De Abdominale wand - bast.be · 9 Hernia inguinalis –Anatomie (1) Liesregio (groin) Fascia...
59
De Abdominale wand
-
Upload
trinhthuan -
Category
Documents
-
view
244 -
download
0
Transcript of De Abdominale wand - bast.be · 9 Hernia inguinalis –Anatomie (1) Liesregio (groin) Fascia...
De Abdominale wand

22
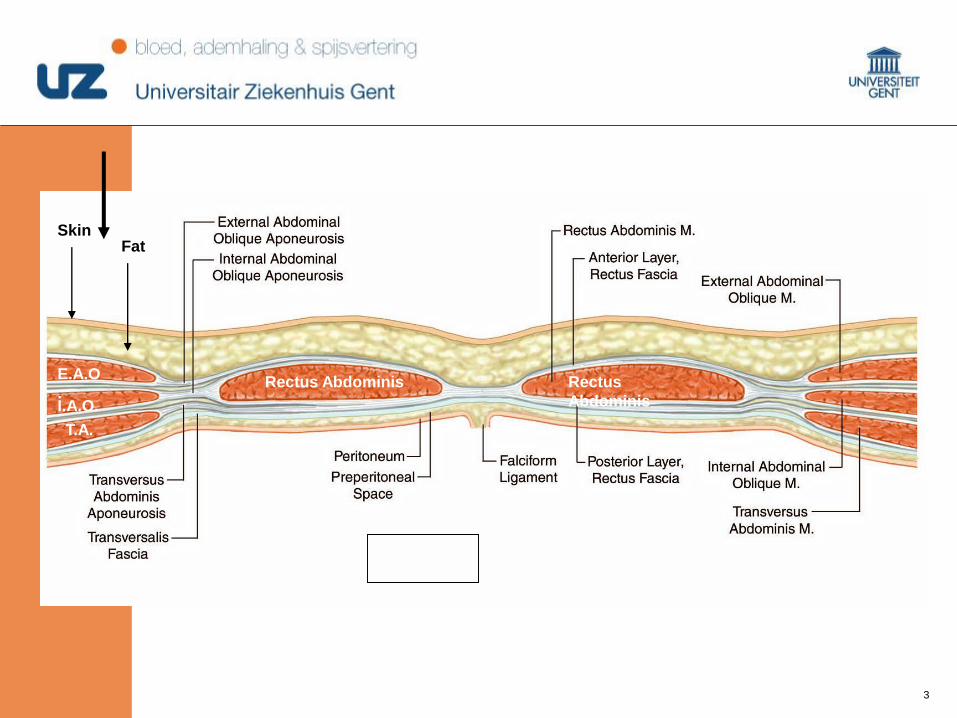
Anterieure buikwand
33
SkinFat
Rectus Abdominis Rectus
Abdominis
E.A.O
.I.A.O.
T.A.
44

55
Hernia
66
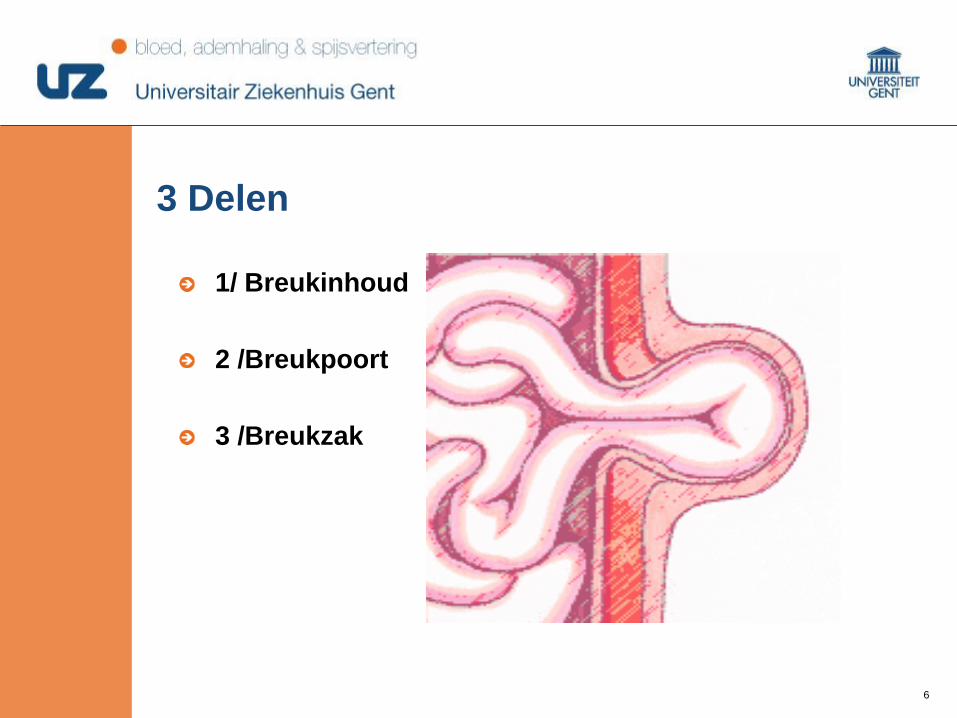
3 Delen
1/ Breukinhoud
2 /Breukpoort
3 /Breukzak
77
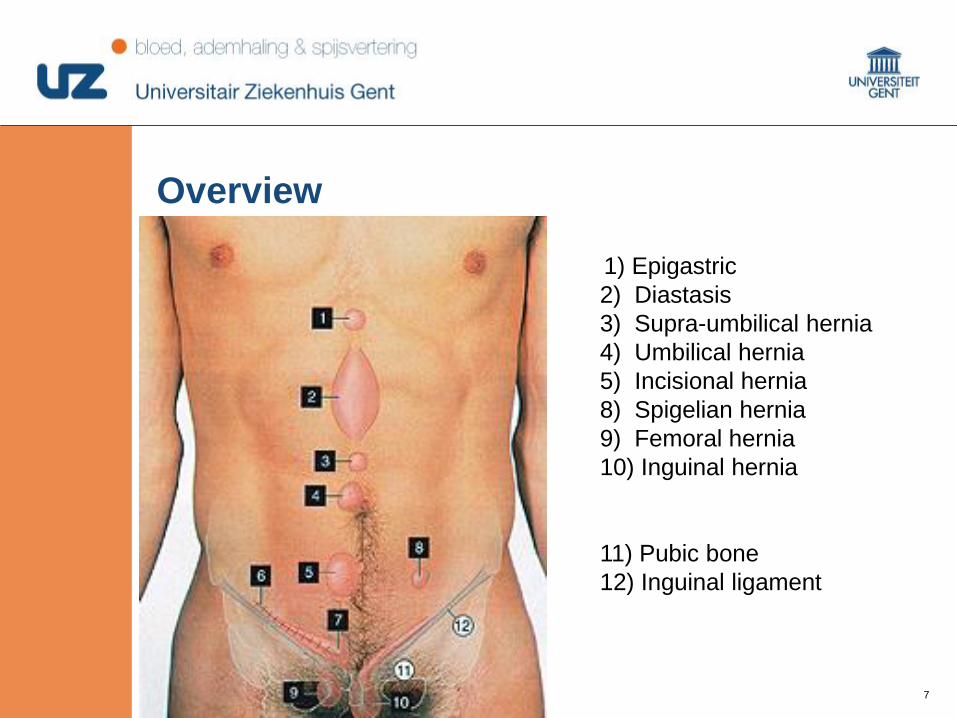
Overview
1) Epigastric
2) Diastasis
3) Supra-umbilical hernia
4) Umbilical hernia
5) Incisional hernia
8) Spigelian hernia
9) Femoral hernia
10) Inguinal hernia
11) Pubic bone
12) Inguinal ligament
88
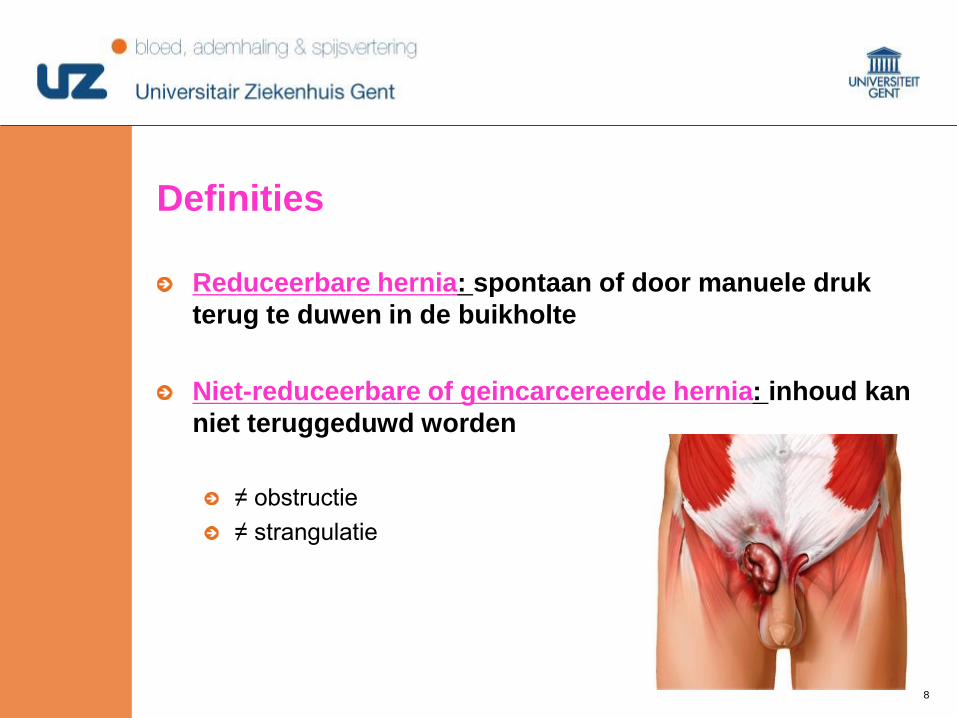
Definities
Reduceerbare hernia: spontaan of door manuele druk
terug te duwen in de buikholte
Niet-reduceerbare of geincarcereerde hernia: inhoud kan
niet teruggeduwd worden
≠ obstructie
≠ strangulatie
99
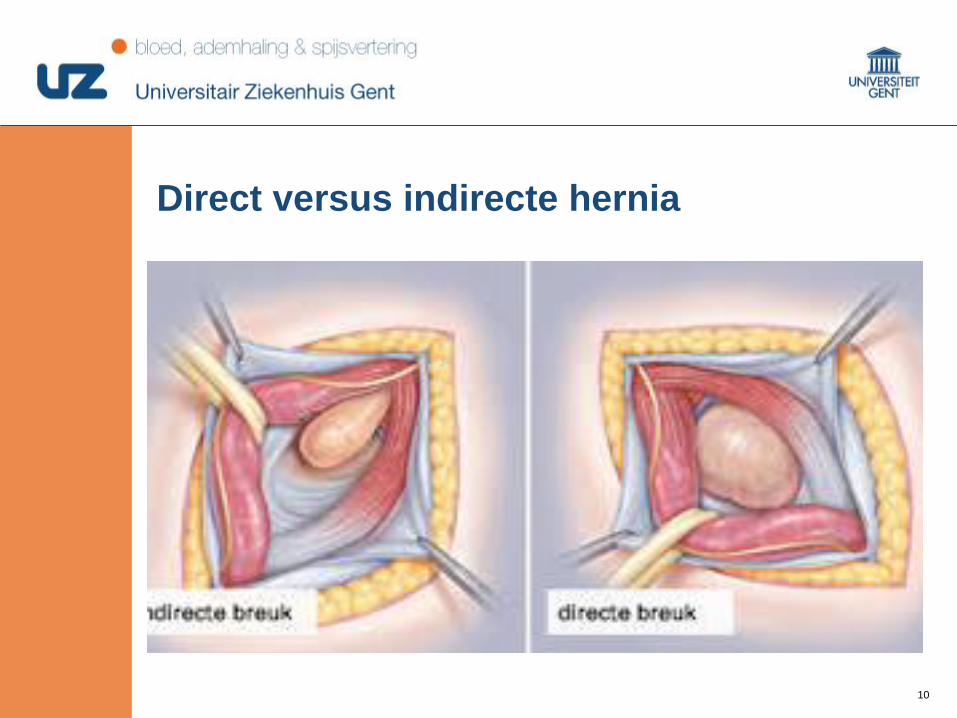
Hernia inguinalis – Anatomie (1)
Liesregio (groin)
Fascia transversalis
Ligamentum inguinale (Poupart)
Ligamentum pectineale (Cooper)
Conjoint tendon (falx inguinalis)
Fascia MOAE en MOAI
Ruimte van Bogros
Skandalakis JE et al. World J Surg 1989;13:490
1010
Direct versus indirecte hernia

1111
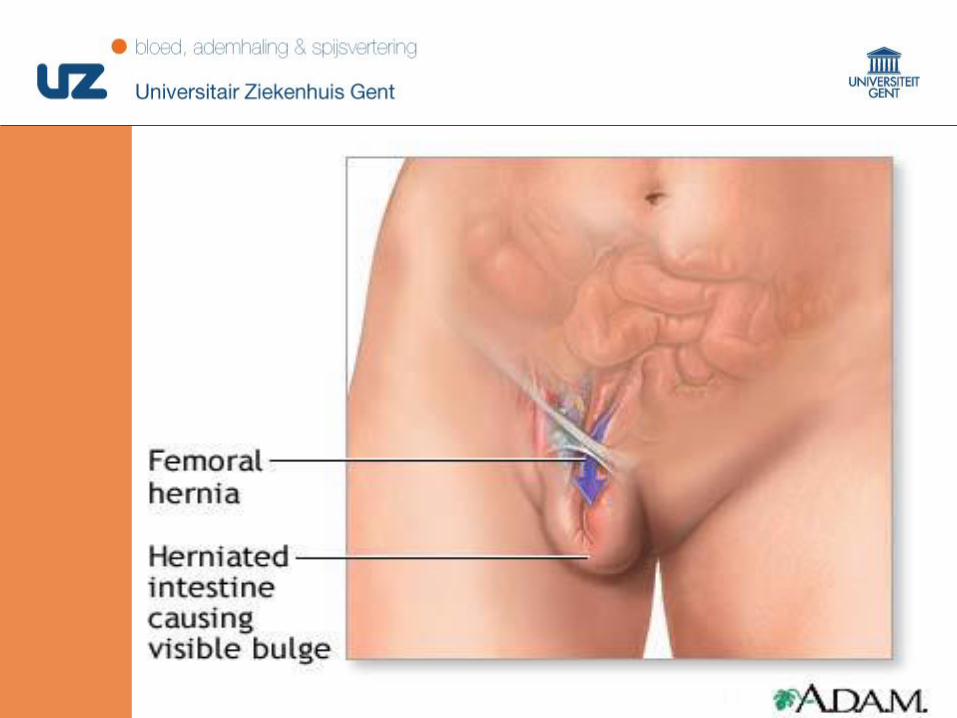
Hernia femoralis
4x meer bij vrouwen dan bij mannen
Altijd controle bij repair van een liesbreuk
33% van de breuken bij vrouwen, 2% bij de man
Meer strangulatie
Onder het ligamentum inguinale
Repair: ver schillende mogelijkheden met sluiten van het femoraal kanaal
1212
1313
Current guidelines (EHS 2009)
• Lichtenstein tension free repair reported recurrence
rates of 1-2%, although underestimated.
• Easy to perform at relatively low cost.
• Laparoscopic repair (TAP and TEP) reports low
recurrence rates and very quick recovery to normal
daily recovery.
So, why look for other techniques ?
1414
Lichtenstein
Referentie
Anterieur herstel
Tension free - prothese
Recidieven 1 à 2 %
Chronische pijn
Niet voor femoraalbreuken
1616
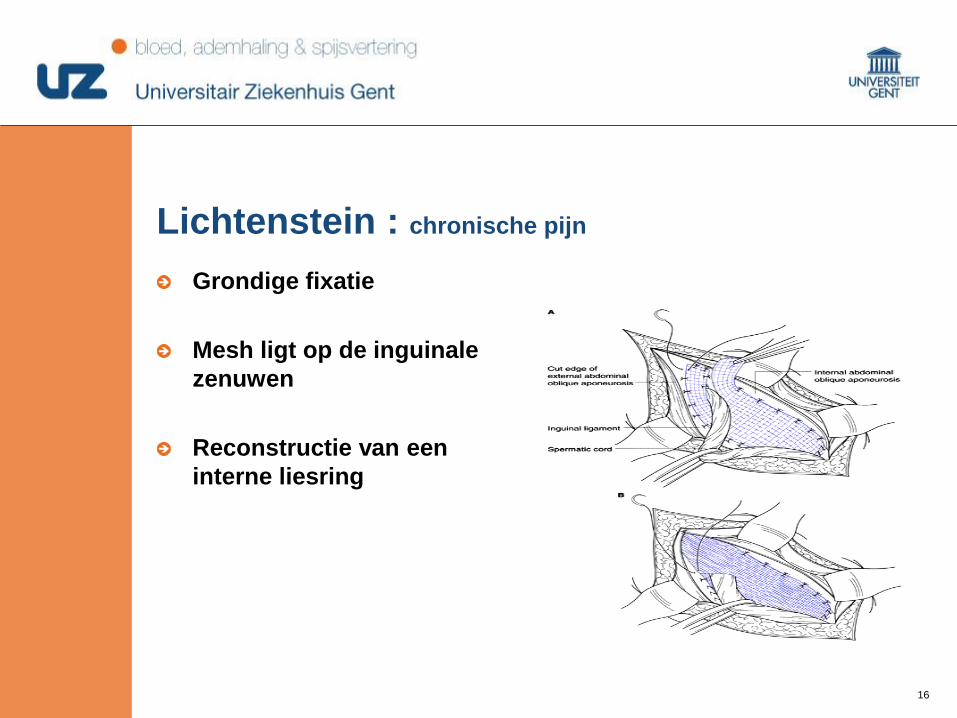
Lichtenstein : chronische pijn
Grondige fixatie
Mesh ligt op de inguinale
zenuwen
Reconstructie van een
interne liesring
1717
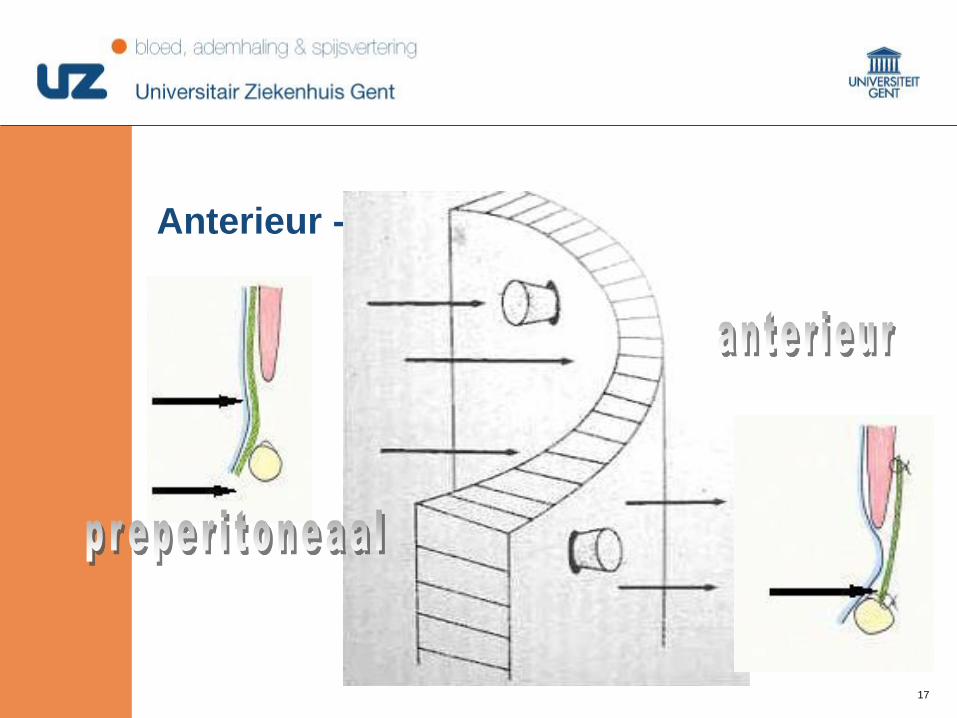
Anterieur - posterieur
1818
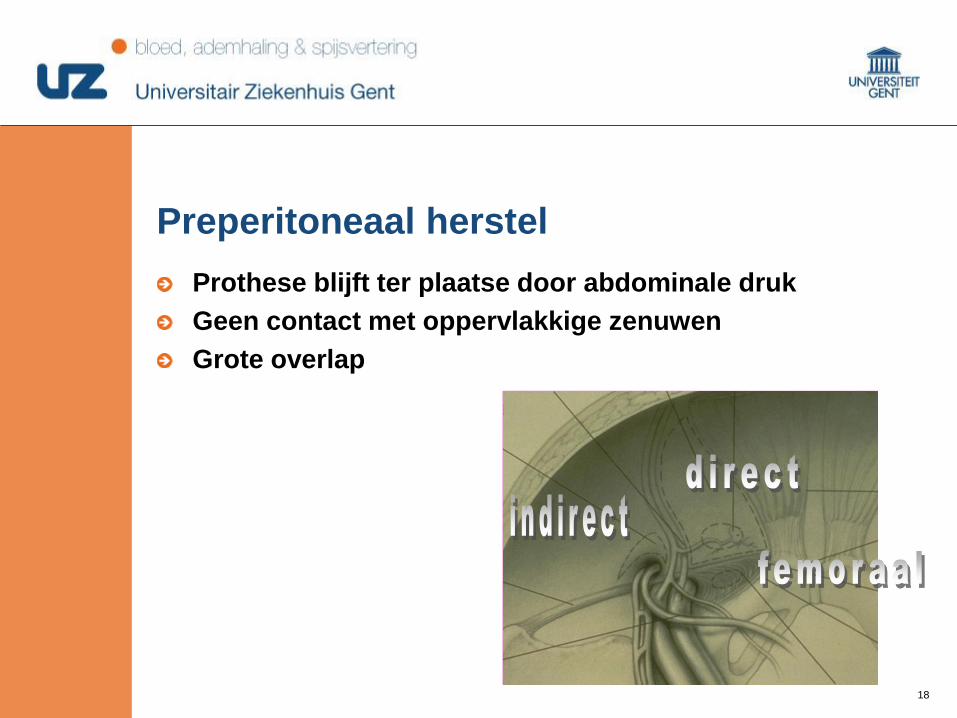
Preperitoneaal herstel
Prothese blijft ter plaatse door abdominale druk
Geen contact met oppervlakkige zenuwen
Grote overlap
1919
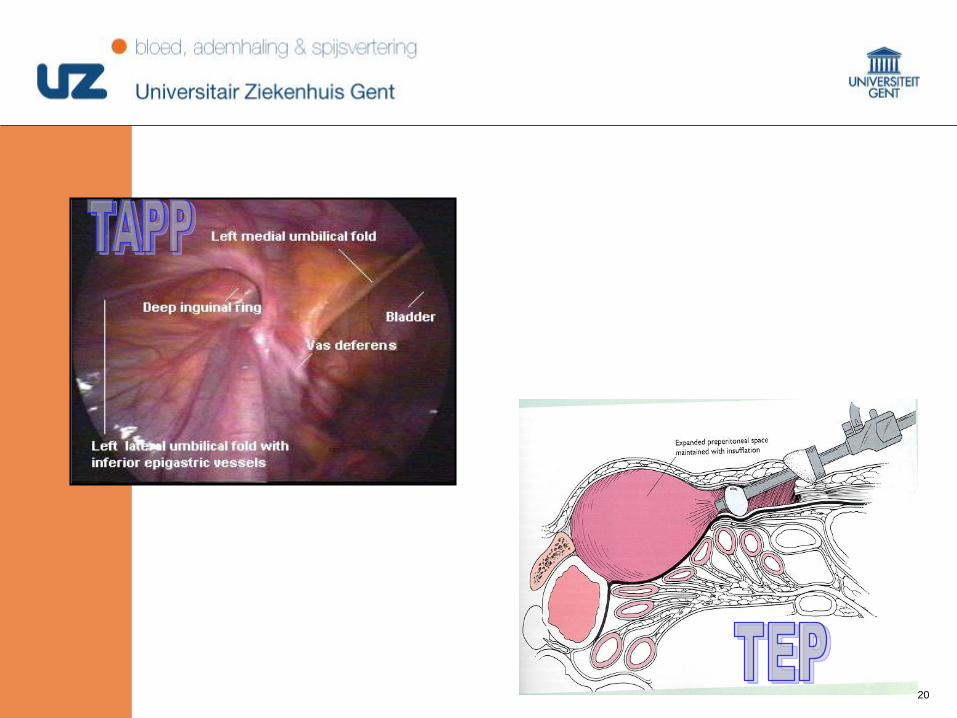
laparoscopie
TAPP
Trans abdominal pre-peritoneal repair
Toegang preperitoneaal via de abdominale caviteit met openen van peritoneum
TEP
Totally extra-peritoneal repair
Preperitoneale ruimte wordt bekomen zonder peritoneum te openen.
2020
laparoscopie

2121
Film TAPP
2323
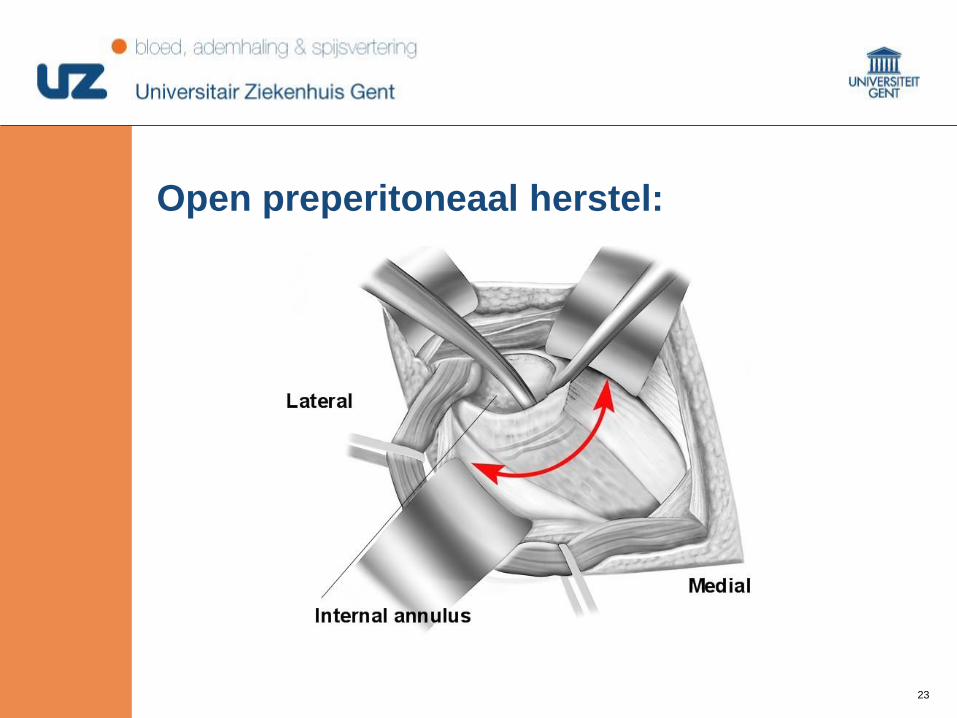
Open preperitoneaal herstel:
2424
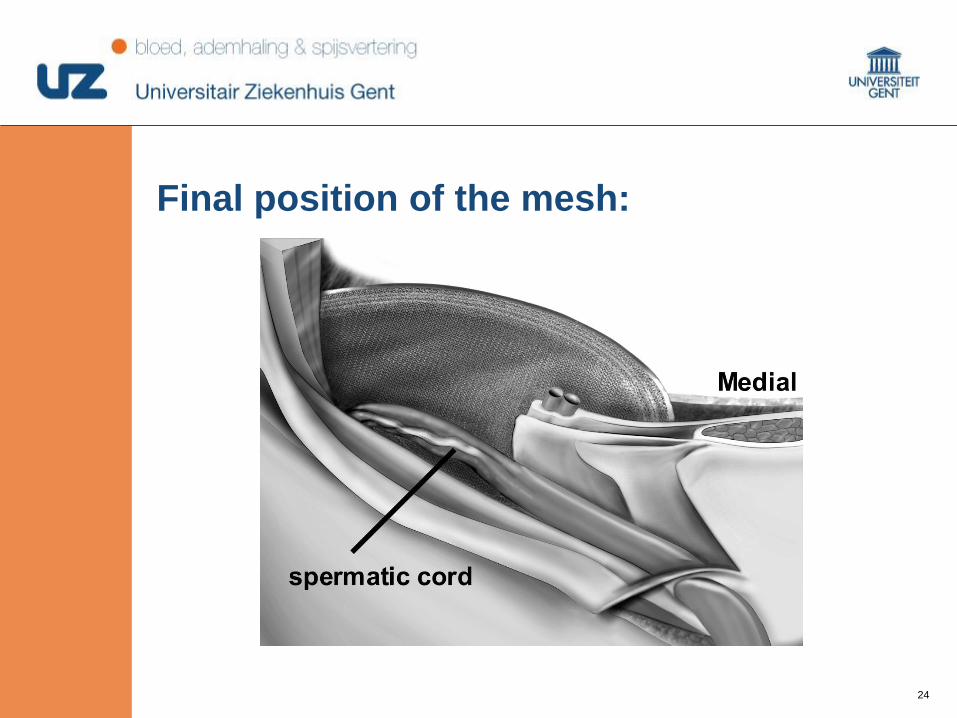
Final position of the mesh:
2525
Hernia umbilicalis
Meer bij vrouwen
Risicofactoren: zwangerschap, ascites, obesiteit
Kinderen: kan verdwijnen in de eerste levensjaren
Volwassenen: chirurgisch herstel
Repair: primair kan bij breukpoorten tot 1cm
Groter dan 1cm: prothese
Laparoscopisch of open
Igv cirrhose: geen consensus over mesh of geen mesh
Eerst controle over de ascites om genezing te bekomen
2626

2727
Closure of the defect
Mayo technique (double layer)
Spitzy technique
Single layer
Non-resorbable vs. resorbable suturematerial
No mesh vs. mesh
Open vs. laparoscopic
2828
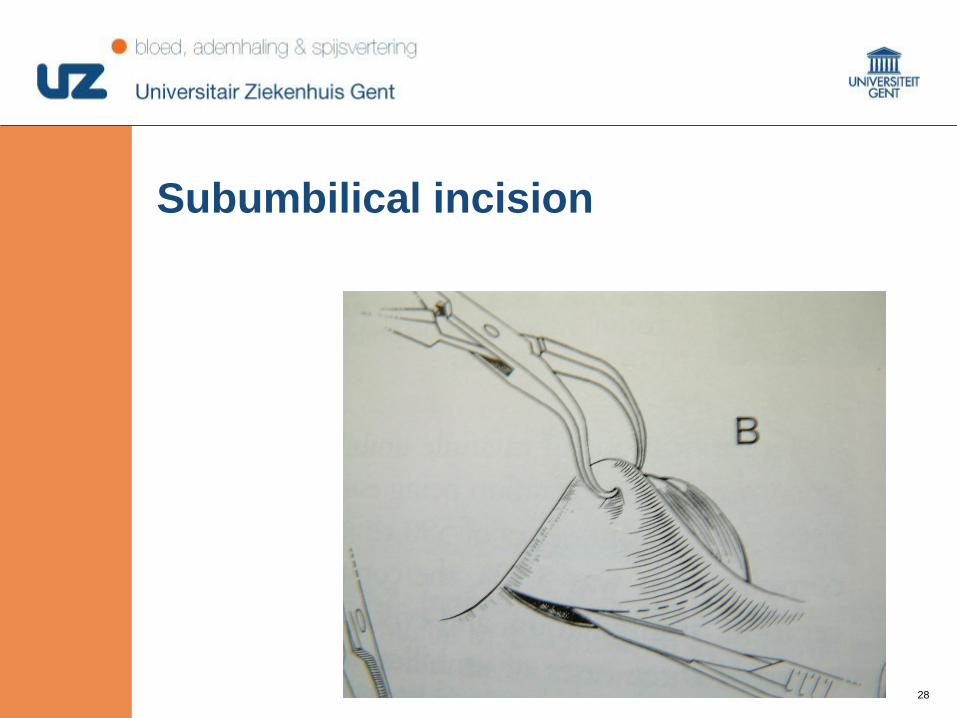
Subumbilical incision
2929
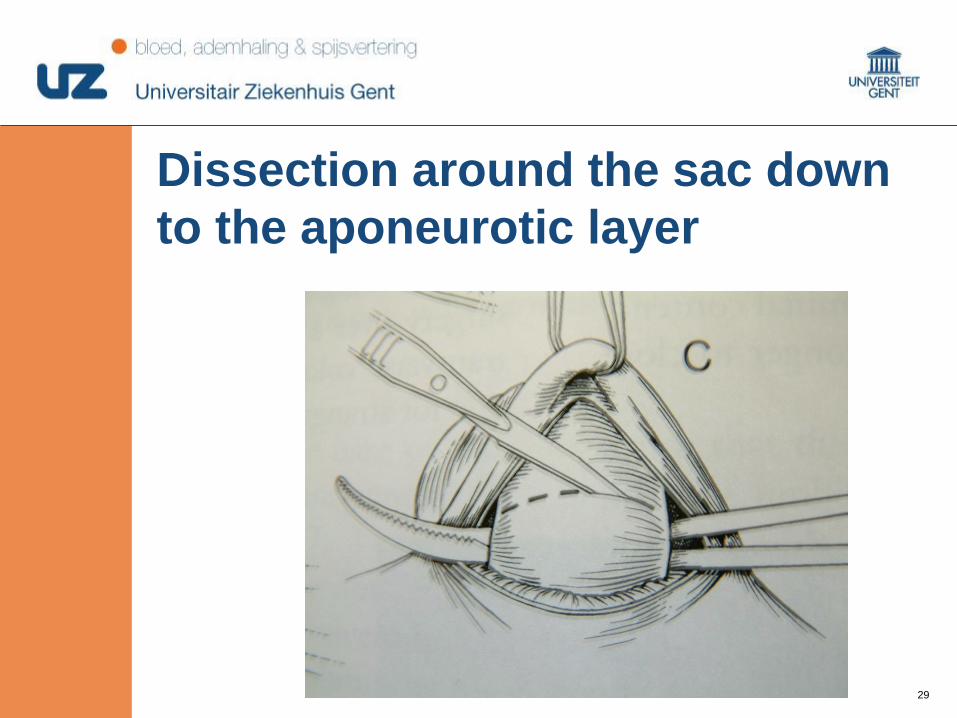
Dissection around the sac down
to the aponeurotic layer
3030
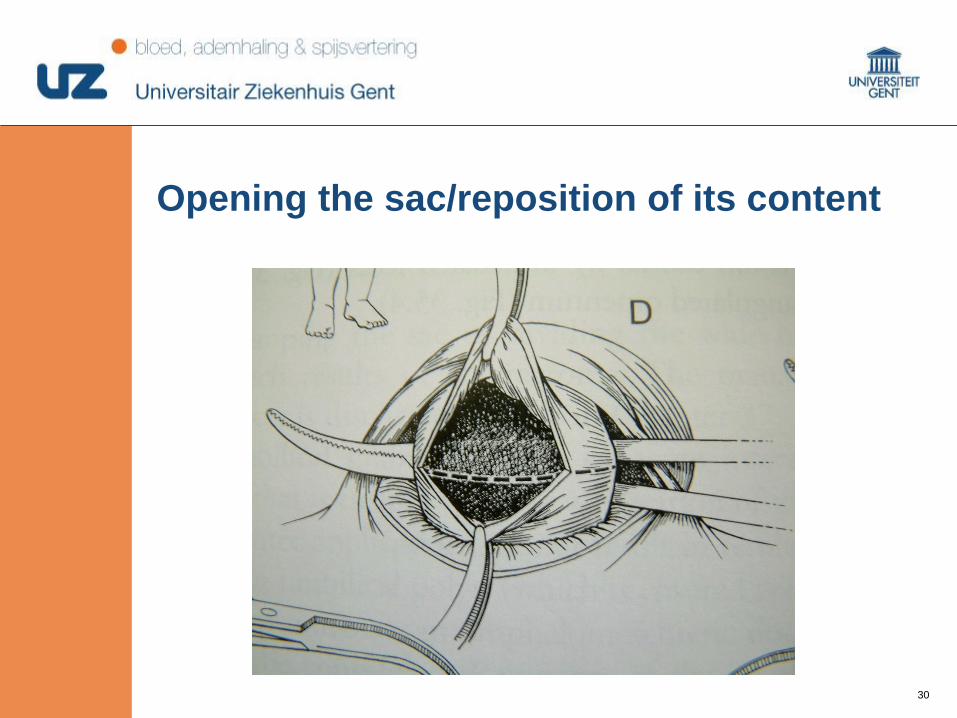
Opening the sac/reposition of its content
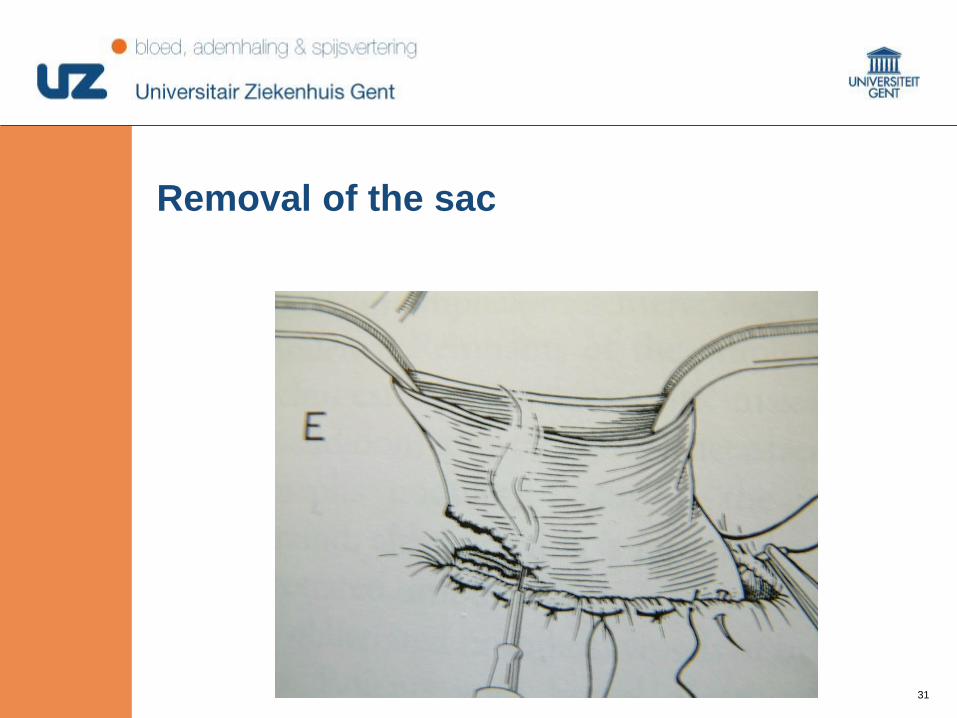
3131
Removal of the sac

3232
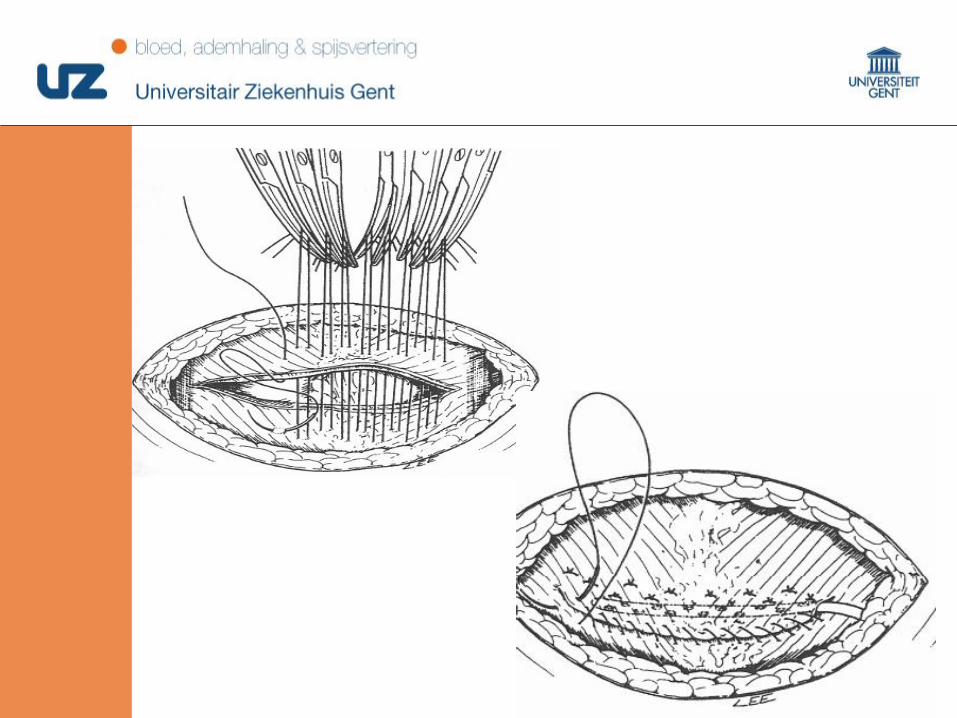
Closure of the fascia
3333
3434
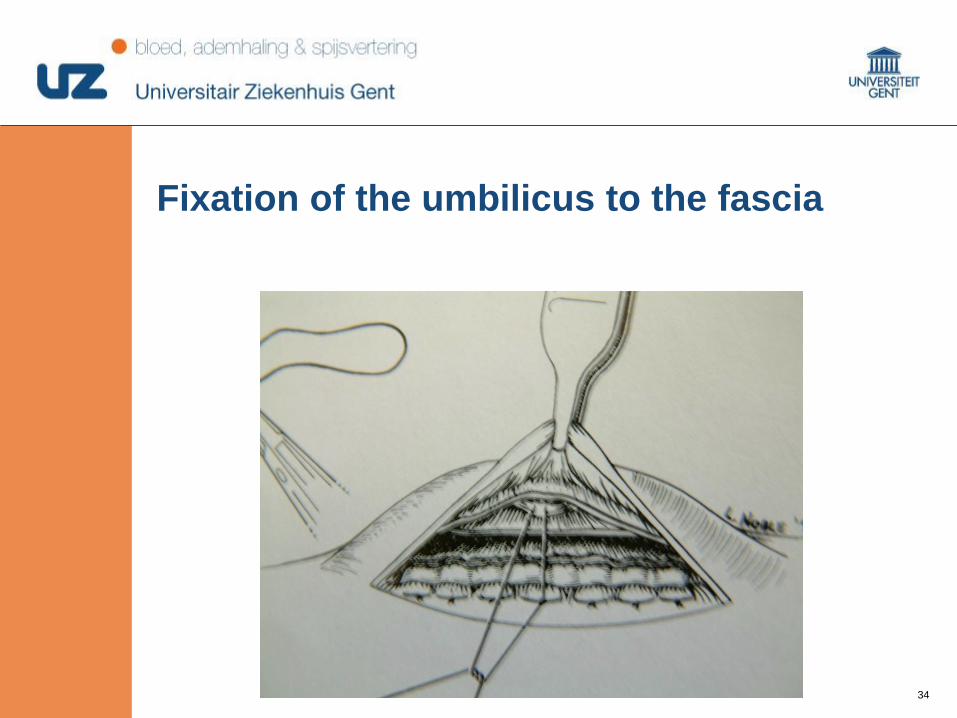
Fixation of the umbilicus to the fascia
3535
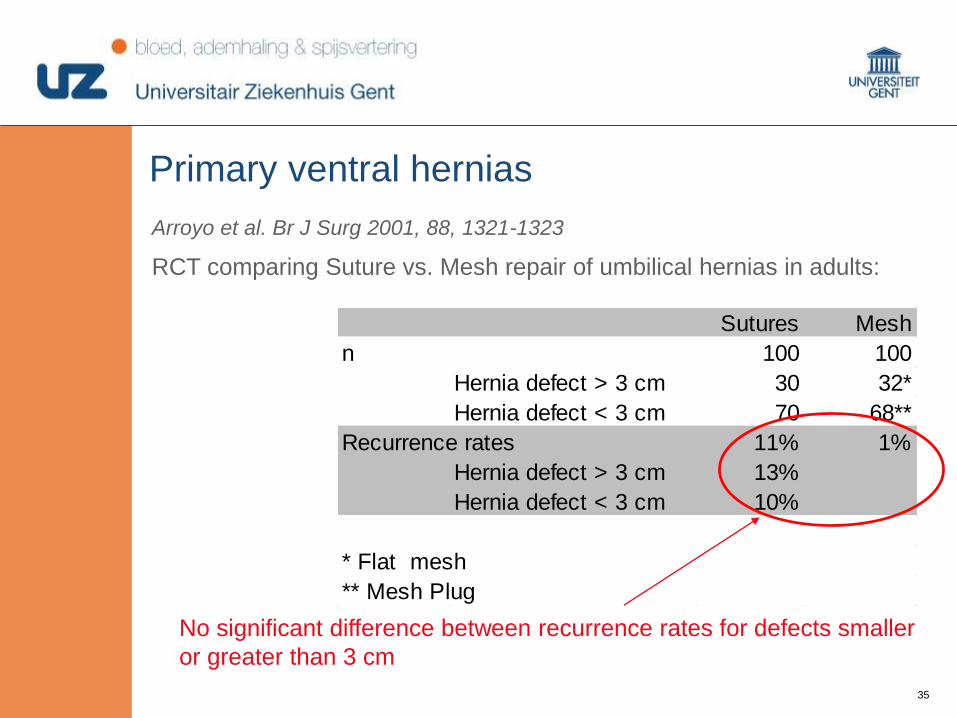
RCT comparing Suture vs. Mesh repair of umbilical hernias in adults:
Arroyo et al. Br J Surg 2001, 88, 1321-1323
Sutures Mesh
n 100 100
Hernia defect > 3 cm 30 32*
Hernia defect < 3 cm 70 68**
Recurrence rates 11% 1%
Hernia defect > 3 cm 13%
Hernia defect < 3 cm 10%
* Flat mesh
** Mesh Plug
No significant difference between recurrence rates for defects smaller
or greater than 3 cm
Primary ventral hernias
3636
Primary ventral hernias
Mesh is no longer optional, not even for defects smaller
than 1cm
Which mesh?
What position?
3737
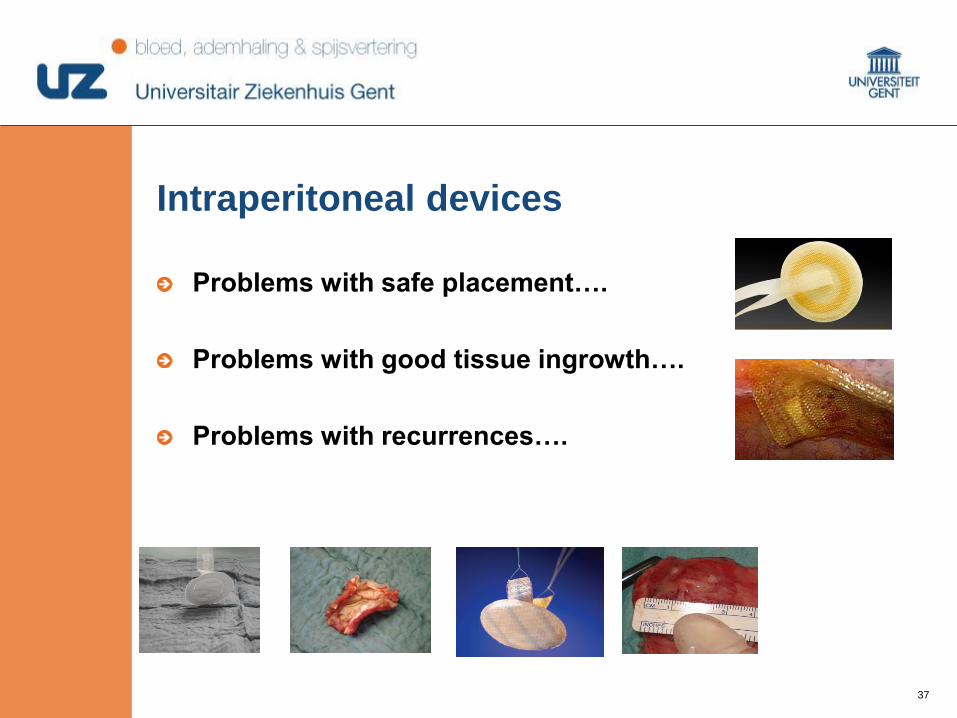
Problems with safe placement….
Problems with good tissue ingrowth….
Problems with recurrences….
Intraperitoneal devices
3838
Safe placement might be a serious problem
Inflammatory reaction , mesh contraction
No “ideal” device has been developed yet….
Limit your hernia size to 2cm or less for such devices
Or is tailoring: going back to preperitoneal mesh
reinforcement with flat mesh??
Caution is warranted….
3939
Film umbilical met mesh
4040
Incisionele hernia (1)
10% na laparotomie
Slechte sluitingstechniek
Multiple ingrepen
Wondinfecties
Leeftijd
Onderliggend lijden
Obesiteit
Pulmonale complicaties postoperatief
4141
Herstel steeds middels mesh-placement
Verschillende technieken:
Rives-Stoppa (sublay), inlay, onlay etc.
Component separation techniek
Ramirez-incisies
Laparoscopisch: geen verwijderen van de breukzak
Gebruik van suturen aan te raden
Cave: seroomvorming!!
Incisionele hernia (2)
4242
Incisional hernias: incidence
31,5% in the first 6 months
54,4% after 12 months
74,8% after 2 years
88,9% after 5 years
Höer J et al. Factors influencing the development of incisional hernia. A retrospective
study of 2983 laparotomy patients over a period of 10 years. (2002) Chirurg; 73:474-480
4343
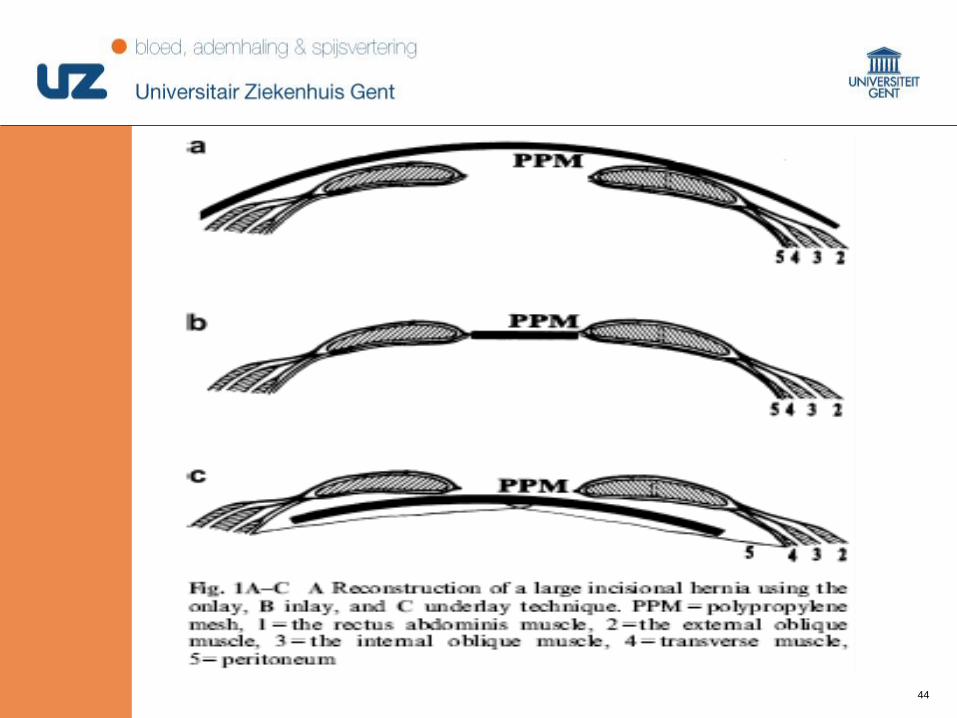
Techniques of repair
Primary repair
Prosthetic mesh repair
Onlay mesh repair
Inlay mesh repair
Retrorectus mesh repair
Intraperitoneal underlay mesh repair
4444
4545
Primary repair
For small defects < 5 cm
Continuous or interrupted sutures to approximate the
edges of the fascial defects (1 cm of the fascial edge 1
cm advancement) = Mayo repair
Recurrence rates > 50 %
Always tension on the repair
NOT DONE ANYMORE
4646
Prosthetic mesh repair
Onlay mesh is sutured to the anterior rectus sheath,
after primary closure of the fascial defect
Advantage
Mesh not in contact with abdominal content
Disadvantages
Repair under tension
Large subcutaneous dissection > seroma formation > mesh
infection
4747
Prosthetic mesh repair
Onlay only (no primary closure of fascial defect)
Advantage
Less tension
4848
Prosthetic mesh repair
Inlay mesh repair
Hernia sac is excised
Recurrence rates 30 – 40 %
Only when retrorectus or intraperitoneal mesh repair is not
possible
4949
Prosthetic mesh repair
Retrorectus mesh repair = Stoppa
Hernia sac in place as a buffer
Above umbilicus
Dissection above posterior rectus fascia and underneath the rectus
muscle
Below the umbilicus
No posterior rectus fascia, dissection in preperitoneal space
5050
Prosthetic mesh repair
Retrorectus mesh repair = Stoppa
Polypropylene mesh in space created and fixated to the muscle
layer above with full or partial thickness sutures
Recurrence rate < 10 %
Mesh infection 5 - 12 %
Pain > 10 %, usually resolves after complete ingrowth of the
mesh
5151
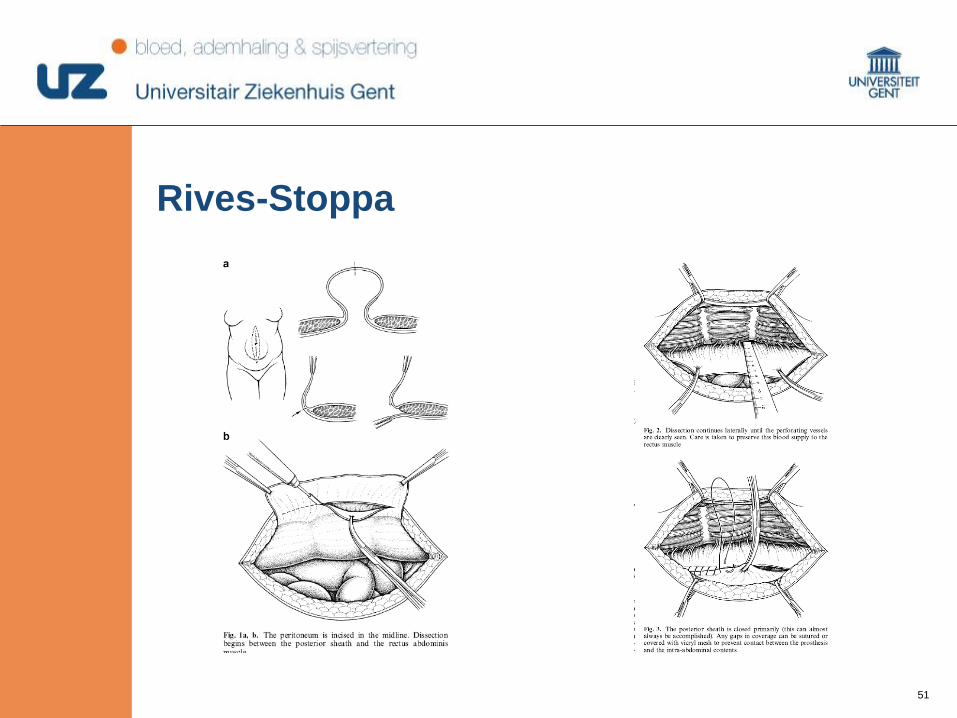
Rives-Stoppa
5252
Prosthetic mesh repair
Intraperitoneal underlay mesh repair
Open
Opening hernia sac, adhesiolysis and fixation of the mesh
intraperitoneal
Laparoscopic
Entering abdomen away from the defect, mesh fixed to the
abdominal wall with partial thickness tacks or full thickness
abdominal/fascial wall sutures
5353
Prosthetic mesh repair
Intraperitoneal underlay mesh repair
Laparoscopic
Significant seroma rate 10 – 15 %
Unrecognized bowel injuries
Recurrence rate < 5 %
5454
Film LVHR
5555
Rationale of Defect Closure
Promote tissue ingrowth into entire surface of mesh
Improve overall outcome
Lower recurrence rates
Lower seroma rates
Improvement of body image
5656
Influencing factors for tailoring
Hernia related factors
Patient related factors
Surgeon related factors
Choice of fabric
Available evidence
Surgeon
Technique
PATIENT
Choice of mesh
5757
Experience (lap vs. open; onlay versus sublay; suture
vs. mesh)
Favorism (for company, i.e. sales rep, laparoscopy etc.)
Belief (augmentation vs. bridging, closure of the defect
or not ….)
Cost-effectiveness (in function of hospital costs, patient
reimbursement etc.)
Surgeon related factors ~ available evidence

5858
Tailoring towards laparoscopic repair?
Cosmetic results?
Obesity?
Recurrent hernias
5959
Why an open repair?
Benefits
Ease of acces peritoneal
cavity
Familiarity with lysis of
adhesions
Ease of concomitant
operation
Mesh introdiction
Midline fascial closure
Scar excision
Disadvantages
Wound complications
Mesh complications
Complexity of techniques
Retromuscular space
Component separation
Pain
(Cosmesis)
6060
Why a laparoscopic repair?
Benefits
Decreased wound complications!
Easier exploration of the whole scar
Simplicity of mesh placement (POM)
Shorter hospital stay?
Cosmesis
Pain?
Disadvantages
Safe acces to multiply operated abdomen
Incarcerated hernia contents
Mesh introduction
Complexity of mesh fixation
Mesh-bowel adhesions
Missed enterotomy
Bridged repair
More expensive material
Trocar site hernias
Bulging
6161
Bedankt voor uw aandacht…..










