Centrum voor Revalidatie (CvR), locatie Beatrixoord Haren. Binnen Beatrixoord heeft ze
als ergotherapeut met name gewerkt binnen de pijnrevalidatie, maar ook binnen de diabetes-
en neurorevalidatie. Na een aantal jaren was Franka op zoek naar een nieuwe uitdaging. Deze
uitdaging startte in september 2009 met een parttime promotietraject met dit proefschrift als
eindresultaat. Sinds oktober 2014 heeft Franka de shift gemaakt van de patiëntenzorg naar
de kwaliteit van de zorg en zet ze haar kennis en expertise in voor projecten binnen het CvR.
Momenteel is ze projectleider van de implementatie van de landelijke behandelmodules binnen
het CvR en van de werkgroep die zich bezig houdt met de zorglogistiek ten behoeve van een
gastvrij en patiëntgericht CvR. Daarnaast is ze coördinator van innovaties in relatie tot ehealth en
zorglogistieke processen binnen het pijnteam.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
148 | Research Institute SHARE
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Research Institute SHARE | 149
R
Research Institute SHARE
This thesis is published within the Research Institute SHARE (Science in Healthy
Ageing and healthcaRE) of the University Medical Center Groningen / University of
Groningen.
Further information regarding the institute and its research can be obtained from our internetsite:
http://www.share.umcg.nl/
More recent theses can be found in the list below.
((co-) supervisors are between brackets)
Janse M
The art of adjustment
(prof AV Ranchor, prof MAG Sprangers, dr J Fleer)
Nigatu YT
Obesity and depression; an intertwined public health challenge
(prof U Bültmann, prof SA Reijneveld)
Aris-Meijer JL
Stormy clouds in seventh heaven; a study on anxiety and depression around
childbirth
(prof CLH Bockting, prof RP Stolk, dr H Burger)
Kluitenberg B
The NLstart2run study; running related injuries in novice runners
(prof RL Diercks, dr H van der Worp, dr M van Middelkoop)
Benjaminse A
Motor learning in ACL injury prevention
(Prof E Otten, prof KAPM Lemmink, prof RL Diecks)
Potijk MR
Moderate prematurity, socioeconomic status, and neurodevelopment in early
childhood; a life course perspective
(prof SA Reijneveld, prof AF Bos, dr AF de Winter)
R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
150 | Research Institute SHARE
Beyer AR
The human dimension in the assessment of medicines; perception, preferences,
and decision making in the European regulatory environment
(prof JL Hillege, prof PA de Graeff, prof B Fasolo)
Alferink M
Psychological factors related to Buruli ulcer and tuberculosis in Sub-saharan Africa
(prof AV Ranchor, prof TS van der Werf, dr Y Stienstra)
Bennik EC
Every dark cloud has a colored lining; the relation between positive and negative
affect and reactivity to positive and negative events
(prof AJ Oldehinkel, prof J Ormel, dr E Nederhof, dr JACJ Bastiaansen)
Stallinga HA
Human functioning in health care; application of the International Classifi cation of
Functioning, Disability and Health (ICF)
(prof RF Roodbol, prof PU Dijkstra, dr G Jansen)
Papageorgiou A
How is depression valued?
(prof AV Ranchor, prof E Buskens, dr KM Vermeulen, dr MJ Schroevers)
Spijkers W
Parenting and child psychosocial problems; effectiveness of parenting support in
preventive child healthcare
(prof SA Reijneveld, dr DEMC Jansen)
Ark M van
Patellar tendinopathy; physical therapy and injection treatments
(prof RL Diercks, prof JL Cook)
Boven JFM van
Enhancing adherence in patients with COPD: targets, interventions and cost-
effectiveness
(prof MJ Postma, prof T van der Molen)
R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Research Institute SHARE | 151
R
Gerbers JG
Computer assisted surgery in orthopedaedic oncology; indications, applications
and surgical workfl ow
(prof SK Bulstra, dr PC Jutte, dr M Stevens)
Niet A van der
Physical activity and cognition in children
(prof C Visscher, dr E Hartman, dr J Smith)
For more 2015 and earlier theses visit our website

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
154 | EXPAND

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
EXPAND | 155
E
Wetenschappelijk onderzoek afdeling Revalidatiegeneeskunde –Centrum voor Revalidatie UMCG
EXPANDExtremities, Pain and Disability
Missie: EXPAND draagt bij aan participatie en kwaliteit van leven van mensen met aandoeningen en
amputaties van de extremiteiten of met pijn aan het bewegingsapparaat.
EXPAND omvat twee speerpunten:• onderzoek naar aandoeningen aan en amputaties van extremiteiten met nadruk op
stoornissen, activiteiten en participatie,• onderzoek naar chronische pijn en arbeidsparticipatie.
EXPAND draagt bij aan het UMCG-brede thema Healthy Ageing.
Research Department of Rehabilitation Medicine –Center for Rehabilitation UMCG
EXPANDExtremities, Pain and Disability
Mission:EXPAND contributes to participation and quality of life of people with health conditions and
amputations of the extremities and musculoskeletal pain.
EXPAND includes two spearheads:• research on the health conditions and amputations of the extremities with emphasis on
body functions and structures, activities and participations,• chronic pain and work participation.
EXPAND contributes to Healthy Aging, the focus of the UMCG.