Voortgezette Lineaire Algebra Prof. dr. J. van Mill Dr. F. van Schagen
Ocular Emergencies Dr Eva Diltoer oftalmologie
Dr Lien Mestdagh urgentiegeneeskunde
Voortgezette Opleiding
Urgentiegeneeskunde
Aanmeldingsklacht : Wie? Bv man 35jaar
Wat? Bv Pijn, roodheid, tranen
Waar? Bv rechter oog
Wanneer? Sinds deze middag na sl i jpen van metaal
Visus?
Contactlensdrager?
Oogheelkundige antecedenten Bv cataractoperatie
Algemene antecedenten Bv diabetes, reuma
Familiale antecedenten Bv glaucoom
Thuismedicatie
ANAMNESE
Gezichtsscherpte van het centrale zien / veraf
Met bril/contactlenzen
Oog per oog
ONDERZOEK: VISUS
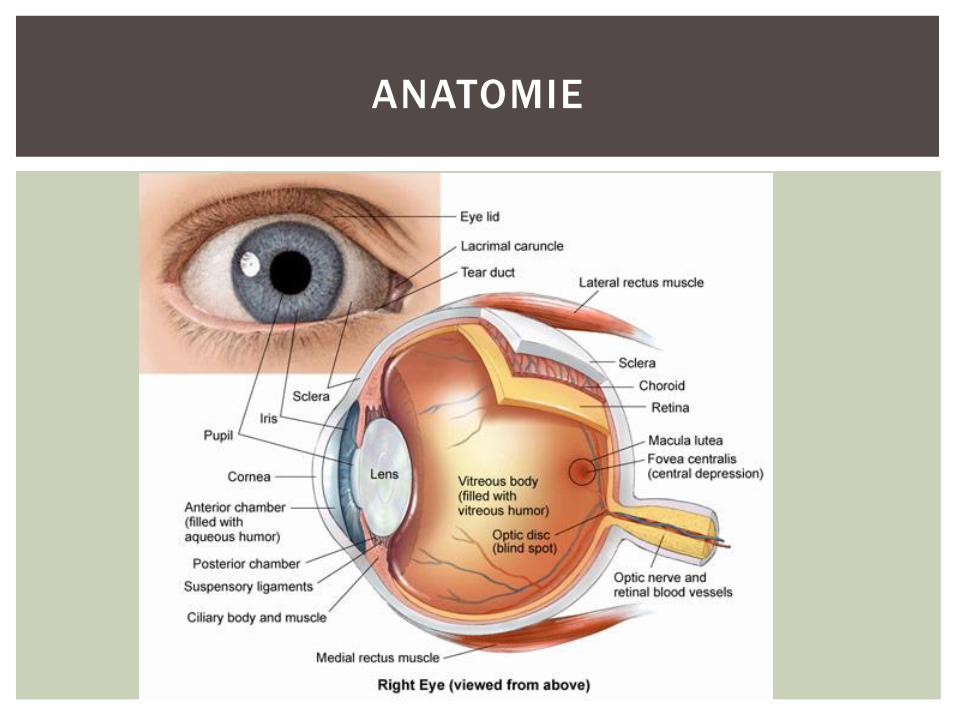
ANATOMIE
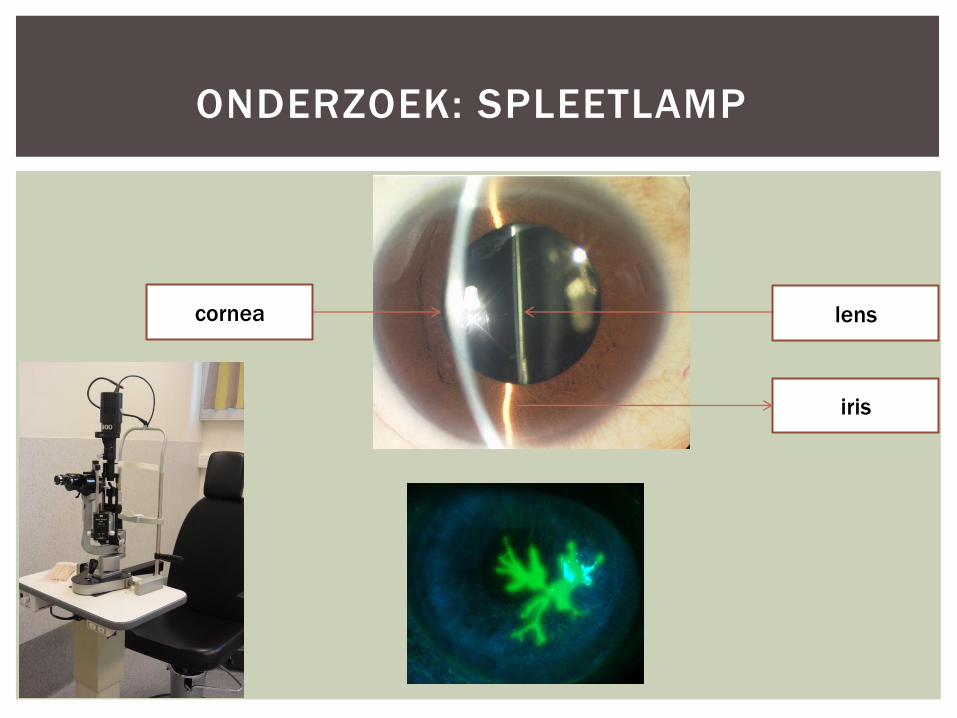
ONDERZOEK: SPLEETLAMP
cornea lens
iris
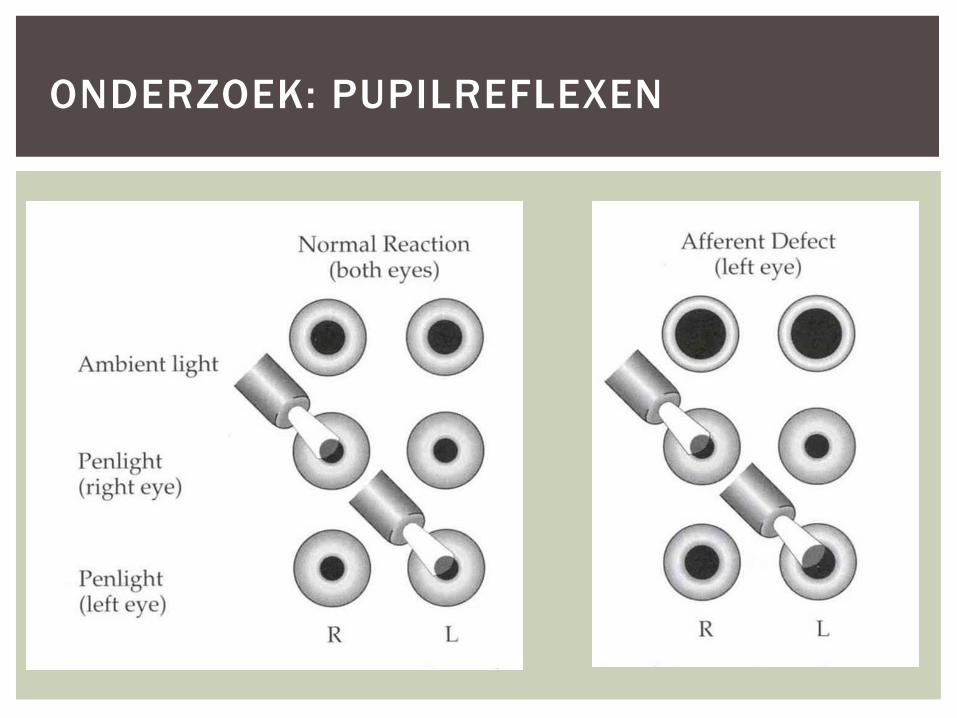
ONDERZOEK: PUPILREFLEXEN
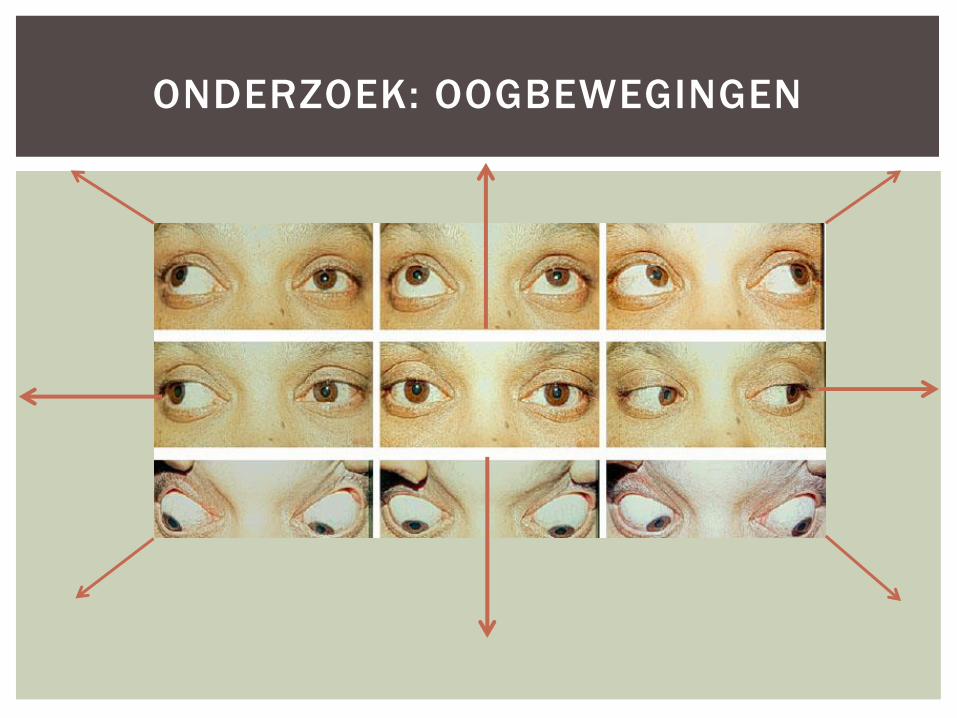
ONDERZOEK: OOGBEWEGINGEN
Patiënt dekt één oog af
Patiënt zit op één meter afstand
Patiënt kijkt naar de neus van de onderzoeker
Vingers opsteken in 4 kwadranten
Evt vingers bewegen
ONDERZOEK: GEZICHTSVELD
Infecties
Pre- en postseptale cellulitis
Chalazion
Allergische, virale en bacteriële conjunctivitis
Herpes Simplex en Herpes Zoster
Corneaal infiltraat/ulcus
Iritis
Endophtalmitis
Trauma
Visusdaling of –verlies
OCULAR EMERGENCIES
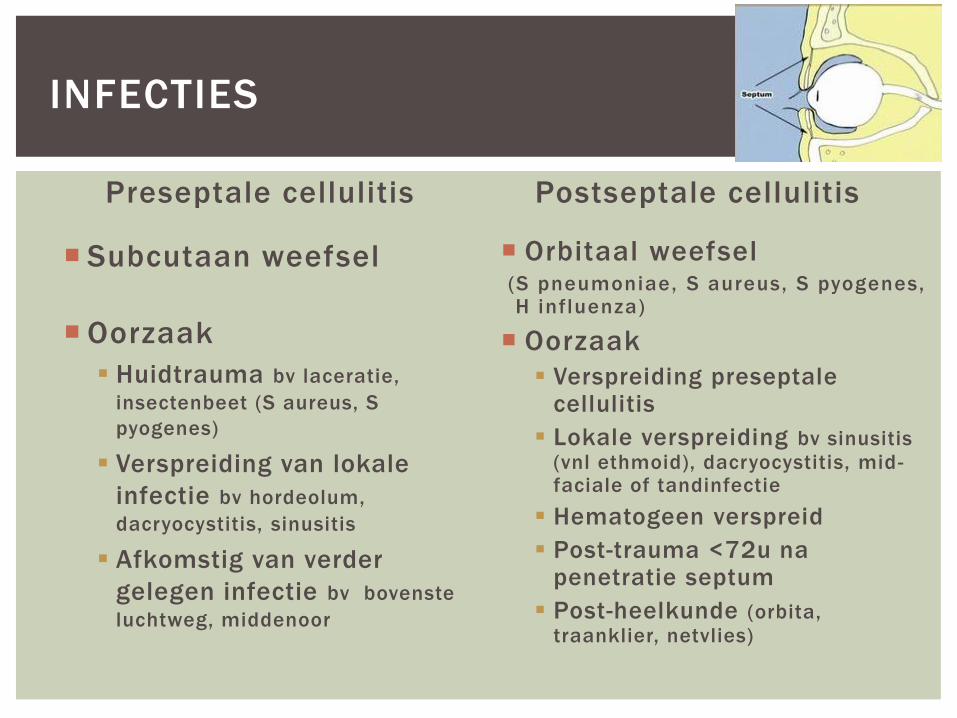
Preseptale cellulitis
Subcutaan weefsel
Oorzaak
Huidtrauma bv laceratie,
insectenbeet (S aureus, S
pyogenes)
Verspreiding van lokale
infectie bv hordeolum,
dacryocystitis, sinusitis
Afkomstig van verder
gelegen infectie bv bovenste
luchtweg, middenoor
Postseptale cellulitis
Orbitaal weefsel (S pneumoniae, S aureus, S pyogenes, H influenza)
Oorzaak
Verspreiding preseptale cellulitis
Lokale verspreiding bv sinusitis
(vnl ethmoid), dacryocystitis, mid-faciale of tandinfectie
Hematogeen verspreid
Post-trauma <72u na penetratie septum
Post-heelkunde (orbita,
traanklier, netvlies)
INFECTIES
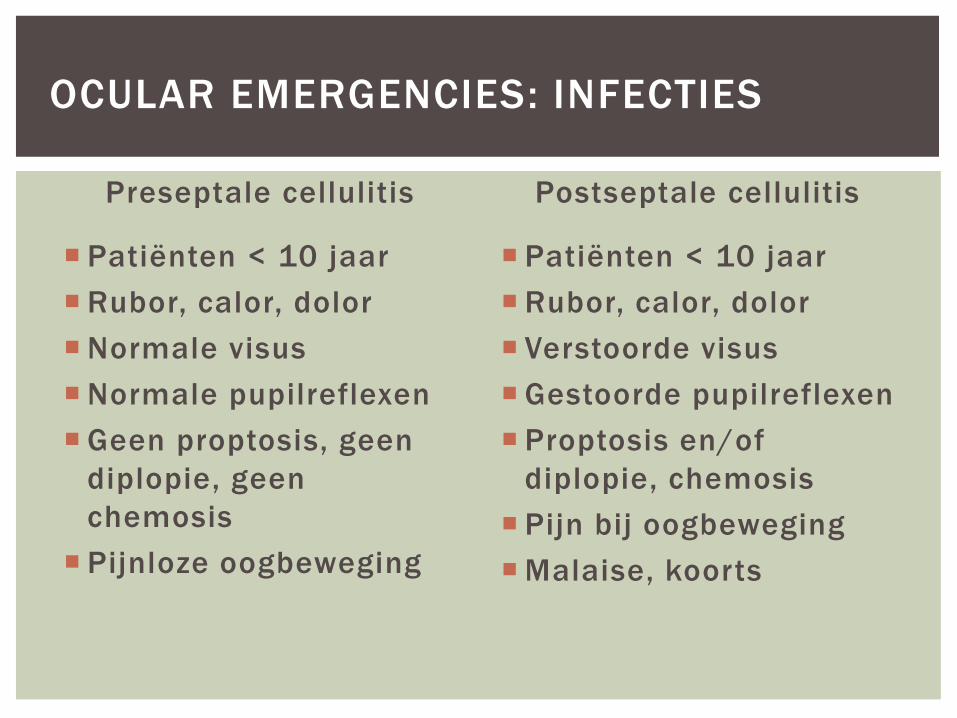
Preseptale cellulitis
Patiënten < 10 jaar
Rubor, calor, dolor
Normale visus
Normale pupilreflexen
Geen proptosis, geen
diplopie, geen
chemosis
Pijnloze oogbeweging
Postseptale cellulitis
Patiënten < 10 jaar
Rubor, calor, dolor
Verstoorde visus
Gestoorde pupilreflexen
Proptosis en/of
diplopie, chemosis
Pijn bij oogbeweging
Malaise, koorts
OCULAR EMERGENCIES: INFECTIES
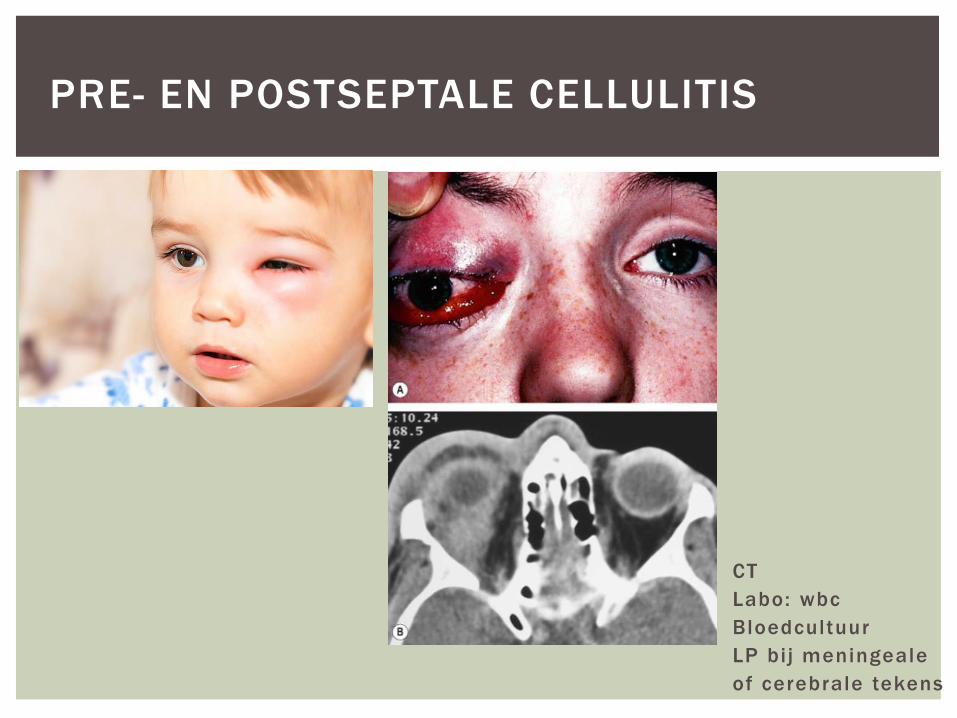
PRE- EN POSTSEPTALE CELLULITIS
CT
Labo: wbc
Bloedcultuur
LP bi j meningeale
of cerebrale tekens
PRE- EN POSTSEPTALE CELLULITIS
Indien niet ziek
- Kind: Amoxiclav 10mg/kg 2dd
- Volw: Amoxiclav 500mg 2dd
- Binnen 24 uur controle of talmo
Ziek of < 5 jaar
- Urgente consultatie of talmo
IV cef tazidime met p.o.
metronidazole (anaeroben)
Vancomycine bi j penicil l ine
al lergie
Urgente consultatie of talmo
Biopsie bi j atypische beeld
Heelkunde (sinus, orbita)
wanneer geen respons op AB,
subperiostaal of intracraniaal
abces

Meiboomklier cyste
Chronische steriele granulomateuze
inflammatoire lesie door obstructie
(vastgehouden talg)
Therapie: droge warmte en massage 2/dag,
Terracortril 3/dag
(cave herpes)
CHALAZION
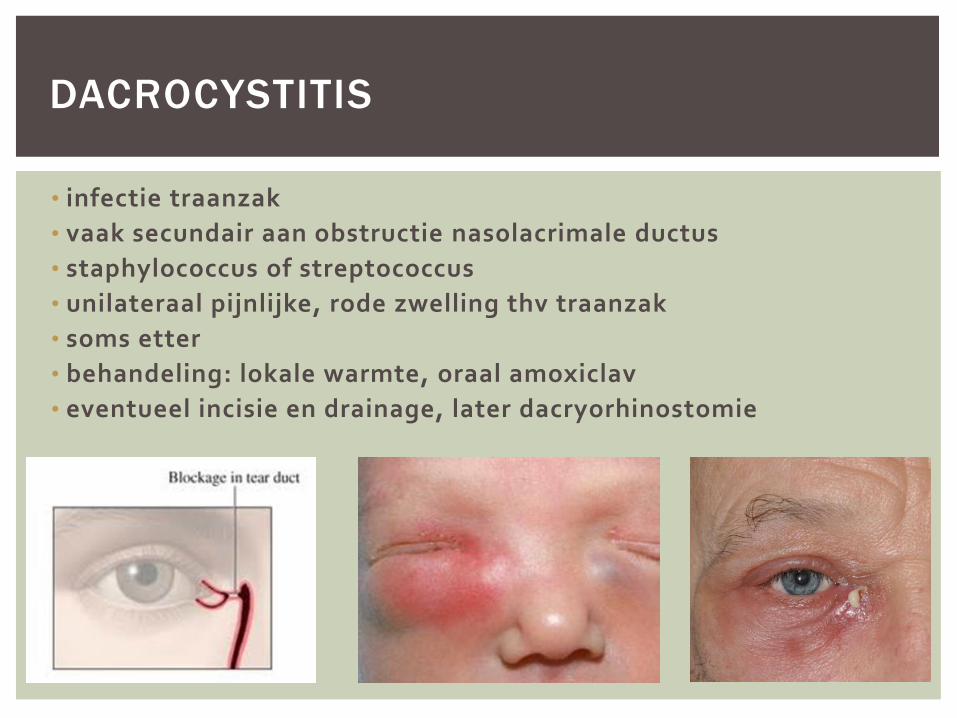
• infectie traanzak
• vaak secundair aan obstructie nasolacrimale ductus
• staphylococcus of streptococcus
• unilateraal pijnlijke, rode zwelling thv traanzak
• soms etter
• behandeling: lokale warmte, oraal amoxiclav
• eventueel incisie en drainage, later dacryorhinostomie
DACROCYSTITIS
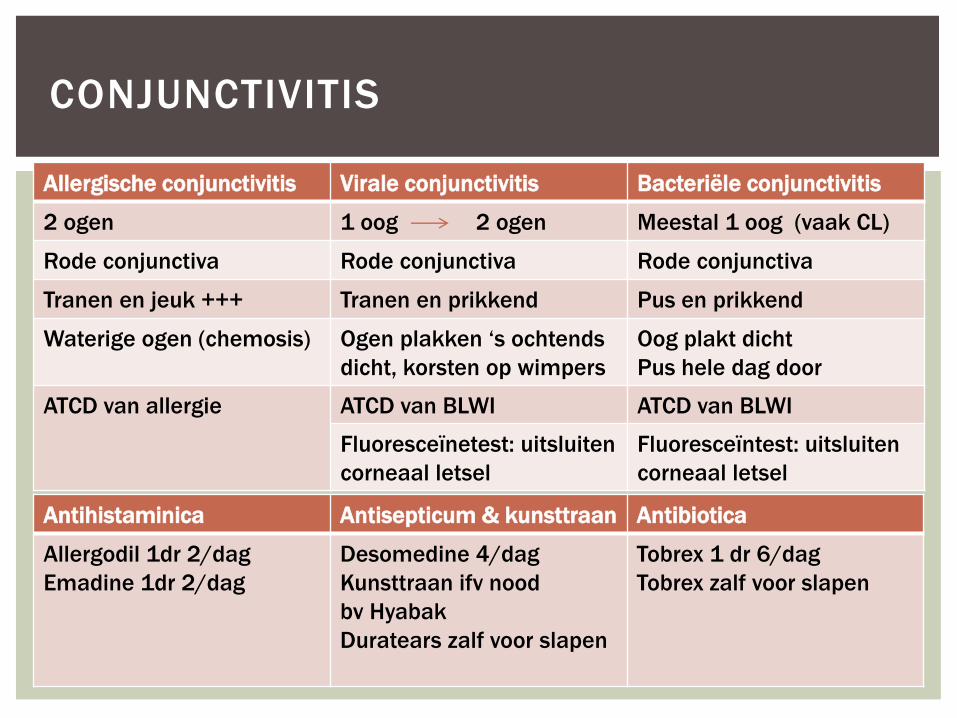
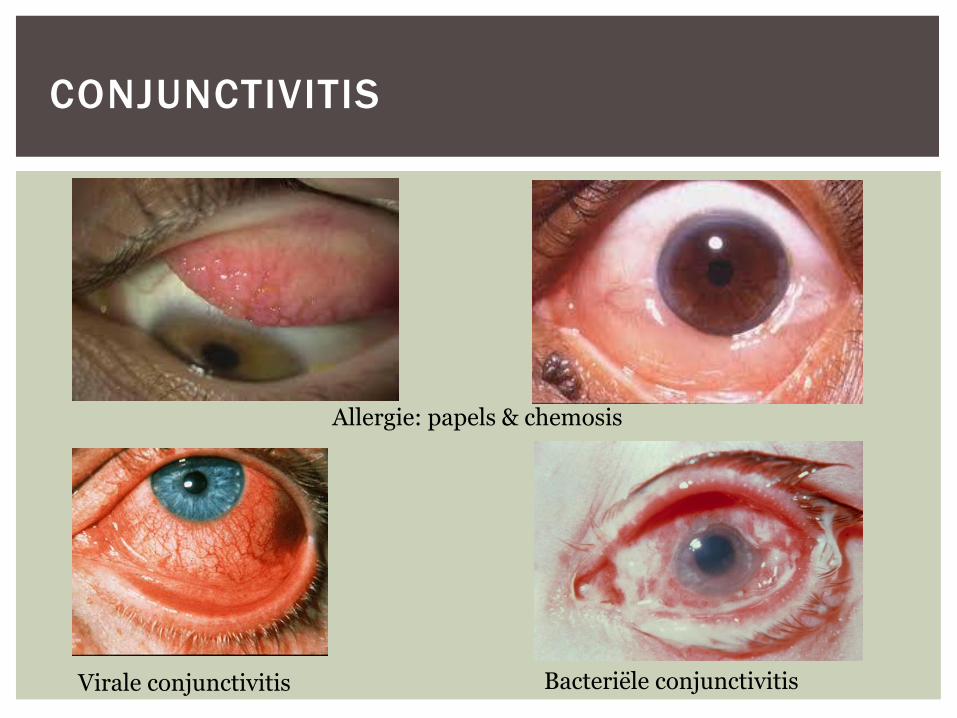
CONJUNCTIVITIS
Allergische conjunctivitis Virale conjunctivitis Bacteriële conjunctivitis
2 ogen 1 oog 2 ogen Meestal 1 oog (vaak CL)
Rode conjunctiva Rode conjunctiva Rode conjunctiva
Tranen en jeuk +++ Tranen en prikkend Pus en prikkend
Waterige ogen (chemosis) Ogen plakken ‘s ochtends
dicht, korsten op wimpers
Oog plakt dicht
Pus hele dag door
ATCD van allergie ATCD van BLWI ATCD van BLWI
Fluoresceïnetest: uitsluiten
corneaal letsel
Fluoresceïntest: uitsluiten
corneaal letsel
Antihistaminica Antisepticum & kunsttraan Antibiotica
Allergodil 1dr 2/dag
Emadine 1dr 2/dag
Desomedine 4/dag
Kunsttraan ifv nood
bv Hyabak
Duratears zalf voor slapen
Tobrex 1 dr 6/dag
Tobrex zalf voor slapen
CONJUNCTIVITIS
Allergie: papels & chemosis
Virale conjunctivitis Bacteriële conjunctivitis
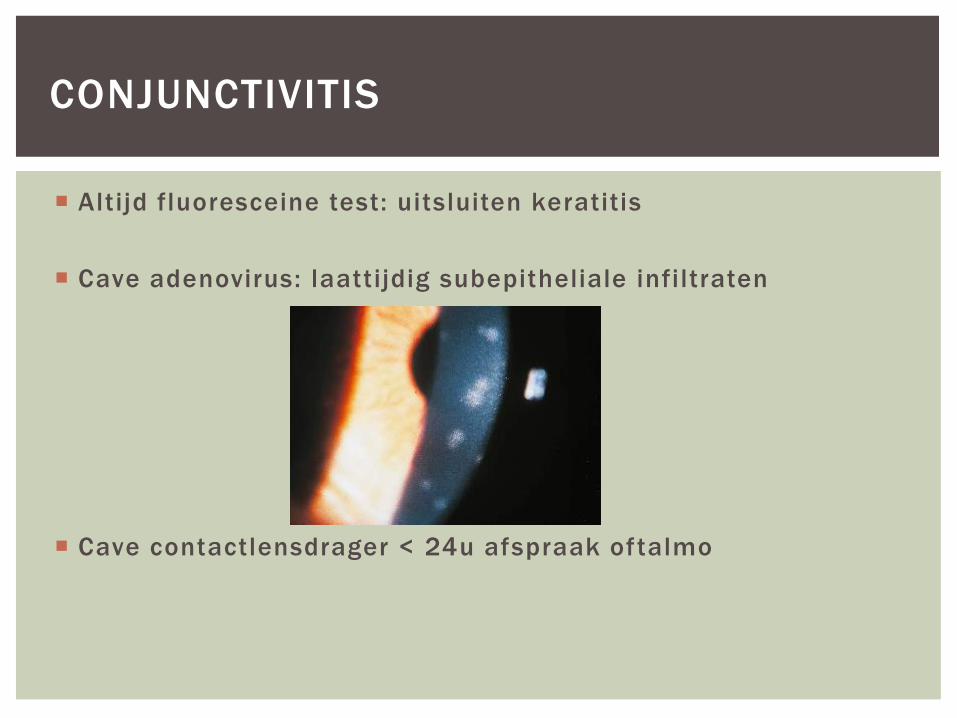
Altijd fluoresceine test: uitsluiten keratitis
Cave adenovirus: laattijdig subepitheliale infiltraten
Cave contactlensdrager < 24u afspraak oftalmo
CONJUNCTIVITIS
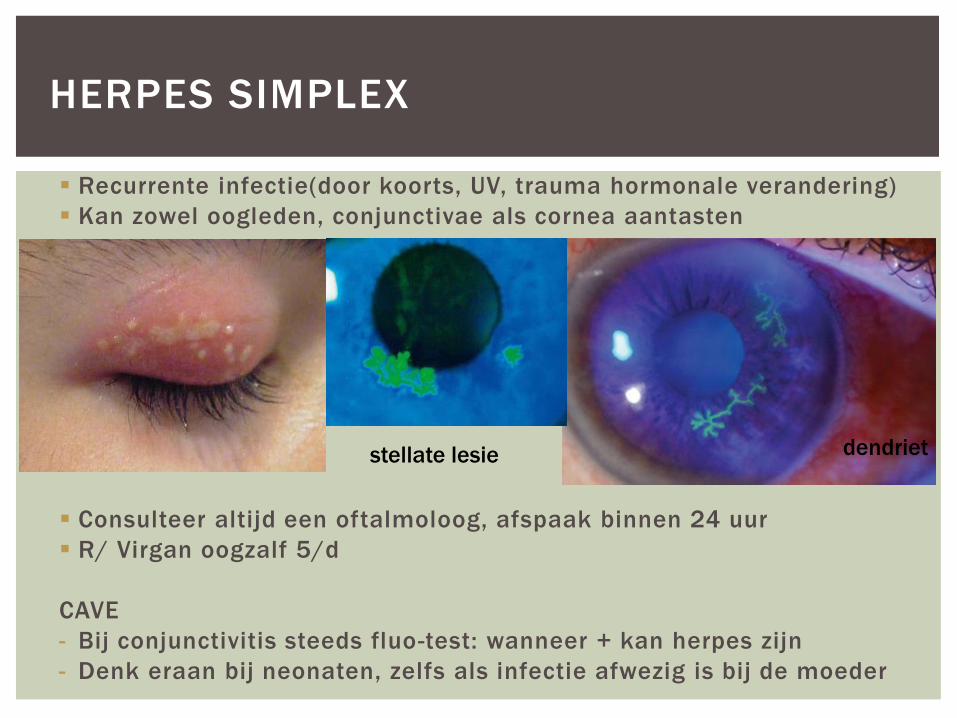
Recurrente infectie(door koorts, UV, trauma hormonale verandering)
Kan zowel oogleden, conjunctivae als cornea aantasten
Consulteer altijd een oftalmoloog, afspaak binnen 24 uur
R/ Virgan oogzalf 5/d
CAVE
- Bij conjunctivitis steeds fluo-test: wanneer + kan herpes zijn
- Denk eraan bij neonaten, zelfs als infectie afwezig is bij de moeder
HERPES SIMPLEX
dendriet stellate lesie
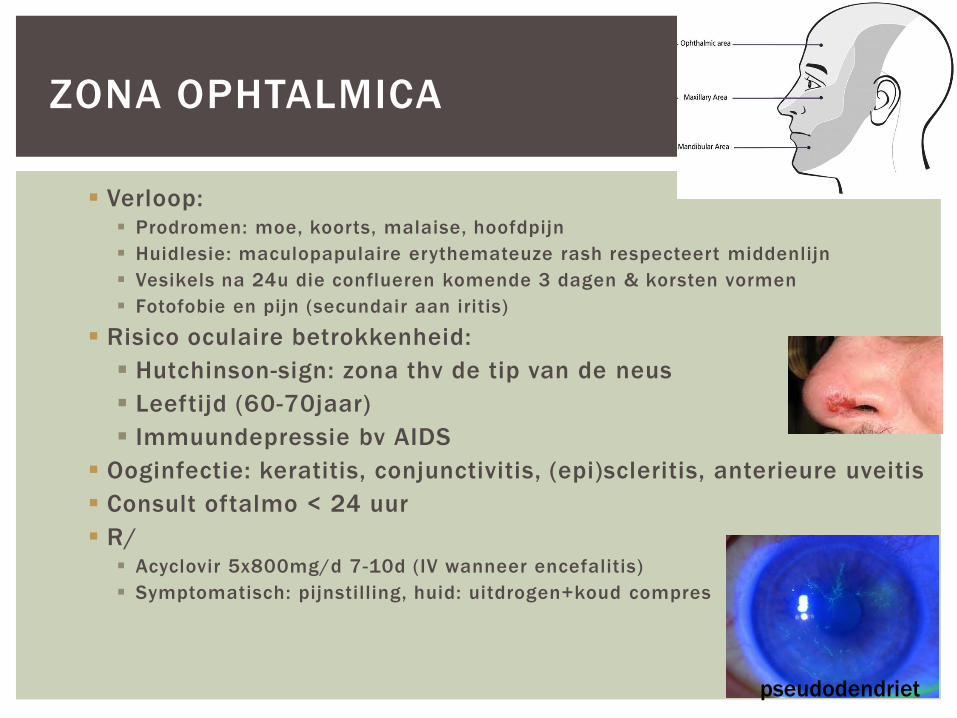
Verloop: Prodromen: moe, koorts, malaise, hoofdpijn
Huidlesie: maculopapulaire erythemateuze rash respecteert middenlijn
Vesikels na 24u die conflueren komende 3 dagen & korsten vormen
Fotofobie en pijn (secundair aan iritis)
Risico oculaire betrokkenheid:
Hutchinson-sign: zona thv de tip van de neus
Leeftijd (60-70jaar)
Immuundepressie bv AIDS
Ooginfectie: keratitis, conjunctivitis, (epi)scleritis, anterieure uveitis
Consult oftalmo < 24 uur
R/ Acyclovir 5x800mg/d 7-10d (IV wanneer encefalitis)
Symptomatisch: pijnstilling, huid: uitdrogen+koud compres
ZONA OPHTALMICA
pseudodendriet
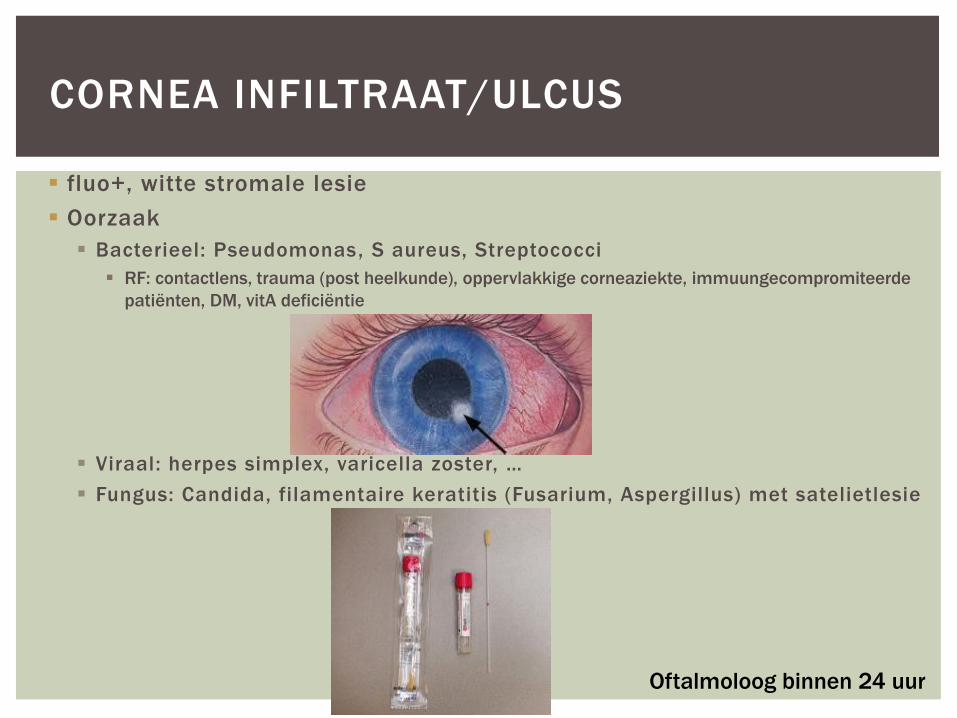
fluo+, witte stromale lesie
Oorzaak
Bacterieel: Pseudomonas, S aureus, Streptococci
RF: contactlens, trauma (post heelkunde), oppervlakkige corneaziekte, immuungecompromiteerde
patiënten, DM, vitA deficiëntie
Viraal: herpes simplex, varicella zoster, …
Fungus: Candida, filamentaire keratitis (Fusarium, Aspergillus) met satelietlesie
CORNEA INFILTRAAT/ULCUS
Oftalmoloog binnen 24 uur
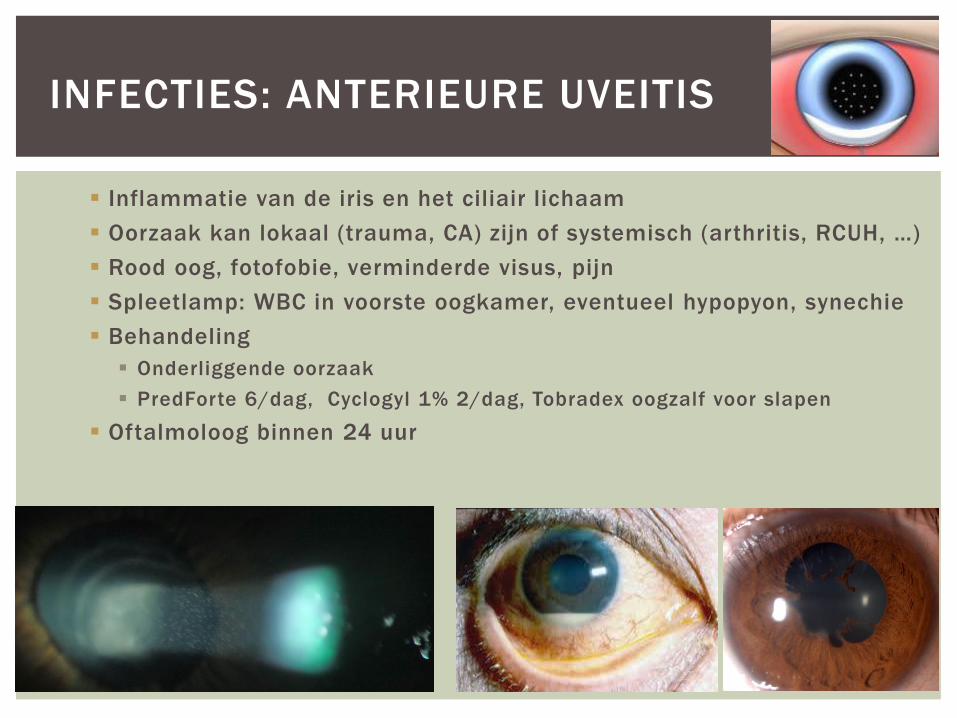
Inflammatie van de iris en het ciliair lichaam
Oorzaak kan lokaal (trauma, CA) zijn of systemisch (arthritis, RCUH, …)
Rood oog, fotofobie, verminderde visus, pijn
Spleetlamp: WBC in voorste oogkamer, eventueel hypopyon, synechie
Behandeling
Onderliggende oorzaak
PredForte 6/dag, Cyclogyl 1% 2/dag, Tobradex oogzalf voor slapen
Oftalmoloog binnen 24 uur
INFECTIES: ANTERIEURE UVEITIS
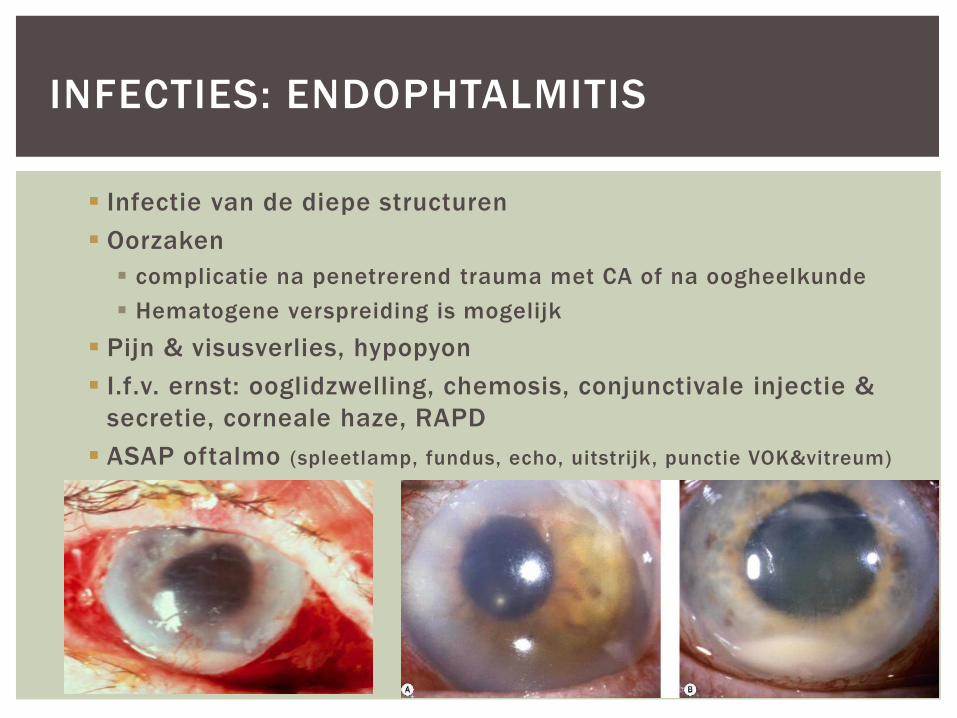
Infectie van de diepe structuren
Oorzaken
complicatie na penetrerend trauma met CA of na oogheelkunde
Hematogene verspreiding is mogelijk
Pijn & visusverlies, hypopyon
I.f.v. ernst: ooglidzwelling, chemosis, conjunctivale injectie &
secretie, corneale haze, RAPD
ASAP oftalmo (spleetlamp, fundus, echo, uitstrijk, punctie VOK&vitreum)
INFECTIES: ENDOPHTALMITIS
Infecties
Trauma
Subconjunctivale bloeding
Corneale abrasie
UV-keratitis
Vreemde lichamen
Chemische verwondingen/lijm
Laceraties van het ooglid
Stomp trauma
Hyphema
Blow-out fracturen
Penetrerend trauma
Visusdaling of –verlies
OCULAR EMERGENCIES
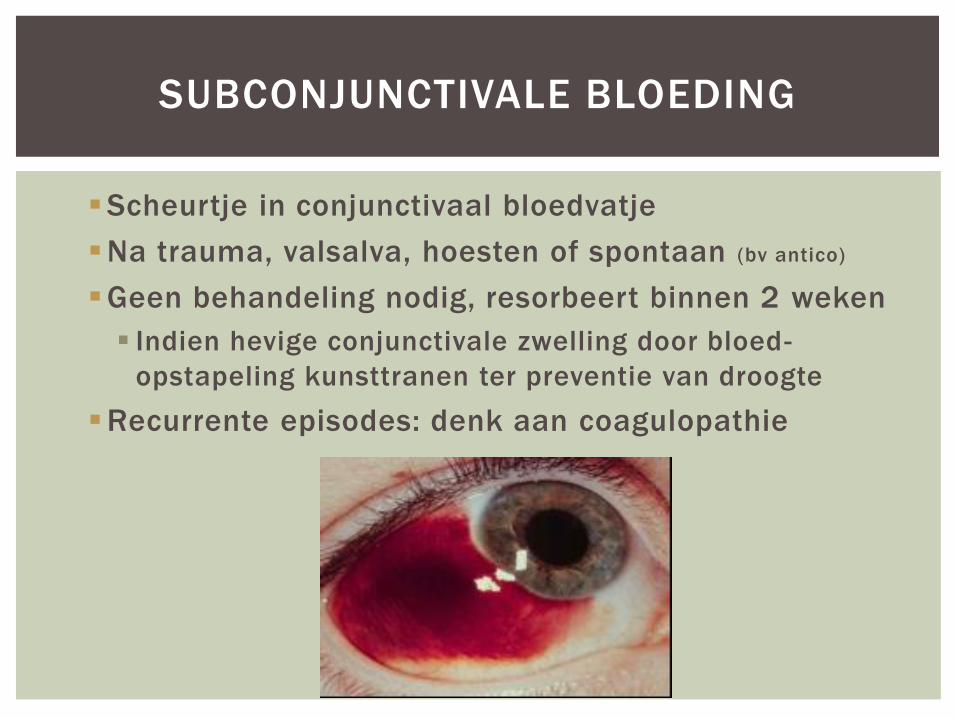
Scheurtje in conjunctivaal bloedvatje
Na trauma, valsalva, hoesten of spontaan (bv antico)
Geen behandeling nodig, resorbeert binnen 2 weken
Indien hevige conjunctivale zwelling door bloed-
opstapeling kunsttranen ter preventie van droogte
Recurrente episodes: denk aan coagulopathie
SUBCONJUNCTIVALE BLOEDING

Oppervlakkig epitheliaal defect
Tranen, fotofobie, zandkorrelgevoel
Onderzoek: verdoving (oxybuprocaine) + fluoresceine
Zoek naar vreemd voorwerp, everteer bovenste ooglid
CORNEALE EROSIE
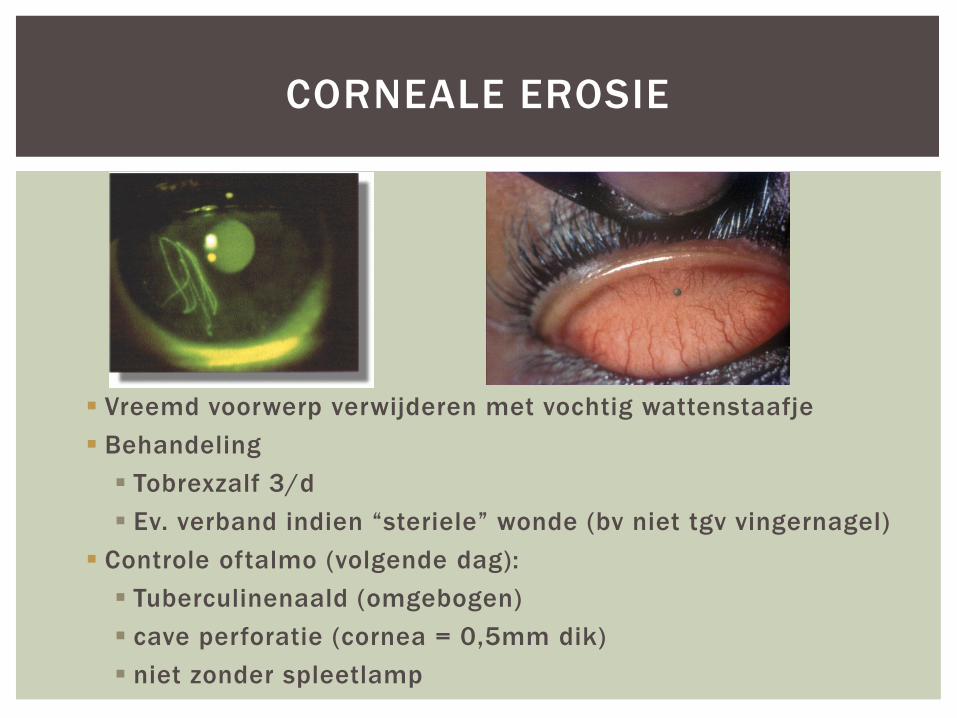
Vreemd voorwerp verwijderen met vochtig wattenstaafje
Behandeling
Tobrexzalf 3/d
Ev. verband indien “steriele” wonde (bv niet tgv vingernagel)
Controle oftalmo (volgende dag):
Tuberculinenaald (omgebogen)
cave perforatie (cornea = 0,5mm dik)
niet zonder spleetlamp
CORNEALE EROSIE
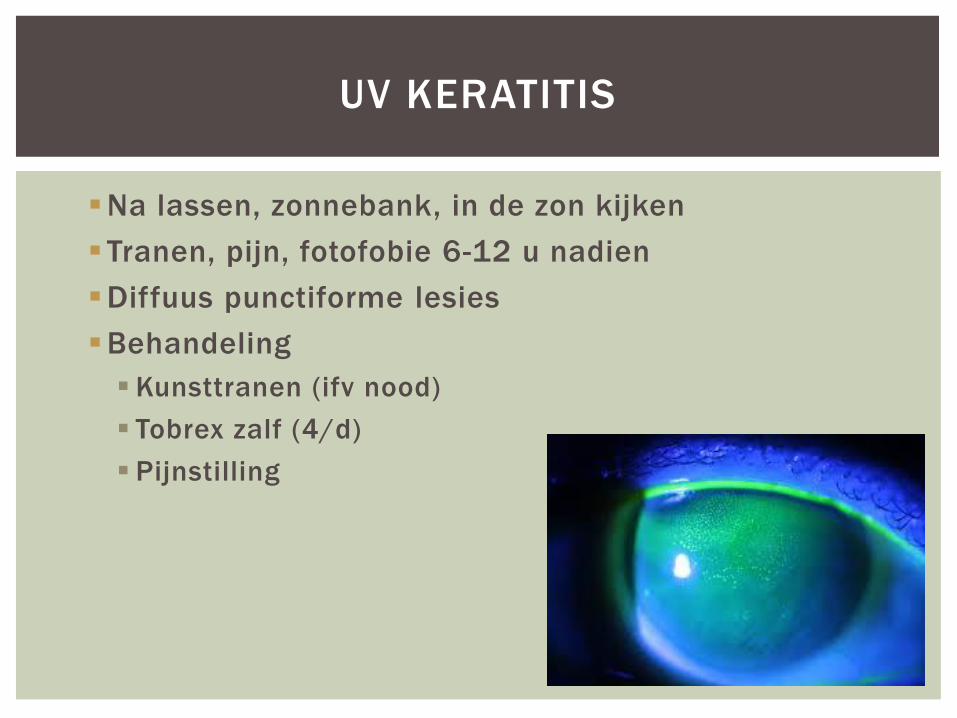
Na lassen, zonnebank, in de zon kijken
Tranen, pijn, fotofobie 6-12 u nadien
Diffuus punctiforme lesies
Behandeling
Kunsttranen (ifv nood)
Tobrex zalf (4/d)
Pijnstilling
UV KERATITIS
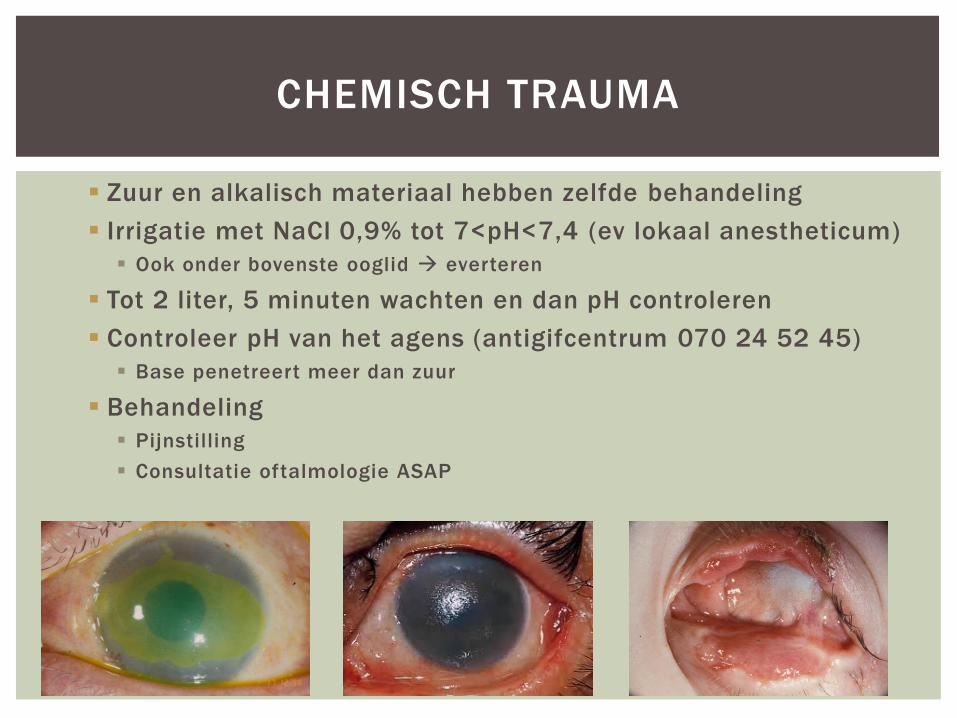
Zuur en alkalisch materiaal hebben zelfde behandeling
Irrigatie met NaCl 0,9% tot 7<pH<7,4 (ev lokaal anestheticum)
Ook onder bovenste ooglid everteren
Tot 2 liter, 5 minuten wachten en dan pH controleren
Controleer pH van het agens (antigifcentrum 070 24 52 45)
Base penetreert meer dan zuur
Behandeling
Pijnstilling
Consultatie oftalmologie ASAP
CHEMISCH TRAUMA
Corneale abrasie door hard geworden deeltjes
Verwijderen deeltjes
Erythromycine 0,5% 5/dag
Follow-up binnen 24 uur
Zelden zware problemen
SUPERLIJM EXPOSURE
Doorverwijzing oftalmo indien
Rand van ooglid betrokken
Tarsale plaat of m.levator palpebrae
< 6-8 mm van de mediale ooghoek
Traanbuis betrokken
Behandeling in afwachting heelkunde
Cephalosporine 500 mg PO 4/dag
Erythromycine 2% oogdruppels 4/dag
koude compressen
OOGLID LACERATIE

Kleine voorwerpen komen op oog zelf terecht
Cave perforatie (vb. BB gun, steenslag bij slijpen)
Geen MRI wanneer mogelijks metalen vreemd voorwerp
Grote voorwerpen worden tegengehouden door
orbitae
Controleer op fracturen
STOMP TRAUMA
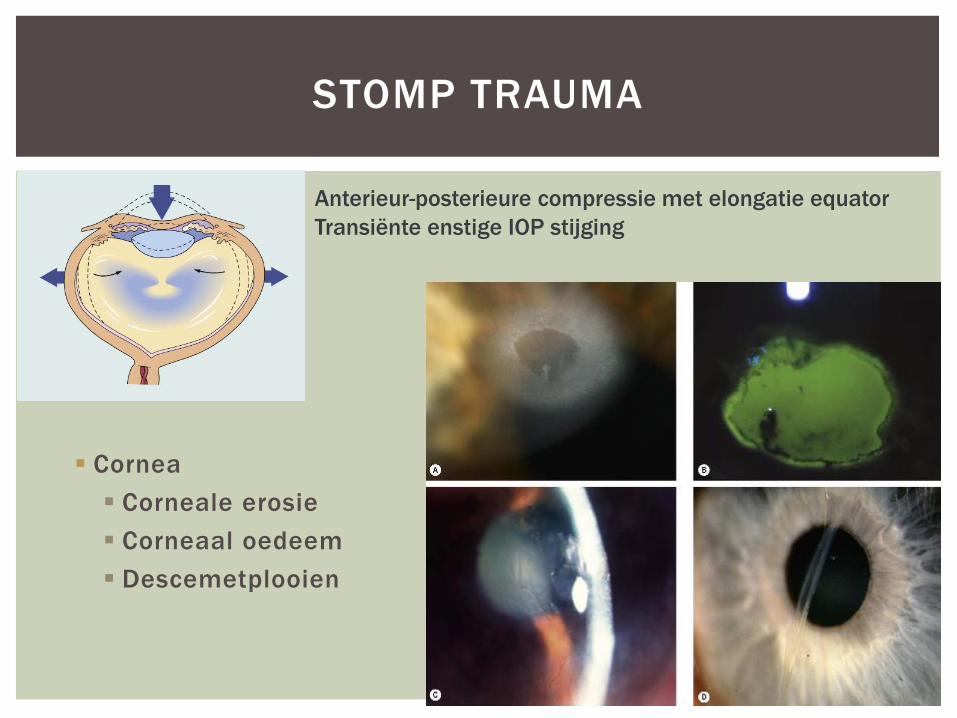
Cornea
Corneale erosie
Corneaal oedeem
Descemetplooien
STOMP TRAUMA
Anterieur-posterieure compressie met elongatie equator
Transiënte enstige IOP stijging
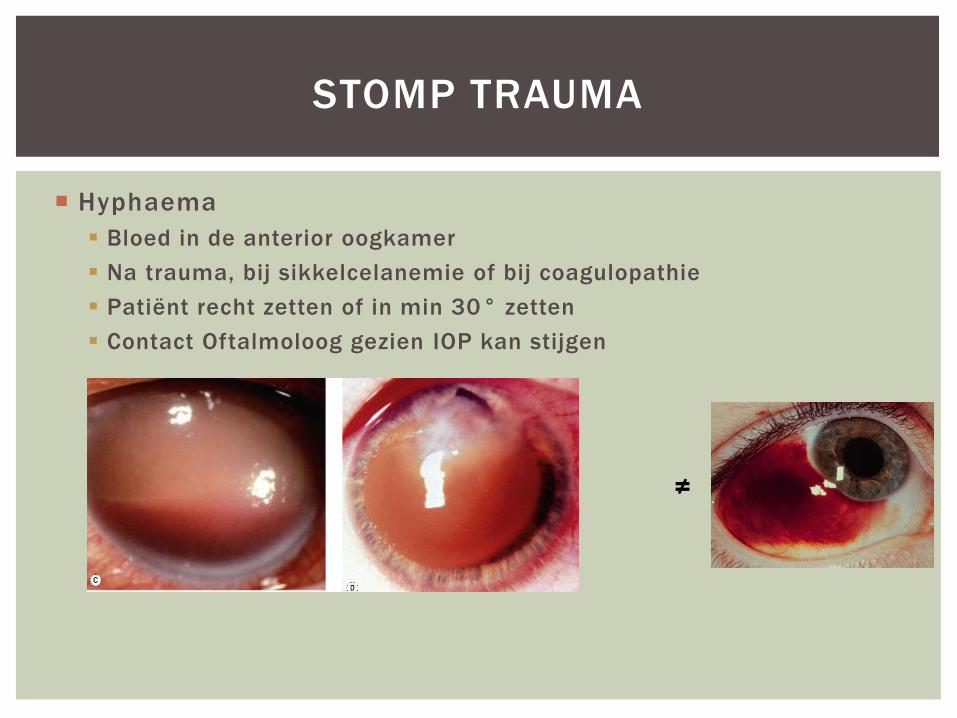
Hyphaema
Bloed in de anterior oogkamer
Na trauma, bij sikkelcelanemie of bij coagulopathie
Patiënt recht zetten of in min 30° zetten
Contact Oftalmoloog gezien IOP kan stijgen
STOMP TRAUMA
≠
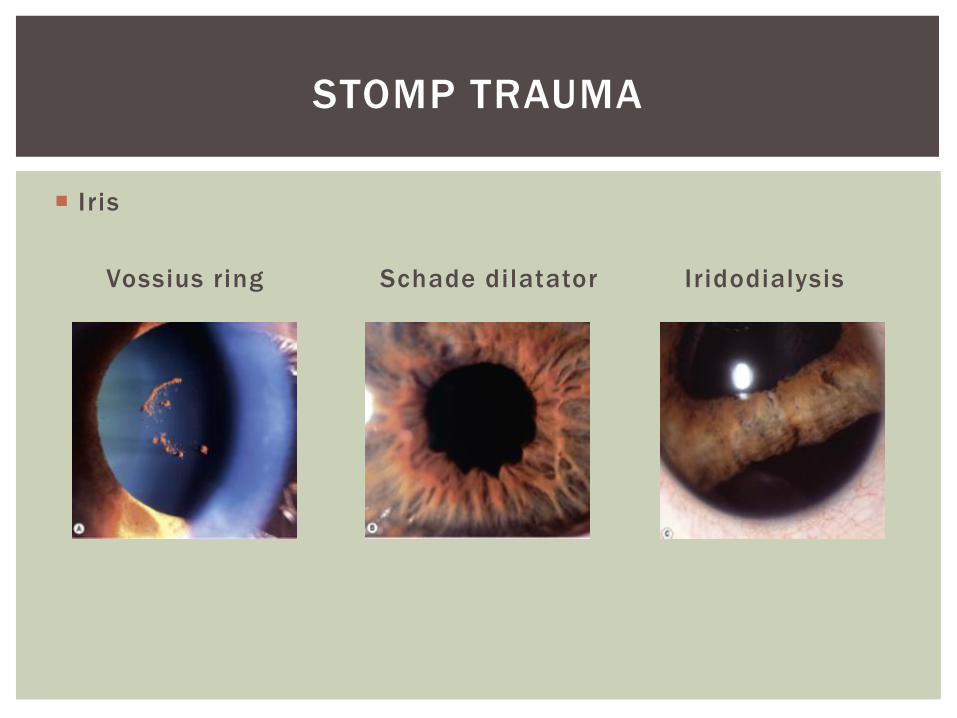
Iris
Vossius ring Schade dilatator Iridodialysis
STOMP TRAUMA
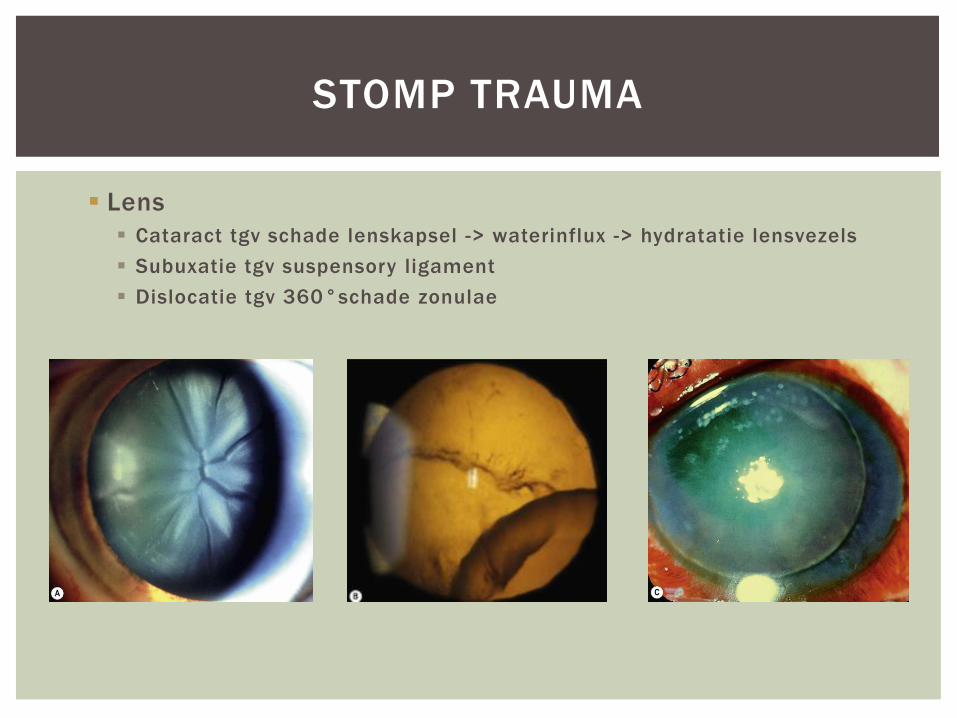
Lens
Cataract tgv schade lenskapsel -> waterinflux -> hydratatie lensvezels
Subuxatie tgv suspensory ligament
Dislocatie tgv 360°schade zonulae
STOMP TRAUMA
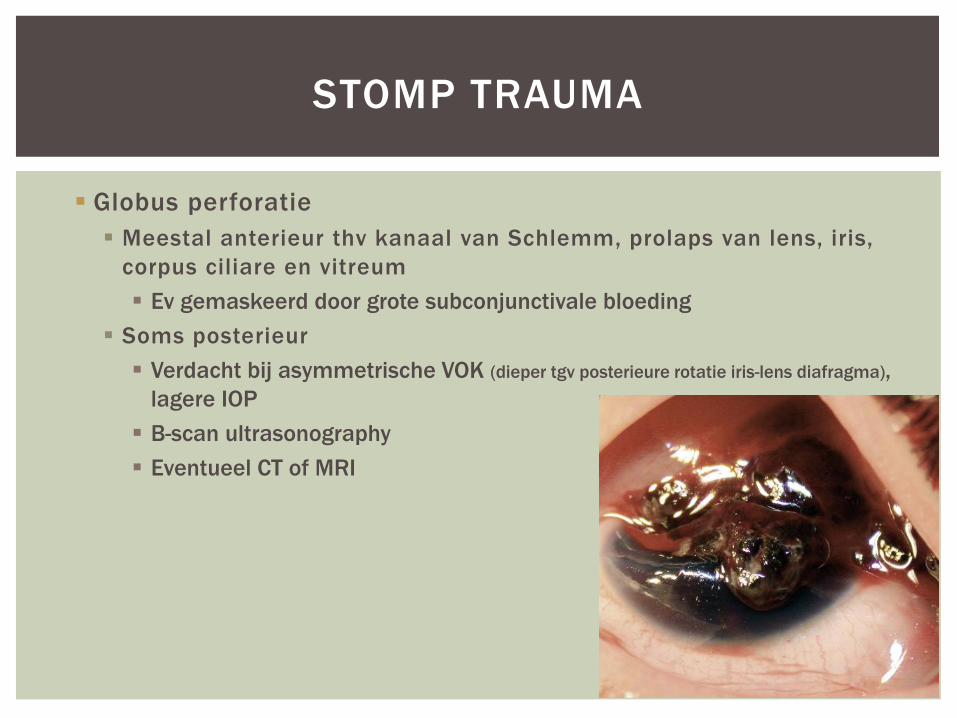
Globus perforatie
Meestal anterieur thv kanaal van Schlemm, prolaps van lens, iris,
corpus ciliare en vitreum
Ev gemaskeerd door grote subconjunctivale bloeding
Soms posterieur
Verdacht bij asymmetrische VOK (dieper tgv posterieure rotatie iris-lens diafragma),
lagere IOP
B-scan ultrasonography
Eventueel CT of MRI
STOMP TRAUMA

Seidel positief = wanneer er met fluo wordt
gekeken zie je dat er water van in het oog
naar buiten komt waardoor er een groen
waterval veroorzaakt wordt
STOMP TRAUMA
Nauwe voorste oogkamer: afstand tussen 2
lichtbundels is klein tgv verlies van vocht
door de perforatie
Bij vermoeden: stop verder onderzoek, plaats oogschelp
ASAP oftalmoloog
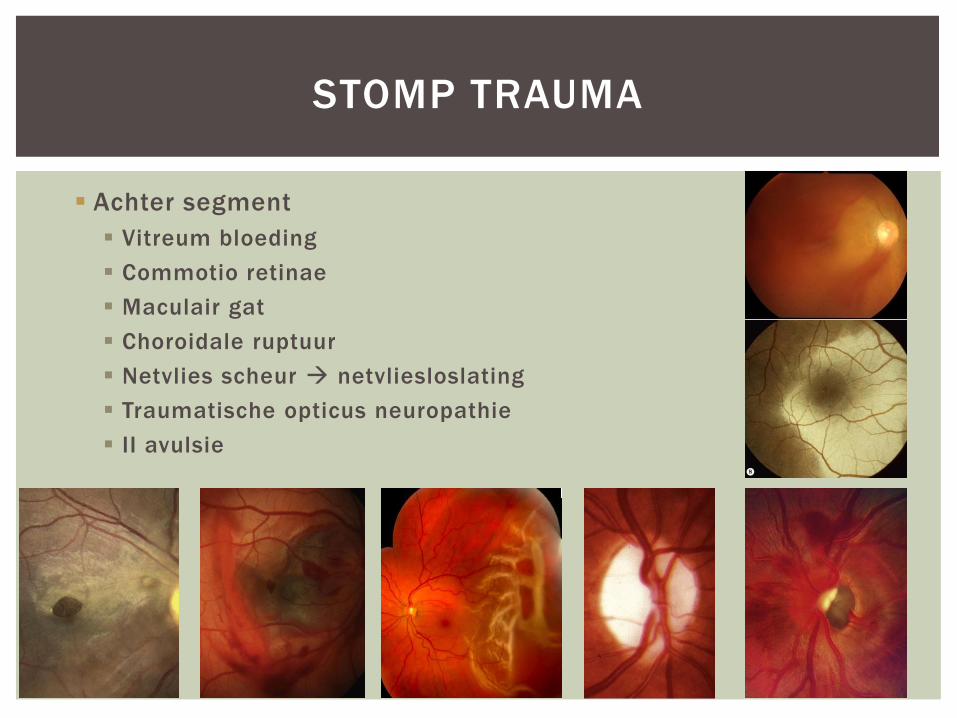
Achter segment
Vitreum bloeding
Commotio retinae
Maculair gat
Choroidale ruptuur
Netvlies scheur netvliesloslating
Traumatische opticus neuropathie
II avulsie
STOMP TRAUMA
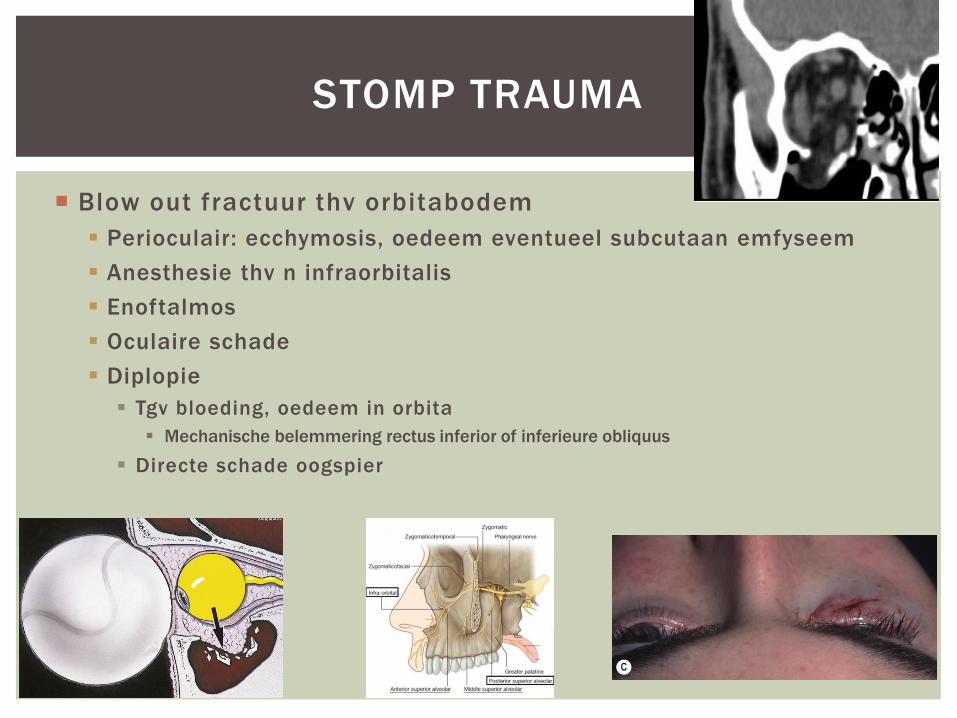
Blow out fractuur thv orbitabodem
Perioculair: ecchymosis, oedeem eventueel subcutaan emfyseem
Anesthesie thv n infraorbitalis
Enoftalmos
Oculaire schade
Diplopie
Tgv bloeding, oedeem in orbita
Mechanische belemmering rectus inferior of inferieure obliquus
Directe schade oogspier
STOMP TRAUMA
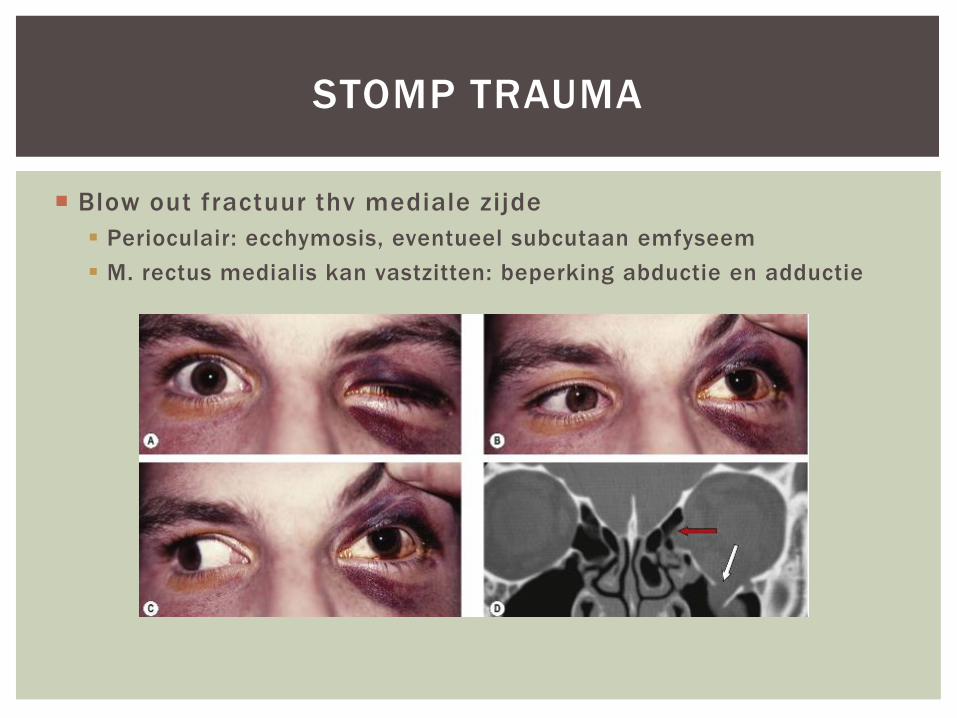
Blow out fractuur thv mediale zijde
Perioculair: ecchymosis, eventueel subcutaan emfyseem
M. rectus medialis kan vastzitten: beperking abductie en adductie
STOMP TRAUMA
STOMP TRAUMA
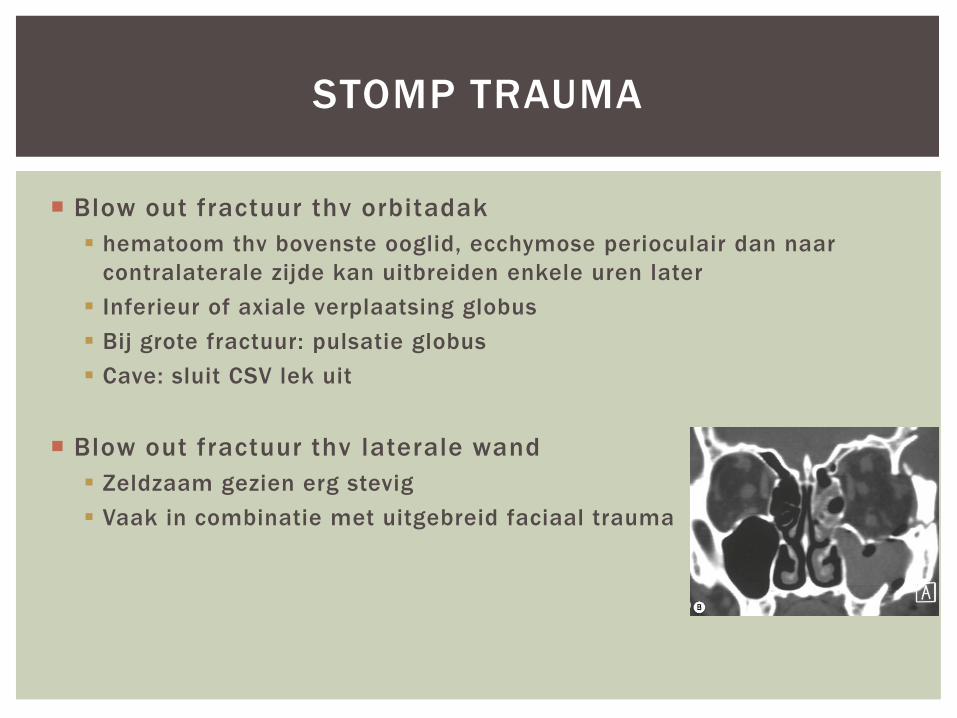
Blow out fractuur thv orbitadak
hematoom thv bovenste ooglid, ecchymose perioculair dan naar
contralaterale zijde kan uitbreiden enkele uren later
Inferieur of axiale verplaatsing globus
Bij grote fractuur: pulsatie globus
Cave: sluit CSV lek uit
Blow out fractuur thv laterale wand
Zeldzaam gezien erg stevig
Vaak in combinatie met uitgebreid faciaal trauma
Onderzoek
Visus
Motiliteit
Pupilreflex
CT (controleer spieren + n.opticus)
Cave: hoge incidentie geassocieerd trauma aan oogbol
Behandeling
Cfr oftalmo/mka
Antibiotica profylaxe igv sinustrauma
Snuitverbod
Hoge dosis cortisone bij schade oogzenuw
BLOW OUT FRACTUUR
Oorzaken :
Trauma
Iatrogeen : repositie peri-orbitaal fractuur, endoscopische sinuschirurgie, thrombolysis, ooglidchirurgie
Bloedende tumor
Pathofysiologie :
Bloeding in de orbitale ruimte
Verminderde veneuse outflow
Verhoogde intraoculaire druk
Verminderde perfusie druk: ischemie II en netvlies
RETROBULBAIRE BLOEDING
Klachten :
Pijn, diplopie, rood gezwollen oog, verminderde visus/blindheid
Oogleden zijn heel stram en moeilijk te openen
Pupilreflex : RAPD en mydriasis
Oogmotiliteit : oftalmoplegie
Proptosis
Spleetlamponderzoek :
Chemosis
Subconjunctivale bloeding
RETROBULBAIRE BLOEDING
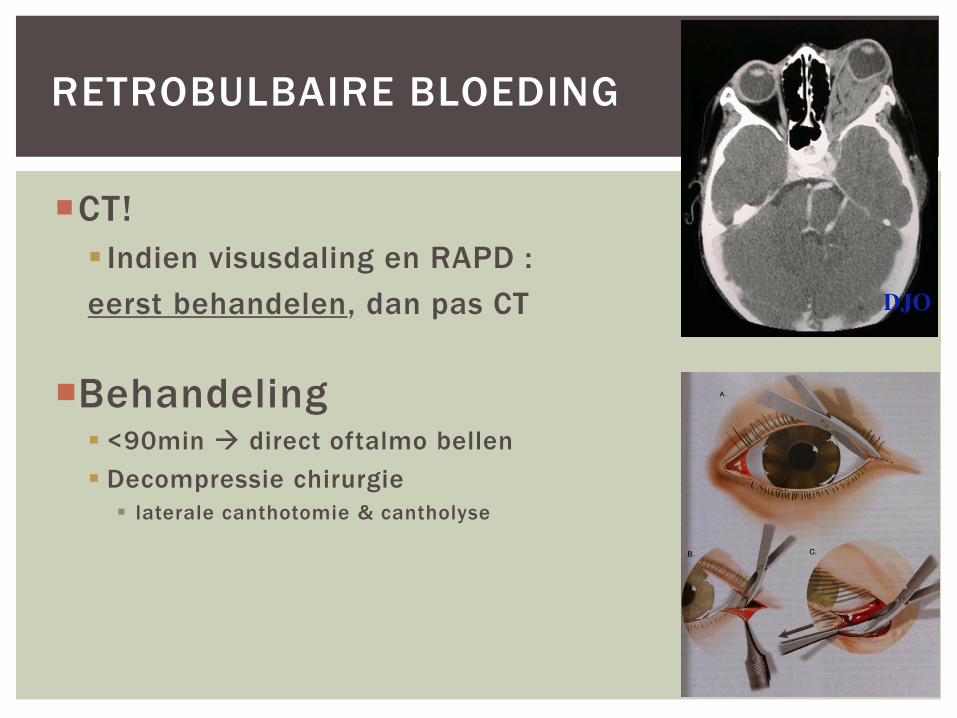
CT!
Indien visusdaling en RAPD :
eerst behandelen, dan pas CT
Behandeling
<90min direct oftalmo bellen
Decompressie chirurgie
laterale canthotomie & cantholyse
RETROBULBAIRE BLOEDING
Infecties
Trauma
Visusdaling of –verlies
Acuut gesloten hoekglaucoom
Opticus neuritis
Occlusie van de a. centralis retinae
Occlusie van de v. centralis retinae
Retinaloslating en floaters
Arteritis temporalis
OCULAR EMERGENCIES
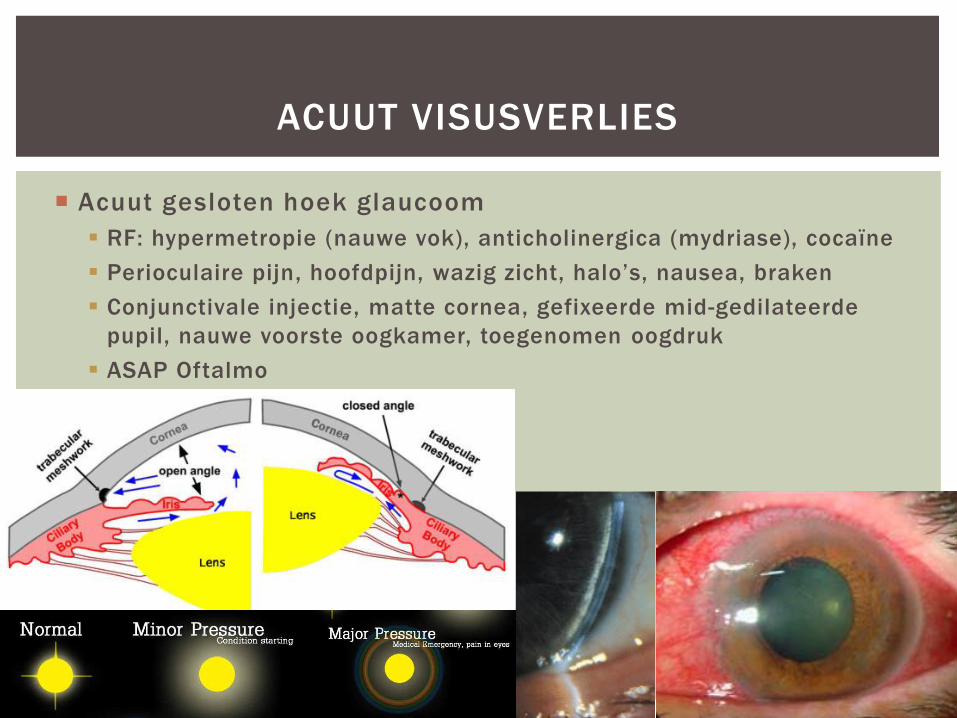
Acuut gesloten hoek glaucoom
RF: hypermetropie (nauwe vok), anticholinergica (mydriase), cocaïne
Perioculaire pijn, hoofdpijn, wazig zicht, halo’s, nausea, braken
Conjunctivale injectie, matte cornea, gefixeerde mid-gedilateerde
pupil, nauwe voorste oogkamer, toegenomen oogdruk
ASAP Oftalmo
ACUUT VISUSVERLIES
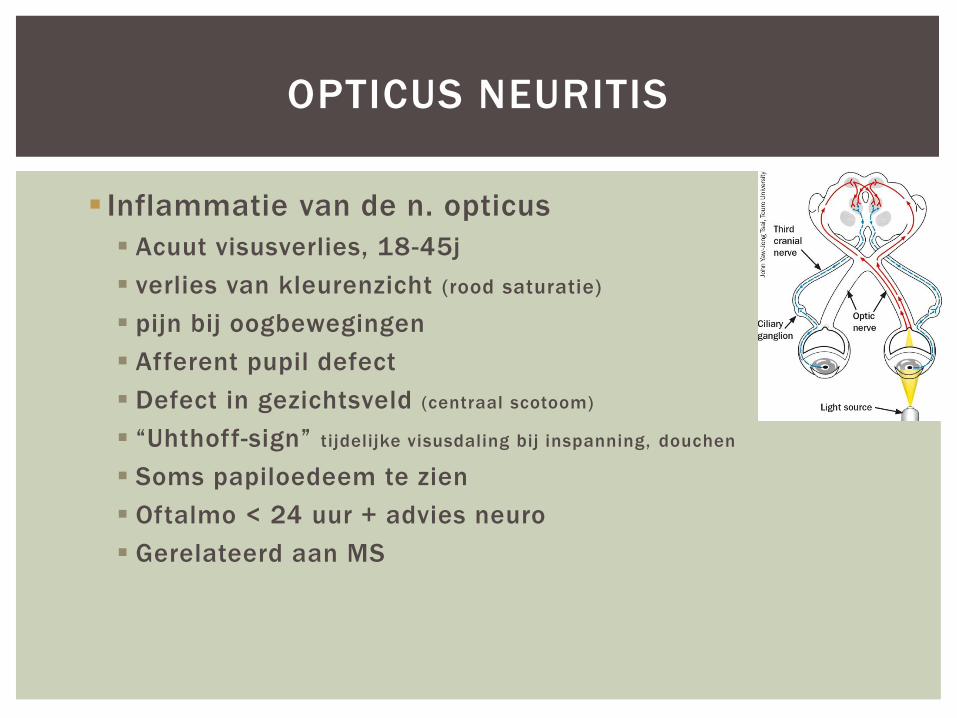
Inflammatie van de n. opticus
Acuut visusverlies, 18-45j
verlies van kleurenzicht (rood saturatie)
pijn bij oogbewegingen
Afferent pupil defect
Defect in gezichtsveld (centraal scotoom)
“Uhthoff-sign” tijdelijke visusdaling bij inspanning, douchen
Soms papiloedeem te zien
Oftalmo < 24 uur + advies neuro
Gerelateerd aan MS
OPTICUS NEURITIS
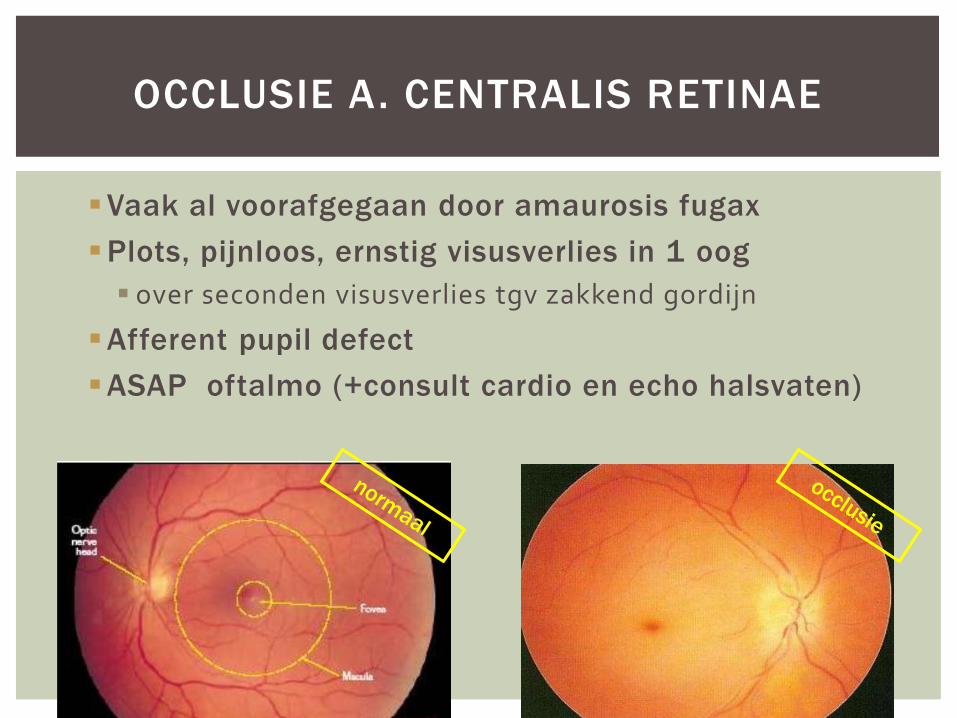
Vaak al voorafgegaan door amaurosis fugax
Plots, pijnloos, ernstig visusverlies in 1 oog
over seconden visusverlies tgv zakkend gordijn
Afferent pupil defect
ASAP oftalmo (+consult cardio en echo halsvaten)
OCCLUSIE A. CENTRALIS RETINAE
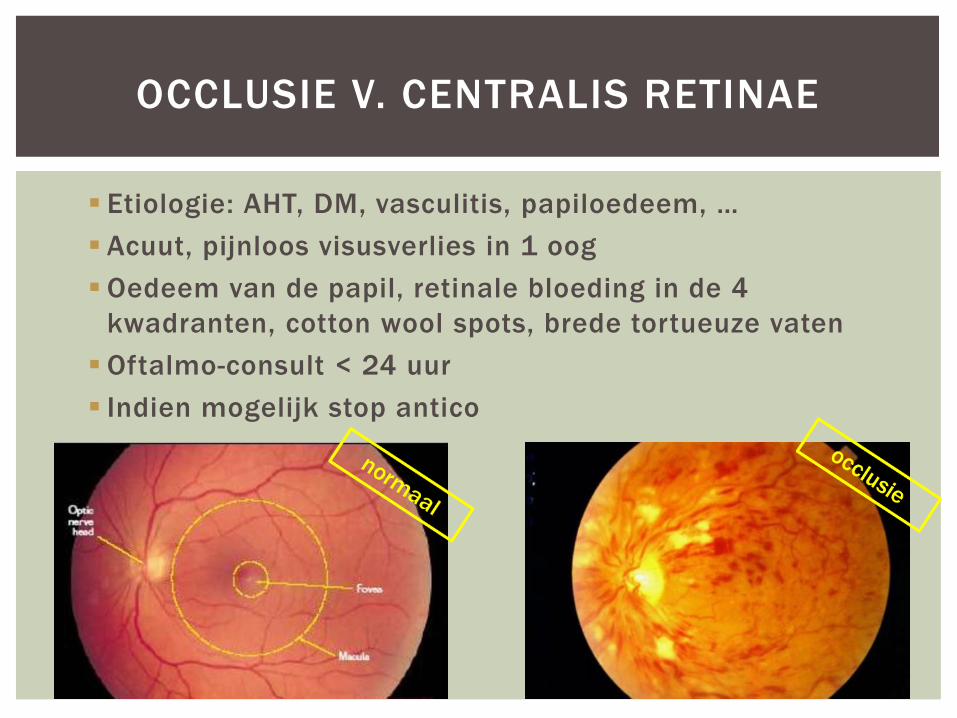
Etiologie: AHT, DM, vasculitis, papiloedeem, …
Acuut, pijnloos visusverlies in 1 oog
Oedeem van de papil, retinale bloeding in de 4
kwadranten, cotton wool spots, brede tortueuze vaten
Oftalmo-consult < 24 uur
Indien mogelijk stop antico
OCCLUSIE V. CENTRALIS RETINAE
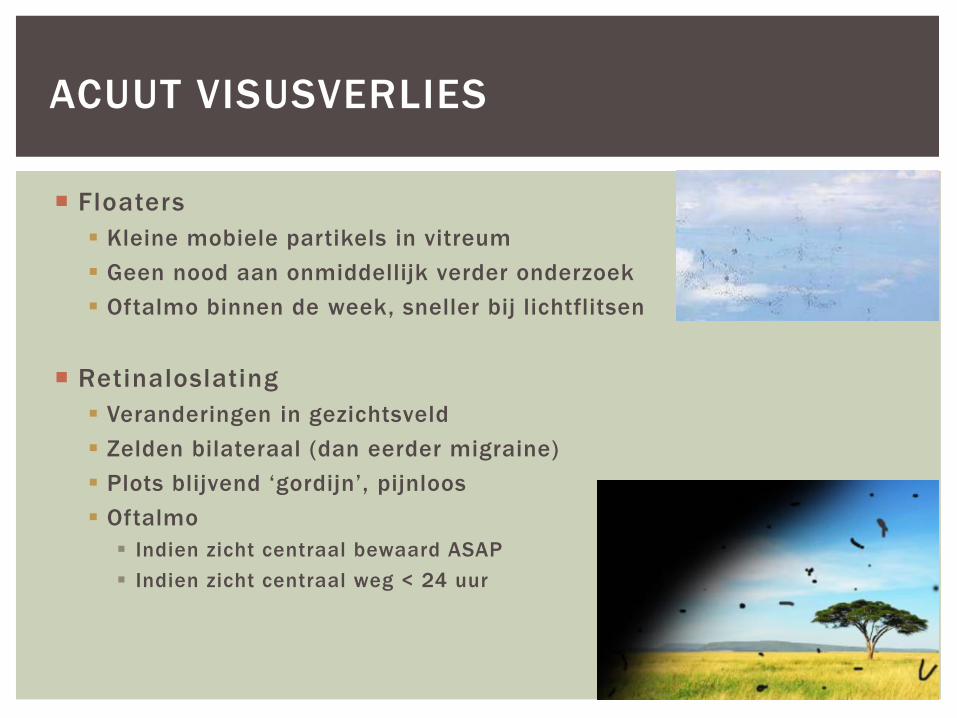
Floaters
Kleine mobiele partikels in vitreum
Geen nood aan onmiddellijk verder onderzoek
Oftalmo binnen de week, sneller bij lichtflitsen
Retinaloslating
Veranderingen in gezichtsveld
Zelden bilateraal (dan eerder migraine)
Plots blijvend ‘gordijn’, pijnloos
Oftalmo
Indien zicht centraal bewaard ASAP
Indien zicht centraal weg < 24 uur
ACUUT VISUSVERLIES
Pijnloze, ischemische opticus neuropathie
Vrouwen > 50 jaar met ATCD van polymyalgia
Visusveranderingen, hoofdpijn, kaakclaudicatio, pijn thv a.
temporalis, moeheid, koorts, keelpijn, anorexie
BS bepalen, biopsie binnen de 10 dagen
Advies oftalmo
Behandeling
Indien sterk vermoeden:
opname met IV methylprednisolone 250 mg IV elke 6 uur
Indien minder sterk vermoeden:
ontslag met prednisone 80-100 mg po /dag, met strikte follow up
ARTERITIS TEMPORALIS





![Weefsel regeneratie met RGTA® technologie - cdn3.cacipliq.nlcdn3.cacipliq.nl/uploads/Editor/cacipliqbrochure[nl].pdf · 4 Ulcus Cruris 4 Radiologische wonden ... RGTA technologie](https://static.fdocuments.nl/doc/165x107/5cedaef488c99396038cbe1e/weefsel-regeneratie-met-rgta-technologie-cdn3-nlpdf-4-ulcus-cruris-4.jpg)