NEGLECTED DISEASE RESEARCH AND DEVELOPMENT ......Delfina Rampone, Allisa Robertson, Gautam Kumar...
121
NEGLECTED DISEASE RESEARCH AND DEVELOPMENT: REFLECTING ON A DECADE OF GLOBAL INVESTMENT POLICY CURES RESEARCH 2017 Dr Nick Chapman Anna Doubell Lisette Oversteegen Dr Vipul Chowdhary Dr George Rugarabamu Renata Zanetti Ming Ong Juliette Borri
Transcript of NEGLECTED DISEASE RESEARCH AND DEVELOPMENT ......Delfina Rampone, Allisa Robertson, Gautam Kumar...

NEGLECTED DISEASE RESEARCH AND DEVELOPMENT:REFLECTING ON A DECADE OF GLOBAL INVESTMENT
POLICY CURES RESEARCH
2017
Dr Nick ChapmanAnna DoubellLisette OversteegenDr Vipul ChowdharyDr George RugarabamuRenata ZanettiMing OngJuliette Borri
POLIC
Y CU
RES RESEARC
HG
-FIND
ER 2017 N
EGLEC
TED D
ISEASE RESEA
RCH
& DEVELO
PMEN
T : REFLECTIN
G O
N A D
ECA
DE O
F GLO
BAL IN
VESTMEN
T

ACKNOWLEDGEMENTS
This is the tenth in a series of annual reports published as part of the G-FINDER project. We are very grateful to all of the survey participants who have contributed to this effort. With their commitment, we have been able to continue to provide accurate, up-to-date financial information in the field of research and development (R&D) for neglected diseases. The patience and engagement of the participating government and multilateral agencies, academic and research institutions, product development partnerships (PDPs), philanthropic institutions and pharmaceutical and biotechnology companies have made this project possible.
We would like to extend our gratitude to our Advisory Committee and other experts for their invaluable advice on the design and scope of our study. A particularly warm thank you goes to the HIV Vaccines and Microbicides Resource Tracking Working Group, and to the International Federation of Anti-Leprosy Associations for coordinating their initiatives with ours where possible.
We are especially grateful to Richard Fisher, our CEO; Philippa Telford, our executive assistant and office manager; Lee Sternberg, our accounting manager; and our contract researchers Delfina Rampone, Allisa Robertson, Gautam Kumar Saha, Sarah Serhal and Margaret Shi. Their dedicated efforts were key to the survey’s success.
Finally, Policy Cures Research would like to thank the project funder, the Bill & Melinda Gates Foundation, for their ongoing support.
We would also like to acknowledge the following organisations for their commitment and patience in collating large datasets for the G-FINDER survey this year: Argentinian Ministry of Science, Technology and Productive Innovation (MINCYT); Australian National Health and Medical Research Council (NHMRC); Bill & Melinda Gates Foundation; Brazilian Ministry of Health: Department of Science and Technology (DECIT); Brazilian Support Foundation for Research in the State of Minas Gerais (FAPEMIG); Brazilian Support Foundation for Research in the State of São Paolo (FAPESP); Canadian Institutes of Health Research (CIHR); Carlos III Health Institute; European and Developing Countries Clinical Trials Partnership (EDCTP); European Commission (EC); Institut Pasteur; Liverpool School of Tropical Medicine (LSTM); South African Medical Research Council (MRC); Swiss National Science Foundation (SNSF); UK Medical Research Council (MRC); University of Pittsburgh; US National Institutes of Health – National Institute of Allergy and Infectious Disease (NIAID); Wellcome Trust; and all of the PDPs.
In addition, we would like to acknowledge the following organisations for their collaboration with Dr Vipul Chowdhary: Indian Council of Medical Research (ICMR); Indian Department of Biotechnology, Ministry of Science and Technology (DBT); Indian Department of Science and Technology; International Centre for Genetic Engineering and Biotechnology, New Delhi (ICGEB); and the Indian Council of Scientific and Industrial Research (CSIR) labs – Indian Institute of Chemical Biology (IICB), Kolkata; Central Drug Research Institute (CDRI), Lucknow; Institute of Microbial Technology (IMTECH), Chandigarh; Institute of Genomics and Integrative Biology (IGIB), Delhi; Centre for Cellular and Molecular Biology (CCMB), Hyderabad; Indian Institute of Integrative Medicine (IIIM); and the Biotechnology Industry Research Assistance Council (BIRAC).
POLICY CURES RESEARCHwww.policycuresresearch.org
FOR FURTHER COPIES PLEASE CONTACT
55 Brisbane Street Surry Hills NSW 2010
Australia Tel: +61 (2) 8218 2109
Published by Policy Cures Research
December 2017
This report was prepared by Policy Cures Research through a project supported by the Bill & Melinda Gates Foundation.
The views expressed are those of the authors.

NEGLECTED DISEASE RESEARCH AND DEVELOPMENT:REFLECTING ON A DECADE OF GLOBAL INVESTMENT
Dr Nick ChapmanAnna DoubellLisette OversteegenDr Vipul ChowdharyDr George RugarabamuRenata ZanettiMing OngJuliette Borri
2017
POLICY CURES RESEARCH

CO
NT
ENT
S
PAGE3
CONTENTS
GLOSSARY 4EXECUTIVE SUMMARY 7INTRODUCTION 12
Background to the G-FINDER survey 12The survey scope 12Survey methodology 16Reading the G-FINDER report 17The latest G-FINDER survey 19
FUNDING BY DISEASE 22HIV/AIDS 25Malaria 29Tuberculosis 33Diarrhoeal diseases 37Kinetoplastids 41Dengue 45Bacterial pneumonia & meningitis 49Salmonella infections 53Helminth infections 57Hepatitis C 61Leprosy 64Cryptococcal meningitis 66Buruli ulcer 68Leptospirosis 70Trachoma 72Rheumatic fever 74
NEGLECTED DISEASE FUNDERS 76Funder overview 76Public funders 77Philanthropic funders 84Private sector funders 87Funding by organisation 92
FUNDING FLOWS 94Funding flow trends 95Funding flows by R&D stage 96Funding for product development partnerships 97Funding for other intermediaries 100
DISCUSSION 103ANNEXES 107
Annexe 1: Advisory Committee members & additional experts 107Annexe 2: Survey respondent list 108Annexe 3: References 112

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE4
GLO
SSA
RY GLOSSARY
ACT Artemisinin-based combination therapy
Aggregate industry Aggregate pharmaceutical and
biotechnology companiesAIDS AcquiredImmuneDeficiency
Syndrome AmB Amphotericin BARV AntiretroviralAustralia - India SRF Australia - India Strategic Research
FundAustralian ACH2 Australian Centre for HIV and
Hepatitis Virology Research Australian DFAT Australian Department of Foreign
AffairsandTrade(formerlyAusAID)Australian DIIS Australian Department of Industry,
Innovation and ScienceAustralian NHF Australian National Heart
FoundationAustralian NHMRC Australian National Health and
Medical Research CouncilbNAbs Broadly neutralising anti-HIV
antibodies Brazilian BNDES Brazilian Development BankBrazilian DECIT Brazilian Ministry of Health:
Department of Science and Technology
Brazilian FAPEMIG Brazilian Support Foundation for
Research in the State of Minas Gerais
Brazilian FAPESP State of São Paulo Research
FoundationBrazilian FINEP Brazilian Innovation AgencyCanadian CIHR Canadian Institutes of Health
ResearchChilean FONDECYT ChileanNationalFundforScientific
andTechnologicalDevelopmentCLTRF CebuLeprosyandTuberculosis
Research FoundationColombian Colciencias Colombian Department for
Science,TechnologyandInnovation
CORDIS Community Research and Development Information Service
DAA Direct-acting antiviralsDAHW GermanLeprosyandTBRelief
AssociationDALY Disability adjusted life yearDNDi Drugs for Neglected Diseases
initiativeDutch DGIS Dutch Ministry of Foreign
Affairs-DirectorateGeneralofDevelopment Cooperation
EAggEC Enteroaggregative E. coliEC European Commission: Research
Directorate-GeneralEDCTP European & Developing Countries
ClinicalTrialsPartnershipEID Emerging infectious diseaseEMA European Medicines AgencyETEC Enterotoxigenic E. coliEVI European Vaccine InitiativeFIND Foundation for Innovative New
Diagnostics
GLOSSARY

PAGE5
GLO
SSA
RY
Flemish EWI Flemish Department of Economics,
Science and InnovationFrench ANR French National Research AgencyFrench ANRS French National Agency for
Research on AIDS and Viral Hepatitis
French IRD French Research Institute for Development
FY Financial yearGates Foundation Bill & Melinda Gates FoundationGavi Gavi, the Vaccine AllianceGBD Global Burden of Disease StudyGDP Gross domestic productGerman BMBF German Federal Ministry of
Education and ResearchGerman DFG German Research FoundationG-FINDER Global Funding of Innovation for
Neglected DiseasesGHE Global Health EstimatesGHIT Fund Global Health Innovative
TechnologyFundHCV Hepatitis C virusHIC High-income countryHIV HumanimmunodeficiencyvirusIAVI International AIDS Vaccine InitiativeIDC Innovative developing countryIDRI Infectious Disease Research
InstituteIHME Institute for Health Metrics and
EvaluationIMF International Monetary FundIndian DBT Indian Department of
BiotechnologyIndian ICMR Indian Council of Medical Research
IPM International Partnership for Microbicides
IRS Indoor residual sprayingISGlobal Barcelona Institute for Global
HealthIVCC Innovative Vector Control
ConsortiumIVI International Vaccine InstituteLAMP Loop-mediated isothermal
amplificationLLIN Long-lasting insecticide treated netLMIC Low- and middle-income countryLRI Leprosy Research InitiativeMDR-TB Multidrug-resistant tuberculosisMIC Middle-income countryMMV Medicines for Malaria VentureMNC Multinational pharmaceutical
companyMSF Médecins Sans FrontièresNew Zealand HRC Health Research Council of New
ZealandNTS Non-typhoidal Salmonella entericaOAR OfficeofAIDSResearchOECD Organisation for Economic
Cooperation and DevelopmentOWH OneWorld HealthPCV Pneumococcal conjugate vaccinePDP Product development partnershipR&D Research and developmentRCDC US NIH’s Research, Condition and
Disease Categorization ProcessRDT Rapid diagnostic testRePORTER US NIH’s Research Portfolio Online
ReportingToolsRT-PCR Reverse transcription polymerase
chain reaction S&T Science and technologySFI Science Foundation Ireland
GLOSSARY

PAGE6
GLO
SSA
RY
SME Small pharmaceutical and biotechnologyfirms
South African DST South African Department of
ScienceandTechnologySouth African MRC South African Medical Research
CouncilSSI Statens Serum InstituteSwedish SIDA Swedish International Development
AgencySwiss SDC Swiss Agency for Development
and CooperationSwiss SERI Swiss State Secretariat for
Education, Research and Innovation
Swiss SNSF Swiss National Science FoundationTB TuberculosisTBVI TuBerculosisVaccineInitiativeThailand GPO ThailandGovernment
Pharmaceutical OrganisationThe Union International Union Against
TuberculosisandLungDiseaseTLMI TheLeprosyMissionInternationalUK United KingdomUK DFID UK Department for International
DevelopmentUK MRC UK Medical Research CouncilUS United StatesUS BARDA US Biomedical Advanced
Research and Development Authority
US CDC US Centers for Disease Control and Prevention
US DOD US Department of DefenseUS FDA US Food and Drug AdministrationUS NIAID US National Institute of Allergy and
Infectious DiseasesUS NIH US National Institutes of Health
GLOSSARY
USAID US Agency for International Development
VCP Vector control productVHF Viral haemorrhagic feverWHO World Health OrganizationWHO/TDR World Health Organization Special
Programme for Research and TraininginTropicalDiseases
XDR-TB Extensively drug-resistant tuberculosis
YOY Year-on-year

PAGE7
The survey
Each year since 2007, the G-FINDER project has provided policy-makers, donors, researchers and industrywithacomprehensiveanalysisofglobalinvestmentintoresearchanddevelopment(R&D)of new products to prevent, diagnose, control or cure neglected diseases in developing countries. It provides an up-to-date analysis of how R&D investments are being allocated across diseases and product types, funding trends over time, and where the potential gaps lie.
ThisisthetenthannualG-FINDERreport.Inadditiontothepreviousnineyearsoffundingdata,itreportsoninvestmentsmadeinfinancialyear2016.Inall,187organisationscompletedthesurveyforFY2016,whichcovered33neglecteddiseasesandallrelevantproducttypes:drugs,vaccines(preventiveandtherapeutic),diagnostics,microbicidesandvectorcontrolproducts (pesticides,biologicalcontrolagentsandvaccinestargetinganimalreservoirs)–aswellasbasicresearch.
In2016, followinga reviewby theG-FINDERAdvisoryCommittee, thebacterialpneumonia&meningitis category was expanded to include developing country-focused basic research for both Streptococcus pneumoniae and/or Neisseria meningitidis.Developingcountry-specificresearchinto therapeutic vaccines for HIV/AIDS was also added as a restricted category.
While included in the last two G-FINDER reports, analysis of R&D funding for African viral haemorrhagicfevers(includingEbola)wasseparatedfromtheneglecteddiseasefundinganalysisin2016.Aseparatescopedefinitionhasbeendevelopedto identify investments inR&DforallpriorityemerginginfectiousdiseasesidentifiedintheWorldHealthOrganizationR&DBlueprintforaction to prevent epidemics. EID data is not included in this G-FINDER neglected disease report, and will be reported separately.
Findings
In2016,areported$3,203mwasinvestedinneglecteddiseaseR&D,consistingof$3,024mfromrepeatsurveyparticipants(calledyear-on-year–YOY–funders)and$179mfromirregularsurveyparticipants.TotalYOYfundingforneglecteddiseaseR&Dincreasedforthefirsttimesince2012(up$99m,3.4%).
FUNDING BY DISEASE
As inpreviousyears, threediseases–HIV/AIDS,malariaandtuberculosis(TB)–collectivelyreceivedmorethantwo-thirds($2,247m,70%)ofallglobalfundingforneglecteddiseaseR&Din2016.Overallfunding to this group of diseases increased slightly (up$60m,2.9%),drivenby increased investmentinHIV/AIDS(up$83m,8.3%).Fundingformalariaincreasedmodestly (up $13m, 2.5%),whileinvestmentinTBfellby$37m(down6.8%).
EXECUTIVE SUMMARY
EXEC
UT
IVE
SUM
MA
RYGlobal funding for neglected disease R&D increased for the first time since 2012

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE8
EXEC
UT
IVE
SUM
MA
RY
Diseases in thesecondfundingtier receivebetween0.5%and6.0%of total fundingeachyear.Thisgroupincludesdiarrhoealdiseases,kinetoplastids,dengue,bacterialpneumonia&meningitis,Salmonellainfections,helminthsandhepatitisC(genotypes4,5&6).Fundingforthistierwasessentiallyunchangedfromthepreviousyear(up$0.9m,0.2%).Onlythreesecondtierdiseasessawfundingincreasesin2016:Salmonellainfections(up$21m,32%),kinetoplastids(up$12m,12%)anddengue(up$8.4m,8.7%).Fundingfellforallothersecondtierdiseases,withthelargestdropbeingfordiarrhoealdiseases(down$21m,-14%),followedbyhepatitisC(down$12m,-36%),helminths(down$3.9m,-5.5%)andbacterialpneumonia&meningitis(down$3.1m,-3.8%).ThemostpoorlyfundedneglecteddiseasescoveredbytheG-FINDERsurvey–thoseinthethirdtieroffunding–eachreceivelessthan0.5%ofglobalfunding.Thistier includesleprosy,cryptococcalmeningitis,Buruliulcer, leptospirosis,trachomaandrheumaticfever.In2016,leprosywasthebest-fundedofthesediseases($11m,0.3%),whilerheumaticfeverreceivedlessthananyotherneglecteddisease($1.3m,<0.1%).
Non-disease-specific investment increasedto$261min2016,an increaseof$37m(up17%).Corefunding–non-earmarkedfundsgiventoorganisationsworkingonmultipleneglecteddiseases–accountedforjustoverhalf($136m,52%)ofallnon-disease-specificinvestmentin2016,anincreaseof$15m(up14%).Platformtechnologies–toolsthatcanpotentiallybeappliedtoarangeofareas,butwhicharenotyetfocusedonaspecificproductordisease–received$52min2016(20%ofallnon-disease-specificfunding);thelargestinvestmenteverreportedforthisarea.
FUNDERS
All threesectors increased their funding forneglecteddiseaseR&D in2016.Thiswas the firstincreaseinseveralyearsfromboththepublicsector(up$49m,2.6%)andthephilanthropicsector(up$28m,4.4%),whileindustry(up$22m,5.3%)increaseditsinvestmentforthefifthyearinarow.ThepublicsectorremainedthemostsignificantsourceofneglecteddiseaseR&Dfundingin2016,contributing justunder two-thirds ($2,034m,64%)of theglobal total.As inpreviousyears,mostpublicsectorfundingcamefromHICgovernmentsandmultilaterals($1,951m,96%).
Thetopthreepublic funders in2016weretheUS,theUKandtheEuropeanCommission (EC)1, with the US contributing nearly three-quarters of all public investment in neglected disease R&D ($1,490m,73%).TheUSalsoprovided the largest increase inpublic funding (up$78m,5.5%),followedby theNetherlands (up$18m,447%)and theUK (up$9.3m,10%).Allof thenotabledecreases inpublic funding forneglecteddiseaseR&D in2016came fromEuropean funders.ThemostsignificantreductioncamefromtheEC(down$49m,-39%),althoughthiswas largelylinkedtounevendisbursementstotheEuropean&DevelopingCountriesClinicalTrialsPartnership(EDCTP).Nearly two-thirds (59%)ofallHICgovernmentandmultilateral fundingwent tobasicandearlystageresearch,withonlyaquarter(27%)goingtoclinicalorfielddevelopmentandpostregistration studies.
Thephilanthropicsectorprovided$671mforneglecteddiseaseR&Din2016,representing21%oftotalglobal funding.TheGatesFoundationandtheWellcomeTrustcollectivelyprovidedthevastmajority($642m,96%)ofallphilanthropicfunding,andbothincreasedtheirinvestmentin2016(up$12m,2.3%andup$17m,21%,respectively).Athird(34%)ofallphilanthropicfundingforneglecteddisease R&D was for basic and early stage research, most of which was for discovery and pre-clinicalR&D,aquarter (26%)was forclinicalorfielddevelopmentandpost registrationstudies,andtheremaining40%was largelyprovided inaportfolio-basedapproach, tosupportproductdevelopment from discovery through to registration.
1 The term ‘EC’ refers to funding from the EU budget that is managed by the European Commission or related EU partnerships and initiatives,suchastheEuropean&DevelopingCountriesClinicalTrialsPartnershipandInnovativeMedicinesInitiative

PAGE9
EXEC
UT
IVE
SUM
MA
RY
The pr ivate sector invested $497m inneglecteddiseaseR&Din2016,accountingfor 16%of total global funding. For thesecond year in a row, the increase in industry investment was entirely driven by small pharmaceutical and biotechnology firms (SMEs,up$23m,30%).Mostof thisincrease came from SMEs in innovative developing countr ies ( IDCs), and wasdirected towards bacterial pneumonia & meningitis (up$10m,43%)andSalmonella (up$9.4m,86%).Morethanthree-quartersofallSMEinvestmentwasinclinicalorfielddevelopment and post registration studies ($82m,78%),withmostof the remainderinvested in basic and early stage research ($16m,15%).
FUNDING FLOWS
Almostthree-quarters($2,352m,73%)ofallneglecteddiseaseR&Dfundingin2016wasexternalinvestment intheformofgrants.Ofthisfunding,79%($1,851m)wentdirectlytoresearchersanddevelopers,18%($420m)was forproductdevelopmentpartnerships (PDPs),andtheremaining$80m (3.4%)waschannelled throughother intermediaryorganisations.DirectYOY funding toresearchersanddevelopersincreasedforthefirsttimesince2012(up$147m,9.1%),drivenbybothS&Tagenciesandphilanthropicorganisations.FundingtoPDPsdecreasedby$29m(-6.8%), tothelowestlevelrecordedinthehistoryoftheG-FINDERsurvey,althoughmostofthedropin2016could be attributed to the highly cyclical nature of grant funding to PDPs, especially from the Gates Foundation.Fundingtootherintermediaryorganisationsdecreasedby$23m(-25%),primarilyduetolowerfundingfromtheECtoEDCTP.
Almosttwo-thirds (62%)ofall fundinggivendirectlytoresearchersanddeveloperswenttobasicandearlystage research,with just22%forclinicalor fielddevelopmentandpost registrationstudies.Theverydifferentpatternof fundinggiven toPDPsreflects theirproduct-developmentfocus.More than two-fifths (42%)ofall funding toPDPswas forclinicalor fielddevelopmentandpost registrationstudies,more thandouble theamount (19%) thatwas forbasicandearlystageresearch (essentiallyallofwhichwasfordiscoveryandpre-clinicalR&D,rather thanbasicresearch).
Internal investmentaccountedfor$851m(27%)oftotalneglecteddiseaseR&Dfunding.Thiswasessentiallysteady(up$4.7m,0.6%),withongoinggrowthin industry investment(up$20m,4.6%),particularlyfromSMEs,offsetbyinternalinvestmentbygovernmentagencies(down$19m,-5.1%).Theallocationofinternalinvestmentdependedonthetypeoforganisation;wheretwo-thirds(66%)of industry self-funding was for clinical or field development and post registration studies, non-industryself-fundingwasfocusedmoreonbasicandearlystageresearch(49%).
Two-thirds of funding to researchers and developers was for basic and early stage research

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE10
EXEC
UT
IVE
SUM
MA
RY
DISCUSSION
Global funding for neglected disease R&D increased for the first time since 2012, driven by an increase in funding from the US government
• GlobalfundingforneglecteddiseaseR&Dincreased(up$99m,3.4%)to$3,203min2016.Thiswasthefirstincreaseinglobalfundingsince2012,andwasdrivenbyincreasedinvestmentfromtheUSgovernment(up$78m,5.5%).
• TheUSgovernmentwasnotalone in increasing funding forneglecteddiseaseR&D in2016.Thephilanthropicsectorand thepharmaceutical industry (particularlySMEs)also increasedtheir investment,asdidtheUK,Dutchandanumberofnon-Europeangovernments,which–inconjunctionwiththeUSgovernmentincrease–wasenoughtoresultinanoverallincreaseinpublic funding, despite lower investment from the EC and several other European governments.
• However, as the largest funder, the US government is the primary driver of changes in global funding for neglected disease R&D: every increase or decrease in US government funding over the last decade has been accompanied by a corresponding change in global investment.
An overreliance on US government funding is defining the shape of R&D for neglected diseases
• TheUSgovernment’sinvestmentof$1,490min2016wastriplethecombinedinvestmentoftherestoftheworld’sgovernments,andfifteentimeslargerthanthatofthenextbiggestgovernmentfunder(theUK,with$101m).
• 82%ofallUSgovernmentfundingforneglecteddiseaseR&Din2016–andconsequently70%ofallglobalfunding–wasforHIV/AIDS,TBandmalaria.
• Excluding the quarter of a billion dollars the US government invested in HIV vaccine clinical trials in2016,80%ofallremainingUSgovernmentfundingforneglecteddiseaseR&D–and70%ofallfundingfromHICgovernments–wasforbasicandearlystageresearch,comparedtojust14%forclinicalorfielddevelopmentandpostregistrationstudies.
The sustained growth in industry investment in neglected disease R&D – lately driven by SMEs – continues to be a good news story
• IndustryinvestmentinneglecteddiseaseR&Dhasincreasedineveryoneofthelastfiveyears,andreachednewrecordhighs ineachof the last threeyears.Since2008, reported industryinvestmenthas increasedbynearly50%,while fundingfromboththepublicandphilanthropicsectors has fallen.
• Thevastbulkofindustryinvestment–andthemajorityoftheincreaseinindustryfundingsince2008–hascomefromMNCs.Since2014however,MNCinvestmenthasessentiallyplateaued,withannualincreasesoflessthan1%inboth2015and2016.
• IncreasedinvestmentbySMEssince2012,particularlyfromthoseinIndia,hashelpedtosustainthe growth of overall industry investment. Importantly, much of this investment growth has also been innewareas: two-thirdsofallSME investment in2016was forbacterialpneumonia&meningitis, Salmonella infections and diarrhoeal diseases.

PAGE11
EXEC
UT
IVE
SUM
MA
RY
In addition to SMEs, a number of other funders have been making a small but growing contribution in areas of need
• Anumberofkeyglobalhealthinitiatives–Unitaid,MSFandGavi–haveexpandedtheirfocustoincludesupportforneglecteddiseaseR&D,particularlyforclinicalorfielddevelopmentandpostregistration studies.
• TheJapanesegovernment–alongwithJapanesepharmaceuticalcompanies– is increasinglyinvesting inneglecteddiseaseproductdevelopment following theestablishmentof theGHITFund,recordingitshighesteverinvestmentin2016.
• FundingfromLMICgovernmentsgrewby$18m(up30%)in2016,to$84m,withIndiabecomingthe fourth largest government funder of neglected disease R&D, ahead of both France and Germany.
Conclusion
TheUSgovernment’scontribution toneglecteddiseaseR&D funding isunparalleled.ButanoverrelianceonUSgovernment funding isreflected in theheavyconcentrationofglobal fundingonHIV/AIDS,malariaandTB,andtheoverwhelming focusofHICgovernment fundingonbasicandearlystageresearch.Thegrowthofnon-traditional funders ispromising,but theircollectivecontribution is still just a fraction of overall global funding. And while Gates Foundation investment in product development has consistently been relied on to balance the public sector focus on basicresearch– ithasprovided55%ofall fundingtoPDPsand47%ofall funding forplatformtechnologiesoverthelastdecade–thisisagainareflectionofoverrelianceonasinglefunder.TheworldcanillaffordtokeeprelyingontheUSgovernmentandtheGatesFoundationtoprovidetwo-thirds of all global funding for neglected disease R&D over the next ten years, as they have done for the last decade.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE12
INT
RO
DU
CT
ION INTRODUCTION
Background to the G-FINDER survey
Each year since 2007, the G-FINDER project has provided policy-makers, donors, researchers and industrywithacomprehensiveanalysisofglobalinvestmentintoresearchanddevelopment(R&D)of new products to prevent, diagnose, control or cure neglected diseases in developing countries. It provides an up-to-date analysis of how R&D investments are being allocated across diseases and product types, funding trends over time, and where the potential gaps lie. G-FINDER is the primary sourceofneglecteddiseaseR&Dfundingdata forboth theWorldHealthOrganization’s (WHO)GlobalObservatoryonHealthR&DandDonorTracker,andhelpssupporttheworkofmanyothergroups in the broader global health community.
ThisisthetenthannualG-FINDERreport;inadditiontothepreviousnineyearsoffundingdata,itreportsoninvestmentsmadeinfinancialyear2016,referredtoas2016inthetext.
The survey scope
DEFINING NEGLECTED DISEASES AND PRODUCTS
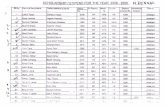
Thescopeof theG-FINDERsurvey isdetermined inconsultationwith theG-FINDERAdvisoryCommittee, which is made up of a broad cross-section of international experts in neglected diseasesandproductdevelopment (seeAnnexe1 for the listofcurrentAdvisoryCommitteemembers).WhendefiningtheG-FINDERscopeat theproject’s inception,andatallsubsequentreviews,threekeycriteria(seeFigure1)havebeenappliedinordertoestablishalistofneglecteddiseases and products for which R&D would cease or wane if left to market forces.
Figure 1. Filter to determine G-FINDER inclusions
The disease disproportionately affects people in developing countries
YES
There is a need for new products (i.e.thereisnoexistingproductORimproved
oradditionalproductsareneeded)
There is market failure (i.e.thereisinsufficientcommercialmarket
toattractR&Dbyprivateindustry)
YES
YES
NO
Included in G-FINDER survey
NO
NO
Excluded from G-FINDER survey

PAGE13
INT
RO
DU
CT
ION
Althoughall relevantproduct types–drugs,vaccines (preventiveandtherapeutic),diagnostics,microbicidesandvectorcontrolproducts (pesticides,biologicalcontrolagentsandvaccinestargetinganimal reservoirs)–aswellasbasic researchwereconsidered foralldiseases, it isimportant to note that not all product types are included in the G-FINDER scope for all diseases, and some are included only with restrictions. For example, pneumonia drugs are excluded because thereisasufficientcommercialmarket;whilepneumoniavaccineinvestmentsareonly includedifthey meet G-FINDER requirements for strain, vaccine type and target age group.
Platformtechnologies (adjuvants,diagnosticplatformsanddeliverydevices)arealso included inthe scope of G-FINDER. Platform technologies can potentially be applied to a range of neglected diseasesandproducts,buthavenotyetbeenattachedtoaspecificproductforaspecificdisease.
Investmentsthatdonotmeet theG-FINDERscopeareexcludedfromtheresults.This includesactivitiessuchasadvocacyandbehavioural research,whichare importantandcritical toeffectchange, however are distinct from product development and fall outside the G-FINDER criteria.
A comprehensive explanation of all inclusions, exclusions and restrictions is outlined in the detailed G-FINDER R&D scope document, which is available online. A matrix summarising the neglected diseases,productsandtechnologiesincludedinthisyear’sG-FINDERreportisshowninTable1.
CHANGES TO THE G-FINDER R&D SCOPE FOR NEGLECTED DISEASES
Although it is important to maintain a consistent scope in order to allow comparable, long-term analysis of multi-year R&D funding trends, the scope of the G-FINDER survey is reviewed annually in consultation with the Advisory Committee.
InyeartwooftheG-FINDERsurvey(FY2008),thetyphoidandparatyphoidfeverdiseasecategorywas expanded to include non-typhoidal Salmonella enterica (NTS)andmultipleSalmonella infections,andR&Dforlymphaticfilariasisdiagnosticswasadded.
InFY2013(theseventhsurveyyear),thesurveywasexpandedtoincludethreeadditionaldiseases:cryptococcalmeningitis,hepatitisC (genotype4)and leptospirosis.Denguevaccinesweredeterminedtonolongerfitthecriteriafor inclusion intheG-FINDERsurveygiventheemergenceofacommercialmarket,anddenguevaccineR&D funding (includingallpreviously reportedinvestment)wasremovedfromthesurvey.Allotherdengueproductareaswereretained.
InFY2014(theeighthsurveyyear),thehepatitisCcategorywasexpandedtocapture investmentinR&Dfortwoadditionalgenotypes(genotypes5and6) thatdisproportionatelyaffectpeople indeveloping countries.
Thisyear (FY2016, thetenthyearof thesurvey), thebacterialpneumonia&meningitiscategorywas expanded to include developing country-focused basic research for both Streptococcus pneumoniae (S. pneumoniae)and/orNeisseria meningitidis (N. meningitidis).Developingcountry-specificresearchintotherapeuticvaccinesforHIV/AIDSwasalsoaddedasarestrictedcategory,reflectingemerging research intobroadlyneutralisinganti-HIVantibodies (bNAbs)and theirpotential use in developing countries.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE14
INT
RO
DU
CT
ION Table 1. G-FINDER neglected diseases, products and technologies
HIV/AIDS Restricted Restricted Restricted -
Malaria P. falciparum - -
P. vivax - -
Multiple and/or other malaria strains - -
Tuberculosis - -
Diarrhoeal diseases Rotavirus - - Restricted - - - -
Shigella Restricted - - -
Cholera Restricted - - -
Cryptosporidium Restricted - - -
Enterotoxigenic E. coli (ETEC) - - - - -
Enteroaggregative E. coli (EAggEC) - - - - -
Giardia - - - - - -
Multiple diarrhoeal diseases Restricted - - -
Kinetoplastids Leishmaniasis - -
Sleepingsickness(HAT) - -
Chagas’ disease -
Multiple kinetoplastid diseases -
Dengue - - -
Bacterial pneumonia & meningitis S. pneumoniae Restricted - Restricted - - -
N. meningitidis Restricted - Restricted - - -
Both S. pneumoniae and N. meningitidis Restricted - - - - -
Salmonella infections Typhoidandparatyphoidfever (S. Typhi, S. ParatyphiA) - - -
Non-typhoidal S. enterica (NTS) - - -
Multiple Salmonella infections - - -
Helminth infections (worms & flukes) Schistosomiasis(bilharziasis) - -
Lymphaticfilariasis(elephantiasis) - - -
Onchocerciasis(riverblindness) - -Hookworm (ancylostomiasis&necatoriasis) - - - -
Tapeworm(taeniasis/cysticercosis) - - - -
Whipworm(trichuriasis) - - - - -Strongyloidiasis & other intestinal roundworms - - -
Roundworm(ascariasis) - - - - -
Multiple helminth infections - -
Hepatitis C (genotypes 4, 5 & 6) - Restricted - - -
Leprosy - - - -
Cryptococcal meningitis - - - - - -
Buruli ulcer - - -
Leptospirosis - - - - Restricted - -
Trachoma - - - - -
Rheumatic fever - - - - - -
Other investment applicable to more than one neglected disease
Platform technologiesCore funding of a multi-disease
R&D organisationGeneral diagnostic platforms Adjuvants and immunomodulators Delivery technologies and devices
Restricted Restricted Restricted
Basic research
Drugs Vaccines
(preventive)Vaccines
(therapeutic)
Diagnostics
MicrobicidesVector control
productsDisease

PAGE15
HANDLING OF EMERGING INFECTIOUS DISEASES
Inresponsetothe2014WestAfricanEbolaepidemic, theFY2014(yeareight)G-FINDERsurveyscope was expanded to capture investments in Ebola R&D for diagnostics, drugs and preventive vaccines,aswellasbasicresearch.ForFY2015(yearnine),thesurveyscopewasfurtherexpandedto includeotherAfricanviralhaemorrhagic fevers (VHFs). InadditiontoEbola, thisnewcategoryallowed respondents to report R&D funding for Marburg and other African VHFs.
BecauseoftheuniquenatureoftheEbolathreatandglobalresponse,anditsdistortingeffectonanalysis of the R&D funding landscape for neglected diseases, R&D funding for Ebola and other African VHFs was analysed separately in the year nine G-FINDER report.
Theseparationofemerging infectiousdiseases (EIDs)andneglecteddiseaseswas formalisedthisyear.FortheFY2016(yearten)survey,aseparatescopedefinitionwasdevelopedto identifyinvestments inR&DforallpriorityEIDs identified intheWHOR&DBlueprint foractiontopreventepidemics. EID data is not included in this G-FINDER neglected disease report, and will be reported separately.
TYPES OF RESEARCH INCLUDED
ThepurposeofG-FINDER is to track andanalyseglobal investment in the research anddevelopment of new health technologies for neglected diseases. It does not, and is not intended to, captureinvestmentintheentirespectrumofneglecteddiseaseresearch.Thereisabroadrangeofresearch activities that are extremely important for improving global health, but which are excluded from this report because they are not related to the development of new tools for neglected diseases,includinghealthsystemsandoperations/implementationresearch(forexample,researchinto health systems or policy issues, or research into the programmatic delivery of non-product interventions,orexistinghealth technologies),andsociological,behaviouralandepidemiologicalresearch not related to the development of new health technologies. We also exclude investment into non-pharmaceutical tools such as untreated bed nets, or interventions such as circumcision. General therapies such as painkillers or nutritional supplements are excluded, as these investments cannot be ring-fenced to neglected disease treatment only. Investment that is not research-related is similarly excluded: although we recognise the vital importance of activities such as health programme delivery, advocacy, routine disease surveillance programmes, community education and general capacity building to address neglected diseases, investment in these activities falls outside the scope of G-FINDER.
G-FINDERquantifiesneglecteddiseaseR&D investments intotwooverarchingcategories,eachbroken down into a number of further categories:
• Basic and early stage research, including: • Basic research • Product discovery and pre-clinical development• Clinicalandfielddevelopmentandpostregistrationstudies,including: • Baseline epidemiology in preparation for product trials • Clinicalorfieldproductdevelopment • Phase IV/pharmacovigilance studies of new products
A detailed explanation of what types of R&D activities are included in each of these categories, aswellasspecific inclusionsandexclusionsrelatedto theG-FINDERscope, isprovided in theG-FINDER neglected disease R&D scope document, which is available online.
INT
RO
DU
CT
ION

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE16
Survey methodology
DATA COLLECTION
Over the past decade, the G-FINDER survey has operated according to two key principles: capturing and analysing data in a manner that is consistent and comparable across all funders and diseases;andpresentingfundingdatathatisascloseaspossibleto‘real’investmentfigures.
G-FINDER was originally designed as an online survey. An online survey platform was developed tocapturegrantdataandisstillusedbythemajorityofsurveyparticipants.Anofflinegrant-basedreporting tool isalsoavailable. Industry (pharmaceuticalcompaniesandbiotechnology firms)investment in R&D is not grant-based, so the reporting tool has been tailored for these participants. Insteadofgrants,companiesenterthenumberofstaffworkingonneglecteddiseaseprogrammes,their salaries, and direct project costs related to these programmes. Companies are required to exclude‘softfigures’suchasin-kindcontributionsandcostsofcapital.
Forsomeorganisationswithverylargedatasets,theonlinesurveyandequivalentofflinereportingtool aredifficult touse.TheG-FINDER teamwas thereforeasked tousepubliclyavailabledatabasesto identify therelevant funding.For theUSNational InstitutesofHealth (NIH),grantswerecollectedusingtheResearchPortfolioOnlineReportingTools(RePORTER)andtheResearch,ConditionandDiseaseCategorization (RCDC)process.For theBiomedicalAdvancedResearchandDevelopmentAuthority (BARDA), funding informationwas identifiedusing the internationaland domestic ‘Project Maps’ retrieved from the Medical Countermeasures website. Funding from theEuropeanCommission (EC)^ was retrieved from the Community Research and Development InformationService (CORDIS)publicdatabaseand InnovativeMedicines Initiative’s (IMI)onlineproject list. Supplementary data was provided by the EC.
Allparticipatingorganisationswereaskedtoonly includedisbursements (orreceipts), ratherthancommitmentsmadebutnotyetdisbursed.Ingeneral,onlyprimarygrantdatawasaccepted;theonly exception is in the case of data collection collaborations between G-FINDER and other R&D fundingsurveys,suchasAVAC.Datafromallsourceswassubjecttoverificationusingthesameprocesses and inclusion criteria.
VALIDATION
Allentriesover$0.5mwereverifiedagainstthe inclusioncriteria.Cross-checkingwasconductedusingautomated reconciliation reports–whichmatch investments reportedasdisbursedbyfunderswith investments reportedas receivedby intermediariesandproductdevelopers–followed by manual grant-level review of the report outputs. Any discrepancies were resolved by contactingbothgroupstoidentifythecorrectfigure.ForgrantsfromtheUSNIH,fundingdatawassupplementedandcross-referencedwith informationreceivedfromtheOfficeofAIDSResearch(OAR)andtheNationalInstituteofAllergyandInfectiousDiseases(NIAID).
UNSPECIFIED FUNDING
Around2.3% ($73m)of fundingwas reported to thesurveyas ‘unspecified’,usually formulti-disease programmes where funds could not easily be apportioned by disease. A proportion of fundingforsomediseaseswasalso‘unspecified’,forinstance,whenfundersreportedagrantforresearch into tuberculosis (TB)basic researchanddrugswithoutapportioning funding toeachproductcategory.Thismeansthatreportedfundingforsomediseasesandproductswillbeslightlylowerthanactualfunding,withthedifferencebeingincludedas‘unspecified’funding.
INT
RO
DU
CT
ION
^ The term ‘EC’ used here and throughout the report refers to funding from the European Union budget that is managed by the European Commissionor relatedEuropeanUnionpartnershipsand initiatives,suchas theEuropean&DevelopingCountriesClinicalTrialsPartnership(EDCTP)andInnovativeMedicinesInitiative(IMI)

PAGE17
A further4.2% ($136m)wasgivenascore funding toR&Dorganisations thatwork inmultiplediseaseareas,forexample,theEuropean&DevelopingCountriesClinicalTrialsPartnership(EDCTP)andtheFoundationforInnovativeNewDiagnostics(FIND).Asthisfundingcouldnotbeaccuratelyallocated by disease it was reported as unallocated core funding. In cases where grants to a multi-diseaseorganisationwereearmarkedforaspecificdiseaseorproduct,theywereincludedunderthespecificdisease-productarea.
DATA AGGREGATION
Allpharmaceutical industryfundingdatahasbeenaggregatedandanonymisedforconfidentialitypurposes. Rather than being attributed to individual companies, pharmaceutical company investment is instead reported according to the type of company, with a distinction made between multinationalpharmaceuticalcompanies (MNCs)andsmallpharmaceuticalandbiotechnologycompanies(SMEs).
INFLATION ADJUSTMENTS
Fundingdatahasbeenadjusted for inflationandconverted toUSdollars (US$) toeliminateartefactualeffectscausedbyinflationandexchangeratefluctuations,allowingaccuratecomparisonofannualchanges.Duetotheseadjustments,historicalG-FINDERdataintablesandfiguresinthisreportwilldiffertodatainpreviousG-FINDERreports.Allfundingdatainthisreportisin2016US$.
LIMITATIONS
Whilethesurveymethodologyhasbeenrefinedoverthepastdecade,therearelimitationstothedata presented, including survey non-completion, time lags in the funding process, an inability to disaggregate some investments, and non-comparable or missing data. Please see the G-FINDER methodologydocument,availableonlineatwww.policycuresresearch.org/g-finder-2017,foramorein-depth discussion of these limitations.
Reading the G-FINDER report
STRUCTURE
TheG-FINDERreportisstructuredinfourmainparts:1)analysisoffundingbyneglecteddisease;2)analysisofneglecteddisease funders;3)analysisof funding flows;and4)discussionofkeyfindings.
YEARS
Throughoutthetext,referencestoyears,otherthansurveyyears,refertofinancialyears.
INT
RO
DU
CT
ION

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE18
YEAR-ON-YEAR CHANGES
It is important when comparing figures between survey years to distinguish between genuine changes in funding and apparent changes due to fluctuating numbers of survey participants. Therefore,toclearlydemonstrategenuinefundingchanges,anyincreasesordecreasesinfundingexplicitly described in the report rely only on data from organisations that have participated in every yearofthesurvey,referredtoas‘year-on-year(YOY)funders’.Newfundingstreams,forexampletheintroductionoftheGlobalHealthInnovativeTechnologyFund(GHIT),arealsoincludedinYOYanalysis.TheYOYamountsreportedmaynotalwaysmatchtheYOYamountsreportedinpreviousyears due to participation changes.
COUNTRY GROUPINGS
For brevity, we use the terms ‘LMICs’ and ‘developing countries’ to denote low- and middle-income countriesand‘HICs’ todenotehigh-incomecountriesasdefinedbytheWorldBank.1 Innovative developingcountries(IDCs)aredevelopingcountrieswithastrongR&Dbase,whichinthecontextof this report refers to Brazil, India and South Africa.
BURDEN OF DISEASE FIGURES
Estimating the burden of disease is a complex process, and estimates may differ substantially betweensourcesdependingon thedataandmethodologyused.This reportpresentsdiseaseburdenestimates fromtwokeysources: the Institute forHealthMetricsandEvaluation’s (IHME)GlobalBurdenofDiseaseStudy2015 (GBD2015),2 and the World Health Organization’s Global HealthEstimates2015(GHE2015).3Estimatesofmortalityanddisability-adjustedlifeyears(DALYs)inLMICs fromGBD2015arepresented forallG-FINDERneglecteddiseases,whereavailable.EstimatesofglobalandLMICmortalityfromGHE2015arealsoincluded,whereavailable.WenotesomeGBD2015estimatesmaydifferfromthosepublishedinpreviousG-FINDERreportsduetoupdates to IHME’s methodology.4
Pathogen specific diagnosis for diarrhoeal diseases, and bacterial pneumonia & meningitis is challenging,whichaffectsestimatesforburdenofdisease.Thediarrhoealdiseasegroup inGBD2015 ispresentedbycauseand includesdiseasesoutside thescopeofG-FINDER,anddoesnot includeestimates forGiardia.Therefore,estimatesofmortalityandDALYsfor thediarrhoealdiseasegrouppresented inthisreporthavebeencalculatedbysubtractingpathogens identifiedbyaetiologyasoutofscopefromtheGBD2015diarrhoealdiseasegroupingbycausetotals.GBD2015includesan‘Othermeningitis’aetiologycategorythatisnotdisaggregatedtoalevelwhereitcan be established what proportion of the data falls in or out of the scope of G-FINDER. Estimates of mortality and DALYs for bacterial pneumonia & meningitis presented in this report include ‘Other meningitis’, and may therefore include some burden of disease caused by pathogens outside the scopeofG-FINDER.Forhelminthinfections(wormsandflukes),GBD2015figurespresentedinthisreport do not include estimates for strongyloidiasis.
INT
RO
DU
CT
ION

PAGE19
The latest G-FINDER survey
ThetenthG-FINDERsurveywasopenforaseven-weekperiodfromJunetoJuly2017. Intensivefollow-upandsupportforkeyparticipantsledtoatotalof10,144recordedentriesinthedatabaseforfinancialyear2016.
PARTICIPANTS
G-FINDER is primarily focused on funding, and therefore the emphasis is on surveying funding organisations.Atotalof187organisationsparticipatedintheG-FINDERsurveyin2017,reportingonbehalfof194organisations.123of the187directparticipantswerefunders.Awiderangeoffundingintermediaries,productdevelopmentpartnerships(PDPs),andresearchersanddeveloperswho received funding also participated. Data from funding recipients was used to collect data on investments fromfunderswhodidnotparticipate in thesurvey; tobetterunderstandhowandwhereR&Dinvestmentsweremade;totrackfundingflowsthroughthesystem;topreventdoublecounting;andtoverifyreporteddata.
Participantsoriginatedfrom32countries.Organisationsincluded:
• Public,privateandphilanthropicfundersfrom21HICs• TheEC• PublicfundersinthreeIDCs(Brazil,IndiaandSouthAfrica)• PublicfundersinanadditionalfourMICs(Argentina,Colombia,MexicoandThailand)• PrivatesectorfundersintwoMICs(BrazilandIndia)• Academic organisations from six MICs.
INT
RO
DU
CT
ION
ONLINE SEARCH TOOL
All of the data behind the G-FINDER report is available through the online search tool at https://gfinder.policycuresresearch.org/PublicSearchTool

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE20
Table 2. Disease and product R&D funding 2016 (US$ millions)
INT
RO
DU
CT
ION
HIV/AIDS 169.87 24.26 724.29 9.18 28.91 124.59 21.21 1,102.30
Malaria 138.90 218.11 115.54 20.53 59.89 23.42 576.40
P. falciparum 68.78 89.76 73.98 8.04 6.99 7.11 254.66
P. vivax 9.73 59.49 7.02 5.97 0.47 0.48 83.15
Multiple and/or other malaria strains 60.40 68.87 34.54 6.53 52.42 15.83 238.58
Tuberculosis 151.84 262.19 74.34 5.81 51.33 22.60 568.11
Diarrhoeal diseases 34.14 6.83 84.75 11.90 7.78 145.39
Rotavirus 37.94 0.92 38.86
Shigella 5.67 0.42 15.44 1.36 0.99 23.89
Cholera 15.19 0.54 6.46 1.10 0.07 23.37
Cryptosporidium 6.24 5.74 1.01 0.25 0.26 13.50
Enterotoxigenic E. coli(ETEC) 9.18 0.41 0.09 9.68
Enteroaggregative E. coli (EAggEC) 0.54 0.21 0.08 0.82
Giardia 0.02 0.12 0.14
Multiple diarrhoeal diseases 7.04 0.12 14.19 8.56 5.25 35.16
Kinetoplastids 50.30 61.10 6.40 2.00 4.70 0.78 5.88 131.17
Leishmaniasis 15.81 14.35 4.91 0.30 1.79 4.09 41.25
Sleepingsickness(HAT) 19.00 13.88 0.59 0.96 0.72 1.39 36.54
Chagas' disease 12.07 7.85 0.89 1.70 1.93 0.06 0.05 24.55
Multiple kinetoplastid diseases 3.43 25.02 0.01 - 0.02 - 0.35 28.82
Dengue 49.92 28.43 9.38 19.73 5.36 112.82
Bacterial pneumonia & meningitis 9.29 81.39 0.86 - 91.55
S. pneumoniae 7.52 57.87 0.71 - 66.10
N. meningitidis 0.98 23.52 0.07 - 24.58
Both S. pneumoniae and N. meningitidis 0.79 0.08 - 0.87
Salmonella infections 45.49 3.77 36.84 4.22 1.14 91.46
Typhoidandparatyphoidfever(S. Typhi, S. ParatyphiA) 31.13 2.99 34.53 2.77 - 71.42
Non-typhoidal S. enterica (NTS) 2.96 0.48 0.41 0.81 - 4.66
Multiple Salmonella infections 11.40 0.30 1.91 0.64 1.14 15.38
Helminth infections (worms & flukes) 29.49 30.90 7.70 2.46 0.10 3.90 74.56
Schistosomiasis(bilharziasis) 10.13 2.90 2.24 1.45 0.07 1.58 18.37
Lymphaticfilariasis(elephantiasis) 6.64 7.27 0.12 0.02 1.78 15.82
Onchocerciasis(riverblindness) 1.31 7.36 0.45 0.65 0.02 0.48 10.25
Hookworm(ancylostomiasis&necatoriasis) 0.27 0.85 2.71 0.05 3.87
Tapeworm(taeniasis/cysticercosis) 1.76 1.85 - - 3.61
Whipworm(trichuriasis) 0.87 0.94 - 1.81
Strongyloidiasis & other intestinal roundworms 0.68 0.47 <0.01 0.24 - 1.39
Roundworm(ascariasis) 0.83 0.45 - 1.28
Multiple helminth infections 7.01 8.82 2.30 - - 0.02 18.15
Basic research
Drugs Vaccines
(preventive)Vaccines
(therapeutic)
Diagnostics
MicrobicidesVector control
productsDisease or
R&D areaUnspecified
Total

PAGE21
- No reported funding Category not included in G-FINDER
INT
RO
DU
CT
ION
Hepatitis C (genotypes 4, 5 & 6) 11.92 3.47 6.95 0.03 22.37
Leprosy 6.57 0.18 0.39 3.91 11.06
Cryptococcal meningitis 5.64 5.64
Buruli ulcer 1.05 1.17 - 0.48 0.05 2.76
Leptospirosis 2.31 2.31
Trachoma 1.19 0.22 0.76 2.18
Rheumatic fever 1.18 0.10 1.28
Core funding of a multi-disease R&D organisation 135.99
Unspecified disease 73.18
Platform technologies General diagnostic platforms
Adjuvants and immunomodulators
Delivery technologies and devices
18.30 17.68 16.23 52.21
Total R&D funding 3,202.74
Basic research
Drugs Vaccines
(preventive)Vaccines
(therapeutic)
Diagnostics
MicrobicidesVector control
productsDisease or
R&D areaUnspecified
Total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE22
FUNDING BY DISEASE
Global investment in R&D for neglected diseases in 2016 was $3,203m. Of this total, $3,024m was reported by regular survey participants (called year-on-year – YOY – funders), and the remaining $179m by irregular participants. YOY funding for neglected disease R&D increased for the first time since 2012 (up $99m, 3.4%).
Neglected diseases can be grouped into three distinct tiers according to the amount of R&D funding that each disease receives annually (noting that this does not necessarily reflect the relative burden or funding need of each disease). HIV/AIDS, malaria and tuberculosis (TB) represent the ‘top tier’ of diseases based on the amount of funding received. These three diseases collectively accounted for more than two-thirds ($2,247m, 70%) of total global neglected disease R&D funding in 2016, with HIV/AIDS receiving 34%, and malaria and TB 18% each. Overall funding for top tier diseases increased slightly (up $60m, 2.9%), mainly due to an increased investment in HIV/AIDS (up $83m, 8.3%). Funding for malaria increased modestly (up $13m, 2.5%), while investment in TB fell by $37m (-6.8%).
‘Second tier’ diseases are those that receive between 0.5% and 6.0% of total funding. This group includes diarrhoeal diseases, kinetoplastids, dengue, bacterial pneumonia & meningitis, Salmonella infections, helminth infections and hepatitis C (genotypes 4, 5 & 6). Funding for second tier diseases represented one-fifth ($670m, 21%) of all neglected disease R&D funding in 2016, and total investment in this tier was essentially unchanged from the previous year (up $0.9m, 0.2%). Only three second tier diseases saw funding increases in 2016: Salmonella infections (up $21m, 32%), kinetoplastids (up $12m, 12%) and dengue (up $8.4m, 8.7%). Funding fell for all other second tier diseases, with the largest drop being for diarrhoeal diseases (down $21m, -14%), followed by hepatitis C (down $12m, -36%), helminths (down $3.9m, -5.5%) and bacterial pneumonia & meningitis (down $3.1m, -3.8%).
Figure 2. Total R&D funding for neglected diseases 2007-2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US
$ (m
illio
ns)
2,200
2,400
2,600
2,800
3,000
3,200
3,400
3,600
0

FIN
DIN
GS
- D
ISEA
SES
PAGE23
The most poorly funded neglected diseases covered by the G-FINDER survey – those in the third tier of funding – each receive less than 0.5% of global funding. This tier includes leprosy, cryptococcal meningitis, Buruli ulcer, leptospirosis, trachoma and rheumatic fever. Total funding for this third tier made up just under one percent ($25m, 0.8%) of global investment, unchanged from 2015. Leprosy received the most funding of all third tier diseases ($11m, 0.3%) while rheumatic fever received the least ($1.3m, <0.1%). Due to the small numbers of funders and grants for each of these diseases in any given year, it is not possible to meaningfully comment on funding trends.
New disease added to G-FINDER in 2013^ Please note that some of the diseases listed are actually groups of diseases, such as the diarrhoeal illnesses and helminth
infections. This reflects common practice and also the shared nature of research in some areas. For example, Streptococcus pneumoniae R&D is often targeted at both pneumonia and meningitis
Table 3. R&D funding by disease 2007-2016^
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
HIV/AIDS 1,225 1,316 1,285 1,216 1,171 1,207 1,110 1,081 1,031 1,102 34.4
Malaria 492 585 641 567 590 577 531 577 563 576 18.0
Tuberculosis 452 495 605 622 577 553 564 569 576 568 17.7
Diarrhoeal diseases 128 149 204 177 167 169 200 175 161 145 4.5
Kinetoplastids 133 149 173 156 139 141 119 139 114 131 4.1
Dengue 51.5 52.7 79.9 68.7 79.3 79.8 76.0 85.9 101 113 3.5
Bacterial pneumonia & meningitis 33.0 99.9 75.1 102 106 110 102 74.8 93.3 91.5 2.9
Salmonella infections 10.4 44.5 44.2 48.8 48.3 58.1 65.5 66.1 69.1 91.5 2.9
Helminth infections (worms & flukes) 56.7 75.2 87.2 80.8 87.0 92.2 92.8 92.8 78.1 74.6 2.3
Hepatitis C (genotypes 4, 5 & 6) 47.3 45.4 34.1 22.4 0.7
Leprosy 6.2 10.9 11.9 10.3 8.9 15.1 12.9 10.7 11.0 11.1 0.3
Cryptococcal meningitis 3.1 5.6 5.6 5.6 0.2
Buruli ulcer 2.4 1.9 1.9 5.5 5.7 6.0 6.4 3.7 1.9 2.8 0.1
Leptospirosis 0.4 1.3 1.3 2.3 0.1
Trachoma 1.4 1.8 1.3 3.5 5.9 2.1 2.2 1.4 1.2 2.2 0.1
Rheumatic fever 1.9 2.5 3.4 2.0 0.9 1.0 0.9 1.3 2.3 1.3 <0.1
Platform technologies 9.8 17.8 24.6 30.6 18.2 50.6 44.7 22.8 33.7 52.2 1.6
General diagnostic platforms 5.2 5.9 9.9 10.6 10.6 17.4 16.9 9.8 13.8 18.3 0.6
Adjuvants and immunomodulators 2.6 2.6 5.6 10.3 5.8 28.3 21.7 8.6 12.2 17.7 0.6
Delivery technologies and devices 2.0 9.3 9.0 9.7 1.9 5.0 6.2 4.4 7.6 16.2 0.5
Core funding of a multi-disease R&D organisation
108 97.2 70.6 73.1 87.5 105 107 88.2 115 136 4.2
Unspecified disease 59.2 85.6 85.0 55.3 76.0 110 91.8 70.4 79.9 73.2 2.3
Total 2,771 3,185 3,393 3,219 3,168 3,277 3,177 3,112 3,073 3,203 100
2016 % of total
US$ (millio
ns)
Disease or
R&D area

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE24
Figure 3. Funding distribution 2007-2016^
Non-disease-specific R&D investment totalled $261m in 2016 (8.2% of global funding), with YOY funding for this category increasing by $37m (up 17%). Core funding accounted for just over half ($136m, 52%) of all non-disease-specific investment in 2016, and increased by $15m (up 14%). Notably, this increase occurred despite a significant drop in core funding from the EC (down $32m, -79%), which was the result of a number of extraordinary payments to EDCTP in 2015 that would otherwise have been made in 2014 and 2016. The largest increases in core funding came from the Wellcome Trust, with a nearly seven-fold increase (up $32m, 588%), largely to its own clinical research collaborations in LMICs; and the UK Department for International Development (DFID, up $6.2m, 34%), particularly to FIND and EDCTP.
Platform technologies – tools that can potentially be applied to a range of areas, but which are not yet focused on a specific product or disease – received $52m in 2016 (20% of all non-disease specific funding); the largest investment ever reported for this area. Funding for platform technologies was evenly distributed between diagnostic platforms ($18m, 35%), adjuvants and immunomodulators ($18m, 34%) and delivery technologies ($16m, 31%). Funding increased for all three areas: investment in delivery technologies rose by $8.6m (up 113%), almost entirely due to increased funding from the Gates Foundation (up $8.0m, 138%); investment in adjuvants and immunomodulators increased by $5.3m (up 44%), driven by the US NIH (up $6.9m, from a low base); and diagnostic platform investment rose slightly (up $3.8m, 29%), due to a $7.7m (138%) increase in Gates Foundation funding to SMEs.
^ Percentages do not add to 100% because of non-disease specific and unclassified funding
gTop tier diseases
gSecond tier diseases
gThird tier diseases
Top tier diseases (%)
Second tier diseases (%)
Third tier diseases (%)0
10
20
30
40
50
60
70
80
90
100
500
1,000
1,500
2,000
2,500
3,000
3,500
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US
$ (m
illio
ns)
% o
f fun
ding
0

FIN
DIN
GS
- D
ISEA
SES
PAGE25
HIV/AIDS
The Human Immunodeficiency Virus (HIV) attacks and destroys CD4 cells in the human immune system. Without treatment, HIV-infected individuals gradually become more susceptible to other diseases, and eventually develop the Acquired Immunodeficiency Syndrome (AIDS); people with AIDS often die from opportunistic infections like TB or cryptococcal meningitis, or cancers like Kaposi’s sarcoma.5
According to the IHME Global Burden of Disease study, HIV/AIDS ranked as the second highest cause of mortality and morbidity of all the G-FINDER neglected diseases in 2015, causing 1.2 million deaths and 66 million DALYs in developing countries.2 The WHO Global Health Estimates suggest a slightly lower mortality figure, estimating that HIV/AIDS was responsible for 1.1 million deaths in developing countries in 2015.3
There is currently no vaccine against HIV, and the rapid mutation of the HIV virus has posed a significant challenge to vaccine development. The most advanced vaccine candidates to date demonstrated only modest efficacy in the RV144 Phase III clinical trials in 2009.6 HVTN 702, a Phase IIb/III trial investigating a modified version of the RV144 vaccine regimen, started in South Africa in 2016.7 There are several other preventive approaches in Phase I and II trials: NIAID’s VRC01 candidate, currently in Phase IIb, is based on broadly neutralising anti-HIV antibodies (bNAbs), a new area of investigation for HIV vaccines.8 bNAb-based approaches are also being investigated for use as therapeutic vaccines, which are designed to control HIV infection by boosting the body’s natural immunity; developing country-specif ic therapeutic vaccine R&D was included in the G-FINDER scope for the first time this year. Several therapeutic vaccine candidates are in Phase I and II clinical trials, including plasmid and viral vector DNA vaccines, and bNAb immunotherapies.9,10
Commercially-driven R&D of antiretroviral (ARV) drugs is excluded from the G-FINDER scope; only R&D targeting the unmet needs of developing countries (for example, paediatric formulations or long-acting injectable drugs for PrEP) is included. The Drugs for Neglected Diseases initiative (DNDi) is developing two ‘4-in-1′ taste-masked fixed-dose formulations designed specifically for children which combine LPV/r with two NRTIs; these are currently in Phase I trials.11 One long-acting injectable PrEP candidate, cabotegravir, is in Phase IIb/III trials.12 Microbicides are preventive tools designed to block transmission of HIV through the vaginal and/or rectal mucosa; the International Partnership for Microbicides’ (IPM) dapivirine ring has completed Phase III trials, and is currently undergoing regulatory review by the European Medicines Agency (EMA).13
Current methods for early diagnosis are often not adapted to, or suitable for, developing countries, especially for early infant diagnosis. There has been progress towards robust, simple, rapid point-of-care diagnostics, with several promising candidates in development. These include Alere’s q HIV-1/2 Detect and Cepheid’s Xpert HIV-1 Qual Assay, both of which are WHO prequalified for early infant diagnostic use and are currently undergoing field evaluations.14
TOTAL SPEND ON HIV/AIDS
R&D IN 2016
$1.10 BILLION
OF GLOBAL R&D FUNDING
IN SCOPE
OUT OF SCOPE
IN SCOPE
RESTRICTED
RESTRICTED
RESTRICTED
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
MICROBICIDES
32%
34%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE26
Global funding for HIV/AIDS R&D in 2016 was $1,102m. This was the most of any neglected disease, and represented one-third (34%) of all neglected disease R&D investment in 2016. Regular survey participants (YOY funders) increased their investment by $83m (up 8.3%) to $1,092m, ending a three year decline in HIV/AIDS funding and restoring investment to 2013 levels. Irregular participants provided the remaining $10m.
Around two-thirds of HIV/AIDS R&D funding in 2016 went to preventive vaccines ($724m, 66%), with most of the remainder going to basic research ($170m, 15%) and microbicides ($125m, 11%). Diagnostics ($29m, 2.6%) and developing country-focused drug R&D ($24m, 2.2%) each received relatively little funding in comparison. R&D for therapeutic vaccines specifically meeting developing country needs – a product category included for the first time in this year’s G-FINDER report – received $9.2m (0.8%), mainly from the Gates Foundation.
There was a major funding increase for preventive vaccine R&D (up $97m, 16%), resulting in the largest investment in this product area since 2009, and its highest share of total HIV/AIDS R&D funding since the start of the survey. Almost all of this increase came from three sources: the US National Institutes of Health (NIH, up $35m, 8.2%), for the pre-clinical development of HIV vaccine candidates; and industry (up $27m, 65%) and the Gates Foundation (up $23m, 32%), for clinical trials. Diagnostics was the only other product area to receive more funding than last year (up $9.8m, 55%), due to increases from the US NIH (up $6.4m, 60%) and the Gates Foundation (up $4.4m, from a low base). In contrast, funding for microbicides fell to historically low levels (down $24m, -16%), with reduced investment by the two main funders of this area – the US NIH (down $12m, -12%) and the US Agency for International Development (USAID, down $11m, -37%) – reflecting the conclusion of Phase III trials for the dapivirine ring. Funding for drug development also fell (down $3.2m, -14%), while basic research investment remained essentially steady (down $1.9m, -1.1%).
Figure 4. HIV/AIDS R&D funding by product type 2007-2016
Basic research
Drugs
Vaccines (Preventive)
Vector control products
Microbicides
Diagnostics
Unspecified
Vaccines (Therapeutic)
C84 M11 K9
C49 Y39
C91 M53 Y43 K5
C38 M6
C54 M52 Y76
M5 Y100 K14
M4 Y5 K12
C40 Y93
17% 15% 16% 17% 18% 18% 18% 16% 17% 15%
0.1% 4% 3% 3% 2% 2% 2% 3% 3% 2%
64% 59% 58% 58% 58% 57% 60% 61% 61% 66%
0.8%
18% 20%
18% 17% 16% 17%
17% 15% 15%
11%
1% 2%
4%
3% 3% 3%
2% 2% 2%
3%
0
200
400
600
800
1,000
1,200
1,400
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US
$ (m
illio
n)
gUnspecified
gDiagnostics
gMicrobicides
gVaccines (therapeutic)
gVaccines (preventive)
gDrugs
gBasic research

FIN
DIN
GS
- D
ISEA
SES
PAGE27
Just over half of all HIV/AIDS R&D funding in 2016 was for basic and early stage research ($559m, 51%), with most of the remainder going to clinical development and post registration studies ($455m, 41%). Other funding was not allocated to a specific product or R&D stage ($89m, 8.0%). The US NIH provided the vast majority of funding for discovery and pre-clinical R&D ($311m, 80% for this type of research), and more than half of the funding for clinical development and post registration studies ($253m, 56%). The sheer scale of US NIH investment in HIV/AIDS R&D defines the global funding landscape for this disease; the rest of the world actually invested more in HIV clinical trials and post registration studies ($203m, 52% of non-US NIH investment), than in basic and early stage research ($116m, 30%).
The top 12 funders in 2016 provided 97% of all funding for HIV/AIDS R&D, with the top three funders (the US NIH, the Gates Foundation and industry) providing 84% ($921m) of total investment. The US NIH alone provided just under two-thirds of all HIV/AIDS R&D funding ($710m, 64%), an increase of $31m (up 4.6%) compared to 2015, which was driven by increased funding for preventive vaccines (up $35m, 8.2%). Industry’s strong growth (up $29m, 56%) earned it a place in the top three funders for the first time. After seven years of declining HIV/AIDS investments, the Gates Foundation increased funding (up $19m, 17%), primarily for preventive vaccine development through large grants to the International AIDS Vaccines Initiative (IAVI) and Fred Hutchinson. Funding increases from the Dutch Ministry of Foreign Affairs (DGIS), reflecting the launch of its PDP III fund, placed it in the top 12 funders list (up $7.7m, from a low base). Other funding increases came from the US Department of Defense (DOD) (up $6.3m, 22%, following last year’s decrease), the Swedish Research Council (up $5.7m, from a low base, reflecting better reporting), and the EC (up $4.0m, 33%). USAID had the largest funding decrease (down $12m, -20%) reflecting the end of dapivirine Phase III trials and, as a result, it dropped out of the top three funders. The Wellcome Trust also decreased funding in 2016 (down $5.2m, -31%).
^ Subtotals for 2007–2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 4. Top HIV/AIDS R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 796 755 808 771 740 761 692 682 678 710 64
Gates Foundation 108 188 140 139 130 128 125 114 109 128 12
Aggregate industry 20 50 38 32 24 23 16 47 56 84 7.6
USAID 79 80 80 80 76 75 68 60 59 48 4.3
US DOD 33 29 40 37 49 54 57 64 29 35 3.2
EC 24 25 26 19 20 15 16 13 12 16 1.5
Wellcome Trust 5.8 8.2 8.2 9.6 14 23 19 21 17 11 1.0
Inserm 0.3 1.1 12 13 13 12 12 11 11 10 0.9
Dutch DGIS 12 8.2 6.7 3.6 5.6 3.7 7.2 5.9 1.3 8.9 0.8
Swedish Research Council 1.4 2.0 0.6 0.7 1.2 0.8 0.7 0.5 6.2 0.6
Canadian CIHR 3.2 1.8 5.1 8.1 7.6 7.3 7.7 7.8 6.2 6.2 0.6
German BMBF - 2.4 0.9 1.6 2.1 1.9 3.7 5.9 0.5
Subtotal of top 12^ 1,154 1,223 1,214 1,147 1,104 1,132 1,039 1,040 991 1,069 97
Disease total 1,225 1,316 1,285 1,216 1,171 1,207 1,110 1,081 1,031 1,102 100
2016 % of total
US$ (millio
ns)
Funder

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE28
Figure 5. HIV/AIDS R&D funding by sector 2016
Public (HICs) 79%
Public (LMICs) 0.4%
Private (MNCs) 7%
Private (SMEs) 0.6%
Philanthropic 13%
Public (multilaterals)0.4%
A decade of investment in HIV/AIDS R&D• Despite still receiving by far the most R&D funding of all the neglected diseases, HIV/AIDS is
one of only three diseases to receive less funding in 2016 than it did in 2007 (the others being kinetoplastids and rheumatic fever). Global funding for HIV/AIDS R&D has steadily declined since its peak in 2008, with just two annual increases during this time (in 2012 and 2016, both driven by the US government). Notably, funding for microbicides halved over this period (from $259m in 2008 to $125m in 2016), with the failure of several late stage candidates prior to the regulatory submission (in 2017) of IPM’s dapivirine ring.
• Nearly three-quarters ($8.6bn, 73%) of all global investment in HIV/AIDS R&D over the past decade came from the US government, a far higher proportion than in any other neglected disease. The vast majority of US government funding for HIV/AIDS came from the US NIH ($7.4bn, 86%), with the remainder largely from USAID ($704m, 8.2%) and the US DOD ($427m, 5.0%).
• The drop in funding for HIV/AIDS R&D over the last decade came entirely from the public sector, with philanthropic funding essentially steady, and industry investment increasing substantially (although still accounting for just 3.3% of all funding over the decade).
The public sector provided most HIV/AIDS R&D funding ($877m, 80%), of which $771m (88%) came from S&T agencies, and $65m (7.4%) from aid agencies. Almost all of public sector funding was from HICs ($869m, 99%), with most of this coming from the US NIH ($710m, 82%). The philanthropic sector provided $141m (13%) and industry invested $84m (7.6%), mostly from MNCs ($77m, 92% of industry funding).
YOY funding increased for all sectors. The largest increase came from public funders (up $40m, 4.9%), three-quarters of which was due to the US NIH. Industry investment increased (up $29m, 56%), continuing its rapid and sustained growth since 2013, driven entirely by increased investment from MNCs (up $30m, 62%). Following last year’s historical low, the philanthropic sector increased funding in 2016 (up $14m, 11%).
Public (multilaterals)
Philanthropic
Private (multinational pharmaceutical companies)
Public (LMIC governments)
Private (small pharmaceutical companies and biotech)
Private
Other
Public (HIC governments)

FIN
DIN
GS
- D
ISEA
SES
PAGE29
MALARIA
Malaria is a parasitic disease transmitted through the bite of an infected female Anopheles mosquito.15 The two most common types of malaria are caused by Plasmodium falciparum and Plasmodium vivax. Left untreated, malaria can cause severe illness and death. Children and pregnant women are among the most vulnerable, with 70% of all malaria deaths occurring in children under five years of age.15
According to the IHME Global Burden of Disease study, malaria was the fifth highest cause of mortality and third highest cause of morbidity of all the G-FINDER neglected diseases in 2015, causing 730,290 deaths and 56 million DALYs in developing countries.2 The WHO Global Health Estimates of mortality were lower, estimating that malaria was responsible for 439,025 deaths in developing countries in 2015.3
The most advanced malar ia vaccine candidate, RTS,S, received a positive opinion from the EMA, with large-scale pilot implementations planned in three countries in 2018.16 New vaccines are needed that have greater efficacy than RTS,S; provide protection against both P. falciparum and P. vivax; and can prevent transmission.17 The next most advanced malaria vaccine candidate, Sanaria’s PfSPZ, is currently in Phase II trials.18,19
Ten new malaria drugs have been approved since G-FINDER began in 2007,20 including two artemisinin-based combination therapy (ACT) formulations designed specifically for children.21,22
Nevertheless, new malaria drugs are needed in response to the emergence of resistance to ACTs. A number of promising drugs are in late stage development: tafenoquine, to prevent relapse of P. vivax malaria, has completed Phase III clinical trials;23 artefenomel/ferroquine (previously OZ439/FQ), which has shown potential as a single-exposure, radical cure, is in Phase llb trials;24 and KAF156, also in Phase IIb trials, is the most advanced antimalarial candidate to come from a completely novel compound class.25
Cheap, sensitive and specific rapid diagnostic tests (RDTs) exist, although heat instability can be an issue in hot climates.26
Improved, more sensitive diagnostics are needed to identify non-falciparum species; to distinguish malaria from other febrile illnesses; to detect asymptomatic cases; and to diagnose G6PD enzyme deficiency (key to safely treating P. vivax malaria).26
Diagnostics in the pipeline include Alere’s Malaria Ag P.f, which can detect asymptomatic infections and is undergoing field evaluations,27 and PATH’s point-of-care diagnostic for G6PD deficiency, currently in late development.28
Next-generation vector control products (VCPs) are urgently needed in response to emerging pyrethroid resistance. Currently, Syngenta’s Actellic CS is the only non-pyrethroid-based indoor residual spraying (IRS) formulation;29 BASF’s chlorfenapyr (a crop protection ingredient being re-purposed for IRS) and next-generation long-lasting insecticide treated bed nets (LLINs) such as BASF’s Interceptor G2 and Sumitomo’s Olyset Duo are currently in development. Vector manipulation approaches to reduce mosquito fertility are also being investigated, including a sterile insect technique and Wolbachia-infected mosquitoes.30
TOTAL SPEND ON MALARIA
R&D IN 2016
$576 MILLION
OF GLOBAL R&D FUNDING
IN SCOPE
IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
32%18%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE30
Global funding for malaria R&D in 2016 was $576m, making it the second-highest funded neglected disease once again (after having lost this position to TB in 2015). Investment by regular survey participants (YOY funders) increased by $13m (up 2.5%), with irregular survey participants reporting the remaining $24m.
More than a third of all malaria R&D funding in 2016 was for the development of new drugs ($218m, 38%), followed by basic research ($139m, 24%) and vaccine development ($116m, 20%). Vector control product R&D received $60m (10%) and malaria diagnostics $21m (3.6%).
The largest increase in funding was for vector control products (up $28m, 97%). This near-doubling, which took investment in vector control products for malaria to the highest level ever recorded in the G-FINDER survey, was entirely due to the Gates Foundation almost tripling its funding for this area (up $30m, 193%). This came as the Foundation increased its funding to the Innovative Vector Control Consortium (IVCC) for the second year in a row (up $17m, 156%), and started funding Imperial College London for the first time ($13m in 2016). After declining over the previous two years, investment in basic research increased modestly in 2016 (up $7.3m, 5.9%). Malaria diagnostics was the only other area to receive increased funding (up $3.8m, up 28%), which came from various organisations, including the US NIH (up $1.9m, 75%) and the Gates Foundation (up $1.4m, 17%, mostly towards PDPs). The increase resulted in malaria diagnostics also receiving the largest investment in this area ever recorded in the history of the G-FINDER survey, although this remains a small proportion of overall malaria R&D investment.
Funding for malaria vaccines decreased by $15m (-12%), largely driven by two funders: the Gates Foundation (down $6.5m, -35%), reflecting the progression of RTS,S; and industry (down $5.8m, -15%), whose investment in malaria vaccine discovery programmes was lower than in previous years. Funding for drug development decreased by $11m (-5.1%), after two years of successive increases, partially due to cyclical funding from the Gates Foundation to the Medicines for Malaria Venture (MMV, down $13m, -27%). Industry investment in malaria drugs was essentially steady (up $0.7m, 0.7%), following two years of rapid growth.
Figure 6. Malaria R&D funding by product type 2007-2016
US
$ (m
illio
n)
Basic research
Drugs
Vaccines (preventive)
Diagnostics
Vector control products
Unspecified
2008 2009 2010 2011 2012 2013 2014 2015 2016
4%
4%
2%
5%
6% 5%
6%
8%
3% 6% 10%
0
100
200
300
400
500
600
700
3% 3%
2007
33%
34% 17% 26% 24%
22% 29% 23% 20%
0.4%
1%
2%
2% 3%
3%
2%
24% 24% 24% 30% 28% 30% 35% 27% 23% 24%
46% 32%
30% 41%
35% 34% 30% 34% 41% 38%
19%
gUnspecified
gVector control products
gDiagnostics
gVaccines (preventive)
gDrugs
gBasic research

FIN
DIN
GS
- D
ISEA
SES
PAGE31
Just under half of all malaria R&D funding in 2016 was for basic and early stage research ($259m, 45%), with a further third going to clinical or field development and post registration studies ($184m, 32%). The remainder ($133m, 23%) was not allocated to a specific product or R&D stage.
The top 12 funders of malaria R&D in 2016 provided 92% of all funding, with the top three funders – the US NIH, the Gates Foundation and industry – collectively accounting for three-quarters ($428m, 74%) of total funding.
Six of the top 12 funders increased their investment in 2016, most notably the Gates Foundation (up $15m, 13%), predominantly for vector control products, followed by the US NIH (up $5.9m, 3.7%), the UK Medical Research Council (MRC, up $2.5m, 30%, from historically low levels in 2015) and the Indian Council of Medical Research (ICMR, up $1.2m, 15%). Inserm (up $0.8m, 16%) re-entered the top 12 funders list for the first time since 2012. The largest reductions in funding came from Unitaid (down $3.1m, -42%), which dropped out of the top 12 due to reduced funding to MMV, likely reflecting the end of studies to support WHO prequalification of rectal artesunate, and the EC (down $6.1m, -43%).
Public funders continued to provide more than half of all malaria funding in 2016 ($299m, 52%). The vast majority of public sector funding came from HICs ($280m, 94%), with $166m (59% of total HIC funding) coming from the US NIH. Non-public sector funding for malaria R&D was split almost equally between the philanthropic sector ($140m, 24%) and industry ($137m, 24%). This was a change from 2015, when industry investment in malaria R&D surpassed that of the philanthropic sector for the first time in the history of the G-FINDER survey.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016 Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding
recipients so may be incomplete
Table 5. Top malaria R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 99 123 136 156 143 177 144 153 160 166 29
Aggregate industry 83 85 96 115 93 106 76 118 142 137 24
Gates Foundation 146 204 213 102 170 135 125 146 110 125 22
US DOD 39 36 44 27 21 11 23 19 30 29 5.0
Wellcome Trust 24 23 24 29 27 27 24 22 17 14 2.4
UK DFID 3.4 3.3 3.2 20 18 5.7 25 18 17 12 2.1
UK MRC 16 17 18 19 17 16 16 14 8.2 11 1.9
Indian ICMR 10 7.0 5.0 5.1 6.7 7.5 7.0 7.8 9.0 1.6
USAID 11 9.6 9.6 10 9.1 12 6.6 5.6 9.3 8.7 1.5
EC 20 23 23 23 20 13 20 19 14 8.3 1.4
German BMBF 0.8 0.6 1.6 1.6 2.0 2.6 2.8 3.3 5.8 6.9 1.2
Inserm 0.4 0.4 3.3 4.2 4.7 5.9 5.8 3.8 4.9 5.7 1.0
Subtotal of top 12^ 467 551 593 525 542 531 487 541 528 533 92
Disease total 492 585 641 567 590 577 531 577 563 576 100
2016 % of total
US$ (millio
ns)
Funder

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE32
Public (HICs) 49%
Public (LMICs) 2%
Private (MNCs) 23%
Private (SMEs)0.9%
Philanthropic 24%
Public (multilaterals) 0.8%
Figure 7. Malaria R&D funding by sector 2016
Philanthropic sector funding increased by $12m (up 9.6%), entirely due to increased investment from the Gates Foundation. Public sector funding also increased (up $6.2m, 2.2%), driven by the US NIH across all products. Industry funding dropped its investment slightly (down $5.1m, -3.8%), primarily for vaccine R&D.
A decade of investment in malaria R&D• Annual global funding for malaria R&D peaked at $641m in 2009, but since then has been
essentially steady within the range of $550-600m per year (although dropping to $531m in 2013). Changes in annual funding have reflected the progression of the R&D pipeline, with a spike in vaccine R&D funding in 2008-2009 related to RTS,S clinical trials, and a subsequent sharp drop. Funding for malaria drug R&D had peaks in 2010 and 2015-2016, with the latter peak reflecting an increased focus on clinical development (which accounted for 40% of total drug funding in 2016, up from 23% in 2007), as product candidates advanced through clinical trials.
• Almost a quarter ($1,287m, 23%) of all malaria funding over the past decade went to PDPs – the equal highest share (with diarrhoeal diseases) of all neglected diseases. Nearly three-quarters (72%) of this PDP funding came from the Gates Foundation.
• The Gates Foundation has been a major contributor to malaria R&D, although its share of annual global funding has fallen from a peak of 35% in 2008 to 22% in 2016. The Foundation was responsible for more than two-thirds ($217m, 69%) of all funding for malaria vector control products over the past ten years, and was the main driver for the record investment in this area ($46m) in 2016. Diagnostic R&D investments were also largely shaped by funding from the Gates Foundation, which provided 43% of all funding for this area over the past decade.

FIN
DIN
GS
- D
ISEA
SES
PAGE33
TUBERCULOSIS
Tuberculosis (TB), caused by Mycobacterium tuberculosis, most commonly affects the lungs and is spread via air droplets.31 Most TB cases are latent and non-infectious, but around 5-15% will progress to active TB if left untreated. Active TB usually causes coughing, fever and weight loss, and is highly infectious.31 TB is especially dangerous for people with low immunity, and is a leading cause of death among people with HIV/AIDS.
According to the IHME Global Burden of Disease study, TB ranked as the third highest cause of mortality and the fifth highest cause of morbidity of all the G-FINDER neglected diseases in 2015, causing 1.1 million deaths and 40 million DALYs in developing countries.2 The WHO Global Health Estimates suggest an even higher mortality figure, estimating that TB was responsible for 1.4 million deaths in developing countries in 2015.3
Current TB drug regimens are complex and require up to two years of daily treatment, leading to poor compliance, drug resistance and treatment failure. New drugs are needed that act more rapidly, are effective against multidrug-resistant or extensively drug-resistant TB (MDR-TB and XDR-TB), and are safe to use in conjunction with HIV treatments. The world’s first fixed-dose combination treatments specifically designed for children, HRZ/HR, were rolled out in over 30 countries in 2016.32 Two new drugs (delamanid and bedaquiline) have been approved for treatment for MDR-TB under programmatic conditions in several countries, and both drugs were added to the WHO Essential Medicines List in 2015.33 Despite progress, routine use of these two drugs in high-burden countries remains limited.34,35 Another novel drug (pretomanid) is being tested in different combinations: TB Alliance’s BPaMZ regimen trial is in Phase III,36 and Médecins Sans Frontières (MSF) is conducting TB-PRACTECAL Phase II/III trials.37 Sutezolid, now licenced by the Medicines Patent Pool, will be trialled in combination with other TB drugs by the TB Alliance.38
The only available TB vaccine, BCG, was developed over 90 years ago. While highly effective against disseminated TB in children, a new safe and more effective vaccine is needed that prevents the progression to active TB for adults.39 Several candidates are in clinical development, mostly targeting the same antigens as the existing vaccine.40 VPM1002, specifically developed for infants in endemic areas, is currently in Phase II trials.37 A Phase llb trial of M72+AS01E in adults is underway, after Phase II trials found it to be safe for use in infants.41
There is a need for more effective and appropriate point-of-care TB tests,40 tests to diagnose TB in children, and tests for drug resistance and susceptibility.37 Cepheid’s Xpert MTB/RIF diagnostic platform was a major advance, however cost remains a barrier to access despite discounts offered to developing countries.42 Cepheid’s Xpert Ultra, a more sensitive cartridge-based assay, was endorsed by the WHO in 2017,37 and its GeneXpert Omni point-of-care molecular diagnostic system is expected to undergo field evaluation in 2018.43 The WHO recently recommended use of a number of newly-developed diagnostics, including initial tests to detect resistance to first- and second-line anti-TB drugs, and a replacement for microscopy of pulmonary TB in adults.44
TOTAL SPEND ON TUBERCULOSIS
R&D IN 2016
$568 MILLION
OF GLOBAL R&D FUNDING
IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
32%18%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE34
Global funding for TB R&D in 2016 was $568m, making it the third-highest funded neglected disease by a small margin ( just behind malaria). Of this total, $508m was from regular survey participants (YOY funders), with irregular survey participants providing the remaining $60m. YOY funding for TB R&D fell by $37m (-6.8%), completely reversing the increase in funding over the preceding three years, and reducing YOY funding to the lowest level since 2008. However this drop in YOY funding does not take into account a $26m increase in funding from Unitaid, which (as a relatively new funder of R&D) is not included in the G-FINDER group of YOY funders. If the Unitaid funding increase is included, the drop in YOY investment for TB would have been considerably smaller (down $10m, -1.9%).
Similarly to previous years, almost half of TB R&D funding in 2016 was for drugs ($262m, 46%), followed by basic research ($152m, 27%), preventive vaccines ($74m, 13%), diagnostics ($51m, 9.0%) and therapeutic vaccines ($5.8m, 1.0%).
Funding for TB drug R&D fell by $33m (-13%) in 2016, almost entirely due to a reduction in Gates Foundation funding to the TB Alliance (down $31m, -68%), associated with the start of a new project cycle; although again, if Unitaid’s investment is included the decrease would have been much smaller (down $6.8m, -2.6%). Preventive vaccine investment fell by over a quarter to $74m (down $26m, -28%), to the lowest level ever recorded by the G-FINDER survey. This was in large part due to a halving of industry investment in preventive vaccine R&D (down $11m, -51%), with two candidates approaching the end of Phase II clinical trials, as well as reduced funding from the Gates Foundation (down $8.1m, -20%) and the US NIH (down $4.8m, -31%). These two organisations did however increase their funding of other product areas: the increase in funding for diagnostics (up $12m, 36%) was driven by increased investment in this area by the Gates Foundation (up $11m, 434%); and the increase for basic research (up $11m, 8.5%) was a result of increased investment by the US NIH (up $11m, 12%). Therapeutic vaccine investment increased by $5.6m, after almost no investment in this area in 2015.
Figure 8. TB R&D funding by product type 2007-2016
33% 30% 35%
28% 27% 25% 25% 24% 24% 27%
36% 33%
33% 45%
42% 42% 43% 41%
46% 46%
19% 24%
19% 16%
19% 20% 18% 19%
17% 13%
1%
2%
1% 0.1%
0.1% 0.2% 0.2% 0.1%
0.1% 1%
9%
10%
10% 9%
10% 8% 9% 11% 7% 9%
0
100
200
300
400
500
600
700
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US
$ (m
illio
n)
Basic research
Drugs
Vaccines (preventive)
Vaccines (therapeutic)
Diagnostics
Unspecified
gUnspecified
gDiagnostics
gVaccines (therapeutic)
gVaccines (preventive)
gDrugs
gBasic research

FIN
DIN
GS
- D
ISEA
SES
PAGE35
More than half of all TB R&D funding in 2016 ($329m, 58%) was for basic and early stage research; a further $181m (32%) went towards clinical development and post registration studies, and $58m (10%) was not allocated to a specific product or R&D stage. However, the focus for each product was slightly different, with just under half of all funding for drug R&D going to clinical development ($128m, 49%), while the vast majority of R&D investment in therapeutic vaccines was for the discovery and pre-clinical stages (5.3m, 91%), reflecting the very different state of the R&D pipeline in these two areas.
The top 12 funders provided 92% of total funding for TB R&D, unchanged from 2015. The top three funders collectively contributed just under three quarters of total funding ($404m, 71%): the US NIH invested $210m (37%), the Gates Foundation $99m (17%), and industry $96m (17%).
The largest increase in funding was from Unitaid (up $26m, from a low base), attributable to a large grant to Partners In Health for the endTB project. Smaller increases came from the US NIH (up $9.6m, 4.8%), the Indian ICMR (up $3.9m, 49%) and the German Federal Ministry of Education and Research (BMBF, up $2.6m, 40%). Investment from the Gates Foundation fell significantly (down $33m, -25%), largely reflecting reduced funding to the TB Alliance related to the transition to a new project cycle. Industry investment also fell (down $8.3m, -8.9%), extending the decline in industry investment in TB R&D since 2010. The US Center for Disease Control and Prevention (CDC) dropped out of the top 12, with no reported disbursements to the TB Trials Consortium in 2016.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016 Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding
recipients so may be incomplete
Table 6. Top TB R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 143 132 192 184 178 186 172 192 200 210 37
Gates Foundation 136 155 114 120 101 106 131 137 132 99 17
Aggregate industry 71 96 136 168 162 140 116 107 104 96 17
Unitaid 6.9 0.4 2.0 0.5 6.1 33 5.7
EC 20 26 28 21 18 11 18 15 22 18 3.1
USAID 4.6 7.7 9.6 9.8 9.6 10 8.9 13 13 16 2.8
Indian ICMR 1.0 2.2 3.5 3.5 6.9 8.3 8.3 8.0 12 2.1
German BMBF 4.1 0.4 4.6 4.0 3.7 4.7 4.8 5.7 6.5 9.1 1.6
UK MRC 11 11 11 13 13 13 11 9.5 7.1 9.1 1.6
Wellcome Trust 2.2 4.8 7.3 11 11 12 12 11 9.6 8.8 1.6
UK DFID 1.5 2.9 15 19 11 1.4 13 14 12 7.6 1.3
Inserm 0.3 0.4 5.4 <0.1 3.0 3.7 5.1 2.6 3.9 5.0 0.9
Subtotal of top 12^ 429 458 552 577 529 502 508 525 530 522 92
Disease total 452 495 605 622 577 553 564 569 576 568 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE36
Public (HICs)54%
Public (multilaterals)6%
Public (LMICs)4%
Private (MNCs) 15%
Private (SMEs)2%
Philanthropic 19%
In 2016, the public sector provided around two-thirds ($362m, 64%) of total TB R&D investment, with the remainder split relatively evenly between the philanthropic ($110m, 19%) and private sectors ($96m, 17%). The vast majority of public funding was provided by HICs ($307m, 85%); however this level of HIC contribution is actually one of the lowest proportions of all the tier one and tier two diseases. Multilaterals (largely Unitaid) contributed $33m (9.2% of public funding), which is the largest share of total investment in any single neglected disease (5.8% of all TB R&D funding) that this sector has ever contributed in the history of the G-FINDER survey. Most private sector investment was provided by MNCs ($87m, 90%).
Public sector investment remained essentially flat in 2016 (up $5.1m, 1.6%). Philanthropic sector investment fell to the lowest level ever recorded by the G-FINDER survey (down $33m, -24%), due to reduced funding from the Gates Foundation. Industry investment in TB R&D also fell, in this case to the lowest level seen since the first year of the G-FINDER survey, with the drop in 2016 (down $8.3m, -8.9%) due to reduced investment in TB vaccine R&D.
Figure 9. TB R&D funding by sector 2016
A decade of investment in tuberculosis R&D
• Annual global funding for TB R&D over the last decade followed a similar pattern to malaria. It grew strongly between 2007 and 2010, to a peak of $622m, before plateauing within the range of $550-600m per year.
• Drug development accounted for 41% of all TB R&D investment over the decade, and was the only area to have strong investment growth during this time – driven first by industry investment in TB drug development (which peaked in 2011), and subsequently by the public sector, who have offset the decline in industry investment since 2011. Investment in TB basic research peaked in 2009 (driven by US government fiscal stimulus funding) before falling back to pre-existing levels and plateauing there; funding for all other product areas was essentially steady over the decade.
• 2016 marked the highest ever public investment in TB R&D, driven by that sector’s highest ever investment in TB drug development. Governments in IDCs have more than doubled their investment since 2008 (from $9.6m, to $21m in 2016), with their collective funding now comparable to that of the EC. In contrast, industry investment in 2016 was its lowest since 2007, and more than 40% lower than its 2010 peak.

FIN
DIN
GS
- D
ISEA
SES
PAGE37
DIARRHOEAL DISEASES
Diarrhoeal diseases are a group of illnesses caused by viruses, bacteria and protozoa that often spread through contaminated food or water. Without treatment, diarrhoeal diseases can cause severe illness and death. Children under the age of five and people with compromised immunity are most at risk.45 Rotavirus is the most common cause of severe diarrhoeal disease in young children globally, and causes fever, vomiting and watery diarrhoea.46 Enteroaggregative Escherichia coli, also known as EaggEC, and enterotoxigenic E. coli (ETEC) can also cause fever and diarrhoea. For some people, cholera (caused by Vibrio cholerae) causes no symptoms but for others, infection can cause severe diarrhoea and vomiting, and even kill within hours if left untreated.47 Shigellosis, caused by the Shigella bacterium, is highly contagious.48 Giardia are microscopic parasites found in soil, food and water contaminated by faeces from animals or humans.49 Cryptosporidium is a parasite encased in a hard shell that can survive in soil, food and water, and primarily affects people who work with animals or live in overcrowded settings.50
According to the IHME Global Burden of Disease study, diarrhoeal diseases were the fourth highest cause of mortality and morbidity of all the G-FINDER neglected diseases in 2015, resulting in 922,471 deaths and 50 million DALYs in developing countries.2
Current vaccines against diarrhoeal diseases are not always suitable for infants under the age of one, and some are relatively ineffective. New bi- and multi-valent vaccines that are suitable for infants and that have long durations of protection are needed for most diarrhoeal diseases. Paxvax’s Vaxchora, a cholera vaccine, received US Food and Drug Administration (FDA) approval in 2016, but has not yet been tested in endemic areas and has only been trialled in adults.51 In March 2016, a $1 rotavirus vaccine (ROTAVAC) was included in India’s national immunisation programme. Following an initial rollout in four states, the vaccine will gradually be expanded to cover all of India.52 Another rotavirus vaccine, ROTASIIL, received regulatory approval from Indian authorities in January 2017 after successfully completing Phase III trials.53 ROTASIIL has proven to be heat-stable in another Phase III trial.54 Several vaccine candidates for other diarrhoeal diseases are in Phase I and II trials. Vaccine candidates include ACE527 to address ETEC55; and WRSS1 and Sf2aWC (which entered Phase II in 2017) to address Shigella.56, 57
New safe, ef fective and af fordable drugs are needed to complement supportive interventions such as oral rehydration therapy and zinc supplementation for some diarrhoeal diseases, including for cholera, Shigella and Cryptosporidium.58 New, rapid diagnostic tests capable of distinguishing between diarrhoeal diseases are also required, however there are currently no late stage candidates in the diagnostic pipeline.59
TOTAL SPEND ON DIARRHOEAL DISEASE
R&D IN 2016
$145 MILLION
OF GLOBAL R&D FUNDING
32%5%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE38
Global funding for diarrhoeal disease R&D in 2016 was $145m. Funding from regular survey participants (YOY funders) decreased by $21m (-14%) to $134m. Irregular participants provided the remaining $12m.
Over half of all funding for diarrhoeal disease R&D went to rotavirus ($39m, 27%) and multiple diarrhoeal diseases ($35m, 24%), followed by Shigella ($24m) and cholera ($23m), which accounted for 16% each. Cryptosporidium received $13m (9.3%) and the remaining diarrhoeal diseases collectively received less than 10% of total funding. Funding was either lower or flat for most diarrhoeal diseases in 2016, with the largest reductions seen in rotavirus (down $11m, -24%), multiple diarrhoeal diseases (down $7.2m, -20%) – primarily due to an adjustment to Inserm’s reporting*, ETEC (down $6.5m, -40%) and cholera (down $2.0m, -8.4%). As a result, investment in multiple diarrhoeal diseases was the lowest ever recorded in the history of the G-FINDER survey, and investments in rotavirus and cholera reached the lowest levels seen since 2008. Shigella (up $6.1m, 35%) was the only diarrhoeal disease to receive a notable funding increase in 2016.
For diseases where all product types are in scope (cholera, Shigella and Cryptosporidium) funding profiles varied across product areas. For cholera, basic research received almost two-thirds of funding ($15m, 65%) and preventive vaccines under a third ($6.5m, 28%). For Shigella, preventive vaccines received $15m (65%) and basic research $5.7m (24%). For Cryptosporidium, funding was spread across basic research ($6.2m, 46%) and drugs ($5.7m, 43%).
RESTRICTED
RESTRICTED RESTRICTED
IN SCOPE
IN SCOPE
IN SCOPE IN SCOPE
IN SCOPE
IN SCOPE IN SCOPE IN SCOPE IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
Rotavirus
Shigella
Cholera
CryptosporidiumETECEAggEC Giardia
Multiple diarrhoeal diseases
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Table 7. Diarrhoeal disease R&D funding 2016 (US$ millions)^
^ Please note that there were strict eligibility conditions on drug and vaccine investments for some diarrhoeal disease products to avoid inclusion of overlapping commercial activity. Due to this, total funding between product categories cannot be reasonably compared
Category not included in G-FINDER
* Inserm, historically one of the top five funders of diarrhoeal disease R&D, reported more detailed data for 2016. Given the greater detail, it is apparent that a portion of Inserm’s research reported in 2016 is out of the scope of G-FINDER in this restricted category, and it is possible that Inserm’s investment in prior years is overstated. Since the majority of Inserm’s funding is non-product specific, and allocated to multiple diarrhoeal disease R&D, this adjustment affects the overall YOY changes but not product totals. The only disease-specific funding reported by Inserm has been unspecified funding for Shigella, with a $0.8m (-44%) decrease in 2016.
Rotavirus 38 0.9 39 27
Shigella 5.7 0.4 15 1.4 1.0 24 16
Cholera 15 0.5 6.5 1.1 0.1 23 16
Cryptosporidium 6.2 5.7 1.0 0.2 0.3 13 9.3
Enterotoxigenic E. coli (ETEC) 9.2 0.4 0.1 9.7 6.7
Enteroaggregative E. coli (EAggEC) 0.5 0.2 0.1 0.8 0.6
Giardia <0.1 0.1 0.1 0.1
Multiple diarrhoeal diseases 7.0 0.1 14 8.6 5.2 35 24
Total 34 6.8 85 12 7.8 145 100
Basic research
DiseaseDrugs Vaccines
(preventive)
Diagnostics
Unspec
ified
Total%

FIN
DIN
GS
- D
ISEA
SES
PAGE39
Preventive vaccine funding (down $8.5m, -9.6%) saw the largest decrease by product area reflecting decreases in funding for rotavirus (down $11m, -24%) and ETEC (down $6.5m, -42%), which offset a smaller increase in vaccine funding for Shigella (up $6.0m, 64%). Other decreases were smaller, with basic research down $5.4m (-14%) and diagnostics down $0.9m (-12%). Drug R&D was the only product area to receive more funding in 2016 (up $2.6m, 62%), driven by an increase in funding for Cryptosporidium drug development (up $2.0m, 53%).
Just over half of all diarrhoeal disease R&D funding was for basic and early stage research ($82m, 56%), with clinical development and post registration studies accounting for 30% ($44m). Funding for some of the diarrhoeal diseases had a heavier focus on basic and early stage research, particularly cholera (78%), Cryptosporidium (76%) and Shigella (65%). On the other hand, around half of funding for ETEC and rotavirus was for clinical development and post registration studies (56% and 49%, respectively). Other diarrhoeal disease funding was not allocated to a specific product or R&D stage ($20m, 14% across all diseases).
The top 12 funders in 2016 provided 97% of all funding for diarrhoeal disease R&D. The top three funders alone provided more than three-quarters of all funding, with the Gates Foundation contributing $43m (30%), the US NIH $38m (26%) and industry $30m (21%).
Only three of the top 12 funders increased their investment in diarrhoeal disease R&D in 2016, and even these increases were relatively modest in size: MSF (up $3.0m, 218%), largely due to the start of BRV-PV rotavirus vaccine trials in Niger; Brazilian Development Bank (BNDES, $2.8m), as part of an ongoing multi-year rotavirus vaccine grant to the Butantan Institute that had no reported funding in 2015; and the Gates Foundation (up $2.2m, 5.4%). The largest decrease was a result of the adjustment to Inserm’s reporting (down $9.8m, -91%) with additional smaller reductions spread across a number of funders.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 8. Top diarrhoeal disease R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Gates Foundation 52 31 55 53 36 41 52 42 41 43 30
US NIH 36 46 71 59 62 56 48 44 38 38 26
Aggregate industry 13 26 41 33 28 30 45 40 34 30 21
US DOD 6.4 6.9 13 6.9 5.6 8.6 9.6 9.5 7.2 5.8 4.0
Indian ICMR 4.5 3.8 4.8 2.9 2.7 4.7 4.6 5.2 4.9 3.3
MSF - - 1.4 4.4 3.0
Institut Pasteur 3.1 3.5 4.8 3.9 4.0 3.8 3.7 3.8 3.6 3.9 2.7
UK DFID - - 2.4 4.6 2.6 - 3.2 8.4 4.8 3.5 2.4
Brazilian BNDES 0.7 - 2.8 1.9
Wellcome Trust 0.9 0.4 0.3 0.4 0.4 3.8 2.9 4.7 3.9 2.7 1.9
Gavi 12 17 4.1 7.5 3.4 1.2 0.8
Inserm 0.3 0.3 1.3 1.6 8.0 8.3 12 11 11 1.0 0.7
Subtotal of top 12^ 127 143 199 172 161 163 194 172 156 141 97
Disease total 128 149 204 177 167 169 200 175 161 145 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE40
Just under half of all funding for diarrhoeal disease R&D in 2016 came from the public sector ($64m, 44%), with the majority of this coming from HIC governments ($56m, 88%). The philanthropic sector contributed just over a third of total funding ($51m, 35%) and industry a fifth ($30m, 21%). SMEs – primarily from innovative developing countries (IDCs) – contributed 54% of industry funding, the third highest share of industry funding among neglected diseases.
Philanthropic funding increased (up $4.0m, 8.8%), due to increases from MSF (up $3.0m, 218%) and the Gates Foundation (up $2.2m, 5.4%). Public sector funding fell by $17m (-22%), although this includes the adjustment to Inserm’s reporting (down $9.8m, -91%). The decrease in industry funding (down $8.2m, -26%) reflects reduced industry investment in rotavirus vaccine R&D (down $15m, -49%), which more than offset increased investment in Shigella vaccine R&D (up $5.1m, from a low base).
Public (HICs)39%
Public (LMICs)5%
Private (MNCs) 10%
Private (SMEs)11%
Philanthropic 35%
Figure 10. Diarrhoeal disease R&D funding by sector 2016
A decade of investment in diarrhoeal disease R&D• Funding for diarrhoeal diseases mostly fluctuated between $150m and $200m over the past
decade, with peaks in 2009 (related to US government stimulus spending on vaccines and basic research) and 2013 (driven by philanthropic and industry investment in vaccine trials).
• Rotavirus, which has the highest burden of disease of the diarrhoeal diseases included in G-FINDER, received almost half a billion dollars ($495m) in funding for R&D for developing country-specific vaccines. Half of this ($249m, 50%) came from industry, initially driven by MNCs, followed more recently by increased SME investment in early stage research. A slow decline in funding for rotavirus vaccine research since 2013 reflects the registration of new products.
• Almost a quarter ($387m, 23%) of all diarrhoeal disease funding over the past decade went to PDPs – the equal highest share (with malaria) of all neglected diseases. Unlike malaria however, this funding has steadily declined. Funding to PDPs for diarrhoeal disease R&D more than halved since 2007 (from $55m, to just $22m in 2016), with the share falling from 43% of all funding to 15%. PATH – whose portfolio includes rotavirus, ETEC and Shigella vaccines – was the largest beneficiary of this funding ($300m, 78% all of funding for PDPs over the decade).

FIN
DIN
GS
- D
ISEA
SES
PAGE41
KINETOPLASTIDS
Kinetoplastid infections include three diseases: leishmaniasis; Chagas’ disease (also known as American trypanosomiasis); and sleeping sickness (human African trypanosomiasis, HAT). Leishmaniasis, spread by sand flies, has three forms: visceral (the most severe form, which is often fatal without treatment); cutaneous (the most common); and mucocutaneous.60 Chagas’ disease is caused by Trypanosoma cruzi, and is predominantly spread by the blood-sucking triatomine bug. Chagas’ disease has two stages: symptoms in the acute stage are often mild or absent, resulting in widespread under-diagnosis. If left untreated, all infected individuals will progress to chronic Chagas’ disease, and around 20-30% will develop life-threatening complications.61 Sleeping sickness is caused by the parasite Trypanosoma brucei, and spread by tsetse flies. It also has two stages, with symptoms of early stage disease often difficult to distinguish from non-specific viral illnesses. Late stage sleeping sickness occurs when the parasite infects the brain and central nervous system, causing confusion and – without treatment – coma and death.62
According to available data from the IHME Global Burden of Disease study, kinetoplastids collectively ranked as the ninth highest cause of mortality and the eleventh highest cause of morbidity of all the G-FINDER neglected diseases in 2015, resulting in 35,160 deaths and 1.8 million DALYs in developing countries.2
The WHO Global Health Estimates provide a similar mortality figure, estimating that kinetoplastids were responsible for 33,974 deaths in developing countries in 2015.3
Leishmaniasis needs a vaccine, as well as more effective, oral drug formulations and a diagnostic that can detect early stage disease. At least one vaccine candidate in clinical development is undergoing evaluation for prophylactic and therapeutic indications.63 There are no novel leishmaniasis drugs in clinical development, although a topical formulation of an existing drug (amphotericin B) is currently in clinical trials for the treatment of cutaneous leishmaniasis.64 Diagnostics intended for use in resource-limited settings currently in development include a urine-based test, in early stage development, and a LAMP-based test for visceral and cutaneous leishmaniasis currently undergoing demonstration studies in endemic countries.65
Chagas’ disease needs preventive and therapeutic vaccines; safer, more effective drugs that are suitable for children and effective against the chronic form of the disease; and diagnostics that can reliably detect chronic disease and monitor treatment. A paediatric benznidazole formulation was registered in Brazil in 201166 and received US FDA approval in 2017.67 A combination therapy of benznidazole and fosravuconazole (a new chemical entity, previously called E1224) has entered Phase II.68 A urine-based diagnostic for the detection of congenital Chagas’ disease is in late development.69
Sleeping sickness needs safe, oral drugs that are active against both stages of the disease to replace the current nifurtimox-eflornithine combination therapy (NECT) injectable treatments70, as well as an effective vaccine. Fexinidazole, the first potential new drug for the treatment of late stage sleeping sickness in 30 years, is currently in Phase lllb clinical trials in Africa, and acoziborole (previously SCYX 7158) is in Phase II/III clinical trials.71 There are currently no vaccine candidates for sleeping sickness in the product pipeline.
TOTAL SPEND ON KINETOPLASTID
R&D IN 2016
$131 MILLION
OF GLOBAL R&D FUNDING
32%4%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE42
Global funding for kinetoplastid R&D in 2016 was $131m. Regular survey participants (YOY funders) increased funding to $110m (up $12m, 12%), with irregular participants contributing the remaining $21m.
The largest share of funding was for leishmaniasis ($41m, 31%), followed by sleeping sickness ($37m, 28%), and Chagas’ disease ($25m, 19%); remaining funding was for multiple kinetoplastid diseases ($29m, 22%). Funding was either higher or steady for all kinetoplastid diseases, with many of the changes reflecting cyclical funding to PDPs from philanthropic organisations and government agencies. Funding for sleeping sickness increased by $6.1m (up 23%), after a big drop in 2015, largely due to cyclical funding from the Gates Foundation to DNDi ($7.4m in 2016, after no funding in 2015). Funding also increased for Chagas’ disease (up $3.6m, 27%), driven by the US NIH (up $4.3m, 61%), and multiple kinetoplastid diseases (up $2.2m, 8.8%), due to increased Dutch DGIS funding to DNDi (up $3.7m, 470%) following the start of a new PDP funding round. Funding for leishmaniasis remained stable (down $0.1m, -0.3%), with increased funding from the Gates Foundation (up $2.5m, from a low base) offsetting decreases from the US NIH (down $1.3m, -9.5%) and the EC (down $1.2m, -29%).
Funding increased for all product types with the exception of diagnostics (down $0.7m, -16%), with these changes again being heavily influenced by the pattern of multi-year grant funding to PDPs. Funding for drug R&D increased by $7.8m (up 17%), with the largest increases going to sleeping sickness (up $4.8m, 54%) and leishmaniasis (up $2.1m, 25%), due to an increase in cyclical Gates Foundation funding to DNDi. Preventive vaccine funding for R&D increased (up $1.9m, 46%) due to cyclical Gates Foundation funding to the Infectious Disease Institute (IDRI). Therapeutic vaccine funding for R&D doubled, albeit from a modest amount (up $0.3m, 126%), split across Chagas’ disease (up $0.2m, from a low base) and leishmaniasis (up $0.1m, 24%). The decrease in diagnostic funding reflected cyclical funding from the Gates Foundation to FIND.
IN SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
IN SCOPE IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
LeishmaniasisSleeping sickness (HAT)
Chagas’ diseaseMultiple kinetoplastid diseases
IN SCOPE
IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Table 9. Kinetoplastid R&D funding 2016 (US$ millions)
- No reported funding Category not included in G-FINDER
Leishmaniasis 16 14 4.9 0.3 1.8 4.1 41 31
Sleeping sickness (HAT) 19 14 0.6 1.0 0.7 1.4 37 28
Chagas' disease 12 7.9 0.9 1.7 1.9 0.1 <0.1 25 19
Multiple kinetoplastid diseases 3.4 25 <0.1 - <0.1 - 0.3 29 22
Total 50 61 6.4 2.0 4.7 0.8 5.9 131 100
Basic research
DiseaseDrugs Vaccines
(preventive)Vaccines
(therapeutic)
DiagnosticsVector control
products
Unspec
ified
Total%

FIN
DIN
GS
- D
ISEA
SES
PAGE43
Around three-quarters of kinetoplastid funding went to basic and early stage research ($95m, 73%), with only $19m (15%) going to clinical development and post registration studies. Remaining funding was not allocated to a specific product or R&D stage ($17m, 13%). The focus on basic and early stage research was consistent across each of the kinetoplastid diseases (87% for Chagas’ disease, 69% for sleeping sickness and 68% for leishmaniasis), and reflects the state of the R&D pipeline, which has very few candidates in clinical development.
In 2016, the top 12 funders accounted for 87% of total kinetoplastid R&D funding, with just three funders – the US NIH, industry and the Gates Foundation – accounting for more than half ($68m, 52%) of all funding.
Most of the major funding movements among the top funders were related to cyclical funding patterns to PDPs. The Gates Foundation (up $10m, 371%, mainly owing to multi-year grants to PDPs) went from being the eighth highest funder in 2015 to the third highest funder in 2016. The Dutch DGIS (up $3.7m, from a low base) became the sixth highest funder due to the start of a new PDP funding round. The German BMBF (down $1.5m, -47%) dropped out of the top 12 in 2016 due to decreased funding to DNDi. Funding changes not related to PDPs included increased investment from the US NIH (up $4.2m, 12%), which consolidated its position as the top funder of kinetoplastid R&D, and better reporting from the French Institute for Development (IRD), which moved into the top 12 with an investment of $2.6m across the three kinetoplastid diseases.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 10. Top kinetoplastid R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 33 57 62 66 56 54 47 42 36 40 31
Aggregate industry 4.6 2.9 4.9 11 14 18 17 19 21 15 11
Gates Foundation 53 34 42 23 13 9.3 9.1 19 2.8 13 10
Wellcome Trust 13 11 10 8.1 8.9 11 9.8 13 12 12 9.2
EC 2.6 4.3 9.4 8.3 6.8 5.6 3.7 11 14 12 9.2
Dutch DGIS - - - 1.2 3.7 2.3 4.5 3.7 0.8 4.4 3.4
Brazilian FAPESP - 2.0 3.4 2.6
Indian ICMR - 0.1 2.0 3.7 3.3 4.8 4.2 2.9 3.3 2.5
UK MRC 2.4 3.0 2.1 2.4 2.0 1.4 2.1 2.9 2.3 3.1 2.4
US DOD 5.5 4.8 5.3 1.1 1.0 0.5 - - 3.3 2.8 2.1
French IRD - 2.6 2.0
Institut Pasteur - 2.7 2.9 5.4 4.6 2.8 2.4 2.5 2.1 2.5 1.9
Subtotal of top 12^ 131 136 158 143 124 128 107 128 103 114 87
Disease total 133 149 173 156 139 141 119 139 114 131 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE44
The public sector accounted for more than two-thirds of funding for kinetoplastids ($90m, 69%), with most of this funding coming from HICs ($78m, 86%). The philanthropic sector contributed a fifth of total funding ($26, 20%), with industry providing the remainder ($15m, 11%). The largest funding increase came from the philanthropic sector (up $10m, 67%), followed by the public sector (up $4.5m, 6.4%), with this latter increase coming from both HICs and LMICs. Industry funding for kinetoplastid R&D decreased in 2016 (down $2.8m, -21%).
Public (HICs)59%
Philanthropic20%
Private (MNCs) 10%
Private (SMEs)1%
Public (LMICs)10%
Figure 11. Kinetoplastid R&D funding by sector 2016
A decade of investment in kinetoplastid R&D• Aside from a brief peak from 2008 to 2010, annual global funding for kinetoplastid R&D was
essentially steady over the last decade, at around $120m-$140m per year. Leishmaniasis was the best funded of the three diseases (receiving 37% of all kinetoplastid R&D funding over the decade), followed by sleeping sickness (29%) and then Chagas’ disease (16%), with the remaining 18% not allocated to a single disease.
• The level of funding going to each of the kinetoplastid diseases has converged over the course of the decade: funding for leishmaniasis peaked in 2009 (driving the increase in overall kinetoplastid R&D funding) but has subsequently fallen, while funding for Chagas’ disease has grown, and funding for sleeping sickness has been relatively steady.
• PDPs have been heavily involved in R&D for kinetoplastid diseases, receiving 22% of funding over the past decade. This is the third highest share of any neglected disease, marginally behind malaria and diarrhoeal diseases (both 23%). Like diarrhoeal diseases however, the proportion of all funding for kinetoplastid R&D going to PDPs fell sharply over the decade, from a high of 37% in 2007 to just 16% in 2016.

FIN
DIN
GS
- D
ISEA
SES
PAGE45
DENGUE
Dengue, also known as breakbone fever, is a viral infection transmitted to humans by the female Aedes mosquito – most often Aedes aegypti (common in urban environments) and Aedes albopictus (common in rural environments). The dengue virus has four serotypes, each with multiple subtypes. First time infection rarely results in anything more serious than a severe flu-like illness; subsequent infections with a different serotype (or even subtype) can result in severe disease, and are more likely to lead to dengue haemorrhagic fever.72 For children in affected regions, dengue is a leading cause of serious illness and death. Dengue outbreaks often occur in Asia, Central and South America, and the disease is now present in more than 100 countries, up from nine countries fifty years ago.73
According to the IHME Global Burden of Disease study, dengue was the tenth highest cause of both mortality and morbidity of all the G-FINDER neglected diseases in 2015, resulting in 18,298 deaths and 1.9 million DALYs in developing countries.2 The WHO Global Health Estimates report an even higher mortality figure, estimating that dengue was responsible for 34,462 deaths in developing countries in 2015.3
Dengue’s prevalence in several high- and upper-middle-income countries across Asia and Latin America, coupled with demand from travellers and the military, has created a potential commercial market for a dengue vaccine large enough to attract industry investment in vaccine R&D. For this reason, dengue vaccine R&D investment has been excluded from the scope of G-FINDER. The first dengue vaccine – Dengvaxia (CYDTDV) – was registered in December 2015 for use in individuals 9-45 years of age living in endemic areas.
No curative treatment is available for dengue; management is therefore focused on supportive therapy and the control of onward transmission. Despite the need, there is little advanced activity in dengue drug research. Pipeline candidates include celgosivir (an α-glucosidase inhibitor), currently in Phase I trials,74
and DENV mAb, in pre-clinical development.75
There is a pressing need for diagnostics that can detect dengue across the complete spectrum of disease, and distinguish dengue from other causes of fever.76 The first reverse transcription polymerase chain reaction (RT-PCR) diagnostic test able to detect the presence of all four dengue virus types was approved by the US FDA in 2012 (CDC DENV-1-4), however independent evaluations showed that this product has a lower clinical sensitivity than initially thought.77 Additionally, real-time RT-PCR tests are less suitable than loop-mediated isothermal amplification (LAMP) -based tests for use in low-resource settings.78 Several research groups are developing real-time LAMP-based tests, such the DENV RT-LAMP assay currently in development by the US Naval Medical Research Center.78 A number of point-of-care serological tests (based on antigen and/or antibody detection) are available, however these tests cannot distinguish between serotypes, and may lack sensitivity and specificity. A point-of-care test is needed that can diagnose all four serotypes as well as primary and secondary dengue infection.
TOTAL SPEND ON DENGUE
R&D IN 2016
$113 MILLION
OF GLOBAL R&D FUNDING
OUT OF SCOPE
IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
32%4%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE46
Global funding for dengue R&D in 2016 was $113m. Regular survey participants (YOY funders) increased their investment by $8.4m (up 8.7%) to $106m, with irregular participants providing the remaining $7.1m. This was the third successive year of increasing funding for dengue R&D, at an average of 13% per year; the funding increase in 2016 was primarily driven by the US NIH.
Most dengue R&D funding in 2016 was for basic research ($50m, 44%), followed by drugs ($28m, 25%) and vector control products ($20m, 17%), while diagnostics received less than 10% of total funding ($9.4m, 8.3%). The largest increases were in basic research (up $4.8m, 12%) and drugs (up $4.5m, 19%); funding for diagnostics (up $3.6m, 77%) increased to the highest level ever reported for this area. There was an overall drop in funding for vector control products (down $3.7m, -16%) but this masked opposing changes at the sub-product level. In 2016 funding for vector control products was concentrated in biological control products ($19m, 97%) with pesticides receiving less than $1.0m ($0.6m, 2.8%). This represented a substantial funding drop for pesticide R&D compared to 2015 (down $11m, -95%), reflecting a reduction in the Gates Foundation’s funding to IVCC for dengue pesticide R&D (coinciding with a marked increase in its funding to IVCC for malaria pesticide R&D). Investment in biological control products increased (up $7.0m, 58%), due to new funding from the Gates Foundation ($12m) to Monash University’s World Mosquito Program, formerly known as Eliminate Dengue.
Three-quarters of all funding for dengue R&D in 2016 was for basic and early stage research ($83m, 74%), with only $3.0m (2.7%) going to clinical or field development. A relatively large amount of funding was not allocated to a specific product or R&D stage ($27m, 24%), although it must be noted that some of this includes funding for biological control products which is currently not allocated to a specific R&D stage category in the G-FINDER survey. Funding for drug development focused on discovery and pre-clinical research ($26m, 91%), reflecting the early stage of the pipeline.
Figure 12. Dengue R&D funding by product type 2007-2016
0
20
40
60
80
100
120
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US
$ (m
illio
n)
66% 63%
62% 61% 53%
46% 45% 45% 43% 44%
17% 17%
22%
21%
37% 34%
27% 23%
23%
25%
3% 11%
6%
9%
6%
5%
4% 6%
5%
8%
1% 4%
5%
7%
4% 12%
22%
24%
24%
17%
Basic research
Drugs
Diagnostics
Vector control products
Unspecified gUnspecified
gVector control products
gDiagnostics
gDrugs
gBasic research

FIN
DIN
GS
- D
ISEA
SES
PAGE47
The top 12 funders in 2016 accounted for almost all (97%) of total dengue R&D funding. The increase in dengue R&D funding in 2016 can essentially be attributed to the US NIH (up $11m, 24%), which also contributed exactly half (50%) of all R&D funding for dengue. Half of the top 12 funders decreased funding, most notably the Gates Foundation (down $2.5m, -14%), Inserm (down $2.1m, -67%) and the US CDC, which dropped out of the top 12 after reporting no funding for dengue in 2016. Two key LMICs public funders reported increased dengue R&D investment – the Brazilian Support Fund for Research in the State of Minas Gerais (FAPEMIG) and the Indian ICMR increased investment by $2.7m and $1.5m (from a low base) respectively.
As in previous years, two-thirds of dengue funding came from the public sector ($75m, 66%). Most public sector funding was from HICs ($67m, 90%), and more than three-quarters of HIC funding came from the US NIH ($57m, 85%). The philanthropic sector accounted for just under a fifth ($21m, 18%), and industry for 15% ($17m). Overall public sector funding increased by $9.8m (up 16%), primarily reflecting the US NIH funding increase. Industry investment in dengue R&D also increased slightly (up $1.3m, 9.3%), driven by increased MNC investment (up $1.0m, 7.6%). Philanthropic sector funding fell by $2.7m (-11%).
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 11. Top dengue R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 30 25 45 42 49 44 36 41 46 57 50
Aggregate industry 7.4 3.7 5.3 7.4 11 8.6 7.5 7.8 15 17 15
Gates Foundation 1.2 2.1 1.7 1.2 0.1 5.4 17 19 18 15 14
Wellcome Trust 0.9 1.0 1.4 2.0 6.0 4.7 3.4 6.0 5.5 5.4 4.8
Indian ICMR 0.6 1.0 1.4 1.4 1.2 1.8 1.6 1.8 3.3 3.0
Brazilian FAPEMIG 1.5 <0.1 2.8 2.5
EC 1.8 1.6 1.0 0.5 0.4 1.8 2.5 2.3 2.4 2.4 2.1
Institut Pasteur 3.6 2.2 2.0 3.0 2.3 1.8 1.9 1.8 1.9 1.7 1.5
UK MRC 0.2 0.3 0.2 0.1 0.7 0.4 0.5 0.7 1.6 1.5 1.4
US DOD 1.3 2.6 5.0 0.4 1.1 0.4 0.2 0.2 1.0 1.5 1.4
Inserm - - - - - - - - 3.2 1.1 1.0
Australian NHMRC 0.7 1.1 1.1 1.3 1.9 2.8 1.6 2.9 0.6 0.7 0.6
Subtotal of top 12^ 51 50 73 65 77 77 74 85 97 110 97
Disease total 51 53 80 69 79 80 76 86 101 113 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE48
Public (HICs)60%
Philanthropic18%
Private (MNCs) 13%
Private (SMEs)2%
Public (LMICs)7%
Figure 13. Dengue R&D funding by sector 2016
A decade of investment in dengue R&D• Global funding for dengue R&D has more than doubled over the last decade (from $51m in
2007 to $113m in 2016). All product categories benefited from this increase, as did basic research, although the most striking growth was in vector control products, which increased from $0.8m in 2007 to $20m in 2016.
• The increase in dengue R&D funding between 2007 and 2016 came primarily from the public sector (largely the US NIH) and the philanthropic sector (almost entirely from the Gates Foundation), but was also supported by smaller but steady growth in industry investment.
• Just over half (51%) of all dengue R&D funding over the past 10 years was for basic research, with the US NIH providing nearly three-quarters (71%) of this amount. Meanwhile, the Gates Foundation was responsible for nearly two-thirds (62%) of all R&D investment in dengue vector control products over the last decade.

FIN
DIN
GS
- D
ISEA
SES
PAGE49
Pneumonia is an infection of the lungs that is transmitted when infected individuals cough or sneeze. Symptoms include coughing, fever, chest pain and shortness of breath, and the illness can be deadly, especially for young children and elderly patients.79 Although pneumonia can be caused by a range of bacteria and viruses, pneumococcal pneumonia caused by the bacterium Streptococcus pneumoniae is by far the most common in developing countries.
Bacterial meningitis is an infection of the fluid that surrounds the brain and spinal cord, most commonly caused by S. pneumoniae or Neisseria meningitidis. Symptoms of bacterial meningitis can include severe headaches, fever, chills, a stiff neck, nausea and vomiting, sensitivity to light, and an altered mental state.80 Bacterial meningitis is also often transmitted from person to person through coughing or sneezing. Even with early diagnosis and treatment, 5-10% of infected individuals die within 24-48 hours of showing symptoms.80
According to the IHME Global Burden of Disease study, bacterial pneumonia & meningitis was the leading cause of both mortality and morbidity of all the G-FINDER neglected diseases in 2015, resulting in 1.6 million deaths and 75 million DALYs in developing countries.2
Pneumococcal conjugate vaccines (PCVs) are highly effective and widely used in high-income countries, but until recently did not offer protection against the most prevalent serotypes in developing countries. The WHO prequalified PCV10 and PCV13 vaccines, which offer broader protection, have been rolled out in a number of developing countries with positive results.81,82
However PCVs are expensive to make and do not cover all of the 90 plus pneumococcal strains.81,82 New vaccines are needed that are more affordable, while still providing specific protection for children against serotypes predominant in developing countries, or across all serotypes. Pneumococcal protein vaccines are one potential approach to achieve this, as they offer broad protection while being less expensive to manufacture; several protein vaccine candidates are currently in Phase II clinical trials.82
Historically, most epidemic and endemic bacterial meningitis in the meningitis belt of sub-Saharan Africa has been caused by serogroup A meningococci. MenAfriVac, a 50c per dose monovalent conjugate meningitis A vaccine developed by the Meningitis Vaccine Project, has been rolled out in mass vaccination campaigns across the meningitis belt of Africa since 2010, with much success. An infant version of MenAfriVac was prequalified by the WHO in early 2015. But as rates of meningitis A have fallen, other serogroups have become increasingly prominent. Two multivalent meningococcal conjugate vaccines (developed for high-income country needs) are currently available, but are too expensive for widespread use in developing countries, ranging between $12 and $40 per dose.83 There is an ongoing need for cheaper polyvalent conjugate vaccines, with one candidate in Phase II trials.84
BACTERIAL PNEUMONIA & MENINGITIS
TOTAL SPEND ON BACTERIAL PNEUMONIA
& MENINGITISR&D IN 2016
$91.5 MILLION
OF GLOBAL R&D FUNDING
32%3%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE50
Global funding for bacterial pneumonia & meningitis R&D was $92m in 2016. Regular sur vey par t ic ipants ( YOY funders) were responsible for $78m of this total, with irregular participants providing the remaining $14m. YOY funding fell slightly (down $3.1m, -3.8%), however there are two caveats to this number: the G-FINDER scope was expanded in 2016 to include developing country-focused basic research, which received $6.9m from YOY funders; and Inserm’s investment was adjusted, resulting in a $10m decrease#. Excluding these two changes, YOY funding actually remained stable (up <$0.1m, <0.1%).
S. pneumoniae received the majority of funding ($66m, 72%), despite reduced investment in this area in 2016 (down $9.1m, -14%) related to cyclical funding from the Gates Foundation to PATH. N. meningitidis received $25m (27%); this was an increase of $17m (up 371%), due to larger reported industry investment in meningitis vaccine R&D. Just $0.9m (0.9% of total funding) was not allocated to a specific pathogen; this was a decrease of $11m (-93%) compared to 2015, mostly due to the adjustment to Inserm’s reporting.
As in previous years, vaccine R&D received the majority of funding with $81m (89%); the newly-included basic research category received $9.3m (10%), and diagnostics just $0.9m (0.9%).
RESTRICTED
OUT OF SCOPE
OUT OF SCOPE
RESTRICTED
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
RESTRICTED
S. pneumoniaeN. meningitidis
Both S. pneumoniae and N. meningitidis
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
# Inserm, the third highest funder in 2015, reported more detailed data for 2016, resulting in a proportion of its reported 2016 investment being considered outside the scope of G-FINDER; it is therefore possible that Inserm’s investment in prior years is overstated. Since the majority of Inserm’s historical funding is not pathogen- or product-specific, this adjustment affects overall YOY changes but not pathogen or product totals.
Figure 14. Bacterial pneumonia & meningitis R&D funding by product type 2007-2016
Unspecified
Diagnostics
Vaccines (preventive)
Basic research
US
$ (m
illio
n)
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
10%
83%
68% 87%
85% 81% 83%
80% 80%
83%
89%
7%
20%
6%
4% 5% 5%
2%
2%
3%
1%
0
20
40
60
80
100
120
gUnspecified
gDiagnostics
gVaccines (preventive)
gBasic research

FIN
DIN
GS
- D
ISEA
SES
PAGE51
Funding for vaccine R&D was relatively stable (up $3.1m, 4.6%), but this hid major changes in pathogen-specific funding. Almost two-thirds of all funding for bacterial pneumonia & meningitis in 2016 went to pneumococcal vaccines ($49m, 63%), however this represented a significant decrease from 2015 (down $14m, -22%), due to cyclical Gates Foundation funding to PATH. Conversely, vaccine funding for meningitis increased more than five times (up $17m, 464%), as a result of the increased industry investment noted earlier. Funding for diagnostics decreased (down $1.8m, -67%).
Funding for bacterial pneumonia & meningitis R&D in 2016 was heavily focused on clinical development and post registration studies ($73m, 80%), followed by basic and early stage research ($15m, 16%). However, this split is influenced by scope restrictions on basic and early stage research in the G-FINDER survey. The remaining investment was not allocated to a specific product or R&D stage ($3.9m, 4.3%).
Funding for bacterial pneumonia & meningitis R&D remained highly concentrated in 2016, with the top two funders – industry and the Gates Foundation – providing the vast majority ($74m, 80%) of total funding. This was even higher than the 75% share these two funders accounted for in 2015, and came despite sharply diverging funding in 2016: aggregate industry remained the top funder, and increased its investment by $16m (up 52%) after a sharp decrease the previous year. In contrast, Gates Foundation funding was down $15m (-45%) due to cyclical funding to PATH. Other notable changes include the UK DFID moving into the top 12, following the disbursement of $2.9m to PATH (after not having reported any funding for bacterial pneumonia & meningitis in 2015), and the downward adjustment to Inserm’s reporting.
Table 12. Top bacterial pneumonia & meningitis R&D funders 2016
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Aggregate industry 14 54 36 32 38 41 49 49 36 55 60
Gates Foundation 6.6 31 25 46 39 44 15 5.5 34 19 20
Gavi 2.5 5.5 11 6.4 4.7 5.1
US NIH 4.9 4.7 4.3 10 16 8.8 6.5 2.2 1.3 3.4 3.7
UK DFID - - - - - 0.1 0.8 1.8 - 2.9 3.2
German DFG - 0.5 0.6 - 0.4 2.5 2.6 1.6 2.2 2.4
UK MRC 1.5 1.7 1.8 0.9 0.6 0.3 0.6 0.5 0.8 1.7 1.9
Wellcome Trust 0.2 0.2 0.1 0.2 0.7 3.2 1.8 1.9 1.1 0.9 1.0
Institut Pasteur 0.4 0.2 0.3 0.3 0.7 0.5 0.3 0.3 0.4 0.6 0.7
French ANR 0.3 - - - - 1.0 - 0.8 0.4 0.4
South African DST - - - - - - - - - 0.3 0.3
Indian ICMR - - - - - - - - 0.2 0.2
Subtotal of top 12^ 33 99 74 99 106 109 101 75 93 91 99
Disease total 33 100 75 102 106 110 102 75 93 92 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE52
Philanthropic 27%
Private (SMEs)38%
Public (HICs) 13%
Private (MNCs)22%
Bacterial pneumonia & meningitis had the highest proportion of industry involvement and the lowest proportion of public sector funding for any G-FINDER neglected disease in 2016. Industry was responsible for nearly two-thirds of all funding ($55m, 60%) in 2016. Notably, SMEs invested more than MNCs, accounting for $35m (38%) of all funding for bacterial pneumonia & meningitis R&D; this was also the highest proportion of any of the neglected diseases, and primarily came from Indian firms. The philanthropic sector contributed $25m (27%), and public sector funders just $12m (13%). The increase in industry investment (up $16m, 52%) came from both SMEs† (up $10m, 43%) and MNCs (up $8.1m, 69%). Public sector funding decreased by $4.5m (-32%), due to reduced investment from HICs. Philanthropic funding fell by $15m (-43%), entirely reflecting the cyclical reduction in funding from the Gates Foundation.
† SME increases or decreases refer to organisations that had funding data included in both 2015 and 2016, rather than in every year of the survey, as SME survey participation is inconsistent from year to year
A decade of investment in bacterial pneumonia & meningitis R&D• Since 2008, annual global funding for bacterial pneumonia & meningitis R&D has been
relatively steady (albeit within quite a wide range) at between $75m and $110m per year, with peak investment recorded in 2012.
• Industry investment accounted for nearly half (45%) of all global funding for bacterial pneumonia & meningitis R&D over the past decade. Philanthropic funders (primarily the Gates Foundation) provided a further 35%, and the public sector just 20%.
• SME investment in vaccines, particularly for S. pneumoniae, has grown strongly in the past four years (from $5.5m in 2012 to $35m in 2016), with much of this investment coming from firms in IDCs. SME investment has exceeded MNC investment for each of the last two years.
Public (LMICs) 0.5%
Figure 15. Bacterial pneumonia & meningitis R&D funding by sector 2016

FIN
DIN
GS
- D
ISEA
SES
PAGE53
SALMONELLA INFECTIONS
Salmonella infections are a group of diseases caused by the Salmonella enterica bacteria, and transmitted through contaminated food or drink. These include typhoid (Salmonella Typhi) and paratyphoid fever (Salmonella Paratyphi A, B or C), collectively referred to as enteric fever (which affect humans); and thousands of serotypes that are non-typhoidal, referred to as non-typhoidal Salmonella (NTS), which affect both humans and animals.85
Salmonella infections are more common where there is dirty water and poor sanitation or hygiene. Symptoms can include fever, malaise, headache, constipation or diarrhoea, and an enlarged spleen and liver. Occasionally rose-coloured spots appear on the chest.86 In the case of typhoid fever, a small percentage of people can recover but still carry and spread the bacteria for as long as a year after infection. Diagnosis of Salmonella infections may require a blood, stool or bone marrow sample.
According to the IHME Global Burden of Disease study, Salmonella infections were the eighth highest cause of mortality and the sixth highest cause of morbidity of all the G-FINDER neglected diseases in 2015, resulting in 265,947 deaths and 18 million DALYs in developing countries.2
Medicines exist to treat enteric fever, however data from endemic regions show antimicrobial resistance is increasing, rendering treatment ineffective.87 Therefore, there is a need for more efficacious drugs including those suitable for children. There are currently two safe and effective vaccines to prevent typhoid, however more suitable vaccines are required that are appropriate for HIV coinfection or children under the age of two.88,89 Paratyphoid fever is increasingly causing most enteric fever in Asia, however despite this there are no vaccines that specifically target paratyphoid fever;90 nor any bivalent vaccines that target both typhoid and paratyphoid fever.91
There are some bivalent vaccines in development: the most advanced product is O:2-TT + Vi-TT, however this candidate has not progressed in the past five years. For typhoid, there are several vaccines in the pipeline. The most advanced is a conjugate typhoid vaccine (Typbar TCV) that was licensed in India in 2013 based on immunogenicity data. In October 2017, following a Typbar TCV Phase IIb clinical trial using a controlled human infection model,92,93 the WHO’s Strategic Advisory Group of Experts (SAGE) on Immunization recommended the introduction of typhoid conjugate vaccines for infants and children over six months of age as a single dose in typhoid endemic countries.94
For NTS, antibiotics are only recommended for high-risk indiv iduals such as young chi ldren, elder ly people and immunocompromised patients. There is currently no NTS vaccine available. There are several NTS vaccine candidates in development, although they are all are currently in the pre-clinical stage or earlier.95
TOTAL SPEND ON SALMONELLA R&D IN 2016
$91.5 MILLION
OF GLOBAL R&D FUNDING
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
32%3%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE54
Global funding for Salmonella infections R&D in 2016 was $91m, which was the highest reported level of investment since the start of the G-FINDER survey. After three years of stable funding, investment by regular survey participants (YOY funders) increased considerably in 2016 (up $21m, 32%) to a total of $86m. Irregular survey participants reported the remaining $5.9m.
More than three-quarters of all Salmonella R&D funding in 2016 was for typhoid and paratyphoid fever ($71m, 78%), with only $4.7m (5.1%) going to NTS. Most of the overall YOY funding increase was for typhoid and paratyphoid fever (up $16m, 29%) although funding for NTS also increased (up $0.3m, 12%) after investment in this area halved in 2015.
Basic research received half ($45m, 50%) of all Salmonella R&D funding in 2016, with vaccine development receiving most of the remainder ($37m, 40%). Almost all of the vaccine funding was for typhoid and paratyphoid fever ($35m, 94% of vaccine funding), with comparatively little investment in NTS vaccine R&D ($0.4m, 1.1% of vaccine funding). As in previous years, only a small proportion of total funding was for diagnostics ($4.2m, 4.6%) and drugs ($3.8m, 4.1%).
YOY funding for Salmonella R&D increased across the board, with the largest increase for vaccine development (up $11m, 40%), mainly due to additional SME investment (up $9.5m, 89%). Funding for basic research increased by $7.1m (up 22%), driven by increased investment in basic research by the US NIH (up $6.8m, 32%), which was also the driving force behind the smaller increases in funding for drugs (up $1.3m, 51%) and diagnostics (up $0.7m, 21%).
Almost two-thirds of all Salmonella R&D funding in 2016 was for basic and early stage research ($58m, 63%), with a further third going to clinical development and post registration studies ($29m, 31%). A relatively small amount of funding was not allocated to a specific product or R&D stage ($5.3m, 5.8%). However, the R&D focus for each product was slightly different, with more than two-thirds of funding for vaccine R&D going to clinical development ($25m, 68%), reflecting the progression of conjugate typhoid vaccine candidates through the pipeline. Conversely, investment in Salmonella drug R&D was predominantly focused on the discovery and pre-clinical stages ($3.3m, 87%), and was entirely funded by the US NIH.
The top 12 funders accounted for almost all ($89m, 98%) of total funding for Salmonella R&D in 2016, with 82% of total investment ($75m) provided by only three funders – the US NIH, industry and the Gates Foundation. Industry investment ($24m, 26%) was the highest recorded since the start of the G-FINDER survey, reflecting the clinical development of conjugate typhoid vaccine candidates. After small funding decreases in 2015, both industry (up $10m, 71%) and the US NIH (up $9.7m, 33%) increased their investment in Salmonella R&D considerably in 2016. Relatively small increases in investment by Inserm (up $1.1m, having not funded Salmonella before) and the Swiss National Science Foundation (SNSF, up $0.2m, 36%) meant they entered the top 12 funders. The Chilean National Fund for Scientific and Technological Development (FONDECYT, down $0.1m, -0.2%) and Swedish Research Council (down $0.3m, -78%) dropped out of the top 12. Funding from the Gates Foundation was essentially steady (up $0.3m, 2.2%).
Table 13. Salmonella R&D funding 2016 (US$ millions)
Typhoid and paratyphoid fever (S. Typhi, S. Paratyphi A) 31 3.0 35 2.8 71 78
Non-typhoidal S. enterica (NTS) 3.0 0.5 0.4 0.8 4.7 5.1
Multiple Salmonella infections 11 0.3 1.9 0.6 15 17
Total 45 3.8 37 4.2 91 100
Basic research
DiseaseDrugs Vaccines
(preventive)
Diagnostics
Total%

FIN
DIN
GS
- D
ISEA
SES
PAGE55
As in previous years, public funders accounted for just over half ($52m, 57%) of all Salmonella R&D funding in 2016; most of this came from HICs ($51m, 99%), largely from the US NIH ($39m, 76% of HIC funding). Industry invested a further quarter ($24m, 26%) of total funding, with this mainly coming from SMEs ($20m, 84% of industry funding) rather than MNCs ($3.8m, 16%). The philanthropic sector provided the remaining $15m (17% of all funding for Salmonella R&D in 2016).
The public sector saw the highest YOY increase in Salmonella funding (up $12m, 33%), which was driven by the US NIH. After a halt in industry funding growth in 2015, investment increased once again in 2016 (up $10m, 71%) to a historically high level. As in previous years, this increase was driven by additional investment by Indian SMEs (up $9.5m, 89%). Philanthropic sector funding fell slightly in 2016 (down $0.7m, -4.2%), following an increase the previous year.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 14. Top Salmonella R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 9.5 24 30 32 26 35 32 31 29 39 42
Aggregate industry - 14 3.9 3.3 5.0 4.5 10 16 14 24 26
Gates Foundation - - 1.9 3.8 4.5 5.4 9.8 7.0 13 13 14
Wellcome Trust - 0.9 1.8 2.5 4.3 5.0 4.6 3.7 3.3 2.9 3.2
SFI 0.4 0.4 - 2.1 2.1 2.3
UK MRC 0.8 1.1 0.8 0.6 1.5 1.2 1.3 1.8 2.2 2.0 2.2
Institut Pasteur - 1.3 1.5 1.4 2.2 1.4 1.6 1.9 1.7 1.9 2.0
German DFG - 0.5 1.2 1.2 0.9 1.2 1.8 0.4 1.8 1.9
Inserm - - - - - - - - - 1.1 1.2
French ANR 0.5 - - - - 1.6 - 0.6 1.0 1.1
Australian NHMRC - 0.5 0.5 0.5 0.1 0.3 0.5 0.7 0.3 0.7 0.8
Swiss SNSF - 0.7 0.7 - 0.8 0.5 0.6 0.7
Subtotal of top 12^ 10 44 44 48 47 57 65 65 68 89 98
Disease total 10 45 44 49 48 58 66 66 69 91 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE56
A decade of investment in Salmonella R&D• Global funding for Salmonella R&D has increased markedly over the past decade. From just
$10m in 2007, and $45m in 2008 when the category was expanded to also include non-typhoidal Salmonella enterica, total investment reached a record high of $91m in 2016. All of this growth was driven by investment in typhoid/paratyphoid fever R&D, which saw a seven-fold increase over the decade, with funding for NTS R&D actually falling (from $16m in 2008 to just $4.7m in 2016).
• The number of organisations investing in Salmonella R&D also increased over the course of the decade, from just three in 2007 to 30 in 2016.
• While public funders have always provided the backbone for Salmonella R&D funding, and were the main driver of increased funding over the decade, funding from the philanthropic sector steadily increased over the decade, and SME investment has grown rapidly in the last 2-3 years.
Public (LMICs) 0.7%
Philanthropic 17%
Private (SMEs)22%
Public (HICs) 56%Private (MNCs)
4%
Figure 16. Salmonella R&D funding by sector 2016

FIN
DIN
GS
- D
ISEA
SES
PAGE57
Helminths are parasitic worms and flukes that can cause disease in humans. The most common mode of transmission to humans is through ingesting or coming into contact with contaminated food, water, or soil. Helminth infections transmitted in this manner include ancylostomiasis and necatoriasis (hookworm), ascariasis (roundworm), trichuriasis (whipworm) and strongyloidiasis (intestinal roundworms) – collectively referred to as soil-transmitted helminths – as well as taeniasis/cysticercosis (tapeworm) and schistosomiasis (bilharziasis, also known as snail fever). Other helminth infections are transmitted by bites of blood-sucking arthropods: these include lymphatic filariasis, which is transmitted by mosquitoes, and river blindness (onchocerciasis), which is transmitted by the black fly.
Adult worms can live in the intestines and other organs, causing malnutrition and impaired mental development (hookworms), or progressive damage to the bladder, ureter and kidneys (schistosomiasis). Onchocerciasis is a major cause of blindness in many African and some Latin American countries, while lymphatic filariasis can cause painful, disfiguring swelling of the scrotum (hydrocele) and limbs (elephantiasis).
According to the IHME Global Burden of Disease study, helminth infections were the eleventh highest cause of mortality and the ninth highest cause of morbidity of all the G-FINDER neglected diseases in 2015, resulting in 7,443 deaths and 9.5 million DALYs in developing countries.2
There are currently no l icensed vaccines for any of the helminth infections. Instead, treatment and prevention relies predominantly on annual or twice-yearly large-scale mass drug administration programmes.96 The variable efficacy of available drugs and the need to control transmission means that these treatment programmes must continue for many years, increasing the risk of emerging drug resistance.97 New and more effective drugs are needed for many helminth infections, as are paediatric formulations of some existing drugs. Current diagnostic products for detection of some helminths are outdated or complex; new and effective diagnostics that can measure infection intensity and detect drug resistance are needed.97
There are several schistosomiasis vaccines in development, the most advanced is Bilhvax in Phase III.98 Two vaccine candidates against human hookworm infection are in Phase l, and two vaccines against onchocerciasis are in pre-clinical development.99,100 Three drug candidates for helminth infections have completed or are in Phase III clinical trials: moxidectin for onchocerciasis, Co-Arinate FDC for schistosomiasis and oxantel pamoate for whipworm.101,102 An orodispersible praziquantel tablet for schistosomiasis for children from three months to six years old is in Phase II trials.103 There are several diagnostic tests in development for helminth infections, including the Ov16/Wb123 biplex rapid test, a dual detection point-of-care test for onchocerciasis and lymphatic filariasis currently in field evaluation;104 and the UCP-LF CAA assay to diagnose schistosomiasis in low-prevalence settings is in clinical development.105
TOTAL SPEND ON HELMINTH
R&D IN 2016
$74.6 MILLION
OF GLOBAL R&D FUNDING
HELMINTH INFECTIONS (WORMS AND FLUKES)
32%2%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE58
Total funding for helminth infections R&D in 2016 was $75m. Investment by regular survey participants (YOY funders) fell (down $3.9m, -5.5%) for the third year in a row, to $67m. Irregular participants contributed the remaining $7.4m.
A little under two-thirds (60%) of all funding for helminth infection R&D in 2016 was invested in just three diseases: schistosomiasis ($18m, 25%), lymphatic filariasis ($16m, 21%) and onchocerciasis ($10m, 14%), which collectively received $44m. All other helminth infections received less than $4.0m each. The overall YOY decrease for helminths was driven by a drop in funding for onchocerciasis (down $3.4, -28%), which was partly due to reduced diagnostics investment from the Gates Foundation to PATH (down $2.1m, -82%) following the conclusion of evaluation studies for the Ov-16 rapid diagnostic test. Funding for hookworm (down $2.0m, -34%) and schistosomiasis (down $1.3m, -7.2%) also declined. Relatively small funding increases were seen for lymphatic filariasis (up $1.7m, 14%), due to increased investment in basic research by the US NIH and US DOD, tapeworm (up $0.9m, 33%) and whipworm (up $0.5m, 33%).
IN SCOPE
IN SCOPE IN SCOPE IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE OUT OF SCOPE IN SCOPE
IN SCOPE IN SCOPE
IN SCOPE OUT OF SCOPE OUT OF SCOPE OUT OF SCOPE IN SCOPE
IN SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
Schistosomiasis (bilharziasis)Onchocerciasis (river blindness)Multiple helminth infections
Lymphatic filariasis (elephantiasis)
Hookworm (ancylostomiasis & necatoriasis)
Tapeworm (taeniasis/cysticercosis)
Whipworm (trichuriasis)Roundworm (ascariasis)
Strongyloidiasis & other intestinal roundworms
IN SCOPE
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE OUT OF SCOPE OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE OUT OF SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Table 15. Helminth R&D funding 2016 (US$ millions)
- No reported funding Category not included in G-FINDER
Schistosomiasis (bilharziasis) 10 2.9 2.2 1.4 0.1 1.6 18 25
Lymphatic filariasis (elephantiasis) 6.6 7.3 0.1 <0.1 1.8 16 21
Onchocerciasis (river blindness) 1.3 7.4 0.4 0.6 <0.1 0.5 10 14
Hookworm (ancylostomiasis & nectoriasis) 0.3 0.8 2.7 <0.1 3.9 5.2
Tapeworm (taeniasis/cysticercosis) 1.8 1.9 - - 3.6 4.8
Whipworm (trichuriasis) 0.9 0.9 - 1.8 2.4
Strongyloidiasis & other intestinal roundworms 0.7 0.5 <0.1 0.2 - 1.4 1.9
Roundworm (ascariasis) 0.8 0.4 - 1.3 1.7
Multiple helminth infections 7.0 8.8 2.3 - - <0.1 18 24
Total 29 31 7.7 2.5 0.1 3.8 75 100
Basic research
DiseaseDrugs Vaccines
(preventive)
DiagnosticsVector control
productsUns
pecified
Total%

FIN
DIN
GS
- D
ISEA
SES
PAGE59
Investment for helminth R&D was concentrated on drug development ($31m, 41%) and basic research ($29m, 40%), although it should be noted that these are the only two product areas that are included for all helminth infections. All other product areas received 10% of funding or less: preventive vaccines ($7.7m, 10%), diagnostics ($2.5m, 3.3%) and vector control products ($0.1m, 0.1%). Drug R&D (up $0.9m, 3.4%) was the only product area to receive increased funding in 2016, with investment declining in all other product areas. Funding for diagnostics saw the largest YOY drop (down $3.8m, -61%) partly due to the conclusion of evaluation studies for the Ov-16 rapid diagnostic test for onchocerciasis noted earlier. Vaccine investment also declined (down $1.0m, -15%).
More than two-thirds of all R&D funding for helminth infections in 2016 was focused on basic and early stage research ($51m, 69%), while a quarter was for clinical or field development and post registration studies ($19m, 25%). Remaining funding ($4.6m, 6.2%) was not allocated to a specific product or R&D stage. Funding for some helminth infections was more heavily focused on basic and early stage research, particularly schistosomiasis (82%), and tapeworm (77%), while 81% of hookworm funding was for clinical development.
The top 12 funders provided 97% of all funding for helminth R&D in 2016. The top three funders – the US NIH, Gates Foundation and industry – were responsible for over three-quarters ($58m, 77%) of total funding, which was the highest share ever recorded by the G-FINDER survey. Two-thirds of the top 12 funders reduced their investment in 2016, with the largest decreases coming from industry (down $4.1m, -42%) and the EC (down $1.3m, -27%). The Dutch DGIS also fell out of the top 12, with no reported helminths R&D funding in 2016. The top funder of helminth R&D, the US NIH, was responsible for the largest increase in funding (up $2.7m, 9.3%).
Table 16. Top helminth R&D funders 2016
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 33 27 33 35 28 38 30 30 29 31 42
Gates Foundation 8.5 25 19 17 22 20 22 24 18 18 24
Aggregate industry 0.8 5.6 10 6.9 8.0 4.2 8.5 15 12 8.5 11
Wellcome Trust 2.7 3.4 4.4 4.8 7.3 5.6 6.7 4.4 3.6 3.5 4.7
EC 3.9 2.9 2.7 7.3 6.2 7.1 6.8 6.5 4.7 3.4 4.6
Texas Children's Hospital 0.1 0.9 1.3 1.2 1.5 1.5 2.1
German DFG - 6.3 0.5 0.6 2.5 2.8 - 2.0 1.4 1.8
Indian ICMR 0.4 0.4 1.1 1.2 1.4 1.6 1.4 1.3 1.1 1.5
UK MRC 0.9 1.2 1.0 1.0 3.0 2.0 1.8 2.5 1.3 1.1 1.5
Inserm 0.3 0.5 1.9 <0.1 1.8 1.9 2.2 1.5 1.2 1.0 1.3
Australian NHMRC 1.2 1.8 2.0 2.5 1.3 1.1 0.7 0.8 0.4 0.8 1.1
Swiss SNSF 0.3 0.3 0.1 0.5 0.5 0.3 0.3 0.2 0.7 1.0
Subtotal of top 12^ 56 71 83 78 82 87 88 90 76 72 97
Disease total 57 75 87 81 87 92 93 93 78 75 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE60
Nearly two-thirds of all funding for helminth R&D in 2016 came from the public sector ($45m, 60%), with the remainder provided by the philanthropic sector ($21m, 28%) and industry ($8.5m, 11%). The vast majority of public funding came from HICs ($43m, 96%). Industry funding was almost entirely provided by MNCs ($8.5m, 99%), with SMEs investing less than $0.1m in 2016.
Industry funding fell significantly in 2016 (down $4.1m, -42%), due to reduced MNC investment in helminth drug R&D, while public (up $1.1m, 2.8%) and philanthropic (down $0.9m, -4.2%) funding remained relatively steady.
Note: The G-FINDER survey does not include loans but would like to acknowledge a particular project which has taken an innovative approach to financing neglected disease R&D. Medicines Development for Global Health (MDGH), an Australian not for profit company, is seeking to register moxidectin, an existing veterinary drug, for the treatment of onchocerciasis. An approval from the FDA could make it eligible for a priority review voucher (PRV). On the basis of the potential sale of the PRV, MDGH has secured a $10m loan from the Global Health Investment Fund for the registration process.
A decade of investment in helminth infections• Annual global funding for helminth R&D grew steadily over most of the last decade, from $57m
in 2007 to a peak of $93m in 2014, but has fallen off slightly since then.
• The US NIH and the Gates Foundation have been the two largest funders of helminth R&D, collectively contributing more than half of total global funding every year, and nearly two-thirds (62%) of all funding over the decade.
• Most of the growth in helminth R&D funding over the decade has been for drug development, which has steadily increased from negligible levels in 2007 to become the highest funded product area in 2016.
Public (LMICs) 2%
Philanthropic 28%
Private (SMEs)0.1%
Public (HICs) 58%
Private (MNCs)11%
Figure 17. Helminth R&D funding by sector 2016

FIN
DIN
GS
- D
ISEA
SES
PAGE61
HEPATITIS C
Hepatitis C is an infectious disease caused by the blood-borne hepatitis C virus (HCV), primarily affecting the liver. HCV causes both acute and chronic infection, with symptoms in the acute phase including fever, fatigue and jaundice.106 However, up to 80% of acute cases are asymptomatic, meaning that many HCV infections will go undetected until chronic disease develops, sometimes decades later. Although 20-40% of acute infections resolve spontaneously without treatment, the remaining 60-80% of people will progress to chronic infection.106 Without treatment, chronic hepatitis C is a lifelong disease which can lead to serious liver damage (cirrhosis and fibrosis) and hepatocellular carcinoma (liver cancer), both of which can be life threatening.106
There are six main genotypes of HCV. Although hepatitis C is a globally-prevalent disease, three genotypes (genotypes 4, 5 and 6) disproportionately affect developing countries, while having a low prevalence in high income countries. As a result, these genotypes are neglected from an R&D perspective. Developing country-specific R&D investment for hepatitis C genotype 4 was included in G-FINDER in 2014, and genotypes 5 and 6 were added in 2015. Genotype 4 is most prevalent in Central Africa and the Middle East, genotype 5 in Southern Africa, and genotype 6 in South-East Asia.107
Reliable genotype-specific estimates of morbidity and mortality do not exist. According to the IHME Global Burden of Disease study, hepatitis C (all genotypes) was the sixth highest cause of mortality and the eighth highest cause of morbidity of the thirteen G FINDER neglected disease categories covered by IHME, resulting in 345,600 deaths and 9.6 million DALYs in developing countries in 2015.2 The WHO Global Health Estimates present a slightly lower mortality figure, estimating that hepatitis C was responsible for 284,946 deaths in developing countries in 2015.3
A number of new direct-acting antiviral (DAA) drugs have been approved since 2013. DAA-based regimens are more effective, require a shorter duration of treatment, and have fewer side effects than previous interferon- and ribavirin-based treatments. While appropriate for most patients (including those with HIV co-infection) and covering multiple genotypes, DAA-based regimens are expensive, and access remains limited in developing countries despite discounted pricing. More research is also needed to support the use of DAA-based regimens in developing country populations. There are several multi- or pan-genotypic DAA-based regimens in late stage development, including uprifosbuvir/ruzasvir/grazoprevir; odalasvir/AL-335/SIM; and sofosbuvir/ravidasvir.108
There is also a need for hepatitis C diagnostic tests that are affordable, simple to use in developing country contexts,109 and can differentiate between genotypes. WHO has prequalified six hepatitis C diagnostic tests, including five RDTs and one viral load test, however none of the prequalified RDTs is able to differentiate between genotypes.110
There is no vaccine for hepatitis C, although there are some pan-genotypic candidates in early stage development, such as the Burnet Institute’s Delta3 candidate.111
TOTAL SPEND ON HEPATITIS CR&D IN 2016
$22.4MILLION
OF GLOBAL R&D FUNDING
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
RESTRICTED
OUT OF SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
32%1%

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE62
In order to exclude commercially-driven R&D investment ta rget ing HIC markets, G-FINDER on ly t racks investment in R&D for hepatitis C that is specifically focused on the genotypes that disproportionately affect developing countries (genotypes 4, 5, 6); or developing country-specific R&D investment in multi- or pan-genotypic technologies.
Global funding for developing countr y-speci f ic hepatitis C R&D in 2016 was $22m. Almost all of this was reported by regular survey participants (YOY funders), with only $0.7m coming from irregular survey participants. YOY funding dropped significantly for the second year in a row (down $12m, -36%), to the lowest level since hepatitis C was included in the G-FINDER survey in 2013.
More than half of all hepatitis C R&D funding in 2016 was for drug development ($12m, 53%), followed by diagnostics ($7.0m, 31%) and vaccine development ($3.5m, 16%). Funding for hepatitis C drug R&D fell markedly for the second year in a row (down $15m, -56%), entirely due to reduced industry investment (down $15m, -68%) as several late stage clinical trials reached completion. Funding for diagnostics increased (up $2.7m, 67%), on the back of the first reported SME investment in hepatitis C diagnostic development ($3.5m). Funding for vaccine development increased modestly (up $0.3m, 12%).
A little under half ($9.4m, 42%) of all funding for hepatitis C R&D in 2016 was for clinical development and post registration studies, with a further $6.3m (28%) for early stage research. Remaining funding ($6.6m, 30%) was not allocated to a specific product or R&D stage. However, the focus within each product area was slightly different, reflecting the state of the respective R&D pipelines as well the G-FINDER scope. Almost one-fifth ($2.3m, 19%) of investment in drug development was for Phase IV research – the highest proportion of any neglected disease – reflecting the advanced pipeline and the fact that most early stage drug R&D investments are not developing country-specific, and therefore outside the G-FINDER scope. In contrast, investment in vaccine R&D was overwhelmingly focused on the discovery and pre-clinical stages ($2.9m, 82%) reflecting the much less advanced pipeline, and the fact that developing country-specific vaccine R&D investment is largely limited to public sector science and technology agencies or research institutes.
Despite halving its investment, industry remained the top funder of hepatitis C R&D in 2016, accounting for just under half ($10m, 46%) of total funding. Remaining funding came primarily from the French National Agency for Research on AIDS and Viral Hepatitis (ANRS, $4.5m, 20%), the US NIH ($4.2m, 19%) and the EC ($2.1m, 9.3%). The drop in industry investment (down $11m, -52%) was by far the largest funding decrease, with the next largest coming from the EC (down $0.7m, -26%). The largest increase in hepatitis C funding in 2016 came from the French ANRS (up $0.4m, 11%), after a significant drop the previous year.
gUnspecified
gDiagnostics
gVaccines (preventive)
gDrugs
2013 2014 2015 2016
US
$ (m
illio
n)
Drugs
Vaccines (preventive)
Diagnostics
Unspecified
87% 87%
79%
53%
9% 6%
8%
16%
2% 7%
12%
31%
0
5
10
15
20
25
30
35
40
45
50
Figure 18. Hepatitis C (genotypes 4, 5 & 6) R&D funding by product type 2013-2016

FIN
DIN
GS
- D
ISEA
SES
PAGE63
The publ ic sector provided more than half ($12m, 54%) of all funding for hepatitis C R&D in 2016, with industr y responsible for almost all of the remainder ($10m, 46%); this was the first time since hepatitis C was included in G-FINDER that the public sector invested more than industry. However, this was not due to an increase in public sector funding – which in fact dropped slightly (down $0.9m, -7.7%) – but rather the substantia l decrease in industry funding. This industry drop came entirely from MNCs (down $15m, -68%), with SMEs reporting investment in hepatitis C (totalling $3.5m) for the first time.
Public (LMICs) 2%
Philanthropic 0.1%
Private (MNCs)30%
Public (HICs) 52%
Investment in hepatitis C (genotypes 4, 5 & 6) R&D since 2013• Global funding for hepatitis C R&D has more than halved, from $47m in 2013 to $22m in 2016,
with the decline in funding accelerating in the last two years.
• For most of the past four years, hepatitis C funding was dominated by industry, only to be overtaken by public funding in 2016. Philanthropic funding, on the other hand, was essentially absent.
• Industry, and to a lesser extent the public sector, have decreased their investment in hepatitis C drug R&D over the past four years. As drugs have been the main focus of hepatitis C investment, this decline drove the overall drop in funding. Funding for diagnostics steadily increased over the past decade, but reached a high of only $7.0m in 2016.
Private (SMEs)16%
Figure 19. Hepatitis C (genotypes 4, 5 & 6) R&D funding by sector 2016
Table 17 . Top hepatitis C (genotypes 4, 5 & 6) R&D funders 2016
^ Subtotals for 2013-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016
- No reported funding Funding organisation did not participate in the survey for this year. Any
contributions listed are based on data reported by funding recipients so may be incomplete
2013 2014 2015 2016
Aggregate industry 28 26 21 10 46
French ANRS 1.8 8.6 4.1 4.5 20
US NIH 11 6.6 4.7 4.2 19
EC 0.6 2.8 2.8 2.1 9.3
UK MRC 0.4 0.4 0.4 0.4 1.7
Brazilian FINEP - 0.2 0.2 1.0
Burnet Institute 0.1 0.1 0.2 1.0
Austrade 0.1 0.7
Australian ACH2 <0.1 0.2 0.1 0.6
Thai GPO 0.1 <0.1 0.2 0.1 0.5
Indian DBT 1.1 <0.1 0.4 0.1 0.5
Wellcome Trust 0.1 0.1 <0.1 <0.1 <0.1
Subtotal of top 12^ 47 45 34 22 100
Disease total 47 45 34 22 100
Funder US$ (millio
ns)
2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE64
LEPROSY
Leprosy, also known as Hansen’s disease, is caused by Mycobacterium leprae and is transmitted via air droplets from the nose or mouth of infected people. Leprosy mainly affects the skin and nerves and has an incubation period that can be as long as 20 years.112 The disease is curable with multidrug therapy using a combination of rifampicin, clofazimine and dapsone (for multibacillary leprosy), or rifampicin and dapsone (for paucibacillary leprosy).112 However, if left untreated, leprosy can cause nerve damage, muscle weakness and permanent impairments.
According to the IHME Global Burden of Disease study, leprosy was the thirteenth highest cause of morbidity of all the G-FINDER neglected diseases, resulting in 30,797 DALYs in developing countries in 2015.2 IHME estimates do not attribute any mortality to leprosy, but according to the WHO Global Health Estimates, leprosy was responsible for 15,893 deaths in developing countries in 2015.3
Diagnosis of leprosy is primarily based on identifying key clinical features of infection, meaning that asymptomatic early-stage cases are often missed or diagnosed late, leading to continued disease transmission. Elimination of leprosy will likely need new and improved diagnostics capable of identifying asymptomatic cases, as well as al l symptomatic forms (paucibacillary, borderline tuberculoid, borderline, borderline lepromatous or multibacillary) of the disease.113 The current drug regimen for leprosy has been standard treatment for 30 years and, although highly effective, it requires 6-24 months of treatment.114 Further research is needed to improve and simplify drug regimens, and to provide products for nerve function management.114, 115
Bedaquiline, an antibiotic approved for the treatment of MDR-TB, has been found to be effective in the treatment of leprosy in animal models,116 and may hold some promise. The Infectious Disease Research Institute (IDRI) is currently developing rapid diagnostic tests for leprosy.113, 117
TOTAL SPEND ON LEPROSY
R&D IN 2016
$11.1 MILLION
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Global funding for leprosy R&D in 2016 was $11m, meaning that funding levels were essentially unchanged from the preceding year. A little under two-thirds of this funding ($6.6m, 59%) was for basic research, with just $0.6m (5.2%) for product development, reflecting the paucity of the R&D pipeline for leprosy. Diagnostics ($0.4m, 3.5%) received marginally more than drugs ($0.2m, 1.7%). The remaining third ($3.9m, 35%) of all R&D funding for leprosy was for unspecified R&D.
Table 18. Leprosy R&D funding by product type 2007-2016
- No reported funding
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Basic research 4.7 6.1 7.0 5.0 7.3 10 12 7.0 5.5 6.6 59
Diagnostics 0.7 0.6 1.5 1.4 1.3 1.5 0.8 0.2 0.8 0.4 3.5
Drugs <0.1 0.8 0.9 1.1 0.3 0.8 0.2 <0.1 0.3 0.2 1.7
Unspecified 0.7 3.4 2.5 2.8 - 2.8 0.1 3.5 4.4 3.9 35
Total 6.2 11 12 10 8.9 15 13 11 11 11 100
US$ (millio
ns)
Product 2016 % of total

FIN
DIN
GS
- D
ISEA
SES
PAGE65
A decade of investment in leprosy R&D• Although the total quantum of investment remains small, more organisations have provided
funding for leprosy R&D over the past decade than for any other ‘least funded disease’, with a particularly high representation of charitable organisations.
• Since 2007, LMIC government funding for leprosy, as a proportion of public funding, has been far higher than for any other neglected disease. This can largely be credited to India (which has high leprosy prevalence), and Brazil.
Table 19. Top leprosy R&D funders 2016
## The Leprosy Research Initiative (LRI) was established in 2014 and pools funding of its member organisations, including the Netherlands Leprosy Relief (NLR), American Leprosy Missions (ALM), the German Leprosy and Tuberculosis Relief Association (GLRA) and effect:hope (The Leprosy Mission Canada) who may have individually appeared in this report as a top leprosy funder in the past. This does therefore not imply that these individual organisations have decreased their leprosy funding, rather that they are now funding some projects through the LRI ($0.5m in 2016).
Almost two-thirds of leprosy funding went to basic and early stage research ($6.9m, 62%), with a small amount going to clinical development and post registration studies ($0.2m, 1.6%). More than a third of funding was not allocated to a specific product or R&D stage ($4.0m, 36%), however the vast majority of this was core funding given to the Indian National JALMA Institute for Leprosy and Other Mycobacterial Diseases, which typically conducts basic and early stage research, meaning that this type of research actually likely accounted for as much as 95% of all leprosy R&D funding.
As in previous years, the public sector made up the vast majority ($9.4m, 85%) of leprosy R&D funding, all of which came from just two public funders (the US NIH and the Indian ICMR). The philanthropic sector provided $1.3m (12%),## and the remaining $0.4m (3.3%) came from industry (all from MNCs).
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 2.3 3.7 6.0 3.8 4.5 11 6.0 5.7 4.3 4.8 44
Indian ICMR 3.3 2.0 3.0 2.4 0.8 3.5 3.5 4.5 3.8 35
LRI 0.5 0.5 4.5
TLMI 0.3 0.4 0.4 0.7 0.6 0.5 0.5 4.3
Aggregate industry - - - 0.1 0.1 - 0.1 0.1 0.7 0.4 3.3
French ANR - 0.5 - - - - - - 0.2 2.1
UK MRC - - - - - - - <0.1 0.1 0.2 1.5
DAHW <0.1 0.1 0.1 0.1 0.1 0.1 <0.1 0.1 1.0
effect:hope 0.1 1.0
CLTRF - - - - - 0.1 0.9
Institut Pasteur 0.1 0.2 0.2 0.2 0.1 0.2 0.1 0.1 0.1 0.1 0.9
Swiss SNSF - - - - - - 0.1 0.8
Subtotal of top 12^ 6.2 11 12 10 8.9 15 13 11 11 11 99
Disease total 6.2 11 12 10 8.9 15 13 11 11 11 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE66
CRYPTOCOCCAL MENINGITIS
Cryptococcal meningitis is an opportunistic infection that causes inflammation of the tissue covering the brain and spinal cord. It is caused primarily by Cryptococcus neoformans, a microscopic and easily inhaled fungus found in the environment throughout the world. In healthy individuals, inhalation of the fungal spores rarely leads to serious illness; but for people with weakened immune systems, such as those with HIV/AIDS, cryptococcal infection (cryptococcosis) can be both serious and deadly. Cryptococcosis can affect multiple organs, but the primary site of infection is usually the lungs. Cryptococcal meningitis occurs when the infection spreads to the brain and central nervous system, with symptoms including headaches, fever, neck pain, light sensitivity and altered mental state (ranging from confusion to coma).118 Mortality rates for cryptococcal meningitis can be as high as 70%.119
An estimated 181,100 deaths each year are attributed to HIV-associated cryptococcal meningitis infections, predominantly in sub-Saharan African countries that have a high burden of HIV/AIDS.120 Global mortality estimates have dropped since 2009, when cryptococcal meningitis caused an estimated 624,700 deaths annually.121 The reduction in deaths was primarily in high income countries, through access to antiretroviral therapy, advances in rapid point-of-care diagnosis122 and pre-emptive antifungal therapy for people with HIV/AIDS.120
Cryptococcal meningitis can be ef fectively treated with medicines such as amphotericin B (AmB) and flucytosine, but these are poorly suited to developing country use. AmB is both expensive and requires administration at a hospital, and flucytosine requires careful blood monitoring. As a result, in developing countries cryptococcal meningitis is usually treated with fluconazole, which is only partially effective.123 Affordable, efficacious drugs, adapted for resource poor settings, are needed. A new long-acting azole-like compound (VT-1129) is currently in Phase I and received orphan drug status from the US FDA in 2014.124 Several oral formulations of AmB are in early stage development.125
Accurate rapid diagnostic tests for cryptococcal infection are available and appropriate for use in developing country settings; therefore diagnostics are excluded from the G-FINDER scope.
TOTAL SPEND ON CRYPTOCOCCAL
MENINGITIS R&D IN 2016
$5.6 MILLION
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs

FIN
DIN
GS
- D
ISEA
SES
PAGE67
Global investment in cryptococcal meningitis R&D in 2016 was $5.6m.
Drug R&D is the only product for cryptococcal meningitis included in the G-FINDER scope. More than two-thirds of all investment ($3.9m, 68%) was for discovery and pre-clinical R&D, with a further $1.1m (19%) for clinical development, and $0.7m (12%) not allocated to a specific R&D stage.
Just five organisations were the source of all reported global investment in cryptococcal meningitis R&D in 2016. Two public HIC organisations, the US NIH and the UK MRC, provided almost all ($5.4m, 96%) of this funding. The French ANRS, another public organisation, reported funding for the first time ($0.2m, 2.8%) making it the only new funder for cryptococcal meningitis R&D since 2013. The remaining investment came from two philanthropic funders: the Wellcome Trust ($0.1m, 1.4%) and the Mérieux Foundation (<$0.1m, 0.2%).
Public HIC organisations accounted for essentially all (98%) cryptococcal meningitis R&D investment in 2016.
Investment in cryptococcal meningitis R&D since 2013• Since G-FINDER began tracking cryptococcal meningitis R&D in 2013, funding has been
essentially stable, with a total of $5.6m contributed each year for the past three years.
• Almost all (98%) of the reported investment in cryptococcal meningitis R&D since its inclusion in G-FINDER has come from the public sector, with philanthropic organisations providing the remainder. There has been no reported investment by industry.
Table 20. Cryptococcal meningitis R&D funders 2016
- No reported funding
2013 2014 2015 2016
US NIH 1.4 4.2 3.5 4.3 76
UK MRC 1.3 1.2 2.0 1.1 20
French ANRS - - - 0.2 2.8
Wellcome Trust 0.3 <0.1 0.1 0.1 1.4
Mérieux Foundation <0.1 <0.1 <0.1 <0.1 <0.1
Australian NHMRC 0.1 0.1 - - -
Disease total 3.1 5.6 5.6 5.6 100
Funder US$ (millio
ns)
2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE68
BURULI ULCER
Buruli ulcer, also known as Bairnsdale ulcer, is a chronic disease caused by Mycobacterium ulcerans. In developing countries, children under the age of 15 are at greatest risk. While the exact transmission mode is unknown, living around marshy areas with stagnant or slow-moving water can be a risk factor in endemic regions. Buruli ulcer usually appears as a painless lump or nodule that can later develop into an ulcer, usually on the arms or legs. M. ulcerans produces a toxin known as mycolactone, which causes tissue damage and can depress the immune response.126 As a result, co-infection with HIV can make Buruli ulcer more complex to address.126 If left undiagnosed or untreated, M. ulcerans can lead to skin, tissue or bone damage, with amputation or surgery sometimes required.
Buruli ulcer occurs in more than 30 countries, predominantly in sub-Saharan Africa. In 2015, 11 developing countries reported 1,924 new cases to the WHO.127
Treatment options including antibiotics and surgery are effective if the disease is diagnosed early, however current diagnostics are both costly and complex.128 Combination antibiotics (oral and injectable) are effective but cumbersome, as they must be given daily for eight weeks. Treatment failure and resistance are emerging issues, highlighting the need for new drugs that are less complicated to administer or can be given for a shorter period. There are few new drug candidates in development for Buruli ulcer.
The BCG vaccine (designed for TB) provides short-term protection, but this is insuf f icient. Burul i ulcer vaccine development is in the very early stages of research.129
FIND is developing several Burul i u lcer diagnostics in collaboration with the WHO and other partners. These include an instrument-free point-of-care test, and tools that can be used at peripheral health centers.130
TOTAL SPEND ON BURULI ULCER
R&D IN 2016
$2.8 MILLION
Global investment in Buruli ulcer R&D in 2016 was $2.8m. The bulk of this funding was relatively evenly split between drug R&D ($1.2m, 43%) and basic research ($1.0m, 38%), while diagnostics received $0.5m (18%). No funding has been reported for vaccine R&D since 2013.
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
IN SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Table 21. Buruli ulcer R&D funding by product type 2007-2016
- No reported funding
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Drugs - 0.2 0.3 0.7 0.7 0.7 0.8 0.2 0.2 1.2 43
Basic research 1.0 1.4 1.0 1.3 0.9 1.7 3.4 1.5 0.9 1.0 38
Diagnostics <0.1 0.1 0.3 0.7 0.3 1.0 0.7 1.2 0.4 0.5 18
Vaccines (preventive) - <0.1 0.2 2.0 1.9 1.9 0.8 - - - -
Unspecified 1.4 0.2 0.1 0.7 2.0 0.8 0.7 0.8 0.4 0.1 1.8
Total 2.4 1.9 1.9 5.5 5.7 6.0 6.4 3.7 1.9 2.8 100
US$ (millio
ns)
Product 2016 % of total

FIN
DIN
GS
- D
ISEA
SES
PAGE69
The vast majority of all R&D funding for Buruli ulcer in 2016 was for basic and early stage research ($2.4m, 85%), with no reported investment in clinical development. Remaining funding was not allocated to a specific product or R&D stage ($0.4m, 15%).
All reported funding for Buruli ulcer R&D globally in 2016 came from just 11 organisations, although this was an increase from the nine organisations who provided funding in 2015. The US NIH ($1.1m, 38% of total funding) invested in Buruli ulcer R&D for the first time since 2013, and was both the largest funder and the only organisation with an investment over $1.0m. Funding from two new funders was captured for the first time; the Flemish Department of Economics, Science and Innovation (EWI) and Inserm, who contributed $0.2m and $0.1m respectively.
The majority of funding for Buruli ulcer R&D was provided by the public sector ($2.2m, 80%), with the philanthropic sector providing the remainder ($0.6m, 20%).
A decade of investment in Buruli ulcer R&D• Annual global investment in Buruli ulcer has more than halved since its peak in 2013, when
there were a number of relatively large concurrent projects, including funding from the UBS Optimus Foundation for the Stop Buruli project and funding for basic research from the German Research Foundation (DFG).
• In 2007 there were only six funders for Buruli ulcer. The base has expanded to 11 in 2016, but the field of funders remains highly concentrated. UBS Optimus Foundation has been the most consistent funder of Buruli ulcer R&D since 2008, having invested $9.5m over the past ten years. The majority of this ($7.8m, 81%) was invested in the Stop Buruli consortium.
Table 22. Buruli ulcer R&D funders 2016
- No reported funding Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding
recipients so may be incomplete
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 0.8 0.5 0.9 1.2 1.3 1.1 1.0 - - 1.1 38
Institut Pasteur 0.6 0.3 0.3 0.4 0.2 0.4 0.3 0.4 0.4 0.5 18
UBS Optimus Foundation 0.1 0.1 1.0 1.8 2.0 1.5 2.2 0.4 0.4 15
Flemish EWI 0.2 8.5
French ANR - - - - 0.1 - - 0.3 0.2 8.4
Medicor Foundation 0.4 0.1 0.2 0.2 0.2 0.4 0.1 4.4
UK MRC - - - - - - 0.1 0.1 0.1 0.1 3.7
Inserm - - - - - - - - - 0.1 1.8
Australian NHMRC 0.2 0.1 0.1 0.1 0.1 0.1 - 0.1 0.1 <0.1 1.5
DAHW - - <0.1 <0.1 - - <0.1 0.6
Wellcome Trust - <0.1 <0.1 <0.1 0.3 0.3 0.3 0.2 <0.1 <0.1 0.1
Volkswagen-Stiftung 0.1 <0.1 <0.1 <0.1 0.1
Disease total 2.4 1.9 1.9 5.5 5.7 6.0 6.4 3.7 1.9 2.8 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE70
LEPTOSPIROSIS
Leptospirosis is an infection caused by bacteria of the genus Leptospira, affecting both humans and animals. The infection is transmitted to humans through contact with the urine or blood of infected animals, either directly or via contaminated water, food or soil. People who live in tropical climates, who work in flooded areas such as rice paddies and sugar cane plantations, or who work with animals are most at risk.131 The bacteria can survive for several weeks in water or soil, and outbreaks often occur after flooding.
Diagnosis of leptospirosis can be challenging due to the non-specific symptoms of early infection, which are shared with a number of other diseases, as well as the fact that some infected individuals may remain asymptomatic. Without treatment, the infection can progress to a more severe second phase, causing meningitis, kidney and liver failure, respiratory distress, and sometimes death.
Available estimates suggest that leptospirosis is responsible for an estimated 58,900 deaths and 2.9 mil l ion DALYs globally each year, the majority of which occur in developing countries.132 Although not directly comparable to the IHME Global Burden of Disease data (because of major differences in methodology), these estimates would rank leptospirosis as the tenth highest cause of both mortality and morbidity of all the G-FINDER neglected diseases in 2015, ahead of kinetoplastids and dengue, respectively.
Effective, appropriate drugs exist for leptospirosis, and therefore infection can be successfully treated if it is diagnosed. However accurate diagnosis of leptospirosis during the acute phase of the disease is currently only possible with sophisticated laboratory tests, which are unsuitable for remote settings. New, easy to use tests are needed that can quickly and accurately diagnose acute infection in the field. A rapid point-of-care test using chromatographic immunoassay technology is currently in development, demonstrating a sensitivity of 85% and specificity of 90% in early studies.133
TOTAL SPEND ON LEPTOSPIROSIS
R&D IN 2016
$2.3 MILLION
Global funding for leptospirosis R&D in 2016 was $2.3m. This was nearly double the amount invested in this disease in 2015, and the most it has ever received since it was included in the G-FINDER survey. Diagnostics are the only product area for leptospirosis included within the scope of G-FINDER.
No reported funding for leptospirosis R&D in 2016 was allocated to a specific R&D stage.
The largest funder of leptospirosis R&D in 2016 was the Indian ICMR, who reported leptospirosis R&D investment for the first time, and provided nearly half of all funding ($1.1m, 48%). The remainder was provided by two French organisations: Institut Pasteur ($1.0m, 45%); and Inserm ($0.2m, 6.9%), who also reported funding leptospirosis R&D for the first time. The US NIH, which usually provides funding for leptospirosis R&D, did not report any investment in 2016.
All funding was provided by the public sector in 2016, with HICs ($1.2m, 52%) only providing marginally more than LMICs ($1.1m, 48%).
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
RESTRICTED
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs

FIN
DIN
GS
- D
ISEA
SES
PAGE71
Investment in leptospirosis R&D since 2013• R&D investment for leptospirosis has only been tracked by G-FINDER since 2013; during this
time, global funding has grown from $0.4m to $2.3m per year.
• R&D for leptospirosis has almost exclusively been funded by the public sector, with only one small grant contributed by the philanthropic sector. Institut Pasteur has been the most consistent funder, having provided over 45% of all funding each year, and 62% of all funding for leptospirosis R&D over the last four years.
Table 23. Leptospirosis R&D funders 2016
- No reported funding Funding organisation did not participate in the survey for this year. Any
contributions listed are based on data reported by funding recipients so may be incomplete
2013 2014 2015 2016
Indian ICMR - - - 1.1 48
Institut Pasteur 0.4 0.9 0.9 1.0 45
Inserm - - - 0.2 6.9
US NIH - 0.3 0.3 - -
Colombian Colciencias 0.1 - - -
Disease total 0.4 1.3 1.3 2.3 100
Funder US$ (millio
ns)
2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE72
TRACHOMA
Trachoma is an infectious eye disease caused by the bacterium Chlamydia trachomatis. The infection can be spread by contact with infected eyes or nose discharge, including by contact from flies and shared use of clothing and towels.134 Trachoma is common among children and in areas where there is unclean water and poor sanitation.135 After repeat infection and without medical treatment, the eyelid can turn inwards, causing the eyelashes to rub against the eyeball, resulting in scarring, visual impairment or irreversible blindness.135
Trachoma is not a fatal condition but it is the leading infectious cause of blindness. According to IHME Global Burden of Disease 2015 estimates, trachoma was responsible for 278,190 DALYs in developing countries,2 the twelfth highest cause of morbidity of G-FINDER neglected diseases.
WHO recommends a combination of interventions known as the SAFE strategy135 for the elimination of trachoma, which is an acronym for surgery (which has low acceptance and high recurrence rates); antibiotics (including treatment with azithromycin, however over-reliance on a single drug therapy can increase the risk of drug resistance); facial cleanliness; and environmental improvement to reduce transmission.
Because of the chal lenges associated with successful implementation (and sustainability) of the SAFE strategy, a vaccine is needed. There are several trachoma vaccines in development, mostly in the early (pre-clinical and discovery) stages.
Clinical diagnosis of trachoma is not always reliable, and current diagnostic tests are expensive and complex.136 Studies have shown that an antibody-based multiplex assay could be used to diagnose trachoma in low prevalence settings.137
TOTAL SPEND ON TRACHOMA R&D IN 2016
$2.2MILLION
Note that historical figures for trachoma R&D investment by the US NIH have been amended following a review and refinement of the search terms applied to data mine NIH databases. The G-FINDER figures now exclude investment made in R&D for Chlamydia trachomatis if that work was conducted specifically to progress research into chlamydia (the sexually transmitted infection), rather than trachoma (ocular infection). Historical US NIH and global funding for trachoma R&D is therefore lower than previously reported.
In 2016, funding for trachoma R&D was $2.2m. Vaccines and diagnostics are the only two product areas for trachoma that are included in the G-FINDER scope: more than half ($1.2m, 55%) of all reported funding was for vaccine R&D, while diagnostics received just $0.2m (10%). The remaining $0.8m (35%) of funding was not allocated to a specific product area.
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
IN SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Table 24. Trachoma R&D funding by product type 2007-2016
- No reported funding
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Vaccines (preventive) - 0.8 0.8 0.8 0.7 1.0 1.1 1.0 1.2 1.2 55
Diagnostics 0.8 <0.1 0.5 2.6 5.1 0.6 0.6 0.2 - 0.2 10
Unspecified 0.6 1.0 0.1 - - 0.4 0.5 0.1 - 0.8 35
Total 1.4 1.8 1.3 3.5 5.9 2.1 2.2 1.4 1.2 2.2 100
US$ (millio
ns)
Product 2016 % of total

FIN
DIN
GS
- D
ISEA
SES
PAGE73
More than half of all funding for trachoma R&D in 2016 was for clinical development ($1.1m, 52%), with very little funding reported for basic and early stage research ($0.2m, 10%). The remaining funding was not allocated to a specific product or R&D stage ($0.8m, 37%). This split was very different between product areas: funding for vaccine R&D was almost exclusively for clinical development ($1.1m, 96%) – entirely because of a US NIH grant to support planning for a Phase I trial of a live attenuated vaccine – while funding for diagnostic R&D was solely for discovery and pre-clinical research.
In 2016 the funder base for trachoma R&D expanded to four organisations, up from only two in 2015. The US NIH was the top funder, providing nearly two-thirds ($1.4m, 63%) of total investment. The German DFG provided just under a third ($0.7m, 30%), having been absent since 2013, while the Institut Pasteur and the Wellcome Trust accounted for 5.3% ($0.1m) and 1.8% (<$0.1m) of total funding respectively.
Trachoma was almost exclusively funded by the public sector ($2.1m, 98%).
A decade of investment in trachoma R&D• The US NIH has been the most consistent funder of trachoma R&D over the past decade,
having reported funding every year since 2008. The next most consistent funder is the Wellcome Trust, which has provided funding in just 6 of the last 10 years.
• Despite having invested nearly a third ($7.0m, 31%) of the ten year total, participation from industry in trachoma R&D has been intermittent, and absent since 2011.
Table 25. Trachoma R&D funders 2016
- No reported funding Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding
recipients so may be incomplete
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH - 0.8 1.2 1.2 1.1 1.5 1.5 0.9 1.0 1.4 63
German DFG - - - - - 0.2 - - 0.7 30
Institut Pasteur - <0.1 - <0.1 <0.1 - 0.1 0.1 - 0.1 5.3
Wellcome Trust 1.2 - - - - 0.5 0.4 0.3 0.2 <0.1 1.8
US CDC - - - - - - - 0.1 - - -
Aggregate industry 0.1 0.1 - 2.2 4.6 - - - - - -
Lygature 0.1
Swedish Research Council <0.1 0.1 - - - - - - - -
SSI - 0.7 - - - - - - - - -
Brazilian DECIT - 0.2 - - - - - - - - -
All other funders 0.1 - - - - - - - - - -
Disease total 1.4 1.8 1.3 3.5 5.9 2.1 2.2 1.4 1.2 2.2 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- D
ISEA
SES
PAGE74
RHEUMATIC FEVER
Rheumatic fever is a bacterial infection caused by Group A streptococcus that most commonly affects children aged 5-14 years. It usually follows untreated bacterial throat infections, and without treatment can lead to complications such as rheumatic heart disease, in which the heart valves are permanently damaged. It may also progress to heart failure and stroke.
According to the IMHE Global Burden of Disease study, rheumatic fever was the seventh highest cause of both mortality and morbidity of all the G-FINDER neglected diseases in 2015, resulting in 278,996 deaths and 10 million DALYs in developing countries.2
Acute rheumatic fever can be treated using currently available drugs (although post-infection prophylaxis requires multiple doses of antibiotics); however, treatment of rheumatic heart disease of ten requires surgery. The main R&D need is therefore the development of a vaccine. Several vaccines are in development, the most advanced is a Group A streptococcus vaccine in Phase I.138
TOTAL SPEND ON RHEUMATIC FEVER
R&D IN 2016
$1.3 MILLION
Global funding for rheumatic fever R&D in 2016 was $1.3m.
Preventive vaccines is the only product area for rheumatic fever included in the G-FINDER scope. All funding in 2016 was for early stage research, as there are no vaccine candidates currently in clinical development.
There were just two reported funders for rheumatic fever vaccine R&D in 2016. The US NIH contributed the majority of funding ($0.9m, 73%) and the Health Research Council of New Zealand (New Zealand HRC) provided the remainder ($0.3m, 27%). The Brazilian BNDES, which provided $0.6m in 2015, did not report any funding for 2016.
There was no investment from the philanthropic sector or industry in rheumatic fever R&D in 2016.
IN SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
OUT OF SCOPE
BASIC RESEARCH
DRUGS
VACCINES (PREVENTIVE)
VACCINES (THERAPEUTIC)
DIAGNOSTICS
VCPs
Table 26. Rheumatic fever R&D funding by product type 2007-2016
- No reported funding
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Vaccines (preventive) 1.7 2.2 3.3 2.0 0.8 0.8 0.9 1.2 2.2 1.2 92
Unspecified 0.3 0.3 0.2 - 0.1 0.1 - 0.1 <0.1 0.1 7.7
Total 1.9 2.5 3.4 2.0 0.9 1.0 0.9 1.3 2.3 1.3 100
US$ (millio
ns)
Product 2016 % of total

FIN
DIN
GS
- D
ISEA
SES
PAGE75
Table 27. Rheumatic fever R&D funders 2016
A decade of investment in rheumatic fever R&D• There are very few funders of rheumatic fever R&D; the US NIH and Australian NHMRC have
been the only consistent funders over the past decade, and the latter has not reported any funding for rheumatic fever since 2014. Industry provided sizeable contributions in 2008 and 2009, but since then has largely been absent.
• Almost all funding for rheumatic fever vaccine R&D over the last decade has been for discovery and pre-clinical development. Although this reflects the state of the R&D pipeline – with only one candidate in clinical development – the lack of clinic-ready candidates is not helped by the incredibly small annual global investment in rheumatic fever R&D.
- No reported funding Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding
recipients so may be incomplete
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 1.5 0.7 0.9 0.9 0.4 0.5 0.6 0.5 1.0 0.9 73
New Zealand HRC - - - - - - - - 0.6 0.3 27
Brazilian BNDES - 0.6 - -
Australian NHMRC 0.4 0.4 0.6 0.8 0.3 0.3 0.3 0.6 - - -
Aggregate industry - 1.1 1.7 - - - - 0.1 - - -
Swedish Research Council <0.1 0.1 - 0.1 0.1 - - - - -
Australian NHF 0.1 0.1 0.2 - -
Australia - India SRF 0.1
Fondazione Cariplo - 0.1 -
Australian DIIS 0.1 - - - - - - - - -
Anonymous funder <0.1
Disease total 1.9 2.5 3.4 2.0 0.9 1.0 0.9 1.3 2.3 1.3 100
US$ (millio
ns)
Funder 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE76
FUNDER OVERVIEW
Funding for neglected disease R&D was higher across all three sectors in 2016, the first time since 2012 that this had occurred. The largest increase came from the public sector (up $49m, 2.6%), with smaller but still significant increases in both philanthropic (up $28m, 4.4%) and industry investment (up $22m, 5.3%). This was the first funding increase in several years from either the public or philanthropic sectors, but marked the fifth consecutive year of increasing industry investment. As a result of the across the board increases in sector funding, the share of total funding coming from each of the public, philanthropic and industry sectors remained unchanged from 2015.
The public sector remained the most significant source of neglected disease R&D funding in 2016, contributing just under two-thirds ($2,034m, 64%) of the global total. As in previous years, most public sector funding came from HIC governments and multilaterals ($1,951m, 96%), with the remainder from LMIC governments. The philanthropic sector provided $671m (21%), and industry $497m (16%); of the industry investment, $391m (79%) came from MNCs, and $106m (21%) from SMEs.
For the first time in the history of the G-FINDER survey, funding increased from every sub-sector – from HIC governments to SMEs – with a notable contribution from organisations in LMICs. While the $49m increase in public sector funding was primarily driven by HIC governments and multilaterals (up $41m, 2.3%), it was supported by strong funding growth from LMIC governments††
(up $18m, 30%). And with only a marginal increase in MNC investment (up $0.8m, 0.2%) in 2016, essentially all of the increase in industry investment came from SMEs†† (up $23m, 30%), primarily from those based in LMICs.
NEGLECTED DISEASE FUNDERS
Figure 20. Total R&D funding by sector 2007-2016
†† Reported changes in LMIC public funding and SME investment are based on organisations with funding data in both 2015 and 2016 (rather than in every year of the survey, as is the case in the remainder of the report) as survey participation from these sectors is inconsistent year to year.
gOther
gPrivate (SMEs)
gPrivate (MNCs)
gPhilanthropic
gPublic (LMICs)
gPublic (multilaterals)
gPublic (HICs)
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US
$ (m
illio
ns)
Other Private (SMEs) Private (MNCs) Philanthropic Public (LMICs) Public (multilaterals) Public (HICs) 0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
68% 61% 65% 65% 65% 65%
62% 62% 61% 60%
0.2% 0.3%
0.4% 0.2% 0.3% 0.1%
0.5% 0.3% 0.6% 1% 2% 3%
2% 2% 2% 3%
3% 2% 2% 3%
22%
25%
21% 20% 20%
21% 22%
21% 21% 21%
6%
8%
9% 11% 10%
10% 10%
12% 13% 12% 2%
3% 2%
2% 2% 1%
2% 3% 3% 3%

FIN
DIN
GS
- FU
ND
ERS
PAGE77
PUBLIC FUNDERS
As has been the case in every year of the G-FINDER survey, the top three public funders in 2016 were the US, the UK and the EC. The US is by far the largest funder of these three; it was responsible for nearly three-quarters ($1,490m, 73%) of all global public funding in 2016, with the UK ($101m, 5.0%) and the EC ($77m, 3.8%) collectively contributing less than 10%. And while the UK again became the second largest public funder of neglected disease R&D in 2016 after falling behind the EC the previous year, the gap between the US and the second largest public funder was the largest since 2012.
2016 also saw the first increase in YOY public funding for neglected disease R&D since 2012 (up $49m, 2.6%). The largest increases came from the US government (up $78m, 5.5%), mainly due to increased US NIH investment (up $89m, 7.2%), and two European governments: the Netherlands (up $18m, 447%), who returned to the top 12 after dropping out in 2015, due to a new PDP funding round from the Dutch DGIS; and the UK (up $9.3m, 10%), with increased funding from both the UK MRC and UK DFID. Most of the other notable increases in public funding came from governments outside of North America and Europe. These increases came from Brazil (up $9.0m, 265%), partly due to more accurate reporting by Brazilian FAPEMIG (up $5.1m, from a low base); Sweden (up $6.4m, 78%), Japan (up $5.5m, 50%), which funds neglected disease R&D through the Global Health Innovative Technology (GHIT) Fund, and which made its largest ever investment in 2016; India (up $4.9m, 11%), which overtook France and Germany to become the fourth largest government funder of neglected disease R&D globally in 2016; Germany (up $4.3m, 19%); and South Africa (up $3.3m, 59%). As a result of the increases from Brazil, India and South Africa, public funding from IDCs in 2016 was the highest recorded since 2013 by the G-FINDER survey (up $17m, 32%, to $78m).
All of the notable decreases in public funding for neglected disease R&D in 2016 came from European funders. The most significant reduction came from the EC (down $49m, -39%), although this was linked to reduced funding of EDCTP (down $32m, -80%) as a result of a number of extraordinary payments to EDCTP in 2015 that would otherwise have been made in 2014 and 2016. Reported funding from France decreased (down $16m, -28%), but this was entirely due to more accurate reporting by Inserm (down $20m, -43%). Switzerland was the only other top public funder to invest less in 2016 (down $6.9m, -52%), with lower funding from both the Swiss State Secretariat for Education, Research and Innovation (SERI) and Swiss Agency for Development and Cooperation (SDC). Canada and Ireland both dropped out of the top 12 in 2016.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE78
PUBLIC FUNDING BY GDP
Absolute funding can be a misleading measure of public R&D investment, as it can underplay the relative contributions of smaller countries and LMICs. For this reason, we have also analysed country investments in neglected disease R&D in relation to their gross domestic product (GDP).
When analysed by proportion of GDP rather than absolute funding, a slightly different picture of public funding emerges. Three countries not ranked in the top 12 funders by absolute funding appear in this list when ranked by contribution relative to GDP: South Africa, Ireland and Norway. In contrast, Brazil and Japan drop out of the list when GDP is factored in, as does the EC (which cannot be fairly analysed with this measure). The US, UK, India, France, Germany, Netherlands, Australia, Switzerland and Sweden all ranked in the top 12 using either metrics. South Africa, an IDC, provided the third highest contribution as a percentage of GDP of all countries in 2016, behind only the US and the UK.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016 No funding organisations from this country participated in the survey for this year
Table 28. Top public R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
United States of America 1,442 1,463 1,687 1,606 1,568 1,668 1,491 1,457 1,415 1,490 73
United Kingdom 88 90 126 138 112 79 107 112 92 101 5.0
EC 113 122 112 87 104 89 106 104 126 77 3.8
India 40 27 40 45 45 53 40 45 50 2.5
France 14 27 45 37 56 50 73 60 60 47 2.3
Germany 12 3.5 32 35 30 51 42 45 51 43 2.1
Netherlands 31 25 25 17 23 14 22 17 4.9 23 1.1
Australia 20 28 25 28 35 44 23 34 20 22 1.1
Brazil 22 24 29 10 11 19 15 8.7 7.4 18 0.9
Switzerland 7.5 4.7 8.5 15 15 17 17 19 21 18 0.9
Japan 4.5 7.3 6.1 9.3 3.4 2.5 11 11 14 17 0.9
Sweden 19 22 28 17 17 16 5.9 6.0 8.3 15 0.7
Subtotal of top 12^ 1,827 1,909 2,172 2,045 2,026 2,108 1,979 1,921 1,870 1,922 94
Total public funding 1,932 2,041 2,295 2,176 2,143 2,207 2,095 1,994 1,954 2,034 100
US$ (millio
ns)
Country2016 % of to
tal

FIN
DIN
GS
- FU
ND
ERS
PAGE79
Figure 21. Public R&D funding by GDP^ 2016 (A value of 10 is equivalent to an investment of 0.01% of GDP)
‡ Inserm reported more detailed data for 2016, resulting in a proportion of its reported 2016 investment being considered outside the scope of G-FINDER; it is therefore possible that Inserm’s investment in prior years is overstated.
HIGH-INCOME COUNTRIES AND MULTILATERALS
HIC governments and multilaterals once again provided almost all ($1,951m, 96%) public funding for neglected disease R&D in 2016. YOY investment increased for the first time since 2012 (up $41m, 2.3%), with a large increase in US funding (up $78m, 5.5%) – also for the first time since 2012. There were also smaller but notable increases from the Netherlands (up $18m, 447%), the UK (up $9.3m, 10%), Sweden (up $6.4m, 78%), Japan (up $5.5m, 50%) and Germany (up $4.3m, 19%). These increases were enough to outweigh decreased funding from a number of other HICs, most notably the EC (down $49m, -39%), France (down $16m, -28%) and Switzerland (down $6.9m, -52%). Funding from the EC fell largely due to a number of extraordinary payments made to EDCTP in 2015 that otherwise would have been made in 2014 and 2016. Reported funding from France dropped to the lowest level since 2010, as a result of Inserm (down $20m, -43%) reporting more detailed data for 2016‡.
Multilaterals invested a total of $42m in 2016, the largest contribution from this sector in G-FINDER history, providing 1.3% of global total funding.
Once again, funding from HIC governments and multilaterals in 2016 was heavily concentrated in just three diseases: HIV/AIDS, TB and malaria, which collectively received over three-quarters ($1,499m, 77%) of total funding. YOY funding increased for HIV/AIDS (up $42m, 5.0%) and malaria (up $6.1m, 2.3%), while funding for TB (down $0.4m, -0.1%) remained essentially steady. The increase in HIV/AIDS was the first since 2012, and was primarily due to increased investment in this disease by the US NIH (up $31m, 4.6%).
^ GDP figures taken from International Monetary Fund (IMF) World Economic Outlook database Figure provides value of (US$ funding / GDP) * 100,000
US
8.0
UK
3.8
So
uth Africa
3.2
France
1.9Sw
itzerland
2.8Ne
therlandsNorway
1.3
India
2.2
Sweden
2.9
Ireland
2.6
Australia
1.8
Germany
1.2
2.9

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE80
The US NIH was also the driving force behind the majority of increases in HIC government and multilateral funding for other neglected diseases in 2016. Strong growth in funding for Salmonella infections (up $12m, 33%) and dengue (up $9.0m, 16%), both primarily from the US NIH, took these two diseases to historically high levels of investment. The US NIH was also responsible for the more modest increases in HIC government and multilateral funding for kinetoplastids (up $4.1m, 6.4%), assisted by renewed investment in this area from the Dutch DGIS, and helminth infections (up $1.2m, 3.1%).
New disease added to G-FINDER in 2013- No reported funding
Table 29. Public (HIC and multilaterals) R&D funding by disease 2007-2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
HIV/AIDS 1,055 1,038 1,084 1,013 977 1,005 927 893 841 873 45
Tuberculosis 238 226 335 307 281 274 271 298 312 341 17
Malaria 232 252 285 307 284 284 283 280 280 285 15
Kinetoplastids 50 86 102 103 93 90 74 79 69 78 4.0
Dengue 40 43 58 51 58 54 45 50 59 67 3.5
Diarrhoeal diseases 50 68 102 84 91 85 87 83 73 56 2.9
Salmonella infections 10 29 37 38 33 41 40 39 38 51 2.6
Helminth infections (worms & flukes) 42 37 51 50 47 59 50 45 42 43 2.2
Hepatitis C (genotypes 4, 5 & 6) 14 19 12 12 0.6
Bacterial pneumonia & meningitis 11 10 13 18 28 16 25 18 16 12 0.6
Cryptococcal meningitis 2.8 5.6 5.5 5.6 0.3
Leprosy 3.9 4.1 7.0 4.0 4.6 11 6.2 5.8 4.5 5.4 0.3
Buruli ulcer 2.3 1.5 1.6 3.7 3.4 3.4 4.0 0.7 0.9 2.2 0.1
Trachoma - 1.5 1.3 1.2 1.1 1.5 1.8 1.1 1.0 2.1 0.1
Rheumatic fever 1.9 1.3 1.6 1.8 0.9 1.0 0.9 1.2 1.6 1.3 0.1
Leptospirosis 0.4 1.2 1.3 1.2 0.1
Platform technologies 3.1 6.0 7.7 11 11 26 29 11 13 16 0.8
Adjuvants and immunomodulators <0.1 0.9 3.1 3.9 1.9 19 17 3.4 3.3 11 0.5
General diagnostic platforms 1.2 2.2 2.1 5.7 8.5 7.4 8.5 5.9 9.6 5.5 0.3
Delivery technologies and devices 1.9 2.9 2.6 1.2 0.4 0.4 4.1 1.6 0.6 0.3 <0.1
Core funding of a multi-disease R&D organisation
91 82 62 66 82 66 63 60 75 58 3.0
Unspecified disease 55 65 76 48 69 103 69 45 45 41 2.1
Total public funding (HICs/multilaterals) 1,885 1,950 2,225 2,105 2,064 2,121 1,993 1,935 1,891 1,951 100
US$ (millio
ns)
Disease or
R&D area 2016 % of total

FIN
DIN
GS
- FU
ND
ERS
PAGE81
The most notable drops in disease-specific HIC government and multilateral funding were for diarrhoeal diseases (down $16m, -23%) and bacterial pneumonia & meningitis (down $5.0m, -35%), however these were both primarily due to more detailed reporting by Inserm.
Nearly two-thirds (59%) of all HIC government and multilateral funding for neglected disease R&D in 2016 went to basic and early stage research, with only a quarter (27%) going to clinical development and post registration studies. Remaining funding (14%) was not allocated to a specific R&D stage. US NIH funding for the clinical development of HIV/AIDS preventive vaccines accounted for over one-third (37%) of all HIC government and multilateral investment in late stage research. If this funding is excluded, the focus of all remaining HIC government and multilateral funding for neglected disease R&D becomes even more apparent; excluding US NIH funding for HIV/AIDS vaccine clinical trials, just 19% of all other HIC government and multilateral investment is for clinical research and post registration studies, while 66% is for basic and early stage research.
A decade of HIC government and multilateral funding for neglected disease R&D• HIC governments and multilaterals have provided 96% of all public funding for neglected
disease R&D over the last decade. The US, the UK and the EC have consistently been the top three funders, and have contributed more than 85% of all HIC and multilateral funding over this period, with the US government alone accounting for over three-quarters (76%) of this investment.
• Funding from HIC governments and multilaterals was heavily concentrated on HIV/AIDS, TB and malaria, which collectively accounted for three-quarters (76%) of all funding from this group over the past decade.
• HIV/AIDS alone accounted for nearly half (48%) of all funding from HIC governments and multilaterals since 2007, however funding for HIV/AIDS declined over the decade from $1,055m in 2007 to $873m in 2016.
LOW- AND MIDDLE-INCOME COUNTRIES
Public funders in LMICs invested $84m in neglected disease R&D in 2016, representing 4.1% of all global public funding. Inconsistent survey participation by many LMIC organisations makes long-term or multi-year comparisons of neglected disease R&D funding difficult, but investments from LMIC public funders who participated in both 2015 and 2016 grew by $18m (up 30%).§
As in previous years, the vast majority of LMIC public funding for neglected disease R&D ($78m, 93%) came from the three IDCs (India, Brazil, and South Africa) all of which increased their funding in 2016. Although nearly two-thirds ($50m, 60%) of all LMIC public funding in 2016 came from Indian organisations, the largest YOY increase came from Brazil (up $9.0m, from a low base), although this was partly a reflection of more accurate reporting by the Brazilian Support Foundation for Research in the State of Minas Gerais (FAPEMIG, up $5.1m, from a low base). Indian government funding for neglected disease R&D increased by $4.9m (up 11%) and South African government funding by $3.3m (up 59%).
§ As LMIC survey participation is inconsistent from year to year, reported changes in LMIC public funding are based on organisations with funding data in both 2015 and 2016 (rather than in every year of the survey, as is the case in the remainder of the report). This group of funders provided $77m of the $84m in total LMIC public funding for 2016.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE82
LMIC public funding in 2016 remained concentrated on TB, malaria, and kinetoplastids, which collectively received more than half of all funding ($49m, 58%) in 2016. YOY LMIC funding either increased or was steady for each of these diseases in 2016. The largest increase was in TB (up $5.4m, 35%), with record high funding from the Indian ICMR (up $3.9m, 49%) and a large disbursement from the South African MRC (up $2.3m, after not funding TB R&D in 2015). Kinetoplastid R&D funding also increased (up $2.7m, 41%) in 2016, due to large disbursements from three Brazilian organisations: FAPEMIG (up $1.9m, from a low base), the Brazilian State of São Paulo Research Foundation (FAPESP, up $1.4m, 72%) and BNDES (up $0.9m, after not funding kinetoplastid R&D since 2009). Following an increase in 2015, LMIC public funding for malaria R&D was steady (down $0.1m, -0.7%) in 2016. Outside of these three diseases, LMIC public funding also increased for dengue (up $4.1m, 117%) and diarrhoeal diseases (up $2.2m, 38%), both largely due to increased funding from Brazilian public sector organisations.
LMIC public funding for most of the remaining diseases fell in 2016, although all of these drops were relatively small. Funding for HIV/AIDS (down $0.9m, -19%) accounted for the lowest share ($4.0m, 4.7%) of LMIC public funding invested in this disease in G-FINDER history, while funding was also lower for leprosy (down $0.6m, -12%), and hepatitis C (down $0.3m, -39%). Rheumatic fever did not receive any LMIC public funding in 2016, after being funded for the first time (with $0.6m) in 2015.
Inconsistent levels of grant detail provided by LMIC public funders makes any analysis of funding by R&D stage difficult, with most LMIC funding in 2016 not allocated to a specific product or R&D stage ($52m, 62%). Where funding was allocated to a specific R&D stage, it was largely for basic and early stage research ($27m, 32% of total LMIC funding), rather than clinical development and post registration studies ($4.9m, 5.8%).

FIN
DIN
GS
- FU
ND
ERS
PAGE83
^ Please note that no funding organisations from India participated in the survey in 2007 New disease added to G-FINDER in 2013
- No reported funding
Table 30. Public (LMIC) R&D funding by disease 2007-2016^
A decade of LMIC government funding for neglected disease R&D• The Indian government has steadily increased its investment in neglected disease R&D over
the last decade. It has been the top LMIC government funder in every year since 2010, and became the fourth largest government funder globally in 2016.
• The next largest LMIC public funder was the Brazilian government, which has had far more variable levels of investment, ranging from a high of $29m in 2009 to a low of $7.4m in 2015.
• In 2007, LMIC governments invested more in HIV/AIDS than in any other neglected disease, just like HIC governments and multilaterals. By 2016 however, TB had become the highest funded disease by LMIC governments, and HIV had dropped to seventh place.
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Tuberculosis 3.3 11 9.5 11 17 17 32 14 16 22 26
Malaria 2.9 18 18 9.9 13 20 20 9.1 13 14 17
Kinetoplastids 4.9 7.9 8.1 10 9.0 12 8.2 8.5 8.5 13 15
Diarrhoeal diseases - 6.0 4.5 7.2 11 4.7 5.4 5.8 5.7 7.9 9.5
Dengue 1.6 3.0 13 5.6 4.0 6.3 3.3 3.2 4.0 7.6 9.1
Leprosy 1.4 5.5 3.8 3.6 2.5 2.1 4.6 3.5 4.7 4.0 4.8
HIV/AIDS 24 26 9.6 17 18 12 18 6.0 5.5 4.0 4.7
Helminth infections (worms & flukes) 2.6 3.0 1.3 1.2 1.9 2.9 1.8 2.7 2.0 1.8 2.2
Leptospirosis - 0.1 - 1.1 1.3
Salmonella infections - 0.1 <0.1 0.7 0.5 0.4 0.6 0.6 0.2 0.6 0.8
Bacterial pneumonia & meningitis - 4.5 0.3 0.3 0.1 0.3 <0.1 0.3 <0.1 0.5 0.6
Hepatitis C (genotypes 4, 5 & 6) 5.5 0.2 0.8 0.5 0.6
Rheumatic fever - - - - - - - - 0.6 - -
Trachoma - 0.2 - - - - - - - - -
Platform technologies 4.3 2.0 - 3.5 0.5 4.5 0.6 0.4 1.3 3.0 3.6
Delivery technologies and devices - 1.3 - 1.9 <0.1 3.9 0.4 0.3 1.2 2.2 2.6
General diagnostic platforms 1.7 0.5 - 0.9 0.4 0.6 <0.1 0.1 0.1 0.8 1.0
Adjuvants and immunomodulators 2.6 0.2 - 0.6 - 0.1 0.1 <0.1 <0.1 <0.1 <0.1
Core funding of a multi-disease R&D organisation
1.3 4.1 0.7 0.8 0.3 - 0.4 0.3 1.5 1.9 2.3
Unspecified disease 0.1 0.6 0.1 - 0.4 3.7 2.3 3.9 0.2 2.2 2.6
Total public funding (LMICs) 46 92 70 71 79 86 102 59 64 84 100
US$ (millio
ns)
Disease or
R&D area 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE84
PHILANTHROPIC FUNDERS
The philanthropic sector provided $671m for neglected disease R&D in 2016, representing 21% of total global funding. As in previous years, the Gates Foundation and the Wellcome Trust collectively provided the vast majority ($642m, 96%) of all philanthropic funding.
YOY philanthropic funding for neglected disease R&D increased in 2016 (up $28m, 4.4%), after two consecutive years of decreasing investment. The largest increase came from the Wellcome Trust (up $17m, 21%) – the result of large core funding disbursements to its international research programmes in Kenya, Thailand, Vietnam and Malawi – followed by the Gates Foundation (up $12m, 2.3%) and MSF (up $4.5m, 77%).
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 31. Top philanthropic R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Gates Foundation 530 707 641 528 525 520 538 532 530 542 81
Wellcome Trust 50 53 58 68 80 124 114 107 83 101 15
MSF 6.6 6.7 4.2 4.3 4.8 5.4 5.5 4.4 5.8 10 1.5
Gavi 12 17 2.5 9.8 19 10 5.8 0.9
Fundació La Caixa 0.3 0.3 3.2 2.6 3.0 3.4 3.3 0.5
Funds raised from the general public 2.3 1.4 0.5 0.4 0.5 0.4 0.7 0.9 1.2 1.1 0.2
UBS Optimus Foundation 0.5 1.1 1.1 6.7 5.0 3.1 2.5 3.4 1.4 0.8 0.1
Kleberg Foundation 0.2 0.6 0.1
Sidaction 0.2 0.4 0.7 0.5 0.1
LRI 0.5 0.5 0.1
ExxonMobil Foundation 2.2 2.1 1.6 0.8 0.3 0.5 0.5 0.5 0.5 0.1
All other philanthropic organisations 6.4 14 18 18 15 20 13 6.4 12 4.9 0.7
Total philanthropic funding 611 803 724 630 634 687 696 655 648 671 100
US$ (millio
ns)
Funder 2016 % of total

FIN
DIN
GS
- FU
ND
ERS
PAGE85
As has been the case in every year of the G-FINDER survey, the three diseases to receive the most philanthropic R&D funding were HIV/AIDS, malaria and TB, which collectively received more than half of all funding ($391m, 58%) in 2016. TB was the only one of these three to see a reduction in YOY philanthropic funding in 2016 (down $33m, -24%), with a drop in Gates Foundation funding to TB Alliance associated with the start of a new project cycle. Philanthropic funding for HIV/AIDS grew by $14m (up 11%), also entirely due to the Gates Foundation, whose increased funding for preventive vaccine development (up $23m, 32%) and $7.1m in funding for therapeutic vaccines more than offset its reduced investment in other product areas. Philanthropic funding for malaria R&D increased by $12m (up 9.6%), due to an almost tripling of Gates Foundation funding for vector control products (up $30m, 193%) which offset decreases in its funding for malaria drugs (down $13m, -24%) and vaccines (down $6.5m, -35%).
Philanthropic funding also increased for kinetoplastids (up $10m, 67%), driven by a grant cycle-related boost from the Gates Foundation to DNDi, and diarrhoeal diseases (up $4.0m, 8.8%), with MSF funding a Phase III trial of a pentavalent rotavirus vaccine candidate. The only other notable decrease in philanthropic funding in 2016 was for bacterial pneumonia & meningitis (down $15m, -43%), however, as with the previous year’s increase, this was due to cyclical funding from the Gates Foundation to PATH.
A third of all philanthropic funding for neglected disease R&D in 2016 was for basic and early stage research ($229m, 34%), most of which was for discovery and pre-clinical R&D ($133m, 20% of total philanthropic funding). Clinical or field development and post registration studies accounted for 26% ($172m) of philanthropic funding in 2016. Most remaining funding was also for product development (rather than basic research) but not allocated to a specific R&D stage, mainly for PDP portfolio projects, biological control products and platform technologies ($172m, 26%), or as core funding to multi-disease R&D organisations ($64m, 9.6%). A relatively small amount was not allocated to a specific disease or product ($34m, 5.0%).

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE86
New disease added to G-FINDER in 2013- No reported funding
Table 32. Philanthropic R&D funding by disease 2007-2016
A decade of philanthropic funding for neglected disease R&D• As the second largest funder of neglected disease R&D globally, the Gates Foundation
has been the dominant philanthropic funder over the past decade, providing 83% of all philanthropic funding. Along with the next largest philanthropic funder (the Wellcome Trust, with 12%), these two organisations accounted for 95% of philanthropic funding for neglected disease R&D over the past ten years.
• While the Wellcome Trust doubled its investment between 2007 and 2016 (from $50m to $101m), Gates Foundation funding peaked at $707m in 2008, and since 2010 has been essentially steady at an average of around $530m per year.
• Philanthropic funding has also been heavily concentrated on malaria, HIV/AIDS, and TB over the past ten years, with these three diseases accounting for 68% of all philanthropic funding.
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
HIV/AIDS 118 202 153 154 152 160 149 136 129 141 21
Malaria 173 230 242 136 200 167 152 169 129 140 21
Tuberculosis 138 161 124 136 117 122 145 150 143 110 16
Diarrhoeal diseases 65 49 55 53 37 49 63 47 50 51 7.6
Kinetoplastids 73 52 58 32 23 21 20 33 16 26 3.9
Bacterial pneumonia & meningitis 7.0 31 27 51 40 52 28 7.4 41 25 3.7
Helminth infections (worms & flukes) 12 30 25 22 30 26 33 29 22 21 3.2
Dengue 2.1 3.2 3.1 4.3 6.3 10 21 25 24 21 3.1
Salmonella infections 0.1 0.9 3.7 7.1 9.3 12 15 11 16 15 2.3
Leprosy 0.8 1.1 1.1 2.7 1.7 2.2 2.0 1.2 1.1 1.3 0.2
Buruli ulcer - 0.2 0.3 1.8 2.3 2.6 2.4 3.0 1.0 0.6 0.1
Cryptococcal meningitis 0.3 <0.1 0.1 0.1 <0.1
Trachoma 1.2 - - - 0.1 0.5 0.4 0.3 0.2 <0.1 <0.1
Hepatitis C (genotypes 4, 5 & 6) 0.1 0.1 <0.1 <0.1 <0.1
Rheumatic fever - 0.1 0.2 0.2 - - - - - - -
Leptospirosis <0.1 - - - -
Platform technologies 2.4 9.6 17 15 7.0 20 15 11 19 33 4.9
Delivery technologies and devices 0.1 4.8 6.4 5.1 1.5 0.7 1.7 2.4 5.8 14 2.1
General diagnostic platforms 2.3 3.2 7.8 4.0 1.6 9.3 8.4 3.9 4.1 12 1.8
Adjuvants and immunomodulators - 1.6 2.6 5.7 3.9 9.5 5.0 5.1 8.7 6.9 1.0
Core funding of a multi-disease R&D organisation
15 12 6.4 5.9 4.8 39 40 20 30 64 9.6
Unspecified disease 3.8 20 8.7 7.5 3.3 2.4 11 11 28 22 3.2
Total philanthropic funding 611 803 724 630 634 687 696 655 648 671 100
US$ (millio
ns)
Disease or
R&D area 2016 % of total

FIN
DIN
GS
- FU
ND
ERS
PAGE87
PRIVATE SECTOR FUNDERS
The private sector invested $497m in neglected disease R&D in 2016, accounting for 16% of total global funding. For the third year in a row, this represented both the largest ever industry investment and the largest industry share of total funding in the history of the G-FINDER survey. Although the majority of industry investment in neglected disease R&D once again came from MNCs ($391m, 79%), SME investment in 2016 ($106m, 21%) was the highest ever recorded, and the largest share of total industry investment since 2008.
For the fifth year in a row, YOY industry investment increased (up $22m, 5.3%) in 2016. This also marked the second consecutive year in which the growth in industry investment in neglected disease R&D came from regular SME survey participants (up $23m, 30%), while MNC investment remained steady (up $0.8m, 0.2%).
MULTINATIONAL PHARMACEUTICAL COMPANIES
Just over three-quarters ($296m, 76%) of all MNC investment in neglected disease R&D in 2016 went to malaria, TB and HIV/AIDS, up from 72% in 2015. HIV/AIDS was the only one of these three diseases to see an increase in MNC investment (up $30m, 62%) in 2016. Coming as a result of record high MNC investment in HIV/AIDS preventive vaccine R&D (up $26m, 65%) in 2016, this increase resulted in the largest investment in HIV/AIDS R&D by MNCs in the history of the G-FINDER survey. MNC investment in TB R&D fell in 2016 (down $10m, -11%), continuing the sustained decline seen since 2010, and there was also a slight drop in malaria R&D investment (down $3.8m, -2.9%), although this followed two consecutive years of large funding increases.
Other than HIV/AIDS, the only other notable increase in MNC R&D investment was for bacterial pneumonia & meningitis (up $8.1m, 69%), with a sharp increase in reported investment in meningococcal vaccine development (up $11m, 609%). In contrast, MNC investment in hepatitis C decreased (down $15m, -68%) to its lowest level since G-FINDER started tracking hepatitis C R&D funding, likely associated with the conclusion of late stage clinical trials and the regulatory approval of new DAAs. For the third year in a row, MNC investment in diarrhoeal diseases also decreased (down $6.1m, -31%), in this case driven by reduced investment in rotavirus R&D, likely associated with the conclusion of post registration safety and impact studies for approved rotavirus vaccines.
Almost two-thirds of all MNC investment in neglected disease R&D in 2016 was for clinical development and post registration studies ($239m, 61%), with a further 31% ($121m) going to basic and early stage research, essentially all of which was for discovery and pre-clinical R&D (rather than basic research). Remaining MNC investment ($30m, 7.7%) was not allocated to a specific product or R&D stage.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE88
New disease added to G-FINDER in 2013- No reported funding
Table 33. MNC R&D funding by disease 2007-2016
A decade of MNC investment in neglected disease R&D• MNC R&D investment grew rapidly between 2007 and 2010, driven by investment in TB
and malaria drug development, with a further small increase in 2014, driven by increased investment in malaria drug development, but has otherwise been relatively stable.
• Nearly three-quarters (71%) of all MNC investment in neglected disease R&D over the last decade went to TB, malaria and HIV/AIDS.
• MNC R&D investment in TB has declined considerably since its peak in 2010, driven by falling investments in drug R&D. In contrast, MNC investment in malaria and HIV/AIDS has increased sharply, especially since 2013.
SMALL PHARMACEUTICAL AND BIOTECHNOLOGY FIRMS
SMEs invested $106m in neglected disease R&D in 2016. Not only was this the highest reported investment by SMEs in the history of the G-FINDER survey, it also accounted for the largest share (21%) of total industry investment in neglected disease R&D that this sector has contributed since 2008. More than two-thirds ($73m, 69%) of all SME investment in neglected disease R&D in 2016 came from firms in innovative developing countries, with firms from developed countries contributing the remainder ($33m, 31%).
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Malaria 72 75 77 104 85 99 70 112 135 132 34
Tuberculosis 54 81 118 151 147 131 111 99 94 87 22
HIV/AIDS 7.5 21 19 17 14 15 9.8 40 48 77 20
Bacterial pneumonia & meningitis 14 32 27 24 32 35 31 31 12 20 5.1
Dengue 4.9 3.4 4.3 6.9 11 8.1 7.2 7.3 14 15 3.7
Diarrhoeal diseases 9.8 24 36 33 23 28 38 31 20 14 3.5
Kinetoplastids 4.6 1.2 3.6 9.4 9.7 17 16 12 16 13 3.3
Helminth infections (worms & flukes) 0.1 4.6 9.5 3.7 2.6 3.5 8.4 6.8 11 8.5 2.2
Hepatitis C (genotypes 4, 5 & 6) 28 26 21 6.7 1.7
Salmonella infections - 1.3 2.0 3.1 5.0 4.1 4.1 3.8 3.3 3.8 1.0
Leprosy - - - - - - 0.1 0.1 0.7 0.4 0.1
Rheumatic fever - 1.1 1.7 - - - - 0.1 - - -
Trachoma 0.1 0.1 - - - - - - - - -
Buruli ulcer - 0.1 - - - - - - - - -
Core funding of a multi-disease R&D organisation
- - - - - - 2.2 8.0 8.2 11 2.9
Unspecified disease - - - - 3.1 1.5 7.7 4.1 2.5 2.5 0.6
Total MNC funding 167 246 297 352 333 343 333 381 385 391 100
US$ (millio
ns)
Disease or
R&D area 2016 % of total

FIN
DIN
GS
- FU
ND
ERS
PAGE89
Just over two-thirds ($71m, 67%) of all SME funding was invested in three disease groups: bacterial pneumonia & meningitis, Salmonella infections and diarrhoeal diseases. SMEs, along with LMIC public funders, are the only sectors that did not have HIV/AIDS, malaria and TB as their top three highest funded diseases.
Irregular survey participation among SMEs makes analysis of funding trends difficult, but investment from regular survey participants‡ increased significantly in 2016, highlighted by historically high levels of investment in a number of diseases. SME investment in bacterial pneumonia & meningitis R&D (up $10m, 43%) was the highest ever recorded by G-FINDER, reflecting increased investment in the clinical development of new pneumococcal conjugate vaccines. SME investment in Salmonella R&D almost doubled in 2016 (up $9.4m, 86%), also to its highest recorded level, reflecting the progression of new vaccine candidates for typhoid fever through the pipeline. SME investment in R&D for diarrhoeal diseases increased (up $2.5m, 18%) for the fourth year in a row, also to historically high levels, while 2016 also saw the first reported SME investment in hepatitis C R&D ($3.5m).
Reductions in SME investment in 2016 – where they did occur – were generally smaller, with the largest drops seen in kinetoplastids (down $2.4m, -56%) and malaria (down $1.6m, -32%), followed by helminth infections (down $0.8m, -92%) and TB (down $0.8m, -7.8%).
New disease added to G-FINDER in 2013- No reported funding
Table 34. SME R&D funding by disease 2007-2016
‡ SME increases or decreases refer to organisations that had funding data included for both 2015 and 2016, rather than in every year of the survey, as SME survey participation is inconsistent from year to year
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Bacterial pneumonia & meningitis 0.5 22 9.1 7.7 6.0 5.5 18 17 24 35 33
Salmonella infections - 13 2.0 0.2 0.1 0.3 6.0 12 11 20 19
Diarrhoeal diseases 2.8 1.9 5.4 0.7 5.2 2.7 6.3 8.9 14 16 15
Tuberculosis 17 15 18 18 15 9.3 5.1 8.2 10 9.1 8.6
HIV/AIDS 12 28 19 14 9.6 7.6 6.4 6.4 8.5 6.7 6.3
Malaria 10 9.8 19 11 7.2 7.1 5.8 6.3 6.6 5.2 4.9
Hepatitis C (genotypes 4, 5 & 6) - - - 3.5 3.3
Dengue 2.5 0.2 0.9 0.5 0.5 0.5 0.3 0.5 1.0 2.4 2.3
Kinetoplastids <0.1 1.7 1.4 1.4 3.8 0.8 0.6 7.0 4.8 1.9 1.8
Helminth infections (worms & flukes) 0.7 1.1 0.4 3.2 5.3 0.8 0.1 8.5 0.9 0.1 0.1
Trachoma - - - 2.2 4.6 - - - - - -
Leprosy - - - 0.1 0.1 - - - - - -
Buruli ulcer <0.1 0.2 - - - - - - - - -
Core funding of a multi-disease R&D organisation
- - - - - - - 0.2 - - -
Unspecified disease 0.7 - - - - <0.1 1.9 5.5 3.6 5.9 5.6
Total SME funding 47 93 76 61 58 35 51 81 84 106 100
US$ (millio
ns)
Disease or
R&D area 2016 % of total

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE90
More than three-quarters of all SME investment in neglected disease R&D in 2016 was in clinical or field development and post registration studies ($82m, 78%), with most of the remainder invested in basic and early stage research ($16m, 15%), the vast majority of which was for discovery and pre-clinical R&D, rather than basic research. Remaining investment was not allocated to a specific product or R&D stage ($7.9m, 7.5%).
A decade of SME investment in neglected disease R&D• Annual global SME investment in neglected disease R&D first peaked at $93m in 2008, before
declining to a low of $35m in 2012. Since then, SME investment has grown rapidly, to reach a record high of $106m in 2016.
• The largest increases in SME investment since 2012 have been for bacterial pneumonia & meningitis (up $29m, from $5.5m), Salmonella infections (up $20m, from $0.3m) and diarrhoeal diseases (up $13m, from $2.7m).
• Firms from India and the US have contributed more than two-thirds (68%) of all SME investment in neglected diseases since 2007. In 2016, SMEs from India alone accounted for 66% of all SME investment in neglected diseases.
IN-KIND CONTRIBUTIONS
In addition to their direct R&D spend, companies conducting neglected disease R&D incur a range of other costs, such as infrastructure costs and costs of capital. These costs are not included in G-FINDER, due to the difficulty of accurately quantifying or allocating them to neglected disease programmes. G-FINDER also does not include the cost of companies’ non-R&D contributions to combating neglected diseases, such as drug donations for mass drug administration programmes.
Companies also provide in-kind contributions that are specifically targeted to neglected disease R&D, but cannot easily be captured in monetary terms. Although difficult to quantify, these inputs are of substantial value to their recipients, and may represent a significant cost to companies.
We note that while some companies have nominated areas where they provide such contributions, others wished to remain anonymous.

FIN
DIN
GS
- FU
ND
ERS
PAGE91
^ Company donors listed do not necessarily engage in all activities listed as examples of in-kind contributions
Table 35. Typical industry in-kind contributions 2016
In-kind contribution Examples Some company donors^
Transfer of technology and technical expertise to develop, manufacture, register and distribute neglected disease products
• Identifying scientific obstacles• Sharing best practices and developing systems for clinical, technical and
regulatory support• Developing capacity for pharmacovigilance• Donating equipment
EisaiGSKJohnson and JohnsonMSDNovartisSanofiOtsuka
Provision of expertise
• Supporting clinical trials• Collaboration of scientists, sharing trial results and facilitating parallel, concurrent
testing• Participation on scientific advisory or management boards of external
organisations conducting neglected disease R&D• Providing expertise in toxicology/ADME and medicinal chemistry• Evaluating new compounds proposed by external partners• Allowing senior staff to take sabbaticals to work with neglected disease groups
AbbvieEisaiGSKJohnson and JohnsonMSDNovartisPfizerSanofiOtsuka
Teaching and training
• In-house attachments offered to Developing Country trainees in medicinal chemistry, clinical trial training etc
• Providing training courses for Developing Country researchers at academic institutions globally
• Organising health care provider training in Developing Country for pharmacovigilance of new treatments
• Organising conferences and symposia on neglected disease-specific topics
AbbvieGSKJohnson and JohnsonMSDNovartisSanofiOtsuka
Intellectual property
• Access to proprietary research tools and databases• Sharing compound libraries with WHO or with researchers who can test and
screen them for possible treatments• Providing public and non-for-profit groups with information on proprietary
compounds they are seeking to develop for a neglected disease indication• Forgoing license or providing royalty-free license on co-developed products
AbbvieGSKJohnson and JohnsonMSDNovartisPfizerSanofi
Regulatory assistance
• Allowing right of reference to confidential dossiers and product registration files to facilitate approval of generic combination products
• Covering the cost of regulatory filings• Providing regulatory expertise to explore optimal registration options for
compounds in development
GSKJohnson and JohnsonNovartisSanofi

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
FIN
DIN
GS
- FU
ND
ERS
PAGE92
FUNDING BY ORGANISATION
Neglected disease R&D funding remained highly concentrated in 2016, with the top 12 funders (including aggregate industry) providing 91% ($2,908m) of all global funding. The US NIH, Gates Foundation and aggregate industry collectively contributed almost three-quarters of total investment ($2,373m, 74%), up from 73% in 2015, and 72% in 2014.
Nine of the 11 individual organisations in the top 12 (i.e. excluding aggregate industry) increased their investment in 2016, compared to just five in 2015. The largest increase came from the largest global funder of neglected disease R&D, the US NIH (up $89m, 7.2%), following three consecutive years of diminishing funding. Unitaid, which gave a $28m grant to Partners In Health for the endTB project, entered the top 12 funders for the first time (up $24m, 150%). The Wellcome Trust also increased its funding in 2016 (up $17m, 21%), following a big drop the preceding year, with the increase due to large core funding disbursements to its international research programmes in Kenya, Thailand, Vietnam and Malawi. The next largest increase came from the Gates Foundation (up $12m, 2.3%), followed by the Indian ICMR (up $7.2m, 22%), UK MRC (up $6.2m, 17%), US DOD (up $5.5m, 7.5%), German BMBF (up $4.3m, 19%) and UK DFID (up $3.1m, 5.8%).
Only two of the top 12 funders in 2016 reduced their investment: the EC and USAID. Funding from the EC decreased significantly (down $49m, -39%), however this was largely due to a number of extraordinary payments made to EDCTP in 2015 that would otherwise have been made in 2014 and 2016. The smaller drop in USAID funding (down $9.8m, -12%) reflected the conclusion of a multi-year grant to IPM for the development of the dapivirine ring for HIV/AIDS.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016 Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding
recipients so may be incomplete
Table 36. Top neglected disease R&D funders 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
US NIH 1,238 1,258 1,455 1,407 1,371 1,478 1,298 1,259 1,245 1,335 42
Gates Foundation 530 707 641 528 525 520 538 532 530 542 17
Aggregate industry 214 339 373 413 391 377 384 462 469 497 16
Wellcome Trust 50 53 58 68 80 124 114 107 83 101 3.1
US DOD 86 79 108 76 85 83 97 98 73 79 2.5
EC 113 122 112 87 104 89 106 104 126 77 2.4
USAID 95 98 99 101 95 96 83 78 82 72 2.3
UK DFID 40 38 75 82 64 38 62 67 53 56 1.8
UK MRC 44 46 46 52 45 40 42 42 36 42 1.3
Indian ICMR 24 19 23 22 23 36 33 33 41 1.3
Unitaid 6.9 0.4 11 10 16 40 1.2
German BMBF 4.8 1.0 6.5 8.9 8.1 16 14 17 23 28 0.9
Subtotal of top 12^ 2,492 2,813 3,042 2,899 2,853 2,940 2,835 2,847 2,801 2,908 91
Total R&D funding 2,771 3,185 3,393 3,219 3,168 3,277 3,177 3,112 3,073 3,203 100
US$ (millio
ns)
Funder 2016 % of total

FIN
DIN
GS
- FU
ND
ERS
PAGE93
Top funders of neglected disease R&D over the last decade• In every year of the G-FINDER survey, the top three funders have been the US NIH (always by
far the largest contributor); the Gates Foundation and the aggregate pharmaceutical industry.
• The top 12 funders have consistently contributed over 85% of total funding each year.
• There has been very little variation in the top 12 funding organisations over the last decade, with eight individual organisations consistently making it into the top 12 funders list each year – the US NIH, Gates Foundation, EC, USAID, US DOD, Wellcome Trust, UK DFID and UK MRC – along with the aggregate pharmaceutical industry.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE94
FIN
DIN
GS
- FU
ND
ING
FLO
WS
** Although there is no single universally-accepted definition of PDPs, they are typically public health driven, not-for-profit intermediary organisations that use private sector management practices to drive product development in conjunction with external partners. Some PDPs focus on a single disease or product type, while others work across multiple diseases and products, but all share a common goal to develop products that are suitable for developing country use in areas of market failure. While their primary aim is the advancement of public health rather than commercial gain, PDPs generally use industry practices in their R&D activities, for instance portfolio management and industrial project management. Additionally, many PDPs conduct global advocacy to raise awareness of their targeted neglected diseases.
Organisations can invest in neglected disease R&D in two main ways: by funding their own in-house research (internal investment, also referred to as intramural or self-funding); or by giving grants to others (external investment). This external investment can either be given directly to researchers and developers, or it can be provided via PDPs**and other intermediaries. Some organisations invest only internally (for example, most pharmaceutical companies); others, such as the Wellcome Trust, only invest externally (i.e. they do not conduct R&D themselves). Other organisations, such as the US NIH and the Indian ICMR, use a mixed model, providing external grants to others in addition to funding their own research programmes.
FUNDING FLOWS
Figure 22. R&D funding flows 2016
A key point to note when analysing external investment flows is that different types of funders generally invest in different types of recipients. Science and technology (S&T) agencies, for example, mainly provide funding directly to researchers and developers (usually providing around three-quarters of their funding). Philanthropic and aid agency funders are the source of the vast majority of PDP funding (approximately 90%). In contrast, non-PDP intermediary organisations generally have a broad funding base, supported by both S&T and development agencies, as well as philanthropic funders.
As a result, changes in S&T agency funding are more likely to affect researchers and developers; changes in philanthropic or aid agency funding are more likely to affect PDPs; and non-PDP intermediary organisations are least vulnerable to changes from one donor funding stream.
$3,203mGlobal investment in
neglected disease R&D
$851mInternal R&D expenditure
$2,352mExternal investment
(grants given to others)
$1,851mDirect funding to
researchers and developers
$80mFunding to other intermediaries
$420mFunding to PDPs
Indirect funding to researchers and developers via PDPs and other intermediaries
73% 27%
18%
79%
3.4%

PAGE95
FIN
DIN
GS
- FU
ND
ING
FLO
WS
FUNDING FLOW TRENDS
Nearly three-quarters ($2,352m, 73%) of all funding for neglected disease R&D in 2016 was given externally in the form of grants (or contracts), with internal investments ($851m, 27%) making up the remainder. External funding increased in 2016 (up $95m, 4.4%) for the first time since 2012, driven by the US NIH. Self-funding was essentially flat (up $4.7m, 0.6%), with ongoing growth in industry investment (up $20m, 4.6%), particularly from SMEs, offset by a decrease in internal investment by government agencies (down $19m, -5.1%).
Almost four-fifths ($1,851m, 79%) of all external funding disbursed in 2016 was given directly to researchers and developers. In line with overall external investment, YOY funding to researchers and developers also increased for the first time since 2012 (up $147m, 9.1%), driven by both S&T agencies and philanthropic organisations. The increase in S&T agency funding to researchers and developers (up $80m, 6.4%) was almost entirely due to increased external grant funding from the US NIH (up $77m, 9.7%). Philanthropic funding given directly to researchers and developers increased by $62m (up 18%) due to increased funding from the Gates Foundation (up $43m, 16%) and the Wellcome Trust (up $19m, 24%).
As noted earlier, not all external grant funding for neglected disease R&D is given directly to researchers and developers. Approximately one-fifth ($501m, 21%) of all external funding disbursed in 2016 was given to fund managers (PDPs and other intermediaries), who then either pass this funding on to researchers and developers or invest it in their own internal R&D activities. This was a marked reduction in funding given to fund managers compared to 2015 (down $52m, -10%), with this drop affecting both PDPs and other intermediaries.
A total of $420m (18% of all external investment) was channelled through PDPs in 2016. This was the lowest level of PDP funding recorded in the history of the G-FINDER survey, although this should be interpreted with caution given the highly cyclical nature of funding to PDPs and other intermediaries, especially from the Gates Foundation. Funding to PDPs decreased by $29m in 2016 (-6.8%), as disbursements from the top three funders of PDPs – the Gates Foundation, USAID and the UK DFID – collectively decreased by $42m (-11%). The only notable increase in funding to PDPs came from the Dutch DGIS (up $18m, 447%), which started a new PDP funding round, with funding from all other sources either down or flat.
Other intermediaries received $80m (3.4% of all external investment) in 2016, a decrease of $23m (-25%). This drop was the result of sharply lower funding from the EC to EDCTP (down $32m, -80%) – reflecting a number of extraordinary payments from the EC to the EDCTP in 2015 that would otherwise have been made in 2014 and 2016 – which more than offset slightly increased member state funding to EDCTP, and smaller increases in funding to the International Union Against Tuberculosis and Lung Disease (The Union) and the GHIT Fund.
A more in-depth analysis of funding for PDPs and other intermediaries is presented from page 97 onwards.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE96
FIN
DIN
GS
- FU
ND
ING
FLO
WS Figure 23. R&D funding flow trends 2007-2016
FUNDING FLOWS BY R&D STAGE
Nearly half of all funding for neglected disease R&D in 2016 was allocated to basic and early stage research (48%), followed by clinical or field development and post registration studies (32%), with the remaining funding comprising of core funding (4.2%), platform technologies (1.6%) and other R&D (14%).
Exactly half (50%) of all self-funding in 2016 was allocated to clinical or field development and post registration studies, with 37% allocated to basic and early stage research. The remaining 14% was not allocated to a specific disease or product area. However, this overall pattern obscures the very focus of industry investments compared to non-industry self-funding. Industry investment accounted for 57% of all self-funding; two-thirds (66%) of this industry investment was for clinical or field development and post registration studies, and less than one-third (28%) for basic and early stage research (all of which was for discovery and pre-clinical R&D, rather than basic research). In contrast, non-industry self-funding – primarily from government S&T agencies, and in particular the US NIH – was focused more on basic and early stage research (49%) than on clinical or field development and post registration studies (27%). The true extent of the upstream focus of non-industry self-funding is likely even higher, given that much of the remaining 24% of funding that was not allocated to a specific product or R&D stage is in fact highly likely to be for basic research.
Reflecting the fact that this funding stream is also dominated by S&T agencies (and especially the US NIH), almost two-thirds (62%) of all funding given directly to researchers and developers went to basic and early stage research, with just 22% for clinical or field development and post registration studies; the remaining 16% was not allocated to a specific product or R&D stage.
g�External investment going to intermediaries
g�External investment going to PDPs
gExternal investment going to researchers & developers
gTotal internal investment
External investment going to researchers & developers
External investment going to PDPs
External investment going to intermediaries
Total internal investment
US
$ (m
illio
ns)
0
500
1,000
1,500
2,000
2,500
3,000
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016

PAGE97
FIN
DIN
GS
- FU
ND
ING
FLO
WS
The very different pattern of funding given to PDPs reflects their product-development focus. More than two-fifths (42%) of all funding to PDPs was for clinical or field development and post registration studies, more than double the amount (19%) that was for basic and early stage research (essentially all of which was for discovery and pre-clinical R&D, rather than basic research). The remaining 38% of funding given to PDPs was not allocated to a specific R&D stage, but instead used to support the development of a portfolio of products from discovery through to post registration.
The small number of other intermediaries and the specific focus of each organisation results in different patterns of funding by R&D stage. For example, almost all (96%) of TB funding that went to other intermediaries was for The Union, all of which was allocated to clinical development and post registration studies for drugs. On the other hand, 88% of HIV/AIDS funding to other intermediaries went to the Aaron Diamond AIDS Research Center, with the vast majority (93%) of this allocated to basic and early stage research for vaccines. The EDCTP and the GHIT Fund received 88% of all non-disease-specific funding for other intermediaries, none of which was product- or R&D stage-specific.
FUNDING FOR PRODUCT DEVELOPMENT PARTNERSHIPS
PDPs received $420m in 2016, accounting for 13% of all neglected disease R&D funding and 18% of all external investment. This was the lowest level of PDP funding recorded in the history of the G-FINDER survey, corresponding to the lowest funding from the Gates Foundation to PDPs recorded by G-FINDER. Annual changes in funding to PDPs should be interpreted with caution given the highly cyclical nature of this funding, especially from the Gates Foundation.
It is important to note that the central role of PDPs is somewhat obscured by the ‘NIH factor’. The US NIH was by far the largest funder of neglected disease R&D, but allocated only a small portion of its funding to PDPs ($8.8m or 0.7% of its total investment). If the US NIH is excluded, the role of PDPs in product development for neglected diseases becomes clearer, with PDPs collectively managing 34% of all non-NIH external grant funding for neglected disease R&D.
Although the cyclical pattern of funding to PDPs from philanthropic organisations and government aid agencies – the main funders of PDPs – means that their identities change, the three highest funded PDPs in any given year consistently account for between 40% and 50% of annual PDP funding. In 2016, these three PDPs were IAVI, MMV and PATH, who collectively received just under half ($196m, 47%) of all PDP funding.
There were some large shifts in funding to PDPs in 2016, including decreases to the TB Alliance (down $32m, -49%), PATH (down $27m, -37%) and MMV (down $14m, -20%); and increases to IAVI (up $22m, 34%) and DNDi (up $15m, 54%) – with these changes mostly attributable to cyclical funding from the Gates Foundation. The increased funding to DNDi was also due to the start of a new PDP funding round for the Dutch DGIS. The conclusion of Phase III trials of the dapivirine ring in 2016 led to a $5.8m (-22%) reduction in funding to IPM, with USAID’s contribution dropping by $10m (-77%).
Most funding to PDPs in 2016 ($315m, 75%) was invested in three diseases that received the most funding overall: of this amount, $121m was for HIV/AIDS, $113m was for malaria, and $81m was for TB.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE98
FIN
DIN
GS
- FU
ND
ING
FLO
WS
A The totals attributed to TBVI in 2014-2016 do not include funds from the EC that were paid directly to researchers under the auspices of TBVI’s PDP activities. The totals only include EC’s financial support for TBVI’s services, as well as funding from other organisationsB TDR’s mission extends beyond product development, but it operated as a de facto PDP from the 1970s until 2012, when it decided to focus on implementation research and research capacity strengthening. Funds received in 2014-2016 are related to the pooled fund demonstration projects C As of 2013, OWH funding is included under PATH - No reported funding
Table 37. Funds received by PDPs 2007-2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
IAVI 85 93 75 70 64 63 61 41 66 88 21
MMV 85 50 45 73 76 52 67 74 77 60 14
PATH 45 130 145 77 102 87 84 122 76 47 11
DNDi 28 22 32 33 36 30 33 53 31 47 11
TB Alliance 44 38 39 52 38 46 52 56 71 38 8.9
IVCC - 11 16 17 <0.1 11 22 9.9 29 33 7.7
Aeras 45 74 59 43 44 40 41 55 32 31 7.3
FIND 26 35 23 27 23 22 23 24 15 22 5.3
IPM 46 65 34 32 14 23 30 26 26 20 4.8
CONRAD 18 17 24 19 26 32 27 18 3.9 9.2 2.2
IDRI 9.5 17 19 13 24 11 6.1 14 6.3 8.2 2.0
IVI 15 2.3 13 9.9 5.7 8.4 9.8 6.5 7.1 6.5 1.5
Sabin Vaccine Institute 8.9 17 10 4.3 8.9 6.5 6.6 5.5 3.1 5.0 1.2
EVI 7.1 4.0 3.5 4.8 7.1 2.0 6.0 2.8 3.4 1.8 0.4
FHI360 15 20 19 20 12 6.0 4.6 0.2 - 1.3 0.3
TBVIA - - 0.1 3.8 3.5 4.9 5.3 1.3 1.5 1.3 0.3
WHO/TDRB 34 38 35 28 31 - - 2.2 2.5 1.0 0.2
OWHC 32 33 17 23 11 7.3 - - - - -
Total funding to PDPs 544 667 609 550 526 452 478 512 452 420 100
US$ (millio
ns)
PDPs2016 % of to
tal

PAGE99
FIN
DIN
GS
- FU
ND
ING
FLO
WS
FUNDERS OF PDPs
Philanthropic organisations provided over half of all funding to PDPs ($239m, 57%). Almost all remaining funding came from HIC governments ($164m, 39%), mostly via their aid agencies ($142m, 87% of HIC funding to PDPs).
Funding from almost all the top PDP funders was either lower or flat in 2016, with an overall decrease of $29m (-6.8%). The largest decrease came from the Gates Foundation (down $30m, -12%). Although it remained the largest funder of PDPs, with a contribution of $229m (54% of all funding to PDPs), this represents the lowest investment in PDPs by the Gates Foundation recorded in the history of the G-FINDER survey. Funding from USAID to PDPs also declined (down $12m, -21%), reflecting reduced funding to IPM (down $10m, -77%) associated with the conclusion of its dapivirine ring Phase III clinical trials. The largest increase was the result of the Dutch DGIS opening a new funding round for PDPs (up $18m, 447%). Three of the top 12 funders of PDPs – Dutch DGIS, Australian Department of Foreign Affairs and Trade (DFAT) and Irish Aid – once again allocated 100% of their funding for R&D to PDPs.
Public sector multilateral organisations gave $14m to PDPs in 2016 (3.4% of all PDP funding). Almost all multilateral funding came from Unitaid ($12m, 84% of all multilateral PDP funding), though Unitaid’s funding to PDPs decreased (down $3.9m, -25%) after a peak in 2015.
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 38. Top funders of PDPs 2016
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Gates Foundation 273 399 334 297 266 252 244 301 260 229 42 54
UK DFID 28 24 69 82 64 38 62 67 50 51 90 12
USAID 79 79 81 80 78 77 64 58 59 47 65 11
Dutch DGIS 29 18 18 15 19 11 21 17 4.1 22 100 5.3
Unitaid 6.9 0.4 8.6 10 16 12 30 2.8
US NIH 4.9 3.9 8.8 3.0 21 8.2 12 9.5 4.7 8.8 0.7 2.1
German BMBF - - 1.2 5.7 4.8 6.6 8.2 7.6 27 1.8
Australian DFAT 8.0 - 7.6 7.5 7.4 100 1.8
Swiss SDC 2.3 2.3 2.5 4.6 3.6 3.3 4.4 6.6 7.8 5.7 97 1.4
Irish Aid 22 6.3 4.8 6.0 5.8 5.7 7.8 2.2 5.6 4.8 100 1.1
MSF 6.6 6.7 4.2 4.3 4.6 5.4 5.5 4.4 4.4 4.4 43 1.1
Aggregate industry 1.1 6.6 2.1 2.2 1.7 1.7 1.5 1.8 1.4 3.2 0.7 0.8
Subtotal of top 12 funders of PDPs^ 498 611 561 518 486 423 445 494 430 403
Total PDP funding 544 667 609 550 526 452 478 512 452 420
% of total PDP funding (top 12) 92 92 92 94 93 94 93 97 95 96
US$ (millio
ns)
Funder2016 % of org’s
funds given to PDPs
2016 % of total
PDP funding

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE100
FIN
DIN
GS
- FU
ND
ING
FLO
WS
FUNDING FOR OTHER INTERMEDIARIES
‘Other’ intermediary organisations (i.e. those that are not PDPs) also aim to accelerate neglected disease product development, but do so without managing a product portfolio of their own. Instead, they generally act as coordinating agencies, receiving funding from multiple sources and passing this on to researchers and developers (either directly or via PDPs). They may also perform research themselves (often operational research or research into existing treatment regimens) or be involved in clinical trials of novel products being developed by other organisations.
Non-PDP intermediaries collectively received $80m in 2016, representing 2.5% of all neglected disease funding, and 3.4% of all external funding. The organisations that received the most funding were the GHIT Fund ($32m, 39%), EDCTP ($23m, 29%), The Union ($12m, 15%) and the Barcelona Institute for Global Health (ISGlobal, $9.2m, 11%).
The $23m decrease in funding to other intermediaries (-25%) was a reflection of a number of extraordinary payments from the EC to the EDCTP in 2015 that would otherwise have been made in 2014 and 2016, rather than a structural shift away from funding for these organisations. YOY funding for EDCTP decreased (down $26m, -53%), while funding for most other non-PDP intermediaries increased – led by The Union (up $3.2m, 37%) and the GHIT Fund (up $1.7m, 5.9%).
Most funding for intermediaries ($63m, 78%) was not earmarked for a specific disease by the funder. Of the $18m (22%) of funding given to non-PDP intermediaries that was disease-specific, $12m was for TB, $3.2m was for HIV/AIDS, $1.9m was for malaria and $0.4m was for kinetoplastid diseases.
A decade of neglected disease R&D funding for PDPs• PDPs are highly dependent on the Gates Foundation and government aid agencies, which
have collectively provided almost 90% of all PDP funding over the last decade. The Gates Foundation alone has accounted for more than half (55%) of all funding for PDPs over this period.
• Global funding of PDPs and Gates Foundation funding of PDPs both fell to record lows in 2016. Although a number of the year-to-year drops can be explained by funding cycles, total funding to PDPs in 2016 is down a quarter of a billion dollars ($246m, -37%) from its 2008 peak.
• PATH has been the largest recipient of all PDP funding over the last decade, and has been the top funded PDP in seven of the last ten years, with the others to hold this spot being IAVI (twice) and MMV.

PAGE101
FIN
DIN
GS
- FU
ND
ING
FLO
WS
FUNDERS OF OTHER INTERMEDIARIES
Non-PDP intermediary organisations receive funding from a relatively diverse range of sources, with less reliance on a single ‘type’ of funding organisation than either PDPs or researchers and developers. The majority of funding for other intermediaries comes from government agencies, with S&T agencies usually providing approximately half of all funding to other intermediaries, and aid agencies around one-fifth.
In 2016, funding for other intermediaries was uncharacteristic, with a marked decrease in the share of funding from S&T agencies (to 22% of all funding for other intermediaries) and an increase in funding from the Japanese government (up to 23% of all funding for other intermediaries). However, these irregularities were due to the EC’s extraordinary payments to the EDCTP in 2015 and an increase in Japanese government investments in the GHIT Fund.
The EC is usually the largest funder of non-PDP intermediaries, due to its support for EDCTP. The large drop in EC funding to EDCTP in 2016 (down $32m, -79%) meant that it fell to third place in the list of top funders of intermediaries, behind the Japanese government, which increased its investment in the GHIT Fund (up $5.5m, 50%), and USAID, which increased its funding to The Union (up $3.2m, 37%). The drop in EC funding to EDCTP (which was due to extraordinary payments made in 2015), meant that European Union member state contributions to EDCTP in 2016 exceeded the EC’s for only the second time. These included the UK DFID ($5.4m), the Swedish International Development Agency (SIDA, $4.4m), the UK MRC ($2.7m), the German BMBF ($2.3m), the Portuguese Foundation for Science and Technology ($0.2m) and the Dutch Organisation for Scientific Research ($0.2m).
Funding to other intermediaries is geographically driven. Of the top 12 funders, essentially all funding to intermediaries from the EC, the UK DFID, the Swedish SIDA and the German BMBF went to the EDCTP; Japanese government and industry investment went to the GHIT Fund; and Spanish public sector organisations funded ISGlobal. Few funders – beyond the EC, the US NIH and the Gates Foundation – support more than one non-PDP intermediary organisation.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
PAGE102
FIN
DIN
GS
- FU
ND
ING
FLO
WS
^ Subtotals for 2007-2015 top 12 reflect the top funders for those respective years, not the top 12 for 2016- No reported funding
Funding organisation did not participate in the survey for this year. Any contributions listed are based on data reported by funding recipients so may be incomplete
Table 39. Top funders of intermediaries 2016
A decade of neglected disease R&D funding for other intermediaries• The EC has been the largest contributor of funding to other intermediaries for neglected
disease R&D. It has provided 38% of all funding to other intermediaries over the last decade, primarily to EDCTP.
• The US government has been the next largest funder (providing 14% of all funding to other intermediaries over the last decade), followed by the Gates Foundation (12%), both of whom have supported a wide range of recipient organisations. The Japanese government has also become a notable funder, averaging $12m per year to the GHIT Fund since its creation in 2013.
• The two largest recipients of funding of all the other intermediaries are the EDCTP (which received 48% of all funding to other intermediaries over the last decade) and the GHIT Fund (17% of all funding, despite only having been established in 2013).
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Japanese government 10 10 11 17 100 21
USAID <0.1 4.3 5.4 5.9 5.8 5.6 5.1 9.4 8.7 12 16 15
EC 39 36 18 2.0 23 24 24 22 41 8.7 11 11
Aggregate industry - 1.4 3.2 - - - 3.8 8.3 5.5 7.7 1.6 9.6
Gates Foundation 11 8.4 14 6.0 5.3 4.2 6.9 7.6 7.6 7.5 1.4 9.3
UK DFID 12 13 6.1 - - - - - 3.1 5.4 9.7 6.8
Swedish SIDA 4.0 1.9 2.1 1.9 <0.1 - 0.6 - 3.0 4.4 79 5.5
Fundació La Caixa 1.0 1.0 1.0 1.8 3.3 100 4.1
Catalan Department of Health
- 1.0 0.7 3.2 100 3.9
US NIH - 1.1 3.5 3.2 1.3 2.1 1.8 3.6 3.3 2.8 0.2 3.5
UK MRC - - - 4.4 - <0.1 - - 2.7 2.7 6.4 3.4
German BMBF - 1.1 0.2 <0.1 0.1 0.1 0.1 2.7 9.8 3.4
Subtotal of top 12 funders of intermediaries^
70 76 55 31 41 53 56 64 97 77
Total funding to intermediaries 70 76 55 32 41 54 57 64 98 80
% of total intermediary funding (top 12)
100 100 99 97 100 98 99 100 99 96
US$ (millio
ns)
Funder2016 % of org’s funds
given to intermediaries
2016 % of total
intermediary funding

DIS
CU
SSIO
N
PAGE103
Global funding for neglected disease R&D increased for the first time since 2012, driven by an increase in funding from the US government
Global funding for neglected disease R&D increased (up $99m, 3.4%) to $3,203m in 2016. This was the first increase in global funding since 2012, and came on the back of an increase in neglected disease R&D investment by the US government (up $78m, 5.5%), also for the first time since 2012. This in turn was due to increased investment in neglected disease R&D by the US NIH (up $89m, 7.2%) – again, for the first time since 2012.
The US government was not alone in increasing funding for neglected disease R&D in 2016. The philanthropic sector (up $28m, 4.4%) and the pharmaceutical industry (up $22m, 5.3%) both increased their investment, with the latter driven by increased SME investment. There were also notable increases from the Dutch and UK governments, as a well as from a host of governments outside of North America and Europe – Brazil, Japan and India in particular – which helped to offset reduced funding from the EC and a number of other European governments.
The US government is just one funder among many making critical contributions to neglected disease R&D. But as the largest funder of all, changes in total global investment are closely aligned to changes in US government funding: every increase or decrease in US government investment in neglected disease R&D over the last decade has been accompanied by a corresponding change in total global funding.
DISCUSSION
Ann
ual c
hang
e, U
S$
(mill
ions
)
-300
-200
-100
100
200
300
400
2008 2009 2010 2011 2012 2013 2014 2015 2016
Global funding
US government funding
Figure 24. The US government’s influence on changes in annual funding for neglected disease R&D

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
DIS
CU
SSIO
N
PAGE104
An overreliance on US government funding is defining the shape of R&D for neglected diseases
In 2016, the US government was the source of 47% of global funding for neglected disease R&D, and 73% of all public sector funding. Its investment of $1,490m was triple the combined investment of the rest of the world’s governments, and fifteen times larger than that of the next biggest government funder (the UK, with $101m).
The fact that the US government contributes such a large share of global funding means that not only are changes in US government funding the main driver of changes in total global funding for neglected disease R&D, but that the nature of neglected disease R&D is being defined by the focus of US government funding.
US government funding for neglected disease R&D is overwhelmingly focused on HIV/AIDS, TB and malaria, which received 82% of all US government funding for neglected disease R&D in 2016 (and 81% of its funding over the last decade). Despite the rest of the world (across all funding sectors) only directing 60% of their collective investment to these three diseases, they account for a full 70% of global funding.
US government funding for neglected disease R&D is also overwhelmingly focused on basic and early stage research. Two-thirds (67%) of all US government funding for neglected disease R&D in 2016 was for basic and early stage research, compared to just 28% for clinical or field development and post registration studies, with the remaining 5% not allocated to a specific R&D stage. But this headline figure doesn’t quite tell the whole story, due to the US government’s massive investment in clinical trials for HIV/AIDS vaccines, which totalled a quarter of a billion dollars ($245m) in 2016.
If US government funding for HIV vaccine clinical trials is excluded, 80% of all US government funding for neglected disease R&D – and 70% of all funding from HIC governments – was for basic and early stage research, compared to just 14% for clinical or field development and post registration studies.
The sustained growth in industry investment in neglected disease R&D – lately driven by SMEs – continues to be a good news story
After a brief dip in 2011, industry investment in neglected disease R&D has increased in every one of the last five years, and reached new record highs in each of the last three years. In 2016, total industry investment was $497m, accounting for 16% of all global funding for neglected disease R&D. Since 2008, reported industry investment in neglected disease R&D has increased by nearly 50%, while funding from both the public and philanthropic sectors has fallen over the same period.
The vast bulk of industry investment (79% in 2016) comes from MNCs, who have also been responsible for much of the growth in industry investment in neglected disease R&D over the last decade – driven by increased activity in malaria and HIV/AIDS especially. Since 2014 however, MNC investment has essentially plateaued, with annual increases of less than 1% in both 2015 and 2016.
Increased investment by SMEs since 2012, particularly from those in India, has helped to sustain the growth of overall industry investment. SME investment in neglected disease R&D tripled between 2012 and 2016 (from $35m to $106m); this was driven by Indian SMEs, whose investment increased from $9.3m to $70m over the same period, and now exceeds that of the Indian government. The $22m increase in industry investment in 2016 came entirely from SMEs (up $23m, 30%), who also provided their highest ever recorded investment, and the largest share of total industry investment (21%) since 2008. Importantly, much of this investment growth has also been in new areas: while 76% of MNC investment in 2016 was for malaria, TB and HIV/AIDS, none of these three diseases was in the top three diseases invested in by SMEs. Instead, 67% of SME investment in 2016 was for bacterial pneumonia & meningitis, Salmonella infections and diarrhoeal diseases.

DIS
CU
SSIO
N
PAGE105
In addition to SMEs, a number of other funders have been making a small but growing contribution in areas of need
As well as SMEs, a number of other traditionally smaller funders have been noticeably increasing their investment in neglected disease R&D: key global health initiatives (Unitaid, MSF and Gavi, the Vaccine Alliance), the Japanese government, and governments in LMICs.
Unitaid, MSF and Gavi have each expanded their focus to include support for neglected disease R&D, particularly for clinical or field development and post registration studies. Unitaid has expanded its focus from affordability, procurement and pricing to also include support for drug and diagnostic R&D for TB, malaria and HIV/AIDS. The first reported R&D funding from Unitaid was to FIND ($6.9m in 2009), and the organisation has increased funding in four of the last five years. Unitaid invested $40m in neglected disease R&D in 2016, providing more funding than all but six governments globally. This included $28m for clinical development and post registration studies to the endTB partnership, which is focused on the development of new treatments for MDR-TB.
MSF supports R&D across multiple diseases and product areas. It helped found the product development partnership DNDi, and support to DNDi represents the vast majority ($51m, 87%) of MSF’s funding for neglected disease R&D over the last decade. But in recent years MSF has also become increasingly involved in direct collaborations with other R&D organisations – such as the recent Phase III trial of Serum Institute of India’s BRV-PV rotavirus vaccine candidate in Niger – with non-DNDi funding accounting for over half of MSF’s $10m investment in neglected disease R&D in 2016.
Gavi has made a similar adjustment to Unitaid, expanding its focus from vaccine financing and supply to include support for clinical development and post registration studies of new vaccines for bacterial pneumonia & meningitis, diarrhoeal diseases and Salmonella infections. Gavi was the only one of the three global health initiatives to reduce its funding in 2016 (providing $5.8m, down from a peak of $19m in 2013), but it has the second highest contribution of the three over the last decade, with $76m.
The Japanese government – along with Japanese pharmaceutical companies – is increasingly investing in neglected disease product development following the establishment of the GHIT Fund in 2013. Between 2007 and 2012, the Japanese government invested an average of $5.5m per year in neglected disease R&D; since then, its annual investment has never been lower than $10m, and reached a record high of $17m in 2016. And, reflecting the focus of the GHIT Fund, this increased investment has been directed towards product development (both early and late stage), rather than basic research.
Finally, funding from LMIC governments increased strongly in 2016, to $84m. More than 90% of this funding ($78m, 93%) came from the three IDCs (India, Brazil, and South Africa) – all of whom increased their investment in 2016 – with India becoming the fourth largest government funder of neglected disease R&D, ahead of both France and Germany. And unlike HIC governments, which directed nearly half of all their funding for neglected disease R&D in 2016 to HIV/AIDS, LMIC governments invested more in each of TB, malaria, kinetoplastids, diarrhoeal diseases, dengue and leprosy in 2016 than they did in HIV/AIDS.

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
DIS
CU
SSIO
N
PAGE106
Conclusion
The US government’s contribution to neglected disease R&D funding is unparalleled. But an overreliance on US government funding is reflected in the heavy concentration of global funding on HIV/AIDS, malaria and TB, and the overwhelming focus of HIC government funding on basic and early stage research. The growth of non-traditional funders is promising, but their collective contribution is still just a fraction of overall global funding. And while Gates Foundation investment in product development has consistently been relied on to balance the public sector focus on basic research – it has provided 55% of all funding to PDPs and 47% of all funding for platform technologies over the last decade – this is again a reflection of overreliance on a single funder. The world can ill afford to keep relying on the US government and the Gates Foundation to provide two-thirds of all global funding for neglected disease R&D over the next ten years, as they have done for the last decade.

AN
NEX
ES
PAGE107
ANNEXE 1
Advisory Committee members & additional experts
ADVISORY COMMITTEE MEMBER ORGANISATION TITLE
Dr Ripley Ballou GlaxoSmithKline Biologicals Vice President and Head, Global Vaccines US R&D Center
Dr Graeme Bilbe Drugs for Neglected Diseases initiative (DNDi)
Research & Development Director
Dr François Bompart Sanofi Vice President, Access to Medicines
Dr Wanderley de Souza Financiadora de Estudos e Projetos (FINEP)
Former President
Professor Alan Fenwick Imperial College London Professor of Tropical Parasitology
Dr Arnaud Fontanet Institut Pasteur Head of the Emerging Diseases Epidemiology Unit
Dr Sue Kinn UK Department for International Development (DFID)
Team Leader and Research Manager
Dr Line Matthiessen European Commission (EC) Head of Infectious Diseases and Public Health Unit, Directorate-General for Research and Innovation
Dr Carl Mendel TB Alliance Senior Vice President, Research and Development
Dr Firdausi Qadri International Centre for Diarrhoeal Disease and Research (icddr,b)
Emeritus Scientist and Acting Senior Director, Infectious Diseases Division
Dr John Reeder World Health Organization: Special Programme for Research and Training in Tropical Diseases (WHO/TDR)
Director
Professor Nelson Sewankambo Makerere University College of Health Sciences
Principal (Head)
Dr Soumya Swaminathan Indian Council of Medical Research (ICMR) Director General
Wendy Taylor United States Agency for International Development (USAID)
Former Director, Center for Accelerating Innovation and Impact
Dr Tim Wells Medicines for Malaria Venture (MMV) Chief Scientific Officer
Dr Judith Mueller Institut Pasteur Research affiliate, Institut Pasteur and Professor in epidemiology at EHESP French School of Public Health
Dr Rashmi Arora Indian Council of Medical Research (ICMR)
Senior Deputy Director General and Head, Division of Epidemiology and Communicable Diseases
ADDITIONAL EXPERT ORGANISATION TITLE

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
AN
NEX
ES
PAGE108
ANNEXE 2
Survey respondent listORGANISATION NAME
• AbbVie
• Aeras
• Aidsfonds*
• American Leprosy Missions (ALM)
• amfAR, The Foundation for AIDS Research*
• Apopo
• Argentinian Ministry of Science, Technology and
Productive Innovation (MINCYT)
• Argentinian National Council for Scientific and
Technical Research (CONICET)
• Arisan Therapeutics
• Atomo Diagnostics
• Austrade
• Australian Commonwealth Scientific and Industrial
Research Organisation (CSIRO)
• Australian Department of Foreign Affairs and Trade
(DFAT)
• Australian Department of Industry, Innovation and
Science (DIIS)
• Australian National Health and Medical Research
Council (NHMRC)
• Australian National Heart Foundation
• Australian Research Council (ARC)
• Austrian Leprosy Relief Association (ALRA)
• Barcelona Institute for Global Health (ISGlobal)
including Clinic Foundation for Biomedical Research
(FCRB), Barcelona Centre for International Health
Research (CRESIB), and Centre for Research in
Environmental Epidemiology (CREAL)
• BASF
• Baylor College of Medicine
• Becton, Dickinson and Company (BD)
• Belgian Ministry of Foreign Affairs, Foreign Trade and
Development Cooperation (DGDC)
• Bernhard Nocht Institute for Tropical Medicine (BNI)
• Bill & Melinda Gates Foundation
• Biological E
• Biotechnology Industry Research Assistance Council
(BIRAC)
• Brazilian Development Bank (BNDES)
• Brazilian Innovation Agency (FINEP)
• Brazilian Ministry of Health: Department of Science
and Technology (DECIT)
• Brazilian Ministry of Health: National STD and AIDS
Programme
• Brazilian Research Support Foundation of the State
of Bahia (FAPESB)
• Brazilian Research Support Foundation of the State
of Minas Gerais (FAPEMIG)
• Brazilian Support Foundation for Research and
Innovation in the State of Santa Catarina (FAPESC)
• Brazilian Support Foundation for Research in the
State of São Paolo (FAPESP)
• Burnet Institute
• Cairo University
• Campbell Foundation*
• Canadian Institutes of Health Research (CIHR)
• Carlos III Health Institute
• Cebu Leprosy and Tuberculosis Research
Foundation (CLTRF)
• Cepheid
• Chilean National Commission for Scientific and
Technological Research (CONICYT)
• Chilean National Fund for Scientific and
Technological Development (FONDECYT)
• Coalition for Epidemic Preparedness Innovations
(CEPI)
• Colombian Department for Science, Technology and
Innovation (Colciencias)
• CONRAD*
• Daiichi-Sankyo
• Damien Foundation (DFB)
• Danish Ministry of Foreign Affairs and the Danish
International Development Agency (DANIDA)
* Denotes organisations where funding data was only received via the HIV Vaccines and Microbicides Resource Tracking Working Group

AN
NEX
ES
PAGE109
* Denotes organisations where funding data was only received via the HIV Vaccines and Microbicides Resource Tracking Working Group# Denotes organisations where funding data was taken from publicly available sources
• DesignMedix
• Drugs for Neglected Diseases initiative (DNDi)
• Dutch Ministry of Foreign Affairs - Directorate General
of Development Cooperation (DGIS)
• Dutch Organisation for Scientific Research (NWO)
• effect:hope (The Leprosy Mission Canada)
• Eisai
• European & Developing Countries Clinical Trials
Partnership (EDCTP)
• European Commission including the Directorate
General for Research and Innovation
• European Vaccine Initiative (EVI)
• FAIRMED
• FHI 360
• Finnish Funding Agency for Technology and
Innovation (TEKES)
• Fio
• FK Biotec
• Fontilles
• Foundation for Innovative New Diagnostics (FIND)
• French National Agency for Research on AIDS and
Viral Hepatitis (ANRS)
• French National Institute of Health and Medical
Research (Inserm)
• French National Research Agency (ANR)
• French Research Institute for Development (IRD)
• Gavi, The Vaccine Alliance
• GeoVax
• German Federal Ministry for Economic Cooperation
and Development (BMZ)
• German Federal Ministry of Education and Research
(BMBF)
• German Federal Ministry of Health (BMG)
• German Leprosy and TB Relief Association (DAHW)
• German Research Foundation (DFG)
• GlaxoSmithKline (GSK)
• Global Affairs Canada
• Global Health Innovative Technology Fund (GHIT
Fund)
• GSK Bio
• Hawaii Biotech
• Health Research Council of New Zealand (HRC)
• Hebron
• Indian Council of Medical Research (ICMR)
• Indian Council of Scientific and Industrial Research
(CSIR)
• Indian Department of Biotechnology, Ministry of
Science and Technology (DBT)
• Indian Department of Health Research, Union
Ministry of Health and Family Welfare
• Indian Department of Science and Technology (DST)
• Innovative Medicines Initiative (IMI)#
• Innovative Vector Control Consortium (IVCC)
• Inovio
• InPheno
• Institut Pasteur
• Institute of Tropical Medicine Antwerp (ITM)
• Integral Molecular
• International AIDS Vaccine Initiative (IAVI)
• International Centre for Genetic Engineering and
Biotechnology (ICGEB)
• International Partnership for Microbicides (IPM)*
• International Union Against Tuberculosis and Lung
Disease
• International Vaccine Institute (IVI)
• Irish Aid
• Japanese National Institute of Infectious Diseases
(NIID)*
• Jarvis Laboratory
• Johnson & Johnson
• KNCV Tuberculosis Foundation
• Korean Institute of Tuberculosis
• Leadiant Biosciences (previously Sigma-Tau)
• Lepra India - Blue Peter Public Health & Research

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
AN
NEX
ES
PAGE110
Centre (BPHRC)
• Leprosy Relief Canada (SLC)
• Leprosy Research Initiative (LRI)
• Lilly
• Liverpool School of Tropical Medicine (LSTM)
• Mapp Biopharmaceutical
• Max Planck Institute for Infection Biology (MPIIB)
• Médecins Sans Frontières (MSF)
• Medicines for Malaria Venture (MMV)
• Meningitis Research Foundation (MRF)
• Mérieux Foundation
• Mexican National Council of Science and Technology
(CONACYT)
• Mexican National Institute of Public Health (INSP)
• MSD / Merck
• Mymetics
• Netherlands Leprosy Relief (NLR)
• Noguchi Memorial Institute for Medical Research
• Norwegian Institute of Public Health
• Novartis
• Ontario HIV Treatment Network*
• Osel*
• Otsuka
• Ouro Fino
• Partners in Health
• PATH including the Malaria Vaccine Initiative (MVI)
• Pfizer
• Pharmaceutical Laboratory of the State of
Pernambuco (LAFEPE)
• ProtoPharma
• Public Health Agency of Canada (PHAC)*
• Public Health England (PHE)
• Research Centre Borstel
• Research Council of Norway
• Royal Norwegian Ministry of Foreign Affairs and the
Norwegian Agency for Development Cooperation
(NORAD)
• Royal Society of New Zealand (RSNZ)
• Sabin Vaccine Institute
• San Raffaele Scientific Institute (IRCCS)*
• Sanofi
• Science Foundation Ireland (SFI)
• Serum Institute of India
• Shionogi
• Sidaction*
• South Africa Medical Research Council (MRC)
• South African Department of Science and
Technology (DST)
• South African Technology Innovation Agency (TIA)
• Statens Serum Institute (SSI)
• Sumagen*
• Swedish International Development Agency (SIDA)
• Swedish Research Council
• Swiss Agency for Development and Cooperation
(SDC)
• Swiss National Science Foundation (SNSF)
• Swiss State Secretariat for Education, Research and
Innovation (SERI)
• Swiss Tropical & Public Health Institute (Swiss TPH)
• Syngenta
• Synstar Japan
• Sysmex
• Takeda Pharmaceutical Company
• TB Alliance
• Thai Government Pharmaceutical Organisation (GPO)
• Thai Red Cross AIDS Research Center (TRC-ARC)*
• Thailand National Science and Technology
Development Agency (NSTDA)
• The Leprosy Mission International (TLMI)
• The Wellcome Trust
• TuBerculosis Vaccine Initiative (TBVI)
• Turing Foundation
• UBS Optimus Foundation
• UK Department for International Development (DFID)
* Denotes organisations where funding data was only received via the HIV Vaccines and Microbicides Resource Tracking Working Group

AN
NEX
ES
PAGE111
• UK Medical Research Council (MRC)
• University of Georgia
• University of Lagos
• University of Nebraska Medical Center
• University of Pittsburgh
• US Agency for International Development (USAID)
• US Centers for Disease Control and Prevention (CDC)
including the CDC Foundation
• US Department of Defense (DOD) including Defense
Advanced Research Projects Agency (DARPA),
US Army Medical Research Institute of Infectious
Diseases (USAMRIID), the US Naval Medical
Research Center (NMRC), Defense Threat Reduction
Agency (DTRA) and the Walter Reed Army Institute of
Research (WRAIR)
• US National Institutes of Health (NIH) including the
US National Institute of Allergy and Infectious Disease
(NIAID)
• Vestergaard
• World Bank
• World Health Organization: Special Programme for
Research and Training in Tropical Diseases (WHO/
TDR)
* Denotes organisations where funding data was only received via the HIV Vaccines and Microbicides Resource Tracking Working Group

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
AN
NEX
ES
PAGE112
1. World Bank. Data: country and lending groups [Internet]. [cited 2017 Nov 18]. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
2. Institute for Health Metrics and Evaluation (IHME). Global Health Data Exchange (GHDx) [Internet]. GBD Results Tool. 2017 [cited 2017 Jun 21]. Available from: http://www.healthdata.org/institute-health-metrics-and-evaluation
3. World Health Organization (WHO). Global Health Estimates 2015: deaths by cause, age, sex, by country and by region, 2000-2015 [Internet]. Geneva, Switzerland: World Health Organization; 2016 [cited 2017 Jun 14]. Available from: http://www.who.int/healthinfo/global_burden_disease/estimates/en/
4. GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016 Oct 8;388:1459–544.
5. World Health Organization (WHO). HIV/AIDS fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs360/en/
6. Rerks-Ngarm S, Pitisuttithum P, Nitayaphan S, Kaewkungwal J, Chiu J, Paris R, et al. Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N Engl J Med. 2009;361:2209–20.
7. US National Institute of Allergy and Infectious Diseases (NIAID). First new HIV vaccine efficacy study in seven years has begun [Internet]. National Institutes of Health (NIH). 2016 [cited 2017 Mar 23]. Available from: https://www.nih.gov/news-events/news-releases/first-new-hiv-vaccine-efficacy-study-seven-years-has-begun
8. AVAC: Global Advocacy for HIV Prevention. HVTN 703/HPTN 081 (the AMP study) [Internet]. AVAC. 2016 [cited 2017 Sep 18]. Available from: http://www.avac.org/trial/hvtn-703hptn-081-amp-study
9. Vieillard V, Gharakhanian S, Lucar O, Katlama C, Launay O, Autran B, et al. Perspectives for immunotherapy: which applications might achieve an HIV functional cure? Oncotarget. 2016 Feb 29;7(25):38946–58.
10. Pantaleo G, Levy Y. Therapeutic vaccines and immunological intervention in HIV infection: a paradigm change. Curr Opin HIV AIDS. 2016 Nov 1;11(6):576–84.
11. Drugs for Neglected Diseases initiative (DNDi). Two “4-in-1” LPV/r/ABC/3TC [Internet]. 2017 [cited 2017 Sep 18]. Available from: https://www.dndi.org/diseases-projects/portfolio/two-4-in-1-lpv-r-based-fixed-dose-combinations/
12. The HIV Prevention Trials Network. HPTN 084 [Internet]. 2017 [cited 2017 Sep 18]. Available from: https://www.hptn.org/research/studies/hptn084
13. International Partnership for Microbicides (IPM). IPM’s application for dapivirine vaginal ring for reducing HIV risk in women now under review by European Medicines Agency [Internet]. 2017 [cited 2017 Sep 18]. Available from: http://www.ipmglobal.org/content/ipm%E2%80%99s-application-dapivirine-vaginal-ring-reducing-hiv-risk-women-now-under-review-european
14. World Health Organization (WHO). Two cutting-edge technologies for HIV detection in infants receive WHO prequalification [Internet]. WHO. [cited 2017 Sep 18]. Available from: http://www.who.int/diagnostics_laboratory/cutting-edge-hiv-prequal/en/
15. World Health Organization (WHO). Malaria fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs094/en/
16. World Health Organization (WHO). WHO welcomes support from Gavi for malaria vaccine pilot programme [Internet]. WHO. 2016 [cited 2017 Sep 19]. Available from: http://www.who.int/malaria/news/2016/gavi-malaria-vaccine/en/
17. Malaria Vaccine Funders Group. Malaria vaccine technology roadmap [Internet]. Malaria Vaccine Initiative. 2013 [cited 2017 Nov 9]. Available from: http://www.malariavaccine.org/malaria-and-vaccines/malaria-vaccine-roadmap
18. ClinicalTrials.gov. Safety, tolerability and efficacy of PfSPZ vaccine in healthy children and infants 5 months - 9 years living in Kenya [Internet]. 2017 [cited 2017 Sep 19]. Available from: https://clinicaltrials.gov/ct2/show/NCT02687373
19. Epstein JE, Paolino KM, Richie TL, Sedegah M, Singer A, Ruben AJ, et al. Protection against plasmodium falciparum malaria by PfSPZ vaccine. JCI Insight [Internet]. 2017 Jan 12 [cited 2017 Nov 18];2(1). Available from: https://insight.jci.org/articles/view/89154
20. Medicines for Malaria Venture. Interactive R&D portfolio [Internet]. 2017 [cited 2016 Oct 26]. Available from: http://www.mmv.org/research-development/interactive-rd-portfolio
ANNEXE 3
REFERENCES

AN
NEX
ES
PAGE113
21. Medicines for Malaria Venture. Pyramax [Internet]. 2017 [cited 2016 Oct 26]. Available from: http://www.mmv.org/about-us/achievements-challenges/achievements/pyramax
22. GSK. GSK submits US regulatory application for single-dose tafenoquine for Plasmodium vivax malaria [Internet]. 2017 [cited 2017 Nov 29]. Available from: http://www-origin.gsk.com/en-gb/media/press-releases/gsk-submits-us-regulatory-application-for-single-dose-tafenoquine-for-plasmodium-vivax-malaria/
23. GSK. GSK and MMV announce positive headline phase III results showing single-dose tafenoquine reduces risk of relapse in patients with plasmodium vivax malaria [Internet]. 2017 [cited 2017 Sep 19]. Available from: http://www.gsk.com/en-gb/media/press-releases/gsk-and-mmv-announce-positive-headline-phase-iii-results-showing-single-dose-tafenoquine-reduces-risk-of-relapse-in-patients-with-plasmodium-vivax-malaria/
24. ClinicalTrials.gov. To evaluate the efficacy of a single dose regimen of ferroquine and artefenomel in adults and children with uncomplicated plasmodium falciparum malaria [Internet]. 2017 [cited 2017 Sep 19]. Available from: https://clinicaltrials.gov/ct2/show/NCT02497612
25. Medicines for Malaria Venture. KAF156 enters phase IIb combination studies [Internet]. 2017 [cited 2017 Sep 27]. Available from: https://www.mmv.org/newsroom/press-releases/kaf156-enters-phase-iib-combination-studies
26. PATH. From pipeline to product: malaria R&D funding needs into the next decade [Internet]. 2013 [cited 2016 Sep 16]. Available from: http://www.path.org/publications/files/MVI_pipeline_to_product_r-d_rpt.pdf
27. Das S, Jang IK, Barney B, Peck R, Rek JC, Arinaitwe E, et al. Performance of a high-sensitivity rapid diagnostic test for Plasmodium falciparum malaria in asymptomatic individuals from Uganda and Myanmar and naive human challenge infections. Am J Trop Med Hyg. 2017 Aug 7;
28. PATH. PATH announces agreement with BD to advance new diagnostic technologies to support malaria elimination [Internet]. PATH.org. 2016 [cited 2017 Sep 20]. Available from: http://www.path.org/news/press-room/784/
29. Innovative Vector Control Consortium (IVCC). Annual report 2015-2016 [Internet]. 2016 [cited 2017 Sep 30]. Available from: http://www.ivcc.com/about/governance/annual-reports
30. World Health Organization (WHO). Sixth meeting of the Vector Control Advisory Group (VCAG) [Internet]. WHO. 2017 [cited 2017 Sep 30]. Available from: http://www.who.int/neglected_diseases/vector_ecology/resources/WHO_HTM_NTD_VEM_2017.05/en/
31. World Health Organization (WHO). Tuberculosis fact sheet [Internet]. 2017 [cited 2017 Sep 14]. Available from: http://www.who.int/mediacentre/factsheets/fs104/en/
32. Bernadette Bourdin Trunz, Miranda Brouwer. Global Alliance for TB drug development (TB Alliance) Speeding Treatments to End Paediatric Tuberculosis (STEP-TB) end of project evaluation [Internet]. Euro Health Group; 2017 May [cited 2017 Nov 24]. Available from: http://marketbookshelf.com/publications/global-alliance-tb-drug-development-tb-alliance-speeding-treatments-end-paediatric-tuberculosis-step-tb-end-project-evaluation/
33. World Health Organization (WHO). WHO moves to improve access to lifesaving medicines for hepatitis C, drug-resistant TB and cancers [Internet]. 2015 May [cited 2017 Oct 27]. Available from: http://www.who.int/mediacentre/news/releases/2015/new-essential-medicines-list/en/
34. MSF Access. Four years and counting [Internet]. 2017 Oct [cited 2017 Sep 19]. Available from: https://www.msfaccess.org/sites/default/files/TB_Brief_Four_Years_and_Counting_ENG_2017.pdf
35. Otsuka, Mylan. Otsuka and Mylan announce license agreement to commercialize delamanid (deltyba) for multidrug-resistant tuberculosis (MDR-TB) in high-burden countries [Internet]. 2017 Aug [cited 2017 Oct 27]. Available from: http://www.otsuka.co.jp/en/company/release/detail.php?id=3310&date=201%20%3E%207-08-24
36. TB Alliance. TB Alliance product pipeline [Internet]. 2017 [cited 2016 Oct 5]. Available from: http://www.tballiance.org/portfolio/node/99
37. World Health Organization (WHO). Global tuberculosis report 2017 [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://apps.who.int/iris/bitstream/10665/137094/1/9789241564809_eng.pdf?ua=1
38. TB Alliance. TB Alliance sublicenses promising anti-tuberculosis drug from the Medicines Patent Pool [Internet]. 2017 [cited 2017 Sep 19]. Available from: https://www.tballiance.org/news/tb-alliance-sublicenses-promising-anti-tuberculosis-drug-medicines-patent-pool
39. World Health Organization (WHO). BCG vaccine [Internet]. [cited 2017 Sep 14]. Available from: http://www.who.int/biologicals/areas/vaccines/bcg/en
REFERENCES

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
AN
NEX
ES
PAGE114
40. Frick M, Harrington M, Horn T, Jeffreys R, Lessem E, McKenna L, et al. HIV, TB, and HCV 2017 pipeline report [Internet]. HIV i-BASE/Treatment Action Group (TAG); 2017 [cited 2016 Oct 3]. Available from: www.pipelinereport.org
41. ClinicalTrials.gov. Study to evaluate the efficacy of GlaxoSmithKline (GSK) Biologicals’ candidate tuberculosis vaccine in adults [Internet]. 2017 [cited 2017 Nov 24]. Available from: https://clinicaltrials.gov/ct2/show/NCT01755598
42. FIND. Price for Xpert MTB/RIF and FIND country list [Internet]. 2017 [cited 2016 Sep 15]. Available from: http://www.finddx.org/find-negotiated-product-pricing/#xpert
43. Unitaid. TB diagnostic technology landscape [Internet]. 2017 [cited 2017 Sep 19]. Available from: https://unitaid.eu/news-blog/unitaid-publishes-latest-tb-diagnostic-technology-landscape/
44. World Health Organization (WHO). Global tuberculosis report 2016 [Internet]. 2016 [cited 2016 Sep 26]. Available from: http://www.who.int/tb/publications/global_report/archive/en/
45. World Health Organization (WHO). Diarrhoeal disease fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs330/en/
46. World Health Organization (WHO). Rotavirus [Internet]. Immunization, Vaccines and Biologicals. 2010 [cited 2017 Nov 10]. Available from: http://who.int/immunization/topics/rotavirus/en/
47. World Health Organization (WHO). Cholera fact sheet [Internet]. WHO. 2017 [cited 2017 Nov 24]. Available from: http://www.who.int/mediacentre/factsheets/fs107/en/
48. Centers for Disease Control and Prevention (CDC). Shigella and shigellosis [Internet]. 2017 [cited 2017 Nov 10]. Available from: https://www.cdc.gov/shigella/general-information.html
49. World Health Organization (WHO). Giardiasis [Internet]. International travel and health. [cited 2017 Nov 10]. Available from: http://who.int/ith/diseases/giardiasis/en/
50. Centers for Disease Control and Prevention (CDC). Parasites - cryptosporidium (also known as “Crypto”) [Internet]. 2017 [cited 2017 Nov 9]. Available from: https://www.cdc.gov/parasites/crypto/index.html
51. US Food and Drug Administration. Press announcements - FDA approves vaccine to prevent cholera for travelers [Internet]. 2016 [cited 2017 Sep 20]. Available from: https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm506305.htm
52. India’s rotavirus vaccine to combat diarrhoeal deaths launched. The Hindu [Internet]. 2016 Mar 26 [cited 2017 Sep 20]; Available from: http://www.thehindu.com/news/national/India%E2%80%99s-rotavirus-vaccine-to-combat-diarrhoeal-deaths-launched/article14176433.ece
53. PATH. Rotasiil clinical trial results [Internet]. Defeat DD. 2017 [cited 2017 Sep 29]. Available from: https://www.defeatdd.org/rotasiil
54. Isanaka S, Guindo O, Langendorf C, Matar Seck A, Plikaytis BD, Sayinzoga-Makombe N, et al. Efficacy of a low-cost, heat-stable oral rotavirus vaccine in Niger. N Engl J Med [Internet]. 2017 Mar 22 [cited 2017 Nov 27];376. Available from: http://www.nejm.org/doi/full/10.1056/NEJMoa1609462
55. PATH. ETEC and Shigella vaccine development [Internet]. [cited 2017 Sep 14]. Available from: http://sites.path.org/vaccinedevelopment/diarrhea-rotavirus-shigella-etec/shigella-and-etec-vaccine-development/
56. ClinicalTrials.gov. Safety, immunogenicity and efficacy study of inactivated whole cell Shigella Flexneri 2a vaccine with and without dmLT in adults [Internet]. 2017 [cited 2017 Sep 20]. Available from: https://clinicaltrials.gov/ct2/show/NCT03038243
57. Pitisuttithum P, Islam D, Chamnanchanunt S, Ruamsap N, Khantapura P, Kaewkungwal J, et al. Clinical trial of an oral live shigella sonnei vaccine candidate, WRSS1, in Thai adults. Clin Vaccine Immunol CVI. 2016;23(7):564–75.
58. PATH. DefeatDD - drug development [Internet]. 2017 [cited 2017 Sep 23]. Available from: https://www.defeatdd.org/solution/drug-development
59. PATH. Reducing deadly diarrhea [Internet]. [cited 2017 Sep 21]. Available from: http://www.path.org/projects/edd.php
60. World Health Organization (WHO). Leishmaniasis fact sheet [Internet]. 2017 [cited 2017 Sep 15]. Available from: http://www.who.int/mediacentre/factsheets/fs375/en/
REFERENCES

AN
NEX
ES
PAGE115
61. Centers for Disease Control and Prevention (CDC). Parasites - American trypanosomiasis (also known as Chagas disease) [Internet]. 2016 [cited 2017 Nov 9]. Available from: https://www.cdc.gov/parasites/chagas/index.html
62. World Health Organization (WHO). Trypanosomiasis, human African (sleeping sickness) [Internet]. 2017 [cited 2017 Nov 9]. Available from: http://www.who.int/mediacentre/factsheets/fs259/en/
63. Gillespie PM, Beaumier CM, Strych U, Hayward T, Hotez PJ, Bottazzi ME. Status of vaccine research and development of vaccines for leishmaniasis. Vaccine. 2016 Jun 3;34(26):2992–5.
64. ClinicalTrials.gov. Topical liposomal amphotericin B gel treatment for cutaneous leishmaniasis [Internet]. 2017 [cited 2017 Sep 29]. Available from: https://clinicaltrials.gov/ct2/show/NCT02656797
65. FIND. Leishmaniasis fact sheet [Internet]. 2017 [cited 2017 Nov 24]. Available from: https://www.finddx.org/wp-content/uploads/2017/08/LE-factsheet-Aug2017-WEB.pdf
66. Drugs for Neglected Diseases initiative (DNDi). Paediatric benznidazole (Chagas) [Internet]. 2017 [cited 2017 Sep 15]. Available from: https://www.dndi.org/diseases-projects/portfolio/paediatric-benznidazole/
67. US Food and Drug Administration. FDA approves first U.S. treatment for Chagas disease [Internet]. 2017 [cited 2017 Sep 30]. Available from: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm573942.htm?source=govdelivery&utm_medium=email&utm_source=govdelivery
68. Drugs for Neglected Diseases initiative (DNDi). New benz regimens +/- fosravuconazole [Internet]. 2017 [cited 2017 Sep 20]. Available from: https://www.dndi.org/diseases-projects/portfolio/new-benz-regimens/
69. Castro-Sesquen YE, Gilman RH, Galdos-Cardenas G, Ferrufino L, Sanchez G, Valencia Ayala E, et al. Use of a novel Chagas urine nanoparticle test (Chunap) for diagnosis of congenital Chagas disease. PLoS Negl Trop Dis. 2014 Feb 10;8(10):e3211.
70. Drugs for Neglected Diseases initiative (DNDi). Human African trypanosomiasis fact sheet [Internet]. 2016 [cited 2017 Jul 23]. Available from: https://www.dndi.org/wp-content/uploads/2017/08/Factsheet_2016_HAT.pdf
71. Drugs for Neglected Diseases initiative (DNDi). DNDi Portfolio [Internet]. 2017 [cited 2017 Nov 24]. Available from: https://www.dndi.org/diseases-projects/portfolio/
72. OhAinle M, Balmaseda A, Macalalad AR, Tellez Y, Zody MC, Saborío S, et al. Dynamics of dengue disease severity determined by the interplay between viral genetics and serotype-specific immunity. Sci Transl Med. 2011 Dec 21;3(114):114ra128.
73. World Health Organization (WHO). Dengue and severe dengue fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs117/en/
74. Low JG, Sung C, Wijaya L, Wei Y, Rathore APS, Watanabe S, et al. Efficacy and safety of celgosivir in patients with dengue fever (CELADEN): a Phase 1b, randomised, double-blind, placebo-controlled, proof-of-concept trial. Lancet Infect Dis. 2014 Aug;14(8):706–15.
75. Global Health Innovative Technology Fund (GHIT). Preclinical development of an anti-dengue virus antibody that neutralizes all four serotypes [Internet]. GHIT Fund (Global Health Innovative Technology Fund). 2016 [cited 2017 Sep 20]. Available from: https://www.ghitfund.org/impact/portfolio/awpdetail/detail/100/en
76. Hunsperger EA, Yoksan S, Buchy P, Nguyen VC, Sekaran SD, Enria DA, et al. Evaluation of commercially available diagnostic tests for the detection of dengue virus NS1 antigen and anti-dengue virus IgM antibody. PLoS Negl Trop Dis. 2014 Oct 16;8(10):e3171.
77. Waggoner JJ, Abeynayake J, Sahoo MK, Gresh L, Tellez Y, Gonzalez K, et al. Comparison of the FDA-approved CDC DENV-1-4 real-time reverse transcription-PCR with a laboratory-developed assay for dengue virus detection and serotyping. J Clin Microbiol. 2013 Oct;51(10):3418–20.
78. Dauner AL, Mitra I, Gilliland T, Seales S, Pal S, Yang S-C, et al. Development of a pan-serotype reverse transcription loop-mediated isothermal amplification assay for the detection of dengue virus. Diagn Microbiol Infect Dis. 2015 Sep;83(1):30–6.
79. World Health Organization (WHO). Pneumonia fact sheet [Internet]. 2016 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs331/en/
80. World Health Organization (WHO). Meningococcal meningitis fact sheet [Internet]. WHO. 2015 [cited 2017 Nov 9]. Available from: http://www.who.int/mediacentre/factsheets/fs141/en/
REFERENCES

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
AN
NEX
ES
PAGE116
REFERENCES
81. World Health Organization (WHO). Pneumococcal vaccines WHO position paper 2012 [Internet]. 2012 Jun [cited 2017 Jul 23]. Available from: http://www.who.int/wer/2012/wer8714.pdf?ua=1
82. Alderson MR. Status of research and development of pediatric vaccines for Streptococcus pneumoniae. Vaccine. 2016 Jun 3;34(26):2959–61.
83. UNICEF Supply Division. Meningitis vaccine market supply update [Internet]. UNICEF; 2015 [cited 2017 Nov 18]. Available from: https://www.unicef.org/supply/index_vaccines.html
84. ClinicalTrials.gov. Clinical study of meningococcal ACYWX conjugate vaccine, in 12-16 month olds [Internet]. 2017 [cited 2017 Nov 24]. Available from: https://clinicaltrials.gov/ct2/show/NCT03295318
85. Feasey NA, Dougan G, Kingsley RA, Heyderman RS, Gordon MA. Invasive non-typhoidal salmonella disease: an emerging and neglected tropical disease in Africa. Lancet Lond Engl. 2012;379(9835):2489–99.
86. Centers for Disease Control and Prevention (CDC). Typhoid & paratyphoid fever - chapter 3. In: 2018 Yellow Book [Internet]. 2017 [cited 2017 Nov 10]. Available from: https://wwwnc.cdc.gov/travel/yellowbook/2018/infectious-diseases-related-to-travel/typhoid-paratyphoid-fever
87. Kariuki S, Gordon MA, Feasey N, Parry CM. Antimicrobial resistance and management of invasive salmonella disease. Vaccine. 2015;33:S21–9.
88. Centers for Disease Control and Prevention (CDC). Vaccine information statement - Typhoid [Internet]. 2012 [cited 2017 Nov 24]. Available from: https://www.cdc.gov/vaccines/hcp/vis/vis-statements/typhoid.pdf
89. World Health Organization (WHO). Weekly epidemiological record - No. 32, 2000, 75, 257–264 [Internet]. 2000 [cited 2017 Nov 24]. Available from: http://www.who.int/immunization/wer7532typhoid_Aug00_position_paper.pdf?ua=1
90. Martin LB, Simon R, MacLennan CA, Tennant SM, Sahastrabuddhe S, Khan MI. Status of paratyphoid fever vaccine research and development. Vaccine. 2016;34(26):2900–2.
91. Shuan Ju Teh C, Heng Chua K, Lin Thong K. Paratyphoid fever: splicing the global analyses. Int J Med Sci. 2014;11(7):732–41.
92. Jin C, Gibani MM, Moore M, Juel HB, Jones E, Meiring J, et al. Efficacy and immunogenicity of a Vi-tetanus toxoid conjugate vaccine in the prevention of typhoid fever using a controlled human infection model of Salmonella Typhi: a randomised controlled, phase 2b trial. The Lancet [Internet]. 2017 Sep 28 [cited 2017 Oct 27];0(0). Available from: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)32149-9/abstract
93. University of Oxford. New typhoid vaccine offers hope of protection for children [Internet]. 2017 [cited 2017 Oct 27]. Available from: http://www.ox.ac.uk/news/2017-09-29-new-typhoid-vaccine-offers-hope-protection-children
94. Strategic Advisory Group of Experts (SAGE) on Immunization. Summary of the October 2017 meeting of the Strategic Advisory Group of Experts on Immunization [Internet]. 2017 [cited 2017 Oct 27]. Available from: http://www.who.int/immunization/sage/meetings/2017/october/presentations_background_docs/en/
95. Tennant SM, MacLennan CA, Simon R, Martin LB, Khan MI. Nontyphoidal salmonella disease: Current status of vaccine research and development. Vaccine. 2016 Jun 3;34(26):2907–10.
96. Keenan JD, Hotez PJ, Amza A, Stoller NE, Gaynor BD, Porco TC, et al. Elimination and eradication of neglected tropical diseases with mass drug administrations: a survey of experts. PLoS Negl Trop Dis. 2013 Dec 5;7(12):e2562.
97. TDR Disease Reference Group on Helminth Infections. Research priorities for helminth infections [Internet]. 2012 [cited 2017 Nov 18]. (WHO Technical Report Series on Helminth Infections). Report No.: 972. Available from: http://apps.who.int/iris/bitstream/10665/75922/1/WHO_TRS_972_eng.pdf
98. Seghi P. L’institut Pasteur de Lille teste un vaccin contre un parasite: 200 millions de personnes concernées [Internet]. 2014 [cited 2017 Nov 18]. Available from: http://www.lavoixdunord.fr/region/l-institut-pasteur-de-lille-teste-un-vaccin-contre-un-ia19b0n2315957
99. Baylor College of Medicine. Human hookworm vaccine [Internet]. Texas Children’s Hospital Center for Vaccine Development. [cited 2017 Nov 24]. Available from: https://www.bcm.edu/departments/pediatrics/sections-divisions-centers/tropical-medicine/research/vaccine-development/hookworm
100. Sabin Vaccine Institute. Onchocerciasis [Internet]. 2017 [cited 2017 Nov 24]. Available from: http://www.sabin.org/programs/onchocerciasis

AN
NEX
ES
PAGE117
REFERENCES
101. ClinicalTrials.gov. Study comparing moxidectin and ivermectin in subjects with onchocerca volvulus infection [Internet]. 2017 [cited 2017 Nov 24]. Available from: https://clinicaltrials.gov/ct2/show/NCT00790998
102. ClinicalTrials.gov. Comparing praziquantel versus artesunate + sulfamethoxypyrazine/pyrimethamine for treating schistosomiasis [Internet]. 2008 [cited 2017 Nov 24]. Available from: https://clinicaltrials.gov/ct2/show/NCT00510159
103. Pediatric Praziquantel Consortium. First patient dosed in Phase II clinical trial [Internet]. 2016 [cited 2016 Oct 25]. Available from: http://www.pediatricpraziquantelconsortium.org/news-events/first-patient-dosed-phase-ii-clinical-trial
104. PATH. Oncho/LF biplex test – diagnostic technologies [Internet]. [cited 2017 Sep 20]. Available from: http://sites.path.org/dx/ntd/onchocerciasis-the-disease/oncholf-dual-detection-test/
105. Knopp S, Corstjens PLAM, Koukounari A, Cercamondi CI, Ame SM, Ali SM, et al. Sensitivity and specificity of a urine circulating anodic antigen test for the diagnosis of schistosoma haematobium in low endemic settings. PLoS Negl Trop Dis. 2015;9(5):e0003752.
106. World Health Organization (WHO). Hepatitis C fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs164/en/
107. Messina J, Humphreys I, Flaxman A, Brown A, Cooke G, Pybus O, et al. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology. 2015 Jan;61(1):77–87.
108. Unitaid. Technology and market landscape for hepatitis C medicines [Internet]. 2017 [cited 2017 Nov 24]. Available from: https://unitaid.eu/assets/HCV-Medicines-Landscape_Aug-2017.pdf
109. World Health Organization (WHO). Guidelines for the screening, care and treatment of persons with hepatitis C infection [Internet]. 2014 [cited 2017 Oct 10]. Available from: http://www.who.int/hiv/pub/hepatitis/hepatitis-c-guidelines/en/
110. World Health Organization (WHO). WHO list of prequalified in vitro diagnostic products [Internet]. WHO. [cited 2017 Sep 30]. Available from: http://www.who.int/diagnostics_laboratory/evaluations/PQ_list/en/
111. Burnet Institute. HCV vaccine [Internet]. [cited 2017 Sep 4]. Available from: https://www.burnet.edu.au/projects/14_hcv_vaccine
112. World Health Organization (WHO). Leprosy fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs101/en/
113. Bahmanyar E, Smith WC, Brennan P, Cummings R, Duthie M, Richardus JH, et al. Leprosy diagnostic test development as a prerequisite towards elimination: requirements from the user’s perspective. PLoS Negl Trop Dis. 2016;10(2):e0004331.
114. World Health Organization (WHO). Global leprosy strategy 2016-2020 [Internet]. 2016 [cited 2017 Sep 30]. Available from: http://www.searo.who.int/global_leprosy_programme/documents/global_leprosy_strategy_2020/en/
115. Hotez P, Pecoul B. “Manifesto” for advancing the control and elimination of neglected tropical diseases. PLoS Negl Trop Dis. 2010;4(5):e718.
116. Gelber R, Andries K, Paredes RMD, Andaya CES, Burgos J. The diarylquinoline R207910 is bactericidal against mycobacterium leprae in mice at low dose and administered intermittently. Antimicrob Agents Chemother. 2009 Sep;53(9):3989–3991.
117. Infectious Disease Research Institute (IDRI). Our products [Internet]. [cited 2017 Aug 20]. Available from: http://www.idri.org/products/pipeline/
118. Centers for Disease Control and Prevention (CDC). Cryptococcus: screening for opportunistic infection among people living with HIV/AIDS [Internet]. [cited 2017 Nov 18]. Available from: https://www.cdc.gov/fungal/pdf/at-a-glance-508c.pdf
119. Williamson PR, Jarvis JN, Panackal AA, Fisher MC, Molloy SF, Loyse A, et al. Cryptococcal meningitis: epidemiology, immunology, diagnosis and therapy. Nat Rev Neurol. 2017 Jan;13(1):13–24.
120. Rajasingham R, Smith RM, Park BJ, Jarvis JN, Govender NP, Chiller TM, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis [Internet]. 2017 May 5 [cited 2017 Jun 22];0(0). Available from: http://www.thelancet.com/journals/laninf/article/PIIS1473-3099(17)30243-8/abstract

0
ガル図法(赤道縮尺) 1:47,000,000
1000 2000 3000 4000 5000km
75゜
60゜
45゜
30゜
15゜
0゜
15゜
30゜
45゜
60゜
75゜
90゜
180゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜ 30゜ 15゜ 15゜ 0゜ 165゜ 150゜ 135゜ 120゜ 105゜ 90゜ 75゜ 60゜ 45゜
AN
NEX
ES
PAGE118
REFERENCES
121. Park B, Wannemuehler K, Marston B, Govender N, Chiller T. Estimation of the global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23(4):525–30.
122. Centers for Disease Control and Prevention (CDC). Preventing deaths from cryptococcal meningitis [Internet]. 2017 [cited 2017 Nov 10]. Available from: https://www.cdc.gov/fungal/global/cryptococcal-meningitis.html
123. Sloan D, Parris V. Cryptococcal meningitis: epidemiology and therapeutic options. Clin Epidemiol. 2014 May;13(6):169–82.
124. Viamet. VT-1129 product pipeline [Internet]. [cited 2017 Sep 21]. Available from: http://www.viamet.com/pipeline/vt-1129.php
125. Loyse A, Thangaraj H, Easterbrook P, Ford N, Roy M, Chiller T, et al. Cryptococcal meningitis: improving access to essential antifungal medicines in resource-poor countries. Lancet Infect Dis. 2013 Jul;13(7):629–37.
126. World Health Organization (WHO). Buruli ulcer fact sheet [Internet]. 2017 [cited 2017 Nov 10]. Available from: http://www.who.int/mediacentre/factsheets/fs199/en/
127. World Health Organization (WHO). Buruli ulcer, number of new reported cases. Data by country [Internet]. WHO Global Health Observatory. 2017 [cited 2017 Jun 21]. Available from: http://apps.who.int/gho/data/node.main.A1631
128. Sakyi SA, Aboagye SY, Darko Otchere I, Yeboah-Manu D. Clinical and laboratory diagnosis of buruli ulcer disease: a systematic review. Can J Infect Dis Med Microbiol J Can Mal Infect Microbiol Médicale [Internet]. 2016 [cited 2017 Nov 18];2016. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4931084/
129. Roupie V, Pidot SJ, Einarsdottir T, Poel CVD, Jurion F, Stinear TP, et al. Analysis of the vaccine potential of plasmid DNA encoding nine mycolactone polyketide synthase domains in mycobacterium ulcerans infected mice. PLoS Negl Trop Dis. 2014 Jan 2;8(1):e2604.
130. FIND. The fight against buruli ulcer starts with diagnosis [Internet]. 2014 [cited 2017 Nov 18]. Available from: http://www.finddiagnostics.org/resource-centre/news/141020.html
131. World Health Organization Western Pacific Region (WPRO). Leptospirosis fact sheet [Internet]. WPRO. 2012 [cited 2017 Nov 9]. Available from: http://www.wpro.who.int/mediacentre/factsheets/fs_13082012_leptospirosis/en/
132. Torgerson PR, Hagan JE, Costa F, Calcagno J, Kane M, Martinez-Silveira MS, et al. Global burden of leptospirosis: estimated in terms of Disability Adjusted Life Years. PLoS Negl Trop Dis [Internet]. 2015 Oct 2 [cited 2017 Apr 21];9(10). Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4591975/
133. Chembio Diagnostic Systems. Chembio awarded $3M grant to complete DPP test for human leptospirosis [Internet]. 2009 [cited 2017 Nov 18]. Available from: http://www.clpmag.com/2009/06/chembio-awarded-3m-grant-to-complete-dpp-test-for-human-leptospirosis/
134. Centers for Disease Control and Prevention (CDC). Trachoma (hygiene-related diseases) [Internet]. 2009 [cited 2017 Nov 9]. Available from: https://www.cdc.gov/healthywater/hygiene/disease/trachoma.html
135. World Health Organization (WHO). Trachoma fact sheet [Internet]. 2017 [cited 2017 Nov 18]. Available from: http://www.who.int/mediacentre/factsheets/fs382/en/
136. Goodhew EB, Priest JW, Moss DM, Zhong G, Munoz B, Mkocha H, et al. CT694 and pgp3 as serological tools for monitoring trachoma programs. PLoS Negl Trop Dis. 2012 Jan 11;6(11):e1873.
137. Migchelsen SJ, Martin DL, Southisombath K, Turyaguma P, Heggen A, Rubangakene PP, et al. Defining seropositivity thresholds for use in trachoma elimination studies. PLoS Negl Trop Dis. 2017 Jan 18;11(1):e0005230.
138. National Foundation for Medical Research and Innovation’s (NFMRI). Rheumatic heart disease vaccine gets the final push [Internet]. 2014 [cited 2017 Nov 18]. Available from: http://www.nfmri.org.au/wp-content/uploads/2014/12/141210-Michael-Good-Media-Release-Final.pdf

ACKNOWLEDGEMENTS
This is the tenth in a series of annual reports published as part of the G-FINDER project. We are very grateful to all of the survey participants who have contributed to this effort. With their commitment, we have been able to continue to provide accurate, up-to-date financial information in the field of research and development (R&D) for neglected diseases. The patience and engagement of the participating government and multilateral agencies, academic and research institutions, product development partnerships (PDPs), philanthropic institutions and pharmaceutical and biotechnology companies have made this project possible.
We would like to extend our gratitude to our Advisory Committee and other experts for their invaluable advice on the design and scope of our study. A particularly warm thank you goes to the HIV Vaccines and Microbicides Resource Tracking Working Group, and to the International Federation of Anti-Leprosy Associations for coordinating their initiatives with ours where possible.
We are especially grateful to Richard Fisher, our CEO; Philippa Telford, our executive assistant and office manager; Lee Sternberg, our accounting manager; and our contract researchers Delfina Rampone, Allisa Robertson, Gautam Kumar Saha, Sarah Serhal and Margaret Shi. Their dedicated efforts were key to the survey’s success.
Finally, Policy Cures Research would like to thank the project funder, the Bill & Melinda Gates Foundation, for their ongoing support.
We would also like to acknowledge the following organisations for their commitment and patience in collating large datasets for the G-FINDER survey this year: Argentinian Ministry of Science, Technology and Productive Innovation (MINCYT); Australian National Health and Medical Research Council (NHMRC); Bill & Melinda Gates Foundation; Brazilian Ministry of Health: Department of Science and Technology (DECIT); Brazilian Support Foundation for Research in the State of Minas Gerais (FAPEMIG); Brazilian Support Foundation for Research in the State of São Paolo (FAPESP); Canadian Institutes of Health Research (CIHR); Carlos III Health Institute; European and Developing Countries Clinical Trials Partnership (EDCTP); European Commission (EC); Institut Pasteur; Liverpool School of Tropical Medicine (LSTM); South African Medical Research Council (MRC); Swiss National Science Foundation (SNSF); UK Medical Research Council (MRC); University of Pittsburgh; US National Institutes of Health – National Institute of Allergy and Infectious Disease (NIAID); Wellcome Trust; and all of the PDPs.
In addition, we would like to acknowledge the following organisations for their collaboration with Dr Vipul Chowdhary: Indian Council of Medical Research (ICMR); Indian Department of Biotechnology, Ministry of Science and Technology (DBT); Indian Department of Science and Technology; International Centre for Genetic Engineering and Biotechnology, New Delhi (ICGEB); and the Indian Council of Scientific and Industrial Research (CSIR) labs – Indian Institute of Chemical Biology (IICB), Kolkata; Central Drug Research Institute (CDRI), Lucknow; Institute of Microbial Technology (IMTECH), Chandigarh; Institute of Genomics and Integrative Biology (IGIB), Delhi; Centre for Cellular and Molecular Biology (CCMB), Hyderabad; Indian Institute of Integrative Medicine (IIIM); and the Biotechnology Industry Research Assistance Council (BIRAC).
POLICY CURES RESEARCHwww.policycuresresearch.org
FOR FURTHER COPIES PLEASE CONTACT
55 Brisbane Street Surry Hills NSW 2010
Australia Tel: +61 (2) 8218 2109
Published by Policy Cures Research
December 2017
This report was prepared by Policy Cures Research through a project supported by the Bill & Melinda Gates Foundation.
The views expressed are those of the authors.

NEGLECTED DISEASE RESEARCH AND DEVELOPMENT:REFLECTING ON A DECADE OF GLOBAL INVESTMENT
POLICY CURES RESEARCH
2017
Dr Nick ChapmanAnna DoubellLisette OversteegenDr Vipul ChowdharyDr George RugarabamuRenata ZanettiMing OngJuliette Borri
POLIC
Y CU
RES RESEARC
HG
-FIND
ER 2017 N
EGLEC
TED D
ISEASE RESEA
RCH
& DEVELO
PMEN
T : REFLECTIN
G O
N A D
ECA
DE O
F GLO
BAL IN
VESTMEN
T