





Talen
Pages
Wettelijk


FETAL RENAL ANOMALIES: diagnosis, management and outcome.

cover: Albert Damen sr. print Budde-Elinkwijk, Nieuwegein

FETAL RENAL ANOMALIES: diagnosis, management and outcome
Afwijkingen aan nieren en urinewegen bij de foetus: diagnose, behandeling en uitkomst.
(met een samenvatting in het Nederlands)
Proefschrift
ter verkrijging van de graad van doctor
aan de Universiteit Utrecht
op gezag van de Rector Magnificus, Prof. dr. W.H. Gispen,
ingevolge het besluit van het College voor Promoties
in het openbaar te verdedigen op
dinsdag 14 december 2004 des middags te 14.30 uur
door
Henrica Antonia Maria Damen – Elias
geboren te Tegelen, 27 mei 1941

Promotor: Prof. dr. G.H.A. Visser Department of Perinatology and Gynaecology
University Medical Centre Utrecht
Copromotores: Dr. T.P.V.M. de Jong Department of Paediatric Urology University Medical Centre Utrecht
Dr. P.H. Stoutenbeek Department of Perinatology and Gynaecology University Medical Centre Utrecht
ISBN: 90-9018851-7
CIP-DATA KONINKLIJKE BIBLIOTHEEK DEN HAAG Damen-Elias, Henrica Antonia Maria FETAL RENAL ANOMALIES: diagnosis, management and outcome Utrecht, Universiteit Utrecht, Faculteit Geneeskunde Thesis Universiteit Utrecht
Financial support for the publication of the this thesis is gratefully acknowledged: Stichting Kindernierziekten Easote Pie Medical Toshiba Medical Systems Europe Nierstichting Nederland

What does wisdom benefits us, if we do not possess love.

Referents: Prof. dr. F. van Bel Department of Neonatology
University Medical Centre Utrecht
Prof. dr. J.L.H.R. Bosch Department of Urology University Medical Centre Utrecht
Prof. dr. H.W. Bruinse
Department of Perinatology and Gynaecology University Medical Centre Utrecht
Prof. dr. J.M. Nijman
Department of Urology University Medical Centre Groningen
Prof. dr. J.W. Wladimiroff
Department of Obstetrics and Gynaecology Erasmus Medical Centre Rotterdam
Paranimfen: Drs. P.J. Damen
Mevr. M.J. Korenromp

Table of contents 7
Chapter 1 Introduction and aims of the thesis Chapter 2 Intra- and interobserver variability of fetal kidney and adrenal gland measurements
revised version resubmitted to Ultrasound in Obstetrics and Gynaecology
Chapter 3 Growth and size charts of the fetal kidney and the renal pelvis
revised version resubmitted to Ultrasound in Obstetrics and Gynaecology
Chapter 4 Growth and size charts of the fetal adrenal gland
revised version resubmitted to Ultrasound in Obstetrics and Gynaecology
Chapter 5 Congenital renal tract anomalies: outcome and follow-up of 402 cases detected antenatally over a period of 15 years.
in press: Ultrasound in Obstetrics and Gynaecology
Chapter 6 Concomitant anomalies in 100 children with unilateral multicystic kidney
in press: Ultrasound in Obstetrics and Gynaecology
Chapter 7 Mild pyelectasis diagnosed by prenatal ultrasound is not a predictor of urinary tract morbidity in childhood
in press: Ultrasound in Obstetrics and Gynaecology
Chapter 8 Variability in dilatation of the fetal renal pelvis during a bladder filling cycle
in press: Ultrasound in Obstetrics and Gynaecology
Chapter 9 Summary, discussion and conclusion
Nederlandse samenvatting
Dankwoord
Curriculum Vitae


Chapter 1 Introduction, aims and outline of the thesis

10 Chapter 1
introduction
Interest in fetal development has grown enormously in the past decades. Till then
non-invasive methods were used to asses fetal health such as the feeling of
movements by the pregnant woman, measuring growth by palpation of the fundal
height and auscultation of the fetal heart tones with a wooden stethoscope. X-ray
examination was used in search for fetal abnormalities and to diagnose multiple
pregnancies but the questionable safety of such investigation in pregnancy made this
method unsuitable for routine examinations.
All changed when it became possible to observe the fetus in utero by ultrasound. As
early as 1958, Donald et al1 showed the outline of the fetal skull. The technical and
methodological development of this technique made it possible to investigate the
fetus directly and the consequence of this quickly expanding and improving new
technique has been an increasing amount of information concerning fetal
morphological and physiological development during pregnancy. Further
improvement of the equipment with high-resolution real-time ultrasound has given the
possibility to more detailed information of the fetus and later on transvaginal
sonography has made it possible to obtain detailed information of early embryonic
development.
The introduction of routine prenatal ultrasound scanning since the early 1980’s in
several countries in Europe has increased our knowledge on morphology and
functional development of the fetus. Moreover it became possible to diagnose
anomalies in utero. In population studies minor or major structural anomalies are
detected in 2 to 3 % of cases2-5. Abnormalities of the urinary tract account for 15-20%
of these anomalies with a detection rate of approximately 90%2, 4.
The fetal kidneys can first be visualised by transabdominal ultrasound at 9 weeks
gestational age and can be seen in all cases from 12 weeks onwards. In early
pregnancy the echogenity of the fetal kidneys is high but this decreases in the course
of gestation when they become hypoechoic6. At about 28 weeks the renal pyramids
can be detected and also the borders of the kidneys can be seen more clearly with
progressing gestational age, since fat tissue is developing around the kidneys from
that moment on.

introduction, aims and outline 11
The fetal bladder can be visualised from the onset of urine production, which occurs
at about 10 weeks gestation7. At 11 weeks of gestation the bladder can be visualised,
both transvaginally and transabdominally, in 80% of fetuses and at 13 weeks
almost in all fetuses8, 9. It should always be possible to visualize the bladder when
the crown-rump length is more than 67 mm (13+ weeks).
The fetal adrenal glands are visible by ultrasonography as early as 9 weeks of
gestation and in all cases from 12 weeks onwards. In the second trimester they
appear as a disc-like structure in a transverse plane, cranially and medially to the
kidney. Three layers can clearly be distinguished of which the outer layer is
hypoechogenic and the central medulla hyperechoic. In the sagittal view they appear
as heart-shaped figures of low echogenicity.
During the last three decades numerous papers have dealed with the fetal renal
system and its anomalies. Follow-up studies on (long term) outcome are, however,
scarce and this hampers adequate counselling of parents and giving appropriate
treatment advice. Moreover, up to date charts on normal fetal kidney size and growth
are scarce. We therefore formulated the following aims of this thesis.
aims of the thesis
1 – To develop charts of size and growth of the fetal kidney, renal pelvis and adrenal
gland.
2 – To study long-term follow-up of a large cohort of infants with an antenatally
diagnosed renal tract anomaly.
3 – To answer the question whether mild pyelectasis (anteroposterior diameter of the
fetal renal pelvis of 5 – 10 mm) as diagnosed around 18 to 20 weeks of gestation
results in increased morbidity in childhood and therefore requires postnatal
treatment.
4 – To study the relationship between the size of the renal pelvis and the fetal
bladder-filling cycle, to answer the question if fixed cut-off values regarding renal
pelvis dilatation can be used or whether bladder filling has to be taken into account.

12 Chapter 1
outline of the thesis
In Chapters 2 to 4 a prospective longitudinal study is described on size and growth of
the fetal kidney, the fetal renal pelvis and the fetal adrenal gland in 111 fetuses from
16 weeks gestational age onwards till term. These studies were preceded by a study
on intra- and inter-observer variation.
In Chapter 5 we describe the findings and outcome of a large cohort of 402 fetuses in
which urogenital anomalies were detected antenatally. We could use the database of
the ultrasound unit of the department of obstetrics of the University Medical Centre,
Utrecht, The Netherlands, which was established in 1986. At follow-up the youngest
infant was 3 years and the oldest was 17 years (median 7 years 11 months).
In Chapter 6 we present the outcome of 100 fetuses with an antenatally detected
unilateral multicystic kidney. All additional urogenital and other anomalies are
described. According to the advice of the Dutch Society of Paediatric Urology the
non-functioning cystic kidney is removed at approximately 6 months of age to prevent
life-time follow-up of these children because of an increased risk of hypertension10,
infection11 or malignancy12, 13. When the parents decided to do so, each child
underwent a cystoscopy and girls also a colposopy prior to the operation. All these
findings are included in the follow-up of these children (median 5 years and 4
months).
For Chapter 7 we could use the data of the ultrasound department of the Amphia
Hospital, Oosterhout, The Netherlands, which was established since 1982. Two
hundred and eight children, who had had a mild pyelectasis of 5 – 10 mm at 18 to 20
weeks gestation, were compared with 416 matched controls regarding voiding and
defecation patrons and urinary tract infections. A validated questionnaire, as used in
the International Reflux Study in children, was used for this purpose.
In Chapter 8 we describe a study in which 18 third trimester pregnant women are
examined by ultrasound during several fetal bladder-filling cycles, to investigate if
there is a correlation between the size of the renal pelvis and the extent of bladder
filling.
In Chapter 9 a summary and general discussion is described.

introduction, aims and outline 13
references 1 Donald I, Macvicar J, Brown TG. Investigation of abdominal masses by pulsed ultrasound. Lancet 1958;1(7032):1188-95. 2. Grandjean H, Larroque D, Levi S. Sensitivity of routine ultrasound screening of pregnancies in the Eurofetus database. The Eurofetus Team. Ann N Y Acad Sci 1998;847:118-24. 3. Levi S. Ultrasound in prenatal diagnosis: polemics around routine ultrasound screening for second trimester fetal malformations. Prenat Diagn 2002;22(4):285-95. 4. Levi S. Mass screening for fetal malformations: the Eurofetus study. Ultrasound Obstet Gynecol 2003;22(6):555-8. 5. Stoll C, Clementi M. Prenatal diagnosis of dysmorphic syndromes by routine fetal ultrasound examination across Europe. Ultrasound Obstet Gynecol 2003;21(6):543-51. 6. Green JJ, Hobbins JC. Abdominal ultrasound examination of the first-trimester fetus. Am J Obstet Gynecol 1988;159(1):165-75. 7. McHugo J, Whittle M. Enlarged fetal bladders: aetiology, management and outcome.Prenat Diagn 2001;21(11):958-63. 8. Rosati P, Guariglia L. Transvaginal sonographic assessment of the fetal urinary tract in early pregnancy. Ultrasound Obstet Gynecol 1996;7(2):95-100. 9. Braithwaite JM, Armstrong MA, Economides DL. Assessment of fetal anatomy at 12 to 13 weeks of gestation by transabdominal and transvaginal sonography. Br J Obstet Gynaecol 1996;103(1):82-5. 10. Webb NJ, Lewis MA, Bruce J, Gough DC, Ladusans EJ, Thomson AP, et al. Unilateral multicystic dysplastic kidney: the case for nephrectomy. Arch Dis Child 1997;76(1):31-4. 11. Wacksman J, Phipps L. Report of the Multicystic Kidney Registry: preliminary findings. J Urol 1993;150(6):1870-2. 12. Elder JS, Hladky D, Selzman AA. Outpatient nephrectomy for nonfunctioning kidneys. J Urol 1995;154(2 Pt 2):712-4; discussion 714-5. 13. LaSalle MD, Stock JA, Hanna MK. Insurability of children with congenital urological anomalies. J Urol 1997;158(3 Pt 2):1312-5.


Chapter 2 Intra- and interobserver variability of fetal kidney and adrenal gland
measurements
H.A.M. Damen - Eliasa, G.H.A. Vissera, P. Westers b, L. Pistorius a
a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Centre for Biostatistics, Utrecht University, The Netherlands

16 Chapter 2
ABSTRACT
Objectives: To assess the intra- and interobserver variability of fetal kidney and fetal
adrenal gland measurement by ultrasound.
Methods: Data were obtained prospectively by experienced ultrasonographers. Thirty
fetuses were measured for the intraobserver analysis and 20 fetuses for the
interobserver analysis. Length, anteroposterior and transverse diameter from both
the right and left kidney and from the length of the right and left adrenal gland were
measured 3 times. Statistical analysis was performed by SPSS.
Results: The reproducibility of the measurements of the kidney and of the adrenal
gland were good with an intraclass correlation above 0,80 for all measurements for
both the intraobserver and interobserver analysis.
Conclusions: The high degree of intra- and interobserver reproducibility indicates that
the three dimensions of the kidney and adrenal gland length are technically feasible
to measure.

Intra- and interobserver variability 17
INTRODUCTION
Many reference curves of the fetal renal kidney have been published1-7. Knowledge of
the normal range of the measurements of the fetus is essential when during
screening an anomaly is identified. No intraobserver and interobserver variation
analysis was done prior to any of these studies. Only Bertagnoli2 in 1983 reported on
the differences in measurements between 3 operators who each used a different
ultrasound machine. Some studies describe the design, the patient selection and the
methods of analysis8-10 but do not involve differences in intraobserver and
interobserver measurements. The discriminatory ability of a diagnostic test is in large
extent depending on the repeatability of the test.
The aim of this study was to assess the intra- and interobserver reproducibility of the
length, the anteroposterior and the transverse measurements of the fetal kidney and
of the length of the adrenal gland by ultrasound.
MATERIALS AND METHODS
Thirty pregnant women were asked to participate in the study for the intraobserver
variation analysis and another twenty for the interobserver variation analysis. All
women consented to participate in the study There were no exclusion criteria. Two
experienced ultrasonographers, (HDE, LP) examined the fetuses. Each observer
attempted to obtain three measurements with different time intervals between each
measurement. The sonographers were not allowed to see their own measurements
or to watch each other performing the measurements to avoid any possible
influence.
In both investigations the length, the anteroposterior and transverse diameter of the
kidney and the length of the adrenal gland were measured transabdominally with the
multifrequency transducer PVM 375 AT of the Toshiba Power Vision 6000, type SSA
370 A (manufacturer Toshiba, Tokyo, Japan).
In a sagittal plane when the full length of the kidney with the renal pelvis was
visualised the length of the kidney was measured and in the same sectional plane
the length of the combination of the kidney and the adrenal gland. Subsequently the
length of the adrenal gland was determined by subtraction of the kidney length from
the combined length. Perpendicular to this plane in the largest sectional plane, the
anteroposterior and transverse diameter of both kidneys were measured. The data

18 Chapter 2
were recorded on a photograph and stored in a database.
Statistical analysis was performed by using SPSS, version 10.1 (Statistical Product
and Service Solutions, Chicago). The mean and standard deviation were calculated
to determine if there was a good consistency between the measurements. In addition
the range, the Cronbachs alpha (α) and the intra class correlation (ICC) were
calculated. The range is the distance between the highest and lowest value.
Cronbachs α is a statistical index for internal consistency between the
measurements. The index ranges from 0 = bad to 1 = excellent. The ICC is the
measure of concordance and is a statistic that describes the reproducibility of
repeated measures in the same subject and indicates true variance as a fraction of
the total variance. Landis and Koch11 have indicated the meaning of the different
values of the ICC and a value of 0.61-0.80 has a good agreement and larger > 0.81
an excellent one. The value of ICC of 1 for repeated measurements indicates perfect
reproducibility while a value of 0 is interpreted as no better or worse than that
expected by chance.
RESULTS
intraobserver variation analysis
The kidney length, kidney anteroposterior diameter, kidney transverse diameter and
adrenal gland length could be measured 3 times in all 30 women. Intraobserver
agreement is given in Table 1. Statistic analysis shows a high alpha above the 0,9
and also a high IC above 0,8 for all different measurements.
Table 1 – Intraobserver variation of length, anteroposterior and transverse diameter of the kidney and of length of the adrenal gland.
variable mean ± std.dev alpha intra class correlation (95% CI) RiKiL 22,706 ± 3.486 0.956 0.955 (0.924 – 0.976) LeKiL 22,413 ± 3.434 0.970 0.969 (0.947 – 0.983) RiKiAP 15,217 ± 2.292 0.912 0.911 (0.850 – 0.952) LeKiAP 15,190 ± 2.232 0.919 0.918 (0.862 – 0.956) RiKiTr 15,172 ± 2.238 0.933 0.931 (0.883 – 0.963) LeKiTr 15,412 ± 2.391 0.939 0.937 (0.893 – 0.967) RiGL 5,316 ± 1.259 0.935 0.931 (0.885 – 0.963) LeGL 5,275 ± 1.345 0.930 0.928 (0.879 – 0.962)
RiKiL = right kidney length, LeKiL = left kidney length, RiKiAP = right kidney anterior/ posterior diameter, LeKiAP = left kidney anterior/ posterior diameter, RiKiTr = right kidney transverse diameter, LeKiTr = left kidney transverse diameter, RiGL = right adrenal gland length, LeGL = left adrenal gland length.

Intra- and interobserver variability 19
interobserver variation analysis
Both investigators could take all measurements 3 times in all 20 women. The
interobserver analysis is given in Table 2. There was a high alpha above 0,9 for all
measurements as well as a high IC above 0,8. There was a high level of agreement
between the two observers.
Table 2 - Interobserver variation of length, anteroposterior diameter and transverse diameter of the kidney and of length of the adrenal gland.
HDE* = observer 1, LP# = observer 2 RiKiL = right kidney length, LeKiL = left kidney length, RiKiAP = right kidney anterior/ posterior diameter, LeKiAP = left kidney anterior/ posterior diameter, RiKiTr = right kidney transverse diameter, LeKiTr = left kidney transverse diameter, RiGL = right adrenal gland length, LeGL = left adrenal gland length. DISCUSSION
Measurements of the kidney are of importance when an anomaly is identified.
Measurements of the adrenal gland may be of importance in high-risk pregnancies
when intra uterine growth retardation is suspected12-14, when mothers use
glucocosteriods15 for a prolonged period of time or in case of congenital adrenal
hyperplasia16, 17. A valuable screenings test should be both feasible and repeatable.
An intra- and interobserver analysis should be evaluated and measurements should
only be introduced in routine setting if a good sensitivity and specificity is
demonstrated. It was technically feasible to take three measurements of the fetal
kidney and the length of the adrenal gland. We used various indices and coefficients
to assess intra- and interobserver variability and found a good agreement of both for
the intraobserver analysis and for the interobserver analysis. Comparison of our
results with those of others is not possible because there is no study in literature on
intra- and interobserver analysis of fetal kidney and adrenal gland measurements.
variable mean ± st.dev observer 1 observer 2
range .
alpha intraclass correlation 95% CI)
HDE* LP# HDE LP RiKiL 34.320 ± 8.155 34.530 ± 8.043 0.265 0.460 0.997 0.9822 (0.967 – 0.992) LeKiL 33.823 ± 7.782 34.115 ± 7.611 0.185 0.265 0.999 0.9928 (0.987 – 0.997) RiKiAP 19.936 ± 3.848 19.090 ± 3.907 0.315 0.100 0.992 0.9513 (0.912 – 0.978) LeKiAP 19.260 ± 4.271 18.960 ± 4.032 0.245 0.075 0.998 0.9392 (0.891 – 0.997) RiKiTr 23.411 ± 5.754 23.460 ± 5.955 0.992 0.110 0.996 0.9786 (0.961 – 0.990) LeKiTR 22.676 ± 5.043 22.045 ± 5.200 0.115 0.115 0.978 0.9445 (0.900 – 0.972) RiGL 8.916 ± 2.068 8.696 ± 1.841 0.996 0.973 0.986 0.9094 (0.841 – 0.957) LeGL 8.921 ± 1.975 8.738 ± 1.803 0.215 0.145 0.971 0.8481 (0.744 – 0.926)

20 Chapter 2
REFERENCES 1. Jeanty P, Dramaix-Wilmet M, Elkhazen N, Hubinont C, van Regemorter N. Measurements of fetal kidney
growth on ultrasound. Radiology 1982;144(1):159-62.
2. Bertagnoli L, Lalatta F, Gallicchio R, Fantuzzi M, Rusca M, Zorzoli A, et al. Quantitative characterization of
the growth of the fetal kidney. J Clin Ultrasound 1983;11(7):349-56.
3. Sagi J, Vagman I, David MP, Van Dongen LG, Goudie E, Butterworth A, et al. Fetal kidney size related to
gestational age. Gynecol Obstet Invest 1987;23(1):1-4.
4. Pruggmayer M, Terinde R. [Fetal kidney screening: growth curves and indices]. Geburtshilfe Frauenheilkd
1989;49(8):705-10.
5. Cohen HL, Cooper J, Eisenberg P, Mandel FS, Gross BR, Goldman MA, et al. Normal length of fetal
kidneys: sonographic study in 397 obstetric patients. AJR Am J Roentgenol 1991;157(3):545-8.
6. Scott JE, Wright B, Wilson G, Pearson IA, Matthews JN, Rose PG. Measuring the fetal kidney with
ultrasonography. Br J Urol 1995;76(6):769-74.
7. Chitty LS, Altman DG. Charts of fetal size: kidney and renal pelvis measurements. Prenat Diagn
2003;23(11):891-7.
8. Royston P, Wright EM. How to construct 'normal ranges' for fetal variables. Ultrasound Obstet Gynecol
1998;11(1):30-8
9. Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound Obstet
Gynecol 1993;3(6):378-84.
10. Altman DG, Chitty LS. Charts of fetal size: 1. Methodology. Br J Obstet Gynaecol 1994;101(1):29-34.
11. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics
1977;33(1):159-74.
13. Hata K, Hata T, Kitao M. Ultrasonographic identification and measurement of the human fetal adrenal gland
in utero. Int J Gynaecol Obstet 1985;23(5):355-9.
14. Hata K, Hata T, Kitao M. Ultrasonographic identification and measurement of the human fetal adrenal gland
in utero: clinical application. Gynecol Obstet Invest 1988;25(1):16-22.
15. Bronshtein M, Tzidony D, Dimant M, Hajos J, Jaeger M, Blumenfeld Z. Transvaginal ultrasonographic
measurements of the fetal adrenal glands at 12 to 17 weeks of gestation. Am J Obstet Gynecol
1993;169(5):1205-10.

Intra- and interobserver variability 21 16. Esser T, Chaoui R. Enlarged adrenal glands as a prenatal marker of congenital adrenal hyperplasia: a
report of two cases. Ultrasound Obstet Gynecol 2004;23(3):293-7.
17. Saada J, Grebille AG, Aubry MC, Rafii A, Dumez Y, Benachi A. Sonography in prenatal diagnosis of
congenital adrenal hyperplasia. Prenat Diagn 2004;24(8):627-30.


Chapter 3 Growth and size charts of the fetal kidney and the renal pelvis.
H.A.M. Damen - Eliasa, R.H. Stigtera,c, P. Westers b, G.H.A. Vissera
a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Centre for Biostatistics, Utrecht University, The Netherlands c Department of Obstetrics and Gynaecology, Deventer Hospital, Deventer, The Netherlands

24 Chapter 3
ABSTRACT
Objectives The aim of this study was to develop a reference curve for the size and
growth of the fetal kidney and of the fetal renal pelvis.
Methods Prospective longitudinal study including 111 fetuses. Ultrasound
examinations were made every four weeks beginning in one half of the cases at 16
weeks and in the other half at 18 weeks. Length, anteroposterior and transverse
diameter from both the right and left kidney and the anteroposterior diameter and
transverse diameter from the right and left renal pelvis were measured. Statistical
analysis was performed by multilevel analysis.
Results Fitted 5th, 50th and 95th centile charts are presented with the raw data.
Comparisons were made with previously published data.
Conclusions The new charts for size and growth are of use for the three dimensions
and for the perimeter of the fetal kidney and for the size of the renal pelvis.

Charts of fetal kidney and renal pelvis 25
INTRODUCTION
Knowledge of the normal range of the dimensions of the fetal kidney and renal pelvis
is essential. Various papers on the intrauterine growth of the renal size have been
published but many failed to validate gestational age by measuring crown-rump
length1-5, do not cover the whole of the second and third trimester of pregnancy1, 2, 6-8,
did not measure the kidney in three dimensions1, 2, 4-6 or used only pre-term born
children or post-mortem specimens9-11. Several studies used a mixture of cross-
sectional and longitudinal data1, 3-6, 8, 11.
Cross-sectional data obtained by measurements of each fetus on a single occasion
give information on size, whereas longitudinal data obtained by measurements of
fetuses on a series of occasions may be used for a reference curve for size and
growth12-15. The difficulty of any longitudinal study to construct nomograms is that
there are some missing data. This problem has been overcome by the approach of
multilevel analysis, which is able to correct for this problem16. This statistical
technique allows for the dependency of measurements in hierarchically structured
data, whereas traditional regression analysis presupposes the independence of
observations. Another advantage of this technique is that it can separately examine
the effects of variables of different levels (repeated measures) and can also be used
when measurements have been made at different times (e.g. recordings at 16
weeks, at 16 2/7 weeks or 16 6/7 weeks of gestation).
An intraobserver and interobserver variation analysis forms no part of any publication
of reference curves of the fetal renal kidney. Only Bertagnoli6 in 1983 performed an
interobserver analysis between 3 operators who each used a different ultrasound
machine. Some studies describe the design, the patient selection and the methods of
analysis but do not report on intra- or interobserver error12, 13, 15.
The aim of this study was to estimate a reference curve for the size and growth of the
fetal kidney and fetal renal pelvis.

26 Chapter 3
MATERIAL AND METHODS
One hundred and twelve low risk women with 116 fetuses (4 twin pregnancies) were
asked during an ultrasound scan for validating gestational age by measuring the
crown-rump length, to participate in the study. After written informed consent the
women were divided in two groups in order of registration. One half was examined at
around 16 – 20 – 24 - 28 - 32 - 36 and 40 weeks of gestational age and the other half
at around 18 – 22 – 26 – 30 – 34 - 38 and 42 weeks of gestational age. All
examinations were made by one ultrasonographer (HDE), using the multifrequency,
abdominal transducer PVM 375 AT of the Toshiba Power Vision 6000, type SSA 370
A with (manufacturer Toshiba, Tokyo, Japan). An intra- and interobserver variation
analysis preceded the study resulting in a good consistency in measurements.
Exclusion criteria were: mono-chorionic twin pregnancies, chromosomal or congenital
defects of the fetus, small for gestational age at birth (SGA = weight at birth <2.3%(17)
percentile for gestational age) and maternal disease which might effect fetal growth
(diabetes mellitus, hypertension requiring treatment).
The length of the kidney was measured when in a sagittal plane the full length with
the renal pelvis was visualised. Perpendicular to this, in the largest sectional plane,
the anteroposterior (AP) and transverse diameter of the kidney were measured by
placing the callipers from outer to outer border. In the same sectional plane the AP
and transverse diameters of the renal pelvis were measured by placing the callipers
on the inner borders of the renal tissue. All measurements were obtained three times
and the data were averaged and stored in a database.
Statistical analysis was performed by multilevel analysis with the software program
Mln (Multilevel Model Project, London, UK)16 and SPSS, version 10.1 (Statistical
Product and Service Solutions, Chicago) to construct nomograms (medians and the
5th and 95th centiles).
RESULTS
Five fetuses were excluded: small for gestational age (n=2), congenital anomalies
(n=3; triploidy, clubfoot and hydronephrosis >10mm anteroposterior diameter of the
renal pelvis). Of the remaining 107 woman and 111 fetuses all measurements could
be obtained from both kidneys and both renal pelves with a total of 628 data for each
separate measurement for length, anteroposterior diameter and transverse diameter

Charts of fetal kidney and renal pelvis 27
of both kidneys and for the anteroposterior and transverse diameter of both renal
pelves.
Statistical analysis was performed on all separate measurement from the right and
left fetal kidney. The charts of length, anteroposterior and transverse diameter and
perimeter of the left and right kidney were about identical with a high correlation
coefficient between the measurements from the right and left side: R = 0.993 for
length, R = 0.976 for AP-diameter, R = 0.969 for transverse diameter and R = 0.986
for perimeter.
There was no asymmetry between the right and left renal pelvic measurements
(Table 1: Kappa 0,459). The charts made of the anteroposterior and transverse
diameter of the right and left renal pelvis were similar with correlation coefficients
between measurements of the right and left side of: R = 0.777 for the AP-diameter
and R = 0.795 for the transverse diameter. In only 16 of 628 comparisons between
right and left pelvic size there was a difference of more than 2 millimetres between
the measurements (Table 1).
Table 1 – Partition of the dimensions of the right and left renal pelvis. Kappa 0,459
The data of all right and left kidney and renal pelvis measurements were averaged to
obtain the reference charts. The account of the nomograms of the 5th, 50th and 95th
fitted centiles of length, anteroposterior and transverse diameter and of the perimeter
from the kidney are shown in Table 2 with the corresponding charts (Figures 1 to 4).
right renal pelvis measurements (mm) 0–<2 mm 2–<4 mm 4–<6 mm 6–<8 mm 8–<10 mm total 0 – < 2 mm 93 34 2 - - 129 2 – < 4 mm* 23 240 71 7 1 342 4 – < 6 mm - 46 74 10 - 130 6 – < 8 mm 1 5 10 8 1 25 8 – <10 mm - - - 2 - 2
left renal pelvis measurements (mm)
total 117 325 157 27 2 628

28 Chapter 3
gestational age in weeks
4238343026221814
kidn
ey
leng
th (
mm
)
60
55
50
45
40
35
30
25
20
15
10
5
0
Figure 1 – Fitted 5th, 50th and 95th centiles for the kidney length and the raw data.
gestational age in weeks
4238343026221814
kidn
ey
AP
-dia
me
ter
(mm
)
30
25
20
15
10
5
0
Figure 2 – Fitted 5th, 50th and 95th centiles for the anteroposterior kidney diameter and the raw data.

Charts of fetal kidney and renal pelvis 29
gestational age in weeks
4238343026221814
kidn
ey t
rans
vers
e d
iam
eter
(m
m)
40
35
30
25
20
15
10
5
0
Figure 3 – Fitted 5th, 50th and 95th centiles of the transverse kidney diameter and the raw data.
gestational age in weeks
4238343026221814
kidn
ey
perim
ete
r
100
90
80
70
60
50
40
30
20
10
0
Figure 4 – Fitted 5th, 50th and 95th centiles of the perimeter of the kidney and the raw data.

Tab
le 2
– F
itted
cen
tiles
of f
etal
ren
al k
idne
y le
ngth
, ant
erop
oste
rior
diam
eter
, tra
nsve
rse
diam
eter
and
per
imet
er w
ith th
e nu
mbe
r of
fetu
ses
for
exac
t wee
ks b
etw
een
16 a
nd 4
2 w
eeks
of g
esta
tiona
l age
.
wee
ks o
f ge
stat
ion
N
fetu
ses
fitte
d ce
ntile
s ki
dney
leng
th
fitte
d ce
ntile
s ki
dney
ant
erop
oste
rior
diam
eter
fit
ted
cent
iles
kidn
ey tr
ansv
erse
dia
met
er
fitte
d ce
ntile
s ki
dney
per
imet
er
5th
50
th
95th
SD
5th
50
th
95th
SD
5th
50
th
95th
SD
5th
50
th
95th
SD
16
55
12
,9
14,3
15
,7
0,70
7
,4
8,6
9
,8
0,
60
7,3
8,6
9,
9
0,
66
23,5
27
,0
30,6
1,
80
17
14
,3
15,7
17
,2
0,74
8
,2
9,5
10
,7
0,
64
8,3
9,7
11
,1
0,
70
26,2
29
,9
33,7
1,
91
18
56
15,6
17
,1
18,7
0,
79
9,0
10
,4
11,7
0,68
9,
3 10
,8
12,2
0,74
29
,2
33,2
37
,2
2,03
19
16,9
18
,5
20,2
0,
84
9,8
11
,2
12,6
0,71
10
,3
11,8
13
,2
0,
78
31,8
36
,0
40,2
2,
14
20
55
18,2
19
,9
21,6
0,
88
10,6
12
,1
13,5
0,75
11
,2
12,8
14
,4
0,
82
34,6
39
,1
43,5
2,
26
21
20
,0
21,8
23
,7
0,94
11
,3
12,8
14
,4
0,
79
12,1
13
,9
15,4
0,86
37
,9
42,3
46
,9
2,39
22
56
20
,7
22,6
24
,5
0,96
12
,0
13,6
15
,3
0,
83
13
14,8
16
,5
0,
90
39,8
44
,6
49,5
2,
48
23
22
,0
24,0
25
,9
1,00
12
,7
14,4
16
,1
0,
86
13,9
15
,7
17,6
0,94
42
,3
47,3
52
,4
2,59
24
55
23
,2
25,3
27
,3
1,05
13
,4
15,1
16
,9
0,
90
14,7
16
,6
18,6
0,99
44
,6
49,9
55
,2
2,71
25
24,5
26
,6
28,7
1,
10
14,0
15
,8
17,7
0,95
15
,5
17,5
19
,5
1,
03
46,8
52
,4
57,8
2,
84
26
56
25,6
27
,9
30,1
1,
14
14,6
16
,5
18,4
0,98
16
,3
18,4
20
,5
1,
07
49,1
54
,8
60,6
2,
93
27
26
,8
29,0
31
,3
1,19
15
,2
17,2
19
,2
1,
00
17
19,3
21
,4
1,
10
50,9
57
,2
62,8
3,
05
28
55
28,0
30
,4
32,8
1,
23
15,7
17
,8
19,9
1,05
17
,8
20,1
22
,3
1,
15
53,3
59
,5
65,7
3,
16
29
29
,2
31,7
34
,2
1,27
16
,3
18,4
20
,6
1,
10
18,5
20
,8
23,2
1,19
55
,3
61,7
68
,1
3,27
30
54
30
,3
32,9
35
,5
1,31
16
,8
19,0
21
,2
1,
13
19,2
21
,6
24
1,
23
57,2
63
,8
70,5
3,
38
31
31
,5
34,2
36
,8
1,35
17
,3
19,6
21
,8
1,
17
19,9
22
,4
24,9
1,27
59
,0
65,9
72
,7
3,50
32
55
32
,6
35,3
38
,1
1,40
17
,7
20,1
22
,5
1,
20
20,5
23
,1
25,7
1,31
60
,8
67,9
74
,9
3,61
33
34,3
36
,5
40,1
1,
43
18,4
20
,6
23,4
1,23
21
,2
23,7
26
,5
1,
35
63,1
69
,5
77,5
3,
71
34
53
35,0
37
,7
40,8
1,
49
18,6
21
,1
23,6
1,28
21
,8
24,5
27
,2
1,
40
64,1
71
,6
79,1
3,
83
35
36
,0
38,9
41
,9
1,52
19
,0
21,6
24
,1
1,
31
22,4
25
27
,9
1,
43
65,7
73
,4
81,2
3,
92
36
52
37,0
40
,0
43,1
1,
57
19,3
22
,0
24,7
1,35
22
,9
25,8
28
,7
1,
48
67,1
75
,0
83,0
4,
06
37
37
,9
41,0
44
,2
1,61
19
,7
22,4
25
,1
1,
39
23,5
26
,4
29,5
1,52
68
,5
76,7
84
,8
4,17
38
51
38
,8
42,0
45
,2
1,66
20
,0
22,8
25
,6
1,
43
23,9
27
30
1,56
69
,8
78,2
86
,6
4,29
39
39,6
42
,9
46,2
1,
71
20,3
23
,2
26,0
1,47
24
,4
27,5
30
,7
1,
60
71,0
79
,6
88,3
4,
40
40
21
40,4
43
,8
47,1
1,
75
20,6
23
,5
26,5
1,50
24
,8
28,1
31
,3
1,
64
72,2
81
,0
89,9
4,
51
41
41
,1
44,8
48
1,
79
20,8
23
,8
26,8
1,54
25
,2
28,5
31
,8
1,
68
73,3
82
,3
91,4
4,
61
42
2 41
,8
45,6
48
,8
1,81
21
,1
24,1
27
,2
1,
57
25,6
28
,9
32,2
1,72
74
,4
83,6
92
,9
4,68
to
tal
111

Charts of fetal kidney and renal pelvis 31
The account of the nomograms of the 5th, 50th and 95th fitted centiles of the
anteroposterior and transverse diameter from the renal pelvis are given in Table 3
with the corresponding charts (Figures 5 and 6).
Table 3 - Fitted centiles of the anteroposterior and transverse diameter of the fetal renal pelvis with the number of fetuses for exact weeks between 16 and 42 weeks of gestational age
weeks of gestation
N fetuses
fitted centiles pelvis anteroposterior diameter
fitted centiles pelvis transverse diameter
5th 50th 95th SD 5th 50th 95th SD 16 55 0,2 1,1 1,9 0,4 - 0,8 1,4 3,6 1,1 17 0,5 1,3 2,2 0,5 - 0,6 1,7 4,0 1,2 18 56 0,7 1,6 2,5 0,5 - 0,1 2,3 4,7 1,2 19 0,9 1,8 2,8 0,5 0,1 2,6 5,1 1,3 20 55 1,2 2,1 3,1 0,5 0,5 3,1 5,6 1,3 21 1,3 2,3 3,3 0,5 0,9 3,4 6,0 1,3 22 56 1,6 2,6 3,6 0,5 1,0 3,7 6,5 1,4 23 1,7 2,7 3,8 0,5 1,2 4,0 6,8 1,4 24 55 1,9 3,0 4,0 0,5 1,4 4,3 7,2 1,5 25 2,0 3,1 4,2 0,6 1,6 4,5 7,5 1,5 26 56 2,2 3,3 4,4 0,6 1,7 4,8 7,9 1,6 27 2,3 3,4 4,6 0,6 1,9 5,0 8,2 1,6 28 55 2,4 3,6 4,7 0,6 2,0 5,2 8,5 1,7 29 2,5 3,7 4,9 0,6 2,0 5,4 8,8 1,7 30 54 2,5 3,8 5,0 0,6 2,1 5,5 9,0 1,8 31 2,6 3,8 5,1 0,6 2,1 5,7 9,2 1,8 32 55 2,6 3,9 5,2 0,7 2,1 5,8 9,4 1,9 33 2,7 4,0 5,3 0,7 2,1 5,8 9,6 1,9 34 53 2,7 4,0 5,4 0,7 2,0 5,9 9,7 2,0 35 2,6 4,0 5,4 0,7 2,0 5,9 9,8 2,0 36 52 2,6 4,0 5,5 0,7 1,9 6,0 10,0 2,1 37 2,6 4,0 5,5 0,7 1,8 5,9 10,0 2,1 38 51 2,5 4,0 5,5 0,8 1,6 5,9 10,1 2,2 39 2,5 4,0 5,5 0,8 1,5 5,8 10,1 2,2 40 21 2,4 4,0 5,5 0,8 1,3 5,7 10,1 2,3 41 2,3 3,9 5,4 0,8 1,1 5,6 10,1 2,3 42 2 2,3 3,9 5,4 0,8 1,0 5,5 10,0 2,3
total 111

32 Chapter 3
gestational age in weeks
4238343026221814
pye
lum
AP
-dia
me
ter
(mm
)10
8
6
4
2
0
-2
Figure 5 – Fitted 5th, 50th and 95th centiles of the A-P diameter of the renal pelvis and the raw data.
gestational age in weeks
4238343026221814
tra
nsve
rse
pye
lum
dia
me
ter
(mm
)
14
12
10
8
6
4
2
0
-2
Figure 6 – Fitted 5th, 50th and 95th centiles of the transverse diameter of the renal pelvis and the raw data.

Charts of fetal kidney and renal pelvis 33
The centile charts were compared with previously published charts from Chitty and
Altman18 for length, AP-diameter, transverse diameter and renal pelvis
measurements and from Pruggmayer and Terinde3 for length and transverse
diameter. See figures 7, 8, 9 and 10.
0
10
20
30
40
50
60
14 16 18 20 22 24 26 28 30 32 34 36 38 40 42
gestational age in weeks
kidn
ey le
ngth
(m
m)
Figure 7 – Comparison of 5th, 50th and 95th centiles for kidney length measurements obtained in this study (solid lines) and the 10th, 50th and 90th centiles of Chitty (dashed lines – – – – ) and the 5th, 50th and 95th centiles of Pruggmayer (dashed lines - - - - ).
0
5
10
15
20
25
30
35
14 16 18 20 22 24 26 28 30 32 34 36 38 40 42
gestational age in weeks
kidn
ey A
-P d
iam
eter
(m
m)
Figure 8 – Comparison of 5th, 50th and 95th centiles for kidney anteroposterior diameter obtained in this study (solid lines) and the 10th, 50th and 90th centiles of Chitty (dashed lines – – – –).

34 Chapter 3
0
5
10
15
20
25
30
35
40
45
14 16 18 20 22 24 26 28 30 32 34 36 38 40 42
gestational age in weeks
kidn
ey tr
ansv
erse
dia
met
er (
mm
)
Figure 9 – Comparison of 5th, 50th and 95th centiles for kidney transverse diameter obtained in this study (solid lines) and the 10th, 50th and 90th centiles of Chitty (dashed lines – – – –) and the 5th, 50th and 95th centiles of Pruggmayer (dashed lines - - - -).
0
1
2
3
4
5
6
7
8
16 20 24 28 32 36 40
gestational age in weeks
rena
l pel
vis
(mm
)
Figure 10 – Comparison of 5th, 50th and 95th centiles for anteroposterior renal pelvis measurements obtained in this study (solid lines) and the 10th, 50th and 90th centiles of Chitty (dashed lines). DISCUSSION
Several charts of fetal kidney sizes have been published before, but some with
shortcomings in data collection or with methodological weaknesses. Our charts of the
fetal kidney and fetal renal pelvis were obtained from longitudinal data derived from
prospective investigations that were done specifically for the development of the
centile charts. The data were obtained from a large longitudinal sample and therefore
the charts are suitable for size and growth measurements i.e. for comparing renal
size at a known gestational age between 16 and 42 weeks of gestation and for

Charts of fetal kidney and renal pelvis 35
following the growth of the fetal kidney by comparing the measured data of the fetus
between two separate occasions with the fitted data. Until now there had not been a
chart published, which combines both possibilities, when taken into account
methodological pitfalls and incorrect methods in design such as not validating
gestational age1-5, only partly covering the second and third trimester1, 2, 6-8,
measuring only one or two dimensions of the kidney1, 2, 4-6 or averaging both cross-
sectional and longitudinal data1, 3-6, 8, 11. Moreover this study has the added
advantage that the statistical analysis used is able to correct for missing data.
We were limited in comparing our findings with previously published charts of kidney
size because several studies gave no raw data or when they did so they gave
evidence of methodological weakness or did not cover the whole second and third
trimester of pregnancy. None of the previous studies had carried out an intra- and
interobserver variation analysis before data collecting, as we did.
Chitty and Altman18 obtained their data in a cross-sectional study, including
approximately 15 to 20 cases per week. Measurements were only done once. They
published the 3rd, 10th, 50th, 90th and 97th centile. Pruggmayer and Terinde3 also
performed a cross-sectional study including 612 fetuses. They did not give data on
the number of fetuses measured each week and excluded 18.6% of infants because
they were either large or small for dates. The most obvious differences between our
kidney charts and those of the other two groups relate to the smaller ranges that we
found. The 50th centile of measurements of Chitty and Altman was higher than ours at
around 30 weeks of gestation, but almost the same near term. The 50th centile for the
transverse kidney diameter was about the same in the three studies, apart from term
age, when our data were in between those of the two other groups. It is difficult to
explain the differences between the findings of the three studies. The fact that we
have repeated the measurements three times may have resulted in narrowed ranges.
Regarding the fetal renal pelvic dimensions only two charts have been published
before. Chitty et al18 published a chart based on cross-sectional data from fetuses
measured only once for the purpose of the study but examined only a low number of
fetuses at each week of gestation (3 to 11: mean 7). Scott5 published a chart with a
mixture of cross-sectional and longitudinal data obtained during routine scanning and

36 Chapter 3
as a consequence some fetuses were only included once whereas others were
included at many ages; the resulting scatter diagrams of kidney and pelvis sizes
show many data at around 18-20 weeks and at around 32-34 weeks and a lack data
beyond 36 weeks of gestational age. They did not publish the raw data. We therefore
only compared our chart with the one published by Chitty and Altman. Their chart
suggests a linear growth of the renal pelvis size, with a wide range, whereas ours
shows a curved line, with no increase size from 32 weeks onwards, an a
considerable narrower range (especially, when taken into account the fact that we
gave the 5th, 50th and 95th centile and Chitty and Altman the 10th, 50th and 90th
centiles) (Figure 8).
Renal pathology often presents itself late in pregnancy. A chart for size and growth
chart of the kidney may be useful in case of diagnostic problems. The same holds for
renal pelvic dilatation, which is a common sonographic finding in pregnancy.

Charts of fetal kidney and renal pelvis 37
REFERENCES
1. Cohen HL, Cooper J, Eisenberg P, Mandel FS, Gross BR, Goldman MA, et al. Normal length of fetal kidneys: sonographic study in 397 obstetric patients. AJR Am J Roentgenol 1991;157(3):545-8. 2. Gloor JM, Breckle RJ, Gehrking WC, Rosenquist RG, Mulholland TA, Bergstralh EJ, et al. Fetal renal growth evaluated by prenatal ultrasound examination. Mayo Clin Proc 1997;72(2):124-9. 3. Pruggmayer M, Terinde R. [Fetal kidney screening: growth curves and indices]. Geburtshilfe Frauenheilkd 1989;49(8):705-10. 4. Sagi J, Vagman I, David MP, Van Dongen LG, Goudie E, Butterworth A, et al. Fetal kidney size related to gestational age. Gynecol Obstet Invest 1987;23(1):1-4. 5. Scott JE, Wright B, Wilson G, Pearson IA, Matthews JN, Rose PG. Measuring the fetal kidney with ultrasonography. Br J Urol 1995;76(6):769-74. 6. Bertagnoli L, Lalatta F, Gallicchio R, Fantuzzi M, Rusca M, Zorzoli A, et al. Quantitative characterization of the growth of the fetal kidney. J Clin Ultrasound 1983;11(7):349-56. 7. Bernaschek G, Kratochwil A. [Ultra-sound study on the growth of the fetal kidney in the second half of pregnancy (author's transl)]. Geburtshilfe Frauenheilkd 1980;40(12):1059-64. 8. Jeanty P, Dramaix-Wilmet M, Elkhazen N, Hubinont C, van Regemorter N. Measurements of fetal kidney growth on ultrasound. Radiology 1982;144(1):159-62. 9. Chiara A, Chirico G, Barbarini M, De Vecchi E, Rondini G. Ultrasonic evaluation of kidney length in term and preterm infants. Eur J Pediatr 1989;149(2):94-5. 10. Gonzales J. [Anatomical measurements during fetal growth of the kidney. Its value for the ultrasonographer and the anatomo-pathologist (author's transl)]. J Gynecol Obstet Biol Reprod (Paris) 1981;10(2):113-7. 11. Vries de L, Levene MI. Measurement of renal size in preterm and term infants by real-time ultrasound. Arch Dis Child 1983;58(2):145-7. 12. Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound Obstet Gynecol 1993;3(6):378-84. 13. Altman DG, Chitty LS.Charts of fetal size: 1. Methodology. Br J Obstet Gynaecol 1994;101(1):29-34. 14. Royston P, Altman DG. Design and analysis of longitudinal studies of fetal size. Ultrasound Obstet Gynecol 1995;6(5):307-12. 15. Royston P, Wright EM. How to construct 'normal ranges' for fetal variables. Ultrasound Obstet Gynecol 1998;11(1):30-8. 16. Goldstein H. Multilevel statistical models. 2nd ed. London: University of London. ed; 1995. 17. Kloosterman GJ. On intrauterine growth. Int J Gynaecol Obstet 1970;8:895-912. 18. Chitty LS, Altman DG. Charts of fetal size: kidney and renal pelvis measurements. Prenat Diagn 2003;23(11):891-7.


Chapter 4 Growth and size charts of the fetal adrenal gland H.A.M. Damen - Eliasa, R.H. Stigtera,c, P. Westers b, G.H.A. Vissera a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Centre for Biostatistics, Utrecht University, The Netherlands c Department of Obstetrics and Gynaecology, Deventer Hospital, Deventer, The Netherlands

40 Chapter 4
ABSTRACT
Objectives It was the aim of this study was to develop a reference curve for size and
growth of the length of the fetal adrenal gland.
Methods Longitudinal prospective study of one hundred eleven fetuses that were
scanned every four weeks. The ultrasound measurements started in one half of the
cases at sixteen weeks of gestation and in the other half at eighteen weeks.
Statistical analysis was performed by multilevel analysis.
Results Fitted 5th, 50th and 95th centile charts for the length of the adrenal gland are
presented with the raw data. There was a high correlation between adrenal and
kidney length (R = 0,932) with a ratio of 2 to 7.
Conclusions The chart for size and growth is of use for measurements of the length
and growth of the adrenal gland.

Charts of fetal adrenal gland 41
INTRODUCTION
Knowledge of the normal range of the growth and size of the fetal adrenal gland is of
importance for the identification of morphological changes once an anomaly is
suspected.
A number of reference values of adrenal gland measurements have been published1-
7, but none covers the whole second and third trimester of the pregnancy. Moreover
in none of these studies data were used with an ultrasound validated gestational age
and in some publications only post-mortem specimens were used1, 2. All studies used
cross-sectional data. Since 1990 there has been no study using abdominal
investigations. In 1993 a study has been published using transvaginal ultrasound
between 12 and 17 weeks of gestation.
It was the aim of this prospective study to develop a reference curve for the size and
growth of fetal adrenal gland length.
MATERIAL AND METHODS
Data of the length of the adrenal gland were collected in a longitudinal, prospective
study. Measurements of the fetal kidney and fetal renal pelvis were collected
simultaneously and will be published in a separate paper.
One hundred and twelve low risk women with 116 fetuses (4 twin-pregnancies) were
included after written informed consent had been obtained. They were divided in two
groups who were scanned at four weeks interval starting at 16 weeks or at 18 weeks
gestational age, respectively. All women had had a dating scan before 13 weeks of
gestation. One experienced ultrasonographer (HDE) made all the examinations using
the multifrequency transducer PVM 375 AT of the Toshiba Power Vision 6000, type
SSA 370 A (manufacturer Toshiba, Tokyo, Japan).
An intra- and interobserver variation analysis was performed before carrying out this
study. The results of which will be published elsewhere.
Women were excluded when they had a mono-chorionic twin pregnancy, a
chromosomal or congenital defect of the fetus, a small for gestational age infant
(SGA = birth weight according to growth charts <2.3% percentile8) or a maternal
disease which might effect fetal growth (diabetes mellitus, hypertension requiring
treatment).

42 Chapter 4
The suprarenal adrenal glands are heart-shaped structures located cranially to the
kidney like little helmets placed askew on top of the kidneys. They are imaged as
relatively anechoic pyramidal structures but sometimes the echogenicity of the
adrenal glands is similar to that of the adjacent kidney. In a transverse scan three
layers can usually be distinguished; the cortex is hypoechoic and the central medulla
hyperechoic. When visualising the full length of the kidney in a sagittal plane the
length of the kidney was measured and in the same plane the length of the kidney
including the adrenal gland was measured by placing the callipers from the outer to
outer border. The adrenal gland length was determined by subtraction of the kidney
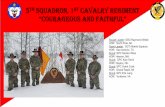
length from the total length (Figure 1).
Statistical analysis was performed by using SPSS, version 10.1 (Statistical Product
and Service Solutions, Chicago) and by multilevel analysis using the software
program Mln (Multilevel Model Project, London, UK9) to construct nomograms
(medians and the 5th and 95th centiles). The latter method is able to rectify the
problem of missing data inherent to any study with longitudinal data.
A adrenal gland B D kidney ureter C Figure 1 – The length of the fetal adrenal gland is AC – BC.

Charts of fetal adrenal gland 43
RESULTS
Five fetuses were excluded, SGA (n=2), congenital anomalies (n=3; triploidy, clubfoot
and hydronephrosis >10mm anteroposterior diameter of the renal pelvis), leaving
data from 111 fetuses for analysis. At each gestational age all measurements could
be obtained from both the right and the left adrenal gland with a total of 628 data for
each side.
Statistical analysis was performed on the separate measurements of the length of the
right and left adrenal gland. The charts were virtually identical with a high correlation
of R = 0.979. (Figure 2).
rigth adrenal gland length (mm)
1412108642
left
adre
nal g
land
leng
th (
mm
)
14
12
10
8
6
4
2
Figure 2 – Scatter from the data of the right and left adrenal gland length with the fitted
correlation line (correlation R = 0,979).
The data of the length of right and left adrenal gland were averaged to construct the
reference chart. The account of the nomograms of the 5th, 50th and 95th fitted centiles
are given in Table 1 with the corresponding chart in Figure 3.

44 Chapter 4
Table 1 – Fitted centiles of the fetal adrenal gland with the number of fetuses for exact weeks between 16 and 42 weeks of gestational age. weeks of gestation
fetuses N
fitted centiles adrenal length
5th 50th 95th SD 16 3.6 4.2 4.8 0.3 17
55 4.0 4.6 5.2 0.3
18 4.4 5.0 5.6 0.3 19
56 4.8 5.4 6.1 0.3
20 5.2 5.8 6.4 0.3 21
55 5.6 6.2 6.8 0.3
22 6.0 6.6 7.2 0.3 23
56 6.3 7.0 7.6 0.3
24 6.7 7.3 7.9 0.3 25
55 7.0 7.6 8.3 0.3
26 7.3 8.0 8.6 0.3 27
56 7.6 8.3 9.0 0.3
28 7.9 8.6 9.3 0.3 29
55 8.2 8.9 9.6 0.3
30 8.5 9.2 9.8 0.4 31
54 8.7 9.4 10.1 0.4
32 9.0 9.7 10.4 0.4 33
55 9.4 9.9 10.8 0.4
34 9.5 10.2 11.0 0.4 35
53 9.6 10.3 11.0 0.4
36 9.9 10.6 11.3 0.4 37
52 10.1 10.8 11.5 0.4
38 10.3 11.0 11.7 0.4 39
51 10.4 11.2 12.0 0.4
40 10.6 11.3 12.1 0.4 41
21 10.7 11.5 12.3 0.4
42 2 10.9 11.7 12.5 0.4 total 111
gestational age in weeks
4238343026221814
adre
nal g
land
leng
th (
mm
)
14
12
10
8
6
4
2
Figure 3 – Fitted 5th, 50th and 95th centiles for the adrenal gland and the raw data.

Charts of fetal adrenal gland 45
The adrenal-to-kidney length correlation was calculated using the data of the kidney
length chart (separate article) and those from the adrenal length. A strong linear
correlation was found between kidney length and adrenal gland length: R = 0,932
(Figure 4). The length of the adrenal gland was on average 27% (range 25 to 29%) of
that of the kidney (ratio 2 to 7) and this relation did not change with gestation/ kidney
size.
adrenal gland length in mm
14121086420
kidn
ey le
ngth
in m
m
60
50
40
30
20
10
0
Figure 4 - Scatter from the data of the length of the kidney and the adrenal gland with the
fitted correlation line (correlation R = 0,932).
DISCUSSION
Fetal adrenal glands are relatively large in comparison to early postnatal life. After
delivery their size rapidly decreases and increases again at the end of the first year
to attain their maximal weight and size by adulthood10. The fetal adrenal gland has
been the subject of only a few previous ultrasonographic investigations1-7, 11 with the
latest study published in the early 1990”s. Insufficient resolution of the equipment at
that time resulted in an inability to obtain accurate data especially during the second
trimester3 - 5, 7. In the early 1980’s Rosenberg et al7 could identify the adrenal glands
in only 12% of cases before 26 weeks gestational age and in 90% beyond that age.
In the same period, Jeanty et al5 were, not able to detect the adrenal gland in 30% of
cases before 25 weeks gestational age, decreasing to 6.5% in term fetuses.

46 Chapter 4
All previous charts have been made using cross-sectional data and several charts
showed evidence of methodological weaknesses such as the use of post-mortem
specimens1, 2 or the measurement of only one adrenal gland6.
We calculated the correlation between adrenal and kidney length since that may be
of significance in high-risk pregnancies. Naeye et al12 found in post mortem
examinations that fetal adrenal glands were relatively more reduced in weight than
body weight, in case of intra-uterine growth retardation. Hata et al3, 4 found a
decrease in the calculated adrenal gland surface in growth retarded fetuses and
others found small fetal adrenal glands when the mother was using glucocosteriods
because of congenital adrenal hyperplasia11. There are two case-reports on
ultrasound diagnosis of congenital adrenal hyperplasia13-14.
Our charts of the length of the fetal adrenal gland were obtained using longitudinal
data derived from a large prospective investigation that was done especially for the
development of a reference curve. The chart is suitable for size and growth of the
adrenal gland i.e. first of all for comparing adrenal size at a known gestational age
between 16 and 42 weeks of gestation and secondly for following the growth of the
adrenal gland by comparing the measured data of the fetus between two separate
occasions with the fitted data15-18. Until now there had not been a chart published,
which combines both possibilities.
Comparison of previously published charts with ours was not possible. Hata et al3, 4
published two studies: in one study he gave no raw data and in the other study the
data can not be used because he measured the length of the adrenal gland in
another way than we did by placing the callipers at A and D (Figure 1). We have
chosen for the distance A to B since this measure can be standardized better
because the borders of the adrenal gland are better visible at these points. Jeanty at
al5 gave averaged data with a range for every 5 weeks from 20 weeks gestation
onwards. Lewis et al6 published data between 30 and 39 weeks gestation but they
did only provide information on the length in comparison with kidney length and
biparietal diameter.

Charts of fetal adrenal gland 47
Fetal adrenal gland measurements can be an important ultrasonographic parameter
especially when a fetus is at risk for intra uterine growth retardation. The ratio of 2 to
7 between the adrenal gland and kidney length does not change with gestational age
and that may also be helpful.

48 Chapter 4
REFERENCES
1. Aragao de AH, Mandarim-de-Lacerda CA. Allometric growth of the adrenal gland in Brazilian fetuses. Okajimas Folia Anat Jpn 1990;67(2-3):165-8. 2. Gaillard DA, Lallemand AV, Moirot HH, Visseaux-Coletto BJ, Paradis PH. Fetal adrenal development during the second trimester of gestation. Pediatr Pathol 1990;10(3):335-50. 3. Hata K, Hata T, Kitao M. Ultrasonographic identification and measurement of the human fetal adrenal gland in utero. Int J Gynaecol Obstet 1985;23(5):355-9. 4. Hata K, Hata T, Kitao M. Ultrasonographic identification and measurement of the human fetal adrenal gland in utero: clinical application. Gynecol Obstet Invest 1988;25(1):16-22. 5. Jeanty P, Chervenak F, Grannum P, Hobbins JC. Normal ultrasonic size and characteristics of the fetal adrenal glands. Prenat Diagn 1984;4(1):21-8. 6. Lewis E, Kurtz AB, Dubbins PA, Wapner RJ, Goldberg BB. Real-time ultrasonographic evaluation of normal fetal adrenal glands. J Ultrasound Med 1982;1(7):265-70. 7. Rosenberg ER, Bowie JD, Andreotti RF, Fields SI. Sonographic evaluation of fetal adrenal glands. AJR Am J Roentgenol 1982;139(6):1145-7. 8. Kloosterman GJ. [Intrauterine growth and intrauterine growth curves]. Ned Tijdschr Verloskd Gynaecol 1969;69(5):349-65. 9. Goldstein H. Multilevel statistical models. 2nd ed. London: University of London. ed; 1995. 10. Potter EL, Craig JM. Pathology of the fetus and infant. St.Louis: A.S. Patterson; 1997. 11. Bronshtein M, Tzidony D, Dimant M, Hajos J, Jaeger M, Blumenfeld Z. Transvaginal ultrasonographic measurements of the fetal adrenal glands at 12 to 17 weeks of gestation. Am J Obstet Gynecol 1993;169(5):1205-10. 12. Naeye RL. Malnutrition: Probable Cause of Fetal Growth Retardation. Arch Pathol 1965;79:284-91. 13. Esser T, Chaoui R. Enlarged adrenal glands as a prenatal marker of congenital adrenal hyperplasia: a report of two cases. Ultrasound Obstet Gynecol 2004;23(3):293-7. 14. Saada J, Grebille AG, Aubry MC, Rafii A, Dumez Y, Benachi A. Sonography in prenatal diagnosis of congenital adrenal hyperplasia. Prenat Diagn 2004;24(8):627-30. 15. Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound Obstet Gynecol 1993;3(6):378-84. 16. Altman DG, Chitty LS. Charts of fetal size: 1. Methodology. Br J Obstet Gynaecol 1994;101(1):29-34. 17. Royston P, Altman DG. Design and analysis of longitudinal studies of fetal size.Ultrasound Obstet Gynecol 1995;6(5):307-12. 18. Royston P, Wright EM. How to construct 'normal ranges' for fetal variables. Ultrasound Obstet Gynecol 1998;11(1):30-8.

Chapter 5 Congenital renal tract anomalies: outcome and follow-up of 402 cases detected antenatally over a period of 15 years. H.A.M. Damen - Eliasa, T.P.V.M. de Jongb, R.H. Stigtera,c, G.H.A. Vissera, P.H. Stoutenbeeka a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Department of Paediatric Urology, University Hospital Utrecht, The Netherlands c Department of Obstetrics and Gynaecology, Deventer Hospital, Deventer, The Netherlands

50 Chapter 5
ABSTRACT
Objectives To determine the long-term prognosis of antenatally detected renal tract
anomalies in order to optimise counselling of the parents.
Methods Follow-up study of all renal tract abnormalities detected antenatally in a
level three-ultrasound department between 1986 and 2001. Follow-up data (medium
age 8 years) were retrieved from the records of the Paediatric Urology Department or
the attending paediatrician.
Results A urinary tract anomaly was detected in 408 fetuses. There were 4 false
positive diagnoses. From 2 children follow-up data were incomplete, leaving 402
cases for analysis. A chromosomal abnormality was present in 7 of 81 fetuses that
had karyotyping (8,6%). Termination of pregnancy occurred in 55 cases (13,7%) and
a further 66 children (16,4%) died during the perinatal period and up to 1 year of age.
In 106 of the 121 deceased children the cause of death was directly related to the
renal tract anomaly (26,4%). In the 281 surviving children a total of 545 renal tract
anomalies were diagnosed postnatally, requiring a total of 351 surgical interventions
in 160 infants. Outcome in survivors was generally good, with impaired renal function
in 9 infants and hypertension in 3 (4% of the survivors).
Conclusions Congenital renal tract anomalies are associated with a high mortality
rate, especially when they are structural developmental anomalies of the kidneys.
Survivors require multiple operations, but outcome is generally favourable.
Ultrasound diagnosis, especially when made early, of non-lethal urinary tract
anomalies may prevent additional renal damage by timing of delivery and early
postnatal treatment.

Congenital renal tract anomalies: 402 cases 51
INTRODUCTION
High-resolution ultrasound equipment increasingly gives the opportunity to identify
congenital anomalies antenatally. The prevalence of any detected congenital
anomaly during pregnancy is approximately 1-2%1-4. Abnormalities of the urinary
tract account for 15-20% with a detection rate of approximately 89%3,4. Evidence
exists that the number of antenatally detected malformations of the urinary tract is
increasing. This is attributed to the widespread use of ultrasound in pregnancy and
not to epidemiological changes5,6.
Data on antenatal diagnosis and postnatal follow-up are important for assessing
prognosis and counselling of the parents. They may be helpful in making difficult
decisions as to whether or not to terminate a pregnancy before viability, in
determining the need for further diagnostic procedures and on the best management
before and after birth. Data on large cohorts are scarce7 and most follow-up data are
confined to specific urological anomalies, such as hydronephrosis or multicystic
dysplastic kidneys8-11.
The aim of this study was to determine the long-term prognosis of antenatally
detected renal tract anomalies in order to optimise counselling of the parents.
MATERIALS AND METHODS
A cohort study was carried out by reviewing the database of the obstetric ultrasound
unit of the University Medical Centre, Utrecht, The Netherlands. The unit is a tertiary
referral centre and the database contains all cases from the population attending the
antenatal clinic of the hospital including those referred from District General
Hospitals. In the Netherlands tertiary centres only provide level 3 ultrasound facilities
and examinations are performed for specific, well-defined indications without doing
routine antenatal screening. The database was reviewed for urinary tract anomalies
detected between January 1st, 1986 and December 31st, 2000.
There were no exclusion criteria.
The cut-off point used in dilated renal pelves was >5 mm for the anteroposterior
diameter before 32 weeks in pregnancy and >10mm thereafter. The diagnosis of
polycystic kidney disease was made when there was the typical in utero presentation
of two enlarged hyperechogenic kidneys with loss of cortical differentiation and
oligohydramnios12,13. We defined kidneys as multicystic dysplastic when cysts of

52 Chapter 5
various size without connection between the cysts were located in the mostly bright
echogenic parenchyma of a structurally abnormal kidney in which no renal pelvis
could be demonstrated13. The term dysplastic kidney was used when the kidney was
echogenic in isolation, had no normal parenchyma and was structurally abnormal
without large cysts13,14. The diagnosis of an isolated megabladder was made
antenatally, when the distended bladder reached the insertion of the umbilical vein
independently of oligohydramnios. Prune Belly syndrome was diagnosed postnatally,
when the triad of abnormalities15,16 (abdominal wall deficient muscular tissue, dilated
urinary tract and bilateral cryptorchidism) with proven absence of urethral obstruction
was present, thus excluding female fetuses.
Follow-up data were obtained by chart review of the department of Paediatric
Urology and by contacting the paediatricians and general practitioners for information
having obtained consent from the parents. Clinical findings and/ or autopsy reports
were used to determine postnatal outcome. Prenatal diagnosis was confirmed by
postnatal ultrasound scans, radiological investigations, biochemical data on kidney
function and surgical records.
During the 15-year study period 2070 fetuses were seen with confirmed congenital
anomalies of which 408 cases (19,7%) were for urinary tract abnormalities. There
were four infants in whom the urinary tract appeared normal at follow-up and two
cases were lost to follow-up, due to relocation abroad, leaving 402 patients for further
analysis.
From all these cases follow-up data were available up to the age of between 3 and
17 years (median 7 years, 11 months).
RESULTS
diagnosis (n = 402)
Table 1 shows the antenatal diagnosis in the 402 fetuses. 151/402 (37,6%) fetuses
had a structural kidney anomaly, 247/402 (61,5%) had urinary tract dilatation, and
4/402 (1,0%) had anomalies of miscellaneous origin. The anomaly was bilateral in
206/402 (51,2%) fetuses and unilateral in 173/402 (43,1%) fetuses. 20/402 (4,9%)
fetuses had an isolated megabladder, and 3/402 (0,8%) had postnatally confirmed
Prune Belly syndrome. Forty-nine percent of the 173 unilateral anomalies were on
the right (n=84) side and 51 percent were on the left side (n=89).

Table 1 – A list of all ch
ildren, alive or dead, with
a structural d
eve
lopmental k
idney anomaly, urinary tract dilatatio
n or misce
llaneous uropathy
along with
prenatal a
nd postnatal d
iagnosis, details of abnorm
alities, su
rgery and renal function.
prenatal d
iagnosis
postnatal d
iagnosis
all
dead
dead ≠
renal a
nomaly
alive
infants w
ith
surgery
No. of
operatio
ns
renal function
structural d
eve
lopmental a
nomaly n = 151
unila
teral renal a
genesis
unila
teral renal a
genesis
8
8 3
7 8 norm
al
bila
teral renal a
genesis
bila
teral renal a
genesis
33
33
n.a.
unila
teral e
nlarged
ech
ogenic/ cy
stic kidney
unila
teral M
CKD
64
10
351
45
54
50 norm
al
1 m
ild failu
reunila
teral d
ysplasia
2
2 1
1
2 norm
al
bila
teral e
nlarged
ech
ogenic/ cy
stic kidneys
bila
teral M
CKD
22
22
n.a.
bila
teral d
ysplasia
2
2 1
8
1 dialysis
1 m
ild failure
PKD
13
13
n.a.
Meck
el G
ruber sy
ndrome
5
5
n.a.
Perlman syn
drome
1 1
n.a.
bila
teral e
chogenic kidneys
norm
al s
ize
norm
al
11
1 norm
al
total
151
84
364
50
70
urinary tract dilatatio
n n = 247
unila
teral d
ilatation
94
391
51
133
91 norm
al
bila
teral d
ilatatio
n127
28
117
52
169
1 transp
lant
4 chronic failure
3 hyp
ertension
109 norm
al
unila
teral m
egaureter
1
1 1
2
1 norm
al
bila
teral m
egaureter
2
2 1
3
2 norm
al
isolated m
egabladder
Prune Belly
3
3megabladder
20
17
31
4
3 norm
al
total
247
22
11
214
106
311
misce
llaneous anomaly n = 4
pelvic kidney
2
1
1 1 norm
al
horseshoe kidney
2
2 2 norm
al
total
4
1
30
0
total
402
106
15
281
156
381
8 failure
3 hyp
ertension
MCKD = m
ulticy
stic kidney disease
, PKD = polycystic kidney disease
, n.a. = not applicable

54 Chapter 5
The overall male to female ratio was 7 : 3. In the structural kidneys anomaly group
this ratio was 5 : 3 and in the urinary tract dilatation group it was 9 : 3,4.
The mortality rate was 30,1% (121/402).
At the end of the follow-up 9 children of the 281 surviving infants had impaired renal
function and 3 children had hypertension, 12/281 (4,3%). 7/281 (2,5%) children had
one dysplastic and one normal kidney left but they had overall normal renal function.
mortality (n = 121)
In 106/402 (26,4%) deceased children the cause of death was directly related to the
renal tract anomaly. Perinatal mortality (Table 1) was highest in the group with
structural kidney anomalies, namely 87/150 (58%). Mortality in the group with urinary
tract dilatation was 13,4% (33/247). Perinatal mortality included all cases with
polycystic kidney disease, bilateral renal agenesis and bilateral multicystic kidney
disease (MCKD) and these cases accounted for 61,2% (74/121) of total mortality.
Moreover, mortality in case of an isolated megabladder was high (17 out of 20).
Autopsy in 9 of these fetuses revealed 3 cases of urethral stenosis, 4 cases of
urethral obstruction and 2 cases of urethral atresia. The parents of 8 fetuses refused
autopsy: 5 times stillbirth occurred, 1 fetus had caudal regression syndrome, 1 a
cloacal anomaly and another one no visible anomalies. Ten of 64 children (15,6%)
with unilateral MCKD died because of contralateral renal anomalies: renal agenesis
in 9 and renal dysplasia in one. In the miscellaneous group one child died with a
unilateral pelvic kidney and Arnold Chiari syndrome.
Table 2 lists all 121 deceased children with the main renal anomaly and additional
renal and extrarenal anomalies. Autopsy was performed in 72/121 (59,5%) deceased
fetuses, and in all but 1 of them the main antenatal diagnosis was confirmed. Fifty-
five pregnancies were terminated on parental request, 55/402 (13,7%), at a mean
gestational age of 22,7 (range 15-35) weeks. In 54 of those cases there was a lethal
anomaly and in one case a suspected poor quality of life especially of the newborn
(Table 2). 12/402 (3,0%) fetuses were stillborn, and a further 50/402 (13,4%) children
died during the first 28 days after birth, and 4 others during the first year of life: 1 due
to the renal tract anomaly and 3 for other reasons, 4/402 (1,0%).
Sixty-nine percent of all perinatal deaths were boys.

Table 2 - O
verview of all ch
ildren who died, class
ified acc
ording to the anomaly. Data on additional renal a
nd extrarenal m
alfo
rmatio
ns are given as
well as the tim
e of death.
renal a
nomaly
total
No.
additional
malfo
rmations
renal
additional
malfo
rmations
extrarenal
additional
malfo
rmations
TOP
stillborn
neonatal death <
28 days
late in
fant death
> 28 days
total
renal
agenesis
bila
teral
33
10
1 absent bladder
1 urethral s
tenosis
2 agenesis of the ureters
1 hyd
roce
phalus
1 diaphragmatic
hernia
3 heart defects
1 anal/ oesophageal a
tresia
16
215
33 (27,3%)
MCKD bila
teral
22
9
2 cloacal m
alfo
rmation
1 m
ultiple anomalie
s of
the renal tract
2 sirenomelia
3 heart defect
1 anal/ oesophageal a
tresia
13
23
22 (18,2%)
MCKD unilateral
13
13
9 agenesis co
ntralateral
1 dys
plasia contralateral
2 pulm
onary hyp
oplasia
1 preterm
labour
51
713 (10,7%)
PKD
19
6
5 M
eck
el G
ruber
1 Perlman’s syn
drome
71
14
119 (15,7%)
Prune Belly syn
drome
31
2 3 (2,5%)
obstructive uropathy
= reaso
n death
19
3
1 cloacal m
alfo
rmation*
1 omphaloce
le1 caudal regress
ion
10*
36
19 (15,7%)
obstructive uropathy
≠ reaso
n death
11
11
1 triso
my 13
2 heart defects = N
oonan
1 hyp
operistaltis sy
ndrome
1 in
tra-uterine in
fection
1 m
egabladder, cloaca
l anomaly and preterm
labour
1 Arnold C
hiari m
alfo
rmation
1 D
andy Walker malfo
rmation
1 obstructive uropathy + anal/ oeso
phageal atresia =
VACTERL ass
ociation
1 obstructive uropathy + anal atresia, genotype 46 xx,
phenotype m
ale = VACTERL ass
ociation
1 obstructive uropathy + anal/ oeso
phageal atresia
+ VSD = VACTERL ass
ociation
31
43
11 (9,1%)
uropathy
≠
reaso
ndeath
11
1 pelvic kidney + Arnold C
hiari m
alfo
rmatio
n1
1 (0,8%)
total
121
53
18
35
55
(45,5%)
12
(9,9%)
50
(41,3%)
4 (3,3%)
121
(100%)
TOP = term
inatio
n of pregnancy
, all had a le
thal a
nomaly exc
ept one*, PKD = polycystic kidney disease
, VACTERL= vertebral d
efects (V
), anal a
tresia (A), cardiac
anomaly (C), trach
eal-eso
phageal fistula w
ith eso
phageal a
tresia (TE), renal d
efects (R
), radial lim
b dys
plasia (L), VSD = ventricle), septal d
efect

56 Chapter 5
survivors (n = 281)
Altogether 281 infants survived the perinatal period (Table 1). In these infants a total
of 545 anomalies was identified, resulting in 381 surgical interventions in 156 infants
(55,5% of the 281 survivors). Indications for surgery were upper tract dilatation with
split function on renal scan <40%, deteriorating function at follow-up renography or
renal colics based on UPJ obstruction. Table 3 shows all diagnosed renal tract
anomalies and all surgical interventions.
Table 3 - Summary of all 545 renal tract anomalies diagnosed in the 281 survivors (most had more than one anomaly diagnosed) and details of the number and type of surgical procedures in 156 of these children. diagnosis of the renal tract surgery on the renal tract pyelo-ureteric junction obstruction 113 kidney transplant 1 vesico-ureteric junction obstruction 8 nephrectomy 51 multicystic kidney 51 hemi-nephrectomy 21 posterior urethral valves 45 reimplantation (mega-) ureter 53 narrowed urethra 15 ureterectomy 22 megaureter 129 pyeloplasty 36 vesico ureteric reflux 46 incision posterior urethral valves 64 megabladder 45 vesicostomy 6 agenesis kidney 8 pull through vagina (Mayer Rokitanski) 3 dysplastic kidney 4 reconstruction vagina (cloacal malformation) 2 duplex system 43 ureterocele excision /reconstruction lower tract 19 urinary ascites 3 diverticulectomy 3 unclear 35 drainage of the upper tract 43 VUR - endoscopic treatment 13 closure of bladder rupture 1 excision/ incision syringocele or utriculus cyst 22 miscellaneous small interventions 21 number of diagnosis 545
total number of surgical interventions 381
Most children had more than one renal tract anomaly diagnosed and approximately
half of the survivors needed on average two to three surgical interventions.

Congenital renal tract anomalies: 402 cases 57
surviving infants with structural kidney anomaly (n=64)
Most (51/64 (79,7%)) children in this group had unilateral MCKD, and 12/51 (23,5%)
infants had contralateral renal anomalies: a dysplastic kidney in 3, pyelectasis in 6, a
megaureter in 1 and vesicoureteral reflux (VUR) in 2 (one grade IV and one grade V).
There was one fetus with bilateral echogenic kidneys of normal size and normal
amniotic fluid at 24 weeks’ gestational age of which the echogenicity normalized
during pregnancy. The child had normal function after birth.
Surgery in the infants with a structural anomaly mainly consisted of unilateral
nephrectomy (Table 1). In 43 of 45 cases with nephrectomy of the multicystic kidney
there was no functioning at all on the renogram, whereas the other 2 had an overall
function of less than 10%.
At histology of the multicystic kidneys the diagnosis of MCKD was confirmed in all
cases including the two cases with minimal function on the isotope scan. Of the 63
survivors 61 children have normal renal function at follow-up. The two cases with
impaired outcome are:
1 - One child with bilateral echogenic, dysplastic kidneys due to bilateral obstructive
uropathy based on ectopic ureter with ureterocele, contralateral megaureter and
bilateral VUR. The girl had several operations and eventually developed end-stage
renal failure at the age of 8 (2002) and started peritoneal dialysis.
2 - One girl with bilateral echogenic, dysplastic kidneys, who was finally diagnosed as
having the hereditary branchio-oto-renal (BOR)-syndrome(17), which includes renal
failure and impaired hearing (Creatinine 71 µmol/l at 7½ years).

58 Chapter 5
surviving infants with urinary tract dilatation (n = 214)
Table 5 gives an overview of the age of diagnosis, size of the dilatation at diagnosis
and outcome of the 118 surviving infants with a solitary uni- or bilateral renal pelvis
dilatation. Forty-five infants needed a total of 88 interventions. One child has chronic
renal failure and 1 hypertension; both children had bilateral dilated pelves.
Another 96 infants had a uni- or bilateral urinary tract dilatation in combination with a
uni- or bilateral megaureter and/ or megabladder. There was a high intervention rate
of 227 interventions in 62 of these children, 62/96 (64,6%). Forty-five of these 96
children had posterior urethral valves (PUV) with an intervention rate of 100%,
leaving 4 infants with impaired function and 1 infant with hypertension. In 14 of these
infants labour had been induced (Table 7). Moreover the intervention rate was high
(39/45 (86,6%)) in case of VUR.
Outcome in all 39 children with a unilateral renal tract dilatation was favourable. Most
of the 54 infants with a bilateral dilatation had a good outcome. There were six
infants with chronic renal failure, one requiring kidney transplant (Table 4) and 2 with
hypertension. Impaired outcome was not related to the time of diagnosis or to the
size of dilatation at diagnosis.
Table 4 - Children with obstructive uropathy and impaired renal function. Induced labour = No. corresponding with those in Table 7 2 Boy with bilateral pyelectasis = 5/ 5 mm, megaureter and megabladder in week 16 of gestational
age. He had PUV and bilateral VUR (gr IV and IV). After two years of renal dialysis and multiple operations he had a kidney transplant at the age of five. He is 16 years of age and doing well.
7 Boy with unilateral megaureter and contralateral MCKD. He had MCKD nephrectomy and reimplantation of the ureter at the opposite side, excision of ureterocele and relief of urethral obstruction. He is now 9½ years old with creatinine levels of 81 µmol/l.
8 Boy with bilateral hydronephrosis =10/ 10 mm, megaureter and megabladder in week 27 of gestational age. He had PUV and extensive surgery with temporary diversion by vesicostomy and drainage of the upper tract. He is 9 years old with creatinine levels of 74 µmol/l.
9 Boy with bilateral hydronephrosis =10/ 13 mm, megaureter and megabladder in week 23 of gestational age. He had PUV and bilateral VUR (gr IV and V). He has dysplastic kidneys with immature parenchyma and underwent ample surgical reconstructions. At 10 years of age he has a preterminal renal failure (creatinine 179 µmol/l).
18 Boy with bilateral hydronephrosis= 25/ 25 mm, megaureter and megabladder in week 34 of gestational age. He had PUV. After multiple operations he has mild chronic renal failure (creatinine 80 µmol/l) and a renal urine concentration defect at 10 years of age.
19 Boy with bilateral hydronephrosis = 10/ 10 mm, megaureter and megabladder in week 34 of gestational age. He had bilateral VUR (gr III and IV). At 10 years and after multiple operations he has mild renal failure = reflux nephropathy (creatinine 74 µmol/l) and hypertension.
No induced labour Boy with bilateral pyelectasis = 9/ 7 mm in week 29 of gestational age. He had bilateral VUR (gr V
and V) and developed pyelonephritis in spite of antibiotic prophylaxis. He underwent bilateral reimplantation and recalibration of the ureter. He has a creatinine of 74 µmol/l at three years of age.

Table 5
- C
hildren w
ith solitary u
ni- o
r bila
teral renal pelvis d
ilatatio
n a
long w
ith g
estatio
nal age a
nd size o
f dilatatio
n a
t first d
iagnosis. F
igures in
parenthese
s indicate operated children. Total n
umber of su
rgical interventio
ns and renal failu
re after su
rgery are prese
nted in
the la
st columns.
5 -10 m
munilateral
2
2 ( 1)
13
11
10 ( 1 = 10 %)
2
bilateral
11
42 ( 1)
118 ( 1 = 5,5 %
) 5
1 chronic renal failure
10 -15 m
munilateral
2 ( 1)
1 ( 1)
3 ( 1)
5 ( 2)
3 ( 1)
14 ( 6 = 42,9 %
) 11
bilateral
5 ( 1)
6 ( 2)
66
23 ( 3 = 13,0 %
) 5
15– 20 m
munilateral
1 ( 1)
4 ( 3)
6 ( 2)
11 ( 6 = 54,5 %
) 7
bilateral
21
3 ( 2)
3 ( 2)
9 ( 4 = 44,4 %
) 8
20– 25 m
munilateral
1 ( 1)
2 ( 2)
2 5 ( 3 = 60 %)
5
bilateral
14 ( 1)
2 ( 2)
7 ( 3 = 42,9 %
) 8
1 hyp
ertension
25– 30 m
munilateral
2 ( 2)
1 ( 1)
1 4 ( 3 = 75 %)
10
bilateral
1 ( 1)
1 ( 1 = 100 %)
1
30– 35 m
munilateral
11 ( 1)
2 ( 1 = 50 %)
1
bilateral
1 ( 1)
11 ( 1)
3 ( 2 = 66,6 %
) 3
> 35 m
munilateral
2 ( 2)
3 ( 3)
1 ( 1)
6 ( 6 =100 %
) 8
bilateral
1 ( 1)
1 ( 1)
2 ( 2 =100 %
) 5
unilateral
1 ( 1)
1 ( 1 =100 %
) 2
solitaire
megaureter
bilateral
11 ( 1)
2 ( 1 = 50 %
) 3
total
14
13 ( 3)
16 ( 8)
26 (10)
30 (16)
22 ( 8)
118 (44 = 37,3 %
) 84

60 Chapter 5
In 21 of the 119 cases (17,7%) with a bilateral dilatation labour was electively
induced before 37 weeks of gestation (mean 34,9 weeks: range 29 – 37) because of
the development of anhydramnios. Only one fetus had solitary bilateral
hydronephrosis (Table 7). All 21 neonates (19 boys and 2 girls) had surgery within a
few days after birth. Almost all children with impaired outcome can be found in this
group (6 chronic renal failure, 1 hypertension).
VUR was diagnosed in 45 of the 214 children (21,0%) with urinary tract dilatation
after evaluation by voiding cystourethrography; 39 infants needed a total of 123
interventions, 39/45 (86,6%). The male : female ratio was 7 : 2. Table 6 gives an
overview of all cases with uni- and bilateral VUR, surgical interventions and final
renal function.
Table 6- Summary of interventions and outcome in 45 infants with unilateral or bilateral VUR. urinary tract anomaly with VUR
children with surgery
No. of operations
final renal function
13 = unilateral urinary tract anomaly with VUR
11 26 1 unilateral reflux nephropathy 2 dysplasia in operated kidney
10 = bilateral urinary tract anomaly with unilateral VUR
10 13* 1 hypertension and mental delay
22 = bilateral urinary tract anomaly with bilateral VUR
18
84 1 kidney transplant 1 peritoneal dialysis 1 hypertension, bilateral reflux nephropathy, unilateral hypoplasia 1 chronic renal failure 1 preterminal insufficient 1 hypertension 1 dysplasia in operated kidney
*7 in reflux kidney, 6 in the contralateral hydronephrotic kidney.
surviving infants with miscellaneous anomaly (n = 4)
These four infants (Table 1) had a developmental kidney anomaly without
consequences for renal function and were all normal at follow-up.

Table 7 - C
ase
s in w
hich labour was induce
d along w
ith sex, gestatio
nal age, antenatal diagnosis, typ
e of anomaly, su
rgery and renal function after
surgery. (PUV = posterior urethral v
alves)
in
duce
d la
bour n =21
No.
sex
inducing
labour
antenatal d
iagnosis
postnatal a
nomaly - surgery
renal function after su
rgery
1
xy32 w
eeks
bilateral h
ydronephrosis and m
egaureters
PUV - excision urethral v
alves
good
2
xy36 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
PUV-bilateral V
UR (gr IV + IV) -extensive
surgery
kidney transp
lant
3
xy33 w
eeks
bilateral h
ydronephrosis and m
egaureters
PUV - extensive
surgery
good
4
xy35 w
eeks
bilateral h
ydronephrosis
bilateral h
ydronephrosis - bilateral p
yeloplasty
good
5
xy36 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
PUV - extensive
surgery
good (unila
teral d
ysplasia)
6
xy35 w
eeks
bilateral h
ydronephrosis and urinary asc
ites
PUV - extensive
surgery
good
7
xy36 w
eeks
unilateral m
egaureter and contralateral M
CKD
unilateral m
egaureter and contralateral M
CKD –
ureter reim
plantatio
n and nephrectomy
mild failure
8
xy37 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
PUV - extensive
surgery
mild failure
9
xy33 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
PUV-bilateral V
UR (gr IV + V) - extensive
surgery
preterm
inal failure
10
xy29 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
premature la
bour after amnion in
fusion - PUV -
extensive
surgery
good
11
xy35 w
eeks
megabladder and urinary asc
ites
PUV and spontaneous bladder rupture -
extensive
surgery
good
12
xy33 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
PUV - extensive
surgery
good
13
xy37 w
eeks
unilateral h
ydronephrosis,co
ntralateral m
egaureter
and utereoce
lePUV - extensive
surgery
good - hyp
ertension
14
xy36 w
eeks
bilateral h
ydronephrosis, m
egabladder - urinary
asc
ites
bilateral h
ydronephrosis
died during heart su
rgery –
DORV, TGA
15
xy36 w
eeks
bilateral h
ydronephrosis, megabladder - urinary
asc
ites
PUV and bila
teral V
UR (gr III and IV)
extensive
surgery
good
16
xy37 w
eeks
unilateral h
ydronephrosis with
megaureter,
contralateral M
CKD
UVJ stenosis with
unilateral M
CKD, unilateral
megaureter with
VUR gr V- extensive
surgery
good
17
xy36 w
eeks
bilateral h
ydronephrosis, m
egabladder
PUV- excision urethral v
alves
good
18
xy34 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
PUV- extensive
surgery
mild failure
19
xy37 w
eeks
bilateral h
ydronephrosis, m
egaureter-megabladder
bilateral V
UR (gr III and IV) and m
egaureter
– bila
teral u
reteral reim
plantatio
nbilateral
reflu
x nephropathy
and hyp
ertension
20
xx
34 w
eeks
bilateral h
ydronephrosis and m
egaureters
bilateral h
ydronephrosis - extensive
surgery
good
21
xx
37 w
eeks
unilateral h
ydronephrosis with
megaureter,
contralateral M
CKD
unilateral M
CKD, co
ntralateral V
UR gr V -
extensive
surgery
good
DORV = double outle
t of the right ve
ntricle, TGA = transp
ositio
n of the great arteries

62 Chapter 5
infants with chromosomal anomalies (n=7)
Karyotyping was done antenatally in 77 fetuses (in 13 cases because of maternal
age >36 years) and postnatally in another 4 children, in total 81/402 (20,2%). Seven
children had a chromosomal anomaly, 7/81 (8,6%). (Table 8). In another three
stillborn fetuses a chromosomal anomaly was suspected but parents refused
karyotyping and autopsy.
Four children had trisomy 21 and these 4 infants accounted for 1,8% of all 221 living
children with uni- or bilateral renal tract dilatation.
Table 8 - Overview of fetuses with a chromosomal anomaly. No.
urinary tract anomaly chromosomal anomaly
extra renal anomaly
postnatal management renal function
1 bilateral MCKD Klinefelter syndr. XXY none n.a. n.a. 2 bilateral pyelectasis,
Ø 8 mm trisomy 13 multiple n.a. n.a.
3 bilateral hydronephrosis >20 mm and megaureter
mosaicism chromosome 8
none resection urethral valve normal
4 hydronephrosis >20mm, megaureter,megabladder
trisomy 21 none resection urethral valve diverticulectomy
normal
5 bilateral megaureter trisomy 21 hydrops foetalis polyhydramnios
prophylactic antibiotics normal
6 bilateral hydronephrosis > 15 mm and megabladder
trisomy 21 VSD, stenosis of pulmonary artery, unilateral clubfoot
closure VSD defect clubfoot correction
normal
7 bilateral hydronephrosis L > 30 mm, R > 6 mm
trisomy 21 VSD prophylactic antibiotics normal
n.a. = not applicable, VSD = ventricle septal defect
false positive diagnosis (n=4)
There were 4/402 (1,0%) infants in whom the urinary tract appeared to be normal at
follow-up. The antenatal diagnoses in these four cases were:
a) pelvic kidney (appeared to be normal position),
b) extrarenal dilatation of the kidney (appeared to be adrenal gland haemorrhage),
c) cyst of upper moiety of a duplex kidney (appeared to be extralobar sequestration
of the lung),
d) dysplastic kidneys with increased echogenicity (appeared to be normal).

Congenital renal tract anomalies: 402 cases 63
DISCUSSION
The population in this study may not be representative of the overall obstetric
population, since severe anomalies are likely to be referred more frequently to our
tertiary centre, than minor ones. Nevertheless, our data may be helpful in assessing
the prognosis of the various anomalies and be of help in counselling parents.
Urinary tract anomalies accounted for 20% of all congenital anomalies, detected
antenatally, with a very low false positive rate of 1,0% that never caused
inappropriate treatment. Mortality due to the renal tract anomaly was high,
approximately one quarter of all cases and was mainly restricted to the perinatal
period (including TOP in half of these cases). The mortality rate, almost 60%, was
especially high in infants with a structural kidney anomaly and relatively low, with
13,3% in the group with urinary tract dilatation. Approximately half of the survivors
needed an average of two to three surgical interventions.
Outcome in the surviving infants was generally good, with impaired renal function in 9
children and hypertension in 3 (12 out of 281 survivors = 4,3%). This favourable
outcome applied both to infants with a structural anomaly and to these with a urinary
tract dilatation. There were seven children with one dysplastic and one normal kidney
left but they all have overall normal renal function at follow-up. We did not include
data on the incidence of urine incontinence.
One may rightly argue that the incidence of impaired outcome may increase with
increasing age, but the median duration of follow up was already considerable
(almost 8 years).
Large bright kidneys in polycystic kidney disease are well documented12 and the
typical multicystic kidney usually does not present a diagnostic problem7,13,18,19.
Increased echogenicity of the renal parenchyma may represent significant disease
with poor outcome especially when there is oligo- or anhydramnios but with normal
amniotic fluid there may be normal function14, 20. The degree of echogenicity had to
be judged by comparing the kidneys to the echogenicity of the liver because normally
they should appear with similar brightness. In our series structural anomalies
represented approximately one third of anomalies. Postnatally most of the multicystic
kidneys had a non-functioning parenchyma and they were removed to avoid the need
for lifetime follow-up when the kidney is left in place, according to the guidelines of

64 Chapter 5
the Dutch Society for Paediatric Urology21,22. Fetuses with a unilateral MCKD had 34%
chance of having contralateral renal anomalies with a high mortality rate of 15,6%.
Thus, the finding of a unilateral MCKD must lead to meticulous screening of the
complete urinary tract, both pre- and postnatally.
Agreement exists that in case of urinary tract dilatation different thresholds are used for
measurements of the antero-posterior diameter of the renal pelvis in the second and
third trimester of pregnancy but the size and gestational age at diagnosis vary because
of the lack of diagnostic criteria23-26. Some authors suggest that the risk of surgery is
minimal when the dilatation is <10 mm in late pregnancy26,27 but Thomas28 has stated
that the size of the prenatal dilatation is not a sensitive predictor of pathology but that
increasing dilatation is associated with morbidity and mortality. An antero-posterior
diameter of > 10 mm is usually considered of significance27,29 but the Great Ormond
Street Experience30 showed that there is a very low risk of clinically significant
obstruction when the dilatation does not exceed 15 mm at any gestational age.
However, in our series 11 out of 65 infants with an isolated uni- or bilateral mild
dilatation (<15 mm) still required surgery.
It is the policy in our clinic that in case of an early and mild pyelectasis (<10 mm) and
after scanning for additional anomalies, patients are advised to have the ultrasound
investigation repeated at around 32 weeks of gestation and when the dilatation is the
same or less to refrain from further investigations before or after birth. (The two cases
with a dilatation <10 mm and surgery postnatally had both a dilatation >10 mm at the
32 week ultrasound scan.) Low grade VUR may be missed, although in our series none
of the infants with VUR had a dilatation less than 10 mm. We inform the parents that
there may be an enhanced risk for urinary tract infection due to VUR and when their
child feels listless or has fever of unknown origin a urinary tract infection must be ruled
out. With such a policy unnecessary parental anxiety may be prevented as well as
unnecessary costs of follow-up.
Surgery can be needed in case of an isolated uni- or bilateral dilatation of the renal
renal pelvis of >10 mm and in our study nearly half of these infants had surgery.
Especially high was the intervention rate in the 45 boys with PUV (100%). Labour
was induced in 14 of these infants and 6 have impaired renal function and 1

Congenital renal tract anomalies: 402 cases 65
hypertension. The overall conclusion for obstructive uropathy that can be drawn from
this series is that, regardless of the presence of 1 or 2 kidneys and regardless of the
degree of urinary tract dilatation, the prognosis for renal function is excellent when
oligohydramnios is absent before birth and when proper urological care is given
postnatally. Almost all renal failures were located in the group with progressive
oligohydramnios in which labour was induced preterm (6 of 21 infants). Poor
outcome of fetuses with bilateral urinary tract dilation combined with prolonged
periods of oligohydramnios has been repeatedly described31-33. Intrauterine therapy
still has a poor outcome with about 50% fetal loss and 40% end-stage renal disease
in the survivors34,35 but such a therapy is only a possible option when there is a
megabladder at midgestation. Our policy of preterm induction of labour when
oligohydramnios develops seems to result in a relatively favourable outcome
although the timing of induction is still uncertain and the proof that we actually gave
them better chances is non-existent.
Isolated megabladder was diagnosed in 23 cases antenatally, of which 3 boys had
Prune Belly syndrome diagnosed postnatally. In literature usually a high number of
Prune Belly is given15,16 without looking for urethral obstruction. Our number is low
because of the definitions we use for the Prune Belly syndrome15, 16 with proven
patent ureter and excluding female fetuses.
VUR accounted for approximately 21% of antenatally diagnosed urinary tract
dilatations, which is slightly higher than the 15% described by others36-39. There was
a high surgical intervention rate in 86,6% of the infants who needed approximately
one third of all surgical interventions (Table 6). VUR predisposes to urinary tract
infection and can lead to renal scarring and chronic renal failure but approximately
60% of kidneys with reflux already have an abnormal renogram even in the absence
of urinary tract infection40-42. Therefore all children with an anteroposterior renal
pelvis dilatation >10 mm around 32 weeks of gestation should be carefully managed
postnatally (low-dosed antibiotics, voiding cystourethrography).
We did antenatal karyotyping only when additional anomalies next to that of the
urogenital tract were found and postnatally only when there was a suspicion of
chromosomal abnormalities. Also at autopsy it is not routine in our unit to karyotype
the child. Seventeen parents refused autopsy and/ or karyotyping. Seven of 81

66 Chapter 5
fetuses, which were karyotyped, had a chromosomal disorder, 8,6%. See Table 8.
Others mentioned chromosomal disorders in 11-12%1,43 and even 25%44. However,
these studies are not quite comparable with ours because Stoll et al1 did not mention
the percentage of cases in which karyotyping was carried out, Nicolaides et al45
performed karyotyping at all children with the prenatal diagnosis of urogenital tract
anomalies and Isaksen et al44 described a selected group of deceased children.
Fetuses with a pyelectasis have a higher chance of having chromosomal anomalies
(mostly trisomy 21 followed by trisomy 13 and 18)43,46,47. In our series all the 7
fetuses (3,2%) with a chromosomal defect had a uni- or bilateral pyelectasis which is
in accordance with the 3,2 till 5,4% as reported in literature43,46,47. However, it is the
prevalent opinion that there is not an indication for fetal karyotyping in isolated
pyelectasis45.
Autopsy was performed in 72 of the 121 deceased fetuses (59,5%). The main
urological, prenatal diagnosis was confirmed in all but one of these fetuses (98,6%).
A suspected bilateral MCKD was a unilateral one with a normal contralateral kidney.
The child had also severe idiopathic pulmonary hypoplasia and anhydramnios and
did not die as a result of the inappropriate diagnosis. In 18 fetuses additional autopsy
findings, such as anal atresia in 5 fetuses, had not been found antenatally by
ultrasonography mostly due to the anhydramnios. Isaksen et al found a slightly lower
91% agreement between prenatal diagnosis of severe urogenital tract anomalies and
autopsy findings.
CONCLUSIONS
The overall value of antenatal diagnosis is that it indicates early termination of
fetuses with fatal renal disease, prepares parents and medical staff for the likelihood
of serious neonatal problems, and shows dangerous abnormalities of the urinary tract
that may not easily be detected postnatally. The drawback of antenatal diagnosis is
that the majority of detected mild dilatations has no therapeutic consequences at all
but still causes unnecessary anxiety in many cases. This study was undertaken to
ameliorate insight into which parents should have anxiety and which can be
congratulated with the fact that they can expect a healthy child with, possibly, a minor
problem without consequences for life or life expectancy. More studies about this will
be needed in future.

Congenital renal tract anomalies: 402 cases 67
REFERENCES
1. Stoll C, Clementi M. Prenatal diagnosis of dysmorphic syndromes by routine fetal ultrasound examination across Europe. Ultrasound Obstet Gynecol 2003;21(6):543-51. 2. Levi S. Ultrasound in prenatal diagnosis: polemics around routine ultrasound screening for second trimester fetal malformations. Prenat Diagn 2002;22(4):285-95. 3. Levi S. Mass screening for fetal malformations: the Eurofetus study. Ultrasound Obstet Gynecol 2003;22(6):555-8. 4. Grandjean H, Larroque D, Levi S. Sensitivity of routine ultrasound screening of pregnancies in the Eurofetus database. The Eurofetus Team. Ann N Y Acad Sci 1998;847:118-24. 5. Alladi A, Agarwala S, Gupta AK, Bal CS, Mitra DK, Bhatnagar V. Postnatal outcome and natural history of antenatally-detected hydronephrosis. Pediatr Surg Int 2000;16(8):569-72. 6. Barker AP, Cave MM, Thomas DF, Lilford RJ, Irving HC, Arthur RJ, et al. Fetal pelvi-ureteric junction obstruction: predictors of outcome. Br J Urol 1995;76(5):649-52. 7. Dillon E, Ryall A. A 10 year audit of antenatal ultrasound detection of renal disease. Br J Radiol 1998;71(845):497-500. 8. Broadley P, McHugo J, Morgan I, Whittle MJ, Kilby MD. The 4 year outcome following the demonstration of bilateral renal pelvic dilatation on pre-natal renal ultrasound. Br J Radiol 1999;72(855):265-70. 9. Feldman DM, DeCambre M, Kong E, Borgida A, Jamil M, McKenna P, et al. Evaluation and follow-up of fetal hydronephrosis. J Ultrasound Med 2001;20(10):1065-9. 10. Thomas DF, Madden NP, Irving HC, Arthur RJ, Smith SE. Mild dilatation of the fetal kidney: a follow-up study. Br J Urol 1994;74(2):236-9. 11. Onen A, Jayanthi VR, Koff SA. Long-term followup of prenatally detected severe bilateral newborn hydronephrosis initially managed nonoperatively. J Urol 2002;168(3):1118-20. 12. Reuss A, Wladimiroff JW, Stewart PA, Niermeijer MF. Prenatal diagnosis by ultrasound in pregnancies at risk for autosomal recessive polycystic kidney disease. Ultrasound Med Biol 1990;16(4):355-9. 13. Winyard P, Chitty L. Dysplastic and polycystic kidneys: diagnosis, associations and management Prenat Diagn 2001;21(11):924-35. 14. Wellesley D, Howe DT. Fetal renal anomalies and genetic syndromes. Prenat Diagn 2001;21(11):992-1003. 15. Jennings RW. Prune belly syndrome. Semin Pediatr Surg 2000;9(3):115-20. 16. Sutherland RS, Mevorach RA, Kogan BA. The prune-belly syndrome: current insights. Pediatr Nephrol 1995;9(6):770-8. 17. Rodriguez Soriano J. Branchio-oto-renal syndrome. J Nephrol 2003;16(4):603-5. 18. Aubertin G, Cripps S, Coleman G, McGillivray B, Yong SL, Van Allen M, et al. Prenatal diagnosis of apparently isolated unilateral multicystic kidney: implications for counselling and management. Prenat Diagn 2002;22(5):388-94. 19. Lam BC, Wong SN, Yeung CY, Tang MH, Ghosh A. Outcome and management of babies with prenatal ultrasonographic renal abnormalities. Am J Perinatol 1993;10(4):263-8.

68 Chapter 5
20. Estroff JA, Mandell J, Benacerraf BR. Increased renal parenchymal echogenicity in the fetus: importance and clinical outcome. Radiology 1991;181(1):135-9. 21. Oliveira EA, Diniz JS, Vilasboas AS, Rabelo EA, Silva JM, Filgueiras MT. Multicystic dysplastic kidney detected by fetal sonography: conservative management and follow-up. Pediatr Surg Int 2001;17(1):54-7. 22. Webb NJ, Lewis MA, Bruce J, Gough DC, Ladusans EJ, Thomson AP, et al.Unilateral multicystic dysplastic kidney: the case for nephrectomy. Arch Dis Child 1997;76(1):31-4. 23. Kent A, Cox D, Downey P, James SL. A study of mild fetal pyelectasia - outcome and proposed strategy of management. Prenat Diagn 2000;20(3):206-9. 24. Langer B. Fetal pyelectasis. Ultrasound Obstet Gynecol. 2000;Jul;16(1):1-5. 25. Ismaili K, Hall M, Donner C, Thomas D, Vermeylen D, Avni FE. Results of systematic screening for minor degrees of fetal renal pelvis dilatation in an unselected population. Am J Obstet Gynecol 2003;188(1):242-6. 26. Sairam S, Al-Habib A, Sasson S, Thilaganathan B. Natural history of fetal hydronephrosis diagnosed on mid-trimester ultrasound. Ultrasound Obstet Gynecol 2001;17(3):191-6. 27. Dremsek PA, Gindl K, Voitl P, Strobl R, Hafner E, Geissler W, et al. Renal Pyelectasis in fetuses and neonates: Diagnostic value of renal pelvis diameter in pre and postnatal sonographic screening. AJR Am J Roentgenol 1997(Apr;168(4)):1017-9. 28. Thomas DF. Prenatal diagnosis: does it alter outcome? Prenat Diagn 2001;21(11):1004-11. 29. Adra AM, Mejides AA, Dennaoui MS, Beydoun SN. Fetal pyelectasis: is it always 'physiologic'? Am J Obstet Gynecol 1995(Oct;173(4)):1263-6. 30. Dhillon HK. Prenatally diagnosed hydronephrosis: the Great Ormond Street experience. British Journal of Urology 1998(81,Suppl.2):39-44. 31. Brumfield CG, Guinn D, Davis R, Owen J, Wenstrom K, Mize P. The significance of non-visualization of the fetal bladder during an ultrasound examination to evaluate second-trimester oligohydramnios. Ultrasound Obstet Gynecol 1996;8(3):186-91. 32. Eckoldt F, Woderich R, Gellermann J, Hammer H, Tennstedt C, Heling KS. Survival in second trimester oligohydramnios secondary to bilateral pelviureteral junction obstruction. Urology 2003;61(5):1036. 33. Winn HN, Chen M, Amon E, Leet TL, Shumway JB, Mostello D. Neonatal pulmonary hypoplasia and perinatal mortality in patients with midtrimester rupture of amniotic membranes--a critical analysis. Am J Obstet Gynecol 2000;182(6):1638-44. 34. Freedman AL, Johnson MP, Smith CA, Gonzalez R, Evans MI. Long-term outcome in children after antenatal intervention for obstructive uropathies. Lancet 1999;354(9176):374-7. 35. Holmes N, Harrison MR, Baskin LS. Fetal surgery for posterior urethral valves: long-term postnatal outcomes. Pediatrics 2001;108(1):E7. 36. Anderson NG, Abbott GD, Mogridge N, Allan RB, Maling TM, Wells JE. Vesicoureteric reflux in the newborn: relationship to fetal renal pelvic diameter. Pediatr Nephrol 1997;11(5):610-6. 37. Arena F, Romeo C, Cruccetti A, Centonze A, Basile M, Arena S, et al. Fetal vesicoureteral reflux: neonatal findings and follow-up study. Pediatr Med Chir 2001;23(1):31-4.

Congenital renal tract anomalies: 402 cases 69
38. Herndon CD, McKenna PH, Kolon TF, Gonzales ET, Baker LA, Docimo SG. A multicenter outcomes analysis of patients with neonatal reflux presenting with prenatal hydronephrosis. J Urol 1999;162(3 Pt 2):1203-8.
39. Shapiro E, Elder JS. The office management of recurrent urinary tract infection and vesicoureteral reflux in children. Urol Clin North Am 1998;25(4):725-34, x. 40. Anderson PA, Rickwood AM. Features of primary vesicoureteric reflux detected by prenatal sonography. Br J Urol 1991;67(3):267-71. 41. Gordon AC, Thomas DF, Arthur RJ, Irving HC, Smith SE. Prenatally diagnosed reflux: a follow-up study. Br J Urol 1990;65(4):407-12. 42. de Jong TP, van Gool JD, Van Wijk AA, Stoutenbeek P, Van Isselt HW. Antenatally diagnosed obstructive uropathy--kidney imaging vs kidney function. Acta Urol Belg 1989;57(2):413-6. 43. Nicolaides KH, Cheng HH, Abbas A, Snijders RJ, Gosden C. Fetal renal defects: associated malformations and chromosomal defects. Fetal Diagn Ther 1992;7(1):1-11. 44. Isaksen CV, Eik-Nes SH, Blaas HG, Torp SH. Fetuses and infants with congenital urinary system anomalies: correlation between prenatal ultrasound and postmortem findings. Ultrasound Obstet Gynecol 2000;15(3):177-85. 45. Nicolaides KH. Screening for chromosomal defects. Ultrasound Obstet Gynecol 2003;21(4):313-21. 46. Benacerraf BR, Mandell J, Estroff JA, Harlow BL, Frigoletto FDJ. Fetal pyelectasis: a possible association with Down syndrome. Obstet Gynecol 1990(Jul;76(1)):58-60. 47. Corteville JE, Dicke JM, Crane JP. Fetal pyelectasis and Down syndrome: is genetic amniocentesis warranted? Obstet Gynecol 1992;79(5 ( Pt 1)):770-2.


Chapter 6 Concomitant anomalies in 100 children with unilateral multicystic kidney Henny A.M. Damen - Eliasa, Philip H. Stoutenbeeka, Gerard H.A. Vissera, Peter G.J. Nikkelsb, Tom P.V.M. de Jongc.
a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Department of Pathology, University Medical Centre Utrecht, The Netherlands. c Department of Paediatric Urology, University Medical Centre Utrecht, The Netherlands.

72 Chapter 6
ABSTRACT
Objectives To determine the incidence and type of associated urogenital anomalies
in children with unilateral multicystic kidney disease and to assess the additional
diagnostic value of cystoscopy and colposcopy (in girls) in children with
nephrectomy.
Methods Follow-up study of 100 children with antenatally detected unilateral
multicystic kidney disease. After ultrasound confirmation of the diagnosis a voiding
cystourethrography and isotope scan were done in each child to exclude vesico
ureteral reflux and to establish renal function. Eighty-one children had a nephrectomy
and prior to surgery all had a cystoscopy and girls also had a colposcopy.
Results Seventy-five children had one or more additional urogenital anomalies: 39
infants of the contralateral kidney, 42 of the ipsilateral kidney and 28 one or more on
the lower urogenital tract. With cystoscopy 54 anomalies of the genitourinary tract
were detected in 48 children and with colposcopy 3 anomalies in 35 girls. Eighty-one
children had a (hemi-) nephrectomy and 33 of them needed other urological
interventions. Thirteen fetuses died (mostly on agenesis of the contralateral kidney)
and 6 infants had no surgery at all.
Conclusion Children with unilateral multicystic kidney disease have a considerable
risk of having other urogenital anomalies. When cystoscopy and colposcopy are
added to the routine investigations the rate of detected anomalies is 75%, twice as
much as reported in literature.

Concomitant anomalies with unilateral multicystic kidney 73
INTRODUCTION
MCKD gives only rarely diagnostic dilemmas on prenatal ultrasound1 due to the
typical manifestation with in general multiple non-communicating cysts that are
randomly arranged with a size of less than 1 mm up to several centimetres in
diameter. The multicystic kidney is frequently enlarged, misshapen and irregularly
cystic with often a pyelo-calyceal occlusion and an atretic ureter and may go into
involution, pre- or postnatally and may become a small non-functional solid mass
with or without cystic lesions in the retroperitoneum2.
A multicystic dysplastic kidney is an aberrant developmental disturbance secondary
to an early obstruction3-8. They can be of any size ranging between kidneys with
multiple large cysts, commonly termed as multicystic dysplastic kidneys (MCKD), to
normal or small kidney remnants without cysts. A severe pyeloureteric junction
obstruction with dilated calices and hardly visible parenchyma may mimic a
multicystic kidney so in strictest terms renal dysplasia can only be diagnosed at
histology5.
The multicystic kidney can be affected unilateral, bilateral or as segmental part of a
duplex kidney. The incidence of unilateral MCKD is between 1 in 2500 - 4300 live
births9. Rarely inheritance10 has been reported but in that case it can be a feature of
syndromes or chromosomal disorders11. An abnormal karyotype has only been found
in cases with associated non-urological anomalies12, 13.
The function of the affected kidney is absent or poor. Therefore, bilateral MCKD is
invariably associated with a fatal outcome. The prognosis of unilateral MCKD is
favourable and depends on the integrity of the contralateral kidney14, 15. Contralateral
ureteropelvic junction (UPJ) stenosis, vesico ureteral reflux (VUR) and renal
agenesis have been reported in 15 – 50% of children2, 16, 17 and extrarenal associated
anomalies in 16 - 35%1, 12.
Removal of the multicystic kidney as standard procedure is still under debate. In
some studies the affected kidney is removed because of fear for potential
complications such as hypertension18, infection15 or malignancy17, 19 and in others the
children were examined periodically because their opinion is that the risk of
developing a malignancy or hypertension is considered very low or even non-
existing2, 15.

74 Chapter 6
It was the aim of our study to determine the incidence and type of associated
urogenital anomalies when prenatally a unilateral MCKD was diagnosed and to
assess the additional diagnostic value of cystoscopy and colposcopy (in girls) when a
nephrectomy was performed.
MATERIALS AND METHODS
One hundred children with a prenatally diagnosed unilateral MCKD, between January
1986 and December 2001, were evaluated. Data were obtained by reviewing the
database of the obstetric ultrasound department and of the paediatric urology
department of the University Medical Centre Utrecht, The Netherlands. In all children
postnatal ultrasound examination within a few days after birth confirmed the
presence and location of the multicystic kidney. Within four weeks all infants had a
voiding cystourethrography (VCUG) without anaesthesia to exclude reflux in the
opposite kidney and a MAG3 renography or DMSA scan to measure function. In case
of VUR antibiotic prophylaxis was given. All surviving children were offered a
nephrectomy at the age of approximately six months, under general anaesthesia,
combined with cystoscopy and the girls were also offered a colposcopy.
RESULTS
Unilateral MCKD was diagnosed in 100 fetuses between 15 and 42 weeks of
gestation: 21% before 20 weeks gestation, 49% between 20 and 30 weeks gestation
and 30% thereafter (mean 26.7 weeks). The left to right affected kidney ratio was 47 :
53. There were 58 boys, 41 girls and 1 fetus with unknown sex because of
sirenomelia. Thirteen fetuses died in the perinatal period: 9 with an agenesis of the
contralateral kidney, 1 with a contralateral dysplastic kidney, megabladder and
arrhythmia, 1 with a contralateral dysplastic kidney, pulmonary hypoplasia and
sirenomelia and 2 with idiopathic pulmonary hypoplasia. Autopsy was performed in 7
of these infants and the diagnoses were confirmed.
The other 87 infants survived and were between 0 -16 years (mean 5 years and 4
months) at follow-up. All living infants were morphologically normal. Four parents
refused investigations after birth. In the remaining 83 an ultrasonography, a VCUG
and an isotope scan were performed within a few weeks after birth. The multicystic
kidney was non-functional in 80 children and had a function of 3% to 7% of total renal

Concomitant anomalies with unilateral multicystic kidney 75
function in the other three. Seventy-five of the 100 children had one or more
additional anomalies. Thirty-nine of these infants had 52 renal anomalies of the
contralateral kidney of which agenesis, hydronephrosis and pyelectasis as most
occurring. Forty-two infants had 56 renal anomalies of the ipsilateral kidney so
besides the multicystic kidney an ectopic or megaureter as most common and
another 28 infants had altogether 32 anomalies of the lower urogenital tract with as
most diagnosed an infravesical obstruction (Table 1). No differences were made
between minor or major anomalies neither between primary or secondary developed
abnormalities. Reflux was seen in 9 children, 7 boys and 2 girls. It was bilateral in 3
cases. Three children had a reimplantation of the ureter and 1 endoscopic treatment
by subureteric injection of a bulking agent.
Table 1 – 100 infants with unilateral MCKD. Total number of minor and major anomalies ofthe contralateral kidney (39 infants), ipsilateral kidney (42 infants) and of the lower urogenitaltract (27 infants), which were primary or secondary developed.
contralateral kidney ipsilateral kidney lower urogenital tract
kidney agenesis 9
kidney non-cystic dysplasia 5
duplex system 1 4
ectopic pelvic kidney 1 3
horseshoe kidney 1
spider kidney 1
hydronephrosis* 7
VUR 9 3
megaureter 5 10
ectopic ureter 32
partially doubled urethra 2
ureterocele 2 2
infravesical obstruction 18
megabladder↑
3
diverticulum of the bladder wall 3
urethral meatus stenosis 5
multicystic testicle 1
Mayer-Rokitansky syndrome 1
hymen imperforates 1
total anomalies 41 56 32
* renal pelvis diameter >10mm anteroposterior, # renal pelvis diameter 5-10 mm anteroposterior, ↑ topof the bladder reached the umbilical height
Two of the 5 infants with a contralateral kidney dysplasia died perinatally. The other
three are 2, 4 and 10 years old and have creatinine levels of 94, 35 and 75 µmol/l.,
respectively. The two-year-old boy is mentally and motor retarded with syndromal

76 Chapter 6
anomalies without a specific diagnosis, the 4-year-old boy is idiopathic motor
retarded and the 10-year-old boy is otherwise healthy.
Nine infants had also extra renal anomalies (Table 2). One of the latter died
neonatally and four are mentally and/ or motor retarded.
Table 2 - Associated extrarenal anomalies in 9 cases with unilateral MCKD
infant alive anomaly 1 anomaly 2 anomaly 3 structural anomalies male yes anus atresia partial sacral agenesis male yes multiple congenital spina bifida neurogenic bladder male yes pulmonary valve male* no cheilo-gnatho- - - functional anomalies male yes hypertension mental retardation motor retardation female yes dimorphism hypotonic motor retardation female yes dimorphism mental retardation motor retardation male yes panhypopituitarism male yes mental retardation motor retardation - * Fetus died; there was a contralateral kidney agenesis.
In general, anomalies were divided equally between boys and girls except for
predominance in males of contralateral kidney agenesis (8 out of 9), ectopic ureter
(23 out of 32) and infravesical obstruction (18 out of 21).
Eighty-one infants were operated: 79 had a nephrectomy and 2 a hemi-nephrectomy
and thirty-seven of these 81 children needed 53 other interventions for urological
anomalies (Table 3). At histology of the 81 multicystic kidneys the diagnosis of
MCKD was confirmed in all cases including the three cases with minimal function on
the isotope scan. Cartilage was found in 54 specimens (66,6%) and a nephrogenic
rest lesion in 6 kidneys (7,4%).
Table 3 - Interventions in 81 children with unilateral MCKD surgery No. nephrectomy 79 hemi-nephrectomy 2 reimplantation of a ureter 7 pyeloplasty 4 resection of urethral valves 18 meatotomy 5 excision ureterocele/ diverticulum 6 incision partial double urethra 1 excision multicystic testis 1 endoscopic treatment by subureteric injection of a bulking agent in VUR 1 orchidopexy 1 other small incisions/ excisions 9 total interventions 134

Concomitant anomalies with unilateral multicystic kidney 77
In two cases there was a bladder incision made to remove the distal segment of the
ectopic ureter that ended in both cases in an ureterocele. In all other cases the ureter
was removed as far as possible at the nephrectomy. Reimplantation of a ureter was
performed in 7 cases: 3 times because of VUR (grade III, IV and V), twice the
remaining ureter after heminephro-urethrectomy, once it was a solitary obstructive
megaureter and once it was together with a pyeloplasty and ureteral obstruction.
Directly before nephrectomy cystoscopy was performed. Thirty-six of the 81 infants
(44,4%) had one or more anomalies: 18 had urethral obstruction, 5 meatal stenosis,
3 a secondary diverticulum of the bladder and 32 an ectopic ureter of which 1 ended
in a utricular cyst and 2 in an ectopic ureterocele. In 10 of the 18 children with a
urethral obstruction an excision of urethral valves was performed and in the other 8
an incision was done because of a narrow bladder neck or mid-urethral stenosis. In 2
of the 5 children with a meatal stenosis the meatus was obstructive for the
cystoscope and in three other girls calibration of the meatus was narrow for age and
the jet of urine was anomalous.
In 35 girls colposcopy was performed. In 3 of them (8,6%) anomalies of the genital
tract were found. One girl had Mayer-Rokitansky’s syndrome (vaginal atresia, uterus
duplex, abnormal pelvic blood vessels) and 1 child had an imperforate hymen.
Another 4 girls had an ectopic ureter ending into a Gartner’s duct of (in 1 case with
an opening into the vagina, diagnosed at colposcopy). Six girls had no colposcopy: 3
had died perinatally and 3 had no surgery at all.
The diagnosis of an ectopic ureter was made at the cystoscopy by seeing a
hemitrigonum and an absent orifice. At nephrectomy 10 ureters could not be traced
and the histology of the remaining 22 ectopic ureters showed that 2 had a double
lumen, that 7 were atretic, that 1 was fibrotic, that 6 were mega dilated (2 ending in a
ureterocele, 1 ending in a seminal vesicle), that 1 was totally obstructed, that 4 ended
in the duct of Gartner and that 1 ended in a ureterocele. There was one boy with a
scrotally located multicystic testicle removed from the same side as the multicystic
kidney.
Six children had no surgery at all because two parents refused surgery, two children
have one moiety of a well functioning duplex system affected and 2 were under
control elsewhere and conservative management was recommended by their
paediatricians.

78 Chapter 6
DISCUSSION
Children with unilateral MCKD have an increased risk of abnormalities of the
contralateral kidney and the lower urogenital tract9, 14, 15, 20. The finding of a unilateral
MCKD must therefore lead to meticulous screening of the complete urinary tract,
both pre- and postnatally, as most studies also recommend, which implies a full
urologic investigation to verify the diagnosis, to assess renal functioning and to
exclude or confirm additional anomalies, which may require additional urologic
treatment.
There is no uniformity of opinion on the role of nephrectomy in the management of
MCKD. Most authors stated that indications for surgery include a large mass
compromising respiration or feeding, pain or an enlarging mass. The increased
incidence of hypertension warrants routine blood pressure monitoring by some
authors and others stated that there is no increased risk2, 8, 15, 21, 22. An every 3 to 6
months ultrasound scan is recommended by some authors because of a higher risk
on malignant degeneration18 while others claimed the opposite2, 15. Webb et al18
recommend nephrectomy because of a higher risk on hypertension and malignancy
and Ranke et al23 advices the same because of money saving on the long-term.
Manzoni et al8 describe indications for management but admitted that long-term
follow-up is requested and because of poor parental compliance nephrectomy should
strongly be considered.
The view of the Dutch Society for Paediatric Urology is that nephrectomy done at the
early age of approximately six months, because flank musculature is hardly used at
that time because most of the children cannot yet sit, is as a minor operation with
negligible morbidity. This allows for day-care nephrectomy or short stay due to limited
need of post operation analgesia. There will be no need for the lifetime follow-up in
case the kidney is left in place because this long-term follow-up will easily be
neglected in the course of years. Furthermore parents need not to be anxious when
their child has abdominal pain.
Different to all referred sources we performed a cystoscopy and in girls a colposcopy
prior to nephrectomy. With these examinations a high number of anomalies of the

Concomitant anomalies with unilateral multicystic kidney 79
urinary tract and of the internal genital organs was detected with ectopic ureters in
40% of the children, infravesical obstructions in 26% and - in girls - an ectopic ending
ureter into the duct of Gartner in 11%, as most common findings. Some may argue
that only 3 anomalies discovered by colposcopy can lead to the conclusion that this
examination is superfluous. But an atresia of the vagina and hymen imperforates
would not have been found at the standard investigation after birth (department of
neonatology: personal communication) and probably not earlier than the beginning
of the puberty. In our opinion colposcopy is a minor intervention in a child already
under anaesthesia and every anomaly found is of importance for the child and for her
parents. Moreover we found 4 ectopic ending ureters into a Gartner’s duct, one with
an opening into the vagina, which otherwise would not have been detected.
Nephrectomy, preferably at the age of approximately six months was proposed to all
parents according to the guidelines of the Dutch Society for Paediatric Urology.
At histology cartilage was found in 66,6% of the removed multicystic kidneys which is
thought to be a sign of dysplasia as a result of obstruction11, 24. A nephrogenic rest
lesion was found in 7,4% of the removed MCKD kidneys and is considered a risk
factor for developing a Wilms tumor25 later in life. A similar percentage (6,4%) was
found by Dimmick et al26.
The differences in outcome for anomalies on the contralateral or ipsilateral kidney
and the lower urogenital tract are remarkable when we compare our series with
others. In our study 39 children had 41 anomalies of the contralateral kidney. We
found agenesis of the kidney in 9% of cases comparable with Lazebnik et al12 but
higher than the 2,3 to 2,6% of others14, 20. A hydronephrosis was seen in 18% of
children higher than the 7,9 to 12 % of others12. In approximately 11% of the children
VUR was diagnosed hardly higher than the 8% of van Eijk et al20 but lower than the
14 to 20% of others20, Wacksman et al15 mentioned even 43%.
In our study 42 children had 56 abnormalities on the ipsilateral side with an ectopic
ureter in 38,6% and a megaureter in 12,1% as most common. Those anomalies are
mentioned sporadically or not at all in the literature in which VUR and UPJ stenosis

Table 4 – An ove
rview of co
nco
mita
nt anomalies in children with
a unila
teral m
ulticy
stic kidney in seven studies.
anomaly
contralateral
ipsilateral
lower tract
extrarenal
author
total
No.
N (%) with
additional renal
anomalies
total N
o.
agenesis
dys
plasia
hyd
ronephrosis
/ pye
lectasis
VUR
Atiy
eh 1992
49
25 = 51 %
39%
4%
12%
18%
6,1%
6,1%
Al-Khaldi
1994
30
17 = 57 %
23,3%
2,3%
20%
13,3%
Rudnik –
Sch
onebőrn
1998
204
? = 27 %
27%
14%
Laze
bnik
1999
102
27 = 23 %
32%
9%
9,8%
3,8%
3,8%
35%
Aubertin
2002
54
18 = 33 %
24,1%
5,5%
3,7%
16%
Eijk van 2002
38
8 = 21 %
13%
2,6%
7,9%
8%
8%
5,3%
prese
nt
study
100
75 = 75 %
48,1%
9%
5%
18%
10,8%
48,3%
33%
10%

Concomitant anomalies with unilateral multicystic kidney 81
were mostly mentioned9, 20. We found ureteroceles in 4 cases (4,8%) comparable
with Lazebnik et al12 with an incidence of 3.8%. VUR was found in 9 children (10,8%)
comparable with the 8% of van Eijk et al20 but lower than the 14% till 43% mentioned
by others2, 9, 14, 15.
A lower urinary tract anomaly was only mentioned by Atiyeh et al9, 12 in 6% of cases.
This study found 32 anomalies in 26 infants (31.3%): an infravesical obstruction in
21,7% (18 infants), a diverticulum in 3,6% (3 infants) and a stenosis of the urethral
meatus in 6,0% (5 infants) as most common. Posterior urethral valve incision was
done at the judgment of the paediatric urologist at the time of cystoscopy and we are
aware that the incidence of infravesical obstruction and consequently incision of
urethral valves is high compared to other studies. There was no urodynamic study
done routinely before the valve incision to proof the obstruction and it was up to the,
subjective, judgment of the surgeon whether or not to incise the folds.
Associated extrarenal anomalies were found with an incidence of 10%, less than the
16% of Aubertin et al1, 12 and the 35% as reported by Lazebnik et al1, 12. Outcome,
however, is not comparable because in most studies another target group was
included e.g. both bilateral and unilateral MCKD or a different population limited to
fetuses with chromosomal analysis. Only van Eijk et al20 described a comparable
population and reported an incidence of 5,3% of extrarenal anomalies. Mental and
motor retardation in 4 cases was the most common extrarenal anomaly in our study
followed by a cardiac abnormality in 2 children. Table 4 shows an overview of all
additional anomalies found in our study in comparison with literature.
The male to female ratio (58 : 41) showed a predominance of males similar to the
literature.
The left to right affected kidney ratio in our series was 47 : 53. This is in contrast with
literature that reports more left-sided multicystic kidneys identical with the explanation
that the left kidney is more often associated with primary obstruction(27, 28). We have
no explanation for this difference and It is probably “simply chance” that our ratio is
the opposite.

82 Chapter 6
We agree that the benefice for the child is not demonstrated with our invasive
management. The problem is that a large randomised controlled study is needed to
prove whether a nephrectomy or an expectant policy has the preference. In addition
follow-up will be needed during several decades because hypertension or
malignancy can develop later in life.
CONCLUSIONS
Children with unilateral MCKD have a considerable chance of having other
congenital anomalies of the urinary tract and therefore they need to be precisely
screened pre- and postnatally. We recommend that a routine postnatal examination
consist of an ultrasound examination, an isotope scan and a VCUG and when a
nephrectomy is done also a cystoscopy and a colposcopy to detect possibly hidden
anomalies of the genitourinary tract.

Concomitant anomalies with unilateral multicystic kidney 83
REFERENCES
1. Aubertin G, Cripps S, Coleman G, McGillivray B, Yong SL, Van Allen M, et al. Prenatal diagnosis of apparently isolated unilateral multicystic kidney: implications for counselling and management. Prenat Diagn 2002;22(5):388-94. 2. Rudnik-Schoneborn S, John U, Deget F, Ehrich JH, Misselwitz J, Zerres K. Clinical features of unilateral multicystic renal dysplasia in children. Eur J Pediatr 1998;157(8):666-72. 3. Beck AD. The effect of intra-uterine urinary obstruction upon the development of the fetal kidney. J Urol 1971;105(6):784-9. 4. Peters CA. Animal models of fetal renal disease. Prenat Diagn 2001;21(11):917-23. 5. Winyard P, Chitty L. Dysplastic and polycystic kidneys: diagnosis, associations and management. Prenat Diagn 2001;21(11):924-35. 6. Felson B, Cussen LJ. The hydronephrotic type of unilateral congenital multicystic disease of the kidney. Semin Roentgenol 1975;10(2):113-23. 7. Peters CA, Carr MC, Lais A, Retik AB, Mandell J. The response of the fetal kidney to obstruction. J Urol 1992;148(2 Pt 2):503-9. 8. Manzoni GM, Caldamone AA. Pediatric Surgery and Urology: Long Term Outcome. London: W.B. Saunders; 1998. 9. Atiyeh B, Husmann D, Baum M. Contralateral renal abnormalities in multicystic-dysplastic kidney disease. J Pediatr 1992;121(1):65-7. 10. Srivastava T, Garola RE, Hellerstein S. Autosomal dominant inheritance of multicystic dysplastic kidney. Pediatr Nephrol 1999;13(6):481-3. 11. Zerres K, Volpel MC, Weiss H. Cystic kidneys. Genetics, pathologic anatomy, clinical picture, and prenatal diagnosis. Hum Genet 1984;68(2):104-35. 12. Lazebnik N, Bellinger MF, Ferguson JE, 2nd, Hogge JS, Hogge WA. Insights into the pathogenesis and natural history of fetuses with multicystic dysplastic kidney disease. Prenat Diagn 1999;19(5):418-23. 13. Nicolaides KH, Cheng HH, Abbas A, Snijders RJ, Gosden C. Fetal renal defects: associated malformations and chromosomal defects. Fetal Diagn Ther 1992;7(1):1-11. 14. Al-Khaldi N, Watson AR, Zuccollo J, Twining P, Rose DH. Outcome of antenatally detected cystic dysplastic kidney disease. Arch Dis Child 1994;70(6):520-2. 15. Wacksman J, Phipps L. Report of the Multicystic Kidney Registry: preliminary findings. J Urol 1993;150(6):1870-2. 16. Lippert MC. Renal Cystic Disease. In: (eds) LWW, editor. Adult and Pediatric Urology. Philadelphia; 2002. p. 829-878. 17. Elder JS, Hladky D, Selzman AA. Outpatient nephrectomy for nonfunctioning kidneys. J Urol 1995;154(2 Pt 2):712-4; discussion 714-5. 18. Webb NJ, Lewis MA, Bruce J, Gough DC, Ladusans EJ, Thomson AP, et al. Unilateral multicystic dysplastic kidney: the case for nephrectomy. Arch Dis Child 1997;76(1):31-4. 19. LaSalle MD, Stock JA, Hanna MK. Insurability of children with congenital urological anomalies. J Urol 1997;158(3 Pt 2):1312-5.

84 Chapter 6
20. Eijk van L, Cohen-Overbeek TE, den Hollander NS, Nijman JM, Wladimiroff JW. Unilateral multicystic dysplastic kidney: a combined pre- and postnatal assessment. Ultrasound Obstet Gynecol 2002;19(2):180-3. 21. Sukthankar S, Watson AR. Unilateral multicystic dysplastic kidney disease: defining the natural history. Anglia Paediatric Nephrourology Group. Acta Paediatr 2000;89(7):811-3. 22. Oliveira EA, Diniz JS, Vilasboas AS, Rabelo EA, Silva JM, Filgueiras MT. Multicystic dysplastic kidney detected by fetal sonography: conservative management and follow-up. Pediatr Surg Int 2001;17(1):54-7. 23. Ranke A, Schmitt M, Didier F, Droulle P. Antenatal diagnosis of Multicystic Renal Dysplasia. Eur J Pediatr Surg 2001;11(4):246-54. 24 Glassberg KI, Stephens FD, Lebowitz RL, Braren V, Duckett JW, Jacobs EC, et al. Renal dysgenesis and cystic disease of the kidney: a report of the Committee on Terminology, Nomenclature and Classification, Section on Urology, American Academy of Pediatrics. J Urol 1987;138(4 Pt 2):1085-92. 25. Beckwith JB. Nephrogenic rests and the pathogenesis of Wilms tumor: developmental and clinical considerations. Am J Med Genet 1998;79(4):268-73. 26. Dimmick JE, Johnson HW, Coleman GU, Carter M. Wilms tumorlet, nodular renal blastema and multicystic renal dysplasia. J Urol 1989;142(2 Pt 2):484-5; discussion 489. 27 Glassberg KI. Dilated ureter. Classification and approach. Urology 1977;9(1):1-7. 28. Johnston JH, Evans JP, Glassberg KI, Shapiro SR. Pelvic hydronephrosis in children: a review of 219 personal cases. J Urol 1977;117(1):97-101.

Chapter 7 Mild pyelectasis diagnosed by prenatal ultrasound is not a predictor of urinary tract morbidity in childhood H.A. Damen–Eliasa, S.E. Luijnenburga, G.H.A. Vissera, P.H. Stoutenbeeka, T. P.V.M. de Jongb a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Department of Paediatric Urology, University Hospital Utrecht, The Netherlands

86 Chapter 7
ABSTRACT
Objectives To determine children whether with an antenatally diagnosed mild
pyelectasis have more urinary tract morbidity during childhood than children without
this finding.
Methods Case-control study in children with pyelectasis (anteroposterior diameter of
the fetal renal pelvis of 5-10 mm) detected at about 20 weeks of gestational age by
ultrasound. A validated questionnaire, regarding voiding and defecation habits and
urinary tract infections (UTI), was send to the parents of 208 cases and 416 matched
controls.
Results The questionnaire was returned by 146 cases and 250 controls. There was a
male predominance in the case group as compared to the controls (p=<0,000). There
were neither differences in voiding habits nor in incidence of UTI. The incidence of
infections was high in both groups: 11,6% in cases and 10,0% in controls. The only
difference between the groups was a higher incidence of constipation (stools
frequency of 2 times a week or less) in the case group (p=0,003).
Postnatally forty-one children had an ultrasound examination and 16 were referred to
a paediatrician or urologist: 3 had persisting pyelectasis, 3 had a recurrent urinary
tract infection (one girl also VUR grade I) and 1 required surgery (a pyeloplasty).
Four of the controls were referred to a paediatrician or urologist: 3 had recurrent UTI
and 1 was urinary incontinent.
Conclusion Children with a mild fetal pyelectasis do not have more urinary tract
morbidity during childhood than children without this finding. Therefore, there seems
to be no need for additional investigation after birth.

Mild pyelectasis 87
INTRODUCTION
Mild uni- or bilateral fetal pyelectasis is a frequent finding at prenatal ultrasound
examination, with a considerable variation in the reported incidence, from 0,6% to
5,5%1-4. This wide variation is likely to be due to differences in criteria as to the
definition of pyelectasis, in particular regarding size and gestational age at diagnosis.
The clinical significance of mild fetal pyelectasis is still unclear; it may resolve,
stabilize or be the first indicator of significant urinary tract pathology. The
anteroposterior diameter of the renal pelvis above which further investigation during
or after pregnancy is required is still controversial3, 5-7. Some investigators consider
an anteroposterior diameter of the renal pelvis <10 mm as physiological, since this
will resolve or improve within a couple of years after birth8-11. Others recommend a
full postnatal investigation for all fetuses with mild pyelectasis1, 12-14. In their opinion a
significant percentage of these infants will have vesico ureteral reflux (VUR) or need
postnatal surgery, when the pyelectasis persists at a follow-up scan around 32 weeks
of gestation.
Evidence exists that pyelectasis may result in clinical complications such as
obstructive uropathy or VUR. A single observation of a pyelectasis puts the fetus at
risk for VUR but a normal scan does not exclude the possibility of VUR13, 15. So far no
correlation has been found between antenatal and postnatal dilatation and the
severity of VUR13. There is a suggestion of a between-pregnancy consistency in fetal
pyelectasis in subsequent pregnancies and this emphasizes the possibility that
genetic and/or environmental factors play a role in its development16-19.
Counselling the parents is difficult due to our limited understanding of the natural
history of pyelectasis. False positive diagnosis of fetal pyelectasis may lead to
unwarranted anxiety, as well as unnecessary and expensive diagnostic investigations
after delivery.
Pyelectasis is still a controversial problem since renal pelvis measurements are not
well standardized and since there are no consistent guidelines in relating the severity
of pyelectasis to appropriate perinatal and postnatal management. Because of the
lack of data on possible long-term morbidity in late childhood in infants who had been
antenatally diagnosed as having mild pyelectasis, it was the aim of this study to
investigate the occurrence of urinary tract morbidity in childhood in these infants in

88 Chapter 7
comparison to a control group, to assess if there is an indication for postnatal
follow-up of these children.
METHODS
In the Netherlands standard screening for fetal anomalies has not yet been
introduced, in spite of an extensive debate. Nonetheless, in the Amphia hospital (a
District General Hospital, location Oosterhout, The Netherlands), the anomaly scan
has been introduced for all pregnant women in the early 1980’s. Two midwives–
ultrasonographer examined all women at 18 – 20 weeks gestational age using the
same ultrasound machine. Data were recorded in a standardized way.
When a pyelectasis was noticed, defined as an anteroposterior diameter (A-P
diameter) of the renal pelvis of 5–10 mm, the anteroposterior diameter of the renal
pelvis was measured when in a sagittal plane the full length with the renal pelvis was
visualised and perpendicular to this, in the largest sectional plane, the
anteroposterior diameter of the pelvis by placing the callipers on the inner borders of
the renal tissue. No dilatation of the calices was noticed unless the pyelectasis
exceeded 10 mm. All examinations were carried out during daytime. Maternal fluid
intake was not specified because it is questionable whether maternal hydration
influences fetal pyelectasis20-22.
When a mild pyelectasis was found, it was customary to re-exam the women at
approximately 32 weeks of gestation. When the A-P diameter exceeded 10 mm, the
child was referred to a paediatrician or urologist for urological follow-up during the
first weeks of life. When the mild pyelectasis had stabilized or resolved, the parents
were advised to refrain from further investigations before or after birth and were told
that their child might have an increased risk for urinary tract infection (UTI) due to
VUR and that, in case of feeling listless or fever of unknown origin, UTI should be
ruled out. This advice corresponds to the current opinion about pyelectasis in the
Netherlands.
The archives of the obstetric ultrasound department were reviewed over the period
January 1st, 1994 till December 31st, 1998. All accounts of fetuses with an isolated
mild uni- or bilateral pyelectasis were extracted, in common with the notes of controls
(two per case) seen on the same day, in which no anomaly had been found.

Mild pyelectasis 89
The local ethical review board and the board of the University Medical Centre
Utrecht, The Netherlands, authorized the study.
After written informed consent was obtained, the parents of the cases and controls
were asked, to fill out a standardized questionnaire (Appendix 1) regarding voiding
and defecation patrons and urinary tract infections. The questionnaire, we used, was
based on the validated questionnaire used in the International Reflux Study in
Children(23). Simultaneously they answered questions about day and night potty
training of the child and consultations of the general practitioner or other doctors
(Appendix 2). We choose the study period 1994-1998 because for answering the
questionnaires the children had to be potty-trained.
Statistical analyses were performed using Statistical Product and Service Solutions
package 10.1 (SPSSR)24. For the calculations the t-test, the chi-square test or the
Fisher’s exact test (we appropriate) were used, with p<0.05 considered significant.
RESULTS
During the 5-year study period the 18-20 weeks anomaly scan was performed in
4532 pregnant women. Uni- or bilateral pyelectasis was diagnosed in 208 fetuses,
giving an incidence of 4,6 %. In 164 fetuses (78,8%) there was a bilateral pyelectasis
and in 44 (21,2%) a unilateral pyelectasis. The ratio of bilateral to unilateral affected
kidneys was 4 : 1 and in the group with a unilateral pyelectasis the ratio of the right to
left kidney was 1 : 1.
One hundred and seventy-nine fetuses with pyelectasis, 179/208 (86,1%), were
rescanned at approximately 32 weeks (range 28 till 38 weeks). The pyelectasis was
resolved in 67 fetuses (37,4%) was stable in 96 fetuses (53,6%) and had progressed
to >10 mm in 16 fetuses (8,9%). These 16 cases were excluded from the present
study since these children were referred for urological follow-up during the first week
of life. In 20 fetuses (11,2%) the pyelectasis had changed from bilateral to unilateral
and in 4 children (2,2%) from unilateral to bilateral.
The response rate was 146 out of 192 cases (208 – 16 excluded cases) and 250 out
of 416 controls. Five cases and 4 controls could not be traced and were lost to
follow-up, giving corrected response rates of 76,0% (146/192) and 60,7% (250/412),
respectively. In the case group another 17 fetuses were excluded because no repeat

90 Chapter 7
scan had been made at 32 weeks gestation and we therefore lacked information
about dilatation of the renal pelvis during the third trimester. So, finally the
calculations were made on 129 cases and 250 controls. There were no significant
differences between responders and non-responders except for maternal age at the
first ultrasound examination (p=0,005; see Table 1).
Table 1 - Comparison between patient characteristics of responders and non-responders inthe casegroup.
variable respondersn = 146
non-respondersn = 57
significantdifference?
mean maternal age at time of the firstgestational ultrasound examination
30 years, 10months
28 years, 11months
p =0,005 *
mean age (wks) of detection of pyelectasis 21,6 22,1 p = 0,449mean number of antenatal ultrasoundexaminations
2,5 2,7 p = 0,221
mean number of previous deliveries of themother
0,77 0,75 p = 0,939
unilateral pyelectasis at time of detection 31 12 p = 0,977bilateral pyelectasis at time of detection 115 45 p = 0,977no follow-up ultrasound examination± 32 weeks
17 12 p = 0,085
pyelectasis resolved (<5mm) duringpregnancy
47 18 p = 0,933
pyelectasis stabilized (5-10mm) duringpregnancy
72 21 p = 0,109
pyelectasis progressed (>10mm) duringpregnancy
10 6 p = 1,000
pyelectasis changed from bilateral tounilateral
11 8 p = 0,153
pyelectasis changed from unilateral tobilateral
4 0 p = 0,578
* significant difference
The responders in the case and control group were comparable on the most
important items (Table 2).
Table 2 - Comparison between patients’ characteristics of the responders in the case andcontrol group.
variable case-groupn = 146
control-groupn = 250
significantdifference?
mean maternal age at time of delivery 31 years, 2months
30 years, 5months
p = 0,057
mean number of pregnancies 1,98 1,84 p = 0,207mean number of previous deliveries 0,77 0,63 p = 0,094mean current age of the children 6 years, 1month 5 years, 9
monthsp = 0,314
mean number of antenatal ultrasoundexaminations
2,52 1,63 p = <0,000*
* significant difference

Mild pyelectasis 91
As expected, the only variable that showed a significant difference was the number of
antenatal ultrasound examinations (p=<0,000) because of the repeated ultrasound
scan in the third trimester of pregnancy in the case group; median of number of
examinations in the case group 2,52 and in the control group 1,63.
Data on voiding and defecation habits and urinary tract infections are shown in Table
3. On three items there were significant differences: a) the male to female ratio in the
case group was 2,17:1 and in the control group 1:1,02 (p=<0,000), b) children in the
case-group were more often constipated, when constipation was defined as a stool
frequency of 2 times a week or less (p=0,003), c) children in the case group were
potty trained during daytime at a slightly higher age (p=0,026).
Table 3 - Voiding and defecation habits and urinary tract infections in the case and controlgroup.
variable case-group
n = 129
control-group
n = 250
significant
difference?
number of males 88 124
number of females 41 126
Male : Female ratio 2,17 : 1 1 : 1,02 p = <0,000*
daytime urinary incontinence 22 = 17,1% 34 = 13,6% p = 0,476
nocturnal enuresis 30 = 23,3% 49 = 19,6% p = 0,794
urinary tract infection 17 = 11,6 % 25 = 10 % p = 0,601
soiling 17 = 11,6 % 45 = 18,0% p = 0,095
constipation A = stool frequency of <2 times a
week
9 = 7,0% 2 = 0,8% p = 0,003*
constipation B = hard stools 9 = 7,0% 14 = 5,6% p = 0,811
constipation C = stool frequency of <2 times a
week and hard stools
1 = 0,8% 0 p = 0,368
constipation treatment 4 = 3,1% 2 = 0,8% p = 0,195
mean number of months in which the children
were trained in voiding during daytime
3 years,
1 month
2 years,
10 months
p = 0,026*
mean number of months in which the children
were trained in voiding during nighttime
3 years,
4 months
3 years,
2 months
p = 0,128
mean number of months in which the children
were trained in stools
3 years,
0 months
2 years,
11 months
p = 0,108
* significant difference

92 Chapter 7
In Table 4 data are presented separately for males and females. There were no
significant differences between the boys and girls except for a higher incidence of
constipation A in the females in the case group (p=0,005). The incidence of UTI was
not different in boys and girls of case and control groups: 17 cases, 17/129 (13,2%):
6 males and 11 females and in 25 controls, 25/250 (10,0%): 6 males and 19 females.
Table 4 - Voiding and defecation habits and urinary tract infections (in numbers or mean agein years and months) in males and females from the case and control group.
malesn = 212
females n = 167
variable
casen = 88
controln = 124
p-value casen = 41
controln = 126
p-value
daytime urinary incontinence 17 17 p=0,743 5 17 p = 0,873
nocturnal enuresis 24 30 p=0,993 6 19 p = 0,737
urinary tract infection 6 6 p=0,699 11 19 p = 0,177
soiling 12 21 p=0,314 5 24 p = 0,198
constipation A = stool frequency
of <2 times a week
3 0 p=0,088 6 2 p =0,005*
constipation B = hard stools 5 6 p=1,000 4 8 p = 1,000
constipation C = stool frequency
of <2 times a week or less and
hard stools
0 0 ---- 1 0 p = 0,267
constipation treatment 3 1 p=0,321 1 1 p = 1,000
mean age (n of years/ months) of
potty-training during daytime
3 years,
1 month
3 years,
0 months
p=0,420 3 years,
4 months
2 years,
9 months
p = 0,245
mean age (n of years/ months) of
potty-training during nighttime
3 years,
5 months
3 years,
4 months
p=0,256 3 years,
0 months
3 years,
0 months
p = 0,915
mean age (n of years/ months) at
which the children were trained in
stools
3 years,
1 month
3 years,
0 months
p=0,543 2 years,
10 months
2 years,
9 months
p = 0,464
* significant difference
In spite of our advice to refrain from any investigation postnatally, 41 children, 41/129
(31,8%), in the case-group received a postnatal ultrasound examination of the urinary
tract. Sixteen of them were subsequently referred to a paediatrician or urologist. Nine
of these infants received prophylactic antibiotics, 9/129 (7,0%). The dilatation
resolved spontaneously in 7 of the 16 referred children; in 3 infants the dilatation
persisted but no further treatment was necessary; 3 infants had recurrent UTI (with a

Mild pyelectasis 93
VUR grade I in one female); 1 child had a dilatation of an extrarenal pelvis; 1 child
had transient haematuria but normal anatomy of the urinary tract and 1 infant
required surgery. This child, a boy, showed a unilateral pyelectasis at 20 weeks
gestational age of 8mm, which had stabilized (9 mm) at the 31 weeks ultrasound
scan. The boy required surgery 36 months after birth because of progressive
pelvicalyceal dilatation and deterioration of the renal function. In the control group 4
children were referred to a paediatrician or urologist: 3 had recurrent UTI and 1 had
problems with urinary incontinence. All infants in the case and control group are
doing well and have normal renal function.
Thirty children of the remaining 88 children (129-41) in the case group consulted a
general practitioner 48 times, mindful of our advice to have the urine checked
because of lethargy or fever of unknown origin and 5 were treated with antibiotics
because of a proven UTI.
DISCUSSION
Little is known about urinary tract morbidity during childhood in children who had a
mild prenatal pyelectasis. Fetuses with a mild fetal pyelectasis are frequently
encountered during ultrasound examination, but the aetiology and clinical
significance are unclear. Distinguishing cases in which the pyelectasis has no clinical
consequences from those with underlying renal pathology is not yet possible and
consistent guidelines about antenatal and postnatal follow up are absent.
Questionnaires, which are a good method of studying large groups or to study a
population, were used to interview the children. A drawback is that the physical
examination and other tests are lacking and that the parents or guardians have to fill
in the test, which implies the possibility of subjective opinion. But an advantage is
that the information can be gathered without too much bother for the children and
their parents. Questionnaires can be used to screen on health, on the prevalence of
diseases or to investigate the quality of life25, 26. They should be tested before for
reproducibility and should be validated23.
Studies on antenatal detection of pyelectasis show considerable differences in
outcome3, 15, 27-31. Percentages for resolving of the pyelectasis range from 5 to 51%,
for remaining stable from 21 to 39% and for worsening from 9 till 27% (Table 5).
These wide variations are understandable given the different criteria for pyelectasis.

94 Chapter 7
Some authors have stated that the size of the prenatal dilatation is not a sensitive
predictor of pathology but that an increasing size during pregnancy is associated with
morbidity and mortality32. An A-P diameter of >10 mm is usually considered of
significance9, 15, but the Great Ormond Street Experience33 showed that there is a
very low risk of clinically significant obstruction when the dilatation does not exceed
15 mm at any gestational age.
We found hardly any (significant) differences in morbidity between children with or
without mild prenatal pyelectasis. There was a male predominance in the case group,
which is in concordance with findings of others (Table 5).
Table 5 - An overview of studies about mild fetal pyelectasis: definitions, course during pregnancy, sex ratio and advice given.
No. of fetuses
cut-off points pyelectasis
resolution stable progression ♂ : ♀ ratio
advice
Adra 1997 68 ≥4mm <33wks
≥7mm ≤10mm
at ≥33wks
31% ? ? 2 : 1 repeat scan 28 wks
gestation; full post natal
investigation in case
>8mm
Feldman
2001
347 ≥4mm ≤7mm
at ≤21wks
≥5mm ≤8mm
at >20wks
51% 39% 10% ? ?
Harding
1999
70 <10mm 30,4 21,4 19,6 2,2 : 1 repeat scan 34wks
gestation
ultrasound week 1 and 6
after birth
Morin
1996
122 ≥4mm ≤10mm
at < 20wks
≥5mm ≤10mm
at ≥20wks
29% 25% 9% ? ultrasound after >72 hours
after birth
Persutte
1997
294 ≥4mm ≤10mm
4,7% ? 27,1% 2,3 : 1 antibiotic prophylaxis -
ultrasound < 1 month after
birth + voiding
cystourethrography
present
study
208 ≥5mm ≤10mm 37,4% 53,6% 8,9% 2,2 : 1 repeat scan 32wks
gestation - after birth: urine
check in case of lethargy
or fever of unknown origin

Mild pyelectasis 95
Furthermore we found in the case group a low stool frequency and a higher age at
toilet training. There are no reports published in literature suggesting a correlation
between mild fetal pyelectasis and constipation during childhood.
There was no statistical significant difference in UTI between both groups, although
the incidence of 11,6% in cases and 10,0% in controls is higher than the 3,3% - 8,6%
found by others9, 34 and also higher than Dutch figures obtained from general
practitioners’ practices. Accordingly to those data the incidence of UTI’s in the
Netherlands is 2,9% (♂ 0,5%, ♀ 2,4%) in infants of 0 – 4 years of age and 3,2% (♂
0,4%, ♀ 2,8%)(35) in children of 5-9 years of age. It might be that the higher
incidence of UTI’s that we found in this study is due to the very detailed questions on
voiding and defecation habits in the questionnaire. De Kort et al36 have used the
same questionnaire in a study of hypermobility of joints in children of the same age
as in our study and found an incidence of UTI 15,7% in cases and 7,8% in controls.
Another reason for the high incidence of UTI – at least in the case group – might be
that general practitioners in this area are more focused on a UTI because of the
advice given to the parents to have the urine checked if their child is lethargic or
develops a fever of unknown origin. Earlier studies have reported that UTI’s are
underdiagnosed in children and concluded that a greater awareness of the
importance of investigation and management of UTI in children is needed because
as already known infections may lead to renal scarring37-39. Shaw et al40 reported that
even the presence of another potential source of fever, such as otitis media or
respiratory infection, does not reliably exclude UTI.
In spite of our advice, corresponding to the current opinion about pyelectasis in the
Netherlands, that in case of a mild fetal pyelectasis no further investigations were
needed after birth, 41 infants of these infants still had an ultrasound examination at
request of the general practitioner or gynaecologist. Sixteen children were referred to
a paediatrician or urologist (12,4%). Finally 1 child underwent surgery at the age of 3
years, because of an UPJ-obstruction. This resulted in a surgical intervention rate of
2,5% (1/41), or may be 0,8% (1/129), although we cannot completely exclude renal
pathology requiring surgery in the other infants. Anyhow the intervention rate seems
much lower than reported by others (3,6%-24,3%)1, 3, 27.

96 Chapter 7
CONCLUSIONS
The finding of fetal pyelectasis often generates considerable parental anxiety32, 34. At
birth the “affected” infants seem healthy and outwardly normal, but parental relief is
short-lived if their asymptomatic infant is then required to undergo intensive and
invasive investigations. Our study demonstrated similar incidence UTI’s. Therefore,
there seems to be no need for postnatal investigations. In case of a mild renal
pyelectasis at 20 weeks of gestation we suggest a single follow-up scan in the third
trimester to determine if the pyelectasis has resolved, stabilized or progressed. The
child should only be referred for postnatal examination if there is progression >10mm.
With this policy there is only a very small chance of missing an occasional case of
VUR or potential obstruction. On the other hand, however, this policy may reduce
parental anxiety and minimizes the burden of unnecessary invasive investigations in
healthy infants as well as unnecessary costs. Parents should be advised to visit their
general practitioner if their child is lethargic or has fever of unknown origin to have
urine tested to rule out UTI or treat infection effectively in order to prevent renal
damage.

Mild pyelectasis 97
APPENDIX 1
Questionnaire for children with voiding dysfunction and/or urinary tract infection,
translated from Dutch.
A2 Age .. years
A3 Gender □ boy
□ girl
A4 Date of filling out questionnaire .. .. ….
B Daytime incontinence
B1 Does your child wet his pants □ yes
□ no >> go to question B2
B1a If yes, at what age started the wetting
B1b If yes, how often does it happen □ < 3 times a week
□ 3-4 times a week
□ > 4 times a week
B1c If yes, are the pants □ damp
□ soaking
□ variable
□ don’t know
B1d If yes, wet pants □ all day
□ in the afternoon
□ variable
□ with physical activity
□ don’t know
B1e If yes, only in certain situations (playing) □ yes
□ no
□ don’t know
B1f If yes, does your child ignore the wet pants □ yes
□ no
□ don’t know
Continue with question C1
B2 When dry at daytime, at what age did your child
achieve continence .. years and .. months

98 Chapter 7
C Voiding habits yes no don’t know
C1 Is there normal early morning voiding □ □ □
C2 Do you have to send your child to the bathroom □ □ □
C3 Does your child void hasty and sloppy □ □ □
C4 Does your child strain during voiding □ □ □
C5 Is the stream interrupted or staccato □ □ □
C7 Is voiding painful □ □ □
C8 For girls: does she wet the toilet seat □ □ □
C9 For girls: is the meatus irritated □ □ □
C6 How often does your child void during day time □ < 4 □ 4-7 □ >7
D Urge and reaction on urge never sometimes always don’t know
D1 Does your child have difficult to suppress urgency □ □ □ □
D2 If yes, does your child take an urge position, like
squatting, crossing the legs, hand to the genitals □ □ □ □
D3 Is there adequate reaction to urge (timely voiding) □ □ □ □
D4 Does your child postpone voiding □ □ □ □
E Bedwetting
E1 Does your child wet the bed or diaper □ yes >> go to question E1b
□ no
E2 If no, at what age was your child continent at night .. years and .. months
E1b If yes, how many times a week . . times
E1c Are the sheets/diapers □ damp
□ soaking
E1d If yes, has your child been dry for > ½ year □ yes
□ no >> E2
E1da If yes, at what age started the bedwetting .. years and .. months
yes no sometimes don’t know
E2 Are there family members who wet their beds □ □ □ □
E3 Does your child wake up by itself to void □ □ □ □
E4 Is it hard to wake up your child to void □ □ □ □

Mild pyelectasis 99
F Urinary tract infection
F1 Has your child ever been treated by medication □ yes
for urinary tract infection □ no >> go to question G
F1a If yes, how often □ < 3
□ 3-10
□ > 10
F1b Since when …. (year)
F1c If yes, when was the last infection .. (month) …. (year)
F1d Does your child have low dose antibiotics □ yes
At the moment to prevent new infections □ no
F1da If yes, what kind of medication □ nitrofurantoin
□ norfloxacin
□ trimethoprim
□ other
G Defecation
G1 Frequency of defecation/stools □ once a day or more often
□ every 2 days
□ 1-2 a week
□ less than once a week
yes no sometimes don’t know
G2 Is defecation painful □ □ □ □
G3 Does your child feel urge to defecate □ □ □ □
G4 Form of stools □ soft but molded
□ firm and dry
□ very soft, not molded
□ otherwise, explain…
G5 Does your child have abdominal pain □ yes
□ no
G6 Is there fecal soiling □ yes
□ no >> go to question G8
G6a If yes, how often a week □ < 3 times a week
□ 3-4 times a week
□ > 4 times a week
G6b If yes, at what age started the soiling .. years and .. months
G7 Does your child ever defecate in its pants □ yes
□ no

100 Chapter 7
G8 Is your child being treated for constipation □ yes
□ no >> go to question G10
G8a If yes, in what way □ high fiber diet
□ lactulose
□ suppository
□ enema
□ bowel lavage
□ otherwise
G10 At what age did your child achieve fecal continence .. years and .. months
G11 How many cups does your child drink a day .. cups a day
Thank you for filling out the questionnaire.

Mild pyelectasis 101
APPENDIX 2
Does a mild dilatation of the urinary tract give morbidity in childhood? Last name mother:__________________________________________________________________ Date of birth mother: �� �� �� Ultrasound investigation: date �� �� year���� Code-number: ���� Name child (forename + family name) _____________________________________ boy / girl Address: _________________________________________________________________________ Zip code/ residence: ________________________________________________________________ Phone number: ______________________ Date of birth child: �� �� �� Is your child healthy? Yes O No O Don’t know O Is your child toilet trained? by day Yes O No O
at night Yes O No O
At what age your child was toilet trained? by day ______ year _____ months
at night ______ year _____ months
Had your child a little bit liquid in one or both kidneys??
Yes O No O → Go further on the next page.
If, yes, this was the right kidney O left kidney O both kidneys O You became the advice that if your child was lethargic to go to your general practitioner to have the
urine checked. Was did ever necessary? Yes O No O
If so, how often? 1 time O 2 times O 3 till 5 times O more than 5 times O
Has your child been to a doctor to have his kidneys checked? Yes O No O If so, did you become an advice? Yes O No O If so, which advice? ________________________________________________________________ _____________________________________________________________________________________________________ Became your child medication? Yes O No O Is your child still under control? Yes O No O If so, do you agree that we asked for information? Yes O No O If so, put your signature please? ______________________________________________________ What is the name of the doctor? ______________________________________________________ In which hospital? ______________________________________________________
Thank you for filling out the questionnaire.

102 Chapter 7
REFERENCES
1. Kent A, Cox D, Downey P, James SL. A study of mild fetal pyelectasia - outcome and proposed strategy of management. Prenat Diagn 2000;20(3):206-9. 2. Langer B, Simeoni U, Montoya Y, Casanova R, Schlaeder G. Antenatal diagnosis of upper urinary tract dilation by ultrasonography. Fetal Diagn Ther 1996;11(3):191-8. 3. Persutte WH, Koyle M, Lenke RR, Klas J, Ryan C, Hobbins JC. Mild pyelectasis ascertained with prenatal ultrasonography is pediatrically significant. Ultrasound Obstet Gynecol 1997;10(1):12-8. 4. Scott JE, Renwick M. Antenatal renal pelvic measurements: what do they mean? BJU Int 2001;87(4):376-80. 5. Ismaili K, Hall M, Donner C, Thomas D, Vermeylen D, Avni FE. Results of systematic screening for minor degrees of fetal renal pelvis dilatation in an unselected population. Am J Obstet Gynecol 2003;188(1):242-6. 6. Langer B. Fetal pyelectasis. Ultrasound Obstet Gynecol 2000;16(1):1-5. 7. Ouzounian JG, Castro MA, Fresquez M, al-Sulyman OM, Kovacs BW. Prognostic significance of antenatally detected fetal pyelectasis. Ultrasound Obstet Gynecol 1996;7(6):424-8. 8. Broadley P, McHugo J, Morgan I, Whittle MJ, Kilby MD. The 4 year outcome following the demonstration of bilateral renal pelvic dilatation on pre-natal renal ultrasound. Br J Radiol 1999;72(855):265-70. 9. Dremsek PA, Gindl K, Voitl P, Strobl R, Hafner E, Geissler W, et al. Renal Pyelectasis in fetuses and neonates: Diagnostic value of renal pelvis diameter in pre and postnatal sonographic screening. AJR Am J Roentgenol 1997(Apr;168(4)):1017-9. 10. Grignon A, Filion R, Filiatrault D, Robitaille P, Homsy Y, Boutin H, et al. Urinary tract dilatation in utero: classification and clinical applications. Mild dilatation of the fetal kidney: a follow-up study. Radiology 1986;160(3):645-7. 11. Thomas DF, Madden NP, Irving HC, Arthur RJ, Smith SE. Mild dilatation of the fetal kidney: a follow-up study. Br J Urol 1994;74(2):236-9. 12. Corteville JE, Gray DL, Crane JP. Congenital hydronephrosis: correlation of fetal ultrasonographic findings with infant outcome. Am J Obstet Gynecol 1991;165(2):384-8. 13. Jaswon MS, Dibble L, Puri S, Davis J, Young J, Dave R, et al. Prospective study of outcome in antenatally diagnosed renal pelvis dilatation. Arch Dis Child Fetal Neonatal Ed 1999;80(2):F135-8. 14. Wilson RD, Lynch S, Lessoway VA. Fetal pyelectasis: comparison of postnatal renal pathology with unilateral and bilateral pyelectasis. Prenat Diagn 1997;17(5):451-5. 15. Adra AM, Mejides AA, Dennaoui MS, Beydoun SN. Fetal pyelectasis: is it always "physiologic"? Am J Obstet Gynecol 1995;173(4):1263-6. 16. Chertin B, Puri P. Familial vesicoureteral reflux. J Urol 2003;169(5):1804-8. 17. Degani S, Leibovitz Z, Shapiro I, Gonen R, Ohel G. Fetal pyelectasis in consecutive pregnancies: a possible genetic predisposition. Ultrasound Obstet Gynecol 1997;10(1):19-21. 18. Hollowell JG, Greenfield SP. Screening siblings for vesicoureteral reflux. J Urol 2002;168(5):2138-41.

Mild pyelectasis 103 19. Scott JE, Swallow V, Coulthard MG, Lambert HJ, Lee RE. Screening of newborn babies for familial ureteric reflux. Lancet 1997;350(9075):396-400. 20. Allen KS, Arger PH, Mennuti M, Coleman BG, Mintz MC, Fishman M. Effects of maternal hydration on fetal renal pyelectasis. Radiology 1987;163(3):807-9. 21. Babcook CJ, Silvera M, Drake C, Levine D. Effect of maternal hydration on mild fetal pyelectasis. J Ultrasound Med 1998;17(9):539-44; quiz 545-6. 22. Robinson JN, Tice K, Kolm P, Abuhamad AZ. Effect of maternal hydration on fetal renal pyelectasis. Obstet Gynecol 1998;92(1):137-41. 23. Gool van JD, Hjalmas K, Tamminen-Mobius T, Olbing H. Historical clues to the complex of dysfunctional voiding, urinary tract infection and vesicoureteral reflux. The International Reflux Study in Children. J Urol 1992;148(5 Pt 2):1699-702. 24. SPSS Inc. Chicago. 2004. 25. Hellstrom AL, Hanson E, Hansson S, Hjalmas K, Jodal U. Micturition habits and incontinence in 7-year-old Swedish school entrants. Eur J Pediatr 1990;149(6):434-7. 26. Jones MA, Breckman B, Hendry WF. Life with an ileal conduit: results of questionnaire surveys of patients and urological surgeons. Br J Urol 1980;52(1):21-5. 27. Dudley JA, Haworth JM, McGraw ME, Frank JD, Tizard EJ. Clinical relevance and implications of antenatal hydronephrosis. Arch Dis Child Fetal Neonatal Ed 1997;76(1):F31-4. 28. Feldman DM, DeCambre M, Kong E, Borgida A, Jamil M, McKenna P, et al. Evaluation and follow-up of fetal hydronephrosis. J Ultrasound Med 2001;20(10):1065-9. 29. Harding LJ, Malone PSJ, Wellesley DG. Antenatal minimal hydronephrosis: is its follow-up an unnecessary cause of concern? Prenat Diagn 1999(19):701-705. 30. Mandell J, Blyth BR, Peters CA, Retik AB, Estroff JA, Benacerraf BR. Structural genitourinary defects detected in utero. Radiology 1991;178(1):193-6. 31. Morin L, Cendron M, Crombleholme TM, Garmel SH, Klauber GT, D'Alton ME. Minimal hydronephrosis in the fetus: clinical significance and implications for management. J Urol 1996;155(6):2047-9. 32. Thomas DF. Prenatal diagnosis: does it alter outcome? Prenat Diagn 2001;21(11):1004-11. 33. Dhillon HK. Prenatally diagnosed hydronephrosis: the Great Ormond Street experience. British Journal of Urology 1998(81,Suppl.2):39-44. 34. Harding LJ, Malone PS, Wellesley DG. Antenatal minimal hydronephrosis: is its follow-up an unnecessary cause of concern? Prenat Diagn 1999;19(8):701-5. 35. Wolfhagen MJ, Weezenlanden HM. Incidentie en sterfte naar leeftijd en geslacht in: Volksgezondheid. Toekomst Verkenning, Nationaal Kompas Volksgezondheid, Bilthoven, RIVM, Gezondheidstoestand/ Ziekten en aandoeningen/ Urinewegen en de geslachtsorganen/ acute urineweginfecties, 2001(24 sept.2001). 36. de Kort LM, Verhulst JA, Engelbert RH, Uiterwaal CS, de Jong TP. Lower urinary tract dysfunction in children with generalized hypermobility of joints. J Urol 2003;170(5):1971-4. 37. Jadresic L, Cartwright K, Cowie N, Witcombe B, Stevens D. Investigation of urinary tract infection in childhood. Bmj 1993;307(6907):761-4.

104 Chapter 7
38. van der Voort J, Edwards A, Roberts R, Verrier Jones K. The struggle to diagnose UTI in children under two in primary care. Fam Pract 1997;14(1):44-8. 39. Van Der Voort JH, Edwards AG, Roberts R, Newcombe RG, Jones KV. Unexplained extra visits to general practitioners before the diagnosis of first urinary tract infection: a case-control study. Arch Dis Child 2002;87(6):530-2. 40. Shaw KN, Gorelick M, McGowan KL, Yakscoe NM, Schwartz JS. Prevalence of urinary tract infection in febrile young children in the emergency department. Pediatrics 1998;102(2):e16.

Chapter 8 Variability in dilatation of the fetal renal pelvis during a bladder filling cycle H.A.M. Damen - Eliasa, R.H. Stigterb, T. P.V.M. de Jong c, G.H.A. Vissera. a Department of Perinatology and Gynaecology, University Hospital Utrecht, The Netherlands b Department of Obstetrics and Gynaecology, Deventer Hospital, Deventer, The Netherlands c Department of Paediatric Urology, University Hospital Utrecht, The Netherlands

106 Chapter 8
ABSTRACT
Objective To investigate the variation of the dimensions of the fetal renal pelvis in
relation to the degree of bladder filling in fetuses with mild pyelectasis.
Methods Eighteen third trimester pregnant women with mild uni- or bilateral fetal
pyelectasis, defined as an anteroposterior diameter of the renal pelvis between 5-10
mm, were recruited for the study. The women were examined for 2 – 3 hours by
ultrasound. The anteroposterior and transverse dilatation of the renal pelvis and the
bladder dimensions (to calculate fetal bladder volume) were measured at 2 to 3
minutes intervals.
Results In 6 of the 18 fetuses a consistent relationship between size of the renal
pelvis and bladder filling was found, with a mean difference in renal pelvis diameter
between before and after voiding of 6,7mm and a largest observed difference of
14,3mm. In the other two third of infants no such relationship was found. Postnatally
all children had an ultrasonography and 5 infants were referred to the paediatric
urologist. The investigations in these 5 children could not confirm the hypothesis that
variation in renal pelvis size in relation to bladder size may predict prenatal
vesicoureteral reflux.
Conclusions In case of mild pyelectasis, the size of the renal pelvis is highly variable
in one third of cases. The association with bladder volume and micturition suggests
evidence of vesicoureteral reflux, but this could not be proven. If cut-off values are
used to differentiate between normal and abnormal renal pelvis size than not only
gestational age but also the degree of bladder filling at the time of measurement
should be taken in account. Caution should be expressed when the diagnosis of a
possible urological anomaly is based on one single measurement during only one
investigation.

Variability in dilatation of the fetal renal pelvis 107
INTRODUCTION
A mild uni- or bilateral fetal pyelectasis is a frequent finding with a considerable
variation in the reported incidence of 0,6-5,5%1-4 due to different criteria being used to
define pyelectasis, in particular regarding size and gestational age at diagnosis.
Evidence exists that the antenatal detection of pyelectasis can predict postnatal
complications such as obstructive uropathy or vesico ureteral reflux (VUR) and is
related to an increased risk of aneuploidy (1.6 tot 3.9%)5-8. During routine
examinations we have often noted that the size of the renal pelvis varies considerably
over time. This variation may be relevant, since a diagnosis of abnormal dilatation of
the urinary system is usually based on fixed cut-off values. So far two studies had
addressed the relationship between dimensions of the renal pelvis in relation to the
degree of bladder filling9,10. In one study such a relationship was found and in the
other one not.
It was the aim of the present study to investigate systematically the variation in the
dimensions of the fetal renal pelvis in relation to the degree of bladder filling in fetuses
with a mild pyelectasis.

108 Chapter 8
METHODS
Eighteen women participated in the study. Measuring crown-rump length by
ultrasound validated gestational age. None of the women used any medication and
all had an uncomplicated, singleton pregnancy. No congenital anomaly was present
except a uni- or bilateral pyelectasis at the 18 - 20 week anomaly scan. Pyelectasis
was defined as an anteroposterior diameter (A-P diameter) of the fetal renal pelvis of
5-10 mm. All women were rescanned at approximately 32 weeks gestational age and
were included in the study, only, when the A-P diameter of the renal pelvis did not
exceed 10mm. (In the institution this is the cut-off point where the child was referred
for urological follow-up during the first weeks of life.) The parents were advised to
refrain from further investigations before or after birth and were told that their child
might have an increased risk for urinary tract infection (UTI) due to VUR and that, in
case of feeling listless or fever of unknown origin, UTI should be ruled out. This
advice is in accordance with the policy in our institution.
All investigations were done between 36 and 38 weeks gestational age since it has
been shown that fetuses at that age have prolonged cycles of bladder filling/
emptying, related to fetal behavioural states11,12. All examinations were carried out
between 8 and 12 a.m. after a normal breakfast. Maternal fluid intake was not
specified because it is questionable whether maternal hydration influences fetal
pyelectasy13-15.
Every scan was made by one midwife-ultrasonographer (HDE), using the abdominal
multifrequency transducer PVM 375 AT of the Toshiba Power Vision 6000, type SSA
370, Toshiba Medical Systems Europe, Zoetermeer, The Netherlands. As part of
another study the same investigator carried out an intra-observer study before the
data of this study were collected (Article in preparation). After obtaining informed
consent, measurements of the renal pelvis and the bladder were taken during a 2 to
3 hour period with 2 to 3 minutes intervals. After identification of the fetal spine or the
aorta and perpendicular on this plane with both kidneys in the largest sectional
plane, the diameters of the renal pelvis were obtained by placing the callipers on the
inner borders of the renal pelvis. In every fetus the right and left renal pelvis was
measured in A-P and transverse diameter. The area of the bladder was measured,

Variability in dilatation of the fetal renal pelvis 109
by hand tracing, in a longitudinal plane with the largest outline to calculate the
volume of the bladder as previously described by Stigter et al16.
Data from all measurements were plotted in a graph separately for every bladder
filling cycle. The A-P and transverse diameter of the right and left renal pelvis and the
perimeter derived from these measurements (mathematical formula for an ellipse =
(.(½a+½b), where a = the long axis and b= the short axis), together with the
calculated bladder volumes were all marked against time and standardized according
to the moment of fetal voiding. All graphs were printed and visually judged by a
gynaecologist who did not participate in the study, to assess if there was relationship
between the various measurements obtained from the renal pelvis and the degree of
bladder filling, especially around the moment of bladder emptying. Statistical
analyses were performed using Statistical Product and Service Solutions version
10.1 (SPSSR).
Postnatally, all children were investigated by ultrasound within 3 or 4 months after
birth by the same investigator (HDE). Parents were asked to take care of a large fluid
intake by their child so that the examination could be done both before and after
voiding comparatively the same investigation as the investigations at approximately
37 weeks gestational age.

Table 1 - O
verview of all antenatal m
easu
rements and postnatal findings of the 18 children.
*Measu
red at 20 and 32 w
eeks
and postnatally ۲
numbers corresp
ond to the anteroposterior diameter of the renal p
elvis befio
re and after vo
iding
Patie
nt
number
and sex
Dilatation Dilatatio
nright kidney* le
ft kidney*
±20 ±32 pn ±20 ±32 pn
No. of
fillin
gcy
cles
No. of
measu
-rements
Right renal
pelvis positiv
eco
rrelatio
n
Left renal
pelvis positiv
eco
rrelatio
n
Postnatally ultraso
nographic in
vestigatio
n۲
1 ♂
7
8
0
6
10
7
139
Right 8>6 m
m, left 7>6 m
m referred beca
use
of restless
ness
crying,
VUR L=gr I R=gr II = 1 year antib
iotic
prophylaxis
2 ♂
7
9
0
7
10
8
269
+ both cyc
les
+ both cyc
les
Right 10>6 m
m and le
ft 20>8 m
m U
rine conce
ntratio
n problem ju
st like
his older brother and m
other
3 ♂
6
9
0
6
6
0
259
+ both cyc
les
+ both cyc
les
No dilatatio
n of renal p
elves, nl b
ladder wall
4 ♂
10
10
5
0
7
0
136
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
5 ♀
0
10
0
7
8
5
256
No dilatatio
n of renal p
elves, nl b
ladder wall
6 ♀
7
10
5
8
9
7
245
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
7 ♂
6
9
8
6
7
3
367
Right 8>4 m
m, left no dilatatio
n of renal p
elvis, residue after vo
iding,
renogram: high press
ure voiding, incision urethral v
alve
8 ♂
8
7
0
6
7
8
480
Right < 5 m
m dilatatio
n, left 10>8 m
m, nl b
ladder wall
9 ♂
8
7
1
6
5
8
254
+ both cyc
les
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
10 ♂
6
9
4
8
6
4
248
No dilatatio
n of renal p
elves, nl b
ladder wall
11 ♂
8
7
3
7
9
0
358
Right 3>9 m
m, left no dilatatio
n, nl b
ladder wall
12 ♀
7
8
3
10
7
2
353
+ three cyc
les
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
13 ♂
6
5
1
0
7
2
134
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
14 ♂
7
8
2
10
6
2
350
+ three cyc
les
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
15 ♂
0
5
3
8
7
2
242
No dilatatio
n of renal p
elves, nl b
ladder wall
16 ♂
0
0
5
8
8
5
258
Right < 5 m
m dilatatio
n, left 22>18 m
m, no high press
ure, under co
ntrol
17 ♂
8
6
5
7
7
3
232
< 5 m
m dilatatio
n of the renal p
elves, nl b
ladder wall
18 ♂
6
7
17
8
10
29
365
+ three cyc
les
Right 16>15 m
m, left 29>28 m
m w
ith dilated calices, residue after
voiding, no VUR, nl renogram, rese
ction urethral v
alve
Total =
3 girls
15 boys
40
945
7 cycles =
3 kidneys
12 cyc
les =
5 kidneys

Variability in dilatation of the fetal renal pelvis 111
RESULTS
In the 18 patients 40 bladder filling/emptying cycles (range 1 – 4) could be evaluated.
In 4 patients it was not possible to record more than one filling cycle because of a
maternal supine hypotension syndrome. All measurements were obtained from all 18
fetuses with a total of 945 measurements of the right as well as of the left kidney
(Table 1). The mean interval between first and last measurement in one cycle was 33
minutes (range 11 - 64) with an average of 17 renal pelves and bladder volume
measurements per cycle (range 7 - 33).
Assessed visually, in 6 of the 18 fetuses (33,3%) there were concomitant volume
changes of the renal pelvis in association with those of the bladder (data: Table 2).
Twice this concerned both kidneys (Number 2 and 3, Table 1) and in four fetuses one
kidney (Number 9, 12, 14, 18, Table 1). In these fetuses these associations occurred
during all the observed bladder cycles and this concerned for the A-P diameter, for
the transverse diameter and for the perimeter of the renal pelvis as well, each
separately, by comparison with the bladder volume.
Figure 1 (a) gives an example of such a correlation between fetal renal pelvis
dimensions and bladder volumes and figure 1 (b) shows the same measurements in
a fetus in whom no such correlations were present.
(a) (b)
0
5
10
15
20
25
-12 -8 -4 0 -4 -8 -12
time
mm
/ cm
/ cm
3 .
pyelum L anteroposterior w idth L pyelumperimeter L pyelum volume bladder
0
5
10
15
20
25
-12 -8 -4 0 4 8 12time
mm
/ cm
/ cm
3 .
pyelum R anteroposterior w idth R pyelumperimeter re pyelum volume bladder
Figure 1 a = Example of a case in which there is a concomitant variation in renal pelvis size and fetal bladder filling/ emptying. Figure 1 b = Example in which no such association was found. The x-axis is the time in minutes to the time of fetal micturition (point 0). The y-axis shows the size of the anterior/ posterior pelvis diameter and of the width of the pelvis, in millimetres. As to the perimeter of the pelvis in cm and bladder volume in cubic mm, respectively.

112 Chapter 8
Figure 2 (a) shows the measurements of decreasing and increasing size of renal
pelves, in relation to bladder filling and micturition (figure 2 b) of the 19 cycles in the 6
children in whom changes in renal pelvis dilatation were related to the bladder
filling/emptying cycle. It concerned 7 times the right kidney and 12 times the left
kidney (Table 1) in 6 fetuses.
(a) (b)
0
5
10
15
20
25
-10 -8 -6 -4 -2 0 2 4 6 8 10time
mill
imet
res
pyelum
0
5
10
15
20
25
-10 -8 -6 -4 -2 0 2 4 6 8 10
time
cent
imet
res3
volume bladdervolume bladder
Figure 2 a = Diameter of the pelvis in relation to the time of fetal micturition (0 minutes; 19 observations) Figure 2 b = The corresponding lines of bladder volume in these cases.
The x-axis is the time in minutes to the time of fetal micturition (point 0). The y-axis shows the size of the anterior/ posterior pelvis diameter and of the width of the pelvis, in millimetres. As to the perimeter of the pelvis in cm and bladder volume in cubic mm, respectively.
The mean difference between renal pelvis diameter 4 minutes before voiding and
directly after voiding was 6,7 millimetre, range 2,9 to 14,3. In five of these cases the
diameter was more than 15 mm before voiding, 16,8/ 18,1/ 18,0/ 18,9/ 19,8 mm,
respectively and 9,1/ 3,8/ 10,6/ 8,9 and 10,8 mm, respectively, thereafter. The
maximal renal pelvis diameter 4 minutes before voiding was related to the maximal
bladder volume (r=0,95) and the minimal renal pelvis diameter after voiding was
related to the minimal bladder volume (r=0,91).
Postnatally all children had an ultrasound scan at the age of approximately 3 or 4
months to measure renal pelvis size once again before and after voiding (Table 1).
None of the children were reported to have had urinary tract problems and all were
clinically well. Only one child had visited a paediatrician because of excessive crying
and restlessness at night but no conclusive diagnosis had been made.

Variability in dilatation of the fetal renal pelvis 113
Five of the eighteen investigated infants (27,7%) were referred to the paediatric
urologist because of dilated renal pelves and/or hydronephrosis (n=3), residual
bladder volume after voiding (n=1) or restlessness and excessive crying (n=1).
Table 1.
Antenatally, two of these children (No. 2 and 18) had shown a clear correlation
between the dilatation of the renal pelvis and bladder volume during a filling cycle in
contrast to the three others (No 1, 7 and 16). The referred children were:
- No. 1, a boy, referred because of restlessness and crying at night, to exclude an
underlying renal cause. A voiding cystourethrography (VCUG) showed grade I VUR
on the left and grade II on the right side. The child was put on antibiotic prophylaxis
for one year.
- No. 2, a boy, referred because of visible reduction of the dilated renal pelves
(before and after voiding, left 20 mm>5mm, right 10>6mm) and excessive drinking.
The child drank 2 litres per day and even 500 ml by night. Further information from
the mother, led to the diagnosis of a renal concentration disorder that also affected
her other son and also herself. No VUR was demonstrable during VCUG in this
infant.
- No. 7, a boy referred because of residual urine after voiding. An urodynamic study
notified suspicion on a urethral obstruction and high pressure at voiding. No VUR
was noted at VCUG. Posterior urethral valves were resected during a subsequent
cystoscopy.
- No. 16, a boy referred because of a unilateral hydronephrosis with a renal pelvis of
>20mm and dilated calices. An ultrasound showed a kidney with a plump collecting
system and no evidence for high pressure. The child will be followed up at 3 months
intervals.
- No. 18, a boy referred with bilateral hydronephrosis (right 17 and left 30 mm) with
dilated calices. A renogram showed normal function and no important obstruction. A
VCUG showed no VUR but a megabladder with significant residual urine after
voiding and a suspicion for obstruction of the bladder neck. At cystoscopy no
obstruction was found and the child will be followed up at 3 months intervals.

Table 2 – The distributio
n of measu
rements, 10 m
inutes before till 10 m
inutes after vo
iding, of the fetuse
s with
a correlatio
n between the pelvis of the
right and/ or left kidney and bladder vo
lume plotted against the tim
e in
minutes.
patië
nt
/ cycle
time
min.
renal p
elvis
dilatatio
n right left
bladder
volume
patië
nt
/ cycle
time
min.
renal p
elvis
dilatatio
n right le
ft
bladder
volume
patië
nt
/ cycle
time
min.
renal p
elvis
dilatatio
n right left
bladder
volume
patië
nt
/ cycle
time
min.
renal p
elvis
dilatatio
n right left
bladder
volume
2 / 1
-10
9,9
12,2
10,65
9 / 1
-10
8,7
25,07
12 / 3
-10
15,9
17,32
18 / 1
-10
16,8
12,46
- 8
10,3
12,1
10,22
- 8
9,1
26,06
- 8
16,3
15,35
- 8
17,1
13,07
- 6
10,1
11,3
9,34
- 6
9,9
26,18
- 6
15,6
13,76
- 6
17,4
13,13
- 4
9,3
11,8
7,32
- 4
10,2
28,02
- 4
17,9
12,35
- 4
18
13,88
- 2
8,8
12,2
7,01
- 2
10,6
16,34
- 2
16,8
11,89
- 2
17,5
14,12
0
5,7
7,7
1,61
0
3,4
5,74
0
9,1
2,35
0
10,6
6,31
2
6,4
7,7
2,57
2
6,9
8,18
2
10,2
3,51
2
11,1
7,17
4
6,8
9,5
3,34
4
7,4
10,45
4
11,1
5,55
4
12
7,81
6
6,7
9,2
4,51
6
8,8
10,70
6
13,6
6,41
6
13,1
8,13
8
8,2
9,7
6,17
8
10,2
14,62
8
14,2
9,22
8
14,2
8,98
10
8,9
10,0
6,85
10
11,1
14,99
10
15,1
10,86
10
16,8
9,81
2 / 2
-10
9,5
10,5
9,04
9 / 2
-10
8,8
14,62
14 / 1
-10
8,7
9,91
18 / 2
-10
19
12,11
- 8
9,4
11,3
9,13
- 8
10,2
14,99
- 8
7,8
10,94
- 8
18,9
12,92
- 6
10,4
11,4
9,54
- 6
11,1
15,97
- 6
9,1
11,34
- 6
17,9
13,39
- 4
10,2
10,6
10,69
- 4
11,4
18,31
- 4
10,6
12,22
- 4
19,3
13,51
- 2
10,5
10,6
11,02
- 2
12,6
17,69
- 2
10,3
12,32
- 2
18,9
14,12
0
7,6
5,8
2,01
0
6,2
2,51
0
6,4
2,56
0
8,9
2,09
2
8,2
6,4
3,42
2
7,4
3,46
2
7,1
3,79
2
9,8
2,75
4
8,9
7,6
4,10
4
8,8
4,15
4
7,8
4,05
4
11,8
3,16
6
8,7
8,1
5,00
6
9,2
4,65
6
8,7
6,09
6
12,4
3,79
8
9,9
8,6
5,38
8
9,4
4,92
8
9,4
7,08
8
13,1
5,32
10
9,6
10,1
5,92
10
9,8
5,71
10
9,6
7,70
10
16,2
5,29
3 / 1
-10
7,5
9,5
10,10
12 / 1
-10
13,9
13,48
14 / 2
-10
12,9
10,19
18 / 3
-10
18,6
14,12
- 8
7,8
10,7
10,36
- 8
13
11,13
- 8
13,8
11,14
- 8
20,1
13,39
- 6
8,3
11
10,24
- 6
14,3
9,48
- 6
14,6
17,81
- 6
19,8
13,51
- 4
9,4
11,6
11,52
- 4
15
7,13
- 4
16,8
20,40
- 4
17,3
14,37
- 2
9,4
11,5
7,72
- 2
10,6
6,74
- 2
18,1
21,14
- 2
19,8
14,37
0
5,7
8,1
1,80
0
7,4
4,42
0
3,8
2,80
0
10,8
4,47
2
6,4
8,8
2,82
2
8,9
6,12
2
4,5
3,60
2
11,6
6,31
4
6,9
93,08
4
12,2
7,49
4
6,2
4,17
4
12,6
7,19
6
7,7
9,6
4,32
6
14,6
8,93
6
6,9
4,43
6
13,3
8,29
8
7,9
9,5
4,51
8
15,3
10,21
8
7,1
5,18
8
15,4
8,90
10
89,9
6,39
10
15,6
12,34
10
7,2
6,79
10
14,9
10,99
3 / 2
-10
8,7
10,8
9,22
12 / 2
-10
14,6
12,54
14 / 3
-10
8,3
7,17
- 8
7,8
10,9
9,91
- 8
15,3
12,14
- 8
8,9
7,97
- 6
9,1
11
10,94
- 6
15,6
10,21
- 6
9,1
9,45
- 4
10,6
11,2
12,32
- 4
16
8,93
- 4
9,9
10,70
- 2
10,3
11,8
12,22
- 2
12,7
7,49
- 2
9,9
11,85
0
6,4
7,9
2,56
0
4,6
2,29
0
5,6
4,19
2
7,1
8,6
3,79
2
6,7
2,49
2
75,98
4
7,8
9,5
4,05
4
7,5
3,66
4
9,7
10,13
6
8,7
10,2
6,09
6
11,4
5,34
6
10,4
13,76
8
9,4
10,8
7,08
8
12
5,74
8
10,9
14,74
10
9,6
11,4
7,70
10
13,3
6,95
10
13,8
16,58

Variability in dilatation of the fetal renal pelvis 115
DISCUSSION
This study shows that in approximately one-third of term fetuses with a mild
pyelectasis the diameter of the renal pelvis varies according to bladder volume, with
a mean difference in renal pelvis diameter before and after voiding of 6,7 mm and a
largest observed difference of 14,3 mm. So the volume of the bladder should be
considered when fetal hydronephrosis is suspected. In the other two-third of fetuses
with a mild pyelectasis no changes in dilatation of the renal pelvis in relationship to
voiding were observed.
Petrikosky et al10 studied the overall relationship between renal pelvis diameter and
bladder volume in 43 fetuses with hydronephrosis between 18 and 24 weeks
gestational age. No criteria of the definition of hydronephrosis were given. The
anterior posterior diameter of the fetal renal pelvis diminished from 6,8 to 4,5 mm
when the bladder was emptied and the size of the fetal renal pelvis was correlated to
the bladder area (r=0,55). They only studied the overall effect in the total group and
did not distinguish between fetuses in which a relationship with bladder volume was
present or not. This explains the low correlation coefficient between pelvic size and
bladder volume as compared to our data but they also concluded that the volume of
the bladder should be considered when fetal hydronephrosis is diagnosed.
In contrast, Persutte et al9 found no relationship between bladder size and
pyelectasis (A-P diameter >4 mm and <10mm), but they took their measurements
every 15 minutes and therefore may have missed the changes in diameter, which
occur specifically around fetal micturition. However, they did find a highly variable
size of the fetal renal collecting system.
These studies are not quite comparable with ours because of the differences in
intervals of the measurements and the use of the data of all the fetuses for the
calculations instead of a selected part of the total group were the diameter of the
renal pelvis varies according to bladder volume, as we did.
One of the reasons of the variations in dilatation has been suggested to be an
association between maternal hydration and fetal renal pyelectasis14,15 although
another study has claimed the opposite13. Another possible reason for the
association between renal pelvis size and bladder filling, might be the presence of

116 Chapter 8
VUR, a renal tract anomaly that can be diagnosed antenatally only by the invasive
procedure of adding cystourethrography to a diagnostic puncture of the fetal
bladder17.
Pyelectasis, hydronephrosis or a dilated ureter suggests the need for postnatal
investigations to rule out VUR. However, thus far no correlation has been found
between antenatal and postnatal dilatation and the severity of VUR18. Even postnatal
ultrasound is falsely negative in 18 to 30% of the infants with VUR19-21 and until now
the golden standard for the diagnosis of VUR is a VCUG.
We had not the possibility to offer all 18 children a VCUG and so we could not
confirm the hypothesis that cyclic variation in bladder and renal pelvis size are
diagnostic regarding VUR.
After the postnatal ultrasound investigation only 5 children in our study group showed
abnormal dilatation of the renal pelvis and had subsequent investigations. Two of
these children (No 2 and 18; Table1) showed a correlation between the size of the
renal pelvis dilatation and the bladder volume but a VCUG did not confirm the
diagnosis of VUR. In another fetus (No 1) no correlation between bladder and renal
pelvis fluctuations had been found and nevertheless the child appeared to have
bilateral VUR.
We suggest another study in a greater cohort of third trimester pregnant woman with
measurements of the fetal renal pelves every 2 or 3 minutes from 15 minutes before
till 15 minutes after fetal voiding occurs and, if concomitant changes in size of the
renal pelvis in relation to that of the fetal bladder volume occur a postnatal VCUG.

Variability in dilatation of the fetal renal pelvis 117
REFERENCES 1. Kent A, Cox D, Downey P and James SL: A study of mild fetal pyelectasis - outcome andproposed strategy of management. Prenat Diagn. 20: 206-9, 2000. 2. Langer B, Simeoni U, Montoya Y, Casanova R and Schlaeder G: Antenatal diagnosis of upper urinary tract dilation by ultrasonography. Fetal Diagn Ther. 11: 191-8, 1996. 3. Persutte WH, Koyle M, Lenke RR, Klas J, Ryan C and Hobbins JC: Mild pyelectasis ascertained with prenatal ultrasonography is pediatrically significant. Ultrasound Obstet Gynecol. 10: 12-8, 1997. 4. Scott JE and Renwick M: Antenatal renal pelvic measurements: what do they mean? BJU Int . 87: 376-80, 2001. 5. Aviram R, Pomeranz A, Sharony R, Beyth Y, Rathaus V, Tepper R and Pomeran A: The increase of renal pelvis dilatation in the fetus and its significance. Ultrasound Obstet Gynecol. 16: 60-2, 2000. 6. Chudleigh PM, Chitty LS, Pembrey M and Campbell S: The association of aneuploidy and mild fetal pyelectasis in an unselected population: the results of a multicenter study. Ultrasound Obstet Gynecol. 17: 197-202, 2001. 7. Corteville JE, Dicke JM and Crane JP: Fetal pyelectasis and Down syndrome: is genetic amniocentesis warranted? Obstet Gynecol. 79: 770-2, 1992. 8. Nicolaides KH, Cheng HH, Abbas A, Snijders RJ and Gosden C: Fetal renal defects: associated malformations and chromosomal defects. Fetal Diagn Ther. 7: 1-11, 1992. 9. Persutte WH, Hussey M, Chyu J and Hobbins JC: Striking findings concerning the variability in the measurement of the fetal renal collecting system. Ultrasound Obstet Gynecol. 15: 186-90, 2000. 10. Petrikovsky BM, Cuomo MI, Schneider EP, Wyse LJ, Cohen HL and Lesser M: Isolated fetal hydronephrosis: beware the effect of bladder filling. Prenat Diagn. 15: 827-9, 1995. 11. Visser GH, Goodman JD, Levine DH and Dawes GS: Micturition and the heart period cycle in the human fetus. Br J Obstet Gynaecol. 88: 803-5, 1981. 12. Stigter RH, Mulder EJ and Visser GH: Hourly fetal urine production rate in the near-term fetusis it really increased during fetal quiet sleep? Early Hum Dev. 50: 263-72, 1998 . 13. Allen KS, Arger PH, Mennuti M, Coleman BG, Mintz MC and Fishman M: Effects of maternal hydration on fetal renal pyelectasis. Radiology. 163: 807-9, 1987. 14. Babcook CJ, Silvera M, Drake C and Levine D: Effect of maternal hydration on mild fetal pyelectasis. J Ultrasound Med. 17: 539-44; quiz 545-6, 1998. 15. Robinson JN, Tice K, Kolm P and Abuhamad AZ: Effect of maternal hydration on fetal renal pyelectasis. Obstet Gynecol. 92: 137-41, 1998. 16. Stigter RH, Schelven van LJ, Bruinse HW, Mulder EJH, Gemert van MJC. On the measurement of fetal bladder volume and urine production: methodological consideration. Prenat Neonat Med 2000; 5: 169-76. 17. Stoutenbeek P, de Jong TP, van Gool JD and Drogtrop AP: Intra-uterine cystography for evaluation of prenatal obstructive uropathy. Pediatr Radiol. 19: 247-9, 1989. 18. Jaswon MS, Dibble L, Puri S, Davis J, Young J, Dave R and Morgan H: Prospective study of outcome in antenatally diagnosed renal pelvis dilatation. Arch Dis Child Fetal Neonatal Ed. 80: F135-8, 1999. 19. Najmaldin A, Burge DM and Atwell JD: Fetal vesicoureteric reflux. Br J Urol. 65: 403-6, 1990

118 Chapter 8
20. Tibballs JM and De Bruyn R: Primary vesicoureteric reflux--how useful is postnatal ultrasound? Arch Dis Child. 75: 444-7, 1996. 21. Zerin JM, Ritchey ML and Chang AC: Incidental vesicoureteral reflux in neonates with antenatally detected hydronephrosis and other renal abnormalities. Radiology. 187: 157-60, 1993.

Chapter 9 Summary and discussion Nederlandse samenvatting Dankwoord Curriculum Vitae

120 Chapter 9
SUMMARY, DISCUSSION AND CONCLUSION
introduction
In two to three percent of fetuses structural anomalies can be found with prenatal
ultrasound investigation1-4. Anomalies of the urinary tract account for 15 to 20% of
these anomalies with a detection rate of approximately of 90%3, 4. During the latest
decades numerous papers have been published on the fetal renal system and its
anomalies. However, follow-up studies on long-term outcome are still scarce and this
hampers adequate counselling of parents and of giving adequate treatment advises.
Moreover, up-to-date charts on normal fetal kidney and adrenal gland development
are scarce. We therefore formulated the following aims of this thesis (Chapter 1):
1 – To develop charts of size and growth of the fetal kidney, renal pelvis and adrenal
gland.
2 – To study long-term follow-up of a large cohort of infants with a prenatally
diagnosed renal tract anomaly.
3 – To answer the question whether mild pyelectasis (anteroposterior diameter of the
fetal renal pelvis of 5 – 10 mm) as diagnosed around 18 to 20 weeks of gestation
results in increased morbidity in childhood and therefore requires postnatal
treatment.
4 – To study the relationship between the size of the renal pelvis and the fetal
bladder-filling cycle, to answer the question if fixed cut-off values regarding renal
pelvis dilatation can be used or whether bladder filling has to be taken into account.
charts for size and growth of kidney, renal pelvis and adrenal gland
A reference curve for size and growth of fetal kidney, renal pelvis and adrenal gland
is of importance to judge the growth of these organs during pregnancy, especially
when during an ultrasound investigation an anomaly is suspected. Several charts of
fetal kidney sizes have been published, but mostly with shortcomings in data
collection or with methodological weaknesses i.e. not validating gestational age5-9,
not covering the whole of the second and third trimester of pregnancy5, 6, 10-12, not
measuring the kidney in three dimensions5, 6, 8-10 or using data from infants born
preterm or from post-mortem specimens13-15. Moreover several studies averaged
both cross-sectional and longitudinal data5, 7-10, 12, 15. In none of these publications an
intraobserver and interobserver variation analysis had preceded the study.

Summary, discussion and conclusion 121
We performed an intraobserver and interobserver variation analysis for the
measurements of length, anteroposterior diameter and transverse diameter of the
kidney and for length of the adrenal gland (Chapter 2). Data regarding an
intraobserver variation were obtained from 30 fetuses and by comparing three
measurements with different time intervals between each measurement. Statistical
analysis showed that there was a high intraobserver agreement with Cronbach’s
alpha (α) above 0.9 and the intra class correlation (IC) above 0.8. Interobeserver
agreement was studied in 20 fetuses by two experienced ultrasonographers. Also
these data were satisfactory (α above 0.9, IC above 0.8). All measurements could be
taken in each fetus both in the intra- and interobserver study.
In a prospective longitudinal study in 111 low risk fetuses we measured length,
anteroposterior diameter and transverse diameter of both kidneys, anteroposterior
and transverse diameter of both renal pelves and the length of both adrenal glands
(Chapter 3 and 4). Data were obtained every 4 weeks from 16 weeks onwards.
Data obtained in a longitudinal study by measurements of a considerable cohort of
fetuses on a series of occasions may be used for a reference curve for size and
growth. Cross-sectional data obtained by measurements of each fetus on a single
occasion give only information on size21-24.
Statistical analysis was performed by multilevel analysis a recently developed new
technique that can be used when some data are missing and when measurements
have been made at variable times16. It allows for the dependency in hierarchically
structured data in contrast to multiple regression analysis that presupposes the
independency of observations. Repeated measurements in the same individual with
investigations at different gestational ages belong to a low level. Computed means of
an individual measurement (e.g. kidney length) belong to a higher level.
There was hardly any difference between the curves of the right and left kidney, the
right and left renal pelvis and the right and left adrenal gland. Definitive charts were
made after averaging the data from both sides.
It was difficult to compare our charts with those of others because several studies did
not cover the whole second and third trimester of pregnancy or gave no raw data or
when they did so they gave evidence of methodological weakness. We compared our

122 Chapter 9
charts with those of Chitty and Altman7, 17 and of Pruggmayer and Terinde7. Both
studies used cross-sectional data and measured every fetus only once. Chitty et al
measured every week approximately 15 to 20 fetuses while Pruggmayer et al gave
no data on numbers/ week and excluded nearly 20% of infants because they were
either large or small for dates. Our charts differ from theirs in having smaller ranges.
This may be due to the fact that we did each measurement three times whereafter
we averaged the data.
A strong linear correlation was found between adrenal gland length and kidney length
with a ratio 2 to 7 and this relation did not change with gestation/ kidney size.
Comparing our chart of the length of the adrenal gland with others was not possible
because another measure of the adrenal was measured18 or data were published
only for every 5 weeks19 or were compared with biparietal diameter and kidney length
and not with weeks of gestation20.
structural anomalies of the fetal renal tract
The prevalence of any congenital anomaly that can be detected by ultrasound during
pregnancy is approximately 1 to 2% 1-4. Urinary tract abnormalities account for 15 to
20% of these anomalies with a detection rate of approximately 90%3, 4. Data on
antenatal diagnosis and postnatal follow-up are important for assessing prognosis of
the individual fetus with a diagnosed anomaly and for subsequent counselling of the
parents. Such data may also be helpful in making difficult decisions as to whether or
not to terminate a pregnancy before viability and in determining the need for further
diagnostic procedures and best management before and after birth.
In Chapter 5 we describe the ultrasound findings and outcome of a large cohort of
402 fetuses with a prenatally diagnosed urinary tract anomaly. We could use the
database of the ultrasound unit of the department of obstetrics of the University
Medical Centre, Utrecht, and The Netherlands, which was established in 1986. At
follow-up the youngest infant was 3 years and the oldest was 17 years (median 7
years 11 months).

Summary, discussion and conclusion 123
We made a distinction between a structural kidney anomaly and urinary tract
dilatation to gain insight into the prognosis and outcome of these two district groups
of anomalies. A structural anomaly exists when in the very beginning aberrant
development or defects in maturation have taken place in the embryologic urinary
tract. Dilatation of the urinary tract may result from slow maturation and canalisation
of the excretory system25.
One hundred and twenty-one of the 402 fetuses died before or after birth in 106
cases the reason of death was directly related to the renal tract anomaly (26,4%).
Eighty-four of these fetuses had a structural anomaly and died mostly due to bilateral
renal agenesis (33 fetuses), bilateral multicystic kidneys (22 fetuses) or bilateral
polycystic kidneys (19 fetuses). Another 22 fetuses had a urinary tract dilatation and
they died mainly due to an isolated megabladder (17 fetuses).
Two hundred and eighty-one fetuses survived of which 64 had a structural anomaly
and 213 had a urinary tract dilatation. The structural anomaly was in approximately
80% a unilateral multicystic kidney and 12 of these infants had a contralateral
anomaly. Surgery consisted mainly of nephrectomy of the multicystic kidney. Only
two children, both with bilateral echogenic dysplastic kidneys, had impaired function
at follow-up (one with peritoneal dialysis, one with an increased creatinine level of 71
µmol/l at 7½ years of age).
The dilatation in the 213 fetuses was approximately equally divided in uni- or
bilaterally. One hundred and eighteen fetuses had a solitary uni- or bilateral dilatation
of the renal pelvis while the 95 others had a combination with a uni- or bilateral
megaureter and/ or megabladder. Approximately 50% of these children had surgery
with a total of 315 interventions. Especially high was the intervention rate in 45
children with posterior urethral valves (100%) as in the 45 cases of vesico ureteral
reflux (86,6%). In 21 cases with a bilateral dilatation labour was electively induced
before 37 weeks of gestation (mean 34,9 weeks: range 29 – 37) because of the
development of anhydramnios. Almost all children with impaired outcome can be
found in this group (6 chronic renal failure, 1 hypertension). The overall conclusion
for obstructive uropathy that can be drawn from this series is that, regardless of the
presence of 1 or 2 kidneys and regardless of the degree of urinary tract dilatation, the

124 Chapter 9
prognosis for renal function is excellent when oligohydramnios is absent before birth
and when proper urological care is given postnatally.
All in all, at follow-up 9 of the 281 surviving infants had impaired renal function and 3
children had hypertension, 12/281 (4,3%). So, overall outcome in the children was
generally good.
In Chapter 6 a large cohort of 100 fetuses with unilateral multicystic kidney disease
(MCKD), prenatally diagnosed between 15 and 42 weeks of gestation (mean 26.7
weeks), is described. Data were obtained by reviewing the databases of the obstetric
ultrasound department and of the paediatric urology department of the University
Medical Centre Utrecht, The Netherlands. The children were at follow-up 0 -16 years
of age (mean 5 years and 4 months).
MCKD only gives rarely diagnostic dilemmas on prenatal ultrasound(26) due to its
typical manifestation with (in general) multiple non-communicating cysts. The
function of the affected kidney is absent or poor. Therefore, bilateral MCKD is
invariably associated with a fatal outcome. The prognosis of unilateral MCKD is
favourable and depends on the integrity of the contralateral kidney27, 28
It is known from literature that children with unilateral MCKD have an increased risk
of abnormalities of the contralateral kidney and of the lower urogenital tract27-30. The
finding of a unilateral MCKD must therefore lead to meticulous screening of the
complete urinary tract, both pre- and postnatally, as most studies also recommend.
There is no unanimous opinion as to whether the multicystic kidney should be
removed. In some studies the children are examined periodically28, 31 after birth while
others remove the affected kidney because of possible higher risks of hypertension,
infection or malignancy28, 32-34. It is the view of the Dutch Society for Paediatric
Urology to remove the non-functioning cystic kidney to prevent lifetime follow-up of
these children, which could easily be neglected in the course of years. Furthermore
parents need not to be anxious when their child has abdominal pain. In our
population nephrectomy has been performed in 93% of surviving children and this
operation was combined with cystoscopy and in the girls also with colposcopy.

Summary, discussion and conclusion 125
Comparing our results with others is difficult because in some studies another target
group was included e.g. both the uni- and bilateral MCKD27 or a different population
limited to fetuses with a chromosomal anomaly35. We found an additional anomaly in
75% of the fetuses. This is much higher than the 21 to 57% as found by others26, 27,
29-31, 35. There were anomalies in the contralateral kidney in 48% of cases, as
compared to 13 to 39% in literature, in the ipsilateral kidney in 48% of cases (4 to
14% in literature) and in the lower urogenital tract in 33% as compared to 4 to 6% in
literature. We have no real explanation for the higher incidence of anomalies that we
found in the contralateral kidney and in the lower urogenital tract.
The higher incidence of anomalies of the ipsilateral kidney is probably the result of
the cystoscopy and the colposcopy in girls and concerned mainly an ectopic ureter or
a megaureter. Other studies only mentions an ureteral reflux or an ureteropelvic
junction stenosis27, 29, 30.
Once a multicystic kidney is diagnosed we advice a thorough screening both pre-
and postnatally since the chance of having other congenital anomalies of the urinary
tract appears high. Moreover we recommend a routine postnatal examination
consisting of an ultrasound examination, an isotope scan and a VCUG and when a
nephrectomy is done also cystoscopy and colposcopy to detect possibly hidden
anomalies of the genitourinary tract.
pyelectasis
In Chapter 7 a study is described that was done to investigate urinary tract morbidity
in late childhood in infants with a prenatally diagnosed mild pyelectasis. We defined
pyelectasis as an anteroposterior diameter of the fetal renal pelvis of 5-10 mm
without a specified gestational age at diagnosis. In literature there is no consensus
as to the cut-off points to use before birth to diagnose pyelectasis36-39.
Mild uni- or bilateral fetal pyelectasis is a frequent finding at prenatal ultrasound
examination, with a considerable variation in the reported incidence, from 0,6% to
5,5%(36-39), due to differences in criteria of the definition of pyelectasis, in particular
regarding size and gestational age at diagnosis. Guidelines relating the severity of
pyelectasis to perinatal and postnatal management are not well standardized. The
clinical significance of mild fetal pyelectasis is still unclear; it may resolve, stabilize or

126 Chapter 9
be the first indicator of significant urinary tract pathology. Evidence exists that
pyelectasis may result in clinical complications such as obstructive uropathy or
vesico ureteric reflux.
Because of the lack of data on possible long-term morbidity we investigated the
occurrence of urinary tract morbidity in childhood. We could use the data of the
Amphia hospital (a District General Hospital, location Oosterhout, The Netherlands).
All women in that region have an anomaly scan at 18 – 20 weeks gestation. It was
customary to reexam the women at approximately 32 weeks of gestation when at the
first ultrasound scan a uni- or bilateral pyelectasis was found. When the dilatation
had progressed to > 10 millimetres the child was referred to a paediatrician or
urologist for urological follow-up during the first weeks of life. When the dilatation was
stable or disappeared parents were advised to refrain from follow-up before and after
birth and were told that their child might have an increased risk for urinary tract
infection due to vesico ureteral reflux and that, in case of feeling listless or of fever of
unknown origin, urinary tract infection should be ruled out.
A large group of 208 cases and 416 matched controls were examined by a validated
questionnaire, developed by a group of The International Reflux Study in Children(40),
containing questions about urinary tract infections, incontinence, voiding and bowel
patrons. No significant differences in morbidity between children with or without mild
prenatal pyelectasis were found. Of interest is the higher incidence of urinary tract
infections in both the cases and controls as compared to literature41, 42. This high
incidence of infections was also found in another study of our group43. The surgical
intervention rate in our case-group was only 0,8% much lower than reported by
others (3,6%-24,3%) 36, 38, 44.
Based on these findings we advocate in case of a mild renal pyelectasis at about 20
weeks of gestation a single follow-up scan in the third trimester to determine if the
pyelectasis has resolved, stabilized or progressed. The child should only be referred
for postnatal examination if there is progression of the pyelectasis to >10mm. With
this policy there seems to be only a very low chance of missing an occasional case of
VUR or potential obstruction. Parents should be advised to visit the general
practitioner in case their child is lethargic or has fever of unknown origin to have the

Summary, discussion and conclusion 127
child’s urine tested to rule out urinary tract infection or treat infection effectively in
order to prevent renal damage.
In Chapter 8 a study is described on the variation of the dimensions of the fetal renal
pelvis in relation to the degree of bladder filling in fetuses with mild pyelectasis.
Pyelectasis, defined as an anteroposterior diameter of the fetal renal pelvis of 5-10
mm, might predict postnatal complications such as obstructive uropathy or vesico
ureteral reflux.
Until now two studies have been published on the variation over time of the fetal
renal pelvis in relation to bladder filling45, 46. In one study such a relationship had been
found, in the other not. This existence – or not – of a variation in pelvic size in relation
to bladder filling is relevant since the diagnosis of abnormal dilatation of the upper
tract is usually based on fixed cut-off values.
We investigated 18 pregnant women who had fetus with a uni- or bilateral pyelectasis
at the 18 – 20 weeks anomaly scan, which did not exceed 10 mm at the repeat scan
at approximately 32 weeks of gestation. Investigations were made in the late third
trimester since it has been shown that fetuses at that age have prolonged cycles of
bladder filling/ emptying, related to fetal behavioural states47, 48. We found in one third
of the fetuses that the dilatation of the renal pelvis varied according to bladder
volume with a mean difference of 6,7 mm and a largest observed difference of 14,3
mm. So the filling state of the bladder should be taken into account when fetal
hydronephrosis is suspected.
CONCLUSION
The mortality rate in fetuses is high once a renal anomaly is identified. The prognosis
for the surviving children is relatively good and these infants have only a little chance
on lifelong damage, if during pregnancy the right diagnosis has been made and if
these children have had good urological care after birth. It is important that
paediatricians and urologists are acquainted with the advices, which were given
when antenatally anomalies at the urinary tract are diagnosed, because they will be
consulted often about these anomalies after birth.

128 Chapter 9
REFERENCES
1. Stoll C, Clementi M. Prenatal diagnosis of dysmorphic syndromes by routine fetal ultrasound examination across Europe. Ultrasound Obstet Gynecol 2003;21(6):543-51. 2. Levi S. Ultrasound in prenatal diagnosis: polemics around routine ultrasound screening for second trimester fetal malformations. Prenat Diagn 2002;22(4):285-95. 3. Levi S. Mass screening for fetal malformations: the Eurofetus study. Ultrasound Obstet Gynecol 2003;22(6):555-8. 4. Grandjean H, Larroque D, Levi S. Sensitivity of routine ultrasound screening of pregnancies in the Eurofetus database. The Eurofetus Team. Ann N Y Acad Sci 1998;847:118-24. 5. Cohen HL, Cooper J, Eisenberg P, Mandel FS, Gross BR, Goldman MA, et al. Normal length of fetal kidneys: sonographic study in 397 obstetric patients. AJR Am J Roentgenol 1991;157(3):545-8. 6. Gloor JM, Breckle RJ, Gehrking WC, Rosenquist RG, Mulholland TA, Bergstralh EJ, et al. Fetal renal growth evaluated by prenatal ultrasound examination. Mayo Clin Proc 1997;72(2):124-9. 7. Pruggmayer M, Terinde R. [Fetal kidney screening: growth curves and indices]. Geburtshilfe Frauenheilkd 1989;49(8):705-10. 8. Sagi J, Vagman I, David MP, Van Dongen LG, Goudie E, Butterworth A, et al. Fetal kidney size related to gestational age. Gynecol Obstet Invest 1987;23(1):1-4. 9. Scott JE, Wright B, Wilson G, Pearson IA, Matthews JN, Rose PG. Measuring the fetal kidney with ultrasonography. Br J Urol 1995;76(6):769-74. 10. Bertagnoli L, Lalatta F, Gallicchio R, Fantuzzi M, Rusca M, Zorzoli A, et al. Quantitative characterization of the growth of the fetal kidney. J Clin Ultrasound 1983;11(7):349-56. 11. Bernaschek G, Kratochwil A. [Ultra-sound study on the growth of the fetal kidney in the second half of pregnancy (author's transl)]. Geburtshilfe Frauenheilkd 1980;40(12):1059-64. 12. Jeanty P, Dramaix-Wilmet M, Elkhazen N, Hubinont C, van Regemorter N. Measurements of fetal kidney growth on ultrasound. Radiology 1982;144(1):159-62. 13. Chiara A, Chirico G, Barbarini M, De Vecchi E, Rondini G. Ultrasonic evaluation of kidney length in term and preterm infants. Eur J Pediatr 1989;149(2):94-5. 14. Gonzales J. [Anatomical measurements during fetal growth of the kidney. Its value for the ultrasonographer and the anatomo-pathologist (author's transl)]. J Gynecol Obstet Biol Reprod (Paris) 1981;10(2):113-7. 15. Vries de L, Levene MI. Measurement of renal size in preterm and term infants by real-time ultrasound. Arch Dis Child 1983;58(2):145-7. 16. Goldstein H. Multilevel statistical models. 2nd ed. London: University of London. ed; 1995. 17. Chitty LS, Altman DG. Charts of fetal size: kidney and renal pelvis measurements. Prenat Diagn 2003;23(11):891-7. 18. Hata K, Hata T, Kitao M. Ultrasonographic identification and measurement of the human fetal adrenal gland in utero: clinical application. Gynecol Obstet Invest 1988;25(1):16-22. 19. Jeanty P, Chervenak F, Grannum P, Hobbins JC. Normal ultrasonic size and characteristics of the fetal adrenal glands. Prenat Diagn 1984;4(1):21-8.

Summary, discussion and conclusion 129 20. Lewis E, Kurtz AB, Dubbins PA, Wapner RJ, Goldberg BB. Real-time ultrasonographic evaluation of normal fetal adrenal glands. J Ultrasound Med 1982;1(7):265-70. 21. Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound Obstet Gynecol 1993;3(6):378-84. 22. Altman DG, Chitty LS. Charts of fetal size: 1. Methodology. Br J Obstet Gynaecol 1994;101(1):29-34. 23. Royston P, Altman DG. Design and analysis of longitudinal studies of fetal size. Ultrasound Obstet Gynecol 1995;6(5):307-12. 24. Royston P, Wright EM. How to construct 'normal ranges' for fetal variables. Ultrasound Obstet Gynecol 1998;11(1):30-8. 25. Cuckow PM, Nyirady P, Winyard PJ. Normal and abnormal development of the urogenital tract. Prenat Diagn 2001;21(11):908-16. 26. Aubertin G, Cripps S, Coleman G, McGillivray B, Yong SL, Van Allen M, et al. Prenatal diagnosis of apparently isolated unilateral multicystic kidney: implications for counselling and management. Prenat Diagn 2002;22(5):388-94. 27. Al-Khaldi N, Watson AR, Zuccollo J, Twining P, Rose DH. Outcome of antenatally detected cystic dysplastic kidney disease. Arch Dis Child 1994;70(6):520-2. 28. Wacksman J, Phipps L. Report of the Multicystic Kidney Registry: preliminary findings. J Urol 1993;150(6):1870-2. 29. Atiyeh B, Husmann D, Baum M. Contralateral renal abnormalities in multicystic-dysplastic kidney disease. J Pediatr 1992;121(1):65-7. 30. Eijk van L, Cohen-Overbeek TE, den Hollander NS, Nijman JM, Wladimiroff JW. Unilateral multicystic dysplastic kidney: a combined pre- and postnatal assessment. Ultrasound Obstet Gynecol 2002;19(2):180-3. 31. Rudnik-Schoneborn S, John U, Deget F, Ehrich JH, Misselwitz J, Zerres K. Clinical features of unilateral multicystic renal dysplasia in children. Eur J Pediatr 1998;157(8):666-72. 32. Elder JS, Hladky D, Selzman AA. Outpatient nephrectomy for nonfunctioning kidneys. J Urol 1995;154(2 Pt 2):712-4; discussion 714-5. 33. LaSalle MD, Stock JA, Hanna MK. Insurability of children with congenital urological anomalies. J Urol 1997;158(3 Pt 2):1312-5. 34. Webb NJ, Lewis MA, Bruce J, Gough DC, Ladusans EJ, Thomson AP, et al. Unilateral multicystic dysplastic kidney: the case for nephrectomy. Arch Dis Child 1997;76(1):31-4. 35. Lazebnik N, Bellinger MF, Ferguson JE, 2nd, Hogge JS, Hogge WA. Insights into the pathogenesis and natural history of fetuses with multicystic dysplastic kidney disease. Prenat Diagn 1999;19(5):418-23. 36. Kent A, Cox D, Downey P, James SL. A study of mild fetal pyelectasia - outcome and proposed strategy of management. Prenat Diagn 2000;20(3):206-9. 37. Langer B, Simeoni U, Montoya Y, Casanova R, Schlaeder G. Antenatal diagnosis of upper urinary tract dilation by ultrasonography. Fetal Diagn Ther 1996;11(3):191-8. 38. Persutte WH, Koyle M, Lenke RR, Klas J, Ryan C, Hobbins JC. Mild pyelectasis ascertained with prenatal ultrasonography is pediatrically significant. Ultrasound Obstet Gynecol 1997;10(1):12-8.

130 Chapter 9
39. Scott JE, Renwick M. Antenatal renal pelvic measurements: what do they mean? BJU Int 2001;87(4):376-80. 40. Gool van JD, Hjalmas K, Tamminen-Mobius T, Olbing H. Historical clues to the complex of dysfunctional voiding, urinary tract infection and vesicoureteral reflux. The International Reflux Study in Children. J Urol 1992;148(5 Pt 2):1699-702. 41. Dremsek PA, Gindl K, Voitl P, Strobl R, Hafner E, Geissler W, et al. Renal Pyelectasis in fetuses and neonates: Diagnostic value of renal pelvis diameter in pre and postnatal sonographic screening. AJR Am J Roentgenol 1997(Apr;168(4)):1017-9. 42. Harding LJ, Malone PS, Wellesley DG. Antenatal minimal hydronephrosis: is its follow-up an unnecessary cause of concern? Prenat Diagn 1999;19(8):701-5. 43. Kort de LM, Verhulst JA, Engelbert RH, Uiterwaal CS, de Jong TP. Lower urinary tract dysfunction in children with generalized hypermobility of joints. J Urol 2003;170(5):1971-4. 44. Dudley JA, Haworth JM, McGraw ME, Frank JD, Tizard EJ. Clinical relevance and implications of antenatal hydronephrosis. Arch Dis Child Fetal Neonatal Ed 1997;76(1):F31-4. 45. Petrikovsky BM, Cuomo MI, Schneider EP, Wyse LJ, Cohen HL, Lesser M. Isolated fetal hydronephrosis: beware the effect of bladder filling. Prenat Diagn 1995;15(9):827-9. 46. Persutte WH, Hussey M, Chyu J, Hobbins JC. Striking findings concerning the variability in the measurement of the fetal renal collecting system. Ultrasound Obstet Gynecol 2000;15(3):186-90. 47. Visser GH, Goodman JD, Levine DH, Dawes GS. Micturition and the heart period cycle in the human fetus. Br J Obstet Gynaecol 1981;88(8):803-5. 48. Stigter RH, Mulder EJ, Visser GH. Hourly fetal urine production rate in the near-term fetus: is it really increased during fetal quiet sleep? Early Hum Dev 1998;50(3):263-72.

Nederlandse samenvatting 131
NEDERLANDSE SAMENVATTING
Sinds in 1950 Ian Donald e.a. voor het eerst ultrageluid toepasten voor onderzoek
van de ongeborene, heeft deze techniek een enorme invloed gehad op de dagelijkse
praktijk in de verloskunde. Tot dan toe was uitwendig onderzoek van de zwangere
buik de enige manier om foetale groei te bepalen. Informatie over de foetale conditie
werd verkregen door het voelen van kindsbewegingen door de zwangere en het
beluisteren van de foetale harttonen met behulp van een houten stethoscoop.
Aanvankelijk werd echoscopie alleen gebruikt om de zwangerschapsduur vast te
stellen, de ligging van het kind en de placenta te bepalen, of om een
tweelingzwangerschap vast te stellen.
Door het voortdurend verbeteren van de apparatuur werden het oplossend vermogen
en de beeldkwaliteit steeds beter. Hierdoor nam de kennis over ontwikkeling en groei
van foetale organen snel toe en werden toenemend foetale afwijkingen ontdekt.
Heden ten dage is het opsporen van aangeboren afwijkingen een van de meest
belangrijke redenen voor echoscopisch onderzoek in de zwangerschap.
Bij 1 tot 2% van alle foetussen kan met behulp van echoscopie een ernstige of
minder ernstige afwijking worden vastgesteld. Hiervan hebben 15 tot 20% betrekking
op de urinewegen. In het begin van de jaren tachtig werd ongeveer 15% van alle
nierafwijkingen tijdens de zwangerschap opgespoord, momenteel is dit ruim 90%. Dit
percentage is zo hoog, omdat afwijkingen aan de urinewegen veelal gepaard gaan
met vochtophoping in de nieren en vocht is met echoscopie goed te zien. Hierdoor
kunnen afwijkingen, die meestal symptoomloos zijn in de zwangerschap, worden
ontdekt zodat een behandelbeleid voor na de geboorte tijdig kan worden vastgesteld
en nierschade zo veel mogelijk kan worden voorkomen. Bovendien hebben de
ouders, in voorkomende gevallen, de mogelijkheid om de zwangerschap te laten
afbreken, indien een niet met het leven verenigbare afwijking is aangetoond of
afwijkingen die zo ernstig zijn dat zij de kwaliteit van leven ernstig aantasten. Hierbij
moet men bijvoorbeeld denken aan het beiderzijds ontbreken van de nieren of aan
beiderzijds multicysteuze nieren waarbij door een zeer vroege afsluiting een
vochtophoping in beide nieren ontstaat waardoor het aanvankelijk gezonde
nierweefsel te gronde gaat.

132 Chapter 9
In de voorbije decennia zijn vele onderzoeken verschenen over nierafwijkingen bij
ongeborenen. Studies waarin langdurige vervolgonderzoek van deze kinderen
worden beschreven zijn echter schaars. Hierdoor is het moeilijk om de ouders juist
voor te lichten over wat er met hun kind aan de hand is en over de eventuele
gevolgen met betrekking tot het verdere leven. Ook advisering omtrent de juiste
behandeling na de geboorte wordt hierdoor bemoeilijkt. In het kader van dit
proefschrift werden daarom de volgende studies gedaan:
1 – Het vaststellen van grootte en groei van de foetale nier, het nierbekken en de
bijnier in het verloop van de zwangerschap.
2 – Het verzamelen van de lange termijn follow-up gegevens van een grote groep
kinderen bij wie vóór de geboorte nierafwijkingen waren vastgesteld.
3 – Onderzoek naar bijkomende afwijkingen bij kinderen bij wie vóór de geboorte
een enkelzijdige multicysteuze nier is vastgesteld.
4 – Het beantwoorden van de vraag of kinderen bij wie rond 20 weken
zwangerschapsduur met echoscopie een lichte verwijding van het nierbekken (tussen
de 5 en 10 mm) werd gezien, meer kans hebben op problemen aan de urinewegen
op de kinderleeftijd, dan kinderen bij wie dit niet was waargenomen.
5 – Het bestuderen van de relatie tussen de mate van verwijding van het nierbekken
en de vulling van de foetale blaas.
groeicurven van foetale nier, nierbekken en bijnier
Groeicurven van foetale organen zijn van belang als een afwijking wordt vermoed.
Eerdere groeicurven van foetale nieren vertoonden veelal beperkingen zoals: het niet
nauwkeurig bepalen van de duur van de zwangerschap met een vroege echoscopie,
alleen curven voor het tweede en derde trimester van de zwangerschap, bepaling
van uitsluitend de lengte van de nier, of ontwikkeling van de groeicurven op basis
van metingen gedaan bij te vroeg geboren kinderen of met de nieren van overleden
kinderen.
In hoofdstuk 2 wordt een zogeheten intra- en interobserver variantie analyse
beschreven, die is uitgevoerd om vast te stellen of herhaalde metingen gedaan door
één persoon tot dezelfde resultaten leiden èn of er een goede overeenkomst is
tussen de metingen gedaan door twee echoscopisten. De afmetingen van nier en

Nederlandse samenvatting 133
bijnier blijken door één persoon consistent gemeten te worden en de overeenkomst
tussen de metingen van twee onderzoekers was groot.
Hoofdstuk 3 en 4 beschrijven de longitudinale onderzoeken waarbij de grootte en
groei van lengte, voorachterwaartse diameter en dwarse diameter van de foetale nier
en van de voorachterwaartse en dwarse diameter van het nierbekken en de lengte
van de bijnier zijn bepaald. Bij 111 zwangeren werden deze afmetingen iedere vier
weken gemeten waarbij alle metingen drie maal achterelkaar werden gedaan. Bij de
ene helft van de zwangeren startte dit onderzoek bij 16 weken en bij de andere helft
bij 18 weken zwangerschapsduur.
Omdat de verzamelde gegevens een groot aantal foetussen betreffen, die
herhaaldelijk in de zwangerschap werden gemeten, kunnen de verkregen curven
gebruikt worden om de groei van de organen te meten maar ook om tijdens de
zwangerschap te beoordelen of de grootte overeenkomt met de zwangerschapsduur.
De statische berekeningen werden gedaan met behulp van de ‘multilevel analysis’.
Dit is een recent ontwikkelde methode die corrigeert voor ontbrekende data èn
berekeningen kan doen met gegevens die van elkaar afhankelijk zijn. De curven voor
linker en rechter nier, linker en rechter nierbekken en linker en rechter bijnier bleken
nagenoeg identiek. De uiteindelijke curven werden dan ook gemaakt op basis van de
gemiddelde gegevens van links en rechts.
Het vergelijken van onze niercurven met eerdere studies was moeilijk vanwege de
genoemde gebreken in de opzet van die studies. Daar waar vergeleken kon worden
bleken onze curven een aanzienlijk geringere spreiding te hebben ten opzichte van
de 50ste percentiel-lijn. De reden hiervan is vermoedelijk het grote aantal door ons
geïncludeerde foetussen en het feit dat wij gemiddelde waarden gebruikten van drie
achtereenvolgende metingen.
Voor de bijniercurve was er geen mogelijkheid om deze te vergelijken met eerdere
studies. Er werd een lineair verband gevonden tussen de lengte van de bijnier en de
nier met een verhouding van 2 tot 7. Deze bevinding kan gebruikt worden bij het
vermoeden op vergrote nieren ten gevolge van een afwijking, of bij aandoeningen
waarbij de bijnier te groot of te klein is.

134 Chapter 9
afwijkingen aan urinewegen
In hoofdstuk 5 beschrijven we de bevindingen en follow-up van 402 foetussen bij wie
prenataal afwijkingen aan de urinewegen waren vastgesteld. Er werd gebruik
gemaakt van de database van de afdeling obstetrische echoscopie van het
Universitair Medisch Centrum in Utrecht. Tijdens het na-onderzoek was de
gemiddelde leeftijd van deze kinderen bijna 8 jaar (spreiding 3 tot 17 jaar). Er werd
onderscheid gemaakt tussen structurele afwijkingen en afwijkingen tengevolge van
uitzetting van de nieren en urinewegen omdat deze afwijkingen een verschillende
ontstaanswijze kennen. De bedoeling was om inzicht te krijgen in de prognose voor
en de uiteindelijke uitkomst van deze kinderen.
Van de 402 foetussen hadden 151 een structurele afwijking, 247 een uitzetting van
nieren en/ of urinewegen en 4 een afwijking zonder invloed op de functie van de nier.
In totaal overleden ruim 25% van de foetussen als gevolg van de afwijking aan de
urinewegen.
Van de overlevende kinderen met een structurele afwijking had ongeveer 80% een
enkelzijdige multicysteuze nier, waarvan een kwart een bijkomende afwijking had
aan de andere nier. De Nederlandse kinderurologen adviseren de aangedane nier te
verwijderen. Dit betreft een relatief kleine ingreep die meestal verricht wordt rondom
de leeftijd van 6 maanden en veelal slechts één dag opname vereist. Tot verwijdering
van de nier wordt overgegaan nadat met een renogram is aangetoond dat er
inderdaad geen functie meer is in de aangedane nier. Een renogram is een
functieonderzoek van de nieren met radioactieve isotopen waarbij door de
uitscheiding van deze isotopen de functie van de nier kan worden bepaald. Het
voordeel van een dergelijke ingreep is dat geen levenslange follow-up meer
noodzakelijk is om de bloeddruk te meten vanwege een kans op verhoogde
bloeddruk en om het nierrestant te onderzoeken op een mogelijke eventuele
kwaadaardige ontwikkeling.
Tot de onderzoekspopulatie met een structurele afwijking behoorden verder twee
kinderen, die beiderzijds dysplastische nieren hadden. Dysplasie is een
ontwikkelingsstoornis van het nierweefsel waardoor dit slecht functioneert. Het ene
kind krijgt buikdialyse en het andere heeft een gestoorde nierfunctie.
Bij de kinderen met een verwijding van de nieren en urineleiders kwam deze
afwijking ongeveer even vaak een- als tweezijdig voor. Ruim de helft van de kinderen

Nederlandse samenvatting 135
had een enkel- of dubbelzijdige verwijding van het nierbekken terwijl de overigen ook
afwijkingen hadden aan de urineleiders en/ of blaas. Bijna de helft van de kinderen
(n=107) werd geopereerd en bij hen werden in totaal 315 ingrepen verricht. Alle
kinderen met afsluitende kleppen in de plasbuis werden geopereerd evenals 87%
van de kinderen met reflux (terugstroom van urine vanuit de blaas naar het
nierbekken tijdens het plassen).
Bij 21 kinderen werd de bevalling vóór 37 weken zwangerschapsduur ingeleid, omdat
er naast een toenemende uitzetting van het nierbekken een sterke afname van de
hoeveelheid vruchtwater plaatsvond. Afname van de hoeveelheid vruchtwater bij
deze kinderen wijst meestal op afname van de foetale mictie (hoeveelheid urine in
het vruchtwater geloosd) en daarmee op een afname van de nierfunctie. Al deze
kinderen werden binnen enkele dagen na de geboorte geopereerd. Zes van hen
hebben een verminderde nierfunctie en één kind heeft een hoge bloeddruk.
Tijdens de follow-up van alle 402 kinderen met een prenataal gediagnosticeerde
nierafwijking, bleek dat 9 van de 281 levende kinderen een gestoorde nierfunctie
hadden, waaronder één jongen een niertransplantatie heeft ondergaan en één
meisje wordt behandeld met buikdialyse. Drie kinderen hebben een verhoogde
bloeddruk. Geconcludeerd kan worden dat, kinderen met een vóór de geboorte
vastgestelde nierafwijking, 25% kans hebben om voor of na de geboorte te
overlijden. Als aan de overlevende kinderen na de geboorte goede zorg gegeven
wordt is de prognose, ongeacht of een of beide nieren zijn aangedaan en ongeacht
de ernst van de eventuele verwijding van de urinewegen, goed. Uitzondering vormt
de groep met een sterke afname van de hoeveelheid vruchtwater.
In hoofdstuk 6 wordt een groep van 100 kinderen besproken die allen een prenataal
vastgestelde enkelzijdige multicysteuze nier hadden. De gegevens werden verkregen
van de afdeling obstetrische echoscopie en van de afdeling kinderurologie van het
Wilhelmina Kinderziekenhuis te Utrecht. Uit de literatuur is bekend dat deze kinderen
vaak bijkomende afwijkingen hebben aan de overige urinewegen; reden waarom het
gehele kind tijdens het echoscopisch onderzoek goed nagekeken dient te worden als
een multicysteuze nier wordt gediagnostiseerd.

136 Chapter 9
Wij vonden bij 75% van deze kinderen een bijkomende afwijking. Dit is veel hoger
dan de 21 tot 57% die in de literatuur wordt vermeld. Achtenveertig procent had een
afwijking aan de andere nier (literatuur: 13 tot 39%). Aan de primair aangedane nier
werd in 48% van de kinderen nog een bijkomende afwijking gevonden (literatuur: 4
tot 14%) en aan het lagere urogenitale stelsel in 33% van de gevallen (literatuur: 4 tot
6%). Een gedeeltelijke verklaring voor deze door ons gevonden hoge incidenties in
vergelijking met de literatuur, vormt de in ons onderzoek routinematig uitgevoerde
cystoscopie (onderzoek van de blaas en plasbuis) bij alle kinderen en daarnaast nog
een colposcopie (onderzoek van de vagina en baarmoedermond) bij meisjes
voorafgaand aan de operatie waarbij de nier werd verwijderd. Deze onderzoeken zijn
eenvoudig uitvoerbaar en weinig belastend bij het kind dat al onder narcose is. Bij
cystoscopie werden 54 afwijkingen gevonden bij 48 kinderen. Hierbij betrof het
meestal een ectope ureter (een niet in de blaas eindigende urineleider) of een
vernauwing van de plasbuis. Bij de colposcopie bij de meisjes werden 3 afwijkingen
gevonden: eenmaal meerdere afwijkingen aan de inwendige geslachtsorganen
waaronder een afwezige vagina, eenmaal een afgesloten maagdenvlies en eenmaal
een ectope ureter die in de vagina uitmondde waardoor het meisje grote kans had
onophoudelijk ‘nat’ te zijn als deze afwijking niet gevonden was.
pyelectasie = milde verwijding van het nierbekken
In hoofdstuk 7 wordt een onderzoek beschreven naar het voorkomen van
urinewegproblemen op kinderleeftijd bij kinderen, bij wie tijdens een echoscopisch
onderzoek bij ongeveer 20 weken zwangerschapsduur een pyelectasie, een milde
verwijding tussen de 5 en 10 mm, gevonden was van één of beide nierbekkens. Er
werd gebruik gemaakt van de echoscopieverslagen van het Amphia ziekenhuis in
Oosterhout. Aldaar is gebruikelijk om patiënten, bij wie tijdens de 20-weken
echoscopie een pyelectasie wordt gezien, een herhaling van dit onderzoek te
adviseren bij ongeveer 32 weken zwangerschapsduur. Als de verwijding groter is dan
10 mm wordt de zwangere verwezen naar een tertiair centrum voor nader
onderzoek. Aldaar krijgt zij tevens een advies voor onderzoek en/ of behandeling van
het kind na de geboorte. De andere patiënten krijgen het advies geen verder
onderzoek te laten doen in de zwangerschap en na de geboorte, onafhankelijk van
het feit of de pyelectasie bij 32 weken nog wel of niet meer aanwezig was. Hen wordt

Nederlandse samenvatting 137
uitgelegd dat kinderen bij wie een pyelectasie is gezien mogelijk een hoger risico
hebben op reflux en dat als hun kind lusteloos of koortsig is zonder duidelijk
aanwijsbare reden zij de huisarts moeten vragen de urine na te kijken om een
eventuele urineweginfectie te kunnen behandelen.
Deze studie toonde aan dat 4,6% van de ruim 4500 onderzochte kinderen een enkel-
of dubbelzijdige milde pyelectasie had bij 20 weken zwangerschapsduur (literatuur:
0,6 tot 5,5%). De spreiding in de literatuur is het gevolg van het gebruik van
verschillende definities met betrekking tot verwijding van het nierbekken en van het
meten op verschillende tijdstippen in de zwangerschap. Over de klinische betekenis
van milde pyelectasie heerst nog veel onduidelijkheid. Er is overeenstemming dat
pyelectasie kan verergeren tot obstructie van het nierbekken of een uiting kan zijn
van reflux. Het is echter ook mogelijk dat de pyelectasie restloos verdwijnt. Sommige
onderzoekers adviseren om al deze kinderen na de geboorte laaggedoseerde
antibiotica te geven en hen te onderzoeken met een mictiecystogram (onderzoek met
contrastvloeistof in de blaas onder röntgendoorlichting) om reflux uit te sluiten, terwijl
andere een verwijding tot 10 mm als fysiologisch beschouwen.
Wij vergeleken twee groepen kinderen, één groep van 208 kinderen met een een- of
tweezijdige pyelectasie van 5 tot 10 mm tijdens de echoscopie rondom 20 weken
zwangerschap en een groep van 416 controle kinderen zonder deze afwijking. De
kinderen die werden geselecteerd waren tussen 4 en 9 jaar oud omdat zij zindelijk
moesten zijn om de vragen van de vragenlijsten te kunnen beantwoorden. De ouders
kregen een gestandaardiseerde vragenlijst toegezonden waarin gevraagd werd naar
plasgedrag, urine incontinentie, urineweginfecties, bedplassen en ontlastingspatroon
van het kind. Ruim 70% van de ouders van de kinderen met pyelectasie en 60% van
de controlegroep stuurden de vragenlijsten terug. Het bleek dat jongens significant
vaker vóór de geboorte een pyelectasie hadden dan de meisjes.
Er was geen verschil in de incidentie van urineweginfecties en plasgedrag. Wel werd
in beide groepen een hoger percentage urineweginfecties gevonden dan beschreven
is in de literatuur en in een onderzoek van het RIVM onder huisartsenpraktijken. Dit
hogere percentage is ook gevonden in een andere studie van onze onderzoeksgroep
en wordt mogelijk verklaard door het feit dat de vragenlijsten zeer gedetailleerd naar
plasgedrag en stoelgang vragen. Een andere mogelijkheid is misschien dat
huisartsen in de onderzoeksregio sneller urine onderzoeken op een infectie, omdat

138 Chapter 9
zij daar expliciet om gevraagd worden zulks te doen conform het advies dat aan de
ouders is gegeven en daardoor misschien ook eerder de urine nakijken bij kinderen
vanuit de controle groep als die met onbegrepen klachten op het spreekuur komen..
Ondanks het advies het kind na de geboorte niet te laten onderzoeken werd dit bij
ruim 30% van de kinderen toch gedaan. Meestal betrof het vrouwen die in het
ziekenhuis bevallen waren en waarvan het kind door de kinderarts gecontroleerd was
waarbij melding werd gemaakt van de bevinding van pyelectasie in de
zwangerschap. Van al deze kinderen maakten slechts drie een urineweginfectie
door. Eén kind werd geopereerd op de leeftijd van drie jaar omdat het nierbekken
verder verwijdde en de nierfunctie verslechterde. Slechts één kind vertoonde een
geringe reflux die spontaan verdween.
Op grond van dit onderzoek kan geconcludeerd worden dat als een enkel- of
dubbelzijdige pyelectasie wordt gezien tijdens de echoscopie bij 20 weken
zwangerschapsduur het onderzoek herhaald dient te worden rondom de 32e week.
Alleen als de pyelectasie meer dan 10 mm bedraagt dient de zwangere verwezen te
worden (in dit onderzoek bij 9% van de vrouwen; deze groep maakte overigens geen
deel van het huidige onderzoek uit). De andere ouders dient geadviseerd te worden
dat, indien hun kind hangerig of koortsig is zonder duidelijk aanwijsbare reden, zij de
huisarts moeten vragen urine van het kind na te kijken om een eventuele
urineweginfectie te kunnen diagnosticeren en zonodig te behandelen om nierschade
te voorkomen.
In hoofdstuk 8 werd onderzocht of er een relatie bestond tussen een verwijding van
het nierbekken en de vulling van de blaas. Bij het doen van echoscopisch onderzoek
was het regelmatig opgevallen dat de uitzetting van het nierbekken gedurende het
onderzoek wisselde. Omdat vervolgonderzoek in de zwangerschap of na de
geboorte meestal is gebaseerd op één enkele meting van het nierbekken is het van
belang of deze relatie inderdaad aanwezig is. Achttien zwangeren werden
onderzocht bij wie bij het echoscopisch onderzoek rondom 20 weken
zwangerschapsduur een enkel- of dubbelzijdige foetale pyelectasie werd gezien. Bij
de herhalingsechoscopie bij 32 weken was de verwijding niet tot meer dan 10 mm

Nederlandse samenvatting 139
toegenomen. Tijdens het onderzoek waren de patiënten 37 à 38 weken zwanger
omdat aan het einde van de zwangerschap foetussen een lange blaasvullings/
ledigingscyclus hebben, die gerelateerd is aan foetale gedragstoestanden.
Bij eenderde van de onderzochte foetussen werd een relatie gevonden tussen de
mate van verwijding van het nierbekken en de vulling van de blaas. Bij deze
subgroep was het gemiddelde verschil in de verwijding van het nierbekken bij volle
of lege blaas 6,7 mm, en bedroeg het grootste gemeten verschil 14,3 mm.
Uit dit onderzoek concluderen wij dat in geval van foetale milde pyelectasie, niet
volstaan kan worden met één enkel meetmoment, maar dat tijdens het onderzoek
meerdere keren gemeten dient te worden, bij voorkeur binnen een kwartier voor en
na leegplassen. Anderzijds houdt dit onderzoek in dat een eenmalige normale
bevinding een milde pyelectasie (een half uur later) niet uitsluit.
conclusie
Afwijkingen aan de foetale urinewegen kennen een hoge mortaliteit. Overlevende
kinderen hebben echter slechts een geringe kans op blijvende schade indien de
juiste diagnose in de zwangerschap wordt gesteld en indien deze kinderen na de
geboorte goede urologische opvang hebben. Het is van belang dat kinderartsen en
urologen bekend zijn met de adviezen die gegeven worden indien prenataal
afwijkingen aan de urinewegen worden vastgesteld, omdat zij na de geboorte
hieromtrent vaak geconsulteerd zullen worden.

140 Chapter 9 Dankwoord
Ik wil graag al diegenen bedanken zonder wie dit proefschrift niet tot stand was
gekomen. Hun inzet en steun waren van onschatbare waarde.
Allereerst gaat heel veel dank naar alle 1316 zwangeren, bij wie tijdens 3091
consulten 27.546 metingen werden verricht ten behoeve van alle onderzoeken die
beschreven zijn in dit proefschrift. Deze vrouwen deden geheel belangeloos mee,
soms moeizaam liggend, gedurende vaak urenlange onderzoeken maar tegelijkertijd
veel interesse tonend in het onderzoek en blij dat zij mee konden doen ten behoeve
van andere toekomstige moeders en kinderen.
Dr. G. H.A. Visser Gerard, ik ben je onbenoembaar dankbaar dat je mij de
gelegenheid hebt geboden onderzoek te gaan doen. Je zei erbij “Als het een beetje
goed gaat, mag je van mij promoveren.” Ik was perplex. Jouw stimulans,
opbouwende kritiek en waardevolle adviezen hebben me enorm gestimuleerd vooral
als ik het eens niet zag zitten. Je straalde het uit en ging er ook van uit dat ik het een
en ander tot een goed einde zou brengen. En ziedaar het proefschrift is klaar. Dank
voor je vertrouwen in me.
Dr. P.H. Stoutenbeek Philip, jouw database, opgestart in een fase van de IT dat dit
nog niet zo gewoon was, vormt een belangrijk deel van dit proefschrift. Dank dat ik
van al die gegevens gebruik mocht maken. Je kritische beoordeling en suggesties
waren een waardevolle en welkome aanvulling van het manuscript. Ik denk met
plezier terug aan al de jaren dat ik bij jou op de echokamer werkte.
Dr. T.P.V.M. de Jong Tom, jij was degene die de basis hebt gelegd voor wat betreft
mijn kennis van de foetale nieren. Altijd gaf je uitgebreid uitleg en was je behulpzaam
met adviezen als ik weer eens vragen had met betrekking tot patiënten uit
Oosterhout. Onbewust, heb jij daardoor aan het begin van dit proefschrift gestaan.
Tom, jouw aanmoediging, het vaak ‘even’ langs komen, “hoe gaat het ermee?” zijn
voor mij een grote steun en stimulans geweest. Nooit was je iets teveel, je las
manuscripten razendsnel en had altijd opbouwend kritiek hetgeen me grote steun
gaf. Dank je wel.

Dankwoord 141
Dr. R.H. Stigter Rob, veel dank ben ik jou verschuldigd. Allereerst dat je me
uitnodigde op jouw kamer om aan dit proefschrift te gaan werken. Ik heb dat enorm
gewaardeerd. Van jou heb ik geleerd wetenschappelijk te gaan denken, vaak via
‘losse’ opmerkingen van je die me tot denken aanzetten en op het goede spoor
brachten. Maar vooral ben ik je dank verschuldigd door je kritische beoordeling van
de diverse artikelen en natuurlijk je onmisbare hulp bij de correctie tot
wetenschappelijk en leesbaar engels. Met groot genoegen denk ik terug aan onze
gezamenlijke jaren op de echokamer en prenatale ‘prik’spreekuren.
Drs. L.R. Pistorius Lou, sinds een klein jaar zijn we kamergenoten en hebben heel
wat afgekletst. Ik dank je voor deze gezellige tijd. Het was heerlijk een ‘native
speaker’ naast me te hebben voor een lastig engels woord of uitdrukking.
Samen hebben we de metingen voor de interobserver variatie in een sneltreinvaart
afgerond. Je deed het naast je ‘normale’ werk en ik kon je altijd bellen als een
zwangere was ‘gestrikt’ om mee te doen aan het onderzoek. Veel dank hiervoor.
Dr. P. Westers Paul, jij was mijn steun en toeverlaat bij de statistische berekeningen.
Voor mij vaak een abracadabra waarmee jij me vertrouwd hebt gemaakt en
geholpen. Je beantwoordde altijd razendsnel per mail de vragen die ik op je
afvuurde, hetgeen bijzonder aangenaam was als ik weer eens vastzat. Je hebt een
humor die de vaak ‘droge’ statistiek verteerbaar maakt. Dank voor alles..
Mevrouw M.J. Korenromp Marijke, ik ben heel blij dat je mijn paranimf wilt zijn. We
kennen elkaar van de opleiding en waren dit jaar 40 jaar vroedvrouw! In al die jaren
hebben we samen veel meegemaakt. Je was altijd een enorme steun voor me in
moeilijke tijden en ik ben blij dat jij mijn vriendin bent.
Drs. P.J. Damen, Pieter Jan, het geeft een bijzonder en trots gevoel dat jij tijdens de
promotie naast me staat. Mijn jongste zoon die ook het medische vak is ingegaan en
mijn paranimf wil zijn. Dank je wel.

142 Chapter 9
Verder dank ik alle familieleden en vrienden voor de interesse die zij getoond hebben
de afgelopen jaren. Sommigen hoofdschuddend: Dat je dat leuk vindt! Waar begin je
aan? Ga met de VUT! Anderen ook met ‘bewondering’: echt iets voor Hen! Maar van
iedereen was er steun en aandacht. Dank jullie wel.
En natuurlijk gaat heel, heel veel dank naar het thuisfront. Naar mijn man, Albert, die
ik dank voor zijn onvoorwaardelijke geduld en steun. Ik kon altijd mijn verhaal kwijt
van dit voor hem vaak onbegrijpelijke onderzoek. Ik hoop dat we nog vele jaren
samen mogen delen.
Veel te danken heb ik aan mijn kinderen, Annette, Albert jr. en Pieter Jan, die indien
nodig altijd klaar staan om te helpen en steunen waar maar nodig is. Ik ben trots op
jullie. En jullie kunnen me niet meer plagen want de enige HBO-er in het gezin
verslaat jullie nu in één klap!
Verder dank ik jullie partners, die wat meer vanaf de zijlijn toezien maar door hun
aandacht en interesse veel steun gaven.
En last but not least mijn twee kleinzonen, Joost en Ties. Oma is blij met jullie en nu
kunnen jullie nog vaker komen logeren.

Curriculum vitae 143
Geboren 27 mei 1941, te Tegelen
HBS-b, 1961, Sint Bonifacius Lyceum, Utrecht
opleiding van Verloskundigen, 1961-1964, Vroedvrouwenschool, Heerlen
Verloskundige, 1964 – 1965, Privé-kliniek: Dr.Bohler te Luxemburg, Luxemburg
Verloskundige, 1965 – 1977, Sint Joseph ziekenhuis, Eindhoven.
Aanvankelijk werkzaam op de verloskamers en polikliniek, later speciaal belast met het maken van een jaarverslag van de afdeling, verloskunde, gynaecologie en fertiliteit.
Verloskundige – echoscopiste, 1980 – 2003, Pasteur Ziekenhuis, Oosterhout N-Br.
Verloskundige – echoscopiste, 1989 – nov. 1999, UMCU, Utrecht
Verloskundige – onderzoeker, nov. 1999 – 2004, UMCU, Utrecht
1985 – 1977, Lid Commissie Ultrageluid, Koninklijke Nederlandse Organisatie van
Verloskundigen (KNOV)
1985 – heden, bestuurslid Werkgroep Foetale Echoscopie van de Nederlandse
Vereniging voor Obstetrie en Gynaecologie
!988 – 1996, lid van het hoofdbestuur van de KNOV
1990 – 1996, voorzitter van de afdeling Noord Brabant van de KNOV
1990 – 1992, gedelegeerde Stuurgroep Toekomst Scenario’s Gezondheidszorg
namens de KNOV
1995 – 2003, lid Subwerkgroep Echoscopisch Onderzoek van het Verloskundig
Overleg bij de Ziekenfondsraad namens de KNOV ten behoeve van het Verloskundig
Vademecum, uitgave 1 en 2
1995 – heden, initiator en cursusmanager van de “Cursus Echoscopie voor
verloskundigen werkzaam in de eerste lijn”.
Top Related