UZ Antwerpen Universiteit Antwerpen - BeSEDiM · UZ Antwerpen Universiteit Antwerpen TRIADE VAN ACS...
27
1 Acute coronaire syndromen Prof dr M Claeys UZ Antwerpen Universiteit Antwerpen TRIADE VAN ACS Anamnese Cardiac enzymes Surface ECG
Transcript of UZ Antwerpen Universiteit Antwerpen - BeSEDiM · UZ Antwerpen Universiteit Antwerpen TRIADE VAN ACS...
1
Acute coronaire syndromen
Prof dr M ClaeysUZ Antwerpen
Universiteit Antwerpen
TRIADE VAN ACS
AnamneseCardiac enzymes
Surface ECG
2
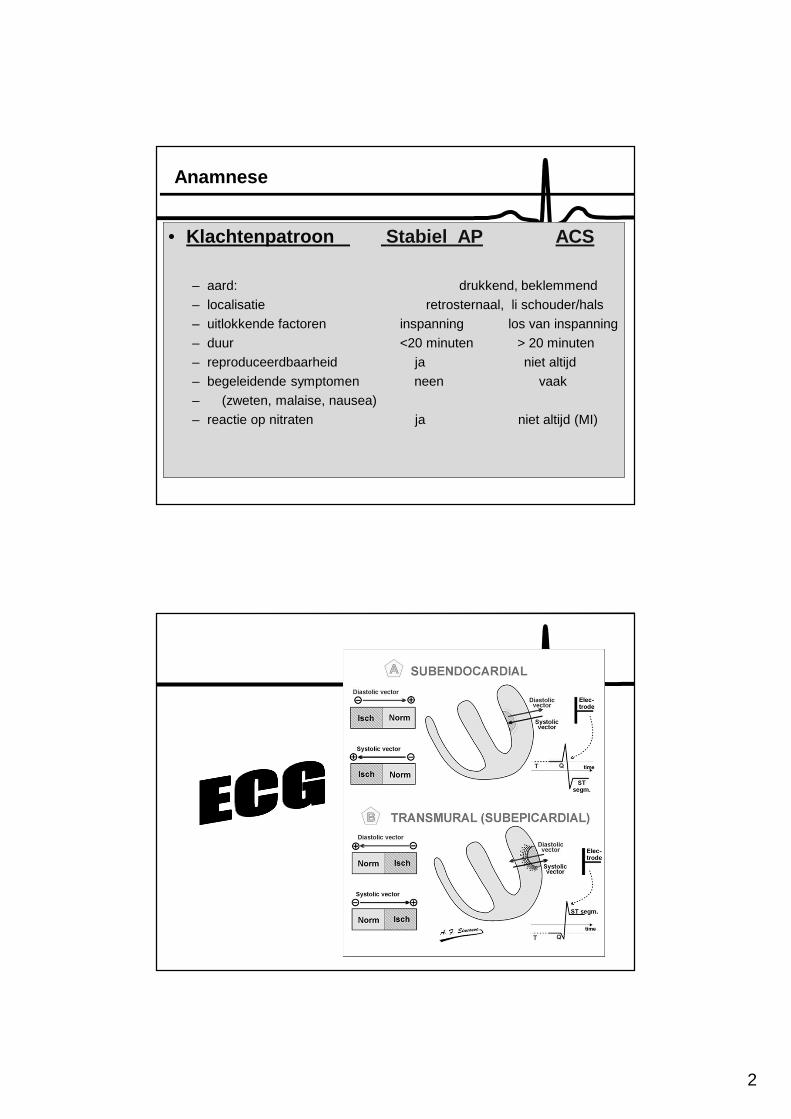
Anamnese
• Klachtenpatroon Stabiel AP ACS
– aard: drukkend, beklemmend
– localisatie retrosternaal, li schouder/hals
– uitlokkende factoren inspanning los van inspanning
– duur <20 minuten > 20 minuten
– reproduceerdbaarheid ja niet altijd
– begeleidende symptomen neen vaak
– (zweten, malaise, nausea)
– reactie op nitraten ja niet altijd (MI)
3
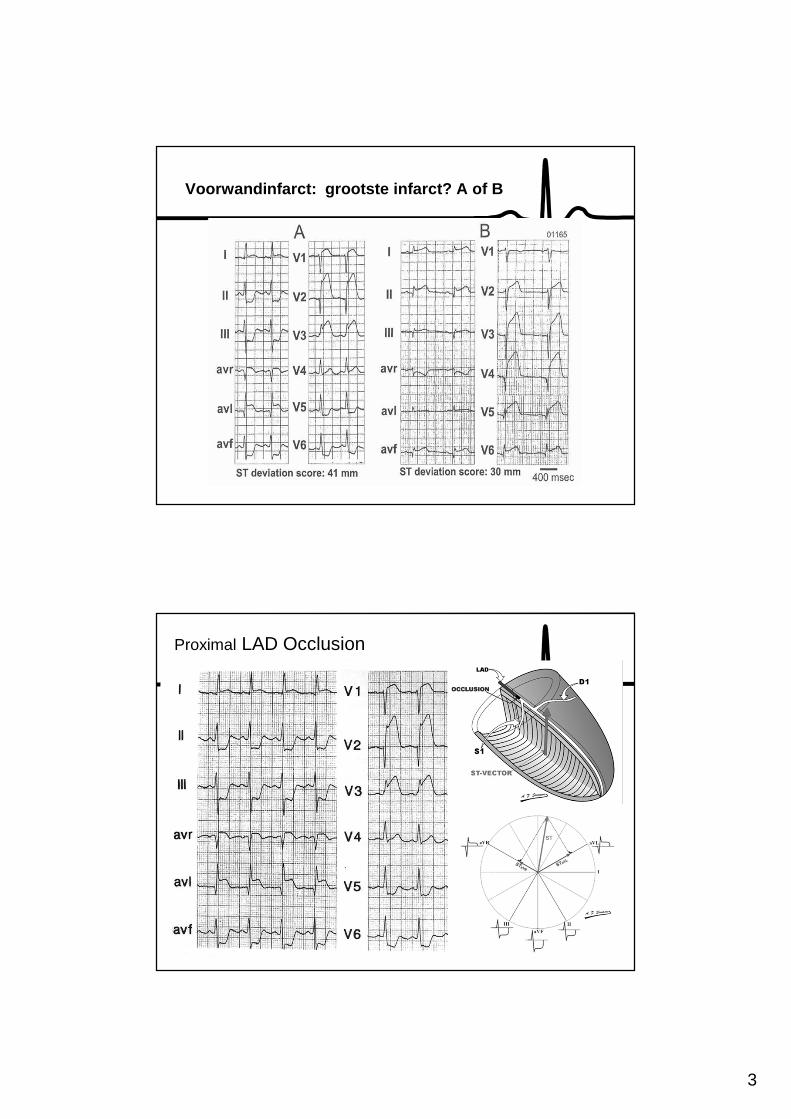
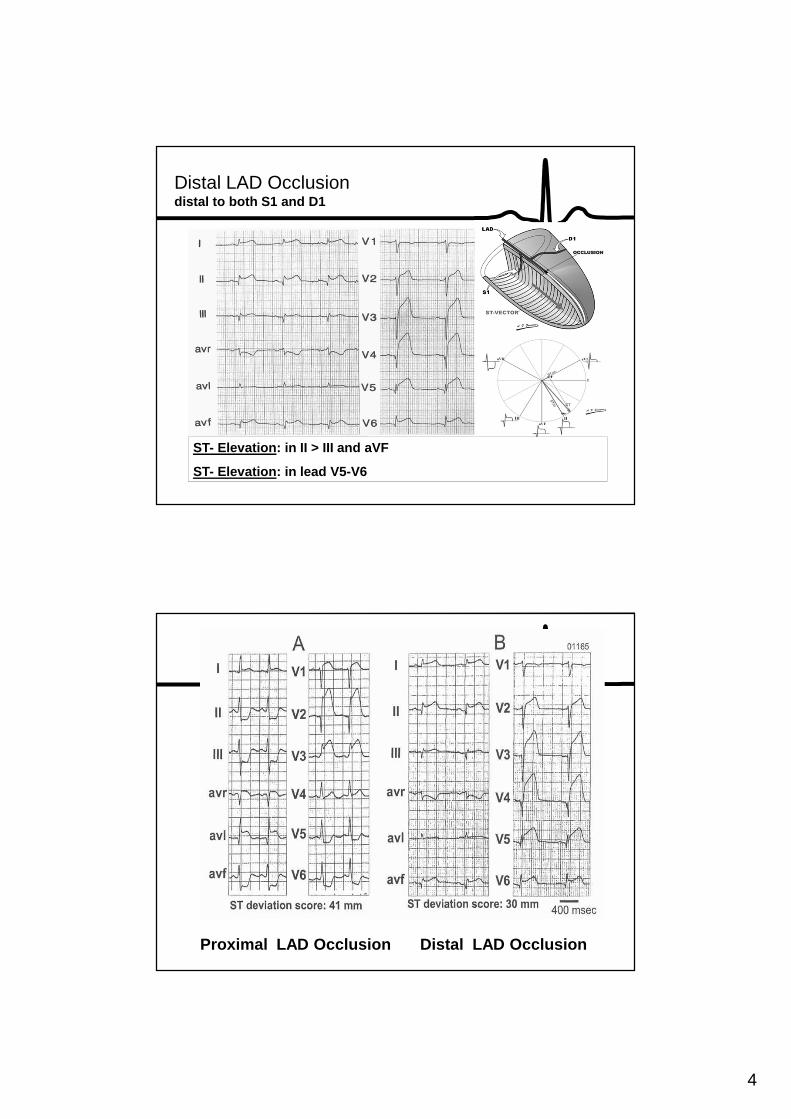
Voorwandinfarct: grootste infarct? A of B
Proximal LAD Occlusion
4
Distal LAD Occlusiondistal to both S1 and D1
ST- Elevation: in II > III and aVF
ST- Elevation: in lead V5-V6
Proximal LAD Occlusion Distal LAD Occlusion
5
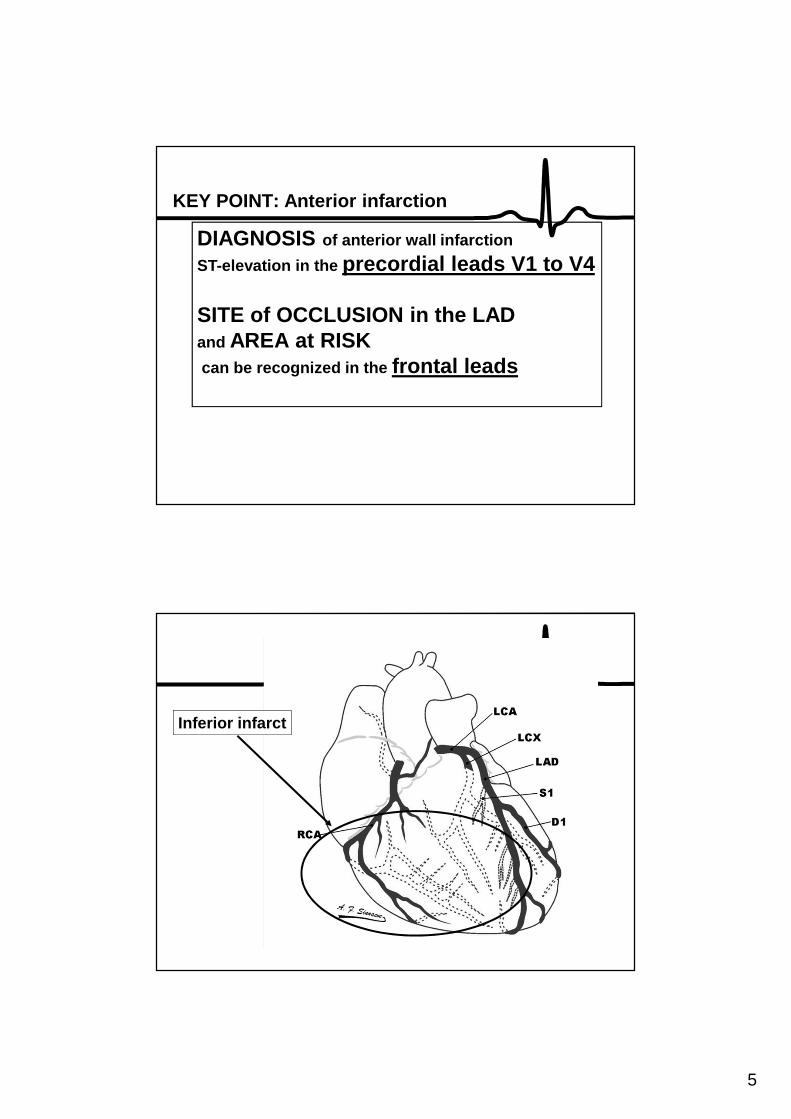
KEY POINT: Anterior infarction
DIAGNOSIS of anterior wall infarction
ST-elevation in the precordial leads V1 to V4
SITE of OCCLUSION in the LAD and AREA at RISKcan be recognized in the frontal leads
Inferior infarct
6
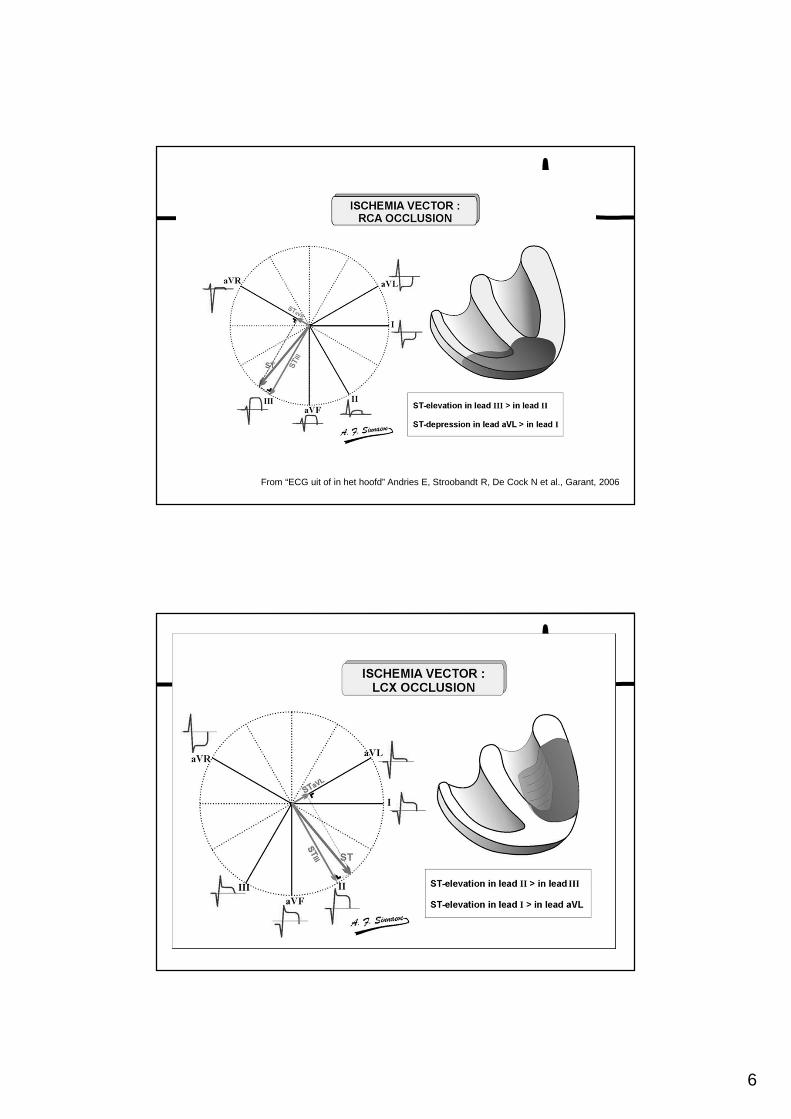
From “ECG uit of in het hoofd” Andries E, Stroobandt R, De Cock N et al., Garant, 2006
7
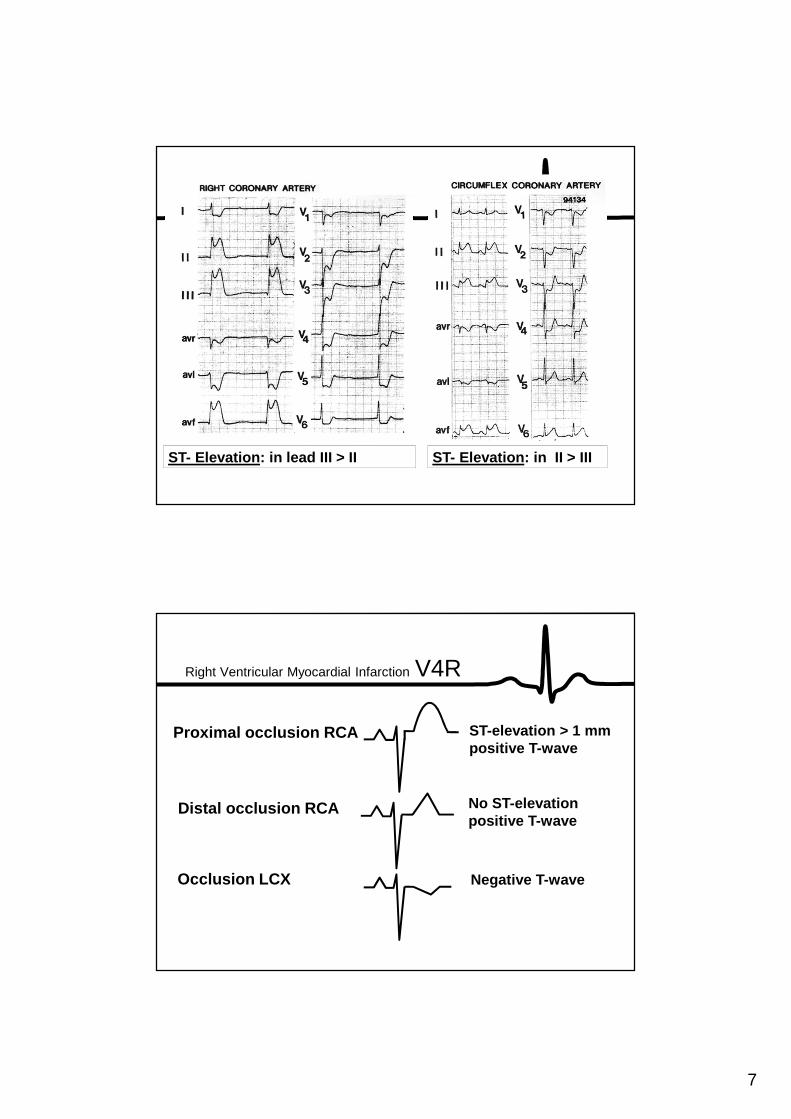
ST- Elevation: in lead III > II ST- Elevation: in II > III
Proximal occlusion RCA ST-elevation > 1 mmpositive T-wave
Distal occlusion RCA No ST-elevationpositive T-wave
Occlusion LCX Negative T-wave
Right Ventricular Myocardial Infarction V4R
8
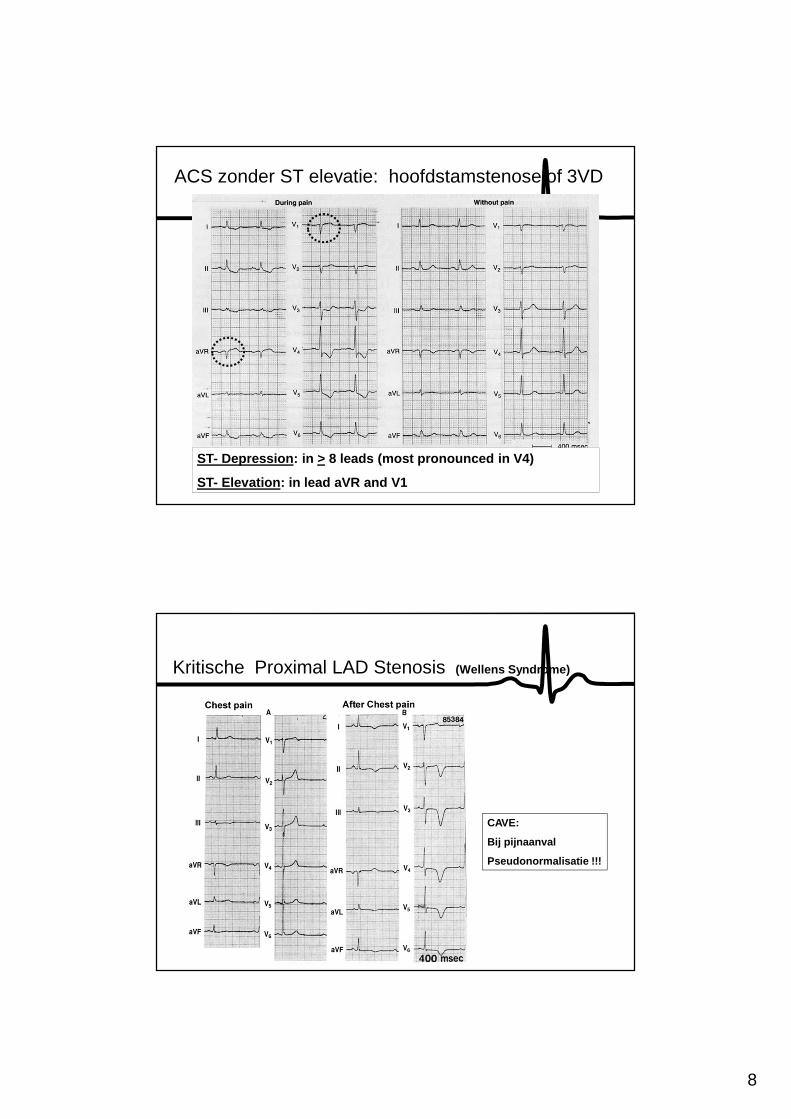
ACS zonder ST elevatie: hoofdstamstenose of 3VD
ST- Depression: in > 8 leads (most pronounced in V4)
ST- Elevation: in lead aVR and V1
Kritische Proximal LAD Stenosis (Wellens Syndrome)
CAVE:
Bij pijnaanval
Pseudonormalisatie !!!
9
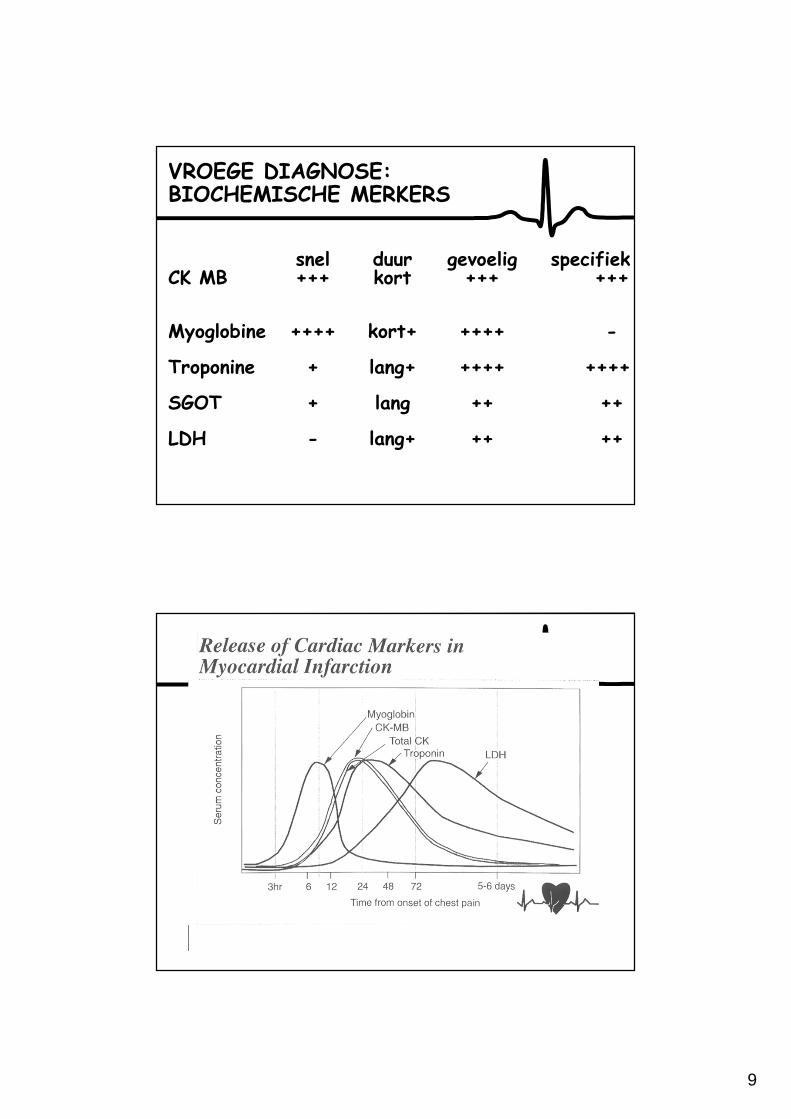
VROEGE DIAGNOSE:BIOCHEMISCHE MERKERS
snel duur gevoelig specifiekCK MB +++ kort +++ +++
Myoglobine ++++ kort+ ++++ -
Troponine + lang+ ++++ ++++
SGOT + lang ++ ++
LDH - lang+ ++ ++
10
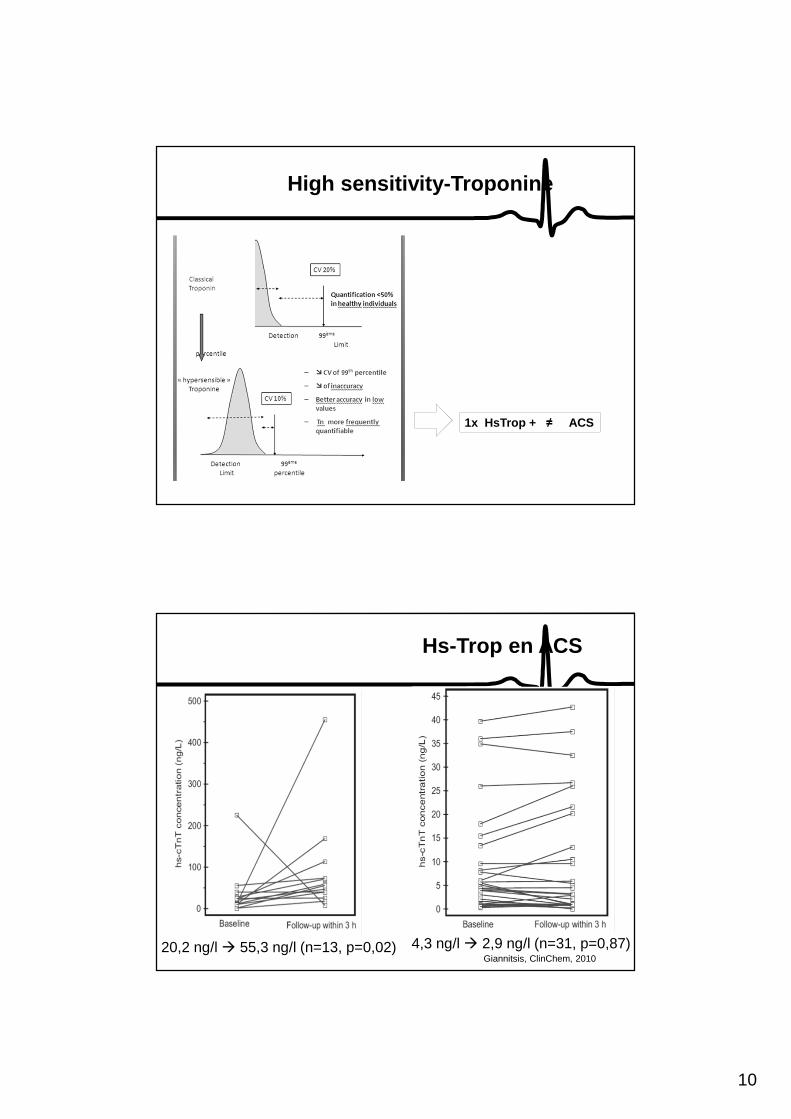
High sensitivity-Troponine
1x HsTrop + ≠ ACS
Giannitsis, ClinChem, 201020,2 ng/l � 55,3 ng/l (n=13, p=0,02) 4,3 ng/l � 2,9 ng/l (n=31, p=0,87)
Hs-Trop en ACS
11
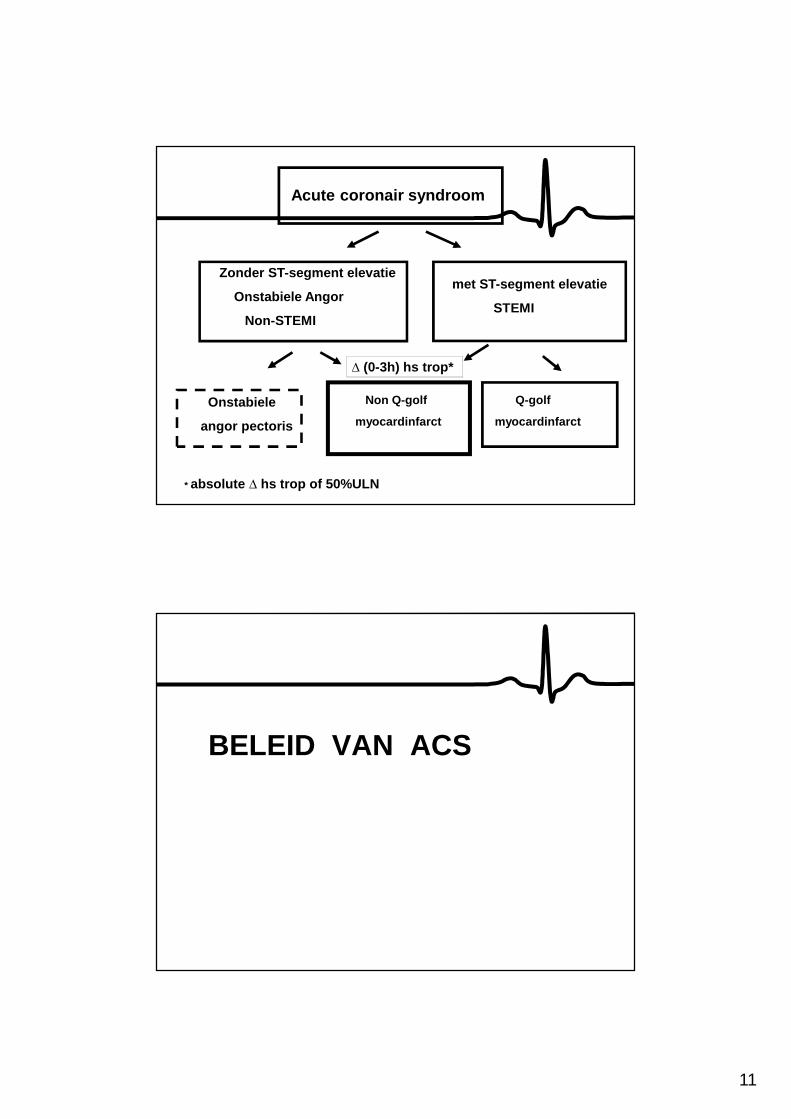
Acute coronair syndroom
Zonder ST-segment elevatie
Onstabiele Angor
Non-STEMI
met ST-segment elevatie
STEMI
Onstabiele
angor pectoris
Non Q-golf
myocardinfarct
Q-golf
myocardinfarct
* absolute ∆ hs trop of 50%ULN
∆ (0-3h) hs trop*
BELEID VAN ACS
12
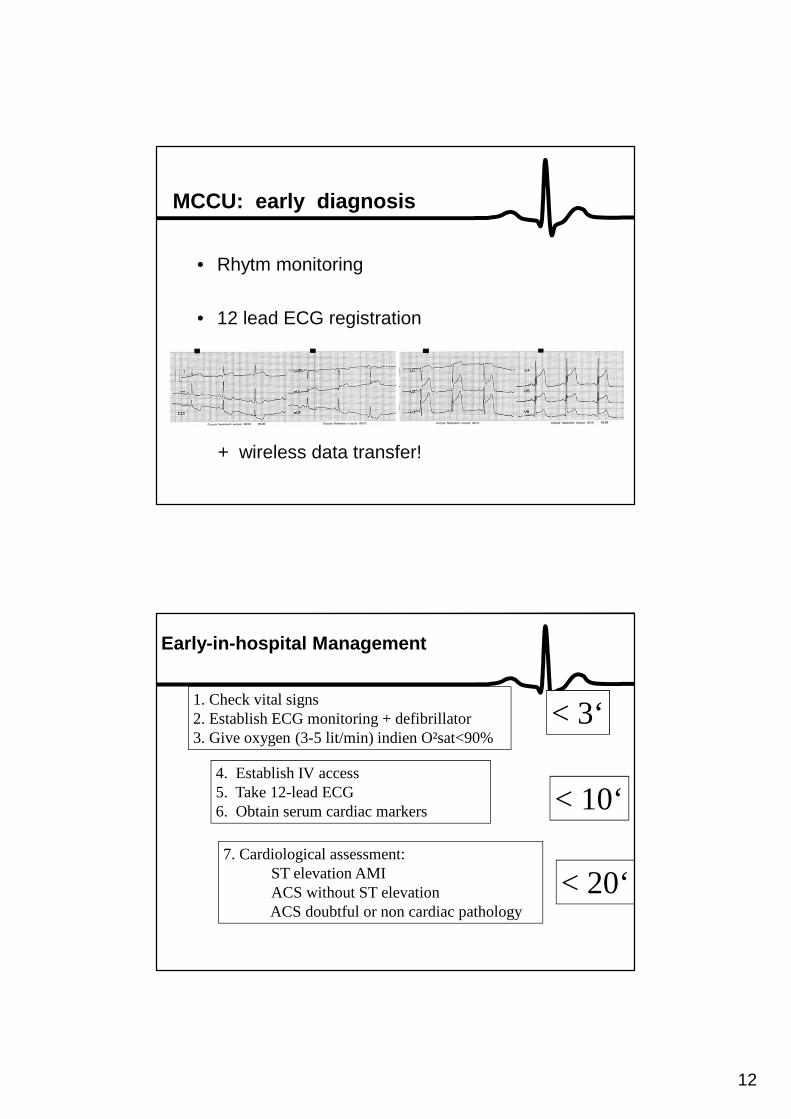
MCCU: early diagnosis
• Rhytm monitoring
• 12 lead ECG registration
+ wireless data transfer!
Early-in-hospital Management
1. Check vital signs2. Establish ECG monitoring + defibrillator 3. Give oxygen (3-5 lit/min) indien O²sat<90%
4. Establish IV access5. Take 12-lead ECG6. Obtain serum cardiac markers
7. Cardiological assessment:ST elevation AMI ACS without ST elevationACS doubtful or non cardiac pathology
< 3‘
< 10‘
< 20‘
13
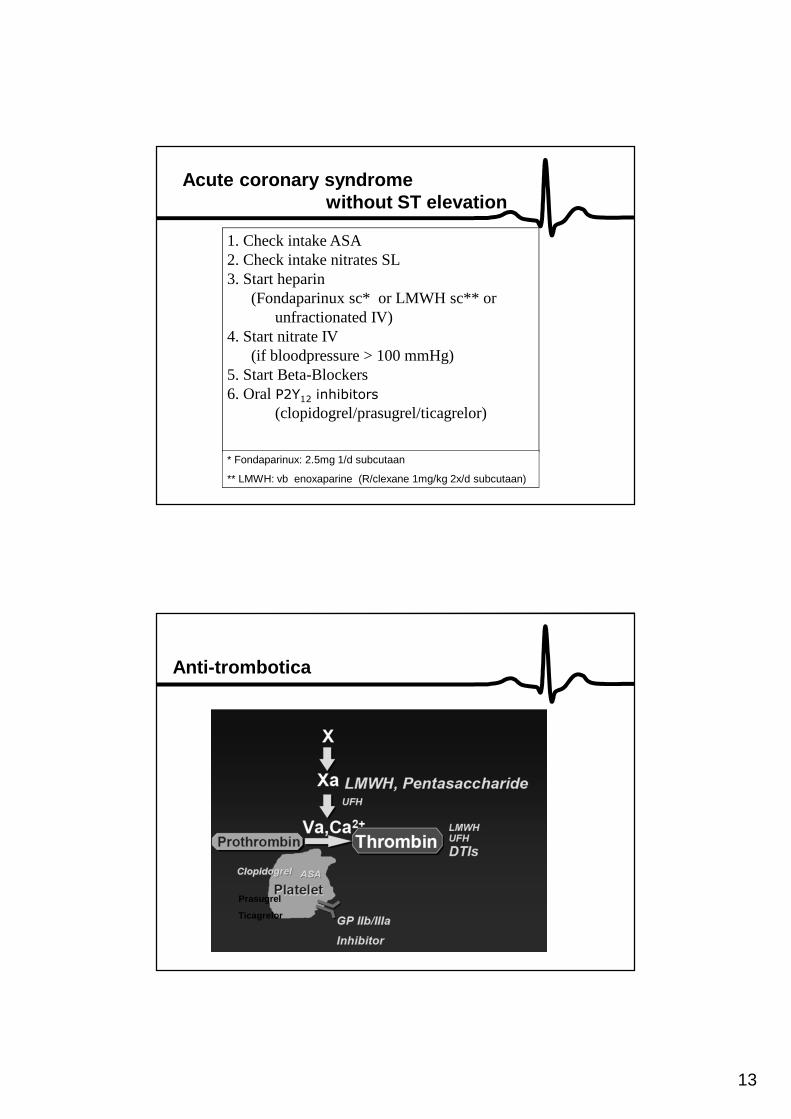
Acute coronary syndrome without ST elevation
1. Check intake ASA 2. Check intake nitrates SL3. Start heparin
(Fondaparinux sc* or LMWH sc** orunfractionated IV)
4. Start nitrate IV (if bloodpressure > 100 mmHg)
5. Start Beta-Blockers6. OralP2Y12 inhibitors
(clopidogrel/prasugrel/ticagrelor)
* Fondaparinux: 2.5mg 1/d subcutaan
** LMWH: vb enoxaparine (R/clexane 1mg/kg 2x/d subcutaan)
Anti-trombotica
Prasugrel
Ticagrelor
14
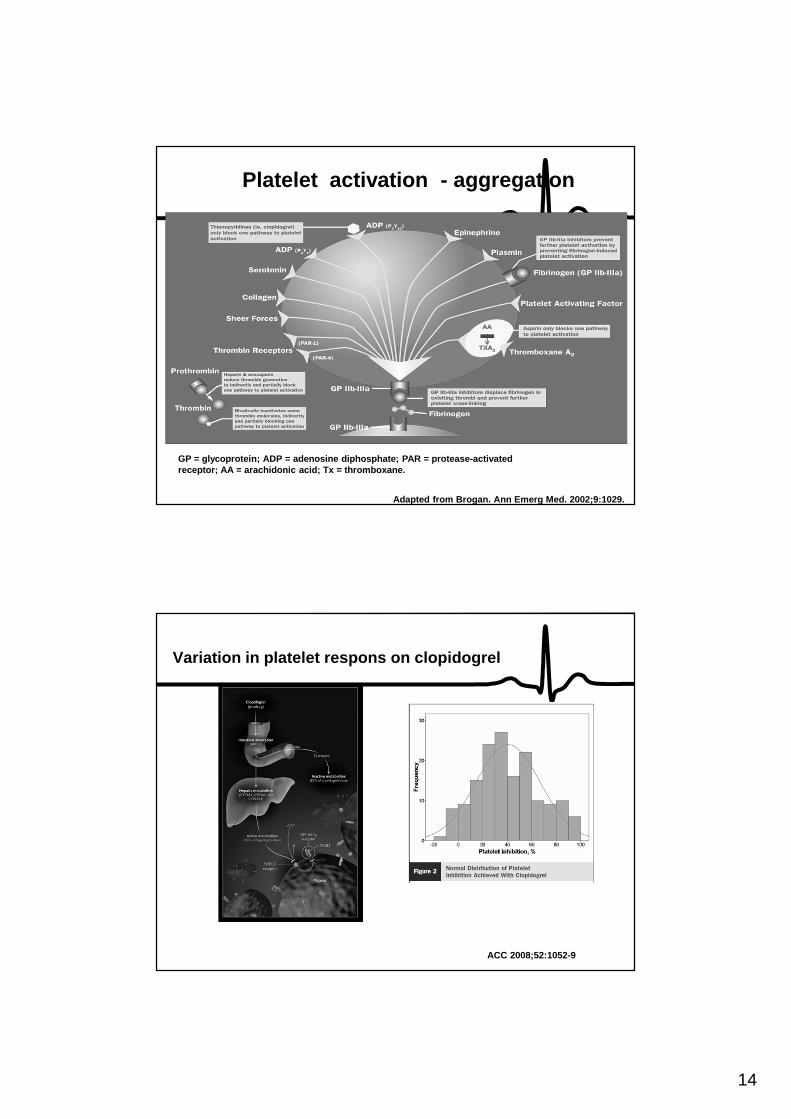
GP = glycoprotein; ADP = adenosine diphosphate; PAR = protease-activated receptor; AA = arachidonic acid; Tx = thromboxane.
Adapted from Brogan. Ann Emerg Med. 2002;9:1029.
Platelet activation - aggregation
Variation in platelet respons on clopidogrel
ACC 2008;52:1052-9
15
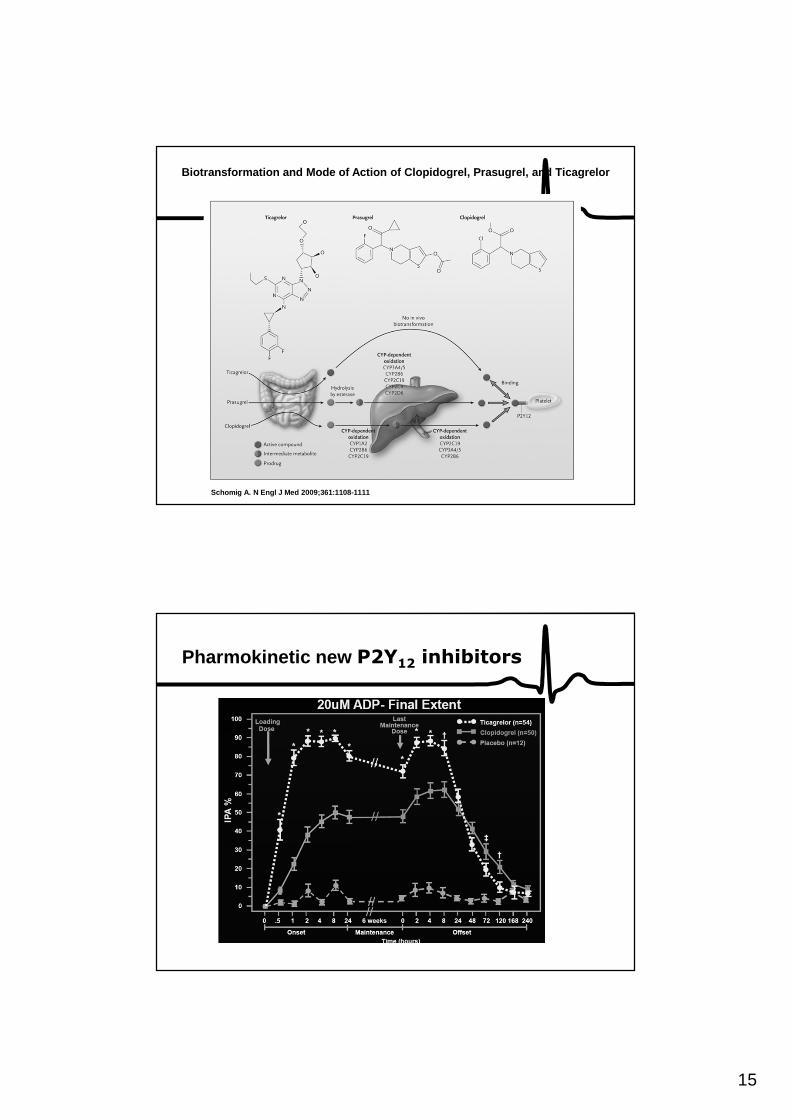
Schomig A. N Engl J Med 2009;361:1108-1111
Biotransformation and Mode of Action of Clopidogrel , Prasugrel, and Ticagrelor
Pharmokinetic new P2Y12 inhibitors
16
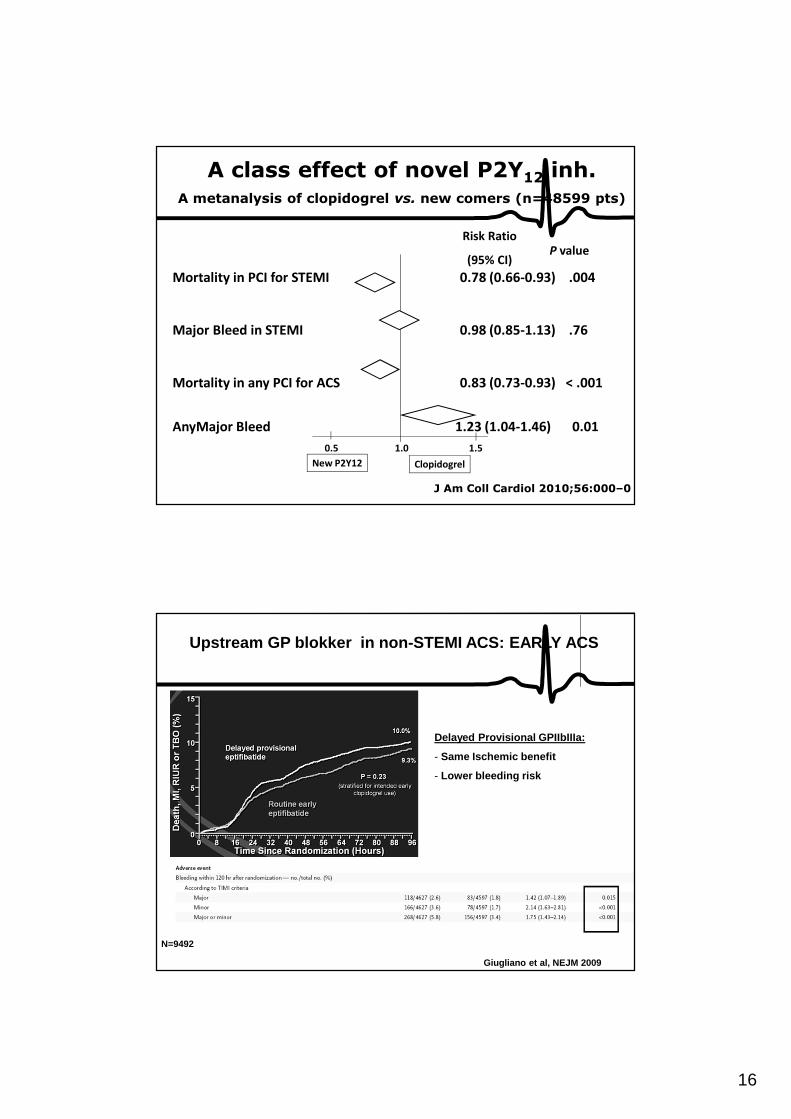
Mortality in PCI for STEMI 0.78 (0.66-0.93) .004
Major Bleed in STEMI 0.98 (0.85-1.13) .76
Mortality in any PCI for ACS 0.83 (0.73-0.93) < .001
AnyMajor Bleed 1.23 (1.04-1.46) 0.01
Risk Ratio
(95% CI)P value
0.5 1.0 1.5
ClopidogrelNew P2Y12
A class effect of novel P2Y12 inh.A metanalysis of clopidogrel vs. new comers (n=48599 pts)
J Am Coll Cardiol 2010;56:000–0
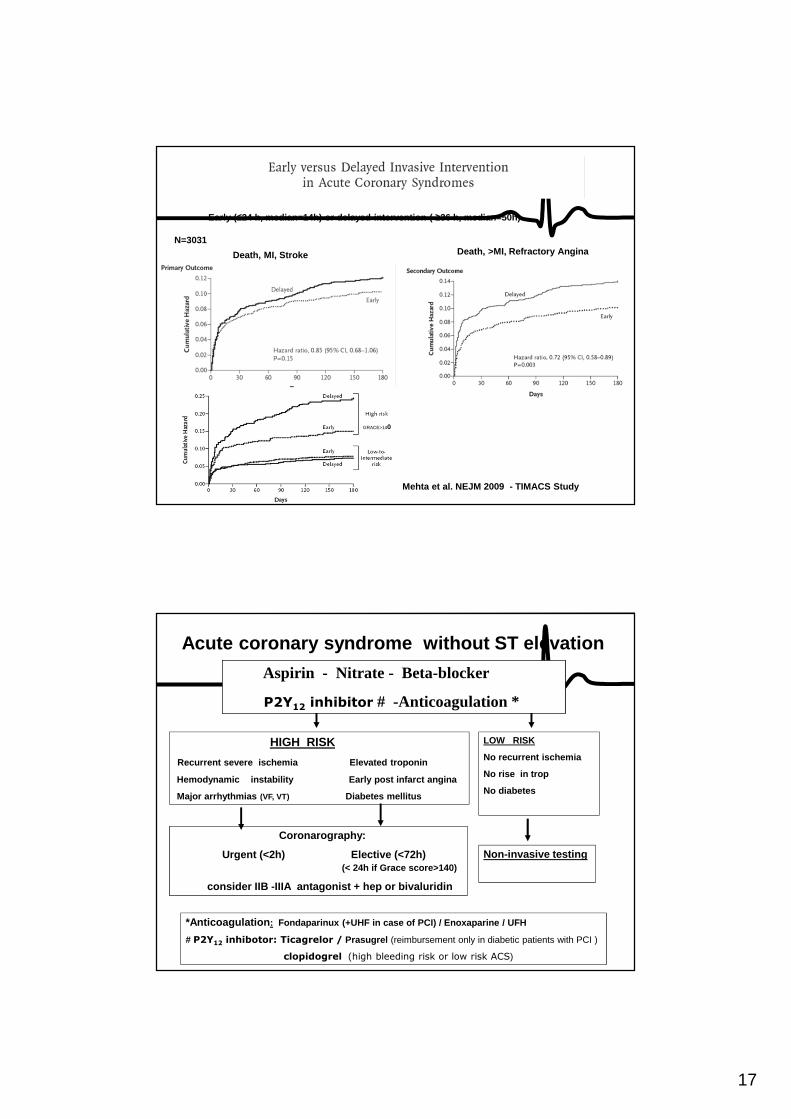
Giugliano et al, NEJM 2009
Delayed Provisional GPIIbIIIa:
- Same Ischemic benefit
- Lower bleeding risk
N=9492
Upstream GP blokker in non-STEMI ACS: EARLY ACS
17
Mehta et al. NEJM 2009 - TIMACS Study
Early (≤24 h, median=14h) or delayed intervention ( ≥36 h, median=50h)
Death, >MI, Refractory AnginaDeath, MI, Stroke
N=3031
GRACE>140
Acute coronary syndrome without ST elevation
Aspirin - Nitrate - Beta-blocker
P2Y12 inhibitor # -Anticoagulation *
*Anticoagulation : Fondaparinux (+UHF in case of PCI) / Enoxaparine / U FH
# P2Y12 inhibotor: Ticagrelor / Prasugrel (reimbursement only in diabetic patients with PCI )
clopidogrel (high bleeding risk or low risk ACS)
HIGH RISK
Recurrent severe ischemia Elevated troponin
Hemodynamic instability Early post infarct angina
Major arrhythmias (VF, VT) Diabetes mellitus
Coronarography:
Urgent (<2h) Elective (<72h)(< 24h if Grace score>140)
consider IIB -IIIA antagonist + hep or bivaluridin
LOW RISK
No recurrent ischemia
No rise in trop
No diabetes
Non-invasive testing
18
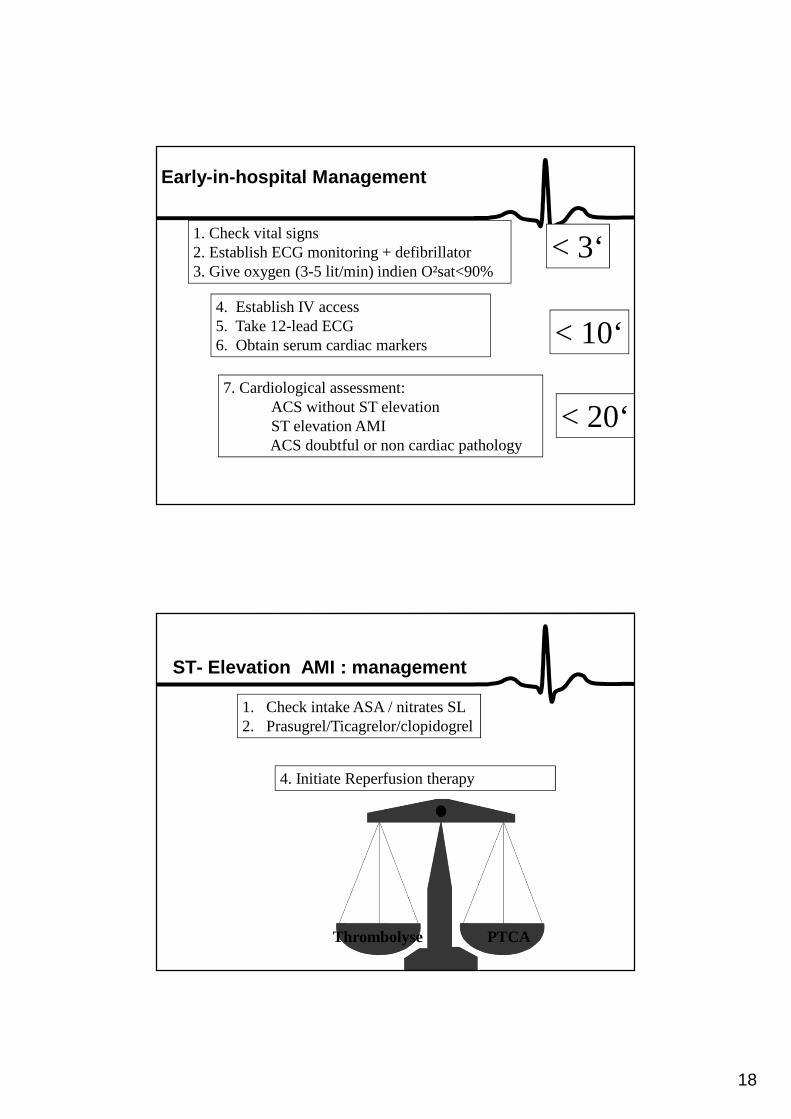
Early-in-hospital Management
1. Check vital signs2. Establish ECG monitoring + defibrillator 3. Give oxygen (3-5 lit/min) indien O²sat<90%
4. Establish IV access5. Take 12-lead ECG6. Obtain serum cardiac markers
7. Cardiological assessment:ACS without ST elevation ST elevation AMI ACS doubtful or non cardiac pathology
< 3‘
< 10‘
< 20‘
ST- Elevation AMI : management
1. Check intake ASA / nitrates SL2. Prasugrel/Ticagrelor/clopidogrel
4. Initiate Reperfusion therapy
Thrombolyse PTCA
19
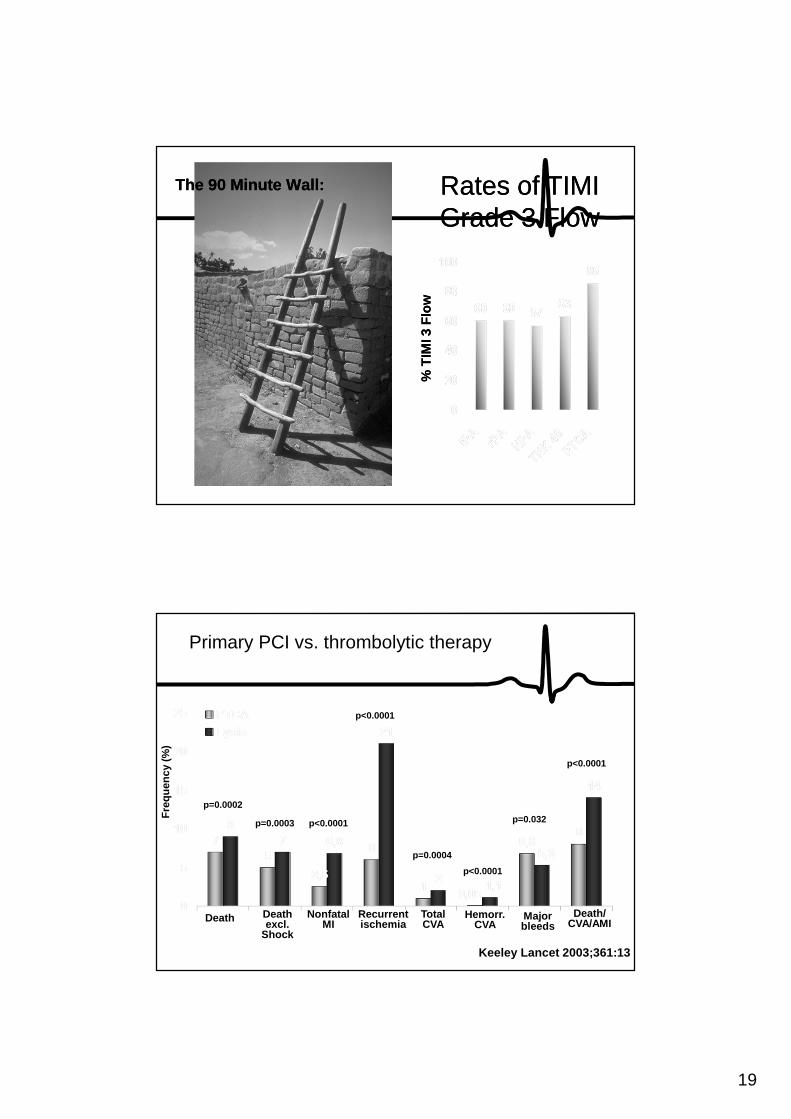
The 90 Minute Wall:The 90 Minute Wall: Rates of TIMI Grade 3 FlowRates of TIMI Grade 3 Flow
% T
IMI 3
Flo
w%
TIM
I 3 F
low
Primary PCI vs. thrombolytic therapy
Keeley Lancet 2003;361:13
Death Death excl.
Shock
Nonfatal MI
Recurrent ischemia
Total CVA
Hemorr. CVA
Major bleeds
Death/ CVA/AMI
p=0.0002
p=0.0003 p<0.0001
p<0.0001
p=0.0004
p<0.0001
p=0.032
p<0.0001
Fre
quen
cy (
%)
20
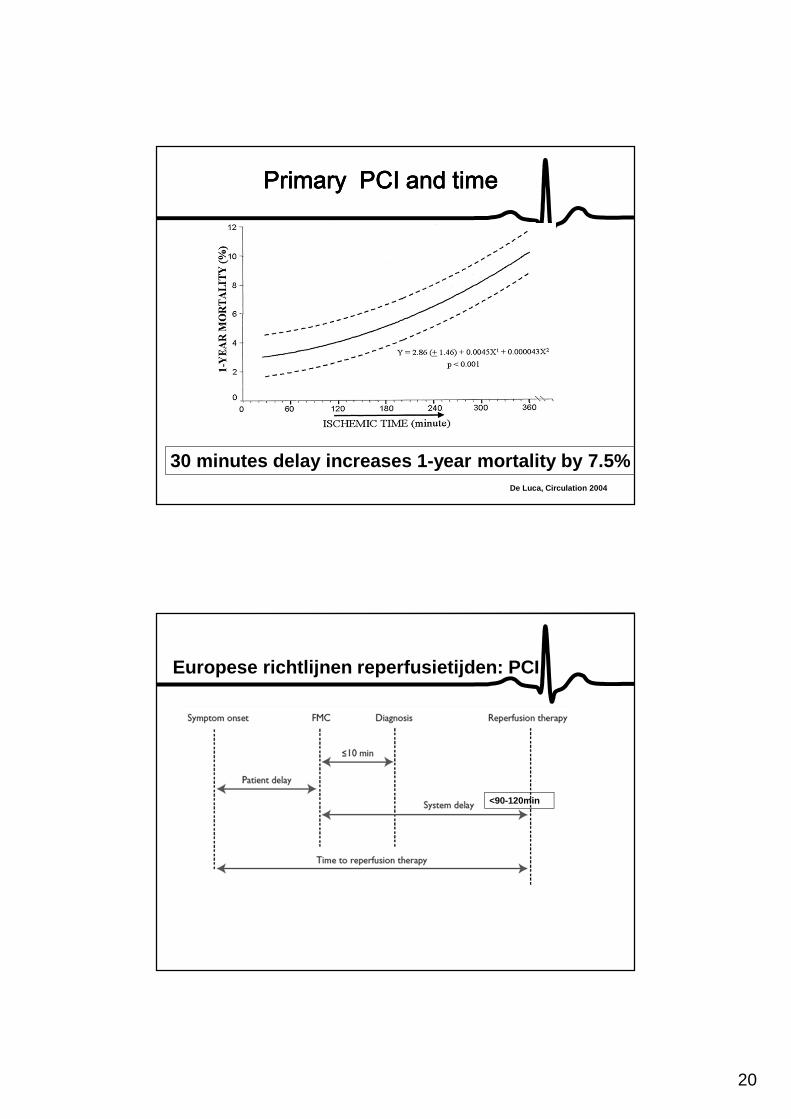
De Luca, Circulation 2004
Primary PCI and timePrimary PCI and timePrimary PCI and timePrimary PCI and time
30 minutes delay increases 1-year mortality by 7.5%
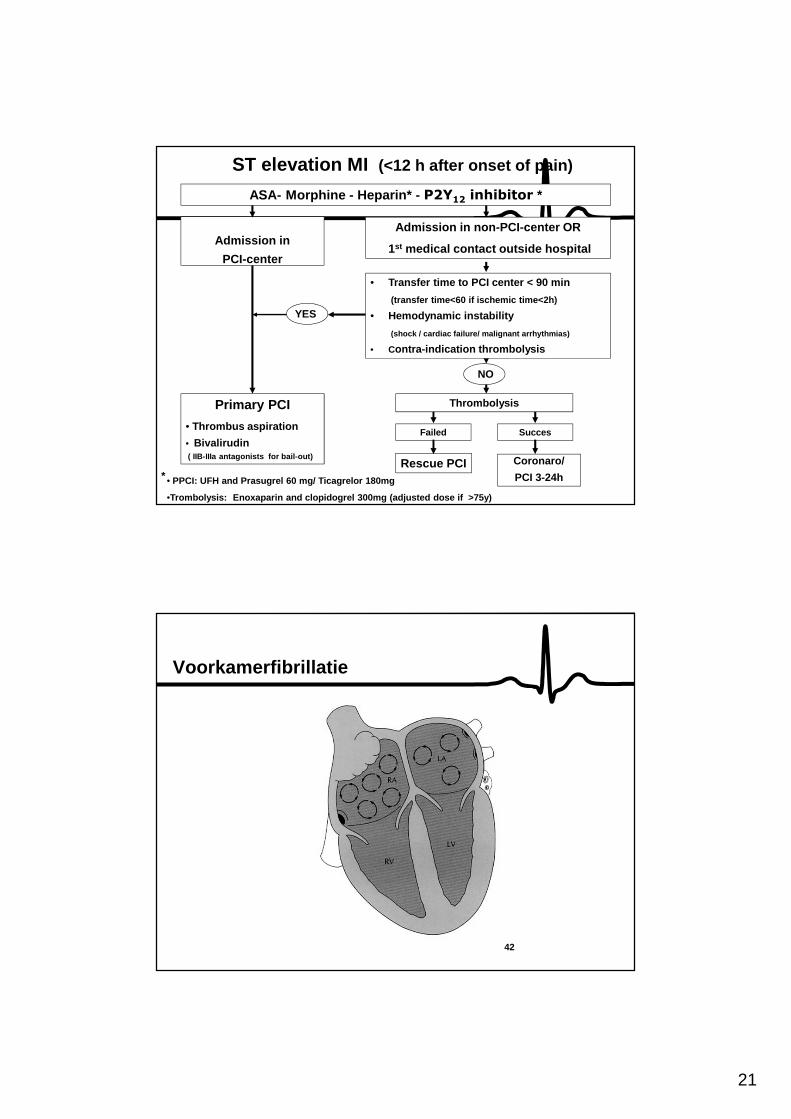
Europese richtlijnen reperfusietijden: PCI
<90-120min
21
ST elevation MI (<12 h after onset of pain)
Admission in
PCI-center
Primary PCI
• Thrombus aspiration
• Bivalirudin( IIB-IIIa antagonists for bail-out)
Admission in non-PCI-center OR
1st medical contact outside hospital
• Transfer time to PCI center < 90 min
(transfer time<60 if ischemic time<2h)
• Hemodynamic instability
(shock / cardiac failure/ malignant arrhythmias)
• Contra-indication thrombolysis
Thrombolysis
YES
NO
• PPCI: UFH and Prasugrel 60 mg/ Ticagrelor 180mg
•Trombolysis: Enoxaparin and clopidogrel 300mg (adjus ted dose if >75y)
ASA- Morphine - Heparin* - P2Y12 inhibitor *
Failed
Rescue PCI
Succes
Coronaro/
PCI 3-24h*
42
Voorkamerfibrillatie
22
43
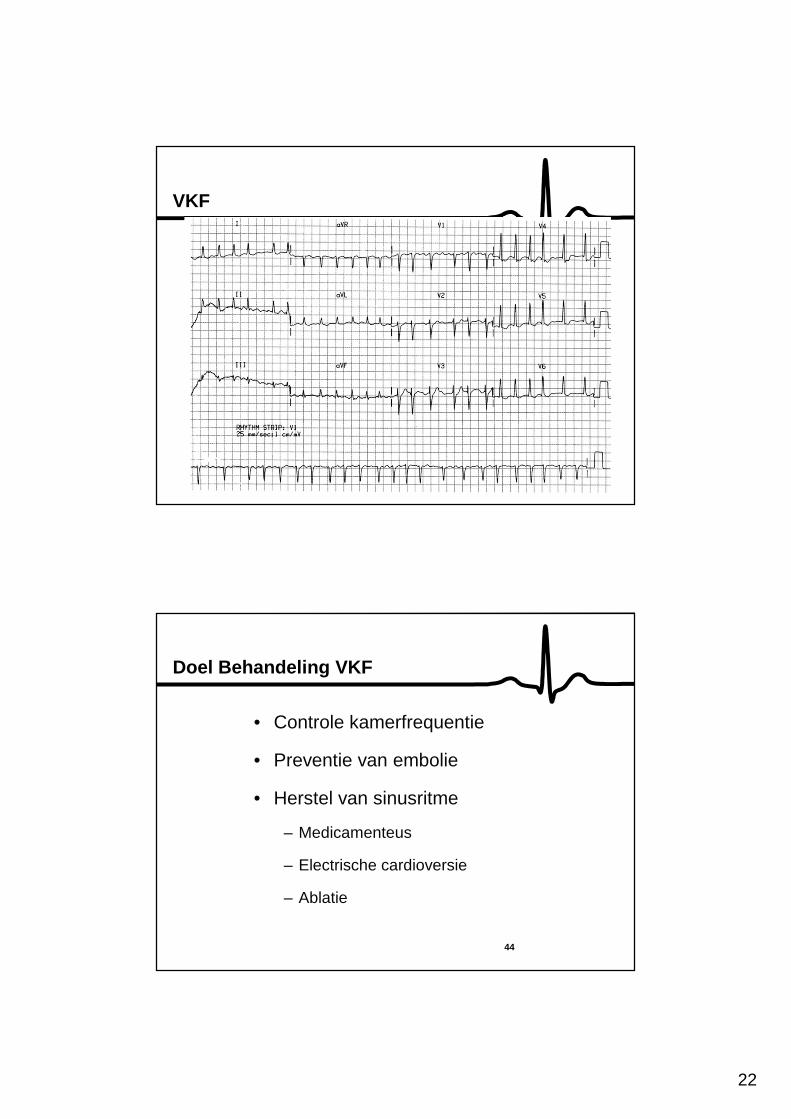
VKF
44
Doel Behandeling VKF
• Controle kamerfrequentie
• Preventie van embolie
• Herstel van sinusritme
– Medicamenteus
– Electrische cardioversie
– Ablatie
23
Stabilisatie Hartritme
Betablokkers CAVE bronchospasme, cardiodepressie
Calcium-antagonist: verapamil/diltiazem
CAVE: WPW, HOCM, cardiodepressie
Digitalis: vooral bij hartfalen
CAVE: WPW, HOCM
Amiodarone IV: bij hartfalen
bij refractaire tachycardie
Cardioversie en Cardiale Embolen
Risico cardiale embolen
VKF> 2 d: 5-8 %
VKF< 2d: <1%
ANTICO indien VKF > 2 dagen !! of TEE
24
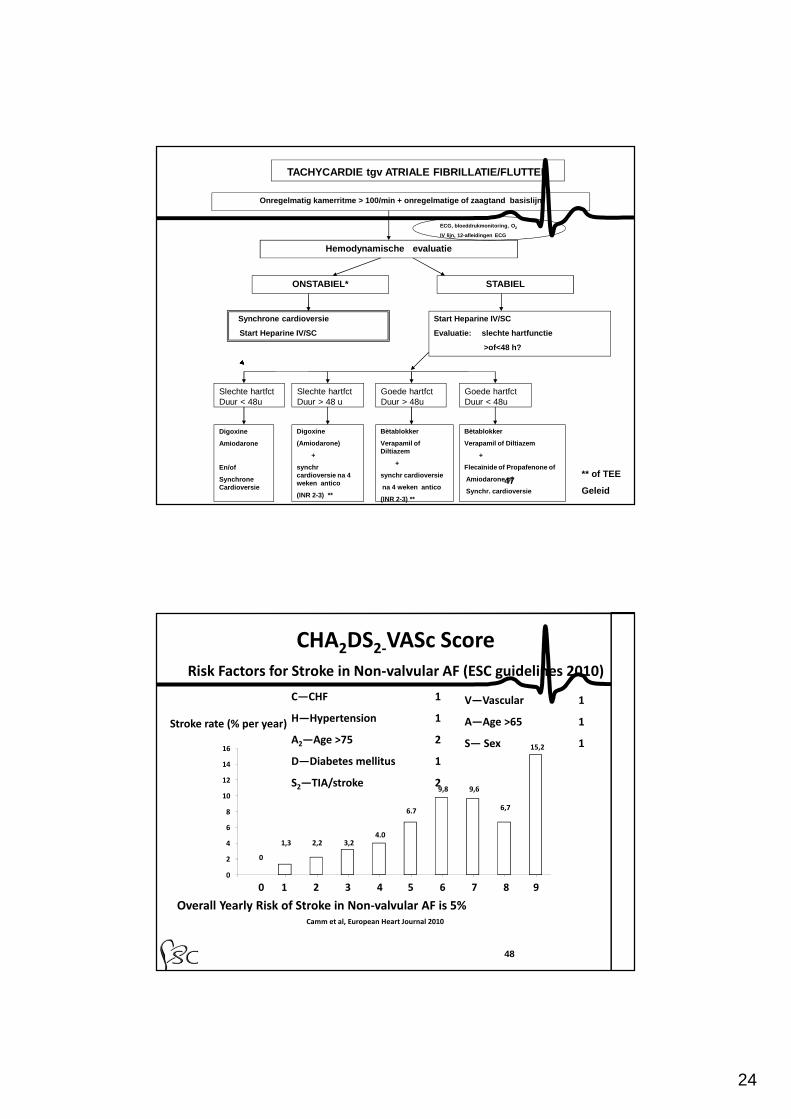
47
Onregelmatig kamerritme > 100/min + onregelmatige o f zaagtand basislijn
ECG, bloeddrukmonitoring, O 2
IV lijn, 12-afleidingen ECG
Hemodynamische evaluatie
ONSTABIEL* STABIEL
Synchrone cardioversie
Start Heparine IV/SC
Start Heparine IV/SC
Evaluatie: slechte hartfunctie
>of<48 h?
Goede hartfct Duur < 48u
Goede hartfctDuur > 48u
Slechte hartfctDuur < 48u
Digoxine
(Amiodarone)
+
synchrcardioversie na 4 weken antico
(INR 2-3) **
Digoxine
Amiodarone
En/of
Synchrone Cardioversie
Slechte hartfctDuur > 48 u
Bètablokker
Verapamil of Diltiazem
+
synchr cardioversie
na 4 weken antico
(INR 2-3) **
Bètablokker
Verapamil of Diltiazem
+
Flecaïnide of Propafenone of
Amiodarone of
Synchr. cardioversie
TACHYCARDIE tgv ATRIALE FIBRILLATIE/FLUTTER
** of TEE
Geleid
C—CHF 1
H—Hypertension 1
A2—Age >75 2
D—Diabetes mellitus 1
S2—TIA/stroke 2
Risk Factors for Stroke in Non-valvular AF (ESC guidelines 2010)
Overall Yearly Risk of Stroke in Non-valvular AF is 5%Camm et al, European Heart Journal 2010
0
2
4
6
8
10
12
14
16
1,3 2,2 3,24.0
6.7
9,8 9,6
6,7
15,2
Stroke rate (% per year)
0
0 1 2 3 4 5 6 7 8 9
V—Vascular 1
A—Age >65 1
S— Sex 1
CHA2DS2-VASc Score
48
25
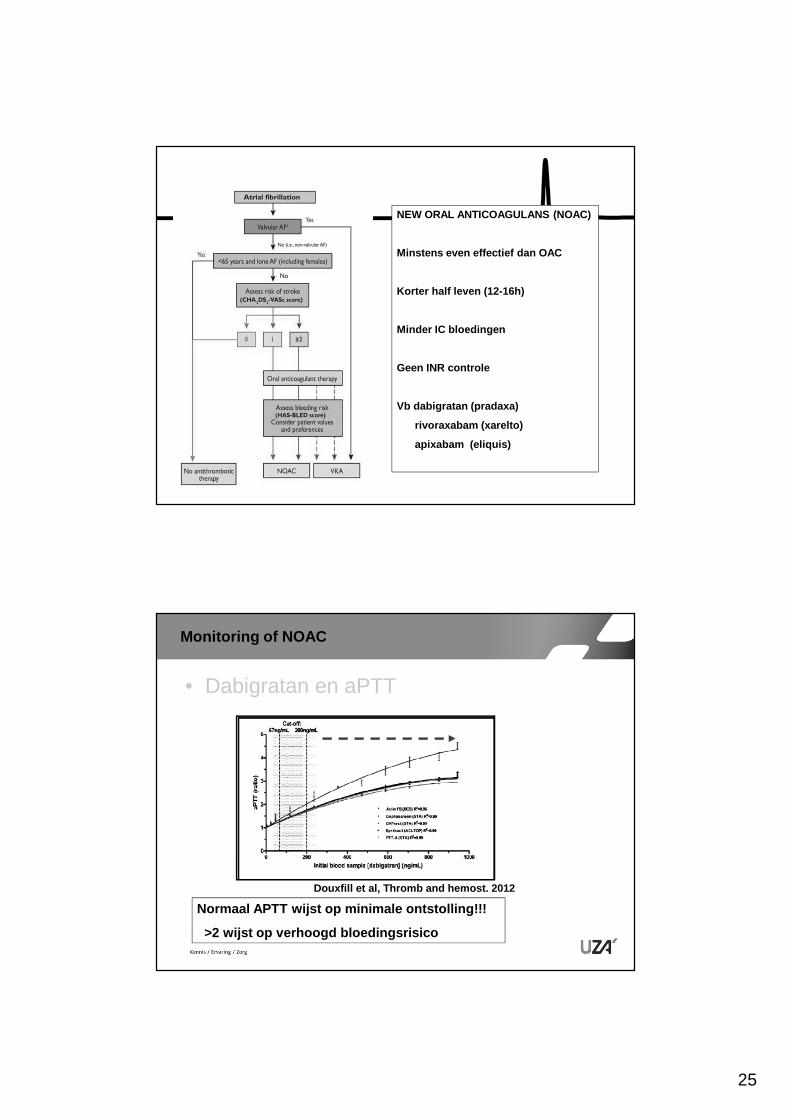
NEW ORAL ANTICOAGULANS (NOAC)
Minstens even effectief dan OAC
Korter half leven (12-16h)
Minder IC bloedingen
Geen INR controle
Vb dabigratan (pradaxa)
rivoraxabam (xarelto)
apixabam (eliquis)
Monitoring of NOAC
• Dabigratan en aPTT
Normaal APTT wijst op minimale ontstolling!!!
>2 wijst op verhoogd bloedingsrisico
Douxfill et al, Thromb and hemost. 2012
26
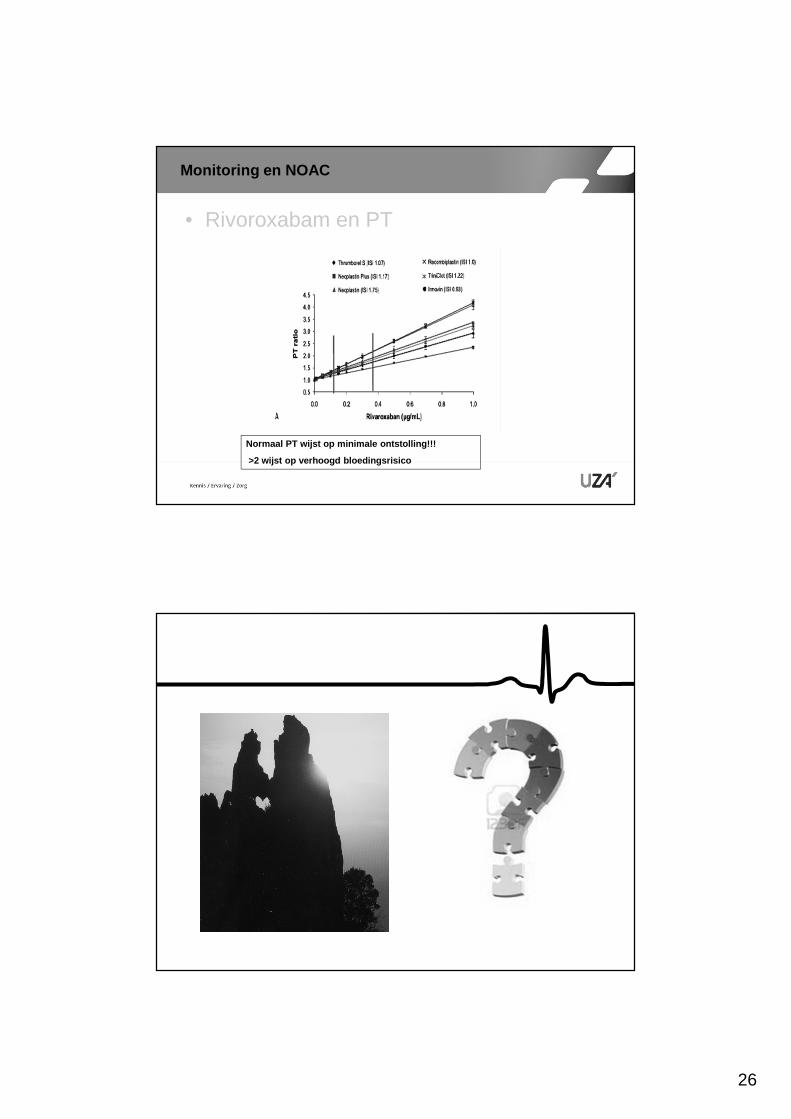
Monitoring en NOAC
• Rivoroxabam en PT
Normaal PT wijst op minimale ontstolling!!!
>2 wijst op verhoogd bloedingsrisico
27
Dosis aanpassing - interacties
Dabigratan® pradaxa
Rivoraxabam® xarelto
Apixabam® Eliquis
Standaard dosis 2x150mg/d 20mg/d 2x5mg/d
Dosisaanpassing GFR<50 ml/min GFR<50ml/min GFR <30ml/min
Aangepast dosis 2x110mg/d 15mg/d 2x2.5mg/d
Niet aanbevolen GFR <30 ml/min GFR<15 ml/min GFR <15ml/min
Niet te associeren(cf CYP3A4)
Antifungal(Ketoconazole, )HIV protease inh
Antifungal(Ketoconazole, )HIV protease inh(fluconazole wel)
Antifungal(Ketoconazole, )HIV protease inh
Referenties
• European Task force report on management of AMI. EHJ 2012
• European Task force report on management of ACS without persistent ST elevation. EHJ 2011
• European Task force report onrevascularisation, EHJ 2010