Proefschrift Cuperus
186
Strategies to improve non-pharmacological care in generalized osteoarthris Nienke Cuperus
-
Upload
nicole-nijhuis -
Category
Documents
-
view
224 -
download
6
description
Â
Transcript of Proefschrift Cuperus

Strategies to improve non-pharmacological
care in generalized osteoarthritis
Nienke Cuperus
Strategies to improve non-pharm
acological care in generalized osteoarthritis
N
ienke Cuperus
Uitnodiging
voor het bijwonen van de
openbare verdediging van
mijn proefschrift
Strategies to improve non-pharmacological
care in generalized osteoarthritis
Op maandag 6 juli
om 14.30 uur precies
in de aula van de Radboud
Universiteit Nijmegen,
Comeniuslaan 2 6525 HP
Nijmegen
U bent van harte welkom bij
deze plechtigheid en de
aansluitende receptie
Nienke Cuperus
Vermeerstraat 17,
6961 ZC Eerbeek
Paranimfen
Hans Cuperus (06-52481673)
Sanne Cuperus (06-42663351)


Strategies to improve non-pharmacological care
in generalized osteoarthritis
Nienke Cuperus

ISBN: 978-94-6108-992-2Cover design, layout and printing: Gildeprint, Enschede, the NetherlandsCopyright © 2015 by Nienke Cuperus. All rights reserved. No part of this thesis may be reproduced or transmitted in any form or by any means without the prior permission of the author.

Strategies to improve non-pharmacological care
in generalized osteoarthritis
Proefschrift
ter verkrijging van de graad van doctor aan de Radboud Universiteit Nijmegen
op gezag van de rector magnificus prof. dr. Th.L.M. Engelen, volgens besluit van het college van decanen
in het openbaar te verdedigen op maandag 6 juli 2015 om 14.30 uur precies
door
Nienke Cuperusgeboren op 25 november 1986
te Apeldoorn

Promotoren: Prof. dr. F.H.J. van den Hoogen Prof. dr. T.P.M. Vliet Vlieland (LUMC)
Copromotoren: Dr. C.H.M. van den Ende (St. Maartenskliniek, Nijmegen) Dr. T.J. Hoogeboom (UM)
Manuscriptcommissie: Prof. dr. M.W.G. Nijhuis-van der Sanden Prof. dr. C. Veenhof (UMCU) Prof. dr. A.E.R.C.H. Boonen (UM)

CONTENTS
Chapter 1 General introduction 7
Chapter 2 The clinical burden of generalized osteoarthritis represented by 23 self-reported health-related quality of life and activity limitations: a cross-sectional study
Chapter 3 Randomized trial of the effectiveness of a non-pharmacological 37 multidisciplinary face-to-face treatment program on daily function compared to a telephone-based treatment program in patients with generalized osteoarthritis
Chapter 4 Cost-utility and cost-effectiveness analysis of face-to-face versus 57 telephone-based non-pharmacological multidisciplinary treatment for patients with generalized osteoarthritis
Chapter 5 Measurement properties of the Health Assessment Questionnaire 75 Disability Index for generalized osteoarthritis
Chapter 6 Assessment and comparison of responsiveness of four patient 89 reported outcome measures to assess physical function in knee OA: WOMAC-PF subscale responds best
Chapter 7 Patient reported barriers and facilitators to using a self-management 107 booklet for hip and knee osteoarthritis in primary care: Results of a qualitative interview study
Chapter 8 Characterizing the concept of activity pacing as a 125 non-pharmacological intervention in rheumatology care: results of an international Delphi survey
Chapter 9 Summary and general discussion 143
Nederlandse samenvatting 163 List of publications 171 About the author 175 Dankwoord 179


CHAPTER 1
General introduction

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
8 | Chapter 1

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 9
1Why this thesis?Osteoarthritis (OA) is the most prevalent chronic joint disease, with a substantial impact on individuals and society1-3. Current OA research and daily clinical practice are mainly focused on a specific localization, whereas in many patients with OA, multiple joint sites are involved. The hand, spine and lower limb weight-bearing joints i.e. the hip and knee are the most common sites of disease involvement4. Generalized osteoarthritis (GOA) includes a subset of patients with clinically polyarticular OA and is an important and widely used OA phenotype5-7. However, to date research on (the management of) GOA is very limited. The purpose of this thesis is to improve knowledge on the non-pharmacological, non-surgical management of patients clinically diagnosed with GOA. In particular, we examined the clinical burden of patients with GOA and evaluated the efficacy of a non-pharmacological treatment program for patients with GOA. This chapter outlines the definition of GOA, as well as the epidemiology, pathophysiology and clinical symptoms. Furthermore, it summarizes evidence of the current non-pharmacological management of patients with GOA in daily practice and finally it introduces the research questions discussed in this thesis.
Definition of generalized osteoarthritisThe term GOA was introduced by Kellgren and Moore in 19528. Since then, multiple definitions of GOA have been suggested in the literature7. In Table 1, studies reporting explicit definitions of GOA are summarized. This table makes it clear that so far no agreed and validated definition of GOA is available; the threshold number of affected joints as well as the pattern of joint involvement have been described differently. The table shows 14 different definitions of GOA. Most definitions state that GOA involves at least three joints or joint groups. Besides, most definitions include the interphalangeal joints of the hands. In the literature, it has even been proposed that hand OA might be a marker for GOA9-13. However, defining GOA by the presence of hand OA is not widely accepted since GOA is also used to describe patients with OA in multiple joints without hand involvement14. The involvement of the knee in the definition of GOA is also common as shown in the table. However, there is little agreement on the necessity or appropriateness of the involvement of other joints such as the hip, spine or feet7,15,16. Indeed, increasing evidence shows that hand and knee OA aggregate together much more often than other joints11,17-19. In summary, we can state that most definitions of GOA include at least 3 joints or joint groups involving both the upper and lower extremities. Most definitions of GOA are based on radiographic findings independent of clinical symptoms. Since there is an imperfect correlation between symptoms and radiographic OA20 and symptoms are likely to be more important in functional outcomes, it is important to consider clinical symptoms next to structural changes in the definition of GOA21.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
10 | Chapter 1
Definition of GOA in this thesisIn this thesis we used a pragmatic definition of GOA formulated by Hoogeboom et al.22 which was based upon the current scientific literature and combined both radiological findings and clinical symptoms. We defined GOA as:
- Having complaints in three or more of eight joint areas (i.e. feet, knees, hips, lumbar spine, neck, shoulders, elbows and hands), and
- Having at least two objective signs that indicate OA in at least two of eight joint areas (objective signs indicating OA are: malalignment, crepitation, limited range of motion, palpable osteophytes/nodules or radiographic signs including the presence of joint space narrowing and/or osteophytes).
Epidemiology of GOAIn Table 1, data on the prevalence of GOA are summarized. To date, it is very difficult to accurately assess the prevalence of GOA given the variability of GOA definitions used and populations (setting, gender, age etc.) being assessed. As shown in the table, estimates of the frequency of GOA range from 1-90%, depending on the population studied. Despite the limited scientific literature on the prevalence of GOA, it has been suggested that patients with GOA represent a relatively large subgroup of patients with OA23-26. The number of patients with GOA is expected to grow substantially due to the aging population and the increasing prevalence of obesity throughout the world1,27.
Table 1. Summary of studies reporting explicit definitions of GOA and data on its prevalenceAuthor (year) GOA definition Setting Prevalence of
GOA (%)
Kellgren (1952)8 Heberden’s nodes and OA in CMC joint; radiological and clinical
Patients with OA attending an outpatient rheumatology clinic
52%
Lawrence (1969)28 OA in ≥ 3 joints or OA in ≥ 5 joints, at least one joint K&L grade ≥ 2; radiological
General population 20-25% ≥ 3 joints8-9% ≥ 5 joints
Doherty (1983)29 OA in > 3 IP joints; radiological Patients who had undergone unilateral knee meniscectomy
43%
Hart (1993)30 OA in DIP/PIP and CMC joint in addition to the knee; radiological and clinical
Women aged 45-64 years from the general population
Radiological: 2%Radiological and clinical: 1%
Loughlin (1994)31 Heberden’s nodes before age 60 and OA in ≥ 3 joint groups
ns 100% (population selected for GOA)
Dougados (1996)32 Either bilateral digital OA or spine and bilateral knee OA; radiological and clinical
Patients with OA from a hospital rheumatology department
44%
Cooper (1996)33 Age based: OA in ≥ 2 joints age 45-47 years or OA in ≥ 5 joints age 60-64; radiological K&L grade ≥ 2
Women from the general population
7% overall

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 11
1Gunther (1998)24 OA in ≥ 2 DIP/PIP joints and ≥ 1 CMC
joint in addition to the hip or knee; radiological K&L grade ≥ 2
Hospital-based population awaiting hip or knee arthroplasty
Knee OA: 35%Hip OA: 19%Overall: 27%
Malaviya (1998)34 Heberden’s nodes and DIP and PIP OA; radiological and clinical
Patients with OA attending an outpatient rheumatology clinic
4%
Naito (1999)35 OA in > 3 IP joints in each hand; radiological K&L score ≥ 2
Women with knee OA from an orthopaedic outpatient clinic
45%
Huang (2000)36 Hand OA (≥ 3 IP joints), hip OA and knee OA; radiological K&L score ≥2
Women with knee, hip, or hand OA visiting an orthopaedic outpatient clinic
17%
Min (2005)37 OA at multiple joints of the hand or OA in ≥ 2 of 4 joint sites (hand, knee, hip, spine); radiological*Ɨ and symptomaticƗ
Rotterdam study* and GARP studyƗ
23% 66%
Miura (2008)38 Bilateral knee and lumbar spine OA; radiological K&L score ≥ 2
General population 13%
Riyazi (2008)39 OA at multiple joints of the hand or OA in ≥ 2 joint sites (hand, spine, knee, hip); symptomatic and radiological
GARP studyƗ 90%
Carroll (2009)9 Type I: OA in ≥ 2 DIP or PIP joints and both knees or MTP1 joints Type II: OA in ≥ 2 MCP joints and OA in ≥ 1 atypical joint; clinical and radiological criteria
Patients with OA referred to a hospital rheumatology department
Type I: 58%
Type II: 42%
Forestier (2011)23 3 GOA criteria sets:1: Heberden’s nodes or OA in IP joint2: OA in ≥ 2 joints and spine OA3: bilateral digital OA or spine and bilateral knee OA; radiological and clinical manifestations
Patients with established knee OA
1: 14%2: 41%3: 42%52% met at least one of the three definitions
Abbreviations: OA = osteoarthritis, CMC = carpometacarpal, IP = interphalangeal, DIP = distal interphalangeal, MTP = Metatarsophalangeal, ns = not specified or no data, K&L = Kellgren & Lawrence*Population-based cohort study on the determinants and prognosis of chronic diseases in the elderlyƗ Genetics, Arthrosis and Progression (GARP) Study on Dutch Caucasian sib pairs with predominantly symptomatic OA at multiple sites to identify determinants of OA susceptibility and progression
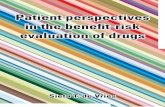
Pathophysiology and risk factorsOsteoarthritis is a complex disease in which all structures that constitute a joint might be involved. The pathophysiology of OA has long been thought to be a failure of the repair process of damaged cartilage due to biomechanical changes in the joint. However, recent evidence shows an additional and integrated role of bone, synovial tissue and peri-articular tissues such as ligaments and muscles1 (Figure 1). Moreover, it has been recognized that synovial inflammation (synovitis) is common in OA, resulting clinically in joint swelling and pain40. The role of genetic factors in the development of GOA has received considerable attention during the last decade. Increasing evidence shows that genetic factors are a major risk factor for GOA, probably more than in other forms of OA17,37,39,41,42. This finding has been

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
12 | Chapter 1
shown especially by the GARP study, defining GOA as having OA at multiple joints of the hand or OA in ≥ 2 joint sites (hand, spine, knee, hip). Furthermore, an increased frequency of GOA or higher risk of GOA progression was found to be associated with a higher age, a higher BMI15,43,44 and a higher bone mineral density45,46. Results are, however inconsistent across studies, what might be explained by the lack of a uniform definition of GOA.
9general introduction
OA is characterized by a failure of the repair process of damaged cartilage due to bio-
mechanical changes in the joint.7 However, recent evidence shows an additional and inte-
grated role of bone and synovial tissue, and patchy chronic synovitis that is evident in the
disease.8 Patients with hip or knee OA present similar symptoms (Figure 2). Usage-related
pain is the most important symptom, often worse towards the end of the day, relieved by
rest. Other typical symptoms are morning or inactivity stiffness, impaired function, and
bone deformation; all contributing to the disability of OA and diminishing of patients’
quality of life.7 The extent and severity of symptoms vary considerably among patients.9
Identified risk factors of hip and knee OA are increasing age, intense sport activity, higher
body mass index, previous injury, and genetic predisposition. Additional risk factors of
knee OA are muscle weakness, smoking, malalignment, and female gender.7,10 However,
the prevention of OA is difficult, as these factors increase the risk for OA only moderately
and the presence of single factors might not be strong enough to justify their use in iden-
tifying subjects who should receive preventive interventions.10 The presence of multiple
risk factors and their interaction with each other, are probably the key factors to identify
people at major risk.
In general, hip and knee OA develops progressively over several years. An extensive syste-
matic review shows a deterioration of pain and functional status in patients with hip or
knee OA after 3 years of follow-up.9 However, this was not seen for the first 3 years of fol-
low-up. Prognostic factors of the progression of OA include biomechanical, psychological,
and clinical factors.11-13 Those factors that are modifiable, e.g. reduced muscle strength,
laxity of the knee joint, proprioceptive inaccuracy, overweight, and a lack of physical activity,
are therefore considered important elements for treatment.
Figure 2. A normal joint and osteoarthritic joint
Subchondral bone changes (sclerosis)
Joint space narrowing
Cartilage damageInflammation of the synovium (synovitis)
New bone formation (osteophyte)Thickening of the joint capsule
Muscle weakness
Dutch Arthritis Foundation ©. Printed with permission.
AS proefschrift binnenwerk.indd 9 13-04-14 20:57
Figure 1. Normal joint and osteoarthritic joint
Clinical symptoms of GOAThe predominant symptoms of GOA are pain, joint stiffness and loss of function, mostly related to mobility (in particular walking) and doing household chores. However, the impact of GOA on clinical outcomes is largely unknown since OA populations are mostly examined for a specific joint or group of joints without considering the involvement of multiple joints. Previous studies have examined the association between multiple joint involvement (e.g. joint pain comorbidity) and clinical outcomes in joint specific OA cohorts (hip or knee OA), showing poorer outcomes for pain, function and quality of life than in single joint OA25,26,47,48. However, in those studies, the nature of the additional musculoskeletal complaints is unknown and might be unrelated to OA. So far, only one study assessed the impact of GOA on health status, showing that patients with GOA did not have a poorer quality of life than individuals with hip or knee OA only49. However, the limited sample size in that study (n = 30) prevents firm conclusions. Improved understanding of the health status of patients with GOA can be used by clinicians and researchers to improve the management and quality of care for patients with GOA.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 13
1Assessment of GOAThe assessment of daily function has emerged as an integral part of OA clinical practice and research, using health-related patient-reported outcome measures (HR-PROs). As such, numerous disease-specific validated HR-PROs are available to assess functional limitations in patients with OA, such as the Western Ontario and McMaster Universities Arthritis Index (WOMAC). However, existing OA-specific HR-PROs all focus on a specific localization of OA (e.g. the hands, hips or knees), reflecting either activities of lower extremity or upper extremity function. Since individuals with GOA typically suffer from limitations of both upper and lower extremity function, existing OA specific instruments inadequately reflect functional limitations, limiting their use in GOA. In addition, no studies have reported on the measurement properties of existing HR-PROs to assess functional limitations in patients with GOA. As such, we lack a validated instrument. To increase the body of knowledge on the functional limitations of patients with GOA, instruments with adequate measurement properties, in particular content validity and responsiveness, are warranted. In this thesis, we evaluated the measurement properties of the Health Assessment Questionnaire Disability Index (HAQ-DI), widely used in rheumatoid arthritis (RA), to assess daily function in patients with GOA. These results can be used to guide clinicians and researchers in the assessment of functional limitations in patients with GOA.
Non-pharmacological treatment for people with GOASeveral international consensus-based clinical guidelines for the management of OA are available, emphasizing the importance and efficacy of non-pharmacological, non-surgical treatment modalities50-54. However, these guidelines all focus on single joint involvement (i.e. the hand, hip or knee), without considering the involvement of multiple joints50,51,53,54. Recently, the Osteoarthritis Research Society International (OARSI) published the first recommendations for the non-surgical management of OA for several OA subpopulations, including multiple joint OA (defined as OA in other joints in addition to the knee)52. However, due to the limited research performed on the management of multiple joint OA, the authors only considered balneotherapy/spa therapy (defined as the use of baths containing thermal mineral waters) appropriate for patients with multiple joint OA, whereas no other recommendations could be formulated. Indeed, studies evaluating the effectiveness of non-pharmacological treatment for patients with GOA are very scarce. To our knowlegde, only two studies investigated the effect of a non-pharmacological intervention for patients with GOA. Recently, Foresterier et al.55 showed that crenobaltherapy (spa therapy) in combination with home exercises provided better improvements in pain and function than home exercises alone. However, in that study the primary outcome measure was physcial function measured with the WOMAC which comprises only items of lower extremity function. Another study by Bolthuis et al.57 investigated the efficacy of an intensive exercise program for patients

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
14 | Chapter 1
with GOA. In that study however, the definition of GOA was unclear and patients recently underwent joint replacement, hampering the generalizability of the findings. The lack of research on the management of GOA and the substantial group of patients with GOA warrant the development and evaluation of a non-pharmacological, non-surgical treatment program for patients with GOA necessitating a clinically relevant GOA definition and appropriate outcome measures. In absence of recommendations for the management of GOA, guidelines for the treatment of single joint OA could be considered as starting point to develop interventions for patients with GOA. Recommendations in these guidelines could be used to tailor treatment options to the needs of patients with GOA. In a recently published systematic review evaluating OA guidelines, three non-pharmacological core interventions have been identified which should be included in the management of patients with GOA: (1.) education and self-management; (2.) exercise and weight loss; and (3.) assistive devices and home adaptations53.
Education and self-managementExisting guidelines uniformly recommend education, lifestyle advices and self-management. Self-management interventions can be described as behavioural interventions designed to encourage people to take an active role in the management of their own condition56,57. These interventions often target on patient education and lifestyle modification57. Substantial variation exists in the delivery of self-management interventions, such as the mode of care delivery (face-to-face, internet, telephone or written information such as care booklets), the audience (group, individual) or the duration and frequency57. In general, small effect sizes of self-management programs for people with OA have been reported in systematic reviews and clinical guidelines for the management of hip and knee OA (ES = 0.06 for pain, 95% CI 0.02 to 0.10 and ES = 0.06 for physical function, 95% CI 0.02 to 0.10)50,58. Nevertheless, the importance of self-management is uniformly advocated in international clinical guidelines in order to manage the disease effectively50,51,53,58. It is therefore conceivable that recommendations regarding self-management are rather based on clinical expertise and patient values than on research evidence.
A recommended and widely endorsed component of OA self-management programs within the context of multidisciplinary treatment is activity pacing. Activity pacing is the advice most frequently given by British and Dutch rheumatology nurses to patients with RA and it is one of the self-management strategies most frequently applied by patients to decrease pain and fatigue59-63. In OA research and clinical practice, activity pacing is mainly based on the principle of energy conservation. However, the use of activity pacing is purely pragmatic and it remains a poorly understood concept64-66. The implications of a poor conceptualization of activity pacing are significant in both research and rheumatology practice. Therefore in this thesis we attempt to clarify the concept of activity pacing among an international, multidisciplinary group of experts.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 15
1Exercises and weight lossThere is strong agreement within guidelines regarding the effectiveness of exercises, especially for patients with hip and knee OA. There is less agreement on the benefits of exercises related to hand OA53,67. A recently published systematic review showed land-based therapeutic exercises to reduce pain (ES = -0.49, 95% CI -0.39 to -0.59), improve physical function (ES = -0.52, 95% CI -0.39 to -0.65) and improve quality of life (ES = 0.28, 95% CI 0.15 to 0.40) in people with knee OA68. The authors concluded that the magnitude of the treatment effect for pain and physical function was influenced by the number of individual face-to-face contact occasions with the healthcare provider supervising the program. In hip OA, exercises have shown to reduce pain (ES = -0.38, 95% CI -0.55 to -0.20) and improve physical function (ES = -0.33, 95% CI -0.53 to -0.13)69. Furthermore, water-based exercises showed small to moderate effect sizes for pain (ES = 0.19, 95% CI 0.04 to 0.35) and function (ES = 0.26, 95% CI 0.11 to 0.42) in people with hip and knee OA58,70. Weight loss is strongly recommended in overweight individuals with knee OA. Small to moderate effect sizes for pain (ES = 0.20, 95% CI 0.00 to 0.39) and function (ES = 0.23, 95% CI 0.04 to 0.42) have been shown71. Currently, no evidence is available supporting the effect of weight loss in patients with hip OA50,58. Increasing evidence recognizes that the combination of exercises and weight loss should be the mainstays of rehabilitation for people with knee and hip OA72,73. Furthermore, evidence is growing for beneficial effects of tai chi. A systematic review showed tai chi to improve pain in patients with hip or knee OA with effect sizes ranging from 0.28 to 1.6774.
Assistive devices and home adaptationsAssistive devices and home adaptations can help patients to improve or maintain activities of daily living and/or reduce pain. Walking aids, assistive technology and adaptations at home are therefore important and often used by people with hip or knee OA50. The value of some of these interventions is so obvious and has an immediate effect that further research into the effectiveness of these interventions can hardly be expected50. The use of a cane in patients with knee OA has been investigated, showing that daily cane use can reduce pain (ES = 0.18, 95% CI -0.42 to 0.87) and improve physical function (ES = 0.13, 95% CI -0.11 to 0.42)75. International guidelines generally recommend that in all patients with hip or knee OA walking aids, assistive technology and adaptations at home should be considered systematically and recurrently50,53,76. Several guidelines recommend to discuss appropriate footwear in patients with hip or knee OA50,76,77.
Cost-effectiveness of non-pharmacological treatment for people with GOADespite evidence for non-pharmacological, non-surgical interventions to manage OA, evidence for the cost-effectiveness of these interventions is limited as concluded in a systematic review on the cost-effectiveness of non-pharmacological interventions for patients with hip and

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
16 | Chapter 1
knee OA78. Based on the available studies, the authors suggested that exercise programs appear to be the best value for money in the management of hip and knee OA. In hand OA, it has also been shown that exercises are the most cost-effective management strategy79. However, no economic evaluations are available for non-pharmacological interventions for the management of patients with GOA. In this thesis, we evaluated the cost-effectiveness of two non-pharmacological treatment programs for patients with GOA.
Outline of this thesisThe primary aim of this thesis is to examine the health status of patients with GOA and to evaluate the (cost)effectiveness of a non-pharmacological multidisciplinary face-to-face group-based treatment program for patients with GOA compared to a telephone-based treatment program during the first year after treatment was started. The content of the chapters in this thesis is outlined below.
In chapter 2, the health status of patients with GOA as measured by self-reported health realted quality of life and activity limitations is described. In chapter 3, results of a randomzed clinical trial comparing the effectiveness of a non-pharmacological multidisciplinary face-to-face group-based treatment program with a telephone-based treatment program on daily function for patients with GOA (during the first year after treatment was started) are presented. Chapter 4 describes from a societal perspective a cost-effectiveness and cost-utility analysis alongside the randomized clinical trial described in Chapter 4. In chapter 5, the measurement properties, i.e. interpretability, validity, reliability and responsiveness of the Health Assessment Questionnaire Disability Index (HAQ-DI) to measure daily function in patients with GOA are evaluated.In chapter 6, a comparison of the responsiveness of four widely used patient reported outcome measures (i.e. the McMaster University Osteoarthritis Index (WOMAC), the Lower Extremity Functional Scale (LEFS), the Knee disability and Osteoarthritis Outcome Score (KOOS) and the Lequesne Algofunctional index (LAI)) to measure physical function in patients with knee OA is described. These results can be used to guide clinicians and researchers in selecting the most appropriate physical function measure in clinical trials to evaluate the effectiveness of an intervention in patients with knee OA.In chapter 7, patients’ views on a tailored-made self-management tool for patients with hip or knee osteoarthritis, i.e. the self-management booklet “Care for Osteoarthritis” (in Dutch: “Zorgwijzer Artrose ©”) are presented. This booklet was developed to educate patients about their disease and existing treatment options and to improve self-management and patient-healthcare provider communication.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 17
1In chapter 8, the results of an international Delphi survey to clarify the concept of activity pacing as a non-pharmacological intervention in rheumatology care are presented. This study is a collaboration between clinicians and healthcare professionals experienced with activity pacing among 12 different countries. Chapter 9 summarizes the results of this thesis and discusses the main findings. Furthermore, implications for clinical practice and directions for future research are provided.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
18 | Chapter 1
References
1. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet 2011; 377: 2115-26
2. Breedveld FC. Osteoarthritis--the impact of a serious disease. Rheumatology.(Oxford) 2004; 43 Suppl 1: i4-i8
3. Brooks PM. Impact of osteoarthritis on individuals and society: how much disability? Social consequences and health economic implications. Curr.Opin.Rheumatol. 2002; 14: 573-7
4. Petersson IF, Jacobsson LT. Osteoarthritis of the peripheral joints. Best.Pract.Res.Clin.Rheumatol. 2002; 16: 741-60
5. Bierma-Zeinstra SM, Verhagen AP. Osteoarthritis subpopulations and implications for clinical trial design. Arthritis Res.Ther. 2011; 13: 213
6. Felson DT. Identifying different osteoarthritis phenotypes through epidemiology. Osteoarthritis.Cartilage. 2010; 18: 601-4
7. Nelson AE, Smith MW, Golightly YM, Jordan JM. “Generalized osteoarthritis”: A systematic review. Semin.Arthritis Rheum. 2014; 43: 713-20
8. KELLGREN JH, MOORE R. Generalized osteoarthritis and Heberden’s nodes. Br.Med.J. 1952; 1: 181-7
9. Carroll GJ, Breidahl WH, Jazayeri J. Confirmation of two major polyarticular osteoarthritis (POA) phenotypes--differentiation on the basis of joint topography. Osteoarthritis.Cartilage. 2009; 17: 891-5
10. Haugen IK, Cotofana S, Englund M, Kvien TK, Dreher D, Nevitt M et al. Hand joint space narrowing and osteophytes are associated with magnetic resonance imaging-defined knee cartilage thickness and radiographic knee osteoarthritis: data from the Osteoarthritis Initiative. J.Rheumatol. 2012; 39: 161-6
11. Haugen IK. The puzzle of generalized osteoarthritis (OA) -- is OA a systemic enthesopathy? J.Rheumatol. 2012; 39: 203-5
12. Irlenbusch U, Schaller T. Investigations in generalized osteoarthritis. Part 1: genetic study of Heberden’s nodes. Osteoarthritis.Cartilage. 2006; 14: 423-7
13. Irlenbusch U, Dominick G. Investigations in generalized osteoarthritis. Part 2: special histological features in generalized osteoarthritis (histological investigations in Heberden’s nodes using a histological score). Osteoarthritis.Cartilage. 2006; 14: 428-34
14. Vignon E. Hand osteoarthritis and generalized osteoarthritis: a need for clarification. Osteoarthritis.Cartilage. 2000; 8 Suppl A: S22-S24
15. Riyazi N, Meulenbelt I, Kroon HM, Ronday KH, Hellio le Graverand MP, Rosendaal FR et al. Evidence for familial aggregation of hand, hip, and spine but not knee osteoarthritis in siblings with multiple joint involvement: the GARP study. Ann.Rheum.Dis. 2005; 64: 438-43
16. Sun Y, Brenner H, Sauerland S, Gunther KP, Puhl W, Sturmer T. Serum uric acid and patterns of radiographic osteoarthritis--the Ulm Osteoarthritis Study. Scand.J.Rheumatol. 2000; 29: 380-6
17. Bijsterbosch J, Meulenbelt I, Watt I, Rosendaal FR, Huizinga TW, Kloppenburg M. Clustering of hand osteoarthritis progression and its relationship to progression of osteoarthritis at the knee. Ann.Rheum.Dis. 2014; 73: 567-72
18. Dahaghin S, Bierma-Zeinstra SM, Reijman M, Pols HA, Hazes JM, Koes BW. Does hand osteoarthritis predict future hip or knee osteoarthritis? Arthritis Rheum. 2005; 52: 3520-7
19. Hirsch R, Lethbridge-Cejku M, Scott WW, Jr., Reichle R, Plato CC, Tobin J et al. Association of hand and knee osteoarthritis: evidence for a polyarticular disease subset. Ann.Rheum.Dis. 1996; 55: 25-9
20. Bedson J, Croft PR. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the literature. BMC.Musculoskelet.Disord. 2008; 9: 116
21. Nelson AE, Elstad E, Devellis RF, Schwartz TA, Golightly YM, Renner JB et al. Composite measures of multi-joint symptoms, but not of radiographic osteoarthritis, are associated with functional outcomes: the Johnston County Osteoarthritis Project. Disabil.Rehabil. 2014; 36: 300-6

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 19
1 22. Hoogeboom TJ, Stukstette MJ, de Bie RA,
Cornelissen J, den Broeder AA, van den Ende CH. Non-pharmacological care for patients with generalized osteoarthritis: design of a randomized clinical trial. BMC.Musculoskelet.Disord. 2010; 11: 142
23. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011; 78: 275-8
24. Gunther KP, Sturmer T, Sauerland S, Zeissig I, Sun Y, Kessler S et al. Prevalence of generalised osteoarthritis in patients with advanced hip and knee osteoarthritis: the Ulm Osteoarthritis Study. Ann.Rheum.Dis. 1998; 57: 717-23
25. Perruccio AV, Power JD, Evans HM, Mahomed SR, Gandhi R, Mahomed NN et al. Multiple joint involvement in total knee replacement for osteoarthritis: Effects on patient-reported outcomes. Arthritis Care Res.(Hoboken.) 2012; 64: 838-46
26. Suri P, Morgenroth DC, Kwoh CK, Bean JF, Kalichman L, Hunter DJ. Low back pain and other musculoskeletal pain comorbidities in individuals with symptomatic osteoarthritis of the knee: data from the osteoarthritis initiative. Arthritis Care Res.(Hoboken.) 2010; 62: 1715-23
27. Laberge MA, Baum T, Virayavanich W, Nardo L, Nevitt MC, Lynch J et al. Obesity increases the prevalence and severity of focal knee abnormalities diagnosed using 3T MRI in middle-aged subjects--data from the Osteoarthritis Initiative. Skeletal Radiol. 2012; 41: 633-41
28. Lawrence JS. Generalized osteoarthrosis in a population sample. Am.J.Epidemiol. 1969; 90: 381-9
29. Doherty M, Watt I, Dieppe P. Influence of primary generalised osteoarthritis on development of secondary osteoarthritis. Lancet 1983; 2: 8-11
30. Hart DJ, Spector TD. Cigarette smoking and risk of osteoarthritis in women in the general population: the Chingford study. Ann.Rheum.Dis. 1993; 52: 93-6
31. Loughlin J, Irven C, Fergusson C, Sykes B. Sibling pair analysis shows no linkage of generalized osteoarthritis to the loci encoding type II collagen, cartilage link protein or cartilage matrix protein. Br.J.Rheumatol. 1994; 33: 1103-6
32. Dougados M, Nakache JP, Gueguen A. Criteria for generalized and focal osteoarthritis. Rev.Rhum.Engl.Ed 1996; 63: 569-75
33. Cooper C, Egger P, Coggon D, Hart DJ, Masud T, Cicuttini F et al. Generalized osteoarthritis in women: pattern of joint involvement and approaches to definition for epidemiological studies. J.Rheumatol. 1996; 23: 1938-42
34. Malaviya AN, Shebab D, Bhargava S, Al-Jarallah K, Al-Awadi A, Sharma PN et al. Characteristics of osteoarthritis among Kuwaitis: a hospital-based study. Clin Rheumatol 1998; 17: 210-3
35. Naito K, Takahashi M, Kushida K, Suzuki M, Ohishi T, Miura M et al. Measurement of matrix metalloproteinases (MMPs) and tissue inhibitor of metalloproteinases-1 (TIMP-1) in patients with knee osteoarthritis: comparison with generalized osteoarthritis. Rheumatology.(Oxford) 1999; 38: 510-5
36. Huang J, Ushiyama T, Inoue K, Kawasaki T, Hukuda S. Vitamin D receptor gene polymorphisms and osteoarthritis of the hand, hip, and knee: acase-control study in Japan. Rheumatology.(Oxford) 2000; 39: 79-84
37. Min JL, Meulenbelt I, Riyazi N, Kloppenburg M, Houwing-Duistermaat JJ, Seymour AB et al. Association of the Frizzled-related protein gene with symptomatic osteoarthritis at multiple sites. Arthritis Rheum. 2005; 52: 1077-80
38. Miura H, Kawano T, Takasugi S, Manabe T, Hosokawa A, Iwamoto Y. Two subtypes of radiographic osteoarthritis in the distal interphalangeal joint of the hand. J.Orthop.Sci. 2008; 13: 487-91
39. Riyazi N, Rosendaal FR, Slagboom E, Kroon HM, Breedveld FC, Kloppenburg M. Risk factors in familial osteoarthritis: the GARP sibling study. Osteoarthritis.Cartilage. 2008; 16: 654-9
40. Wenham CY, Conaghan PG. The role of synovitis in osteoarthritis. Ther.Adv.Musculoskelet.Dis. 2010; 2: 349-59
41. Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM et al. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann.Intern.Med. 2000; 133: 635-46
42. Kraus VB, Jordan JM, Doherty M, Wilson AG, Moskowitz R, Hochberg M et al. The Genetics of Generalized Osteoarthritis (GOGO) study: study design and evaluation of osteoarthritis phenotypes. Osteoarthritis.Cartilage. 2007; 15: 120-7

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
20 | Chapter 1
43. Cerhan JR, Wallace RB, el-Khoury GY, Moore TE. Risk factors for progression to new sites of radiographically defined osteoarthritis in women. J.Rheumatol. 1996; 23: 1565-78
44. Sturmer T, Gunther KP, Brenner H. Obesity, overweight and patterns of osteoarthritis: the Ulm Osteoarthritis Study. J.Clin.Epidemiol. 2000; 53: 307-13
45. Hordon LD, Stewart SP, Troughton PR, Wright V, Horsman A, Smith MA. Primary generalized osteoarthritis and bone mass. Br.J.Rheumatol. 1993; 32: 1059-61
46. Price T, Hesp R, Mitchell R. Bone density in generalized osteoarthritis. J.Rheumatol. 1987; 14: 560-2
47. Hoogeboom TJ, den Broeder AA, Swierstra BA, de Bie RA, van den Ende CH. Joint-pain comorbidity, health status, and medication use in hip and knee osteoarthritis: a cross-sectional study. Arthritis Care Res.(Hoboken.) 2012; 64: 54-8
48. Hoogeboom TJ, den Broeder AA, de Bie RA, van den Ende CH. Longitudinal impact of joint pain comorbidity on quality of life and activity levels in knee osteoarthritis: data from the Osteoarthritis Initiative. Rheumatology.(Oxford) 2013; 52: 543-6
49. Moe RH, Grotle M, Kjeken I, Hagen KB, Kvien TK, Uhlig T. Disease impact of hand OA compared with hip, knee and generalized disease in specialist rheumatology health care. Rheumatology.(Oxford) 2013; 52: 189-96
50. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann.Rheum.Dis. 2013; 72: 1125-35
51. Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res.(Hoboken.) 2012; 64: 465-74
52. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis.Cartilage. 2014; 22: 363-88
53. Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of
recommendations and guidelines for the management of osteoarthritis: The Chronic Osteoarthritis Management Initiative of the U.S. Bone and Joint Initiative. Semin.Arthritis Rheum. 2014; 43: 701-12
54. Zhang W, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann.Rheum.Dis. 2010; 69: 483-9
55. Forestier R, Genty C, Waller B, Francon A, Desfour H, Rolland C et al. Crenobalneotherapy (spa therapy) in patients with knee and generalized osteoarthritis: A post-hoc subgroup analysis of a large multicentre randomized trial. Ann.Phys.Rehabil.Med. 2014; 57: 213-27
56. Iversen MD, Hammond A, Betteridge N. Self-management of rheumatic diseases: state of the art and future perspectives. Ann.Rheum.Dis. 2010; 69: 955-63
57. Kroon FP, van der Burg LR, Buchbinder R, Osborne RH, Johnston RV, Pitt V. Self-management education programmes for osteoarthritis. Cochrane.Database.Syst.Rev. 2014; 1: CD008963
58. Zhang W, Nuki G, Moskowitz RW, Abramson S, Altman RD, Arden NK et al. OARSI recommendations for the management of hip and knee osteoarthritis: part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis.Cartilage. 2010; 18: 476-99
59. Gong G, Li J, Li X, Mao J. Pain experiences and self-management strategies among middle-aged and older adults with arthritis. J.Clin.Nurs. 2013; 22: 1857-69
60. Kjeken I, Darre S, Slatkowsky-Cristensen B, Hermann M, Nilsen T, Eriksen CS et al. Self-management strategies to support performance of daily activities in hand osteoarthritis. Scand.J.Occup.Ther. 2013; 20: 29-36
61. Repping-Wuts H, Uitterhoeve R, van RP, van AT. Fatigue as experienced by patients with rheumatoid arthritis (RA): a qualitative study. Int.J.Nurs.Stud. 2008; 45: 995-1002
62. Repping-Wuts H, Hewlett S, van RP, van AT. Fatigue in patients with rheumatoid arthritis: British and Dutch nurses’ knowledge, attitudes and management. J.Adv.Nurs. 2009; 65: 901-11

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction | 21
1 63. Sandstrom MJ, Keefe FJ. Self-management
of fibromyalgia: the role of formal coping skills training and physical exercise training programs. Arthritis Care Res. 1998; 11: 432-47
64. Murphy SL, Smith DM, Lyden AK. Type of activity pacing instruction affects physical activity variability in adults with symptomatic knee or hip osteoarthritis. J.Phys.Act.Health 2012; 9: 360-6
65. Nielson WR, Jensen MP, Karsdorp PA, Vlaeyen JW. Activity Pacing in Chronic Pain: Concepts, Evidence, and Future Directions. Clin.J.Pain 2013; 29: 461-8
66. Schepens SL, Braun ME, Murphy SL. Effect of tailored activity pacing on self-perceived joint stiffness in adults with knee or hip osteoarthritis. Am.J.Occup.Ther. 2012; 66: 363-7
67. Kjeken I, Smedslund G, Moe RH, Slatkowsky-Christensen B, Uhlig T, Hagen KB. Systematic review of design and effects of splints and exercise programs in hand osteoarthritis. Arthritis Care Res.(Hoboken.) 2011; 63: 834-48
68. Fransen M, McConnell S, Harmer AR, van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee. Cochrane.Database.Syst.Rev. 2015; 1: CD004376
69. Fransen M, McConnell S, Hernandez-Molina G, Reichenbach S. Exercise for osteoarthritis of the hip. Cochrane.Database.Syst.Rev. 2014; 4: CD007912
70. Bartels EM, Lund H, Hagen KB, Dagfinrud H, Christensen R, Danneskiold-Samsoe B. Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane.Database.Syst.Rev. 2007; CD005523
71. Christensen R, Bartels EM, Astrup A, Bliddal H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann.Rheum.Dis. 2007; 66: 433-9
72. Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes.Rev. 2014; 15: 578-86
73. Maly MR, Robbins SM. Osteoarthritis Year in Review 2014: rehabilitation and outcomes. Osteoarthritis.Cartilage. 2014; 22: 1958-88
74. Lee MS, Lee EN, Ernst E. Is tai chi beneficial for improving aerobic capacity? A systematic review. Br.J.Sports Med. 2009; 43: 569-73
75. Jones A, Silva PG, Silva AC, Colucci M, Tuffanin A, Jardim JR et al. Impact of cane use on pain, function, general health and energy expenditure during gait in patients with knee osteoarthritis: a randomised controlled trial. Ann.Rheum.Dis. 2012; 71: 172-9
76. National Collaborating Centre for Chronic Conditions. Osteoarthritis: national clinical guideline for care and management in adults. London: Royal College of Physicians. 2008
77. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
78. Pinto D, Robertson MC, Hansen P, Abbott JH. Cost-Effectiveness of Nonpharmacologic, Nonsurgical interventions for Hip and/or Knee Osteoarthritis: Systematic Review. Value Health 2012; 15: 1-12
79. Oppong R, Jowett S, Nicholls E, Whitehurst DG, Hill S, Hammond A et al. Joint protection and hand exercises for hand osteoarthritis: an economic evaluation comparing methods for the analysis of factorial trials. Rheumatology.(Oxford) 2015; 54: 876-83


CHAPTER 2
The clinical burden of generalized osteoarthritis
represented by self-reported health-related quality of life
and activity limitations: a cross-sectional study
Nienke Cuperus, Thea P.M. Vliet Vlieland, Elien A.M. Mahler, Clarinda C. Kersten, Thomas J. Hoogeboom, Cornelia H.M. van den Ende
Published in: Rheumatology International. 2015; 35(5): 871-877

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
24 | Chapter 2
Abstract
ObjectiveThe involvement of multiple joints is common in osteoarthritis (OA), often referred to as generalized osteoarthritis (GOA). However, since research and practice mainly focus on a specific OA localization, the health status of patients with GOA is largely unknown. Therefore, we aimed to describe the clinical burden of GOA in terms of self-reported health related quality of life (HRQoL) and activity limitations.
MethodsIn this cross-sectional study, individuals clinically diagnosed with GOA and referred to multidisciplinary treatment, completed questionnaires on socio-demographics, joint involvement, HRQoL (SF-36) and activity limitations (HAQ-DI). SF-36 physical (PCS) and mental component summary scores (MCS) were calculated using norm-based data. The patient’s specific most important activity limitations were linked to the International Classification of Functioning, Disability and Health.
ResultsA total of 147 patients participated (85% female; mean (SD) age 60 (8) years). The majority (93%) had symptomatic OA in both the upper and lower extremities. Predominant joints with symptomatic OA were the hands (85%) and knees (82%). Mean (SD) SF-36 PCS and MCS scores were 37 (7) and 48 (10) respectively, showing a broad impact of GOA on the physical component of health. The mean (SD) HAQ-DI score was 1.27 (0.50) indicating moderate to severe functional limitations. Activities concerning mobility and domestic life were considered most important activity limitations, especially walking.
ConclusionsThe results show a high clinical burden of GOA in terms of HRQoL and activity limitations. This study point to the need of developing non-pharmacological interventions for patients with GOA that should target on improving the physical component of health and mobility limitations.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
The clinical burden of GOA | 25
2
Introduction
Osteoarthritis (OA) is the most prevalent chronic joint disease that can affect multiple joints1. The hands and the lower limb weight-bearing joints i.e. the hip and knee are the most common sites of disease involvement2. Generalized osteoarthritis (GOA) is an important and widely accepted OA phenotype, describing the often polyarticular nature of OA3-5. The term GOA was first used by Kellgren and Moore in 19526. Since then multiple definitions of GOA have been suggested. However, a recently published review showed that there is still no widely accepted and validated definition of GOA5. Nevertheless, it has been suggested that individuals with GOA might represent a relatively large subgroup of patients with OA7-9. In knee OA populations, approximately 50% of patients can be classified as GOA according to three different criteria sets7.
Current research and clinical practice mostly examine OA populations for a specific localization of OA, without considering the involvement of multiple joints. As such, research on GOA is very limited. The impact of GOA on patient’s health status is therefore largely unknown. A few previous studies have examined the association between multiple joint involvement (e.g. joint pain comorbidity) and health outcomes in patients with hip and knee OA, showing poorer outcomes for pain, function and quality of life than in single joint OA10-13. However, in those studies the nature of the additional musculoskeletal complaints is unknown and might be unrelated to OA. To the best of our knowledge there are no studies that comprehensively assessed the health status of patients clinically diagnosed with GOA. So far, only one study assessed the impact of GOA on health status, showing that patients with GOA (radiographic OA in ≥ 2 joints) did not have a poorer quality of life than individuals with hip or knee OA only14. However, the limited sample size in that study (n = 30) prevents firm conclusions.
Improved understanding of the health status of patients with GOA is warranted considering the high prevalence of GOA and the lack of research. Information on the health status of patients with GOA might be used by clinicians and researchers to improve the management and quality of care for patients with GOA. Therefore the aim of the current study was (1) to describe the clinical burden of patients clinically diagnosed with GOA in terms of self-reported health related quality of life (HRQoL) and activity limitations, and (2) to identify commonly reported, self-perceived activity limitations and participation restrictions in patients with GOA.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
26 | Chapter 2
Method
Study DesignFor this cross-sectional study, we used baseline data from a randomized clinical trial comparing the effectiveness of two multidisciplinary non-pharmacological treatment programs for patients with GOA, performed at the outpatient rheumatology departments of the Sint Maartenskliniek Hospitals in the Netherlands. Participants were allocated to either a multidisciplinary group-based self-management program or a telephone-based self-management program. The complete study design has been described previously15. The Institutional Review Board of the Radboud University Medical Nijmegen Centre approved the study and all patients signed informed consent.
ParticipantsRecruitment to the study took place between January 2010 and March 2013. During an outpatient visit, patients clinically diagnosed with GOA and referred by their rheumatologist for treatment were invited for a screening visit with an occupational therapist, physical therapist and researcher to consider eligibility to participate in the trial. Patients were eligible when meeting all of the following inclusion criteria: (1) aged ≥ 18 years; (2) having objective signs of OA in at least two joint areas on the basis of the patient’s medical file (objective signs included: malalignment, crepitation, limited range of motion, palpable osteophytes/nodules or radiographic signs including the presence of joint space narrowing and/or osteophytes); (3) having clinical symptoms in ≥ 3 out of 8 joint areas; (4) being limited in the performance of daily activities (Health Assessment Questionnaire Disability Index (HAQ-DI) score > 0.5); and (5) being motivated to alter your lifestyle and willing to participate in a group. Excluded were patients who were: (1) diagnosed with another rheumatic disease; (2) awaiting surgery; (3) already participated unsuccessfully in a self-management program; (4) having psychosocial problems interfering with the scope of the treatment program (on the basis of clinical judgement of a physical therapist and occupational therapist); (5) incapable of coming to the hospital; or (6) unable to write and or understand the Dutch language.
Data collectionPrior to the start of the treatment programs all patients completed a standardized set of health related patient-reported outcome measures to assess socio-demographic characteristics, fatigue, joint involvement, activity limitations and HRQoL. Socio-demographic characteristics included age, sex, education, marital status and occupation. Height and weight were recorded to calculate the body mass index (BMI). Fatigue was measured with the “Subjective Fatigue” subscale of the Checklist Individual Strength (CIS) (score range 8-56 points, scores of ≥ 35 represent severe fatigue16).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
The clinical burden of GOA | 27
2
Joint involvementTo identify the localization of symptomatic OA in eight joint areas (i.e. feet (including ankles), knees, hips, lumbar spine, neck, shoulders, elbows and hands (including wrists)) the following question was assessed in the baseline questionnaire: “In which of these joints do you experience symptoms (pain/stiffness) for more than half of the time?” The locations of symptoms were identified by each patient on a paper manikin, which permitted the identification of symptom locations on either side of the body17. In addition, objective signs of OA and its localization were registered by the first author by screening each patient’s medical file.
Health related quality of lifeHealth related quality of life was measured with the Short Form 36 Health Survey (SF-36), a widely used generic questionnaire that comprises eight areas of health status: physical functioning, physical role limitations, bodily pain, general health, vitality, social functioning, emotional role limitations and mental health18. Additionally, the SF-36 comprises two summary scores: the Physical Component Summary (PCS) and the Mental Component Summary (MCS) score. We used SF-36 scores of the Dutch general population to standardize the scores of the patients in the current study in order to apply the norm based scoring whereby we adjusted for age19,20. All scores were standardized to a mean (SD) of 50 (10). Lower scores represent worse health status.
Activity limitations measured with the HAQ-DIParticipants completed the Dutch consensus HAQ-DI21. The HAQ-DI measures difficulties with the performance of 20 daily activities retrospectively over the preceding week with four response categories: no difficulty (0), some difficulty (1), much difficulty (2) and unable to do (3). The activities are classified into eight categories with two or three activities each: dressing and grooming, arising, eating, walking, personal hygiene, reaching, gripping and usual activities (i.e. shopping, doing chores, getting in and out of a car)22. The highest scores of each category are summed and averaged resulting in a disability index ranging from 0 to 3, where scores of 0-1 are generally considered to represent mild to moderate disability, 1-2 moderate to severe disability and 2-3 severe to very severe disability22. We did not correct HAQ-DI scores for using assistive devices.
Activity limitations and participation restrictions measured with the patient specific complaints questionnaire (PSK)The PSK was administered by an occupational therapist with the aim to elicit activity limitations and participation restrictions that are specific and relevant to the individual patient23. Patients were asked to identify the three most important activities, currently

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
28 | Chapter 2
difficult to perform because of their GOA. No list of activities was used to allow patients freedom in their responses. In addition, patients rated the severity of each activity on a 10 cm visual analogue scale (VAS) (0 = no difficulty, 10 = impossible)23. Patient specific approaches to measure functional limitations have been shown to be reliable, valid and responsive in patients with several musculoskeletal conditions23,24. These activity limitations were then linked to the Activities and Participation component of the International Classification of Functioning, Disability and Health (ICF)25. This component describes a person’s functional status whereby Activities refer to the execution of specific tasks and Participation refer to the involvement in life situations. The ICF categories of the Activities and Participation component are designated by the letter d, followed by a numeric classification that indicates the chapter and specific category within the ICF classification. In the current study, each activity limitation was systematically linked to the most precise ICF category (3rd or 4th level) independently by three assessors (SK, DK, JG) using established linking rules26. In case of disagreement, agreement was established through a consensus meeting. When a patient reported different activity limitations or participation restrictions within the same PSK item, different ICF categories were identified. This process resulted in a list of ICF codes on different levels of the ICF within the area of Activities and Participation.
Statistical analysisDescriptive statistics were used to describe the main characteristics of the study population and to explore comparability between the participants and eligible patients. Mean (SD) SF-36 subscale and component summary scores were calculated to identify the patient’s health status. The mean (SD) total HAQ-DI score as well as mean (SD) HAQ-DI scores of each HAQ-DI category were calculated to identify the patient’s functional status. Additionally, we assessed for each HAQ-DI category, the percentage of patients that reported to have either no/some difficulty (score 0 or 1) or much difficulty (score 2 or 3) with performing everyday activities. The most commonly reported activity limitations and participation restrictions by patients with GOA were identified by analysing the frequencies of the assigned ICF categories from the PSK. All statistical analyses were performed using STATA 10.1.
Results
Patient characteristicsIn total, 236 patients were eligible to participate in the study of whom 158 (67%) agreed to. Main reasons for patients not to participate were having a preference for the multidisciplinary group-based treatment (n = 46; 59%) or lacking confidence towards the telephone-based treatment (n = 24; 31%). No differences were found between the group of eligible patients and the participants with regard to age, whereas there were relatively less women in the

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
The clinical burden of GOA | 29
2
group of eligible patients (72% vs. 85%, p = 0.01). Of the 158 participants, 11 were lost before the first measurement (i.e. provided no data), meaning that 147 patients were included in the analysis of the current study. Characteristics of the study population are summarized in Table 1.
Table 1. Socio demographic and disease related characteristics of 147 individuals with GOAa
Patient characteristicsFemale 125 (85)Age, years; mean ± SD 60 ± 8Body Mass Index, kg/m2; mean ± SD 28.1 ± 4.7Education > 12 years 43 (29)Marital status, married 113 (77)Work status, currently employed 55 (37)Duration of complaints ≥ 5 years 110 (75)Localization of symptoms:
Upper extremities (neck, shoulder, elbow, hand) 138 (94)Lower extremities (lumbar spine, hip, knee, foot) 145 (99)Combination of upper and lower extremities 136 (93)
Activity limitations, HAQ-DI (0-3); mean (SD) 1.27 (0.50)Severe fatigued, CIS score ≥ 35 83 (56)
a Values are the numbers (percentage) unless indicated otherwiseAbbreviations: SD = Standard Deviation; HAQ-DI = Health Assessment Questionnaire Disability Index; CIS = Checklist Individual Strength
Joint involvementThe median number of self-reported joint areas with symptomatic OA was 5 (interquartile range 4-6) and the median number of joint areas with objective signs of OA was 2 (interquartile range 2-3). The majority of patients (n = 136; 93%) had symptomatic OA in both the upper half (neck, shoulder, elbow, hand) and lower half (lumbar spine, hip, knee, foot) of the body. The prevalence of self-reported and objective signs of OA for each joint area is depicted in Figure 1. The predominant joints with symptomatic OA were the hands (n = 125; 85%) and knees (n = 121; 82%), whereas symptoms in the elbow joints were the least often reported (n = 41; 28%). The predominant joints with objective signs of OA were also the hands (n = 114; 78%) and knees (n = 78; 53%) as recorded in the patient’s medical files, whereas objective OA signs in the elbows were the least often recorded (n = 3; 2%). We found the combination of hand and knee OA to be most common, both self-reported (n = 106; 72%) as well as recorded in the medical files (n = 58; 39%).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
30 | Chapter 2
0102030405060708090100
Figure 1. Percentages of symptomatic and objective signs of OA for each joint area. The green bars represent the percentage of self-reported symptomatic OA, the blue bars represent the percentage of objective OA signs as recorded in the patient’s medical files and the red bars represent the percentage of both self-reported symptoms and objective signs of OA
Health related quality of lifeMean scores for the PCS, MCS and subscales of the SF-36 are presented in Figure 2. Mean (SD) PCS and MCS scores were 37.4 (6.9) and 47.8 (10.5), respectively. Mean (SD) scores were worst for the subscales physical function, physical role limitations, bodily pain and vitality, i.e. 37.4 (7.7), 39.0 (8.3), 40.0 (6.6) and 40.3 (5.5), respectively. Highest scores were obtained for the subscales mental health and emotional role limitations i.e. 47.7 (8.6) and 45.4 (12.0).
Activity limitations measured with the HAQ-DIThe mean (SD) total HAQ-DI score for the total study population was 1.27 (0.50), indicating moderate to severe activity limitations22. One hundred-eleven patients (76%) obtained a HAQ-DI score ≥ 1. The analysis of the HAQ-DI categories revealed that patients in the current study reported the greatest amount of difficulty with performing activities in the categories usual activities (i.e. shopping, doing chores, get in and out of a car) and reaching (i.e. bending down to pick up clothing from the floor, reach and get down a 5 pound object from above your head). Mean HAQ-DI scores for these categories were 1.61 and 1.58 respectively (Figure 3). More than half of the patients reported to have “much difficulty” with performing these activities. Patients reported the least amount of difficulty with performing activities in the category dressing and grooming (dress yourself, shampoo your hair) as this category obtained the lowest mean (SD) HAQ-DI score i.e. 0.86 (0.66). Thirteen percent of the patients reported to have “much difficulty” with performing these activities.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
The clinical burden of GOA | 31
2
0102030405060708090
100N
orm
bas
ed sc
orin
g
Figure 2. SF-36 physical and mental component summary and subscale scores of 147 patients with generalized osteoarthritis. The bars show the mean scores and standard deviations
87.1
75.5
61.9
68.0
54.4
49.0
70.8
44.9
12.9
24.5
38.1
32.0
45.6
51.0
29.3
55.1
0% 20% 40% 60% 80% 100%
Dressing and grooming
Arising
Eating
Walking
Hygiene
Reaching
Gripping
Usual activities
No/some difficulty Much difficulty/unable to do
1.61
1.03
1.58
1.50
1.21
1.20
1.17
0.86
Mean HAQ-DI score
Figure 3. Mean HAQ-DI scores for each HAQ-DI category and the percentage of patients that reported to have either no/some difficulty or at least much difficulty with performing everyday activities represented for each category

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
32 | Chapter 2
Activity limitations measured with the PSKThe total number of self-perceived activity limitations and participation restrictions obtained with the PSK was 440 (one patient mentioned only two limitations). These were linked to 463 ICF codes within the area of Activities and Participation of the ICF (d-codes), comprising 30 unique ICF categories. Of these 463 codes, 316 (68%) pertained to the chapter mobility (d4), 85 (18%) to domestic life (d6), 27 (6%) to community, social and civic life (d9) and 19 (4%) to self-care (d5). The remaining codes pertained to the chapters major life areas (d8), learning and applying knowledge (d1) and general tasks and demands (d2). Patients reported a broad spectrum of activity limitations and participation restrictions. The ten most frequently reported GOA-related activity problems and participation restrictions with corresponding ICF codes and mean (SD) severity scores are presented in hierarchical order in Table 2. Activities concerning mobility (d4) and domestic life (d6) were most frequently mentioned as being important activity limitations by patients with GOA; walking (d450) was most commonly reported. The category moving around (d455) can be further specified to the 4th level of the ICF as all activities in this category concerned climbing stairs (d4551). The severity of the activity limitations and participation restrictions were all above 6.0 with the highest score of 7.3 (on a 10 points scale) for caring for household objects (d650).
Table 2. Ten most frequently reported activity limitations and participation restrictions with corresponding ICF codes and severity scores in 147 patients with GOA.
ICF code Activity Number of patients (%) Mean (SD) severityd450 Walking 72 (16) 6.7 (2.1)d415 Maintaining a body position 59 (13) 6.4 (2.4)d410 Changing basic body position 52 (11) 7.1 (1.8)d640 Doing housework 45 (10) 6.9 (1.7)d455 Moving around 35 (8) 6.5 (2.0)d430 Lifting and carrying objects 31 (7) 6.1 (2.0)d440 Fine hand use 28 (6) 6.5 (2.0)d650 Caring for household objects 27 (6) 7.3 (1.7)d920 Recreation and leisure 26 (6) 6.1 (2.2)d475 Driving 20 (4) 6.2 (2.9)
Abbreviations: SD = Standard Deviation

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
The clinical burden of GOA | 33
2
Discussion
This is the first study that comprehensively describes the health status of patients clinically diagnosed with GOA. The results show that GOA has a broad impact on the physical component of health. Furthermore, the majority of our patients were moderate to severely impaired in performing daily activities. Patients reported a broad spectrum of important activity limitations and participation restrictions; activities concerning mobility and domestic life were considered as most important activity limitations, especially walking. In addition, more than half of the patients reported having “much difficulty” with activities such as shopping or doing chores and activities concerning reaching. These results offer starting points for clinicians and researchers to improve treatment programs for patients with GOA tailored to their needs and problems.
The present study showed that patients with GOA experience a markedly reduced quality of life, reflecting a high clinical burden. In particular, the physical component of health was affected. The observed level of physical health in the present study is comparable to that of patients with chronic, inflammatory arthritis such as rheumatoid arthritis (RA)27,28. Mental health was less affected compared to physical health in our study sample. One previous study assessed the PCS and MCS scores in a relatively small number of patients with GOA (n = 30)14, showing comparable scores as obtained in the current study. Our results indicate that effective interventions for GOA should be developed focussing on improving the physical component of health.
Patients in this study were moderately to severely impaired in performing daily activities as reflected by a mean HAQ-DI score of 1.27. This score is considerably higher than the average HAQ-DI score of 0.50 observed in Dutch patients with symptomatic OA at multiple joint sites participating in the Genetics, Arthrosis and Progression (GARP) study29. In another study among Dutch patients with OA (localization not specified) visiting an outpatient rheumatology department, a mean HAQ-DI score of 1.00 was reported30. Considering the abovementioned, it seems that the functional status of patients with GOA is more affected compared to other Dutch OA populations. Comparisons are however hampered by the fact that the patients in the current study were a selected group of patients with functional disability who were referred to multidisciplinary treatment. However, since our study population represents patients seeking help, this is probably the most interesting group for clinicians.
Understanding the nature of GOA related activity limitations and participation restrictions might be important to develop treatment targets tailored to the patients’ needs and problems. The results of the PSK showed that our patients reported a broad spectrum of activity limitations and participation restrictions. Activities involving the lower extremities were considered to be the most important activity limitations, especially walking. This finding cannot be explained by a predominance of lower limb OA by our patients, but might be

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
34 | Chapter 2
due to a high impact of mobility limitations on a patient’s well-being. Moreover, self-care limitations were rarely reported as being important activity limitations. This is in contrast with the ICF core sets for OA in which self-care activities are assumed to be key issues for patients with OA31. Dressing is even one out of three ICF categories of the brief core set for OA representing activities that minimally should be addressed when measuring disability in clinical studies31,32. Only one of these three activities was identified as an important activity limitation in our study. This discrepancy might be due to that we restricted patients to identify only three activity limitations. Nonetheless, our results point to the need of developing effective interventions to improve mobility, especially walking.
This study has some potential limitations that should be addressed. In this study we used a pragmatic definition of GOA in the absence of a widely accepted and validated definition. In the literature, the threshold number of affected joints as well as the localization of involved joints have been described differently5. Besides, previous GOA definitions mainly rely on radiographic findings independent of clinical symptoms, whereas symptoms are likely to be more important in functional outcomes33. We are one of the first that defined GOA from a clinical rather than a radiographic perspective. Second, due to pragmatic reasons we were not able to systematically obtain radiographs of all joint areas of each participant. Since we recorded objective signs of OA on the basis of information available in the patient’s medical file, it is conceivable that there is an underestimation of the number of joint areas with objective OA in our study population. Another limitation is that we did not assess co-morbidities in this study population. The presence of co-morbidities might have influenced the reported functional limitations and quality of life.
In conclusion, we generated empirical data showing a high clinical burden in terms of HRQoL and activity limitations in patients clinically diagnosed with GOA. This study contributes to the understanding of the deprived health status of individuals with GOA which is warranted considering the high prevalence of GOA and the lack of research on GOA. The results point to the need of developing effective interventions for patients with GOA to improve the physical component of health and to improve mobility, especially walking. Moreover, the broad spectrum of activity limitations underlines that treatment should be individualised according to the problems of the individual patient.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
The clinical burden of GOA | 35
2
References
1. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet 2011; 377: 2115-26
2. Petersson IF, Jacobsson LT. Osteoarthritis of the peripheral joints. Best.Pract.Res.Clin.Rheumatol. 2002; 16: 741-60
3. Bierma-Zeinstra SM, Verhagen AP. Osteoarthritis subpopulations and implications for clinical trial design. Arthritis Res.Ther. 2011; 13: 213
4. Felson DT. Identifying different osteoarthritis phenotypes through epidemiology. Osteoarthritis.Cartilage. 2010; 18: 601-4
5. Nelson AE, Smith MW, Golightly YM, Jordan JM. “Generalized osteoarthritis”: A systematic review. Semin.Arthritis Rheum. 2014; 43: 713-20
6. KELLGREN JH, MOORE R. Generalized osteoarthritis and Heberden’s nodes. Br.Med.J. 1952; 1: 181-7
7. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011; 78: 275-8
8. Gunther KP, Sturmer T, Sauerland S, Zeissig I, Sun Y, Kessler S et al. Prevalence of generalised osteoarthritis in patients with advanced hip and knee osteoarthritis: the Ulm Osteoarthritis Study. Ann.Rheum.Dis. 1998; 57: 717-23
9. Min JL, Meulenbelt I, Riyazi N, Kloppenburg M, Houwing-Duistermaat JJ, Seymour AB et al. Association of the Frizzled-related protein gene with symptomatic osteoarthritis at multiple sites. Arthritis Rheum. 2005; 52: 1077-80
10. Hoogeboom TJ, den Broeder AA, Swierstra BA, de Bie RA, van den Ende CH. Joint-pain comorbidity, health status, and medication use in hip and knee osteoarthritis: a cross-sectional study. Arthritis Care Res.(Hoboken.) 2012; 64: 54-8
11. Hoogeboom TJ, den Broeder AA, de Bie RA, van den Ende CH. Longitudinal impact of joint pain comorbidity on quality of life and activity levels in knee osteoarthritis: data from the Osteoarthritis Initiative. Rheumatology.(Oxford) 2013; 52: 543-6
12. Perruccio AV, Power JD, Evans HM, Mahomed SR, Gandhi R, Mahomed NN et al. Multiple joint involvement in total knee replacement for osteoarthritis: Effects on patient-reported outcomes. Arthritis Care Res.(Hoboken.) 2012; 64: 838-46
13. Suri P, Morgenroth DC, Kwoh CK, Bean JF, Kalichman L, Hunter DJ. Low back pain and other musculoskeletal pain comorbidities in individuals with symptomatic osteoarthritis of the knee: data from the osteoarthritis initiative. Arthritis Care Res.(Hoboken.) 2010; 62: 1715-23
14. Moe RH, Grotle M, Kjeken I, Hagen KB, Kvien TK, Uhlig T. Disease impact of hand OA compared with hip, knee and generalized disease in specialist rheumatology health care. Rheumatology.(Oxford) 2013; 52: 189-96
15. Hoogeboom TJ, Stukstette MJ, de Bie RA, Cornelissen J, den Broeder AA, van den Ende CH. Non-pharmacological care for patients with generalized osteoarthritis: design of a randomized clinical trial. BMC.Musculoskelet.Disord. 2010; 11: 142
16. Vercoulen JH, Swanink CM, Fennis JF, Galama JM, van der Meer JW, Bleijenberg G. Dimensional assessment of chronic fatigue syndrome. J.Psychosom.Res. 1994; 38: 383-92
17. van den Hoven LH, Gorter KJ, Picavet HS. Measuring musculoskeletal pain by questionnaires: the manikin versus written questions. Eur.J.Pain 2010; 14: 335-8
18. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med.Care 1992; 30: 473-83
19. Aaronson NK, Muller M, Cohen PD, Essink-Bot ML, Fekkes M, Sanderman R et al. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J.Clin.Epidemiol. 1998; 51: 1055-68
20. Ware JE, Jr., Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. Med.Care 1995; 33: AS264-AS279

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
36 | Chapter 2
21. Boers M, Jacobs JW, Vliet Vlieland TP, van Riel PL. Consensus Dutch health assessment questionnaire. Ann.Rheum.Dis. 2007; 66: 132-3
22. Bruce B, Fries JF. The Stanford Health Assessment Questionnaire: dimensions and practical applications. Health Qual.Life Outcomes. 2003; 1: 20
23. Beurskens AJ, de Vet HC, Koke AJ, Lindeman E, van der Heijden GJ, Regtop W et al. A patient-specific approach for measuring functional status in low back pain. J.Manipulative Physiol Ther. 1999; 22: 144-8
24. Rosengren J, Brodin N. Validity and reliability of the Swedish version of the Patient Specific Functional Scale in patients treated surgically for carpometacarpal joint osteoarthritis. J.Hand Ther. 2012; 26: 53-60
25. International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization. 2001
26. Cieza A, Brockow T, Ewert T, Amman E, Kollerits B, Chatterji S et al. Linking health-status measurements to the international classification of functioning, disability and health. J.Rehabil.Med. 2002; 34: 205-10
27. Rupp I, Boshuizen HC, Roorda LD, Dinant HJ, Jacobi CE, van den Bos G. Course of patient-reported health outcomes in rheumatoid arthritis: comparison of longitudinal and cross-sectional approaches. J.Rheumatol. 2006; 33: 228-33
28. Wolfe F, Michaud K, Li T, Katz RS. EQ-5D and SF-36 quality of life measures in systemic
lupus erythematosus: comparisons with rheumatoid arthritis, noninflammatory rheumatic disorders, and fibromyalgia. J.Rheumatol. 2010; 37: 296-304
29. Bijsterbosch J, Scharloo M, Visser AW, Watt I, Meulenbelt I, Huizinga TW et al. Illness perceptions in patients with osteoarthritis: change over time and association with disability. Arthritis Rheum. 2009; 61: 1054-61
30. van Groen MM, ten Klooster PM, Taal E, van de Laar MA, Glas CA. Application of the health assessment questionnaire disability index to various rheumatic diseases. Qual.Life Res. 2010; 19: 1255-63
31. Dreinhofer K, Stucki G, Ewert T, Huber E, Ebenbichler G, Gutenbrunner C et al. ICF Core Sets for osteoarthritis. J.Rehabil.Med. 2004; 75-80
32. Oberhauser C, Escorpizo R, Boonen A, Stucki G, Cieza A. Statistical validation of the brief International Classification of Functioning, Disability and Health Core Set for osteoarthritis based on a large international sample of patients with osteoarthritis. Arthritis Care Res.(Hoboken.) 2013; 65: 177-86
33. Nelson AE, Elstad E, DeVellis RF, Schwartz TA, Golightly YM, Renner JB et al. Composite measures of multi-joint symptoms, but not of radiographic osteoarthritis, are associated with functional outcomes: the Johnston County Osteoarthritis Project. Disabil.Rehabil. 2014; 36: 300-6

CHAPTER 3
Randomized trial of the effectiveness of a non-
pharmacological multidisciplinary face-to-face treatment
program on daily function compared to a telephone-
based treatment program in patients with generalized
osteoarthritis
Nienke Cuperus, Thomas J. Hoogeboom, Clarinda C. Kersten, Alfons A. den Broeder, Thea P.M. Vliet Vlieland, Cornelia H.M. van den Ende
Published in: Osteoarthritis & Cartilage. 2015 [Epub ahead of print]

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
38 | Chapter 3
Abstract
ObjectiveTo compare the effectiveness of a non-pharmacological multidisciplinary face-to-face self-management treatment program with a telephone-based program on daily function in patients with generalized osteoarthritis (GOA).
MethodsA pragmatic single-blind randomized clinical superiority trial involving 147 patients clinically diagnosed with GOA, randomly allocated to either a six week non-pharmacological multidisciplinary face-to-face treatment program comprising seven group sessions or a six week telephone-based treatment program comprising two group sessions combined with four telephone contacts. Both programs aimed to improve daily function and to enhance self-management to control the disease. The programs critically differed in mode of delivery and intensity. Daily function (primary outcome) and secondary outcomes were assessed at baseline, 6, 26 and 52 weeks. Data were analyzed using linear or logistic multilevel regression models corrected for baseline, sex and group-wise treatment.
ResultsNo differences in effectiveness between both treatment programs were observed on the primary outcome (group difference (95% CI): -0.03 (-0.14, 0.07)) or on secondary outcome measures, except for a larger improvement in pain in the face-to-face treatment group (group difference (95% CI): 1.61 (0.01, 3.21)). Within groups, significant improvements were observed on several domains, especially in the face-to-face group. However, these benefits are relatively small and unlikely to be of clinical importance.
ConclusionsWe found no differences in treatment effect between patients with GOA who followed a non-pharmacological multidisciplinary face-to-face self-management program and those who received a telephone-based program. Besides, our findings demonstrated limited benefits of a self-management program for individuals with GOA.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 39
3
Introduction
Osteoarthritis (OA) can affect multiple joints, but is most common in the hand, spine and the weight-bearing joints i.e. the hip and knee1,2. In recent years, clinically relevant OA subpopulations or so called phenotypes have been classified whereby different joint groups are generally seen as distinct phenotypes1,3,4. A commonly used and widely accepted phenotype is generalized osteoarthritis (GOA)3,4, describing a subset of patients with clinically polyarticular OA5. To date, a wide variety of GOA definitions have been described in the literature, however no agreed and validated definition is available so far5. Most definitions of GOA include at least 3 joints or joint groups, but there is little agreement on the necessity or appropriateness of including a specific joint or combination of joints. It has been suggested that individuals with GOA might represent a relatively large subgroup of patients with OA. In knee OA, approximately 50% of patients can be classified as GOA6-8.
Several international guidelines for the management of OA are available emphasizing the effectiveness of non-pharmacological, non-surgical interventions, such as education, self-management, weight reduction and exercise therapy9-14. However, these guidelines all focus on single joint involvement (i.e. hand, hip or knee), without considering the involvement of multiple joints. Recently, the Osteoarthritis Research Society International (OARSI) was the first to publish recommendations for the non-surgical management of OA for several subpopulations, including multiple joint OA (i.e. OA in other joints in addition to the knee)12. However, due to the limited research on the management of multiple joint OA, the authors only considered balneotherapy (defined as the use of baths containing thermal mineral waters) appropriate for patients with multiple joint OA, whereas no other recommendations could be formulated. Yet, it is likely that recommendations for hip and knee OA also apply for individuals with GOA.
Considering the substantial group of patients with GOA, the lack of knowledge on the non-pharmacological management of GOA and the high physical and psychological burden associated with GOA7,8,13,15,16, the development and evaluation of a treatment program for patients with GOA is warranted. Therefore, our research group systematically developed a non-pharmacological, multidisciplinary face-to-face treatment program for individuals with GOA based on recommendations for the management of hip and knee OA14 and tailored to the needs of patients with GOA17. Treatment components of the program included education, self-management and exercises. Besides, a less intensive telephone-based treatment program was developed since increasing evidence shows telephone-based interventions to be cost-efficient18 and to improve symptoms and promote lifestyle changes19,20. The aim of the current study was to compare the effectiveness of both treatment programs on daily function during the first year after treatment. We hypothesized the face-to-face treatment program to be superior in effect on daily function, since this program is more extensive and more strictly supervised.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
40 | Chapter 3
Methods
Study Design This study was a pragmatic parallel group, single-blind randomized clinical superiority trial comparing the effectiveness of a six week non-pharmacological multidisciplinary supervised face-to-face treatment program with a six week telephone-based treatment program on daily function in patients with GOA. The effectiveness over one year was examined. Details of the trial development and design have been published previously17. The protocol adhered to the CONSORT guidelines for non-pharmacological interventions21. The study was performed at the outpatient rheumatology departments of the Sint Maartenskliniek Nijmegen and Woerden, the Netherlands from January 2010 to April 2014 and was approved by the local ethics committee (CMO region Arnhem, Nijmegen) and registered in the Dutch Trial Register (trial number NTR2137). All participants signed informed consent prior to the baseline data collection.
Setting and participantsDuring an outpatient visit, patients clinically diagnosed with GOA and referred by their rheumatologist for treatment were invited for a screening visit to consider eligibility for the trial. Patients were included when: (1) having at least two objective signs indicating OA in ≥ 2 joint areas on the basis of the patient’s medical record (objective signs included: malalignment, crepitation, limited range of motion, palpable osteophytes or nodules or radiographic signs including the presence of joint space narrowing and/or osteophytes); (2) having complaints in ≥ 3 out of 8 joint areas (i.e. feet, knees, hips, lumbar spine, neck, shoulders, elbows and hands); (3) being limited in the performance of daily activities (Health Assessment Questionnaire Disability Index (HAQ-DI) score ≥ 0.5); and (4) motivated to alter their lifestyle and willing to participate in a group (assessed by a standardized set of questions). Excluded were patients who were: (1) diagnosed with another rheumatic disease; (2) awaiting surgery; (3) already participated unsuccessfully in a self-management program; (4) having psychosocial problems interfering with the scope of the treatment; (5) incapable of coming to the hospital; or (6) unable to write and or understand the Dutch language.
InterventionsThe overall goals of both treatment programs were to improve daily function and to enhance self-management skills to control the disease. The face-to-face treatment program was provided by a multidisciplinary team comprising a physical therapist, occupational therapist, specialized rheumatology nurse and dietician. The telephone-based treatment was provided by a specialized rheumatology nurse and physical therapist. The most critical differences between both treatments were the mode of care delivery, the number of involved healthcare

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 41
3
providers, the number of group sessions and the number of sessions including an exercise program. For an overview of the content of both programs see Appendix 1. The healthcare providers were trained in techniques of motivational interviewing22 and were specialized in treating patients with musculoskeletal disorders and teaching self-management principles. To standardize both programs, slide presentations for all sessions and manuals for healthcare providers and patients were used. Protocol adherence of healthcare providers was maintained by meetings during the trial.
Face-to-face treatment groupThe multidisciplinary face-to-face program comprised six therapeutic group sessions (6-8 patients and 2-4 hours) and a group evaluation delivered during six weeks, supervised by a physical therapist. In the first session information about the program was given, expectations were discussed and patients filled in activity and diet diaries. Information about OA, pain management and medication was also provided in this session. Additionally, patients participated in a general exercise program to improve the quality of movement and posture (i.e. walking, sitting) and to implement exercises in the home situation. This exercise program was continued in session two (standing, kneeling, lifting) and three (stair climbing, lying). Information on physical activity and activity pacing was given in session two and information on food consumption was given in sessions three and four. Furthermore, in session three patients were asked to set personal goals regarding pain management, physical activity and activity pacing which were closely monitored and discussed in the next three sessions. Besides, patients participated in a specific exercise program based on the principles of graded activity and tailored to the patient’s health problems in sessions four, five and six. Acceptance as a strategy to cope with the disease was discussed in session five. To introduce patients with other strategies to manage their symptoms, introduction lessons of tai chi, brisk walking and hydrotherapy were given. The program was evaluated in the final session and future personal goals were formulated.
Telephone-based treatment groupPatients allocated to the telephone-based treatment attended two face-to-face group sessions (6-8 patients) with a duration of 2-2.5 hours and were further monitored by four individual telephone contacts (15-30 minutes per contact) with a specialized rheumatology nurse. In the first group session, patients were educated about the program, OA, pain management, medication, physical activity, activity pacing, food consumption and acceptance of the disease. Besides, patients completed activity and diet diaries. During the individual telephone contacts, patients set personal goals regarding pain management, physical activity and activity pacing which were closely monitored and discussed. The second group session included an exercise program tailored to the patient’s health problems to improve the quality

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
42 | Chapter 3
of movement and posture and to implement the exercises in the home situation. Besides, patient’s personal goals were discussed. The treatment program was evaluated during the final telephone contact.
Randomization and blindingPatients were allocated to the treatment groups (allocation ratio 1:1) by an independent person using a computer generated randomization sequence table consisting of randomly varied block sizes (2 to 6). Assignments were communicated by e-mail to the outpatient clinics and patients were informed by mail. This study has a partly blinded design as due to the nature of the interventions neither patients nor healthcare providers could be blinded for allocation. The assessor (NC) was blinded for randomization and allocation and the statistical analyses were performed blindly. Participants were instructed not to disclose details about their group allocation with the assessor. The allocation of healthcare providers was done on basis of availability.
Measurements and outcomesPrimary and secondary outcome measures were collected prior to the start of the treatment (i.e. baseline), after finishing the treatment (i.e. 6 weeks) and 26 and 52 weeks after starting the treatment. Demographic data were collected at baseline.
Primary outcome measureThe primary outcome measure was daily function measured with the Dutch consensus HAQ-DI23. The HAQ-DI examines difficulties with the performance of 20 daily activities (classified into 8 categories) scored from 0 (without any difficulty) to 3 (unable to do). The highest scores of each category are summed and averaged resulting in a disability index ranging from 0 (no disability) to 3 (very severe disability).
Secondary outcome measuresHealth related quality of life (HRQoL) was measured with the Short Form 36 Health Survey (SF-36), comprising eight areas of health status and a physical (PCS) and mental component summary score (MCS)24. Pain was assessed using the SF-36 bodily pain subscale. Fatigue was measured with the eight-itemed “Subjective Fatigue” subscale of the Checklist Individual Strength (CIS)25. The patient specific complaints questionnaire (PSK) was administered to elicit patient specific and relevant activity limitations26. Patients identified the three most important GOA-related functional limitations and scored the severity on a 0-10 scale, with higher total scores indicating more severe limitations. Self-efficacy was assessed with the General Self-Efficacy Scale (GSES)27 and illness cognitions were measured using the subscales acceptance and helplessness of the Illness Cognitions Questionnaire (ICQ)28. Pain-related fear for moving

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 43
3
was measured with the Tampa scale for kinesiophobia (TSK) with total scores ranging from 17-68 (higher scores indicating more fear)29. Physical activity levels were measured with the Short Questionnaire to Assess Health enhancing physical activity (SQUASH) and presented as the number of patients meeting the Dutch recommendation for physical activity (moderate physical activity for >30 minutes for 5 days/week)30. Moreover, patients rated their health status on a visual analogue scale (EQ VAS) ranging from 0 (worst imaginable health status) to 100 (best imaginable health status). After finishing the treatment, change in daily function was rated on a 7-point Likert transition question ranging from completely recovered to vastly worsened. Costs were also assessed, but these results are presented elsewhere.
Study endpointsThe primary endpoint was the difference in mean HAQ-DI score between both treatment groups i.e. the average score obtained from the 6, 26 and 52 week time points (long-term effect). The six week time point of the HAQ-DI provided a secondary endpoint. Other secondary endpoints were the between group differences of the secondary outcome measures and the within group differences of all outcome measures. Furthermore, as there is no validated outcome measure to asses the health status of patients with GOA, we evaluated both programs with a responder analysis using a set of self-constructed responder criteria17 adapted from the OMERACT-OARSI knee and hip responder criteria31. Patients were classified as responder if ≥ 3 of the following 6 areas improved by ≥ 20% (average from the 6, 26 and 52 week time points): physical function (PSK), pain (SF-36), fatigue (CIS), physical activity (SQUASH), acceptance (ICQ) and patient global assessment (PGA) (EQ VAS).
Statistical analysisWe estimated that a sample size of 170 patients was needed to provide a power of 80% to show superiority of the face-to-face treatment by at least 0.26 points on the HAQ-DI32, assuming a standard deviation (SD) of 0.66, a significance level of 0.05 and a 15% drop-out rate17.
Data were analysed using Stata/IC 13.1. Missing data were estimated using multiple imputation by changed equation in order to preserve power and reduce bias33,34. A total of 20 imputed data sets were predicted based on all other observed variables. Primary analyses were done according to the intention-to-treat (ITT) principle35. Secondary analysis included per-protocol analysis excluding major protocol violations (i.e. patients who either discontinued treatment, crossed over to the other group or missed >3 sessions). Descriptive statistics were used to describe the characteristics of the study population and to explore baseline comparability. Data were analysed with a multilevel mixed linear regression model with the mean scores obtained from the 6, 26 and 52 week time points as dependent variable and treatment group, sex and baseline value as covariates. In order to account for the group-

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
44 | Chapter 3
wise treatment, group was included as random effect. Scores obtained immediately after treatment were also evaluated using the same multilevel mixed linear regression model. Within group changes were evaluated by analysing the mean changes scores from baseline with associated 95% confidence intervals (CI). The number of responders were analysed similar to the continuous outcomes using multilevel mixed logistic regression and were presented as odds ratios. No statistical adjustment was made for multiple testing.
Results
Participant’s flow diagram is presented in Figure 1. A total of 236 (70%) patients were considered eligible for the trial of whom 158 (67%) were enrolled. Main reasons not to participate were having a preference for the face-to-face treatment (n = 46; 59%) or lacking confidence towards the telephone-based treatment (n = 24; 31%). Due to time constraints, we needed to stop the inclusion after 158 patients out of the targeted 170 patients were enrolled. No differences were found between the eligible patients who did not participate and the study population with regard to age, whereas there were relatively less women in the group of eligible patients (72% vs. 85%, p = 0.01). The majority of participants (n = 116; 73%) were included in the Maartenskliniek Nijmegen. Eighty-one participants were allocated to the face-to-face treatment and 77 to the telephone-based treatment. Six patients from the face-to-face group and five from the telephone group were lost before the baseline measurement meaning that data from 147 participants were available for the ITT analysis. These drop-outs can be explained by the time between inclusion and start of the treatment (up to six weeks) due to the group-wise treatment. The percentage of missing data on the primary outcome was 0%, 7%, 12% and 14% at baseline, 6, 26 and 52 weeks, respectively.
Baseline characteristics of the study population are presented in Table 1. The majority was female, nearly 90% of patients reported symptoms in both the upper and lower extremities and the mean (SD) HAQ-DI score was 1.27 (0.50) for the face-to-face group and 1.26 (0.49) for the telephone-based treatment group. There were no relevant differences in baseline characteristics between groups. A total of 19 healthcare providers were involved.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 45
3
Excluded (n = 103) - Not meeting inclusion criteria (n = 79) - Randomization not possible (n = 8) - No complaints/no need for help (n = 14) - Other reasons (n = 2)
Invited to participate in trial (n = 236)
Assessed for eligibility (n = 339)
Randomization (n = 158)
Declined (n = 78) - Preference for face-to-face group (n = 46) - Lack of confidence telephone group (n = 24) - Other (n = 8)
Allocated to face-to-face treatment (n =81) Received treatment (n = 76)
- Lost to follow-up; no data available (n=1) Did not receive treatment (n = 5)
- Time constraints/too much effort (n = 4) - Referred back to rheumatologist (n = 1)
Allocated to telephone-based treatment (n = 77) Received treatment (n = 73)
- Lost to follow-up; no data available (n = 1) Did not receive treatment (n = 4)
- Time constraints/ too much effort (n = 2) - Comorbidity (n = 2)
6 week follow-up assessment (n = 70) Missing (n = 4) Lost to follow-up (n = 1)
- No benefit of participating (n = 1)
6 week follow-up assessment (n = 67) Lost to follow-up (n = 5)
- Too much effort (n = 3) - Diagnosed with RA (n = 1) - Illness partner (n = 1)
26 week follow-up (n = 68) Missing (n = 2) Lost to follow-up (n = 4)
- Comorbidity (n = 1) - Too much effort (n = 1) - Unknown (n = 2)
26 week follow-up (n = 64) Missing (n = 1) Lost to follow-up (n = 2)
- Too much effort (n = 1) - Unknown (n = 1)
52 week follow-up (n = 67) Missing (n = 3)
52 week follow-up (n = 61) Missing (n = 3) Lost to follow-up; comorbidity (n = 1)
Intention to treat analysis (n = 75) Excluded from analysis; no data available (n = 6)
Per-protocol analysis (n = 72)
Excluded from analysis (n = 9) - No data available (n = 6) - Protocol violation (n = 3) o Crossed over to telephone group (n = 2) o Discontinued treatment (n = 1)
Intention to treat analysis (n = 72) Excluded from analysis; no data available (n = 5)
Per-protocol analysis (n = 67)
Excluded from analysis (n = 10) - No data available (n = 5) - Protocol violation (n = 5) o Crossed over to face-to-face group (n = 2) o Missed > 3 sessions (n = 2) o Discontinued treatment (n = 1)
Figure1. Flow diagram

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
46 | Chapter 3
Table 1. Baseline characteristics of participants allocated to the face-to-face and telephone-based treatment group
Face-to-face treatment
(n = 75)
Telephone-based treatment
(n = 72)
Age, years; mean (SD) 61 (8) 59 (8)Female; n (%) 64 (85) 61 (85)Body Mass Index, kg/m2; mean (SD) 28 (5) 28 (5)Currently employed; n (%) 28 (37) 27 (38)Number of symptomatic joint areas; median (IQR) 5 (4-6) 5 (4-6)Localization of symptoms; n (%)
Upper extremities (shoulder, elbow, hand) 68 (91) 66 (92)Neck/lumbar spine 54 (72) 53 (74)Lower extremities (hip, knee, foot) 72 (96) 69 (96)Combination of upper and lower extremities 65 (87) 63 (88)
Daily function, HAQ-DI (0-3); mean (SD) 1.27 (0.50) 1.26 (0.49)
Abbreviations: SD = Standard deviation; IQR = interquartile range; HAQ-DI = Health Assessment Questionnaire Disability Index
Primary endpointPatients in the face-to-face treatment group showed a larger improvement in daily function over one year follow-up compared to the patients in the telephone-based treatment group, however this difference was not statistically significant (mean group difference HAQ-DI (95% CI): -0.03 (-0.14, 0.07)) (Table 2). The limits of the 95% CI do not reach the predefined relevant difference in treatment effect of 0.26 points.
Table 2. Baseline data, mean changes from baseline (95% CI) and mean differences (95% CI) in change scores between groups on the primary outcome measure1.
Face-to-face treatment
(n = 75)
Telephone-based treatment
(n = 72)
Δ 95% CI Δ 95% CIGroup difference2
(95%CI)Daily function (HAQ-DI)
Baseline; mean (SD) 1.27 (0.50) 1.26 (0.49)Δ 6 weeks -0.03 (-0.11, 0.05) -0.06 (-0.15, 0.03) 0.01 (-0.10, 0.13)Δ average 1 year -0.06 (-0.14, 0.02) -0.02 (-0.11, 0.06) -0.03 (-0.14, 0.07)
1Results are described as intention-to-treat2Multilevel mixed linear regression analyses corrected for baseline values, sex and group-wise treatment.Abbreviations: SD = standard deviation; CI = confidence interval

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 47
3
Secondary endpointsAt the six week time point of the HAQ-DI, a small, non-significant difference in effectiveness between groups was observed (mean group difference (95% CI): 0.01 (-0.10, 0.13)). The upper and lower confidence limits exclude a clinically important difference in treatment effect. A small significant difference between groups was observed for pain at the long term in favor of the face-to-face treatment program, indicating that this program was more effective in reducing pain than the telephone-based program (mean group difference (95% CI): 1.61 (0.01, 3.21)) (Table 3). Directly after treatment, significantly fewer patients in the face-to-face group met the self-reported Dutch recommendation for physical activity compared to the telephone group (odds ratio (95% CI): 0.32 (0.11, 0.97)). Within groups, no significant improvements were found on our primary outcome measure. On several secondary outcome measures significant, but relatively small improvements were observed at the short and long-term, especially in the face-to-face group. After one year, 17 (22%) participants in the face-to-face treatment group and 13 (18%) participants in the telephone-based group fulfilled the responder criteria (odds ratio (95% CI): 1.22 (0.50, 3.00)) (Table 4).
Per-protocol analysisPer-protocol analysis of the primary endpoint was performed excluding eight protocol violators i.e. three participants in the face-to-face group (crossed-over to the telephone-based treatment group n = 2, discontinued treatment n =1) and five participants in the telephone-based treatment group (crossed over to the face-to-face treatment group n = 2, missed > 3 sessions n = 2, discontinued treatment n = 1). The estimated between group difference of the primary endpoint did not change (mean group difference (95% CI): -0.04 (-0.14, 0.07)).
Treatment adherence and adverse effectsThe mean number of sessions participants attended was 6.6 (out of 7) in the face-to-face group and 5.5 (out of 6) in the telephone-based treatment group. We did not systematically assess adverse effects, though patients were encouraged to report adverse effects to the supervised healthcare professional. However, no adverse effects related to the treatment programs were reported.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
48 | Chapter 3
Table 3. Baseline data, mean changes from baseline (95% CI) and mean differences (95% CI) in change scores between groups on secondary outcome measures1.
Face-to-facetreatment
(n = 75)
Telephone-based treatment
(n = 72)
Δ 95% CI Δ 95% CIGroup difference2
(95% CI)Pain (SF-36)
Baseline; mean (SD) 39.60 (7.31) 40.45 (5.81)Δ 6 weeks 3.19 (1.53, 4.85) 0.96 (-0.76, 2.67) 1.82 (-0.15, 3.80)Δ average 1 year 2.83 (1.32, 4.33) 0.76 (-0.71, 2.23) 1.64 (0.06, 3.22)
Patient specific function (PSK)Baseline; mean (SD) 19.81 (5.51) 19.88 (4.17)Δ 6 weeks -1.16 (-2.44, 0.13) -1.53 (-2.78, -0.28) 0.19 (-1.45, 1.82)Δ average 1 year -1.87 (-2.93, -0.81) -1.43 (-2.56, -0.29) -0.49 (-1.87, 0.89)
Fatigue (CIS)Baseline; mean (SD) 36.12 (7.23) 36.13 (7.52)Δ 6 weeks -1.08 (-3.28, 1.11) -1.04 (-2.76, 0.69) -0.32 (-2.81, 2.17)Δ average 1 year -2.03 (-3.76, -0.29) -1.10 (-2.73, 0.52) -1.09 (-2.95, 0.78)
Physical function (PCS SF-36)Baseline; mean (SD) 37.65 (6.65) 37.17 (7.33)Δ 6 weeks 2.25 (0.64, 3.85) 1.58 (0.11, 3.04) 0.89 (-1.09, 2.86)Δ average 1 year 1.58 (-0.08, 2.81) 1.13 (-0.32, 2.58) 0.49 (-1.15, 2.12)
Mental function (MCS SF-36)Baseline; mean (SD) 47.59 (10.31) 47.96 (10.96)Δ 6 weeks 0.34 (-1.85, 2.52) 0.82 (-1.57, 3.21) -0.37 (-3.36, 2.63)Δ average 1 year 1.97 (0.12, 3.81) 0.21 (-1.87, 2.29) 1.74 (-0.42, 3.90)
Acceptance (ICQ)Baseline; mean (SD) 14.52 (3.82) 14.86 (4.21)Δ 6 weeks 0.93 (-0.01, 1.87) 1.17 (0.32, 2.02) -0.29 (-1.41, 0.84)Δ average 1 year 1.36 (0.61, 2.12) 0.93 (0.17, 1.70) 0.33 (-0.58, 1.24)
Helplessness (ICQ)Baseline; mean (SD) 12.65 (3.70) 12.87 (3.32)Δ 6 weeks -0.41 (-1.18, 0.35) -0.48 (-1.24, 0.28) -0.10 (-1.12, 0.91)Δ average 1 year -0.61 (-1.26, 0.05) -0.56 (-1.26, 0.13) -0.21 (-1.05, 0.63)
Self-efficacy (GSES)Baseline; mean (SD) 31.13 (4.48) 31.06 (4.43)Δ 6 weeks -0.21 (-1.46, 1.04) 0.03 (-1.24, 1.31) -0.11 (-1.79, 1.58)Δ average 1 year 0.28 (-0.65, 1.21) -0.44 (-1.51, 0.63) 0.84 (-0.44, 2.12)
Kinesiophobia (TSK)Baseline; mean (SD) 36.60 (7.65) 36.79 (7.05)Δ 6 weeks -1.34 (-3.27, 0.58) -1.91 (-3.89, 0.06) 0.49 (-2.24, 3.23)Δ average 1 year -1.41 (-2.95, 0.12) -1.05 (-2.70, 0.60) -0.48 (-2.52, 1.56)
PGA (EQ VAS)Baseline; mean (SD) 53.84 (17.59) 53.42 (14.70)Δ 6 weeks 8.43 (3.67, 13.20) 5.22 (0.83, 9.61) 3.26 (-1.14, 7.67)Δ average 1 year 6.59 (2.63, 10.55) 3.73 (-0.06, 7.51) 3.18 (-0.32, 6.68)
Physical activity (SQUASH)3
Baseline; n (%) 54 (72) 50 (70)6 weeks; n (%) 50 (67) 58 (80) 0.32 (0.11, 0.97)4
1 year; n (%) 56 (75) 48 (67) 1.55 (0.65, 3.74)1Results are described as intention-to-treat2Multilevel mixed linear regression analyses corrected for baseline values, sex and group-wise treatment.3Number of participants (%) meeting recommendation for physical activity 4Multilevel mixed logistic regression corrected for baseline values, sex and group-wise treatment, presented as odds ratios with associated confidence intervalAbbreviations: SD = standard deviation; CI = confidence interval; PGA = patient global assessment

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 49
3
Table 4. Patients classified as responder for both treatment groups including odds ratios (95% CI)1
Face-to-face treatment
(n = 75)
Telephone-based treatment
(n = 72)Odds ratio
(95% CI)
Physical function (PSK) 20 (27) 17 (23) 1.28 (0.51, 3.21)Pain (SF-36) 15 (20) 9 (12) 1.78 (0.69, 4.63)Fatigue (CIS) 17 (22) 10 (14) 1.73 (0.66, 4.55)Physical activity (SQUASH) 28 (37) 27 (38) 0.98 (0.45, 2.13)Acceptance (ICQ) 23 (31) 22 (30) 1.05 (0.50, 2.27)PGA (EQ VAS) 26 (34) 23 (32) 1.05 (0.47, 2.33)Responders2 17 (22) 13 (18) 1.22 (0.50, 3.00)
1Results are the numbers (percentage) unless indicated otherwise2Patients are considered responder if ≥ 3 of the areas presented in the table improved by ≥ 20%. Abbreviations: CI = confidence interval; PGA = patient global assessment
Discussion
This is the first study on the effectiveness of a self-management program for patients clinically diagnosed with GOA. We compared the effectiveness of two modes of therapy delivery i.e. face-to-face versus telephone. Based on the results, there is insufficient evidence of an important difference in effect on daily function between both groups. The results indicate absence of evidence because the limits of the 95% CI do not cover the predefined relevant change of 0.26 points36. Furthermore, we found no significant differences in effectiveness between both groups on the secondary outcomes, except for pain, the face-to-face program was more effective in reducing pain at the long-term. Within groups, significant improvements were observed on several domains, especially in the face-to-face treatment group, although these benefits are relatively small and unlikely to be of clinical importance.
The observed small within group changes indicate an insufficient content of our treatment programs to achieve important changes. Nevertheless, both programs comprised numerous treatment elements that should be included in self-management programs as recommended in international guidelines for the management of OA, like education, exercises and goal-setting10,37. Probably, our programs addressed too much treatment elements what might have hampered patients to pick up relevant information for themselves. In order to achieve important changes in daily function, it might be more beneficial to include fewer treatment elements. Increasing evidence supports the existence of only small effects of OA self-management programs as reported in systematic reviews38,39 and clinical guidelines10,37. Nevertheless, the importance of self-management is uniformly recognized in international clinical guidelines in order to manage the disease effectively10,11,13,37.It is therefore conceivable

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
50 | Chapter 3
that recommendations regarding self-management are based on clinical expertise and patient values rather than on research evidence.
The choice of our primary outcome measure could be argued. To date, there is a significant heterogeneity in outcome measures to evaluate OA self-management interventions and no validated outcome measure is available39. Usually, main outcome measures are pain and/or physical function39. However, self-management programs are often not intended to only reduce pain or improve physical function, but typically target on multiple domains of daily living. Since there are no validated outcome measures for clinical improvement in GOA, we chose the HAQ-DI as primary outcome measure in the current study. However, our interventions also targeted other dimensions relevant in GOA, such as pain, fatigue, physical activity and acceptance. We therefore evaluated our treatment programs with a responder criteria set adapted from the OMERACT-OARSI responder criteria31 including the areas our interventions aimed to address. Future research is needed to understand which outcomes are most relevant to assess the effectiveness of self-management programs in GOA.
Interestingly, during the inclusion period we observed that many patients preferred the face-to-face treatment program and were somewhat reluctant towards the telephone-based treatment. Ninety percent of the eligible patients who declined to participate did so because they preferred the face-to-face treatment. This preference can be supported by a study examining the acceptability of face-to-face, internet and telephone treatment delivery in primary care, showing the highest level of interest in face-to-face treatment delivery40.
There are some important limitations that need to be addressed. First, this study was developed as a pragmatic trial implemented in daily clinical practice, so due to pragmatic considerations we did not include a control group receiving no treatment (e.g. waiting list). Second, this study involved patients clinically diagnosed with GOA referred for rehabilitation which might hamper the generalizability of our findings to other OA populations. In the absence of a widely accepted and validated definition of GOA, we used a pragmatic definition. Future research is needed to determine an appropriate definition for clinical and research use5. Third, as we did not make statistical adjustments for multiple testing, there is a risk of positive results arising by chance alone (type 1 error), whereas the small loss of power might have increased the chance of a type 2 error. The inclusion proceeded at a lower pace than expected as many patients declined to participate because they preferred the face-to-face treatment group. So, due to time constraints we needed to stop the inclusion after 158 out of 236 patients agreed to participate. Finally, we did not measure adherence to homework assignments in order to ensure blinding to group assignment of the assessor who was responsible for the data collection. The success of blinding was however not evaluated.
In this clinical trial we demonstrated no evidence of important differences in treatment effect between patients with GOA who followed a non-pharmacological multidisciplinary face-to-face self-management program and those who received a telephone-based treatment

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 51
3
program. Furthermore, both treatment programs showed small significant improvements on several domains, however these are unlikely to be of clinical importance. We also observed that many participants preferred face-to-face treatment delivery above telephone delivery. The results imply that the choice of treatment delivery can be based on the patients and healthcare providers preferences, costs or the availability of facilities and/or healthcare systems. Furthermore, our findings contribute to the increasing evidence of the limited effect of self-management programs for patients with OA. Future research is needed to understand which outcomes are most relevant to assess the effectiveness of GOA self-management programs.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
52 | Chapter 3
References
1. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet 2011; 377: 2115-26
2. Petersson IF, Jacobsson LT. Osteoarthritis of the peripheral joints. Best.Pract.Res.Clin.Rheumatol. 2002; 16: 741-60
3. Bierma-Zeinstra SM, Verhagen AP. Osteoarthritis subpopulations and implications for clinical trial design. Arthritis Res.Ther. 2011; 13: 213
4. Felson DT. Identifying different osteoarthritis phenotypes through epidemiology. Osteoarthritis.Cartilage. 2010; 18: 601-4
5. Nelson AE, Smith MW, Golightly YM, Jordan JM. “Generalized osteoarthritis”: A systematic review. Semin.Arthritis Rheum. 2014; 43: 713-20
6. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011; 78: 275-8
7. Hoogeboom TJ, den Broeder AA, Swierstra BA, de Bie RA, van den Ende CH. Joint-pain comorbidity, health status, and medication use in hip and knee osteoarthritis: a cross-sectional study. Arthritis Care Res.(Hoboken.) 2012; 64: 54-8
8. Perruccio AV, Power JD, Evans HM, Mahomed SR, Gandhi R, Mahomed NN et al. Multiple joint involvement in total knee replacement for osteoarthritis: Effects on patient-reported outcomes. Arthritis Care Res.(Hoboken.) 2012; 64: 838-46
9. National Collaborating Centre for Chronic Conditions. Osteoarthritis: national clinical guideline for care and management in adults. London: Royal College of Physicians, 2008.
10. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann.Rheum.Dis. 2013; 72: 1125-35
11. Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip,
and knee. Arthritis Care Res.(Hoboken.) 2012; 64: 465-74
12. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis.Cartilage. 2014; 22: 363-88
13. Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: The Chronic Osteoarthritis Management Initiative of the U.S. Bone and Joint Initiative. Semin.Arthritis Rheum. 2014; 43: 701-12
14. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
15. Hoogeboom TJ, den Broeder AA, de Bie RA, van den Ende CH. Longitudinal impact of joint pain comorbidity on quality of life and activity levels in knee osteoarthritis: data from the Osteoarthritis Initiative. Rheumatology.(Oxford) 2013; 52: 543-6
16. Suri P, Morgenroth DC, Kwoh CK, Bean JF, Kalichman L, Hunter DJ. Low back pain and other musculoskeletal pain comorbidities in individuals with symptomatic osteoarthritis of the knee: data from the osteoarthritis initiative. Arthritis Care Res.(Hoboken.) 2010; 62: 1715-23
17. Hoogeboom TJ, Stukstette MJ, de Bie RA, Cornelissen J, den Broeder AA, van den Ende CH. Non-pharmacological care for patients with generalized osteoarthritis: design of a randomized clinical trial. BMC.Musculoskelet.Disord. 2010; 11: 142
18. Weinberger M, Tierney WM, Cowper PA, Katz BP, Booher PA. Cost-effectiveness of increased telephone contact for patients with osteoarthritis. A randomized, controlled trial. Arthritis Rheum. 1993; 36: 243-6
19. Eakin E, Reeves M, Winkler E, Lawler S, Owen N. Maintenance of physical activity and dietary change following a telephone-delivered intervention. Health Psychol. 2010; 29: 566-73

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 53
3
20. Goode AD, Reeves MM, Eakin EG. Telephone-delivered interventions for physical activity and dietary behavior change: an updated systematic review. Am.J.Prev.Med. 2012; 42: 81-8
21. Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Ann.Intern.Med. 2008; 148: 295-309
22. O’Halloran PD, Blackstock F, Shields N, Holland A, Iles R, Kingsley M et al. Motivational interviewing to increase physical activity in people with chronic health conditions: a systematic review and meta-analysis. Clin.Rehabil. 2014; 28: 1159-71
23. Boers M, Jacobs JW, Vliet Vlieland TP, van Riel PL. Consensus Dutch health assessment questionnaire. Ann.Rheum.Dis. 2007; 66: 132-3
24. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med.Care 1992; 30: 473-83
25. Vercoulen JH, Swanink CM, Fennis JF, Galama JM, van der Meer JW, Bleijenberg G. Dimensional assessment of chronic fatigue syndrome. J.Psychosom.Res. 1994; 38: 383-92
26. Beurskens AJ, de Vet HC, Koke AJ, Lindeman E, van der Heijden GJ, Regtop W et al. A patient-specific approach for measuring functional status in low back pain. J.Manipulative Physiol Ther. 1999; 22: 144-8
27. Luszczynska A, Scholz U, Schwarzer R. The general self-efficacy scale: multicultural validation studies. J.Psychol. 2005; 139: 439-57
28. Maas M, Taal E, van der Linden S, Boonen A. A review of instruments to assess illness representations in patients with rheumatic diseases. Ann.Rheum.Dis. 2009; 68: 305-9
29. Vlaeyen JW, Kole-Snijders AM, Boeren RG, van EH. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain 1995; 62: 363-72
30. Wendel-Vos GC, Schuit AJ, Saris WH, Kromhout D. Reproducibility and relative
validity of the short questionnaire to assess health-enhancing physical activity. J.Clin.Epidemiol. 2003; 56: 1163-9
31. Pham T, Van Der Heijde D, Lassere M, Altman RD, Anderson JJ, Bellamy N et al. Outcome variables for osteoarthritis clinical trials: The OMERACT-OARSI set of responder criteria. J.Rheumatol. 2003; 30: 1648-54
32. Kosinski M, Zhao SZ, Dedhiya S, Osterhaus JT, Ware JE, Jr. Determining minimally important changes in generic and disease-specific health-related quality of life questionnaires in clinical trials of rheumatoid arthritis. Arthritis Rheum. 2000; 43: 1478-87
33. Royston P. Multiple imputation of missing values: Update of ice. Stata Journal 2005; 5: 527-36
34. Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 2009; 338: b2393
35. Gupta SK. Intention-to-treat concept: A review. Perspect.Clin.Res. 2011; 2: 109-12
36. Alderson P. Absence of evidence is not evidence of absence. BMJ 2004; 328: 476-7
37. Zhang W, Nuki G, Moskowitz RW, Abramson S, Altman RD, Arden NK et al. OARSI recommendations for the management of hip and knee osteoarthritis: part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis.Cartilage. 2010; 18: 476-99
38. Kloppenburg M. Hand osteoarthritis-nonpharmacological and pharmacological treatments. Nat.Rev.Rheumatol 2014; 10: 242-51
39. Kroon FP, van der Burg LR, Buchbinder R, Osborne RH, Johnston RV, Pitt V. Self-management education programmes for osteoarthritis. Cochrane.Database.Syst.Rev. 2014; 1: CD008963
40. Mohr DC, Siddique J, Ho J, Duffecy J, Jin L, Fokuo JK. Interest in behavioral and psychological treatments delivered face-to-face, by telephone, and by internet. Ann.Behav.Med. 2010; 40: 89-98

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
54 | Chapter 3
App
endi
x 1.
Con
tent
of a
non
-pha
rmac
olog
ical
face
-to-
face
trea
tmen
t pro
gram
and
a te
leph
one-
base
d tr
eatm
ent p
rogr
am fo
r pati
ents
with
GO
AFa
ce-t
o-fa
ce tr
eatm
ent
Tele
phon
e-ba
sed
trea
tmen
tSe
ssio
nCo
nten
t of t
he s
essi
onH
ealt
hcar
e pr
ovid
erCo
nten
t of t
he s
essi
onH
ealt
hcar
e pr
ovid
er
1•
60 m
inut
es g
roup
edu
catio
n on
the
trea
tmen
t pro
gram
, di
scus
sion
of e
xpec
tatio
ns a
nd in
form
ation
on
activ
ity a
nd fo
od
cons
umpti
on d
iarie
s
PT•
60 m
inut
es g
roup
edu
catio
n on
the
trea
tmen
t pro
gram
, GO
A,
pain
man
agem
ent,
pain
, med
icati
on, p
hysic
al (i
n)ac
tivity
, ac
tivity
pac
ing,
food
con
sum
ption
and
acc
epta
nce
of th
e di
seas
e
SN
•90
min
utes
gro
up e
duca
tion
on G
OA,
pai
n m
anag
emen
t, pa
in
and
med
icati
onSN
•60
min
utes
form
ulati
ng p
erso
nal g
oals
rega
rdin
g pa
in
man
agem
ent,
phys
ical
acti
vity
and
/or a
ctivi
ty p
acin
gSN
•60
min
utes
gen
eral
exe
rcise
pro
gram
to im
prov
e th
e qu
ality
of
mov
emen
t and
to im
plem
ent e
xerc
ises
in th
e ho
me
situa
tion
OT
& P
T
2•
60 m
inut
es g
roup
edu
catio
n on
the
bene
fits
of p
hysic
al a
ctivi
ty
and
nega
tive
cons
eque
nces
of i
nacti
vity
PT
•15
min
utes
indi
vidu
al m
onito
ring
of p
erso
nal g
oals
via
tele
phon
eSN
•60
min
utes
gro
up e
duca
tion
on a
ctivi
ty p
acin
g an
d di
scus
sion
of th
e ac
tivity
dia
ries
OT
•60
min
utes
gen
eral
exe
rcise
pro
gram
to im
prov
e th
e qu
ality
of
mov
emen
t and
to im
plem
ent e
xerc
ises
in th
e ho
me
situa
tion
OT
& P
T
•60
min
utes
tai-c
hiPT
3•
60 m
inut
es g
roup
edu
catio
n on
food
con
sum
ption
D
•60
min
utes
gen
eral
exe
rcise
pro
gram
to im
prov
e th
e qu
ality
of
mov
emen
t and
to im
plem
ent e
xerc
ises
in th
e ho
me
situa
tion
OT
& P
T
•60
min
utes
form
ulati
ng p
erso
nal g
oals
rega
rdin
g pa
in
man
agem
ent,
phys
ical
acti
vity
and
/or a
ctivi
ty p
acin
gPT
4•
60 m
inut
es g
roup
edu
catio
n on
food
con
sum
ption
and
di
scus
sion
of th
e fo
od c
onsu
mpti
on d
iarie
sD
•30
min
utes
indi
vidu
al m
onito
ring
of p
erso
nal g
oals
via
tele
phon
eSN
•30
min
utes
Bris
k w
alki
ng (w
alki
ng a
t a fa
st p
ace)
PT
•60
min
utes
gro
up-b
ased
mon
itorin
g an
d di
scus
sion
of p
erso
nal
goal
sPT
•60
min
utes
spe
cific
exe
rcise
pro
gram
tailo
red
to th
e pa
tient
’s in
divi
dual
ly h
ealth
pro
blem
s to
impl
emen
t the
exe
rcise
s in
the
hom
e sit
uatio
n
OT
5•
60 m
inut
es g
roup
edu
catio
n on
acc
epta
nce
of th
e di
seas
e an
d di
scus
sion
of st
artin
g po
ints
to im
plem
ent t
his
in th
e ho
me
situa
tion
SN•
60 m
inut
es g
roup
-bas
ed m
onito
ring
and
disc
ussio
n of
per
sona
l go
als
SN

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Effectiveness of two non-pharmacological treatment programs for GOA | 55
3
App
endi
x 1.
Con
tent
of a
non
-pha
rmac
olog
ical
face
-to-
face
trea
tmen
t pro
gram
and
a te
leph
one-
base
d tr
eatm
ent p
rogr
am fo
r pati
ents
with
GO
AFa
ce-t
o-fa
ce tr
eatm
ent
Tele
phon
e-ba
sed
trea
tmen
tSe
ssio
nCo
nten
t of t
he s
essi
onH
ealt
hcar
e pr
ovid
erCo
nten
t of t
he s
essi
onH
ealt
hcar
e pr
ovid
er
1•
60 m
inut
es g
roup
edu
catio
n on
the
trea
tmen
t pro
gram
, di
scus
sion
of e
xpec
tatio
ns a
nd in
form
ation
on
activ
ity a
nd fo
od
cons
umpti
on d
iarie
s
PT•
60 m
inut
es g
roup
edu
catio
n on
the
trea
tmen
t pro
gram
, GO
A,
pain
man
agem
ent,
pain
, med
icati
on, p
hysic
al (i
n)ac
tivity
, ac
tivity
pac
ing,
food
con
sum
ption
and
acc
epta
nce
of th
e di
seas
e
SN
•90
min
utes
gro
up e
duca
tion
on G
OA,
pai
n m
anag
emen
t, pa
in
and
med
icati
onSN
•60
min
utes
form
ulati
ng p
erso
nal g
oals
rega
rdin
g pa
in
man
agem
ent,
phys
ical
acti
vity
and
/or a
ctivi
ty p
acin
gSN
•60
min
utes
gen
eral
exe
rcise
pro
gram
to im
prov
e th
e qu
ality
of
mov
emen
t and
to im
plem
ent e
xerc
ises
in th
e ho
me
situa
tion
OT
& P
T
2•
60 m
inut
es g
roup
edu
catio
n on
the
bene
fits
of p
hysic
al a
ctivi
ty
and
nega
tive
cons
eque
nces
of i
nacti
vity
PT
•15
min
utes
indi
vidu
al m
onito
ring
of p
erso
nal g
oals
via
tele
phon
eSN
•60
min
utes
gro
up e
duca
tion
on a
ctivi
ty p
acin
g an
d di
scus
sion
of th
e ac
tivity
dia
ries
OT
•60
min
utes
gen
eral
exe
rcise
pro
gram
to im
prov
e th
e qu
ality
of
mov
emen
t and
to im
plem
ent e
xerc
ises
in th
e ho
me
situa
tion
OT
& P
T
•60
min
utes
tai-c
hiPT
3•
60 m
inut
es g
roup
edu
catio
n on
food
con
sum
ption
D
•60
min
utes
gen
eral
exe
rcise
pro
gram
to im
prov
e th
e qu
ality
of
mov
emen
t and
to im
plem
ent e
xerc
ises
in th
e ho
me
situa
tion
OT
& P
T
•60
min
utes
form
ulati
ng p
erso
nal g
oals
rega
rdin
g pa
in
man
agem
ent,
phys
ical
acti
vity
and
/or a
ctivi
ty p
acin
gPT
4•
60 m
inut
es g
roup
edu
catio
n on
food
con
sum
ption
and
di
scus
sion
of th
e fo
od c
onsu
mpti
on d
iarie
sD
•30
min
utes
indi
vidu
al m
onito
ring
of p
erso
nal g
oals
via
tele
phon
eSN
•30
min
utes
Bris
k w
alki
ng (w
alki
ng a
t a fa
st p
ace)
PT
•60
min
utes
gro
up-b
ased
mon
itorin
g an
d di
scus
sion
of p
erso
nal
goal
sPT
•60
min
utes
spe
cific
exe
rcise
pro
gram
tailo
red
to th
e pa
tient
’s in
divi
dual
ly h
ealth
pro
blem
s to
impl
emen
t the
exe
rcise
s in
the
hom
e sit
uatio
n
OT
5•
60 m
inut
es g
roup
edu
catio
n on
acc
epta
nce
of th
e di
seas
e an
d di
scus
sion
of st
artin
g po
ints
to im
plem
ent t
his
in th
e ho
me
situa
tion
SN•
60 m
inut
es g
roup
-bas
ed m
onito
ring
and
disc
ussio
n of
per
sona
l go
als
SN
•60
min
utes
spe
cific
exe
rcise
pro
gram
tailo
red
to th
e pa
tient
’s in
divi
dual
ly h
ealth
pro
blem
s to
impl
emen
t the
exe
rcise
s in
the
hom
e sit
uatio
n
PT•
60 m
inut
es s
peci
fic e
xerc
ise p
rogr
am ta
ilore
d to
the
patie
nt’s
indi
vidu
ally
hea
lth p
robl
ems
to im
plem
ent t
he e
xerc
ises
in th
e ho
me
situa
tion
SN &
PT
•60
min
utes
gro
up-b
ased
mon
itorin
g an
d di
scus
sion
of p
erso
nal
goal
sO
T
6•
60 m
inut
es g
roup
-bas
ed m
onito
ring
and
disc
ussio
n of
per
sona
l go
als
PT•
20 m
inut
es s
etting
futu
re g
oals
and
eval
uatin
g th
e tr
eatm
ent
prog
ram
via
tele
phon
eSN
•30
min
utes
hyd
roth
erap
yPT
•60
min
utes
spe
cific
exe
rcise
pro
gram
tailo
red
to th
e pa
tient
’s in
divi
dual
ly h
ealth
pro
blem
s to
impl
emen
t the
exe
rcise
s in
the
hom
e sit
uatio
n
OT
7•
120
min
utes
setti
ng fu
ture
per
sona
l goa
ls an
d ev
alua
ting
the
trea
tmen
t pro
gram
O
T &
PT
•20
min
utes
indi
vidu
al m
onito
ring
of p
erso
nal g
oals
via
tele
phon
eSN
Abbr
evia
tions
: PT
= ph
ysic
al th
erap
ist; S
N =
spe
cial
ized
rheu
mat
olog
y nu
rse;
OT
= oc
cupa
tiona
l the
rapi
st; D
= d
ietic
ian


CHAPTER 4
Cost-utility and cost-effectiveness analysis of
face-to-face versus telephone-based non-pharmacological
multidisciplinary treatment for patients with generalized
osteoarthritis
Nienke Cuperus, Wilbert B. van den Hout, Thomas J. Hoogeboom, Frank J. van den Hoogen, Thea P.M. Vliet Vlieland, Cornelia H.M. van den Ende
Submitted

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
58 | Chapter 4
Abstract
ObjectiveTo evaluate from a societal perspective the cost-utility and cost-effectiveness of a non-pharmacological face-to-face treatment program compared with a telephone-based treatment program for patients with generalized osteoarthritis (GOA).
MethodsAn economic evaluation was carried out alongside a randomized clinical trial involving 147 patients with GOA. Program costs were estimated from time registrations. One year medical and non-medical costs were estimated using cost questionnaires. Quality adjusted life years (QALYs) were estimated using the EuroQol classification system, EuroQol rating scale and Short Form-6D. Daily function was measured using the Health Assessment Questionnaire (HAQ-DI). Cost and effect differences were estimated using multilevel regression analysis and cost-effectiveness acceptability curves.
ResultsThe medical costs of both programs were estimated at €387 and €252, respectively. The difference in total societal costs was non-significantly in favour of the face-to-face program (difference (95% CI): €708 (€-5058, 3642)). QALYs were similar for both groups according to the EuroQol, but were significantly in favour of the face-to-face group according to the SF-6D (difference (95% CI): 0.022 (0.000, 0.045)). Daily function was similar according to the HAQ-DI. Since both societal costs and effects were in favour of the face-to-face program, the economic assessment favoured this program, regardless society’s willingness to pay. For a range between €20.000-€80.000 per QALY, there was a 65%-90% chance that the face-to-face program had better cost utility.
ConclusionThis economic evaluation from a societal perspective showed that a non-pharmacological, face-to-face treatment program for patients with GOA was likely to be cost-effective relative to a telephone-based program.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 59
4
Introduction
Osteoarthritis (OA) is the most prevalent chronic joint disease affecting mainly the hand, knee and hip joints1. Next to the health burden, OA represent a significant economic burden on individuals, healthcare systems and society with costs accounting for 1%-2.5% of the gross domestic product in Western countries2-4. Because OA leads to considerable costs, it is important that clinical evaluations of OA interventions are accompanied by economic evaluations in order to inform decision makers about the efficiency of healthcare resources and to guide healthcare policy and decision processes5,6.
Non-pharmacological, non-surgical interventions like education, self-management, exercises and weight reduction have been emphasized as first line treatments for the management of patients with OA in international evidence-based clinical guidelines7,8. Many trials have demonstrated positive effects of these interventions on the predominant symptoms of OA i.e. pain and function9,10. However, high quality evidence of the cost-effectiveness of non-pharmacological interventions for OA is limited as shown by a recently published systematic review on the cost-effectiveness of non-pharmacological, non-surgical interventions for patients with hip and knee OA11. Based on the available studies, the authors suggested that exercise programs appear to be the best value for money in the management of patients with hip and knee OA. Yet, high quality economic evaluations alongside clinical studies are needed6,11.
To date, there have been no economic evaluations of non-pharmacological interventions for patients diagnosed with generalized osteoarthritis (GOA). GOA is a widely used and accepted OA phenotype describing the often polyarticular nature of OA12. Although it has been suggested that individuals with GOA represent a relatively large subgroup of patients with OA (e.g. approximately 50% of patients with knee OA can be classified as having GOA)13, OA populations are mostly examined for a specific localization of the disease (usually the hands, hips or knees) without considering the involvement of multiple joints. As such, research on (the management of) GOA is very limited. Recently, we evaluated the effectiveness of a non-pharmacological multidisciplinary, face-to-face treatment program versus a telephone-based treatment program on daily function for individuals with GOA (accepted for publication). That study showed small, non-significant differences in effectiveness on daily function and other clinical outcomes between both treatment programs. In this article, we present the results of an incremental cost-effectiveness and cost-utility analysis of the face-to-face treatment program in comparison to the telephone-based treatment program.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
60 | Chapter 4
Methods
Study designWe conducted an economic evaluation alongside a randomized single-blind clinical superiority trial comparing the effectiveness of a non-pharmacological multidisciplinary face-to-face treatment program with a telephone-based treatment program for patients with GOA. Details of the trial design have been published previously14. The economic evaluation was conducted from a societal perspective in accordance with current Dutch guidelines for economic evaluations15. The time horizon of the study was limited to the duration of the trial (i.e. one year). The study was performed at the outpatient rheumatology departments of the Sint Maartenskliniek Nijmegen and Woerden, the Netherlands from January 2010 to April 2014 and was approved by the local ethics committee (CMO region Arnhem, Nijmegen) and registered in the Dutch Trial Register (Trial Register Number NTR2137). All participants signed informed consent.
Study populationPatients recently diagnosed with GOA by their rheumatologist and referred for non-pharmacological multidisciplinary treatment, were screened for eligibility to participate in the trial during a screening visit. Patients were included when: (1) having at least two objective signs indicating OA in ≥ 2 joint areas on the basis of the patient’s medical record (objective signs included: malalignment, crepitation, limited range of motion, palpable osteophytes or nodules or radiographic signs including the presence of joint space narrowing and/or osteophytes); (2) having complaints in ≥ 3 out of eight joint areas; and (3) being limited in the performance of daily activities (Health Assessment Questionnaire Disability Index (HAQ-DI) score ≥ 0.5). Excluded were patients who were: (1) diagnosed with another rheumatic disease; (2) awaiting surgery; (3) having psychosocial problems interfering with the scope of the treatment; (4) already participated unsuccessfully in a self-management program; (5) incapable of coming to the hospital; and (6) unable to write/understand the Dutch language. In total, 158 patients were included. For more details on the study population, we refer to the clinical paper.
Treatment programsThe overall goals of both treatment programs were to improve daily function by optimizing the patient’s lifestyle and to enhance self-management skills to control the consequences of the disease. The contents of the treatment programs were comparable, but several critical differences were apparent i.e. the mode of care delivery, the number of involved healthcare providers, the number of group sessions and the number of sessions including an exercise program. The multidisciplinary face-to-face treatment program comprised seven

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 61
4
therapeutic group sessions during six weeks with a total duration of 21.5 hours per patient, all performed at the outpatient department. This program was provided by a multidisciplinary team comprising a physical therapist, occupational therapist, specialized rheumatology nurse and dietician. Main components were education, goal setting with respect to multiple domains of daily living and improving self-management skills to cope with the consequences of the disease. Additionally, patients participated in a general and individually tailored exercise program to improve the quality of movement and to implement exercises in the home situation. Patients allocated to the telephone-based treatment program attended two face-to-face group sessions at the outpatient clinic, which were further monitored by four individual telephone contact moments. This program was provided by a specialized rheumatology nurse and physical therapist. The total duration of this program was 5.4 hours per patient. Main components of this program were education and goal setting with respect to multiple domains of daily living. These goals were closely monitored and discussed during the telephone contact moments. In both programs, the involved healthcare providers were trained in techniques of motivational interviewing and were specialized in treating patients with musculoskeletal disorders and teaching self-management principles.
Outcome measures
Clinical outcome and utility measuresThe primary outcome measure of the clinical trial was daily function measured with the Dutch consensus HAQ-DI16 assessed at baseline, 6, 26 and 52 weeks. The HAQ-DI examines difficulties with performing 20 daily activities, resulting in a disability index ranging from 0 (no disability) to 3 (very severe disability). The primary endpoint of the clinical trial was the difference in mean HAQ-DI score between both treatment programs over one year follow-up i.e. the average score obtained from the 6, 26 and 52 week time points.
We measured utility in three ways. Utility is the valuation of a patients’ health state on a scale anchored at 0 (as bad as death) to 1 (full health). Patients described their general health status using the EuroQol-5D (EQ-5D)17 assessed at baseline, 6, 13, 26, 36 and 52 weeks. From the EQ-5D classification system, a utility index was calculated. The EQ-5D is the most commonly used and validated utility measure for use in economic evaluations18. Furthermore, patients rated their health status using the EuroQol rating scale (RS) from 0-100, where 0 indicates worst imaginable health and 100 indicates best imaginable health. The rating scale was transformed (TRS) into a utility score using the formula: TRS = 1-(1-RS/100)1.61 19. Quality of life was also measured using the widely used and validated Short Form 36 Health Survey (SF-36) assessed at baseline, 6, 26 and 52 weeks. This measure was converted into a six-dimensional health state classification; the Short Form 6D (SF-6D) utility index, describing a patient’s health status20. The SF-6D is a more recent instrument which is increasingly used

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
62 | Chapter 4
for economic evaluations of clinical interventions18,21. Currently, there is no consensus on the best utility measure for use in economic evaluations22. We estimated quality adjusted life years (QALYs) for each patient by the area under the EQ-5D, SF-6D and TRS utility curves. A QALY integrates effects in terms of both quality of life and the duration of time in such a health state and is a frequently used measure for healthcare resource allocation decisions22.
CostsIn addition to the program costs, during the one year follow-up period, participants reported all GOA-related direct medical costs (i.e. healthcare-related) and non-medical costs (i.e. other health-related) using cost questionnaires at 6, 13, 26, 39 and 52 weeks23. Prices were generally obtained from standard cost prices (including overhead costs) published in the Dutch costing guideline designed to reflect societal costs and to standardize economic evaluations15. Otherwise, we used published cost prices or market prices. Costs were converted to a 2014 price level using the price index rate for the Dutch healthcare sector (www.cbs.nl). Because the follow-up period of this study was limited to one year, no discounting was applied.
Costs of both treatment programsCosts of the treatment programs per patient were estimated using a bottom-up cost price analysis, based on time registrations. The medical costs included direct consultation time and the indirect time required to prepare sessions and administration time. Program costs also included non-medical costs i.e. the patient’s invested time and travel costs. Furthermore, costs for accommodation were included. The group-based treatment sessions are assumed to take place in gyms, rented at €20 per hour based on market prices. This includes costs for materials.
Medical costsDirect medical costs included in the current study were costs of GOA-related healthcare resource utilization. Resources comprised the number of consultations with all relevant healthcare providers (e.g. general practitioner, physical therapist, rheumatology nurse, medical specialist etc.), GOA-related hospitalization and type and dose of medication used over the period of one year. We computed the costs of healthcare resource use by multiplying the price per resource by the number of consultations consumed. To estimate the costs of GOA-related surgery, prices of surgical operations were obtained from the Dutch Health Authority (www.nza.nl). Type and dose of medication was reported by the patients, or otherwise we used the standard daily dose (https://kennisbank.knmp.nl). Purchased medication was valued using prices of medication (www.medicijnkosten.nl) plus €6 for each purchase other than over-the-counter medications15,24.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 63
4
Non-medical costsThe reported healthcare costs included time and travel costs (direct non-medical costs) required to visit healthcare providers. Patient time was valued at €12.50 per hour (price for informal care) and travel costs at 20 cents per kilometre travelled plus €3 parking costs15. Patients reported their means of transportation and travel distance to the healthcare resources. Other direct non-medical costs were costs for home care, assistive devices and house adaptations. The number of hours of home care or domestic help needed by patients was extracted from the questionnaire. Assistive devices at home and house adaptations were valued as reported by patients, or otherwise market prices were used. Productivity costs assessed in the current study were costs due to absenteeism from paid work. Patients reported their working status and absenteeism in the questionnaires. We used the friction cost method to calculate the costs of productivity losses, considering productivity loss due to absenteeism only for the period that is needed to replace an employee25. Current guidelines set this friction period at 23 weeks26. Production loss was valued using age and sex specific incomes of the Dutch population taking into account an elasticity of 0.8 between reduced labour time and productivity15.
Statistical analysisData were analysed using Stata/IC 13.1. Multiple imputation by changed equation was used to estimate missing data in order to preserve power and reduce bias27,28. A total of 20 imputed data sets were predicted based on available data. Analyses were done according to the intention-to-treat principle, meaning that patients were analysed according to randomized treatment assignment29. The sample size was based on clinical outcomes14.
In our economic evaluation, the net benefits of both treatment programs were estimated for a range of society’s willingness to pay (WTP) values using the formula: net benefit = WTP × effect (QALY or HAQ-DI) – costs30. This net benefit was calculated for each patient individually and compared between groups. The more cost-effective treatment program is the program with the higher average net benefits, depending on a range of thresholds for the society’s WTP. When none of the treatment programs appeared to be dominant (i.e. was more effective and less costly), then the incremental cost-effectiveness ratio (ICER) was estimated by dividing the difference in mean costs between both treatment programs by the difference in mean HAQ-DI score or QALYs gained. Given the statistical uncertainty of differences between costs and QALYs, cost-effectiveness acceptability curves (CEAC) were constructed to evaluate the probability that the face-to-face treatment program was cost-effective compared to the telephone-based program, depending on a range of thresholds for the WTP for an additional QALY or HAQ-DI point31,32. Differences in costs and QALYs between both treatment groups were analysed using multilevel mixed linear regression models with mean scores as dependent variable and treatment group, sex and baseline value as covariates with group included as random effect.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
64 | Chapter 4
Results
In total, 147 patients were included in the economic evaluation; 75 allocated to the face-to-face treatment group and 72 allocated to the telephone-based treatment group. The mean (SD) age across both treatment groups was 60 (8), 85% of participants were female and ≥ 90% reported symptoms in both the upper and lower extremities. There were no relevant differences in baseline characteristics between groups. On average, 8% of the HAQ-DI measurements, 11% of the utility measurements and 12% of the healthcare resource use measurements were missing.
Utilities and clinical outcomeTable 1 reports EQ5D, TRS, and SF-6D scores at each time point. For all three utility measures, the valuation of health after one year follow-up was more favourable in the face-to-face treatment group, however these differences were not statistically significant (Figure 1). A statistically significant (p = 0.049) difference in QALYs between both treatment groups was observed for the SF-6D (mean group difference (95% CI): 0.022 (0.000, 0.045)). At baseline, the mean (SD) HAQ-DI score was 1.27 (0.50) for the face-to-face group and 1.26 (0.49) for the telephone-based treatment group. Patients in the face-to-face treatment group showed a larger improvement in daily function over one year follow-up compared to the patients in the telephone-based treatment group, however this difference was not statistically significant (mean group difference HAQ-DI (95% CI): -0.03 (-0.14, 0.07), p = 0.58).
Costs of both treatment programsThe medical costs of the face-to-face treatment and telephone-based treatment programs were estimated at €387 and €252 per patient, respectively (Table 2). Including the non-medical costs, the total program costs were estimated at €762 per patient for the face-to-face treatment program and €358 for the telephone-based treatment program. The higher total program costs for the face-to-face program were primarily due to the patients’ time costs.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 65
4
Table 1. Utility scores, quality-adjusted life years (QALYs) and mean differences between both treatment groups1
Face-to-facetreatment group
(n = 75)
Telephone-basedtreatment group
(n = 72)Group difference
(95% CI)2p
EQ-5D utility scoreBaseline 0.57 ± 0.25 0.57 ± 0.26 0.000 (-0.081, 0.082) 0.996 weeks 0.63 ± 0.24 0.58 ± 0.26 0.048 (-0.026, 0.123) 0.2013 weeks 0.61 ± 0.27 0.58 ± 0.32 0.030 (-0.050, 0.110) 0.4626 weeks 0.59 ± 0.30 0.59 ± 0.26 -0.000 (-0.084, 0.082) 0.9839 weeks 0.59 ± 0.30 0.59 ± 0.31 -0.011 (-0.099, 0.077) 0.8152 weeks 0.59 ± 0.25 0.57 ± 0.26 0.019 (-0.069, 0.106) 0.67
EQ-5D QALY 0.60 ± 0.21 0.59 ± 0.21 0.012 (-0.042, 0.066) 0.67TRS utility score
Baseline 0.70 ± 0.20 0.69 ± 0.16 0.009 (-0.042, 0.060) 0.746 weeks 0.78 ± 0.12 0.75 ± 0.11 0.033 (-0.007, 0.074) 0.1113 weeks 0.76 ± 0.12 0.75 ± 0.18 0.012 (-0.035, 0.060) 0.6126 weeks 0.76 ± 0.14 0.73 ± 0.13 0.025 (-0.022, 0.071) 0.3139 weeks 0.75 ± 0.20 0.74 ± 0.16 0.007 (-0.044, 0.058) 0.7952 weeks 0.74 ± 0.15 0.73 ± 0.13 0.015 (-0.039, 0.068) 0.59
TRS QALY 0.75 ± 0.10 0.74 ± 0.09 0.016 (-0.012, 0.044) 0.28SF-6D utility score
Baseline 0.66 ± 0.10 0.68 ± 0.07 -0.017 (-0.045, 0.012) 0.256 weeks 0.69 ± 0.09 0.68 ± 0.08 0.021 (-0.005, 0.047) 0.1226 weeks 0.69 ± 0.09 0.68 ± 0.09 0.022 (-0.010, 0.053) 0.1852 weeks 0.70 ± 0.11 0.67 ± 0.10 0.033 (-0.004, 0.074) 0.08
SF-6D QALY 0.69 ± 0.08 0.68 ± 0.07 0.022 (0.000, 0.045) 0.05
1Values are the mean ± SD unless indicated otherwise2Multilevel mixed linear regression analyses corrected for baseline values, sex and group-wise treatmentAbbreviations: SD = standard deviation; CI = confidence interval
Healthcare resource utilization and costsThe average annual volumes of healthcare and non-healthcare resource utilization, the percentage of patients using each resource and the costs per patient are presented for both treatment groups in Table 3. Over the one year follow-up period, the difference between both randomization groups in total one year non-program medical costs was estimated at €780 (95% CI: -2151, 590), non-significantly in favour of the face-to-face treatment group. Outside the treatment program, the mean number of sessions with a physical therapist per patient was 21 in both groups. Almost all patients purchased medication during the one year follow-up period i.e. 100% in the telephone-based treatment group and 97% in the face-

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
66 | Chapter 4
to-face treatment group. Furthermore, in both groups less than 20% of patients visited a dietician.
0,3
0,4
0,5
0,6
0,7
0,8
0,9
0 6 26 52
Util
ity
Weeks since randomization
Figure 1. Average utility per patient for both treatment groups. Abbreviations: EQ-5D = European Quality of life; SF-6D = Short-Form-6D; TRS = Transformed Rating Scale
The difference in total one year non-program non-medical costs between both treatment groups was estimated at €393 (95% CI: -3870, 3085), non-significantly in favour of the face-to-face treatment program. Most of the non-medical costs were attributable to productivity losses. Including program costs, the mean total societal costs per patient was estimated at €10,324 for the face-to-face treatment program and €11,023 for the telephone-based treatment program, meaning a difference in total societal costs of €708 (95% CI: -5058, 3642) between both programs in favour of the face-to-face treatment program. This difference was not statistically significant.
Cost-effectiveness and cost-utilityThe primary economic evaluation of the current study was the cost-utility analysis comparing the difference between both treatment groups in total societal costs to the difference in QALY based on the EQ-5D14. Because costs as well as QALYs were in favour of the face-to-face treatment program (i.e. the face-to-face program dominates the telephone program), the net benefit was also in favour of the face-to-face program, regardless society’s WTP (and
• EQ-5D SF-6D TRS
— Face-to-face treatment-- Telephone-based treatment

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 67
4
effectiveness and utility ratios were not estimated). Accordingly, the acceptability curve showed a 65 to 70% probability that the face-to-face treatment program was cost-effective for any WTP (Figure 2). The difference in net benefit between both programs did not reach statistical significance.
In the secondary analyses, cost-utility was also in favour of the face-to-face treatment program according to the SF-6D and TRS for all levels of society’s WTP. Since both costs and improvement in daily function (i.e. HAQ-DI) were in favour of the face-to-face treatment program, this program was more cost-effective, however differences in net benefits were not statistically significant. Over all analyses, there was a 65% to 90% chance that the face-to-face treatment program was more cost-effective at a range of WTP thresholds between €20.000 and €80.000.
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 50000 100000 150000 200000
Prop
abili
ty fa
ce-t
o-fa
ce is
cos
t-ef
fect
ive
WTP
EQ-5DSF-6DTRSHAQ-DI
Figure 2. Cost-effectiveness acceptability curve showing the probability that the face-to-face treatment program is cost-effective compared to the telephone-based treatment program over a range of values for the willingness to pay for an additional QALY Abbreviations: WTP = Willingness To Pay; EQ-5D = European Quality of life; SF-6D = Short-Form-6D; TRS = Transformed Rating Scale; HAQ-DI = Health Assessment Questionnaire Disability Index

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
68 | Chapter 4
Tabl
e 2.
Cos
ts p
er p
atien
t of b
oth
trea
tmen
t pro
gram
s
Face
-to-
face
tr
eatm
ent g
roup
Tele
phon
e-ba
sed
trea
tmen
t gro
upD
irec
tti
me,
hou
rsIn
dire
ct ti
me,
ho
urs
Tota
l tim
e,ho
urs
Cost
s,
€D
irec
tti
me,
hou
rsIn
dire
ct ti
me,
ho
urs
Tota
l tim
e, h
ours
Cost
s,
€M
edic
al c
osts
Gro
up Phys
ical
ther
apist
10.5
4.0
14.5
1149
0.5
0.5
40O
ccup
ation
al th
erap
ist6.
54.
010
.563
00
00
Spec
ializ
ed n
urse
, in
grou
p2.
52.
515
03.
52.
56.
036
0Sp
ecia
lized
nur
se, w
ith in
divi
dual
05.
32.
78.
047
9Di
etici
an2.
02.
012
00
00
Acco
mm
odati
on21
.543
04.
080
Tota
l med
ical
cos
ts, p
er g
roup
124
7995
9To
tal m
edic
al c
osts
, per
pati
ent
387
252
Non
-med
ical
cos
tsIn
divi
dual
Patie
nt ti
me
cost
s21
.526
95.
468
Patie
nt tr
avel
cos
ts10
638
Tota
l non
-med
ical
cos
ts, p
er p
atien
t137
510
6To
tal p
rogr
am c
osts
, per
pati
ent1
762
358
1 The
mea
n nu
mbe
r of p
artic
ipan
ts w
as 6
.4 fo
r the
face
-to-
face
trea
tmen
t gro
up a
nd 3
.8 fo
r the
tele
phon
e-ba
sed
trea
tmen
t gro
up

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 69
4
Tabl
e 3.
Ave
rage
ann
ual h
ealth
care
and
non
-hea
lthca
re re
sour
ce u
tiliza
tion,
per
cent
age
of p
atien
ts u
sing
each
reso
urce
and
cos
ts p
er p
atien
t by
trea
tmen
t gro
up.
Face
-to-
face
trea
tmen
t gro
upTe
leph
one-
base
dtr
eatm
ent
grou
pG
roup
di
ffer
ence
3
Uni
t Cos
t, €
1Vo
lum
es (%
)2Co
sts,
€Vo
lum
es (%
)Co
sts,
€Co
sts,
€p
Tota
l tre
atm
ent p
rogr
am c
osts
762
358
339
Non
-pro
gram
med
ical
cos
tsG
ener
al p
racti
tione
rVi
sit a
t pra
ctice
413.
6 (7
9)15
04.
0 (8
3)16
7-1
90.
53Te
leph
one
cont
act
161.
0 (4
0)17
1.0
(36)
161
0.90
Visit
at h
ome
500.
2 (1
0)12
0.4
(14)
19-7
0.44
Hea
lthca
re p
rofe
ssio
nal (
sess
ion)
Phys
ical
ther
apist
5821
.5 (7
0)12
3921
.8 (7
6)12
563
0.99
Occ
upati
onal
ther
apist
471.
4 (2
3)64
2.2
(29)
106
-41
0.36
Exer
cise
ther
apist
602.
3 (1
3)14
0.4.
3 (1
8)26
0-1
220.
44M
anua
l the
rapi
st63
3.2
(22)
201
4.1
(29)
259
-59
0.61
Spec
ializ
ed rh
eum
atol
ogy
nurs
e63
0.3
(19)
210.
6 (2
0)39
-17
0.24
Dieti
cian
490.
8 (1
9)39
1.2
(18)
60-2
40.
37So
cial
wor
ker
910.
3 (7
)29
0.5
(8)
42-1
70.
66Ps
ycho
logi
st17
21.
7 (1
4)28
83.
3 (2
2)56
4-3
250.
19O
ther
hea
lthca
re p
rofe
ssio
nal
602.
5 (2
3)15
12.
3 (2
3)13
5-8
0.92
Com
plem
enta
ry/a
ltern
ative
car
e10
31.
8 (1
9)18
41.
9 (2
7)19
9-1
80.
86Sp
ecia
list c
are
(visi
t)11
64.
8 (7
8)55
95.
7 (7
9)66
1-1
080.
37O
utpa
tient
car
e (d
ay)
376
0.8
(25)
319
0.7
(23)
276
430.
75Su
rger
y(1
5)69
(27)
145
-76
0.12
Med
icati
on u
se(9
7)16
2(1
00)
157
30.
91To
tal n
on-p
rogr
am m
edic
al c
osts
± S
D3,
645
± 4,
040
4,35
9 ±
5,23
8-7
810.
26N
on-p
rogr
am n
on-m
edic
al c
osts
Prof
essio
nal h
ome
care
(hou
r)39
19.2
(22)
741
21.4
(19)
826
-77
0.84
Dom
estic
hel
p (h
our)
2624
.7 (3
0)65
136
.8 (3
2)97
2-3
240.
36Ai
ds a
nd a
pplia
nces
at h
ome
(67)
508
(62)
669
-108
0.37
Abse
ntee
ism fr
om p
aid
labo
ur (h
our)
115
(29)
4017
120
(30)
3839
-104
0.94
Tota
l non
-pro
gram
non
-med
ical
cos
ts ±
SD
5,91
7 ±
10,6
336,
305
± 12
,160
-393
0.83
Tota
l soc
ieta
l cos
ts ±
SD
10,3
24 ±
12,
792
11,0
23 ±
15,
500
-707
0.75
1 Stan
dard
cos
t pric
es p
ublis
hed
in th
e Du
tch
costi
ng g
uide
line15
con
vert
ed to
201
4 us
ing
the
gene
ral D
utch
pric
e in
dex
rate
(ww
.cbs
.nl),
incl
udin
g tr
avel
and
tim
e co
sts
2 Volu
mes
of c
are
indi
cate
the
num
ber o
f con
sulta
tions
, visi
ts, d
ays,
or h
ours
. Per
cent
ages
indi
cate
the
num
ber o
f pati
ents
with
the
spec
ific
type
of c
are
3 Mul
tilev
el m
ixed
line
ar re
gres
sion
anal
yses
cor
rect
ed fo
r sex
and
gro
up-w
ise tr
eatm
ent
Abbr
evia
tion:
SD
= st
anda
rd d
evia
tion

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
70 | Chapter 4
Discussion
We conducted an economic evaluation of two modes of non-pharmacological multidisciplinary therapy delivery i.e. face-to-face vs. telephone for patients clinically diagnosed with GOA. No differences in effectiveness between both treatment programs were found according to the HAQ-DI and EuroQol, whereas QALYs were significantly in favour of the face-to-face treatment group according to the SF-6D. The results showed that from a societal perspective, the face-to-face treatment program was more likely to be cost-effective. The medical costs of both treatment programs were estimated at €387 and €252, respectively. The higher total program costs for the face-to-face treatment program were primarily due to the patients’ time costs. The total societal costs were lower for the face-to-face treatment program than for the telephone-based program, however this difference was not statistically significant. The net benefit of the treatment programs was in favour of the face-to-face program, regardless society’s WTP. Over all analyses, there was a 65% to 90% chance that the face-to-face program was more cost-effective at a range of WTP thresholds between €20.000 and €80.000 per QALY.
In view of the limited healthcare budgets, economic evaluations of interventions are needed to inform decision makers about the efficiency of healthcare resources. Prior to this economic evaluation, we expected the face-to-face treatment program to be considerably more costly since this program was more intensive and more strictly supervised. However, the medical program costs of both treatments were not that different. When accounting patients’ time and travel costs, the face-to-face program was more costly. However, from a societal perspective, the face-to-face treatment program resulted (non-significant) in less costs than the telephone-based program. These results imply that, from the societal perspective, the choice of treatment delivery does not have to be based on costs. During the trial, patients reported their level of satisfaction with the treatment programs showing that patients in the face-to-face group were significantly more satisfied than patients in the telephone-based treatment group. Probably, the choice of treatment delivery could be based on the preferences of patients and healthcare providers or on the availability of facilities and/or healthcare systems.
Interestingly, in both treatment groups less than 20% of patients consulted a dietician, while the majority of patients (> 70% in both groups) were overweight (body mass index > 25 kg/m2). The underutilization of dietary therapy by patients with OA is consistent with a previous study investigating the healthcare use of patients with hip or knee OA33. This is striking as the impact of weight reduction on the predominant OA-related symptoms i.e. pain and function has been well demonstrated34 and is considered to be one of the mainstays of rehabilitation for people with knee and hip OA35,36.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 71
4
Currently, no cost-effectiveness studies of non-pharmacological interventions for patients with GOA are available, hampering a proper comparison of our results with other studies. In patients with hip and knee OA exercise programs appear to be the best value for money, as shown in a systematic review11. However, high quality studies were limited. Also in hand OA, exercises are the most cost-effective treatment strategy37. Increasing evidence shows that non-pharmacological interventions can reduce the need for total joint replacement surgery or postpone surgery after more than five years in patients with hip OA38,39. This in turn might reduce healthcare costs substantially. Future high quality economic evaluations of non-pharmacological interventions for patients with GOA or its effect on the long-term need for joint replacement surgery are needed.
A number of methodological issues should be considered. First, the cost data reported by the patients were not ascertained by consulting other data sources. Self-reported healthcare utilization questionnaires are known to underreport healthcare use, whereby the degree of inaccuracy depends on the type of utilization (underreporting of utilization is exacerbated by increased utilization)40,41. Furthermore, cost questionnaires are susceptible to recall bias, however we tried to reduce recall bias by selecting a recall time frame of at most 13 weeks40,41. Second, we restricted the costs to GOA-related direct medical costs and non-medical costs. Although we asked participants about their GOA-related healthcare use, we are aware that the reported healthcare use cannot be exclusively attributed to GOA. No data were available on the utilization of informal care. Another limitation of the current study is the relatively small sample size. The clinical trial was powered based on the primary clinical outcome measure. Yet, the utility measures we used in the economic evaluation are known to be less responsive to measure changes in health status. As a consequence, it is possible that our economic evaluation was underpowered, a common limitation of economic evaluations conducted alongside clinical trials42. Finally, the generalizability of the study findings is restricted to Dutch patients clinically diagnosed with GOA who were referred for multidisciplinary treatment in a specialized outpatient rheumatology department.
In conclusion, this economic evaluation showed from a societal perspective that a non-pharmacological, multidisciplinary face-to-face treatment program for patients clinically diagnosed with GOA was at least twice as likely cost-effective relative to a telephone-based treatment program.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
72 | Chapter 4
References
1. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet 2011; 377: 2115-26
2. Elske van den Akker-van Marle, Chorus AM, Vliet Vlieland TP, van den Hout WB. Cost of rheumatic disorders in the Netherlands. Best.Pract.Res.Clin.Rheumatol. 2012; 26: 721-31
3. March LM, Bachmeier CJ. Economics of osteoarthritis: a global perspective. Baillieres Clin.Rheumatol. 1997; 11: 817-34
4. Puig-Junoy J, Ruiz Zamora BEcon A. Socio-economic costs of osteoarthritis: A systematic review of cost-of-illness studies. Seminars in Arthritis and Rheumatism. 2015; 44: 531-541
5. Hiligsmann M, Cooper C, Arden N, Boers M, Branco JC, Luisa BM et al. Health economics in the field of osteoarthritis: an expert’s consensus paper from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin.Arthritis Rheum. 2013; 43: 303-13
6. van den Hout WB, Bremander A, Vliet Vlieland TP. Recommendations for economic evaluations of non-pharmacological arthritis care: results from the CARE VI meeting 2010. Musculoskeletal.Care 2011; 9: 120-3
7. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann.Rheum.Dis. 2013; 72: 1125-35
8. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis.Cartilage. 2014; 22: 363-88
9. Fransen M, McConnell S, Harmer AR, van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee. Cochrane.Database.Syst.Rev. 2015; 1: CD004376
10. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
11. Pinto D, Robertson MC, Hansen P, Abbott JH. Cost-Effectiveness of Nonpharmacologic, Nonsurgical interventions for Hip and/or Knee Osteoarthritis: Systematic Review. Value Health 2012; 15: 1-12
12. Nelson AE, Smith MW, Golightly YM, Jordan JM. “Generalized osteoarthritis”: A systematic review. Semin.Arthritis Rheum. 2014; 43: 713-20
13. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011; 78: 275-8
14. Hoogeboom TJ, Stukstette MJ, de Bie RA, Cornelissen J, den Broeder AA, van den Ende CH. Non-pharmacological care for patients with generalized osteoarthritis: design of a randomized clinical trial. BMC.Musculoskelet.Disord. 2010; 11: 142
15. Hakkaart-van Roijen L, Tan S, Bouwmans C. Manual for Costing: Methods and Standard Costs for Economic Evaluations in Healthcare [Dutch]. Institute for Medical Technology Assessment, Erasmus University Rotterdam.Health Care Insurance Board, 2010
16. Boers M, Jacobs JW, Vliet Vlieland TP, van Riel PL. Consensus Dutch health assessment questionnaire. Ann.Rheum.Dis. 2007; 66: 132-3
17. EuroQol--a new facility for the measurement of health-related quality of life. The EuroQol Group. Health Policy 1990; 16: 199-208
18. Harrison MJ, Davies LM, Bansback NJ, Ingram M, Anis AH, Symmons DP. The validity and responsiveness of generic utility measures in rheumatoid arthritis: a review. J.Rheumatol. 2008; 35: 592-602
19. Stiggelbout AM, Eijkemans MJ, Kiebert GM, Kievit J, Leer JW, De Haes HJ. The ‘utility’ of the visual analog scale in medical decision making and technology assessment. Is it an alternative to the time trade-off? Int J.Technol.Assess.Health Care 1996; 12: 291-8
20. Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J.Health Econ. 2002; 21: 271-92
21. Gaujoux-Viala C, Rat AC, Guillemin F, Flipo RM, Fardellone P, Bourgeois P et al.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Economic evaluation of two non-pharmacological treatment programs for GOA | 73
4
Responsiveness of EQ-5D and SF-6D in patients with early arthritis: results from the ESPOIR cohort. Ann.Rheum.Dis. 2012; 71: 1478-83
22. Harrison MJ, Bansback NJ, Marra CA, Drummond M, Tugwell PS, Boonen A. Valuing health for clinical and economic decisions: directions relevant for rheumatologists. J.Rheumatol 2011; 38: 1770-5
23. van den Brink M, van den Hout WB, Stiggelbout AM, Putter H, van de Velde CJ, Kievit J. Self-reports of health-care utilization: diary or questionnaire? Int J.Technol.Assess.Health Care 2005; 21: 298-304
24. van den Hout WB, Tijhuis GJ, Hazes JM, Breedveld FC, Vliet Vlieland TP. Cost effectiveness and cost utility analysis of multidisciplinary care in patients with rheumatoid arthritis: a randomised comparison of clinical nurse specialist care, inpatient team care, and day patient team care. Ann.Rheum.Dis. 2003; 62: 308-15
25. Koopmanschap MA, Rutten FF, van Ineveld BM, van RL. The friction cost method for measuring indirect costs of disease. J.Health Econ. 1995; 14: 171-89
26. van den Hout WB. The value of productivity: human-capital versus friction-cost method. Ann.Rheum.Dis. 2010; 69 Suppl 1: i89-i91
27. Royston P. Multiple imputation of missing values: Update of ice. Stata Journal 2005; 5: 527-36
28. Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 2009; 338: b2393
29. Gupta SK. Intention-to-treat concept: A review. Perspect.Clin.Res. 2011; 2: 109-12
30. O’Brien BJ, Briggs AH. Analysis of uncertainty in health care cost-effectiveness studies: an introduction to statistical issues and methods. Stat.Methods Med.Res. 2002; 11: 455-68
31. Fenwick E, Byford S. A guide to cost-effectiveness acceptability curves. Br.J.Psychiatry 2005; 187: 106-8
32. Fenwick E, Marshall DA, Levy AR, Nichol G. Using and interpreting cost-effectiveness acceptability curves: an example using data from a trial of management strategies for atrial fibrillation. BMC.Health Serv.Res. 2006; 6: 52
33. Smink AJ, Dekker J, Vliet Vlieland TP, Swierstra BA, Kortland JH, Bijlsma JW et al. Health care use of patients with osteoarthritis of the hip or knee after implementation of a stepped-care strategy: an observational study. Arthritis Care Res.(Hoboken.) 2014; 66: 817-27
34. Christensen R, Bartels EM, Astrup A, Bliddal H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann.Rheum.Dis. 2007; 66: 433-9
35. Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes.Rev. 2014; 15: 578-86
36. Maly MR, Robbins SM. Osteoarthritis Year in Review 2014: rehabilitation and outcomes. Osteoarthritis.Cartilage. 2014; 22: 1958-88
37. Oppong R, Jowett S, Nicholls E, Whitehurst DG, Hill S, Hammond A et al. Joint protection and hand exercises for hand osteoarthritis: an economic evaluation comparing methods for the analysis of factorial trials. Rheumatology.(Oxford) 2015; 54: 876-83
38. Pisters MF, Veenhof C, Schellevis FG, de Bakker DH, Dekker J. Long-term effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a randomized controlled trial comparing two different physical therapy interventions. Osteoarthritis.Cartilage. 2010; 18: 1019-26
39. Svege I, Nordsletten L, Fernandes L, Risberg MA. Exercise therapy may postpone total hip replacement surgery in patients with hip osteoarthritis: a long-term follow-up of a randomised trial. Ann.Rheum.Dis. 2015; 74: 164-9
40. Bhandari A, Wagner T. Self-reported utilization of health care services: improving measurement and accuracy. Med.Care Res.Rev. 2006; 63: 217-35
41. Cronan TA, Walen HR. Accuracy of self-reported healthcare use in patients with osteoarthritis. J.Rheumatol 2002; 29: 2181-4
42. Ramsey S, Willke R, Briggs A, Brown R, Buxton M, Chawla A et al. Good research practices for cost-effectiveness analysis alongside clinical trials: the ISPOR RCT-CEA Task Force report. Value Health 2005; 8: 521-33


CHAPTER 5
Measurement properties of the Health
Assessment Questionnaire Disability Index
for generalized osteoarthritis
Nienke Cuperus, Elien A.M. Mahler, Thea P.M. Vliet Vlieland, Thomas J. Hoogeboom, Cornelia H.M. van den Ende
Published in: Rheumatology (Oxford). 2015; 54(5): 821-826

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
76 | Chapter 5
Abstract
ObjectiveGeneralized osteoarthritis (GOA) is highly prevalent in OA. Individuals with GOA typically suffer from limitations of both upper and lower extremity function, yet we lack a validated instrument to assess their activity limitations. An appropriate instrument might be the Health Assessment Questionnaire Disability Index (HAQ-DI). Therefore, the aim of this study was to evaluate the measurement properties of the HAQ-DI in GOA.
MethodsData were used from a randomized controlled trial comparing the effectiveness of two multidisciplinary treatment programs for patients with GOA. One hundred and thirty-seven of 147 included patients completed a standardized set of questionnaires before and after treatment. Interpretability, validity, reliability and responsiveness of the HAQ-DI were assessed using the Consensus Based Standards for the Selection of health Status Measurement Instruments Checklist (COSMIN).
ResultsFloor and ceiling effects were present. The content validity was questionable since the HAQ-DI encompasses activities that are either not relevant or too easy to perform as judged by patients and experts. Construct validity was good since 90% of the hypotheses were confirmed. Factor analysis confirmed the unidimensionality of the HAQ-DI (root mean square error of approximation = 0.057, χ2/df ratio = 1.48). Cronbach’s alpha was 0.90, confirming internal consistency and the ICC was 0.81, reflecting good reliability. The minimal important change was 0.25 and the smallest detectable change was 0.60. We could not establish the responsiveness of the HAQ-DI.
ConclusionsThe HAQ-DI showed good construct validity, internal consistency and reliability, whereas its content validity and responsiveness were limited. We recommend updating the items of the HAQ-DI in future research focusing on functional limitations in GOA.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Measurement properties of the HAQ-DI in GOA | 77
5
Introduction
Patient-reported assessments of functional limitations have emerged as an integral part of clinical practice and research in osteoarthritis (OA). Numerous self-administered instruments (such as the Western Ontario and McMaster Universities Arthritis Index (WOMAC)) are available to assess activity limitations in OA1. However, many of these questionnaires focus on a specific localization of OA (e.g. hands, hips or knees), limiting their use in the assessment of patients with generalized osteoarthritis (GOA). Individuals with GOA typically suffer from OA in multiple joints2 resulting in limitations of both upper and lower extremity function. To comprehensively assess activity limitations in people with GOA, instruments should contain items of both upper and lower extremity function. A growing body of evidence suggests that GOA is highly prevalent in patients with OA3,4, yet we lack a validated instrument to assess their activity limitations.
An appropriate instrument to measure activity limitations in patients with GOA might be the Stanford Health Assessment Questionnaire Disability Index (HAQ-DI), as it comprises activities of fine movement of the upper extremities, locomotor activities of the lower extremities, and activities that involve both upper and lower extremities5. Since the HAQ-DI has been designed for individuals with rheumatoid arthritis (RA), it comprises activities frequently impaired in RA patients. The HAQ-DI could be a useful instrument to assess and monitor functional limitations in patients with GOA as well as the two conditions have many similarities. In both RA and GOA, pain and stiffness are major symptoms and multiple joints, involving the upper and lower extremities, are affected. However, there are also differences, such as the pattern of joint involvement. Functional disabilities might therefore differ between the two conditions. Therefore an assessment of the measurement properties of the HAQ-DI in patients with GOA seems warranted. The aim of this study was to evaluate the measurement properties (i.e. interpretability, validity, reliability and responsiveness) of the HAQ-DI in patients with GOA. Methods
Study design and participantsThe current study was part of a randomized controlled trial comparing the effectiveness of two non-pharmacological multidisciplinary treatment programs for patients with GOA. The Institutional Review Board of the Radboud University Nijmegen Medical Centre approved the study and patients signed informed consent. The complete study design has been described previously (Dutch Trial Register NTR2137)2.
Patients clinically diagnosed with GOA were included when they had at least two objective signs indicating OA in two or more joint areas (malalignment, crepitation, limited range of

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
78 | Chapter 5
motion, palpable osteophytes or nodules or radiographic signs including the presence of joint space narrowing and/or osteophytes); complaints in three or more out of eight joint areas; and were limited in daily activities (HAQ-DI score ≥ 0.5). Patients diagnosed with another rheumatic disease were excluded2.
Data collection and procedureParticipants completed a standardized set of questionnaires prior to the start of the treatment (baseline) and at 6, 26, and 52 weeks. Data from baseline and the six week follow-up were used. Patients were included if they completed the baseline measurement. The recommendations of the Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN)6 and the quality criteria for measurement properties proposed by Terwee et al.7 were followed to assess the measurement properties of the HAQ-DI.
Outcome measuresParticipants completed the Dutch consensus HAQ-DI8 determining difficulties with the performance of 20 daily activities scored from 0 (without difficulty) to 3 (unable to do) and classified into 8 categories: dressing and grooming, arising, eating, walking, personal hygiene, reaching, gripping and usual activities5. The total HAQ-DI score represents a disability index ranging from 0 (no disability) to 3 (very severe disability). We did not correct HAQ-DI scores for using assistive devices, preventing an overestimation of the patients’ functional disability.
In addition, we measured quality of life (36-item Short Form Health Survey (SF-36) and the EuroQol five-dimension questionnaire (EQ-5D)), fatigue (Checklist of Individual Strength (CIS)), self-efficacy (General Self-efficacy scale (GSES)) and illness cognitions (Illness Cognition Questionnaire (ICQ)). Patient-specific complaints (Patient Specific Complaints questionnaire (PSK)) was measured by asking patients to select the three most important GOA-related activity limitations and to score their severity on a 0-10 scale. In the follow-up questionnaire, a seven-point Likert transition question was used to measure changes in daily function ranging from completely recovered to vastly worsened9.
InterpretabilityThe scale and category scores of the HAQ-DI were assessed for normality and missing data. We assessed floor and ceiling effects at baseline for each HAQ-DI category, which were considered present if > 15% of patients scored the worst (3) or best (0) possible score. We determined the minimal important change (MIC) score using an anchor-based method10.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Measurement properties of the HAQ-DI in GOA | 79
5
Content validityWe assessed whether the HAQ-DI items adequately represent daily function from both the patient’s and health professional’s perspective. We compared the International Classification of Functioning, Disability and Health (ICF) codes of all HAQ-DI items presented in a study of Stamm et al.11 with the ICF codes of an aggregated list (unpublished observations) representing the 10 most important activity limitations reported by patients with GOA. Content validity was arbitrarily considered good when all 10 activity limitations were covered by the HAQ-DI. Second, we asked 17 health professionals experienced with GOA to estimate the relevance of each HAQ-DI item, expressed as the percentage of GOA patients having actual difficulty performing that item. Items were considered not relevant when health professionals expected items were difficult to perform for ≤ 50% of patients.
Construct validity and responsivenessWe assessed construct validity by testing predefined hypotheses about expected correlations between HAQ-DI scores and scores on related measures (convergent), unrelated measures (discriminant) or differences between groups (discriminative)7. Since we consider responsiveness as a measure of longitudinal validity, we assessed responsiveness in analogy with construct validity by testing pre-defined hypotheses using change scores7. In this way, responsiveness is independent of the magnitude of a change but measures the quality of the measurement instrument. In addition, for our responsiveness analysis we formulated two hypotheses on the size of the area under the receiver operating characteristic (ROC) curve (AUC)7. An expert group of researchers, health professionals and a rheumatologist independently formulated hypotheses that were discussed during a consensus meeting. Construct validity and responsiveness were considered positive if > 75% of the hypotheses were confirmed7.
Internal consistency and reliabilityConfirmatory factor analysis (CFA) was performed using the following thresholds for a good model fit: Root Mean Square Error of Approximation (RMSEA) ≤ 0.06, Comparative Fit Index (CFI) ≥ 0.95 and χ2/df ratio ≤ 312. Internal consistency was considered adequate if Cronbach’s alpha > 0.7. Test-retest reliability was acceptable when the intra-class correlation coefficient (ICC(2,1)) ≥ 0.70 in stable patients (i.e. patients reported no change on the transition question). We determined the limits of agreement as a parameter of agreement13 and we quantified the smallest detectable change (SDC = SEM*1.96*√2)7.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
80 | Chapter 5
Statistical analysisPearson or Spearman Rank correlation coefficients (when appropriate) were computed to test the hypotheses. The CFA was conducted using LISREL software (Scientific Software International, Skokie, IL, USA). All other analyses were performed using STATA 10.1 (StataCorp, College Station, TX, USA).
Results
Patient characteristicsA total of 147 patients completed the baseline measurement (93%) of whom 137 completed the follow-up measurement (93%). The majority of patients remained stable in their daily function after 6 weeks (Table 1).
Table 1. Socio demographic and disease related characteristics of 147 individuals with GOA
Patient and disease-related characteristicsFemale, n (%) 125 (85)Age, mean (SD), years 60 ± 8BMI, mean (SD), kg/m2 28 ± 4.5Education > 12 years, n (%) 43 (29)Marital status, married, n (%) 113 (77)Currently employed, n (%) 55 (37)Duration of complaints ≥ 5 years, n (%) 110 (75)Joint areas with symptomatic OA; median (IQR) 5 (4-6)Localization of symptoms, n (%):
Upper extremities (neck, shoulder, elbow, hand) 138 (94)Lower extremities (lumbar spine, hip, knee, foot) 145 (99)Combination of upper and lower extremities 136 (93)
Changes in daily function rated on the transition question, n (%):Completely recovered 1 (1)Much improvement 7 (5)Some improvement 57 (42)No change 62 (45)Some deterioration 8 (6)Much deterioration 2 (1)
Abbreviations: SD = Standard Deviation; IQR = Interquartile Range

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Measurement properties of the HAQ-DI in GOA | 81
5
InterpretabilityThe item “getting in or out of bath” was returned with > 10% missing values. HAQ-DI scores were normally distributed with a mean (SD) score of 1.27 (0.50) at baseline and 1.20 (0.47) at follow-up. Ceiling effects were present in the categories eating, dressing and gripping, and a floor effect was present in the category hygiene. The MIC for improvement was 0.25 points.
Content validity Seven of 10 ICF codes representing the most relevant activity limitations for patients with GOA were covered by the HAQ-DI items. Activities that were not covered were maintaining a body position (d415), recreation and leisure (d920) and driving (d475). Health professionals considered nine items of the HAQ-DI relevant for ≤ 50% of GOA patients, whereas 11 items were considered relevant for >50% of patients. The least relevant items were: lifting a cup to your mouth, shampoo your hair, wash your body and opening car doors. The most relevant items were: getting down a 5 pound object from above your head, opening a new milk carton and doing chores.
Construct validity and responsivenessThe HAQ-DI showed good construct validity since 9 out of 10 hypotheses (90%) were confirmed (Table 2). We were not able to confirm the hypothesized strong correlation between HAQ-DI scores and the EQ-5D item usual activities since we found a correlation of 0.23. Four out of 10 hypotheses (40%) to assess the responsiveness of the HAQ-DI were confirmed (Table 3). The correlation between change in HAQ-DI scores and change in SF-36 physical function scores was weak (-0.20), whereas we hypothesized a moderate correlation because of the associated constructs. We could not confirm the hypotheses on the AUC.
Internal consistency and reliabilityThe initial CFA (with uncorrelated measurement errors between categories) did not meet adequate fit criteria. Modification indices provided by LISREL suggested a correlated error term between eating and gripping. The modified model resulted in a good fit to the data: RMSEA = 0.057, CFI = 0.98 and χ2/df ratio = 1.48. Cronbach’s alpha was 0.90 (lower limit 95% CI: 0.88) confirming internal consistency. The ICC(2,1) was 0.81 (95% CI: 0.71, 0.88) reflecting good reliability. The Bland-Altman plot showed a mean difference of 0.05 (95% CI: -0.03, 0.13) between baseline and follow-up and the limits of agreement ranged from -0.54 to 0.65 points. The SDC was 0.60 points.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
82 | Chapter 5
Tabl
e 2.
Res
ults
of p
rede
fined
hyp
othe
ses
to a
sses
s th
e co
nstr
uct v
alid
ity o
f the
HAQ
-DI i
n pa
tient
s w
ith G
OA
Hyp
othe
sis
cons
truc
t val
idit
yRe
sult
saCo
nfirm
ed1.
Th
ere
is a
stro
ng c
orre
latio
n (r
> - 0
.5) b
etw
een
HAQ
-DI a
nd S
F-36
phy
sical
func
tion
-0.6
8 (-0
.76 -
-0.5
8)Ye
s2.
The
corr
elati
on b
etw
een
HAQ
-DI a
nd S
F-36
phy
sical
fun
ction
is s
tron
ger
than
the
cor
rela
tion
betw
een
HAQ
-DI a
nd S
F-36
pai
n-0
.68
(-0.7
6 - -0
.58)
vs.
-0.5
6 (-0
.67 -
-0.4
4)b
Yes
3.Th
ere
is a
stro
ng c
orre
latio
n (r
> 0
.5) b
etw
een
HAQ
-DI a
nd th
e EQ
-5D
item
usu
al a
ctivi
ties
0.23
(0.0
7 –
0.37
)N
o4.
Ther
e is
a m
oder
ate
corr
elati
on (0
.3 <
r <
0.5)
bet
wee
n H
AQ-D
I and
PSK
0.
34 (0
.19
– 0.
48)
Yes
5.Th
ere
is a
wea
k co
rrel
ation
(r <
-0.3
) bet
wee
n H
AQ-D
I and
SF-
36 m
enta
l fun
ction
-0
.11
(-0.2
7 –
0.05
)Ye
s6.
Ther
e is
a w
eak
corr
elati
on (r
< 0
.3) b
etw
een
HAQ
-DI a
nd fa
tigue
0.27
(0.1
1 –
0.41
)Ye
s7.
Ther
e is
a w
eak
corr
elati
on (r
< -/
+ 0.
3) b
etw
een
HAQ
-DI a
nd s
ocio
dem
ogra
phic
cha
ract
eristi
cs
-0.2
7 (-0
.41 -
-0.1
1)c
Yes
8.Th
ere
is a
wea
k co
rrel
ation
(r <
-0.3
) bet
wee
n H
AQ-D
I and
sel
f-effi
cacy
-0.0
5 (-0
.21
– 0.
12)
Yes
9.Th
ere
is a
wea
k co
rrel
ation
(r <
-0.3
) bet
wee
n H
AQ-D
I and
illn
ess
cogn
ition
s su
bsca
le a
ccep
tanc
e -0
.18
(-0.3
3 - -0
.01)
Yes
10.
Patie
nts w
ith m
uscu
losk
elet
al c
ompl
aint
s in
mor
e th
an fi
ve jo
int a
reas
hav
e hi
gher
HAQ
-DI s
core
s th
an p
atien
ts w
ith m
uscu
losk
elet
al c
ompl
aint
s th
ree
to fi
ve jo
int a
reas
0.38
(0.2
2 - 0
.54)
dYe
s
Confi
rmed
, n/n
(%)
9/10
(90%
)
a Va
lues
are
cor
rela
tions
(95%
CI)
unle
ss in
dica
ted
othe
rwise
b Si
gnifi
cant
ly h
ighe
r cor
rela
tion,
p <
0.0
5c So
cio
dem
ogra
phic
cha
ract
eristi
cs in
clud
ed B
ody
Mas
s In
dex,
age
, edu
catio
n le
vel,
wor
k an
d fa
mily
sta
tus.
The
str
onge
st c
orre
latio
n is
depi
cted
i.e.
ed
ucati
on le
vel
d M
ean
diffe
renc
e in
sco
res
(95%
CI),
p <
0.0
1Ab
brev
iatio
ns: H
AQ-D
I = H
ealth
Ass
essm
ent Q
uesti
onna
ire D
isabi
lity
Inde
x; S
F-36
= S
hort
For
m 3
6 H
ealth
Sur
vey;
PSK
= P
atien
t Spe
cific
Com
plai
nts

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Measurement properties of the HAQ-DI in GOA | 83
5
Tabl
e 3.
Res
ults
of p
rede
fined
hyp
othe
ses
to a
sses
s lo
ngitu
dina
l val
idity
(res
pons
iven
ess)
of t
he H
AQ-D
I in
patie
nts
with
GO
A
Hyp
othe
sis
long
itud
inal
val
idit
y (r
espo
nsiv
enes
s)Re
sult
saCo
nfirm
ed1.
Th
e H
AQ-D
I ca
n di
sting
uish
pati
ents
who
rep
orte
d m
ajor
im
prov
emen
ts (
muc
h im
prov
ed,
com
plet
ely
reco
vere
d) f
rom
tho
se w
ho r
epor
ted
no im
port
ant
chan
ges
(slig
htly
impr
oved
, no
chan
ge, s
light
ly w
orse
) bas
ed o
n th
e tr
ansiti
on q
uesti
on (A
UC
> 0.7
)
AUC
= 0.
69N
o
2.Th
e H
AQ-D
I can
disti
ngui
sh p
atien
ts w
ho w
ere
impr
oved
(sli
ghtly
impr
oved
, muc
h im
prov
ed,
com
plet
ely
reco
vere
d) f
rom
tho
se w
ho w
ere
unch
ange
d (n
o ch
ange
) ba
sed
on t
he t
rans
ition
qu
estio
n (A
UC
> 0.7
)
AUC
= 0.
53N
o
3.Th
ere
is a
mod
erat
e co
rrel
ation
(0.3
< r
< 0.
5) b
etw
een
Δ H
AQ-D
I and
the
tran
sition
que
stion
0.14
(-0.
03 - 0
.30)
No
4.Th
ere
is a
mod
erat
e co
rrel
ation
(-0.
3 <
r < -0
.5) b
etw
een
Δ H
AQ-D
I and
Δ S
F-36
phy
sical
func
tion
-0.2
0 (0
.36 -
-0.0
3)N
o5.
The
corr
elati
on b
etw
een
Δ H
AQ-D
I and
Δ S
F-36
phy
sical
func
tion
is st
rong
er th
an th
e co
rrel
ation
be
twee
n Δ
HAQ
-DI a
nd Δ
SF-
36 p
ain
-0.2
0 (0
.36 -
-0.0
3) v
s.
-0.2
1 (-0
.6 - -
0.04
)bN
o
6.Th
ere
is a
wea
k co
rrel
ation
(r <
-0.3
) bet
wee
n Δ
HAQ
-DI a
nd Δ
SF-
36 m
enta
l fun
ction
-0.0
5 (-0
.22 -
-0.1
2)Ye
s7.
Ther
e is
a w
eak
corr
elati
on (r
< 0
.3) b
etw
een
Δ H
AQ-D
I and
Δ fa
tigue
0.
09 (-
0.08
– 0
.26)
Yes
8.Th
ere
is a
wea
k co
rrel
ation
(r <
-0.3
) bet
wee
n Δ
HAQ
-DI a
nd Δ
sel
f-effi
cacy
-0.1
3 (-0
.30
– 0.
04)
Yes
9.Th
ere
is a
wea
k co
rrel
ation
(r
< -0
.3)
betw
een
Δ H
AQ-D
I an
d Δ
illne
ss c
ogni
tions
sub
scal
e ac
cept
ance
-0
.14
(-0.3
0 –
0.03
)Ye
s
10.
The
effec
t size
of t
he H
AQ-D
I in
the
grou
p of
pati
ents
with
maj
or im
prov
emen
ts is
> 0
.80.
49c
No
Confi
rmed
, n/n
(%)
4/10
(40%
)
a Va
lues
are
cor
rela
tions
(95%
CI)
unle
ss in
dica
ted
othe
rwise
b Di
ffere
nce
betw
een
corr
elati
on is
not
sig
nific
ant,
p >
0.05
c Eff
ect s
ize =
mea
n ch
ange
in H
AQ-D
I / S
D m
ean
base
line
HAQ
-DI
Abbr
evia
tions
: HAQ
-DI =
Hea
lth A
sses
smen
t Que
stion
naire
Disa
bilit
y In
dex;
SF-
36 =
Sho
rt F
orm
36
Hea
lth S
urve
y; A
UC
= Ar
ea U
nder
rece
iver
ope
rato
r ch
arac
teris
tic C
urve

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
84 | Chapter 5
Discussion
This is the first study to comprehensively assess the measurement properties of the HAQ-DI in patients clinically diagnosed with GOA. The results showed a questionable content validity. The construct validity, internal consistency and reliability were confirmed; however, the responsiveness was limited.
Based on the results, we need to question the content validity of the HAQ-DI. Important activities frequently impaired in patients with GOA were not assessed by the HAQ-DI. Moreover, the ceiling effects suggest that the HAQ-DI measures activities that are either not relevant or too easy to perform for patients with GOA, a finding supported in RA. In particular, these activities are lifting a cup to your mouth, shampoo your hair and opening car doors which were also rated by the health professionals as least relevant. The activity getting in or out of bath also seems less relevant given the high number of missing values, a result supported in RA14. An explanation for our findings might be that certain activities of the HAQ-DI are “outdated” since the questionnaire was developed three decades ago5, a period during which some activities have become easier to perform due to technological and social developments.
We were not able to confirm the responsiveness of the HAQ-DI. This might be explained by the reported floor and ceiling effects in four of eight HAQ-DI categories, a finding supported by other studies15. Several studies examining the responsiveness of the HAQ-DI in rheumatic diseases showed conflicting results and/or used different approaches14-16. There is no consensus on which method is best to assess responsiveness; however, it has been recommended that anchor-based methods should be used, as traditionally accepted methods (e.g. effect size) measure the magnitude of change rather than longitudinal validity17. An important limitation in our responsiveness analysis is the very small number of patients with major improvements, which prevents firm conclusions. In addition, there is debate regarding the use of transition questions since they are biased by patients’ current status, particularly as the time span increases18. To limit recall bias, we decided to use only the six week follow-up measurement.
The MIC of 0.25 in this study is comparable to that of patients with RA19. The SDC was 0.60, indicating that important changes cannot be distinguished from measurement error in individuals. The HAQ-DI is therefore not suitable to monitor individual GOA patients in daily clinical practice.
Some limitations need to be addressed. One could question the extent to which our study population adequately represents GOA patients. We used a pragmatic GOA definition, as there is no widely accepted definition20. Moreover, we did not assess the WOMAC. We considered the face validity of the WOMAC inadequate as it only contains items on lower extremity function. However, in future research it would be worthwhile comparing the

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Measurement properties of the HAQ-DI in GOA | 85
5
measurement properties of existing physical function measures in GOA, such as the WOMAC or the SF-36, before making a start with developing new measurement instruments assessing functional limitations in patients with GOA.
In conclusion, the HAQ-DI showed good construct validity and reliability. Given the unsatisfactory content validity, we recommend an update of the items of the HAQ-DI when using the HAQ-DI in future clinical practice and research focusing on functional limitations in GOA. This update might also be worthwhile for RA and all other rheumatic diseases.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
86 | Chapter 5
References
1. Bellamy N, Kirwan J, Boers M, Brooks P, Strand V, Tugwell P et al. Recommendations for a core set of outcome measures for future phase III clinical trials in knee, hip, and hand osteoarthritis. Consensus development at OMERACT III. J.Rheumatol. 1997; 24: 799-802
2. Hoogeboom TJ, Stukstette MJ, de Bie RA, Cornelissen J, den Broeder AA, van den Ende CH. Non-pharmacological care for patients with generalized osteoarthritis: design of a randomized clinical trial. BMC.Musculoskelet.Disord. 2010; 11: 142
3. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011; 78: 275-8
4. Gunther KP, Sturmer T, Sauerland S, Zeissig I, Sun Y, Kessler S et al. Prevalence of generalised osteoarthritis in patients with advanced hip and knee osteoarthritis: the Ulm Osteoarthritis Study. Ann.Rheum.Dis. 1998; 57: 717-23
5. Bruce B, Fries JF. The Stanford Health Assessment Questionnaire: dimensions and practical applications. Health Qual.Life Outcomes. 2003; 1: 20
6. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual.Life Res. 2010; 19: 539-49
7. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J et al. Quality criteria were proposed for measurement properties of health status questionnaires. J.Clin.Epidemiol. 2007; 60: 34-42
8. Boers M, Jacobs JW, Vliet Vlieland TP, van Riel PL. Consensus Dutch health assessment questionnaire. Ann.Rheum.Dis. 2007; 66: 132-3
9. Lauridsen HH, Hartvigsen J, Korsholm L, Grunnet-Nilsson N, Manniche C. Choice of external criteria in back pain research: Does it matter? Recommendations based on analysis of responsiveness. Pain 2007; 131: 112-20
10. de Vet HC, Terluin B, Knol DL, Roorda LD, Mokkink LB, Ostelo RW et al. Three ways to quantify uncertainty in individually applied “minimally important change” values. J.Clin.Epidemiol. 2010; 63: 37-45
11. Stamm T, Geyh S, Cieza A, Machold K, Kollerits B, Kloppenburg M et al. Measuring functioning in patients with hand osteoarthritis--content comparison of questionnaires based on the International Classification of Functioning, Disability and Health (ICF). Rheumatology.(Oxford) 2006; 45: 1534-41
12. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equation Model 1999; 6: 1-55
13. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307-10
14. Linde L, Sorensen J, Ostergaard M, Horslev-Petersen K, Hetland ML. Health-related quality of life: validity, reliability, and responsiveness of SF-36, 15D, EQ-5D [corrected] RAQoL, and HAQ in patients with rheumatoid arthritis. J.Rheumatol. 2008; 35: 1528-37
15. Oude Voshaar MA, ten Klooster PM, Taal E, van de Laar MA. Measurement properties of physical function scales validated for use in patients with rheumatoid arthritis: a systematic review of the literature. Health Qual.Life Outcomes. 2011; 9: 99
16. Veehof MM, ten Klooster PM, Taal E, van Riel PL, van de Laar MA. Comparison of internal and external responsiveness of the generic Medical Outcome Study Short Form-36 (SF-36) with disease-specific measures in rheumatoid arthritis. J.Rheumatol. 2008; 35: 610-7
17. Mokkink LB, Terwee CB, Knol DL, Stratford PW, Alonso J, Patrick DL et al. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC.Med.Res.Methodol. 2010; 10: 22
18. Kamper SJ, Ostelo RW, Knol DL, Maher CG, de Vet HC, Hancock MJ. Global Perceived Effect scales provided reliable assessments

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Measurement properties of the HAQ-DI in GOA | 87
5
of health transition in people with musculoskeletal disorders, but ratings are strongly influenced by current status. J.Clin.Epidemiol. 2010; 63: 760-6
19. Kosinski M, Zhao SZ, Dedhiya S, Osterhaus JT, Ware JE, Jr. Determining minimally important changes in generic and disease-specific
health-related quality of life questionnaires in clinical trials of rheumatoid arthritis. Arthritis Rheum. 2000; 43: 1478-87
20. Nelson AE, Smith MW, Golightly YM, Jordan JM. “Generalized osteoarthritis”: A systematic review. Semin.Arthritis Rheum. 2014; 43: 713-20


CHAPTER 6
Assessment and comparison of responsiveness of
four patient reported outcome measures to assess
physical function in patients with knee osteoarthritis:
WOMAC-PF subscale responds best
Elien A.M. Mahler, Nienke Cuperus, Johannes J.W. Bijlsma, Thea P.M. Vliet Vlieland, Frank H.J. van den Hoogen, Alfons A. den Broeder, Cornelia H.M. van den Ende
Submitted

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
90 | Chapter 6
Abstract
ObjectiveThe aim of this study was to evaluate the responsiveness of physical function of four disease-specific patient reported outcome measures (PROMs) in patients with knee osteoarthritis (OA) following currently recommended standards.
MethodsPatients with knee OA receiving conservative treatment following a stepped care approach at an outpatient clinic were invited to complete a set of questionnaires at baseline and three months. Questionnaires included four commonly used measures of physical function i.e. Knee Injury and Osteoarthritis Outcome Function Short Form (KOOS-PS), Lequesne Algofunctional index (LAI), Lower Extremity Functional Scale (LEFS) and Western Ontario and McMaster University Osteoarthritis Index Physical Function subscale (WOMAC-PF). Responsiveness of physical function was investigated according to the COSMIN standard by testing 15 a priori defined hypotheses and was considered positive if > 75% of the hypotheses could be confirmed.
ResultsOf the 161 included patients, 61% was female with a mean age of 59.0 years. We could confirm 12 out of 15 predefined hypotheses (80%) about expected correlations for the WOMAC-PF whereas for the KOOS-PS, LAI and LEFS, 11 (73%), 10 (67%) and 11 (73%) hypotheses could be confirmed.
ConclusionsThis is the first study that comprehensively evaluated and compared the responsiveness of physical function assessed with KOOS-PS, LAI, LEFS and WOMAC-PF according to the latest standards. Our results suggest that the WOMAC-PF is potentially better able to detect changes over time in physical function and therefore should be the measure of first choice in clinical trials evaluating the effectiveness of an intervention in knee OA patients.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 91
6
Introduction
Knee osteoarthritis (OA) is a common chronic and degenerative musculoskeletal disorder and a major cause of reduced physical function1-3. Physical function is therefore one of the core outcome dimensions in clinical practice and research in knee OA4. Since no curative treatment is currently available for knee OA2, treatment is usually aimed at improving symptoms (function, pain, stiffness) using a variety of pharmacological and non-pharmacological interventions including surgery5. The effectiveness of such interventions are frequently evaluated by clinicians in daily practice and researchers in clinical trials using core outcome measures that address the domains of pain and function as advocated6,7. Therefore the ability of a measurement instrument to detect changes over time (i.e. the responsiveness) regarding the construct being measured8-10, is of particular importance when selecting an instrument.
Several disease-specific patient reported outcome measures (PROMs) are available to evaluate physical function in patients with knee OA. Among those, the Lequesne Algofunctional index (LAI) and the physical function subscale of the Western Ontario and McMaster University Osteoarthritis Index (WOMAC-PF) are recommended as measures of first choice in OA trials11,12. Recently, two new disease specific measures have been developed to evaluate physical function in patients with knee OA: the short version of the Knee disability and Osteoarthritis Outcome Score (KOOS-PS)13 and the Lower Extremity Functional Scale (LEFS)14. So far, no studies have examined the responsiveness of these latter instruments and compared them head-to-head in a single study.
A large number of definitions and methods have been proposed for assessing responsiveness, but the most adequate method to evaluate responsiveness is still under debate in the literature15. There is growing consensus that responsiveness should be considered as a measure of longitudinal construct validity since responsiveness refers to measuring changes in the construct to be measured. In accordance, responsiveness should, analogue to construct validity, be evaluated by testing predefined hypotheses about expected correlations between changes in (un)related measurements or expected differences in changes10,12. With this approach, the validity of the change scores can be assessed in contrast to the magnitude of the change score as assessed with traditionally accepted methods such as effect sizes (ES) or standardized response mean (SRM)15. These latter methods are known to be related to the treatment effect, rather than the quality of a measurement instrument.
To our knowledge, no studies evaluated the responsiveness of PROMs assessing physical function by postulating a priori hypotheses using the Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN) methodology in patients with knee OA in a head to head comparison. In the current study we compared the responsiveness of physical function of the disease-specific PROMs KOOS-PS, LAI, LEFS and WOMAC-PF in patients with knee OA by testing predefined hypotheses about expected correlations between changes in measurements or expected differences in changes.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
92 | Chapter 6
Methods
Participants and interventionRecruitment to the study took place between July 2012 and January 2014. Consecutive patients referred by orthopedic surgeons to a specialized knee and hip OA rheumatology outpatient clinic were invited for this cohort study. All patients fulfilled the American College of Rheumatology clinical OA criteria16,17 and were invited the day after their first outpatient visit to our department. The main exclusion criterion was: short term indication (within 3 months) for knee replacement surgery. The local Medical Research Ethics Committee, region Arnhem-Nijmegen (The Netherlands) approved the study design (study number 2012/375). All patients signed informed consent.
Stepped care approachAll patients received multimodal conservative treatment based on a published Dutch multidisciplinary stepped care approach for diagnosis and treatment of knee and hip OA18. At the rheumatology outpatient department, during a 90 minute group visit (4-6 patients) led by a physician assistant and a specialized nurse and supervised by a rheumatologist (as described elsewhere19) patients received education, physical therapy (referral for both aerobic and strengthening exercises according to the graded activity principle), step up analgesics guided by a patient’s pain level (change of policy regarding pain medication was considered in case of pain > 4 on a numeric rating scale), life style advice concerning physical activity and advice on weight loss in patients with a BMI ≥ 28. In this group visit, most components of individual visits were retained such as private one-to-one conversations, while creating more time for patient education and discussion20. If prescription of analgesics was considered necessary, we started with paracetamol (acetaminophen) in a fixed dose of thrice a day 1000 mg. In case of lack of efficacy of recent consistent use of paracetamol, a non-steroidal anti-inflammatory drugs (NSAID) was added. After 4 weeks patients were contacted by telephone and if necessary the analgesics were switched.
Data acquisitionAt baseline and at three months, patients completed a standardized set of questionnaires including socio-demographic information (age, sex, duration of complaints, and localization of symptoms). The set of questionnaires included four disease-specific PROMs to measure physical function. Other outcome measures included in the set of questionnaires were derived from hypotheses that were a priori postulated by an expert group (see responsiveness). A reminder was sent to those patients who did not respond within three weeks. Patients were included in the analysis of the current study if they completed both the baseline and follow-up measurement.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 93
6
Patient Reported Outcome Measures (PROMs)
Knee injury and Osteoarthritis Outcome Physical Function Short Form (KOOS-PS)The 7-item short measure of physical function (KOOS-PS) is derived from the subscale “activities of daily living” (four items) and “sport and recreation” (three items) of the KOOS13. With every item, patients rate the degree of difficulty they have experienced over the previous week due to their knee pain on a 5-point Likert scale (0-4). Raw scores can range from 0-28 which were converted to normalized scores ranging from 0-100 with a score of 0 indicating no difficulty. The KOOS-PS has shown to be valid and reliable in knee OA13,21-23.
Lequesne Algofunctional index (LAI)The LAI is an 11-item questionnaire measuring the degree of functional disability24 with 4 questions pertaining to activities of daily living. The total score can range from 0-24 points. The degree of functional disability corresponds with the following scores: a score ≥ 14 points indicates extremely severe disability, a score of 11-13 indicates very severe disability, a score of 8-10 severe disability, a score of 5-7 indicates moderate disability and a score of 1-4 indicates minimal disability. The LAI has demonstrated good reliability, whereas its validity has been questioned25.
Lower Extremity Functional Scale (LEFS)The LEFS is a 20-item condition-specific questionnaire designed for use in patients with musculoskeletal conditions affecting lower extremity function, including knee OA26. The instrument asks patients about their ability to perform general activities of daily living, general recreational activities, specific daily physical tasks, and specific recreational or occupational related tasks on the day of filling in (0-4). The total score ranges from 0 to 80 points, with higher scores representing higher levels of functioning. The LEFS has been shown to be valid and reliable in patients with knee OA14,27.
Western Ontario and McMaster University Osteoarthritis Index Physical Function (WOMAC PF) The KOOS includes the WOMAC OA index in its complete and original format (with permission, (www.koos.nu). We used the 17-item subscale Activities of Daily Living (Likert scale version) from the KOOS to calculate the WOMAC physical function (WOMAC-PF) score (and thus four items are overlapping with the KOOS-PS). Standardized scores, ranging from 0-100 were used, where higher scores reflect better health status. The WOMAC has been the most extensively studied instrument in individuals with knee OA and has shown to be valid and reliable28.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
94 | Chapter 6
Patient’s assessment of changeIn the follow-up questionnaire, patients were asked to rate the extent to which their daily function and pain had been changed since the start of the treatment on a 7-point Likert scale, i.e. very much worsened, much worsened, slightly worsened, no change, slightly improved, much improved and very much improved.
Other patient related outcome measuresIn addition to the abovementioned PROMs, patients were asked to rate their functioning and pain in the preceding week on a 0-10 point Numeric Rating Scale (NRS) where 0 equals no symptoms. The patient global assessment (PGA) of knee OA impact during the last week before visit was assessed on this NRS scale as well. Moreover, physical function and mental health were measured with corresponding subscales of the Short Form 36 Health Survey (SF-36), a widely used generic health status questionnaire comprising eight areas of health status, with higher scores indicating better health (range 0-100)29,30. Fatigue was measured with the 8-itemed “Subjective Fatigue” subscale of the Checklist Individual Strength (CIS)31. The total score can range from 8-56 points where scores of ≥ 35 represent severe fatigue. Self-efficacy was assessed with the Dutch General Self Efficacy Scale (DGSS)32 and higher scores, ranging from 10 to 40, reflect higher self-efficacy. Pain coping was assessed with the Pain Coping Inventory List (PCI)33, which is a 33-item questionnaire and measures active and passive pain coping strategies on a 4-point Likert scale ranging from ‘hardly ever’ to ‘very often’. Higher scores on the subscales active or passive coping indicate more use of an active or passive coping style. The Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety and depression34-36. Both subscales consist of 7 items with possible scores ranging from 0 to 21 for each subscale. Higher scores indicate higher levels of disorder.
ResponsivenessThe Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN) and the quality criteria for measurement properties as proposed by Terwee et al. were followed for the assessment of responsiveness9,10. We defined responsiveness as the ability of an instrument to detect changes over time in the construct to be measured9,15. Since we considered responsiveness as a measure of longitudinal validity, the basic approach we used to assess responsiveness was to postulate and test predefined specific hypotheses formulated by an expert group in analogy to construct validity9. These a priori defined hypotheses addressed expected correlations between changes in scores on the KOOS-PS, LAI, LEFS and WOMAC-PF with changes in scores on other clinical (un)related measures (pain, mental health, fatigue, self-efficacy, coping, anxiety and depression) or expected differences in correlation in changes between groups. In this way, responsiveness is independent of the magnitude of a change but measures the quality of the measurement instrument. We

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 95
6
installed an expert group consisting of researchers, epidemiologists and physical therapists with published studies on OA and well versed with the current literature providing PROMs and a rheumatologist with clinical and research experience in the field of knee OA. Members of the expert group independently formulated hypotheses that were discussed in a group meeting until consensus was reached. In addition, we added one hypothesis on the size of the area under (AUC) the receiver operating characteristic (ROC) curve10, measuring the ability of a questionnaire to distinguish patients who have and have not changed, according to an external anchor. We calculated the ROC curve for the improved patients using the change in physical function scores of the PROMs and the patients’ rating of change in physical function assessed by the transition question. The rating of change was dichotomized to identify patients that were (very) much improved in physical function and remained stable (slightly improved, not changed, slightly worse). A correlation of -0.3 ≤ r ≤ 0.3 was considered weak, whereas a correlation of r > 0.3 or r < -0.3 was considered moderate. An AUC of at least 0.70 was considered adequate10. Responsiveness was considered positive if > 75% of the hypotheses were confirmed10.
Statistical analysisThe distributions of the study variables were inspected. Descriptive statistics were provided as mean and standard deviation (SD) or median and interquartile range (IQR) when appropriate for continuous variables and numbers with percentages for categorical variables. Descriptive statistics were used to describe the study population. Paired t-tests were used to compare baseline with three-month values. First, the scale scores of the KOOS-PS, LAI, LEFS and WOMAC-PF were assessed for normality and missing data. We assessed floor and ceiling effects for each questionnaire at baseline which were considered present if > 15% of the patients scored the worst or best possible score, respectively. Pearson or Spearman rank correlation coefficients when appropriate were computed to test the hypotheses. ROC curves were estimated for the change in KOOS-PS, LAI, LEFS and WOMAC-PF to distinguish between patients who indicated to be (very) much improved and who indicated to be stable in physical function after 3 months. All analyses were performed using STATA 13.1.
Results
Patient characteristicsIn total, we invited 272 patients to participate in the current study of whom 185 (68%) completed the baseline measurement. Of these patients, 161 (87%) completed the follow-up measurement and were included in the current analysis. No differences were found between the participants and non-participants with regard to sex, whereas the group of participants had a significantly higher age than the non-participants (59 years vs. 56 years, p = 0.02).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
96 | Chapter 6
The majority of the cohort consisted of women (61%), with a mean (SD) age of 59 (9.3) years and BMI of 29.7 kg/m2 (SD 5.0). The demographic and disease related characteristics at baseline are presented in Table 1. Scores of the KOOS-PS, LAI, LEFS and WOMAC-PF were normally distributed at both baseline and follow-up. At the scale level of the abovementioned instruments, there were ≤ 5% missing values at both time points. Ceiling or floor effects were not present regarding the measures of KOOS-PS, LAI, LEFS and WOMAC-PF.
Three month follow-upFor the whole group of patients, the majority of the PROMs remained stable after 3 months, but significant improvements were observed in physical function measured with the KOOS-PS (p=0.03) and for fatigue (assessed by the CIS, p=0.03). The majority of patients (n=129, 80.6%) indicated on the transition question that they had remained stable in their daily function after 3 months (Table 1). Fourteen (8.8%) patients indicated (very) much worsening in their physical function. The 17 patients (10.6%) who indicated (very) much improvement, showed significant improvements in physical function after 3 months in all four disease-specific PROMs compared with baseline (p<0.05) (Table 2) and in most of the other assessed PROMs (NRS function, NRS pain, NRS PGA, physical function SF-36, mental health SF-36, fatigue, passive coping and depression, data not shown). ResponsivenessTable 3 presents the correlation coefficients between changes in physical function in the four PROMs and changes in scores on related and unrelated constructs. We could confirm 12 out of 15 predefined hypotheses (80%) about expected (or absence of) correlations using the WOMAC-PF. The responsiveness of the WOMAC-PF could therefore be established as >75% of the hypotheses were confirmed (Table 4). For the KOOS-PS, LAI and LEFS, respectively 11 (73%), 10 (67%) and 11 (73%) hypotheses were confirmed and the 75% according to our definition of positive rating for responsiveness was not reached. For all four PROMs, we were unable to confirm the hypothesized weak correlation between change in physical function and change in NRS pain since we found a moderate correlation ranging between 0.33 and 0.49 (hypothesis 2). Concerning hypothesis 12, for three of the four questionnaires, we were unable to confirm the hypothesized weak correlation between change in physical function and transition in pain since we found a moderate correlation above 0.33, except for the KOOS-PS where the weak correlation with transition in pain was confirmed (r=-0.28). In addition, for all questionnaires we were unable to confirm a higher strength of correlation between change in physical function with change in NRS function than between change in physical function and change in NRS pain (hypothesis 13).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 97
6
Table 1 Socio-demographic and disease-related characteristics of 161 patients with knee OA1
Socio-demographic characteristicsFemale; n (%) 99 (61)Age, years; n (%) 59 (9)Body Mass Index (BMI), kg/m2 29.7 (5.0)Localization of symptoms:
Left knee; n (%) 39 (24))Right knee; n (%) 56 (35)Both sides; n (%) 66 (41)
Duration of complaints > 5 years 59 (37)PROMs regarding physical functionKOOS-PS (range 0-100) 53.6 (16.8)LAI (range 0-24) 11.0 (4.0)LEFS (range 0-80) 40.6 (14.1)WOMAC-PF (range 0-100) 51.8 (19.4)Other PROMsNRS function (range 0-10) 5.5 (2.4)NRS pain (range 0-10) 5.6 (2.1)NRS PGA (range 0-10) 5.6 (2.6)Physical function (SF-36) (range 0-100) 31.8 (9.1)Mental health (SF-36) (range 0-100) 39.8 (4.7)Fatigue (CIS) (range 8-56) 34.4 (11.8)Self-efficacy (DGSS) (range 0-100) 32.3 (5.0)Active coping (PCI) (range 0-4) 2.3 (0.5)Passive coping (PCI) (range 0-4) 2.0 (0.4)Anxiety (HADS) (range 0-21) 6.0 (4.4)Depression (HADS) (range 0-21) 5.8 (3.8)Changes in daily function rated on the transition question
Very much improved 4 (2.5)Much improved 13 (8.1)Slightly improved 28 (17.5)No change 59 (36.9)Slightly worsened 42 (26.3)Much worsened 13 (8.1)Very much worsened 1 (0.6)
1Values are the mean (SD) unless indicated otherwise.Abbreviations: KOOS-PS = Knee Injury and Osteoarthritis Outcome Physical Function Short Form; LAI = Lequesne Algofunctinal index; LEFS = Lower Extremity Functional Scale; WOMAC-PF = Western Ontario and McMaster University Osteoarthritis Index; NRS = Numeric Rating Scale; PGA = Patient Global Assessment; SF-36 = Short Form 36 Health Survey; CIS = Checklist Individual Strength; DGSS = Dutch General Self Efficacy; PCI = Pain Coping Inventory; HADS = Hospital Anxiety and Depression Scale.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
98 | Chapter 6
Tabl
e 2.
Bas
elin
e va
lue
(SD)
and
cha
nge
scor
es a
fter
3 m
onth
s (9
5% c
onfid
ence
inte
rval
) of p
hysic
al fu
nctio
n of
four
PRO
Ms
by t
rans
ition
rep
ly fo
r pa
tient
s w
ith k
nee
OA
(Ver
y) m
uch
impr
oved
Stab
le(V
ery)
muc
h w
orse
ned
n=17
(10.
6%)
n=12
9 (8
0.6%
)n=
14 (8
.8%
)
Base
line
(SD)
Chan
ge (9
5% C
I)Ba
selin
e (S
D)Ch
ange
(95%
CI)
Base
line
(SD)
Chan
ge (9
5% C
I)KO
OS-
PS (r
ange
0-1
00)
51.9
(19.
0)9.
4(3
.1 to
15.
8)52
.9(1
5.8)
2.1
(-0.1
to 4
.3)
66.4
(18.
7)-2
.5(-1
5.8
to 1
0.7)
LAI (
rang
e 0-
24)
10.7
(4.7
)3.
0(1
.4 to
4.7
)10
.7(3
.9)
0.0
(-0.5
to 0
.5)
13.9
(3.5
)-2
.0(-3
.6 to
-0.5
)LE
FS (r
ange
0-8
0)43
.2(1
3.7)
-11.
4(-1
5.6
to -7
.2)
41.1
(14.
6)-0
.3(-2
.0 to
1.3
)33
.7(9
.2)
12.3
(7.7
to 1
7.0)
WO
MAC
-PF
(ran
ge 0
-100
)55
.3(2
0.3)
-12.
4(-1
7.9
to -7
.0)
53.0
(19.
0)-0
.8(-3
.0 to
1.4
)13
.9(3
.5)
7.6
(1.2
to 1
4.0)
Abbr
evia
tions
: KO
OS-
PS =
Kne
e In
jury
and
Ost
eoar
thriti
s O
utco
me
Phys
ical
Fun
ction
Sho
rt F
orm
; LAI
= L
eque
sne
Algo
func
tinal
inde
x; L
EFS
= Lo
wer
Ex
trem
ity F
uncti
onal
Sca
le; W
OM
AC-P
F =
Wes
tern
Ont
ario
and
McM
aste
r Uni
vers
ity O
steo
arth
ritis
Inde
x.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 99
6
Tabl
e 3.
Cor
rela
tion
coeffi
cien
ts (r
, 95%
con
fiden
ce in
terv
al) b
etw
een
chan
ges (
Δ) in
phy
sical
func
tion
in K
OO
S-PS
, LAI
, LEF
S an
d W
OM
AC-P
F sc
ores
and
ch
ange
s (Δ
) in
scor
es o
n re
late
d an
d un
rela
ted
cons
truc
ts.
Δ KO
OS-
PSr
(95%
CI)
Δ LA
Ir
(95%
CI)
Δ LE
FS r(9
5% C
I)Δ
WO
MAC
-PF
r(9
5% C
I)
Δ N
RS p
hysic
al fu
nctio
n0.
32(0
.16
to 0
.46)
0.49
(0.3
6 to
0.6
0)-0
.45
(0.5
6 to
-0.3
1)-0
.45
(-0.5
6 to
-0.3
1)Δ
NRS
pai
n0.
33(0
.17
to 0
.46)
0.49
(0.3
6 to
0.6
0)-0
.45
(-0.5
7 to
-0.3
2)-0
.45
(-0.5
7 to
-0.3
1)Δ
Phys
ical
func
tion
(SF-
36)
-0.4
0(-0
.53
to -0
.25)
-0.4
4(-0
.56
to -0
.31)
0.53
(0.4
0 to
0.6
3)0.
47(0
.34
to 0
.59)
Δ M
enta
l hea
lth (S
F-36
)-0
.10
(-0.2
6 to
0.0
6)-0
.12
(-0.2
7 to
0.0
4)0.
17(0
.01
to 0
.32)
0.15
(-0.0
0 to
0.3
0)Δ
Fatig
ue (C
IS)
0.22
(0.0
6 to
0.3
7)0.
21(0
.06
to 0
.36)
-0.2
1(-0
.36
to -0
.05)
-0.1
7(-0
.32
to -0
.01)
Δ Se
lf-ef
ficac
y (D
GSS
)-0
.07
(-0.2
3 to
0.0
9)0.
11(-0
.05
to 0
.27)
0.01
(-0.1
5 to
0.1
6)-0
.01
(-0.1
7 to
0.1
4)Δ
Activ
e co
ping
(PCI
)0.
09(-0
.07
to 0
.25)
0.13
(-0.0
3 to
0.2
9)-0
.07
(-0.2
2 to
0.0
9)-0
.09
(-0.2
4 to
0.0
7)Δ
Pass
ive
copi
ng (P
CI)
0.24
(0.0
8 to
0.4
0)0.
32(0
.17
to 0
.46)
-0.2
4(-0
.38
to -0
.09)
-0.2
0(-0
.35
to -0
.05)
Δ An
xiet
y (H
ADS)
0.25
(0.0
8 to
0.4
0)0.
16(-0
.00
to 0
.31)
-0.1
4(-0
.29
to 0
.02)
-0.1
6(-0
.31
to -0
.00)
Δ De
pres
sion
(HAD
S)0.
26(0
.10
to 0
.41)
0.22
(0.0
6 to
0.3
7)-0
.18
(-0.3
3 to
-0.0
2)-0
.20
(-0.3
5 to
-0.0
5)Tr
ansiti
on p
hysic
al fu
nctio
n-0
.33
(-0.4
7 to
-0.1
8)-0
.42
(-0.5
4 to
-0.2
8)0.
53(0
.41
to 0
.64)
0.41
(0.2
7 to
0.5
3)Tr
ansiti
on p
ain
-0.2
8(-0
.42
to -0
.12)
-0.3
7(-0
.50
to -0
.23)
0.48
(0.3
4 to
0.5
9)0.
34(0
.20
to 0
.47)
In b
old,
sig
nific
ant c
orre
latio
n, p
< 0
.05
Abbr
evia
tions
: KO
OS-
PS =
Kne
e In
jury
and
Ost
eoar
thriti
s O
utco
me
Phys
ical
Fun
ction
Sho
rt F
orm
; LAI
= L
eque
sne
Algo
func
tinal
inde
x; L
EFS
= Lo
wer
Ex
trem
ity F
uncti
onal
Sca
le; W
OM
AC-P
F =
Wes
tern
Ont
ario
and
McM
aste
r Uni
vers
ity O
steo
arth
ritis
Inde
x; N
RS =
Num
eric
Rati
ng S
cale
; SF-
36 =
Sho
rt
Form
36
Hea
lth S
urve
y; C
IS =
Che
cklis
t Ind
ivid
ual S
tren
gth;
DG
SS =
Dut
ch G
ener
al S
elf E
ffica
cy; P
CI =
Pai
n Co
ping
Inve
ntor
y; H
ADS
= H
ospi
tal A
nxie
ty
and
Depr
essio
n Sc
ale.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
100 | Chapter 6
Tabl
e 4.
Res
ults
of p
rede
fined
hyp
othe
ses
to a
sses
s th
e re
spon
siven
ess
of th
e KO
OS-
PS, L
AI, L
EFS
and
WO
MAC
-PF
in p
atien
ts w
ith k
nee
OA.
Hyp
othe
sis
KOO
S-PS
LAI
LEFS
WO
MA
C-PF
1.Th
ere
is at
leas
t a m
oder
ate
corr
elati
on (r
> 0
.3) w
ith Δ
NRS
func
tion
yes
yes
yes
yes
2.Th
ere
is a
wea
k co
rrel
ation
r ≤
0.3
with
Δ N
RS p
ain
nono
nono
3.Th
ere
is at
leas
t a m
oder
ate
corr
elati
on (r
> 0
.3) w
ith Δ
SF-
36 s
ubsc
ale
phys
ical
func
tion
yes
yes
yes
yes
4.Th
ere
a w
eak
corr
elati
on r
≤ 0.
3 w
ith Δ
SF-
36 s
ubsc
ale
men
tal h
ealth
yes
yes
yes
yes
5.Th
ere
is a
wea
k co
rrel
ation
r ≤
0.3
with
Δ fa
tigue
yes
yes
yes
yes
6.Th
ere
is a
wea
k co
rrel
ation
r ≤
0.3
with
Δ s
elf-e
ffica
cyye
sye
sye
sye
s7.
Ther
e is
a w
eak
corr
elati
on r
≤0.3
with
Δ a
ctive
cop
ing
yes
yes
yes
yes
8.Th
ere
is a
wea
k co
rrel
ation
r ≤
0.3
with
Δ p
assiv
e co
ping
yes
noye
sye
s9.
Ther
e is
a w
eak
corr
elati
on r
≤ 0.
3 w
ith Δ
anx
iety
yes
yes
yes
yes
10.
Ther
e is
a w
eak
corr
elati
on r
≤ 0.
3 w
ith Δ
dep
ress
ion
yes
yes
yes
yes
11.
Ther
e is
at le
ast a
mod
erat
e co
rrel
ation
(r >
0.3
) with
tran
sition
phy
sical
func
tion
yes
yes
yes
yes
12.
Ther
e is
a w
eak
corr
elati
on r
≤ 0.
3 w
ith tr
ansiti
on p
ain
yes
nono
no13
.Th
e co
rrel
ation
with
ΔN
RS fu
nctio
n is
stro
nger
than
the
corr
elati
on w
ith Δ
NRS
pai
nno
nono
no14
.Th
e co
rrel
ation
with
tran
sition
func
tion
is st
rong
er th
an th
e co
rrel
ation
with
tran
sition
pai
nno
nono
yes*
15.
The
abili
ty t
o di
sting
uish
pati
ents
who
wer
e (v
ery)
muc
h im
prov
ed a
nd w
ho w
ere
stab
le in
ph
ysic
al fu
nctio
n (A
UC
≥ 0.
7)no
yes
yes
yes
Confi
rmed
, n/n
(%)
11/1
5 (7
3)10
/15
(67)
11/1
5 (7
3)12
/15
(80)
Abbr
evia
tions
: KO
OS-
PS =
Kne
e In
jury
and
Ost
eoar
thriti
s O
utco
me
Phys
ical
Fun
ction
Sho
rt F
orm
; LAI
= L
eque
sne
Algo
func
tinal
inde
x; L
EFS
= Lo
wer
Ex
trem
ity F
uncti
onal
Sca
le; W
OM
AC-P
F =
Wes
tern
Ont
ario
and
McM
aste
r Uni
vers
ity O
steo
arth
ritis
Inde
x; Δ
= c
hang
e in
; NRS
= N
umer
ic R
ating
Sca
le;
SF-3
6 =
Shor
t For
m 3
6 H
ealth
Sur
vey;
AU
C =
area
und
er th
e re
ceiv
er o
pera
ting
char
acte
ristic
cur
ve.
*: s
igni
fican
tly st
rong
er c
orre
latio
n, p
< 0
.05

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 101
6
Only for the WOMAC-PF we could confirm the stronger correlation between change in physical function with transition function than the correlation with transition pain (hypothesis 14). The LAI, LEFS and WOMAC-PF showed a good ability to distinguish patients who were (very) much improved and who were stable in physical function with an AUC of ≥ 0.7 (Figure 1).
For all four PROMs, we were unable to confirm the hypothesized weak correlation between change
in physical function and change in NRS pain since we found a moderate correlation ranging between
0.33 and 0.49 (hypothesis 2). Concerning hypothesis 12, for three of the four questionnaires, we
were unable to confirm the hypothesized weak correlation between change in physical function and
transition in pain since we found a moderate correlation above 0.33, except for the KOOS-PS where
the weak correlation with transition in pain was confirmed (r=-0.28). In addition, for all
questionnaires we were unable to confirm a higher strength of correlation between change in
physical function with change in NRS function than between change in physical function and change
in NRS pain (hypothesis 13). Only for the WOMAC-PF we could confirm the stronger correlation
between change in physical function with transition function than the correlation with transition pain
(hypothesis 14). The LAI, LEFS and WOMAC-PF showed a good ability to distinguish patients who
were (very) much improved and who were stable in physical function with an AUC of ≥ 0.7 (Figure 1).
Figure 1. ROC curves showing the sensitivity and 1-specificity of the change in four PROMs assessing physical function in patients who indicated to be (very) much improved compared with patients who indicated to be stable after 3 months.
Abbreviations: KOOS-PS = Knee Injury and Osteoarthritis Outcome Physical Function Short Form; LAI = Lequesne Algofunctinal index; LEFS = Lower Extremity Functional Scale; WOMAC-PF = Western Ontario and McMaster University Osteoarthritis Index
0.00
0.25
0.50
0.75
1.00
Sen
sitiv
ity
0.00 0.25 0.50 0.75 1.001-Specificity
LEFS ROC area: 0.8168 WOMAC-PF ROC area: 0.7605
KOOS-PS ROC area: 0.6406 LAI ROC area: 0.7582
Reference
Figure 1. ROC curves showing the sensitivity and 1-specificity of the change in four PROMs assessing physical function in patients who indicated to be (very) much improved compared with patients who indicated to be stable after 3 months.Abbreviations: KOOS-PS = Knee Injury and Osteoarthritis Outcome Physical Function Short Form; LAI = Lequesne Algofunctinal index; LEFS = Lower Extremity Functional Scale; WOMAC-PF = Western Ontario and McMaster University Osteoarthritis Index
Discussion
This is the first study that comprehensively assessed and compared the responsiveness of the disease-specific PROMs KOOS-PS, LAI, LEFS, and WOMAC-PF to assess physical function in patients with clinical knee OA. According to the COSMIN standard we tested predefined hypotheses about expected (or absence of) correlations between changes in constructs. Our results suggest that the WOMAC-PF is potentially better able to detect physical function changes over time in patients with knee OA than the KOOS-PS, LAI and LEFS.
The strengths of our study are that a stringent study protocol was developed and that an anchor-based approach was used to assess responsiveness with 15 predefined hypotheses

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
102 | Chapter 6
according the latest COSMIN standard. Secondly, the responsiveness of four PROMs was measured at the same time in the same population of patients with knee OA undergoing the same treatment, which increases the comparability between the four PROMs9,12,37. Results of previous studies assessing responsiveness were based on traditional methods, e.g. ES and SRM which are known to be dependent of the kind of intervention. This could explain the inconsistency of previous findings on the responsiveness of PROMs assessing physical function in knee OA. For example: the LAI has been found to be more responsive than the WOMAC-PF in patients with knee OA following exercise therapy and rehabilitation25,38, whilst the WOMAC-PF subscale was found to be more responsive after hip or knee replacement39, but not superior to the LEFS40. Because the responsiveness measured with the COSMIN standard is expected not to impact differently in different interventions, further research is warranted to assess, preferably in a head-to-head comparison, whether our results are valid for other interventions as well.
Contrary to our hypotheses, for all four PROMs, the strength of association of changes in physical function with changes in NRS pain and transition in pain was stronger than hypothesized. Whether physical function and pain can be assessed independently with PROMs is much debated14,27,40-43. Our findings suggest that the PROMs examined in this study suffer from construct contamination when assessing physical functioning. A previous finding from our research group that the LEFS can discriminate better between these two constructs, could not be confirmed in the current study. It has been suggested that performance-based physical functioning is less influenced by pain than self-reported physical functioning44 and, thus, that performance-based measures are probably better than questionnaires to capture the construct of physical functioning. So far, there is little insight in the measurement properties of performance-based measures in knee OA43,45,46. Further research addressing the added value of performance-based measures above questionnaires to measure physical function in knee OA is warranted. Further research to measure physical function is warranted.
There were some limitations in this study. Firstly, a response shift could have influenced our results, although we deemed a time frame of 3 months long enough to detect improvement and brief enough to minimize the risk of a response shift47,48. Secondly, because of the homogenous population, the results of our study seem to be reserved to patients with symptomatic knee OA in secondary care. Nevertheless, our cohort is comparable with other cohorts, consisting mainly of obese women with knee OA49,50. In addition, because we studied the responsiveness head-to-head, it is unlikely that our sample characteristics could have influenced the results of the comparability between the four PROMs. Finally, fewer patients than expected indicated (very) much improvement in their daily function after 3 months19. Although the COSMIN standard stresses that responsiveness is independent of the magnitude of the change, it is possible that the relatively small number of improved patients could have influenced the strength of the correlations we found. This warrants further research.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 103
6
In conclusion, our results suggest that the WOMAC-PF should be the measure of first choice in clinical trials evaluating the effectiveness of an intervention to assess physical function in patients with knee OA.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
104 | Chapter 6
References
1. Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best.Pract.Res.Clin.Rheumatol. 2006; 20: 3-25
2. Felson DT, Lawrence RC, Hochberg MC, McAlindon T, Dieppe PA, Minor MA et al. Osteoarthritis: new insights. Part 2: treatment approaches. Ann.Intern.Med. 2000; 133: 726-37
3. Jinks C, Jordan K, Croft P. Osteoarthritis as a public health problem: the impact of developing knee pain on physical function in adults living in the community: (KNEST 3). Rheumatology.(Oxford) 2007; 46: 877-81
4. Bellamy N, Kirwan J, Boers M, Brooks P, Strand V, Tugwell P et al. Recommendations for a core set of outcome measures for future phase III clinical trials in knee, hip, and hand osteoarthritis. Consensus development at OMERACT III. J.Rheumatol. 1997; 24: 799-802
5. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
6. Altman R, Brandt K, Hochberg M, Moskowitz R, Bellamy N, Bloch DA et al. Design and conduct of clinical trials in patients with osteoarthritis: recommendations from a task force of the Osteoarthritis Research Society. Results from a workshop. Osteoarthritis.Cartilage. 1996; 4: 217-43
7. Pham T, van der Heijde D, Altman RD, Anderson JJ, Bellamy N, Hochberg M et al. OMERACT-OARSI initiative: Osteoarthritis Research Society International set of responder criteria for osteoarthritis clinical trials revisited. Osteoarthritis.Cartilage. 2004; 12: 389-99
8. Guyatt GH, Deyo RA, Charlson M, Levine MN, Mitchell A. Responsiveness and validity in health status measurement: a clarification. J.Clin.Epidemiol. 1989; 42: 403-8
9. Mokkink LB, Terwee CB, Knol DL, Stratford PW, Alonso J, Patrick DL et al. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC.Med.Res.Methodol. 2010; 10: 22
10. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J et al. Quality criteria were proposed for measurement properties of health status questionnaires. J.Clin.Epidemiol. 2007; 60: 34-42
11. Sun Y, Sturmer T, Gunther KP, Brenner H. Reliability and validity of clinical outcome measurements of osteoarthritis of the hip and knee--a review of the literature. Clin.Rheumatol. 1997; 16: 185-98
12. Veenhof C, Bijlsma JW, van den Ende CH, van Dijk GM, Pisters MF, Dekker J. Psychometric evaluation of osteoarthritis questionnaires: a systematic review of the literature. Arthritis Rheum. 2006; 55: 480-92
13. Perruccio AV, Stefan LL, Canizares M, Tennant A, Hawker GA, Conaghan PG et al. The development of a short measure of physical function for knee OA KOOS-Physical Function Shortform (KOOS-PS) - an OARSI/OMERACT initiative. Osteoarthritis.Cartilage. 2008; 16: 542-50
14. Hoogeboom TJ, de Bie RA, den Broeder AA, van den Ende CH. The Dutch Lower Extremity Functional Scale was highly reliable, valid and responsive in individuals with hip/knee osteoarthritis: a validation study. BMC.Musculoskelet.Disord. 2012; 13: 117
15. Terwee CB, Dekker FW, Wiersinga WM, Prummel MF, Bossuyt PM. On assessing responsiveness of health-related quality of life instruments: guidelines for instrument evaluation. Qual.Life Res. 2003; 12: 349-62
16. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986; 29: 1039-49
17. Altman R, Alarcon G, Appelrouth D, Bloch D, Borenstein D, Brandt K et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991; 34: 505-14
18. Smink AJ, van den Ende CH, Vliet Vlieland TP, Swierstra BA, Kortland JH, Bijlsma JW et al. “Beating osteoARThritis”: development of a

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Comparison of responsiveness to assess physical function in knee OA | 105
6
stepped care strategy to optimize utilization and timing of non-surgical treatment modalities for patients with hip or knee osteoarthritis. Clin Rheumatol 2011; 30: 1623-9
19. Snijders GF, den Broeder AA, van Riel PL, Straten VH, de Man FH, van den Hoogen FH et al. Evidence-based tailored conservative treatment of knee and hip osteoarthritis: between knowing and doing. Scand.J.Rheumatol. 2011; 40: 225-31
20. Jaber R, Braksmajer A, Trilling JS. Group visits: a qualitative review of current research. J.Am.Board Fam.Med. 2006; 19: 276-90
21. Bond M, Davis A, Lohmander S, Hawker G. Responsiveness of the OARSI-OMERACT osteoarthritis pain and function measures. Osteoarthritis.Cartilage. 2012; 20: 541-7
22. Ruyssen-Witrand A, Fernandez-Lopez CJ, Gossec L, Anract P, Courpied JP, Dougados M. Psychometric properties of the OARSI/OMERACT osteoarthritis pain and functional impairment scales: ICOAP, KOOS-PS and HOOS-PS. Clin.Exp.Rheumatol. 2011; 29: 231-7
23. Singh JA, Luo R, Landon GC, Suarez-Almazor M. Reliability and clinically important improvement thresholds for osteoarthritis pain and function scales: a multicenter study. J.Rheumatol. 2014; 41: 509-15
24. Lequesne MG. The algofunctional indices for hip and knee osteoarthritis. J.Rheumatol. 1997; 24: 779-81
25. French HP, Fitzpatrick M, FitzGerald O. Responsiveness of physical function outcomes following physiotherapy intervention for osteoarthritis of the knee: an outcome comparison study. Physiotherapy. 2011; 97: 302-8
26. Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys.Ther. 1999; 79: 371-83
27. Pua YH, Cowan SM, Wrigley TV, Bennell KL. The Lower Extremity Functional Scale could be an alternative to the Western Ontario and McMaster Universities Osteoarthritis Index physical function scale. J.Clin.Epidemiol. 2009; 62: 1103-11
28. McConnell S, Kolopack P, Davis AM. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): a review of its utility and measurement properties. Arthritis Rheum. 2001; 45: 453-61
29. Aaronson NK, Muller M, Cohen PD, Essink-Bot ML, Fekkes M, Sanderman R et al. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J.Clin.Epidemiol. 1998; 51: 1055-68
30. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med.Care 1992; 30: 473-83
31. Vercoulen JH, Swanink CM, Fennis JF, Galama JM, van der Meer JW, Bleijenberg G. Dimensional assessment of chronic fatigue syndrome. J.Psychosom.Res. 1994; 38: 383-92
32. Teeuw B, Schwarzer R, Jerusalem M. Dutch adaptation of the General Self-Efficacy Scale. 1994. URL: http://userpage.fu.berlin.de/~health/dutch.htm
33. Kraaimaat FW, Evers AW. Pain-coping strategies in chronic pain patients: psychometric characteristics of the pain-coping inventory (PCI). Int.J.Behav.Med. 2003; 10: 343-63
34. Axford J, Butt A, Heron C, Hammond J, Morgan J, Alavi A et al. Prevalence of anxiety and depression in osteoarthritis: use of the Hospital Anxiety and Depression Scale as a screening tool. Clin.Rheumatol. 2010; 29: 1277-83
35. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J.Psychosom.Res. 2002; 52: 69-77
36. Spinhoven P, Ormel J, Sloekers PP, Kempen GI, Speckens AE, Van Hemert AM. A validation study of the Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychol.Med. 1997; 27: 363-70
37. Dobson F, Hinman RS, Hall M, Terwee CB, Roos EM, Bennell KL. Measurement properties of performance-based measures to assess physical function in hip and knee osteoarthritis: a systematic review. Osteoarthritis.Cartilage. 2012; 20: 1548-62
38. Silva LE, Valim V, Pessanha AP, Oliveira LM, Myamoto S, Jones A et al. Hydrotherapy

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
106 | Chapter 6
versus conventional land-based exercise for the management of patients with osteoarthritis of the knee: a randomized clinical trial. Phys.Ther. 2008; 88: 12-21
39. Theiler R, Sangha O, Schaeren S, Michel BA, Tyndall A, Dick W et al. Superior responsiveness of the pain and function sections of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) as compared to the Lequesne-Algofunctional Index in patients with osteoarthritis of the lower extremities. Osteoarthritis.Cartilage. 1999; 7: 515-9
40. Stratford PW, Kennedy DM, Hanna SE. Condition-specific Western Ontario McMaster Osteoarthritis Index was not superior to region-specific Lower Extremity Functional Scale at detecting change. J.Clin.Epidemiol. 2004; 57: 1025-32
41. Gandek B. Measurement properties of the Western Ontario and McMaster Universities Osteoarthritis Index: A systematic review. Arthritis Care Res.(Hoboken.) 2015; 67: 216-29
42. Ryser L, Wright BD, Aeschlimann A, Mariacher-Gehler S, Stucki G. A new look at the Western Ontario and McMaster Universities Osteoarthritis Index using Rasch analysis. Arthritis Care Res. 1999; 12: 331-5
43. Terwee CB, van der Slikke RM, van Lummel RC, Benink RJ, Meijers WG, de Vet HC. Self-reported physical functioning was more influenced by pain than performance-based physical functioning in knee-osteoarthritis patients. J.Clin.Epidemiol. 2006; 59: 724-31
44. Terwee CB, Mokkink LB, Steultjens MP, Dekker J. Performance-based methods
for measuring the physical function of patients with osteoarthritis of the hip or knee: a systematic review of measurement properties. Rheumatology.(Oxford) 2006; 45: 890-902
45. Barten JA, Pisters MF, Huisman PA, Takken T, Veenhof C. Measurement properties of patient-specific instruments measuring physical function. J.Clin.Epidemiol. 2012; 65: 590-601
46. Kroman SL, Roos EM, Bennell KL, Hinman RS, Dobson F. Measurement properties of performance-based outcome measures to assess physical function in young and middle-aged people known to be at high risk of hip and/or knee osteoarthritis: a systematic review. Osteoarthritis.Cartilage. 2014; 22: 26-39
47. Robling M, Hood K. Response shift, responsiveness or recall bias? Br.J.Gen.Pract. 2002; 52: 585
48. Sprangers MA, Schwartz CE. Integrating response shift into health-related quality of life research: a theoretical model. Soc.Sci.Med. 1999; 48: 1507-15
49. van Dijk GM, Veenhof C, Spreeuwenberg P, Coene N, Burger BJ, van SD et al. Prognosis of limitations in activities in osteoarthritis of the hip or knee: a 3-year cohort study. Arch.Phys.Med.Rehabil. 2010; 91: 58-66
50. Wesseling J, Dekker J, van den Berg WB, Bierma-Zeinstra SM, Boers M, Cats HA et al. CHECK (Cohort Hip and Cohort Knee): similarities and differences with the Osteoarthritis Initiative. Ann.Rheum.Dis. 2009; 68: 1413-9

CHAPTER 7
Patient reported barriers and facilitators to using a self-
management booklet for hip and knee osteoarthritis in
primary care: Results of a qualitative interview study
Nienke Cuperus, Agnes J. Smink, Sita M.A. Bierma-Zeinstra, Joost Dekker, Henk J. Schers, Fijgje de Boer, Cornelia H.M. van den Ende, Thea P.M. Vliet Vlieland
Published in: BMC Family Practice. 2013 Dec 1; 14(1): 181

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
108 | Chapter 7
Abstract
ObjectiveTo enhance guideline-based non-surgical management of hip or knee osteoarthritis (OA), a multidisciplinary, stepped care strategy has been implemented in primary care in a region of the Netherlands. To facilitate this implementation, the self-management booklet “Care for Osteoarthritis” was developed and introduced. The aim of the booklet was to educate patients about OA, to enhance the patient’s active role in the treatment course, and to improve the communication with healthcare providers. To successfully introduce the booklet on a large scale we assessed barriers and facilitators for patients to using this booklet.
MethodsSeventeen primary care patients with hip or knee OA who received the self-management booklet participated in this qualitative study using semi-structured interviews. Purposive sampling was used to ensure diversity of the patients’ view about the booklet. The interviews were transcribed verbatim and analysed using a thematic analysis approach.
ResultsThree core themes with patient perceived barriers and facilitators to use the booklet emerged from the interviews: 1) the role of healthcare providers, 2) the patient’s perceptions about OA and its manageability, and 3) the patient’s perceptions about the usefulness of the booklet and patient’s information needs. Regarding the first theme, a barrier was the lack of encouragement from healthcare providers to use the booklet in the treatment course of OA. Moreover, patients had doubts concerning the healthcare providers’ endorsement of non-surgical treatment for OA. Barriers from the second theme were: thinking that OA is not treatable or that being pro-active during the treatment course is not important. In contrast, being convinced about the importance of an active participation in the treatment course was a facilitator. Third, patients’ perceptions about the usefulness of the booklet and patients’ information needs were both identified as barriers as well as facilitators for booklet use.
ConclusionsThis study contributes to the understanding of patient perceived barriers and facilitators to use a self-management booklet in the treatment course of OA. The results offer practical starting points to tailor the implementation activities of the booklet nationwide and to introduce comparable educational tools in OA primary care or in other chronic diseases.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 109
7
Introduction
Osteoarthritis (OA) is the most common joint disorder and the major cause of chronic musculoskeletal pain and disability in elderly worldwide1. About 18.0% of women and 9.6% of men older than 60 have symptomatic OA; its prevalence is increasing due to the increased life expectancy2. General practitioners (GPs) are frequently consulted by patients with hip or knee OA. The core treatment for OA, a combination of pharmacological and non-pharmacological treatment modalities such as weight management and exercise are mainly performed in primary health care3,4. The success of those interventions are often related to adequate self-management, therefore international guidelines stress the importance of self-management in OA5. Self-management refers to interventions, training, and skills with which patients with a chronic condition can learn how to effectively take care of themselves6. In the last decade, a growing number of studies have examined the effectiveness of self-management programs for OA, with some studies showing improvements in pain and disability7-9.
One strategy to enhance self-management in the treatment of chronic diseases is the use of patient booklets. Based on the evidence-based, multidisciplinary, patient-centred, stepped care strategy for hip or knee OA i.e. BART (Beating osteoARThritis)10, a patient-friendly self-management booklet “Care for Osteoarthritis” (Zorgwijzer Artrose©)11 was systematically developed in collaboration with OA patients and GPs12 and introduced in primary health care in a region of the Netherlands. This booklet consists of three sections. The first section provides information about OA in general and gives an overview of the healthcare providers involved in OA care. The second section provides information about non-surgical evidence-based treatment options for hip and knee OA and its optimal sequence in three steps which is based on the stepped care strategy for hip or knee OA. To enhance the patient’s active role in the treatment of OA as well as the communication with healthcare providers, the third section of the booklet contains tools to monitor symptoms, to evaluate the effect of treatment, to prepare consultations, and to formulate a comprehensive overview of the treatment options that already have been carried out. To successfully introduce this booklet on a large scale, we should evaluate its implementation among the stakeholder group of end users, i.e. the patient13.
Several studies have demonstrated the outcome of using patient booklets in the management of a chronic disease with small improvements in physical activity14, knowledge15-17, and health status outcome17-22. These studies also showed low dissemination rates of the booklets19,21,22, which could be an explanation for the relatively small effects that were found. Although one study examined potential barriers for the introduction of a diabetes passport using focus groups, participants in that study had never actually used the booklet23. To our knowledge, no studies comprehensively described why patients do or do not use such booklets in the treatment course of a chronic disease.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
110 | Chapter 7
Previous qualitative studies have explored barriers for patients to use other non-surgical management recommendations for OA, such as physical exercise24-28 or medication24,28. Commonly identified barriers that limit the patients’ use of these recommendations were patients’ perceptions about OA and its symptoms25-27,29 and patients’ expectations regarding the benefits of non-surgical treatment for OA25-29. However, barriers and facilitators for patients to use a self-management booklet in OA still seems to be unknown.
The aim of this qualitative interview study was to evaluate the introduction of the booklet “Care for Osteoarthritis” by 1.) exploring how patients used the booklet and 2.) identifying patient reported barriers and facilitators to use the booklet. This knowledge can then be used as starting points to implement the booklet nationwide and to introduce comparable educational tools in OA primary care or in other chronic diseases.
Method
Study DesignA qualitative research approach was used in order to explore patient perceived barriers and facilitators to use the booklet “Care for Osteoarthritis”30. We conducted semi-structured interviews31 guided by theoretical concepts of a broad health-related behaviour model; i.e. the Integrated Change (I-Change) model32. This qualitative approach offers patients the opportunity to present their views in their own words about the use of the booklet and allow them to address themes of which the researchers might not be aware of. Written informed consent from participants to record the interview was obtained prior to the start of the interview. The Institutional Review Board of the University Medical Centre, Nijmegen approved the study (protocol number: 2012/133).
ParticipantsWe invited a sample of patients who had participated in an umbrella project that aims to implement the stepped care strategy for hip and knee OA in primary care in a region of the Netherlands and to evaluate the implementation process (i.e. the BART-project)10. In this broader project executed from August 2010 to March 2013, a cohort of 313 patients who visited their primary care general practices with a new episode of hip or knee complaints due to (symptomatic) hip or knee OA were included by their GP. To implement the stepped care strategy, several implementation activities aligned to patients as well as different healthcare providers were developed, performed and evaluated in the BART-project33,34. Patients received the booklet “Care for Osteoarthritis” from their GP or from one of the researchers and were instructed on how to use it. Every six months for two years quantitative data were collected by patient-reported questionnaires to identify the patient’s health seeking behaviour and health status. Considering the large individual variation in the course of OA

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 111
7
symptoms and the likelihood that the patient would consult the booklet during a period characterized by complaints, we approached the participants for this qualitative study 12 months after they had received the booklet. To ensure diversity of the patients’ view about the booklet, purposive sampling was used to identify potential participants. We randomly selected participants based on their answer to the question included in the questionnaire of the BART-project one year after baseline: “Do you use the booklet “Care for Osteoarthritis”?” (yes, regularly / yes, occasionally / yes, but not in the past six months / no, never). Except the category “yes, regularly”, we selected patients in blocks from all the other categories. We were not able to include patients in the category “yes, regularly” as only one patient selected that answer in the questionnaire but refused to participate in this qualitative study.
Data collectionData collection took place between 12 and 18 months after distributing the booklet through semi-structured interviews at the participants’ homes. Two female researchers (AS, NC) working at the rheumatology research department of a specialized hospital in the Netherlands conducted the interviews. The equipment we used to record the interviews provided both audio and video tapes. However, before the start of the data analysis we decided for pragmatic reasons to use only the audio tapes. Alternately, one of the researchers guided the interview and asked the questions, while the other researcher made field notes. In two cases, the partner of the participant was present during the interview. Both researchers were also responsible for the data collection in the BART-project; no other relationship existed with the participants prior to the interviews.
An interview guide with open-ended questions was developed (Table 1) with topics that were derived from a broad behavioural model i.e. the I-Change model. This model postulates that behaviour is the result of a person’s intention which is in turn influenced by four factors: motivational factors (e.g. attitudes, social influences, efficacy), awareness factors (e.g. knowledge, risk perceptions, cues to action), information factors (e.g. quality of messages or sources used) and predisposing factors (e.g. personality, environment)32. We selected the I-Change model as the theoretical framework for the current study as we aimed to identify a broad spectrum of barriers and facilitators for patients to use the booklet. Since the I-Change model incorporates insights of several behavioural models, its integrated nature made it feasible to explore a broad spectrum of potential barriers and facilitators. The interview guide was structured around four constructs of the I-Change model: behaviour (i.e. booklet use), motivation factors (i.e. attitude towards the booklet and OA, efficacy to use the booklet), awareness factors (knowledge about OA, severity of OA, self-management) and information factors (i.e. information received from healthcare providers). In addition, we were interested if patients had suggestions for improvement of the booklet. We did not ask patients about their current intention with regard to using the booklet as patients were interviewed 12

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
112 | Chapter 7
months after they had received the booklet; predisposing factors were already assessed by the questionnaires of the BART-project. The co-authors reviewed the questions for both content and format. The use of an interview guide ensured that the main issues related to the model would be discussed. The questions had an open-ended format to provide patients with the scope to talk about their experiences and perspectives freely and in their own words. Three pilot interviews were held, which led to an adjustment in the wording of the questions. The number of interviews performed was determined by consensual agreement of the researchers that analytical saturation had been achieved i.e. the coding process (as described below) revealed no new information35.
Table 1. Interview guide
Behaviour Do you use the booklet?How do you use the booklet?
Motivation Why do you use (or not use) the booklet?Are you interested in information about OA and the treatment options?What do you think about the booklet?
Awareness What do you know about OA and the treatment options? How severe are your symptoms in daily life? What can you do to influence OA symptoms?
Information What did your healthcare provider tell you about the booklet when you received it?Did you ever discuss the booklet with a healthcare provider?What did healthcare providers tell you about OA?
Suggestion for improvement Do you have any suggestions to improve the booklet?
Data analysisTo analyse the data, a thematic analysis approach was used in order to systematically organize the data and then to identify repeated patterns (themes) across the data with regard to the research question36. First, each interview was transcribed verbatim to facilitate transparency37. The interview transcripts were carefully read by the researchers who also conducted the interviews to ensure validity of the transcripts. Subsequently fragments of meaning within the text in relation to the research question were coded after each interview had taken place. To increase the reliability of the coding process triangulation of researchers was used: both researchers independently coded the interviews. Afterwards, the two researchers compared, discussed, and, if necessary, adjusted their coding. All interviews were analysed with support of the qualitative analysis software program MAXQDA®10 (VERBI software GmBH, Germany) to order the data. Further analysis was conducted after all the interviews were coded. The two researchers grouped similar codes together into sub-themes, which in turn were

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 113
7
organized and clustered together into core themes. As the analysis progressed, the constant comparison and review of the data yielded a number of core themes and sub-themes. During this iterative process, these core themes became the basis for the exploration of barriers and facilitators in the patients’ use of the booklet. Peer debriefing was used: the emerging themes were discussed with the co-authors and an expert in qualitative research (FdB).
Results
ParticipantsTwenty-six patients were approached by telephone to participate in the study. Of those, nine refused to participate because they either did not believe that they could give meaningful information that would contribute to the research question (n= 5) or were not comfortable with being interviewed (n= 4). Five of these nine non-participants had reported in the questionnaire of the BART-project that they had never used the booklet. Interviews were conducted with 17 patients, of whom 12 were women and 5 men, with a median age of 67 years (52-85) (Table 2). Median Western Ontario and McMaster Universities Arthritis Index (WOMAC) score was 77 (55-94). The median interview duration was 35 minutes (20-58). Due to a technical defect, the audio and video tapes of one interview were missing; field notes of this interview were used for analysis. All other data were complete. Booklet useThe data analysis showed that the booklet was used in different manners: some patients only read the booklet while others used the self-management tools in the third section of the booklet. Based on the interviews, we categorized patients according to their booklet use; we determined which patients were actual ‘users’ (i.e. made notes in the booklet, brought the booklet to the consultation with a healthcare provider, or used the tools), which ‘readers’ (i.e. only read the booklet), and which ‘non-users’ (i.e. neither read nor used the booklet). The answers presented below illustrate the difference in how users, readers and non-users responded to the questions regarding their booklet use.8 (u): “For me the booklet serves as a mnemonic device. When I read the booklet, I mark important information and discuss this with the GP during a consultation.”10 (r): “I only read the booklet once and then put it away. After that I have never used the booklet.”6 (n): “I never read the booklet.”According to the abovementioned categorization, the study population included four users, eight readers, and five non-users. Patients’ answer to the question “do you use the booklet” varied across the method of administration i.e. questionnaire or interview (Table 2). For the categorization of booklet use we decided to use all the information gathered by the

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
114 | Chapter 7
interviews, rather than the information obtained from the self-report questionnaires of the umbrella project, because in the interviews patients received room to explain and clarify the utilization of the booklet in more detail.
Table 2. Characteristics of the 17 participants and their booklet use
Participant number
Gender Age Duration interview (minutes)
Duration of complaints
(years)
OA severity (WOMAC)1
Booklet use questionnaire2
Booklet use interview3
1 F 71 51 >10 71 Ynr R2 F 85 ? <1 73 Ynr U3 M 67 33 1-5 90 Ynr R4 M 67 47 5-10 73 N N5 M 52 30 >10 71 Yo N6 F 68 45 1-5 82 N N7 F 63 25 1-5 71 N N8 M 65 58 1-5 84 Yo U9 F 69 25 >10 79 N R
10 F 59 22 <1 61 Yo R11 F 67 24 1-5 94 Ynr U12 F 60 39 5-10 64 Yo U13 M 71 55 5-10 55 Yo R14 F 59 37 >10 89 N R15 F 71 58 5-10 79 Yo R16 F 76 20 <1 82 Yo N17 F 70 23 1-5 77 N R
1 standardized WOMAC scores (from questionnaire). Higher scores indicate worse pain, stiffness, and functional limitations2 categorization based on answers given in the questionnaire3 categorization based on answers given in the interviewAbbreviations: F = female; M = male; ? = data missing; Ynr = Yes, but not recently; Yo = Yes, occasionally; N = Not ever; U = User; R = Reader; N = Non-user
Barriers and facilitators for booklet useBased on the interviews several patient perceived barriers and facilitators to use the self-management booklet in OA care emerged from the data analysis (Table 3). These barriers and facilitators can be divided into three core themes: 1) the role of healthcare providers, 2) the patient’s perceptions about OA and its manageability and 3) the patient’s perceptions about the usefulness of the booklet and patient’s information needs.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 115
7
Theme 1: the role of healthcare providersWe identified three barriers and a facilitator in booklet use related to healthcare providers. First, the majority of patients reported that they had not received any clear information about how to use the booklet from their healthcare providers. Among those who had been informed to read the booklet, some reported that while having been advised to read the booklet, no instructions were given about how to use it. 7 (n): “The GP did not give me any information about the booklet when I received it.” 13 (r): “When I received the booklet, the GP only told me to have a look inside.”Despite the limited information patients had received about the booklet, this did not impede some patients from using the booklet.11 (u): “The GP did not explain how to use the booklet, I figured it out by myself” The facilitator for booklet use seems to be the encouragement of healthcare providers to use the booklet in the management of OA. One patient reported to be encouraged by the GP to use the booklet to monitor symptoms and to discuss this during their consultation.2 (u): “I take the booklet every time I visit the GP. Together with the GP I fill in the third section of the booklet, I monitor my symptoms by using the booklet and I discuss this with the GP.”None of the other patients reported that they have used the booklet during a consultation after receiving it; in short they were neither encouraged to monitor their symptoms using the booklet nor asked to bring it to subsequent consultations. One patient even suggested that the GP actually discouraged the use of the booklet.12 (u): “When I tried to discuss the content of the booklet with my GP, he told me that the booklet is redundant as they have all the information in the computer.”Patients reported the limited time during a consultation as a reason for the lack of information and the limited encouragement they received from their healthcare providers to use the booklet.4 (n): “The booklet was never discussed with the GP, they do not have time for that, you only have ten minutes.” Thirdly, patients perceived doubts concerning the healthcare providers’ endorsement of non-surgical treatment modalities for OA what might be a barrier for booklet use. Such doubts were reported by the ’non-users’ in particular.13 (r): “The GP told me that a total knee replacement was the only option for me. I asked him about physical therapy, but he told me it would not be useful for me.” 6 (n): “The GP told me that it will only get worse, instead of better.”16 (n): “The orthopaedic surgeon told me that there is nothing we can do.”

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
116 | Chapter 7
Theme 2: the patient’s perceptions about OA and its manageabilityAnalysis of the interviews showed that whether or not patients used the booklet might have been influenced by their own perceptions about OA and how to manage it. Barriers to use the booklet were patients’ perceptions that OA is not treatable, that their complaints were not severe enough, or that being pro-active during the treatment course is not important. 15 (r): “In my opinion, there is nothing to do about OA. Therefore I do not need any advice.”14 (r): “For me, the complaints are not very serious. I am doing fine.”4 (n): “I cannot change anything about OA. The GP is the expert. He knows what to do”. On the other hand, a patient’s perception about OA can also be a facilitator: some perceived that an active participation was important in the treatment course of OA and therefore used the booklet. 8 (u): “I think I can control the symptoms myself. In my opinion, it is important to know what to do, instead of waiting until it gets worse and afterwards regretting that I should have acted earlier.”11 (u): “I think I can minimize the symptoms caused by OA by managing it myself.”In addition, the patients’ concern about the prognosis of OA seems another facilitator to use the booklet.8 (u): “I think the symptoms will deteriorate rather than improve. I hope it will not get worse and I shall make every effort to do so.” After having studied the perceptions about OA among the three patient groups, some differences can be addressed. Non-users and readers were less positive with respect to the extent to which OA is treatable and considered active participation in their own treatment course less important, whereas users perceived that active participation is indeed important in the management of OA.
Theme 3: the patient’s perceptions about the usefulness of the booklet and patient’s information needsThis theme refers to patient perceptions about whether the booklet can be a useful tool in the management of OA as well as to patient information needs; both could serve as either barriers or facilitators. Some patients believed that the booklet is not a useful tool or were not aware of the aims of the booklet. As a consequence, these patients did not read or use the booklet. 6 (n): “I have not read the booklet. In my opinion the booklet is not useful as it will not change anything about my complaints.” In contrast, patient’s perceptions about the usefulness of the booklet might also be a facilitator as some patients thought that the booklet provided the opportunity to make a comprehensive overview of the treatment options that already have been tried (referring to the third section of the booklet) or that it makes information accessible.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 117
7
Table 3. Overview of the patient reported barriers and facilitators to use the self-management booklet
Theme 1: role of healthcare providersBarriers Lack of clear information about how to use the booklet given by the healthcare providers
Lack of encouragement from healthcare providers to use the booklet in the treatment course of OAPatients’ doubts concerning the healthcare providers’ endorsement of non-surgical treatment modalities for OA
Facilitator Encouragement from healthcare providers to use the booklet in the treatment course of OA
Theme 2: patient’s perceptions about OA and its manageabilityBarriers Patients’ perceptions of OA as inevitable or not curable
Patients’ perceptions that the complaints due to OA are not severe enoughThinking that being pro-active during the treatment course is not an effective strategy to control the disease course
Facilitator Being convinced of the importance of an active participation in the treatment course of OA
Theme 3: patient’s perceptions about the usefulness of the booklet and patient’s information needsBarriers Patients’ perceptions that the booklet is not a useful tool to manage their OA or not
being aware of the aims of the bookletHaving already sufficient knowledge about OA or sufficient support from healthcare providersNot willing to know everything about OA or not paying any attention to OA
Facilitators Patients’ perceptions that the booklet is a useful tool to manage their OA Lack of knowledge about OA or being interested in having more information
1 (r): “This tool creates a clear overview of all received treatment options for all healthcare providers.8 (u): “An advantage of the booklet is that you can read it as many times you want. You have all the time to read it. I already have read it three or four times.”The second barrier and facilitator are the patient’s information needs. Patients were not willing to seek information as they believed that they already knew the information found in the booklet, did not want to know everything about OA, did not pay any attention to their OA, or felt to be sufficiently supported by their healthcare providers.4 (n): “I definitely do not want to know everything about my disease.”17 (r): “The booklet is not an appropriate tool for me, I ignore having OA. Only if you are convinced of really having OA, then the booklet might be useful.” 9 (r): “I do not use the booklet, as I have adequate support from my GP, physical therapist, and physician assistant.”On the other hand, information needs of the patient also serve as facilitators: some patients believed that their knowledge about OA was insufficient or were interested in having more information and, therefore, read or used the booklet.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
118 | Chapter 7
8 (u): “I had little knowledge about OA. Therefore, I considered it important to learn more.”In this theme differences between users, readers and non-users could also be addressed. In particular, the non-users did not perceive the booklet to be very useful, whereas readers or users did. Some readers and non-users were not willing to seek information whereas users were interested in more information.
Discussion
To our knowledge, this is the first qualitative study that provides insight into patient perceived barriers and facilitators to use a self-management booklet in the treatment course of OA. Three core themes with barriers and facilitators emerged from the interviews. Regarding the first theme, a barrier to use the booklet was the lack of encouragement from healthcare providers to use the booklet in the treatment course of OA. Moreover, patients had doubts concerning the healthcare providers’ endorsement of non-surgical treatment for OA. In contrast, encouragement from healthcare providers to use the booklet was a facilitator. Barriers from the second theme were: thinking that OA is not treatable or that being pro-active during the treatment course is not important, whereas being convinced of the importance of an active participation was a facilitator. Third, patients’ perceptions about the usefulness of the booklet and patients’ information needs were both identified as barriers as well as facilitators for booklet use.
Before discussing the results, some limitations need to be addressed. First, it is important to recognize that the patients’ perceptions might not coincide with their own or their healthcare providers actual behaviour. We did not cover the healthcare providers’ perceptions about the booklet because this study was restricted to patients, while barriers and facilitators can also act at other levels of the health care system13. Second, we did not include patients who reported to use the booklet regularly in the questionnaire of the BART-project. During the current study, only one patient reported to use the booklet regularly but refused to participate as the patient believed not being able of giving meaningful information. Moreover, the patients answers to the question “do you use the booklet” were inconsistent between the questionnaires and interviews. We categorized booklet use based on the interviews as we considered these answers most valid because in the interviews we were able to explore in more detail how patients used the booklet. Although this could have resulted in missing relevant barriers or facilitators, we believed this was not very likely as the data collection was continued until analytical saturation was achieved. Another limitation might be recall bias, particularly in the non-users as patients were interviewed 12 to 18 months after receiving the booklet. Finally, the identified themes present some of the reasons for patients with OA to make use of a self-management booklet, other themes could emerge due to differences in ethnic background, culture or healthcare systems.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 119
7
According to the interviewed patients, they received little encouragement from their healthcare providers to use the booklet: patients reported that healthcare providers gave no or few instructions regarding how to use the booklet, did not encourage booklet use, and did not refer to it in subsequent consultations. This finding is in line with a study examining booklet use in hypertensive patients; only 10% of these patients were asked by their GP about the booklet after receiving it22. Patients in our study perceived lack of consultation time as an explanation for the limited encouragement they received; probably practice nurses could be involved38. Another explanation might be that patients have low expectations regarding the GP’s encouragement of the booklet what prevented patients from discussing the booklet as has been shown in a study on the implementation of a diabetes passport23. Nonetheless, our results imply that patients need information and encouragement from their healthcare providers to use the booklet in the management of OA.
Interestingly, patients in our study reported doubts concerning the healthcare providers’ endorsement of non-surgical treatment modalities for OA. It has been shown in previous qualitative studies that GPs and rheumatologists consider existing non-surgical treatments insufficiently effective, with a total knee replacement as ultimate and only efficient treatment option24. Rosemann et al.39 showed that GPs hardly tried to motivate patients to change their behaviour to effectively manage OA, as GPs considered its success rate too low. The doubts of patients in our study concerning the healthcare providers’ views of non-surgical treatment for OA might have hindered patients to use the booklet as the healthcare provider’s attitudes and beliefs can affect the patients’ perceptions40 and preferences for treatment41,42. Recently it has been shown that attitudes of healthcare providers remain a major barrier for patients to be more actively involved in their treatment course43. A more explicitly expressed positive attitude of healthcare providers towards the benefits of non-surgical treatment for OA might encourage patients to use the booklet.
Patient’s reluctance to use the booklet might have been caused by the patient’s perceptions of OA as inevitable or not curable, a barrier also found in studies examining the patients’ use of other non-surgical OA recommendations24,27,28. Some patients in our study perceived that being pro-active is not an effective strategy to control the disease course. In a study on illness perceptions it has been stated that patients create their own beliefs about whether the illness is controllable or curable, which determines self-management behaviour44. Considering this, healthcare providers should explore the patient’s illness perceptions before introducing the booklet and if considered inadequate, the perceptions should be discussed in order to improve booklet use. However, it should be noted that, despite additional guidance, the booklet might not be an appropriate tool for every patient. For example, some patients tend to leave the control of their disease to powerful others (the doctor knows best) and do not want to be involved in making decisions regarding their treatment43,45-47; these patients might benefit from a more direct approach such as verbal instruction.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
120 | Chapter 7
The results suggest that some patients did not perceive the booklet as a useful tool to manage OA and therefore did not use it. Perhaps the lack of instructions given in the booklet itself is a contributing factor. Besides, the need for information varied among patients. Some patients were not interested in reading or actively searching for information. These findings are supported in studies on factors influencing patient’s reading and seeking of written information, showing that the patients’ lack of interest in seeking information was associated with their coping styles45,46. For example, some patients search for all kinds of information, whereas others avoid information48. Therefore, healthcare providers need to move from a ‘one size fits all’ method of providing information to a more patient specific approach that considers the unique needs of each patient.
Conclusions
Given the above mentioned findings, patients need encouragement from their healthcare providers to use the self-management booklet in the treatment course of OA, as patients legitimise non-use of the booklet by the lack of encouragement given by their healthcare providers and by their perceived doubts concerning the healthcare providers’ endorsement of non-surgical treatment for OA. Moreover, patients’ illness perceptions, perceptions about the usefulness of the booklet and patients’ information needs are important factors in booklet use. This study contributes to the field of primary health care by understanding barriers and facilitators for patients to use a self-management booklet in the treatment course of OA. The results offer starting points to tailor the implementation activities of the booklet “Care for Osteoarthritis” on a large scale or to introduce comparable tools in OA primary care or in other chronic diseases.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 121
7
References
1. Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best.Pract.Res.Clin.Rheumatol. 2006; 20: 3-25
2. World Health Organization. The global burden of disease: 2004 update. Geneva: World Health Organization.
3. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann.Rheum.Dis. 2013; 72: 1125-35
4. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
5. Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res.(Hoboken.) 2012; 64: 465-74
6. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient.Educ.Couns. 2002; 48: 177-87
7. Coleman S, Briffa NK, Carroll G, Inderjeeth C, Cook N, McQuade J. A randomised controlled trial of a self-management education program for osteoarthritis of the knee delivered by health care professionals. Arthritis Res.Ther. 2012; 14: R21
8. Heuts PH, de BR, Drietelaar M, Aretz K, Hopman-Rock M, Bastiaenen CH et al. Self-management in osteoarthritis of hip or knee: a randomized clinical trial in a primary healthcare setting. J.Rheumatol. 2005; 32: 543-9
9. Warsi A, LaValley MP, Wang PS, Avorn J, Solomon DH. Arthritis self-management education programs: a meta-analysis of the effect on pain and disability. Arthritis Rheum. 2003; 48: 2207-13
10. Smink AJ, van den Ende CH, Vliet Vlieland TP, Swierstra BA, Kortland JH, Bijlsma JW et al. “Beating osteoARThritis”: development of a
stepped care strategy to optimize utilization and timing of non-surgical treatment modalities for patients with hip or knee osteoarthritis. Clin.Rheumatol. 2011; 30: 1623-9
11. Smink AJ. Care booklet “Care for Osteoarthritis” (in Dutch: “Zorgwijzer Artrose©”). Bone & Joint Decade NL 2013. Available at www.artrosezorgnet.nl/diagnose-behandeling/ZorgwijzerArtrose/
12. Francis N, Wood F, Simpson S, Hood K, Butler CC. Developing an ‘interactive’ booklet on respiratory tract infections in children for use in primary care consultations. Patient.Educ.Couns. 2008; 73: 286-93
13. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet 2003; 362: 1225-30
14. Williams NH, Amoakwa E, Belcher J, Edwards RT, Hassani H, Hendry M et al. Activity Increase Despite Arthritis (AIDA): phase II randomised controlled trial of an active management booklet for hip and knee osteoarthritis in primary care. Br.J.Gen.Pract. 2011; 61: e452-e458
15. Barlow JH, Wright CC. Knowledge in patients with rheumatoid arthritis: a longer term follow-up of a randomized controlled study of patient education leaflets. Br.J.Rheumatol. 1998; 37: 373-6
16. Dawes MG, Kaczorowski J, Swanson G, Hickey J, Karwalajtys T. The effect of a patient education booklet and BP ‘tracker’ on knowledge about hypertension. A randomized controlled trial. Fam.Pract. 2010; 27: 472-8
17. Maggs FM, Jubb RW, Kemm JR. Single-blind randomized controlled trial of an educational booklet for patients with chronic arthritis. Br.J.Rheumatol. 1996; 35: 775-7
18. Dijkstra R, Braspenning J, Grol R. Implementing diabetes passports to focus practice reorganization on improving diabetes care. Int.J.Qual.Health Care 2008; 20: 72-7
19. Dijkstra RF, Braspenning JC, Huijsmans Z, Akkermans RP, van BE, ten HP et al. Introduction of diabetes passports involving both patients and professionals to improve hospital outpatient diabetes care. Diabetes Res.Clin.Pract. 2005; 68: 126-34

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
122 | Chapter 7
20. Simmons D, Gamble GD, Foote S, Cole DR, Coster G. The New Zealand Diabetes Passport Study: a randomized controlled trial of the impact of a diabetes passport on risk factors for diabetes-related complications. Diabet.Med. 2004; 21: 214-7
21. Warner JP, King M, Blizard R, McClenahan Z, Tang S. Patient-held shared care records for individuals with mental illness. Randomised controlled evaluation. Br.J.Psychiatry 2000; 177: 319-24
22. Watkins CJ, Papacosta AO, Chinn S, Martin J. A randomized controlled trial of an information booklet for hypertensive patients in general practice. J.R.Coll.Gen.Pract. 1987; 37: 548-50
23. Dijkstra R, Braspenning J, Grol R. Empowering patients: how to implement a diabetes passport in hospital care. Patient.Educ.Couns. 2002; 47: 173-7
24. Alami S, Boutron I, Desjeux D, Hirschhorn M, Meric G, Rannou F et al. Patients’ and practitioners’ views of knee osteoarthritis and its management: a qualitative interview study. PLoS.One. 2011; 6: e19634
25. Campbell R, Evans M, Tucker M, Quilty B, Dieppe P, Donovan JL. Why don’t patients do their exercises? Understanding non-compliance with physiotherapy in patients with osteoarthritis of the knee. J.Epidemiol.Community Health 2001; 55: 132-8
26. Hendry M, Williams NH, Markland D, Wilkinson C, Maddison P. Why should we exercise when our knees hurt? A qualitative study of primary care patients with osteoarthritis of the knee. Fam.Pract. 2006; 23: 558-67
27. Petursdottir U, Arnadottir SA, Halldorsdottir S. Facilitators and barriers to exercising among people with osteoarthritis: a phenomenological study. Phys.Ther. 2010; 90: 1014-25
28. Poitras S, Rossignol M, Avouac J, Avouac B, Cedraschi C, Nordin M et al. Management recommendations for knee osteoarthritis: how usable are they? Joint Bone Spine 2010; 77: 458-65
29. Carr A. Barriers to the effectiveness of any intervention in OA. Best.Pract.Res.Clin.Rheumatol. 2001; 15: 645-56
30. Pope C, Mays N. Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research. BMJ 1995; 311: 42-5
31. Britten N. Qualitative interviews in medical research. BMJ 1995; 311: 251-3
32. Vries H, Mesters I, van de Steeg H, Honing C. The general public’s information needs and perceptions regarding hereditary cancer: an application of the Integrated Change Model. Patient.Educ.Couns. 2005; 56: 154-65
33. Smink AJ, Bierma-Zeinstra SM, Dekker J, Vliet Vlieland TP, Bijlsma JW, Swierstra BA et al. Agreement of general practitioners with the guideline-based stepped-care strategy for patients with osteoarthritis of the hip or knee: a cross-sectional study. BMC.Fam.Pract. 2013; 14: 33
34. Smink AJ, Dekker J, Vliet Vlieland TP, Swierstra BA, Kortland JH, Bijlsma JW, Teerenstra S, Voorn TB, Bierma-Zeinstra SM, Schers HJ, van den Ende CH. Health care use of patients with osteoarthritis of the hip or knee after implementation of a stepped care strategy. Arthritis Care Res.(Hoboken) 2014 Jun;66(6):817-27
35. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int.J.Qual.Health Care 2007; 19: 349-57
36. Braun V, Clarke V. using thematic analysis in psychology. Qualitative Research in Psychology 2006; 3: 77-101
37. Fossey E, Harvey C, McDermott F, Davidson L. Understanding and evaluating qualitative research. Aust.N.Z.J.Psychiatry 2002; 36: 717-32
38. van Eijk-Hustings Y, van TA, Bostrom C, Braychenko E, Buss B, Felix J et al. EULAR recommendations for the role of the nurse in the management of chronic inflammatory arthritis. Ann.Rheum.Dis. 2012; 71: 13-9
39. Rosemann T, Wensing M, Joest K, Backenstrass M, Mahler C, Szecsenyi J. Problems and needs for improving primary care of osteoarthritis patients: the views of patients, general practitioners and practice nurses. BMC.Musculoskelet.Disord. 2006; 7: 48
40. Holden MA, Nicholls EE, Young J, Hay EM, Foster NE. UK-based physical therapists’ attitudes and beliefs regarding exercise and knee osteoarthritis: findings from a mixed-methods study. Arthritis Rheum. 2009; 61: 1511-21
41. Blakeman T, Macdonald W, Bower P, Gately C, Chew-Graham C. A qualitative study

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Qualitative interview study on a self-management booklet for hip and knee OA | 123
7
of GPs’ attitudes to self-management of chronic disease. Br.J.Gen.Pract. 2006; 56: 407-14
42. Carnes D, Anwer Y, Underwood M, Harding G, Parsons S. Influences on older people’s decision making regarding choice of topical or oral NSAIDs for knee pain: qualitative study. BMJ 2008; 336: 142-5
43. Frosch DL, May SG, Rendle KA, Tietbohl C, Elwyn G. Authoritarian physicians and patients’ fear of being labeled ‘difficult’ among key obstacles to shared decision making. Health Aff.(Millwood.) 2012; 31: 1030-8
44. Kaptein AA, Klok T, Moss-Morris R, Brand PL. Illness perceptions: impact on self-management and control in asthma. Curr.Opin.Allergy Clin.Immunol. 2010; 10: 194-9
45. Ek S, Heinstrom J. Monitoring or avoiding health information--the relation to inner inclination and health status. Health Info.Libr.J. 2011; 28: 200-9
46. Koo M, Krass I, Aslani P. Enhancing patient education about medicines: factors influencing reading and seeking of written medicine information. Health Expect. 2006; 9: 174-87
47. Levinson W, Kao A, Kuby A, Thisted RA. Not all patients want to participate in decision making. A national study of public preferences. J.Gen.Intern.Med. 2005; 20: 531-5
48. Husson O, Thong MS, Mols F, Oerlemans S, Kaptein AA, van de Poll-Franse LV. Illness perceptions in cancer survivors: what is the role of information provision? Psychooncology. 2013; 22: 490-8


CHAPTER 8
Characterizing the concept of activity pacing as a non-
pharmacological intervention in rheumatology care:
results of an international Delphi survey
Nienke Cuperus, Thea P.M. Vliet Vlieland, Nina Brodin, Alison Hammond, Ingvild Kjeken, Hans Lund, Susan Murphy, Yvette Neijland, Christina H. Opava,
Sanja Roškar, Ruta Sargautyte, Tanja Stamm, Xavier Torres Mata, Till Uhlig, Heidi Zangi, Cornelia H.M. van den Ende
Submitted

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
126 | Chapter 8
Abstract
ObjectiveTo develop a consensual list of the most important aspects of activity pacing (AP) as an intervention within the context of non-pharmacological rheumatology care.
MethodsAn international, multidisciplinary expert panel comprising 60 clinicians and/or healthcare providers experienced with AP across 12 different countries participated in a Delphi survey. Over four Delphi rounds, the panel identified and ranked the most important goals of AP, behaviours of AP (the actions people take to meet the goal of AP), strategies to change behaviour in AP and contextual factors that should be acknowledged when instructing AP. Additionally, topics for future research on AP were formulated and prioritized.
ResultsThe Delphi panel prioritized 9 goals, 11 behaviours, 9 strategies to change behaviour and 10 contextual factors of AP. These items were integrated into a consensual list containing the most important aspects of AP interventions in non-pharmacological rheumatology care. Nine topics for future research on AP with the highest ranking were included in a research agenda highlighting that future research should focus on the effectiveness of AP interventions and on appropriate outcome measures to assess its effectiveness, as selected by 64% and 82% of the panellists, respectively.
ConclusionThe diversity and number of items included in the consensual list developed in the current study reflect the heterogeneity of the concept of AP. This study is an important first step in achieving more transparency and homogeneity in the concept of AP in both rheumatology daily clinical practice and research.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 127
8
Introduction
Activity pacing (AP) is a recommended non-pharmacological, non-surgical intervention for the management of rheumatic diseases in international clinical guidelines1-3. In daily clinical practice, AP frequently emerges as a primary component of self-management programs within the context of multidisciplinary treatment4-6. Furthermore, AP has been shown to be the advice most frequently given by British and Dutch rheumatology nurses to patients with rheumatoid arthritis (RA)7. It is one of the self-management strategies most frequently applied by patients with a variety of rheumatic conditions8-12. However, despite its wide endorsement in clinical practice, to date AP is still a poorly understood concept with a wide variety in definitions, interpretations and methods of delivery13-15.
In research and clinical rheumatology practice, AP is mainly based on the principle of energy conservation, assuming that individuals with a chronic disease have limited energy resources and therefore need to undertake activity regulation to allow completion of valued activities16. However, the widespread use of AP in rheumatology care is purely pragmatic as stated in a recently published review describing the current knowledge on AP16. There is a large variation in goals and AP behaviours (the actions people take to meet the goal of AP) proposed in the literature5,15,17,18. Also in chronic pain, in which AP is a central concept in theories and treatment, there is no consensus on the interpretation of AP due to a wide variety in how AP has been described (e.g. operant conditioning vs. energy conservation)14,16,19. Recently, various attempts have been made to clarify the concept of AP in the chronic pain literature16,20. In general, AP has now been conceptualized as an intervention whereby individuals balance activity and rest in order to maintain or increase physical function and to participate in necessary and valued activities16,20,21.
The implications of a poor conceptualization of AP are significant in both research and rheumatology practice14. Due to differences in conceptual constructs of AP, empirical evidence of the effectiveness of AP is limited and contradictory14,22. In addition, diversity in perspectives among therapists on what AP is and how it should be applied as an intervention might impede an effective management of the disease14,23. Considering this, we assume the initial issue in research on AP in rheumatology care is to clarify this poorly defined concept. Nielson et al.16 concluded that identifying the goal(s) of AP, behaviours of AP, strategies to change behaviour in AP (e.g. overactivity or underactivity) and contextual factors influencing AP will be a first step towards assessing its effectiveness.
The aim of the current study was to develop a consensual list including the most important aspects of AP interventions related to all rheumatic conditions. An international expert panel prioritized the most important aspects for four dimensions of AP (i.e. the goals, behaviours, strategies to change behaviour and contextual factors that should be acknowledged when teaching AP). This list might be an important first step in achieving more transparency and

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
128 | Chapter 8
homogeneity in the concept of AP in both rheumatology clinical practice and research. Additionally, a research agenda was developed highlighting topics for future research on AP.
Methods
Study designAs we aimed to develop a consensual list containing the most important aspects of AP interventions among international experts, we deemed the Delphi technique to be an appropriate method. The Delphi technique is a widely used and accepted iterative multistage process to transform expert opinion into group consensus within a certain topic24. This method is especially applied when sufficient information or evidence regarding a certain topic is unavailable25. Typically, round 1 is used to generate items and involves open-ended questions, allowing participants freedom in their responses. Subsequently, these items are grouped together and presented to all panellists in a questionnaire form to vote in 2-4 rounds26. During this process the range of items is expected to decrease. The local ethics committee (CMO region Arnhem, Nijmegen) approved the study (protocol number: 2012/523).
International working group and panel selectionPrior to the start of the current study we appointed an international working group (all co-authors) consisting of 15 healthcare professionals or clinicians (i.e. 5 physical therapists, 4 occupational therapists, 3 psychologists, 2 specialized rheumatology nurses and a rheumatologist) experienced with teaching AP to patients with a rheumatic disease and/or with published studies on AP involving a rheumatic disease, across 12 different countries. The working group members participated as panellists and were involved in establishing the final study procedures and preparation of the manuscript. Additionally, we asked each working group member to nominate at least five individuals (preferably working in their own discipline) who were eligible to participate in the Delphi panel (snow-ball technique). To be eligible, individuals had to meet one of the following two criteria: 1.) having at least five years experience in treating patients with a rheumatic disease or 2.) having a publication record in the area of AP involving a rheumatic disease. Potential participants were contacted by e-mail to inform them about the study and to request their participation. There is no agreement on the optimal panel size for Delphi studies and no clear guidelines exists25,27. Most studies use panels of between 15 to 35 experts28. We considered 50 experts sufficient to ensure validity of the study results i.e. to cover the entire spectrum of perspectives from healthcare providers with different backgrounds and expertise and to allow for drop-outs.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 129
8
Data collection
Literature searchWe conducted a pragmatic literature search in order to gather available evidence on the concept of AP. PubMed was searched for articles published up to July 2013 using the key words ((connective tissue diseases[MeSH] OR rheumatic diseases[MeSH] OR musculoskeletal diseases[MeSH] OR arthritis) AND (activity pacing OR “energy conservation”)). With this search we included all rheumatic conditions. We only searched for energy conservation as different term for AP as in rheumatology care AP is mainly based on the principle of energy conservation. This search yielded 65 hits. Furthermore, included articles were hand searched for additional relevant studies. This literature search was not a systematic review and no judgment was made about the quality of the evidence. The results of the literature search assisted in defining the questions of the first Delphi round. Based on this search, we identified four important dimensions of AP that need to be clarified: i.e. the goal(s) of AP, the behaviours of AP, the strategies to change behaviour in AP and contextual factors influencing AP (such as environmental factors, personal factors or disease characteristics). We therefore formulated the following questions of the first Delphi round, which were first reviewed by the members of the working group: 1.) describe all possible goals of AP; 2.) describe all possible behaviours of AP; 3.) describe all possible strategies to change behaviour in AP; and 4.) describe all contextual factors that should be taken into account when teaching AP. This search did not highlight the need of a validated AP measure. Additionally, the literature search was used to identify individuals with a publication record in the area of AP involving a rheumatic disease who were invited to participate in the Delphi survey.
Delphi surveyThe questionnaires of the Delphi rounds were delivered over four rounds by email. Only panellists who completed the first round questionnaire were invited to participate in the subsequent rounds. When panellists completed the first round questionnaire, non-completion of a preceding round questionnaire did not prohibit them from contributing to subsequent rounds. In order to increase response rates, reminders were sent after each Delphi round. The first round was used to generate items. In order to reduce the number of items generated in the first round, items of the first round were refined during 3 following rounds through merging items with a similar content and prioritizing the most important items26,29. Anonymity among experts was maintained throughout all rounds.
Item generation – Delphi Round 1Following the invitation, individuals who agreed to participate were asked to respond to the previous mentioned four open-ended questions. We used open-ended questions in order to generate items and to allow participants complete freedom in their responses24.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
130 | Chapter 8
The results obtained in this round were collated and categorized according to their content independently by two researchers experienced with qualitative research (NC, CHvdE). During a consensus meeting the researchers discussed their categorization until agreement was reached. In order to guarantee transparency, we decided not to merge items with a more or less similar content in this stage.
Round 2In the second round, we asked the panellists to rate the appropriateness of each item on a scale ranging from 1 (completely inappropriate) to 10 (completely appropriate). Considering the abundance of items generated in the first round, we decided to break up the work in the second round by asking each panellist to rate the items of only one of the four dimensions of AP. In this way we ensured the panellists’ motivation to carefully rank the items and minimized the risk for drop-outs. Each dimension was ranked by 15 panellists. To ensure that all domains were equally distributed with regard to professional background and country, purposive sampling was used to allocate dimensions to the panellists. In order to cover all items, panellists were explicitly encouraged to include additional items that were considered missing in round 1. Furthermore, to collect the key scientific questions on AP, we asked the panellists to formulate topics for further research on AP.
Round 3In order to significantly reduce the number of items and maintain those considered to be ‘very appropriate’ by the panellists, items with a median appropriateness score ≥ 8 in round 2 (arbitrarily defined) and the proposed additional items were subjected to Delphi round 3. In this round we asked all panellists to select the 10 items they felt were most appropriate for each dimension of AP and the topics for future research, respectively.
Round 4Prior to the start of the final Delphi round, redundant items were eliminated by merging items with a similar content. Two researchers independently merged items (NC, CHvdE). Afterwards, the two researchers compared, discussed and finally established the remaining items through a consensus meeting. The researchers agreed on the items that could be merged. In total, 25 goals, 76 behaviours, 25 strategies, 38 contextual factors and 75 topics for further research were merged into 18 goals, 53 behaviours, 20 strategies, 29 contextual factors and 56 research topics. The scores of the merged items were combined. Then, items selected by <20% of the panellists in round 3 were removed. The remaining items were subjected to the final Delphi round. In this final round, we asked panellists to select the ten items they felt were most important for each dimension of AP and the research topics, respectively, and subsequently to rank those ten items from most important (1) to least important (10) within each dimension.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 131
8
Ranking of itemsAfter the panellists completed the final Delphi round, we ranked the remaining items in two ways: 1.) in order of the number of panellists that selected the item as being important and 2.) in order of the weighted sum ranking (0-100%) calculated by giving scores to the ranks given by the panellists in the final round i.e. the most important items (rank 1) scored 10 points and the least important items (rank 10) scored 1 point. For each item, the weighted rank scores were summed and divided by the theoretical maximum score (number of panellists x 10 points) and expressed as a percentage (100% maximum).
Results
Panellists A total of 93 potential panellists were invited to participate in the Delphi survey, of whom 68 (73%) responded positively to the invitation. Of these panellists, 60 (88%) completed the first round questionnaire, whereas eight (12%) panellists only completed the demographic questions and were excluded from the current analysis. Demographic characteristics of the panellists are summarized in Table 1. The multidisciplinary Delphi panel consisted of 20 (33%) physical therapists, 17 (28%) occupational therapists, 12 (20%) specialized rheumatology nurses, 8 (13%) psychologists and 3 (5%) rheumatologists across 12 different countries. The majority was female (88%) and the mean (SD) age was 45 (10) years. Panellists were mainly active in clinical patient care (n = 27; 45%), research (n = 25; 42%), education (n = 6; 10%) or another area (n = 2; 3%). The response rates in rounds 2, 3 and 4 were 49 (82%), 45 (75%) and 46 (77%) panellists, respectively (Table 2). In total, 38 (63%) panellists completed all four Delphi rounds.
Delphi survey
Item generation – Delphi Round 1In the first Delphi round, the panellists formulated 132 goals of AP, 133 behaviours of AP, 165 strategies to change behaviour in AP and 157 contextual factors that should be acknowledged when teaching AP. All items generated in the first round could be categorized into one of the four dimensions of AP.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
132 | Chapter 8
Table 1. Demographic characteristics of the international multidisciplinary Delphi panel
Demographic characteristics (n = 60)Female; n (%) 53 (88)Age, years; mean ± SD 45 ± 10Country: n (%)
Austria 6 (10)Belgium 1 (2)Canada 2 (3)Denmark 1 (2)Italy 1 (2)Lithuania 2 (3)Norway 10 (17)Spain 5 (8)Sweden 11 (18)The Netherlands 16 (27)United Kingdom 2 (3)United States 3 (5)
Primary health profession; n (%)Physical therapist 20 (33)Occupational therapist 17 (28)Specialized rheumatology nurse 12 (20)Psychologist 8 (13)Rheumatologist 3 (5)
Current work setting; n (%)Hospital 29 (48)Ambulatory / Outpatient 32 (53)Primary care 1 (2)University / Professional Education 28 (47)Public health 2 (3)Private practice 6 (10)Other 5 (8)
Mainly active in the last 5 years; n (%)Clinical patient care / Rehabilitation 27 (45)Research 25 (42)Education 6 (10)Other 2 (3)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 133
8
Table 2. Response to each round of the Delphi survey
Round 1 Round 2 Round 3 Round 4 Completed all rounds; n(%)Physical therapist 20 14 14 16 12 (60)Occupational therapist 17 13 13 12 10 (59)Rheumatology nurse 12 11 7 9 7 (58)Psychologist 8 8 8 6 6 (75)Rheumatologist 3 3 3 3 3 (100)
Item reduction – Delphi Rounds 2, 3 and 4In the second round, the Delphi panel rated 22 goals, 61 behaviours, 25 strategies and 34 contextual factors with a median appropriateness score ≥ 8, which were together with the additional items (i.e. 3 behaviours, 15 behaviours and 4 contextual factors) subjected to the next Delphi round. Besides, 75 topics for further research on AP were identified by the panellists in round 2. In the third round, 17 goals, 21 behaviours, 18 strategies, 20 contextual factors and 18 topics for further research on AP were selected by ≥ 20% of the responding panellists as most appropriate items and thus subjected to the final round. Based on the ranks given by the panellists in the final round, we selected for each dimension of AP fifty percent of items with the highest weighted sum ranking. These items were included in our consensual list of most important aspects of AP interventions; resulting in 9 goals, 11 behaviours, 9 strategies and 10 contextual factors (Table 3). Also in this table, the number of panellists that selected an item in the final round as being important, are presented. Furthermore, nine topics for future research on AP with the highest weighted sum ranking were included in a research agenda (Table 4). According to our panellists, future research should focus on the effectiveness of AP interventions and on appropriate outcome measures to assess its effectiveness as selected by 64% and 82% of the panellists, respectively.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
134 | Chapter 8
Table 3. Consensual list of most important aspects of activity pacing as an intervention in rheumatology care
Goals of activity pacing (n = 46) Weightedsum ranking
Selected bypanellists, n (%)
1. To balance between activity and rest according to individual goals, preferences and involvement in meaningful activities
55% 39 (85)
2. To participate in daily activities that are essential or of great value for the individual
51% 37 (80)
3. To enable the patient to make behavioural changes to reduce or avoid the cycle of being overactive or underactive
46% 34 (74)
4. To maintain/improve health, quality of life and well-being 45% 33 (72)5. To increase the ability to participate in patient’s prioritized areas 36% 30 (65)6. To increase awareness of what’s important to one selves 33% 24 (52)7. To improve the level of functioning during the day 31% 29 (63)8. To move pain contingent activity to goal contingent activity 31% 27 (59)9. To be able to deal with fatigue in the activities of daily living 29% 30 (65)
Behaviours of activity pacing (n = 44) Weightedsum ranking
Selected bypanellists, n (%)
1. Plan and prioritize necessary and valued activities 53% 34 (77)2. Break up tasks into manageable pieces depending on individual
patterns and context45% 29 (66)
3. Reflect upon activities and make a plan of how to manage, prioritize and distribute activities without getting exhausted
39% 29 (66)
4. Listen to your body and how it responds to activity 38% 24 (55)5. Realistic planning 36% 27 (61)6. Perform physical exercise regularly 32% 24 (55)7. Be awareness of symptoms and how they are related to activities 30% 24 (55)8. Do activities which give energy 30% 22 (50)9. Perceive oneself as being able to self-manage 26% 22 (50)10. Cognitive reframing; how important is it really to do this? 26% 21 (48)11. Learn to find the right pace of doing activities 24% 23 (52)
Strategies to change behaviour in activity pacing (n = 44) Weightedsum ranking
Selected bypanellists, n (%)
1. Identify activities that are important, meaningful, necessary or enjoyable
58% 37 (84)
2. Identify barriers and support to activity pacing 54% 36 (82)3. Start off with a small change (baseline) and building on this 41% 34 (77)4. Weigh the importance of different activities and prioritize
between them35% 27 (61)
5. Discuss how to implement activity pacing in home and work environment with family and colleagues
35% 27 (61)
6. Be aware of what gives and what takes energy 35% 26 (59)7. Use motivational interviewing 33% 25 (57)8. Set goals together with the health professional: starting with a
goal that is meaningful32% 26 (59)
9. Be aware of thoughts connected to pain, activity and fatigue 31% 26 (59)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 135
8
Contextual factors (n = 44) Weightedsum ranking
Selected bypanellists, n (%)
1. Patient’s readiness and motivation to change behaviour 65% 38 (86)2. Patient’s self-efficacy 47% 33 (75)3. Patient’s opinion on benefits and barriers of behavioural change 45% 31 (70)4. Social support form partner, relatives, friends or colleagues 38% 33 (75)5. Patient’s own goals regarding activity 37% 27 (61)6. Patients need to be seen as experts in their illness and life
situation34% 24 (55)
7. Ability to communicate, reflect on and discuss activity patterns and suggestions for change
31% 27 (61)
8. Patient’s resources and abilities to manage their lives 28% 20 (45)9. Patient’s comorbidities 25% 19 (43)10. Patient’s fear of exercise and injury 24% 23 (51)
Table 4. Research agenda representing consensus topics for future research on activity pacing in rheumatology care
Research topics (n = 44) Weightedsum ranking
Selected bypanellists, n (%)
1. Select appropriate outcome measures to assess the effectiveness of activity pacing
48% 36 (82)
2. Assess whether or not activity pacing is effective 48% 28 (64)3. Develop and evaluate the effectiveness of various interventions
aiming to improve activity pacing40% 27 (61)
4. Study whether activity pacing improves patients’ activity level 38% 27 (61)5. Study whether improved activity pacing improves patients’
well-being35% 25 (57)
6. Develop and test an evidence-based activity pacing group program
32% 24 (55)
7. Study whether activity pacing improves fatigue 32% 22 (50)8. Explore how to help patients to self-manage activity pacing 31% 25 (57)9. Study if work, vocational or leisure activity increase after
activity pacing27% 25 (57)

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
136 | Chapter 8
Discussion
In the current study, we developed a consensual list containing the most important aspects of AP interventions in non-pharmacological rheumatology care. An international, multidisciplinary expert panel prioritized 9 goals of AP, 11 behaviours of AP, 9 strategies to change behaviour in AP and 10 contextual factors that should be acknowledged when teaching AP. Given the poor conceptualization of AP in the literature, such a list is a first step in achieving more transparency and homogeneity in the concept of AP in both rheumatology research and daily clinical practice. Furthermore, the Delphi panel prioritized nine topics for future research on AP, showing that research should focus on the effectiveness of AP interventions and on appropriate outcome measures to assess its effectiveness.
Interestingly, our panellists agreed that the most important overall goal of AP is to facilitate participation in meaningful and valued activities. The two highest ranked goals of AP referring to participation in meaningful activities were selected by the vast majority of panellists. This finding is interesting as previous studies (survey and pilot studies) suggested reducing pain and fatigue, symptoms associated with rheumatic diseases as the most important overall goal of AP7,22,30. Yet, a recent published concept analysis of AP as a chronic pain intervention supports our finding that the overall goal of AP is to participate in meaningful activities20. Considering the findings of our Delphi study and the concept analysis of Jamieson-Lega et al.20 increasing research points to the overall goal of AP to facilitate participation in meaningful and valued activities. Healthcare providers in clinical practice and researchers need to be aware of this overall goal of AP that represents a consensus among an international group of health professions.
Based on a content analysis of AP in chronic pain, the two key categories of AP behaviours are ‘slowing down’ and ‘breaking up activities into smaller pieces’31. These behaviours appear to reflect what most researchers mean when using the term AP31. ‘Breaking up tasks into manageable pieces’ was considered as one of the most important behaviours of AP by our panellists. In contrast, ‘slowing down’ was identified in the first Delphi round, but excluded in the final round. Interestingly, since ‘slowing down’ is reflected in many of the current pacing measures31. It is possible that the panellists expected that ‘slowing down’ might enhance inactivity which is in contrast to the overall goal of AP that was endorsed by the panellists (i.e. facilitating engagement in meaningful and valued activities). The more recently developed activity pacing questionnaire (APQ) supports our finding as the item ‘I did my activities at a slower speed’ was excluded as result of a Delphi technique32. That study also shows ‘breaking up activities into manageable pieces’ to be an important aspect of AP. Planning and prioritizing activities was according to our panellists the most important AP behaviour, which is supported by Antcliff et al.32. Furthermore, this Delphi study was the first to show that a patient’s self-efficacy, motivation to change behaviour and social support are likely to

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 137
8
be the most important contextual factors that should be acknowledged when developing AP interventions.
This is the first consensus study on AP focusing on rheumatic diseases in isolation. Broadly, two approaches of AP can be distinguished i.e. the operant approach and energy conservation16,19. Although similar in some respects, these two approaches emphasize different treatment goals: operant-based interventions aim to decrease disability and increase activity level whereas energy conservation interventions seek to preserve energy for valued activities while reducing pain and fatigue16. In this Delphi study we did not specify the theoretical basis with which we evaluated AP, however it seems that our findings are mainly related to the approach of energy conservation.
Healthcare professionals in daily clinical practice can use the list of most important aspects when setting up AP interventions for patients with a rheumatic disease. Together with the patient, the healthcare professional can go through the list and select one or multiple aspects of each dimension of AP that can be combined into an intervention. The selected items can be individually tailored to the patient’s specific needs and abilities. Tailored AP instruction is important; preliminary studies have shown tailored AP instruction to be more effective in reducing physical activity variability and joint stiffness than a more general approach in patients with hip and knee OA15,18. Furthermore, our list might improve a shared conceptual understanding of AP and reduce variability in applying AP approaches among healthcare professionals working within multidisciplinary treatment. This in turn, might improve alignment of care and a more effective management of rheumatic diseases.
To date, empirical evidence of the effectiveness of AP interventions in rheumatology care is limited and contradictory, which can be explained by a poor conceptualization of AP14,33. For example, in some studies AP has been shown to be associated with lower levels of disability34 or fatigue22, where other studies found AP to be associated with higher levels of disability5, pain and fatigue19,30. A more uniform concept of AP might facilitate intervention studies that are needed to gain consistent empirical evidence on the effectiveness of AP and allows research studies to be more easily replicated and compared in systematic reviews. This need for research on the effectiveness of AP interventions was highlighted by our panellists. Yet, the panel considered the standardization of outcome measures to assess the effectiveness of AP as most important topic for future research. This need is supported by a recently published narrative review on the measurement properties of AP measures developed and used in research to date (like the Chronic Pain Coping Inventory or Coping with Rheumatic Stressors questionnaire)31. The authors concluded that existing questionnaires measure a wide variety of outcome domains and items within the same questionnaire often do not reflect a specific goal of AP. Therefore, the first step in future research might be to reach consensus on the most important outcome domains/goals of AP. Subsequently, appropriate outcome measures reflecting those domains need to be developed.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
138 | Chapter 8
It should be noted that although we achieved agreement on four important dimensions of AP, there was a great variety of experts’ perspectives on the concept of AP given the abundance of goals, behaviours, strategies and contextual factors generated in the first round. Furthermore, as we considered it important to guarantee transparency of the panellists’ responses, some overlap exists in items between the four dimensions of AP. For example, ‘do activities which give energy’ was considered an AP behaviour, whereas ‘be aware of what gives and what takes energy’ was selected as strategy. Future research based upon the consensual list presented here and experiences from clinical practice using our list is needed to further improve the conceptualization of AP.
A particular strength of the current study is the use of an international Delphi panel across 12 different countries, enabling generalization of the findings to other western countries. The results can however not be generalized to non-western societies and unfortunately we did not include panellists from Australia or New Zealand. In total, 60 panellists participated recognizing that no optimal number of experts for a Delphi study exist25,27. In order to enhance external validity of the study results, effort was made to ensure panel diversity with respect to healthcare profession and work setting24. A further strength is the relatively high response rate throughout all Delphi rounds. Although not all panellists were able to contribute to all rounds, results did not differ when analysing only the responses of panellists with complete input. There are a number of limitations inherent to Delphi studies that should be considered when interpreting the results. First, we tried to reduce selection bias by using snow-ball sampling; nevertheless, some selection bias in the composition of the Delphi panel might have occurred as experts from the Netherlands, Norway and Sweden were over-represented. Besides, the majority of panellists were physical and occupational therapists what might have influenced the results. We qualitatively explored noticeable differences in responses across professions, but these differences were not apparent. Another limitation might be researcher bias since cut-off scores were not selected prior to the data collection, but were based on pragmatic considerations (to keep the amount of data manageable to ensure the panellists’ motivation to carefully rank the items and minimize the risk for drop outs). The cut-off scores were discussed with the working group members. Third, due to differences in background and expertise among panellists, items considered important by individual experts might have been eliminated during the four-round Delphi survey. Especially in the second Delphi round where we broke up the work between panellists, items considered important by individual experts might have been removed. Furthermore, the Delphi technique has been criticised as panellists only have a limited opportunity to discuss the issues raised or to elaborate on their views24. In the current study we did not show panellists the group votes on subsequent rounds to re-consider their ideas what might be a limitation. Besides, it is important to note that the results of any Delphi study represent expert opinion rather than a correct answer or indisputable fact24,25,27. Finally, the patient’s viewpoint is lacking in the current study, constituting an important limitation. We recognize that patients might offer an

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 139
8
alternative perspective on the concept of AP. The patient perspective needs to be included in the development of AP interventions or when developing appropriate outcome measures to evaluate its effectiveness.
In conclusion, we generated a consensual list including the most important aspects of AP interventions within rheumatology care. This is an important first step towards achieving more transparency and homogeneity in the concept of AP in rheumatology daily clinical practice and research. This in turn might improve an effective management of rheumatic diseases, facilitate intervention studies that are needed to gain consistent empirical evidence on the effectiveness of AP and allows research studies to be more easily replicated and compared. Future research on AP should focus on the effectiveness of AP interventions and on the development of standardized outcome measures to assess its effectiveness.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
140 | Chapter 8
References
1. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum. 2002; 46: 328-46
2. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann.Rheum.Dis. 2013; 72: 1125-35
3. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
4. Hammond A, Young A, Kidao R. A randomised controlled trial of occupational therapy for people with early rheumatoid arthritis. Ann.Rheum.Dis. 2004; 63: 23-30
5. Karsdorp PA, Vlaeyen JW. Active avoidance but not activity pacing is associated with disability in fibromyalgia. Pain 2009; 147: 29-35
6. Macedo AM, Oakley SP, Panayi GS, Kirkham BW. Functional and work outcomes improve in patients with rheumatoid arthritis who receive targeted, comprehensive occupational therapy. Arthritis Rheum. 2009; 61: 1522-30
7. Repping-Wuts H, Hewlett S, van RP, van AT. Fatigue in patients with rheumatoid arthritis: British and Dutch nurses’ knowledge, attitudes and management. J.Adv.Nurs. 2009; 65: 901-11
8. Boonen A, Van Der Heijde D, Landewe R, Chorus A, van LW, Miedema H et al. Is avoidant coping independent of disease status and stable over time in patients with ankylosing spondylitis? Ann.Rheum.Dis. 2004; 63: 1264-8
9. Gong G, Li J, Li X, Mao J. Pain experiences and self-management strategies among middle-aged and older adults with arthritis. J.Clin.Nurs. 2013; 22: 1857-69
10. Kjeken I, Darre S, Slatkowsky-Cristensen B, Hermann M, Nilsen T, Eriksen CS et al. Self-management strategies to support performance of daily activities in hand osteoarthritis. Scand.J.Occup.Ther. 2013; 20: 29-36
11. Repping-Wuts H, Uitterhoeve R, van RP, van AT. Fatigue as experienced by patients with rheumatoid arthritis (RA): a qualitative study. Int.J.Nurs.Stud. 2008; 45: 995-1002
12. Sandstrom MJ, Keefe FJ. Self-management of fibromyalgia: the role of formal coping skills training and physical exercise training programs. Arthritis Care Res. 1998; 11: 432-47
13. Birkholtz M, Aylwin L, Harman RM. Activity pacing in chronic pain management: One aim, but which method? Part one: introduction and literature review. British Journal of Occuptional Therapy 2004; 67: 447-52
14. Gill JR, Brown CA. A structured review of the evidence for pacing as a chronic pain intervention. Eur.J.Pain 2009; 13: 214-6
15. Murphy SL, Smith DM, Lyden AK. Type of activity pacing instruction affects physical activity variability in adults with symptomatic knee or hip osteoarthritis. J.Phys.Act.Health 2012; 9: 360-6
16. Nielson WR, Jensen MP, Karsdorp PA, Vlaeyen JW. Activity Pacing in Chronic Pain: Concepts, Evidence, and Future Directions. Clin.J.Pain 2013; 29: 461-468
17. Nielson WR, Jensen MP, Hill ML. An activity pacing scale for the chronic pain coping inventory: development in a sample of patients with fibromyalgia syndrome. Pain 2001; 89: 111-5
18. Schepens SL, Braun ME, Murphy SL. Effect of tailored activity pacing on self-perceived joint stiffness in adults with knee or hip osteoarthritis. Am.J.Occup.Ther. 2012; 66: 363-7
19. Murphy SL, Kratz AL. Activity pacing in daily life: A within-day analysis. Pain 2014; 155: 2630-2637
20. Jamieson-Lega K, Berry R, Brown CA. Pacing: a concept analysis of the chronic pain intervention. Pain Res.Manag. 2013; 18: 207-13
21. Murphy SL, Clauw DJ. Activity pacing: what are we measuring and how does that relate to intervention? Pain 2010; 149: 582-3
22. Murphy SL, Lyden AK, Smith DM, Dong Q, Koliba JF. Effects of a tailored activity pacing intervention on pain and fatigue for adults with osteoarthritis. Am.J.Occup.Ther. 2010; 64: 869-76

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Characterizing the concept of activity pacing in rheumatic diseases | 141
8
23. Beissner K, Henderson CR, Jr., Papaleontiou M, Olkhovskaya Y, Wigglesworth J, Reid MC. Physical therapists’ use of cognitive-behavioral therapy for older adults with chronic pain: a nationwide survey. Phys.Ther. 2009; 89: 456-69
24. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J.Adv.Nurs. 2000; 32: 1008-15
25. Powell C. The Delphi technique: myths and realities. J.Adv.Nurs. 2003; 41: 376-82
26. Nair R, Aggarwal R, Khanna D. Methods of formal consensus in classification/diagnostic criteria and guideline development. Semin.Arthritis Rheum. 2011; 41: 95-105
27. Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J.Adv.Nurs. 2006; 53: 205-12
28. Gordon, T. J. (1994). The Delphi method. Washington, DC: American Council for the United Nations University.
29. Fransen J, Johnson SR, van den Hoogen F, Baron M, Allanore Y, Carreira PE et al. Items for developing revised classification criteria in systemic sclerosis: Results of a consensus
exercise. Arthritis Care Res.(Hoboken.) 2012; 64: 351-7
30. Murphy SL, Smith DM, Alexander NB. Measuring activity pacing in women with lower-extremity osteoarthritis: a pilot study. Am.J.Occup.Ther. 2008; 62: 329-34
31. Nielson WR, Jensen MP, Karsdorp PA, Vlaeyen JW. A content analysis of activity pacing in chronic pain: what are we measuring and why? Clin.J.Pain 2014; 30: 639-45
32. Antcliff D, Keeley P, Campbell M, Oldham J, Woby S. The development of an activity pacing questionnaire for chronic pain and/or fatigue: a Delphi technique. Physiotherapy. 2013; 99: 241-6
33. Andrews NE, Strong J, Meredith PJ. Activity pacing, avoidance, endurance, and associations with patient functioning in chronic pain: a systematic review and meta-analysis. Arch.Phys.Med.Rehabil. 2012; 93: 2109-21
34. Nielson WR, Jensen MP. Relationship between changes in coping and treatment outcome in patients with Fibromyalgia Syndrome. Pain 2004; 109: 233-41

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39

CHAPTER 9
Summary and general discussion

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
144 | Chapter 9

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 145
9
To date, research on the non-pharmacological, non-surgical management of generalized osteoarthritis (GOA) is very limited. This is mainly due to the fact that research and clinical practice are commonly focused on a specific localization of OA, usually the hips, knees and hands. Yet, the involvement of multiple joint sites is relatively frequent in patients with OA. In studies enrolling patients based on OA in a specific joint, a relatively large subgroup of patients (approximately 50%) can be classified as having GOA1-4. However, the impact of multiple joint involvement on clinical outcomes has received limited attention in joint specific OA cohorts5. The involvement of multiple joints in OA likely imposes specific demands regarding the optimal management. In order to gain knowledge about the non-pharmacological, non-surgical management of patients with GOA, this thesis focused on the health status of patients with GOA and the (cost)-effectiveness of two non-pharmacological treatment programs for patients with GOA. Furthermore, in order to optimize the non-pharmacological management of patients with rheumatic diseases in general, we performed an international Delphi study among experts from 12 different countries to characterize the concept of activity pacing as a non-pharmacological intervention in rheumatology care. This final chapter summarizes the results of this thesis and discusses the main findings, focusing on the methodological limitations, implications for clinical practice and directions for future research.
Summary
Chapter 2 We comprehensively described the health status of patients clinically diagnosed with GOA who were referred for a non-pharmacological multidisciplinary treatment program. A total of 147 patients completed questionnaires on joint involvement, health related quality of life and daily function. The predominantly affected joints with OA in our study population were the hands and knees, with also the combination of hand and knee OA to be most common. The results showed that patients with GOA experience a markedly reduced physical health related quality of life. Furthermore, patients with GOA experience moderate to severe limitations in performing activities of daily living. The participants reported a broad spectrum of important activity limitations and participation restrictions; activities concerning mobility and domestic life were considered as most important activity limitations, especially walking. The results of this study point to the need of developing interventions for patients with GOA targeting the physical component of health related quality of life and mobility limitations. Furthermore, the broad spectrum of activity limitations as reported by the patients underlines that treatment should be tailored to the problems and needs of the individual patient.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
146 | Chapter 9
Chapter 3In chapter 3, a pragmatic single-blind randomized clinical superiority trial was conducted involving 147 patients clinically diagnosed with GOA randomly allocated to either a six week non-pharmacological multidisciplinary face-to-face treatment program or a six week telephone-based treatment program. The aim of both programs was to improve daily function and to enhance self-management skills to control the consequences of the disease. Daily function (primary outcome) and secondary outcomes were assessed at baseline, 6, 26 and 52 weeks. Data were analysed using multilevel regression models corrected for baseline values, sex and group-wise treatment. We found no differences in effectiveness between both treatment programs on the primary outcome over one year follow-up (group difference (95% CI): -0.03 (-0.14, 0.07)) or on secondary outcome measures, except for pain, where a significant difference favouring the face-to-face treatment group was found (group difference (95% CI): 1.61 (0.01, 3.21)). Within both treatment groups, we observed small significant improvements on several domains, especially in the face-to-face treatment group. However, these improvements were relatively small and unlikely to be of clinical importance. Interestingly, many patients preferred the more traditional face-to-face treatment delivery.
Chapter 4Next to the disease burden, OA represents a significant economic burden on individuals, healthcare systems and society. It is therefore important that a clinical evaluation of an intervention is accompanied by an economic evaluation in order to inform decision makers about the efficiency of healthcare resources and to guide decision making processes. Alongside the randomized clinical trial described previously, we conducted an economic evaluation of our treatment programs. Chapter 4 describes, from a societal perspective, the cost-effectiveness and cost-utility analysis of both treatment programs. Program costs were estimated from time registrations. During the one year follow-up period, participants reported all GOA-related direct medical costs (i.e. healthcare-related) and non-medical costs (i.e. other health-related) using cost questionnaires at 6, 13, 26, 39 and 52 weeks. Quality adjusted life years (QALYs) were estimated using three utility measures i.e. the EuroQol-5D, the EuroQol rating scale and the Short Form-6D. Daily function was measured using the HAQ-DI. The net benefits of both treatment programs were estimated for a range of society’s willingness to pay (WTP) values using the formula: net benefit = WTP × effect (QALY or HAQ-DI) – costs. The more cost-effective treatment program was the program with the higher average net benefits, depending on a range of thresholds for the society’s WTP. Given the statistical uncertainty of differences between costs and QALYs we constructed cost-effectiveness acceptability curves (CEAC). The medical costs of the face-to-face treatment and telephone-based treatment programs were estimated at €387 and €252 per patient, respectively. The difference in total societal costs was non-significantly in favour of the face-to-face program (difference (95% CI):

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 147
9
€708 (€-5058, 3642)). QALYs were similar for both groups according to the EuroQol, but were significantly in favour of the face-to-face group according to the SF-6D (difference (95% CI): 0.022 (0.000, 0.045)). Since both societal costs and effects were in favour of the face-to-face treatment program, the economic assessment favoured this program, regardless society’s willingness to pay. At a range between €20.000-€80.000, there was a 60%-90% chance that the face-to-face program had better cost utility. This economic evaluation showed from a societal perspective that the face-to-face treatment program was at least twice as likely cost-effective relative to the telephone-based treatment program.
Chapter 5The measurement properties of the widely used Health Assessment Questionnaire Disability Index (HAQ-DI) to measure daily function in patients with GOA were evaluated in chapter 5. Individuals with GOA typically suffer from restrictions of both upper and lower extremity function. Yet, we lack a validated instrument to assess their activity limitations since existing questionnaires all focus on a specific localization of OA, limiting their use in GOA. The recommendations of the Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN) checklist were followed to assess the interpretability, validity, reliability and responsiveness of the HAQ-DI. For this study data from the baseline and six week follow-up measurements of the clinical trial were used. First, it was found that floor and ceiling effects were present. Moreover, the content validity appeared to be questionable as the HAQ-DI encompasses activities that are either not relevant or too easy to perform for patients with GOA as judged by patients and healthcare professionals experienced with GOA. The construct validity of the HAQ-DI was rated positive and a confirmatory factor analysis confirmed unidimensionality. Cronbach’s alpha was 0.90, confirming internal consistency and the intra-class correlation coefficient was 0.81, reflecting a good reliability. We could not establish the responsiveness of the HAQ-DI. Considering the limited content validity of the HAQ-DI, we concluded that the items of the HAQ-DI need to be updated when using the HAQ-DI in future clinical practice and research focusing on functional limitations in people with GOA. Probably, certain activities of the HAQ-DI are “outdated” since the questionnaire has been developed more than three decades ago, a period during which some activities have become easier to perform due to technological and social developments. We believe, this update of the HAQ-DI might also be worthwhile for other rheumatic diseases.
Chapter 6In this chapter we compared the responsiveness of four widely used patient reported outcome measures (PROMs) for the assessment of physical function in people with knee OA receiving conservative treatment i.e. the Western Ontario and McMaster University Osteoarthritis Index subscale physical function (WOMAC-PF), the Lequesne Algofunctional

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
148 | Chapter 9
index (LAI), the Lower Extremity Functional Scale (LEFS) and the short measure of the Knee disability and Osteoarthritis Outcome Score (KOOS-PS). Responsiveness was investigated by testing predefined hypotheses formulated by an expert group regarding expected correlations between changes in physical function with changes in other (un)related measures, as currently recommended. Responsiveness was considered positive if > 75% of the hypotheses could be confirmed. We could confirm 12 out of 15 predefined hypotheses (80%) using the physical function subscale of the WOMAC. For the LAI, LEFS and KOOS-PS, respectively 9, 11 and 11 hypotheses were confirmed (60%, 73% and 73% respectively). Our findings suggest that the WOMAC-PF is potentially better able to detect changes over time in physical function than the LAI, LEFS and KOOS-PS in a population of patients with knee OA receiving conservative treatment. We recommend that clinicians and researchers should prefer the WOMAC-PF subscale in future clinical trials to evaluate the effectiveness of an intervention.
Chapter 7To enhance guideline-based non-pharmacological, non-surgical management of patients with hip or knee OA, our research group implemented an evidence-based, multidisciplinary, stepped care strategy for hip and knee OA in one region in the Netherlands. The implementation strategy included the provision of a self-management booklet on the stepped care strategy for patients, entitled “Care for Osteoarthritis”, by general practitioners in primary care. The aim of the booklet was to educate patients about OA, to enhance the patient’s active role in the treatment course, and to improve the communication with healthcare providers. To successfully implement the self-management booklet on a larger scale, chapter 7 describes a qualitative interview study on patients’ barriers and facilitators to using the booklet. Three core themes with patient perceived barriers and facilitators to use the booklet emerged from the interviews: 1) the role of healthcare providers, 2) the patient’s perceptions about OA and its manageability, and 3) the patient’s perceptions about the usefulness of the booklet and patient’s information needs. Regarding the first theme, the lack of encouragement from healthcare providers during the treatment course was reported by patients as barrier. Moreover, patients had doubts concerning the healthcare providers’ endorsement of non-surgical treatment for OA. Barriers from the second theme were thinking that OA is not treatable or that being pro-active during the treatment course is not important. In contrast, being convinced that an active participation in the treatment course is important was reported as a facilitator. Regarding the third theme, patients’ perceptions about the usefulness of the booklet and patients’ information needs were both identified as barriers as well as facilitators for booklet use.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 149
9
Chapter 8Activity pacing frequently emerges as a primary component of self-management programs within the context of multidisciplinary treatment of rheumatic diseases. However, activity pacing is still a poorly understood concept with a wide variety in definitions, interpretations and methods of delivery. The implications of a poor conceptualization of activity pacing are significant in both research and rheumatology practice. Therefore, we developed a consensual list containing the most important aspects of activity pacing interventions in rheumatology care. In a four-round Delphi survey an international, multidisciplinary expert panel consisting of 60 clinicians and healthcare professionals across 12 countries prioritized 9 goals of activity pacing, 11 behaviours of activity pacing (the actions people take to meet the goal of activity pacing), 9 strategies to change behaviour in activity pacing and 10 contextual factors that should be acknowledged when teaching activity pacing. The results of this study are an important first step in achieving more transparency and homogeneity in the conceptualization of activity pacing in daily clinical practice and research. This in turn might facilitate an effective management of the disease and allows research studies to be more easily replicated. Furthermore, the Delphi panel prioritized nine topics for future research on activity pacing, showing that research should focus on the effectiveness of activity pacing interventions and on appropriate outcome measures to assess its effectiveness.
Discussion
In this section the main findings of this thesis are put into perspective and will be discussed. Based on these findings, implications for clinical practice and directions for future research are presented.
No differences in effectiveness between two non-pharmacological treatment programs As shown in our randomized clinical trial we could not confirm our hypothesis that a multidisciplinary face-to-face treatment program was superior with respect to effect on daily function and other clinical outcomes compared to a telephone-based treatment program for patients with GOA. Only on one secondary outcome measure (i.e. pain) we found a significant difference in favour of the face-to-face treatment program. The limited differences in effectiveness between both treatment programs can perhaps be explained by the limited contrast in the content of both programs. The contents of both treatment programs were very comparable, but several critical differences were apparent i.e. the mode of care delivery, the number of involved healthcare providers, the number of group sessions and the number of sessions including an exercise program. Nevertheless, these differences are possibly too small to achieve a sufficient and clinically relevant contrast in effectiveness between both treatment programs.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
150 | Chapter 9
Is there a role for non-pharmacological treatment in patients with GOA?So far, no disease modifying therapies are available for OA. Therefore, current guidelines recommend multimodal treatment combining pharmacological and non-pharmacological treatment modalities. When these modalities do not provide sufficient relief, total joint replacement is known to be a very effective treatment option to significantly improve pain and function in patients with hip and knee OA6,7. However, research showed multiple joint involvement in OA to be an important predictor of worse pain, physical function, fatigue and quality of life after joint replacement surgery4,8. Therefore, it has been hypothesized that in patients with GOA, joint replacement surgery might not be as effective as in patients with single joint OA. Besides, joint replacement surgery is unattractive in relatively young patients due to the frequent need for revision surgery after 10-15 years7. Considering this, there is a major need for effective non-pharmacological treatment options for patients with GOA. Unfortunately, scientific knowledge on the management of patients with GOA is lacking so far. In 2014, the Osteoarthritis Research Society International (OARSI) published recommendations for the non-surgical management of OA including multiple joint OA (i.e. OA in other joints in addition to the knee). However, due to the limited available intervention studies, the authors considered balneotherapy (defined as the use of baths containing thermal mineral waters) the only appropriate recommendation for the management of multiple joint OA, whereas no other recommendations could be formulated9. In absence of recommendations for the management of GOA, we used recommendations for the non-pharmacological management of patients with hip and knee OA7,10 as starting points to develop two treatment programs for individuals with GOA. Unfortunately, within both treatment groups, we observed only small improvements on daily function and other clinical outcomes where we expected larger improvements, especially in the face-to-face treatment group. A number of possible explanations for these limited benefits are discussed below.
First, during the development process, we decided to direct our treatment programs on individual goal setting with respect to multiple domains of daily living. At the start of the treatment program each individual participant formulated adequate and realistic goals which were closely monitored, discussed and if necessary adjusted during the treatment program. As GOA may cause various impairments and limitations in activities, individual treatment goals varied considerably among patients. As a result, the treatment programs evaluated in this thesis targeted on a variety of dimensions important for patients with GOA, such as pain, fatigue, physical activity, acceptance of the disease and social support. A consequence of delivering treatment programs covering a wide variety of dimensions is that it may be difficult for individual patients to select the most relevant information for themselves. It is therefore conceivable that treatment programs with more guidance on individually tailored treatment plans, focussing on a lesser number of treatment modalities would be more beneficial than the treatment programs investigated in this thesis.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 151
9
Another possible explanation for the disappointing benefits of our treatment programs might be our assumption that treatment effects observed in patients with hip or knee OA could be extrapolated to patients with GOA. Since we developed both treatment programs based on the latest evidence in hip and knee OA7,10, we expected clinical relevant improvements in daily function and other clinical outcomes in both groups. However, effect sizes of treatment modalities observed in joint-specific OA cohorts (although including patients with GOA) are likely to be lower for individuals with GOA. Previous studies showed a considerably worse health status of patients with multiple joint involvement compared to patients without multiple joint involvement3,5. Furthermore, the complex involvement of multiple joints in lower extremity function suggests a more compromised health status4. It is therefore conceivable that patients with GOA require more complex and intensive treatment programs than patients with single joint OA. Probably, our treatment programs needed to be more intensive with a longer follow-up period in order to obtain clinically relevant improvements on clinical outcomes.
Third, the choice of our primary outcome measure could be argued. When performing studies on the effectiveness of interventions, researchers should include a primary outcome measure which is related to the main objective of the intervention. In our randomized clinical trial, we aimed to improve daily function in patients with GOA and we therefore considered daily function as primary outcome measure. Since no validated patient reported outcome measures (PROMs) are available to assess daily function in people with GOA, we considered the widely used and validated HAQ-DI to be the most appropriate outcome measure11. During the trial, we evaluated the measurement properties of the HAQ-DI in patients with GOA showing a positive construct validity and reliability, but a limited content validity and responsiveness. Based on these findings, we need to conclude that the HAQ-DI might not have been the most appropriate primary outcome measure to assess daily function in our clinical trial. Ideally, the measurement properties of a primary outcome measure are known before starting a trial, but due to time constraints this is often not feasible in practice. Future research is warranted to evaluate the measurement properties of existing (OA specific) physical function instruments or to develop a new measurement instrument in order to accurately measure daily function in patients with GOA.
Given the limited benefits of our treatment programs, we believe it is important at this point to critically reflect on the following question: “What is the value of self-management support programs in patients with GOA?”. Also in joint specific OA studies increasing evidence supports the existence of no or only small effects (ES = 0.06 for pain and physical function) of self-management programs, as reported in systematic reviews12,13 and clinical guidelines14,15. Furthermore, as shown in our qualitative interview study on the use of a self-management booklet for patients with hip and knee OA (chapter 7) many patients perceive OA as inevitable and not curable and are therefore reluctance towards self-management. Considering the

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
152 | Chapter 9
above-mentioned, we hypothesize that we need to move away from focussing on self-management towards more intensive and supervised treatment programs for patients with GOA. Probably, future non-pharmacological treatment programs for patients with GOA need to combine exercises with weight loss as increasing evidence recognizes that this combination of treatment modalities should be the mainstays of rehabilitation for people with knee and hip OA16,17. Several studies enrolling patients based on OA in a specific joint have reported substantial improvements in pain, physical function and quality of life after long-lasting programs combining exercise with weight loss. First, the high quality Intensive Diet and Exercise for Arthritis (IDEA) randomized clinical trial compared the effectiveness of an exercise-only program, diet for weight loss-only program and a combined exercise and diet for weight loss program of 18 months in 454 overweight adults with knee OA18. After 18 months, patients in the combined treatment group reported less pain, better physical function and quality of life compared to patients in the other groups. In addition, the Arthritis, Diet, and Activity Promotion Trial (ADAPT) showed the combination of modest weight loss plus moderate exercise to provide better improvements in function, pain and performance measures of mobility in overweight patients with knee OA compared with either intervention alone19. Furthermore, preliminary evidence showed a clinically relevant improvement in physical function and pain in people with hip OA following an 8-month exercise in combination with weight loss treatment program20. We hypothesize that patients with GOA might benefit more from a long-term supervised treatment program combining weight loss (10-15% weight reduction) with intensive exercises (1 hour, 3 days/week), rather than a self-management program targeting on multiple domains of daily living. Future research is needed to gain empirical evidence for this.
Patient preferencesDirectly after finishing the treatment program we asked a part of the participants several questions about their perceptions of the treatment programs. The questionnaire used to evaluate this comprised visual analogue scales (score range 0-10) to assess the level of satisfaction with the treatment program and the overall usefulness of the treatment (Table 1). Satisfaction scores showed that patients in the multidisciplinary face-to-face treatment group were significantly more satisfied than patients in the telephone-based treatment group. The face-to-face program was rated with a total mean (SD) score of 7.7 (1.4) whereas the telephone-based program was rated with a total mean (SD) score of 6.4 (1.9) (p <0.00).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 153
9
Table 1. Patients’ perceptions of both treatment programs
Face-to-face treatment (n = 32)
Telephone-based treatment
(n = 21)
p
Was the content of the treatment consistent with your expectations?
7.5 (1.5) 5.7 (2.2) 0.001
Was the content of the treatment consistent with your GOA-related complains and limitations?
7.4 (1.5) 5.8 (2.3) 0.004
How confident are you that the treatment was helpful to cope with the consequences of the disease?
7.3 (1.5) 6.1 (2.5) 0.025
Would you recommend the treatment to family or friends? 7.7 (2.5) 6.1 (2.6) 0.037How useful was the treatment program? 7.6 (1.6) 6.0 (2.3) 0.004Are you satisfied with the treatment program? 7.8 (1.8) 6.1 (2.3) 0.006Where you treated with dignity and respect by the admitting healthcare professionals?
8.5 (1.3) 7.8 (1.7) 0.105
Did you receive adequate information during the treatment program?
7.8 (1.3) 7.0 (1.8) 0.045
Overall, how would you value the treatment program? 7.8 (1.6) 6.5 (1.8) 0.010
These results indicate that patients preferred the more traditional face-to-face treatment program. We also observed a preference for the multidisciplinary face-to-face program during the recruitment phase of the trial. The recruitment of patients proceeded at a slower pace than expected. We expected a relatively high accrual rate (>80%) since our study was a pragmatic trial resembling clinical practice. However, many eligible patients declined to participate in the trial, mainly because they preferred the multidisciplinary face-to-face treatment program or were reluctant towards the telephone-based treatment. This was unexpected because the face-to-face program is much more intensive and requires considerably more time than the telephone-based program. The preference for face-to-face treatment is supported by a study examining the acceptability of face-to-face, internet and telephone treatment delivery in primary care, showing the highest level of interest in face-to-face treatment delivery21. Furthermore, Tijhuis and colleagues22 showed that patients with rheumatoid arthritis (RA) were more satisfied with care provided by a multidisciplinary team than with care provided by a clinical nurse specialist. A number of studies support the effectiveness of multidisciplinary team care, especially in patients with RA23. However, team care has now been questioned for several reasons. One major reason is that there is too little evidence for the cost-effectiveness of team care24,25. Furthermore, it should be kept in mind that more care providers does not always mean better care: greater team size may interfere with patient preferences for continuity of care with a single healthcare provider and might impede communication22,26. Therefore, the choice of treatment delivery could be based on the availability of facilities, the preferences of patients and healthcare providers, healthcare systems and/or economic considerations.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
154 | Chapter 9
Which treatment program is more cost-effective?The effectiveness of interventions has traditionally been evaluated in terms of clinical aspects and patient-related outcomes. In recent years, however, outcome measures have expanded to include economic analyses to inform decision makers about the efficiency of healthcare resources due to the increasing costs of healthcare combined with the limited healthcare budgets. The results of our economic evaluation showed that from a societal perspective, the face-to-face treatment program was more likely to be cost-effective relative to the telephone-based treatment program. However, since the difference in net benefit between both treatment programs did not reach statistical significance, we cannot make any firm treatment recommendations based on these results. The results imply that, from the societal perspective, the choice of treatment delivery does not have to be based on costs, but could be based on the patients and healthcare providers preferences or on the availability of facilities and/or healthcare systems. Future studies on the effectiveness of non-pharmacological interventions for patient with GOA should include high quality economic evaluations to assist healthcare providers to choose the best treatment for the patient, bearing in mind the economic consequences.
Conceptualization of non-pharmacological interventionsA clear description of non-pharmacological interventions is essential for researchers and clinicians in order to replicate interventions, compare results across studies in systematic reviews and implement interventions in practice27,28. However, especially in the context of non-pharmacological treatment, the description of interventions is a challenging task29. Hoffmann and colleagues27 showed that only 39% of non-pharmacological interventions were described in sufficient detail to enable replication of the intervention in practice. Comparable results have been shown in interventions studies of exercise programs for patients with hip and knee OA awaiting joint replacement30. Therefore, guidelines and tools are necessary to facilitate standardization in the description of non-pharmacological interventions. A recommended non-pharmacological intervention within rheumatology care that lacks a clear description is activity pacing. In clinical rheumatology practice, activity pacing frequently emerges as a primary component of multidisciplinary self-management programs to decrease pain and fatigue31,32. In chapter 8 of this thesis we aimed to characterize the concept of activity pacing among healthcare professionals with different backgrounds and expertise (i.e. rheumatologists, physical therapists, occupational therapist, rheumatology nurses and psychologists) from 12 different countries. In a four-round Delphi survey we asked the experts to identify items related to the concept of activity pacing. This resulted in an abundance of items, underlying the great variety of the experts’ perspectives on the concept of activity pacing. The abundance of items was refined through merging and prioritizing until agreement was reached. Subsequently, we developed a consensual list containing the most

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 155
9
important aspects of activity pacing interventions. This is an important first step towards achieving more transparency and homogeneity in the concept of activity pacing interventions in rheumatology care and research. This in turn might facilitate an effective management of rheumatic diseases and allows research studies to gain consistent empirical evidence on the effectiveness of activity pacing interventions. Future research based upon both our consensual list and experiences from clinical practice using the list, is expected to further improve the concept of activity pacing.
Are we adequately measuring physical function in patients with OA? An array of disease specific PROMs is available to assess physical function in patients with knee OA. In addition, the measurement properties of these PROMs have been evaluated extensively33. Within the literature, the LAI and WOMAC are recommended as physical function measures of first choice in OA trials enrolling patients with knee OA33,34. Furthermore, the guideline of the Dutch Society for Physical therapy recommends the LAI as first measure to monitor and evaluate physical function in patients with knee OA35. However, in this thesis (chapter 6) we showed a superior responsiveness of the WOMAC subscale physical function in comparison with the LAI, KOOS-PS and LEFS in patients with knee OA who received multimodal non-pharmacological treatment. Based on these findings, we suggest that the WOMAC-PF is potentially better able to detect changes over time in physical function than the LAI, LEFS and KOOS-PS. We therefore recommend that clinicians and researchers should prefer the WOMAC-PF subscale in future clinical trials to assess self-reported physical function in people with knee OA. Whilst the importance of routinely measuring PROMs to monitor individual patients in clinical practice is well recognised and recommended in clinical practice guidelines, it has largely failed to be delivered in practice36. Research has shown that the implementation of PROMs in clinical practice is hampered by the lack of healthcare providers’ knowledge with respect to the use of PROMS e.g. they often do not know which instrument to use for what patient, how to interpret scores and are not familiar with the clinical application of PROMs36,37. Therefore, strategies need to be developed in order to improve the standardized use of PROMs by healthcare professionals in daily clinical practice.
Methodological issues
In this paragraph, we discuss several limitations that should be considered when interpreting the results of this thesis. These issues mainly consider our randomized clinical trial.
Study designA randomized controlled trial is considered the gold standard to examine the effectiveness of any intervention. Such a trial, however, poses a great challenge in healthcare settings,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
156 | Chapter 9
particularly in multidisciplinary rehabilitation. Until recently, the optimal control group in randomized clinical trials was generally considered to be a group receiving no treatment (e.g. placebo or waiting list)38. However, considering the large array of proven effective treatments and ethical considerations, the use of control groups receiving no treatment when effective therapies exist has been debated during the last decade38,39. Proven effectiveness of a wide variety of OA non-pharmacological treatment modalities within the literature made us decide to conduct a trial on the optimal mode of treatment delivery since research on the optimal modes of therapy delivery is limited. Based on increasing evidence showing telephone-based interventions to be cost-efficient40 and to improve symptoms and promote lifestyle changes41,42, we decided to compare the effectiveness of two modes of care delivery i.e. supervised face-to-face treatment delivery and telephone treatment delivery. This presented us with the issue of design choice i.e. a superiority or non-inferiority trial38,43. After extensive discussions, we decided to design our study as a superiority trial because we expected the multidisciplinary, face-to-face treatment program to be superior in effect since this program is more intensive and more strictly supervised44. However, based on progressive insights on clinical trial designs within our research group, a more appropriate design might have been a non-inferiority trial evaluating whether the telephone-based treatment program was inferior in effect to the face-to-face treatment program by more than a predefined non-inferiority margin43,45,46. In a superiority trial, the aim is to show that a new treatment is more effective than an existing treatment, whereas in a non-inferiority trial the aim is to show that a new treatment is no less effective than an existing treatment (but might have safety advantages or lower costs)38,45,47. In our trial, the face-to face treatment program was an already existing program given at the outpatient department (expected to be effective since the content was based on evidence-based recommendations) and the telephone-based treatment program was the newly developed, less intensive program, with expected lower costs. Therefore, in hindsight a non-inferiority design would have been a more appropriate design. Ideally, the best trial design would have been a three-arm trial including a group receiving no treatment (i.e. waiting list), a group receiving the face-to-face treatment program and a group receiving the telephone-based treatment program38,48,49. Such a design measures effect size (new treatment vs. no treatment) and allows comparison of a new treatment with active control in a setting where the comparison between active control and no treatment provides evidence of the ability of a trial to distinguish active from inactive treatment or whether the study did not work (i.e. assay sensitivity)47,48. Including a third arm would increase the sample size, but it is possible to make the group receiving no treatment smaller than the other groups as the treatment vs. no treatment difference is generally larger than the new treatment vs. active control difference38,47. This makes the trial more acceptable to patients as there is less chance of being randomized to the group receiving no treatment47.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 157
9
Definition of GOAAs previously addressed in this thesis, to date there is no clear and consistent definition for what actually constitutes GOA and a number of alternative terms have been used, such as polyarticular OA, multiple joint involvement, joint pain comorbidity or multi-joint symptoms5. Previous studies which enrolled patients based on OA in a specific joint have established that multiple joints are commonly involved in OA (especially in hip and knee OA)3-5. For example, Peruccio et al.4 showed in a knee OA cohort undergoing joint replacement surgery that 46% of patients reported ≥4 symptomatic joints, other than the surgical knee. Furthermore, the authors showed a significant influence of specific symptomatic joints on post-surgery pain and function, including the ankle/feet/toes, spine/lower back and neck. In patients with hip and knee OA, Hoogeboom et al.3 showed 58% of patients to report symptoms in more than one joint. It should be noted however, that in those studies the nature of the additional musculoskeletal complaints was unknown and might be unrelated to OA. Despite the high prevalence of multiple joint involvement in OA, research and clinical practice do not routinely consider the involvement of multiple joints, but often focus on single joint sites in isolation. As a consequence, there remains a gap in understanding the association between multiple joint involvement and clinical outcomes in patients with OA. We hypothesize that a clear and consistent definition of GOA might contribute to diminish this gap.
In the current thesis we used a pragmatic definition of GOA. At this point, we believe it is important to take a critical look at this definition. An asset of this definition is that we were one of the first to formulate a pragmatic definition of GOA from a clinical rather than a radiographic perspective that was easily applicable in daily clinical practice. Since clinical symptoms are poorly correlated with radiographic OA50 and symptoms are likely to be more important in functional outcomes, we consider it important to include clinical symptoms next to structural changes in the definition of GOA51. Furthermore, we believe that our study population adequately represents patients with GOA considering the observed patterns of joint involvement in chapter 2. We showed the combination of hand and knee OA to be most common in our patient group, which is consistent within the literature on patterns of joint involvement, showing that the hands and knees aggregate together much more often than other joints52-54. A limitation of our definition might be that we used a rather “broad” definition of GOA. We did not require a specific joint or combination of joints to be affected, whereas existing GOA definitions often define GOA by the existence/presence of hand or knee OA53,55-
57. As a consequence of our “broad” definition, we included a very heterogeneous group of patients with a broad range of problems, making individualized treatment within groups difficult. However, the little agreement on the necessity or appropriateness of including a specific joint or combination of joints in the definition of GOA makes it difficult to determine which joints should be involved in the definition of GOA. We believe the initial issue in research on GOA is to obtain international consensus on an appropriate definition of GOA

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
158 | Chapter 9
for clinical and research use, which is supported by a recently published systematic review on GOA5. The authors concluded that a uniform definition will facilitate research studies on possible risk factors of GOA and clinical trials on the effectiveness of therapy. The need for a uniform definition of GOA is also supported by a European League Against Rheumatism (EULAR) expert committee developing a research agenda comprising the most important research needs to improve OA care58. One of their research priorities was to develop criteria to diagnose and classify GOA. Consensus on the definition of GOA could be obtained by use of an international Delphi study among international experts. We further believe that a more comprehensive approach to the management and care of OA is warranted. Both researchers and clinicians in daily clinical practice should account for the involvement of multiple joints in patients with OA3,4.
GeneralizabilityFor the studies described in chapters 2, 3, 4 and 5, all included patients were recruited from two specialized outpatient rheumatology departments of the Sint Maartenskliniek, the Netherlands. The patients enrolled in our randomized clinical trial were diagnosed with GOA and referred by their rheumatologist for multidisciplinary treatment. This might have led to selection bias since we selected patients with a relatively high clinical burden as shown in chapter 2. Therefore our study population might not be representative for the general GOA population. This limited generalizability should be taken into account when interpreting the study results.
To concludeBased on the findings of this thesis, a critical look at these findings and the most recent literature on the non-pharmacological, non-surgical management of patients with OA some final conclusions can be made. We can conclude that GOA has a broad impact on the physical component of quality of life and the performance of daily activities, reflecting a high clinical burden. Furthermore, we demonstrated no differences in treatment effect between patients with GOA who followed a non-pharmacological face-to-face self-management program and those who received a telephone-based self-management program. No clinically important improvements on a range of outcome domains were observed within both treatment programs. These findings contribute to the increasing evidence of the limited benefits of self-management programs for people with OA. We hypothesize that patients with GOA might benefit more from a long-term, individually tailored, supervised treatment program combining weight loss with intensive exercises, rather than a self-management program targeting on multiple domains of daily living. Future research is needed to gain empirical evidence for this. Furthermore, measurement instruments with adequate measurement properties are needed to adequately assess physical function in patients with GOA. Yet,

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 159
9
the initial issue in research on GOA is to obtain international consensus on an appropriate definition of GOA for both clinical and research use. Such a definition might contribute to an improved understanding of the influence of multiple joint involvement on clinical outcomes in OA. We further believe that a more comprehensive approach to the management of OA is warranted. Researchers and clinicians in daily clinical practice should routinely consider the involvement of multiple joints in patients with OA.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
160 | Chapter 9
References
1. Cooper C, Egger P, Coggon D, Hart DJ, Masud T, Cicuttini F et al. Generalized osteoarthritis in women: pattern of joint involvement and approaches to definition for epidemiological studies. J.Rheumatol. 1996; 23: 1938-42
2. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011; 78: 275-8
3. Hoogeboom TJ, den Broeder AA, Swierstra BA, de Bie RA, van den Ende CH. Joint-pain comorbidity, health status, and medication use in hip and knee osteoarthritis: a cross-sectional study. Arthritis Care Res.(Hoboken.) 2012; 64: 54-8
4. Perruccio AV, Power JD, Evans HM, Mahomed SR, Gandhi R, Mahomed NN et al. Multiple joint involvement in total knee replacement for osteoarthritis: Effects on patient-reported outcomes. Arthritis Care Res.(Hoboken.) 2012; 64: 838-46
5. Nelson AE, Smith MW, Golightly YM, Jordan JM. “Generalized osteoarthritis”: A systematic review. Semin.Arthritis Rheum. 2014; 43(6):713-20
6. Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: The Chronic Osteoarthritis Management Initiative of the U.S. Bone and Joint Initiative. Semin.Arthritis Rheum. 2014; 43(6):701-12
7. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis.Cartilage. 2008; 16: 137-62
8. Peter WF, Dekker J, Tilbury C, Tordoir RL, Verdegaal SH, Onstenk R et al. The association between comorbidities and pain, physical function and quality of life following hip and knee arthroplasty. Rheumatol Int 2015 [Epub ahead of print]
9. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis.Cartilage. 2014; 22: 363-88
10. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis.Cartilage. 2007; 15: 981-1000
11. Bruce B, Fries JF. The Stanford Health Assessment Questionnaire: dimensions and practical applications. Health Qual.Life Outcomes. 2003; 1: 20
12. Kloppenburg M. Hand osteoarthritis-nonpharmacological and pharmacological treatments. Nat.Rev.Rheumatol 2014; 10: 242-51
13. Kroon FP, van der Burg LR, Buchbinder R, Osborne RH, Johnston RV, Pitt V. Self-management education programmes for osteoarthritis. Cochrane.Database.Syst.Rev. 2014; 1: CD008963
14. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann.Rheum.Dis. 2013; 72: 1125-35
15. Zhang W, Nuki G, Moskowitz RW, Abramson S, Altman RD, Arden NK et al. OARSI recommendations for the management of hip and knee osteoarthritis: part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis.Cartilage. 2010; 18: 476-99
16. Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes.Rev. 2014; 15: 578-86
17. Maly MR, Robbins SM. Osteoarthritis Year in Review 2014: rehabilitation and outcomes. Osteoarthritis.Cartilage. 2014; 22: 1958-88
18. Messier SP, Mihalko SL, Legault C, Miller GD, Nicklas BJ, DeVita P et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. JAMA 2013; 310: 1263-73
19. Messier SP, Loeser RF, Miller GD, Morgan TM, Rejeski WJ, Sevick MA et al. Exercise and

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary and general discussion | 161
9
dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis Rheum. 2004; 50: 1501-10
20. Paans N, van dA-S, I, Dilling RG, Bos M, van der Meer K, Bulstra SK et al. Effect of exercise and weight loss in people who have hip osteoarthritis and are overweight or obese: a prospective cohort study. Phys.Ther. 2013; 93: 137-46
21. Mohr DC, Siddique J, Ho J, Duffecy J, Jin L, Fokuo JK. Interest in behavioral and psychological treatments delivered face-to-face, by telephone, and by internet. Ann.Behav.Med. 2010; 40: 89-98
22. Tijhuis GJ, Zwinderman AH, Hazes JM, van den Hout WB, Breedveld FC, Vliet Vlieland TP. A randomized comparison of care provided by a clinical nurse specialist, an inpatient team, and a day patient team in rheumatoid arthritis. Arthritis Rheum. 2002; 47: 525-31
23. Vliet Vlieland TP. Multidisciplinary team care and outcomes in rheumatoid arthritis. Curr.Opin.Rheumatol 2004; 16: 153-6
24. Petersson IF, Bremander A, Klareskog L, Stenström CH. Who Cares about Team Care? Conference report from CARE II Spenshult, Sweden, September 18 - 20, 2003.
25. van den Hout WB, Tijhuis GJ, Hazes JM, Breedveld FC, Vliet Vlieland TP. Cost effectiveness and cost utility analysis of multidisciplinary care in patients with rheumatoid arthritis: a randomised comparison of clinical nurse specialist care, inpatient team care, and day patient team care. Ann.Rheum.Dis. 2003; 62: 308-15
26. Vliet Vlieland TP, Li LC, MacKay C, Badley EM. Does everybody need a team? J.Rheumatol 2006; 33: 1897-9
27. Hoffmann TC, Erueti C, Glasziou PP. Poor description of non-pharmacological interventions: analysis of consecutive sample of randomised trials. BMJ 2013; 347: f3755
28. O’Donnell S, Li LC, King J, Lauzon C, Finn H, Vliet Vlieland TP. Development of a framework for reporting health service models for managing rheumatoid arthritis. Clin Rheumatol 2010; 29: 151-65
29. Moe RH, Haavardsholm EA, Grotle M, Steen E, Kjeken I, Hagen KB et al. Development of a brief multidisciplinary education programme for patients with osteoarthritis.
BMC.Musculoskelet.Disord. 2011; 12: 257 30. Hoogeboom TJ, Oosting E, Vriezekolk JE,
Veenhof C, Siemonsma PC, de Bie RA et al. Therapeutic validity and effectiveness of preoperative exercise on functional recovery after joint replacement: a systematic review and meta-analysis. PLoS.One. 2012; 7: e38031
31. Hammond A, Young A, Kidao R. A randomised controlled trial of occupational therapy for people with early rheumatoid arthritis. Ann.Rheum.Dis. 2004; 63: 23-30
32. Karsdorp PA, Vlaeyen JW. Active avoidance but not activity pacing is associated with disability in fibromyalgia. Pain 2009; 147: 29-35
33. Veenhof C, Bijlsma JW, van den Ende CH, van Dijk GM, Pisters MF, Dekker J. Psychometric evaluation of osteoarthritis questionnaires: a systematic review of the literature. Arthritis Rheum. 2006; 55: 480-92
34. Sun Y, Sturmer T, Gunther KP, Brenner H. Reliability and validity of clinical outcome measurements of osteoarthritis of the hip and knee--a review of the literature. Clin Rheumatol 1997; 16: 185-98
35. Peter WFH, Jansen MJ, Bloo H, Dekker-Bakker LMMCJ, Dilling RG, Hilberdink WKHA et al. KNGF guideline for Physical Therapy in patients with Osteoarthritis of the hip and knee. Supplement to the Dutch Journal of Physical Therapy 2010; 120 (1)
36. Duncan EA, Murray J. The barriers and facilitators to routine outcome measurement by allied health professionals in practice: a systematic review. BMC.Health Serv.Res. 2012; 12: 96
37. Swinkels RA, van Peppen RP, Wittink H, Custers JW, Beurskens AJ. Current use and barriers and facilitators for implementation of standardised measures in physical therapy in the Netherlands. BMC.Musculoskelet.Disord. 2011; 12: 106
38. Streiner DL. Alternatives to placebo-controlled trials. Can.J.Neurol.Sci. 2007; 34 Suppl 1: S37-S41
39. Splawinski J, Kuzniar J. Clinical trials: active control vs placebo--what is ethical? Sci.Eng Ethics 2004; 10: 73-9
40. Weinberger M, Tierney WM, Cowper PA, Katz BP, Booher PA. Cost-effectiveness of increased telephone contact for patients with osteoarthritis. A randomized, controlled trial. Arthritis Rheum. 1993; 36: 243-6

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
162 | Chapter 9
41. Eakin E, Reeves M, Winkler E, Lawler S, Owen N. Maintenance of physical activity and dietary change following a telephone-delivered intervention. Health Psychol. 2010; 29: 566-73
42. Goode AD, Reeves MM, Eakin EG. Telephone-delivered interventions for physical activity and dietary behavior change: an updated systematic review. Am.J.Prev.Med. 2012; 42: 81-8
43. Landewe RB, Smolen JS, Weinblatt ME, Emery P, Dougados M, Fleischmann R et al. Can we improve the performance and reporting of investigator-initiated clinical trials? Rheumatoid arthritis as an example. Ann.Rheum.Dis. 2014; 73: 1755-60
44. Hoogeboom TJ, Stukstette MJ, de Bie RA, Cornelissen J, den Broeder AA, van den Ende CH. Non-pharmacological care for patients with generalized osteoarthritis: design of a randomized clinical trial. BMC.Musculoskelet.Disord. 2010; 11: 142
45. Points to consider on switching between superiority and non-inferiority. Br.J.Clin Pharmacol. 2001; 52: 223-8
46. Wiens BL. Choosing an equivalence limit for noninferiority or equivalence studies. Control Clin Trials 2002; 23: 2-14
47. ICH E10. Choice of Control Group in Clinical Trials. (CPCM/ICH/364/396). European Agency for the Evaluation of Medicinal Products, London, 2000
48. Temple R, Ellenberg SS. Placebo-controlled trials and active-control trials in the evaluation of new treatments. Part 1: ethical and scientific issues. Ann.Intern.Med. 2000; 133: 455-63
49. D’Agostino RB, Sr., Massaro JM, Sullivan LM. Non-inferiority trials: design concepts and issues - the encounters of academic consultants in statistics. Stat.Med. 2003; 22: 169-86
50. Bedson J, Croft PR. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the
literature. BMC.Musculoskelet.Disord. 2008; 9: 116
51. Nelson AE, Elstad E, Devellis RF, Schwartz TA, Golightly YM, Renner JB et al. Composite measures of multi-joint symptoms, but not of radiographic osteoarthritis, are associated with functional outcomes: the Johnston County Osteoarthritis Project. Disabil.Rehabil. 2014; 36: 300-6
52. Bijsterbosch J, Meulenbelt I, Watt I, Rosendaal FR, Huizinga TW, Kloppenburg M. Clustering of hand osteoarthritis progression and its relationship to progression of osteoarthritis at the knee. Ann.Rheum.Dis. 2014; 73: 567-72
53. Haugen IK. The puzzle of generalized osteoarthritis (OA) -- is OA a systemic enthesopathy? J.Rheumatol. 2012; 39: 203-5
54. Hirsch R, Lethbridge-Cejku M, Scott WW, Jr., Reichle R, Plato CC, Tobin J et al. Association of hand and knee osteoarthritis: evidence for a polyarticular disease subset. Ann.Rheum.Dis. 1996; 55: 25-9
55. Carroll GJ, Breidahl WH, Jazayeri J. Confirmation of two major polyarticular osteoarthritis (POA) phenotypes--differentiation on the basis of joint topography. Osteoarthritis.Cartilage. 2009; 17: 891-5
56. Dougados M, Nakache JP, Gueguen A. Criteria for generalized and focal osteoarthritis. Rev.Rhum.Engl.Ed 1996; 63: 569-75
57. Gunther KP, Sturmer T, Sauerland S, Zeissig I, Sun Y, Kessler S et al. Prevalence of generalised osteoarthritis in patients with advanced hip and knee osteoarthritis: the Ulm Osteoarthritis Study. Ann.Rheum.Dis. 1998; 57: 717-23
58. Conaghan PG, Kloppenburg M, Schett G, Bijlsma JW. Osteoarthritis research priorities: a report from a EULAR ad hoc expert committee. Ann.Rheum.Dis. 2014; 73(8):1442-5

Nederlandse samenvatting

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
164 | Nederlandse samenvatting

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Nederlandse samenvatting | 165
&
Hoofdstuk 1: inleidingArtrose is de meest voorkomende chronische gewrichtsaandoening. In wetenschappelijk onderzoek en in de klinische praktijk wordt vaak uitgegaan van een mono-articulaire benadering van artrose, terwijl bij artrose vaak meerdere gewrichten tegelijkertijd zijn aangedaan. Behalve de knieën of heupen zijn de handen en de gewrichten van de wervelkolom relatief vaak aangedaan. Een term die veelvuldig gebruikt wordt om artrose in meerdere gewrichten tegelijkertijd te beschrijven is gegeneraliseerde artrose (GOA). Echter, een systematisch literatuuronderzoek liet zien dat er tot op heden geen eenduidige definitie van GOA bekend is. In dit proefschrift wordt GOA als volgt gedefinieerd:
- Klachten aan tenminste 3 gewrichtsgroepen én - Objectieve artrotische afwijkingen aan tenminste 2 gewrichtsgroepen
Prevalentiecijfers van GOA zijn beperkt en inconsistent. Verschillende studies suggereren dat in cohorten van artrose van de heup en/of knie een relatief grote groep patiënten (tot 50%) geclassificeerd kan worden als GOA. Desondanks is er nog weinig bekend over de impact van GOA op het dagelijks functioneren en kwaliteit van leven. De belangrijkste symptomen van GOA zijn pijn, stijfheid, verlies van functie en een verminderde kwaliteit van leven. Momenteel bestaat er nog geen curatieve behandeling voor artrose. Niet-medicamenteuze behandelopties zijn daarom veelal gericht op het verlichten van symptomen, het verbeteren van functioneren en het leren omgaan met de aandoening. Tot op heden is de niet-medicamenteuze behandeling van artrose vrijwel exclusief gericht op mensen met artrose van de heup, knie of hand. Dit geldt ook voor wetenschappelijke studies: er is tot nu toe nauwelijks wetenschappelijk bewijs voor de effectiviteit van niet-medicamenteuze interventies voor mensen met GOA. De belangrijkste doelen van dit proefschrift waren het verkrijgen van inzicht in de impact van GOA op het dagelijks functioneren en kwaliteit van leven en daarnaast de evaluatie van de (kosten)effectiviteit van twee niet-medicamenteuze behandelprogramma’s voor mensen met GOA.
Hoofdstuk 2: de impact van GOA op het dagelijks functioneren en kwaliteit van levenIn deze studie hebben we de impact van GOA op het dagelijks functioneren en kwaliteit van leven onderzocht. In totaal hebben 147 patiënten gediagnosticeerd met GOA door een reumatoloog en verwezen naar multidisciplinaire zorg een set gestandaardiseerde vragenlijsten ingevuld. De resultaten lieten zien dat de handen en knieën het vaakst waren aangedaan. De patiënten ervoeren matig tot ernstige beperkingen in het uitvoeren van dagelijkse activiteiten in een breed spectrum aan activiteiten. Met name activiteiten gerelateerd aan mobiliteit en huishoudelijke activiteiten werden frequent genoemd, met als belangrijkste beperkende activiteit lopen. Daarnaast was de kwaliteit van leven verminderd, met name de fysieke component. Deze studieresultaten suggereren dat de fysieke component van de kwaliteit van leven en activiteiten gerelateerd aan mobiliteit belangrijke aangrijpingspunten zijn voor

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
166 | Nederlandse samenvatting
niet-medicamenteuze interventies voor mensen met GOA. Gezien het brede spectrum aan belangrijke functionele beperkingen is het van belang dat interventies afgestemd worden op de individuele problemen van de patiënt.
Hoofdstuk 3: effectiviteit niet-medicamenteuze behandeling GOAWe hebben een gerandomiseerde, enkelvoudige geblindeerde pragmatische trial uitgevoerd waarin we de effectiviteit van twee niet-medicamenteuze interventies voor mensen met GOA hebben vergeleken tot 1 jaar na de start van de behandeling. In totaal werden 147 patiënten gerandomiseerd in ofwel een 6 weken durende multidisciplinaire face-to-face groepsbehandeling bestaande uit 7 groepssessies of een 6 weken durende telefonische behandeling bestaande uit 2 groepssessies gecombineerd met 4 individuele telefonische contactmomenten. De belangrijkste doelen van beide behandelprogramma’s waren het verbeteren van het dagelijks functioneren en het verbeteren van zelfmanagement vaardigheden om beter om te gaan met de gevolgen van GOA. De hypothese was dat de face-to-face behandeling effectiever was in het verbeteren van het dagelijks functioneren gezien de hogere intensiteit, groepsinteractie en supervisie. De belangrijkste uitkomstmaat van de studie was dagelijks functioneren gemeten met de HAQ-DI op baseline, 6, 26 en 52 weken. Secundaire uitkomstmaten waren onder andere pijn, vermoeidheid, zelf-effectiviteit en acceptatie. We vonden in deze studie geen verschillen in effectiviteit tussen beide behandelprogramma’s op geen van de uitkomstmaten, behalve voor pijn na 1 jaar; de face-to-face behandeling was effectiever in het verminderen van pijn dan de telefonische behandeling. Binnen de groepen vonden we kleine, significante verbeteringen op verschillende uitkomstmaten, maar deze verbeteringen waren niet klinisch relevant. Een interessante bevinding was dat deelnemers meer tevreden waren over de face-to-face behandeling.
Hoofdstuk 4: welk behandelprogramma is kosteneffectief?Voor beleidsmakers is het van belang dat klinische evaluaties van nieuwe therapieën of technologieën gepaard gaan met economische evaluaties. Om deze reden hebben wij vanuit een maatschappelijk perspectief een kosten-effectiviteitsanalyse gedaan waarin we de kosten en effectiviteit van bovengenoemde behandelprogramma’s met elkaar hebben vergeleken. Naast de kosten voor de behandelprogramma’s, hebben we gedurende een jaar alle directe medische en niet-medische kosten als gevolg van GOA gemeten met behulp van vragenlijsten die werden afgenomen op baseline, 6, 13, 26, 39 en 52 weken. Daarnaast hebben we op drie verschillende manieren kwaliteit van leven (en dus utiliteiten) gemeten. De totale maatschappelijke kosten (over één jaar) van de telefonische behandeling waren hoger dan die van de face-to-face behandeling, echter dit verschil was niet significant. De resultaten van deze kosteneffectiviteit analyses toonden dat de face-to-face behandeling een grotere kans had om kosteneffectief te zijn dan de telefonische behandeling.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Nederlandse samenvatting | 167
&
Hoofdstuk 5: klinimetrische eigenschappen HAQ-DIEén van de belangrijkste consequenties van GOA is een vermindering van het dagelijks functioneren. Voor zowel onderzoekers als clinici is het van belang dat het dagelijks functioneren van mensen met GOA valide en betrouwbaar kan worden gemeten. Tot op heden zijn er geen specifieke zelf-gerapporteerde vragenlijsten beschikbaar om het dagelijks functioneren te meten in deze patiënten groep. Artrose specifieke vragenlijsten voor het meten van het dagelijks functioneren zijn beschikbaar, maar deze richten zich op de onderste extremiteiten en zijn daarom niet geschikt voor mensen met GOA aangezien deze groep patiënten beperkingen ervaart in activiteiten van zowel de bovenste als onderste extremiteiten. De Health Assessment Questionnaire Disability Index (HAQ-DI) bevat activiteiten van zowel de bovenste als onderste extremiteiten. Om deze reden hebben we de HAQ-DI als primaire uitkomstmaat gekozen om dagelijks functioneren te meten in onze trial. In dit hoofdstuk hebben we de psychometrische eigenschappen (interpreteerbaarheid, validiteit, betrouwbaarheid en responsiviteit) van de HAQ-DI geëvalueerd. De resultaten lieten zien dat de HAQ-DI vloer- en plafondeffecten heeft. Daarnaast was de content validiteit beperkt aangezien de HAQ-DI activiteiten bevat die niet relevant of te makkelijk uitvoerbaar zijn voor mensen met GOA. De construct validiteit en betrouwbaarheid waren goed. Echter, de responsiviteit was beperkt. Gezien de beperkte content validiteit adviseren wij de items van de HAQ-DI te actualiseren om in de toekomst dagelijks functioneren te meten bij mensen met GOA. Deze actualisatie is hoogstwaarschijnlijk ook relevant voor andere reumatische aandoeningen.
Hoofdstuk 6: welke vragenlijst is het meest responsief? In tegenstelling tot GOA, zijn er voor het meten van het dagelijks functioneren bij mensen met knie artrose verschillende valide en betrouwbare vragenlijsten beschikbaar. Voor het monitoren van patiënten of het evalueren van de effectiviteit van interventies is het van belang dat verandering in dagelijks functioneren adequaat gemeten kan worden. Het meten van verandering wordt ook wel responsiviteit genoemd. In deze studie vergelijken we de responsiviteit van vier veelgebruikte vragenlijsten om dagelijks functioneren te meten bij mensen met knie artrose: 1.) the Western Ontario and McMaster University Osteoarthritis Index subscale physical function (WOMAC-PF), 2.) the Lequesne Algofunctional index (LAI), 3.) the Lower Extremity Functional Scale (LEFS) and 4.) the short measure of the Knee disability en Osteoarthritis Outcome Score (KOOS-PS). We hebben de responsiviteit van deze vragenlijsten gemeten en vergeleken door het opstellen van hypotheses over verwachtte correlaties tussen veranderingen in dagelijks functioneren en veranderingen in andere gerelateerde en niet gerelateerde constructen (zoals pijn, mentaal functioneren, acceptatie). Wanneer >75% van de hypotheses kon worden bevestigd was er sprake van een goede responsiviteit. Een expertgroep bestaande uit onderzoekers, epidemiologen,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
168 | Nederlandse samenvatting
fysiotherapeuten en een reumatoloog formuleerden 15 hypotheses. Voor de WOMAC-PF konden 12 van de 15 hypotheses (80%) bevestigd worden, voor de LAI, LEFS en KOOS-PS konden respectievelijk 9 (60%), 11 (73%) en 11 (73%) hypotheses bevestigd worden. Deze resultaten suggereren dat de WOMAC-PF superieur is in het meten van veranderingen in dagelijks functioneren in patiënten met knie artrose.
Hoofdstuk 7: percepties van patiënten over de “Zorgwijzer Artrose” Om de niet-medicamenteuze zorg voor mensen met heup en knie artrose te optimaliseren, heeft onze onderzoeksgroep een behandelstrategie voor heup en knie artrose geïmplementeerd in een regio in Nederland. Deze implementatie richtte zich ook op patiënten gezien hun belangrijke rol in de behandeling van artrose. Om deze reden is er een patiëntvriendelijk zelfmanagementboekje ontwikkeld, de “Zorgwijzer Artrose ©”. Het doel van deze zorgwijzer was om patiënten te informeren over artrose en de behandelmogelijkheden, een actieve rol van patiënten bij hun behandeling te stimuleren en de communicatie tussen de patiënt en zorgverleners te verbeteren. De meningen van 17 patiënten ten aanzien van de inhoud en het gebruik van deze zorgwijzer werden bestudeerd in een kwalitatieve studie met semigestructureerde interviews. Hierbij werden patiënt-gerapporteerde barrières en faciliterende factoren om de zorgwijzer te gebruiken geïdentificeerd en onderverdeeld in de volgende thema’s: 1.) de rol van zorgverleners, 2.) de perceptie van patiënten ten aanzien van artrose en de behandelmogelijkheden en 3.) de perceptie van patiënten ten aanzien van het nut van het boekje en het krijgen van informatie. In het eerste thema werd ‘het gebrek aan aanmoediging van de zorgverleners’ geïdentificeerd als barrière om de zorgwijzer te gebruiken. Tevens gaven patiënten aan dat zij twijfelden of hun zorgverleners niet-medicamenteuze behandelopties onderschreven. In het tweede thema werden de volgende cognities geïdentificeerd als barrières om de zorgwijzer te gebruiken: ‘artrose is niet te behandelen’ en ‘een proactieve houding is niet belangrijk tijdens de behandeling’. De cognitie ‘een proactieve houding draagt bij aan een goede uitkomst’ was tevens een faciliterende factor om de zorgwijzer wel te gebruiken. In het derde thema werden ‘de perceptie dat de zorgwijzer nuttig is’ en ‘de behoefte om geïnformeerd te worden’ zowel als barrière en faciliterende factor geïdentificeerd om de zorgwijzer te gebruiken.
Hoofdstuk 8: wat is energie verdelen?“Energie verdelen” is een belangrijk component van zelfmanagement interventies voor mensen met een reumatische aandoening om pijn en vermoeidheid te verminderen. Echter, zowel in de literatuur als in de klinische praktijk bestaat er grote variatie in de beschrijving van energie verdelen. Om deze reden hebben wij een internationale werkgroep opgezet en een internationale Delphi studie uitgevoerd. In 4 rondes hebben wij 60 onderzoekers, paramedici en/of reumatologen afkomstig uit 12 verschillende landen en deskundig op het

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Nederlandse samenvatting | 169
&
gebied van energie verdelen gevraagd naar de belangrijkste doelen, gedragingen, strategieën en contextuele factoren van energie verdelen. Dit resulteerde in een “consensual list” met daarin 9 doelen, 11 gedragingen, 9 strategieën en 10 contextuele factoren. Paramedici kunnen deze lijst gebruiken om samen met de patiënt de meest relevante aspecten te selecteren voor een interventie op maat. De resultaten van deze studie dragen bij aan het verkrijgen van transparantie en homogeniteit in het concept energie verdelen in wetenschappelijk onderzoek en in de klinische praktijk.
Hoofdstuk 9: discussie In dit hoofdstuk worden de belangrijkste resultaten van de onderzoeken besproken en bediscussieerd. Ook worden er een aantal implicaties voor de klinische praktijk en suggesties voor verder onderzoek aangegeven.
Onze gerandomiseerde trial liet zien dat er geen verschil in effectiviteit was tussen een multidisciplinaire face-to-face groepsbehandeling en een telefonische behandeling (behalve voor pijn) voor mensen met GOA. Binnen de groepen zagen we kleine verbeteringen op verschillende domeinen die niet klinisch relevant waren. Hiervoor kunnen een aantal mogelijke verklaringen worden gegeven. Ten eerste, goal setting was een belangrijk component in onze behandelprogramma’s. Patiënten werden tijdens de start van de behandeling gevraagd individuele doelen te formuleren die werden gemonitord en bediscussieerd tijdens de behandeling. Omdat GOA kan leiden tot een breed spectrum aan beperkingen ontstond er een grote variatie aan individuele doelen. Hierdoor richtten de behandelprogramma’s zich op veel verschillende dimensies zoals pijn, vermoeidheid, acceptatie, lichamelijke activiteit en sociale ondersteuning. Een gevolg hiervan zou kunnen zijn dat het voor individuele patiënten moeilijk was om voor hen relevante informatie te selecteren. Daarnaast kan het zo zijn dat onze verwachtingen te hoog waren. We verwachtte dat een combinatie van niet-medicamenteuze interventies bewezen effectief bij artrose van de heup en knie ook bij GOA effectief zouden zijn. Echter, aangezien meerdere studies laten zien dat GOA (of multiple joint involvement) een grotere impact heeft op klinische uitkomsten dan artrose aan één gewricht, is het aannemelijk dat patiënten met GOA een intensievere en complexere interventie nodig hebben.
De kleine verbeteringen van onze behandelprogramma’s zijn vergelijkbaar met resultaten van de effectiviteit van zelfmanagement interventies beschreven in de literatuur. Recent laat een systematisch literatuuronderzoek zien dat de effecten van zelfmanagement interventies voor mensen met artrose erg klein zijn. In de literatuur groeit de consensus over de combinatie van intensief oefenen en gewrichtsverlies als belangrijkste behandeling voor mensen met artrose. Op basis van de bevindingen in dit proefschrift en de recente literatuur suggereren wij dat we wellicht meer moeten focussen op intensief oefenen gecombineerd met gewichtsverlies gedurende een langere periode in plaats van zelfmanagement interventies

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
170 | Nederlandse samenvatting
gericht op een breed scala aan domeinen. Onderzoek is nodig om dit aan te tonen. Daarnaast is er onderzoek nodig naar vragenlijsten die op een adequate manier dagelijks functioneren kunnen meten bij mensen met GOA. Bovenal is echter belangrijk dat er internationale consensus wordt bereikt over een uniforme definitie van GOA zodat er meer systematisch en reproduceerbaar (effectiviteits)onderzoek kan worden verricht naar deze aandoening die gekenmerkt wordt door een grote ziektelast.

List of publications

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
172 | List of publications

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
List of publications | 173
&
International publications
Cuperus N, Hoogeboom T.J, Neijland Y, van den Ende C.H.M, Keijsers N.L.W. Are people with rheumatoid arthritis who undertake activity pacing at risk of being too physically inactive? Clinical Rehabilitation 2012; 26(11): 1048-1052.
Cuperus N, Smink A.J, Bierma-Zeinstra S.M.A, Dekker J, Schers H.J, de Boer F, van den Ende C.H.M, Vliet Vlieland T.P.M. Patients’ perceptions of a self-management booklet for hip or knee osteoarthritis: A qualitative interview study. BMC family practice 2013; 14(1): 181.
Cuperus N, Mahler E.A.M, Vliet Vlieland T.P.M, Hoogeboom T.J, van den Ende C.H.M. Measurement properties of the Health Assessment Questionnaire Disability Index for generalized osteoarthritis. Rheumatology (Oxford). 2015; 54(5): 821-826.
Cuperus N, Vliet Vlieland T.P.M, Mahler E.A.M, Kersten C.C, Hoogeboom T.J, van den Ende C.H.M. The clinical burden of generalized osteoarthritis represented by self-reported health-related quality of life and activity limitations: a cross-sectional study. Rheumatology International 2015; 35(5): 871-877.
Cuperus N, Hoogeboom T.J, Kersten C.C, den Broeder A.A, Vliet Vlieland T.P.M, van den Ende C.H.M. Randomized trial of the effectiveness of a non-pharmacological multidisciplinary face-to-face treatment program on daily function compared to a telephone-based treatment program in patients with generalized osteoarthritis. Osteoarthritis & Cartilage. 2015. DOI: 10.1016/j.joca.2015.04.007. [Epub ahead of print].
Conference abstracts
Cuperus N, Hoogeboom T.J, Neijland Y, van den Ende C.H.M, Keijsers N.L.W. Energie verdelen bij patiënten met reumatoïde artritis: een risico op inactiviteit? Fysio Congres Maastricht, 2012 [Oral presentation].
Cuperus N, Vliet Vlieland T.P.M, van den Ende C.H.M. Functional limitations in patients with generalized osteoarthritis. EULAR congress Madrid, Spain, 2013 [Poster presentation].
Cuperus N, Smink A.J, Bierma-Zeinstra S.M.A, Dekker J, Schers H.J, de Boer F, van den Ende C.H.M, Vliet Vlieland T.P.M. Patients’ perceptions of a self-management booklet for hip or knee osteoarthritis: A qualitative interview study. EULAR congress Madrid, Spain, 2013 [Poster tour].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
174 | List of publications
Cuperus N, Vliet Vlieland T.P.M, Mahler E.A.M, Kersten C.C, Hoogeboom T.J, van den Ende C.H.M. The clinical burden of generalized osteoarthritis represented by activity limitations and health related quality of life: a cross-sectional study. ACR congress San Diego, USA, 2013 [Oral presentation].
Cuperus N, Hoogeboom T.J, Neijland Y, van den Ende C.H.M, Keijsers N.L.W. Are people with rheumatoid arthritis who undertake activity pacing at risk of being too physically inactive? Rheumatology Care congress Rotterdam, the Netherlands, 2013 [Oral presentation].
Cuperus N, Vliet Vlieland T.P.M, Mahler E.A.M, Kersten C.C, Rietveld L, den Broeder A.A, Hoogeboom T.J, van den Ende C.H.M. Randomised comparison of the effectiveness of a non-pharmacological multidisciplinary group-based treatment program vs. a telephone-delivered program on daily function in patients with generalized osteoarthritis. EULAR congress Paris, France, 2014 [Oral presentation].
Cuperus N, Mahler E.A.M, Vliet Vlieland T.P.M, Hoogeboom T,J, van den Ende C.H.M. Measurement properties of the Health Assessment Questionnaire Disability Index (HAQ-DI) in patients with generalized osteoarthritis (GOA). EULAR congress Paris, France, 2014 [Poster tour].
Cuperus N, Vliet Vlieland T.P.M, Mahler E.A.M, Kersten C.C, Rietveld L, den Broeder A.A, Hoogeboom T.J, van den Ende C.H.M. Randomised comparison of the effectiveness of a non-pharmacological multidisciplinary group-based treatment program vs. a telephone-delivered program on daily function in patients with generalized osteoarthritis. ACR congress, Boston USA, 2014 [Oral presentation].
Cuperus N, Mahler E.A.M, Vliet Vlieland T.P.M, Hoogeboom T.J, van den Ende C.H.M. Measurement Properties of the Health Assessment Questionnaire Disability Index (HAQ-DI) in Patients with Generalized Osteoarthritis. ACR congress, Boston USA, 2014 [Oral presentation].
Cuperus N, Vliet Vlieland T.P.M, Brodin N, Hammond A, Kjeken I, Lund H, Murphy S, Neijland Y, Opava C.H, Roškar S, Sargautyte R, Stamm T, Torres Mata X, Uhlig T, Zangi H, van den Ende C.H.M. How do we perceive activity pacing in rheumatology care? An international Delphi survey. EULAR congress Rome, Italy, 2015 [Oral presentation].

About the author

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
176 | About the author

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
About the author | 177
&
Nienke Cuperus werd op 25 november 1986 geboren te Apeldoorn. Na het behalen van haar VWO diploma aan de Heemgaard te Apeldoorn begon ze in 2005 met de studie Bewegingswetenschappen aan de Vrije Universiteit te Amsterdam. In 2009 behaalde ze haar diploma. In 2010 begon ze als onderzoeksassistent bij het Reumacentrum van de Sint Maartenskliniek te Nijmegen. Toen de mogelijkheid ontstond voor het starten van een eigen promotietraject, begon zij als junior onderzoeker in 2011 aan haar eigen promotie onderzoek begeleid door Dr. Els van den Ende, Prof. dr. Thea Vliet Vlieland, Prof. dr. Frank van den Hoogen en Dr. Thomas Hoogeboom, waarvan het huidige proefschrift het resultaat is.
Nienke Cuperus was born on November 25, 1986 in Apeldoorn, the Netherlands. After graduating secondary school in 2005, she started to study Human Movement Sciences at the VU University Medical Centre Amsterdam. She graduated in 2009. In 2010, she started working as a research assistant at the department of Rheumatology of the Sint Maartenskliniek in Nijmegen, the Netherlands. Shortly after that, she started her PhD project under supervision of Dr. Els van den Ende, Prof. dr. Thea Vliet Vlieland, Prof. dr. Frank van den Hoogen and Dr. Thomas Hoogeboom. The studies that resulted from this work are presented in this thesis.


Dankwoord

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
180 | Dankwoord

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord | 181
&
Yes, mijn proefschrift is klaar! Vier intensieve jaren werk zit nu gebundeld in dit boekwerk, ik ben dan ook bijzonder trots op het eindresultaat. In dit laatste hoofdstuk wil ik heel graag iedereen bedanken die op welke wijze dan ook een bijdrage heeft geleverd aan dit proefschrift. Daarnaast wil ik graag een aantal mensen in het bijzonder noemen.
Allereerst mijn copromotor en dagelijks begeleider Dr. Els van den Ende. Els, ik heb zoveel van je geleerd. Bedankt voor het vertrouwen dat je in me had om als beginnende onderzoeker het project van Thomas over te nemen. Dankzij jouw gedegen kennis van onderzoek, betrokkenheid en begeleiding is dit proefschrift tot stand gekomen en heb ik me kunnen ontwikkelen tot de onderzoeker die ik nu ben. Ik wil je hier heel erg voor bedanken!
Thomas, wat begon als “jouw” project is uiteindelijk “ons” project geworden. Ik vond het ontzettend leuk dat je mijn tweede copromotor werd. Bedankt voor je grote betrokkenheid, enthousiasme en je zeer snelle reacties op mijn e-mails. Het was nooit erg om jouw feedback te lezen, naast dat het altijd zeer nuttig was, maakte je me vaak aan het lachen met je enthousiasme en grappige opmerkingen. Ik wil er hier graag één citeren: “het was niet de bedoeling dat jouw voorkant gaver zou zijn dan die van mij”. Bedankt en wie weet werken we in de toekomst nog eens samen.
Graag wil ik mijn promotoren Prof. dr. Thea Vliet Vlieland en Prof. dr. Frank van den Hoogen bedanken. Beste Thea, mede dankzij jouw betrokkenheid, gedegen kennis van het vakgebied en zeer waardevolle feedback is dit proefschrift tot stand gekomen. Tijdens onze overleggen (in Leiden, telefonisch en in de trein) had jij vaak net weer een andere visie waardoor ik werd uitgedaagd om het artikel nog beter te maken (wat dan ook lukte). Ik heb hier enorm veel van geleerd en ik ben je hier dan ook erg dankbaar voor. Beste Frank, bedankt voor de mogelijkheid om als jonge onderzoeker binnen het reumacentrum van de Sint Maartenskliniek te werken aan mijn promotie. Ik ben erg trots dat ik één van jouw eerste promovendi mag zijn.
De leden van de manuscriptcommissie bestaande uit Prof. dr. M.W.G. Nijhuis-van der Sanden, Prof. dr. C. Veenhof en Prof. dr. A.E.R.C.H. Boonen wil ik graag erg bedanken voor hun geïnvesteerde tijd in het beoordelen van mijn proefschrift.
Dan wil ik natuurlijk mijn collega’s van de Sint Maartenskliniek bedanken. Ik heb hier een ontzettend leerzame en leuke tijd gehad. Een aantal collega’s wil ik graag in het bijzonder noemen. Dicky, je was mijn eerste kamergenoot en zorgde ervoor dat ik me al snel op mijn gemak voelde binnen ReumaResearch, bedankt hiervoor! Lieve Agnes, wat waren we een goed team. Samen hebben we er voor gezorgd dat het BART project een mooi project is geworden. Ik heb veel van je geleerd, maar ik wil je vooral bedanken voor het feit dat je zo’n fijne collega was! Wat mij betreft zetten we onze “eetdates” voort en wie weet worden we ooit nog eens collega’s. Lieve Hanneke, ik wens je heel erg veel succes met de laatste loodjes van je promotie, je bent er bijna (als je de token nog eens nodig hebt dan hoor ik het wel). Joke, wat fijn dat ik altijd even bij je naar binnen kon lopen, voor inhoudelijke vragen, maar ook om gewoon even bij te kletsen. Onze carpool afspraken vond ik altijd erg gezellig. Ellen,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
182 | Dankwoord
Vera en Michiel, bedankt voor de fijne samenwerking en gezelligheid, ik wens jullie heel erg veel succes met jullie projecten. Lieve Aniek, ook al waren we maar heel kort kamergenootjes, ik vond het ontzettend gezellig. Ik wens je heel veel succes met je eigen promotietraject en ik weet zeker dat jullie een leuk huis gaan vinden. Noortje, ik vond het heel erg leuk om samen de ACR te bezoeken, eerst met z’n tweetjes in San Diego en daarna in Boston met Nienke en Alfons. Clarinda en Leonie, bedankt voor jullie enorme inzet rondom de zorgpaden en de ontzettend fijne samenwerking. Elien, bedankt voor je betrokkenheid bij een aantal van mijn artikelen, ik weet zeker dat ons artikel terecht komt in een mooi tijdschrift. Verder wil ik graag Wilbert en Fijgje bedanken voor een fijne samenwerking. Tot slot, lieve Linda, de laatste 1,5 jaar van ons promotietraject hebben we als kamergenootjes lief en leed met elkaar gedeeld. Wat heerlijk dat we samen konden klagen over de laatste zware loodjes van het promoveren. Maar vooral de leuke momenten blijven me bij, zoals onze tripjes naar Madrid en Parijs en natuurlijk jouw bruiloft (tijdens de voorbereidingen was ik diegene die de meeste details kende). Het is ons allebei gelukt en we promoveren een paar dagen na elkaar. Ik wens je het aller beste en ik hoop dat onze vriendschap blijft!
Meiden, lieve Meike, Wilma, Nienke, Rianne en Yvette, wat zijn we een heerlijk stel bij elkaar. Als we met z’n allen bij elkaar zijn dan is dat garantie voor heel veel gezelligheid. Al meer dan 15 jaar een ontzettend hechte vriendschap. Wat hebben we veel met elkaar meegemaakt; vakanties, feestjes, weekendjes weg, geboortes, verjaardagen, etentjes, borrels en oneindig veel meer. Maar ook tijdens verdrietige gebeurtenissen zijn we er voor elkaar. Ik mag van geluk spreken dat ik zulke fijne vriendinnen heb! Bedankt lieve meiden. Lieve Iris, je bent al jaren een ontzettend goede vriendin. We hebben samen oneindig veel bijzondere en leuke momenten meegemaakt. Dank je wel dat je er altijd voor me bent.
Natuurlijk wil ik ook mijn lieve familie bedanken, want zonder hun steun en vertrouwen was me dit niet gelukt. Sissies, lieve Sanne en Marijn, jullie zijn de beste zussen die ik me kan wensen! Ik weet dat ik altijd bij jullie terecht kan. Even bellen om zomaar even bij te kletsen, maar ook voor raad of advies of als ik het even niet meer weet. We begrijpen elkaar als geen ander en jullie zijn er altijd. Lieve San, ik ben ontzettend trots op je! Al vanaf het moment dat ik begon met mijn promotietraject wist ik heel zeker dat jij mijn paranimf zou zijn. Als tweelingzussen hebben we toch een bijzondere band. Lieve Marijn, ook onze bijzondere band koester ik! Ik kan altijd op je rekenen en je weet me altijd goede raad te geven en aan het lachen te maken. Ik ben heel erg trots dat jij mijn zusje bent. Ik hou van jullie!
Pap en mam, wat ben ik in een ontzettend warm nest opgegroeid en wat fijn dat we zo’n hecht gezin zijn! Jullie zijn er altijd voor me, staan altijd achter me en ik kan voor alles bij jullie terecht. Dit is zeker niet vanzelfsprekend en ik ben jullie hier dan ook enorm dankbaar voor. Jullie onvoorwaardelijke liefde en steun hebben me gemaakt tot wie ik nu ben. Ik heb het getroffen met jullie en ik kan me geen fijnere ouders wensen!

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord | 183
&
Lieve Michel, bedankt voor al je steun, liefde en geduld tijdens mijn promotietraject. Wat is het fijn om te weten dat jij er bent als ik thuis kom. Je staat altijd voor me klaar, maakt me aan het lachen en steunt me in alles wat ik doe. Ik ben super blij met je en ik hou ontzettend veel van je!

Strategies to improve non-pharmacological
care in generalized osteoarthritis
Nienke Cuperus
Strategies to improve non-pharm
acological care in generalized osteoarthritis
N
ienke Cuperus
Uitnodiging
voor het bijwonen van de
openbare verdediging van
mijn proefschrift
Strategies to improve non-pharmacological
care in generalized osteoarthritis
Op maandag 6 juli
om 14.30 uur precies
in de aula van de Radboud
Universiteit Nijmegen,
Comeniuslaan 2 6525 HP
Nijmegen
U bent van harte welkom bij
deze plechtigheid en de
aansluitende receptie
Nienke Cuperus
Vermeerstraat 17,
6961 ZC Eerbeek
Paranimfen
Hans Cuperus (06-52481673)
Sanne Cuperus (06-42663351)