PROEFEXAMEN TER VOORBEREIDING OP EDIC … PROEFEXAMEN EDIC 2001 GENEVE . TER VOORBEREIDING OP HET ....
40
1 PROEFEXAMEN EDIC 2001 GENEVE TER VOORBEREIDING OP HET 13e EUROPEAN DIPLOMA IN INTENSIVE CARE (EDIC) TE GENEVE OP 3 OKTOBER 2001 Voor de Amsterdamse fellows Intensive Care Geneeskunde van het OLVG, VUMC en AMC op dinsdag 11 september 2001 van 19.00 – 21.00 uur in de Prof. dr. Ch.P. Stoutenbeekzaal van de afdeling Intensive Care van het OLVG georganiseerd door de medische staf van de afdeling Intensive Care van het OLVG J.P.J. Wester R.J. Bosman H.M. Oudemans-van Straaten J.I. van der Spoel D.F. Zandstra
Transcript of PROEFEXAMEN TER VOORBEREIDING OP EDIC … PROEFEXAMEN EDIC 2001 GENEVE . TER VOORBEREIDING OP HET ....
1
PROEFEXAMEN EDIC 2001 GENEVE
TER VOORBEREIDING OP HET
13e EUROPEAN DIPLOMA IN INTENSIVE CARE (EDIC)
TE GENEVE
OP 3 OKTOBER 2001
Voor de Amsterdamse fellows Intensive Care Geneeskunde van het OLVG, VUMC en AMC
op dinsdag 11 september 2001 van 19.00 – 21.00 uur
in de Prof. dr. Ch.P. Stoutenbeekzaal van de afdeling Intensive Care van het OLVG
georganiseerd door de medische staf van de afdeling Intensive Care van het OLVG
J.P.J. Wester R.J. Bosman
H.M. Oudemans-van Straaten J.I. van der Spoel
D.F. Zandstra
2
Ten geleide Het proefexamen EDIC 2001 Genève heeft tot doel te ervaren hoe het is om onder tijdsdruk in 2 uur 100 engelstalige meerkeuze vragen te maken. Het is een goede manier om enkele weken voor het echte examen te toetsen waar de sterke en zwakke punten van de examenkandidaten liggen, zodat in de aanloop naar het examen nog extra aandacht besteed kan worden aan de onderwerpen die minder goed beheerst worden. Dit proefexamen kent geen officieel karakter, maar poogt wel een goede afspiegeling van het EDIC te zijn. In 2 uur tijd krijgen jullie 100 engelstalige multiple choice vragen met 5 alternatieven te beantwoorden zonder verdere hulpmiddelen. De vragen zijn onderverdeeld in 3 categorieën: 25 vragen met 1 juist alternatief, 25 vragen met 1 onjuist alternatief en tenslotte 50 vragen met 5 maal juist/onjuist alternatieven. De vragen zijn deels afkomstig uit NVIC Monitor 1999;3(1-6) en NVIC Monitor 2000;4(1-3) en deels uit de VUMC syllabi Vragen & Antwoorden ter voorbereiding op het EDIC–examen te Rome en te Genève. De vragen zijn bewerkt tot het format van het EDIC-examen. De beoordeling van de vragen zal gewogen worden per alternatief en niet per totale vraag. Het uitgangspunt hierbij is 1 punt per alternatief. De 50 vragen met 5 maal juist/onjuist alternatieven kunnen zo in totaal 250 punten opleveren. De 25 vragen met 1 juist alternatief en de 25 vragen met 1 onjuist alternatief worden anders gewogen, daar blind gokken immers bij een fout alternatief al 3 punten oplevert. Het goede alternatief levert 2 punten op en de foute alternatieven 0 punten. In totaal kunnen met deze vragen 100 punten behaald worden. Van de totale hoeveelheid van 350 punten dient conform het EDIC 70% (245 punten) behaald te worden. Iedere proefexamenkandidaat krijgt zijn of haar uitslag uitsluitend persoonlijk terug. Alleen het totale groepsgemiddelde zal aan iedere kandidaat gemeld worden. Veel succes! Jos Wester Amsterdam, 11 september 2001
3
QUESTIONS WITH 1 TRUE ALTERNATIVE 1. Regarding catheter-related infection:
a. it is more common when catheters are sited in the subclavian vein than in the internal jugular vein
b. routine catheter changes decrease the incidence of catheter-related bloodstream infections
c. contamination of the hubs is an important route of colonization d. minocycline/rifampicin impregnated catheters were found to be associated with a
higher incidence of colonization and infection than chlorhexidine/silver sulphadiazine impregnated catheters
e. chlorhexidine/silver sulphadiazine impregnated double lumen hemofiltration (CVVH) catheters were demonstrated to have a lower incidence of colonization and infection than non-impregnated catheters
2. Regarding withdrawal of therapy:
a. It is a common practice in many ICUs. b. The decision to withdraw therapy should be based on the prediction of severity scoring
systems such as APACHE II and MPM II. c. Futility can be accurately predicted. d. In a survey of Swedish physicians and nurses, the chance of long term survival was
found to be a more important factor in deciding to withdraw life support than patient advance directives.
e. Age was not one of the factors rated most important in decision making 3. Regarding the guidelines for the management of traumatic brain injury:
a. raised intracranial pressure should be treated only when it exceeds 30mmHg. b. cerebral perfusion pressure should be maintained at at least 70mmHg c. hyperventilation should be used routinely d. following these guidelines does not improve control of intracranial pressure in
comparison with ad hoc critical care physician guidance e. none of the above is true 4. Regarding femoral venous lines:
a. central venous pressure measured by this route is not an accurate reflection of intrathoracic central venous pressure in mechanically ventilated patients.
b. are associated with a five times relative risk of deep venous thrombosis. c. when used to measure central venous pressure a long catheter should be used so that
the tip lies close to or above the diaphragm. d. the rate of colonization by micro-organisms is reduced by tunnelling. e. Gram negative rods do not play a significant role in colonization of central venous
femoral catheters
4
5. With regard to nitric oxide:
a. administration to adults with ARDS leads to a reduction in mortality b. administration to adults with ARDS results in an improvement in respiratory function c. it may result in nitrogen dioxide toxicity d. an improvement in outcome for children with acute respiratory failure who received
nitric oxide is demonstrated e. all of the above are false
6. Growth hormone:
a. administration of growth hormone has no effect on nitrogen balance in critically ill
patients b. an adequate source of glutamine appears to be important for growth hormone to be
effective c. adverse effects include hypocalcaemia d. routine administration of growth hormone to critically ill patients is associated with
decreased mortality. e. administration of growth hormone does not effect the immune system
7. Spontaneous bacterial peritonitis (SBP):
a. occurs predominantly in patients with acute hepatitis b. is characterised by abdominal rigidity c. is usually associated with a ascitic fluid white cell count > 10 000/ml d. is associated with a lower incidence of renal impairment in patients treated with
albumin as well as cefotaxime e. SBP probably does not originate with bacterial spread from the intestinal lumen via
the systemic circulation to the ascetic fluid 8. Octreotide:
a. the recommendation to fast patients with acute pancreatitis is not based on good
clinical evidence b. Ranson's criteria can be used to predict severe pancreatitis with high specificity. c. ERCP is indicated in all patients with acute pancreatitis and biliary stones d. administration of octreotide to patients with moderate to severe acute pancreatitis
improves outcome e. octreotide is a synthetic analogue of somatomedine-C 9. Gut barrier function:
a. disaccharide absorption test results correlate well with other measures of intestinal permeability
b. increased intestinal permeability has never been demonstrated to be associated with increased morbidity in critically ill patients
c. enteral feeding has been shown to reduce intestinal permeability in critically ill patients
d. a clear relationship is demonstrated between bacterial translocation and septic complications in humans
e. the thoracic duct is a major route of bacterial translocation in patients with MODS
5
10. The classic (topical and systemic) SDD regimen consists of: a. Belcomycin, polymyxin E, amphotericin B, Rocephin b. Colimycin, polymyxin E, amphotericin B, Rocephin c. polymyxin E, tobramycin, amphotericin B, cefotaxim d. colistin, Obracin, Fungizone, Claforan e. colistin, Obracin, Nystatin, ceftriaxon 11. Which is not a common sign of Legionella pneumoniae pneumonia?
a. high fever b. myalgia c. hypernatraemia d. confusion e. diarrhea
12. Which of the following is the most common cause of the metabolic acidosis that occurs after
kidney-pancreas transplant?
a. lactic acidosis b. uremic acidosis c. ketoacidosis d. renal tubular acidosis e. pancreatic secretion loss
13. A 30 year old man presents with hemoptysis, dyspneu and generalised weakness. He has no
upper airway symptoms. Physical examination: pallor and basilar crackles; Lab: hemoglobin 7.8 g/dl (4,8 mmol/l), creatinin 3,0 mg/dl (240 µmol/l), microscopic haematuria and hypoxemia. Chest X ray: bilateral alveolar infiltrates; He needed intubation and mechanical ventilation.
Which one of the following tests would be most helpful at this point?
a. percutaneous kidney biopsy b. surgical lung biopsy c. otolaryngology consult to look for lesions in the upper respiratory tract d. serum assays for ANCA-antibodies e. serum assays for ANA
14. In patients with ARDS prone position ventilation improves oxygenation. Which of the
following statements is proven to be true?
a. the improvement is completely a result of an increased FRC b. the improvement is a result of differences in diafragm movement and abdominal
pressure c. there is a redirection of perfusion to better ventilated ventral lung regions d. there is a better clearance of secretions e. prone position ventilation results in a better outcome and survival
6
15. Which of the following is the most frequent cause of ARDS in the ICU population?
a. multiple transfusions b. diffuse pulmonary infections c. sepsis d. near drowning e. thoracic trauma
16. In ARDS nowadays lung protective strategies are followed in order to reduce the occurence of
VILI. Which of the following strategies will lead to decreased mortality?
a. volume-limited ventilation b. increased PEEP levels (open lung concept) c. inverse-ratio ventilation d. prone position e. ECMO; extra corporal carbon dioxide removal
17. The diagnosis of pulmonary embolism in a mechanically ventilated ICU patient can be most
adequately be made by: a. arterial blood gas analysis b. echocardiography c. according to the diagnostic work-up of the Dutch CBO consensus on Diagnosis of
Pulmonary Embolism d. pulmonary angiography e. increase in pACO2-paCO2 difference
18. Statements on cerebrospinal fluid:
a. the production of cerebrospinal fluid is 180 ml per 24 hour b. total fluid in cerebrospinal fluid system is 120-180 ml c. liquor is produced in the arachnoidal villi d. In meningitis glucose in liquor is high and protein is low. e. The Queckensted maneuver is positive when there is a disturbed passage of liquor
between cerebrum and lumbar puncture site 19. Statements about the thyroid gland:
a. peripheral conversion of T4 to T3 is the only source of T3 b. in the sick euthyroid syndrome reverse T3 concentration is low and T3 concentration
is in the normal range c. reverse T3 is a more biologically active hormone than T3 d. amiodarone can induce hyperthyroidism as well as hypothyroidism e. beta adrenergic blocking drugs stimulate T4 to T3 conversion
20. Statements concerning diabetic keto-acidosis:
a. there is always an insulin deficiency b. it can only occur in patients with type I diabetes mellitus c. it is characterized by hyperglycemia, acidemia and low bicarbonate levels d. it is often associated with hypernatremia e. treatment exists of administering insulin
7
21. Which of the following statements concerning thermoregulation is true?
a. the body temperature that the thermoregulatory thermostate weighs and reacts to, is determined in a comparable manner by the core temperature and by the skin temperature
b. shivering thermogenesis occurs sooner (i.e. at a smaller decrease of temperature) than non-shivering thermogenesis, but later than vasoconstriction
c. the vasoconstrictive response to cold is impaired in neonates d. clonidine is effective against postoperative shivering e. transmission of ‘coldness’ information is channelled by the non-myelinised C-fibers
22. Which of the following statements concerning hypothermia is true?
a. the blood temperature as measured with a pulmonary artery catheter is equal to the brain temperature
b. the initial hemodynamic profile in hypothermia is characterised by hypovolemia, a decrease in stroke volume, and bradycardia
c. hypothermia is accompanied by a prolonged APTT but a normal thrombocyte function d. coagulation tests should be adapted in a hypothermic patient
e. the urine of a hypothermic patient has a low osmolality 23. An hypertensive crisis in a pheochromocytoma can be treated adequately with: a. captopril b. phentolamine c. nifidepine d. losartan e. furosemide 24. The most common cause for pathological increased intracranial pressure is: a. meningo-encephalitis b. spontaneous intracranial bleeding c. fulminant hepatic failure d. trauma capitis e. XTC-induced cerebral oedema 25. Statements regarding clinical and toxicological aspects of ecstacy (MDMA): (true/false)
a. MDMA is an indirect serotonine antagonist. b. repeated use of MDMA leads to functional disturbances of the neuro-endocrine system
for at least 12 months. c. the acute somatic complications involve hyperthermia, hypernatriemia and renal
failure. d. when acute liver failure is present, transplantation is successful. e. prozac does not give protection to the neurotoxic effects of XTC.
8
QUESTIONS WITH 1 FALSE ALTERNATIVE 26. Concerning herpes simplex virus (HSV) encephalitis: a. early treatment with aciclovir is crucial
b. temporal lobe focal abnormality with high-voltage spike and slow-wave complexes on EEG is highly suggestive of HSV encephalitis
c. abnormalities in the temporal lobe are visible on CT in most patients d. mortality appears to be lower in children
e. early diagnosis can be made by detection of small amounts of HSV DNA in the cerebrospinal fluid by polymerase chain reaction
27. Regarding carbon monoxide poisoning:
a. elimination half-time of CO is reduced from 250 minutes when breathing air to 59 minutes breathing 100% oxygen
b. neuropsychiatric complications may develop weeks after exposure c. cherry red appearance of the skin is common
d. in a randomised controlled double blind clinical trial in a pressure chamber, hyperbaric oxygen (HBO) therapy has been shown to be ineffective in improving short term neuropsychiatric outcome in comparison with normobaric oxygen (NBO) therapy
e. the incidence of claustrophobia was higher in the HBO than in the NBO group 28. Regarding oxygen delivery and consumption:
a. mathematical coupling may occur if oxygen consumption is measured by the reverse Fick method
b. the point at which oxygen consumption becomes delivery-dependent may be as low as 4 ml/min/kg in septic patients
c. previous studies have demonstrated that increasing oxygen consumption by increasing oxygen delivery in high-risk surgical patients preoperatively is associated with an improved outcome
d. the effect of raising cardiac index, oxygen delivery and consumption to supraphysiological levels in sepsis and septic shock, is inconclusive
e. failure to achieve the oxygen delivery target value may be due to starting the intervention too late in the course of sepsis
29. With reference to ARDS:
a. surfactant therapy has been proven to reduce mortality b. the American-European consensus definition requires a PO2/FIO2 ratio <200 mm Hg c. inhaled nitric oxide has not been shown to improve outcome d. direct damage to surfactant-specific proteins may most likely occur by proteolysis e. surfactant is a mixture of phospholipids and surfactant-specific proteins
30. Regarding cardiac arrest:
a. cardiac arrest within a few days of myocardial infarction is associated with a good outcome
b. associated with malignancy has a poor outcome in all series c. ventricular fibrillation is associated with a better outcome than asystole
d. it is possible to identify a group of inpatients that have no chance of survival to hospital discharge
e. a resuscitation decision rule can only be introduced in clinical practice after prospective validation
9
31. Regarding ceftazidime: a. it is not a useful drug in late onset hospital acquired pneumonia because of low
activity against Pseudomonas aeruginosa b. it has time-dependent killing characteristics for Gram negative organisms c. it may cause thrombocytopaenia d. its pharmacokinetics may be altered in critically ill patients e. its effect is independent of high peak levels
32. With regard to Pseudomonas aeruginosa:
a. there are strains which are resistant to every anti-microbial used to treat it. b. it is an important cause of nosocomial infection c. it is suggested that serious infection should be treated with two anti-Pseudomonal
agents concurrently d. high level of evidence states that colistin may be a suitable agent for treating multi-
resistant strains e. the main adverse effect of i.v. colistin is nephrotoxicity
33. With regard to cardiogenic shock:
a. severe hypotension due to cardiogenic shock should be treated with vasoconstrictors
initially b. thrombolysis for acute myocardial infarction (AMI) is more effective in patients with
cardiogenic shock c. in a patient with an inferior MI cardiogenic shock should alert the clinician to the
possibility of right ventricular infarction d. emergency revascularization by CABG or angioplasty is associated with a lower 6
month mortality e. cardiogenic shock complicates 7-10% of cases of AMI
34. Amiodarone:
a. has Vaughan-Williams class I, II, III and IV actions. b. is a coronary vasodilator c. is predominantly eliminated by the kidneys d. may increase survival in out-of-hospital cardiac arrest
e. it strongly potentiates the effect of coumadins 35. Venous thromboembolism:
a. the incidence of venous thromboembolism in ICU patients is estimated to be 10-13% b. anticoagulation with low molecular weight heparin can be monitored using a factor Xa
assay c. venography is the "gold-standard" method of demonstrating deep venous thrombosis d. low molecular weight heparin is not effective in preventing venous thromboembolism
in acutely ill medical patients. e. the use of gradual compression elastic stockings is advocated in critically ill patients
with paraplegia
10
36. Levofloxacin:
a. inhibits DNA gyrase and topoisomerase IV b. has time-dependent killing characteristics c. has greater activity against pneumococcus than ciprofloxacin d. may be as effective as imipenem/cilastatin in the empiric treatment of suspected
bacteraemia/sepsi e. the bioavailability of levofloxacin is comparably good when administered orally or
intravenously 37. Critical illness polyneuropathy (CIPNP):
a. occurs in up to 70% of patients who spend >5 days in the ICU b. sensory signs predominate c. the absence of cranial nerve involvement helps to distinguish it clinically from
Guillain-Barré syndrome d. a significant proportion of severely affected patients suffer long term disability. e. there is little evidence that the use of corticosteroids or neuromuscular blocking agents
are associated with CIPNP in absence of myopathy 38. Treatment of delayed neurological deficit may include the use of:
a. calcium antagonists b. Hypertension, Hypervolaemia and Hypothermia (triple-H therapy) c. barbiturate coma to burst suppression d. angioplasty e. intrathecal sodium nitroprusside
39. Some questions about cytokines:
a. TNF-α is an anti-inflammatory cytokine b. TNF-α is the first cytokine that enters the circulation in SIRS c. IL-1 and TNF-α have a synergistic effect d. IL-10 is an anti-inflammatory cytokine e. locally produced TNF-α is an important defense mechanism against infections
40. External cardiac massage can be complicated by?
a. pulmonary aspiration b. rupture of the liver
c. rupture of the spleen d. renal injury e. haemopericardium
41. The diagnosis cardiogenic shock can be mimicked by other conditions that resemble shock.
Which of the following conditions can resemble or mimick cardiogenic shock?
a. pneumothorax b. pericardial tamponade c. ruptured aorta d. nitrate overdose e. potassium overdose
11
42. Addition of a PEEP of 10 cm H20 to a high pressure ventilation with a peak pressure of 45 cm H20 results in:
a. a decrease in intra-alveolar oedema b. an increase in surfactant availibility c. a decrease in alveolar permeability
d. addition of dopamine to increase systemic arterial pressure results in increased intra-alveolar oedema
e. a further increase in PEEP keeping tidal volume constant results in increased oedema formation
43. Acalculous cholecystitis in IC patients can be associated with:
a. gallbladder ischemia b. bile stasis in the absence of stimuli for emptying the stomach c. PEEP d. parenteral nutrition e. bacterial invasion
44. Breathing or mechanical ventilation influences through cardiopulmonary interaction: a. the afterload of the right ventricle b. the preload of the right ventricle c. the contractility of the heart d. the preload of the left ventricle e. the afterload of the left ventricle 45. Statements concerning classical heat stroke:
a. besides hyperthermia and neurological disturbances, the patient typically presents with anhydrosis
b. lactic acidosis occurs frequently c. survival is inversely related with the length of time of hyperthermia and does not
correlate with the initial core temperature d. dantrolene does not improve the outcome in these patients e. a careful rehydration management is indicated 46. Shortness of breath during pregnancy can be caused by: a. mitral valve stenosis b. pulmonary embolus c. cardiomyopathy d. pulmonary hypertension of pregnancy e. ketosis due to hyperemesis gravidarum 47. In acute liver failure
a. coagulopathy is common and should be corrected with platelet and fresh frozen
plasma b. hepatopulmonary syndrome is reversible with PEEP c. the cause of liver failure is the most important predictor of survival d. is associated with high circulating levels of insulin e. paracetamol poisoning typically produces a centrilobular pattern of hepatocyte
necrosis
12
48. Statements concerning heparin-induced thrombocytopenia (HIT): a. HIT is regarded as the most frequent drug-induced thrombocytopenia b. HIT can not originate from the use of low-molecular-weight heparins (LMWH)
c. danaparoid sodium is the drug of first choice in the treatment of venous or arterial thrombosis in HITT
d. danaparoid sodium has an in vivo 5-10% cross-reactivity with antibodies to heparin/platelet factor 4
e. the incidence of HIT in ICU patients is unknown 49. Veno-venous hemofiltration: a. predilution decreases the ultrafiltration rate
b. the incidence of adverse effects is high when prostacyclin is used as the sole anticoagulant
c. heparin resistance is usually due to an acquired antithrombin III deficiency d. the use of high ultrafiltration rates is associated with improved uotcome e. very high ultrafiltration rates (6 liters/hour) have only been tested in animal models 50. Experimental studies in acute non-haemorrhagic stroke show: a. lubelazole may improve functional outcome if given within 6 hours b. streptokinase causes unacceptably high rates of intracerebral haemorrhage c. rtPA may improve functional outcome if given within 3 hours d. rtPA improved outcome at 60 days when given within 6 hours e. reperfusion injury after thrombolysis may increase morbidity and mortality
13
QUESTIONS WITH 5 ALTERNATIVES TRUE OR FALSE 51. Amphotericin:
a. dose should be reduced in patients with pre-existing renal function disturbances b. acts on the cell wall c. may cause a renal tubular defect d. nephrotoxicity has been demonstrated to be reduced by low-dose dopamine in bone
marrow transplant patients e. nephrotoxicity has been demonstrated to be reduced by low-dose dopamine in ICU
patients 52. Enteral feeding of critically ill patients:
a. reduces villous atrophy in the small intestine b. improves intestinal permeability
c. should not be attempted until bowel sounds are present d. is poorly tolerated if given in the first 24 hours after major surgery
e. postoperative enteral feeding supplemented with arginine and omega-3 fatty acids reduces the incidence of postoperative infections
53. Concerning ventilator associated pneumonia (VAP):
a. Pseudomonas aeruginosa infection is common b. the clinical features are highly specific c. it has been firmly established that H2 blockers do not increase the incidence d. use of paralyzing agents to facilitate mechanical ventilation has been found to be
associated with an increased incidence of VAP e. burns are not an independent risk factor for VAP
54. Regarding croup:
a. the decision to intubate a child with croup should be based on arterial blood gas results b. croup is always due to viral infection c. nebulised adrenaline usually provides temporary relief d. there is evidence that nebulized budesonide and oral dexamethasone are equally
efficacious for the treatment of mild to moderate severe croup e. regarding cost-effectiveness, nebulized budesonide is the drug of first choice
55. Concerning tirilazad mesylate:
a. it is a 21-aminosteroid b. its mode of action is thought to be by inhibition of lipid peroxidation c. in a dose of 2.5 mg/kg 6 hourly for 48 hours it leads to a greater improvement in
outcome than methylprednisolone 5.4 mg/kg/h for 48 hours in traumatic spinal cord injury in humans
d. in a dose of 2.5 mg/kg 6 hourly for 48 hours it leads to a greater improvement in outcome than methylprednisolone 5.4 mg/kg/h for 48 hours in ischemic spinal cord injury in humans
e. it has been shown to improve outcome following traumatic brain injury
14
56. Concerning lactate:
a. blood concentrations are a good guide to tissue hypoxia in sepsis. b. therapy titrated against blood concentrations improves outcome. c. the liver is the major site of blood lactate clearance. d. serum lactate concentration is independently associated with early hepatic
dysfunction. e. lactate acidosis can be induced by metformin 57. With regard to meningococcal disease:
a. samples for microbiological culture should be taken prior to the administration of antibiotics
b. case reports of protein C and antithrombin III administration in adults strongly suggest a beneficial effect
c. a fulminant course is common d. a study in the Netherlands indicates that the risk of contracting meningococcal disease
is far higher amongst people with complement deficiency e. in complement-deficient patients, C3-deficiency accounts for most of the deficiencies 58. Acute colonic pseudo-obstruction:
a. occurs in 1.5% of renal transplant recipients b. may be complicated by colonic perforation c. is conventionally treated by colonoscopic decompression d. may respond beneficially to neostigmine e. neostigmine is an acetylcholinesterase inhibitor
59. Ventilator associated pneumonia (VAP):
a. in patients hospitalised for more than 5 days should be treated with two anti-
Pseudomonal agents initially, according to American Thoracic Society guidelines b. is associated with severe underlying disease c. is difficult to diagnose with certainty d. the aetiology varies markedly from hospital to hospital e. antimicrobial prescription practice for VAP should be based on up-to-date information
of the pattern of multiresistant isolates in a specific ICU 60. Selective decontamination of the digestive tract (SDD) is one of the most studied
interventions in Intensive Care Medicine, but its application still remains controversial. Which of the following can be regarded as historical landmarks?
a. shortly after the discovery of penicillin, Fleming observed in 1951 the broad
bactericide spectrum of the non-absorbable procaςnbenzylpenicillin against Gram-negative intestinal bacteria
b. SDD is based on the concept of colonization resistance as described by Van der Waay in 1971
c. SDD is based on the concept of selective decolonization sensitivity as described by Van der Waay in 1971
d. the first succesful application of SDD was in non-ICU granulocytopenic patients by Van der Waay in 1980
e. the first succesful application of SDD in ICU patients was in 1984 by Stoutenbeek in haematological ICU patients with refractory leukemia
15
61. Intubated patients are frequently sedated: true or false?
a. more than 80 % of intubated patients are routinely sedated in ICU’s. b. in most hospitals depth of sedation or efficacy of medication are frequently monitored. c. sedation can have adverse effects on the nervous system. d. agitation in patients is only deleterious for doctors and nurses. e. todate, there are not yet objective scoring systems to assess depth of sedation.
62. Statements concerning amino acids:
a. arginine is a non essential amino acid b. arginine promotes insulin and glucagon release c. glutamine is a neurotransmitter d. glutamine is the primary metabolic substrate for lymphocytes and macrophages e. glutamine is an essential amino acid
63. O2 forms an easily reversible combination with Hb to give oxyhemeglobin. Many factors
influence the O2 dissociation curve. The following factors shift the curve to the right:
a. increased temperature b. increased pCO2 c. increased 2,3 DPG d. the presence of CO e. increased pH
64. Which techniques can be used to determine the amount of extravascular lung water?
a. ventilation/perfusion scan b. chest X-ray c. CT scan d. thermodilution double indicator method e. double radiotracer indicator dilution
65. Statements concerning fluid replacement:
a. in septic patients infusion of 1000 ml of NaCl 0,9% will lead to the following redistribution: 25% will stay intravascular and 75% extravascular
b. of a 1000 ml glucose 5% infusion 85 ml will stay intravascular c. prolonged infusion of HES can lead to a lowering of coagulation factor VII d. HES 200/0,6 has a shorter halflife than HES 200/0,5 but a longer half life than HES
450/0,7 e. both dextrans as HES can lead to a coagulopathy.
66. Questions about other mechanisms in sepsis:
a. nitric oxide (NO) is produced by endothelium, smooth muscle and monocytes and produces vasodilation
b. in sepsis cNOS is stimulated c. methylene blue is a L-arginine analogon and inhibits guanylaat cyclase d. circulating levels of ICAM and VCAM seem to be high in sepsis e. prostacyclin is a vasodilator and inhibits platelet aggregation
16
67. Questions about pathophysiology of shock:
a. the renine-angiotensine-aldosteron-system (RAAS): in shock the decrease in renal flow is detected by the macula densa. As a response on this the juxtaglomerulal cells produce angiotensinogen
b. angiotensin I is actived by ACE in the lungs c. infection with beta-haemolytic streptococ can result in toxic shock syndrome d. sepsis/septic shock in S. aureus infection is caused by an endotoxin e. when LBP binds with free endotoxin it forms a complex which is a much more potent
inflammatory stimulant than endotoxin alone. 68. Toxic shock syndrome (TSS) is a multisystem disorder manifested by high fever, hypotension
and erythrodermia. Are the following statements about TSS right or wrong?
a. the bacterial etiology are streptococci b. TSS is limited to young menstruating female c. the absence of preexisting antibody against TSS toxins is associated with TSS d. complications are hepatitis and rhabdomyolysis e. intravenous gamma-globulin should be used in the treatment
69. Statements about pathological supply dependency during septic shock:
a. the oxygen extraction is impaired b. SvO2 is decreased c. Ca-vO2 is narrowed d. VO2 is often decreased e. the slope of the VO2/DO2 relationship is flattened and moved to the right
70. What factors contribute to Gram-negative sepsis? a. endotoxin, the bacterial lipopolysaccharide (LPS)
b. by interacting with macrophages the release of TNF, IL-1, IL-6 are stimulated c. complement and clotting cascades are activated d. production of bacterial super antigens (toxins) activates T-cell receptors of a large
percentage of circulating leucocytes e. cytochrome c is released, thereby directly stimulating apoptosis
71. Acute toxicologic emergencies are often a reason to start advanced cardiovascular life support.
Are the following statements true or false?
a. cocaine use is associated with serious atrial arrythmias and acute myocardial disease b. tricyclic overdose can lead to hypotension and ventricular arrythmias c. opiate overdose may lead to myocardial infarction d. alcohol abuse may lead to sudden death e. nicotine overdose can contribute to ventricular fibrillation
72. Resuscitation guidelines 2000: Pharmacology of resuscitation:
a. lidocaine and adenosine are recomended for the initial treatment of hemodynamically stable widecomplex tachycardia
b. amiodarone is a good first-choice antiarrhytmic for shock-refractory VF/VT c. calcium is effective in the treatment of torsades de pointes d. high dose epinephrine improves survival in cardiac arrest e. vasopressin may be a more effective pressor agent than epinephrine for promoting the
return of spontaneous circulation in cardiac arrest.
17
73. Statements on postresuscitation care:
a. positive bloodcultures with Gram-negative rods after after succesful resuscitation are strong evidence for a septic shock
b. splanchnic perfusion can be monitored with tonometry by measurement of the systemic:gastric mucosal pCO2 gradient. Postresuscitation one can expect an increase of the systemic:gastric mucosal pCO2 gradient
c. the cerebral metabolic rate increases approximately 8% per degree Celsius d. hypothermia postresuscitation should be treated with active warming
e. hyperventilation with hypocarbia during the period of delayed hypoperfusion may worsen cerebral ischemia.
74. Hepatic encephalopathy may be due to:
a. an increase in brain glutamine b. reduced CBF c. a loss of cerebral autoregulation d. a reduction in the cerebral metabolism of oxygen and glucose e. an underlying oxygen debt
75. Statements about stress ulcer prophylaxis:
a. gastric erosions are present in up to 30% of patients on admission to the ICU b. the incidence of clinically important bleeding from stress ulceration is 1.5-2.5% c. the presence of luminal gastric acid is essential in the pathogenesis d. enteral feeds protect against stress ulceration e. stress ulcer prophylaxis increases the risk for nosocomial pneumonia
76. Statements concerning acute liver failure:
a. worldwide, paracetamol-induced hepatotoxicity constitutes the most common cause of ALF
b. factor VII is used in the Clichy Criteria for liver transplantation c. in hepatorenal syndrome urine sodium is low d. hypoglycaemia is due to a failure of hepatic glucogenolysis e. inhibition of Na/K-ATPase may contribute to cerebral oedema
77. Statements concerning the pathophysiology of ARDS:
a. Diffusion impairment is an important cause of hypoxaemia b. An increase in PVR is a feature c. Lymphocytes are the most important source of cellular inflammatory mediators d. The early hyaline membrane is composed primarily of collagen e. Inflammatory edema is generally evenly distributed throughout the lung parenchyma
from sternum to vertebrae. 78. Statements concerning the prone position in the treatment of ARDS: a. 80% of patients are likely to have a good response as signified by an increase in PaO2
b. Re-direction of perfusion to the aerated and now dependant ventral regions of the lung is primarily responsible for the observed increase in PaO2
c. Secretion removal is generally enhanced d. Reciprocal increases in the density of the ventral regions of the lung are usually
observed after a period of time, reducing the effectiveness of the prone position. e. The gravitational gradient in Ppl is abolished in the prone position.
18
79. Respiratory support in status asthmaticus and COPD:
a. Due to air trapping in COPD there is decrease in FRC b. The amount of air trapping can be assessed by measuring VEI (= end inspiratory
volume) c. In obstructive pulmonary disease the alveoli have a short time constant. d. Due to airtrapping in COPD there is intrinsic PEEP (PEEPI); that’s why PEEP given
by the ventilator is contraindicated e. patients with acute asthma have to be ventilated with low frequency, low tidal
volumes. 80. Statements concerning fever in the ICU:
a. Fever is caused by an increased synthesis of prostaglandin E2 which acts on the pre-optic region of the anterior hypothalamus
b. In fever oxygen consumption increases by approximately 5% per degree Celsius. c. Patients with “late”ARDS can develop fever in the absence of pulmonary infection
due to an inflammatory fibrotic proces in the lungs. d. Enterococci are the most common infecting (and colonizing) organisms in catheter
associated sepsis. e. The most common ICU-acquired infection is catheter-related sepsis.
81. Statements concerning hypothermia and hyperthermia:
a. At temperatures below 31 degrees Celsius often a J-wave or Osborne wave is seen on the ECG
b. Cold diuresis/polyuria in hypothermia is caused by an inappropriate antidiuretic hormone production.
c. Ventricular fibrillation at temperatures below 28 degrees Celsius can usually be treated succesfully with defibrillation.
d. In severe hypothermia (core temperature below 28 degrees Celsius) complicated by cardiac arrest cardiopulmonary bypass appears to be an efficacious rewarming technique.
e. In the treatment of neuroleptic malignant syndrome dantrolene can be used to prevent muscle contraction.
82. The symptoms of the classical fat embolism syndrome are the following:
a. Petechial rash, pulmonary distress, mental disturbances, pelvic or long bone fracture. b. Petechial rash, hypovolaemic shock, mental disturbances, pelvic or long bone fracture. c. Petechial rash, hypovolaemic shock, pulmonary distress, mental disturbances, recent
pelvic or long bone fracture. d. Petechial rash, pulmonary distress, mental disturbances, recent pelvic or long bone
fracture. e. Petechial rash, MOF, recent pelvic or long bone fracture.
83. Traumatic aorta disruption:
a. Is usually seen after a relatively mild trauma b. Is more often lethal in younger than more elderly persons c. Is diagnosed quite easily by a broadened mediastinum on the chest X-ray d. Can be diagnosed on examination by a discrepancy of left and right arm blood
pressure e. Must be confirmed by angiography (gold standard)
19
84. Statements about the abdominal compartment syndrome (ACS):
a. Intra-abdominal pressure (IAP) is normally 0 mm Hg or slightly subatmospheric in the spontaneously breathing patient.
b. Intra-abdominal hypertension (IAH) is defined as an increased IAP >25 mm Hg c. Morbidly obese patients with normal compliant abdominal walls do not tolerate IAH
better than nonobese patients. d. A compartment syndrome occurs when the pressure within a closed anatomic space
increases to the point that vascular inflow is compromised and the function and viability of the tissues within the compartment are threatened.
e. Deep venous thrombosis of the lower extremities, pulmonary embolism, and cholestasis are features of ACS.
85. Regarding critical illness polyneuropathy:
a. disuse atrophy is the major reason for weakness b. demyelination is the usual neuronal pathology detected c. nerve biopsy is the best investigation d. High dose steroids have been associated with a rapid onset (≤ 48 hours) acquired
myopathy e. Onset of the condition is often detectable in the first 72 hours after ICU admission
with sepsis. 86. Regarding severe traumatic brain injury:
a. more than 50% of patients require urgent craniotomy b. a single reported episode of hypotension doubles the risk of mortality c. if possible, an ICP monitoring catheter should be placed on the same side as any focal
lesion d. SjO2 may be useful in establishing the preservation of autoregulation e. If other injuries allow it, the head should be raised to 45 degrees to help reduce ICP.
87. Regarding care of the brainstem dead patient awaiting organ harvest:
a. Thyroxine supplementation is recommended b. Cortisol deficiency is usual and hydrocortisone is given as standard c. The doses of adrenergic inotropes is unimportant as long as a reasonable MAP is
maintained d. DIC is common and should be taken into account in the management of donation e. Hypothermia is more commonly seen than hyperthermia
88. A few questions on brain death diagnosis:
a. The first definition of brain death ocurred in 1968 at Harvard Medical School in order to meet the ethical issues incurred by the demand of organ donors to install an effective transplant system
b. Examining the cough reflex tests the afferent function of the N vagus (N.X) and the efferent function of the N. glossopharyngeus (N.IX)
c. If an intoxication with a known substance has occurred, which can not be quantified, the patient should be observed four times the elimination half-life of the substance.
d. Nonfilling of the intracranial arteries during a cerebral angiogram is due to perivascular swelling and the formation of subintimal blebs caused by ischemia of the carotid and vertebral arteries.
e. A full oculomotoric paralysis may cause the eye to deviate inferiorly and laterally („down and out“).
20
89. Statements about cerebral vascular autoregulation:
a. Causes CBF to be constant over a range of CPP from about 60 to 100 mmHg. b. The CPP range of autoregulation in chronic hypertension is decreased.
c. Has a delay of about 1.5 to 2 minutes.
d. Can be overruled by hypercarbia and hypoxia. e. Is always disturbed as a global disfunction of the cerebral vessels.
90. Statements concerning the diagnosis and treatment of SAB:
a. on CT the most blood is seen in the basal cisternes, sometimes with an intracerebral or intraventricular component
b. a hematoma around the fissura Sylvii indicates an aneurysm of the a. cerebri media. c. when clinical suspicion for SAB is present a negative CT should lead to a LP as soon
as possible. d. Cyklokapron should be given to those patients who are not operated early and who
have been admitted within 3 weeks after the last SAB e. More than 50% of patients have ECG abnormalities
91. Statements about pre-eclampsia and HELLP-syndrome:
a. When microangiopathic hemolytic anemia in HELLP syndrome is suspected, a peripheral blood smear possibly can give a clue.
b. In 30% of cases, HELLP syndrome occurs within 48 hours postpartum. c. HELLP syndrome is always accompanied by arterial hypertension d. Trombocytopenia in HELLP is always due to disseminated intravascular coagulation. e. The antihypertensive efficacy of ketanserin seems to be comparable with the efficacy
of dihydralazine. 92. Regarding acute MDMA (ecstasy; XTC) toxicity:
a. The severity of the response is dose related b. Acute hyperthermia is probably a central effect of serotonin c. Dantrolene is an effective treatment in cases of severe hyperthermia d. Hyponatraemic encephalopathy is caused by excessive fluid consumption in the
absence of significant losses. e. Rhabdomyolysis is a well known complication
93. Regarding hypothyroid coma (myxedema coma):
a. Altered mental status and hypothermia are cardinal symptoms b. Hypernatremia secondary to dehydration is usual c. Broad spectrum antibiotic cover should be started prophylactically before culture
results are known d. Large doses of T3 have been associated with a high mortality e. A low dose dopamine infusion is a suitable treatment for hypotension
21
94. Statements regarding adrenal insufficiency:
a. Control of secretion is regulated by the pituitary gland b. The secretion varies during the day, cortisol is higher in the afternoon than in the
morning c. The symptoms are diarrhea, fever, orthostatic dizziness, flank pain, fatigue, and
weakness d. The most common laboratory abnormality is hyponatremia e. It is often seen in patients with metastatic cancer
95. Statements concerning thyroid storm:
a. Patients have multiple manifestations: fever, tachycardia, cardiac arrhythmias, nausea, headache
b. Treatment can only be started after laboratory results are clear c. Treatment consists of propylthiouracil, iodine, dexamethason and propranolol d. Mortality rate is 50% e. Pheochromocytoma is common in patients suffering from thyroid storm
96. In ARDS the following factors are contributing to the disturbed gas exchange:
a. venous admixture b. increased anatomical shunt c. high dead space ventilation d. diffusion disturbance e. fatigue of breathing musculature
97. Interventions which can probably contribute to the decrease of pulmonary oedema in ARDS:
a. diuretics b. ultrafiltration c. dobutamine d. mechanical ventilation e. digoxine
98. Ventilator-associated lung injury is caused by:
a. too high end-expiratory pressure b. too high peak inspiratory pressure c. too large tidal volume d. intermitterent manual compression with the Water’s set e. too high breathing frequency
99. ARDS in critically ill obstetric patients occurs in:
a. HELLP b. dead fetus syndrome c. uncomplicated sectio caesarea d. amniotic fluid embolism syndrome e. sinus cavernosus thrombosis
22
100. Statements concerning serum total hypomagnesemie (HM) in critically ill patients:
a. the prevalence of HM of patients admitted to the ICU ranges from 10-20% b. low magnesium levels are associated with higher fatality c. Intracellular Mg deficiency can be present despite normal measured serum
concentrations, therefor we need to measure erythrocyte magnesium e. HM is often found in concurrently with hypokaliemia and hypochloremia and Mg
repletion has been shown to facilitate correction of potassium and calcium deficiencies e. Urinary Mg declines before serum Mg and is an earlier and more reliable indicator of
evolving Mg deficiency
23
ANSWERS Questions with 1 true alternative 1. a false b false c true d false; N Engl J Med 1999;340:1-8 e false; such a study has never been performed 2. a true b false c false d false; Acta Anaesthesiol Scand 1999;43:167-72 e false 3. a false b true c false d false; J Trauma 1999;46:271-9
e false 4. a false b false c false d true; Ann Intern Med 1999:130:729-35 e false 5. a false b false c true d false; J Pediatr 1999;134:406-12 e false 6. a false b true c false d false; increased mortality: N Engl J Med 1999;341:785-92 e false; either beneficial or detrimental effects 7. a false b false c false d true; N Engl J Med 1999;341:403-9 e false 8. a true b false c false d false; Gut 1999;45:97-104 e false; somatostatine is a synthetic analogue 9. a false b false c true d false; Ann Surg 2000;231:88-95 e false; Ann Surg 1999;229:128-36 10. c true; the classic regimen consists of a magistral (non-commercial) paste and
suspension of polymyxin E (= colistin = Colimycin = Belcomycin), tobramycin (= Obracin), amphotericin B (= Fungizone) and systemic administration of cefotaxim (= Claforan)
11. c. false; more often hyponatraemia
24
12. a-d false e true; pancreatic secretions (amylase) are high in urine; in kidney transplantation the
renal vasculature is anastomosed with the iliac vessels; the endocrine pancreas is connected similarly but the exocrine pancreas is connected with the intestines or preferably the urine bladder, which makes it possible to monitor the exocrine pancreas function in order to detect rejection (increased loss of bicarbonate in the urine or increase in urine amylase); when the transplanted pancreas is viable, conversion to a connection with the intestines will be performed after approximately 1 year.
13. a true; the diagnosis is pulmonary renal syndrome; the differential diagnosis includes Goodpasture's disease, and this disease is diagnosed by circulating anti-GBM antibodies and anti-GBM antibodies in the kidney tissue by immunofluorescence. This disease can be manifested by a rapid progressive glomerulonephritis (RPGN) and needs to be treated immediately by plasma filtration.
14. a false; this effect is only proven in healthy people under anesthesia, not in ICU patients!
b false; unproven c false; there is an improvement in dorsal ventilation d true e. false; unproven, also not in meta-analysis
15. c true; all other alternatives are causes as well, but less frequent causes; review Houston 16. a true; see Brower NEJM
b-e false; nothing has been proven scientifically in prospective randomised trials (review Houston)
17. a false b false; transthoracic echocardiography can reveal right ventricular and atrial dilatation
and sometimes the thrombotic mass itself, transoesophageal echocardiography may be more sensitive and specific, but the diagnostic value has not been evaluated in comparison with pulmonary angiography; advantage is that it can be performed bedside
c false; perfusion scintigraphy – ventilation scintigraphy – ultrasonography lower extremities – pulmonary angiography; its diagnostic value never tested in ICU patients and probably not very high
d true; gold standard despite need of transport; spiral CT-scanning of the thorax can detect central PE adequately, but not peripheral PE; according to the latest Consensus Diagnostiek Longembolie in the Netherlands in December 1999 it can replace ventilation scintigraphy and compression ultrasonography/duplex scanning of the lower extremities, but it is not the gold standard!
e false; result of increased dead space ventilation, but its diagnostic value is not known; interesting would be continuous VCO2 - measurement
18. a false; 500 ml/24 hour b true c false; produced in the choroid plexus in the ventricles and absorbed by the arachnoidal
villi d false; glucose is low and protein high; note that this is true for all kinds of meningitis:
bacterial, viral, and sterile (for example caused by bleeding) e false; the test is negative.Due to the obstruction there is no increment of cerebrospinal
fluid pressure. In the Queckensted maneuver one applies pressure on both jugular veins. This gives a disturbance of venous drainage from the head and an increase of venous bloodvolume in the head. This leads to a higher cerebrospinal fluid pressure which can be measured at the lumbar puncture site, unless there is obstruction between cerebrum and lumbar puncture site
25
19 a false; T3 is also secreted by the thyroid gland. The main source of T3 however is peripheral conversion of T4 to T3. b false; T3 is low and reverse T3 is high.
c false
d true e false; they inhibit this conversion.
20. a false; a diabetic keto-acidosis can occur in NIDDM although it is extremely seldom. Keto-acidosis develops because lipolysis takes place, and lipolysis takes place when there is no insuline anymore; in type II DM (=NIDDM) there is insulin but the defect concerns insulin receptor resistance.
b false; also in NIDDM c true d false; there is often hyponatremia e false; just as important to give large amounts of fluids and electrolytes
21. a false; the core temperature determines 85% of the body temperature
b false; vasoconstriction – non-shivering thermogenesis – shivering thermogenesis
c false; increased in neonates
d true
e false; the ‘warmth’ information is channelled through the C-fibers
22. a false; the blood temperature as measured by the pulmonary artery catheter is the highest temperature
b false; this profile occurs in the later phase of hypothermia
c false; hypothermia gives rise to thrombocytopathy
d false
e true; the low osmolality urine (‘cold diuresis’) persists and finally induces hypovolemia
23. b true; phentolamine is an α-blocker
24. d true; H&W p. 327 25. a false; MDMA is an indirect serotonine agonist; serotonine regulates sleep, mood,
appetite, memory, fear, and impulsive behavior. MDMA leads to massive serotonine depletion (and its metabolites) within 1-3 hrs.
b true: ACTH/prolactine/ADH ↑; GH ↓; even use of XTC of short duration (weeks) can give cognitive disturbances for a year.
c false; hyponatriemia (epilepsia/brain edema) based upon SIADH and liver failure; interstitial nefritis has been described
d false; mortality 50% due to sepsis/MODS; liver transplantation is unsuccesfully in comparison with live failure due to other intoxications
26
e false; selective serotonine reuptake inhibitors bind selectively to the serotonine transport protein and prevent the exchange of MDMA to serotonine.
Questions with 1 false alternative 26. a true; Arch Dis Child 1999;80:69-71 b true c false d true e true 27. a true b true c false d true; Med J Austr 1999;170:203-10 e true 28. a true b true
c false d true; only a small proportion of intervention patients reached their target oxygen
delivery; Chest 1999;115:453-61 e true 29. a false b true c true d true; Lancet 1999;353:1232-7 e true 30. a true b false c true
d true; Arch Intern Med 1999;159:129-34: 1. no pulse 10 minutes after start of CPR, 2. initial cardiac rhythm other than VT/VF, 3. cardiac arrest not witnessed
e true 31. a false b true c true d true; Antimicrob Agents Chemother 1999;43:1798-1802 e true 32. a true b true c true d false; low level of evidence; Clin Infect Dis 1999;28:1008-11 e true 33. a false b true c true d true; N Engl J Med 1999;341:625-34 e true 34. a true b true c false d true; Kudenchuk et al. N Engl J Med 1999;341:871-8 e true
27
35. a true b true c true d false; N Engl J Med 1999;341:793-800 e true 36. a true b false c true d true; J Antimicrob Chemother 1999;44:799-810 e true 37. a true b false c true d true; Eur Neurol 2000;43:61-9 e true 38. a true; nimodipine reduced the risk of neurodeficit by 30% (meta-analysis)
b false; Hypertension, Hypervolaemia and Haemodilution (triple H therapy) c true d true; angioplasty tried but large studies awaited e true; series of three patients reported with good results; Neurosurgery 1999
39. a false; it’s a pro-inflammatory cytokine. Source: klapper NVIC dagen 2000. T. van der Poll: modulatie van de inflammatoire respons bij sepsis.
b true; H&W p69 c true; H&W p69 d true; T. van der Poll: modulatie van de inflammatoire respons bij sepsis e true; T. van der Poll: locally protective, systemically detrimental
40. a true b true; the risk of rupture of the liver is higher than rupture of the spleen, the cause is a
wrong placement of the hands during CPR from the right side of the bed c true d false e true 41. a true b true c true; aortic dissection can lead to tamponnade, for example in M. Marfan
d false; in extreme vasodilation the skin is red (flush) and warm, and not waxy (cutanea marmorata) and cold
e true; a slowly progressive hyperkalemia can lead to bradycardia, hypotension and electrical-mechanical dissociation (EMD)
42. a true; see Dreyfuss D and Saumon G, Ventilator-induced lung injury, Am J Respir Crit Care Med 1998;157:304
b true; the production of surfactant is constant, but the loss is less, so the availibility is higher.
c false; no influence of PEEP on permeability, oedema just remains confined to the
interstitium in the presence of PEEP, whereas alveolar flooding occurrs in its absence
d true; this suggests increased filtration because of higher pulmonary capillary pressure; the answer should be taken with care; the role of dopamine in this is controversial because it also has been shown to reduce oedema.
e true; end-inspiratory volume is the major determinant of ventilator induced oedema 43. a-d true
e false; see article Marik
28
44. a true b true c false d true e true 45. b. false; lactic acidosis is rare in classical heat stroke 46. a true
b true c true; pregnancy is a rare cause of cardiomyopathy, which is not reversible and has a
bad prognosis d false; a mild physiological increase of pulmonary pressures may be present e true 47. a true; however, the answer depends on the hospital you are working in: Cambridge
true, VUMC false, AZG true: when there is no prophylactic correction, the coagulopathy during major bleeding complications appears to be irreversible
b false; HPS can not be influenced, and is not curable c true d true; low glucose level→ high insulin level e true 48. a true
b false; the risk of induction of anti-HEP/PF4 antibodies is estimated to be 50% in comparison with standard unfractionated heparin
c true; for the moment this is true because there is widespread experience with danaparoid sodium, allthough there is a 5-10% cross-reactivity; when there will be more clinical experience with r-hirudine or other direct thrombin-inhibitors these drugs will become drugs of first choice
d true e true
49. a false b true c true d true; Lancet 2000;355:26-30 e true 50. a true b true c true d false; Stroke 2000;31:811-6 e. true Questions with 5 alternatives true or false 51. a false b true c true d false; Antimicrob Agents Chemother 1998;42:3103-6.
e false 52. a true b true c false d false; well tolerated; Crit Care Med 1998;26:24-30 e true
29
53. a true b false c false d true; Ann Intern Med 1998;129:433-40 e false 54. a false b false c true d true; JAMA 1998;279:1629-32 e false; DXM is cheaper 55. a true b true c false d false e false; J Neurosurg 1998;89:519-25 56. a false b false c true d true; J Crit Care 1999;14:7-11 e true 57. a false b false c true d true; Clin Infect Dis 1999;28:98-105
e false; C3-deficiency has the lowest incidence, 17%; properdin-deficiency 30%, late complement component 46%)
58. a true; NVICMon 1999;3(6) b true c true d true e true 59. a true b true c true d true; Am J Respir Crit Care 1999;160:608-13 e true 60. a false; procaïnbenzylpenicillin is a parenteral small-spectrum penicillin, acid-
sensitive, and only Haemophilus influenzae is sensitive for it b true; the intact, anaerobic, intestinal flora has a protective effect against secondary
colonization with Gram-negative aerobic bacteria c false; this concept does not exist d true
e false; in multiple trauma patients with a reduction of nosocomial infections of 81% to 16%; note that this was shown in a non-randomised trial with a historical control group (articles D’Amico and Bonten)
61. a true; in a survey representing 164 teaching hospital ICU’s revealed that 84 % use sedatives frequently or routinely for intubated patients. The depth of sedation or the
efficacy of medication was most often not addressed; be aware that patients do not need sedation per se!
b false c true; e.g, the use of sedative medicine is correlated with critical illness neuropathy. d false; agitation is deliterious for patients as well because it is associated with potential
dangerous complications such as self extubation and removal of venous and arterial catheters, but also with increased systemic and myocardial oxygen consumption.
30
e false; there are currently few objective means to assess depth of sedation, although some work has been done with EEG monitoring and monitoring of parameters circulation. BIS monitoring is promising, but, to date, has hardly been validated in ICU patients.
62. a false; in healthy persons arginine is a semi-essential amino acid, in ill people essential b true c false; glutamate is a neurotransmitter d true e false 63. a true
b true; Bohr effect c true; end product of the red cell metabolism as in hypoxia d false; the presence of HbCO shifts the curve to the left e false; to the left (increase H+)
64. a-c false d,e true 65. a true; total bodywater is 60% of lean body weight. Of this bodywater 2/3 is
intracellular (ICV) and 1/3 extracellular (ECV). ECV is divided in bloodvolume (BV) and interstitial volume (ISV) with a ratio 1:3. The semipermeable membrane between ICV and ECV is only permeable for water and via pump mechanisms for electrolytes. The semipermeable membrane between BV and ISV is permeable for water, sodium, potassium, chloride-ions and glucose. Not for big molecules like proteins. The intravascular proteins create a colloid osmotic pressure. So 1000 ml of infused NaCl 0,9% will distribute in a ratio 1:3 between BV and ISV.
b true; see question 39a: 1000ml of glucose 5% equals 1000 ml of water. Of 1000 ml water 1/3 will distribute in ECV. Of this 1/3x1000 ml water ¼ will distribute in BV=1/3x1/4x1000= 85 ml.
c false; infusion of HES can lead to lowering of factor VIII-activity especially von Willebrand factor
d false; HES 200/0,6 has a longer halflife than HES 200/0,5 but a shorter halflife than HES 450/0,7. Halflife depends on molecular weight (200 kilodalton versus 450 kilodalton) and molair substitution (i.e part of the glucose molecules of amylopectine are substituted by hydroxy-ethyl groups. This leads to less rapid degration of the molecule by amylase. So the higher the molecular weight and the higher the molair substitution the more remains intravascular and so the longer is the halflife.
e true 66. a true; H&W p71
b false; iNOS is stimulated; nieuwe term is eNOS (endothelial); H&W p71 c false; It blocks the enzyme guanylaat cyclase, but it is not a L-arginine analogon; it is
also a radical scavenger. Boerhave cursus 1996. P.H.P Groeneveld. NO-antagonisten bij septische shock
d true; H&W p71 e true; H&W p70
67. a false; the juxtaglomerulal cells produce renine. H&W p67 b true; ACE is in hoge mate aanwezig in pulmonale endothelium; H&W p67 c false; infection with BHS can lead to toxic shock like syndrome according to the old
nomenclature. The term toxic shock syndrome is only used in stafylococcal infections; H&W p81
d false; S. aureus produces exotoxins; H&W p81 e true; H&W p68
68. a false; S. aureus (phage type 1) b false; any staphylococcal infection can predispose to TSS, including wound infections,
furuncles and abcesses. Postpartum cases can occur after vaginal or caeserean delivery. Nasal reconstructive surgery carries an especially high risk.
31
c true; antibody is produced in response to colonization with toxin-producing strains, and rates of seropositivity increase with age (> 90% when > 25 years)
d true; but also ARDS, cerebral oedema, myocardial dysfunction and hypocalcemia. e false; there are no human studies, only animal data, gamma globulin can blunt the
immune response increasing the risk of TSS recurrence, cost aspect, in animal studies the globulin is given before the toxin-challenge; in clinical practice the expert advice is not to withhold globulins but to do give globulins to patients.
69. a true; due to maldistribution of flow in the microcirculation related to inappropriate vasodilatation, exacerbated by microemboli, interstitial oedema, localized vasoconstriction and arteriovenous shunting
b false; it rises c true d false; is often increased as a result of the hypermetabolic response to illness or injury,
but can also be normal or decreased e true; see drawing H&W p75 Figure 4.8
70. a,b,c true d false; bacterial super antigens are produced by Gram-positive organisms
e false; cytochrome c does not work direct but indirect by discontinuation of the electron transport chain, through which NO and superoxide function.
71. a false; cocaine overdose leads to ventricular arrythmyias and acute coronary syndromes b true; tricyclic overdose can lead to hypotension or venticular arrythmias c false; opiate overdose may lead to respiratory arrest d true; in alcohol intoxication there is a sympathic overstimulation which can lead to
mors subita e false; nonsense
72. a false; Resuscitation 46 (2000) p103 b true; Resuscitation 46 (2000) p104 c false; Resuscitation 46 (2000) p104 d false; Resuscitation 46 (2000) p104 e true; Resuscitation 46 (2000) p104
73. a false; Resuscitation 46 (2000) p195,199 b true; Resuscitation 46 (2000) p195 c true; Resuscitation 46 (2000) p196 d false; Resuscitation 46 (2000) p197 e true; Resuscitation 46 (2000) p197
74. a-e true; see Curr Opin Anesthesiol article p115 75. a false; in 10-25%, and in up to 90% on the 3rd ICU day.
b true; Canadian CC Trial (1.5%); Cook meta-analysis (2.6%); in high risk groups, however, up to 10%. Another study by Cook showed in patients undergoing mechanical ventilation (MV) an incidence of 1.7% in patients randomized to receive ranitidine versus 3.8% in the sucralfate group.
c true; the pathogenesis is multifactorial, but H+ ions must be present in the lumen of the stomach. Patients with achlorhydria do not develop stress ulceration. Alterations in the mucosal blood flow, the mucus layer, protein synthesis, bicarbonate and
32
prostaglandins secretion, and epithelial cell renewal alter the mucosal barrier leading to back diffusion of acid and thus leading to mucosal damage. Other factors involved are endothelin and serotonin production, and H. pylori infection; the mucosal perfusion is of utmost importance!
d false; there are only limited clinical data to support this: intragastric pH rises. Cook found that enteral feeding was a positive predictor for clinically important bleeding. Postpyloric feeding may stimulate gastric acid production without buffering the gastric contents, and increase the risk for bleeding
e false; the results are discordant: heterogeneity of studies, anti-ulcer agents used, gastric pH levels attained, proportion of MV, makes comparisons difficult. In the studies that used 'protected brush specimen' (PBS) sampling no association was demonstrated. A deterioration of mucosal perfusion will lead to less acid production by the gastric cells and will give a rise in gastric fluid pH.
76. a false; worldwide infectious hepatitis B constitutes the most common cause of ALF. b false; factor V is used in the Clichy criteria; factor VII is the clotting factor with the
shortest half-life. c true; see H&W p315 d false; hypoglycemia is is due to raised plasma insulin levels combined with a failure of
hepatic gluconeogenesis. e true; see H&W p317
77. a false; hypoxia is predominantly as result of V/Q mismatch and to a lesser extent true shunt.
b true; secondary to compressed areas of lung (atelectasis/consolidation/oedema), small lung volume associated with ALI, adhesion of inflammatory cells to capillary endothelium, hypoxic pulmonary vasoconstriction, and overdistension compressing pulmonary vessels secondary to ventilation.
c false; phagocytic cells initially (macrophages,monocytes); then neutrophils after adhesion to endothelial cells and subsequent activation; platelets also participate with the release of 5-HT, PAF, ADH
d false; the early hyaline membrane is eosinophilic and composed primarily of leaked plasma proteins, mainly fibrin and some complement Collagen is laid down at a later 'organising stage' rapidly and in large quantities by activated fibroblasts. Total lung collagen can double in ARDS in two weeks
e true; the pathological process causing capillary leak and oedema is generally evenly distributed throughout the lung. Increased density as seen on CT in the dorsal regions is due purely to the weight of the above lung.
78. a false; 50 - 75% are responders (Albert) b false; according to a 1990 study of induced ALI in dog lungs there is little change in
regional perfusion on turning prone. Further strudies have confirmed that dorsal regions of the lung are always preferentially perfused (Albert)
c true; prone airways angle down facilitating secretion clearance d false; this remains a contentious issue though. Albert in his review suggests that
reciprocal ventral collapse/atelectasis does not occur because of the fact that Ppl does not become positive. However, early studies by Gattinoni suggest that ventral lung regions will collapse on turning prone
e true; in oedematous lung, Ppl becomes markedly positive with gravity in the supine and lateral positions. This gradient is abolished in the prone position resulting in the requirement for less airway pressure to generate airspace opening and more uniform lung inflation.
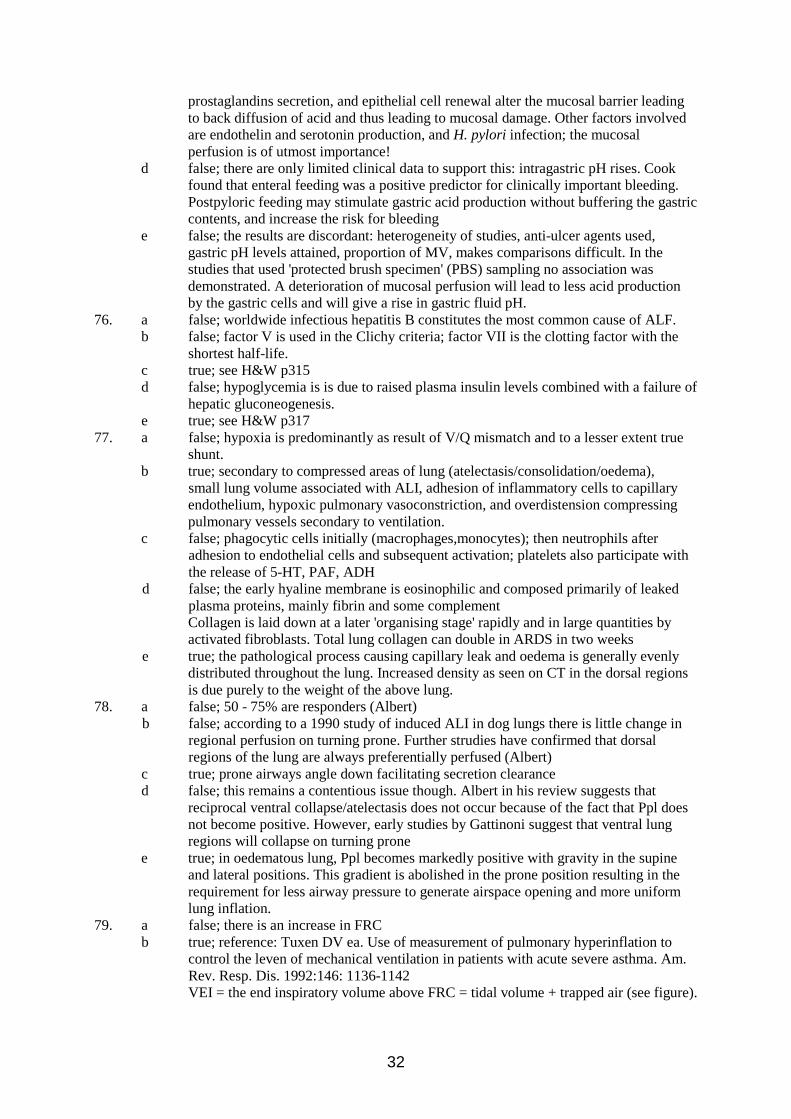
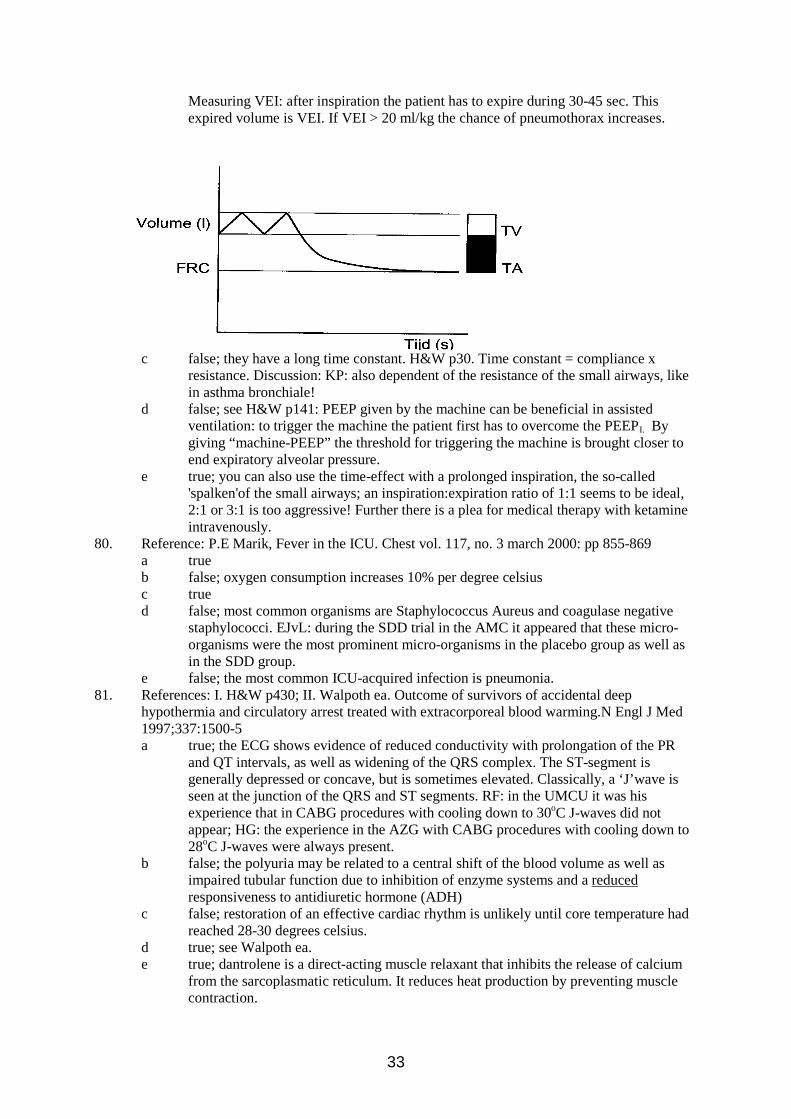
79. a false; there is an increase in FRC b true; reference: Tuxen DV ea. Use of measurement of pulmonary hyperinflation to
control the leven of mechanical ventilation in patients with acute severe asthma. Am. Rev. Resp. Dis. 1992:146: 1136-1142 VEI = the end inspiratory volume above FRC = tidal volume + trapped air (see figure).
33
Measuring VEI: after inspiration the patient has to expire during 30-45 sec. This expired volume is VEI. If VEI > 20 ml/kg the chance of pneumothorax increases.
c false; they have a long time constant. H&W p30. Time constant = compliance x resistance. Discussion: KP: also dependent of the resistance of the small airways, like in asthma bronchiale!
d false; see H&W p141: PEEP given by the machine can be beneficial in assisted ventilation: to trigger the machine the patient first has to overcome the PEEPI. By giving “machine-PEEP” the threshold for triggering the machine is brought closer to end expiratory alveolar pressure.
e true; you can also use the time-effect with a prolonged inspiration, the so-called 'spalken'of the small airways; an inspiration:expiration ratio of 1:1 seems to be ideal, 2:1 or 3:1 is too aggressive! Further there is a plea for medical therapy with ketamine intravenously.
80. Reference: P.E Marik, Fever in the ICU. Chest vol. 117, no. 3 march 2000: pp 855-869 a true b false; oxygen consumption increases 10% per degree celsius c true d false; most common organisms are Staphylococcus Aureus and coagulase negative
staphylococci. EJvL: during the SDD trial in the AMC it appeared that these micro-organisms were the most prominent micro-organisms in the placebo group as well as in the SDD group.
e false; the most common ICU-acquired infection is pneumonia. 81. References: I. H&W p430; II. Walpoth ea. Outcome of survivors of accidental deep
hypothermia and circulatory arrest treated with extracorporeal blood warming.N Engl J Med 1997;337:1500-5 a true; the ECG shows evidence of reduced conductivity with prolongation of the PR
and QT intervals, as well as widening of the QRS complex. The ST-segment is generally depressed or concave, but is sometimes elevated. Classically, a ‘J’wave is seen at the junction of the QRS and ST segments. RF: in the UMCU it was his experience that in CABG procedures with cooling down to 30oC J-waves did not appear; HG: the experience in the AZG with CABG procedures with cooling down to 28oC J-waves were always present.
b false; the polyuria may be related to a central shift of the blood volume as well as impaired tubular function due to inhibition of enzyme systems and a reduced responsiveness to antidiuretic hormone (ADH)
c false; restoration of an effective cardiac rhythm is unlikely until core temperature had reached 28-30 degrees celsius.
d true; see Walpoth ea. e true; dantrolene is a direct-acting muscle relaxant that inhibits the release of calcium
from the sarcoplasmatic reticulum. It reduces heat production by preventing muscle contraction.
34
82. a-c false d true
e false 83. a false; the trauma mechanism is after acceleration/deceleration with relatively high
speed (fall from great height, car accident) b false; more rapidly fatal in elderly where the aorta is rigid c true; does have a broad mediastinum but is not easily discovered on X-ray alone d true; also diminished or absent femoral pulses e false; can be confirmed by TEE, CT-scan, MRI, and angiography; there is discussion
in the literature on the gold standard in traumatic aorta disruption; the deparment of Traumatology in the VUMC regards the angiography as gold standard, but in common clinical practice TEE and CT-scan are more practical.
84. a,d true; reference Cheatham ML. Intra-abdominal hypertension and abdominal compartment syndrome. New Horiz 1999;7:96-115; p. 97-98
b false; one pressure level can not be defined for each individual patient c false; do tolerate IAH better than nonobese patients
e false; a high risk of venous thromboembolism is assumed but never proven; cholestasis is not described as a hepatic complication of ACS.
85. a false; although disuse atrophy is seen, CIPN appears to involve specific pathological processes affecting the nerve axon causing a mixed axonal neuropathy
b false; demyelination is not seen. Nerve conduction velocities are normal thus excluding it. The pathology is axonal.
c false; nerve biopsy is only rarely performed as permanent neurological deficits are inevitable. Electromyography is the key investigation for CIPNP. SP: nerve biopsies are very infrequently performed in the ICU, the main indication is analysis of strange polyneuropathies.
d true; this was described in a group of asthmatic patients receiving high dose steroids and mechanical ventilation.
e true; a recent study demonstrated detectable abnormalities in 80% of all patients admitted with sepsis and in those, 80% had detectable abnormalities in the first 72 hours.
86. a false; the figure is around 25-30% (evacuation of sub/epidural haematomas and fronto/temporal parenchymal lesions). The classification of traumatic brain injury according to Teasdale: severe = GCS ≤8, moderate GCS 9-13, and mild GCS 14-15.
b true; defined as a single recording of less than 90 mm Hg systolic in adults c true; clinically important interhemispheric differences in ICP can be found with a
focal lesion. It is better then to place the ICP catheter on the affected side or ideally have one on both sides. 1 Spanish study has used bilateral ICP monitoring catheters for 24-48 hours and showed the existence of a pressure gradient of 3-8 mmHg between the lesion and normal tissue. In the VUMC the right frontal location is used standardly, like in the rest of the world, to avoid damage of the dominant left hemisphere.
d true; as seen by zero change in SjO2 with changes in MAP. SjO2 depends on the DO2 and VO2 of the brain; we should keep in mind that the SjO2 is a global measure and not a regional measure of cerebral blood flow and oxygen extraction by the brain tissue: while autoregulation can be disturbed in the cerebral lesion it can at the same time be intact in normal brain tissue! Nowadays the accepted indication for use of SjO2 is monitoring of vasoconstrictor therapy, which SjO2 probably can; the accepted critical level of SjO2 in most articles is ≥ 50%; some take ≥ 55% as crititcal level. Compare with the critical level of SvO2: ≥ 60%.
e false; this compromises cerebral blood flow more than any reduction in ICP would prove beneficial. The head should be raised not more than 30 degrees.
87. a false; both T3 and T4 levels are reduced but current recommendations do not support supplementation
b false; again, not as standard but reduced cortisol levels may be responsible for adverse
35
effects such as hypotension and should be considered (see answer c below). Adrenal insufficiency might be quite common in this group of patients as well as in the patients with MODS (Am J Resp Crit Care Med 2001;163:A458)
c false; high dose adrenergic inotropes can result in adverse effects on subsequent organ function after transplant (eg renal vasoconstriction and down regulation of cardiac beta receptors leading to reduced responsiveness to inotropes post transplant)
d true; the mass of dead brain tissue is a potent trigger of DIC. DIC accompanied by bleeding complications can pose serious difficulties for the harvesting of organs.
e true; profound temperature disruption is the norm with hypothermic problems being far the most common problem. It should be treated actively. SAB around the brain stem with a lot of blood in the basal cisterns can give hypothalamic disregulation with hyperthermia; beware that this is a diagnosis per exclusionem! SAB is not often accompanied by hypothermia. In brain death hypothermia can occur spontaneously.
88. a true
b false; the reverse is the case
c true
d false; it causes the collapse of smaller vessles, leading to increased intravascular resistance which results in a higer arterial pressure in the intracranial tree than extracranially; see: N Engl J Med, 2001;344:1215-21
e true; see ATLS Student Course Manual 1997, American College of Surgeons, p.185; SP: when the n. oculomotorius fails, n. trochlearis and n. abducens will dominate.
89. a false; 60-150 mmHg; H&W p328-9 b false; increased
c true
d true e false; very local deficiencies of autoregulation can exist
90. a. right: when the intacerebral/ventricular compnenet dominates, mostly a previous episode with acute headache (=SAB) was present
b. right; this hematoma gets often mixed up with the hypertensive intracerebral hematoma, especially when the RR on admission is high
c. right; as early as possible , but not before 12 hrs (conversion blood to bilirubin) d. right; it will reduce the chance for a rebleeding considerably and should be continued
until 3 weeks after the last SAB e. right; T-top inversion, ST depression, ST elevation, QT increase. The cause is
intracardial ischemia and subendocardial infarctions, possibly secondary to increased cathechloamine secretion. Another mechanism is neurogenic myocardial stunning (sympathic nerve stimulation? Endothelin?)
91. a true; in HELPP syndrome there is a microangiopathic hemolysis and one can see schistocytes in the bloodsmear.
b true; in 70% of cases the HELLP syndrome occurs prepartum and in 30% of cases postpartum; in fact postpartum HELLP is a separate entity.
c false; hypertension may be absent in as many as 50% of patients in the early stages of the syndrome.
d false; some unknown factor leads to undue intravascular platelet activation resulting in the release of thromboxane A2, and serotonin. TA2 and serotonin cause vasospasm, platelet aggregation, and further enhance endothelial damage. Development of DIC in HELLP is mainly secondary to additional inciting conditions such as placental abruption, fetal death or liver hematoma.
36
e true; reference: Bolte, van Eyck, Strack van Schijndel ea. The haemodynamic effects of ketanserin versus dihydralazine in severe early onset hypertension in pregnancy. British Journal of Obstetrics and Gynaecology 1998; 105: 723-731
92. a false; even after ingestion of 1 tablet of XTC death can result; but it is clinically difficult to evaluate the true dose taken. It is the question if the XTC component is the sole cause for the clinical intoxication syndrome, because the tablets can be mixed with other unknown substances and often the patient has taken other substances like benzodiazepines, alcohol et cetera besides XTC. Individual factors that play a role are the intensity of dancing at rave parties, the amount of water drunk, and the severity of dehydration. Further, there is great variation in the individual dose-response relation.
b true; also aggravated by muscle hyperactivity and seizuresresulting in severe hyperthermia of >430C!
c false; this treatment is effective in malignant hyperthermia which is a primary muscle disorder (ie peripheral) but is not effective in the treatment of centrally mediated hyperthermia
d true; also may be aggravated by an SIADH type syndrome. It can rarely lead to cerebral edema and death
e true; common and caused by hyperthermia, seizures and excessive muscular activity. 93. a true
b false; hyponatraemia is always present in this condition and is dilutional in nature. The initial treatment is water restriction.
c true; myxedema coma almost always has a precipitating cause and bacterial infection is the most common. Signs of infection are usually absent because the patient is unable to raise a fever or mount a leucocytosis. The same holds true for a thyroid storm in which there is hyperthermia and an infection can not be excluded.
d true; the current recommendation is for treatment with T4 but in what dose and via which route remains controversial. The dose of T3 suppletion should be slowly increased, but faster than in non-ICU patients, because the risk of mortality in myxoedema is very high and outweighs the risk of cardiac complications; steroids should be administered as well. T3 can be given as intravenous preperation. It is also possible to treat with a combination of T3 and T4; it is possible to make an intravenous T4 preparation.
e false; beta agonists are both ineffective in the presence of low levels of thyroid hormone and dangerous as they can precipitate arrythmias. Hypotension is a poor prognostic sign. Beware that dopamine itself gives rise to the euthyroid sick syndrome.
94. a false; regulated by the hypothalamic-pituitary-adrenal axis b false; higher in the morning; Beware that in ICU patients there is a loss of day rhythm
or clearly a diminished variation. c true d true; hyponatremia occurs in 70% of patients, while hypokalemia occurs in 60-65% of
patients. Beware that again in ICU patients sodium and potassium do not have significant diagnostic value, because they are influenced by many other factors, such as acute renal failure, use of diuretics et cetera, in the ICU setting. The most important clinical symptoms in the ICU setting are fever of unknown origin and hypotension of unknown origin.
e false; cancer does frequently give metastases in the adrenal glands, but this does not often lead to clinical insufficiency
95. a true b false c true; and lots of fluid! The preparation of iodine is solutio lugol forte, which can be
given per os as drops. The administration of iodine was used in the old days as a preoperative technique according to Plummer (“Plummeren”): potassium iodine (KI) was administered to inhibit the thyroid hormone production and to reduce preoperative bleeding.
37
d false; is about 20% e false
96. a true b false; nearly all venous admixture which is not the same as an anatomical shunt c true; in ARDS areas of dead space ventilation develop due to perfusion disturbances
based upon thrombo-embolic processes d false e false 97. a,b,c true; non-cardiogenic pulmonary oedema is also pressure dependent d false; it is not proven that mechanical ventilation decreases pulmonary oedema e false 98. a false b true; static peak inspiratory pressure = plateau pressure c true d false e false 99. a,b,d true
c false; in a complicated sectio caesarea the development of ARDS is possible due to for example aspiration
e false 100. a false; it ranges from 20-60%. In ICM 1996:22;724, 44% of patients on admission were
hypomagnesemic. b false; in contrast to hypermagnesemia (hypotension, respiratory depression,
neuromuscular blockade) which has a strong association with mortality. In severe hypomagnesemia (<0.5 mmol/l) there might be a higher mortality.
c true; but still controversial, erythrocytes may not be representative of other tissues, they lack a nucleus and are probably less metabolically active than some other cells. It correlates with the serum bound fraction of Mg (35% of total Mg), indicating that erythrocytes may not have any greater predictive value of Mg status than does serum Mg. Probably intracellular ionized Mg would be the best test, like the mononuclear blood cell Mg content.
d true; CCM 1996;24:38. Mg (2 gr=8 mmol) in 30 min every 6 hrs for 8 doses results in a net positive improvement in potassium balance.
e true; as is demonstrated in patients with gut failure.
38
Candidate Name : Adress : Hospital : E-mail : Multiple choice questions 1 alternative true 1 alternative false 1. a b c d e 26. a b c d e 2. a b c d e 27. a b c d e 3. a b c d e 28. a b c d e 4. a b c d e 29. a b c d e 5. a b c d e 30. a b c d e 6. a b c d e 31. a b c d e 7. a b c d e 32. a b c d e 8. a b c d e 33. a b c d e 9. a b c d e 34. a b c d e 10. a b c d e 35. a b c d e 11. a b c d e 36. a b c d e 12. a b c d e 37. a b c d e 13. a b c d e 38. a b c d e 14. a b c d e 39. a b c d e 15. a b c d e 40. a b c d e 16. a b c d e 41. a b c d e 17. a b c d e 42. a b c d e 18. a b c d e 43. a b c d e 19. a b c d e 44. a b c d e 20. a b c d e 45. a b c d e 21. a b c d e 46. a b c d e 22. a b c d e 47. a b c d e 23. a b c d e 48. a b c d e 24. a b c d e 49. a b c d e 25. a b c d e 50. a b c d e
39
5 alternatives true/false 51. a true/false 61. a true/false 71. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 52. a true/false 62. a true/false 72. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 53. a true/false 63. a true/false 73. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 54. a true/false 64. a true/false 74. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 55. a true/false 65. a true/false 75. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 56. a true/false 66. a true/false 76. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 57. a true/false 67. a true/false 77. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 58. a true/false 68. a true/false 78. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 59. a true/false 69. a true/false 79. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false 60. a true/false 70. a true/false 80. a true/false b true/false b true/false b true/false c true/false c true/false c true/false d true/false d true/false d true/false e true/false e true/false e true/false
40
81. a true/false 91. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 82. a true/false 92. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 83. a true/false 93. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 84. a true/false 94. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 85. a true/false 95. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 86. a true/false 96. a true/false b true/false b true/false c true/false c true/false d true/false d true/false
e true/false e true/false 87. a true/false 97. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 88. a true/false 98. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 89. a true/false 99. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false 90. a true/false 100. a true/false b true/false b true/false c true/false c true/false d true/false d true/false e true/false e true/false