






Talen
Pages
Wettelijk


8/6/2019 ADHD - Barkley
http://slidepdf.com/reader/full/adhd-barkley 1/6
Attention-Deficit Hyperactivity Disorder66 Scientific American September 1998
Attention-DeficitHyperactivity Disorder
A new theory suggests the disorder results from a failure in self-control.ADHD may arise when key brain circuits do not develop
properly, perhaps because of an altered gene or genes
by Russell A. Barkley
Y A N N A S C I M B E N E
Copyright 1998 Scientific American, Inc.

8/6/2019 ADHD - Barkley
http://slidepdf.com/reader/full/adhd-barkley 2/6
As I watched five-year-old Keithin the waiting room of my of-fice, I could see why his par-
ents said he was having such a toughtime in kindergarten. He hopped fromchair to chair, swinging his arms and legsrestlessly, and then began to fiddle withthe light switches, turning the lights on
and off again to everyone’s annoyance—all the while talking nonstop. When hismother encouraged him to join a groupof other children busy in the playroom,Keith butted into a game that was al-ready in progress and took over, caus-ing the other children to complain of hisbossiness and drift away to other activ-ities. Even when Keith had the toys tohimself, he fidgeted aimlessly with themand seemed unable to entertain himself quietly. Once I examined him more ful-ly, my initial suspicions were confirmed:Keith had attention-deficit hyperactivi-ty disorder (ADHD).
Since the 1940s, psychiatrists have ap-plied various labels to children who arehyperactive and inordinately inattentiveand impulsive. Such youngsters havebeen considered to have “minimal braindysfunction,” “brain-injured child syn-drome,” “hyperkinetic reaction of child-hood,” “hyperactive child syndrome”and, most recently, “attention-deficit dis-order.” The frequent name changes re-flect how uncertain researchers havebeen about the underlying causes of,
and even the precise diagnostic criteriafor, the disorder.
Within the past several years, howev-er, those of us who study ADHD havebegun to clarify its symptoms and caus-es and have found that it may have agenetic underpinning. Today’s view of the basis of the condition is strikinglydifferent from that of just a few yearsago. We are finding that ADHD is not adisorder of attention per se, as had longbeen assumed. Rather it arises as a de-velopmental failure in the brain circuit-
ry that underlies inhibition and self-control. This loss of self-control in turnimpairs other important brain func-tions crucial for maintaining attention,including the ability to defer immediaterewards for later, greater gain.
ADHD involves two sets of symptoms:inattention and a combination of hyper-
active and impulsive behaviors [see tableon next page]. Most children are moreactive, distractible and impulsive thanadults. And they are more inconsistent,affected by momentary events and dom-inated by objects in their immediate en-vironment. The younger the children,the less able they are to be aware of
time or to give priority to future eventsover more immediate wants. Such be-haviors are signs of a problem, howev-er, when children display them signifi-cantly more than their peers do.
Boys are at least three times as likelyas girls to develop the disorder; indeed,some studies have found that boys withADHD outnumber girls with the condi-tion by nine to one, possibly becauseboys are genetically more prone to dis-orders of the nervous system. The be-havior patterns that typify ADHD usu-ally arise between the ages of three andfive. Even so, the age of onset can varywidely: some children do not developsymptoms until late childhood or evenearly adolescence. Why their symptomsare delayed remains unclear.
Huge numbers of people are affected.Many studies estimate that between 2and 9.5 percent of all school-age chil-dren worldwide have ADHD; research-ers have identified it in every nation andculture they have studied. What is more,the condition, which was once thoughtto ease with age, can persist into adult-
hood. For example, roughly two thirdsof 158 children with ADHD my col-leagues and I evaluated in the 1970sstill had the disorder in their twenties.And many of those who no longer fitthe clinical description of ADHD werestill having significant adjustment prob-lems at work, in school or in other so-cial settings.
To help children (and adults) withADHD, psychiatrists and psychologistsmust better understand the causes of thedisorder. Because researchers have tra-
ditionally viewed ADHD as a problemin the realm of attention, some have sug-gested that it stems from an inability of the brain to filter competing sensory in-puts, such as sights and sounds. But re-cently scientists led by Joseph A. Ser-geant of the University of Amsterdamhave shown that children with ADHDdo not have difficulty in that area; in-stead they cannot inhibit their impulsivemotor responses to such input. Otherresearchers have found that childrenwith ADHD are less capable of prepar-
ing motor responses in anticipation of
events and are insensitive to feedbackabout errors made in those responses.For example, in a commonly used testof reaction time, children with ADHDare less able than other children to readythemselves to press one of several keyswhen they see a warning light. They alsodo not slow down after making mis-
takes in such tests in order to improvetheir accuracy.
The Search for a Cause
No one knows the direct and imme-diate causes of the difficulties ex-
perienced by children with ADHD, al-though advances in neurological imag-ing techniques and genetics promise toclarify this issue over the next five years.Already they have yielded clues, albeitones that do not yet fit together into acoherent picture.
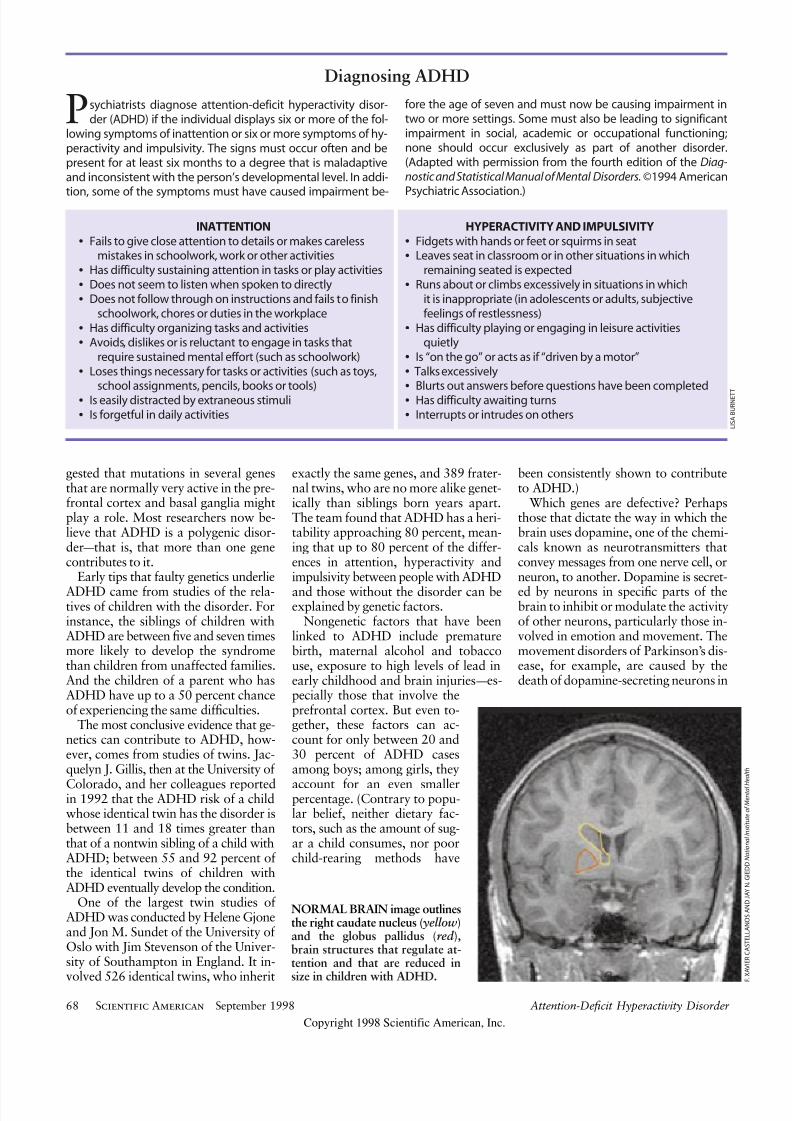
Imaging studies over the past decadehave indicated which brain regions mightmalfunction in patients with ADHD andthus account for the symptoms of thecondition. That work suggests the in-volvement of the prefrontal cortex, partof the cerebellum, and at least two of the clusters of nerve cells deep in thebrain that are collectively known as thebasal ganglia [see illustration on page69]. In a 1996 study F. Xavier Castel-lanos, Judith L. Rapoport and their col-leagues at the National Institute of Men-
tal Health found that the right prefron-tal cortex and two basal ganglia calledthe caudate nucleus and the globus pal-lidus are significantly smaller than nor-mal in children with ADHD. Earlierthis year Castellanos’s group found thatthe vermis region of the cerebellum isalso smaller in ADHD children.
The imaging findings make sense be-cause the brain areas that are reducedin size in children with ADHD are thevery ones that regulate attention. Theright prefrontal cortex, for example, is
involved in “editing” one’s behavior, re-sisting distractions and developing anawareness of self and time. The caudatenucleus and the globus pallidus help toswitch off automatic responses to allowmore careful deliberation by the cortexand to coordinate neurological inputamong various regions of the cortex.The exact role of the cerebellar vermis isunclear, but early studies suggest it mayplay a role in regulating motivation.
What causes these structures to shrinkin the brains of those with ADHD? No
one knows, but many studies have sug-
Attention-Deficit Hyperactivity Disorder Scientific American September 1998 67
CHILDREN WITH ADHD cannot con-trol their responses to their environment.This lack of control makes them hyperac-
tive, inattentive and impulsive.
Copyright 1998 Scientific American, Inc.
8/6/2019 ADHD - Barkley
http://slidepdf.com/reader/full/adhd-barkley 3/6
gested that mutations in several genesthat are normally very active in the pre-frontal cortex and basal ganglia mightplay a role. Most researchers now be-lieve that ADHD is a polygenic disor-der—that is, that more than one genecontributes to it.
Early tips that faulty genetics underlie
ADHD came from studies of the rela-tives of children with the disorder. Forinstance, the siblings of children withADHD are between five and seven timesmore likely to develop the syndromethan children from unaffected families.And the children of a parent who hasADHD have up to a 50 percent chanceof experiencing the same difficulties.
The most conclusive evidence that ge-netics can contribute to ADHD, how-ever, comes from studies of twins. Jac-quelyn J. Gillis, then at the University of
Colorado, and her colleagues reportedin 1992 that the ADHD risk of a childwhose identical twin has the disorder isbetween 11 and 18 times greater thanthat of a nontwin sibling of a child withADHD; between 55 and 92 percent of the identical twins of children withADHD eventually develop the condition.
One of the largest twin studies of ADHD was conducted by Helene Gjoneand Jon M. Sundet of the University of Oslo with Jim Stevenson of the Univer-sity of Southampton in England. It in-
volved 526 identical twins, who inherit
exactly the same genes, and 389 frater-nal twins, who are no more alike genet-ically than siblings born years apart.The team found that ADHD has a heri-tability approaching 80 percent, mean-ing that up to 80 percent of the differ-ences in attention, hyperactivity andimpulsivity between people with ADHD
and those without the disorder can beexplained by genetic factors.
Nongenetic factors that have beenlinked to ADHD include prematurebirth, maternal alcohol and tobaccouse, exposure to high levels of lead inearly childhood and brain injuries—es-pecially those that involve theprefrontal cortex. But even to-gether, these factors can ac-count for only between 20 and30 percent of ADHD casesamong boys; among girls, they
account for an even smallerpercentage. (Contrary to popu-lar belief, neither dietary fac-tors, such as the amount of sug-ar a child consumes, nor poorchild-rearing methods have
been consistently shown to contributeto ADHD.)
Which genes are defective? Perhapsthose that dictate the way in which thebrain uses dopamine, one of the chemi-cals known as neurotransmitters thatconvey messages from one nerve cell, orneuron, to another. Dopamine is secret-
ed by neurons in specific parts of thebrain to inhibit or modulate the activityof other neurons, particularly those in-volved in emotion and movement. Themovement disorders of Parkinson’s dis-ease, for example, are caused by thedeath of dopamine-secreting neurons in
Attention-Deficit Hyperactivity Disorder68 Scientific American September 1998
NORMAL BRAIN image outlinesthe right caudate nucleus ( yellow)and the globus pallidus (red ), brain structures that regulate at-tention and that are reduced in
size in children with ADHD.
Psychiatrists diagnose attention-deficit hyperactivity disor-der (ADHD) if the individual displays six or more of the fol-
lowing symptoms of inattention or six or more symptoms of hy-peractivity and impulsivity. The signs must occur often and bepresent for at least six months to a degree that is maladaptiveand inconsistent with the person’s developmental level. In addi-
tion, some of the symptoms must have caused impairment be-
fore the age of seven and must now be causing impairment intwo or more settings. Some must also be leading to significantimpairment in social, academic or occupational functioning;none should occur exclusively as part of another disorder.(Adapted with permission from the fourth edition of the Diag-nostic and Statistical Manual of Mental Disorders.©1994 American
Psychiatric Association.)
INATTENTION
• Fails to give close attention to details or makes carelessmistakes in schoolwork, work or other activities
• Has difficulty sustaining attention in tasks or play activities
• Does not seem to listen when spoken to directly
• Does not follow through on instructions and fails to finishschoolwork, chores or duties in the workplace
• Has difficulty organizing tasks and activities
• Avoids, dislikes or is reluctant to engage in tasks thatrequire sustained mental effort (such as schoolwork)
• Loses things necessary for tasks or activities (such as toys,school assignments, pencils, books or tools)
• Is easily distracted by extraneous stimuli
• Is forgetful in daily activities
HYPERACTIVITY AND IMPULSIVITY
• Fidgets with hands or feet or squirms in seat
• Leaves seat in classroom or in other situations in whichremaining seated is expected
• Runs about or climbs excessively in situations in whichit is inappropriate (in adolescents or adults, subjectivefeelings of restlessness)
• Has difficulty playing or engaging in leisure activitiesquietly
• Is “on the go” or acts as if “driven by a motor”
• Talks excessively
•Blurts out answers before questions have been completed
• Has difficulty awaiting turns
• Interrupts or intrudes on others
Diagnosing ADHD
F . X A V I E R C A S T E L L A N O S A N D J A Y N . G
I E D D N a t i o n a l I n s t i t u t e o f M e n t a l H e a l t h
L I S A B U R N E T T
Copyright 1998 Scientific American, Inc.
8/6/2019 ADHD - Barkley
http://slidepdf.com/reader/full/adhd-barkley 4/6
a region of the brain underneaththe basal ganglia called the sub-stantia nigra.
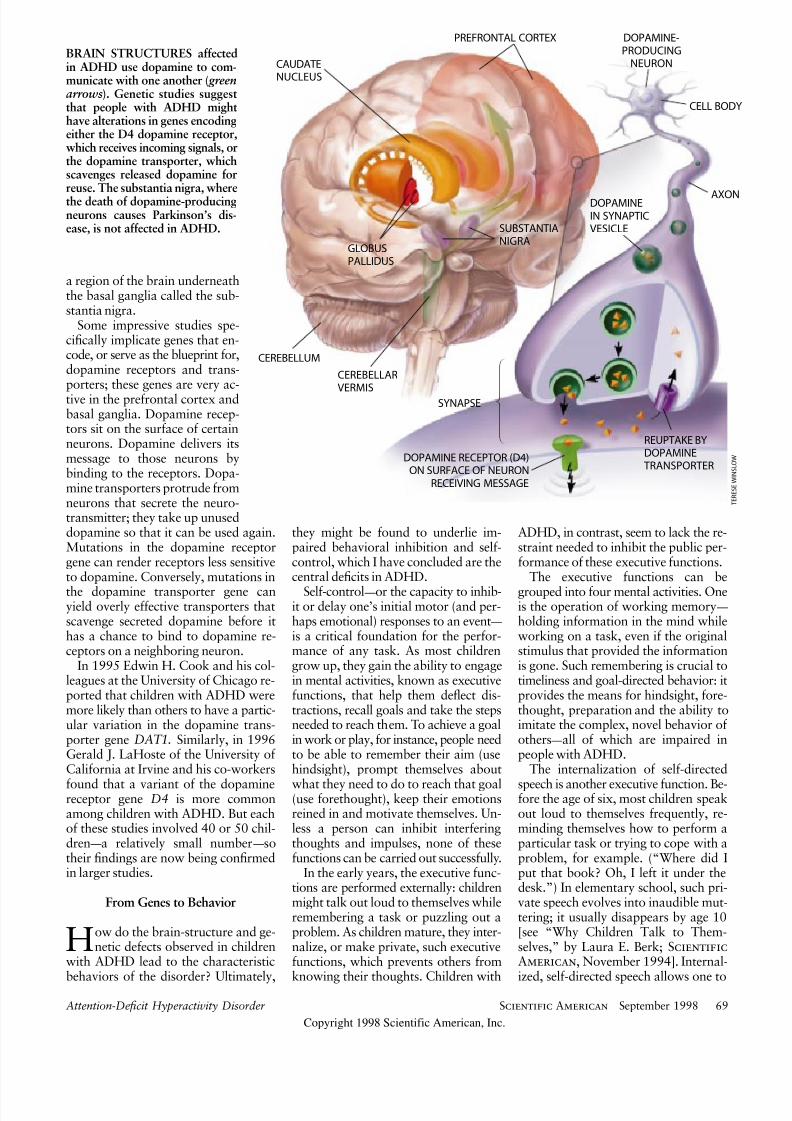
Some impressive studies spe-cifically implicate genes that en-code, or serve as the blueprint for,dopamine receptors and trans-porters; these genes are very ac-tive in the prefrontal cortex andbasal ganglia. Dopamine recep-tors sit on the surface of certainneurons. Dopamine delivers itsmessage to those neurons bybinding to the receptors. Dopa-mine transporters protrude fromneurons that secrete the neuro-transmitter; they take up unuseddopamine so that it can be used again.Mutations in the dopamine receptorgene can render receptors less sensitiveto dopamine. Conversely, mutations in
the dopamine transporter gene canyield overly effective transporters thatscavenge secreted dopamine before ithas a chance to bind to dopamine re-ceptors on a neighboring neuron.
In 1995 Edwin H. Cook and his col-leagues at the University of Chicago re-ported that children with ADHD weremore likely than others to have a partic-ular variation in the dopamine trans-porter gene DAT1. Similarly, in 1996Gerald J. LaHoste of the University of California at Irvine and his co-workers
found that a variant of the dopaminereceptor gene D4 is more commonamong children with ADHD. But eachof these studies involved 40 or 50 chil-dren—a relatively small number—sotheir findings are now being confirmedin larger studies.
From Genes to Behavior
How do the brain-structure and ge-netic defects observed in children
with ADHD lead to the characteristic
behaviors of the disorder? Ultimately,
they might be found to underlie im-paired behavioral inhibition and self-control, which I have concluded are thecentral deficits in ADHD.
Self-control—or the capacity to inhib-it or delay one’s initial motor (and per-haps emotional) responses to an event—is a critical foundation for the perfor-mance of any task. As most childrengrow up, they gain the ability to engagein mental activities, known as executivefunctions, that help them deflect dis-tractions, recall goals and take the stepsneeded to reach them. To achieve a goalin work or play, for instance, people needto be able to remember their aim (usehindsight), prompt themselves about
what they need to do to reach that goal(use forethought), keep their emotionsreined in and motivate themselves. Un-less a person can inhibit interferingthoughts and impulses, none of thesefunctions can be carried out successfully.
In the early years, the executive func-tions are performed externally: childrenmight talk out loud to themselves whileremembering a task or puzzling out aproblem. As children mature, they inter-nalize, or make private, such executivefunctions, which prevents others from
knowing their thoughts. Children with
ADHD, in contrast, seem to lack the re-straint needed to inhibit the public per-formance of these executive functions.
The executive functions can be
grouped into four mental activities. Oneis the operation of working memory—
holding information in the mind whileworking on a task, even if the originalstimulus that provided the informationis gone. Such remembering is crucial totimeliness and goal-directed behavior: itprovides the means for hindsight, fore-thought, preparation and the ability toimitate the complex, novel behavior of others—all of which are impaired inpeople with ADHD.
The internalization of self-directed
speech is another executive function. Be-fore the age of six, most children speakout loud to themselves frequently, re-minding themselves how to perform aparticular task or trying to cope with aproblem, for example. (“Where did Iput that book? Oh, I left it under thedesk.”) In elementary school, such pri-vate speech evolves into inaudible mut-tering; it usually disappears by age 10[see “Why Children Talk to Them-selves,” by Laura E. Berk; ScientificAmerican, November 1994]. Internal-
ized, self-directed speech allows one to
Attention-Deficit Hyperactivity Disorder Scientific American September 1998 69
BRAIN STRUCTURES affectedin ADHD use dopamine to com-municate with one another ( greenarrows). Genetic studies suggestthat people with ADHD mighthave alterations in genes encodingeither the D4 dopamine receptor,which receives incoming signals, orthe dopamine transporter, whichscavenges released dopamine forreuse. The substantia nigra, wherethe death of dopamine-producingneurons causes Parkinson’s dis-ease, is not affected in ADHD.
T E R E S E W I N S L O W
PREFRONTAL CORTEX
CAUDATENUCLEUS
GLOBUSPALLIDUS
CEREBELLAR
VERMIS
CEREBELLUM
SUBSTANTIANIGRA
DOPAMINE-PRODUCING
NEURON
CELL BODY
AXONDOPAMINEIN SYNAPTICVESICLE
SYNAPSE
REUPTAKE BYDOPAMINE
TRANSPORTERDOPAMINE RECEPTOR (D4)
ON SURFACE OF NEURONRECEIVING MESSAGE
Copyright 1998 Scientific American, Inc.

8/6/2019 ADHD - Barkley
http://slidepdf.com/reader/full/adhd-barkley 5/6
reflect to oneself, to follow rules and in-structions, to use self-questioning as aform of problem solving and to con-struct “meta-rules,” the basis for under-standing the rules for using rules—allquickly and without tipping one’s hand
to others. Laura E. Berk and her col-leagues at Illinois State University re-ported in 1991 that the internalizationof self-directed speech is delayed in boyswith ADHD.
A third executive mental function con-sists of controlling emotions, motivationand state of arousal. Such control helpsindividuals achieve goals by enablingthem to delay or alter potentially dis-tracting emotional reactions to a partic-ular event and to generate private emo-tions and motivation. Those who rein
in their immediate passions can also be-have in more socially acceptable ways.
The final executive function, reconsti-tution, actually encompasses two sepa-rate processes: breaking down observedbehaviors and combining the parts intonew actions not previously learned fromexperience. The capacity for reconstitu-tion gives humans a great degree of flu-ency, flexibility and creativity; it allowsindividuals to propel themselves towarda goal without having to learn all theneeded steps by rote. It permits children
as they mature to direct their behavior
across increasingly longer intervals bycombining behaviors into ever longerchains to attain a goal. Initial studiesimply that children with ADHD are lesscapable of reconstitution than are otherchildren.
I suggest that like self-directed speech,the other three executive functions be-come internalized during typical neuraldevelopment in early childhood. Suchprivatization is essential for creating vi-sual imagery and verbal thought. Aschildren grow up, they develop the ca-pacity to behave covertly, to mask someof their behaviors or feelings from oth-ers. Perhaps because of faulty geneticsor embryonic development, childrenwith ADHD have not attained this abil-ity and therefore display too much pub-
lic behavior and speech. It is my asser-tion that the inattention, hyperactivityand impulsivity of children with ADHDare caused by their failure to be guidedby internal instructions and by their in-ability to curb their own inappropriatebehaviors.
Prescribing Self-Control
If, as I have outlined, ADHD is a fail-ure of behavioral inhibition that de-
lays the ability to privatize and execute
the four executive mental functions I
have described, the finding supports thetheory that children with ADHD mightbe helped by a more structured envi-ronment. Greater structure can be animportant complement to any drug ther-apy the children might receive. Current-
ly children (and adults) with ADHD of-ten receive drugs such as Ritalin thatboost their capacity to inhibit and regu-late impulsive behaviors. These drugsact by inhibiting the dopamine trans-porter, increasing the time that dopa-mine has to bind to its receptors on oth-er neurons.
Such compounds (which, despite theirinhibitory effects, are known as psycho-stimulants) have been found to improvethe behavior of between 70 and 90 per-cent of children with ADHD older than
five years. Children with ADHD whotake such medication not only are lessimpulsive, restless and distractible butare also better able to hold importantinformation in mind, to be more pro-ductive academically, and to have moreinternalized speech and better self-con-trol. As a result, they tend to be likedbetter by other children and to experi-ence less punishment for their actions,which improves their self-image.
My model suggests that in additionto psychostimulants—and perhaps an-
tidepressants, for some children—treat-
Attention-Deficit Hyperactivity Disorder70 Scientific American September 1998
A Psychological Model of ADHD
A loss of behavioral inhibition and self-control leads to the following disruptions in brain functioning:
IMPAIRED FUNCTION
Nonverbal working memory
Internalization of self-directed speech
Self-regulation of mood, motivationand level of arousal
Reconstitution (ability to break downobserved behaviors into componentparts that can be recombined intonew behaviors in pursuit of a goal)
CONSEQUENCE
Diminished sense of timeInability to hold events in mindDefective hindsight
Defective forethought
Deficient rule-governed behaviorPoor self-guidance and
self-questioning
Displays all emotions publicly;cannot censor them
Diminished self-regulationof drive and motivation
Limited ability to analyze behaviorsand synthesize new behaviors
Inability to solve problems
EXAMPLE
Nine-year-old Jeff routinely forgets importantresponsibilities, such as deadlines for book reports or an after-school appointment
with the principal
Five-year-old Audrey talks too much andcannot give herself useful directionssilently on how to perform a task
Eight-year-old Adam cannot maintain thepersistent effort required to read a storyappropriate for his age level and is quick to display his anger when frustrated byassigned schoolwork
Fourteen-year-old Ben stops doing ahomework assignment when he realizesthat he has only two of the five assignedquestions; he does not think of a way tosolve the problem, such as calling a friendto get the other three questions
L I S A B U R N E T T
Copyright 1998 Scientific American, Inc.

8/6/2019 ADHD - Barkley
http://slidepdf.com/reader/full/adhd-barkley 6/6
ment for ADHD should include train-
ing parents and teachers in specific andmore effective methods for managingthe behavioral problems of children withthe disorder. Such methods involve mak-ing the consequences of a child’s actionsmore frequent and immediate and in-creasing the external use of promptsand cues about rules and time intervals.Parents and teachers must aid childrenwith ADHD by anticipating events forthem, breaking future tasks down intosmaller and more immediate steps, andusing artificial immediate rewards. All
these steps serve to externalize time,
rules and consequences as a replace-ment for the weak internal forms of in-formation, rules and motivation of chil-dren with ADHD.
In some instances, the problems of ADHD children may be severe enoughto warrant their placement in specialeducation programs. Although suchprograms are not intended as a cure forthe child’s difficulties, they typically doprovide a smaller, less competitive andmore supportive environment in whichthe child can receive individual instruc-
tion. The hope is that once children
learn techniques to overcome their defi-cits in self-control, they will be able tofunction outside such programs.
There is no cure for ADHD, but muchmore is now known about effectivelycoping with and managing this persis-tent and troubling developmental disor-der. The day is not far off when genetictesting for ADHD may become avail-able and more specialized medicationsmay be designed to counter the specificgenetic deficits of the children who suf-fer from it.
Attention-Deficit Hyperactivity Disorder Scientific American September 1998 71
The Author
RUSSELL A. BARKLEY is director of psychology and pro-fessor of psychiatry and neurology at the University of Massa-chusetts Medical Center in Worcester. He received his B.A.from the University of North Carolina at Chapel Hill and hisM.A. and Ph.D. from Bowling Green State University. He hasstudied ADHD for nearly 25 years and has written many scien-tific papers, book chapters and books on the subject, includingADHD and the Nature of Self-Control (Guilford Press, 1997)and Attention-Deficit Hyperactivity Disorder: A Handbookfor Diagnosis and Treatment (Guilford Press, 1998).
Further Reading
The Epidemiology of Attention-Deficit Hyperactivity Disor-der. Peter Szatmari in Child and Adolescent Psychiatric Clinics of North America, Vol. 1. Edited by G. Weiss. W. B. Saunders, 1992.
Hyperactive Children Grown Up. Gabrielle Weiss and Lily Troken-berg Hechtman. Guilford Press, 1993.
Taking Charge of ADHD: The Complete, Authoritative Guidefor Parents. R. A. Barkley. Guilford Press, 1995.
Dopamine D4 Receptor Gene Polymorphism Is Associated withAttention Deficit Hyperactivity Disorder. G. J. LaHoste et al. inMolecular Psychiatry, Vol. 1, No. 2, pages 121–124; May 1996.
PSYCHOLOGICAL TESTS used in ADHD re-search include the four depicted here. The tow-er-building test (upper left ), in which the subjectis asked to assemble balls into a tower to mimican illustration, measures forethought, planningand persistence. The math test (upper right ) as-sesses working memory and problem-solvingability. In the auditory attention test (below),the subject must select the appropriate coloredtile according to taped instructions, despite dis-tracting words. The time estimation test (lower right ) measures visual attention and subjectivesense of time intervals. The subject is asked tohold down a key to illuminate a lightbulb on acomputer screen for the same length of time thatanother bulb was illuminated previously.
P H O T O G R A P H S B Y S T E P H E N R O S E G a m m a L i a i s o n
SA
Copyright 1998 Scientific American, Inc.
Top Related