Seminar 27-11-205 Dr. E. van der Veer
32
Dr. E. van der Veer Zwolle, 28 november 2015 IWO copyright Dr. E. van der Veer
-
Upload
stichting-interdisciplinaire-werkgroep-osteoporose -
Category
Health & Medicine
-
view
194 -
download
0
Transcript of Seminar 27-11-205 Dr. E. van der Veer
Dr. E. van der Veer Zwolle, 28 november 2015 IWO
copyright
Dr. E. van der Veer
• Wat is mastocytose • PrevalenAe mastocytose
• PrevalenAe osteoporoAsche fracturen (laag energeAsch trauma)
• Fractuur risico inschaJng voor individuele paAënt
copyright
Dr. E. van der Veer
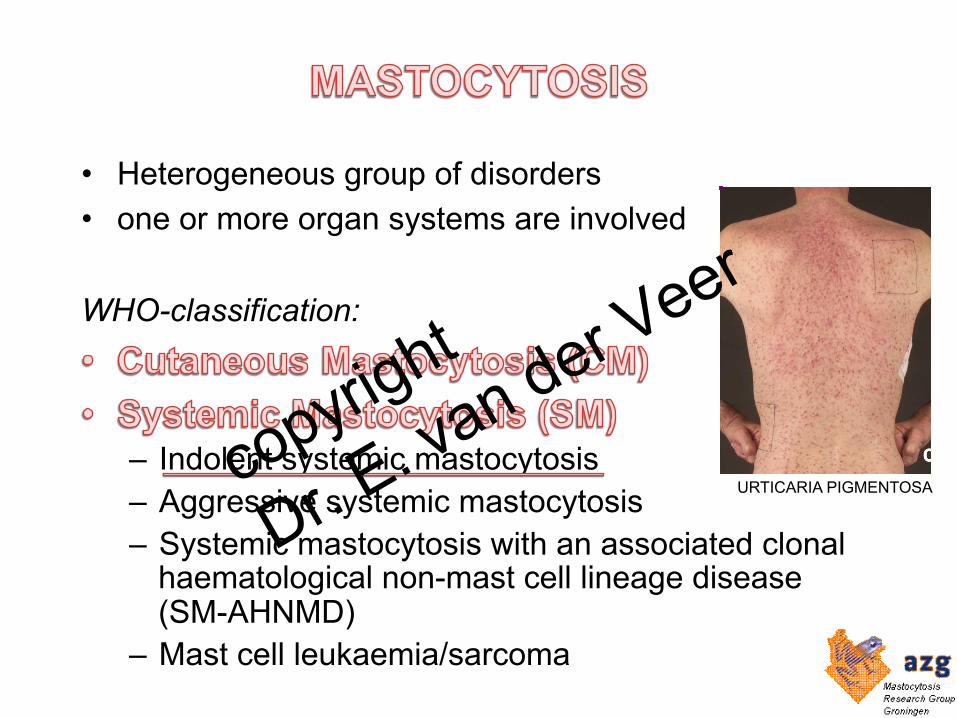
• Heterogeneous group of disorders • one or more organ systems are involved WHO-classification:
– Indolent systemic mastocytosis – Aggressive systemic mastocytosis – Systemic mastocytosis with an associated clonal
haematological non-mast cell lineage disease (SM-AHNMD)
– Mast cell leukaemia/sarcoma
URTICARIA PIGMENTOSA copyright
Dr. E. van der Veer
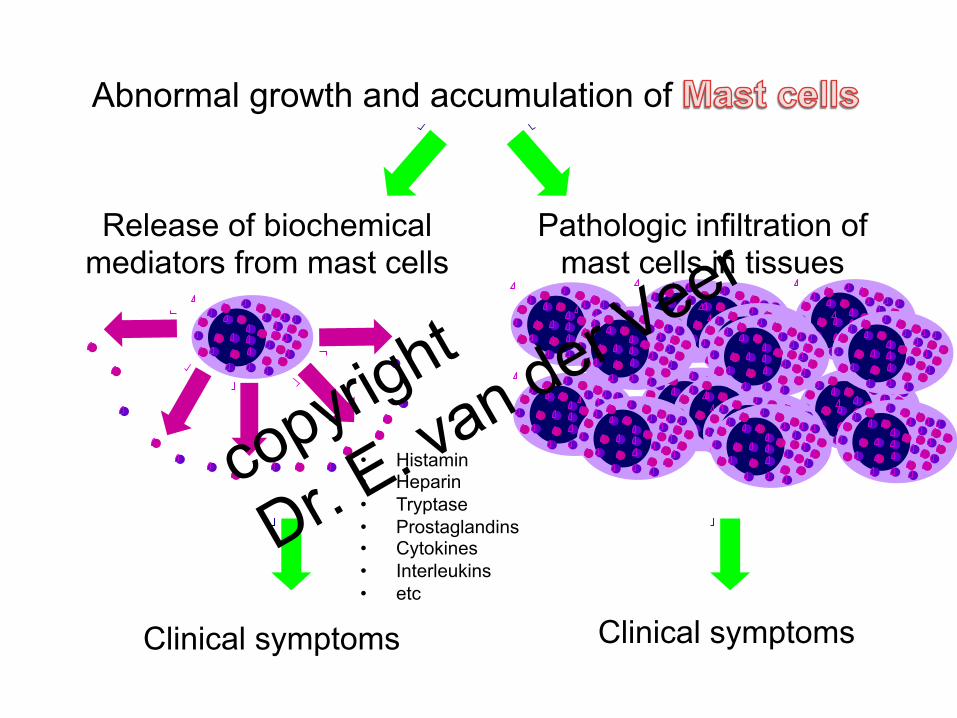
Release of biochemical mediators from mast cells
Pathologic infiltration of mast cells in tissues
Abnormal growth and accumulation of
Clinical symptoms Clinical symptoms
• Histamin • Heparin • Tryptase • Prostaglandins • Cytokines • Interleukins • etc
copyright
Dr. E. van der Veer
• In serum
tryptase > 10 ng/ml • In 2de nuchtere urine histaminemetaboliet
methylimidazolazijnzuur (MIMA) MIMA > 2,0 mmol/mol kreatinine
• Daarna volgt beenmergonderzoek met histologisch, cytologisch en genetisch onderzoek en immunofenotypering
copyright
Dr. E. van der Veer
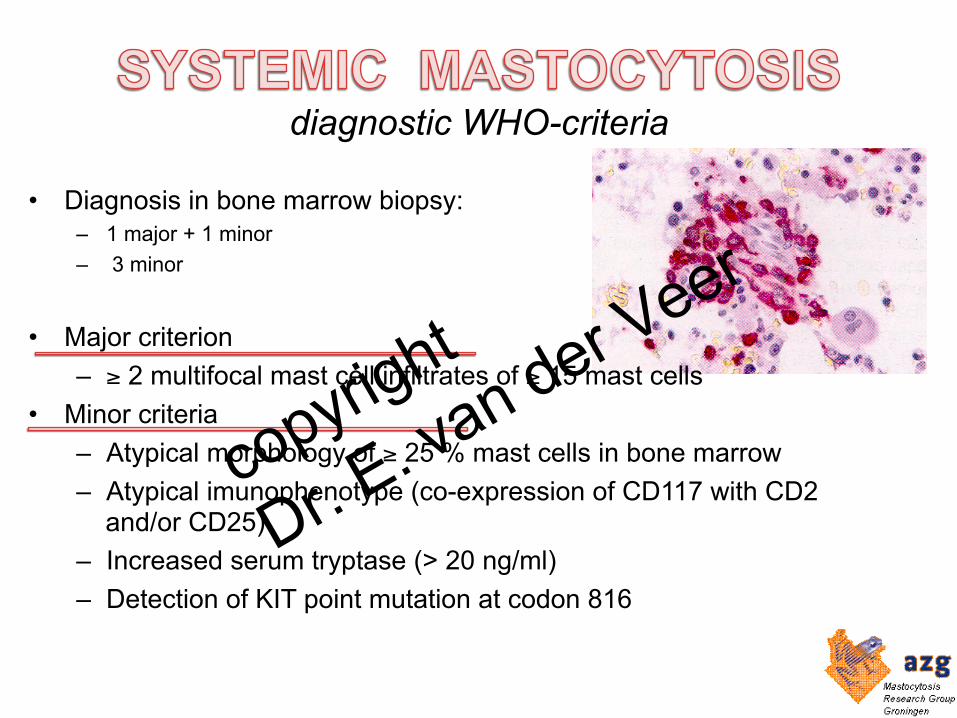
diagnostic WHO-criteria
• Diagnosis in bone marrow biopsy: – 1 major + 1 minor – 3 minor
• Major criterion – ≥ 2 multifocal mast cell infiltrates of ≥ 15 mast cells
• Minor criteria – Atypical morphology of ≥ 25 % mast cells in bone marrow – Atypical imunophenotype (co-expression of CD117 with CD2
and/or CD25) – Increased serum tryptase (> 20 ng/ml) – Detection of KIT point mutation at codon 816
copyright
Dr. E. van der Veer
Heterogeen ziektebeeld Klachten: • Jeuk • Flushing • Diarree • Invaliderende moeheid • Recidiverende anafylaxie • Osteoporose • Fracturen Gevolg van mestcelophoping • Hepatosplenomegalie • Vergrote lymfklieren Sommige mastocytose patiënten hebben geheel geen klachten Puntmutatie in de KIT-stamcelreceptor op de mestcellen (Asp-816-Val)
copyright
Dr. E. van der Veer
• Wat is mastocytose • Prevalentie mastocytose • Prevalentie osteoporotische fracturen
(laag energetisch trauma) • Fractuur risico inschatting voor individuele
patiënt copyright
Dr. E. van der Veer
UMCG & Martini Hospital: 42 Mastocytosis patients
age 55 yrs (19-75) 38% man
copyright
Dr. E. van der Veer

The prevalence of ISM was at least 13.0 cases per 100.000 inhabitants aged ≥15 years. ISM prevalence increased with age.
JJ. van Doormaal et al JACI 2013
copyright
Dr. E. van der Veer

• Wat is mastocytose • Prevalentie mastocytose • Prevalentie osteoporotische fracturen
(laag energetisch trauma) • Fractuur risico inschatting voor individuele
patiënt copyright
Dr. E. van der Veer
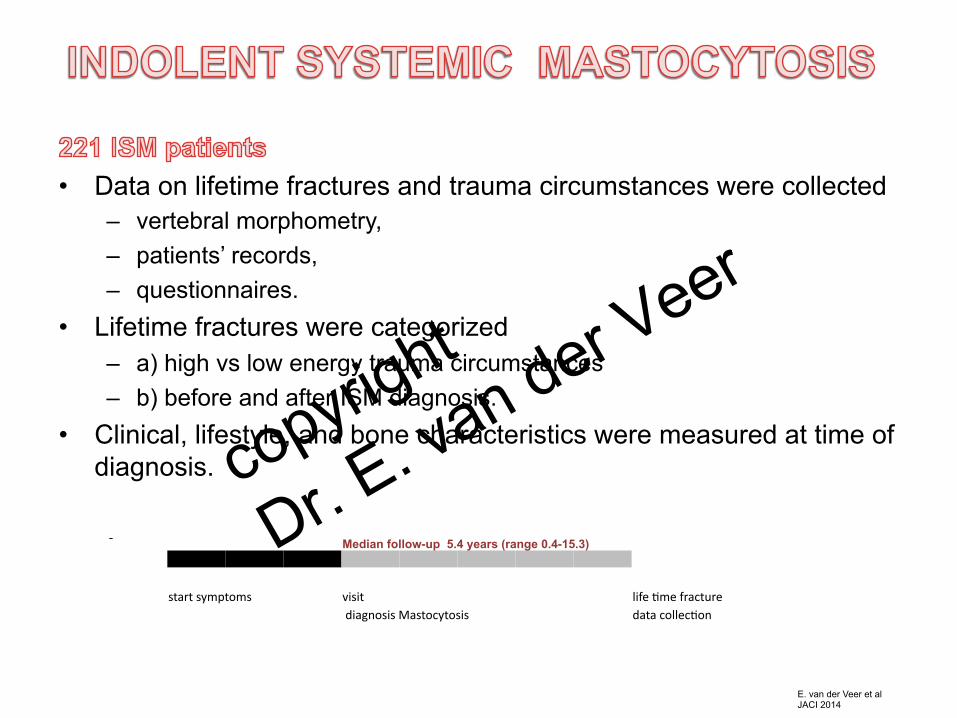
• Data on lifetime fractures and trauma circumstances were collected
– vertebral morphometry, – patients’ records, – questionnaires.
• Lifetime fractures were categorized – a) high vs low energy trauma circumstances – b) before and after ISM diagnosis.
• Clinical, lifestyle, and bone characteristics were measured at time of diagnosis.
E. van der Veer et al JACI 2014
Median follow-up 5.4 years (range 0.4-15.3)
start symptoms visit life Ame fracture
diagnosis Mastocytosis data collecAon
copyright
Dr. E. van der Veer
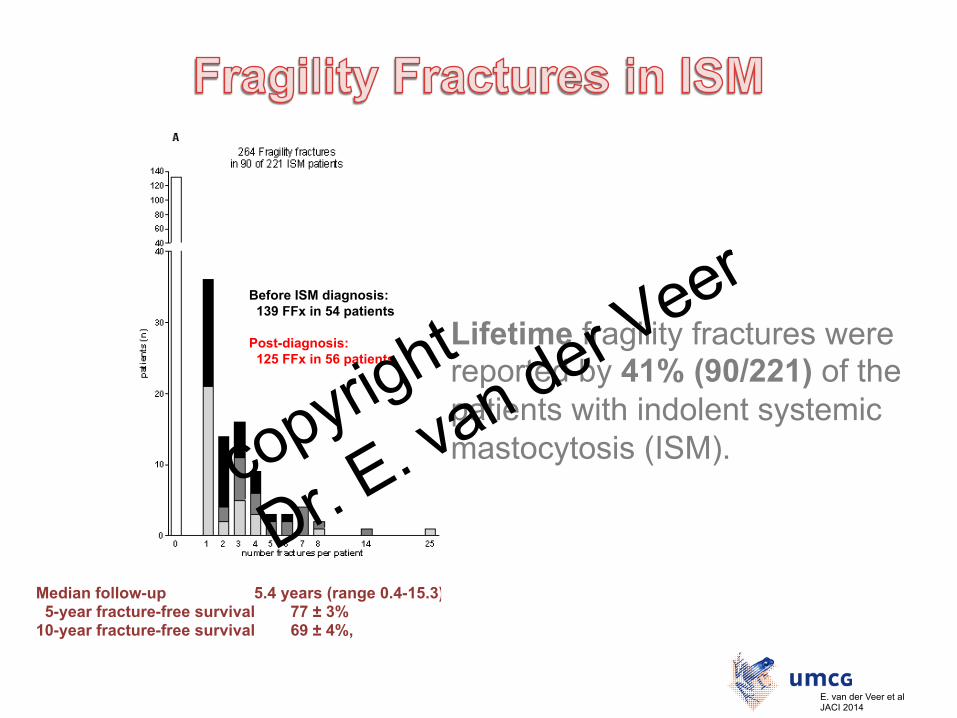
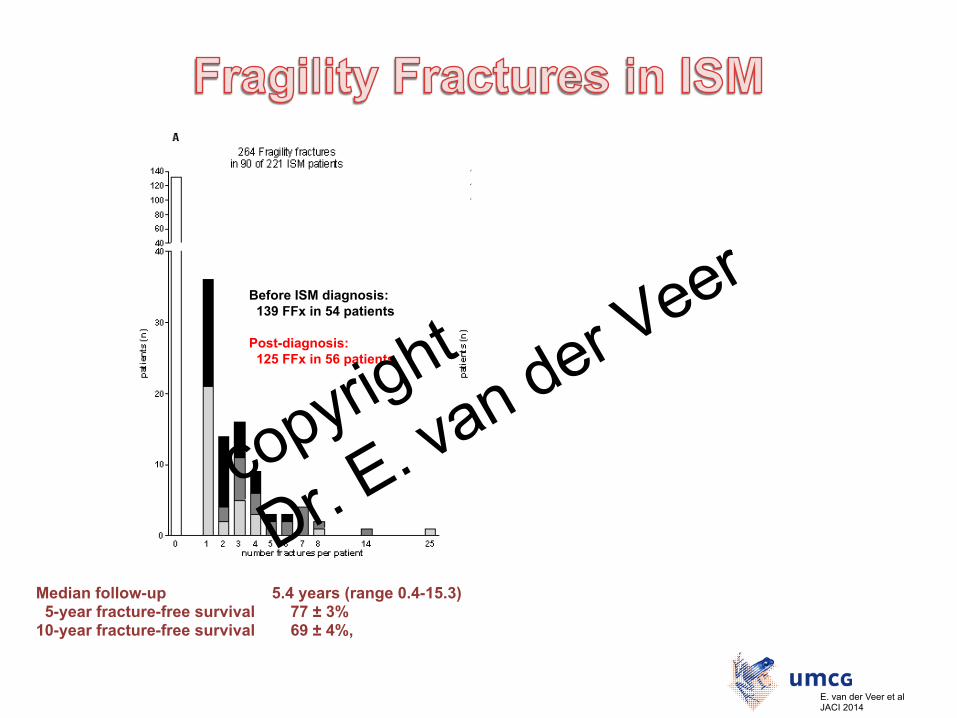
Median follow-up 5.4 years (range 0.4-15.3) 5.3 years; range 0.4-15.3 5-year fracture-free survival 77 ± 3% 78 ± 4% 10-year fracture-free survival 69 ± 4%, 71 ± 4%
E. van der Veer et l JCI 2014 online
Before ISM diagnosis: 139 FFx in 54 patients Post-diagnosis: 125 FFx in 56 patients
Before ISM diagnosis: 40 FFx in 27 patients Post-diagnosis: 88 FFx in 43 patients
Lifetime fragility fractures were reported by 41% (90/221) of the patients with indolent systemic mastocytosis (ISM).
E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer

• Wat is mastocytose • Prevalentie mastocytose • Prevalentie osteoporotische fracturen
(laag energetisch trauma) • Fractuur risico inschatting voor individuele
patiënt copyright
Dr. E. van der Veer
Aim: • to determine the high/low risk of future fragility
fractures in patients presenting with indolent systemic mastocytosis.
E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
• Data on lifetime fractures and trauma circumstances were collected
– vertebral morphometry, – patients’ records, – questionnaires.
• Lifetime fractures were categorized – a) high vs low energy trauma circumstances – b) before and after ISM diagnosis.
• Clinical, lifestyle, and bone characteristics were measured at time of diagnosis.
- 28 patients receiving treatment for osteoporosis before ISM diagnosis - 9 patients with missing bone data (BTM and BMD) - 2 patients with a recent fracture or operation - 1 patient had gender change were excluded from FFx risk assessment. E. van der Veer et al
JACI 2014
copyright
Dr. E. van der Veer
Median follow-up 5.4 years (range 0.4-15.3) 5.3 years; range 0.4-15.3 5-year fracture-free survival 77 ± 3% 78 ± 4% 10-year fracture-free survival 69 ± 4%, 71 ± 4%
E. van der Veer et l JCI 2014 online
Before ISM diagnosis: 139 FFx in 54 patients Post-diagnosis: 125 FFx in 56 patients
Before ISM diagnosis: 40 FFx in 27 patients Post-diagnosis: 88 FFx in 43 patients
E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
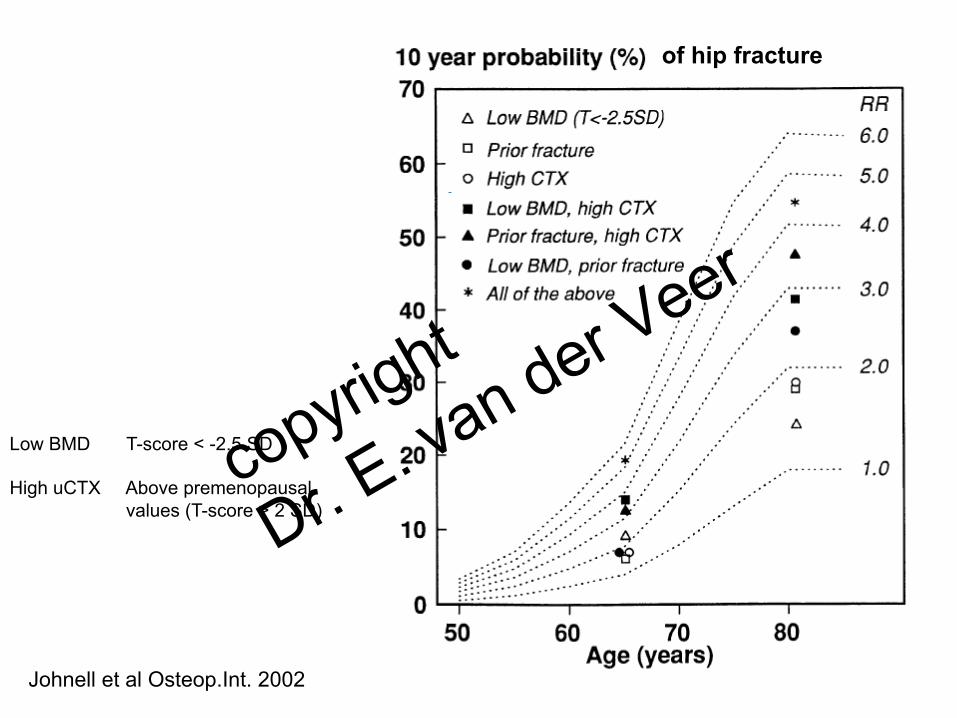
Low BMD T-score < -2.5 SD High uCTX Above premenopausal
values (T-score > 2 SD)
Johnell et al Osteop.Int. 2002
of hip fracture
copyright
Dr. E. van der Veer
Fracture Risk Assessment Tools 10-year probability of hip fracture 10-year probability of a major osteoporotic fracture
(clinical spine, forearm, hip or shoulder fracture).
The model accepts: • FRAX age 40 - 90 years. • Garvan age 50 years or more • Qfracture age 30 – 99 years
181 Indolent Systemic Mastocytosis patients, aged 19-77 years, mean 46 ± 13 years
copyright
Dr. E. van der Veer
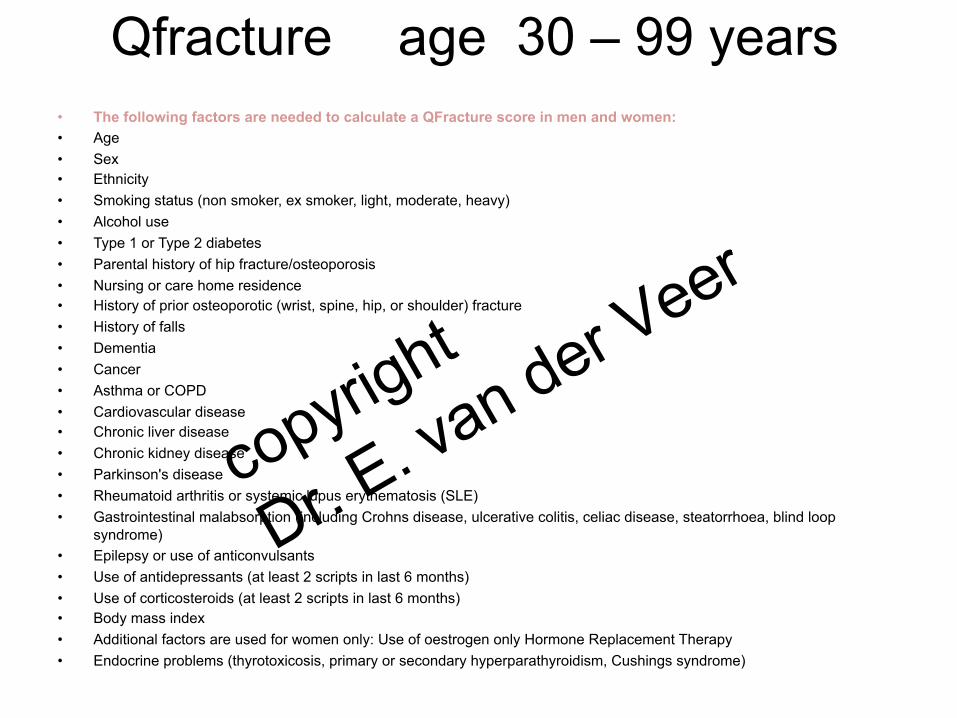
Qfracture age 30 – 99 years • The following factors are needed to calculate a QFracture score in men and women:
• Age • Sex • Ethnicity • Smoking status (non smoker, ex smoker, light, moderate, heavy) • Alcohol use • Type 1 or Type 2 diabetes • Parental history of hip fracture/osteoporosis • Nursing or care home residence • History of prior osteoporotic (wrist, spine, hip, or shoulder) fracture • History of falls • Dementia • Cancer • Asthma or COPD • Cardiovascular disease • Chronic liver disease • Chronic kidney disease • Parkinson's disease • Rheumatoid arthritis or systemic lupus erythematosis (SLE) • Gastrointestinal malabsorption (including Crohns disease, ulcerative colitis, celiac disease, steatorrhoea, blind loop
syndrome) • Epilepsy or use of anticonvulsants • Use of antidepressants (at least 2 scripts in last 6 months) • Use of corticosteroids (at least 2 scripts in last 6 months) • Body mass index • Additional factors are used for women only: Use of oestrogen only Hormone Replacement Therapy • Endocrine problems (thyrotoxicosis, primary or secondary hyperparathyroidism, Cushings syndrome)
copyright
Dr. E. van der Veer
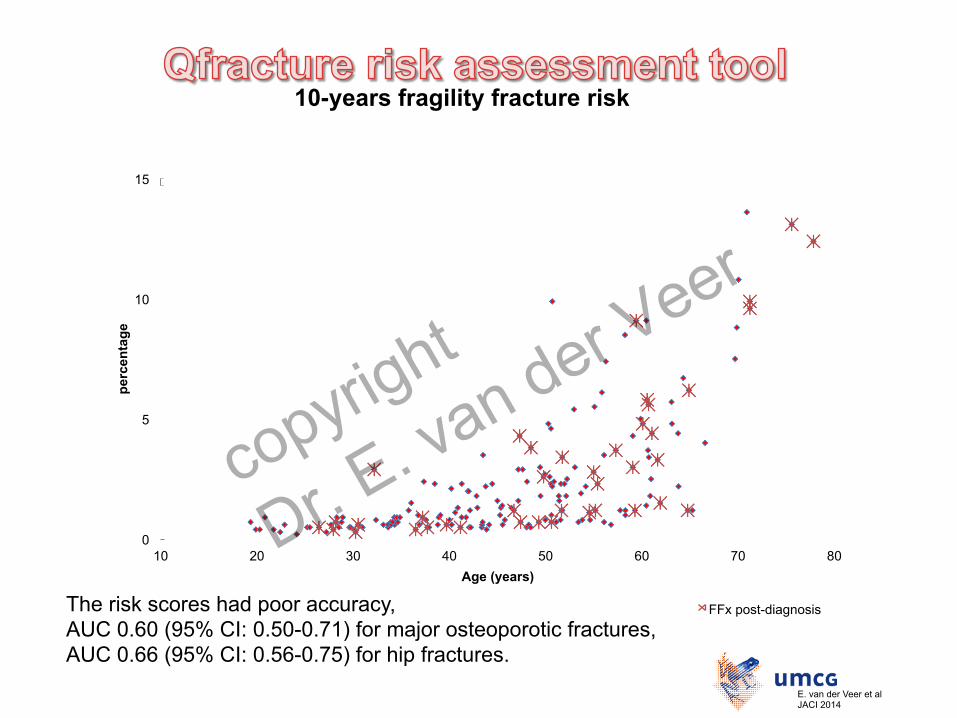
The risk scores had poor accuracy, AUC 0.60 (95% CI: 0.50-0.71) for major osteoporotic fractures, AUC 0.66 (95% CI: 0.56-0.75) for hip fractures.
0
5
10
15
10 20 30 40 50 60 70 80
perc
enta
ge
Age (years)
10-years fragility fracture risk
FFx post-diagnosis
E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
E. van der Veer et al E. van der Veer et al JACI 2014
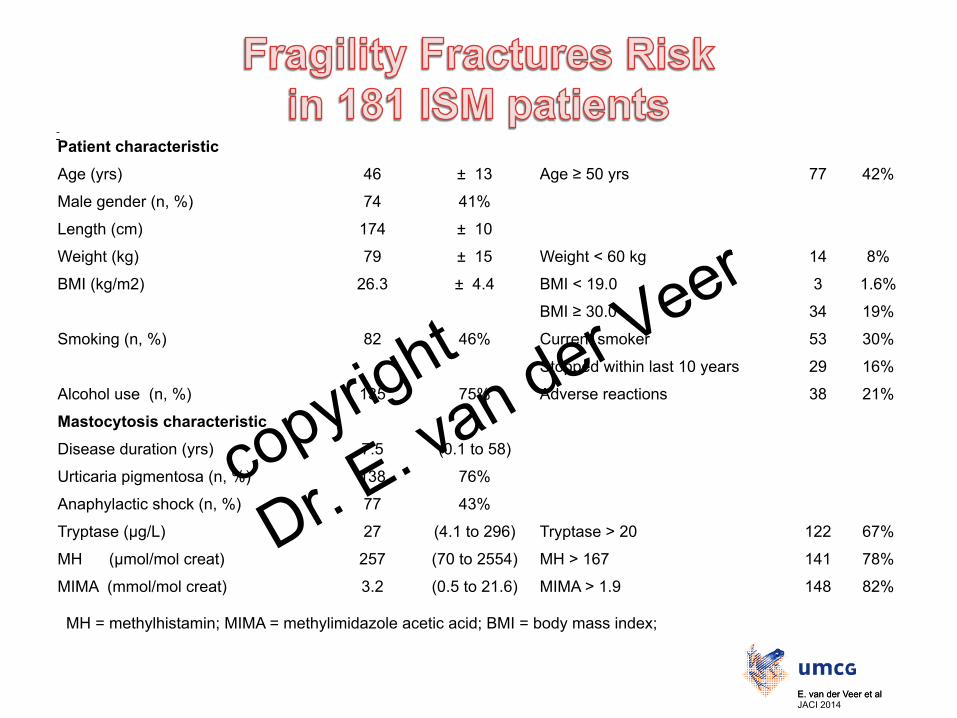
Patient characteristic
Age (yrs) 46 ± 13 Age ≥ 50 yrs 77 42%
Male gender (n, %) 74 41%
Length (cm) 174 ± 10
Weight (kg) 79 ± 15 Weight < 60 kg 14 8%
BMI (kg/m2) 26.3 ± 4.4 BMI < 19.0 3 1.6%
BMI ≥ 30.0 34 19%
Smoking (n, %) 82 46% Current smoker 53 30%
Stopped within last 10 years 29 16%
Alcohol use (n, %) 135 75% Adverse reactions 38 21%
Mastocytosis characteristic
Disease duration (yrs) 7.5 (0.1 to 58)
Urticaria pigmentosa (n, %) 138 76%
Anaphylactic shock (n, %) 77 43%
Tryptase (µg/L) 27 (4.1 to 296) Tryptase > 20 122 67%
MH (µmol/mol creat) 257 (70 to 2554) MH > 167 141 78%
MIMA (mmol/mol creat) 3.2 (0.5 to 21.6) MIMA > 1.9 148 82%
MH = methylhistamin; MIMA = methylimidazole acetic acid; BMI = body mass index;
copyright
Dr. E. van der Veer
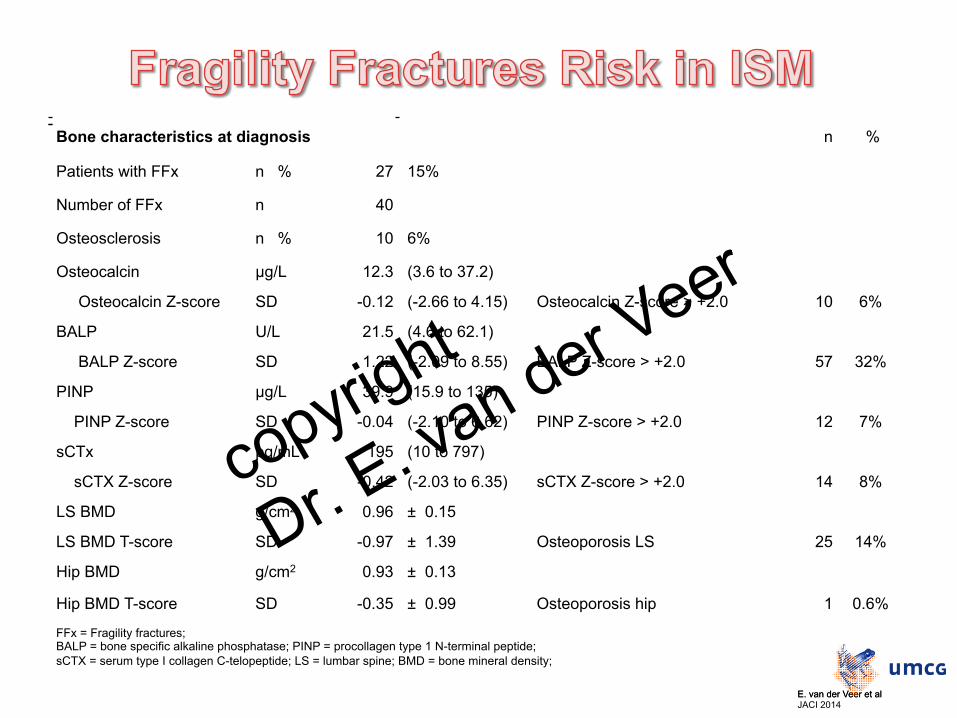
Bone characteristics at diagnosis n %
Patients with FFx n % 27 15%
Number of FFx n 40
Osteosclerosis n % 10 6%
Osteocalcin µg/L 12.3 (3.6 to 37.2)
Osteocalcin Z-score SD -0.12 (-2.66 to 4.15) Osteocalcin Z-score > +2.0 10 6%
BALP U/L 21.5 (4.6 to 62.1)
BALP Z-score SD 1.22 (-2.09 to 8.55) BALP Z-score > +2.0 57 32%
PINP µg/L 39.9 (15.9 to 135)
PINP Z-score SD -0.04 (-2.10 to 6.62) PINP Z-score > +2.0 12 7%
sCTx pg/mL 195 (10 to 797)
sCTX Z-score SD -0.42 (-2.03 to 6.35) sCTX Z-score > +2.0 14 8%
LS BMD g/cm2 0.96 ± 0.15
LS BMD T-score SD -0.97 ± 1.39 Osteoporosis LS 25 14%
Hip BMD g/cm2 0.93 ± 0.13
Hip BMD T-score SD -0.35 ± 0.99 Osteoporosis hip 1 0.6%
FFx = Fragility fractures; BALP = bone specific alkaline phosphatase; PINP = procollagen type 1 N-terminal peptide; sCTX = serum type I collagen C-telopeptide; LS = lumbar spine; BMD = bone mineral density;
E. van der Veer et al E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
• Multivariate Cox regression HR
95% CI P-value B MastFx-
score Lower Upper Male gender 2,043 1,045 3,996 0,037 0,715 1
sCTX Z-score ≥ +1.0 2,632 1,278 5,424 0,009 0,968 1
Hip BMD T-score ≤ -1.0 2,187 1,128 4,240 0,021 0,782 1
UP absence 2,047 1,074 3,899 0,029 0,716 1
Alcohol use 3,445 1,016 11,688 0,047 1,237 1
HR: hazard ratio; CI: confidence interval; B: regression coefficient; sCTX: serum type I collagen C-telopeptide; BMD: bone mineral density; UP: urticaria pigmentosa
E. van der Veer et al E. van der Veer et al JACI 2014
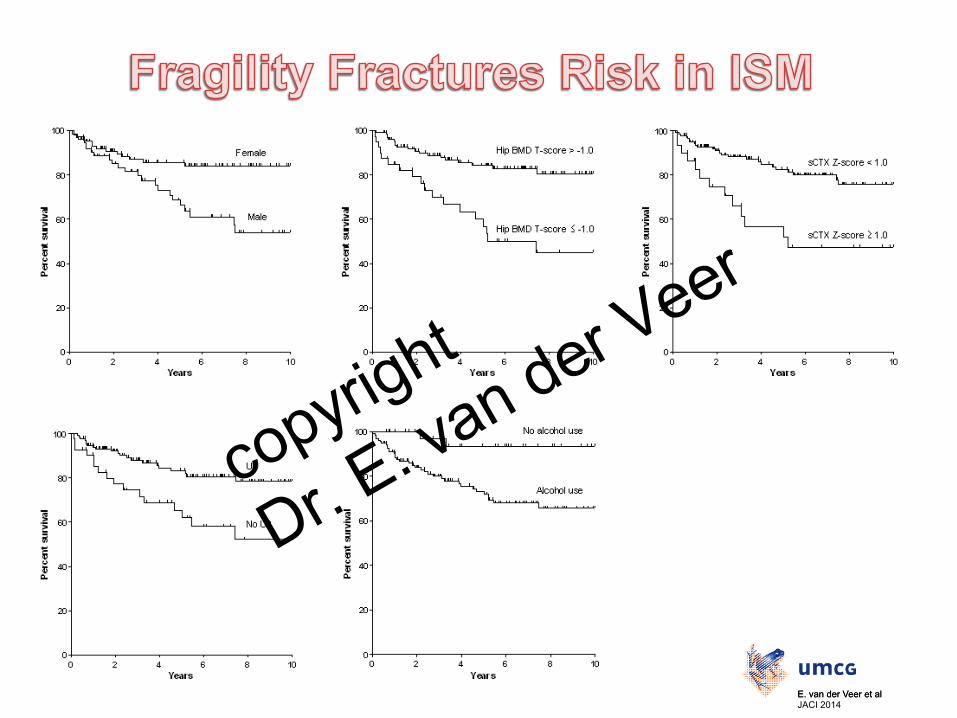
• Univariate Cox regression Patients with fragility fractures post-ISM-diagnosis were:
older more often male more often anaphylactic reactions less often UP higher levels of MIMA, osteocalcin and sCTX lower hip BMD scores reported more often alcohol intake
copyright
Dr. E. van der Veer
E. van der Veer et al E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
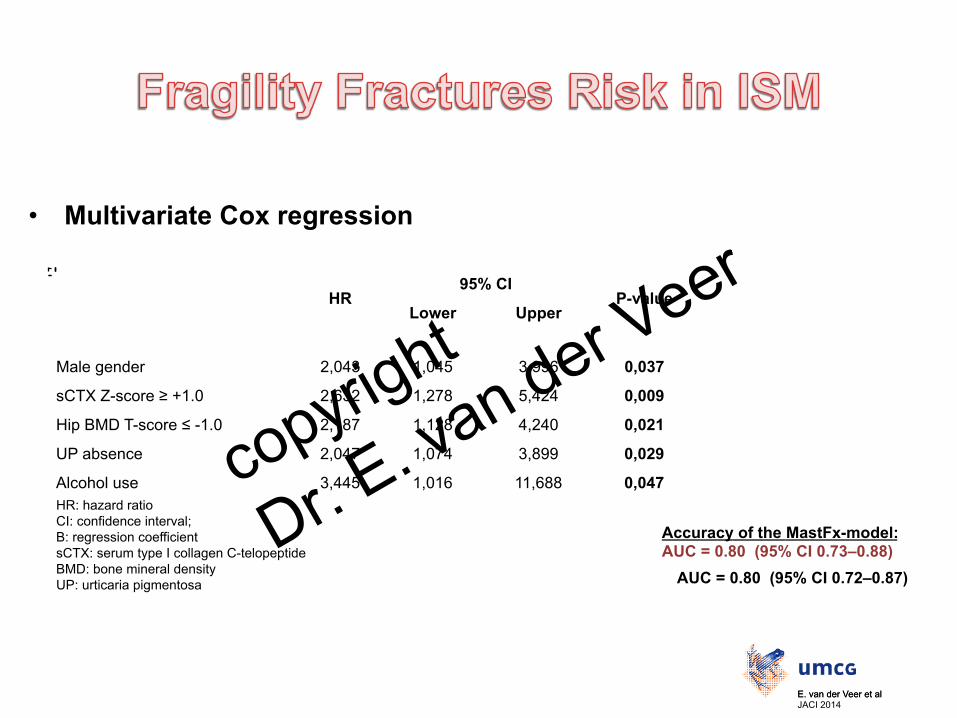
• Multivariate Cox regression HR
95% CI P-value B MastFx-
score Lower Upper
Male gender 2,043 1,045 3,996 0,037 0,715 1
sCTX Z-score ≥ +1.0 2,632 1,278 5,424 0,009 0,968 1
Hip BMD T-score ≤ -1.0 2,187 1,128 4,240 0,021 0,782 1
UP absence 2,047 1,074 3,899 0,029 0,716 1
Alcohol use 3,445 1,016 11,688 0,047 1,237 1 HR: hazard ratio CI: confidence interval; B: regression coefficient sCTX: serum type I collagen C-telopeptide BMD: bone mineral density UP: urticaria pigmentosa
Accuracy of the MastFx-model: AUC = 0.80 (95% CI 0.73–0.88)
AUC = 0.80 (95% CI 0.72–0.87)
E. van der Veer et al E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
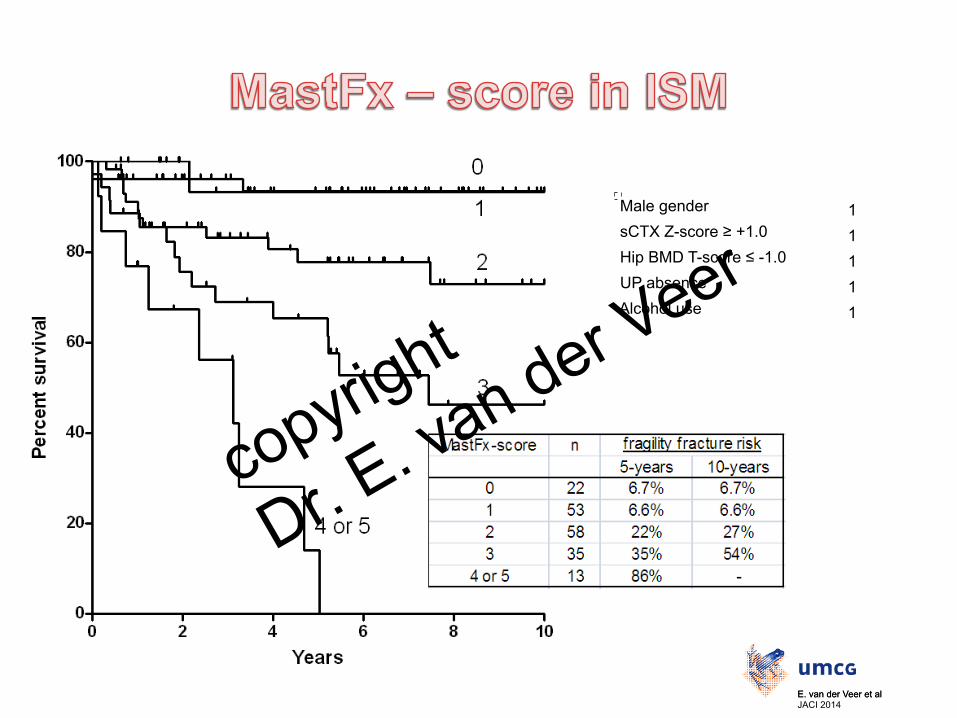
Male gender 1 sCTX Z-score ≥ +1.0 1 Hip BMD T-score ≤ -1.0 1 UP absence 1 Alcohol use 1
E. van der Veer et al E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
Prevalence Mastocytosis • The prevalence of mastocytosis was at least 13.0 cases per 100.000 inhabitants aged ≥15 years. • ISM prevalence increased with age.
Prevalence Mastocytosis • Lifetime fragility fractures were reported by 41% (90/221) of the
patients with indolent systemic mastocytosis (ISM).
• Follow-up from ISM-diagnosis to Fx data collection: – median 5.4 years (range 0.4-15.3) – 5-year fracture-free survival 77 ± 3% – 10-year fracture-free survival 69 ± 4%
E. van der Veer et al E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
• Independent predictors for future fragility fractures
– Male gender – high levels of bone resorption marker sCTX – low hip BMD – absence of urticaria pigmentosa – alcohol intake
• The MastFx-score, a prediction model using five characteristics, showed good accuracy to distinguishes ISM patients at high, intermediate and low risk for new FFx. – ISM patients with a MastFx-score of ≥2 have a high risk for fragility
fractures.
E. van der Veer et al E. van der Veer et al JACI 2014
copyright
Dr. E. van der Veer
• The calculation of the fragility fracture risk should be an important component in the management of patients presenting with ISM
• Efforts should be made by the caretakers to optimize bone quality in all ISM patients Lifestyle changes – Do exercises – Adequate vitamin D and calcium intake – Alcohol cessation is highly recommended
(because drinking is a modifiable risk factor of FFx in ISM) High-risk patients will probably benefit from an early start
of therapeutic intervention
copyright
Dr. E. van der Veer

copyright
Dr. E. van der Veer

q University of Groningen q University Medical Center Groningen q Nederlands Mastocytose Centrum Groningen
• Eveline van der Veer
• Suzanne Arends • Sjoukje van der Hoek • Joris B Versluijs • Jan GR de Monchy • Joanne NG Oude Elberink • Jasper J van Doormaal
Support your
bones
They support
you!
copyright
Dr. E. van der Veer