




Talen
Pages
Wettelijk

8/6/2019 OM Un Grutnieciba
1/41
1
The importance of antioxidant micronutrients in pregnancy1
Hiten D. Mistry1 & Paula J. Williams2*2
1Division ofWomens Health, Maternal and Fetal Research Unit, St. Thomas Hospital , Kings College3
London, London, SE1 7UH, UK;4
2Human Genetics, School of Molecular and Medical Sciences, University of Nottingham, Queens Medical5
Centre, Nottingham, NG7 2UH, UK.6
7
*To whom correspondence should be addressed:8
Dr Paula J Williams9
Human Genetics,10
School of Molecular Medical Sciences,11
University of Nottingham,12
A Floor West Block,13
Queen's Medical Centre,14
Nottingham15
NG7 2UH16
E-mail: [email protected]
18
19
20
21
22
23
24
8/6/2019 OM Un Grutnieciba
2/41
2
Abstract25
Pregnancy places increased demands on the mother to provide adequate nutrition to the26
growing conceptus. A number of micronutrients function as essential cofactors for or27
themselves acting as antioxidants. Oxidative stress is generated during normal placental28
development however, when supply of antioxidant micronutrients is limited, exaggerated29
oxidative stress within both the placenta and maternal circulation occurs, resulting in30
adverse pregnancy outcomes. The present literature review summarises the current31
understanding of selected micronutrient antioxidants selenium, copper, zinc, manganese32
and vitamins C & E in pregnancy. To summarise antioxidant activity of selenium is via33
its incorporation into the glutathione peroxidase enzymes, levels of which have been34
shown to be reduced in miscarriage and pre-eclampsia. Copper, zinc and manganese are35
all essential cofactors for superoxide dismutases, which has reduced activity in36
pathological pregnancy. Larger intervention trials are required to reinforce or refute a37
beneficial role of micronutrient supplementation in disorders of pregnancies.38
39
Keywords: Pregnancy, antioxidants, micronutrients, vitamins.40
41
42
43
44
45
46
47
8/6/2019 OM Un Grutnieciba
3/41
3
Introduction48
Nutrition in Pregnancy49
The importance of proper nutrition prior to and throughout pregnancy has long been50
known for optimising the health and wellbeing of both mother and baby [1]. Pregnancy is51
a period of increased metabolic demands with changes in a womens physiology and the52
requirements of a growing fetus [2, 3]. Insufficient supplies of essential vitamins and53
micronutrients can lead to a state of biological competition between the mother and54
conceptus, which can be detrimental to the health status of both [4] Deficiency of trace55
elements during pregnancy is closely related to mortality and morbidity in the new born56
[5]. Deficiencies of specific antioxidant activities associated with the micronutrients57
selenium, copper, zinc and manganese can result in poor pregnancy outcomes, including58
fetal growth restriction [6], pre-eclampsia [7] and the associated increased risk of diseases59
in adulthood, including cardiovascular disease and type 2 diabetes [8-11].60
61
A large body of research has investigated the role of macronutrients in pregnancy and62
especially the effects of both maternal under and over nutrition on the long term health of63
the offspring [12, 13]. A number of hypotheses have been suggested to explain the64
contribution of maternal nutrition during the fetal and embryonic periods and the65
programming of the cardiovascular and metabolic system of the offspring [14, 15]. In66
addition to the contribution of macronutrition to successful pregnancy more recently67
studies have begun to focus on the role of essential specific micronutrients, so called68
because they are an absolute requirement and are required in only small amounts daily69
[16].70
8/6/2019 OM Un Grutnieciba
4/41
4
The pregnant mother must provide a source of nourishment and gaseous exchange to71
enable maximal embryonic and fetal growth to occur, whilst at the same time preparing72
her body for labour and parturition and the later demands of lactation. In addition a73
careful balance must be maintained between providing immune surveillance to protect the74
mother from infection, whilst at the same time allowing the implantation and survival of75
the semi-allogenic conceptus [17, 18]. The development and establishment of the76
placenta and its circulatory system is crucial in the successful maintenance of both77
maternal health and also enabling development of the embryo and growth of the fetus.78
79
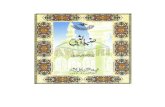
The establishment of the feto-placental circulation requires the invasion of placental80
derived extravillous trophoblast from anchoring cytotrophoblast columns through the81
maternal decidua and into the maternal spiral arteries (Figure 1). During the first 8 weeks82
of pregnancy trophoblast plugs within the spiral arteries which exist to protect embryonic83
DNA from damage by oxidative stress [19], are released allowing the onset of placental84
circulation (Figure 1). The release of trophoblast plugs with flow of blood into the85
intervillous space leads to the generation of oxidative stress [20]. However, the placenta86
is armed with antioxidant defences, including the selenium-dependent glutathione87
peroxidases, thioredoxin reductases, selenoprotein-P and copper/zinc and manganese88
superoxide dismutases (Cu/Zn and Mn SODs) (Figure 2), which protect the placenta from89
any undue harm [21-24]. As the extravillous trophoblast cells migrate through the spiral90
artery wall they are involved in the process of physiological conversion, which serves to91
enlarge the vessel lumen thereby maximising blood supply to the intervillous space,92
enabling maximal perfusion of nutrients and gases through the placental93
8/6/2019 OM Un Grutnieciba
5/41
5
syncytiotrophoblast. Deficient extravillous trophoblast invasion is associated with94
reduced spiral artery remodelling leading to reduced blood flow and increased oxidative95
stress within the placenta and is known to be the primary defect occurring in pre-96
eclampsia [25, 26], fetal growth restriction [27, 28] and sporadic miscarriage [29].97
Additionally, pre-eclampsia has also been associated with reduced levels of antioxidant98
enzyme protection causing further placental damage [30-32].99
100
The pathogenesis of adverse pregnancy outcomes including pre-eclampsia and fetal101
growth restriction [33] and a number of neonatal outcomes [34] have been shown to be102
associated with oxidative stress. Pre-eclampsia (de novo proteinuric hypertension) is103
estimated to occur in ~3% of all pregnancies and is a leading cause of maternal and104
perinatal mortality and morbidity in the Western world [35, 36]; together with other105
hypertensive disorders of pregnancy, pre-eclampsia is responsible for approximately106
60,000 maternal deaths each year [37] and increases perinatal mortality five-fold [38].107
Optimal outcome for the mother and child often dictates that the infant is delivered early108
leading to increased preterm delivery and low infant birthweight rates. Placental and109
maternal systemic oxidative stress are components of the syndrome [39] and contribute to110
a generalised maternal systemic inflammatory activation [40]. Placental ischaemia-111
reperfusion injury has been implicated in excessive production of ROS, causing release of112
placental factors that mediate the inflammatory responses [41].113
114
Fetal growth restriction is associated with increased perinatal mortality and morbidity115
[42]. The mechanisms are still to be elucidated but a likely factor is placental116
8/6/2019 OM Un Grutnieciba
6/41
6
ischemia/hypoxia [43] but it is thought that ischemia-reperfusion injury may contribute to117
the oxidative stress and could result in the release of reactive oxygen species into the118
maternal circulation possibly resulting in oxidative DNA damage and may underlie119
development of fetal growth restriction [44].120
121
The current review focuses specifically on those micronutrients which are associated with122
antioxidant activity due to the importance of oxidative stress in both normal pregnancy123
and pathological pregnancy outcomes. However, it is important to highlight that other124
micronutrients are also important in pregnancy [16] but are outside the scope of the125
current review.126
127
Methods128
A number of micronutrients and vitamins are known to serve as antioxidants or be129
essential cofactors for antioxidant enzymes; these include, selenium, copper, zinc,130
manganese and vitamins C and E. The present literature review summarises current131
understanding of the importance of these micronutrient antioxidants in pregnancy. For132
this review, we included data and relevant information obtained through a search of the133
PubMed database using free text and Medical Subject Headings terms for all articles134
published in English from 1971 through 2011 which included the term selenium, zinc,135
copper, manganese, vitamin E and C and one of the following: pregnancy, pre-136
eclampsia or fetal growth restriction. We further included published and unpublished137
data from our own laboratories and an in-house library of relevant publications. The138
procedurewas concluded by the perusal of the reference sections of allrelevant studies or139
8/6/2019 OM Un Grutnieciba
7/41
7
reviews, a manual search of key journalsand abstracts from the major annual meetings in140
the field ofpregnancy and nutrition and contact with experts on the subject, in an effort to141
identify relevant unpublished data.142
143
Selenium144
Selenium is incorporated into proteins to make selenoproteins, including the glutathione145
peroxidase antioxidant enzymes, thioredoxin reductases and selenoprotein-P [45]. In146
addition, selenium is essential for the production of active thyroid hormones and is147
essential for normal thyroid function [46]. Maternal selenium concentrations and148
glutathione peroxidase activity fall during pregnancy (selenium concentrations in 1st149
trimester: 65 g/L; 3rdtrimester: 50 g/L) [47, 48]. Worldwide differences exist in150
assessment of selenium requirements, adequacy and intakes (Table 1). Most of these151
values have been determined from the intake believed necessary to maximise the activity152
of the antioxidant glutathione peroxidase in plasma [49, 50] and selenium, like vitamins153
C and E has received much attention in recent years. It has been observed that babies on154
average have lower selenium concentrations compared to the mother (Maternal selenium155
58.4 g/L; Umbilical cord selenium: 42.1 g/L) [32, 51], which is expected as selenium156
is transported via the placenta across a concentration gradient via an anion exchange157
pathway, shared with sulphate [52, 53].158
159
Recurrent early pregnancy loss has been associated with reduced serum selenium160
concentrations compared to healthy controls in two observational studies from UK (mean161
SD: 54 19 vs. 76 14 g/L respectively) [54] and Turkey (55 17 vs. 81 16 g/L162
8/6/2019 OM Un Grutnieciba
8/41
8
respectively) [55]. It has therefore been suggested that reduced selenium concentration163
results in reduced glutathione peroxidase activity culminating in reduced antioxidant164
protection of biological membranes and DNA during the early stages of embryonic165
development [54, 56]. Although speculative, and requiring larger placebo-controlled166
randomised trials, women with recurrent early pregnancy loss may benefit from167
optimisation of selenium status.168
169
Recently, our group and others have demonstrated through retrospective studies, the170
association between low serum selenium concentrations and reduced antioxidant function171
of the associated antioxidant glutathione peroxidase enzymes in women with pre-172
eclampsia (defined a de novo proteinuric hypertension) [32, 57, 58]. It has been suggested173
that adequate selenium status is important for antioxidant defence and may be a potential174
factor in women at risk of pre-eclampsia; this hypothesis has been further justified by the175
reduced expression and activities of glutathione peroxidase found in maternal, fetal and176
placental samples taken from 25 pre-eclamptic pregnancies, when compared to 27 normal177
controls in our recent cross-sectional retrospective study [32]. Dawson et al, also178
completed a retrospective study in the US and reported lower amniotic fluid selenium179
concentrations in 29 pre-eclamptics delivering between 33-36 weeks gestation compared180
to 48 gestation-matched controls (10 1 vs. 7 0.7 g/L respectively) [59].181
182
Fetal growth restriction or delivery of a small-for-gestational-age (SGA) is defined as an183
individualised birth weight ratio below the 10th percentile [42]. Reports of selenium184
concentrations with regards to fetal growth restriction are inconsistent. A retrospective185
8/6/2019 OM Un Grutnieciba
9/41
9
study had reported low placental selenium concentrations in 49 mothers affected by fetal186
growth restriction, compared to 36 healthy normal birth weight controls [60], whereas187
others have reported higher [61, 62] or unchanged concentrations [63]. Another188
retrospective study also demonstrated that in 81 SGA babies, infant plasma selenium189
concentrations to be significantly lower compared to controls [64]. A recent retrospective190
study by our group on an adolescent cohort [65] found lower maternal plasma selenium191
concentrations on 28 mothers who delivered SGA babies compared to 143 healthy192
controls [66]. Further studies are warranted to fully investigate the potential link between193
selenium deficiency and fetal growth restriction.194
195
Only a small number of selenium supplementation trials during pregnancy have been196
carried out to date. A prospective, randomised, placebo controlled study of selenium197
supplementation during and after pregnancy in pregnant women positive for thyroid198
peroxidase antibodies (TPOAb(+)) who are prone to develop postpartum thyroid199
dysfunction (PPTD) and permanent hypothyroidism found that supplementation with 200200
g/d selenomethionine significantly reduced the incidence of PPTD and permanent201
hypothyroidism [67]. The authors concluded that selenium supplementation during202
pregnancy and in the postpartum period reduced thyroid inflammatory activity and the203
incidence of hypothyroidism, possibly by increasing the selenoproteins glutathione204
peroxidase or iodothyronine deiodinase activities, thereby contributing in part, to205
counterbalance the postpartum immunological rebound [67].206
207
8/6/2019 OM Un Grutnieciba
10/41
10
To date there have been a couple of small placebo-controlled randomised control trials on208
selenium supplementation, reporting lower rates of pre-eclampsia and/or pregnancy209
induced hypertension in the supplemented groups [68-70]. It must be noted that neither of210
these studies adequately addressed the role of supplementation on the incidence of pre-211
eclampsia. Currently the Selenium in Pregnancy Intervention Trial (SPRINT) is212
underway in the UK, jointly by the University of Surrey and Oxford. This is a small213
randomised controlled trial of selenium supplementation (60 g a day). It is not powered214
to demonstrate clinical benefit but will provide insight into the impact of selenium215
supplements on laboratory measurements of circulating factors that are relevant to the216
development of pre-eclampsia. If this is successful a much larger multicentre trial will be217
needed to analyse clinical benefit.218
219
Copper220
Copper is an essential cofactor for a number of enzymes involved in metabolic reactions,221
angiogenesis, oxygen transport and antioxidant protection, including catalase, superoxide222
dismutase (SOD) (Figure 2) and cytochrome oxidase [71]. During pregnancy, plasma223
copper concentrations significantly increase, returning to normal non-pregnant values224
after delivery (Mean SD - 1st trimester: 147.6 34.6; 3rd trimester: 204.2 41.8 g/L)225
[72-74]. The increase in copper with progression of pregnancy could be partly related to226
synthesis of ceruloplasmin, a major copper binding protein, due to altered levels of227
oestrogen [74]. Approximately 96% of plasma copper is strongly bound to ceruloplasmin228
[75], a protein with antioxidant ferroxidase properties [75, 76]. The dietary intake of229
copper in women aged between 19-24 years is generally below the recommended levels230
8/6/2019 OM Un Grutnieciba
11/41
11
(Table 1) [77] which may cause problems during pregnancy when requirements increase231
[78].232
233
Copper is essential for embryonic development [79]. Maternal dietary deficiency can234
result in both short term consequences including early embryonic death and gross235
structural abnormalities, as well as long term consequences such as increased r isk of236
cardiovascular disease risk and reduced fertilisation rates [71, 80]; current237
recommendations on intakes are summarised in Table 1. Severe copper deficiency can238
lead to reproductive failure and early embryonic death [81], whereas mild or moderate239
deficiency has little effect on either the number of live births or neonatal weight [82].240
241
Cu/Zn SOD is an important antioxidant known to be expressed in both maternal and fetal242
tissues [83]. Copper concentration has been shown to be higher in maternal plasma than243
in umbilical cord plasma [84-86]. It has been suggested that the placenta acts as a244
blockade in the transfer of copper from the mother to the fetus [86, 87]. A recent245
observational Turkish study on 61 placentae from healthy pregnancies between 37 and 40246
weeks gestat ion found that copper concentrations positively correlated with neonatal247
weight; the authors suggested that copper may have interactive connections in human248
placenta [88] and this requires further studies to fully elucidate its role. It is known that249
copper is transferred across the placenta via high affinity copper transporter (CTR1) and250
have been shown to be expressed early in pregnancy and it is also thought that placental251
copper transport is related to iron transport but the mechanism is unknown [78].252
253
8/6/2019 OM Un Grutnieciba
12/41
12
A small retrospective study in the 1980s reported increased placental copper254
concentrations in 8 pre-eclamptic women compared to 10 controls (53 vs. 124 g/Kg255
respectively), suggesting that this increase in pre-eclampsia maybe an exaggerated256
response of normal pregnancies [89]. Further retrospective studies from Turkey have257
shown elevation of maternal serum copper levels in pre-eclampsia after clinical onset of258
the disease compared to controls (mean SD: 159 38 vs. 194 52 g/L respectively)259
[90, 91]. Moreover, increased amniotic fluid copper concentration from 19 pre-eclamptic260
women compared to 53 controls has also been reported (mean SD: 19 5 vs. 29 3261
g/L respectively) [59]. It is thought that as copper is a redox-active transition metal and262
can participate in single electron reactions and catalyse the formation of free radicals,263
including undesirable hydroxyl radicals, it could contribute to oxidative stress264
characteristic of pre-eclampsia [90]. This illustrates that copper itself appears to act as a265
pro-oxidant, but when associated in Cu/Zn SOD functions as an antioxidant.266
Furthermore, studies have reported increased levels of serum ceruloplasmin in women267
with pre-eclampsia; this positively correlated with serum malondialdehyde, suggesting an268
increased production of this antioxidant protein in response to increased lipid269
peroxidation [90, 92, 93], although further studies are required to confirm this hypothesis.270
However, it must be remembered that concentrations early in pregnancy have yet to be271
determined and data on copper status in normal human pregnancies are sparse. This is272
further hampered by the fact that at present there is no reliable biomarker for copper273
status, so whether deficiency is a significant public health problem remains unclear [94].274
275
276
8/6/2019 OM Un Grutnieciba
13/41
13
Zinc277
Zinc is an essential constituent of over 200 metalloenzymes participating in carbohydrate278
and protein metabolism, nucleic acid synthesis, antioxidant functions (through Cu/Zn279
SOD; Fig. 2) and other vital functions such cellular division and differentiation, making it280
essential for successful embryogenesis. [72]. It was estimated in 2002 by the World281
Health Organisation that suboptimal zinc nutrition effected nearly half the worlds282
population [95]. During pregnancy, zinc is also used to assist the fetus to develop the283
brain and also to be an aid to the mother in labour [96]. It has been estimated that the total284
amount of zinc retained during pregnancy is ~ 100 mg [97]. The requirement of zinc285
during the third trimester is approximately twice as high as that in non-pregnant women286
[98]. Plasma zinc concentrations decline as pregnancy progresses (mean SD1st287
trimester: 71.3 12.9 g/L; 3rdtrimester: 58.5 11.5 g/L) [72, 74, 99, 100]. In addition,288
a nutrition analysis revealed that in pregnant women the everyday diet intakes includes289
not more than 50% of the daily requirement of zinc [101].290
291
Alteration in zinc homeostasis may have devastating effects on pregnancy outcome,292
including prolonged labour, fetal growth restriction, or embryonic or fetal death [102].293
Zinc is a trace element with a great importance for fetal growth restriction where it is294
used in order to improve fetal growth [72]. Goldenberg et al completed a randomised295
double-blind placebo-controlled trail of zinc supplementation (25 mg per day) during296
pregnancy from 19 weeks gestation in African-American women (294 in supplemented297
and 286 in placebo group). Those given zinc supplementation had a significantly greater298
birth weight and head circumference compared to the placebo group highlighting the299
8/6/2019 OM Un Grutnieciba
14/41
14
importance of adequate zinc supply during pregnancy [103]. A limitation of many of the300
randomised controlled trails of zinc supplementation and pregnancy outcome is that they301
lacked the sample sizes to detect differences [102].302
303
Many of the zinc supplementation studies have been conducted in developing countries304
where incidence of zinc deficiency is high and these women are often selected as they are305
less well nourished or have low plasma zinc levels [103, 104]; benefits of306
supplementation include reduced incidence of pregnancy-induced hypertension or low307
birth weights [103]. These studies do however suggest the benefits of zinc308
supplementation in developing countries where zinc deficiency is likely, although for309
developed countries there is conflicting data as to the benefits [105-108].310
311
Zinc deficiency has been associated with pre-eclampsia since the 1980s [59, 89, 109]312
including adolescent pregnancies [110]. Placental zinc concentration has also been shown313
to be lower in pre-eclampsia in cross-sectional retrospective studies with placental zinc314
values positively correlating with birth weights [89, 111, 112]. More recently lower315
serum concentrations of zinc in pre-eclampsia compared to controls have been shown in316
two relatively small retrospective studies from Turkey (mean SD: 10.6 4.4 vs. 12.7 317
4.1 g/L respectively) [91, 113]; the authors suggested that this may be useful for early318
diagnosis as lower plasma zinc concentrations have been associated with increased lipid319
peroxidation in rat studies [114]. Moreover, in a recent retrospective study in India320
reported reduced serum zinc concentrations in mild and severe pre-eclamptic mothers321
compared to controls; the authors suggest that the reduction could not only effect the322
8/6/2019 OM Un Grutnieciba
15/41
15
antioxidant protection but could also contribute to the rise in blood pressure [115]. The323
lower serum zinc concentrations in mothers who develop pre-eclampsia has been324
suggested to at least be partly due to reduced oestrogen and zinc binding-protein levels325
[116]. Zinc is transported across the placenta via active transport from the mother to the326
fetus [109]. Studies have shown that the fetus has notably higher zinc concentrations327
compared to the mother, even in cases of pre-eclampsia [109, 117], indicating that the328
fetus itself, can maintain adequate zinc homeostasis. Amniotic fluid zinc concentrations329
have also been reported to be decreased in pre-eclamptic women delivering preterm (33-330
36 weeks gestation) in a small retrospective cross-sectional study from the US [59]. It331
must be noted that as with all these micronutrients, the concentrations early in pregnancy332
in relation to the development of pregnancy complications remains to be established.333
334
Manganese335
Manganese is a free element in nature (often in combination with iron), furthermore336
manganese(II) ions function as cofactors for a number of enzymes; the element is thus a337
required trace mineral for all known living organisms. Manganese is also an important338
cofactor for a number of enzymes, including the antioxidant manganese superoxide339
dismutase (Mn-SOD; Figure 2) which may protect the placenta from oxidative stress by340
detoxifying superoxide anions [118]. Dietary manganese is the main source of exposure341
under normal circumstances; current requirements for manganese, although less studied342
compared to other micronutrients are shown in Table 1 and little is known about the343
effects of deficiency or excess of manganese on the developing human fetus or pregnancy344
outcome [119]. This is further hampered by the fact that at present sensitive biomarkers345
8/6/2019 OM Un Grutnieciba
16/41
16
of manganese exposure and nutritional status are not available other than some estimates346
from blood concentrations [119].347
348
Circulating whole blood manganese concentrations have been shown to be lower in349
women with fetal growth restriction compared to healthy controls (mean SD: 16.7 4.8350
vs. 19.1 5.9 g/L respectively) indicating that this micronutrient may be important in351
maintaining fetal growth [120]. This study also found that manganese concentrations352
were higher in umbilical samples from fetal growth restriction cases compared to controls353
suggesting that manganese contributes to different effects on birth weight in healthy354
mothers [120]. Zota et al retrospective study in the US reported a non- linear relationship355
between manganese concentrations and birth weights in a cohort of 470 full term356
(delivered at > 37 weeks gestation) infant further indicating the potential affect on fetal357
growth [121]. A recent small retrospective study of African-American mothers reported358
reduced umbilical cord whole blood manganese concentrations in neonates born to359
mothers with pre-eclampsia compared to controls (mean [95% CI]: 2.2 [1.5, 3.2] vs. 3.7360
[3.2, 4.2] g/L respectively) [122]. Furthermore, this study found that like other361
micronutrients umbilical cord blood from smoking mothers had reduced manganese362
concentrations [122]. Than et al demonstrated increased fetal membrane MnSOD mRNA363
expression in women with pre-term labour [123]. Manganese is one of the least studied364
micronutrients and at present no supplementation trial has been published which may365
reflect the lack of data on manganese concentrations in pregnancy.366
367
368
8/6/2019 OM Un Grutnieciba
17/41
17
Vitamins C and E369
Vitamin C (ascorbic acid and dihydroascorbic acid) is an essential water-soluble vitamin370
found widely in fruit and vegetables; it has important roles in collagen synthesis, wound371
healing, prevention of anaemia and as an antioxidant as it can quench a variety of reactive372
oxygen species and reactive nitrogen species in aqueous environments [124]. Vitamin C373
is commonly included in low doses (
8/6/2019 OM Un Grutnieciba
18/41
18
multicentre double-blinded randomised trials of a combination of vitamin C and E [129,392
130] also found supplementation did not reduce the rate of pre-eclampsia or gestational393
hypertension and like the Vitamins In Pre-eclampsia trial in 2006 [131] increased the risk394
of fetal loss or perinatal death and preterm prelabour rupture of membranes. Another395
recent multicentre placebo-controlled trial of vitamin C and E in women with type-1396
diabetes in pregnancy (DAPIT) also reported no differences in the rates of pre-eclampsia397
between supplemented or placebo groups [132]. Further investigations are required as the398
concentrations of these vitamins remain significantly reduced in women with pre-399
eclampsia, but in the absence of further evidence, routine supplementation with higher400
dose vitamin C and E is not recommended as they can be potentially dangerous in high401
concentrations.402
403
Adolescent pregnancies404
Another factor to highlight is that pregnancy in adolescent women is a topic of increasing405
health concern in many countries [133]. Pregnant adolescents are of a greater nutritional406
risk as they themselves are undergoing an intense process of growth and development407
[134]. It has been suggested that there is competition for nutrients between a pregnant408
adolescent and her fetus, as both are in critical stages of growth during the gestational409
period [65, 135]. As mentioned throughout above, micronutrient deficiencies have been410
associated with adolescent pregnancies [66, 84, 110]. The recent About Teenage Eating411
study showed that teenage pregnancy in the UK is associated with decreased412
consumption of micronutrients and that this is associated with an increased risk of SGA413
infants [65].414
8/6/2019 OM Un Grutnieciba
19/41
19
Low micronutrient intake poses a health risk to successful pregnancy in the UK,415
especially in adolescence. Socioeconomic deprivation in the UK population has been416
shown to be an independent risk factor for eating less fruit and vegetables and also for417
increased smoking, which is known to cause further depletion of micronutrients [136].418
Although attempts are being made to persuade women of low socioeconomic status of the419
importance of a balanced diet, the central roles that fruit and vegetables have in this and420
that healthy food can be low cost and convenient this is often met with resistance [137].421
422
The increase in pregnancies in mothers of older ages highlights another subgro up at423
increased risk of pregnancy complications. We are not aware of any studies at present424
examining this important group and future investigations are required especially as some425
of these micronutrient concentrations decline with increasing age.426
427
Conclusions428
Increased knowledge about the importance of these specific antioxidant micronutrients429
and the crucial part that they have in maintaining successful pregnancy and determining430
both the long and short term health of both mother and baby needs to be addressed and431
made a key focus for future health strategies in improving pregnancy outcomes. This is432
particularly important with regards to pre-eclampsia and fetal growth restriction, where433
oxidative stress is an essential component to the aetiology of these conditions and so434
these specific antioxidant micronutrient deficiencies may play a contributing role. Only435
by fully understanding the requirements for micronutrients during pregnancy will we be436
able to evaluate the potential use of these dietary antioxidant supplements as a way of437
8/6/2019 OM Un Grutnieciba
20/41
20
preventing pathological pregnancy outcomes. However, it must also be remembered that438
these antioxidant and other micronutrients can be obtained via a healthy diet thereby439
negating the need for supplementation. Future strategies focussing on providing440
nutritional guidance specifically to pregnant women will be pivotal in helping to ensure441
optimal health of both mother and baby.442
443
Key Messages444
1) Further research is needed to accurately quantify levels of micronutrients in445pregnancy and how levels vary over the course of pregnancy.446
2) The actions of antioxidant micronutrients on maternal, fetal and placental health447needs to further elucidated.448
3) Prenatal guidance needs to be made clear to ensure that women and practioners449are aware of the nutritional requirements during pregnancy, and how healthy diet450
can prevent diseases of pregnancy.451
452
Conflict of Interest: None of the authors have any conflict of interest.453
454
Funding: H.D. Mistry was funded by Tommys Charity (Charity No. 3266897) and P.J.455
Williams was supported by the Nottingham University Hospitals Special Trustees Charity456
(RB17B3).457
458
459
460
8/6/2019 OM Un Grutnieciba
21/41
21
References461
[1] Allen LH. Multiple micronutrients in pregnancy and lactation: an overview. Am J462
Clin Nutr 2005;81:1206S.463
[2] Broughton Pipkin F. Maternal Physiology. In: Edmonds DK, editor. Dewhurst's464
textbook of Obstetrics and Gynaecology. Oxford: Blackwell Publishing, 2007.465
[3] Bader RA, Bader ME, Rose DF, Braunwald E. Hemodynamics at rest and during466
exercise in normal pregnancy as studies by cardiac catheterization. J Clin Invest467
1955;34:1524.468
[4] King JC. The risk of maternal nutritional depletion and poor outcomes increases469
in early or closely spaced pregnancies. J Nutr 2003;133:1732S.470
[5] Srivastava S, Mehrotra PK, Srivastava SP, Siddiqui MK. Some essential elements471
in maternal and cord blood in relation to birth weight and gestational age of the baby.472
Biol Trace Elem Res 2002;86:97.473
[6] Fall CH, Yajnik CS, Rao S, Davies AA, Brown N, Farrant HJ. Micronutrients and474
fetal growth. J Nutr 2003;133:1747S.475
[7] Rumbold A, Duley L, Crowther CA, Haslam RR. Antioxidants for preventing pre-476
eclampsia. Cochrane Database Syst Rev 2008:CD004227.477
[8] Bellamy L, Casas JP, Hingorani AD, Williams DJ. Pre-eclampsia and risk of478
cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ479
2007;335:974.480
[9] Lykke JA, Langhoff-Roos J, Sibai BM, Funai EF, Triche EW, Paidas MJ.481
Hypertensive pregnancy disorders and subsequent cardiovascular morbidity and type 2482
diabetes mellitus in the mother. Hypertension 2009;53:944.483
8/6/2019 OM Un Grutnieciba
22/41
22
[10] Vikse BE, Irgens LM, Leivestad T, Skjaerven R, Iversen BM. Preeclampsia and484
the risk of end-stage renal disease. N Engl J Med 2008;359:800.485
[11] Staff AC, Dechend R, Pijnenborg R. Learning From the Placenta. Acute Atherosis486
and Vascular Remodeling in Preeclampsia-Novel Aspects for Atherosclerosis and Future487
Cardiovascular Health. Hypertension 2010.488
[12] Armitage JA, Khan IY, Taylor PD, Nathanielsz PW, Poston L. Developmental489
programming of the metabolic syndrome by maternal nutritional imbalance: how strong490
is the evidence from experimental models in mammals? J Physiol 2004;561:355.491
[13] Armitage JA, Taylor PD, Poston L. Experimental mode ls of developmental492
programming: consequences of exposure to an energy rich diet during development. J493
Physiol 2005;565:3.494
[14] Solomons NW. Developmental origins of hea lth and disease: concepts, caveats,495
and consequences for public health nutrition. Nutr Rev 2009;67 Suppl 1:S12.496
[15] Wells JC. The thrifty phenotype as an adaptive maternal effect. Biol Rev Camb497
Philos Soc 2007;82:143.498
[16] Cetin I, Berti C, Calabrese S. Role of micronutrients in the periconceptional499
period. Hum Reprod Update 2009.500
[17] Challis JR, Lockwood CJ, Myatt L, Norman JE, Strauss JF, 3rd, Petraglia F.501
Inflammation and pregnancy. Reprod Sci 2009;16:206.502
[18] Hanson LA, Silfverdal SA. The mother's immune system is a balanced threat to503
the foetus, turning to protection of the neonate. Acta Paediatr 2009;98:221.504
[19] Ornoy A. Embryonic oxidative stress as a mechanism of teratogenesis with505
special emphasis on diabetic embryopathy. Reprod Toxicol 2007;24:31.506
8/6/2019 OM Un Grutnieciba
23/41
23
[20] Jauniaux E, Watson AL, Hempstock J, Bao YP, Skepper JN, Burton GJ. Onset of507
maternal arterial blood flow and placental oxidative stress. A possible factor in human508
early pregnancy failure. Am J Pathol 2000;157:2111.509
[21] Wang Y, Walsh SW. Antioxidant activities and mRNA expression of superoxide510
dismutase, catalase, and glutathione peroxidase in normal and preeclamptic placentas. J511
Soc Gynecol Investig 1996;3:179.512
[22] Vanderlelie J, Venardos K, Clifton VL, Gude NM, Clarke FM, Perkins AV.513
Increased biological oxidation and reduced anti-oxidant enzyme activity in pre-eclamptic514
placentae. Placenta 2005;26:53.515
[23] Mistry HD, Kurlak LO, Williams PJ, Ramsay MM, Symonds ME, Broughton516
Pipkin F. Differential expression and distribution of placental glutathione peroxidases 1,517
3 and 4 in normal and preeclamptic pregnancy. Placenta 2010;31:401.518
[24] Rayman MP. Selenoproteins and human health: Insights from epidemiological519
data. Biochim Biophys Acta 2009.520
[25] Redman CW, Sargent IL. Placental debris, oxidative stress and pre-eclampsia.521
Placenta 2000;21:597.522
[26] Burton GJ, Jauniaux E. Placental oxidative stress: from miscarriage to523
preeclampsia. J Soc Gynecol Investig 2004;11:342.524
[27] Brosens I, Dixon HG, Robertson WB. Fetal growth retardation and the arteries of525
the placental bed. Br J Obstet Gynaecol 1977;84:656.526
[28] Brosens IA, Robertson WB, Dixon HG. The role of the spiral arteries in the527
pathogenesis of preeclampsia. Obstet Gynecol Annu 1972;1:177.528
8/6/2019 OM Un Grutnieciba
24/41
24
[29] Gupta S, Agarwal A, Banerjee J, Alvarez JG. The role of oxidative stress in529
spontaneous abortion and recurrent pregnancy loss: a systematic review. Obstet Gynecol530
Surv 2007;62:335.531
[30] Perkins AV. Endogenous anti-oxidants in pregnancy and preeclampsia. Aust N Z532
J Obstet Gynaecol 2006;46:77.533
[31] Nakamura M, Sekizawa A, Purwosunu Y, Okazaki S, Farina A, Wibowo N,534
Shimizu H, Okai T. Cellular mRNA expressions of anti-oxidant factors in the blood of535
preeclamptic women. Prenat Diagn 2009;29:691.536
[32] Mistry HD, Wilson V, Ramsay MM, Symonds ME, Broughton Pipkin F. Reduced537
selenium concentrations and glutathione peroxidase activity in pre-eclamptic pregnancies.538
Hypertension 2008;52:881.539
[33] Myatt L, Cui X. Oxidative stress in the placenta. Histochem Cell Biol540
2004;122:369.541
[34] Saugstad OD. Update on oxygen radical disease in neonatology. Curr Opin Obstet542
Gynecol 2001;13:147.543
[35] Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet544
2010.545
[36] Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet 2005;365:785.546
[37] Broughton Pipkin F. Risk factors for preeclampsia. N Engl J Med 2001;344:925.547
[38] Roberts JM, Lain KY. Recent Insights into the pathogenesis of pre-eclampsia.548
Placenta 2002;23:359.549
[39] Poston L. The Role of Oxidative Stress. In: Critchley H, MacLean A, Poston L,550
Walker J, editors. Pre-eclampsia. London: RCOG Press, 2004.551
8/6/2019 OM Un Grutnieciba
25/41
25
[40] Redman CW, Sargent IL. Pre-eclampsia, the placenta and the maternal systemic552
inflammatory response--a review. Placenta 2003;24 Suppl A:S21.553
[41] Hung TH, Burton GJ. Hypoxia and reoxygenation: a possible mechanism for554
placental oxidative stress in preeclampsia. Taiwan J Obstet Gynecol 2006;45:189.555
[42] Cetin I, Foidart JM, Miozzo M, Raun T, Jansson T, Tsatsaris V, Reik W, Cross J,556
Hauguel-de-Mouzon S, Illsley N, Kingdom J, Huppertz B. Fetal growth restriction: a557
workshop report. Placenta 2004;25:753.558
[43] Biri A, Bozkurt N, Turp A, Kavutcu M, Himmetoglu O, Durak I. Role of559
oxidative stress in intrauterine growth restriction. Gynecol Obstet Invest 2007;64:187.560
[44] Takagi Y, Nikaido T, Toki T, Kita N, Kanai M, Ashida T, Ohira S, Konishi I.561
Levels of oxidative stress and redox-related molecules in the placenta in preeclampsia562
and fetal growth restriction. Virchows Arch 2004;444:49.563
[45] Rayman MP. The importance of selenium to human health. Lancet 2000;356:233.564
[46] Beckett GJ, Arthur JR. Selenium and endocrine systems. J Endocrinol565
2005;184:455.566
[47] Zachara BA, Wardak C, Didkowski W, Maciag A, Marchaluk E. Changes in567
blood selenium and glutathione concentrations and glutathione peroxidase activity in568
human pregnancy. Gynecol Obstet Invest 1993;35:12.569
[48] Mihailovic M, Cvetkovic M, Ljubic A, Kosanovic M, Nedeljkovic S, Jovanovic I,570
Pesut O. Selenium and malondialdehyde content and glutathione peroxidase activity in571
maternal and umbilical cord blood and amniotic fluid. Biol Trace Elem Res 2000;73:47.572
[49] Thomson CD. Assessment of requirements for selenium and adequacy of573
selenium status: a review. Eur J Clin Nutr 2004;58:391.574
8/6/2019 OM Un Grutnieciba
26/41
26
[50] Rayman MP. Food-chain selenium and human health: emphasis on intake. Br J575
Nutr 2008;100:254.576
[51] Gathwala G, Yadav OP, Singh I, Sangwan K. Maternal and cord plasma selenium577
levels in full- term neonates. Indian J Pediatr 2000;67:729.578
[52] Shennan DB. A study of selenate efflux from human placental microvillus579
membrane vesicles. Biosci Rep 1987;7:675.580
[53] Shennan DB. Selenium (selenate) transport by human placental brush border581
membrane vesicles. Br J Nutr 1988;59:13.582
[54] Barrington JW, Taylor M, Smith S, Bowen-Simpkins P. Selenium and recurrent583
miscarriage. J Obstet Gynaecol 1997;17:199.584
[55] Kocak I, Aksoy E, Ustun C. Recurrent spontaneous abortion and selenium585
deficiency. Int J Gynaecol Obstet 1999;65:79.586
[56] Zachara BA, Dobrzynski W, Trafikowska U, Szymanski W. Blood selenium and587
glutathione peroxidases in miscarriage. BJOG 2001;108:244.588
[57] Rayman MP, Bode P, Redman CW. Low selenium status is associated with the589
occurrence of the pregnancy disease preeclampsia in women from the United Kingdom.590
Am J Obstet Gynecol 2003;189:1343.591
[58] Maleki A, Fard MK, Zadeh DH, Mamegani MA, Abasaizadeh S, Mazloomzadeh592
S. The Relationship between Plasma Level of Se and Preeclampsia. Hypertens Pregnancy593
2010.594
[59] Dawson EB, Evans DR, Nosovitch J. Third-trimester amniotic fluid metal levels595
associated with preeclampsia. Arch Environ Health 1999;54:412.596
8/6/2019 OM Un Grutnieciba
27/41
27
[60] Klapec T, Cavar S, Kasac Z, Rucevic S, Popinjac A. Selenium in placenta597
predicts birth weight in normal but not intrauterine growth restriction pregnancy. J Trace598
Elem Med Biol 2008;22:54.599
[61] Osada H, Watanabe Y, Nishimura Y, Yukawa M, Seki K, Sekiya S. Profile of600
trace element concentrations in the feto-placental unit in relation to fetal growth. Acta601
Obstet Gynecol Scand 2002;81:931.602
[62] Zadrozna M, Gawlik M, Nowak B, Marcinek A, Mrowiec H, Walas S, Wietecha-603
Posluszny R, Zagrodzki P. Antioxidants activities and concentration of selenium, zinc604
and copper in preterm and IUGR human placentas. J Trace Elem Med Biol 2009;23:144.605
[63] Llanos MN, Ronco AM. Fetal growth restrict ion is related to placental levels of606
cadmium, lead and arsenic but not with antioxidant activities. Reprod Toxicol607
2009;27:88.608
[64] Strambi M, Longini M, Vezzosi P, Berni S, Buoni S. Selenium status, birth609
weight, and breast-feeding: pattern in the first month. Biol Trace Elem Res 2004;99:71.610
[65] Baker PN, Wheeler SJ, Sanders TA, Thomas JE, Hutchinson CJ, Clarke K, Berry611
JL, Jones RL, Seed PT, Poston L. A prospective study of micronutrient status in612
adolescent pregnancy. Am J Clin Nutr 2009;89:1114.613
[66] Mistry HD, Kurlak LO, Young SY, Briley AL, Broughton Pipkin F, Poston L.614
Reduced plasma selenium in adolescent mothers with small for gestational age infants;615
impact of smoking and ethnicity. Society for Gynecologic Investigation. Orlando:616
Reproductive Sciences, 2010.617
8/6/2019 OM Un Grutnieciba
28/41
28
[67] Negro R, Greco G, Mangieri T, Pezzarossa A, Dazzi D, Hassan H. The influence618
of selenium supplementation on postpartum thyroid status in pregnant women with619
thyroid peroxidase autoantibodies. J Clin Endocrinol Metab 2007;92:1263.620
[68] Han L, Zhou SM. Selenium supplement in the prevention of pregnancy induced621
hypertension. Chin Med J (Engl) 1994;107:870.622
[69] Rumiris D, Purwosunu Y, Wibowo N, Farina A, Sekizawa A. Lower rate of623
preeclampsia after antioxidant supplementation in pregnant women with low antioxidant624
status. Hypertens Pregnancy 2006;25:241.625
[70] Tara F, Rayman MP, Boskabadi H, Ghayour-Mobarhan M, Sahebkar A, Yazarlu626
O, Ouladan S, Tavallaie S, Azimi-Nezhad M, Shakeri MT, Teymoori MS, Razavi BS,627
Oladi M, Ferns G. Selenium supplementation and premature (pre-labour) rupture of628
membranes: a randomised double-blind placebo-controlled trial. J Obstet Gynaecol629
2010;30:30.630
[71] Gambling L, Andersen HS, McArdle HJ. Iron and copper, and their interactions631
during development. Biochem Soc Trans 2008;36:1258.632
[72] Izquierdo Alvarez S, Castanon SG, Ruata ML, Aragues EF, Terraz PB, Irazabal633
YG, Gonzalez EG, Rodriguez BG. Updating of normal levels of copper, zinc and634
selenium in serum of pregnant women. J Trace Elem Med Biol 2007;21 Suppl 1:49.635
[73] Huang HM, Leung PL, Sun DZ, Zhu MG. Hair and serum calcium, iron, copper,636
and zinc levels during normal pregnancy at three trimesters. Biol Trace Elem Res637
1999;69:111.638
8/6/2019 OM Un Grutnieciba
29/41
29
[74] Liu J, Yang H, Shi H, Shen C, Zhou W, Dai Q, Jiang Y. Blood copper, zinc,639
calcium, and magnesium levels during different duration of pregnancy in Chinese. Biol640
Trace Elem Res 2010;135:31.641
[75] Fattah MM, Ibrahim FK, Ramadan MA, Sammour MB. Ceruloplasmin and642
copper level in maternal and cord blood and in the placenta in normal pregnancy and in643
pre-eclampsia. Acta Obstet Gynecol Scand 1976;55:383.644
[76] Shakour-Shahabi L, Abbasali-Zadeh S, Rashtchi-Zadeh N. Serum level and645
antioxidant activity of ceruloplasmin in preeclampsia. Pakistan Journal of biological646
Sciences 2010;13:321.647
[77] Institute of Medcine. Dietary Reference Intakes for Vitamin A, Vitamin K,648
Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel,649
Silicon, Vanadium, and Zinc.: National Academy Press, 2001.650
[78] McArdle HJ, Andersen HS, Jones H, Gambling L. Copper and iron transport651
across the placenta: regulation and interactions. J Neuroendocrinol 2008;20:427.652
[79] Kambe T, Weaver BP, Andrews GK. The genetics of essential metal homeostasis653
during development. Genesis 2008;46:spcone.654
[80] Keen CL, Hanna LA, Lanoue L, Uriu-Adams JY, Rucker RB, Clegg MS.655
Developmental consequences of trace mineral deficiencies in rodents: acute and long-656
term effects. J Nutr 2003;133:1477S.657
[81] Prohaska JR, Brokate B. The timing of perinata l copper deficiency in mice658
influences offspring survival. J Nutr 2002;132:3142.659
[82] Masters DG, Keen CL, Lonnerdal B, Hurley LS. Comparative aspects of dietary660
copper and zinc deficiencies in pregnant rats. J Nutr 1983;113:1448.661
8/6/2019 OM Un Grutnieciba
30/41
30
[83] Ali Akbar S, Nicolaides KH, Brown PR. Measurement of Cu/Zn SOD in placenta,662
cultured cells, various fetal tissues, decidua and semen by ELISA. J Obstet Gynaecol663
1998;18:331.664
[84] de Moraes ML, de Faria Barbosa R, Santo RE, da Silva Santos F, de Jesus EF,665
Sardinha FL, Tavares do Carmo MD. Maternal-Fetal Distribution of Calcium, Iron,666
Copper, and Zinc in Pregnant Teenagers and Adults. Biol Trace Elem Res 2010.667
[85] McArdle HJ, Ashworth CJ. Micronutrients in fetal growth and development. Br668
Med Bull 1999;55:499.669
[86] Krachler M, Rossipal E, Micetic-Turk D. Trace element transfer from the mother670
to the newborn--investigations on triplets of colostrum, maternal and umbilical cord sera.671
Eur J Clin Nutr 1999;53:486.672
[87] Rossipal E, Krachler M, Li F, Micetic-Turk D. Investigation of the transport of673
trace elements across barriers in humans: studies of placental and mammary transfer.674
Acta Paediatr 2000;89:1190.675
[88] Ozdemir Y, Borekci B, Levet A, Kurudirek M. Assessment of trace element676
concentration distribution in human placenta by wavelength dispersive X-ray677
fluorescence: effect of neonate weight and maternal age. Appl Radiat Isot 2009;67:1790.678
[89] Brophy MH, Harris NF, Crawford IL. Elevated copper and lowered zinc in the679
placentae of pre-eclamptics. Clin Chim Acta 1985;145:107.680
[90] Serdar Z, Gur E, Develioglu O. Serum iron and copper status and oxidative stress681
in severe and mild preeclampsia. Cell Biochem Funct 2006;24:209.682
8/6/2019 OM Un Grutnieciba
31/41
31
[91] Kolusari A, Kurdoglu M, Yildizhan R, Adali E, Edirne T, Cebi A, Demir H,683
Yoruk IH. Catalase activity, serum trace element and heavy metal concentrations, and684
vitamin A, D and E levels in pre-eclampsia. J Int Med Res 2008;36:1335.685
[92] Aksoy H, Taysi S, Altinkaynak K, Bakan E, Bakan N, Kumtepe Y. Antioxidant686
potential and transferrin, ceruloplasmin, and lipid peroxidation levels in women with687
preeclampsia. J Investig Med 2003;51:284.688
[93] Vitoratos N, Salamalekis E, Dalamaga N, Kassanos D, Creatsas G. Defective689
antioxidant mechanisms via changes in serum ceruloplasmin and total iron binding690
capacity of serum in women with pre-eclampsia. Eur J Obstet Gynecol Reprod Biol691
1999;84:63.692
[94] Arredondo M, Nunez MT. Iron and copper metabolism. Mol Aspects Med693
2005;26:313.694
[95] WHO. The World Health Report 2002: Reducing risks, promoting healthy life.695
Geneva: World Health Organisation, 2002.696
[96] Uriu-Adams JY, Keen CL. Zinc and reproduction: effects of zinc deficiency on697
prenatal and early postnatal development. Birth Defects Res B Dev Reprod Toxicol698
2010;89:313.699
[97] Swanson CA, King JC. Zinc and pregnancy outcome. Am J Clin Nutr700
1987;46:763.701
[98] WHO/FAO/IAEA. Trace Elements in Human Nutrition and Health. Geneva:702
World Health Organisation, 1996.703
8/6/2019 OM Un Grutnieciba
32/41
32
[99] Ilhan N, Ilhan N, Simsek M. The changes of trace elements, malondialdehyde704
levels and superoxide dismutase activities in pregnancy with or without preeclampsia.705
Clin Biochem 2002;35:393.706
[100] Groenen PM, Roes EM, Peer PG, Merkus HM, Steegers EA, Steegers-Theunissen707
RP. Myo-inositol, glucose and zinc concentrations determined in the preconceptional708
period, during and after pregnancy. Eur J Obstet Gynecol Reprod Biol 2006;127:50.709
[101] Harley K, Eskenazi B, Block G. The association of time in the US and diet during710
pregnancy in low-income women of Mexican descent. Paediatr Perinat Epidemiol711
2005;19:125.712
[102] King JC. Determinants of maternal zinc status during pregnancy. Am J Clin Nutr713
2000;71:1334S.714
[103] Goldenberg RL, Tamura T, Neggers Y, Copper RL, Johnston KE, DuBard MB,715
Hauth JC. The effect of zinc supplementation on pregnancy outcome. JAMA716
1995;274:463.717
[104] Black RE. Micronutrients in pregnancy. Br J Nutr 2001;85 Suppl 2:S193.718
[105] Garg HK, Singhal KC, Arshad Z. A study of the effect of oral zinc719
supplementation during pregnancy on pregnancy outcome. Indian J Physiol Pharmacol720
1993;37:276.721
[106] Caulfield LE, Zavaleta N, Figueroa A, Leon Z. Maternal zinc supplementation722
does not affect size at birth or pregnancy duration in Peru. J Nutr 1999;129:1563.723
[107] Osendarp SJ, van Raaij JM, Arifeen SE, Wahed M, Baqui AH, Fuchs GJ. A724
randomized, placebo-controlled trial of the effect of zinc supplementation during725
8/6/2019 OM Un Grutnieciba
33/41
33
pregnancy on pregnancy outcome in Bangladeshi urban poor. Am J Clin Nutr726
2000;71:114.727
[108] Jonsson B, Hauge B, Larsen MF, Hald F. Zinc supplementation during pregnancy:728
a double blind randomised controlled trial. Acta Obstet Gynecol Scand 1996;75:725.729
[109] Kiilholma P, Paul R, Pakarinen P, Gronroos M. Copper and zinc in pre-eclampsia.730
Acta Obstet Gynecol Scand 1984;63:629.731
[110] Cherry FF, Bennett EA, Bazzano GS, Johnson LK, Fosmire GJ, Batson HK.732
Plasma zinc in hypertension/toxemia and other reproductive variables in adolescent733
pregnancy. Am J Clin Nutr 1981;34:2367.734
[111] Diaz E, Halhali A, Luna C, Diaz L, Avila E, Larrea F. Newborn birth weight735
correlates with placental zinc, umbilical insulin-like growth factor I, and leptin levels in736
preeclampsia. Arch Med Res 2002;33:40.737
[112] Acikgoz S, Harma M, Mungan G, Can M, Demirtas S. Comparison of738
angiotensin-converting enzyme, malonaldehyde, zinc, and copper levels in preeclampsia.739
Biol Trace Elem Res 2006;113:1.740
[113] Kumru S, Aydin S, Simsek M, Sahin K, Yaman M, Ay G. Comparison of serum741
copper, zinc, calcium, and magnesium levels in preeclamptic and healthy pregnant742
women. Biol Trace Elem Res 2003;94:105.743
[114] Yousef MI, El-Hendy HA, El-Demerdash FM, Elagamy EI. Dietary zinc744
deficiency induced-changes in the activity of enzymes and the levels of free radicals,745
lipids and protein electrophoretic behavior in growing rats. Toxicology 2002;175:223.746
[115] Jain S, Sharma P, Kulshreshtha S, Mohan G, Singh S. The role of calcium,747
magnesium, and zinc in pre-eclampsia. Biol Trace Elem Res 2010;133:162.748
8/6/2019 OM Un Grutnieciba
34/41
34
[116] Bassiouni BA, Foda AI, Rafei AA. Maternal and fetal plasma zinc in pre-749
eclampsia. Eur J Obstet Gynecol Reprod Biol 1979;9:75.750
[117] Kiilholma P, Gronroos M, Erkkola R, Pakarinen P, Nanto V. The role of calcium,751
copper, iron and zinc in preterm delivery and premature rupture of fetal membranes.752
Gynecol Obstet Invest 1984;17:194.753
[118] Ademuyiwa O, Odusoga OL, Adebawo OO, Ugbaja RN. Endogenous antioxidant754
defences in plasma and erythrocytes of pregnant women during different trimesters of755
pregnancy. Acta Obstet Gynecol Scand 2007:1.756
[119] Wood RJ. Manganese and birth outcome. Nutr Rev 2009;67:416.757
[120] Vigeh M, Yokoyama K, Ramezanzadeh F, Dahaghin M, Fakhriazad E,758
Seyedaghamiri Z, Araki S. Blood manganese concentrations and intrauterine growth759
restriction. Reprod Toxicol 2008;25:219.760
[121] Zota AR, Ettinger AS, Bouchard M, Amarasiriwardena CJ, Schwartz J, Hu H,761
Wright RO. Maternal blood manganese levels and infant birth weight. Epidemiology762
2009;20:367.763
[122] Jones EA, Wright JM, Rice G, Buckley BT, Magsumbol MS, Barr DB, Williams764
BL. Metal exposures in an inner-city neonatal population. Environ Int 2010;36:649.765
[123] Than NG, Romero R, Tarca AL, Draghici S, Erez O, Chaiworapongsa T, Kim766
YM, Kim SK, Vaisbuch E, Tromp G. Mitochondrial manganese superoxide dismutase767
mRNA expression in human chorioamniotic membranes and its association with labor,768
inflammation, and infection. J Matern Fetal Neonatal Med 2009;22:1000.769
[124] Buettner GR. The pecking order of free radicals and antioxidants: lipid770
peroxidation, alpha-tocopherol, and ascorbate. Arch Biochem Biophys 1993;300:535.771
8/6/2019 OM Un Grutnieciba
35/41
35
[125] Poston L, Chappell LC, Seed P, Shennan A. Biomarkers for oxidative stress in772
pre-eclampsia. Pregnancy Hypertension 2011;1:22.773
[126] Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E,774
Selenium, and Carotenoids. National Academy Press, 2000. p.284.775
[127] Packer JE, Slater TF, Willson RL. Direct observation of a free radical interaction776
between vitamin E and vitamin C. Nature 1979;278:737.777
[128] Burton GW, Foster DO, Perly B, Slater TF, Smith IC, Ingold KU. Biological778
antioxidants. Philos Trans R Soc Lond B Biol Sci 1985;311:565.779
[129] Xu H, Perez-Cuevas R, Xiong X, Reyes H, Roy C, Julien P, Smith G, von780
Dadelszen P, Leduc L, Audibert F, Moutquin JM, Piedboeuf B, Shatenstein B, Parra-781
Cabrera S, Choquette P, Winsor S, Wood S, Benjamin A, Walker M, Helewa M, Dube J,782
Tawagi G, Seaward G, Ohlsson A, Magee LA, Olatunbosun F, Gratton R, Shear R,783
Demianczuk N, Collet JP, Wei S, Fraser WD. An international trial of antioxidants in the784
prevention of preeclampsia (INTAPP). Am J Obstet Gynecol 2010;202:239 e1.785
[130] Roberts JM, Myatt L, Spong CY, Thom EA, Hauth JC, Leveno KJ, Pearson GD,786
Wapner RJ, Varner MW, Thorp JM, Jr., Mercer BM, Peaceman AM, Ramin SM,787
Carpenter MW, Samuels P, Sciscione A, Harper M, Smith WJ, Saade G, Sorokin Y,788
Anderson GB. Vitamins C and E to prevent complications of pregnancy-associated789
hypertension. N Engl J Med 2010;362:1282.790
[131] Poston L, Briley AL, Seed PT, Kelly FJ, Shennan AH. Vitamin C and vitamin E791
in pregnant women at risk for pre-eclampsia (VIP trial): randomised placebo-controlled792
trial. Lancet 2006;367:1145.793
8/6/2019 OM Un Grutnieciba
36/41
36
[132] McCance DR, Holmes VA, Maresh MJ, Patterson CC, Walker JD, Pearson DW,794
Young IS. Vitamins C and E for prevention of pre-eclampsia in women with type 1795
diabetes (DAPIT): a randomised placebo-controlled trial. Lancet 2010;376:259.796
[133] Maia PA, Figueiredo RC, Anastacio AS, Porto da Silveira CL, Donangelo CM.797
Zinc and copper metabolism in pregnancy and lactation of adolescent women. Nutrition798
2007;23:248.799
[134] American Dietetic Association. Position of the American Dietetic Association:800
nutrition management of adolescent pregnancy. J Am Diet Assoc 1989;89:104.801
[135] Naeye RL. Teenaged and pre-teenaged pregnancies: consequences of the fetal-802
maternal competition for nutrients. Pediatrics 1981;67:146.803
[136] Amuzu A, Carson C, Watt HC, Lawlor DA, Ebrahim S. Influence of area and804
individual lifecourse deprivation on health behaviours: findings from the British805
Women's Heart and Health Study. Eur J Cardiovasc Prev Rehabil 2009;16:169.806
[137] Hampson SE, Martin J, Jorgensen J, Barker M. A social marketing approach to807
improving the nutrition of low-income women and children: an initial focus group study.808
Public Health Nutr 2009;12:1563.809
[138] Department of Health. Dietary reference values for foodenergy and nutrients for810
the United Kingdom. Report on Social Subjects no. 41. London, 1991.811
812
813
814
815
816
8/6/2019 OM Un Grutnieciba
37/41
37
Table 1: Requirement of micronutrient intakes for selenium, copper, zinc, manganese,817
vitamin C and vitamin E. RDA: Recommended Dietary Allowance; RNI:818
Reference Nutrient Intakes and NR: Normative Requirement Estimate. Values819
taken from 1Institute of Medicine [77, 126], 2Department of Health [138] and820
3WHO/FAO/IAEA [98]821
822
Selenium
(g/d)
Copper
(g/d)
Zinc
(mg/d)
Manganese
(mg/d)
Vitamin C
(mg/d)
Vitamin E
(g/d)
RDA1
Female
Adult 55 900 8 1.8 75 15
Pregnancy 60 1,000 11 2 85 15
Upper
limit 400 10,000 40 2,000 1,000
RNI
2
Female
Adult 60 1,200 7 1.4 40 -
Pregnancy 75 1,500 7 - 50 -
- - -
NR3
Female
Adult 30 1,350 1 - - -
Pregnancy - 1,150 2 -
823
824
825
826
827
8/6/2019 OM Un Grutnieciba
38/41
38
Figure Legends828
829
Figure 1: Diagram of the maternal fetal interface in early pregnancy. Extravillous830
cytotrophoblast cells migrate away from the cell column of the anchoring villus and831
invade through the maternal deciduas and inner third of the myometrium in o rder to gain832
access to maternal blood supply via maternal spiral arteries. Transformation of the833
maternal spiral arteries occurs as endovascular trophoblast help convert the endothelial834
cells lining the arteries into an amorphous fibrinoid matrix which is unresponsive to835
vasoactive stimuli, and serves to enlarge the vascular lumen maximising blood supply to836
the intervillous space.837
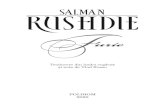
838
Figure 2: Major pathways of reactive oxygen species generation and metabolism.839
Superoxide can be generated by specialised enzymes, such as the xanthine or NADPH840
oxidases, or as a byproduct of cellular metabolism, particularly the mitochondrial electron841
transport chain. Superoxide dismutase (SOD), both Cu/Zn and Mn SOD then converts the842
superoxide to hydrogen peroxide (H2O2) which has to be rapidly removed from the843
system. This is generally achieved by catalase or peroxidases, such as the selenium844
dependent glutathione peroxidases (GPxs) which use reduced glutathione (GSH) as the845
electron donor.846
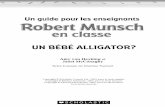
847
Figure 3: Synergistic mechanisms ofvitamin C (ascorbate) and vitamin E (-tocopherol)848
to prevent lipid peroxidation. O2.oxygen free radical.849
850
8/6/2019 OM Un Grutnieciba
39/41
39
Figure 1.851852
853
854855
856
857
858
859
860
861
862
863
864
865
8/6/2019 OM Un Grutnieciba
40/41
40
Figure 2.866867
868869
870
871872
873874
875876877
878879
880881
882883884
885886887
888889
890891892
893894
895
896
897
898
899
900
901
902
H+
O2
O2-.
H2O2
H2O H2O
GSSG
2GSH
Cu/Zn & Mn SOD
NAD(P)H
NAD(P)+
Se GPxsCatalase
Glutathione reductase
Xanthine oxidase
NADPH oxidase
Mitochondrial Electron Transport Chain
8/6/2019 OM Un Grutnieciba
41/41
Figure 3.903904
905906
Ascorbate
Ascorbate
Hydrophilic
-tocopherol
-tocopherol
Lipophilic
Plasma membrane protein
Lipid peroxide
O2
Top Related