![De kantharos van stevensweert - Theelen20130313] Brom, kantharos.pdf · 2013. 3. 17. · DE KANTHAROS VAN STEVENSWEERT DOOR LEO H. M. BROM L'eiude du passe console souvent, elle repose](https://static.fdocuments.nl/doc/165x107/60b95c9a0f9f2021256b7b7f/de-kantharos-van-stevensweert-20130313-brom-kantharospdf-2013-3-17-de.jpg)





Talen
Pages
Wettelijk

Charissa Esmé van den Brom
Dietary modulation of the effects of sevoflurane on myocardial perfusion, function and ischemic injuryin rats
Dietary m
odulation of the effects of sevoflurane on myocardial perfusion, function and ischem
ic injury in rats Charissa Esm
é van den Brom
UITNODIGING
voor het bijwonen van de openbare verdediging van
het proefschrift
Dietary modulation of the effects of sevoflurane on
myocardial perfusion, function and ischemic
injury in rats
door Charissa van den Brom
Donderdag 30 januari 2014 om 15.45 uur
In de aula van het Hoofdgebouw
Vrije UniversiteitDe Boelelaan 1105
te Amsterdam
Receptie na afloop van de promotie
Paranimfen
Ester [email protected]
Marianne de Gruil-van [email protected]

Dietary modulation of the
effects of sevoflurane on
myocardial perfusion,
function and ischemic
injury in rats
Charissa Esmé van den Brom
Het effect van dieetsamenstelling en sevofluraan op de perfusie, functie en
ischemische schade van het hart in ratten
Printed by: Gildeprint Drukkerijen www.gildeprint.nl
ISBN: 978-90-9027989-3
Copyright © 2013 by C.E. van den Brom ([email protected])
All rights reserved. No part of this book may be reproduced or transmitted in any
form or by any means, without prior written permission of the author.
The work presented in this thesis was performed at the Department of
Anesthesiology and Laboratory for Physiology, VU University Medical Center /
Institute of Cardiovascular Research (ICaR-VU), Amsterdam, the Netherlands.
Financial support by the Dutch Heart Foundation for the publication of this thesis is
gratefully acknowledged.
Additional financial support for this thesis was kindly provided by the following
sponsors: UNO roestvaststaal B.V. and AbbVie B.V.
VRIJE UNIVERSITEIT
Dietary modulation of the effects of sevoflurane on myocardial perfusion, function and ischemic
injury in rats
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aan de Vrije Universiteit Amsterdam,
op gezag van de rector magnificus prof.dr. F.A. van der Duyn Schouten,
in het openbaar te verdedigen ten overstaan van de promotiecommissie
van de Faculteit der Geneeskunde op donderdag 30 januari 2014 om 15.45 uur
in de aula van de universiteit, De Boelelaan 1105
door
Charissa Esmé van den Brom
geboren te Nijkerk

promotor: prof.dr. S.A. Loer copromotoren: dr. C. Boer dr. R.A. Bouwman

Voor papa

Contents
Chapter 1: 9
General introduction & Outline of this thesis
Chapter 2: 19
Metabolic disease and perioperative ischemia in the experimental setting:
Consequences of derangements in myocardial substrate metabolism
Chapter 3: 49
High fat diet-induced glucose intolerance impairs myocardial function, but
not myocardial perfusion during hyperemia: a pilot study
Chapter 4: 67
Sevoflurane impairs myocardial systolic function, but not myocardial
perfusion in diet-induced prediabetic rats
Chapter 5: 85
Diet composition modulates sevoflurane-induced myocardial depression in
rats
Chapter 6: 109
Western diet modulates the susceptibility of the heart to ischemic injury
and sevoflurane-induced cardioprotection in rats
Chapter 7: 129
Conclusions & General discussion
Chapter 8: 143
Summary
Chapter 9: 149
Samenvatting
List of abbreviations 155
Dankwoord 161
List of publications 167
Curriculum Vitae 177


1General introduction & Outline of this
thesis
Introduction 11
Perioperative cardiovascular risks
In the Netherlands, about 1.3 million surgical procedures are performed every year
under general or locoregional anesthesia. Surgery and anesthesia are associated
with alterations in systemic and regional perfusion and oxygenation. These
alterations are due to the cardiovascular effects of anesthetics, loss and replacement
of intravascular volume, mechanical positive pressure ventilation and application of
vasoactive drugs. Although the mortality risk of surgery and anesthesia is nowadays
considerably low, patients are still at risk for perioperative cardiovascular
complications. Bainbridge et al. showed a total perioperative mortality of 0.12% and
anesthetic-related mortality of 0.0034% in the 1990s-2000s in developed and
developing countries.1 The risk for cardiovascular complications increases with age
and in the presence of comorbidities like heart disease, pulmonary disease or
diabetes mellitus.2-4 Other well-known predictors of perioperative cardiac
complications are coronary disease, angina pectoris, prior myocardial infarction,
heart failure, stroke/transient ischemic attack, renal dysfunction and diabetes
mellitus requiring insulin therapy.4;5 It is estimated that cardiovascular complications
like myocardial infarction and cardiac arrest occur in 2-5% of all noncardiac surgical
procedures, and globally affect 5-12 million patients each year.4;5
Myocardial ischemia and reperfusion
The most common cardiovascular complication during or after noncardiac surgery is
the development of myocardial ischemia,4;5 which is associated with a significant risk
for morbidity and mortality. Myocardial ischemia occurs when coronary perfusion is
inadequate to maintain a sufficient oxygen supply/demand ratio in the heart. During
surgery, maintenance of the myocardial oxygen balance is challenged by anesthetics
and surgical stress, which directly affect myocardial oxygen supply and consumption.
This altered balance may increase the risk of myocardial ischemia.6;7
While the silent nature of perioperative myocardial ischemia hampers its diagnosis,
Landesberg et al. showed that patients with a large increase in troponin following
major surgery are at risk for cardiac complications and unfavorable outcome.8 More
recently, McFalls et al. described that perioperative elevated cardiac troponin levels
strongly predict long-term mortality.9 From these findings it might be concluded that
myocardial ischemia is often present during and after surgery, and prevention of an
oxygen supply/demand mismatch may contribute to improved postoperative
outcome.
Volatile anesthesia
There is an ongoing debate whether the type of anesthesia could modulate the risk
of perioperative cardiovascular complications. Surgical procedures under general
1
12 Chapter 1
anesthesia are either performed using intravenous anesthetics, like propofol, or
inhalational anesthesics using volatile agents like isoflurane or sevoflurane. Volatile
anesthetics are acknowledged for their cardioprotective effects, which consist of
preservation of cardiovascular function in case of reduced tissue oxygenation.
Volatile anesthetics exert several effects on the heart, peripheral vasculature and
the autonomic nervous system. Sevoflurane alters calcium (Ca2+) handling in the
heart. To be more specific, sevoflurane reduces myocardial Ca2+ availability and
increases sarcoplasmic reticulum Ca2+ content,10 depresses Ca2+ currents,11 reduces
Ca2+ influx via the L-type Ca2+ channels12 and increases Na+/Ca2+ exchanger-
mediated Ca2+ influx.13 In addition, sevoflurane prolongs the QT interval, thereby
prolonging ventricular repolarization.14;15 Moreover, inhalation of volatile anesthetics
causes a dose-dependent decrease in blood pressure, mainly due to a reduction in
systemic vascular resistance.16 In healthy humans, sevoflurane decreases myocardial
blood volume and hyperemic blood flow, while myocardial blood flow during baseline
conditions is not affected.17 Further effects of volatile anesthetics on the heart are
negative inotropic effects, such as depressed myocardial contractility and lusitropic
effects reflected by early diastolic dysfunction.18-20 One might expect that, due to the
general effects of volatile anesthetics on the heart, anesthesia may be associated
with a changed balance between myocardial pefusion and function, although this has
been rarely investigated.
Cardiometabolic disease
Patients with lifestyle risk factors, such as excessive caloric intake and a sedentary
lifestyle, which both contribute to the development of obesity and type 2 diabetes
mellitus, even show a higher risk for postoperative morbidity and mortality in case of
perioperative myocardial ischemia.3;4;9;21 Worldwide, more that 1.4 billion adults
were overweight in 2008, and of these over 500 million people were obese.
Moreover, 344 million people suffer from impaired glucose tolerance, whereas 366
million patients are diagnosed with type 2 diabetes mellitus.22 It is expected that by
the year 2030 almost 400 million people suffer from impaired glucose tolerance and
552 million people from diabetes.22
The higher risk for the development of perioperative myocardial ischemia in
patients with obesity and type 2 diabetes mellitus may partly be due to reduced
coronary vasodilation in response to pharmacological stimuli, atherosclerosis,
oxidative stress and insulin resistance.23-25 With the expanding epidemic of obesity
and type 2 diabetes mellitus it is therefore expected that the number of patients that
are prone to develop perioperative myocardial ischemia will increase within the next
decades. The number of studies focusing on the impact of cardiometabolic disease
on myocardial perfusion and function during anesthesia is however limited, and the
underlying pathophysiology is not well understood.
Introduction 13
Dietary intake
While obesity and type 2 diabetes mellitus are acknowledged as factors that
accelerate the risk of perioperative myocardial ischemia, there is only limited
information available with respect to the association between the development of
cardiometabolic disease with myocardial perfusion, function and ischemia and
reperfusion injury. It is commonly acknowledged that excessive caloric intake, in
combination with a sedentary lifestyle, is the main contributor to the development of
obesity and type 2 diabetes mellitus. Most lifestyle programs therefore focus on
changes in dietary behavior in combination with physical activity. In addition to the
number of calories that contribute to the development of cardiometabolic disease,
there is increasing interest in the role of dietary composition on the development of
cardiometabolic disease. A western or cafetaria diet, which is characterized by a high
percentage of saturated fatty acids and simple carbohydrates such as fructose or
sucrose, is one of the most common causes for overweight, obesity and diabetes
mellitus. Animal studies provide evidence that excessive availability of dietary lipids
or simple carbohydrates leads to accumulation of metabolic intermediates, thereby
inducing myocardial insulin resistance and impairment of myocardial function.26-29 In
humans, myocardial triglyceride accumulation is associated with alterations in
myocardial function and has been demonstrated to occur in the diabetic heart.30
During normal physiologic conditions the heart derives its energy requirements from
fatty acid oxidation (60-70%), glucose oxidation (30-40%) and amongst others,
lactate (10%). However, this process is restricted as myocardial substrate
metabolism is largely determined by the availability of the substrate.31-35 The above
described observations contribute to the emerging concept that myocardial substrate
metabolism is closely related to myocardial function. Moreover, in case of surgical
stress and anesthesia, diet-induced alterations in myocardial substrate metabolism
may become more abundant with respect to the balance between the supply and
demand of oxygen and cellular nutrients. It might therefore be interesting to
investigate how modulation of dietary intake influences the susceptibiltiy of the heart
to injury, and whether the protective effects of anesthetic strategies may be altered
by dietary composition.31-35
Interestingly, while the negative consequences of obesity and type 2 diabetes
mellitus for the development of cardiometabolic diseases are well acknowledged,
there is increasing evidence that overweight and obesity may also be protective in
case of postoperative risks,36 the so-called obesity paradox. The counterintuitive
observations suggest that the unfavorable cardiometabolic effects of high intake of
saturated fatty acids may shift towards a beneficial condition in case of stress.
Moreover, recent studies suggest that a change in diet before surgery and
anesthesia may be of influence on the risk of postoperative complications.37 Animal
studies further showed that short-term dietary restrictions before surgical stress are
1
14 Chapter 1
associated with improved insulin sensitivity, oxidative protection and organ
preservation during ischemia and reperfusion injury.38;39 It is however unknown
whether dietary changes in the period before exposure to an anesthetic procedure
may alter the effects of volatile anesthetics on myocardial perfusion, function and
injury.
Aim of this thesis
In the light of these considerations, the present thesis particularly focuses on the
interaction of the volatile anesthetic sevoflurane with myocardial perfusion, systolic
function as well as ischemia and reperfusion injury in rats exposed to a normal
healthy or a western diet. Myocardial perfusion and function were studied using
echocardiography as a noninvase technique for the monitoring of myocardial systolic
and diastolic function. The use of a contrast agent expands the use of the technique
for determination of myocardial perfusion.
We hypothesized that sevoflurane-induced changes in myocardial perfusion and
function are distinctly influenced by preoperative dietary composition. Moreover, we
tested the hypothesis that a high intake of saturated fatty acids in combination with
simple carbohydrates alters the cardioprotective effects of sevoflurane in case of
myocardial ischemia and reperfusion. The specific aims per chapter are summarized
below.
Outline of the thesis
This thesis focuses on the effect of dietary changes on myocardial function, perfusion
and injury during sevoflurane anesthesia. In chapter 2 the effects of volatile
anesthetics, diabetes and perioperative ischemia on myocardial substrate
metabolism are reviewed.
In chapter 3, we studied the effect of high fat diet feeding on myocardial perfusion
and function with (contrast) echocardiography. We used dipyridamole infusion to
induce conditions of hyperemia. Chapter 4 describes the effects of a more severe,
western diet on myocardial perfusion and function. Additionally, the effects of
sevoflurane were studied.
Furthermore, we studied the effect of changing dietary intake on myocardial
function and myocardial ischemia and reperfusion injury. Chapter 5 was designed to
study the effect of dietary alterations in combination with sevoflurane exposure on
myocardial function. In Chapter 6 the hypothesis that the cardioprotective effects of
sevoflurane on myocardial ischemia and reperfusion injury are reduced by western
diet-feeding has been tested.
Finally, Chapter 7 provides a general discussion of the findings presented in this
thesis and places these findings in perspective.
Introduction 15
References
1. Bainbridge D, Martin J, Arango M, Cheng D: Perioperative and anaesthetic-related mortality in
developed and developing countries: a systematic review and meta-analysis. Lancet 2012,
380:1075-1081.
2. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ,
Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L: Derivation and prospective
validation of a simple index for prediction of cardiac risk of major noncardiac surgery.
Circulation 1999, 100:1043-1049.
3. Eagle KA, Berger PB, Calkins H, Chaitman BR, Ewy GA, Fleischmann KE, Fleisher LA, Froehlich
JB, Gusberg RJ, Leppo JA, Ryan T, Schlant RC, Winters WL, Jr., Gibbons RJ, Antman EM, Alpert
JS, Faxon DP, Fuster V, Gregoratos G, Jacobs AK, Hiratzka LF, Russell RO, Smith SC, Jr.:
ACC/AHA Guideline Update for Perioperative Cardiovascular Evaluation for Noncardiac Surgery--
Executive Summary. A report of the American College of Cardiology/American Heart Association
Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on Perioperative
Cardiovascular Evaluation for Noncardiac Surgery). Anesth Analg 2002, 94:1052-1064.
4. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, Freeman WK,
Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF, Smith SC, Jr., Jacobs AK, Adams CD,
Anderson JL, Antman EM, Buller CE, Creager MA, Ettinger SM, Faxon DP, Fuster V, Halperin JL,
Hiratzka LF, Hunt SA et al.: ACC/AHA 2007 guidelines on perioperative cardiovascular
evaluation and care for noncardiac surgery: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to
Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery):
developed in collaboration with the American Society of Echocardiography, American Society of
Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society
for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology,
and Society for Vascular Surgery. Circulation 2007, 116:e418-e499.
5. Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, Esterbrooks DJ, Hunter CB,
Pipinos II, Johanning JM, Lynch TG, Forse RA, Mohiuddin SM, Mooss AN: Development and
validation of a risk calculator for prediction of cardiac risk after surgery. Circulation 2011,
124:381-387.
6. Dole WP: Autoregulation of the coronary circulation. Prog Cardiovasc Dis 1987, 29:293-323.
7. Hoffman JI, Spaan JA: Pressure-flow relations in coronary circulation. Physiol Rev 1990,
70:331-390.
8. Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, Weissman C, Mosseri M:
Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term
survival after major vascular surgery. J Am Coll Cardiol 2003, 42:1547-1554.
9. McFalls EO, Ward HB, Moritz TE, Apple FS, Goldman S, Pierpont G, Larsen GC, Hattler B, Shunk
K, Littooy F, Santilli S, Rapp J, Thottapurathu L, Krupski W, Reda DJ, Henderson WG: Predictors
and outcomes of a perioperative myocardial infarction following elective vascular surgery in
patients with documented coronary artery disease: results of the CARP trial. Eur Heart J 2008,
29:394-401.
10.Hannon JD, Cody MJ: Effects of volatile anesthetics on sarcolemmal calcium transport and
sarcoplasmic reticulum calcium content in isolated myocytes. Anesthesiology 2002, 96:1457-
1464.
1
16 Chapter 1
11.Fassl J, Halaszovich CR, Huneke R, Jungling E, Rossaint R, Luckhoff A: Effects of inhalational
anesthetics on L-type Ca2+ currents in human atrial cardiomyocytes during beta-adrenergic
stimulation. Anesthesiology 2003, 99:90-96.
12.Hanley PJ, ter Keurs HE, Cannell MB: Excitation-contraction coupling in the heart and the
negative inotropic action of volatile anesthetics. Anesthesiology 2004, 101:999-1014.
13.Bouwman RA, Salic K, Padding FG, Eringa EC, van Beek-Harmsen BJ, Matsuda T, Baba A,
Musters RJ, Paulus WJ, de Lange JJ, Boer C: Cardioprotection via activation of protein kinase C-
delta depends on modulation of the reverse mode of the Na+/Ca2+ exchanger. Circulation
2006, 114:I226-I232.
14.Kang J, Reynolds WP, Chen XL, Ji J, Wang H, Rampe DE: Mechanisms underlying the QT
interval-prolonging effects of sevoflurane and its interactions with other QT-prolonging drugs.
Anesthesiology 2006, 104:1015-1022.
15.Nakao S, Hatano K, Sumi C, Masuzawa M, Sakamoto S, Ikeda S, Shingu K: Sevoflurane causes
greater QTc interval prolongation in elderly patients than in younger patients. Anesth Analg
2010, 110:775-779.
16.Malan TP, Jr., DiNardo JA, Isner RJ, Frink EJ, Jr., Goldberg M, Fenster PE, Brown EA, Depa R,
Hammond LC, Mata H: Cardiovascular effects of sevoflurane compared with those of isoflurane
in volunteers. Anesthesiology 1995, 83:918-928.
17.Bulte CS, Slikkerveer J, Kamp O, Heymans MW, Loer SA, de Marchi SF, Vogel R, Boer C,
Bouwman RA: General anesthesia with sevoflurane decreases myocardial blood volume and
hyperemic blood flow in healthy humans. Anesth Analg 2013, 116:767-774.
18.Humphrey LS, Stinson DC, Humphrey MJ, Finney RS, Zeller PA, Judd MR, Blanck TJ: Volatile
anesthetic effects on left ventricular relaxation in swine. Anesthesiology 1990, 73:731-738.
19.Yamada T, Takeda J, Koyama K, Sekiguchi H, Fukushima K, Kawazoe T: Effects of sevoflurane,
isoflurane, enflurane, and halothane on left ventricular diastolic performance in dogs. J
Cardiothorac Vasc Anesth 1994, 8:618-624.
20.Harkin CP, Pagel PS, Kersten JR, Hettrick DA, Warltier DC: Direct negative inotropic and
lusitropic effects of sevoflurane. Anesthesiology 1994, 81:156-167.
21.Preis SR, Pencina MJ, Hwang SJ, D'Agostino RB, Sr., Savage PJ, Levy D, Fox CS: Trends in
cardiovascular disease risk factors in individuals with and without diabetes mellitus in the
Framingham Heart Study. Circulation 2009, 120:212-220.
22.Unwin N, Whiting D, Guariguata L, Hennis A, Husseini A, Ji L, Kissimova-Skarbek K, Libman I,
Mayer-Davis E, Motala A, Narayan V, Ramachandran A, Roglic G, Sham J, Wareham N, Zhang P.
IDF diabetes atlas 2011. 5th ed. Brussels: International Diabetes Federation; 2011.
23.Ansley DM, Wang B: Oxidative stress and myocardial injury in the diabetic heart. J Pathol 2013,
229:232-241.
24.Candiotti K, Sharma S, Shankar R: Obesity, obstructive sleep apnoea, and diabetes mellitus:
anaesthetic implications. Br J Anaesth 2009, 103 Suppl 1:i23-i30.
25.Bagry HS, Raghavendran S, Carli F: Metabolic syndrome and insulin resistance: perioperative
considerations. Anesthesiology 2008, 108:506-523.
26.Ouwens DM, Diamant M, Fodor M, Habets DD, Pelsers MM, El Hasnaoui M, Dang ZC, van den
Brom CE, Vlasblom R, Rietdijk A, Boer C, Coort SL, Glatz JF, Luiken JJ: Cardiac contractile
dysfunction in insulin-resistant rats fed a high-fat diet is associated with elevated CD36-
mediated fatty acid uptake and esterification. Diabetologia 2007, 50:1938-1948.
27.Davidoff AJ, Mason MM, Davidson MB, Carmody MW, Hintz KK, Wold LE, Podolin DA, Ren J:
Sucrose-induced cardiomyocyte dysfunction is both preventable and reversible with clinically
relevant treatments. Am J Physiol Endocrinol Metab 2004, 286:E718-E724.
Introduction 17
28.Marsh SA, Dell'Italia LJ, Chatham JC: Interaction of diet and diabetes on cardiovascular function
in rats. Am J Physiol Heart Circ Physiol 2009, 296:H282-H292.
29.Gonsolin D, Couturier K, Garait B, Rondel S, Novel-Chate V, Peltier S, Faure P, Gachon P, Boirie
Y, Keriel C, Favier R, Pepe S, DeMaison L, Leverve X: High dietary sucrose triggers
hyperinsulinemia, increases myocardial beta-oxidation, reduces glycolytic flux and delays post-
ischemic contractile recovery. Mol Cell Biochem 2007, 295:217-228.
30.van der Meer RW, Rijzewijk LJ, Diamant M, Hammer S, Schar M, Bax JJ, Smit JW, Romijn JA, de
Roos A, Lamb HJ: The ageing male heart: myocardial triglyceride content as independent
predictor of diastolic function. Eur Heart J 2008, 29:1516-1522.
31.Stanley WC, Lopaschuk GD, McCormack JG: Regulation of energy substrate metabolism in the
diabetic heart. Cardiovasc Res 1997, 34:25-33.
32.Carley AN, Severson DL: Fatty acid metabolism is enhanced in type 2 diabetic hearts. Biochim
Biophys Acta 2005, 1734:112-126.
33.Neely JR, Rovetto MJ, Oram JF: Myocardial utilization of carbohydrate and lipids. Prog
Cardiovasc Dis 1972, 15:289-329.
34.van den Brom CE, Bosmans JW, Vlasblom R, Handoko ML, Huisman MC, Lubberink M, Molthoff
CF, Lammertsma AA, Ouwens DM, Diamant M, Boer C: Diabetic cardiomyopathy in Zucker
diabetic fatty rats: the forgotten right ventricle. Cardiovasc Diabetol 2010, 9:25.
35.van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009,
8:39.
36.Valentijn TM, Galal W, Tjeertes EK, Hoeks SE, Verhagen HJ, Stolker RJ: The obesity paradox in
the surgical population. Surgeon 2013, 11:169-176.
37.Mitchell JR, Beckman JA, Nguyen LL, Ozaki CK: Reducing elective vascular surgery perioperative
risk with brief preoperative dietary restriction. Surgery 2013, 153:594-598.
38.Mitchell JR, Verweij M, Brand K, van d, V, Goemaere N, van den Engel S, Chu T, Forrer F, Muller
C, de JM, van IW, IJzermans JN, Hoeijmakers JH, de Bruin RW: Short-term dietary restriction
and fasting precondition against ischemia reperfusion injury in mice. Aging Cell 2010, 9:40-53.
39.Shinmura K, Tamaki K, Bolli R: Short-term caloric restriction improves ischemic tolerance
independent of opening of ATP-sensitive K+ channels in both young and aged hearts. J Mol Cell
Cardiol 2005, 39:285-296.
1

CE van den Brom, CSE Bulte, SA Loer, RA Bouwman,
C Boer
Cardiovascular Diabetology, 2013 12:47
2Metabolic disease and perioperative
ischemia in the experimental setting:
Consequences of derangements in
myocardial substrate metabolism

Metabolic disease and perioperative ischemia 21
Abstract
Volatile anesthetics exert protective effects on the heart against perioperative
ischemic injury. However, there is growing evidence that these cardioprotective
properties are reduced in case of type 2 diabetes mellitus. A strong predictor of
postoperative cardiac function is myocardial substrate metabolism. In the type 2
diabetic heart, substrate metabolism is shifted from glucose utilization to fatty acid
oxidation, resulting in metabolic inflexibility and cardiac dysfunction. The ischemic
heart also loses its metabolic flexibility and can switch to glucose or fatty acid
oxidation as its preferential state, which may deteriorate cardiac function even
further in case of type 2 diabetes mellitus.
Recent experimental studies suggest that the cardioprotective properties of volatile
anesthetics partly rely on changing myocardial substrate metabolism. Interventions
that target at restoration of metabolic derangements, like lifestyle and
pharmacological interventions, may therefore be an interesting candidate to reduce
perioperative complications. This review will focus on the current knowledge
regarding myocardial substrate metabolism during volatile anesthesia in the obese
and type 2 diabetic heart during perioperative ischemia.
2
22 Chapter 2
Introduction
Perioperative cardiac complications occur in 2-5% of all non-cardiac surgical
procedures, which globally affect 5-12 million patients each year.1 More specifically,
0.65% of these patients develop perioperative myocardial infarction or cardiac
arrest.2 Perioperative cardiac complications are an economical, medical and social
burden that warrants optimization of perioperative health and cardiovascular care to
improve patient outcome and reduce health care costs. There are several well-known
predictors for perioperative cardiac complications identified, such as type of surgery,
ASA classification and increasing age.1,2 Additionally, lifestyle risk factors associated
with metabolic alterations, such as excessive dietary intake and physical inactivity,
are strongly associated with clinical risk factors that predict perioperative
cardiovascular complications.1
Lifestyle risk factors related to obesity and type 2 diabetes mellitus (T2DM) have
become an epidemic over the last decade. Worldwide, 366 million people have
T2DM.3 It is predicted that in the year 2030 about 552 million people will have overt
diabetes, mainly T2DM.3 Patients with T2DM are more likely to develop coronary
artery disease and myocardial ischemia4 and have an increased cardiovascular
complication rate after major non-cardiac surgery.5
In addition to prevention programs to reduce the burden of metabolic disease on
the perioperative process, there are intraoperative cardioprotective strategies
available that may reduce the impact of ischemic injury during and after surgery, like
the application of the volatile anesthetics sevoflurane and isoflurane. These volatile
anesthetics exert multiple protective effects that enhance perioperative preservation
of the heart in patients6 and rats.7 Although exposure to volatile anesthetics reduced
infarct size and improved post-ischemic recovery in healthy rats,7 the
cardioprotective effects of these agents are reduced in obese8 and hyperglycemic9
rats. Derangements in myocardial substrate metabolism are one of the hypothetical
mechanisms that may explain the suppressed cardioprotective capacity in T2DM.10-12
It is however not yet understood how these myocardial metabolic alterations affect
intraoperative cardioprotective mechanisms.
In order to elucidate the impact of altered myocardial substrate metabolism on
intraoperative myocardial protection, this review will focus on available preclinical
knowledge regarding myocardial substrate metabolism during volatile anesthesia in
the obese/T2DM heart under normal conditions and in the context of ischemia. We
first describe myocardial substrate metabolism under healthy, obese/T2DM and
ischemic conditions, followed by an overview of the interaction between substrate
metabolism and volatile anesthetics in the context of perioperative ischemia and
reperfusion injury. Finally, we propose strategies to modulate myocardial substrate
Metabolic disease and perioperative ischemia 23
metabolism that may contribute to an improvement of myocardial protective capacity
and perioperative and postoperative outcome in obesity and T2DM.
Myocardial substrate metabolism
Fatty acids and carbohydrates are essential for the pump function of the heart.13
Under physiological conditions, myocardial contractile function relies on oxidation of
fatty acids (60-70%), glucose (30-40%) and to a lesser extent lactate, ketones,
amino acids and pyruvate (10%) to generate adenosine triphosphate (ATP).14-16 The
heart exerts a metabolic flexibility, and myocardial substrate utilization depends on
substrate availability, nutritional status, and exercise level. With glucose as the more
energetically efficient substrate, the healthy heart is able to switch to glucose under
conditions of stress, such as ischemia, pressure overload or in heart failure.
Glucose metabolism is regulated through multiple steps, including uptake,
glycolysis and pyruvate decarboxylation. Myocardial glucose supply is regulated 1)
via circulating glucose levels or 2) by release of glucose from intracellular glycogen
stores.17 Myocardial glucose uptake depends on the sarcolemmal glucose transporter
GLUT1 (insulin-independent) and the dominant glucose transporter GLUT4 (insulin-
dependent) (Figure 2.1).18 After uptake, glucose is broken down into pyruvate by
glycolysis, consumed by the mitochondria and decarboxylated into acetyl-CoA by
pyruvate dehydrogenase. Acetyl-CoA enters the tricarboxylic acid cycle with entry of
reducing equivalents to the electron transport chain and oxidative phosphorylation,
which finally leads to ATP formation (Figure 2.1).
Fatty acid metabolism consists of uptake, oxidation and esterification. There are
two sources of fatty acids for myocardial metabolism: 1) circulating albumin bound
fatty acids derived from adipose tissue via lipolysis or 2) released from triglyceride-
rich lipoproteins from the liver.19 Fatty acids enter cardiomyocytes by simple
diffusion and via transport through three different membrane fatty acid transporters
fatty acid translocase (FAT)/CD36, fatty acid transport protein (FATP1/6) and
plasma membrane fatty acid binding protein (FABPpm) (Figure 2.1).19 After
sarcolemmal uptake, intracellular fatty acids are activated to form fatty acyl-CoA,
which can undergo beta-oxidation or esterification to form intracellular
triglycerides.20 Fatty acid oxidation requires fatty acyl-CoA entry into the
mitochondria, which is dependent on the activity of carnitine palmitoyl transferase
(CPT-1).21 After translocation into the mitochondria, fatty acyl-CoA can enter the
beta-oxidation pathway to form acetyl-CoA and subsequently ATP (Figure 2.1).
Under physiological conditions, 70-90% of the fatty acids that enter cardiomyocytes
are oxidized for ATP generation, whereas 10-30% is converted to triglycerides by
lipoprotein lipase.22 In case of energy expenditure, intracellular triglyceride stores
can be hydrolyzed as an endogenous fatty acid source, which is explanatory for 10%
of the total fatty acid utilization in the heart.23
2
24 Chapter 2
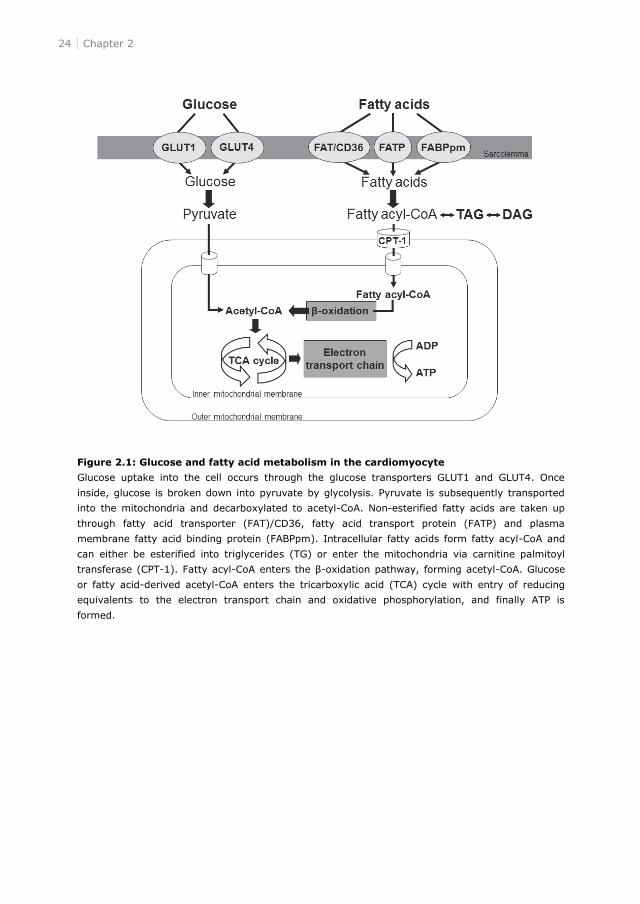
Figure 2.1: Glucose and fatty acid metabolism in the cardiomyocyte
Glucose uptake into the cell occurs through the glucose transporters GLUT1 and GLUT4. Once
inside, glucose is broken down into pyruvate by glycolysis. Pyruvate is subsequently transported
into the mitochondria and decarboxylated to acetyl-CoA. Non-esterified fatty acids are taken up
through fatty acid transporter (FAT)/CD36, fatty acid transport protein (FATP) and plasma
membrane fatty acid binding protein (FABPpm). Intracellular fatty acids form fatty acyl-CoA and
can either be esterified into triglycerides (TG) or enter the mitochondria via carnitine palmitoyl
transferase (CPT-1). Fatty acyl- -oxidation pathway, forming acetyl-CoA. Glucose
or fatty acid-derived acetyl-CoA enters the tricarboxylic acid (TCA) cycle with entry of reducing
equivalents to the electron transport chain and oxidative phosphorylation, and finally ATP is
formed.
Metabolic disease and perioperative ischemia 25
Type 2 diabetes mellitus
Alterations in myocardial substrate metabolism in T2DM hearts are extensively
reviewed by others.15,22,24 In short, myocardial fatty acid metabolism is initially
enhanced in T2DM hearts, with increased rates of fatty acid oxidation and
esterification.25,26 There are two proposed mechanisms that may underlie this
derangement: 1) increased fatty acid uptake due to increased substrate supply and
augmented expression and localization of sarcolemmal fatty acid transporters26 and
2) increased oxidation and esterification due to changes in regulation at both the
enzymatic and transcriptional level.26
In addition, a decreased myocardial glucose metabolism is a concomitant feature of
the T2DM heart.25,26 The slow rate of glucose transport across the sarcolemmal
membrane due to decreased glucose transporters leads to a restriction of glucose
oxidation. Accordingly, fatty acid oxidation has an inhibitory effect on the pyruvate
dehydrogenase complex due to increased fatty acid supply. Taken together, the
T2DM heart has a distinct metabolic phenotype, characterized by enhanced
myocardial fatty acid metabolism and a concomitant reduction in myocardial glucose
metabolism.
Ischemia
Myocardial ischemia occurs when coronary perfusion is inadequate to maintain a
sufficient oxygen supply/demand ratio. Ischemia influences both myocardial
substrate metabolism and myocardial function. The pathophysiological mechanisms
underlying this phenomenon have been reviewed previously.24,27
In the event of ischemia, high-energy phosphates are depleted, ionic homeostasis
is disturbed and contractile dysfunction is caused. The energetic demand of the heart
changes in case of myocardial ischemia. The heart usually responds to injury by
increasing myocardial glucose metabolism to improve its energetic efficiency.22,24
However, increased adipose tissue lipolysis results in increased plasma free fatty acid
concentrations, which may increase myocardial fatty acid utilization and
esterification.27 In this context, glycolysis becomes an important source of energy
due to its ATP-generating ability in the absence of oxygen. It is also suggested that
in the early phase of ischemia, fatty acid oxidation shifts to the more efficient
glucose oxidation, followed by a decrease in total substrate oxidation.24 Increased
glycolysis can parallel depression of myocardial glucose and fatty acid oxidation
depending on the severity of ischemia. Overall, the ischemic heart favors the
energetically more efficient glucose (3.17 ATP/oxygen molecule) over fatty acid
oxidation (2.83 ATP/oxygen molecule).28 This flexibility additionally depends on
substrate availability, oxygen supply, tissue vascularization and myocardial
workload. In conclusion, the metabolic state of the ischemic heart is characterized by
2
26 Chapter 2
imbalances in substrate availability and utilization and is also influenced the severity
of ischemia.
The combination of type 2 diabetes mellitus and ischemia
The cardiometabolic profile of patients with T2DM makes them more prone to
develop plaque formation and intravascular stenosis, leading to the development of
stroke or myocardial infarction. In addition, these patients are more susceptible to
subsequent episodes of ischemia.29,30 Whereas the metabolic undisturbed heart
usually responds to injury by increasing myocardial glucose metabolism,22,24 this
adaptive response is inhibited by insulin resistance, which is a characteristic of
obesity and T2DM. This inhibition results in increased myocardial fatty acid
metabolism,31;32 increased oxygen consumption, decreased cardiac efficiency31 and
altered myocardial perfusion.33 In obese or T2DM animals subjected to myocardial
ischemia the findings are inconclusive. It has been shown that obesity reduced
ischemia and reperfusion injury34 and myocardial function during ischemia (and
reperfusion),35-40 but also similar ischemia and reperfusion injury was found.41
Additionally, increased glucose oxidation and decreased fatty acid oxidation after
myocardial infarction was found, which was ameliorated in obese rats.40 Obese rats
with insulin resistance resulted in preserved myocardial function36 or aggravated36,42-
44 ischemia and reperfusion injury. Moreover, the combination of insulin resistance,
dyslipidaemia and hypertension in obese animals seems to increase the susceptibility
of the heart to ischemia (and reperfusion) injury.45-48 Others however reported that
myocardial injury during ischemia was unaffected in T2DM rats, independent of the
severity of T2DM.49 In case of genetically induced T2DM rats in combination with a
high cholesterol diet, ischemic injury was however exacerbated.50 As stated earlier,
these inconclusive results in animal experiments suggest that the type and severity
of T2DM may influence the sensitivity of the heart to ischemic insults.
With regard to myocardial substrate metabolism, endogenous glycogen stores may
support increased glucose availability as substrate for the heart, and may thus be
beneficial in case of ischemic injury. However, whether pre-ischemic glycogen levels
are beneficial or detrimental depends on the duration of T2DM51 and to the extent of
glycogen depletion during ischemia.52
Overall, the effects of imbalanced myocardial substrate metabolism during ischemia
in T2DM are inconclusive. These observed contrasts may be due to differences in the
severity of ischemia, the measured outcome parameter, exogenous circumstances
and the severity of the experimental model for T2DM.32,53
Metabolic disease and perioperative ischemia 27
Effects of volatile anesthetics in animals
Cardioprotective effects during ischemia
Sevoflurane and isoflurane are commonly used volatile anesthetics. Sevoflurane and
isoflurane make the rat heart more resistant to ischemia and reperfusion injury.54-58
It has been shown that proteins related to myocardial substrate metabolism are,
amongst others, affected by sevoflurane-induced cardioprotection. PI3K and Akt,
which regulate translocation of glucose transporter 4 (GLUT4) to the sarcolemma for
glucose uptake, are increased during sevoflurane in the isolated ischemic rat heart.59
Moreover, sevoflurane enhances GLUT4 expression in lipid rafts, increases glucose
oxidation and decreases fatty acid oxidation after ischemia and reperfusion injury in
isolated working rat hearts compared to untreated ischemic hearts.10 In the same
study, no alterations in AMP activated protein kinase (AMPK) phosphorylation,
pyruvate dehydrogenase activity and glycogen content were found, whereas
sevoflurane decreased triglycerides and ceramide levels after ischemia and
reperfusion injury.10
Moreover, volatile anesthetics are also known to alter mitochondrial function, which
is nicely reviewed by Stadnicka et al.60 In short, it has been shown that sevoflurane
and isoflurane open mitochondrial ATP-activated potassium (mito K+ATP)
channels,61,62 activates reactive oxygen species62 and thereby alters mitochondrial
metabolism.63
Together, these results suggest a role for myocardial substrate metabolism in the
cardioprotective effects of volatile anesthesia during ischemia and reperfusion injury
in animals, although evidence is limited.
Myocardial substrate metabolism during volatile anesthesia
In rats, it has been shown that in vivo myocardial glucose uptake was increased in
the heart during isoflurane (2 vol%) when compared to sevoflurane (3.5 vol%).64 An
explanation could be the differences by more stable blood glucose levels during
sevoflurane. However, a limitation of this study was that the effects were not
compared with findings in awake rats or using non-volatile anesthetics. Others found
that isoflurane (2 vol%) increased myocardial glucose uptake compared to awake
mice.65
The effects of sevoflurane on myocardial substrate metabolism have only been
studied ex vivo. Sevoflurane (2 vol%) decreased FAT/CD36 in lipid rafts and fatty
acid oxidation in isolated rat hearts.12 And, although studied in skeletal muscle cells,
sevoflurane (2.6-5.2%) increased glucose uptake.66 Altogether, these results
suggest that isoflurane and sevoflurane might switch myocardial metabolism to
glucose as energetically more efficient substrate.
2
28 Chapter 2
Volatile anesthesia is also known to affect pancreatic insulin release. In isolated rat
pancreatic islets, enflurane67 and isoflurane68 have an inhibitory effect on glucose-
stimulated insulin release. In rats, isoflurane impaired glucose-induced insulin
release,69 whereas sevoflurane impaired glucose tolerance,70 which both resulted in
hyperglycemia. Therefore it seems that impaired insulin release during volatile
anesthesia might have a negative effect on substrate metabolism. However, the
beneficial cardioprotective effects may outweigh the adverse effects of impaired
insulin secretion, as the American Heart Association 2007 guidelines on
that it can be beneficial to use volatile anesthetics during non cardiac surgery for
maintenance of general anesthesia in hemodynamically stable patients at risk for
myocardial ischemia.1
Alterations in cardioprotective mechanisms in the metabolic altered heart
The healthy heart is capable of protecting itself against stressors like ischemia by the
flexibility to switch between circulating substrates. These cardioprotective properties
might be enlarged during volatile anesthesia. On the other hand, the obese/T2DM
heart is less capable of switching between circulating substrates, which may
contribute to a reduced intrinsic protective capacity. It is generally acknowledged
that the incidence of perioperative cardiovascular complications is increased in
patients with T2DM after non-cardiac surgery.5 Accordingly, blood glucose
concentrations at admission correlated with long-term mortality in diabetic patients
with acute myocardial infarction,71 suggesting that T2DM may affect perioperative
cardiovascular risk. The next paragraphs focus on available experimental knowledge
whether obesity, insulin resistance, hyperlipidemia and hyperglycemia, important
hallmarks of T2DM, exert a cumulative effect on endogenous and exogenous
cardioprotective mechanisms.
Obesity and insulin resistance
It has been shown that obesity and insulin resistance inhibit the cardioprotective
effects of ischemic pre-72 and postconditioning.73 In high fat diet-induced obese rats,
sevoflurane preconditioning failed to induce cardioprotection during myocardial
ischemia and reperfusion injury.41 Moreover, sevoflurane postconditioning did not
protect the heart against myocardial and reperfusion injury in obese and insulin
resistant Zucker rats,8 however, more research is necessary to draw a conclusion.
Hyperlipidemia
The hyperlipidemic heart has difficulties to adapt to stressors like ischemia,
suggesting that cardioprotective mechanisms are impaired. In rats it has been shown
that pacing-induced cardioprotection74 and ischemic-induced preconditioning75 was
inhibited by hypercholesterolemia. Sevoflurane preconditioning reduced myocardial
Metabolic disease and perioperative ischemia 29
infarct size in normocholesterolemic rats, which was blocked in hypercholesterolemic
rats.76 Further research is warranted to study the impact of hyperlipidemia on
anesthesia-induced cardioprotection.
Acute hyperglycemia
Hyperglycemia is an independent predictor of cardiovascular risk.71 The
glycometabolic state upon hospital admission is associated with the mortality risk in
T2DM patients with acute myocardial infarction.77 It has further been shown that
hyperglycemia inhibits the cardioprotective capacity during desflurane-induced
preconditioning,78 isoflurane-induced preconditioning,9,79 and sevoflurane-induced
postconditioning in the experimental setting.80 Accordingly, infarct size was directly
related to the severity of hyperglycemia,81;82 whereas the inhibited cardioprotective
effects of isoflurane-induced preconditioning are concentration dependent and
related to the severity of acute hyperglycemia.9 Moreover, it has been shown that
hyperglycemia attenuated cardioprotection via inhibition of Akt and endothelial nitric
oxide synthase (eNOS) phosphorylation.83 However, interpretation of
abovementioned findings in relation to T2DM is difficult, because experiments were
performed during acute hyperglycemia in otherwise healthy animals without the
typical characteristics of T2DM, such as obesity and insulin resistance.
Type 2 diabetes mellitus
T2DM hinders the cardioprotective effects of ischemic preconditioning,84 which has
been reviewed by Miki et al.85 However, the diabetic rat heart may still benefit when
the preconditioning stimulus is enlarged.86 The effects of anesthesia-induced
cardioprotection in T2DM have however never been studied. In type 1 diabetes, the
protective effects of isoflurane-induced preconditioning were inhibited in case of low
isoflurane concentrations, but not at high concentrations.82 Further, sevoflurane-
induced postconditioning in the type 1 diabetic heart was disturbed, whereas insulin
treatment to reach normoglycemia did not restore the cardioprotective capacity.87
Mechanisms that are suggested to be involved include the inhibition of PI3K/Akt86,87
and inactivity of mito K+ATP.
87 Furthermore, AMPK activation during ischemia protects
the non-obese T2DM Goto-Kakizaki rat heart against reperfusion injury,88 suggesting
a role for AMPK in the cardioprotective properties of the diabetic heart. A limitation
of the above-described studies is that anesthesia-induced cardioprotection is only
studied in type 1 diabetes with insulinopenia and hyperglycemia, but without
characteristics such as obesity, insulin resistance and hyperinsulinemia. Although
current findings suggest that the degree of T2DM, dependent on the presence and
severity of hyperglycemia and hyperlipidemia, is of influence for the cardioprotective
capacity of anesthetics, there are no direct studies available that investigated
cardioprotective strategies in animals with this diabetic entity.
2
30 Chapter 2
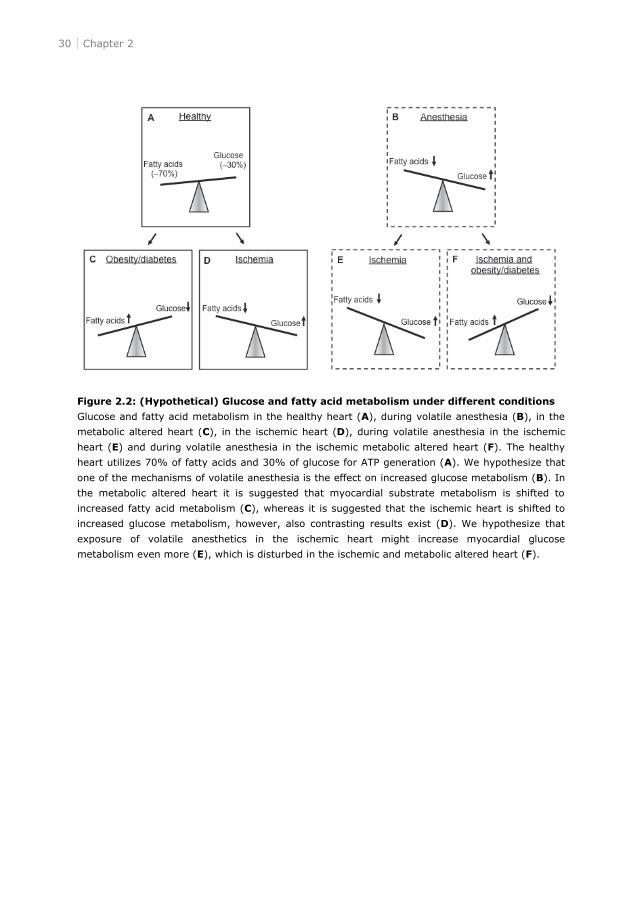
Figure 2.2: (Hypothetical) Glucose and fatty acid metabolism under different conditions
Glucose and fatty acid metabolism in the healthy heart (A), during volatile anesthesia (B), in the
metabolic altered heart (C), in the ischemic heart (D), during volatile anesthesia in the ischemic
heart (E) and during volatile anesthesia in the ischemic metabolic altered heart (F). The healthy
heart utilizes 70% of fatty acids and 30% of glucose for ATP generation (A). We hypothesize that
one of the mechanisms of volatile anesthesia is the effect on increased glucose metabolism (B). In
the metabolic altered heart it is suggested that myocardial substrate metabolism is shifted to
increased fatty acid metabolism (C), whereas it is suggested that the ischemic heart is shifted to
increased glucose metabolism, however, also contrasting results exist (D). We hypothesize that
exposure of volatile anesthetics in the ischemic heart might increase myocardial glucose
metabolism even more (E), which is disturbed in the ischemic and metabolic altered heart (F).
Metabolic disease and perioperative ischemia 31
Experimental options to improve perioperative myocardial
metabolism
The reduced adaptability of the metabolic altered heart to ischemic injury and
cardioprotective interventions warrants further investigation of treatment strategies
that optimize myocardial substrate metabolism before surgery. It is suggested that
volatile anesthesia induces a switch from myocardial fatty acid to glucose
metabolism. In the metabolically altered heart, however, myocardial substrate
metabolism is shifted to increased fatty acid and decreased glucose metabolism.
Accordingly, the effect of volatile anesthetics seems blunted in the metabolic altered
heart. As a consequence, an improvement of the metabolic flexibility of the heart
may be an important target. Figure 2.2 shows a hypothetical overview of the effects
of different conditions on myocardial substrate metabolism.
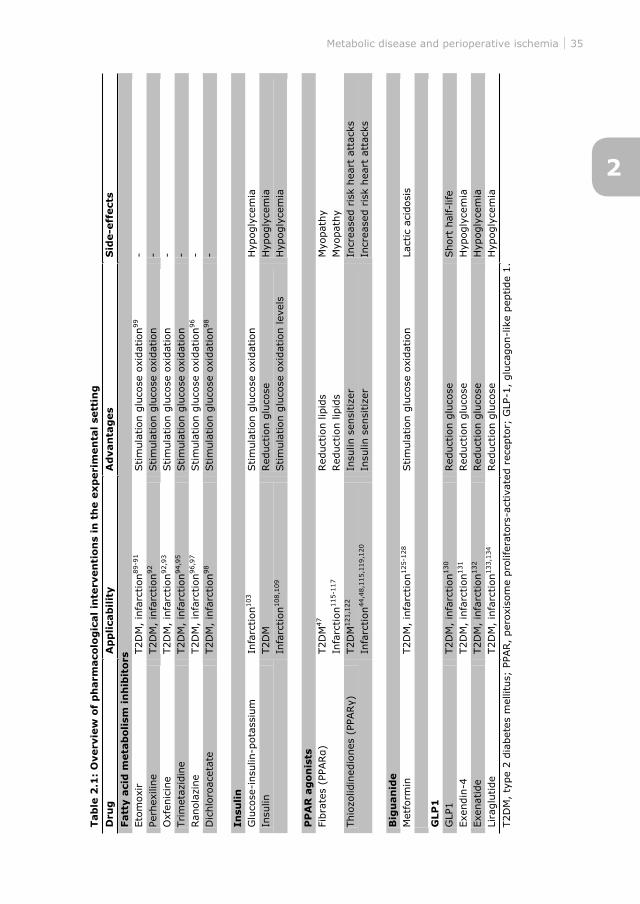
Pharmacological interventions
Improvement of myocardial metabolic flexibility may be achieved by shifting
myocardial substrate metabolism to glucose metabolism. This can be induced by 1)
altering substrate supply, 2) inhibition of fatty acid oxidation and/or 3) improving
insulin sensitivity. The next paragraphs provide an overview of pharmacological
interventions in the experimental setting in the treatment of T2DM and/or
myocardial ischemic injury, which might reduce perioperative risk due to
normalization of metabolic derangements (Table 2.1).
Inhibition of fatty acid metabolism
Carnitine palmitoyl transferase 1 (CPT-1) is a rate-limiting step of fatty acid
oxidation. Several inhibitors of CPT-1 have shown beneficial effects during ischemia
and reperfusion in rats, such as etomoxir,89-91 perhexiline92 and oxfenicine.92;93
However, not all of these variants of CPT-1 inhibitors are yet registered for clinical
use. Other possibilities to reduce fatty acid oxidation are trimetazidine (3-ketoacyl
CoA thiolase inhibitor),94,95 ranolazine (partial fatty acid oxidation inhibitor)96,97 and
dichloroacetate (DCA; pyruvate dehydrogenase kinase inhibitor),98 which have
protective characteristics during myocardial ischemia in rats. One of the suggested
mechanisms underlying the beneficial effects of these substances is the stimulation
of myocardial glucose oxidation.96,98,99 However, as insulin resistance is a hallmark of
the metabolic altered heart, stimulation of glucose metabolism via inhibition of fatty
acid metabolism may be blunted during insulin resistance. Unfortunately, the effect
of volatile anesthesia in combination with inhibition of fatty acid metabolism on
ischemic injury in T2DM hearts has not been studied yet, however, based on the use
of these fatty acid inhibitors in models of T2DM it may be deduced that insulin
2
32 Chapter 2
resistance might be improved, thereby improving the impact of anesthesia-induced
cardioprotection.
Insulin
Glucose-insulin-potassium (GIK) infusion has been shown to reduce mortality in non-
diabetic100,101 and diabetic patients,102 and to reduce infarct size in rats.103 However,
also other results exist.104,105 In the perioperative context, GIK infusion lowered
glucose levels and other metabolic parameters106 and improved perioperative
outcomes, enhanced survival, decreased the incidence of ischemic events107 in T2DM
patients during coronary artery bypass grafting (CABG).
The beneficial effects of GIK include increasing myocardial glucose uptake and
glycogen content. It is suggested that insulin itself might be the major
cardioprotective component. In isolated rat hearts, administration of insulin
protected against ischemia and reperfusion injury.108,109 However, insulin treatment
was not able to restore the lost cardioprotective capacity of sevoflurane in the type 1
diabetic heart.87
Disadvantages of insulin infusion might be hypoglycemia, which could be
circumvented by additional glucose infusion (hyperinsulinemic euglycemic clamping).
Insulin and dextrose infusion normalized postoperative whole body insulin sensitivity
and substrate utilization in healthy patients during elective surgery.110 During cardiac
surgery, insulin and dextrose infusion maintained normoglycemia in healthy111 and
T2DM112 patients, however, hypolipidemia was observed.113 Further, it was shown in
diabetic patients that isoflurane reduced postoperative markers of ischemic injury
after CABG, indicating a cardioprotective effect of isoflurane.114 Preoperative
treatment with glibenclamide prevented this protective effect, which was restored by
changing glibenclamide preoperatively to insulin.114 Taken together, these data
suggest that perioperative glucose control by insulin may decrease the risk of
postoperative mortality and morbidity.
Peroxisome proliferator-activated receptor agonists
Fibrates are selective peroxisome proliferator-activated receptor
which have lipid lowering effects, thereby improving insulin sensitivity. PPAR
activation has been shown to reduce myocardial ischemia and reperfusion injury in
rat hearts.115,116 -Kakizaki rat hearts reduced
ischemic injury,117 whereas in T2DM db/db
sensitivity to ischemia and reperfusion even while myocardial glucose oxidation was
increased and myocardial fatty acid oxidation reduced.47 Moreover, sevoflurane
,118 whereas during CABG
right atrial tissue compared to propofol.11 Based on
agonists combined with volatile anesthesia.
Metabolic disease and perioperative ischemia 33
Insulin-sensitizing drugs, such as thiazolidinediones have beneficial effects by
myocardial ischemia and reperfusion injury in rats.48,115,119,120 Rosiglitazone has been
shown to increase myocardial GLUT4 translocation121 and glucose metabolism122 in
healthy and T2DM rat hearts. During myocardial ischemia and reperfusion, it was
shown that rosiglitazone treatment normalized ischemic injury by improvement of
the reduced glucose uptake in obese Zucker rats,44 and reduced ischemic injury by
improved myocardial insulin sensitivity and glucose oxidation in T2DM Zucker
diabetic fatty rats,48 suggesting a role f
metabolism to optimize metabolic flexibility during myocardial ischemia and
reperfusion. Accordingly, it was shown that desflurane-induced cardioprotection
during ischemia hibition in rabbits,123
Metformin
Metformin, a biguanide with antihyperglycemic properties, has been widely used in
the treatment of obesity and T2DM and exerts its actions by enhancing insulin
sensitivity. It is suggested that the glucose-lowering effects of metformin are
mediated through the activation of AMPK, which has also been indicated to play an
important protective role in the ischemic mouse heart.124,125 In non-diabetic rat
hearts, metformin protects against ischemic injury.126,127 Accordingly, metformin
provides cardioprotection against ischemic injury in T2DM hearts from animals in
vivo,125 but not in vitro.128 The effects of volatile anesthesia and metformin in
ischemic and T2DM hearts has not been studied yet. However, it has been shown
that AMPK is involved in anesthetic cardioprotection.41;129
Glucagon-like peptide 1
Glucagon-like peptide 1 (GLP1) is a gut incretin hormone that is released in response
to nutrient intake, stimulates insulin secretion and exerts insulinotropic and
insulinomimetic properties. GLP1 has been shown to be protective in ischemic rat
hearts.130
GLP1 has a short half-life of several minutes, due to rapid breakdown by dipeptidyl
peptidase IV (DPP4). Exendin-4 is a peptide derived from the saliva of the gila
monster which mimics GLP1, but is resistant to degradation by DPP4. Exenatide and
liraglutide are synthetic GLP1 analogues, which mimic human GLP1 and are currently
used for blood glucose-lowering therapy in T2DM. Exendin-4,131 exenatide132 and
liraglutide133 have been shown to reduce infarct size in animals, but also a neutral
effect of liraglutide on myocardial infarct size was found.134 Another possibility to
circumvent the rapid breakdown of GLP1 is the use of a DPP4 inhibitor. However,
inhibition of DPP4 by valine pyrrolidide in rats130 or in DPP4 knockout mice135 was not
2
34 Chapter 2
protective during myocardial infarction. It is suggested that the cardioprotective
effect is a consequence of insulin, however, GLP1 has cardioprotective effects both in
vivo and in vitro, whereby the latter is in absence of circulating insulin levels,130
suggesting a role for GLP1 in cardioprotection.
The mechanism behind the cardioprotective properties of GLP1 may, amongst
others,136 rely on improving myocardial glucose metabolism. GLP1 increased glucose
uptake in isolated mouse137 and isolated healthy,138 hypertensive139 and
ischemic/reperfused138 rat hearts. Moreover, exenatide increased myocardial glucose
uptake in healthy140 and insulin resistant dilated cardiomyopathy141 mice, whereas it
did not alter myocardial glucose uptake in type 2 diabetic patients.142
Exposure of healthy rats to isoflurane anesthesia decreased GLP1 levels, without
affecting DPP4 activity, insulin and glucose levels,143 suggesting impaired GLP1
secretion during isoflurane anesthesia. However, the effect of volatile anesthetics on
GLP1 is scarcely studied and therefore no conclusion van be drawn.
Taken together, the above-discussed pharmacological interventions suggest that
improving insulin sensitivity, and thereby improving myocardial flexibility, may be
the most beneficial option in metabolically altered hearts in order to restore
cardioprotective mechanisms. However, according to current clinical practice, oral
hypoglycemic agents are usually withheld before surgery in order to avoid associated
adverse effects, such as perioperative hypoglycemia or lactic acidosis. Therefore the
(clinical) feasibility and safety of the proposed interventions should be carefully
studied and weighted against the potential risk of these adverse effects.
Metabolic disease and perioperative ischemia 35
Tab
le 2
.1:
Overv
iew
of
ph
arm
aco
log
ical
inte
rven
tion
s in
th
e e
xp
eri
men
tal
sett
ing
Dru
g
Ap
pli
cab
ilit
y
Ad
van
tag
es
Sid
e-e
ffect
s
Fatt
y a
cid
meta
boli
sm i
nh
ibit
ors
Eto
moxi
r T2D
M,
infa
rction
89-9
1
Stim
ula
tion g
luco
se o
xidat
ion
99
- Per
hex
iline
T2D
M,
infa
rction
92
Stim
ula
tion g
luco
se o
xidat
ion
- O
xfen
icin
e
T2D
M,
infa
rction
92,9
3
Stim
ula
tion g
luco
se o
xidat
ion
- Trim
etazi
din
e
T2D
M,
infa
rction
94,9
5
Stim
ula
tion g
luco
se o
xidat
ion
- Ran
ola
zine
T2D
M,
infa
rction
96,9
7
Stim
ula
tion g
luco
se o
xidat
ion
96
- D
ichlo
roac
etat
e T2D
M,
infa
rction
98
Stim
ula
tion g
luco
se o
xidat
ion
98
- In
suli
n
Glu
cose
-insu
lin-p
ota
ssiu
m
Infa
rction
103
Stim
ula
tion g
luco
se o
xidat
ion
Hyp
ogly
cem
ia
Insu
lin
T2D
M
Infa
rction
108,1
09
Red
uct
ion g
luco
se
Stim
ula
tion g
luco
se o
xidat
ion lev
els
Hyp
ogly
cem
ia
Hyp
ogly
cem
ia
PP
AR
ag
on
ists
T2D
M47
Infa
rction
115-1
17
Red
uct
ion lip
ids
Red
uct
ion lip
ids
Myo
pat
hy
M
yopat
hy
T2D
M121,1
22
Infa
rction
44,4
8,1
15,1
19,1
20
Insu
lin s
ensi
tize
r
Insu
lin s
ensi
tize
r In
crea
sed r
isk
hea
rt a
ttac
ks
Incr
ease
d r
isk
hea
rt a
ttac
ks
Big
uan
ide
Met
form
in
T2D
M,
infa
rction
125-1
28
Stim
ula
tion g
luco
se o
xidat
ion
Lact
ic a
cidosi
s G
LP
1
GLP
1
T2D
M,
infa
rction
130
Red
uct
ion g
luco
se
Short
hal
f-lif
e Exe
ndin
-4
T2D
M,
infa
rction
131
Red
uct
ion g
luco
se
Hyp
ogly
cem
ia
Exe
nat
ide
T2D
M,
infa
rction
132
Red
uct
ion g
luco
se
Hyp
ogly
cem
ia
Lira
glu
tide
T2D
M,
infa
rction
133,1
34
Red
uct
ion g
luco
se
Hyp
ogly
cem
ia
T2D
M,
type
2 d
iabet
es m
ellit
us;
PPA
R,
per
oxi
som
e pro
lifer
ators
-act
ivat
ed r
ecep
tor;
GLP
-1,
glu
cagon-l
ike
pep
tide
1.
2
36 Chapter 2
Preoperative health risk improvement
Based on 7 risk factors (physical inactivity, dietary pattern, obesity, smoking, high
cholesterol, hypertension and elevated blood glucose levels), the 2020 impact goal of
the American Heart Association is: "to improve the cardiovascular health by 20%
while reducing deaths from cardiovascular diseases and stroke by 20%".144 Another
possibility besides pharmacological intervention is preoperative lifestyle intervention,
such as changing the dietary intake and stimulation of physical activity thereby
losing weight and improving insulin sensitivity.
It has been shown by reducing dietary fat in rodents that diet-induced obesity is
reversible.145-147 In contrast, diet-induced obesity was not reversed by withdrawal of
an energy dense diet.148 Reversibility of diet-induced obesity is independent of the
duration of the obese state,146 whereas long-term diet feeding did not reversed
obesity.145 Overall, these data suggest that changing dietary intake may have
beneficial effects on health. However, there is only limited literature available that
describes the effects of changing dietary balance on the heart.
In western diet-fed rats, lowering caloric intake improved systolic and diastolic
function and prevented sevoflurane-induced cardiodepression (van den Brom et al.,
unpublished observations). Accordingly, pacing-induced cardioprotection was lost by
diet-induced hypercholesterolemia, but restored after reversion to control diet,149
whereas caloric restriction by itself in healthy rats also has cardioprotective
properties.150 In conclusion, restriction of dietary fat seems an effective treatment to
improve metabolic flexibility of the heart and thereby may be a possibility to reduce
perioperative risk.
Obesity and T2DM are closely related to physical inactivity, and exercise could be a
possible lifestyle intervention to reduce perioperative risk. The benefits of exercise
with respect to obesity and T2DM are already recognized clinically.151 However, the
effects of exercise on myocardial infarction are contradictory. Exercise did not reduce
myocardial ischemic injury in rats,152 whereas others showed that exercise had
protective effects in rat hearts.153-155 The question remains if exercise has beneficial
effects in obese and T2DM on myocardial function and ischemia and reperfusion
injury. Exercise was shown to reverse diet-induced obesity, insulin resistance and
cardiomyocyte dysfunction,147 however, the effects of exercise on myocardial
infarction in obese and T2DM with and without the effects of volatile anesthesia is
not known. Based on the above described results exercise might be a possible
lifestyle intervention to reduce perioperative risk.
Metabolic disease and perioperative ischemia 37
Conclusions
Over the years, several mechanisms that are involved in anesthesia-induced
cardioprotection have been evaluated in the experimental setting. The existing
evidence suggests that the obese and/or T2DM heart is less adaptable to
cardioprotective interventions and that anesthesia-induced cardioprotection is just a
Differences between experimental models, the type of metabolic disease and the
severity of myocardial substrate derangements challenge the identification of
unifying mechanisms related to anesthesia-induced cardioprotection in cases of
obesity and T2DM. It might be deduced that interventional options should focus on
recovery of the metabolic flexibility of the heart, especially by improving insulin
sensitivity. Although changing lifestyle seems promising to reduce the susceptibility
of the heart to intraoperative ischemia and reperfusion injury, experimental data has
not been translated into clinical data. Therefore more studies are required to
elucidate whether these interventions have beneficial effects on perioperative
outcome.
2
38 Chapter 2
References
1. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, Freeman WK,
Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF, Smith SC, Jr., Jacobs AK, Adams CD,
Anderson JL, Antman EM, Buller CE, Creager MA, Ettinger SM, Faxon DP, Fuster V, Halperin JL,
Hiratzka LF, Hunt SA et al.: ACC/AHA 2007 guidelines on perioperative cardiovascular
evaluation and care for noncardiac surgery: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to
Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery):
developed in collaboration with the American Society of Echocardiography, American Society of
Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society
for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology,
and Society for Vascular Surgery. Circulation 2007, 116:e418-e499.
2. Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, Esterbrooks DJ, Hunter CB,
Pipinos II, Johanning JM, Lynch TG, Forse RA, Mohiuddin SM, Mooss AN: Development and
validation of a risk calculator for prediction of cardiac risk after surgery. Circulation 2011,
124:381-387.
3. Unwin N, Whiting D, Guariguata L, Hennis A, Husseini A, Ji L, Kissimova-Skarbek K, Libman I,
Mayer-Davis E, Motala A, Narayan V, Ramachandran A, Roglic G, Sham J, Wareham N, Zhang P.
IDF diabetes atlas 2011. 5th ed. Brussels: International Diabetes Federation; 2011.
4. Preis SR, Pencina MJ, Hwang SJ, D'Agostino RB, Sr., Savage PJ, Levy D, Fox CS: Trends in
cardiovascular disease risk factors in individuals with and without diabetes mellitus in the
Framingham Heart Study. Circulation 2009, 120:212-220.
5. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ,
Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L: Derivation and prospective
validation of a simple index for prediction of cardiac risk of major noncardiac surgery.
Circulation 1999, 100:1043-1049.
6. Frassdorf J, De Hert S, Schlack W: Anaesthesia and myocardial ischaemia/reperfusion injury. Br
J Anaesth 2009, 103:89-98.
7. De Hert SG, Preckel B, Hollmann MW, Schlack WS: Drugs mediating myocardial protection. Eur
J Anaesthesiol 2009, 26:985-995.
8. Huhn R, Heinen A, Hollmann MW, Schlack W, Preckel B, Weber NC: Cyclosporine A administered
during reperfusion fails to restore cardioprotection in prediabetic Zucker obese rats in vivo. Nutr
Metab Cardiovasc Dis 2010, 20:706-712.
9. Kehl F, Krolikowski JG, Mraovic B, Pagel PS, Warltier DC, Kersten JR: Hyperglycemia prevents
isoflurane-induced preconditioning against myocardial infarction. Anesthesiology 2002, 96:183-
188.
10.Lucchinetti E, Wang L, Ko KW, Troxler H, Hersberger M, Zhang L, Omar MA, Lopaschuk GD,
Clanachan AS, Zaugg M: Enhanced glucose uptake via GLUT4 fuels recovery from calcium
overload after ischaemia-reperfusion injury in sevoflurane- but not propofol-treated hearts. Br J
Anaesth 2011, 106:792-800.
11.Lucchinetti E, Hofer C, Bestmann L, Hersberger M, Feng J, Zhu M, Furrer L, Schaub MC, Tavakoli
R, Genoni M, Zollinger A, Zaugg M: Gene regulatory control of myocardial energy metabolism
predicts postoperative cardiac function in patients undergoing off-pump coronary artery bypass
graft surgery: inhalational versus intravenous anesthetics. Anesthesiology 2007, 106:444-457.
12.Wang L, Ko KW, Lucchinetti E, Zhang L, Troxler H, Hersberger M, Omar MA, Posse de Chaves
EI, Lopaschuk GD, Clanachan AS, Zaugg M: Metabolic profiling of hearts exposed to sevoflurane
Metabolic disease and perioperative ischemia 39
and propofol reveals distinct regulation of fatty acid and glucose oxidation: CD36 and pyruvate
dehydrogenase as key regulators in anesthetic-induced fuel shift. Anesthesiology 2010,
113:541-551.
13.Winterstein H: Ueber die Sauerstoffatmung des isolierten Saeugetierherzens. Z Allg Physiol
1904, 4:339-359.
14.Stanley WC, Lopaschuk GD, McCormack JG: Regulation of energy substrate metabolism in the
diabetic heart. Cardiovasc Res 1997, 34:25-33.
15.Carley AN, Severson DL: Fatty acid metabolism is enhanced in type 2 diabetic hearts. Biochim
Biophys Acta 2005, 1734:112-126.
16.Neely JR, Rovetto MJ, Oram JF: Myocardial utilization of carbohydrate and lipids. Prog
Cardiovasc Dis 1972, 15:289-329.
17.Taegtmeyer H: Glycogen in the heart--an expanded view. J Mol Cell Cardiol 2004, 37:7-10.
18.Shepherd PR, Kahn BB: Glucose transporters and insulin action--implications for insulin
resistance and diabetes mellitus. N Engl J Med 1999, 341:248-257.
19.Coort SL, Bonen A, van der Vusse GJ, Glatz JF, Luiken JJ: Cardiac substrate uptake and
metabolism in obesity and type-2 diabetes: role of sarcolemmal substrate transporters. Mol Cell
Biochem 2007, 299:5-18.
20.Lewin TM, Coleman RA: Regulation of myocardial triacylglycerol synthesis and metabolism.
Biochim Biophys Acta 2003, 1634:63-75.
21.Kerner J, Hoppel C: Fatty acid import into mitochondria. Biochim Biophys Acta 2000, 1486:1-
17.
22.Stanley WC, Recchia FA, Lopaschuk GD: Myocardial substrate metabolism in the normal and
failing heart. Physiol Rev 2005, 85:1093-1129.
23.Saddik M, Lopaschuk GD: Myocardial triglyceride turnover and contribution to energy substrate
utilization in isolated working rat hearts. J Biol Chem 1991, 266:8162-8170.
24.Lopaschuk GD, Ussher JR, Folmes CD, Jaswal JS, Stanley WC: Myocardial fatty acid metabolism
in health and disease. Physiol Rev 2010, 90:207-258.
25.van den Brom CE, Bosmans JW, Vlasblom R, Handoko ML, Huisman MC, Lubberink M, Molthoff
CF, Lammertsma AA, Ouwens DM, Diamant M, Boer C: Diabetic cardiomyopathy in Zucker
diabetic fatty rats: the forgotten right ventricle. Cardiovasc Diabetol 2010, 9:25.
26.van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009,
8:39.
27.Jaswal JS, Keung W, Wang W, Ussher JR, Lopaschuk GD: Targeting fatty acid and carbohydrate
oxidation--a novel therapeutic intervention in the ischemic and failing heart. Biochim Biophys
Acta 2011, 1813:1333-1350.
28.Opie LH. The heart: Physiology and Metabolism. New York Raven Press; 1991.
29.Kannel WB, Hjortland M, Castelli WP: Role of diabetes in congestive heart failure: the
Framingham study. Am J Cardiol 1974, 34:29-34.
30.Rennert G, Saltz-Rennert H, Wanderman K, Weitzman S: Size of acute myocardial infarcts in
patients with diabetes mellitus. Am J Cardiol 1985, 55:1629-1630.
31.How OJ, Aasum E, Severson DL, Chan WY, Essop MF, Larsen TS: Increased myocardial oxygen
consumption reduces cardiac efficiency in diabetic mice. Diabetes 2006, 55:466-473.
32.Paulson DJ: The diabetic heart is more sensitive to ischemic injury. Cardiovasc Res 1997,
34:104-112.
2
40 Chapter 2
33.van den Brom CE, Bulte CS, Kloeze BM, Loer SA, Boer C, Bouwman RA: High fat diet-induced
glucose intolerance impairs myocardial function, but not myocardial perfusion during
hyperaemia: a pilot study. Cardiovasc Diabetol 2012, 11:74.
34.Ivanova M, Janega P, Matejikova J, Simoncikova P, Pancza D, Ravingerova T, Barancik M:
Activation of Akt kinase accompanies increased cardiac resistance to ischemia/reperfusion in
rats after short-term feeding with lard-based high-fat diet and increased sucrose intake. Nutr
Res 2011, 31:631-643.
35.Rennison JH, McElfresh TA, Chen X, Anand VR, Hoit BD, Hoppel CL, Chandler MP: Prolonged
exposure to high dietary lipids is not associated with lipotoxicity in heart failure. J Mol Cell
Cardiol 2009, 46:883-890.
36.Jordan JE, Simandle SA, Tulbert CD, Busija DW, Miller AW: Fructose-fed rats are protected
against ischemia/reperfusion injury. J Pharmacol Exp Ther 2003, 307:1007-1011.
37.Morgan EE, Rennison JH, Young ME, McElfresh TA, Kung TA, Tserng KY, Hoit BD, Stanley WC,
Chandler MP: Effects of chronic activation of peroxisome proliferator-activated receptor-alpha or
high-fat feeding in a rat infarct model of heart failure. Am J Physiol Heart Circ Physiol 2006,
290:H1899-H1904.
38.Rennison JH, McElfresh TA, Okere IC, Vazquez EJ, Patel HV, Foster AB, Patel KK, Chen Q, Hoit
BD, Tserng KY, Hassan MO, Hoppel CL, Chandler MP: High-fat diet postinfarction enhances
mitochondrial function and does not exacerbate left ventricular dysfunction. Am J Physiol Heart
Circ Physiol 2007, 292:H1498-H1506.
39.Mozaffari MS, Patel C, Ballas C, Schaffer SW: Effects of excess salt and fat intake on myocardial
function and infarct size in rat. Life Sci 2006, 78:1808-1813.
40.Berthiaume JM, Young ME, Chen X, McElfresh TA, Yu X, Chandler MP: Normalizing the metabolic
phenotype after myocardial infarction: impact of subchronic high fat feeding. J Mol Cell Cardiol
2012, 53:125-133.
41.Song T, Lv LY, Xu J, Tian ZY, Cui WY, Wang QS, Qu G, Shi XM: Diet-induced obesity suppresses
sevoflurane preconditioning against myocardial ischemia-reperfusion injury: role of AMP-
activated protein kinase pathway. Exp Biol Med (Maywood ) 2011, 236:1427-1436.
42.Morel S, Berthonneche C, Tanguy S, Toufektsian MC, Perret P, Ghezzi C, de Leiris J, Boucher F:
Early pre-diabetic state alters adaptation of myocardial glucose metabolism during ischemia in
rats. Mol Cell Biochem 2005, 272:9-17.
43.Maddaford TG, Russell JC, Pierce GN: Postischemic cardiac performance in the insulin-resistant
JCR:LA-cp rat. Am J Physiol 1997, 273:H1187-H1192.
44.Sidell RJ, Cole MA, Draper NJ, Desrois M, Buckingham RE, Clarke K: Thiazolidinedione treatment
normalizes insulin resistance and ischemic injury in the zucker Fatty rat heart. Diabetes 2002,
51:1110-1117.
45.Mozaffari MS, Schaffer SW: Myocardial ischemic-reperfusion injury in a rat model of metabolic
syndrome. Obesity (Silver Spring) 2008, 16:2253-2258.
46.Thakker GD, Frangogiannis NG, Zymek PT, Sharma S, Raya JL, Barger PM, Taegtmeyer H,
Entman ML, Ballantyne CM: Increased myocardial susceptibility to repetitive ischemia with high-
fat diet-induced obesity. Obesity (Silver Spring) 2008, 16:2593-2600.
47.Aasum E, Hafstad AD, Severson DL, Larsen TS: Age-dependent changes in metabolism,
contractile function, and ischemic sensitivity in hearts from db/db mice. Diabetes 2003, 52:434-
441.
48.Yue TL, Bao W, Gu JL, Cui J, Tao L, Ma XL, Ohlstein EH, Jucker BM: Rosiglitazone treatment in
Zucker diabetic Fatty rats is associated with ameliorated cardiac insulin resistance and
protection from ischemia/reperfusion-induced myocardial injury. Diabetes 2005, 54:554-562.
Metabolic disease and perioperative ischemia 41
49.Wang P, Chatham JC: Onset of diabetes in Zucker diabetic fatty (ZDF) rats leads to improved
recovery of function after ischemia in the isolated perfused heart. Am J Physiol Endocrinol Metab
2004, 286:E725-E736.
50.Hoshida S, Yamashita N, Otsu K, Kuzuya T, Hori M: Cholesterol feeding exacerbates myocardial
injury in Zucker diabetic fatty rats. Am J Physiol Heart Circ Physiol 2000, 278:H256-H262.
51.Higuchi M, Miyagi K, Nakasone J, Sakanashi M: Role of high glycogen in underperfused diabetic
rat hearts with added norepinephrine. J Cardiovasc Pharmacol 1995, 26:899-907.
52.Cross HR, Opie LH, Radda GK, Clarke K: Is a high glycogen content beneficial or detrimental to
the ischemic rat heart? A controversy resolved. Circ Res 1996, 78:482-491.
53.Feuvray D, Lopaschuk GD: Controversies on the sensitivity of the diabetic heart to ischemic
injury: the sensitivity of the diabetic heart to ischemic injury is decreased. Cardiovasc Res 1997,
34:113-120.
54.Yao YT, Fang NX, Shi CX, Li LH: Sevoflurane postconditioning protects isolated rat hearts
against ischemia-reperfusion injury. Chin Med J (Engl ) 2010, 123:1320-1328.
55.Bouwman RA, Vreden MJ, Hamdani N, Wassenaar LE, Smeding L, Loer SA, Stienen GJ,
Lamberts RR: Effect of bupivacaine on sevoflurane-induced preconditioning in isolated rat
hearts. Eur J Pharmacol 2010, 647:132-138.
56.Tosaka S, Tosaka R, Matsumoto S, Maekawa T, Cho S, Sumikawa K: Roles of cyclooxygenase 2
in sevoflurane- and olprinone-induced early phase of preconditioning and postconditioning
against myocardial infarction in rat hearts. J Cardiovasc Pharmacol Ther 2011, 16:72-78.
57.Obal D, Dettwiler S, Favoccia C, Scharbatke H, Preckel B, Schlack W: The influence of
mitochondrial KATP-channels in the cardioprotection of preconditioning and postconditioning by
sevoflurane in the rat in vivo. Anesth Analg 2005, 101:1252-1260.
58.Lang XE, Wang X, Jin JH: Mechanisms of cardioprotection by isoflurane against I/R injury. Front
Biosci 2013, 18:387-393.
59.Yao Y, Li L, Li L, Gao C, Shi C: Sevoflurane postconditioning protects chronically-infarcted rat
hearts against ischemia-reperfusion injury by activation of pro-survival kinases and inhibition of
mitochondrial permeability transition pore opening upon reperfusion. Biol Pharm Bull 2009,
32:1854-1861.
60.Stadnicka A, Marinovic J, Ljubkovic M, Bienengraeber MW, Bosnjak ZJ: Volatile anesthetic-
induced cardiac preconditioning. J Anesth 2007, 21:212-219.
61.Lattermann R, Schricker T, Wachter U, Georgieff M, Goertz A: Understanding the mechanisms
by which isoflurane modifies the hyperglycemic response to surgery. Anesth Analg 2001,
93:121-127.
62.Bouwman RA, Musters RJ, van Beek-Harmsen BJ, de Lange JJ, Boer C: Reactive oxygen species
precede protein kinase C-delta activation independent of adenosine triphosphate-sensitive
mitochondrial channel opening in sevoflurane-induced cardioprotection. Anesthesiology 2004,
100:506-514.
63.Costa AD, Quinlan CL, Andrukhiv A, West IC, Jaburek M, Garlid KD: The direct physiological
effects of mitoK(ATP) opening on heart mitochondria. Am J Physiol Heart Circ Physiol 2006,
290:H406-H415.
64.Flores JE, McFarland LM, Vanderbilt A, Ogasawara AK, Williams SP: The effects of anesthetic
agent and carrier gas on blood glucose and tissue uptake in mice undergoing dynamic FDG-PET
imaging: sevoflurane and isoflurane compared in air and in oxygen. Mol Imaging Biol 2008,
10:192-200.
65.Toyama H, Ichise M, Liow JS, Vines DC, Seneca NM, Modell KJ, Seidel J, Green MV, Innis RB:
Evaluation of anesthesia effects on [18F]FDG uptake in mouse brain and heart using small
animal PET. Nucl Med Biol 2004, 31:251-256.
2
42 Chapter 2
66.Kudoh A, Katagai H, Takazawa T: Sevoflurane increases glucose transport in skeletal muscle
cells. Anesth Analg 2002, 95:123-8.
67.Ewart RB, Rusy BF, Bradford MW: Effects of enflurane on release of insulin by pancreatic islets
in vitro. Anesth Analg 1981, 60:878-884.
68.Tanaka K, Kawano T, Tsutsumi YM, Kinoshita M, Kakuta N, Hirose K, Kimura M, Oshita S:
Differential effects of propofol and isoflurane on glucose utilization and insulin secretion. Life Sci
2011, 88:96-103.
69.Zuurbier CJ, Keijzers PJ, Koeman A, Van Wezel HB, Hollmann MW: Anesthesia's effects on
plasma glucose and insulin and cardiac hexokinase at similar hemodynamics and without major
surgical stress in fed rats. Anesth Analg 2008, 106:135-42.
70.Kitamura T, Ogawa M, Kawamura G, Sato K, Yamada Y: The effects of sevoflurane and propofol
on glucose metabolism under aerobic conditions in fed rats. Anesth Analg 2009, 109:1479-
1485.
71.Kosiborod M, Rathore SS, Inzucchi SE, Masoudi FA, Wang Y, Havranek EP, Krumholz HM:
Admission glucose and mortality in elderly patients hospitalized with acute myocardial
infarction: implications for patients with and without recognized diabetes. Circulation 2005,
111:3078-3086.
72.Katakam PV, Jordan JE, Snipes JA, Tulbert CD, Miller AW, Busija DW: Myocardial
preconditioning against ischemia-reperfusion injury is abolished in Zucker obese rats with
insulin resistance. Am J Physiol Regul Integr Comp Physiol 2007, 292:R920-R926.
73.Wagner C, Kloeting I, Strasser RH, Weinbrenner C: Cardioprotection by postconditioning is lost
in WOKW rats with metabolic syndrome: role of glycogen synthase kinase 3beta. J Cardiovasc
Pharmacol 2008, 52:430-437.
74.Ferdinandy P, Szilvassy Z, Horvath LI, Csont T, Csonka C, Nagy E, Szentgyorgyi R, Nagy I,
Koltai M, Dux L: Loss of pacing-induced preconditioning in rat hearts: role of nitric oxide and
cholesterol-enriched diet. J Mol Cell Cardiol 1997, 29:3321-3333.
75.Kocic I, Konstanski Z, Kaminski M, Dworakowska D, Dworakowski R: Experimental
hyperlipidemia prevents the protective effect of ischemic preconditioning on the contractility and
responsiveness to phenylephrine of rat-isolated stunned papillary muscle. Gen Pharmacol 1999,
33:213-219.
76.Zhang FJ, Ma LL, Wang WN, Qian LB, Yang MJ, Yu J, Chen G, Yu LN, Yan M:
Hypercholesterolemia abrogates sevoflurane-induced delayed preconditioning against
myocardial infarct in rats by alteration of nitric oxide synthase signaling. Shock 2012, 37:485-
491.
77.Malmberg K, Norhammar A, Wedel H, Ryden L: Glycometabolic state at admission: important
risk marker of mortality in conventionally treated patients with diabetes mellitus and acute
myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute
Myocardial Infarction (DIGAMI) study. Circulation 1999, 99:2626-2632.
78.Weber NC, Goletz C, Huhn R, Grueber Y, Preckel B, Schlack W, Ebel D: Blockade of anaesthetic-
induced preconditioning in the hyperglycaemic myocardium: the regulation of different mitogen-
activated protein kinases. Eur J Pharmacol 2008, 592:48-54.
79.Kehl F, Krolikowski JG, Weihrauch D, Pagel PS, Warltier DC, Kersten JR: N-acetylcysteine
restores isoflurane-induced preconditioning against myocardial infarction during hyperglycemia.
Anesthesiology 2003, 98:1384-1390.
80.Huhn R, Heinen A, Weber NC, Hollmann MW, Schlack W, Preckel B: Hyperglycaemia blocks
sevoflurane-induced postconditioning in the rat heart in vivo: cardioprotection can be restored
by blocking the mitochondrial permeability transition pore. Br J Anaesth 2008, 100:465-471.
Metabolic disease and perioperative ischemia 43
81.Kersten JR, Toller WG, Gross ER, Pagel PS, Warltier DC: Diabetes abolishes ischemic
preconditioning: role of glucose, insulin, and osmolality. Am J Physiol Heart Circ Physiol 2000,
278:H1218-H1224.
82.Tanaka K, Kehl F, Gu W, Krolikowski JG, Pagel PS, Warltier DC, Kersten JR: Isoflurane-induced
preconditioning is attenuated by diabetes. Am J Physiol Heart Circ Physiol 2002, 282:H2018-
H2023.
83.Raphael J, Gozal Y, Navot N, Zuo Z: Hyperglycemia inhibits anesthetic-induced postconditioning
in the rabbit heart via modulation of phosphatidylinositol-3-kinase/Akt and endothelial nitric
oxide synthase signaling. J Cardiovasc Pharmacol 2010, 55:348-357.
84.Kristiansen SB, Lofgren B, Stottrup NB, Khatir D, Nielsen-Kudsk JE, Nielsen TT, Botker HE,
Flyvbjerg A: Ischaemic preconditioning does not protect the heart in obese and lean animal
models of type 2 diabetes. Diabetologia 2004, 47:1716-1721.
85.Miki T, Itoh T, Sunaga D, Miura T: Effects of diabetes on myocardial infarct size and
cardioprotection by preconditioning and postconditioning. Cardiovasc Diabetol 2012, 11:67.
86.Tsang A, Hausenloy DJ, Mocanu MM, Carr RD, Yellon DM: Preconditioning the diabetic heart: the
importance of Akt phosphorylation. Diabetes 2005, 54:2360-2364.
87.Drenger B, Ostrovsky IA, Barak M, Nechemia-Arbely Y, Ziv E, Axelrod JH: Diabetes Blockade of
Sevoflurane Postconditioning Is Not Restored by Insulin in the Rat Heart: Phosphorylated Signal
Transducer and Activator of Transcription 3- and Phosphatidylinositol 3-Kinase-mediated
Inhibition. Anesthesiology 2011, 114:1364-1372.
88.Paiva MA, Rutter-Locher Z, Goncalves LM, Providencia LA, Davidson SM, Yellon DM, Mocanu
MM: Enhancing AMPK activation during ischemia protects the diabetic heart against reperfusion
injury. Am J Physiol Heart Circ Physiol 2011, 300:H2123-H2134.
89.Penna C, Mancardi D, Gattullo D, Pagliaro P: Myocardial protection from ischemic
preconditioning is not blocked by sub-chronic inhibition of carnitine palmitoyltransferase I. Life
Sci 2005, 77:2004-2017.
90.Lopaschuk GD, Spafford MA, Davies NJ, Wall SR: Glucose and palmitate oxidation in isolated
working rat hearts reperfused after a period of transient global ischemia. Circ Res 1990,
66:546-553.
91.Lopaschuk GD, Saddik M: The relative contribution of glucose and fatty acids to ATP production
in hearts reperfused following ischemia. Mol Cell Biochem 1992, 116:111-116.
92.Kennedy JA, Kiosoglous AJ, Murphy GA, Pelle MA, Horowitz JD: Effect of perhexiline and
oxfenicine on myocardial function and metabolism during low-flow ischemia/reperfusion in the
isolated rat heart. J Cardiovasc Pharmacol 2000, 36:794-801.
93.Molaparast-Saless F, Liedtke AJ, Nellis SH: Effects of the fatty acid blocking agents, oxfenicine
and 4-bromocrotonic acid, on performance in aerobic and ischemic myocardium. J Mol Cell
Cardiol 1987, 19:509-520.
94.Kara AF, Demiryurek S, Celik A, Tarakcioglu M, Demiryurek AT: Effects of trimetazidine on
myocardial preconditioning in anesthetized rats. Eur J Pharmacol 2004, 503:135-145.
95.Mouquet F, Rousseau D, Domergue-Dupont V, Grynberg A, Liao R: Effects of trimetazidine, a
partial inhibitor of fatty acid oxidation, on ventricular function and survival after myocardial
infarction and reperfusion in the rat. Fundam Clin Pharmacol 2010, 24:469-476.
96.McCormack JG, Barr RL, Wolff AA, Lopaschuk GD: Ranolazine stimulates glucose oxidation in
normoxic, ischemic, and reperfused ischemic rat hearts. Circulation 1996, 93:135-142.
97.Wang P, Fraser H, Lloyd SG, McVeigh JJ, Belardinelli L, Chatham JC: A comparison between
ranolazine and CVT-4325, a novel inhibitor of fatty acid oxidation, on cardiac metabolism and
left ventricular function in rat isolated perfused heart during ischemia and reperfusion. J
Pharmacol Exp Ther 2007, 321:213-220.
2
44 Chapter 2
98.McVeigh JJ, Lopaschuk GD: Dichloroacetate stimulation of glucose oxidation improves recovery
of ischemic rat hearts. Am J Physiol 1990, 259:H1079-H1085.
99.Lopaschuk GD, McNeil GF, McVeigh JJ: Glucose oxidation is stimulated in reperfused ischemic
hearts with the carnitine palmitoyltransferase 1 inhibitor, Etomoxir. Mol Cell Biochem 1989,
88:175-179.
100.Diaz R, Paolasso EA, Piegas LS, Tajer CD, Moreno MG, Corvalan R, Isea JE, Romero G:
Metabolic modulation of acute myocardial infarction. The ECLA (Estudios Cardiologicos
Latinoamerica) Collaborative Group. Circulation 1998, 98:2227-2234.
101.Di MS, Boldrini B, Conti U, Marcucci G, Morgantini C, Ferrannini E, Natali A: Effects of GIK
(glucose-insulin-potassium) on stress-induced myocardial ischaemia. Clin Sci (Lond) 2010,
119:37-44.
102.Malmberg K, Ryden L, Hamsten A, Herlitz J, Waldenstrom A, Wedel H: Effects of insulin
treatment on cause-specific one-year mortality and morbidity in diabetic patients with acute
myocardial infarction. DIGAMI Study Group. Diabetes Insulin-Glucose in Acute Myocardial
Infarction. Eur Heart J 1996, 17:1337-1344.
103.Jonassen AK, Aasum E, Riemersma RA, Mjos OD, Larsen TS: Glucose-insulin-potassium
reduces infarct size when administered during reperfusion. Cardiovasc Drugs Ther 2000,
14:615-623.
104.Ceremuzynski L, Budaj A, Czepiel A, Burzykowski T, Achremczyk P, Smielak-Korombel W,
Maciejewicz J, Dziubinska J, Nartowicz E, Kawka-Urbanek T, Piotrowski W, Hanzlik J, Cieslinski
A, Kawecka-Jaszcz K, Gessek J, Wrabec K: Low-dose glucose-insulin-potassium is ineffective
in acute myocardial infarction: results of a randomized multicenter Pol-GIK trial. Cardiovasc
Drugs Ther 1999, 13:191-200.
105.van der Horst IC, Zijlstra F, van 't Hof AW, Doggen CJ, de Boer MJ, Suryapranata H, Hoorntje
JC, Dambrink JH, Gans RO, Bilo HJ: Glucose-insulin-potassium infusion inpatients treated with
primary angioplasty for acute myocardial infarction: the glucose-insulin-potassium study: a
randomized trial. J Am Coll Cardiol 2003, 42:784-791.
106.Thomas DJ, Platt HS, Alberti KG: Insulin infusion (GIK) in the treatment of type 2 (non-insulin
dependent) diabetes during the perioperative period. Br J Surg 1986, 73:898-901.
107.Lazar HL, Chipkin SR, Fitzgerald CA, Bao Y, Cabral H, Apstein CS: Tight glycemic control in
diabetic coronary artery bypass graft patients improves perioperative outcomes and decreases
recurrent ischemic events. Circulation 2004, 109:1497-1502.
108.Doenst T, Richwine RT, Bray MS, Goodwin GW, Frazier OH, Taegtmeyer H: Insulin improves
functional and metabolic recovery of reperfused working rat heart. Ann Thorac Surg 1999,
67:1682-1688.
109.Jonassen AK, Sack MN, Mjos OD, Yellon DM: Myocardial protection by insulin at reperfusion
requires early administration and is mediated via Akt and p70s6 kinase cell-survival signaling.
Circ Res 2001, 89:1191-1198.
110.Nygren JO, Thorell A, Soop M, Efendic S, Brismar K, Karpe F, Nair KS, Ljungqvist O:
Perioperative insulin and glucose infusion maintains normal insulin sensitivity after surgery.
Am J Physiol 1998, 275:E140-E148.
111.Sato H, Carvalho G, Sato T, Bracco D, Codere-Maruyama T, Lattermann R, Hatzakorzian R,
Matsukawa T, Schricker T: Perioperative tight glucose control with hyperinsulinemic-
normoglycemic clamp technique in cardiac surgery. Nutrition 2010, 26:1122-1129.
112.Carvalho G, Moore A, Qizilbash B, Lachapelle K, Schricker T: Maintenance of normoglycemia
during cardiac surgery. Anesth Analg 2004, 99:319-24.
Metabolic disease and perioperative ischemia 45
113.Zuurbier CJ, Hoek FJ, van Dijk J, Abeling NG, Meijers JC, Levels JH, de Jonge E, de Mol BA,
Van Wezel HB: Perioperative hyperinsulinaemic normoglycaemic clamp causes hypolipidaemia
after coronary artery surgery. Br J Anaesth 2008, 100:442-450.
114.Forlani S, Tomai F, De Paulis R, Turani F, Colella DF, Nardi P, De Notaris S, Moscarelli M,
Magliano G, Crea F, Chiariello L: Preoperative shift from glibenclamide to insulin is
cardioprotective in diabetic patients undergoing coronary artery bypass surgery. J Cardiovasc
Surg (Torino) 2004, 45:117-122.
115.Wayman NS, Hattori Y, McDonald MC, Mota-Filipe H, Cuzzocrea S, Pisano B, Chatterjee PK,
Thiemermann C: Ligands of the peroxisome proliferator-activated receptors (PPAR-gamma and
PPAR-alpha) reduce myocardial infarct size. FASEB J 2002, 16:1027-1040.
116.Yue TL, Bao W, Jucker BM, Gu JL, Romanic AM, Brown PJ, Cui J, Thudium DT, Boyce R, Burns-
Kurtis CL, Mirabile RC, Aravindhan K, Ohlstein EH: Activation of peroxisome proliferator-
activated receptor-alpha protects the heart from ischemia/reperfusion injury. Circulation 2003,
108:2393-2399.
117.Bulhak AA, Jung C, Ostenson CG, Lundberg JO, Sjoquist PO, Pernow J: PPAR-alpha activation
protects the type 2 diabetic myocardium against ischemia-reperfusion injury: involvement of
the PI3-Kinase/Akt and NO pathway. Am J Physiol Heart Circ Physiol 2009, 296:H719-H727.
118.Lucchinetti E, Aguirre J, Feng J, Zhu M, Suter M, Spahn DR, Harter L, Zaugg M: Molecular
evidence of late preconditioning after sevoflurane inhalation in healthy volunteers. Anesth
Analg 2007, 105:629-640.
119.Yue TL, Chen J, Bao W, Narayanan PK, Bril A, Jiang W, Lysko PG, Gu JL, Boyce R, Zimmerman
DM, Hart TK, Buckingham RE, Ohlstein EH: In vivo myocardial protection from
ischemia/reperfusion injury by the peroxisome proliferator-activated receptor-gamma agonist
rosiglitazone. Circulation 2001, 104:2588-2594.
120.Ito H, Nakano A, Kinoshita M, Matsumori A: Pioglitazone, a peroxisome proliferator-activated
receptor-gamma agonist, attenuates myocardial ischemia/reperfusion injury in a rat model.
Lab Invest 2003, 83:1715-1721.
121.Khandoudi N, Delerive P, Berrebi-Bertrand I, Buckingham RE, Staels B, Bril A: Rosiglitazone, a
peroxisome proliferator-activated receptor-gamma, inhibits the Jun NH(2)-terminal
kinase/activating protein 1 pathway and protects the heart from ischemia/reperfusion injury.
Diabetes 2002, 51:1507-1514.
122.Shoghi KI, Finck BN, Schechtman KB, Sharp T, Herrero P, Gropler RJ, Welch MJ: In vivo
metabolic phenotyping of myocardial substrate metabolism in rodents: differential efficacy of
metformin and rosiglitazone monotherapy. Circ Cardiovasc Imaging 2009, 2:373-381.
123.Lotz C, Lange M, Redel A, Stumpner J, Schmidt J, Tischer-Zeitz T, Roewer N, Kehl F:
Peroxisome-proliferator-activated receptor gamma mediates the second window of
anaesthetic-induced preconditioning. Exp Physiol 2011, 96:317-324.
124.Russell RR, III, Li J, Coven DL, Pypaert M, Zechner C, Palmeri M, Giordano FJ, Mu J, Birnbaum
MJ, Young LH: AMP-activated protein kinase mediates ischemic glucose uptake and prevents
postischemic cardiac dysfunction, apoptosis, and injury. J Clin Invest 2004, 114:495-503.
125.Calvert JW, Gundewar S, Jha S, Greer JJ, Bestermann WH, Tian R, Lefer DJ: Acute metformin
therapy confers cardioprotection against myocardial infarction via AMPK-eNOS-mediated
signaling. Diabetes 2008, 57:696-705.
126.Yin M, van der Horst I, van Melle JP, Qian C, van Gilst WH, Sillje HH, de Boer RA: Metformin
improves cardiac function in a non-diabetic rat model of post-MI heart failure. Am J Physiol
Heart Circ Physiol 2011, 301:459-468.
2
46 Chapter 2
127.Paiva MA, Goncalves LM, Providencia LA, Davidson SM, Yellon DM, Mocanu MM: Transitory
activation of AMPK at reperfusion protects the ischaemic-reperfused rat myocardium against
infarction. Cardiovasc Drugs Ther 2010, 24:25-32.
128.Lavanchy N, Christe G, Cand F, Wiernsperger N, Verdetti J: Effects of chronic treatment with
glibenclamide and/or metformin on the resistance to ischaemia of isolated hearts from Zucker
diabetic fatty rats (ZDF/GMI-fa/fa). Br J Diabetes Vasc Dis 2003, 3:375-380.
129.Lamberts RR, Onderwater G, Hamdani N, Vreden MJ, Steenhuisen J, Eringa EC, Loer SA,
Stienen GJ, Bouwman RA: Reactive oxygen species-induced stimulation of 5'AMP-activated
protein kinase mediates sevoflurane-induced cardioprotection. Circulation 2009, 120:S10-S15.
130.Bose AK, Mocanu MM, Carr RD, Brand CL, Yellon DM: Glucagon-like peptide 1 can directly
protect the heart against ischemia/reperfusion injury. Diabetes 2005, 54:146-151.
131.Sonne DP, Engstrom T, Treiman M: Protective effects of GLP-1 analogues exendin-4 and GLP-
1(9-36) amide against ischemia-reperfusion injury in rat heart. Regul Pept 2008, 146:243-
249.
132.Timmers L, Henriques JP, de Kleijn DP, Devries JH, Kemperman H, Steendijk P, Verlaan CW,
Kerver M, Piek JJ, Doevendans PA, Pasterkamp G, Hoefer IE: Exenatide reduces infarct size
and improves cardiac function in a porcine model of ischemia and reperfusion injury. J Am Coll
Cardiol 2009, 53:501-510.
133.Noyan-Ashraf MH, Momen MA, Ban K, Sadi AM, Zhou YQ, Riazi AM, Baggio LL, Henkelman RM,
Husain M, Drucker DJ: GLP-1R agonist liraglutide activates cytoprotective pathways and
improves outcomes after experimental myocardial infarction in mice. Diabetes 2009, 58:975-
983.
134.Kristensen J, Mortensen UM, Schmidt M, Nielsen PH, Nielsen TT, Maeng M: Lack of
cardioprotection from subcutaneously and preischemic administered liraglutide in a closed
chest porcine ischemia reperfusion model. BMC Cardiovasc Disord 2009, 9:31.
135.Sauve M, Ban K, Momen MA, Zhou YQ, Henkelman RM, Husain M, Drucker DJ: Genetic deletion
or pharmacological inhibition of dipeptidyl peptidase-4 improves cardiovascular outcomes after
myocardial infarction in mice. Diabetes 2010, 59:1063-1073.
136.Ravassa S, Zudaire A, Diez J: GLP-1 and cardioprotection: from bench to bedside. Cardiovasc
Res 2012, 94:316-323.
137.Ban K, Noyan-Ashraf MH, Hoefer J, Bolz SS, Drucker DJ, Husain M: Cardioprotective and
vasodilatory actions of glucagon-like peptide 1 receptor are mediated through both glucagon-
like peptide 1 receptor-dependent and -independent pathways. Circulation 2008, 117:2340-
2350.
138.Zhao T, Parikh P, Bhashyam S, Bolukoglu H, Poornima I, Shen YT, Shannon RP: Direct effects
of glucagon-like peptide-1 on myocardial contractility and glucose uptake in normal and
postischemic isolated rat hearts. J Pharmacol Exp Ther 2006, 317:1106-1113.
139.Poornima I, Brown SB, Bhashyam S, Parikh P, Bolukoglu H, Shannon RP: Chronic glucagon-
like-peptide-1 infusion sustains left ventricular systolic function and prolongs survival in the
spontaneosly hypertensive, heart failure prone rat. Circ Heart Fail 2008, 1:153-160.
140.Wang D, Luo P, Wang Y, Li W, Wang C, Sun D, Zhang R, Su T, Ma X, Zeng C, Wang H, Ren J,
Cao F: Glucagon-Like Peptide-1 Protects Against Cardiac Microvascular Injury in Diabetes Via a
cAMP/PKA/Rho-Dependent Mechanism. Diabetes 2013.
141.Vyas AK, Yang KC, Woo D, Tzekov A, Kovacs A, Jay PY, Hruz PW: Exenatide improves glucose
homeostasis and prolongs survival in a murine model of dilated cardiomyopathy. PLoS One
2011, 6:e17178.
142.Gejl M, Sondergaard HM, Stecher C, Bibby BM, Moller N, Botker HE, Hansen SB, Gjedde A,
Rungby J, Brock B: Exenatide alters myocardial glucose transport and uptake depending on

Metabolic disease and perioperative ischemia 47
insulin resistance and increases myocardial blood flow in patients with type 2 diabetes. J Clin
Endocrinol Metab 2012, 97:E1165-E1169.
143.Kawano T, Tanaka K, Chi H, Eguchi S, Yamazaki F, Kitamura S, Kumagai N, Yokoyama M:
Biophysical and pharmacological properties of glucagon-like peptide-1 in rats under isoflurane
anesthesia. Anesth Analg 2012, 115:62-69.
144.Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van HL, Greenlund K, Daniels S,
Nichol G, Tomaselli GF, Arnett DK, Fonarow GC, Ho PM, Lauer MS, Masoudi FA, Robertson RM,
Roger V, Schwamm LH, Sorlie P, Yancy CW, Rosamond WD: Defining and setting national
goals for cardiovascular health promotion and disease reduction: the American Heart
Association's strategic Impact Goal through 2020 and beyond. Circulation 2010, 121:586-613.
145.Hill JO, Dorton J, Sykes MN, DiGirolamo M: Reversal of dietary obesity is influenced by its
duration and severity. Int J Obes 1989, 13:711-722.
146.Bartness TJ, Polk DR, McGriff WR, Youngstrom TG, DiGirolamo M: Reversal of high-fat diet-
induced obesity in female rats. Am J Physiol 1992, 263:R790-R797.
147.Davidoff AJ, Mason MM, Davidson MB, Carmody MW, Hintz KK, Wold LE, Podolin DA, Ren J:
Sucrose-induced cardiomyocyte dysfunction is both preventable and reversible with clinically
relevant treatments. Am J Physiol Endocrinol Metab 2004, 286:E718-E724.
148.Llado I, Proenza AM, Serra F, Palou A, Pons A: Dietary-induced permanent changes in brown
and white adipose tissue composition in rats. Int J Obes 1991, 15:415-419.
149.Szilvassy Z, Ferdinandy P, Szilvassy J, Nagy I, Karcsu S, Lonovics J, Dux L, Koltai M: The loss
of pacing-induced preconditioning in atherosclerotic rabbits: role of hypercholesterolaemia. J
Mol Cell Cardiol 1995, 27:2559-2569.
150.Shinmura K, Tamaki K, Bolli R: Short-term caloric restriction improves ischemic tolerance
independent of opening of ATP-sensitive K+ channels in both young and aged hearts. J Mol
Cell Cardiol 2005, 39:285-296.
151.Hamdy O, Goodyear LJ, Horton ES: Diet and exercise in type 2 diabetes mellitus. Endocrinol
Metab Clin North Am 2001, 30:883-907.
152.Veiga EC, Antonio EL, Bocalini DS, Murad N, Abreu LC, Tucci PJ, Sato MA: Prior exercise
training does not prevent acute cardiac alterations after myocardial infarction in female rats.
Clinics (Sao Paulo) 2011, 66:889-893.
153.Burelle Y, Wambolt RB, Grist M, Parsons HL, Chow JC, Antler C, Bonen A, Keller A, Dunaway
GA, Popov KM, Hochachka PW, Allard MF: Regular exercise is associated with a protective
metabolic phenotype in the rat heart. Am J Physiol Heart Circ Physiol 2004, 287:H1055-
H1063.
154.McElroy CL, Gissen SA, Fishbein MC: Exercise-induced reduction in myocardial infarct size after
coronary artery occlusion in the rat. Circulation 1978, 57:958-962.
155.Freimann S, Scheinowitz M, Yekutieli D, Feinberg MS, Eldar M, Kessler-Icekson G: Prior
exercise training improves the outcome of acute myocardial infarction in the rat. Heart
structure, function, and gene expression. J Am Coll Cardiol 2005, 45:931-938.
2

CE van den Brom, CSE Bulte, BM Kloeze, SA Loer, C Boer,
RA Bouwman
Cardiovascular Diabetology 2012, 11:74
High fat diet-induced glucose intolerance
impairs myocardial function, but not
myocardial perfusion during hyperemia:
a pilot study
3

Myocardial function and perfusion during glucose intolerance 51
Abstract
Introduction
Glucose intolerance is a major health problem and is associated with increased risk
of progression to type 2 diabetes mellitus and cardiovascular disease. However,
whether glucose intolerance is related to impaired myocardial perfusion is not
known. The purpose of the present study was to study the effect of diet-induced
glucose intolerance on myocardial function and perfusion during baseline and
pharmacological induced hyperemia.
Methods
Male Wistar rats were randomly exposed to a high fat diet (HFD) or control diet (CD)
(n=8 per group). After 4 weeks, rats underwent an oral glucose tolerance test.
Subsequently, rats underwent (contrast) echocardiography to determine myocardial
function and perfusion during baseline and dipyridamole-induced hyperemia (20
mg/kg for 10 min).
Results
Four weeks of HFD feeding resulted in glucose intolerance compared to CD-feeding.
Contractile function as represented by fractional shortening was not altered in HFD-
fed rats compared to CD-fed rats under baseline conditions. However, dipyridamole
increased fractional shortening in CD-fed rats, but not in HFD-fed rats. Basal
myocardial perfusion, as measured by estimate of perfusion, was similar in CD- and
HFD-fed rats, whereas dipyridamole increased estimate of perfusion in CD-fed rats,
but not in HFD-fed rats. However, flow reserve was not different between CD- and
HFD-fed rats.
Conclusions
Diet-induced glucose intolerance is associated with impaired myocardial function
during conditions of hyperemia, but myocardial perfusion is maintained. These
findings may result in new insights into the effect of glucose intolerance on
myocardial function and perfusion during hyperemia.
3
52 Chapter 3
Introduction
Glucose intolerance defines the intermittent stage between transition from normal
glucose levels to type 2 diabetes mellitus.1 Glucose intolerance is a predictor of
cardiovascular disease2,3 and known to associate with vascular dysfunction and
consequent impairment of organ perfusion as one of the appearing consequences.4
Myocardial perfusion in combination with myocardial performance plays a central role
in the balance between myocardial energy supply and demand. Under physiological
conditions, myocardial blood flow and function are in balance,5 while
pathophysiological conditions leading to vascular dysfunction, such as glucose
intolerance, could alter balance between energy supply and demand. Although
glucose intolerance-induced vascular dysfunction may impair organ perfusion, data
elucidating the effects of glucose intolerance on the perfusion of vital organs like the
heart are limited. Up to now, only one group showed that insulin resistance in
prediabetic patients was associated with myocardial perfusion defects.6,7
Contrast echocardiography is a non-invasive method for assessment and
quantification of myocardial perfusion that is clinically applied for specific indications
in the cardiology setting. Using this technique it has been shown that myocardial
blood flow reserve, as a measure for vascular function, is reduced in type 1 diabetic
rats8 and type 1 diabetic patients9 when compared to normoglycemic controls. There
are currently limited data available on myocardial perfusion in glucose intolerance. In
the present study we therefore studied myocardial function and perfusion under
baseline and pharmacological-induced hyperemic conditions in a rat model for diet-
induced glucose intolerance using contrast echocardiography. Our hypothesis is that
glucose intolerance reduces the myocardial vasodilating capacity, which blunts the
increase in myocardial perfusion during hyperemia. This study demonstrates that
diet-induced glucose intolerance is associated with impaired myocardial function
during conditions of hyperemia, but not myocardial perfusion.
Myocardial function and perfusion during glucose intolerance 53
Methods
Animals and experimental set-up
All experiments were approved by the Institutional Animal Care and Use Committee
of the VU University, and were conducted following the European Convention for the
Protection of Vertebrate Animals used for Experimental and Other Scientific
Purposes.10 The performed research is in compliance with the modern ARRIVE
guidelines on animal research.11
Adult male Wistar rats (n=16; body weight 262±1 g; Harlan CBP, Horst, the
Netherlands) were fed a high fat diet (HFD) for a period of 4 weeks (n=8). Animals
that received a diet low in fat and sugars (control diet; CD) for 4 weeks served as
controls (n=8). Animals were housed in a temperature-controlled room (20-23°C;
40-60% humidity) under a 12/12 h light/dark cycle starting at 6.00 am. After 4
weeks, rats underwent an oral glucose tolerance test and (contrast)
echocardiography during baseline and after dipyridamole infusion.
Diets
High fat diet was obtained from Research Diets (D12451, New Brunswick, NJ). The
HFD consisted of 24 wt% protein, 24 wt% fat and 41 wt% carbohydrates (8.5 wt%
starch, 20.1 wt% sucrose). Control diet (Teklad 2016) was obtained from Harlan
(Horst, The Netherlands) and consisted of 17 wt% protein, 4 wt% fat and 61 wt%
carbohydrates (45.1 wt% starch, 5.0 wt% sucrose).
Oral glucose tolerance test
Rats fasted overnight received an oral glucose load (2 g/kg of body weight). Blood
glucose levels were measured from tail bleeds with a Precision Xceed Blood Glucose
monitoring system (MediSense, UK) before (0) and 15, 30, 60, 90 and 120 min after
glucose ingestion.12 At similar time points, plasma insulin (LINCO research, St.
Charles, Missouri) levels were measured as described previously.12
Plasma measurements
Plasma hematocrit levels were determined using microcentrifugation. Plasma free
fatty acids (WAKO NEFA-C, Wako Pure Chemical Industries, Osaka, Japan), plasma
high-density lipoprotein (HDL) cholesterol and plasma low-density lipoprotein
(LDL)/very-low-density lipoprotein (VLDL) cholesterol (Abcam, Cambridge, MA) were
measured after overnight fasting as previously described.13,14
3
54 Chapter 3
Cannulation of the jugular vein
For infusion of the contrast agent for echocardiography, a catheter was placed in the
jugular vein under S-Ketamine (Ketanest®, 150 mg/kg, Pfizer, the Netherlands) and
diazepam (3 mg/kg, Centrafarm, the Netherlands) anesthesia intraperitoneally. After
surgery, echocardiography and contrast echocardiography to determine myocardial
function and perfusion, respectively, were performed during baseline and
dipyridamole-induced hyperemia (20 mg/kg for 10 minutes) (Figure 3.1).
Figure 3.1: Protocol (contrast) echocardiography
After 4 weeks of control diet (CD) or high fat diet (HFD) feeding, rats received anesthesia for
cannulation of the jugular vein followed by echocardiography (echo) and contrast echocardiography
(contrast echo) during baseline and dipyridamole-induced hyperemia.
Echocardiography
Echocardiography (Siemens, ACUSON, Sequoia 512) was performed as previously
described.14 Briefly, wall thickness (WT) and left ventricular (LV) dimensions during
end-systole (ES) and end-diastole (ED) were determined in the M- (motion) mode of
the parasternal short-axis view at the level of the papillary muscles. Left ventricular
contractile function was calculated by the fractional shortening = (EDD-
ESD)/E -line (Image-Arena 2.9.1, TomTec
Imaging Systems, Unterschleissheim / Munich, Germany). All parameters were
averaged over at least three cardiac contractile cycles.
Myocardial contrast echocardiography
Contrast echocardiography was performed using a Siemens (ACUSON, Sequoia 512)
equipped with a 14 MHz linear array transducer (Philips Healthcare, Best, The
Netherlands). The contrast agent Sonovue® (Bracco Imaging, Italy), which contains
2x108-5x108/ml sulphur hexafluoride-filled, phospholipid-coated microbubbles with a
diameter of 1
diluted twice by adding 5 ml NaCl (0.9%). Microbubbles were continuously infused
using a dedicated syringe pump
(Vueject, Bracco SA, Switzerland). After two minutes of microbubble infusion,
perfusion images were taken of the short axis view of the left ventricle at the level of
the papillary muscles.
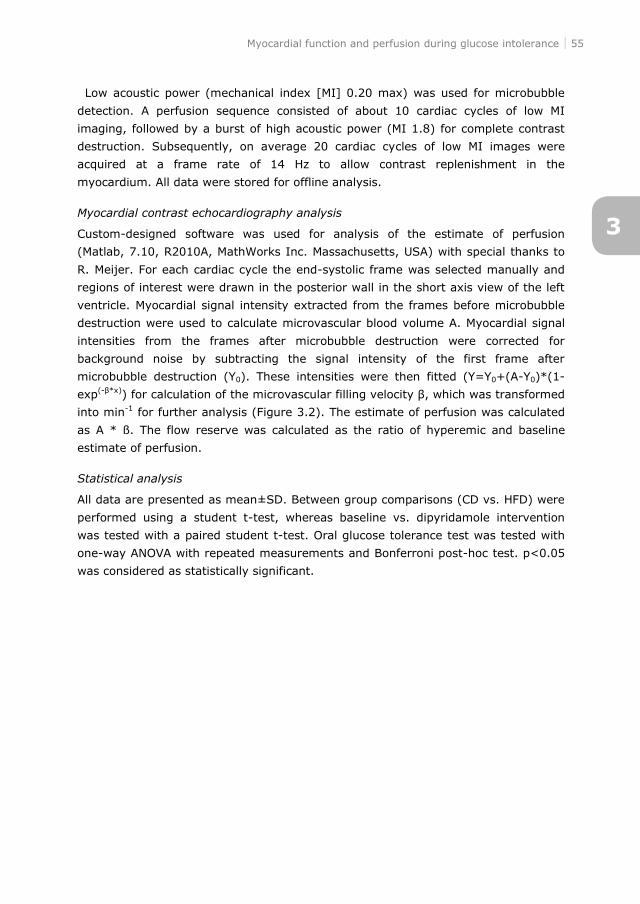
Myocardial function and perfusion during glucose intolerance 55
Low acoustic power (mechanical index [MI] 0.20 max) was used for microbubble
detection. A perfusion sequence consisted of about 10 cardiac cycles of low MI
imaging, followed by a burst of high acoustic power (MI 1.8) for complete contrast
destruction. Subsequently, on average 20 cardiac cycles of low MI images were
acquired at a frame rate of 14 Hz to allow contrast replenishment in the
myocardium. All data were stored for offline analysis.
Myocardial contrast echocardiography analysis
Custom-designed software was used for analysis of the estimate of perfusion
(Matlab, 7.10, R2010A, MathWorks Inc. Massachusetts, USA) with special thanks to
R. Meijer. For each cardiac cycle the end-systolic frame was selected manually and
regions of interest were drawn in the posterior wall in the short axis view of the left
ventricle. Myocardial signal intensity extracted from the frames before microbubble
destruction were used to calculate microvascular blood volume A. Myocardial signal
intensities from the frames after microbubble destruction were corrected for
background noise by subtracting the signal intensity of the first frame after
microbubble destruction (Y0). These intensities were then fitted (Y=Y0+(A-Y0)*(1-
exp(- ) for calculation of the microvascular filling velocity
into min-1 for further analysis (Figure 3.2). The estimate of perfusion was calculated
as A * ß. The flow reserve was calculated as the ratio of hyperemic and baseline
estimate of perfusion.
Statistical analysis
All data are presented as mean±SD. Between group comparisons (CD vs. HFD) were
performed using a student t-test, whereas baseline vs. dipyridamole intervention
was tested with a paired student t-test. Oral glucose tolerance test was tested with
one-way ANOVA with repeated measurements and Bonferroni post-hoc test. p<0.05
was considered as statistically significant.
3
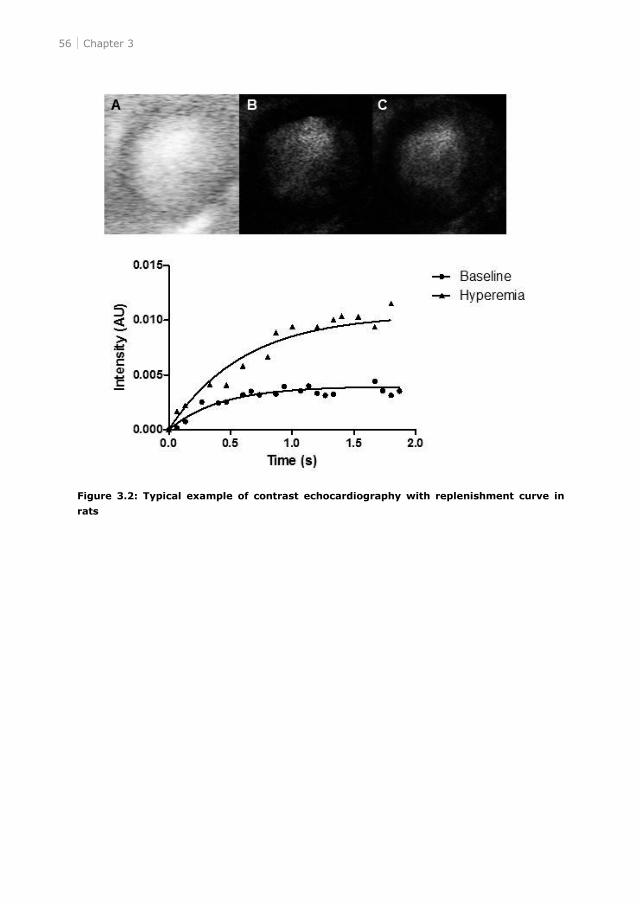
56 Chapter 3
Figure 3.2: Typical example of contrast echocardiography with replenishment curve in
rats
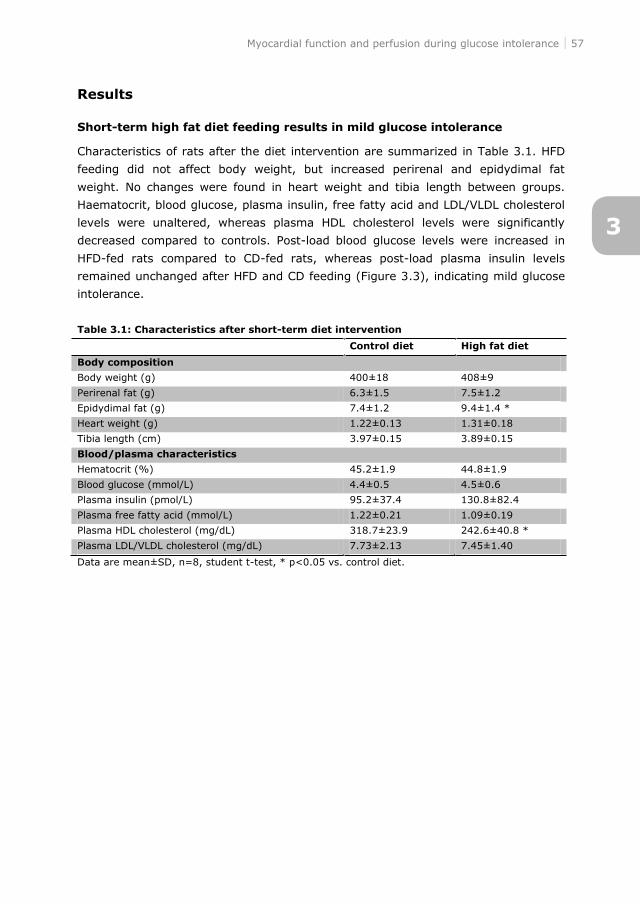
Myocardial function and perfusion during glucose intolerance 57
Results
Short-term high fat diet feeding results in mild glucose intolerance
Characteristics of rats after the diet intervention are summarized in Table 3.1. HFD
feeding did not affect body weight, but increased perirenal and epidydimal fat
weight. No changes were found in heart weight and tibia length between groups.
Haematocrit, blood glucose, plasma insulin, free fatty acid and LDL/VLDL cholesterol
levels were unaltered, whereas plasma HDL cholesterol levels were significantly
decreased compared to controls. Post-load blood glucose levels were increased in
HFD-fed rats compared to CD-fed rats, whereas post-load plasma insulin levels
remained unchanged after HFD and CD feeding (Figure 3.3), indicating mild glucose
intolerance.
Table 3.1: Characteristics after short-term diet intervention
Control diet High fat diet
Body composition
Body weight (g) 400±18 408±9
Perirenal fat (g) 6.3±1.5 7.5±1.2
Epidydimal fat (g) 7.4±1.2 9.4±1.4 *
Heart weight (g) 1.22±0.13 1.31±0.18
Tibia length (cm) 3.97±0.15 3.89±0.15
Blood/plasma characteristics
Hematocrit (%) 45.2±1.9 44.8±1.9
Blood glucose (mmol/L) 4.4±0.5 4.5±0.6
Plasma insulin (pmol/L) 95.2±37.4 130.8±82.4
Plasma free fatty acid (mmol/L) 1.22±0.21 1.09±0.19
Plasma HDL cholesterol (mg/dL) 318.7±23.9 242.6±40.8 *
Plasma LDL/VLDL cholesterol (mg/dL) 7.73±2.13 7.45±1.40
Data are mean±SD, n=8, student t-test, * p<0.05 vs. control diet.
3
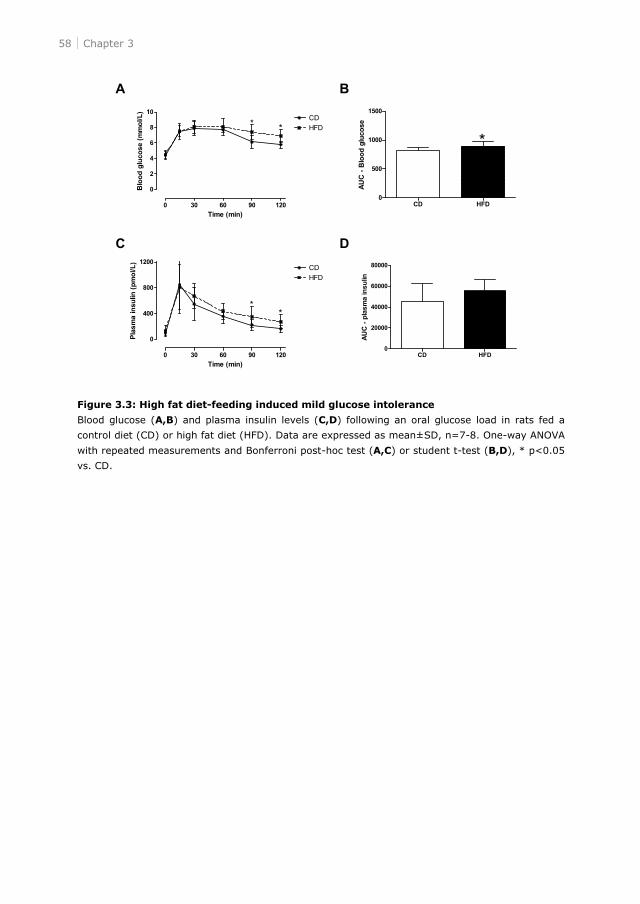
58 Chapter 3
Figure 3.3: High fat diet-feeding induced mild glucose intolerance
Blood glucose (A,B) and plasma insulin levels (C,D) following an oral glucose load in rats fed a
control diet (CD) or high fat diet (HFD). Data are expressed as mean±SD, n=7-8. One-way ANOVA
with repeated measurements and Bonferroni post-hoc test (A,C) or student t-test (B,D), * p<0.05
vs. CD.
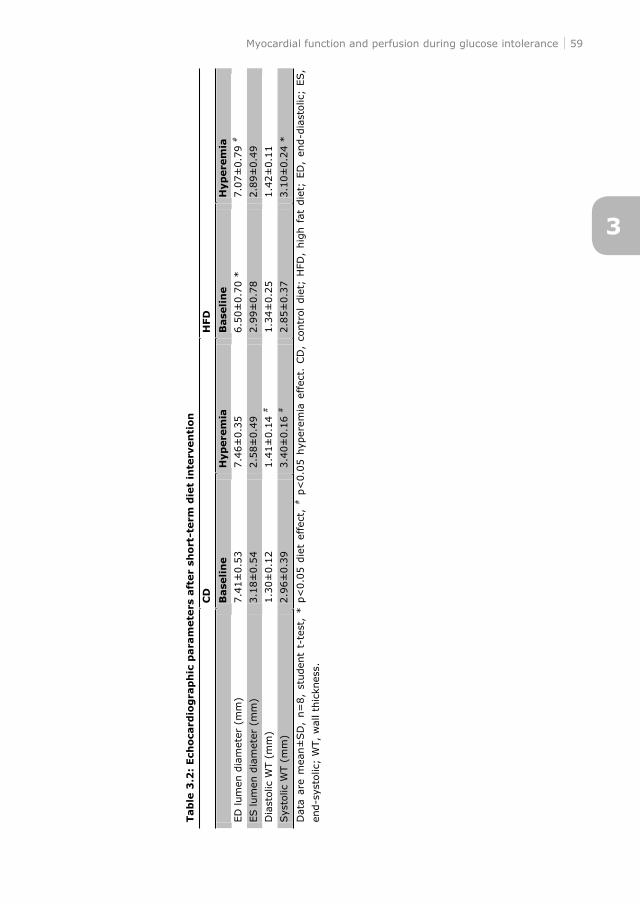
Myocardial function and perfusion during glucose intolerance 59
Tab
le 3
.2:
Ech
oca
rdio
gra
ph
ic p
ara
mete
rs a
fter
sho
rt-t
erm
die
t in
terv
en
tion
C
D
HFD
B
ase
lin
e
Hyp
ere
mia
Base
lin
e
Hyp
ere
mia
ED
lum
en d
iam
eter
(m
m)
7.4
1±
0.5
3
7.4
6±
0.3
5
6.5
0±
0.7
0 *
7.0
7±
0.7
9 #
ES lum
en d
iam
eter
(m
m)
3.1
8±
0.5
4
2.5
8±
0.4
9
2.9
9±
0.7
8
2.8
9±
0.4
9
Dia
stol
ic W
T (
mm
)
1.3
0±
0.1
2
1.4
1±
0.1
4 #
1.3
4±
0.2
5
1.4
2±
0.1
1
Sys
tolic
WT (
mm
) 2.9
6±
0.3
9
3.4
0±
0.1
6 #
2.8
5±
0.3
7
3.1
0±
0.2
4 *
Data
are
mea
n±
SD
, n=
8,
studen
t t-
test
, * p
<0.0
5 d
iet
effe
ct,
# p
<0.0
5 h
yper
emia
effec
t. C
D,
contr
ol d
iet;
HFD
, hig
h f
at d
iet;
ED
, en
d-d
iast
olic
; ES,
end-s
ysto
lic;
WT,
wal
l th
ickn
ess.
3
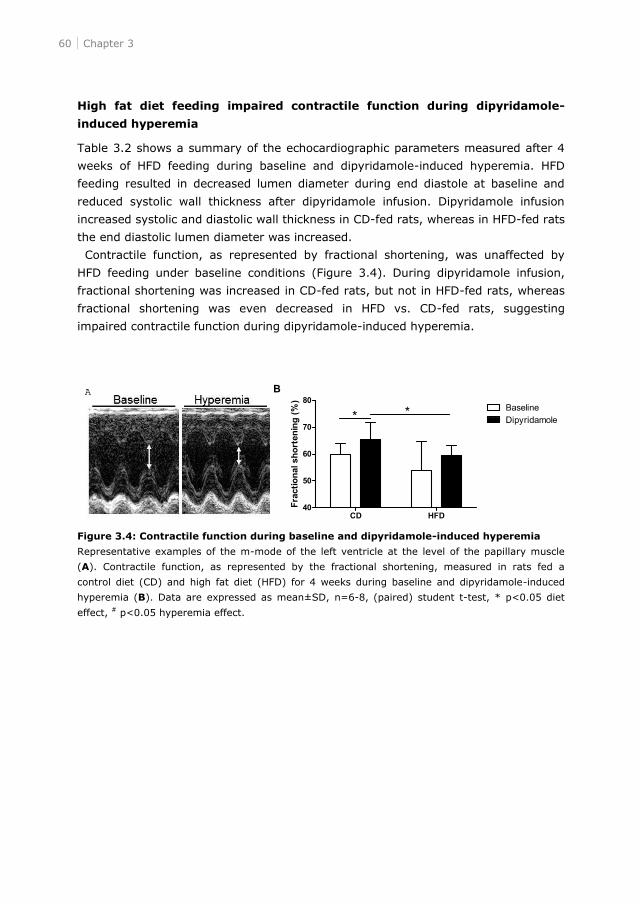
60 Chapter 3
High fat diet feeding impaired contractile function during dipyridamole-
induced hyperemia
Table 3.2 shows a summary of the echocardiographic parameters measured after 4
weeks of HFD feeding during baseline and dipyridamole-induced hyperemia. HFD
feeding resulted in decreased lumen diameter during end diastole at baseline and
reduced systolic wall thickness after dipyridamole infusion. Dipyridamole infusion
increased systolic and diastolic wall thickness in CD-fed rats, whereas in HFD-fed rats
the end diastolic lumen diameter was increased.
Contractile function, as represented by fractional shortening, was unaffected by
HFD feeding under baseline conditions (Figure 3.4). During dipyridamole infusion,
fractional shortening was increased in CD-fed rats, but not in HFD-fed rats, whereas
fractional shortening was even decreased in HFD vs. CD-fed rats, suggesting
impaired contractile function during dipyridamole-induced hyperemia.
Figure 3.4: Contractile function during baseline and dipyridamole-induced hyperemia
Representative examples of the m-mode of the left ventricle at the level of the papillary muscle
(A). Contractile function, as represented by the fractional shortening, measured in rats fed a
control diet (CD) and high fat diet (HFD) for 4 weeks during baseline and dipyridamole-induced
hyperemia (B). Data are expressed as mean±SD, n=6-8, (paired) student t-test, * p<0.05 diet
effect, # p<0.05 hyperemia effect.
A
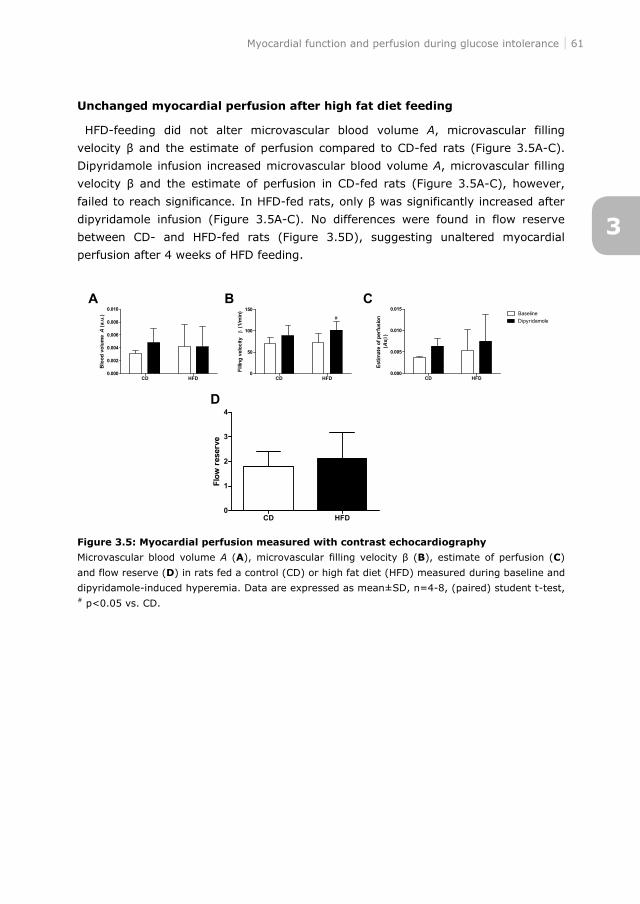
Myocardial function and perfusion during glucose intolerance 61
Unchanged myocardial perfusion after high fat diet feeding
HFD-feeding did not alter microvascular blood volume A, microvascular filling
velocity the estimate of perfusion compared to CD-fed rats (Figure 3.5A-C).
Dipyridamole infusion increased microvascular blood volume A, microvascular filling
velocity the estimate of perfusion in CD-fed rats (Figure 3.5A-C), however,
failed to reach significance. In HFD-
dipyridamole infusion (Figure 3.5A-C). No differences were found in flow reserve
between CD- and HFD-fed rats (Figure 3.5D), suggesting unaltered myocardial
perfusion after 4 weeks of HFD feeding.
Figure 3.5: Myocardial perfusion measured with contrast echocardiography
Microvascular blood volume A (A), microvascular filling velocity B), estimate of perfusion (C)
and flow reserve (D) in rats fed a control (CD) or high fat diet (HFD) measured during baseline and
dipyridamole-induced hyperemia. Data are expressed as mean±SD, n=4-8, (paired) student t-test, # p<0.05 vs. CD.
3
62 Chapter 3
Discussion
In the present study, we examined the effect of glucose intolerance on myocardial
function and perfusion. We found that short-term high fat diet feeding resulted in
glucose intolerance without affecting myocardial function and perfusion under
baseline conditions. Diet-induced glucose intolerance impaired myocardial contractile
function during conditions of hyperemia, in the absence of alterations in myocardial
perfusion.
The present study showed that short-term high fat diet feeding resulted in glucose
intolerance without obesity affecting myocardial contractile function under resting
conditions. Our results confirm previous findings, showing that 4 weeks of high fat
diet feeding in rats resulted in glucose intolerance without affecting function,15
whereas 8 weeks of high fat diet feeding resulted in glucose intolerance with mildly
impaired contractile function.15 One of the suggested mechanisms that may
contribute to alterations in myocardial blood flow during prediabetes or diabetes are
changes in nitric oxide availability. High fat diet feeding in male rats decreased nitric
oxide availability,16 whereas increased nitric oxide bioavailability in eNOS-/- mice has
been shown to attenuate high fat diet-induced metabolic alterations associated with
insulin resistance.17 Taken together, these results suggest that 4 weeks of high fat
diet feeding in a rat results in a mild model of glucose intolerance without impaired
myocardial function.
Under physiological conditions, myocardial perfusion and function are in balance.5
However, a perfusion-contraction mismatch might exist in glucose intolerance. In the
present study, diet-induced glucose intolerance did not affect myocardial perfusion
measured with contrast echocardiography during baseline conditions. These results
are in agreement with Menard et al.,18 who found no differences in myocardial
perfusion index measured by [13N] ammonia PET in rats fed a high fructose and high
fat diet with additional streptozotocin. Accordingly, in patients with insulin resistance
or glucose tolerance it was found that insulin resistance was associated with a defect
in myocardial perfusion measured by single photon emission computed tomography,
which was independent of glucose tolerance and obesity.6 Together, these results
suggest that under baseline conditions diet-induced glucose intolerance does not
affect myocardial function and perfusion.
Dipyridamole is used to pharmacologically induce maximal vasodilation.
Dipyridamole blocks the uptake of adenosine, thereby increasing the circulating
levels of adenosine, which results in maximal coronary blood flow due to decreased
coronary vascular resistance.19 During hyperemia, myocardial contractile function
was increased in healthy rats, but not in rats with diet-induced glucose intolerance.
On the contrary, this hyperemic-induced increase in contractile function was not seen
in healthy and type 1 diabetic rats.8 Besides glucose intolerance, several variables
Myocardial function and perfusion during glucose intolerance 63
could be associated with alterations in myocardial function. Our experimental rat
model with high fat diet feeding resulted in development of glucose intolerance, but
rats did not become obese. Consequently, obesity cannot be explanatory for the
findings of the effect of high fat diet feeding on myocardial function.
Myocardial blood flow reserve is the increase in blood flow that can be achieved
from basal perfusion to maximal vasodilatation, and is therefore a measurement of
the ability of the microvasculature to respond to an increase in oxygen demand. In
type 1 diabetic rats8 and patients9 it was shown that myocardial blood flow reserve
measured with contrast echocardiography was decreased compared to healthy
controls. In the present study, myocardial blood flow reserve was unchanged
between healthy rats and rats with glucose intolerance, suggesting that glucose
intolerance does not reduce the vasodilating capacity of the myocardium. Increases
in myocardial contractile function will lead to a metabolically-mediated increase in
myocardial blood flow, however, an increase in coronary perfusion does not have to
increase myocardial contractile function,5 which might explain the hyperemic-induced
differences in myocardial function and perfusion in rats with glucose intolerance.
A limitation of this study is the small amount of rats used. Although this is a pilot
study, ideally, this data set should have been analyzed with a two-way ANOVA with
Bonferronni post-hoc testing for multiple group comparisons.
In conclusion, the present data demonstrate that diet-induced glucose intolerance
is associated with impaired myocardial function during conditions of hyperemia, but
not myocardial perfusion. These findings may result in new insights into the effect of
glucose intolerance on myocardial function and perfusion during hyperemia.
3
64 Chapter 3
References
1. Zimmet PZ, Gareeboo H, Hemraj F, Tuomilehto J, Alberti KG: Impaired fasting glucose or
impaired glucose tolerance. What best predicts future diabetes in Mauritius? Diabetes Care
1999, 22:399 402.
2. de Veire van, de Winter O, Gillebert TC, de Sutter J: Diabetes and impaired fasting glucose as
predictors of morbidity and mortality in male coronary artery disease patients with reduced
left ventricular function. Acta Cardiol 2006, 61:137 143.
3. Tominaga M, Eguchi H, Manaka H, Igarashi K, Kato T, Sekikawa A: Impaired glucose tolerance
is a risk factor for cardiovascular disease, but not impaired fasting glucose. The Funagata
Diabetes Study. Diabetes Care 1999, 22:920 924.
4. DeFronzo RA, bdul-Ghani M: Assessment and treatment of cardiovascular risk in prediabetes:
impaired glucose tolerance and impaired fasting glucose. Am J Cardiol 2011, 108:3B 24B.
5. Heusch G, Schulz R: The relation of contractile function to myocardial perfusion. Perfusion-
contraction match and mismatch. Herz 1999, 24:509 514.
6. Nasr G, Sliem H: Silent myocardial ischemia in prediabetics in relation to insulin resistance. J
Cardiovasc Dis Res 2010, 1:116 121.
7. Nasr G, Sliem H: Silent ischemia in relation to insulin resistance in normotensive prediabetic
adults: early detection by single photon emission computed tomography (SPECT). Int J
Cardiovasc Imaging 2011, 27:335 341.
8. Cosyns B, Droogmans S, Hernot S, Degaillier C, Garbar C, Weytjens C, Roosens B, Schoors D,
Lahoutte T, Franken PR, Van Camp G: Effect of streptozotocin-induced diabetes on myocardial
blood flow reserve assessed by myocardial contrast echocardiography in rats. Cardiovasc
Diabetol 2008, 7:26.
9. Rana O, Byrne CD, Kerr D, Coppini DV, Zouwail S, Senior R, Begley J, Walker JJ, Greaves K:
Acute hypoglycemia decreases myocardial blood flow reserve in patients with type 1 diabetes
mellitus and in healthy humans. Circulation 2011, 124:1548 1556.
10. http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=CELEX:31986L0609:EN:NOT.
11. Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG: Improving bioscience research
reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol 2010, 8:e1000412.
12. Ouwens DM, Boer C, Fodor M, de Galan P, Heine RJ, Maassen JA, Diamant M: Cardiac
dysfunction induced by high-fat diet is associated with altered myocardial insulin signalling in
rats. Diabetologia 2005, 48:1229 1237.
13. van den Brom CE, Bosmans JW, Vlasblom R, Handoko ML, Huisman MC, Lubberink M, Molthoff
CF, Lammertsma AA, Ouwens DM, Diamant M, Boer C: Diabetic cardiomyopathy in Zucker
diabetic fatty rats: the forgotten right ventricle. Cardiovasc Diabetol 2010, 9:25.
14. van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol
2009, 8:39.
15. Ouwens DM, Diamant M, Fodor M, Habets DD, Pelsers MM, El Hasnaoui M, Dang ZC, van den
Brom CE, Vlasblom R, Rietdijk A, Boer C, Coort SL, Glatz JF, Luiken JJ: Cardiac contractile
dysfunction in insulin-resistant rats fed a high-fat diet is associated with elevated CD36-
mediated fatty acid uptake and esterification. Diabetologia 2007, 50:1938 1948.
Myocardial function and perfusion during glucose intolerance 65
16. Monteiro PF, Morganti RP, Delbin MA, Calixto MC, Lopes-Pires ME, Marcondes S, Zanesco A,
Antunes E: Platelet hyperaggregability in high-fat fed rats: a role for intraplatelet reactive-
oxygen species production. Cardiovasc Diabetol 2012, 11:5.
17. Razny U, Kiec-Wilk B, Wator L, Polus A, Dyduch G, Solnica B, Malecki M, Tomaszewska R,
Cooke JP, mbinska-Kiec A: Increased nitric oxide availability attenuates high fat diet metabolic
alterations and gene expression associated with insulin resistance. Cardiovasc Diabetol 2011,
10:68.
18. Menard SL, Croteau E, Sarrhini O, Gelinas R, Brassard P, Ouellet R, Bentourkia M, van Lier JE,
Des RC, Lecomte R, Carpentier AC: Abnormal in vivo myocardial energy substrate uptake in
diet-induced type 2 diabetic cardiomyopathy in rats. Am J Physiol Endocrinol Metab 2010,
298:E1049 E1057.
19. Leppo JA: Dipyridamole myocardial perfusion imaging. J Nucl Med 1994, 35:730 733.
3

CE van den Brom, CA Boly, CSE Bulte, RPF van den Akker,
RFJ Kwekkeboom, SA Loer, C Boer, RA Bouwman
Submitted
4Sevoflurane impairs myocardial systolic
function, but not myocardial perfusion in
diet-induced prediabetic rats

Sevoflurane and myocardial perfusion in prediabetes 69
Abstract
Introduction
Preservation of myocardial perfusion is particularly important in patients with
increased risk for perioperative cardiac complications, such as patients with diabetes.
Knowledge regarding regulation of myocardial perfusion and function during
anesthesia in subjects with cardiometabolic disease is however limited. In this study
we therefore investigated whether the effect of sevoflurane on myocardial perfusion
and function is altered in healthy and diet-induced prediabetic rats.
Methods
Male Wistar rats were randomly exposed to a western diet (WD; n=18) or control
diet (CD; n=18). After 8 weeks, rats underwent (contrast) echocardiography to
determine myocardial perfusion and function during baseline conditions and
sevoflurane (2%) exposure. Myocardial perfusion was estimated based on the
product of microvascular filling velocity ( and microvascular blood volume (A),
whereas myocardial function was determined by fractional shortening and fractional
area change.
Results
Eight weeks of WD feeding resulted in obesity and hyperglycemia compared to CD-
feeding. At baseline, WD decreased estimate of perfusion compared to control rats.
Systolic function was significantly impaired compared to CD-fed rats. Exposure to
sevoflurane increased the microvascular filling velocity in healthy controls, whereas
the overall estimate of myocardial perfusion remained unchanged in both diet
groups. Moreover, sevoflurane impaired systolic function in both diet groups.
Conclusions
Diet-induced prediabetes is associated with impaired myocardial perfusion and
function in rats. While sevoflurane further impaired systolic function, it did not affect
myocardial perfusion in prediabetic rats. Our findings suggest that sevoflurane leads
to uncoupling of myocardial perfusion and function, irrespective of the metabolic
state.
4
70 Chapter 4
Introduction
Myocardial perfusion in relation with myocardial function determines the balance
between myocardial energy supply and demand. During surgery, maintenance of the
myocardial oxygen balance is challenged, because extrinsic factors, like anesthetics
and surgical stress, and intrinsic factors, like metabolic alterations, affect myocardial
oxygen supply and consumption. This altered balance may increase the vulnerability
of the heart for an oxygen supply and demand mismatch and consequent
ischemia.1;2
Sevoflurane has vasodilating properties and is known to reduce coronary vascular
resistance3 and perfusion pressure.4;5 We recently showed that sevoflurane did not
affect myocardial blood flow in healthy patients, while myocardial flow reserve was
decreased.6 Animal studies however showed that sevoflurane, when perfusion
pressure remained constant, increased coronary blood flow in hearts of dogs7 and
decreased coronary flow reserve in isolated rat hearts.5 In contrast, sevoflurane
lowered blood pressure and decreased myocardial blood flow in healthy rats,8 dogs9
and pigs.10
While sevoflurane exerts contrasting effects on myocardial perfusion in healthy
subjects, its vasodilatory impact may be more abundant in patients with
cardiometabolic disease, like type 2 diabetes mellitus (T2DM). T2DM patients are
more likely to develop coronary artery disease11 and have an increased
cardiovascular complication rate after major non-cardiac surgery.12 Because
myocardial substrate metabolism and myocardial oxygen balance is altered in
T2DM,13 the regulation of myocardial perfusion in these patients is particularly
important during normal and intraoperative circumstances. The number of studies
focusing on myocardial perfusion during anesthesia in subjects with cardiometabolic
disease is however limited. Previously, we found that myocardial perfusion, but not
myocardial function, is preserved during hyperemia in glucose intolerant rats,14 while
others showed myocardial perfusion defects in prediabetic insulin resistant
patients15;16 or T2DM patients during the postprandial state.17;18 The aforementioned
data suggest that a cardiometabolic-compromised state may be associated with
more severe alterations in myocardial perfusion during anesthesia.
Therefore, the purpose of the present study was to investigate the effect of
sevoflurane on myocardial function and perfusion in diet-induced prediabetic rats.
While the effects in healthy subjects seem apparently conflicting, we hypothesized
cardiometabolic disease and thereby challenging myocardial perfusion regulation.
Sevoflurane and myocardial perfusion in prediabetes 71
Methods
Animals and experimental set-up
All experiments were approved by the Institutional Animal Care and Use Committee
of the VU University, and were conducted following the European Convention for the
Protection of Vertebrate Animals used for Experimental and Other Scientific
Purposes.
Adult male Wistar rats (n=36; body weight 265±7 g; Charles River Laboratories,
France) were fed a western diet (WD) for a period of 8 weeks (n=18). Rats that
received a diet low in fat and sugars (control diet; CD) for 8 weeks served as
controls (n=18). Animals were housed in a temperature-controlled room (20-23°C;
40-60% humidity) under a 12/12h light/dark cycle starting at 6.00 am. Body weight
was determined on a weekly basis. After 8 weeks, rats underwent (contrast)
echocardiography during baseline conditions and during sevoflurane (AbbVie, the
Netherlands) exposure, starting after 5 minutes of sevoflurane.
Diets
CD (Teklad 2016, Harlan, Horst, the Netherlands) consisted of 20 %kcal protein,
9 %kcal fat and 74 %kcal carbohydrates (1804 kcal/kg starch, 200 kcal/kg sugars),
whereas WD (D12451, Research Diets, New Brunswick, NJ) consisted of 20 %kcal
protein, 45 %kcal fat and 35 %kcal carbohydrates (291 kcal/kg starch, 691 kcal/kg
sugars) with 20% sucrose water (800 kcal/kg), totally containing 3300 kcal/kg and
4857 kcal/kg for CD and WD with sucrose water, respectively.
Surgery
After 8 weeks of diet exposure, rats were anesthetized with 125 mg/kg S-Ketamine
(Ketanest®, Pfizer, the Netherlands) and 4 mg/kg diazepam (Centrafarm, the
Netherlands) intraperitoneally and were intubated and mechanically ventilated (UNO,
the Netherlands; positive end-expiratory pressure, 1-2 cm H2O; respiratory rate,
~65 breaths/min; tidal volume, ~10 ml/kg) with oxygen-enriched air (40% O2/60%
N2). Anesthesia was maintained by continuous infusion of 50 mg/kg/h S-Ketamine
and 1.3 mg/kg/h diazepam intravenously via the tail vein. Respiratory rate was
adjusted to maintain pH and partial pressure of carbon dioxide within physiological
limits. Body temperature was maintained stable (36.7±1.2°C) using a warm water
underbody heating pad.
A catheter was placed in the right jugular vein for infusion of the contrast agent.
The left carotid artery was cannulated for blood sampling, blood gas analyses
(ABL50, radiometer, Copenhagen, Denmark) and for measurements of arterial blood
pressure (Safedraw Transducer Blood Sampling Set, Argon Medical Devices, Texas,
USA). Arterial blood pressure, ECG and heart rate were continuously recorded using
4
72 Chapter 4
PowerLab software (PowerLab 8/35, Chart 7.0; ADInstruments Pty, Ltd., Castle Hill,
Australia). Mean arterial blood pressure was calculated according the following
product (RPP) was calculated by the product of heart rate and systolic blood pressure
and was used as an estimate of myocardial oxygen demand.
Echocardiography
After surgery, (contrast) echocardiography was performed to determine myocardial
function and perfusion during baseline conditions and after 5 minutes of sevoflurane
(2%) exposure. Echocardiography (Siemens, ACUSON, Sequoia 512) was performed
as previously described.13 Briefly, left ventricular (LV) dimensions during end-systole
(ES) and end-diastole (ED) were determined in the M-(motion) mode of the
parasternal short-axis view at the level of the papillary muscles. LV systolic function
is represented by fractional shortening (FS) and fractional area change (FAC), which
were calculated by the equations: FS = (EDD- 2-
ESD2)/EDD2 100). All parameters were averaged over at least three cardiac
contractile cycles.
Preparation of microbubbles
Microbubbles were prepared from perfluorobutane gas and stabilized with a
monolayer of distearoyl phosphatidylcholine and PEG stearate. 1,2-distearoyl-sn-
glycero-3-phosphocholine (DSPC; Avanti Polar Lipids, Alabama, USA) and
polyoxyethylene stearate (PEG40; Sigma, St Louis, MO, USA) were dissolved in
glycerol (10 mg/ml) and sonicated (Decon FS200, Decon Ultrasonics Ltd, Sussex,
UK) at 40 kHz in an atmosphere of perfluorobutane (F2 Chemicals Ltd, Lancashire,
UK) and vials were shaken a Vialmix at 4500 rpm (Bristol-Myers Squibb Medical
Imaging, Massachusetts, USA). As the gas was dispersed in the aqueous phase,
microbubbles were formed, which were stabilized with a self-assembled
lipid/surfactant monolayer. Freshly made bubbles were then washed twice to remove
excessive DSPC and PEG40 and stored refrigerated in sealed vials in perfluorobutane
atmosphere. A Multisizer 3 coulter counter (Beckman Coulter Inc., Miami, FL, USA)
was used to measure the particle size distribution as well as the number of particles.
The average bubble concentration was 1.578 109 ± 0.364 109 and the particle
range was between 1 and 10 Microbubbles were diluted to a concentration of
200 106 with ungassed water.
Sevoflurane and myocardial perfusion in prediabetes 73
Myocardial contrast echocardiography
Contrast echocardiography was performed using a Siemens (ACUSON, Sequoia 512)
equipped with a 14 MHz linear array transducer (Philips Healthcare, Best, The
Netherlands).14 Microbubbles were continuously infused into the jugular vein with a
rate of 300 μl/min using a dedicated syringe pump (Vueject, Bracco SA,
Switzerland). After two minutes of microbubble infusion, perfusion images were
taken from the long axis view of the left ventricle.
Low acoustic power (mechanical index [MI] 0.20) was used for microbubble
detection with a dynamic range of 50 dB. A perfusion sequence consisted of about 10
cardiac cycles of low MI imaging, followed by a burst of high acoustic power (MI 1.8)
for complete contrast destruction. Subsequently, on average 20 cardiac cycles of low
MI images were acquired to allow contrast replenishment in the myocardium. All
data were stored for offline analysis.
Myocardial contrast echocardiography analysis
Custom-designed software was used for analysis of the estimate of perfusion
(Matlab, 7.10, R2010A, MathWorks Inc. Massachusetts, USA).6;14 For each cardiac
cycle, regions of interest were drawn in the end-systolic frame in the posterior wall in
the long axis view of the left ventricle. Myocardial signal intensities from the frames
after microbubble destruction were corrected for background noise by subtracting
the signal intensity of the first frame after microbubble destruction (Y0). These
intensities were then fitted (Y=Y0 + (A-Y0) (1-exp(-ß x))) for calculation of
microvascular blood volume A and the microvascular filling velocity ß, which
corresponds to the capillary blood exchange rate. The estimate of perfusion was
calculated as the product of A and ß.19
Statistical analysis
Data were analyzed using Graphpad Prism 5.0 (La Jolla, USA) and presented as
mean±SD. Between group comparisons (CD vs. WD) were performed using a
student t-test, whereas the effect of sevoflurane exposure was tested with a two-
way ANOVA with Bonferonni as post-hoc test. p<0.05 was considered as statistically
significant.
4
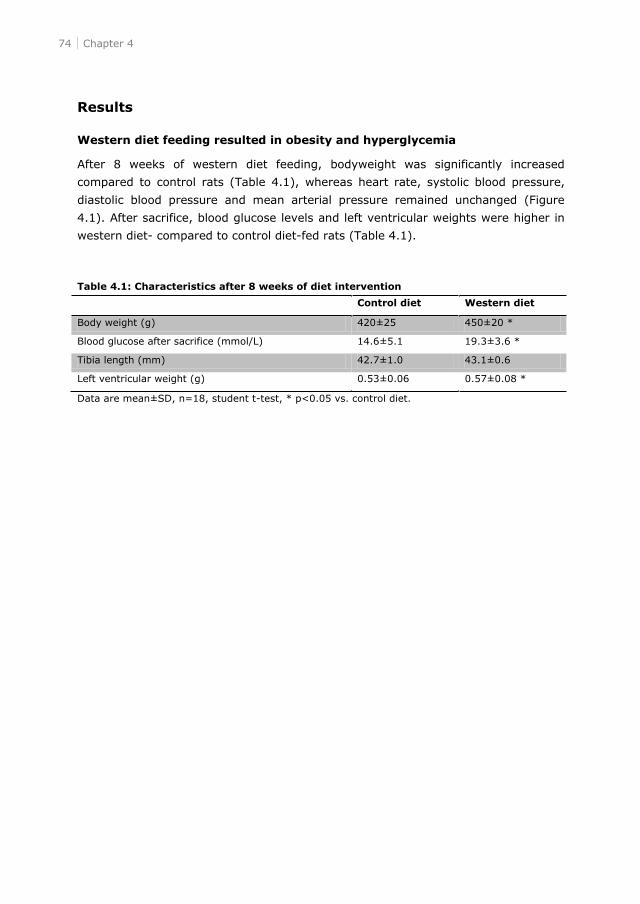
74 Chapter 4
Results
Western diet feeding resulted in obesity and hyperglycemia
After 8 weeks of western diet feeding, bodyweight was significantly increased
compared to control rats (Table 4.1), whereas heart rate, systolic blood pressure,
diastolic blood pressure and mean arterial pressure remained unchanged (Figure
4.1). After sacrifice, blood glucose levels and left ventricular weights were higher in
western diet- compared to control diet-fed rats (Table 4.1).
Table 4.1: Characteristics after 8 weeks of diet intervention
Control diet Western diet
Body weight (g) 420±25 450±20 *
Blood glucose after sacrifice (mmol/L) 14.6±5.1 19.3±3.6 *
Tibia length (mm) 42.7±1.0 43.1±0.6
Left ventricular weight (g) 0.53±0.06 0.57±0.08 *
Data are mean±SD, n=18, student t-test, * p<0.05 vs. control diet.
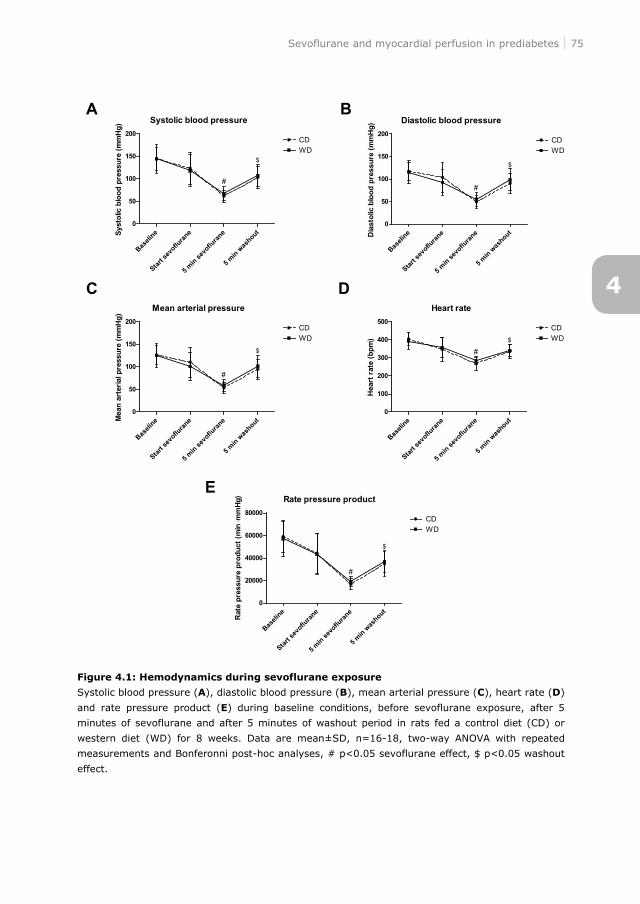
Sevoflurane and myocardial perfusion in prediabetes 75
Figure 4.1: Hemodynamics during sevoflurane exposure
Systolic blood pressure (A), diastolic blood pressure (B), mean arterial pressure (C), heart rate (D)
and rate pressure product (E) during baseline conditions, before sevoflurane exposure, after 5
minutes of sevoflurane and after 5 minutes of washout period in rats fed a control diet (CD) or
western diet (WD) for 8 weeks. Data are mean±SD, n=16-18, two-way ANOVA with repeated
measurements and Bonferonni post-hoc analyses, # p<0.05 sevoflurane effect, $ p<0.05 washout
effect.
4
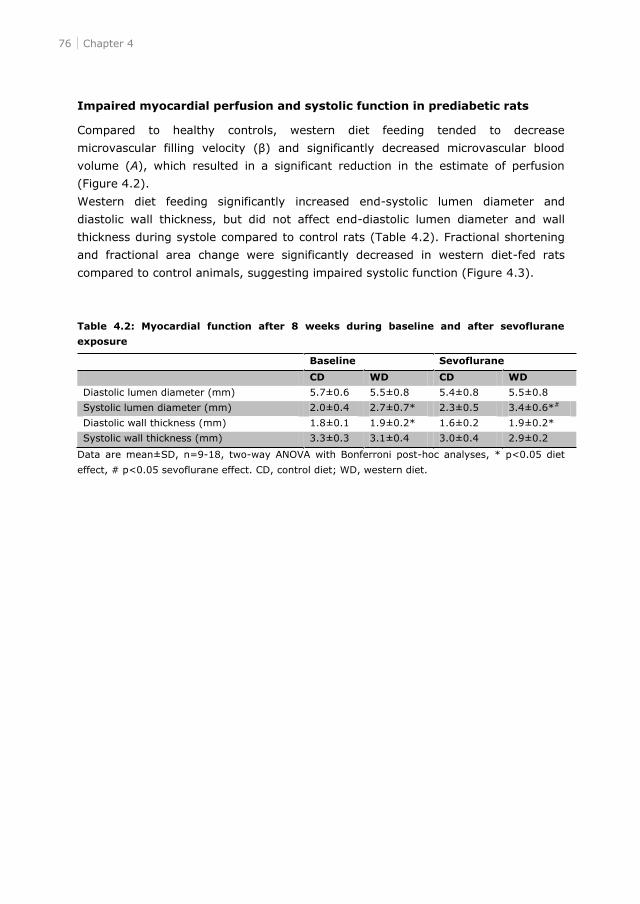
76 Chapter 4
Impaired myocardial perfusion and systolic function in prediabetic rats
Compared to healthy controls, western diet feeding tended to decrease
volume (A), which resulted in a significant reduction in the estimate of perfusion
(Figure 4.2).
Western diet feeding significantly increased end-systolic lumen diameter and
diastolic wall thickness, but did not affect end-diastolic lumen diameter and wall
thickness during systole compared to control rats (Table 4.2). Fractional shortening
and fractional area change were significantly decreased in western diet-fed rats
compared to control animals, suggesting impaired systolic function (Figure 4.3).
Table 4.2: Myocardial function after 8 weeks during baseline and after sevoflurane
exposure
Data are mean±SD, n=9-18, two-way ANOVA with Bonferroni post-hoc analyses, * p<0.05 diet
effect, # p<0.05 sevoflurane effect. CD, control diet; WD, western diet.
Baseline Sevoflurane
CD WD CD WD
Diastolic lumen diameter (mm) 5.7±0.6 5.5±0.8 5.4±0.8 5.5±0.8
Systolic lumen diameter (mm) 2.0±0.4 2.7±0.7* 2.3±0.5 3.4±0.6*#
Diastolic wall thickness (mm) 1.8±0.1 1.9±0.2* 1.6±0.2 1.9±0.2*
Systolic wall thickness (mm) 3.3±0.3 3.1±0.4 3.0±0.4 2.9±0.2
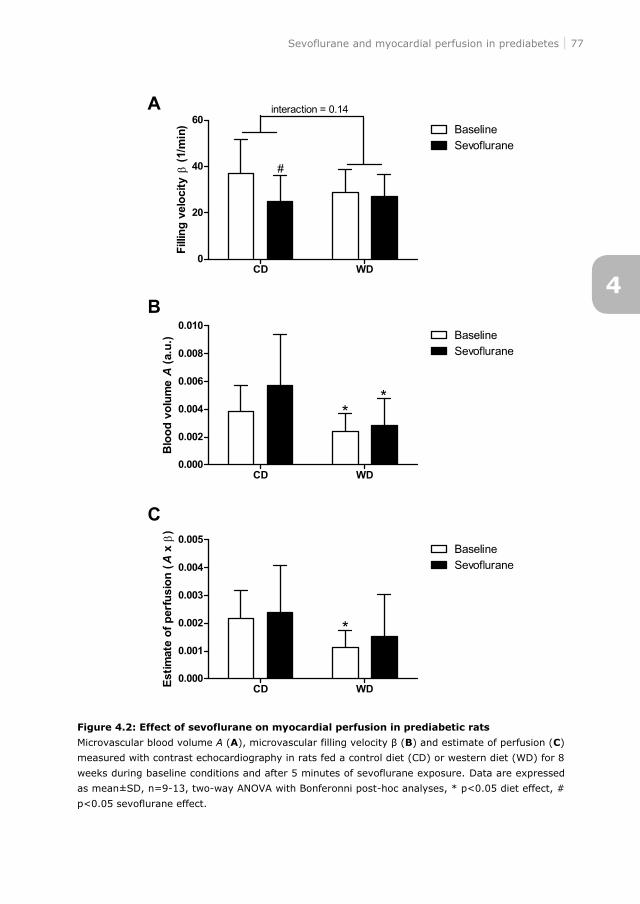
Sevoflurane and myocardial perfusion in prediabetes 77
Figure 4.2: Effect of sevoflurane on myocardial perfusion in prediabetic rats
Microvascular blood volume A (A), microvascular filling velocity B) and estimate of perfusion (C)
measured with contrast echocardiography in rats fed a control diet (CD) or western diet (WD) for 8
weeks during baseline conditions and after 5 minutes of sevoflurane exposure. Data are expressed
as mean±SD, n=9-13, two-way ANOVA with Bonferonni post-hoc analyses, * p<0.05 diet effect, #
p<0.05 sevoflurane effect.
4
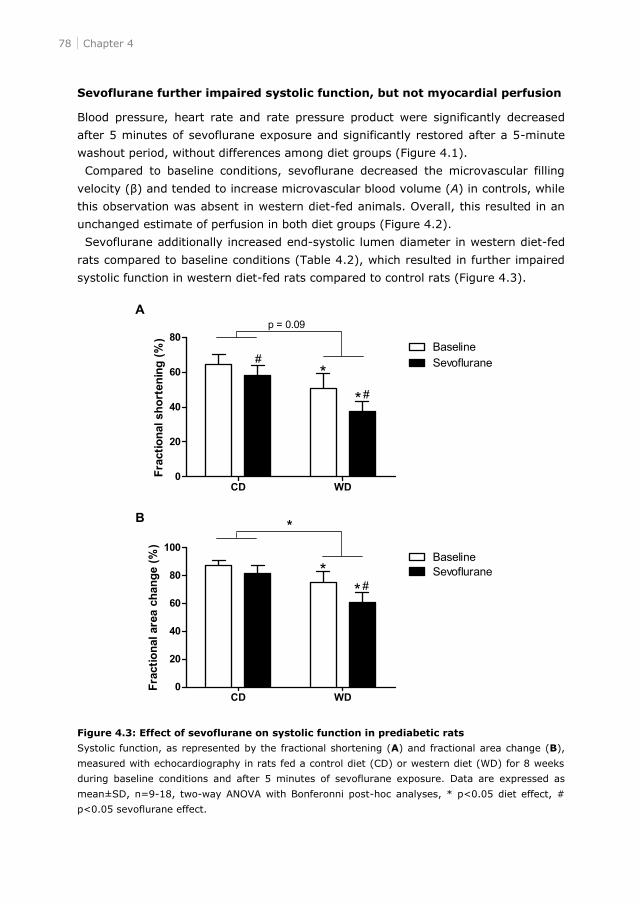
78 Chapter 4
Sevoflurane further impaired systolic function, but not myocardial perfusion
Blood pressure, heart rate and rate pressure product were significantly decreased
after 5 minutes of sevoflurane exposure and significantly restored after a 5-minute
washout period, without differences among diet groups (Figure 4.1).
Compared to baseline conditions, sevoflurane decreased the microvascular filling
tended to increase microvascular blood volume (A) in controls, while
this observation was absent in western diet-fed animals. Overall, this resulted in an
unchanged estimate of perfusion in both diet groups (Figure 4.2).
Sevoflurane additionally increased end-systolic lumen diameter in western diet-fed
rats compared to baseline conditions (Table 4.2), which resulted in further impaired
systolic function in western diet-fed rats compared to control rats (Figure 4.3).
Figure 4.3: Effect of sevoflurane on systolic function in prediabetic rats
Systolic function, as represented by the fractional shortening (A) and fractional area change (B),
measured with echocardiography in rats fed a control diet (CD) or western diet (WD) for 8 weeks
during baseline conditions and after 5 minutes of sevoflurane exposure. Data are expressed as
mean±SD, n=9-18, two-way ANOVA with Bonferonni post-hoc analyses, * p<0.05 diet effect, #
p<0.05 sevoflurane effect.
Sevoflurane and myocardial perfusion in prediabetes 79
Discussion
In the present study, we examined the effect of sevoflurane on myocardial perfusion
and function in western diet-fed rats. We found that short-term western diet feeding
resulted in a prediabetic phenotype characterized by obesity and hyperglycemia.
Further, diet-induced prediabetes was associated with impaired myocardial perfusion
and systolic dysfunction. Sevoflurane had no overall effect on myocardial perfusion in
healthy and prediabetic rats, while systolic function was even further impaired. These
results suggest that sevoflurane leads to uncoupling of myocardial perfusion and
function, irrespective of the metabolic state.
Sevoflurane did not affect myocardial perfusion, despite of decreased arterial blood
pressure, heart frequency and rate pressure product in healthy rats. Previously it has
indeed been shown that sevoflurane did not alter myocardial blood flow in healthy
rats20 and healthy subjects6 compared to the awake condition. In contrast, others
however described decreased myocardial blood flow in healthy rats,8 dogs9 and
pigs.10 In addition to species variation and the use of different experimental
techniques,19 administration of general anesthetics may explain the contrasting
observations, as this may distinctly alter hemodynamics compared to the awake
state. While myocardial perfusion remained unchanged, sevoflurane decreased the
A). The
microvascular filling velocity is a parameter of the capillary exchange rate providing
an estimate of the speed of erythrocytes through the capillaries, while microvascular
blood volume suggests the surface area for exchange of nutrients and correlates with
oxygen consumption. Our observations are in contrast with a previously performed
study in healthy subjects by our group, where we showed that sevoflurane decreased
myocardial blood volume and increased the microvascular filling velocity.6 A possible
mechanism to explain these differences may be derived by the differences in heart
rate among species. We found a decrease in heart rate, while in healthy subjects an
increase in heart rate was shown.6 However, also decreased8 or unchanged20 heart
rate in rats are found. Taken together, although sevoflurane impaired the
microvascular filling velocity, myocardial perfusion was not affected in healthy rats.
Moreover, the present study showed that myocardial perfusion and function were
both decreased in prediabetic rats compared to healthy controls. In detail,
microvascular blood volume was decreased, which resulted in impairment of
myocardial perfusion. Previously, we found that myocardial perfusion was maintained
during baseline conditions in high fat diet-induced glucose intolerant rats.14 The
present study used a more severe diet, which resulted in more pronounced
disturbances in the cardiometabolic condition of the rats. Independent of glucose
tolerance and obesity, myocardial perfusion defects were found in prediabetic insulin
resistant patients.15;16 In T2DM patients, no differences in myocardial blood flow
were found during fasting conditions.17;18 However, during the postprandial state
4
80 Chapter 4
decreased myocardial blood flow was found in T2DM patients,17;18 which is in
agreement with the present study showing decreased myocardial perfusion in non-
fasted prediabetic rats. An underlying mechanism of this impaired myocardial
perfusion might be alterations in insulin-mediated recruitment of the capillaries. In
healthy subjects, insulin increased basal21 and adenosine-stimulated22 myocardial
perfusion. Moreover, insulin directly affects myocardial perfusion by enhancing
hyperemic myocardial blood flow in a dose-dependent manner in healthy subjects.23
However, insulin resistance may block insulin-mediated capillary recruitment.24 In
T2DM patients, the use of an insulin analog partially reversed myocardial perfusion
abnormalities.18
As far as we know, we are the first to study the effect of sevoflurane anesthesia on
myocardial perfusion in prediabetic rats. Our results show that sevoflurane has a
stronger cardiodepressive effect in prediabetic rats, whereas myocardial perfusion
remained unaffected. Under physiological conditions, myocardial blood flow and
function are in balance.25 In our prediabetic rats, myocardial perfusion as well as
myocardial function are decreased. However, during sevoflurane myocardial
perfusion is maintained, while myocardial function is decreased in healthy and
prediabetic rats. This uncoupling of perfusion and function suggests that despite of
increased microvascular blood volume and decreased microvascular filling velocity,
myocardial function cannot be maintained.
In conclusion, the present study showed impaired myocardial function and
perfusion in diet-induced prediabetic rats. Moreover, sevoflurane further impaired
systolic function, but myocardial perfusion was maintained. These results suggest
that sevoflurane leads to uncoupling of myocardial perfusion and function,
irrespective of the metabolic state of the heart.
Sevoflurane and myocardial perfusion in prediabetes 81
References
1. Dole WP: Autoregulation of the coronary circulation. Prog Cardiovasc Dis 1987, 29:293-323.
2. Hoffman JI, Spaan JA: Pressure-flow relations in coronary circulation. Physiol Rev 1990,
70:331-390.
3. Malan TP, Jr., DiNardo JA, Isner RJ, Frink EJ, Jr., Goldberg M, Fenster PE, Brown EA, Depa R,
Hammond LC, Mata H: Cardiovascular effects of sevoflurane compared with those of isoflurane
in volunteers. Anesthesiology 1995, 83:918-928.
4. Park KW: Cardiovascular effects of inhalational anesthetics. Int Anesthesiol Clin 2002, 40:1-14.
5. Larach DR, Schuler HG: Direct vasodilation by sevoflurane, isoflurane, and halothane alters
coronary flow reserve in the isolated rat heart. Anesthesiology 1991, 75:268-278.
6. Bulte CS, Slikkerveer J, Kamp O, Heymans MW, Loer SA, de Marchi SF, Vogel R, Boer C,
Bouwman RA: General anesthesia with sevoflurane decreases myocardial blood volume and
hyperemic blood flow in healthy humans. Anesth Analg 2013, 116:767-774.
7. Crystal GJ, Zhou X, Gurevicius J, Czinn EA, Salem MR, Alam S, Piotrowski A, Hu G: Direct
coronary vasomotor effects of sevoflurane and desflurane in in situ canine hearts.
Anesthesiology 2000, 92:1103-1113.
8. Conzen PF, Vollmar B, Habazettl H, Frink EJ, Peter K, Messmer K: Systemic and regional
hemodynamics of isoflurane and sevoflurane in rats. Anesth Analg 1992, 74:79-88.
9. Hirano M, Fujigaki T, Shibata O, Sumikawa K: A comparison of coronary hemodynamics during
isoflurane and sevoflurane anesthesia in dogs. Anesth Analg 1995, 80:651-656.
10.Manohar M, Parks CM: Porcine systemic and regional organ blood flow during 1.0 and 1.5
minimum alveolar concentrations of sevoflurane anesthesia without and with 50% nitrous oxide.
J Pharmacol Exp Ther 1984, 231:640-648.
11.Preis SR, Pencina MJ, Hwang SJ, D'Agostino RB, Sr., Savage PJ, Levy D, Fox CS: Trends in
cardiovascular disease risk factors in individuals with and without diabetes mellitus in the
Framingham Heart Study. Circulation 2009, 120:212-220.
12.Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ,
Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L: Derivation and prospective
validation of a simple index for prediction of cardiac risk of major noncardiac surgery.
Circulation 1999, 100:1043-1049.
13.van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009,
8:39.
14.van den Brom CE, Bulte CS, Kloeze BM, Loer SA, Boer C, Bouwman RA: High fat diet-induced
glucose intolerance impairs myocardial function, but not myocardial perfusion during
hyperaemia: a pilot study. Cardiovasc Diabetol 2012, 11:74.
15.Nasr G, Sliem H: Silent myocardial ischemia in prediabetics in relation to insulin resistance. J
Cardiovasc Dis Res 2010, 1:116-121.
16.Nasr G, Sliem H: Silent ischemia in relation to insulin resistance in normotensive prediabetic
adults: early detection by single photon emission computed tomography (SPECT). Int J
Cardiovasc Imaging 2011, 27:335-341.
17.Scognamiglio R, Negut C, De Kreutzenberg SV, Tiengo A, Avogaro A: Postprandial myocardial
perfusion in healthy subjects and in type 2 diabetic patients. Circulation 2005, 112:179-184.
4
82 Chapter 4
18.Scognamiglio R, Negut C, De Kreutzenberg SV, Tiengo A, Avogaro A: Effects of different insulin
regimes on postprandial myocardial perfusion defects in type 2 diabetic patients. Diabetes Care
2006, 29:95-100.
19.Bulte CS, Slikkerveer J, Meijer RI, Gort D, Kamp O, Loer SA, de Marchi SF, Vogel R, Boer C,
Bouwman RA: Contrast-enhanced ultrasound for myocardial perfusion imaging. Anesth Analg
2012, 114:938-945.
20.Crawford MW, Lerman J, Saldivia V, Carmichael FJ: Hemodynamic and organ blood flow
responses to halothane and sevoflurane anesthesia during spontaneous ventilation. Anesth
Analg 1992, 75:1000-1006.
21.Liu Z: Insulin at physiological concentrations increases microvascular perfusion in human
myocardium. Am J Physiol Endocrinol Metab 2007, 293:E1250-E1255.
22.Laine H, Nuutila P, Luotolahti M, Meyer C, Elomaa T, Koskinen P, Ronnemaa T, Knuuti J: Insulin-
induced increment of coronary flow reserve is not abolished by dexamethasone in healthy young
men. J Clin Endocrinol Metab 2000, 85:1868-1873.
23.Sundell J, Nuutila P, Laine H, Luotolahti M, Kalliokoski K, Raitakari O, Knuuti J: Dose-dependent
vasodilating effects of insulin on adenosine-stimulated myocardial blood flow. Diabetes 2002,
51:1125-1130.
24.Zhang L, Vincent MA, Richards SM, Clerk LH, Rattigan S, Clark MG, Barrett EJ: Insulin
sensitivity of muscle capillary recruitment in vivo. Diabetes 2004, 53:447-453.
25.Heusch G, Schulz R: The relation of contractile function to myocardial perfusion. Perfusion-
contraction match and mismatch. Herz 1999, 24:509-514.


CE van den Brom, C Boer, RPF van den Akker, J van der Velden,
SA Loer, RA Bouwman
Submitted
5Diet composition modulates sevoflurane-
induced myocardial depression in rats

Dietary effects on the heart during sevoflurane 87
Abstract
Introduction
Cardiometabolic diseases like obesity and/or diabetes mellitus may alter the effects
of sevoflurane on the heart, but current evidence is limited to in vitro studies. This
study evaluated the influence of western diet-induced obesity with glucose
intolerance on the myocardial response to sevoflurane, and further elaborated
whether lowering caloric intake can modulate this effect.
Methods
Male Wistar rats were exposed to a western diet (WD) or control diet (CD) for 8
weeks. A third group of WD-fed rats reversed after 4 weeks to CD for 4 consecutive
weeks. Study parameters included an oral glucose tolerance test, echocardiography
and protein analyses before and after exposure to 2% sevoflurane.
Results
Eight weeks of WD-feeding resulted in a prediabetic phenotype with obesity, glucose
intolerance, mild hyperglycemia, hyperinsulinemia, dyslipidemia and reduced
myocardial systolic and diastolic function. While sevoflurane did not alter myocardial
contractile function in healthy control animals, systolic function in WD-fed rats was
further impaired after sevoflurane exposure. Reversion of WD to control diet
normalized the prediabetic phenotype, and restored myocardial function during
baseline and after sevoflurane exposure to control values. Western diet and diet
reversal exerted distinct effects on myocardial calcium handling proteins, while
changes in proteins related to substrate metabolism were only minimal.
Conclusions
Sevoflurane is a stronger cardiodepressant in prediabetic than in control rats, which
could be restored by lowering caloric intake. These results suggest that normalization
of the cardiometabolic profile by dietary changes are of direct influence on the
myocardial response to sevoflurane in rats.
5
88 Chapter 5
Introduction
Patients with obesity and type 2 diabetes mellitus (T2DM) due to excessive caloric
intake may exert a different response to anesthesia and surgery than healthy
subjects. In healthy subjects, volatile anesthetics like sevoflurane exhibit negative
inotropic effects as shown by depressed myocardial contractility,1;2 lusitropic effects
as reflected by early diastolic dysfunction1;3 and decreased systemic vascular
resistance.3 While it may be expected that cardiometabolic alterations induced by
obesity and/or diabetes mellitus alter the response of the heart to volatile
anesthetics, most studies focusing on this relationship are limited by their in vitro
nature and the use of models for type 1 diabetes mellitus. Moreover, the results are
conflicting, showing either augmentation4 or suppression5 of the cardiodepressive
effects of volatile anesthetics in papillary muscles of type 1 diabetic rats. A third
study suggested that the inotropic effects of several volatile anesthetics were not
altered in single ventricular myocytes from type 1 diabetic rats.6
These findings warrant further exploration of the effects of obesity and/or diabetes
mellitus on the interaction of volatile anesthetics with the heart. Moreover,
increasing evidence suggests that preoperative alterations in dietary composition and
intake may alter the susceptibility of the cardiovascular system to surgical and
anesthetic stress.7 It has indeed been shown that diet-induced obesity8-11 and
T2DM12;13 in small rodents is reversible by reducing caloric intake, which resulted in
weight loss and improved insulin sensitivity. In obese and T2DM patients, a low
caloric diet decreased myocardial fatty acid uptake14 and improved diastolic
function,15 respectively. Additionally, preoperative dietary restriction exerted
favorable effects on surgery-related inflammation, oxidative stress and ischemia.7;16
It is however unknown whether the interaction of volatile anesthesia with myocardial
function can be altered by dietary intake. In the present study we therefore
investigated whether western diet-induced obesity with glucose intolerance alters the
effects of the volatile anesthetic sevoflurane on myocardial function and calcium
handling proteins in rats, and whether changing diet composition can modulate these
alterations.
Dietary effects on the heart during sevoflurane 89
Methods
Animals and experimental set-up
All animal experiments were approved by the Institutional Animal Care and Use
Committee of the VU University, and were conducted following the European
Convention for the Protection of Vertebrate Animals used for Experimental and Other
Scientific Purposes, and the guide for the Care and Use of Laboratory Animals. The
performed research is in compliance with the modern ARRIVE guidelines on animal
research.17
The first part of the study was performed in a group of 24 male Wistar rats
(baseline body weight: 264±5 g; Charles River Laboratories, France). Rats were
exposed to a western diet in combination with sucrose water (20%) (WD, n=16) or
control diet (CD, n=8) for a period of 8 weeks. Four weeks after the start of the diet
exposure, WD (n=8) exposed rats reversed to CD for 4 consecutive weeks. Rats
were housed in a temperature-controlled room (20-23°C; 40-60% humidity) under a
12/12h light/dark cycle starting at 6.00 am. Body weight and caloric intake were
determined on a weekly basis. After 4 and 8 weeks of diet exposure, rats underwent
an oral glucose tolerance test and echocardiography. After a 6h fasting period, rats
were sacrificed by decapitation, trunk blood was collected for plasma determinations
and hearts were removed, rinsed in saline, weighted, snap-frozen in liquid nitrogen
and stored at -80°C until further analysis.
The second part of the study included 30 male Wistar rats (baseline body weight:
262±6 g; Charles River Laboratories, France) that were either exposed to the control
diet (CD, n=10), western diet in combination with sucrose water (20%) (WD, n=10)
or the western diet with reversal to control diet (REV, n=10) as described above.
After 8 weeks, rats were exposed to sevoflurane (AbbVie, the Netherlands). Rats
were sacrificed by decapitation without fasting, trunk blood was collected for plasma
determinations and hearts were removed, rinsed in saline, weighted, snap-frozen in
liquid nitrogen and stored at -80°C until further analysis.
Diets
Control diet (CD; Teklad 2016, Harlan, Horst, the Netherlands) consisted of 20 %kcal
protein, 9 %kcal fat and 74 %kcal carbohydrates (1804 kcal/kg starch, 200 kcal/kg
sugars), whereas western diet (WD; D12451, Research Diets, New Brunswick, NJ)
consisted of 20 %kcal protein, 45 %kcal fat and 35 %kcal carbohydrates (291
kcal/kg starch, 691 kcal/kg sugars) with 20% sucrose water (800 kcal/kg), totally
containing 3300 kcal/kg and 4857 kcal/kg for CD and WD with sucrose water,
respectively.
5
90 Chapter 5
Oral glucose tolerance test
Awake rats fasted overnight received an oral glucose load (2 g/kg of body weight).
Blood glucose was measured from tail bleeds with a Precision Xceed Blood Glucose
monitoring system (MediSense, UK) before and 15, 30, 60, 90 and 120 min after
glucose ingestion. At similar time points, plasma insulin (LINCO research, St.
Charles, Missouri) levels were measured as described previously.18;19
Echocardiography
Echocardiography (ALOKA ProSound SSD 4000, Aloka, Tokyo, Japan) using a 13-MHz
linear interfaced array transducer was performed after 4 and 8 weeks as described
previously.18-21 Briefly, rats received S-Ketamine (Ketanest®, 75 mg/kg, Pfizer, the
Netherlands) and diazepam (4 mg/kg, Centrafarm, the Netherlands) anesthesia
intraperitoneally, allowed spontaneous respiration and placed on a underbody
heating pad. Left ventricular (LV) dimensions during end-systole (ES) and end-
diastole (ED) were determined in the M- (motion) mode of the parasternal short-axis
view at the level of the papillary muscles. LV systolic function is represented by
fractional shortening (FS) and fractional area change (FAC), which were calculated
by the equations: FS = (EDD- 2-ESD2)/EDD2 100).
Diastolic function was measured in the apical four-chamber view and shown as E
flow, E deceleration time and isovolumic relaxation time (IVRT; except 8 weeks
data). LV mass was calculated as described previously.18 All parameters were
averaged over at least three cardiac cycles. Analyses were performed off-line
(Image-Arena 2.9.1, TomTec Imaging Systems, Unterschleissheim/Munich,
Germany).
Sevoflurane intervention
The second group of rats was anesthetized with 125 mg/kg S-ketamine (Ketanest®,
Pfizer, the Netherlands) and 4 mg/kg diazepam (Centrafarm, the Netherlands)
intraperitoneally and maintenance was performed with 40 mg/kg/h S-ketamine and
1 mg/kg/h diazepam intravenously in the tail vein and allowed spontaneous
(AbbVie,
the Netherlands) in 40% O2/60% N2, whereas control rats received only 40%
O2/60% N2 for the same time period (baseline, n=4). Measurement of systolic
performed as described above.
Dietary effects on the heart during sevoflurane 91
Blood and plasma measurements
Plasma hematocrit levels were determined using microcentrifugation. Plasma glucose
levels (Abcam, Cambridge, MA), plasma insulin (LINCO research, St. Charles,
Missouri), plasma free fatty acids (WAKO NEFA-HR, Wako Pure Chemical Industries,
Osaka, Japan), plasma triglyceride (Sigma, Saint Louis, Missouri), and plasma HDL
and LDL/VLDL cholesterol (Abcam, Cambridge, MA) levels were measured from trunk
blood as described previously.18-21
Protein analysis
LV tissues were homogenized to obtain cytoplasmic protein fractions for western blot
analysis as previously described.18;20;21 Phosphorylation and/or expression of
signaling intermediates were analyzed using the following primary antibodies: Akt,
phospho-Akt- - -Ser9,
- -Thr172 (all Cell signaling
Technology, Beverly, MA), pyruvate dehydrogenase kinase 4 (PDK4, Santa Cruz
Biotechnology, Santa Cruz, CA), glucose transporter 4 (GLUT4; Abcam, Cambridge,
MA), phospholamban (PLB), phospho-PLB-Ser16, (Upstate, Lake Placid, NY),
sarcoplasmic reticulum calcium ATPase 2a (SERCA2a)21 and fatty acid transporter
(FAT)/CD36 (MO25).18;21 All signals were normalized to total protein expression or
actin (Sigma, Saint Louis, Missouri).
Myofilament protein phosphorylation was determined using Pro-Q Diamond
Phosphoprotein Stain as described previously.22 LV tissues were separated on
gradient gels (Criterion tris-HCl 4-15% gel, BioRad) and proteins were stained with
Pro-Q Diamond Phosphoprotein Stain. Subsequently gels were stained overnight with
SYPRO Ruby stain (Molecular Probes). Phosphorylation status of myosin binding
protein-C (MyBP-C), troponin T (TnT) and cardiac troponin I (cTnI) were expressed
relative to SYPRO-stained protein bands to correct for differences in sample loading.
Staining was visualized using the LAS-3000 Image Reader (FUJI; 460 nm/605 nm
Ex/Em) and immunoblots were quantified by densitometric analysis of films (AIDA,
4.21.033, Raytest, Strau-benhardt Germany).
Histology
Sections (4 μm) of left ventricular tissue from the free wall at the level of the
papillary muscles were cut in the direction of the fibers and mounted on 3-
aminopropyltriethoxisilane-coated slides (Superfrost® Plus, Menzal, Darmstadt,
Germany). After deparaffinization and rehydration, cardiomyocyte cross-sectional
area was determined in randomly chosen fields of hematoxylin-eosin stained sections
for 20-30 cells per heart and normalized to sarcomere length.18;20;21
5

92 Chapter 5
Statistical analysis
Data were analyzed using Graphpad Prism 5.0 (La Jolla, USA) and are presented as
mean±SD. Statistical analyses were performed using a student t-test after 4 weeks,
one-way ANOVA with Bonferroni post-hoc analysis after 8 weeks, two-way ANOVA
with repeated measures and Bonferroni post-hoc analysis for the oral glucose
tolerance test and two-way ANOVA with Bonferroni post-hoc analysis for data after 8
weeks with sevoflurane intervention. p<0.05 was considered as statistically
significant.
Dietary effects on the heart during sevoflurane 93
Results
Animal model characteristics
Western diet (WD) feeding resulted in a prediabetic phenotype with obesity, mild
hyperglycemia, hyperinsulinemia, hyperlipidemia and glucose intolerance at 4 and 8
weeks after initiation of the diet (Table 5.1 and Figure 5.1 A-F). Reversion to a
control diet (REV) after 4 weeks of western diet feeding resulted in normalization of
caloric intake and body weight, and reversed the prediabetic phenotype in western
diet-fed rats.
Heart weight and the cross sectional area of individual cardiomyocytes were
significantly increased in WD-fed rats compared to controls, and these values
normalized after diet reversal. Additionally, diet reversion following western diet
feeding resulted in a decrease in liver weight and epididymal and perirenal fat pads
(Table 5.1).
At 4 and 8 weeks, western diet feeding decreased myocardial lumen diameter and
increased wall thickness during diastole when compared to control rats (Table 5.2).
Moreover, end-systolic lumen diameter was increased at 4 and 8 weeks of western
diet feeding, while systolic wall thickness was slightly reduced after 4 weeks of diet
exposure. Reversal from western to control diet resulted in normalization of systolic
lumen diameter and myocardial diastolic and systolic wall thickness, while the
diastolic lumen diameter was not affected by lowering caloric intake (Table 5.2).
Western diet feeding induced a reduction in myocardial fractional shortening (Figure
5.2A) and fractional area change (Figure 5.2B), which could be restored by diet
reversal. While E flow was unchanged by WD-feeding, the deceleration time of the E
peak and isovolumic relaxation time at 4 weeks were prolonged in rats fed a WD
when compared to control rats (Table 5.2). After 8 weeks of diet exposure, there
was a trend towards impaired left ventricular relaxation in WD-fed rats. Diet reversal
improved diastolic function as shown by a shortening of the E deceleration time when
compared to WD-fed rats (Table 5.2).
5
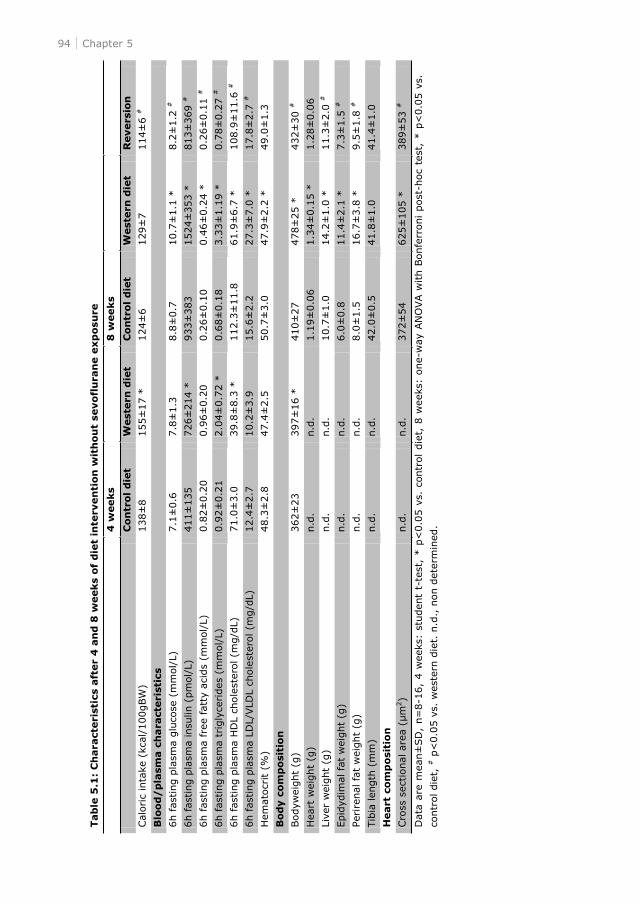
94 Chapter 5 Tab
le 5
.1:
Ch
ara
cteri
stic
s aft
er
4 a
nd
8 w
eeks
of
die
t in
terv
en
tion
wit
hou
t se
vofl
ura
ne e
xp
osu
re
4
weeks
8
weeks
C
on
trol
die
t W
est
ern
die
t C
on
trol
die
t
West
ern
die
t R
evers
ion
Cal
ori
c in
take
(kc
al/1
00gBW
) 138±
8
155±
17 *
124±
6
129±
7
114±
6 #
Blo
od
/p
lasm
a c
hara
cteri
stic
s
6h fas
ting p
lasm
a g
luco
se (
mm
ol/
L)
7.1
±0.6
7.8
±1.3
8.8
±0.7
10.7
±1.1
*
8.2
±1.2
#
6h fas
ting p
lasm
a in
sulin
(pm
ol/
L)
411±
135
726±
214 *
933±
383
1524±
353 *
813±
369 #
6h fas
ting p
lasm
a fr
ee fat
ty a
cids
(mm
ol/
L)
0.8
2±
0.2
0
0.9
6±
0.2
0
0.2
6±
0.1
0
0.4
6±
0.2
4 *
0.2
6±
0.1
1 #
6h fas
ting p
lasm
a tr
igly
cerides
(m
mol/
L)
0.9
2±
0.2
1
2.0
4±
0.7
2 *
0.6
8±
0.1
8
3.3
3±
1.1
9 *
0.7
8±
0.2
7 #
6h fas
ting p
lasm
a H
DL
chole
ster
ol (m
g/d
L)
71.0
±3.0
39.8
±8.3
*
112.3
±11.8
61.9
±6.7
*
108.9
±11.6
#
6h fas
ting p
lasm
a LD
L/VLD
L ch
ole
ster
ol (m
g/d
L)
12.4
±2.7
10.2
±3.9
15.6
±2.2
27.3
±7.0
*
17.8
±2.7
#
Hem
ato
crit (
%)
48.3
±2.8
47.4
±2.5
50.7
±3.0
47.9
±2.2
*
49.0
±1.3
Bod
y c
om
po
siti
on
Bodyw
eight
(g)
362±
23
397±
16 *
410±
27
478±
25 *
432±
30 #
Hea
rt w
eight
(g)
n.d
. n.d
. 1.1
9±
0.0
6
1.3
4±
0.1
5 *
1.2
8±
0.0
6
Live
r w
eight
(g)
n.d
. n.d
. 10.7
±1.0
14.2
±1.0
*
11.3
±2.0
#
Epid
ydim
al fa
t w
eight
(g)
n.d
. n.d
. 6.0
±0.8
11.4
±2.1
*
7.3
±1.5
#
Peri
renal
fat
wei
ght
(g)
n.d
. n.d
. 8.0
±1.5
16.7
±3.8
*
9.5
±1.8
#
Tib
ia len
gth
(m
m)
n.d
. n.d
. 42.0
±0.5
41.8
±1.0
41.4
±1.0
Heart
com
posi
tio
n
Cro
ss s
ectional
are
a (
2)
n.d
. n.d
. 372±
54
625±
105 *
389±
53 #
Dat
a ar
e m
ean±
SD
, n=
8-1
6,
4 w
eeks
: st
uden
t t-
test
, * p
<0.0
5 v
s. c
ontr
ol
die
t, 8
wee
ks:
one-w
ay A
NO
VA w
ith B
onfe
rroni post
-hoc
test
, * p
<0.0
5 v
s.
contr
ol die
t, #
p<
0.0
5 v
s. w
este
rn d
iet.
n.d
., n
on d
eter
min
ed.
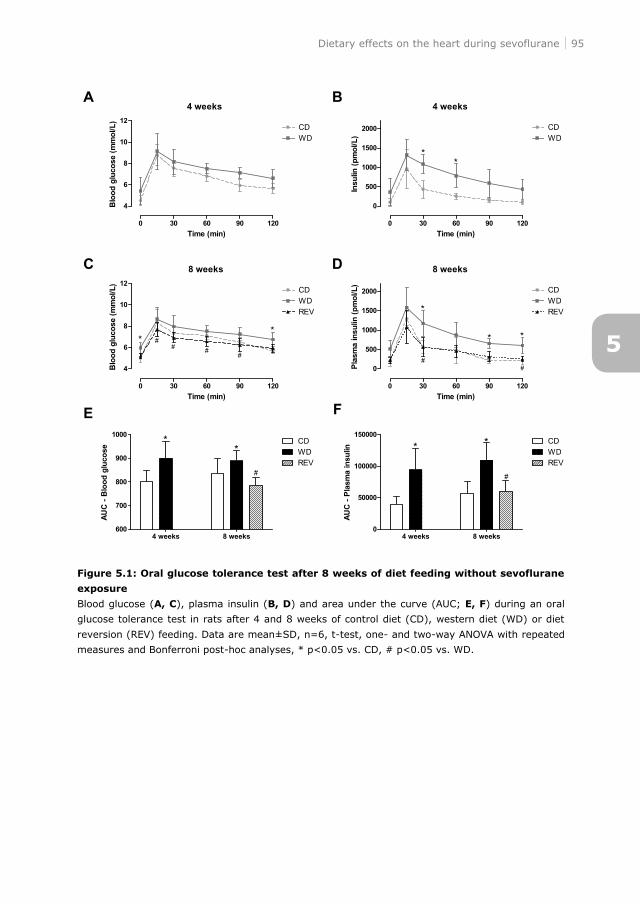
Dietary effects on the heart during sevoflurane 95
Figure 5.1: Oral glucose tolerance test after 8 weeks of diet feeding without sevoflurane
exposure
Blood glucose (A, C), plasma insulin (B, D) and area under the curve (AUC; E, F) during an oral
glucose tolerance test in rats after 4 and 8 weeks of control diet (CD), western diet (WD) or diet
reversion (REV) feeding. Data are mean±SD, n=6, t-test, one- and two-way ANOVA with repeated
measures and Bonferroni post-hoc analyses, * p<0.05 vs. CD, # p<0.05 vs. WD.
5
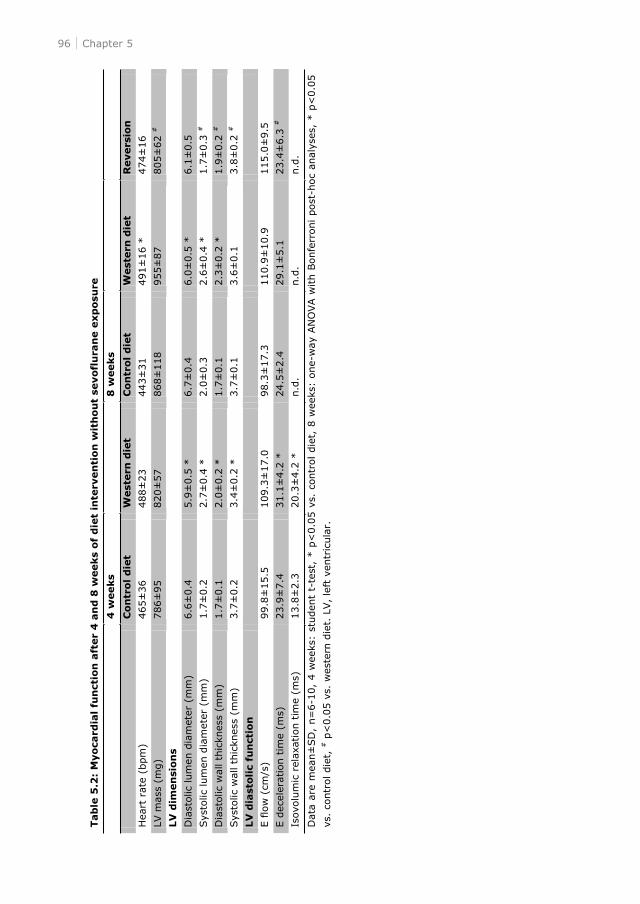
96 Chapter 5 Tab
le 5
.2:
Myoca
rdia
l fu
nct
ion
aft
er
4 a
nd
8 w
eeks
of
die
t in
terv
en
tion
wit
ho
ut
sevofl
ura
ne e
xp
osu
re
4
weeks
8
weeks
C
on
trol
die
t W
est
ern
die
t C
on
trol
die
t W
est
ern
die
t R
evers
ion
Hea
rt r
ate
(bpm
) 465±
36
488±
23
443±
31
491±
16 *
474±
16
LV m
ass
(mg)
786±
95
820±
57
868±
118
955±
87
805±
62 #
LV
dim
en
sion
s
Dia
stol
ic lum
en d
iam
eter
(m
m)
6.6
±0.4
5.9
±0.5
*
6.7
±0.4
6.0
±0.5
*
6.1
±0.5
Sys
tolic
lum
en d
iam
eter
(m
m)
1.7
±0.2
2.7
±0.4
*
2.0
±0.3
2.6
±0.4
*
1.7
±0.3
#
Dia
stol
ic w
all th
ickn
ess
(mm
) 1.7
±0.1
2.0
±0.2
*
1.7
±0.1
2.3
±0.2
*
1.9
±0.2
#
Sys
tolic
wal
l th
ickn
ess
(mm
) 3.7
±0.2
3.4
±0.2
*
3.7
±0.1
3.6
±0.1
3.8
±0.2
#
LV
dia
stoli
c fu
nct
ion
E flo
w (
cm/s
) 99.8
±15.5
109.3
±17.0
98.3
±17.3
110.9
±10.9
115.0
±9.5
E d
ecel
erat
ion t
ime
(ms)
23.9
±7.4
31.1
±4.2
*
24.5
±2.4
29.1
±5.1
23.4
±6.3
#
Isovo
lum
ic r
elaxa
tion t
ime
(ms)
13.8
±2.3
20.3
±4.2
*
n.d
. n.d
. n.d
.
Dat
a ar
e m
ean±
SD
, n=
6-1
0,
4 w
eeks
: st
uden
t t-
test
, * p
<0.0
5 v
s. c
ontr
ol die
t, 8
wee
ks:
one-w
ay A
NO
VA w
ith B
onfe
rroni post
-hoc
anal
yses
, * p
<0.0
5
vs.
contr
ol die
t, #
p<
0.0
5 v
s. w
este
rn d
iet.
LV,
left
ven
tric
ula
r.
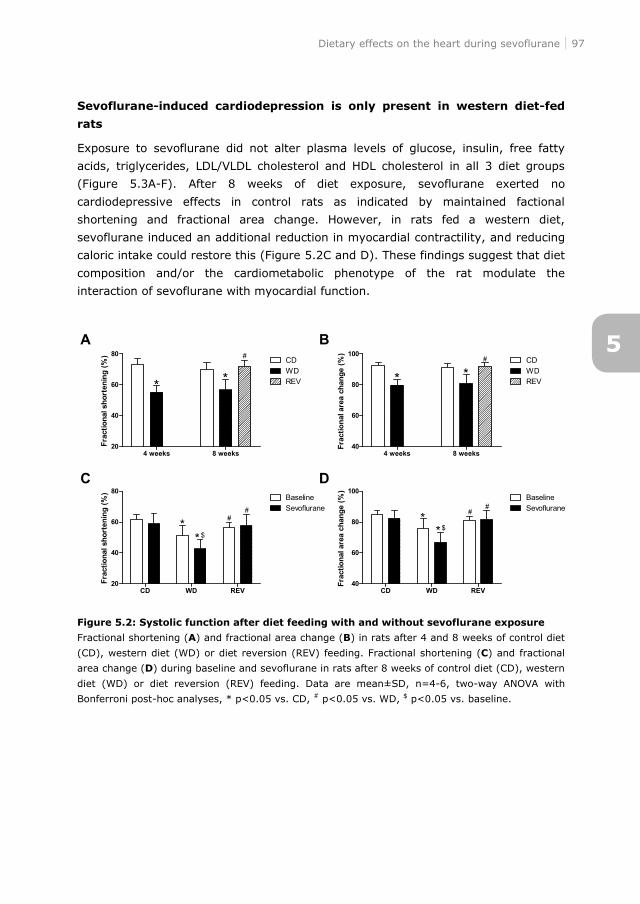
Dietary effects on the heart during sevoflurane 97
Sevoflurane-induced cardiodepression is only present in western diet-fed
rats
Exposure to sevoflurane did not alter plasma levels of glucose, insulin, free fatty
acids, triglycerides, LDL/VLDL cholesterol and HDL cholesterol in all 3 diet groups
(Figure 5.3A-F). After 8 weeks of diet exposure, sevoflurane exerted no
cardiodepressive effects in control rats as indicated by maintained factional
shortening and fractional area change. However, in rats fed a western diet,
sevoflurane induced an additional reduction in myocardial contractility, and reducing
caloric intake could restore this (Figure 5.2C and D). These findings suggest that diet
composition and/or the cardiometabolic phenotype of the rat modulate the
interaction of sevoflurane with myocardial function.
Figure 5.2: Systolic function after diet feeding with and without sevoflurane exposure
Fractional shortening (A) and fractional area change (B) in rats after 4 and 8 weeks of control diet
(CD), western diet (WD) or diet reversion (REV) feeding. Fractional shortening (C) and fractional
area change (D) during baseline and sevoflurane in rats after 8 weeks of control diet (CD), western
diet (WD) or diet reversion (REV) feeding. Data are mean±SD, n=4-6, two-way ANOVA with
Bonferroni post-hoc analyses, * p<0.05 vs. CD, # p<0.05 vs. WD, $ p<0.05 vs. baseline.
5
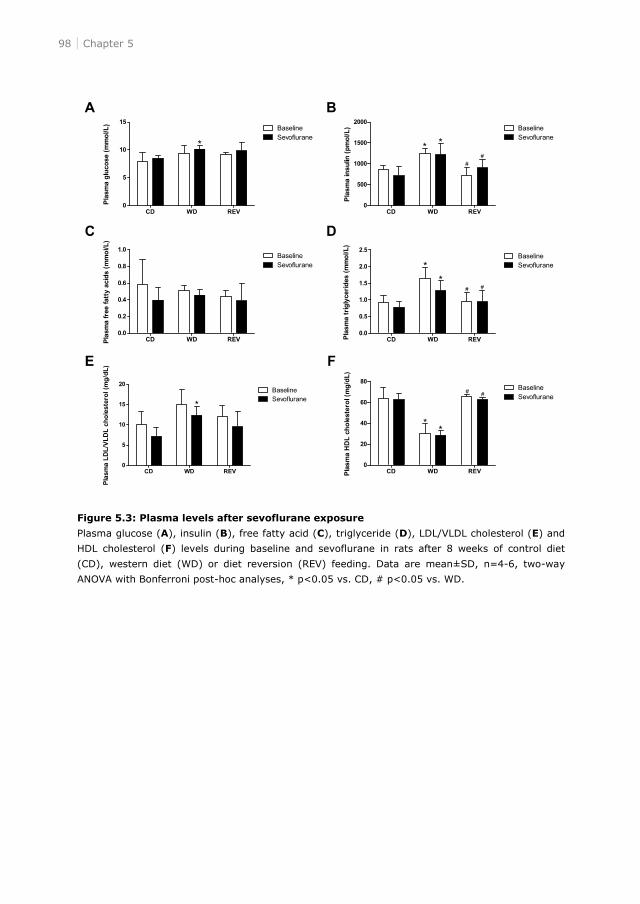
98 Chapter 5
Figure 5.3: Plasma levels after sevoflurane exposure
Plasma glucose (A), insulin (B), free fatty acid (C), triglyceride (D), LDL/VLDL cholesterol (E) and
HDL cholesterol (F) levels during baseline and sevoflurane in rats after 8 weeks of control diet
(CD), western diet (WD) or diet reversion (REV) feeding. Data are mean±SD, n=4-6, two-way
ANOVA with Bonferroni post-hoc analyses, * p<0.05 vs. CD, # p<0.05 vs. WD.
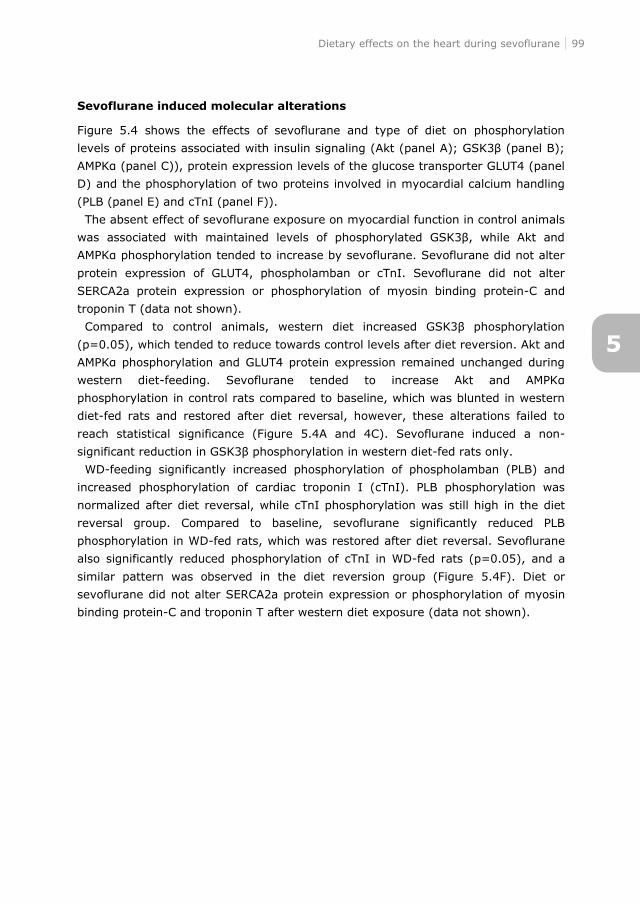
Dietary effects on the heart during sevoflurane 99
Sevoflurane induced molecular alterations
Figure 5.4 shows the effects of sevoflurane and type of diet on phosphorylation
D) and the phosphorylation of two proteins involved in myocardial calcium handling
(PLB (panel E) and cTnI (panel F)).
The absent effect of sevoflurane exposure on myocardial function in control animals
protein expression of GLUT4, phospholamban or cTnI. Sevoflurane did not alter
SERCA2a protein expression or phosphorylation of myosin binding protein-C and
troponin T (data not shown).
(p=0.05), which tended to reduce towards control levels after diet reversion. Akt and
western diet-
phosphorylation in control rats compared to baseline, which was blunted in western
diet-fed rats and restored after diet reversal, however, these alterations failed to
reach statistical significance (Figure 5.4A and 4C). Sevoflurane induced a non-
on in western diet-fed rats only.
WD-feeding significantly increased phosphorylation of phospholamban (PLB) and
increased phosphorylation of cardiac troponin I (cTnI). PLB phosphorylation was
normalized after diet reversal, while cTnI phosphorylation was still high in the diet
reversal group. Compared to baseline, sevoflurane significantly reduced PLB
phosphorylation in WD-fed rats, which was restored after diet reversal. Sevoflurane
also significantly reduced phosphorylation of cTnI in WD-fed rats (p=0.05), and a
similar pattern was observed in the diet reversion group (Figure 5.4F). Diet or
sevoflurane did not alter SERCA2a protein expression or phosphorylation of myosin
binding protein-C and troponin T after western diet exposure (data not shown).
5
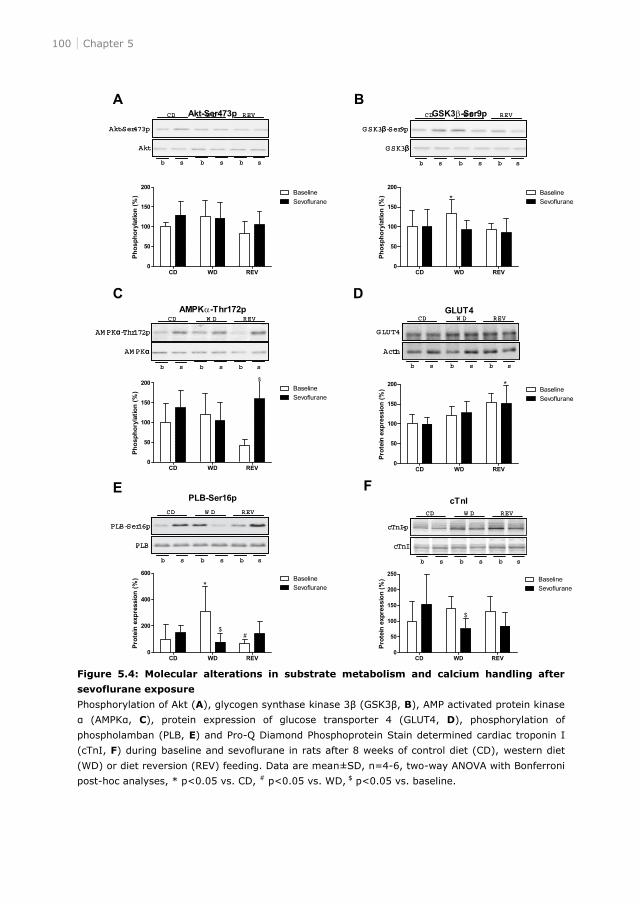
100 Chapter 5
Figure 5.4: Molecular alterations in substrate metabolism and calcium handling after
sevoflurane exposure
Phosphorylation of Akt (A), glycogen synthase kinase 3 B), AMP activated protein kinase
C), protein expression of glucose transporter 4 (GLUT4, D), phosphorylation of
phospholamban (PLB, E) and Pro-Q Diamond Phosphoprotein Stain determined cardiac troponin I
(cTnI, F) during baseline and sevoflurane in rats after 8 weeks of control diet (CD), western diet
(WD) or diet reversion (REV) feeding. Data are mean±SD, n=4-6, two-way ANOVA with Bonferroni
post-hoc analyses, * p<0.05 vs. CD, # p<0.05 vs. WD, $ p<0.05 vs. baseline.
Akt
Akt-Ser473p
CD W D REV
b s b s b s
Akt
Akt-Ser473p
CD W D REV
b s b s b s
G SK3
GSK3 -Ser9p
CD W D REV
b s b s b s
G SK3
GSK3 -Ser9p
CD W D REV
b s b s b s
AM PK
AM PK -Thr172p
CD W D REV
b s b s b s
AM PK
AM PK -Thr172p
CD W D REV
b s b s b s
Actin
GLUT4
CD W D REV
b s b s b s
Actin
GLUT4
CD W D REV
b s b s b s
PLB
PLB-Ser16p
CD W D REV
b s b s b s
PLB
PLB-Ser16p
CD W D REV
b s b s b s
cTnI
cTnI-p
CD W D REV
b s b s b s
cTnI
cTnI-p
CD W D REV
b s b s b s
Dietary effects on the heart during sevoflurane 101
Discussion
Sevoflurane exerts cardiodepressive properties in healthy subjects, therefore its
perioperative use may lead to hemodynamic alterations. Although it has been
suggested that the interaction of sevoflurane with the heart is additionally altered by
cardiometabolic diseases, most available studies are restricted to in vitro
observations and experimental models for type I diabetes mellitus. With the growing
epidemic of obesity and type 2 diabetes mellitus it might be interesting to
understand the influence of this condition on the interaction of sevoflurane with
myocardial function.
Unexpectedly, in an experimental rat model we could not show a direct effect of
sevoflurane on myocardial contractility. However, in western diet-induced obesity,
which was accompanied by glucose intolerance, hyperglycemia, hyperinsulinemia,
dyslipidemia and myocardial dysfunction, sevoflurane exerted cardiodepressive
effects. Interestingly, lowering caloric intake following western diet exposure could
reverse these effects of sevoflurane on myocardial function. These results suggest
that sevoflurane has negative inotropic effects on myocardial function in
metabolically altered hearts, and that a reduction of caloric intake may improve the
effects of sevoflurane on myocardial function. Our results therefore implicate that
diet modification may be explored as an intervention to preserve perioperative
myocardial function in subjects with cardiometabolic disease.
The present study showed that western diet feeding resulted in a prediabetic
phenotype accompanied by myocardial dysfunction. Our results confirm previous
findings showing impaired systolic function after 8 weeks of diet feeding.18
Interestingly, the present study showed that lowering caloric intake completely
normalized diet-induced T2DM. In small rodents, reducing dietary intake has been
shown to reverse diet-induced obesity8-11 and T2DM.12;13 However, it is also shown
that diet-induced obesity was not reversed by withdrawal of an energy dense
diet.23;24 Importantly, our study showed that lowering caloric intake also improved
diet-induced systolic as well as diastolic dysfunction, which is in agreement with the
clinical observation that in obese and T2DM patients a low caloric diet decreased
myocardial fatty acid uptake14 and improved diastolic function,15 respectively. Taken
together, lowering caloric intake normalized the prediabetic phenotype induced by
short-term western diet feeding and improved myocardial function.
Exposure to sevoflurane further impaired systolic function in diet-induced
prediabetes, but not in healthy rats. In contrast, sevoflurane caused a reduction in
left ventricular systolic function at concentrations of 2% and higher compared to
isoflurane in healthy mice.25 An important difference with previous findings is that in
the present study all rats were primary sedated with S-ketamine and diazepam. As
S-ketamine and diazepam may have intrinsic cardiodepressive effects,26;27 this might
5
102 Chapter 5
have blurred the additional effect of sevoflurane on the heart in control animals.
Limited data are available on the effects of sevoflurane in metabolic altered hearts.
In papillary muscles from type 1 diabetic rats, decreased sensitivity to the negative
inotropic interaction of halothane, enflurane and isoflurane was found,5 whereas
sevoflurane resulted in greater negative inotropic effects compared to controls.4 In
contrast, it has been shown that in single ventricular myocytes from type 1 diabetic
rats the inotropic effects of halothane, isoflurane, desflurane and sevoflurane were
not altered compared to controls.6 As far as we know we are the first to show the
negative inotropic effects of sevoflurane on hearts of diet-induced prediabetic rats.
A suggested underlying mechanism in the effect of sevoflurane on myocardial
function is substrate availability and metabolism,28 which is known to be altered by
T2DM.18;20;21 Unexpectedly, sevoflurane did not affect plasma glucose, insulin and
lipid levels. In humans, there is indirect evidence that volatile anesthesia increases
blood glucose; however, these observations may be biased by confounding factors
such as surgical stress.29 Compared to non-anesthetized rats without surgical stress,
sevoflurane increased plasma glucose levels, but not plasma insulin levels.30 It is
possible that glucose levels did not increase in the present study due to short
duration and low concentration of sevoflurane used, but also differences in
nutritional status may exist. Moreover, in the present study rats were sedated with
S-ketamine and diazepam. Ketamine31 and diazepam32 are known to increase blood
glucose levels, which could have abolished the additional effect of sevoflurane on
blood glucose levels.
Sevoflurane may also affect proteins related to myocardial substrate metabolism.
Akt, which regulates translocation of glucose transporter 4 (GLUT4) to the
sarcolemma for glucose uptake, is increased during sevoflurane in the isolated
ischemic rat heart.33 Moreover, sevoflurane enhances GLUT4 expression in lipid rafts,
increases glucose oxidation and decreases fatty acid oxidation after ischemia and
reperfusion injury in isolated working rat hearts.34 Although not in ischemic and
reperfused hearts, the present study showed no significant differences in proteins
related to myocardial substrate metabolism.
Another possible mechanism is altered calcium handling, which also seems a
common target in T2DM and sevoflurane. Sevoflurane reduces myocardial calcium
availability, but increases sarcoplasmic reticulum calcium content.35 In contrast,
sevoflurane decreased fractional calcium release, but maintained sarcoplasmic
reticulum calcium content.36 In papillary muscles of type 1 diabetic rats, sevoflurane
decreased myofilament calcium sensitivity to a greater extent than control rats.4 In
the present study, western diet feeding blunted phosphorylation of phospholamban
and cardiac troponin I during sevoflurane, but not SERCA2a protein expression. In
preconditioned hearts, phosphorylation of phospholamban and SERCA2a protein
expression were unaltered after ischemia and reperfusion injury;37 however, no data
were reported for non-ischemic hearts. Our data indicate that phospholamban and
Dietary effects on the heart during sevoflurane 103
cardiac troponin I might play a role in impaired systolic function in prediabetic rats
during sevoflurane.
In conclusion, sevoflurane induced cardiodepression in prediabetic rats, whereas
lowering caloric intake restored myocardial function during sevoflurane. These
results suggest that a change in dietary intake could be a potential intervention to
support the preservation of myocardial function during sevoflurane in subjects with
obesity and type 2 diabetes mellitus.
5
104 Chapter 5
References
1. Harkin CP, Pagel PS, Kersten JR, Hettrick DA, Warltier DC: Direct negative inotropic and
lusitropic effects of sevoflurane. Anesthesiology 1994, 81:156-167.
2. Pagel PS, Kampine JP, Schmeling WT, Warltier DC: Influence of volatile anesthetics on
myocardial contractility in vivo: desflurane versus isoflurane. Anesthesiology 1991, 74:900-907.
3. Malan TP, Jr., DiNardo JA, Isner RJ, Frink EJ, Jr., Goldberg M, Fenster PE, Brown EA, Depa R,
Hammond LC, Mata H: Cardiovascular effects of sevoflurane compared with those of isoflurane
in volunteers. Anesthesiology 1995, 83:918-928.
4. David JS, Tavernier B, Amour J, Vivien B, Coriat P, Riou B: Myocardial effects of halothane and
sevoflurane in diabetic rats. Anesthesiology 2004, 100:1179-1187.
5. Hattori Y, Azuma M, Gotoh Y, Kanno M: Negative inotropic effects of halothane, enflurane, and
isoflurane in papillary muscles from diabetic rats. Anesth Analg 1987, 66:23-28.
6. Graham M, Qureshi A, Noueihed R, Harrison S, Howarth FC: Effects of halothane, isoflurane,
sevoflurane and desflurane on contraction of ventricular myocytes from streptozotocin-induced
diabetic rats. Mol Cell Biochem 2004, 261:209-215.
7. Mitchell JR, Beckman JA, Nguyen LL, Ozaki CK: Reducing elective vascular surgery perioperative
risk with brief preoperative dietary restriction. Surgery 2013, 153:594-598.
8. Hill JO, Dorton J, Sykes MN, DiGirolamo M: Reversal of dietary obesity is influenced by its
duration and severity. Int J Obes 1989, 13:711-722.
9. Rogers PJ: Returning 'cafeteria-fed' rats to a chow diet: negative contrast and effects of obesity
on feeding behaviour. Physiol Behav 1985, 35:493-499.
10.Bartness TJ, Polk DR, McGriff WR, Youngstrom TG, DiGirolamo M: Reversal of high-fat diet-
induced obesity in female rats. Am J Physiol 1992, 263:R790-R797.
11.Walks D, Lavau M, Presta E, Yang MU, Bjorntorp P: Refeeding after fasting in the rat: effects of
dietary-induced obesity on energy balance regulation. Am J Clin Nutr 1983, 37:387-395.
12.Parekh PI, Petro AE, Tiller JM, Feinglos MN, Surwit RS: Reversal of diet-induced obesity and
diabetes in C57BL/6J mice. Metabolism 1998, 47:1089-1096.
13.Harris RB, Martin RJ: Changes in lipogenesis and lipolysis associated with recovery from
reversible obesity in mature female rats. Proc Soc Exp Biol Med 1989, 191:82-89.
14.Viljanen AP, Karmi A, Borra R, Parkka JP, Lepomaki V, Parkkola R, Lautamaki R, Jarvisalo M,
Taittonen M, Ronnemaa T, Iozzo P, Knuuti J, Nuutila P, Raitakari OT: Effect of caloric restriction
on myocardial fatty acid uptake, left ventricular mass, and cardiac work in obese adults. Am J
Cardiol 2009, 103:1721-1726.
15.Hammer S, Snel M, Lamb HJ, Jazet IM, van der Meer RW, Pijl H, Meinders EA, Romijn JA, de
Roos A, Smit JW: Prolonged caloric restriction in obese patients with type 2 diabetes mellitus
decreases myocardial triglyceride content and improves myocardial function. J Am Coll Cardiol
2008, 52:1006-1012.
16.Mitchell JR, Verweij M, Brand K, van d, V, Goemaere N, van den Engel S, Chu T, Forrer F, Muller
C, de JM, van IW, IJzermans JN, Hoeijmakers JH, de Bruin RW: Short-term dietary restriction
and fasting precondition against ischemia reperfusion injury in mice. Aging Cell 2010, 9:40-53.
17.Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG: Improving bioscience research
reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol 2010, 8:e1000412.
18.Ouwens DM, Diamant M, Fodor M, Habets DD, Pelsers MM, El Hasnaoui M, Dang ZC, van den
Brom CE, Vlasblom R, Rietdijk A, Boer C, Coort SL, Glatz JF, Luiken JJ: Cardiac contractile
dysfunction in insulin-resistant rats fed a high-fat diet is associated with elevated CD36-
mediated fatty acid uptake and esterification. Diabetologia 2007, 50:1938-1948.
Dietary effects on the heart during sevoflurane 105
19.van den Brom CE, Bulte CS, Kloeze BM, Loer SA, Boer C, Bouwman RA: High fat diet-induced
glucose intolerance impairs myocardial function, but not myocardial perfusion during
hyperaemia: a pilot study. Cardiovasc Diabetol 2012, 11:74.
20.van den Brom CE, Bosmans JW, Vlasblom R, Handoko ML, Huisman MC, Lubberink M, Molthoff
CF, Lammertsma AA, Ouwens DM, Diamant M, Boer C: Diabetic cardiomyopathy in Zucker
diabetic fatty rats: the forgotten right ventricle. Cardiovasc Diabetol 2010, 9:25.
21.van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009,
8:39.
22.Zaremba R, Merkus D, Hamdani N, Lamers JML, Paulus WJ, Remedios C, Duncker DJ, Stienen
GJM, Van der Velden J: Quantitative analysis of myofilament protein phosphorylation in small
cardiac biopsies. proteomics Clin Appl 2007, 1:1285-1290.
23.Llado I, Proenza AM, Serra F, Palou A, Pons A: Dietary-induced permanent changes in brown
and white adipose tissue composition in rats. Int J Obes 1991, 15:415-419.
24.Rolls BJ, Rowe EA, Turner RC: Persistent obesity in rats following a period of consumption of a
mixed, high energy diet. J Physiol 1980, 298:415-427.
25.Gentry-Smetana S, Redford D, Moore D, Larson DF: Direct effects of volatile anesthetics on
cardiac function. Perfusion 2008, 23:43-47.
26.Plante E, Lachance D, Roussel E, Drolet MC, Arsenault M, Couet J: Impact of anesthesia on
echocardiographic evaluation of systolic and diastolic function in rats. J Am Soc Echocardiogr
2006, 19:1520-1525.
27.Stein AB, Tiwari S, Thomas P, Hunt G, Levent C, Stoddard MF, Tang XL, Bolli R, Dawn B: Effects
of anesthesia on echocardiographic assessment of left ventricular structure and function in rats.
Basic Res Cardiol 2007, 102:28-41.
28.van den Brom CE, Bulte CSE, Loer SA, Bouwman RA, Boer C: Diabetes, perioperative ischaemia
and volatile anaesthetics: Consequences of derangements in myocardial substrate metabolism.
Cardiovasc Diabetol 2013, In press.
29.Lattermann R, Schricker T, Wachter U, Georgieff M, Goertz A: Understanding the mechanisms
by which isoflurane modifies the hyperglycemic response to surgery. Anesth Analg 2001,
93:121-127.
30.Zuurbier CJ, Keijzers PJ, Koeman A, Van Wezel HB, Hollmann MW: Anesthesia's effects on
plasma glucose and insulin and cardiac hexokinase at similar hemodynamics and without major
surgical stress in fed rats. Anesth Analg 2008, 106:135-42.
31.Saha JK, Xia J, Grondin JM, Engle SK, Jakubowski JA: Acute hyperglycemia induced by
ketamine/xylazine anesthesia in rats: mechanisms and implications for preclinical models. Exp
Biol Med (Maywood ) 2005, 230:777-784.
32.Yamada J, Sugimoto Y, Noma T: Involvement of adrenaline in diazepam-induced hyperglycemia
in mice. Life Sci 2000, 66:1213-1221.
33.Yao Y, Li L, Li L, Gao C, Shi C: Sevoflurane postconditioning protects chronically-infarcted rat
hearts against ischemia-reperfusion injury by activation of pro-survival kinases and inhibition of
mitochondrial permeability transition pore opening upon reperfusion. Biol Pharm Bull 2009,
32:1854-1861.
34.Lucchinetti E, Wang L, Ko KW, Troxler H, Hersberger M, Zhang L, Omar MA, Lopaschuk GD,
Clanachan AS, Zaugg M: Enhanced glucose uptake via GLUT4 fuels recovery from calcium
overload after ischaemia-reperfusion injury in sevoflurane- but not propofol-treated hearts. Br J
Anaesth 2011, 106:792-800.
5

106 Chapter 5
35.Hannon JD, Cody MJ: Effects of volatile anesthetics on sarcolemmal calcium transport and
sarcoplasmic reticulum calcium content in isolated myocytes. Anesthesiology 2002, 96:1457-
1464.
36.Davies LA, Gibson CN, Boyett MR, Hopkins PM, Harrison SM: Effects of isoflurane, sevoflurane,
and halothane on myofilament Ca2+ sensitivity and sarcoplasmic reticulum Ca2+ release in rat
ventricular myocytes. Anesthesiology 2000, 93:1034-1044.
37.An J, Rhodes SS, Jiang MT, Bosnjak ZJ, Tian M, Stowe DF: Anesthetic preconditioning enhances
Ca2+ handling and mechanical and metabolic function elicited by Na+-Ca2+ exchange inhibition
in isolated hearts. Anesthesiology 2006, 105:541-549.

CE van den Brom, C Boer, RPF van den Akker, SA Loer,
RA Bouwman
6Western diet modulates the susceptibility
of the heart to ischemic injury and
sevoflurane-induced cardioprotection in
rats

Effect of diet and sevoflurane on ischemic injury 111
Abstract
Introduction
Sevoflurane is known for its cardioprotective effects during myocardial ischemia and
reperfusion, which however seems blunted in the presence of type 2 diabetes
mellitus. In this study we investigated whether a reduction in caloric intake reverses
the impact of western diet on the cardioprotective potency of sevoflurane in rats
subjected to ischemic injury.
Methods
Male Wistar rats were exposed to a western diet (WD) or control diet (CD). A third
group of WD fed rats reversed after four weeks to CD for 4 consecutive weeks. After
8 weeks, rats underwent 40 minutes of coronary occlusion followed by 120 minutes
of reperfusion with or without 3x 5 min sevoflurane (2 vol%) preconditioning. An
extra group of CD-fed rats underwent myocardial infarction during hyperinsulinemic
euglycemic clamping.
Results
WD feeding resulted in a prediabetic phenotype with obesity and hyperinsulinemia.
Sevoflurane exerted cardioprotective effects in control rats, resulting in a reduction
of infarct size by 59% (p<0.001). Unexpectedly, WD feeding itself reduced infarct
size by 43% (p<0.05) compared to control rats, while sevoflurane even enlarged
infarct size in WD fed rats (31%, p<0.05). Reversion of WD to CD resulted in
normalization of obesity and hyperinsulinemia, but did not affect infarct size and the
protective effect of sevoflurane when compared to WD-fed rats. Interestingly,
sevoflurane prior to myocardial infarction tended to increase insulin levels in control
rats, while sevoflurane exposure in WD-fed rats undergoing myocardial infarction
resulted in a decrease of plasma insulin levels. Our data suggested that the
protective effects of diet feeding may be mediated by insulin. Indeed, exposure of
rats to a hyperinsulinemic intervention also reduced infarct size after myocardial
ischemia.
Conclusion
Unexpectedly, western diet itself had a protective effect against ischemic injury, and
lowering caloric intake did not alter this effect. Sevoflurane anesthesia exerted
cardioprotective effects in control rats, but this effect was blunted in prediabetic rats.
Our data further suggest that the protective effects of sevoflurane in control rats or
western diet are mediated by insulin.
6
112 Chapter 6
Introduction
Cardiometabolic alterations due to excessive dietary intake, insulin resistance and
type 2 diabetes mellitus (T2DM) increase the risk for perioperative myocardial
ischemia.1 In particular, patients with T2DM are more likely to develop coronary
artery disease and myocardial ischemia2 and have an increased cardiovascular
complication rate after major non-cardiac surgery.3
The volatile anesthetic sevoflurane exerts protective effects that enhance
perioperative preservation of the heart.4;5 We previously showed that sevoflurane
reduced the impact of ischemic myocardial injury.6;7 However, there is growing
evidence that these cardioprotective properties are blunted in case of obesity and/or
T2DM. Sevoflurane-induced postconditioning was blocked in hyperglycemic8 and
obese/insulin resistant Zucker rats9 after myocardial ischemia and reperfusion.
Moreover, obesity suppressed sevoflurane preconditioning-induced
cardioprotection.10
Preoperative lifestyle interventions such as lowering caloric intake to induce weight
loss and improve insulin sensitivity may be an attractive approach to improve
perioperative myocardial function in obese or diabetic subjects. We previously
showed that lowering caloric intake restored the cardiodepressive effects of
sevoflurane in western diet-induced prediabetic rats (van den Brom et al.,
unpublished results). This suggests that the myocardial response to sevoflurane
depends on the cardiometabolic state that may be altered by changes in dietary
intake. It remains unknown whether these beneficial effects of caloric restriction also
affect the cardioprotective effect of sevoflurane in the cardiometabolic altered heart.
In this study we investigated whether reversal of western diet-induced prediabetes
by caloric restriction restores the cardioprotective potency of sevoflurane in rats
subjected to ischemic injury.
Effect of diet and sevoflurane on ischemic injury 113
Material and methods
Animals and experimental set-up
All animal experiments were approved by the Institutional Animal Care and Use
Committee of the VU University, and were conducted following the European
Convention for the Protection of Vertebrate Animals used for Experimental and Other
Scientific Purposes, and the guide for the Care and Use of Laboratory Animals.
The first part of the study was performed in male Wistar rats (n=144, baseline
body weight: 263±1 g; Charles River). Rats were exposed to a western diet in
combination with sucrose water (20%) (WD, n=98) or control diet (CD, n=46) for a
period of 8 weeks. Four weeks after the start of diet exposure, 48 WD-fed rats
reversed to CD for 4 weeks (Figure 6.1A).
Rats were housed in a temperature-controlled room (20-23°C; 40-60% humidity)
under a 12/12h light/dark cycle starting at 6.00 am. Body weight was determined on
a weekly basis. After 8 weeks of diet exposure, rats underwent myocardial infarction.
The second part of the study included 14 male Wistar rats (263±3 g) that were
exposed to control diet. After 8 weeks, these rats underwent a myocardial infarction
during hyperinsulinemia. After sacrifice, arterial blood was collected for plasma
determinations and hearts were removed and stored at -20°C until further analysis.
Diets
Control diet (Teklad 2016, Harlan, Horst, the Netherlands) consisted of 20 %kcal
protein, 9 %kcal fat and 74 %kcal carbohydrates (1804 kcal/kg starch, 200 kcal/kg
sugars), whereas western diet (D12451, Research Diets, New Brunswick, NJ)
consisted of 20 %kcal protein, 45 %kcal fat and 35 %kcal carbohydrates (291
kcal/kg starch, 691 kcal/kg sugars) with 20% sucrose water (800 kcal/kg), totally
containing 3300 kcal/kg and 4857 kcal/kg for CD and WD with sucrose water,
respectively.
Surgery
After 8 weeks of diet exposure, rats were anesthetized with 125 mg/kg S-ketamine
(Ketanest®, Pfizer, the Netherlands) and 4 mg/kg diazepam (Centrafarm, the
Netherlands) intraperitoneally and were intubated and mechanically ventilated (UNO,
the Netherlands; positive end-expiratory pressure, 1-2 cm H2O; respiratory rate,
~65 breaths/min; tidal volume, ~10 ml/kg) with oxygen-enriched air (40% O2/60%
N2). Anesthesia was maintained by continuous infusion of 40 mg/kg/h S-ketamine
and 1 mg/kg/h diazepam intravenously via the tail vein or the right jugular vein.
The respiratory rate was adjusted to maintain pH and carbon dioxide within
physiological limits. Body temperature was maintained stabile (37.1±0.05°C) by
using a warm water underbody heating pad.
6
114 Chapter 6
The left carotid artery was cannulated for blood sampling for blood gas analyses
(ABL50, radiometer, Copenhagen, Denmark) and for measurements of arterial blood
pressure (Safedraw Transducer Blood Sampling Set, Argon Medical Devices, Texas,
USA). Arterial blood pressure, ECG and heart rate were continuously recorded using
PowerLab software (PowerLab 8/35, Chart 7.0; ADInstruments Pty, Ltd., Castle Hill,
Australia). Mean arterial blood pressure was calculated according the following
formula: 2/3*diastolic blood pressure + 1/3* systolic blood pressure.
Myocardial infarction
Left thoracotomy was performed between the fourth and fifth rib. A ligature
(Prolene® 6-0; Ethicon LLC, San Lorenzo, Puerto Rico) was placed around the left
anterior descending coronary artery (LAD) with a special ligation device that allowed
to pull the suture in one simple movement in order to reduce the chance of
preconditioning.11 Successful coronary occlusion was verified by ECG changes and
ischemia was maintained for 40 min and followed by 120 min of reperfusion (MI)
(Figure 6.1B). Rats in the control (CON) group received a sham surgery were the
LAD was not occluded. Sevoflurane (AbbVie, the Netherlands) intervention was
induced before ischemia and reperfusion by three periods of 5 minutes exposure to
2% (v/v) sevoflurane, interspersed with washout periods of 5 minutes (MI+SEVO).
In total, n=144 rats were included, from which n=122 rats survived the surgery
(84.7 %). Per diet group the survival rate was 87.0 %, 80.0 % and 85.4 % for CD-,
WD- and REV-fed rats, respectively.
Hyperinsulinemic euglycemic clamp
Rats in the second part of the study were subjected to the same ischemia and
reperfusion protocol during a hyperinsulinemic euglycemic clamp. In total, n=14 rats
were included, from which n=11 rats survived the surgery (78.6 %). Surgery was
performed similarly as described above; only anesthesia was infused intravenously
via the femoral vein due to blood glucose measurements via the tail vein. The
hyperinsulinemic euglycemic clamp was initiated by 3 minutes insulin priming at an
infusion rate of 120 mU/kg/min (Novorapid®, Novo Nordisk, Denmark), followed by
constant infusion of insulin at a rate of 12 mU/kg/min via the jugular vein as
described before.12 Blood glucose was measured every 5 minutes from tail bleeds
with a Precision Xceed Blood Glucose monitoring system (MediSense, UK).
Simultaneously, a 20% glucose solution was infused at a variable rate to maintain
euglycemia. After ± 90 minutes, glucose disposal rate (M-value, mg/kg/min) was
calculated as the average glucose infusion rate during 30 minutes. To prove
hyperinsulinemia, plasma insulin levels were determined during the steady state,
ischemia and reperfusion phase. The M/I index, which is a measure for insulin
sensitivity, was calculated by the amount of glucose metabolized per unit of plasma
insulin.
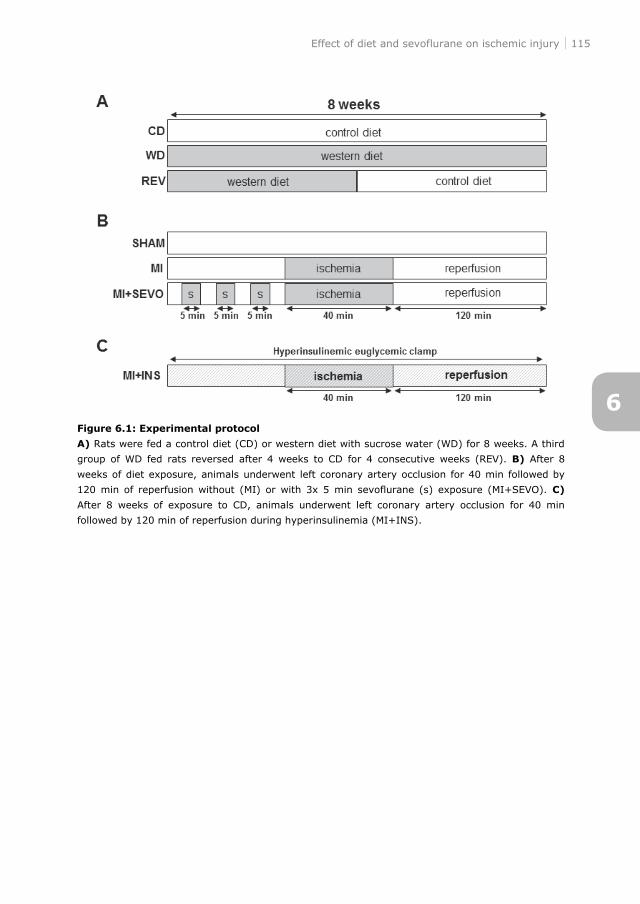
Effect of diet and sevoflurane on ischemic injury 115
Figure 6.1: Experimental protocol
A) Rats were fed a control diet (CD) or western diet with sucrose water (WD) for 8 weeks. A third
group of WD fed rats reversed after 4 weeks to CD for 4 consecutive weeks (REV). B) After 8
weeks of diet exposure, animals underwent left coronary artery occlusion for 40 min followed by
120 min of reperfusion without (MI) or with 3x 5 min sevoflurane (s) exposure (MI+SEVO). C)
After 8 weeks of exposure to CD, animals underwent left coronary artery occlusion for 40 min
followed by 120 min of reperfusion during hyperinsulinemia (MI+INS).
6
116 Chapter 6
Evans blue and TTC staining
After 120 min of reperfusion, the hearts were excised and the aorta was cannulated.
The LAD was re-occluded and 0.2 % Evans Blue (Sigma, St. louis, MO) was infused
to stain the non-ischemic myocardium and leaving the area at risk unstained. After
rinsing with 0.9% NaCl, hearts were stored at -20°C.
For determination of infarct size, frozen hearts were cut in slices of 1 mm,
incubated for 15 min in 2,3,5-triphenyl tetrazolium chloride (TTC; Sigma, St. Louis,
MO) solution at 37°C, followed by fixation in 4% formaldehyde (Klinipath, Duiven,
the Netherlands). Slices were scanned and the area at risk and infarct size were
determined in each slice using ImageJ (1.42q, National Institue of Health). The
infarct size is presented as the percentage of the area at risk.
Plasma measurements
Plasma glucose (Abcam, Cambridge, MA), insulin (Millipore, St. Charles, MO), free
fatty acid (WAKO NEFA-HR, Wako Pure Chemical Industries, Osaka, Japan),
triglyceride (TG; Sigma, St. Louis, MO) and HDL and LDL/VLDL cholesterol (Abcam,
Cambridge, MA) levels were measured from arterial blood as described previously.12-
15
Statistical analysis
Data were analyzed using Graphpad Prism 5.0 (La Jolla, USA) and presented as
mean±SD. Statistical analyses were performed using one-way ANOVA with
Bonferroni post-hoc analysis and two-way ANOVA with Bonferroni post-hoc analysis
(with repeated measurements) for additional interventions, where p<0.05 was
considered as statistically significant.
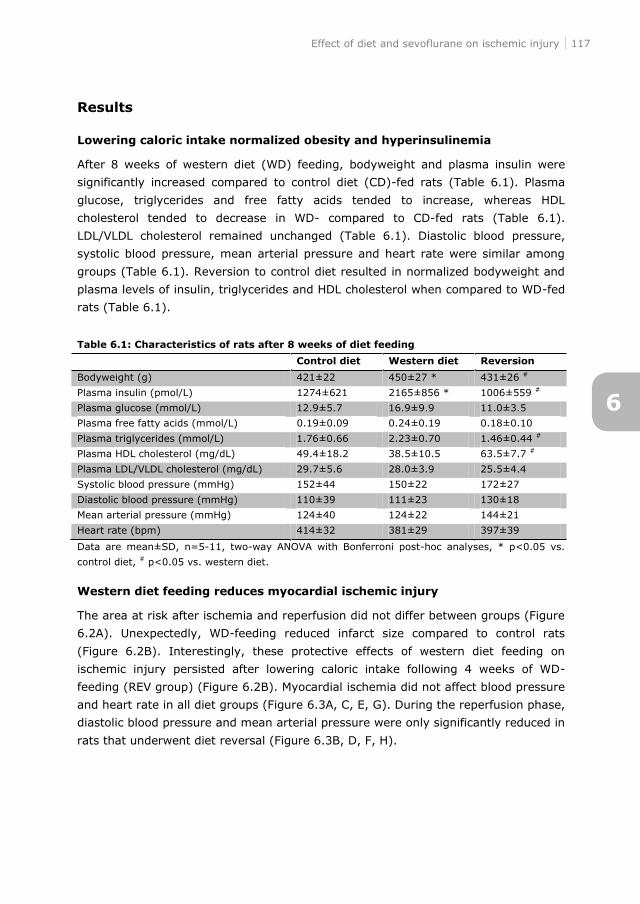
Effect of diet and sevoflurane on ischemic injury 117
Results
Lowering caloric intake normalized obesity and hyperinsulinemia
After 8 weeks of western diet (WD) feeding, bodyweight and plasma insulin were
significantly increased compared to control diet (CD)-fed rats (Table 6.1). Plasma
glucose, triglycerides and free fatty acids tended to increase, whereas HDL
cholesterol tended to decrease in WD- compared to CD-fed rats (Table 6.1).
LDL/VLDL cholesterol remained unchanged (Table 6.1). Diastolic blood pressure,
systolic blood pressure, mean arterial pressure and heart rate were similar among
groups (Table 6.1). Reversion to control diet resulted in normalized bodyweight and
plasma levels of insulin, triglycerides and HDL cholesterol when compared to WD-fed
rats (Table 6.1).
Table 6.1: Characteristics of rats after 8 weeks of diet feeding
Control diet Western diet Reversion
Bodyweight (g) 421±22 450±27 * 431±26 #
Plasma insulin (pmol/L) 1274±621 2165±856 * 1006±559 #
Plasma glucose (mmol/L) 12.9±5.7 16.9±9.9 11.0±3.5
Plasma free fatty acids (mmol/L) 0.19±0.09 0.24±0.19 0.18±0.10
Plasma triglycerides (mmol/L) 1.76±0.66 2.23±0.70 1.46±0.44 #
Plasma HDL cholesterol (mg/dL) 49.4±18.2 38.5±10.5 63.5±7.7 #
Plasma LDL/VLDL cholesterol (mg/dL) 29.7±5.6 28.0±3.9 25.5±4.4
Systolic blood pressure (mmHg) 152±44 150±22 172±27
Diastolic blood pressure (mmHg) 110±39 111±23 130±18
Mean arterial pressure (mmHg) 124±40 124±22 144±21
Heart rate (bpm) 414±32 381±29 397±39
Data are mean±SD, n=5-11, two-way ANOVA with Bonferroni post-hoc analyses, * p<0.05 vs.
control diet, # p<0.05 vs. western diet.
Western diet feeding reduces myocardial ischemic injury
The area at risk after ischemia and reperfusion did not differ between groups (Figure
6.2A). Unexpectedly, WD-feeding reduced infarct size compared to control rats
(Figure 6.2B). Interestingly, these protective effects of western diet feeding on
ischemic injury persisted after lowering caloric intake following 4 weeks of WD-
feeding (REV group) (Figure 6.2B). Myocardial ischemia did not affect blood pressure
and heart rate in all diet groups (Figure 6.3A, C, E, G). During the reperfusion phase,
diastolic blood pressure and mean arterial pressure were only significantly reduced in
rats that underwent diet reversal (Figure 6.3B, D, F, H).
6
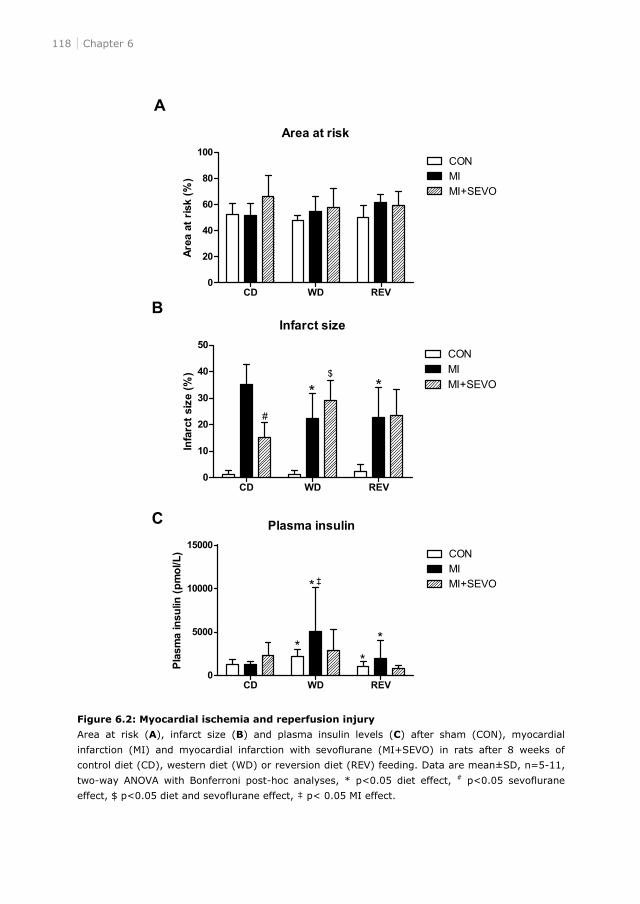
118 Chapter 6
Figure 6.2: Myocardial ischemia and reperfusion injury
Area at risk (A), infarct size (B) and plasma insulin levels (C) after sham (CON), myocardial
infarction (MI) and myocardial infarction with sevoflurane (MI+SEVO) in rats after 8 weeks of
control diet (CD), western diet (WD) or reversion diet (REV) feeding. Data are mean±SD, n=5-11,
two-way ANOVA with Bonferroni post-hoc analyses, * p<0.05 diet effect, # p<0.05 sevoflurane
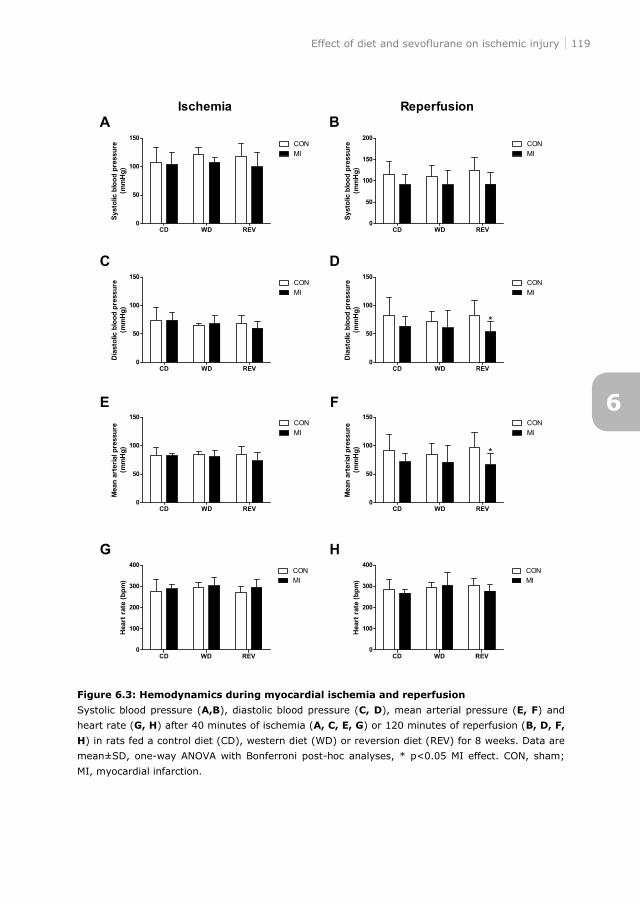
Effect of diet and sevoflurane on ischemic injury 119
Figure 6.3: Hemodynamics during myocardial ischemia and reperfusion
Systolic blood pressure (A,B), diastolic blood pressure (C, D), mean arterial pressure (E, F) and
heart rate (G, H) after 40 minutes of ischemia (A, C, E, G) or 120 minutes of reperfusion (B, D, F,
H) in rats fed a control diet (CD), western diet (WD) or reversion diet (REV) for 8 weeks. Data are
mean±SD, one-way ANOVA with Bonferroni post-hoc analyses, * p<0.05 MI effect. CON, sham;
MI, myocardial infarction.
6
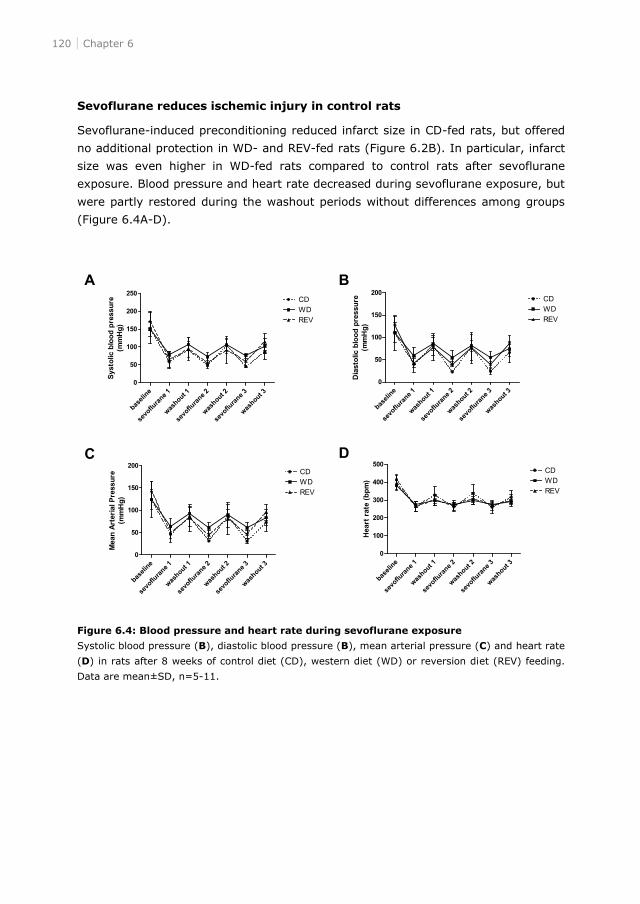
120 Chapter 6
Sevoflurane reduces ischemic injury in control rats
Sevoflurane-induced preconditioning reduced infarct size in CD-fed rats, but offered
no additional protection in WD- and REV-fed rats (Figure 6.2B). In particular, infarct
size was even higher in WD-fed rats compared to control rats after sevoflurane
exposure. Blood pressure and heart rate decreased during sevoflurane exposure, but
were partly restored during the washout periods without differences among groups
(Figure 6.4A-D).
Figure 6.4: Blood pressure and heart rate during sevoflurane exposure
Systolic blood pressure (B), diastolic blood pressure (B), mean arterial pressure (C) and heart rate
(D) in rats after 8 weeks of control diet (CD), western diet (WD) or reversion diet (REV) feeding.
Data are mean±SD, n=5-11.
Effect of diet and sevoflurane on ischemic injury 121
Plasma insulin levels after surgery
Western diet feeding increased plasma insulin levels when compared to control rats,
while this hyperinsulinemic effect was absent in rats subjected to diet reversal. While
myocardial infarction had no effect on insulin levels in control rats, WD-fed rats
showed a hyperinsulinemic response upon cardiac ischemia and reperfusion. This
effect remained present in the diet reversal group, although to a lesser extent.
Sevoflurane prior to myocardial infarction tended to increase insulin levels in control
rats, while sevoflurane exposure in WD-fed rats undergoing myocardial infarction
decreased plasma insulin levels. In rats exposed to diet reversal the rise in insulin
levels during myocardial infarction was abolished after sevoflurane exposure (Figure
6.2C).
Myocardial infarction, but not MI+SEVO, significantly increased HDL cholesterol in
CD-fed rats, which was absent in WD- and REV-fed rats. MI and MI+SEVO had no
effect on plasma glucose, free fatty acids, triglycerides and LDL/VLDL cholesterol
(data not shown).
Hyperinsulinemia protects against ischemic injury in healthy rats
From the findings as shown in figure 6.2C it was hypothesized that the protective
effects of western diet feeding against myocardial ischemia may be the result of
increases in plasma insulin levels. In order to study the direct effects of
hyperinsulinemia on the cardioprotective effects of western diet, control diet-fed rats
were subjected to a hyperinsulinemic euglycemic clamp. Steady-state blood glucose
levels during hyperinsulinemic euglycemic clamping were 5.43±0.05 mmol/L,
whereas the glucose disposal rate (M-value) was 9.83±1.34 mg/kg/min in healthy
CD-fed rats. Plasma insulin levels were 9027±679 pmol/L and the insulin sensitivity
(M/I-index) was 1.19±0.22 in CD-fed rats during the steady state of the clamp.
Hyperinsulinemia combined with euglycemia resulted in a similar area at risk when
compared to control rats, but itself protected the heart against myocardial ischemia
(Figure 6.5A and B).
6
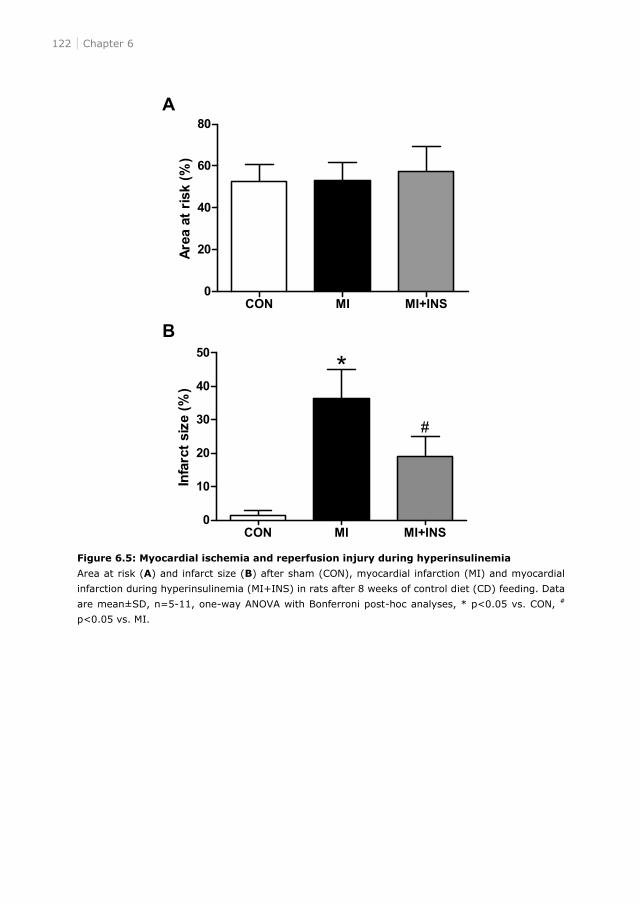
122 Chapter 6
Figure 6.5: Myocardial ischemia and reperfusion injury during hyperinsulinemia
Area at risk (A) and infarct size (B) after sham (CON), myocardial infarction (MI) and myocardial
infarction during hyperinsulinemia (MI+INS) in rats after 8 weeks of control diet (CD) feeding. Data
are mean±SD, n=5-11, one-way ANOVA with Bonferroni post-hoc analyses, * p<0.05 vs. CON, #
p<0.05 vs. MI.
Effect of diet and sevoflurane on ischemic injury 123
Discussion
The present study showed that short-term western diet feeding in rats resulted in a
prediabetic phenotype, and exerted an unexpected cardioprotective effect during
myocardial infarction, which was not abolished by lowering caloric intake.
Sevoflurane preconditioning protected the heart against myocardial ischemia in
healthy control rats. However, in diet-induced prediabetic rats, sevoflurane exposure
paradoxically increased infarct size. Sevoflurane prior to myocardial infarction tended
to increase insulin levels in control rats, while sevoflurane exposure in western diet-
fed rats undergoing myocardial infarction decreased plasma insulin levels. By
mimicking this hyperinsulinemic cardioprotective response using a hyperinsulinemic,
euglycemic clamp in control rats, we suspect a pivotal role for insulin underlying the
protective effects of sevoflurane or western diet against myocardial ischemia.
The present study demonstrated a protective effect of western diet feeding during
myocardial ischemia and reperfusion. We are not unique with respect to this
unexpected finding, as other groups also showed that high caloric diet feeding may
exert cardioprotective properties during ischemia and reperfusion.16-18 In contrast,
there are also reports available that show no effect10;19;20 or aggravation of ischemic
injury after diet feeding in rats.21-24 These conflicting findings may be due to the type
and severity of metabolic disease,25 the used ischemia and reperfusion protocol, the
duration of diet feeding and the composition of the diet.
Several mechanisms may explain diet-mediated cardioprotection, such as the
presence of a high percentage of carbohydrates.16-18 The present diet consisted
mainly of saturated fatty acids and a high percentage of sucrose. Jordan et al.
showed that 3 days or 4 weeks of fructose diet feeding both reduced infarct size,
while only the 4-week fructose intervention was associated with insulin resistance.
These findings suggest a protective effect of fructose.17 It is suggested that
carbohydrates, such as fructose or sucrose, may protect the heart against ischemia
and reperfusion injury via antioxidant mechanisms26,27 or via the response of the
heart to injury by increasing myocardial glucose metabolism to improve its energetic
efficiency.28,29 Glycolysis becomes an important source of energy due to its ATP-
generating ability in the absence of oxygen and is reported to be cardioprotective
during ischemia and reperfusion.30 Sucrose feeding may further stimulate myocardial
substrate metabolism. On the other hand, the high fat content of diets may also be
cardioprotective.31
Another explanatory mechanism is the presence of metabolic alterations, such as
hyperinsulinemia, during ischemic stress. Several studies showed a cardioprotective
effect of insulin in healthy rats during myocardial ischemia and reperfusion32-35 and
positive effects glucose, insulin and potassium (GIK) treatment in patients with
myocardial infarction.36;37 Moreover, infarct size was decreased in diet-induced obese
6
124 Chapter 6
compared to healthy rat hearts in absence of insulin, whereas the presence of insulin
in the coronary perfusate was cardioprotective in healthy and obese hearts,
suggesting the importance of insulin.22 In accordance with the literature, we showed
a cardioprotective effect of insulin during myocardial ischemia and reperfusion using
a hyperinsulinemic euglycemic clamp. Moreover, two independent observations in
our study provide further support for the protective role of insulin. First, sevoflurane
exposure of control rats tended to increase insulin levels, while this was associated
with myocardial protection against ischemic injury. Secondly, while western diet-
associated cardioprotection was paralleled by hyperinsulinemia, the absent
cardioprotective effect of sevoflurane exposure in western diet fed rats undergoing
myocardial infarction resulted in a decrease of plasma insulin levels. However,
further research is needed to discriminate the underlying cardioprotective
mechanism in our diet-induced prediabetic rat model.
Beside the unexpected cardioprotective effect of western diet, the present study
also demonstrated that sevoflurane preconditioning reduced infarct size in healthy
rats, but did had no additive cardioprotective effect in western diet-induced
prediabetic rats nor was affected by lowering caloric intake. Previously, it is shown
that hyperglycemia8 and obesity/insulin resistance9 abolished the cardioprotective
effect of sevoflurane. However, the generalizability of the prediabetic phenotype in
these rat models was limited.8;9 Moreover, Song et al. demonstrated in high fat diet-
induced obese rats that sevoflurane preconditioning-induced cardioprotection is
suppressed.10 Interestingly, our study shows that sevoflurane even increases infarct
size in prediabetic rats when compared to control rats, suggesting that western diet
feeding has negative effects on sevoflurane preconditioning.
In conclusion, western diet feeding resulted in an unexpected cardioprotective
effect during myocardial infarction, which was not affected by lowering caloric intake.
Sevoflurane preconditioning had no additive cardioprotective effect in prediabetic
rats nor was affected by lowering caloric intake. However, the combination of diet
and sevoflurane was less cardioprotective. Moreover, hyperinsulinemia was
cardioprotective in healthy rats, which might be an explanatory mechanism of the
cardioprotective effect of the diet. Future studies will discriminate between the
possible cardioprotective mechanisms of the diet and sevoflurane anesthesia.
Effect of diet and sevoflurane on ischemic injury 125
References
1. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, Freeman WK,
Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF, Smith SC, Jr., Jacobs AK, Adams CD,
Anderson JL, Antman EM, Buller CE, Creager MA, Ettinger SM, Faxon DP, Fuster V, Halperin JL,
Hiratzka LF, Hunt SA et al.: ACC/AHA 2007 guidelines on perioperative cardiovascular
evaluation and care for noncardiac surgery: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to
Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery):
developed in collaboration with the American Society of Echocardiography, American Society of
Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society
for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology,
and Society for Vascular Surgery. Circulation 2007, 116:e418-e499.
2. Preis SR, Pencina MJ, Hwang SJ, D'Agostino RB, Sr., Savage PJ, Levy D, Fox CS: Trends in
cardiovascular disease risk factors in individuals with and without diabetes mellitus in the
Framingham Heart Study. Circulation 2009, 120:212-220.
3. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ,
Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L: Derivation and prospective
validation of a simple index for prediction of cardiac risk of major noncardiac surgery.
Circulation 1999, 100:1043-1049.
4. Frassdorf J, De HS, Schlack W: Anaesthesia and myocardial ischaemia/reperfusion injury. Br J
Anaesth 2009, 103:89-98.
5. De Hert SG, Preckel B, Hollmann MW, Schlack WS: Drugs mediating myocardial protection. Eur
J Anaesthesiol 2009, 26:985-995.
6. Bouwman RA, Vreden MJ, Hamdani N, Wassenaar LE, Smeding L, Loer SA, Stienen GJ,
Lamberts RR: Effect of bupivacaine on sevoflurane-induced preconditioning in isolated rat
hearts. Eur J Pharmacol 2010, 647:132-138.
7. Lamberts RR, Onderwater G, Hamdani N, Vreden MJ, Steenhuisen J, Eringa EC, Loer SA,
Stienen GJ, Bouwman RA: Reactive oxygen species-induced stimulation of 5'AMP-activated
protein kinase mediates sevoflurane-induced cardioprotection. Circulation 2009, 120:S10-S15.
8. Huhn R, Heinen A, Weber NC, Hollmann MW, Schlack W, Preckel B: Hyperglycaemia blocks
sevoflurane-induced postconditioning in the rat heart in vivo: cardioprotection can be restored
by blocking the mitochondrial permeability transition pore. Br J Anaesth 2008, 100:465-471.
9. Huhn R, Heinen A, Hollmann MW, Schlack W, Preckel B, Weber NC: Cyclosporine A
administered during reperfusion fails to restore cardioprotection in prediabetic Zucker obese
rats in vivo. Nutr Metab Cardiovasc Dis 2010, 20:706-712.
10.Song T, Lv LY, Xu J, Tian ZY, Cui WY, Wang QS, Qu G, Shi XM: Diet-induced obesity suppresses
sevoflurane preconditioning against myocardial ischemia-reperfusion injury: role of AMP-
activated protein kinase pathway. Exp Biol Med (Maywood ) 2011, 236:1427-1436.
11.van Dijk A, Krijnen PA, Vermond RA, Pronk A, Spreeuwenberg M, Visser FC, Berney R, Paulus
WJ, Hack CE, van Milligen FJ, Niessen HW: Inhibition of type 2A secretory phospholipase A2
reduces death of cardiomyocytes in acute myocardial infarction. Apoptosis 2009, 14:753-763.
12.van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009,
8:39.
6
126 Chapter 6
13.Ouwens DM, Diamant M, Fodor M, Habets DD, Pelsers MM, El Hasnaoui M, Dang ZC, van den
Brom CE, Vlasblom R, Rietdijk A, Boer C, Coort SL, Glatz JF, Luiken JJ: Cardiac contractile
dysfunction in insulin-resistant rats fed a high-fat diet is associated with elevated CD36-
mediated fatty acid uptake and esterification. Diabetologia 2007, 50:1938-1948.
14.van den Brom CE, Bosmans JW, Vlasblom R, Handoko ML, Huisman MC, Lubberink M, Molthoff
CF, Lammertsma AA, Ouwens DM, Diamant M, Boer C: Diabetic cardiomyopathy in Zucker
diabetic fatty rats: the forgotten right ventricle. Cardiovasc Diabetol 2010, 9:25.
15.van den Brom CE, Bulte CS, Kloeze BM, Loer SA, Boer C, Bouwman RA: High fat diet-induced
glucose intolerance impairs myocardial function, but not myocardial perfusion during
hyperaemia: a pilot study. Cardiovasc Diabetol 2012, 11:74.
16.Ivanova M, Janega P, Matejikova J, Simoncikova P, Pancza D, Ravingerova T, Barancik M:
Activation of Akt kinase accompanies increased cardiac resistance to ischemia/reperfusion in
rats after short-term feeding with lard-based high-fat diet and increased sucrose intake. Nutr
Res 2011, 31:631-643.
17.Jordan JE, Simandle SA, Tulbert CD, Busija DW, Miller AW: Fructose-fed rats are protected
against ischemia/reperfusion injury. J Pharmacol Exp Ther 2003, 307:1007-1011.
18.Joyeux-Faure M, Rossini E, Ribuot C, Faure P: Fructose-fed rat hearts are protected against
ischemia-reperfusion injury. Exp Biol Med (Maywood ) 2006, 231:456-462.
19.Mozaffari MS, Schaffer SW: Myocardial ischemic-reperfusion injury in a rat model of metabolic
syndrome. Obesity (Silver Spring) 2008, 16:2253-2258.
20.Thim T, Bentzon JF, Kristiansen SB, Simonsen U, Andersen HL, Wassermann K, Falk E: Size of
myocardial infarction induced by ischaemia/reperfusion is unaltered in rats with metabolic
syndrome. Clin Sci (Lond) 2006, 110:665-671.
21.Axelsen LN, Lademann JB, Petersen JS, Holstein-Rathlou NH, Ploug T, Prats C, Pedersen HD,
Kjolbye AL: Cardiac and metabolic changes in long-term high fructose-fat fed rats with severe
obesity and extensive intramyocardial lipid accumulation. Am J Physiol Regul Integr Comp
Physiol 2010, 298:R1560-R1570.
22.du Toit EF, Smith W, Muller C, Strijdom H, Stouthammer B, Woodiwiss AJ, Norton GR, Lochner
A: Myocardial susceptibility to ischemic-reperfusion injury in a prediabetic model of dietary-
induced obesity. Am J Physiol Heart Circ Physiol 2008, 294:H2336-H2343.
23.Morel S, Berthonneche C, Tanguy S, Toufektsian MC, Foulon T, de LM, de LJ, Boucher F: Insulin
resistance modifies plasma fatty acid distribution and decreases cardiac tolerance to in vivo
ischaemia/reperfusion in rats. Clin Exp Pharmacol Physiol 2003, 30:446-451.
24.Gonsolin D, Couturier K, Garait B, Rondel S, Novel-Chate V, Peltier S, Faure P, Gachon P, Boirie
Y, Keriel C, Favier R, Pepe S, DeMaison L, Leverve X: High dietary sucrose triggers
hyperinsulinemia, increases myocardial beta-oxidation, reduces glycolytic flux and delays post-
ischemic contractile recovery. Mol Cell Biochem 2007, 295:217-228.
25.van den Brom CE, Bulte CSE, Loer SA, Bouwman RA, Boer C: Diabetes, perioperative ischaemia
and volatile anaesthetics: Consequences of derangements in myocardial substrate metabolism.
Cardiovasc Diabetol 2013, In press.
26.Yoshida T, Watanabe M, Engelman DT, Engelman RM, Schley JA, Maulik N, Ho YS, Oberley TD,
Das DK: Transgenic mice overexpressing glutathione peroxidase are resistant to myocardial
ischemia reperfusion injury. J Mol Cell Cardiol 1996, 28:1759-1767.
27.Dhalla NS, Elmoselhi AB, Hata T, Makino N: Status of myocardial antioxidants in ischemia-
reperfusion injury. Cardiovasc Res 2000, 47:446-456.
28.Stanley WC, Recchia FA, Lopaschuk GD: Myocardial substrate metabolism in the normal and
failing heart. Physiol Rev 2005, 85:1093-1129.
29.Lopaschuk GD, Ussher JR, Folmes CD, Jaswal JS, Stanley WC: Myocardial fatty acid metabolism
Effect of diet and sevoflurane on ischemic injury 127
in health and disease. Physiol Rev 2010, 90:207-258.
30.Vanoverschelde JL, Janier MF, Bakke JE, Marshall DR, Bergmann SR: Rate of glycolysis during
ischemia determines extent of ischemic injury and functional recovery after reperfusion. Am J
Physiol 1994, 267:H1785-H1794.
31.Knapp M: Cardioprotective role of sphingosine-1-phosphate. J Physiol Pharmacol 2011, 62:601-
607.
32.Gao F, Gao E, Yue TL, Ohlstein EH, Lopez BL, Christopher TA, Ma XL: Nitric oxide mediates the
antiapoptotic effect of insulin in myocardial ischemia-reperfusion: the roles of PI3-kinase, Akt,
and endothelial nitric oxide synthase phosphorylation. Circulation 2002, 105:1497-1502.
33.Jonassen AK, Sack MN, Mjos OD, Yellon DM: Myocardial protection by insulin at reperfusion
requires early administration and is mediated via Akt and p70s6 kinase cell-survival signaling.
Circ Res 2001, 89:1191-1198.
34.Jonassen AK, Aasum E, Riemersma RA, Mjos OD, Larsen TS: Glucose-insulin-potassium reduces
infarct size when administered during reperfusion. Cardiovasc Drugs Ther 2000, 14:615-623.
35.Doenst T, Richwine RT, Bray MS, Goodwin GW, Frazier OH, Taegtmeyer H: Insulin improves
functional and metabolic recovery of reperfused working rat heart. Ann Thorac Surg 1999,
67:1682-1688.
36.Di MS, Boldrini B, Conti U, Marcucci G, Morgantini C, Ferrannini E, Natali A: Effects of GIK
(glucose-insulin-potassium) on stress-induced myocardial ischaemia. Clin Sci (Lond) 2010,
119:37-44.
37.Diaz R, Paolasso EA, Piegas LS, Tajer CD, Moreno MG, Corvalan R, Isea JE, Romero G:
Metabolic modulation of acute myocardial infarction. The ECLA (Estudios Cardiologicos
Latinoamerica) Collaborative Group. Circulation 1998, 98:2227-2234.
6

7Conclusions & General discussion
Conclusions & General discussion 131
Patients undergoing surgery and anesthesia are at risk for perioperative cardiac
complications, especially in the presence of comorbidities like obesity and type 2
diabetes mellitus. The inhalational anesthetic sevoflurane has been shown to have
cardioprotective as well as cardiodepressive properties, which might be affected by
metabolic alterations in the heart. While the cardioprotective effects are reduction of
ischemia and reperfusion injury, the cardiodepressive effects are negative inotropic
and lusitropic effects. In the present thesis we investigated the impact of dietary
intake on perioperative myocardial perfusion, function and ischemia and reperfusion
injury, thereby focusing on the interaction of dietary intake and sevoflurane
anesthesia. We specifically hypothesized that anesthesia-induced changes in
perioperative myocardial function are influenced by preoperative dietary alterations.
Critique of methods
We tested our hypotheses in instrumented, anesthetized rats. These rats received a
standardized diet with a high concentration of saturated fatty acids and different
percentages of simple carbohydrates to induce an obese/type 2 diabetic phenotype
as a surrogate model for the human setting. This standardized diet improved the
comparability of diet interventions within our studies. Overall, 4 weeks of high fat
diet (HFD) feeding resulted in glucose intolerance with decreased HDL cholesterol
(chapter 3), while 4 weeks of western diet feeding, a diet consisting of HFD with
additional sucrose, resulted in obesity, hyperglycemia, hyperinsulinemia and
hyperlipidemia, going from a glucose intolerant to a prediabetic rat model (chapter
5). Furthermore, these characteristics were extravagated when the duration of
feeding was doubled from 4 to 8 weeks (chapter 4, 5 and 6). From these data we
can conclude that western diet feeding simulates the human phenotype better than
high fat diet feeding in rats.
Diet-induced models of obesity and diabetes are more human-like than other
models, because obesity is based on excessive caloric intake.1-3 Models such as the
genetic Zucker or Zucker Diabetic Fatty rat are not representative for the human
pathogenesis of obesity and type 2 diabetes mellitus due to a deficient leptin system,
which is uncommon in humans.4 Besides, it is important to realize that untreated
type 2 diabetic patients are rare, and that most patients receive medication leading
to mild or absence of hyperglycemia. The translational character of diet feeding in
rats to humans is still under discussion. There is a large variation in content of the
diet, time of feeding and strain used. Diets can vary in the source and percentages of
fat and carbohydrates. However, in the present thesis western diet feeding
represents a prediabetic phenotype in rats and closely mimics the human diet.
Our studies were performed in instrumented rats. Rats were anesthetized,
endotracheally intubated and mechanically ventilated. During the experiments, ECG
was recorded and arterial blood pressure was measured invasively. Moreover,
7
132 Chapter 7
interventional techniques such as an oral glucose tolerance test to determine glucose
tolerance, hyperinsulinemic euglycemic clamping to induce hyperinsulinemia,
coronary occlusion to induce ischemia and reperfusion injury, and (contrast)
echocardiography to determine myocardial perfusion and diastolic and systolic
function have been performed. These techniques allowed standardized study
conditions such as preservation of hypoglycemia during hyperinsulinemia.
All our results were obtained under strictly standardized conditions with respect to
timing and composition of diet feeding. Nevertheless, as with all animal experiments
extrapolation to the human setting has to be done with caution.
Major findings
Sevoflurane induces cardiodepression without altering myocardial perfusion
Under physiological conditions, myocardial blood flow and systolic function are in
balance.5 The supply of oxygen to the heart depends on the oxygen content in the
blood and coronary blood flow. While oxygen content remains mostly constant,
regulation of coronary blood flow is responsible for matching oxygen supply with
metabolic demands. Major determinants of myocardial blood flow are perfusion
pressure and coronary vascular resistance.
Under pathophysiological conditions, such as obesity and type 2 diabetes mellitus,
the balance between energy supply and demand could be altered. The present thesis
focused on the evaluation of dietary alterations on myocardial systolic function and
blood flow. In high fat diet-induced glucose intolerant rats, myocardial perfusion and
systolic function are not affected (chapter 3), whereas in western diet-induced
prediabetic rats, myocardial perfusion and function are both declined when compared
to control animals (chapter 4). This clearly suggests that the stage of diabetes plays
a role in the development of cardiovascular alterations and that a reduction in
myocardial contractility coincides with a reduction in coronary blood flow. In the
context of these findings the question remains whether these myocardial alterations
in prediabetic rats are additionally associated with changes in myocardial oxygen
demand and supply. It is known that substrate metabolism of diabetic hearts shifts
toward fatty acid utilization, which is paralleled by a decrease in glucose
metabolism.6 However, the consequence of increased use of fatty acids is a higher
demand of ATP which requires more oxygen. In addition to possible alterations in
oxygen supply and demand in the heart of prediabetic rats there are other
pathophysiological mechanisms that may underlie the reduction in myocardial
perfusion and function in our animal model. At first, cardiometabolic alterations may
affect myocardial calcium handling.7-10 The consequent reduction in contractility of
the heart may also lead to alterations in myocardial blood flow. Secondly, myocardial
relaxation is impaired in prediabetic rats, which might result in impairment of
coronary perfusion. As shown in patients undergoing biventricular pacing, coronary
Conclusions & General discussion 133
perfusion is dependent on a suction like effect during diastole, the so-called
backward-traveling decompression effect.11
The present thesis showed that sevoflurane did not affect myocardial perfusion,
while systolic function was decreased in healthy and prediabetic animals (chapter 4).
This suggests that sevoflurane uncouples myocardial perfusion and function
irrespective of the metabolic state of the heart. The uncoupling of perfusion and
function is also observed after prolonged ischemia, which has been describes as a
perfusion-contraction mismatch.5 Moreover, sevoflurane exerts vasodilating
properties, and is known to reduce coronary vascular resistance and perfusion
pressure in addition to myocardial depression.12-14 In addition, the vasodilating
properties of sevoflurane are influenced by vasoactive mediators, such as nitric
oxide.15 Sevoflurane activates nitric oxide; however, altered nitric oxide availability
can significantly impair myocardial perfusion-contraction matching.16 Thus,
sevoflurane seems to uncouple myocardial perfusion and contraction, however, up to
now the mechanisms are unclear.
The cardiodepressive effects of sevoflurane are modulated by dietary composition
Sevoflurane exerts cardiodepressive properties in healthy subjects, therefore its
perioperative use may cause hemodynamic alterations. It has been suggested that
the interaction of sevoflurane with the heart is additionally altered by
cardiometabolic diseases. With the growing epidemic of obesity and type 2 diabetes
mellitus it is important to understand the influence of this condition on the
interaction of sevoflurane with myocardial function. We found that high fat diet-
induced glucose intolerance did not affect myocardial function during baseline
conditions, whereas myocardial function was impaired during conditions of
hyperemia (chapter 3). When prediabetes was induced in rats exposed to a diet high
in saturated fatty acids and simple carbohydrates, a so-called western diet, we
observed impairment of myocardial systolic and diastolic function (Chapter 4 and 5).
Moreover, we found that sevoflurane is a stronger cardiodepressant in prediabetic
rats than in control rats (chapter 4 and 5), which could be restored by lowering
caloric intake (chapter 5). Suggested mechanisms are myocardial substrate
metabolism and calcium handling. Proteins related to myocardial substrate
metabolism, such as the protein kinase Akt17 and glucose transporter 418 are
increased by sevoflurane after ischemia and reperfusion, resulting in increased
glucose and decreased fatty acid oxidation.18 Moreover, sevoflurane reduces
myocardial calcium availability7 and affects sarcoplasmic reticulum calcium
content.7;19 These results suggest that normalization of the cardiometabolic profile
by dietary changes are of direct influence on the myocardial response to sevoflurane
in rats.
7
134 Chapter 7
The cardioprotective effects of sevoflurane during myocardial ischemia are altered by
dietary intake
Western diet, in combination with a sedentary lifestyle, is an important cause for
overweight, obesity and type 2 diabetes mellitus.1 Interestingly, while the overall
negative consequences of western diet feeding for the development of
cardiometabolic diseases are well acknowledged, there is increasing evidence that
diets containing a high percentage of saturated fatty acids and simple carbohydrates
may also be protective during stressful conditions, like surgery and anesthesia.20
In the present thesis we observed that western diet feeding itself exerted
cardioprotective effects in the ischemic heart (Chapter 6). In animals, feeding a diet
high in saturated fatty acids after myocardial ischemia showed preserved myocardial
function even in the presence of insulin resistance, suggesting a possible protective
effect of high fat diet feeding.21;22 Interestingly, it has been suggested that
overweight and obese patients exert a more appropriate inflammatory and immune
response to stress, and have a better outcome that their lean or morbid obese
counterparts.20 However, it should be kept in mind that, despite macronutrient
excess, obese patients remain at risk for perioperative nutritional deficits, such as
iron deficiency, and the development of cardiovascular diseases.20
Moreover, we showed that sevoflurane exerted cardioprotective effects during
myocardial ischemia and reperfusion in healthy rats. In agreement with our
expectations, western diet feeding blunted the protective effects of sevoflurane
during ischemia and reperfusion (Chapter 6). Western diet-induced cardioprotection
was associated with a rise in plasma insulin levels, suggesting that insulin levels may
be involved in the protective response of this diet (chapter 6). Besides a more
appropriate inflammatory and immune response to stress, a possible mechanism
might be hyperinsulinemia. Hyperinsulinemia is cardioprotective during ischemic
stress.23-28 Moreover, high fat diet feeding induces hyperinsulinemia as a
compensatory mechanism. This hyperinsulinemia in the early phase of diabetes may
therefore be a protective mechanisms during conditions of stress. Our experiments
showed that hyperinsulinemia induced by a hyperinsulinemic euglycemic clamp
mimicked the cardioprotective response as observed after western diet feeding
(Chapter 6). These exciting and potentially also clinically relevant findings warrant
future studies in humans.
Normalizing the caloric intake reverses the cardiodepressive effects, but not the
protective characteristics of sevoflurane
Perioperative cardiac complications are an economical, medical and social burden
that warrants optimization of perioperative health and cardiovascular care to
improve patient outcome and reduce health care costs. Preoperative treatment of
obesity and type 2 diabetes mellitus may reduce perioperative cardiac complications.
Current therapies directed at reducing these risk factors focus on weight loss. Weight
Conclusions & General discussion 135
loss is induced by a negative energy balance, such as dietary interventions, physical
activity, pharmacotherapy and surgery.29 Lifestyle interventions, such as changing
dietary intake and increasing physical activity to improve insulin sensitivity and
glucose control in obese and type 2 diabetic patients is an important part of these
treatments.30;31 The evidence for their benefits is nowadays growing and might
reduce perioperative complications and improve short and long-term outcome.
Hyperglycemia, which may be triggered by the stress condition of anesthesia and
surgery, is a strong predictor for morbidity and mortality after non-cardiac
procedures, while high perioperative glucose variability enhances this risk even
further.32-34 Lowering of the incidence of perioperative hyperglycemia in obese and
type 2 diabetic patients may therefore contribute to improved patient outcome and
reduced health care costs after surgery.35 Although the benefits of lifestyle
interventions to improve the incidence of intraoperative hyperglycemia are
increasingly acknowledged, it may be expected that these interventions also
modulate anesthesia-related physiological alterations.
The present thesis showed that lowering caloric intake improved myocardial
systolic and diastolic function (chapter 5 and 6) and that the cardioprotective effect
of western diet feeding during ischemia and reperfusion is sustained (chapter 6).
Further, sevoflurane induced cardiodepression was normalized (chapter 5), whereas
sevoflurane had no additional cardioprotective effect on ischemia and reperfusion
injury (chapter 6). Although studies focusing on preoperative dietary changes in
humans are limited,36 the overall idea is that weight loss reduces risk factors such as
diabetes and cardiovascular disease and extends lifespan and reduces mortality.
Besides the possibility of the sustained cardioprotective effect of western diet
feeding, it is also known that caloric restriction protects against ischemia and
reperfusion injury.36 Mitchell et al. reviewed the feasibility and benefits of caloric
restriction and concluded that caloric restriction has a wide range of benefits against
surgical stress in the experimental setting, which might also account in the human
setting.36 One of the suggested underlying mechanisms is reduced insulin signaling.
Improvement of insulin signaling by caloric restriction results in improved insulin
sensitivity. This might also be an underlying mechanism in improved cardiometabolic
state of western diet-induced prediabetic rats. Overall, dietary modulation by
lowering caloric intake may have a wide range of benefits including improved insulin
sensitivity, altered cardiometabolic state and reduced injury during stress.
7

136 Chapter 7
Future directions
Laboratory investigations already studied the cardioprotective properties of volatile
anesthesia for many years.37 However, the clinical applicability in modulating the risk
of perioperative cardiovascular complications by volatile anesthetics is still an
ongoing debate.38 Several experimental studies showed the protective effects of
volatile anesthetics in human heart tissue. However, recent clinical studies suggest
that propofol and volatile anesthetics are associated with a comparable incidence of
cardiac events. Therefore further research based on large clinical trials is necessary
to conclude on the possible beneficial effects of volatile anesthesia on the heart and
outcome. Moreover, clinical studies need to be performed to investigate the effects
of volatile anesthetics during myocardial infarction in obese and/or type 2 diabetic
patients.
Secondly, drugs might modulate the sensitivity of the heart for ischemic injury,
such as drugs for improvement of insulin sensitivity by glucagon-like peptide 1 (GLP-
1) or metformin. GLP1 is a gut incretin hormone that is released in response to
nutrient intake, stimulates insulin secretion and exerts insulinotropic and
insulinomimetic properties. Metformin is a biguanide with antihyperglycemic
properties and exerts its actions by enhancing insulin sensitivity. Improvement of the
diabetic phenotype might improve the cardioprotective effects of volatile anesthesia
during ischemia and reperfusion.
Thirdly, we found the protective effects of western diet feeding on ischemia and
reperfusion injury. One of the suggested mechanisms is the presence of metabolic
alterations, such as hyperinsulinemia, during ischemic stress. Several studies
showed a cardioprotective effect of insulin in healthy animals and patients with
myocardial infarction. However, the question remains if insulin administration has
protective effects in the diabetic heart, due to the presence of insulin resistance.
Future studies using insulin blockers need to be performed to prove the beneficial
effects of hyperinsulinemia during ischemia and reperfusion in the prediabetic heart.
Conclusions & General discussion 137
Conclusions
Patients with obesity and/or diabetes are at increased risk for perioperative
cardiovascular complications. Moreover, the choice of anesthetic may modulate the
risk of these perioperative cardiovascular complications. In the present thesis we
focused on the modulation of dietary intake on sevoflurane-induced alterations in
myocardial perfusion and function in rats. Moreover, we investigated whether the
cardioprotective effect of sevoflurane is altered by diet composition, and whether
changing the dietary balance by lowering fat and sucrose intake could be useful as
an intervention to influence the effects of sevoflurane on the heart.
Sevoflurane induces cardiodepression without altering myocardial perfusion
In healthy control rats, sevoflurane resulted in reduced systolic function without
altering myocardial blood flow, leading to uncoupling of cardiac systolic function and
perfusion (Chapter 4).
The cardioprotective effects of sevoflurane are modulated by dietary composition
Rats exposed to a diet high in saturated fatty acids (HFD) developed glucose
intolerance, however this phenotype was not associated with alterations in
myocardial perfusion and function (Chapter 3). Though, after induction of hyperemia,
we observed a reduction in myocardial systolic function in rats fed a high fat diet
(HFD) without alterations in myocardial perfusion when compared to control animals
(Chapter 3). When rats were exposed to a diet high in saturated fatty acids and
simple carbohydrates, a so-called western diet (WD), we observed glucose
intolerance and impairment of myocardial perfusion and function at baseline when
compared to control animals (Chapter 4 and 5). In the presence of sevoflurane, the
reduction in myocardial systolic function in rats fed a western diet (WD) was even
more pronounced, while sevoflurane did not alter myocardial perfusion (Chapter 4
and 5).
The cardioprotective effects of sevoflurane during myocardial ischemia are altered by
dietary intake
Sevoflurane exerted cardioprotective effects during myocardial infarction and
reperfusion in healthy rats. In agreement with our expectations, western diet feeding
blunted the protective effects of sevoflurane during ischemia and reperfusion
(Chapter 6). More interestingly, western diet feeding itself exerted cardioprotective
effects in the ischemic heart (Chapter 6). Western diet-induced cardioprotection was
associated with a rise in plasma insulin levels, suggesting that insulin levels may be
involved in the protective response of this diet. Separate experiments showed that
hyperinsulinemia induced by a hyperinsulinemic euglycemic clamp mimicked the
cardioprotective response as observed after western diet feeding (Chapter 6).
7

138 Chapter 7
Normalizing the caloric intake reverses the cardiodepressive effects, but not the
protective characteristics of sevoflurane
Rats subjected to diet reversal, which comprised a period of normal healthy diet
following western diet feeding, showed normalization of their prediabetic phenotype.
(Chapter 5) This was associated with improvement of cardiac systolic as well as
diastolic function (Chapter 5) and a reduction in the cardiodepressive effects of
sevoflurane (Chapter 5). While western diet had a protective effect against ischemia
and reperfusion injury, lowering caloric intake did not alter the cardioprotective
effect of western diet feeding during ischemia and reperfusion (Chapter 6).
Moreover, the absence of sevoflurane-induced cardioprotection during myocardial
infarction in western diet fed rats could not be restored by diet reversal (Chapter 6).
Conclusions & General discussion 139
References
1. Panchal SK, Brown L: Rodent models for metabolic syndrome research. J Biomed Biotechnol
2011, 2011:351982.
2. Kanasaki K, Koya D: Biology of obesity: lessons from animal models of obesity. J Biomed
Biotechnol 2011, 2011:197636.
3. Nilsson C, Raun K, Yan FF, Larsen MO, Tang-Christensen M: Laboratory animals as surrogate
models of human obesity. Acta Pharmacol Sin 2012, 33:173-181.
4. Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham CH, Prentice AM, Hughes IA,
McCamish MA, O'Rahilly S: Effects of recombinant leptin therapy in a child with congenital leptin
deficiency. N Engl J Med 1999, 341:879-884.
5. Heusch G, Schulz R: The relation of contractile function to myocardial perfusion. Perfusion-
contraction match and mismatch. Herz 1999, 24:509-514.
6. van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF,
Lammertsma AA, Van der Velden J, Boer C, Ouwens DM, Diamant M: Altered myocardial
substrate metabolism is associated with myocardial dysfunction in early diabetic
cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009,
8:39.
7. Hannon JD, Cody MJ: Effects of volatile anesthetics on sarcolemmal calcium transport and
sarcoplasmic reticulum calcium content in isolated myocytes. Anesthesiology 2002, 96:1457-
1464.
8. Fassl J, Halaszovich CR, Huneke R, Jungling E, Rossaint R, Luckhoff A: Effects of inhalational
anesthetics on L-type Ca2+ currents in human atrial cardiomyocytes during beta-adrenergic
stimulation. Anesthesiology 2003, 99:90-96.
9. Hanley PJ, ter Keurs HE, Cannell MB: Excitation-contraction coupling in the heart and the
negative inotropic action of volatile anesthetics. Anesthesiology 2004, 101:999-1014.
10.Bouwman RA, Salic K, Padding FG, Eringa EC, van Beek-Harmsen BJ, Matsuda T, Baba A,
Musters RJ, Paulus WJ, de Lange JJ, Boer C: Cardioprotection via activation of protein kinase C-
delta depends on modulation of the reverse mode of the Na+/Ca2+ exchanger. Circulation
2006, 114:I226-I232.
11.Kyriacou A, Whinnett ZI, Sen S, Pabari PA, Wright I, Cornelussen R, Lefroy D, Davies DW,
Peters NS, Kanagaratnam P, Mayet J, Hughes AD, Francis DP, Davies JE: Improvement in
coronary blood flow velocity with acute biventricular pacing is predominantly due to an increase
in a diastolic backward-travelling decompression (suction) wave. Circulation 2012, 126:1334-
1344.
12.Malan TP, Jr., DiNardo JA, Isner RJ, Frink EJ, Jr., Goldberg M, Fenster PE, Brown EA, Depa R,
Hammond LC, Mata H: Cardiovascular effects of sevoflurane compared with those of isoflurane
in volunteers. Anesthesiology 1995, 83:918-928.
13.Park KW: Cardiovascular effects of inhalational anesthetics. Int Anesthesiol Clin 2002, 40:1-14.
14.Larach DR, Schuler HG: Direct vasodilation by sevoflurane, isoflurane, and halothane alters
coronary flow reserve in the isolated rat heart. Anesthesiology 1991, 75:268-278.
15.Nakamura K, Terasako K, Toda H, Miyawaki I, Kakuyama M, Nishiwada M, Hatano Y, Mori K:
Mechanisms of inhibition of endothelium-dependent relaxation by halothane, isoflurane, and
sevoflurane. Can J Anaesth 1994, 41:340-346.
16.Kingma JG, Jr., Simard D, Rouleau JR: Modulation of nitric oxide affects myocardial perfusion-
contraction matching in anaesthetized dogs with recurrent no-flow ischaemia. Exp Physiol 2011,
96:1293-1301.
7
140 Chapter 7
17.Yao Y, Li L, Li L, Gao C, Shi C: Sevoflurane postconditioning protects chronically-infarcted rat
hearts against ischemia-reperfusion injury by activation of pro-survival kinases and inhibition of
mitochondrial permeability transition pore opening upon reperfusion. Biol Pharm Bull 2009,
32:1854-1861.
18.Lucchinetti E, Wang L, Ko KW, Troxler H, Hersberger M, Zhang L, Omar MA, Lopaschuk GD,
Clanachan AS, Zaugg M: Enhanced glucose uptake via GLUT4 fuels recovery from calcium
overload after ischaemia-reperfusion injury in sevoflurane- but not propofol-treated hearts. Br J
Anaesth 2011, 106:792-800.
19.Davies LA, Gibson CN, Boyett MR, Hopkins PM, Harrison SM: Effects of isoflurane, sevoflurane,
and halothane on myofilament Ca2+ sensitivity and sarcoplasmic reticulum Ca2+ release in rat
ventricular myocytes. Anesthesiology 2000, 93:1034-1044.
20.Valentijn TM, Galal W, Tjeertes EK, Hoeks SE, Verhagen HJ, Stolker RJ: The obesity paradox in
the surgical population. Surgeon 2013, 11:169-176.
21.Rennison JH, McElfresh TA, Okere IC, Vazquez EJ, Patel HV, Foster AB, Patel KK, Chen Q, Hoit
BD, Tserng KY, Hassan MO, Hoppel CL, Chandler MP: High-fat diet postinfarction enhances
mitochondrial function and does not exacerbate left ventricular dysfunction. Am J Physiol Heart
Circ Physiol 2007, 292:H1498-H1506.
22.Rennison JH, McElfresh TA, Chen X, Anand VR, Hoit BD, Hoppel CL, Chandler MP: Prolonged
exposure to high dietary lipids is not associated with lipotoxicity in heart failure. J Mol Cell
Cardiol 2009, 46:883-890.
23.Gao F, Gao E, Yue TL, Ohlstein EH, Lopez BL, Christopher TA, Ma XL: Nitric oxide mediates the
antiapoptotic effect of insulin in myocardial ischemia-reperfusion: the roles of PI3-kinase, Akt,
and endothelial nitric oxide synthase phosphorylation. Circulation 2002, 105:1497-1502.
24.Jonassen AK, Sack MN, Mjos OD, Yellon DM: Myocardial protection by insulin at reperfusion
requires early administration and is mediated via Akt and p70s6 kinase cell-survival signaling.
Circ Res 2001, 89:1191-1198.
25.Jonassen AK, Aasum E, Riemersma RA, Mjos OD, Larsen TS: Glucose-insulin-potassium reduces
infarct size when administered during reperfusion. Cardiovasc Drugs Ther 2000, 14:615-623.
26.Doenst T, Richwine RT, Bray MS, Goodwin GW, Frazier OH, Taegtmeyer H: Insulin improves
functional and metabolic recovery of reperfused working rat heart. Ann Thorac Surg 1999,
67:1682-1688.
27.Di MS, Boldrini B, Conti U, Marcucci G, Morgantini C, Ferrannini E, Natali A: Effects of GIK
(glucose-insulin-potassium) on stress-induced myocardial ischaemia. Clin Sci (Lond) 2010,
119:37-44.
28.Diaz R, Paolasso EA, Piegas LS, Tajer CD, Moreno MG, Corvalan R, Isea JE, Romero G:
Metabolic modulation of acute myocardial infarction. The ECLA (Estudios Cardiologicos
Latinoamerica) Collaborative Group. Circulation 1998, 98:2227-2234.
29.Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, Eckel RH: Obesity and
cardiovascular disease: pathophysiology, evaluation, and effect of weight loss. Arterioscler
Thromb Vasc Biol 2006, 26:968-976.
30.Viljanen AP, Karmi A, Borra R, Parkka JP, Lepomaki V, Parkkola R, Lautamaki R, Jarvisalo M,
Taittonen M, Ronnemaa T, Iozzo P, Knuuti J, Nuutila P, Raitakari OT: Effect of caloric restriction
on myocardial fatty acid uptake, left ventricular mass, and cardiac work in obese adults. Am J
Cardiol 2009, 103:1721-1726.
31.Hammer S, Snel M, Lamb HJ, Jazet IM, van der Meer RW, Pijl H, Meinders EA, Romijn JA, de
Roos A, Smit JW: Prolonged caloric restriction in obese patients with type 2 diabetes mellitus
decreases myocardial triglyceride content and improves myocardial function. J Am Coll Cardiol
2008, 52:1006-1012.
Conclusions & General discussion 141
32.Noordzij PG, Boersma E, Schreiner F, Kertai MD, Feringa HH, Dunkelgrun M, Bax JJ, Klein J,
Poldermans D: Increased preoperative glucose levels are associated with perioperative mortality
in patients undergoing noncardiac, nonvascular surgery. Eur J Endocrinol 2007, 156:137-142.
33.Akhtar S, Barash PG, Inzucchi SE: Scientific principles and clinical implications of perioperative
glucose regulation and control. Anesth Analg 2010, 110:478-497.
34.Tung A: Anaesthetic considerations with the metabolic syndrome. Br J Anaesth 2010, 105 Suppl
1:i24-i33.
35.Lipshutz AK, Gropper MA: Perioperative glycemic control: an evidence-based review.
Anesthesiology 2009, 110:408-421.
36.Mitchell JR, Beckman JA, Nguyen LL, Ozaki CK: Reducing elective vascular surgery perioperative
risk with brief preoperative dietary restriction. Surgery 2013, 153:594-598.
37.Frassdorf J, De Hert S, Schlack W: Anaesthesia and myocardial ischaemia/reperfusion injury. Br
J Anaesth 2009, 103:89-98.
38.Pagel PS: Myocardial Protection by Volatile Anesthetics in Patients Undergoing Cardiac Surgery:
A Critical Review of the Laboratory and Clinical Evidence. J Cardiothorac Vasc Anesth 2013.
7

8Summary

Summary 145
In the present thesis we investigated the impact of preoperative dietary composition
on sevoflurane anesthesia-induced changes in myocardial perfusion and function.
Moreover, we studied the effects of high intake of saturated fatty acids in
combination with simple carbohydrates on the cardioprotective effects of sevoflurane
in case of myocardial ischemia. We hypothesized that preoperative dietary intake
influence sevoflurane-induced changes in perioperative myocardial function. To
investigate this we studied myocardial perfusion, function and ischemic injury in diet-
induced glucose intolerant or prediabetic rats.
Patients undergoing anesthesia and surgery are at risk of perioperative cardiac
complications, especially in the presence of comorbidities like obesity and type 2
diabetes mellitus. A general introduction is given in Chapter 1 on perioperative
complications, myocardial performance and ischemia during anesthesia and the
combination with dietary interventions and lifestyle changes.
A broader introduction on diabetes, perioperative ischemia and volatile anesthetics
is given in Chapter 2. Several mechanisms involved in anesthesia-induced
cardioprotection have been evaluated in the experimental setting. However, the
existing evidence suggests that the obese and type 2 diabetic heart is less adaptable
to cardioprotective interventions and that anesthesia-induced cardioprotection is just
substrate metabolism is one of the underlying protective mechanisms; therefore we
focused on the consequences of derangements in myocardial substrate metabolism.
This overview of recent literature reveals the importance of interventional options
focusing on recovery of the metabolic flexibility of the heart, especially by improving
insulin sensitivity.
Myocardial perfusion during diet exposure and sevoflurane anesthesia
This thesis focused on the effect of diet-induced glucose intolerance and prediabetes
on myocardial perfusion. Chapter 3 describes the effect of high fat diet-induced
glucose intolerance on myocardial perfusion and function during baseline and
hyperemic conditions. High fat diet-induced glucose intolerance did not affect
myocardial perfusion and function during baseline conditions. During hyperemia, we
found that diet-induced glucose intolerance is associated with impaired myocardial
function, but myocardial perfusion is maintained. These findings result in new
insights into the effect of glucose intolerance on myocardial function and perfusion
during hyperemia.
Sevoflurane is associated with myocardial depression and these effects seem more
abundant during obesity and type 2 diabetes mellitus. Chapter 4 focused on the
impact of a more severe western, or cafeteria, diet on myocardial perfusion and
function and the interaction with sevoflurane exposure. Western diet-induced
prediabetes impaired myocardial perfusion and function. Exposure to sevoflurane did
8
146 Chapter 8
not affect myocardial perfusion, but impaired systolic function in healthy and
prediabetic conditions. Our findings therefore suggest that sevoflurane leads to
uncoupling of myocardial perfusion and function, irrespective of the metabolic state.
Effect of changing the dietary balance
Furthermore, this thesis investigated the effect of altering the dietary balance on
myocardial function and ischemic injury by lowering the caloric intake. In Chapter 5
we investigated whether lowering the caloric intake can restore the effects of
sevoflurane on myocardial performance in prediabetes. Western diet-induced
prediabetes impaired myocardial systolic and diastolic function, whereas sevoflurane
even further impaired systolic function in prediabetes. Lowering caloric intake
normalized the prediabetic phenotype, improved myocardial function and restored
systolic function during sevoflurane exposure. Therefore, sevoflurane is a stronger
cardiodepressant in prediabetes than in healthy conditions, which could be restored
by lowering caloric intake. These results suggest that dietary changes-related
normalization of the cardiometabolic profile is of direct influence on the myocardial
response to sevoflurane.
Sevoflurane is known for its cardioprotective effects during myocardial ischemia
and reperfusion, which seems blunted in the presence of obesity or type 2 diabetes
mellitus. In Chapter 6 we investigated whether a reduction in caloric intake reverses
the deteriorating impact of western diet feeding on the cardioprotective potency of
sevoflurane during ischemia and reperfusion. In contrast to our hypothesis, western
diet itself protected the heart against ischemic injury, and this effect was maintained
even after lowering caloric intake. Exposure to sevoflurane exerted cardioprotective
effects in healthy conditions, but this effect was blunted in prediabetes. Plasma
insulin levels suggested that the protective effects of diet feeding may be induced by
insulin. Hyperinsulinemia was cardioprotective in healthy conditions, suggesting that
the protective effects of western diet feeding or sevoflurane are mediated by insulin.
The main conclusions of this thesis are 1) sevoflurane induces cardiodepression
without altering myocardial perfusion, 2) the cardiodepressive effects of sevoflurane
are modulated by dietary composition, 3) the cardioprotective effects of sevoflurane
during myocardial ischemia are altered by dietary intake, and 4) normalizing caloric
intake reverses the cardiodepressive effects, but not the protective characteristics of
sevoflurane. In Chapter 7, the conclusions are discussed and this chapter ends with
future directions.


9Samenvatting

Samenvatting 151
Dit proefschrift beschrijft de invloed van dieetsamenstelling op de effecten van het
dampvormige anestheticum sevofluraan op de doorbloeding en pompfunctie van het
hart, en de beschermende werking van sevofluraan op het hart tijdens
zuurstoftekort. Om dit te onderzoeken is de doorbloeding, functie en schade ten
gevolge van zuurstoftekort in het hart bestudeerd in ratten. Deze ratten hebben door
blootstelling aan een vetrijk dieet met of zonder toegevoegde suikers glucose
intolerantie of prediabetes ontwikkeld.
Het is een bekend gegeven dat patiënten die een operatie onder anesthesie
ondergaan een verhoogd risico hebben op het ontwikkelen van complicaties aan het
hart. Aandoeningen zoals ernstig overgewicht (obesitas) en type 2 diabetes mellitus
vergroten dit risico op complicaties. Hoofdstuk 1 geeft een algemene introductie
over deze complicaties, het functioneren van het hart en de schade ten gevolge van
zuurstoftekort tijdens anesthesie in combinatie met dieet-interventies en levensstijl
veranderingen.
Dampvormige anesthetica hebben een beschermend effect op het hart tijdens
zuurstoftekort. Recente literatuur toont aan dat deze beschermende effecten
verminderd zijn in het obese en/of type 2 diabetische hart. Het lijkt er daarbij op dat
deze beschermende effecten alleen worden waargenomen in het gezonde hart. Eén
van de verklaringen hiervoor is dat de beschermende effecten van dampvormige
anesthetica worden beïnvloed door het glucose en vetzuur metabolisme in het hart,
en hier wordt uitgebreid op ingegaan in Hoofdstuk 2. Daarnaast wordt ook het
belang van interventiemogelijkheden beschreven, waarbij de focus ligt op het herstel
van de metabole flexibiliteit van het hart door het verbeteren van de insuline
gevoeligheid. Dit kan bijdragen aan het verminderen van het perioperatieve risico op
de complicaties van zuurstoftekort.
Doorbloeding van het hart tijdens dieetblootstelling en sevofluraan
anesthesie
Dit proefschrift richt zich onder andere op het effect van glucose intolerantie en
prediabetes op de doorbloeding van het hart. Hoofdstuk 3 beschrijft het effect van
een hoog vet dieet op de doorbloeding van het hart in rust en tijdens maximale
vaatverwijding. Inname van een hoog vet dieet resulteerde in glucose intolerantie,
maar had geen effect op de doorbloeding en pompfunctie van het hart. Tijdens
maximale vaatverwijding tonen wij aan dat glucose intolerantie geassocieerd is met
een verstoorde hartfunctie, maar dat de doorbloeding van het hart behouden blijft.
Deze resultaten geven nieuwe inzichten in het effect van glucose intolerantie op de
doorbloeding en functie van het hart tijdens maximale vaatverwijding.
Sevofluraan wordt geassocieerd met een verslechterde functie van het hart en deze
effecten lijken versterkt aanwezig te zijn in obese en type 2 diabetische harten.
Hoofdstuk 4 focust op de invloed van een vet-
9
152 Chapter 9
(westers dieet) op de doorbloeding en functie van het hart in combinatie met
blootstelling aan sevofluraan. Inname van een westers dieet resulteerde in
prediabetes en verslechterde de doorbloeding en functie van het hart. Blootstelling
aan sevofluraan had geen effect op de doorbloeding, maar verslechterde wel de
functie in gezonde en prediabetische harten. Deze bevindingen suggereren dat
sevofluraan de doorbloeding en functie in het hart ontkoppelt, onafhankelijk van de
metabole staat van het hart.
Effect van veranderingen in dieetsamenstelling
Dit proefschrift beschrijft het effect van dieetsamenstelling op de functie en op de
schade ten gevolge van zuurstoftekort in het hart. De resultaten van Hoofdstuk 5
tonen aan dat een westers dieet resulteerde in een prediabetisch fenotype en
verslechtering van de hartfunctie. Daarnaast bleken de ongunstige effecten van
sevofluraan op de functie van het hart versterkt te worden door prediabetes. Het
verlagen van de calorie-inname verbeterde het prediabetische fenotype, de functie
van het hart en verminderde de ongunstige effecten van sevofluraan op het hart.
Hieruit concluderen we dat de negatieve effecten van sevofluraan op het hart
versterkt worden in prediabetische harten. Verlaging van de calorie inname kunnen
deze negatieve effecten herstellen. Deze resultaten suggereren dat veranderingen in
dieet samenstelling van invloed is op de respons van het hart op sevofluraan.
Sevofluraan staat bekend om de beschermende werking op het hart tijdens
zuurstoftekort. Obesitas en type 2 diabetes mellitus lijken deze beschermende
effecten te verstoren. Hoofdstuk 6 beschrijft of een verlaging van de calorie inname
de effecten van sevofluraan op de schade van het prediabetische hart ten gevolge
van zuurstoftekort beïnvloedt. Het hoog vet- en suikerrijke westers dieet
beschermde het hart tegen de schade ten gevolge van zuurstoftekort en dit
beschermende effect bleef behouden na verlaging van de calorie inname.
Blootstelling aan sevofluraan resulteerde in bescherming van het gezonde hart
tijdens zuurstoftekort, maar dit effect was verminderd in prediabetische harten.
Insuline levels in het plasma suggereerden dat de beschermende effecten van het
westers dieet en sevofluraan geïnduceerd worden door insuline. Hoge concentraties
van insuline werkten beschermend op het gezonde hart tijdens zuurstoftekort. Dit
suggereert dat insuline mogelijke een rol speelt bij de beschermende effecten van
het westers dieet en sevofluraan.
De belangrijkste conclusies in dit proefschrift zijn 1) het dampvormige anestheticum
sevofluraan verslechtert de functie, maar niet de doorbloeding van het hart; 2) de
samenstelling van het dieet beïnvloedt de effecten van sevofluraan op de
doorbloeding en functie van het hart; 3) een hoog vet- en suikerrijk dieet heeft een
ongunstige invloed op de beschermende effecten van sevofluraan tijdens
zuurstoftekort in het hart en 4) verlaging van de calorie inname herstelt de
Samenvatting 153
verminderde functie van het prediabetische hart, maar niet de beschermende
kenmerken van sevofluraan. In Hoofdstuk 7 worden deze conclusies bediscussieerd
en staat de toekomstige richting van dit onderzoek beschreven.
9

List of abbreviations

List of abbreviations 157
A
A microvascular blood volume
AMPK AMP-activated protein kinase
ATP adenosine triphosphate
AUC area under the curve
B
microvascular filling velocity
C
Ca2+ calcium
CABG coronary artery bypass grafting
CD control diet
CON control
CPT-1 carnitine palmitoyl transferase 1
cTnI cardiac troponin I
D
DCA dichloroacetate
DPP4 dipeptidyl peptidase IV
DSPC 1,2-distearoyl-sn-glycero-3-phosphocholine
E
echo echocardiography
eNOS endothelial nitric oxide synthase
ED end-diastole
ES end-systole
F
FABPpm plasma membrane fatty acid binding protein
FAC fractional area change
FAT/CD36 fatty acid translocase / CD36
FATP fatty acid transport protein
FS fractional shortening
G
GIK glucose-insulin-potassium
GLP1 glucagon-like peptide 1
GLUT glucose transporter
GSK3 glycogen synthase kinase
L
158 List of abbreviations
H
HDL high-density lipoprotein
HFD high fat diet
I
INS hyperinsulinemia
IVRT isovolumic relaxation time
L
LAD left anterior descending coronary artery
LDL low-density lipoprotein
LV left ventricle / left ventricular
M
MI mechanical index
MI myocardial infarction
mito K+ATP mitochondrial ATP-activated potassium channel
MyBP-C myosin binding protein-C
P
PDK4 pyruvate dehydrogenase kinase 4
PEG polyoxyethylene stearate
PLB phospholamban
PPAR peroxisome proliferator-activated receptor
R
REV reversion
RPP rate pressure product
S
SEVO sevoflurane
SERCA2a sarcoplasmic reticulum calcium ATPase 2a
T
T2DM type 2 diabetes mellitus
TCA tricarboxylic acid
TnT troponin T
TTC 2,3,5-triphenyl tetrazolium chloride
List of abbreviations 159
V
VLDL very-low-density lipoprotein
W
WD western diet
WT wall thickness
Y
Y0 signal intensity of first frame after microbubble destruction
L
Dankwoord

Dankwoord 163
Men zegt dat de laatste loodjes het zwaarst zijn. Maar waar komt dit spreekwoord
eigenlijk vandaan? Er zijn verschilende theorieë over de herkomst. De meest
plausible verklaring: het is ontleend aan het traditionele wegen waarbij de laatste
gewichtjes de l ) de doorslag geven om de weegschaal in balans te krijgen.
Bij mij heeft de weegschaal halverwege al flink geschommeld en alle gewichten eraf
halen en opnieuw plaatsen was op een gegeven moment de enige optie. Om door
deze fase heen te komen en mijn proefschrift af te ronden zijn er vele personen
belangrijk geweest, maar een aantal personen in het bijzonder en deze wil ik graag
bedanken.
Lieve Rob, meestal wordt het dankwoord geëindigd met de partner, maar ik wil heel
graag met jou beginnen, want zonder jouw onvoorwaardelijke steun was dit
proefschrift er nooit geweest. Jij bent mijn alles; mijn man, mijn beste vriend en een
fantastische vader! Op de momenten dat ik druk was regelde je naast je eigen
drukke werk alles; het huishouden, het eten, de zorg voor Thijs en daarnaast was je
er ook nog eens altijd voor mij. Eigenlijk onbeschrijf
Prof.dr. Loer, bedankt dat u mij de mogelijkheid heeft gegeven om bij u dit
proefschrift te maken tot wat het geworden is en daarnaast het onderzoek nog veel
verder uit te breiden. Ik kijk uit naar onze verdere samenwerking! Dr. Boer, lieve Chris. Jij hebt mij mijn verloren passie voor de wetenschap helpen
terug te vinden. Jij gaf mij de zelfverzekerheid en het enthousiasme om opnieuw aan
een proefschrift te beginnen. Zonder jouw passie voor onderzoek en altijd maar weer
motiverende woorden was dit proefschrift er nooit geweest. Zelfs van de kleinste
resultaten word je nog steeds enthousiast. Ik ben erg blij dat we ons onderzoek en
het delen van enthousiasme over nieuwe data blijven voortzetten!
Dr. Bouwman, beste Arthur. Dit project is ooit begonnen als een zijtakje van beide
promotie projecten en uiteindelijk gecombineerd en geëindigd in dit proefschrift. Wie
had dat ooit kunnen denken. Veel succes in Eindhoven!
Prof.dr. Westerhof, beste Nico. Heel erg bedankt voor uw ondersteuning bij mijn
.
Prof.dr. Tangelder, beste Geert Jan. Hartelijk dank voor uw gastvrijheid op de
afdeling fysiologie. Ik heb het er erg naar mijn zin gehad en me altijd thuis gevoeld.
Ik ben dan ook erg blij dat ik nog blijf. Geniet van uw pensioen en alle reizen die u
nog gaat maken!
D
164 Dankwoord
Graag wil ik mijn promotiecommissie, Prof.dr. Preckel, Prof.dr. van Royen, Prof.dr.
Glatz, Prof.dr. den Heijer, Prof.dr. Scheeren, Prof.dr. van der Velden en Prof.dr.
Serné bedanken voor het lezen van mijn proefschrift en het deelnemen aan mijn
verdediging.
Mijn paranimfen, Ester en Marianne. Lieve Ester, bijna gelijk zijn we bij de fysiologie
acht
vriendinnen. Ik vind het fijn d kheid naast me mag
hebben staan!
Lieve Marianne, lief schoonzusje, al 23 jaar ben je in de familie en je bent dan ook
echt mijn grote zus. Jij bent niet alleen mijn voorbeeld van hoe ik als moeder wil
zijn, maar je hebt ook de bijzondere eigenschap om oprecht blij voor me te zijn
zonder altijd exact te weten waarom. Ik ben er trots op dat je naast me wilt staan!
Ik ben van mening dat twee paranimfen te weinig zijn. Ondertussen zijn collega
vriendinnen geworden en hebben een belangrijke plek in mijn leven gekregen.
Carolien, drie jaar hebben we niet alleen een kamer gedeeld, maar ook de nodige
frustaties, irritaties, blijheden, borrels en nog veel meer. Succes met de laatste
loodjes, je bent er echt bijna en je hebt een prachtig proefschrift waar je trots op
mag zijn! Lonneke, jij was de nieuwe generatie, maar ondertussen ben je eerder
gepromoveerd dan ik ;-). Ik vond het geweldig dat ik jouw paranimf mocht zijn en
ben blij dat je nu een nieuw plekje hebt gevonden. Frances, ook bij jou mocht ik je
als paranimf ondersteunen en ik vond het erg bijzonder om dit moment met je te
mogen delen. Ik vind het super dat jij ook nog onderzoek blijft doen bij de fysiologie
en we weer roomies zijn. Sylvia, bedankt voor alle bakkies en onvoorwaardelijke
steun. Ik heb ongelooflijk veel respect voor jouw doorzettingsvermogen en
positivitieit!
In al die jaren heb ik toch heel wat roomies gehad. Louis, Melanie, Frances, Coen,
Carolien, Hein, Karolina, Floor, Bas, Noor, Chantal en Yoni. Bedankt voor de
gezelligheid, mentale steun, alle klaaguurtjes ;-
met bitterballen en natuurlijk de frikandellenlunch.
Na acht jaar werken
Hoe bijzonder is dat! -Lynn, Christine, Ester, Frances, Gerrina, Ingrid,
Lonneke, Nicky, Sylvia, en surrogaat oma Lynda, bedankt voor alle opa
dat we ons uitspreiden over de hele wereld (NY, Zanzibar, AMC), hoop ik dat we
onze opa jaarlijkse oma-de-luxe weekenden blijven voortzetten!
Dankwoord 165
Verder heb ik een mooi onderzoekteam om me heen. Rob, bedankt voor het uit
handen nemen van heel veel dierexperimenteel werk. Chantal, Nick, Rob en
Carolien, samen gaan we het ELVIS lab op de kaart zetten.
en studenten (te veel om op te noemen) op de afdelingen
anesthesiologie, fysiologie, secretariaat, werkplaats, electronica, interne, en UPC:
bedankt voor de ondersteuning op alle vlakken en gezelligheid!
(zijn) super!
Verder wil ik ook graag mijn familie, vrienden en iedereen die mij dierbaar is
bedanken. Ieder heeft op zijn eigen wijze interesse getoond of een bijdrage geleverd
(in de vorm van een wijntje of welke andere vorm van ondersteuning dan ook ):
Michael, Anja, Xander & Justin, Gaby, Marianne Ilse & Maud, Wim, Ton & Lia, Mark,
Lianne, Tim, Chris & Julia, Ronald Vlasblom, Klaas Kramer, Robert-Jan, Silvia,
Xander & Timon, Andu, Maurice & Benji, Kees, Mariska, Lianne & Feline, Jennie, Ivo
& Feline, Diederik, Rik, Connie & Edwin, Tilly & Chelso en nog vele anderen .
Lieve mama en papa. Eindelijk ga ik dan ik niet van jullie
kon verwachten helemaal te begrijpen wat promoveren precies inhoudt, hebben jullie
altijd 200% achter mij gestaan! Papa, jouw doorzettingsvermogen is onbeschrijfbaar
en voor mij een belangrijk voorbeeld. Daarom is mijn proefschrift voor jou.
Lieve Rob, Thijs en onze nieuwe aanwinst, het werk zal er niet minder op worden nu
ik klaar ben , maar zal er wel altijd voor jullie zijn. Jullie maken het leven bijzonder
en promoveren relatief. Ik hou van jullie.
Liefs Charissa
D

List of publications

List of publications 169
Full papers
van den Brom CE, Boly CA, Bulte CSE, Boer C. Perioperative organ perfusion in
obesity and diabetes.
Submitted
van den Brom CE, Boly CA, Bulte CSE, van den Akker RFP, Kwekkeboom RFJ, Loer
SA, Boer C, Bouwman RA. Sevoflurane impairs myocardial systolic function, but not
myocardial perfusion in diet-induced prediabetic rats.
Submitted
van den Brom CE, Boer C, van den Akker RFP, van der Velden J, Loer SA, Bouwman
RA. Diet composition modulates sevoflurane-induced myocardial depression in rats.
Submitted
Bulte CSE, van den Brom CE, SA Loer, Boer C, Bouwman RA. Myocardial blood flow
under sevoflurane anaesthesia in type 2 diabetic patients: a pilot study.
Submitted
Dekker SE, Viersen VA, Duvekot A, de Jong M, van den Brom CE, Schober P, Boer
C. Lysis Onset Time as Diagnostic Rotational Thromboelastometry Parameter for
Fast Detection of Hyperfibrinolysis.
Submitted
Vonk ABA, Veerhoek D, van den Brom CE, van Barneveld LJM, Boer C.
Individualized heparin and protamine management improves rotational
thromboelastometric parameters and postoperative hemostasis in valve surgery.
Accepted at Journal of Cardiothoracic and Vascular Anesthesia
van den Brom CE, Bulte CSE, Loer SA, Bouwman RA, Boer C. Diabetes,
perioperative ischaemia and volatile anaesthetics: Consequences of derangements
in myocardial substrate metabolism.
Cardiovascular Diabetology (2013), 12:42
Koning NJ, Vonk AB, Verkaik M, van Barneveld LJ, Beishuizen A, Atasever B,
Baufreton C, van den Brom CE, Boer C. Pulsatile flow during cardiopulmonary
bypass preserves postoperative microcirculatory perfusion irrespective of systemic
hemodynamics.
Journal of Applied Physiology (2012), 112(10): 1727-1734
L
170 List of publications
van den Brom CE, Bulte CSE, Kloeze BM, Loer SA, Boer C, Bouwman RA. High-fat
diet-induced glucose intolerance impairs myocardial function, but not myocardial
perfusion during hyperaemia: a pilot study.
Cardiovascular Diabetology (2012), 11:74
van den Brom CE, Bosmans JWAM, Vlasblom R, Huisman MC, Lubberink M, Molthoff
CFM, Lammertsma AA, Boer C, Ouwens DM, Diamant M. Diabetic cardiomyopathy in
Zucker diabetic fatty rats: the forgotten right ventricle.
Cardiovascular Diabetology (2010), 9:25
van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M,
Molthoff CFM, Lammertsma AA, van der Velden J, Boer C, Ouwens DM, Diamant M.
Altered myocardial substrate metabolism is associated with myocardial dysfunction
in early diabetic cardiomyopathy in rats: studies using positron emission
tomography.
Cardiovascular diabetology (2009), 8(1):39
de Snoo MW, van den Brom CE, Jeneson JAL, Everts ME. The effect of wheel
running exercise on plasma IL-6 and muscle IL-6 mRNA levels in mice.
Snoo (2009) chapter 6
Ouwens DM, Diamant M, Fodor M, Habets DDJ, Pelsers MMAL, El Hasnaoui M, Dang
ZC, van den Brom CE, Vlasblom R, Rietdijk A, Boer C, Coort SLM, Glatz JCF,
Luiken LLFP. Cardiac contractile dysfunction in insulin resistant high-fat diet fed rats
associates with elevated CD36-mediated fatty acid uptake and esterification.
Diabetologia (2007), 50: 1938-1948
Van Schothorst EM, Keijer J, Pennings JL, Opperhuizen A, van den Brom CE, Kohl
T, Franssen-van Hal NL, Hoebee B. Adipose gene expression response of lean and
obese mice to short-term dietary restriction.
Obesity (2006), 14(6): 974-979
List of publications 171
Papers in preparation
Koning NJ, de Lange F, van den Brom CE, Shelep I, Bogaards SJ, Niessen HW,
Baufreton C, Boer C. Hemodilution and extracorporeal circulation induce distinct
alterations in microcirculatory perfusion and heterogeneity in a rat model of
cardiopulmonary bypass.
Duvekot A, Viersen VA, Dekker SE, van den Brom CE, Geeraedts jr. LMG, Loer SA,
Schober P, de Waard MC, Spoelstra A, Boer C. Hyperfibrinolysis in out-of-hospital
cardiopulmonary arrest is more prevalent in patients with low cerebral tissue
oxygenation during cardiopulmonary resuscitation.
van den Brom CE, Boer C, van den Akker RFP, Loer SA, Bouwman RA. Western diet
modulates the susceptibility of the heart to ischemic injury and sevoflurane-induced
cardioprotection in rats.
Lamberts RR*, van den Brom CE*, Vlasblom R, Duijst S, Loer SA, Boer C, Diamant
M, Bouwman RA. Diet composition modulates resistance to ischemia and
sevoflurane induced preconditioning in the rat heart.
Overmars MAH, Koning NJ, van den Brom CE, van Bezu J, Vonk ABA, van Nieuw
Amerongen GP, Boer C. In vitro endothelial cell barrier function decreases after
exposure to plasma from patients subjected to cardiopulmonary bypass.
L
172 List of publications
Published abstracts
van den Brom CE, Boer C, van den Akker RFP, Loer SA, Bouwman RA. Western diet
modulates the susceptibility of the heart to ischemic injury and sevoflurane-induced
cardioprotection in rats.
Nederlands tijdschrift voor Anesthesiologie (2013)
van den Brom CE, Boly CA, Bulte CSE, van den Akker RFP, Loer SA, Boer C,
Bouwman RA. Sevoflurane additionally impairs myocardial function, but not
myocardial perfusion in diet-induced prediabetic rats.
Nederlands tijdschrift voor Anesthesiologie (2013)
van den Brom CE, Boer C, van den Akker RFP, Loer SA, Bouwman RA. Western diet
feeding protects against myocardial ischaemic injury, but abolishes sevoflurane-
induced cardioprotection in rats.
European Journal of Anaesthesia (2013)
van den Brom CE, Boer C, van den Akker RFP, Loer SA, Bouwman RA. Changing
diet composition normalizes sevoflurane-induced impaired cardiac function in
diabetic rats.
Nederlands tijdschrift voor Anesthesiologie (2012)
van den Brom CE, Bulte CSE, Voogdt C, Kloeze BM, Loer SA, Boer C, Bouwman RA.
Short-term reduction of saturated fatty acids improves glucose tolerance,
myocardial structure and function in western diet-induced obesity.
Anesthesiology (2011)
Bouwman RA, Bulte CSE, Loer SA, Boer C, van den Brom CE. High fat diet feeding
impairs myocardial function during stress, but not during sevoflurane anesthesia.
Anesthesiology (2011)
van den Brom CE, Bulte CSE, Loer SA, Boer C, Bouwman RA. Western diet feeding
impairs myocardial function during stress, but not during sevoflurane anesthesia.
Nederlands tijdschrift voor Anesthesiologie (2011)
van den Brom CE, Bouwman RA, Gräler MH, Ouwens DM, Diamant M, Boer C.
Reversion of high-fat diet normalizes myocardial function and sphingolipid levels.
Nederlands tijdschrift voor Anesthesiologie (2010)
List of publications 173
Bouwman RA, van den Brom CE, Loer SA, Boer C, Lamberts RR. Diet composition
modulates sevoflurane induced cardioprotection in the rat heart.
Anesthesiology (2009)
Huisman MC, van den Brom CE, Buijs FL, Molthoff CFM, Boellaard R, Lammertsma
AA. Implementation of Physiological Gating on the High Resolution Research
Tomograph.
Nuclear Science Symposium Conference Record (2008): 4767-4769
Bouwman RA, van den Brom CE, Loer SA, Boer C, Lamberts RR. Sevoflurane-
induced cardioprotection in a rat model of high-fat diet-induced type 2 diabetes
mellitus.
European Journal of Anaesthesia (2008); 25 [Supl 44]: 4AP6-3
Bouwman RA, van den Brom CE, Vlasblom R, Loer SA, Boer C, Diamant M,
Lamberts RR. Cardioprotection and dietary intake in a rat model of diet-induced
type 2 diabetes mellitus.
Nederlands tijdschrift voor Anesthesiologie (2008)
Ouwens DM, van den Brom CE, Kriek J, Schaart G, Hesselink MK, Schrauwen P,
Vlasblom R, Diamant M. Dietary fish-oil preserves cardiac contractile function by
upregulation of UCP3 in a rat model of high-fat diet-induced glucose tolerance and
cardiomyopathy.
Diabetologia (2007); 50 [Suppl1]: S90 (P-0206)
van den Brom CE, Vlasblom R, Kriek J, Rietdijk A, Duijst S, Salic K, Ouwens DM,
Diamant M. High fat diet-induced relocation of CD36 to the sarcolemma precedes
cardiac dysfunction and associates with activated PKB/AKT.
Nederlands tijdschrift voor diabetes (2007)
Vlasblom R, van den Brom CE, Salic K, Kriek J, Boer C, Ouwens DM, Diamant M.
Western-type diet-induced cardiac contractile dysfunction is associated with
nutrient-specific cardiomyocyte remodeling and activation of the Akt-regulated
transcription factor GATA-4 in mice.
Nederlands tijdschrift voor diabetes (2007)
Salic K, van den Brom CE, Vlasblom R, Kriek J, Schaart G, Hesselink MK,
Schrauwen P,Ouwens DM, Diamant M. Myocardial contractile function is preserved
by dietary fish-oil supplementation through upregulation of UCP3 in a rat model of
high-fat diet-induced impaired glucose tolerance and cardiomyopathy.
Nederlands tijdschrift voor diabetes (2007)
L
174 List of publications
van den Brom CE, Vlasblom R, Fodor M, Boer C, Ouwens DM, Diamant M. Short-
term exposure to polyunsaturated high fat diet preserves cardiac contractile
function in rats.
Diabetologia (2006) 49: [Suppl1] 326(P-0534)
Vlasblom R, Ouwens DM, van den Brom CE, Boer C, Diamant M. In wild type mice
long-term exposure to high-fat diet induces systemic insulin resistance without
affecting cardiac function.
Diabetologia (2006) 49: [Suppl1] 327
Vlasblom R, Ouwens DM, van den Brom CE, Boer C, Diamant M. Long-Term
Exposure to High-Fat Diet Induces Systemic Insulin Resistance without Affecting
Cardiac Function in Wild Type Mice.
Diabetes (2006) 55: [Suppl 1] A338
Vlasblom R, Ouwens DM, van den Brom CE, Fodor M, Boer C, Diamant M. Short
Term Exposure to a High-Fat Diet Results in Impaired Glucose Tolerance, Cardiac
Dysfunction and Epicardial Fat Accumulation in Rats.
Diabetes (2006) 55: [Suppl 1] A338
van den Brom CE, Vlasblom R, Ouwens DM, Fodor M, Boer C, Diamant M. Short
Term Exposure to a High-Fat Diet Results in Impaired Glucose Tolerance, Cardiac
Dysfunction and Epicardial Fat Accumulation in Rats.
Nederlands tijdschrift voor diabetes (2006)


Curriculum Vitae

Curriculum Vitae 179
Charissa Esmé van den Brom was born on July 8th 1982 in Nijkerk, the
Netherlands. After graduating from secondary school (havo, Amersfoort) in 1999 she
started the study Biochemistry at the University of Applied Sciences in Utrecht. She
did a research apprenticeship at the Department of Toxicology, Pathology and
started her master Medical Biology at the VU University in Amsterdam. During her
master she did a research apprenticeship at the Institute of Food Research in
Norwich, England and a research apprenticeship within the Department of Anatomy
and Physiology at Utrecht University. She obtained her Master degree in August
2005 and subsequently started as PhD student at the Department of Internal
Medicine and Laboratory for Physiology at the VU University Medical Center in
Amsterdam. In July 2010 she started her PhD-research at the Department of
Anesthesiology and Laboratory for Physiology at the VU University Medical Center in
Amsterdam. The results of this research are presented in this dissertation. She is
two-time runner-up and in 2011 winner of the best presentation at the Dutch Society
of Anesthesiologists conference. She is co-founder and coordinator of the
Experimental Laboratory for VItal Signs (ELVIS). From January 2013 she is employed
as a postdoctoral researcher at the Department of Anesthesiology of the VU
University Medical Center in Amsterdam. Charissa is married to Rob Morren. They
are the proud parents of Thijs (2012). In May 2014 they are expecting their second
child.
Charissa Esmé van den Brom werd geboren op 8 juli 1982 te Nijkerk. Na het
behalen van haar havo diploma startte zij in 1999 met de studie Biochemie aan de
hogeschool van Utrecht. Haar afstudeerstage heeft zij gelopen op de afdeling
Toxicologie, Pathologie en Genetica van het RIVM te Bilthoven. Na het behalen van
haar ingenieurs titel begon zij in 2003 met de master Medische Biologie aan de Vrije
Universiteit te Amsterdam. Tijdens deze studie verbleef ze voor een half jaar in
Norwich (Verenigd Koninkrijk) voor een onderzoeksstage bij het Institute for Food
Research. Haar afstudeerstage volbracht zij op de afdeling Anatomie en Fysiologie
aan de faculteit Diergeneeskunde van de Universiteit van Utrecht. In augustus 2005
behaalde zij haar doctoraalexamen. In januari 2006 startte zij als promovenda aan
de afdelingen Interne Geneeskunde en Fysiologie van het VU medisch centrum. In
juli 2010 begon zij als promovenda aan de afdelingen Anesthesiologie en Fysiologie
aan het VU medisch centrum te Amsterdam. De resultaten van dit onderzoek staan
in dit proefschrift beschreven. Ze is tweevoudig runner-up en de 2011 winnaar van
de beste presentatie op het congres van de Nederlandse Vereniging voor
Anesthesiologie. Ze is mede oprichtster en coördinator van het Experimental
Laboratory for VItal Signs (ELVIS). Per januari 2013 is zij werkzaam als post-
doctorale onderzoeker op de afdeling Anesthesiologie aan het VU medisch centrum
CV

180 Curriculum Vitae
te Amsterdam. Charissa is getrouwd met Rob Morren. Samen zijn ze de trotse
ouders van hun zoon Thijs (2012). In mei 2014 verwachten ze hun tweede kindje.
Charissa Esmé van den Brom
Dietary modulation of the effects of sevoflurane on myocardial perfusion, function and ischemic injuryin rats
Dietary m
odulation of the effects of sevoflurane on myocardial perfusion, function and ischem
ic injury in rats Charissa Esm
é van den Brom
UITNODIGING
voor het bijwonen van de openbare verdediging van
het proefschrift
Dietary modulation of the effects of sevoflurane on
myocardial perfusion, function and ischemic
injury in rats
door Charissa van den Brom
Donderdag 30 januari 2014 om 15.45 uur
In de aula van het Hoofdgebouw
Vrije UniversiteitDe Boelelaan 1105
te Amsterdam
Receptie na afloop van de promotie
Paranimfen
Ester [email protected]
Marianne de Gruil-van [email protected]
Top Related