Auteursrecht voor onderwijs- zelf lesmateriaal samenstellen - NT2-onderwijs
Upload
victor-viersenCategory
view
464download
1
ROTEM in de praktijk
16 december Victor Viersen
http://www.slideshare.net/VictorViersen
Inhoud• De achtergrond en techniek van de ROTEM
• Het Thromboelastogram
• ROTEM diagnoses
• ROTEM casuïstiek
• ROTEM vs klassieke testen
• Blik op de toekomst

ROTEMTechniek

Het apparaat
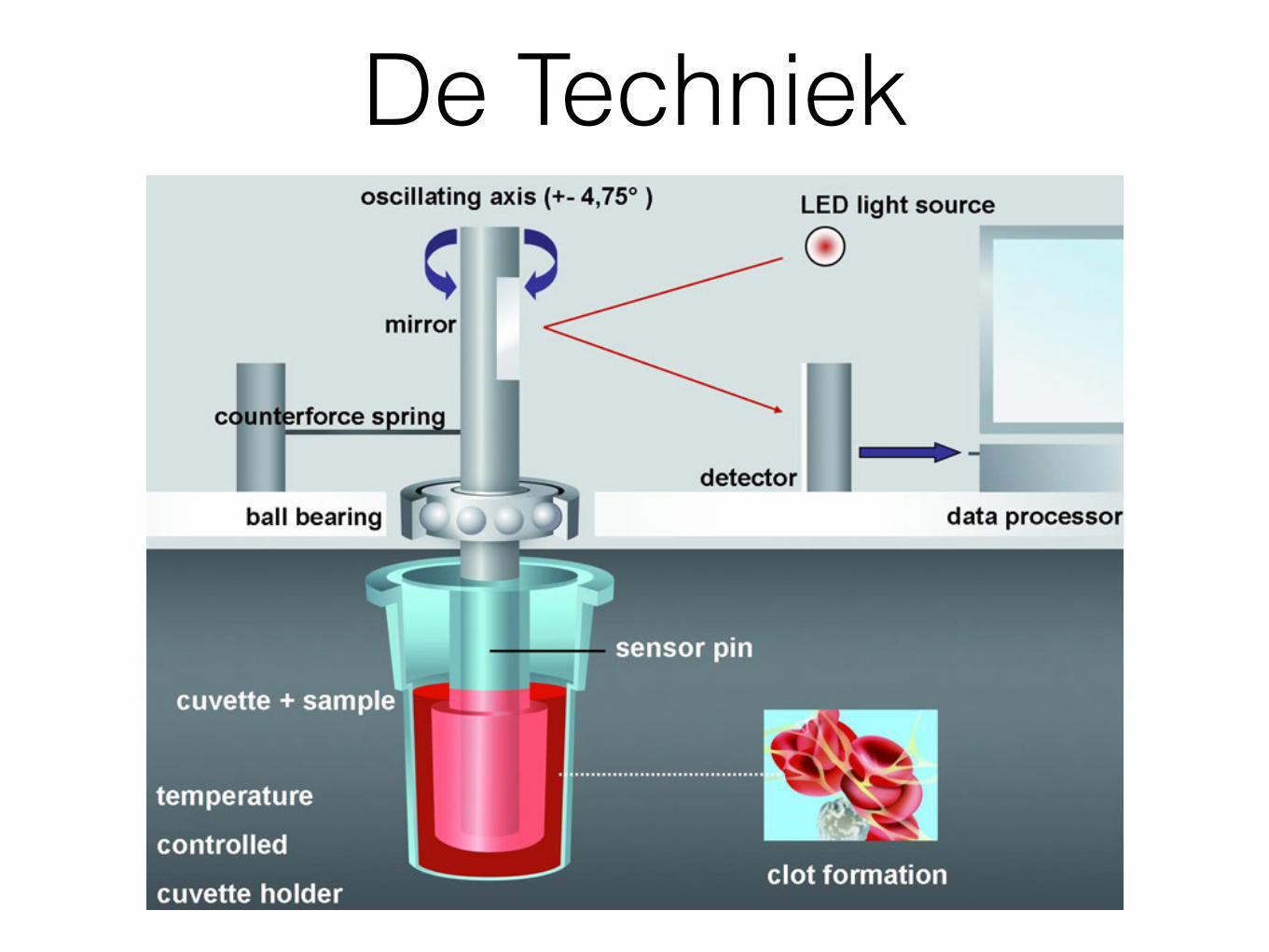
De Techniek
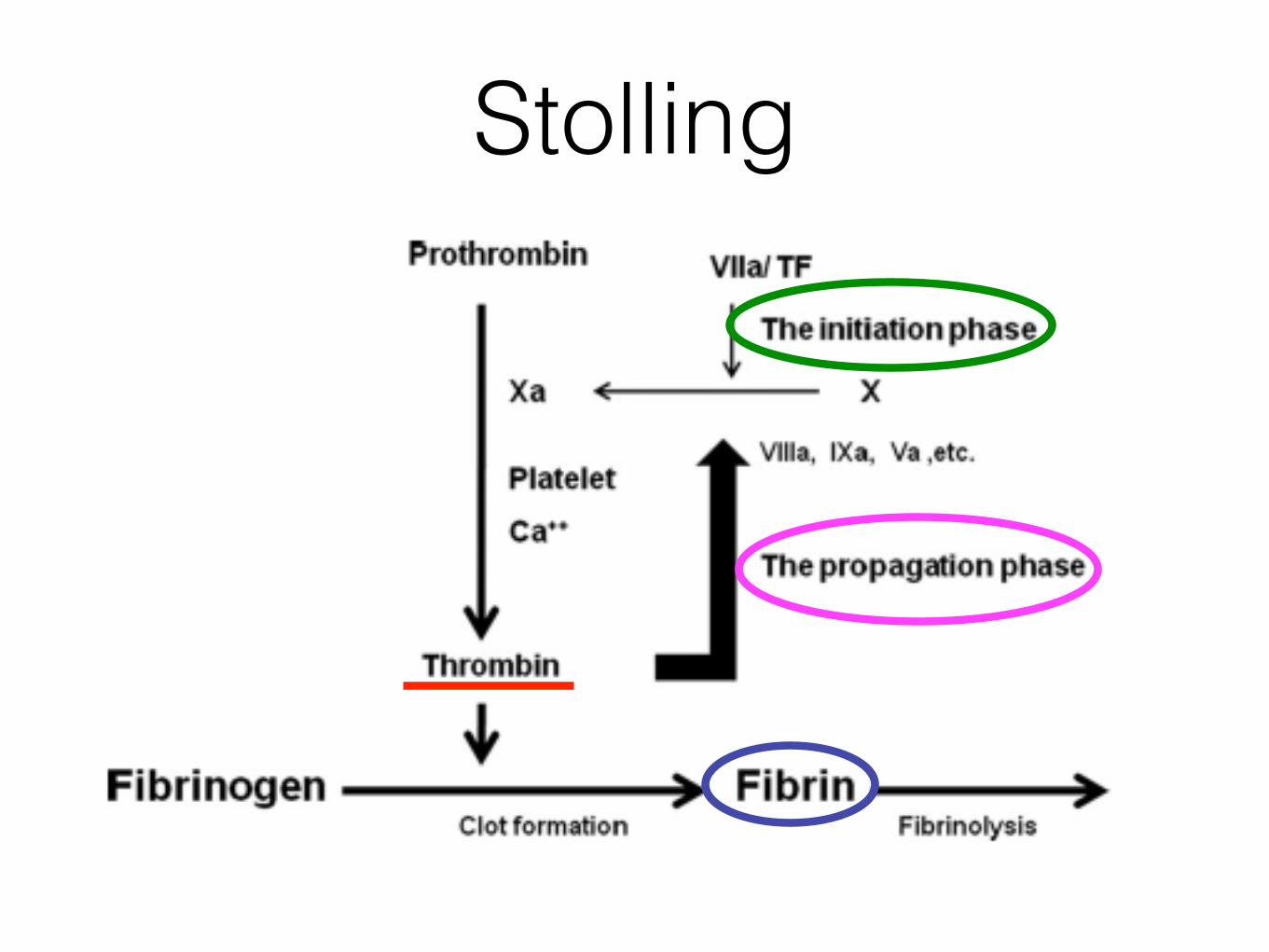
Stolling
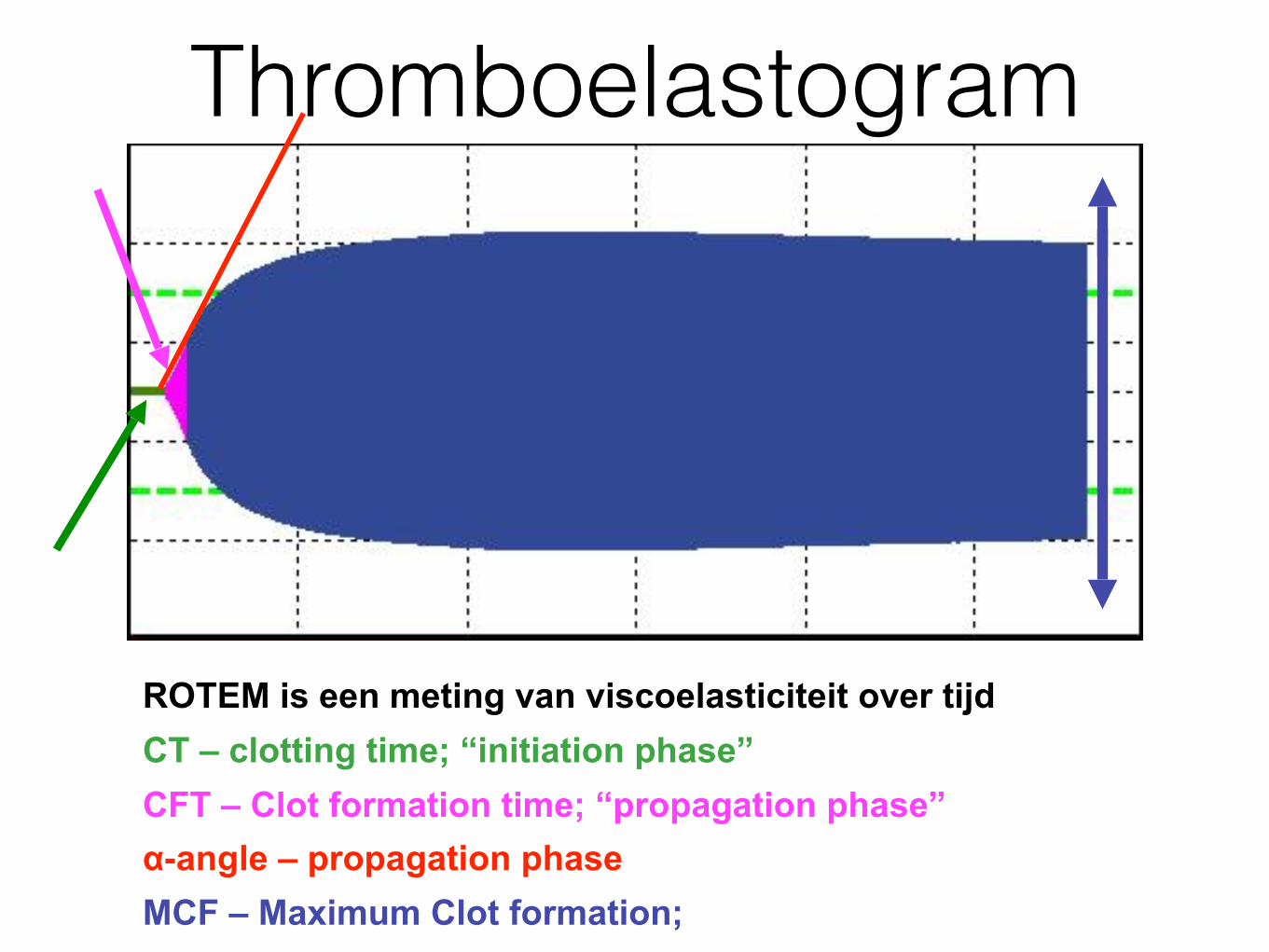
Thromboelastogram
ROTEM is een meting van viscoelasticiteit over tijd
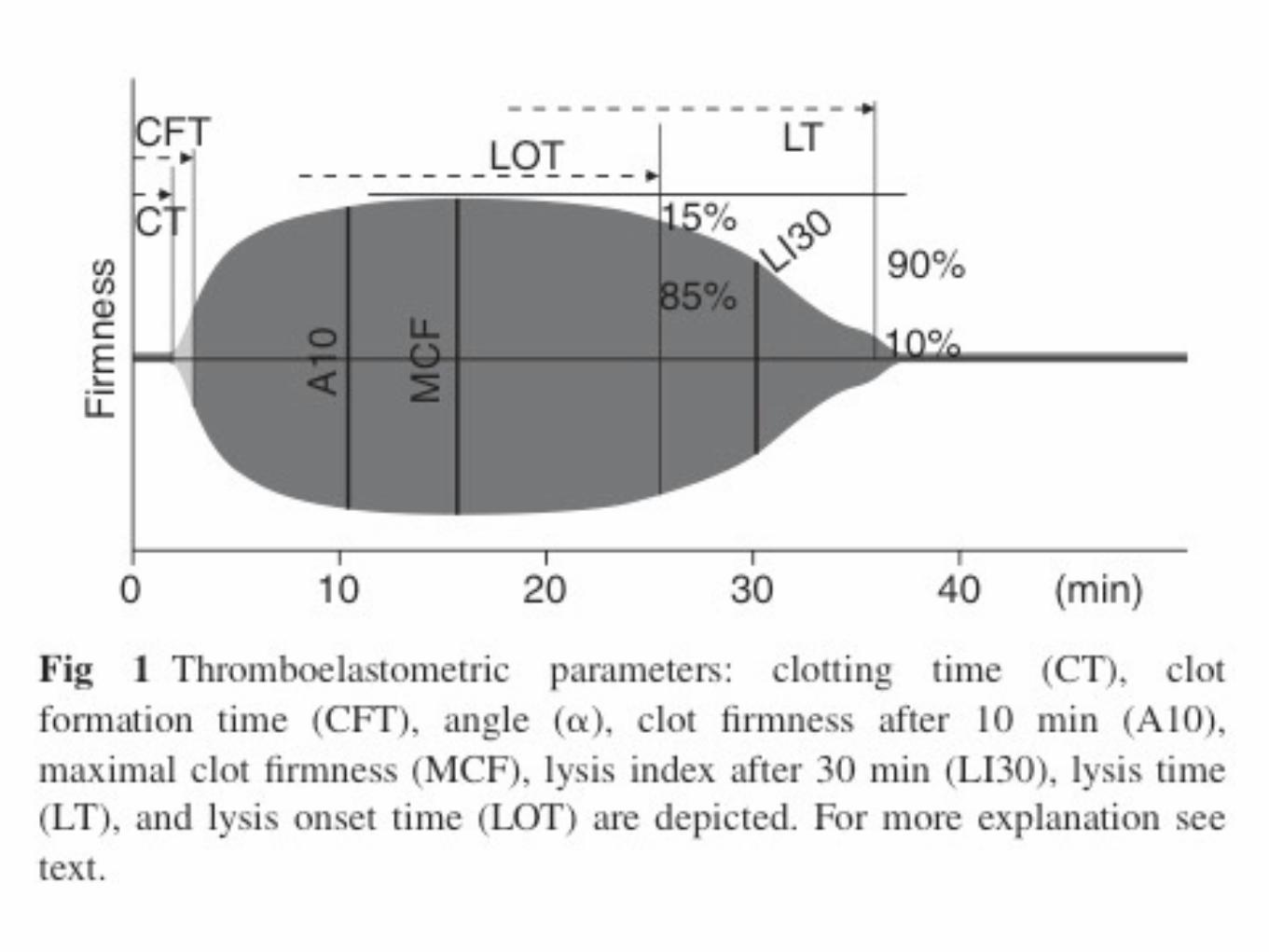
CT – clotting time; “initiation phase” CFT – Clot formation time; “propagation phase” α-angle – propagation phase MCF – Maximum Clot formation;
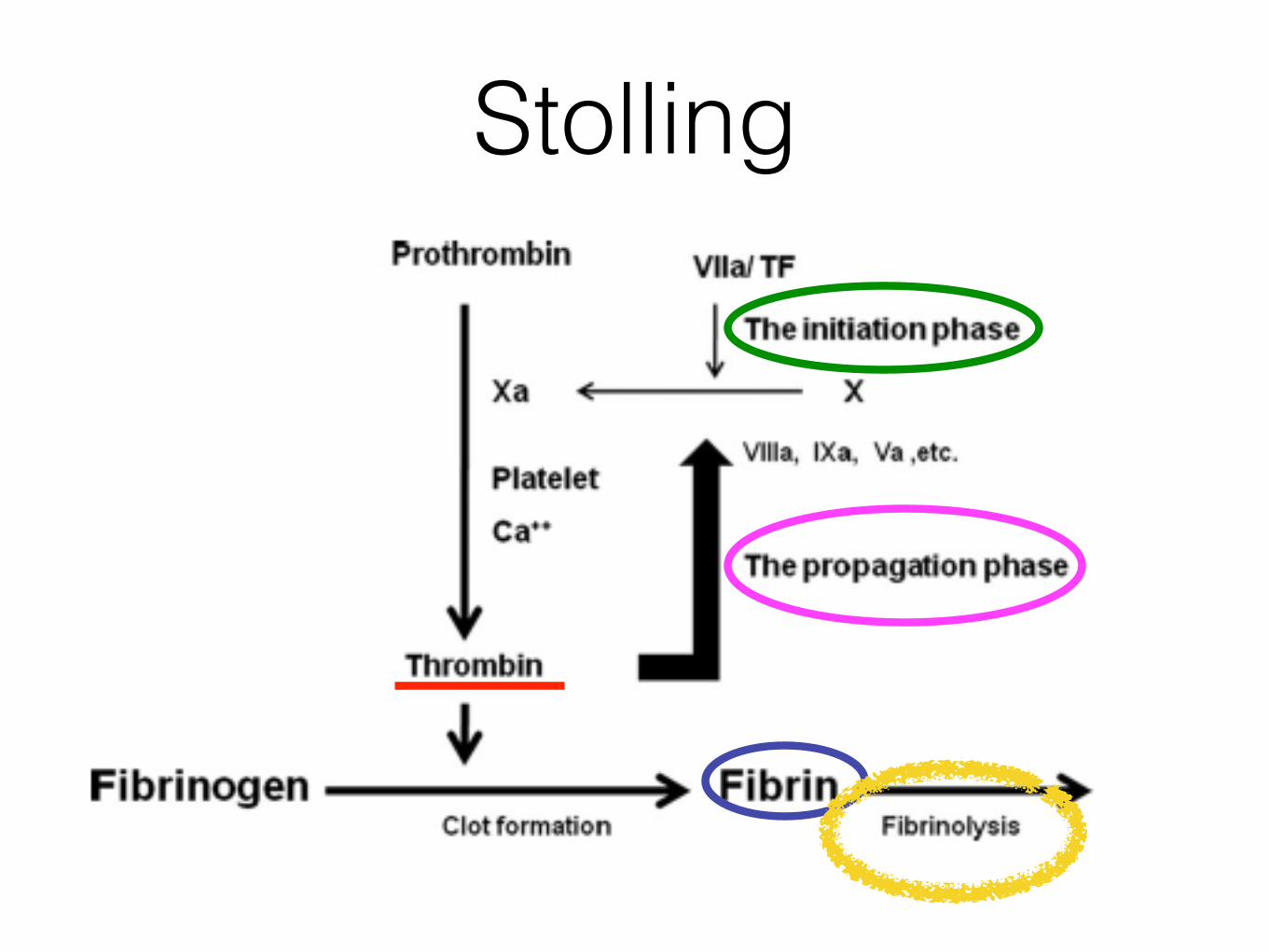
Stolling
Thromboelastogram
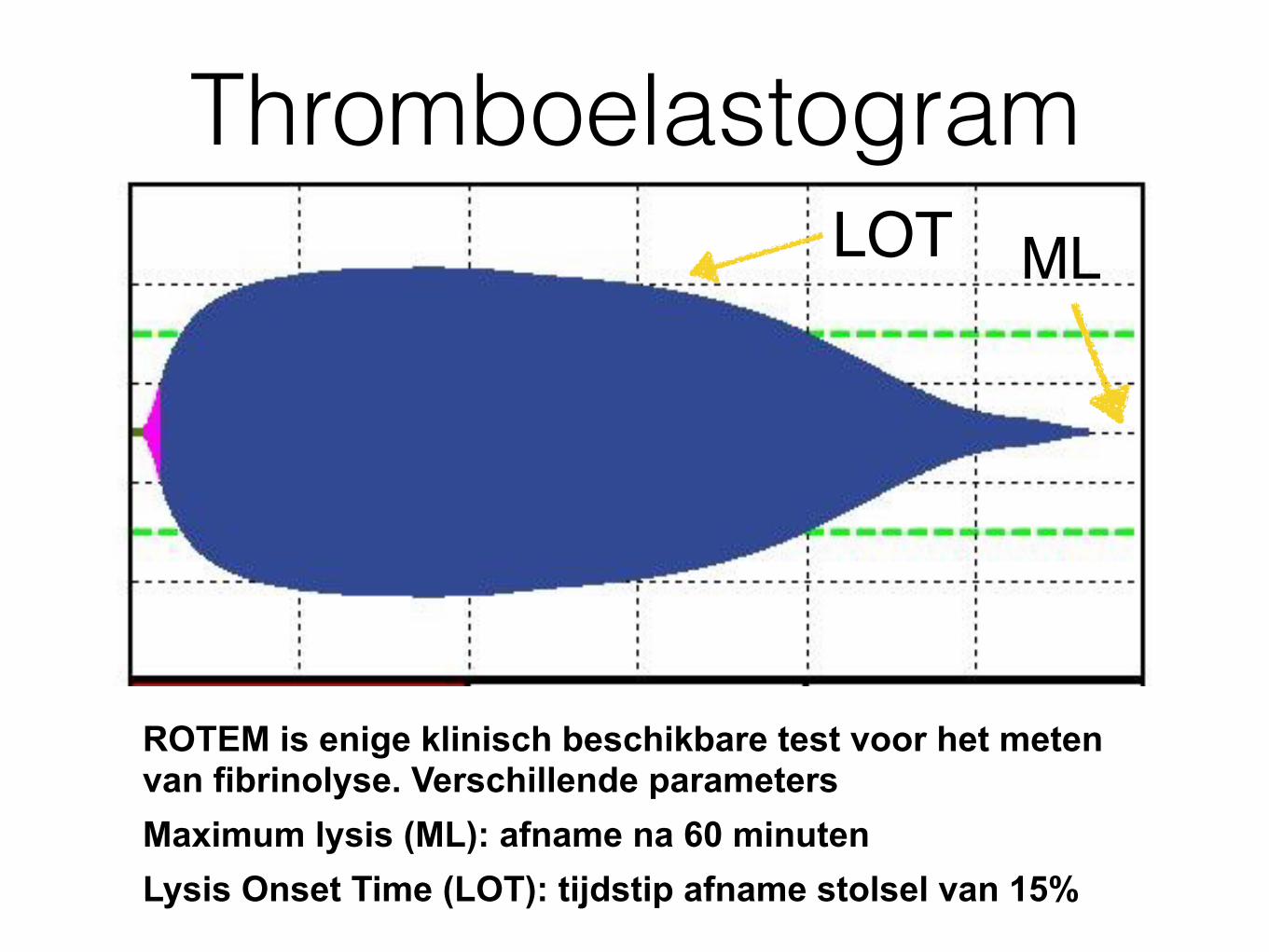
ROTEM is enige klinisch beschikbare test voor het meten van fibrinolyse. Verschillende parameters Maximum lysis (ML): afname na 60 minuten Lysis Onset Time (LOT): tijdstip afname stolsel van 15%
LOT ML
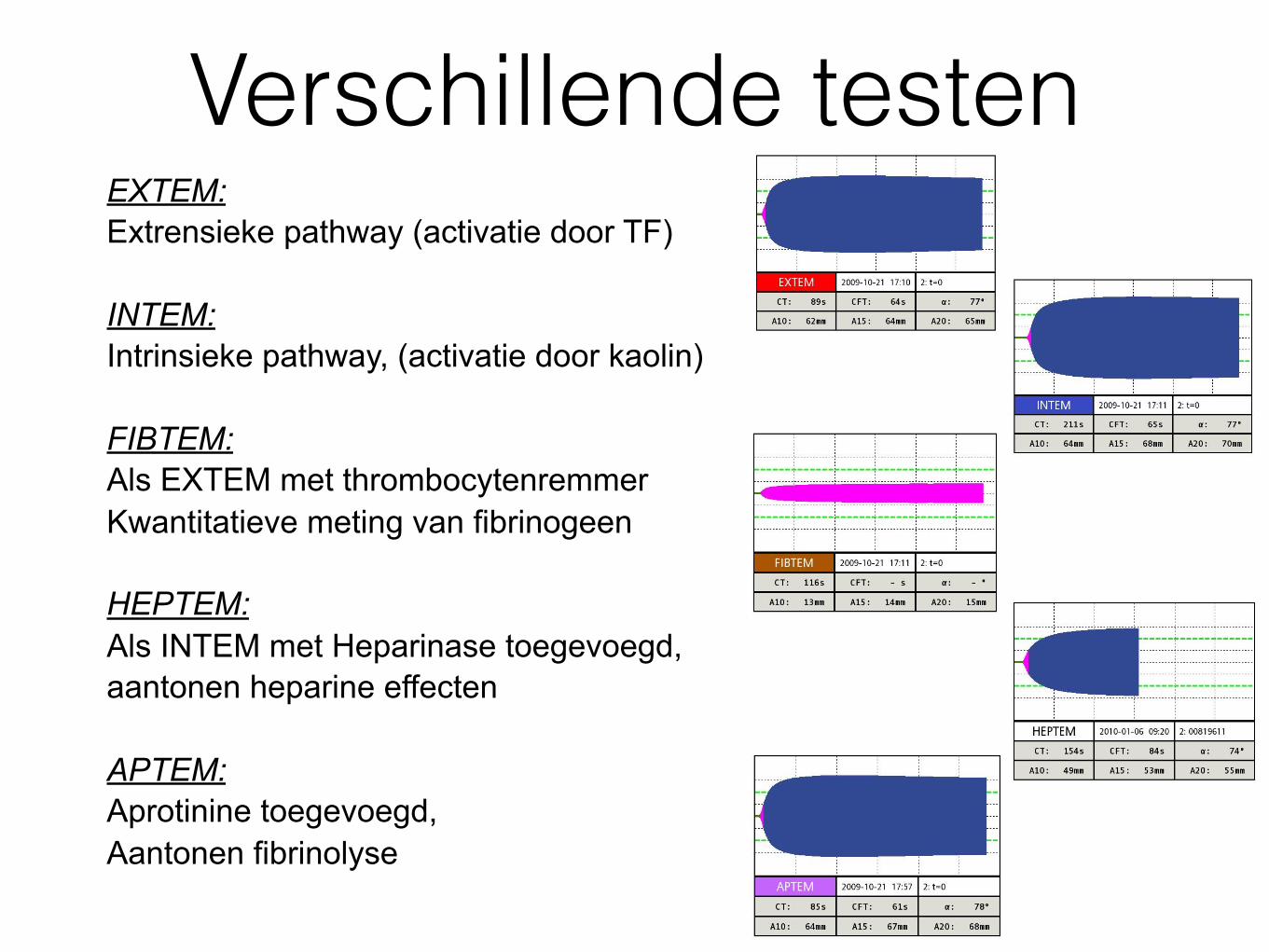
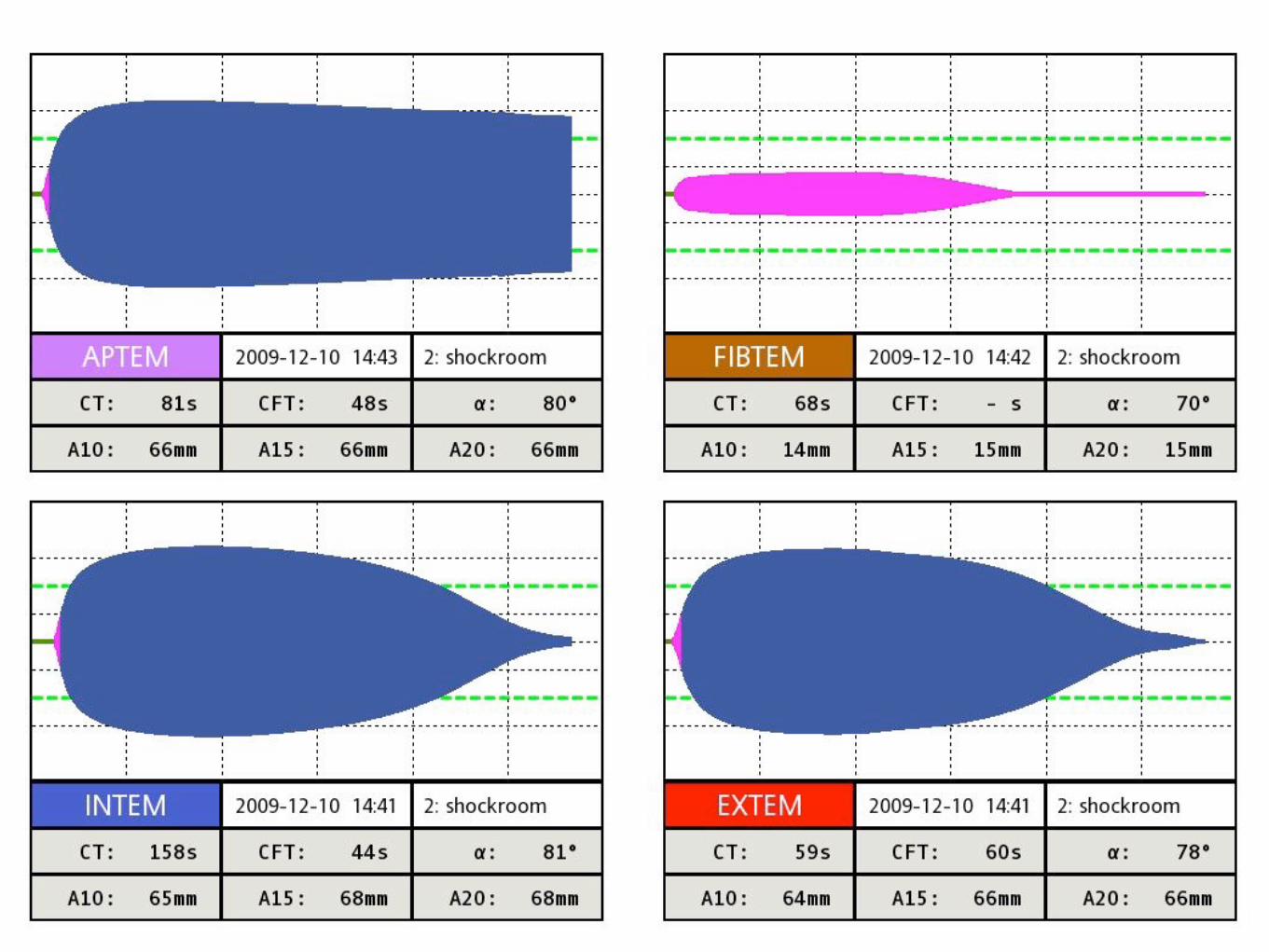
Verschillende testenEXTEM: Extrensieke pathway (activatie door TF)
INTEM: Intrinsieke pathway, (activatie door kaolin)
FIBTEM: Als EXTEM met thrombocytenremmer Kwantitatieve meting van fibrinogeen
HEPTEM: Als INTEM met Heparinase toegevoegd, aantonen heparine effecten
APTEM: Aprotinine toegevoegd, Aantonen fibrinolyse
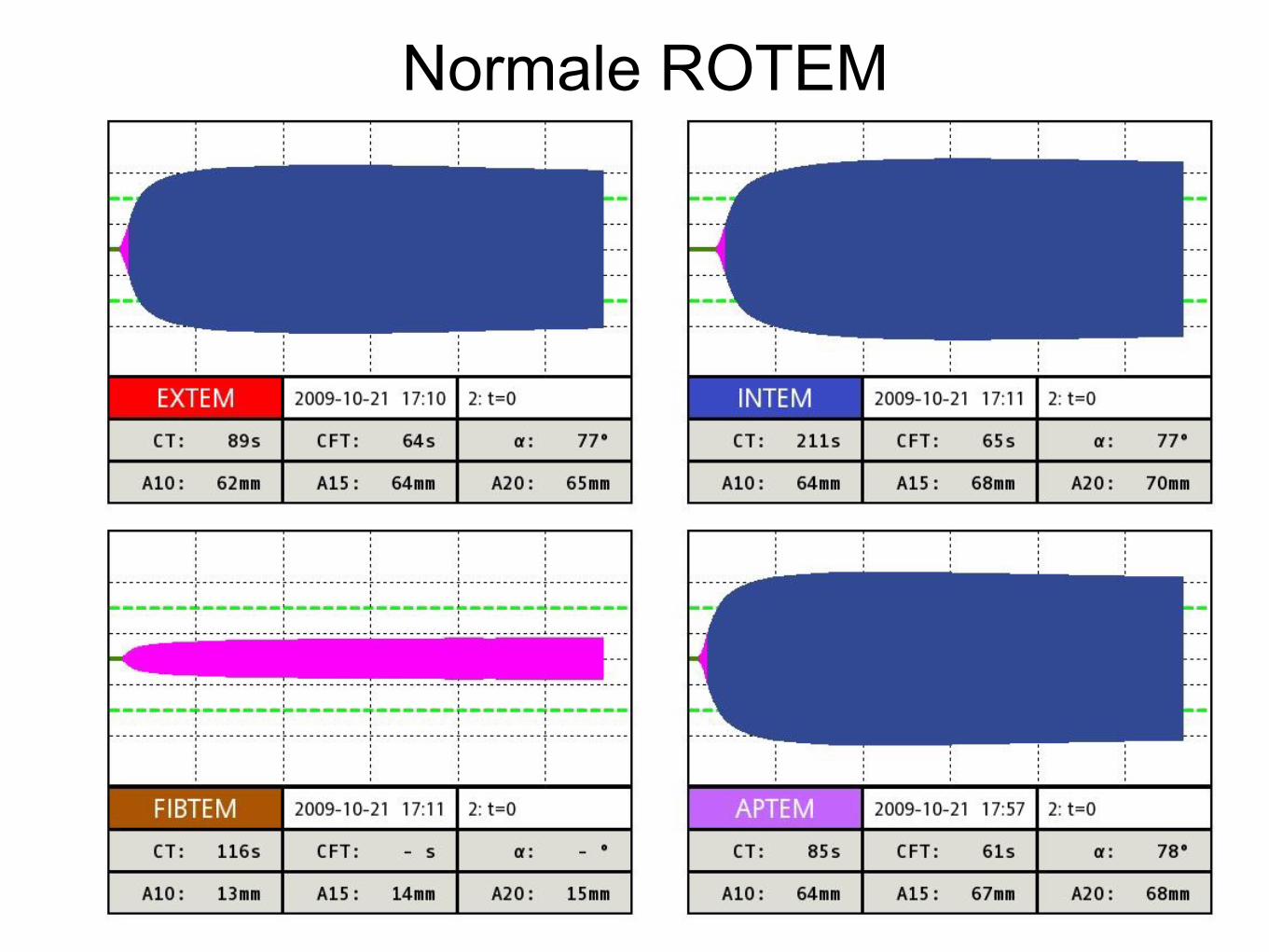
Normale ROTEM
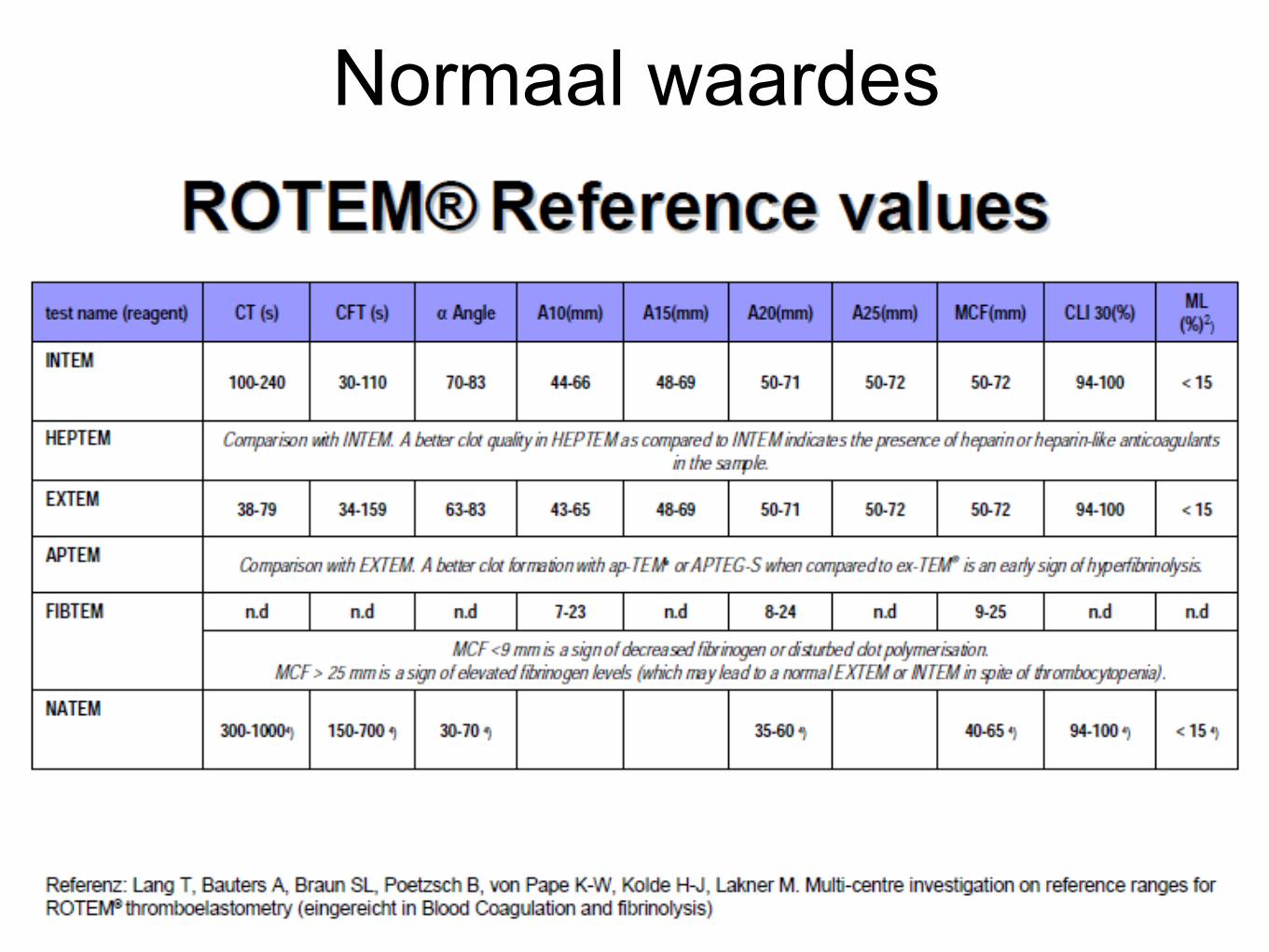
Normaal waardes
ROTEM Diagnoses
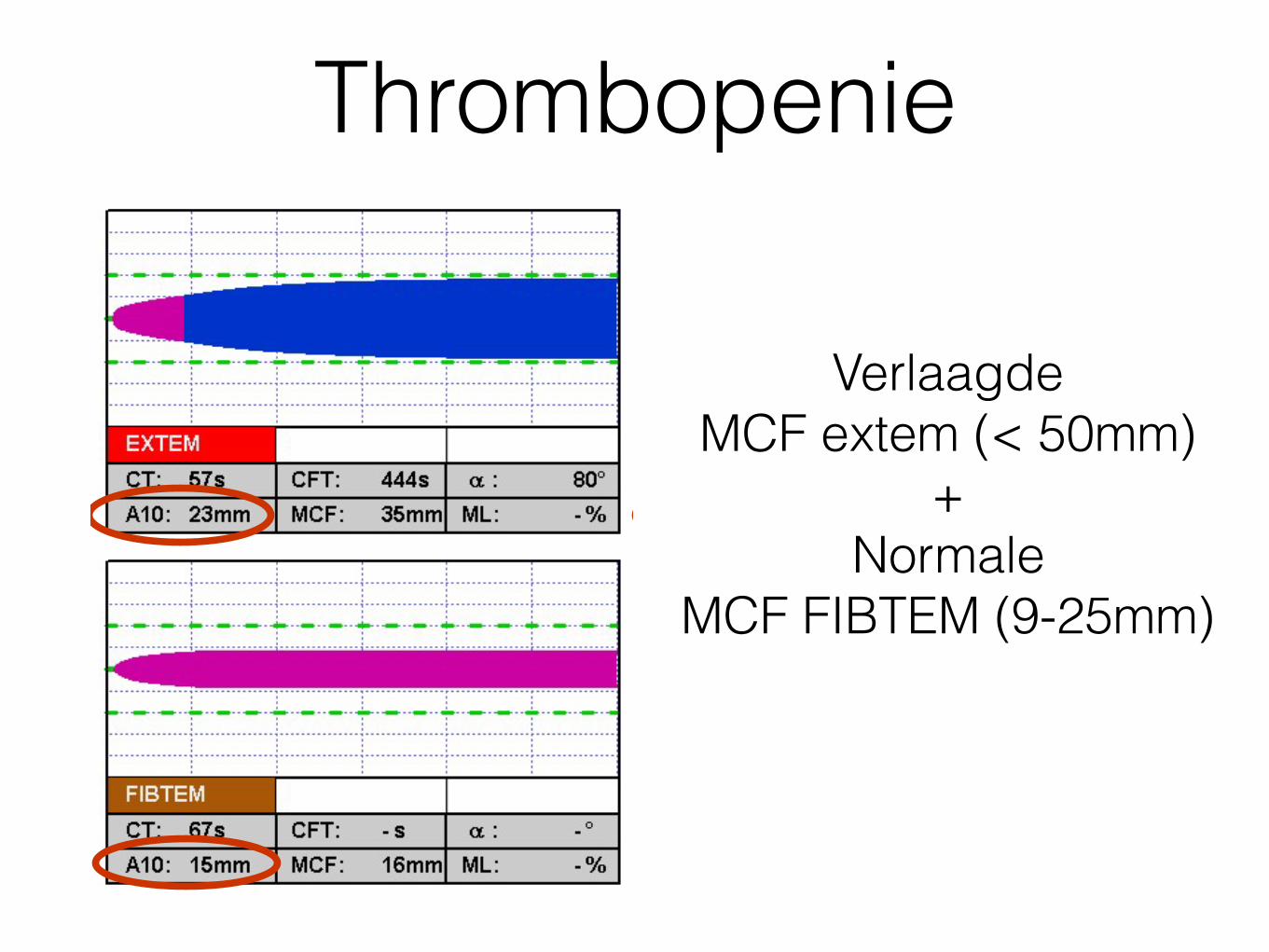
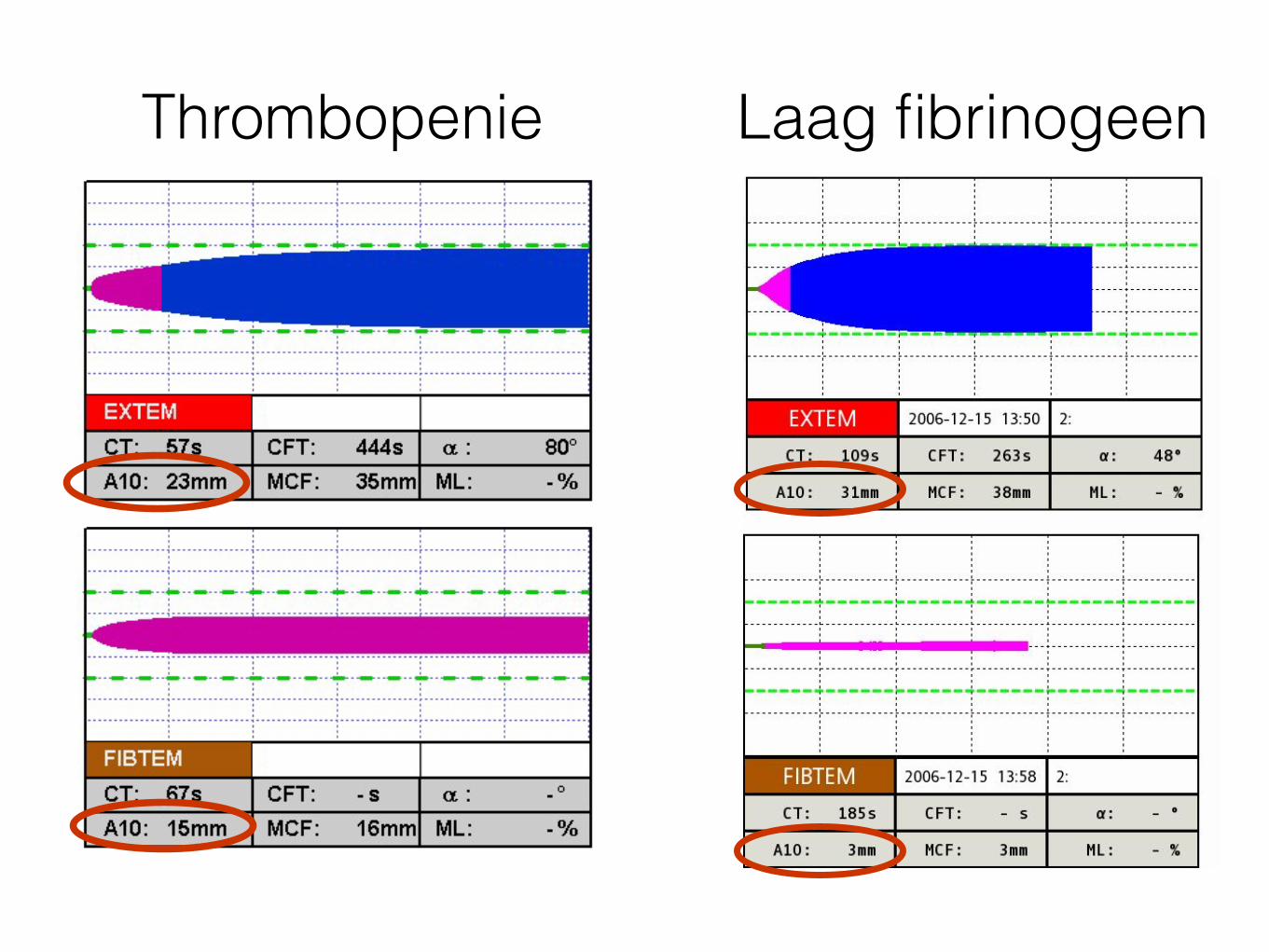
ThrombopenieEXTEM & INTEM : • Normal CT• Low amplitude
FIBTEM: •Normal amplitude
=> fibrinogen sufficient
APTEM ≈ EXTEM
=> No hyperfibrinolysis
Low amplitude in EXTEM & INTEM due tolow platelet count or platelet malfunction
&
Platelet deficiency
Verlaagde MCF extem (< 50mm)
+ Normale
MCF FIBTEM (9-25mm)
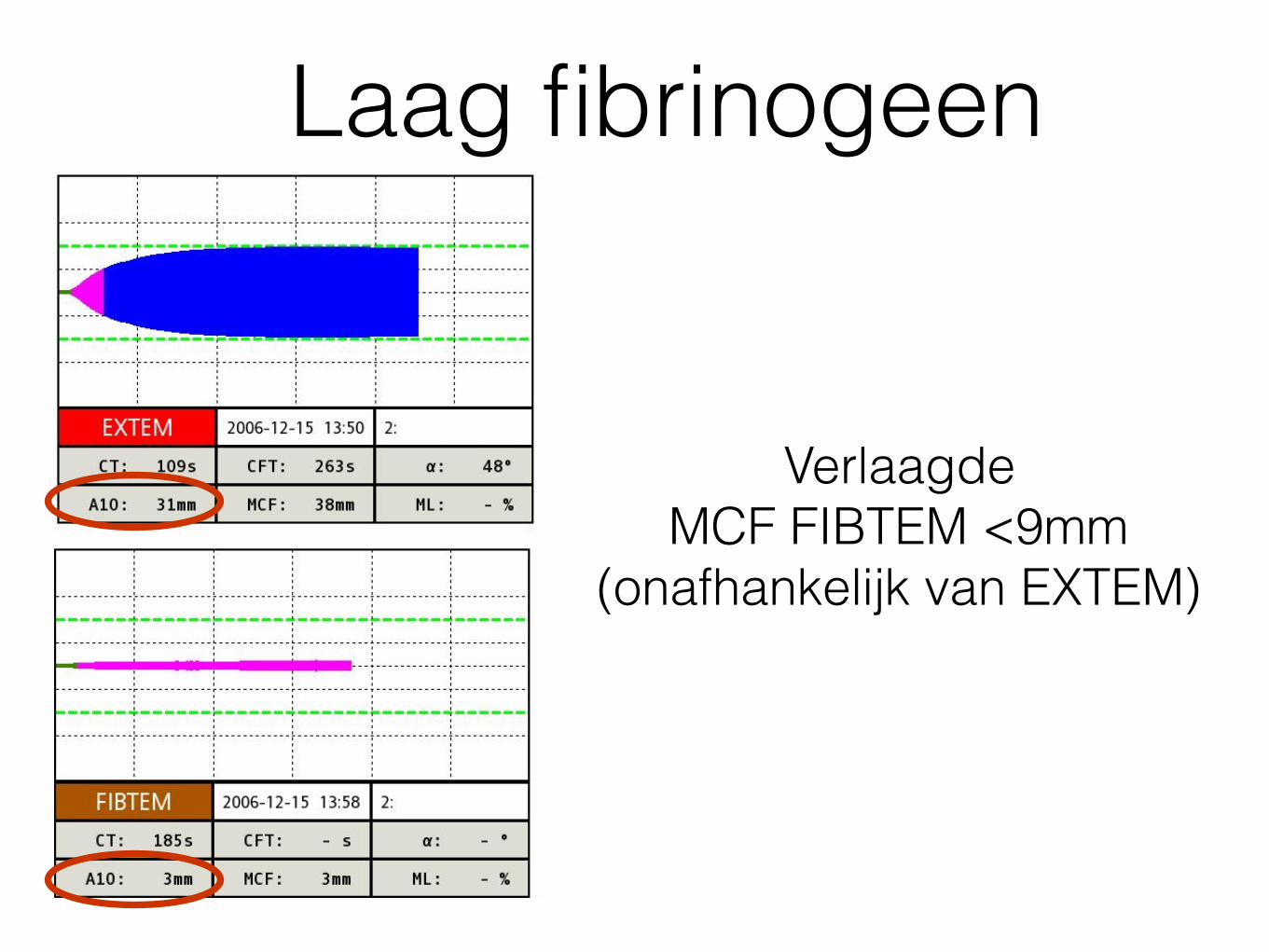
Laag fibrinogeenEXTEM & INTEM : •Normal CT•Low amplitude
APTEM ≈ EXTEM
=> No hyperfibrinolysis
FIBTEM: Low amplitude =>Low fibrinogen
Low amplitude seen in INTEM & EXTEM due tofibringen deficiency
&
Fibrinogen deficiency
Verlaagde MCF FIBTEM <9mm
(onafhankelijk van EXTEM)
EXTEM & INTEM : •Normal CT•Low amplitude
APTEM ≈ EXTEM
=> No hyperfibrinolysis
FIBTEM: Low amplitude =>Low fibrinogen
Low amplitude seen in INTEM & EXTEM due tofibringen deficiency
&
Fibrinogen deficiency
EXTEM & INTEM : • Normal CT• Low amplitude
FIBTEM: •Normal amplitude
=> fibrinogen sufficient
APTEM ≈ EXTEM
=> No hyperfibrinolysis
Low amplitude in EXTEM & INTEM due tolow platelet count or platelet malfunction
&
Platelet deficiencyThrombopenie Laag fibrinogeen
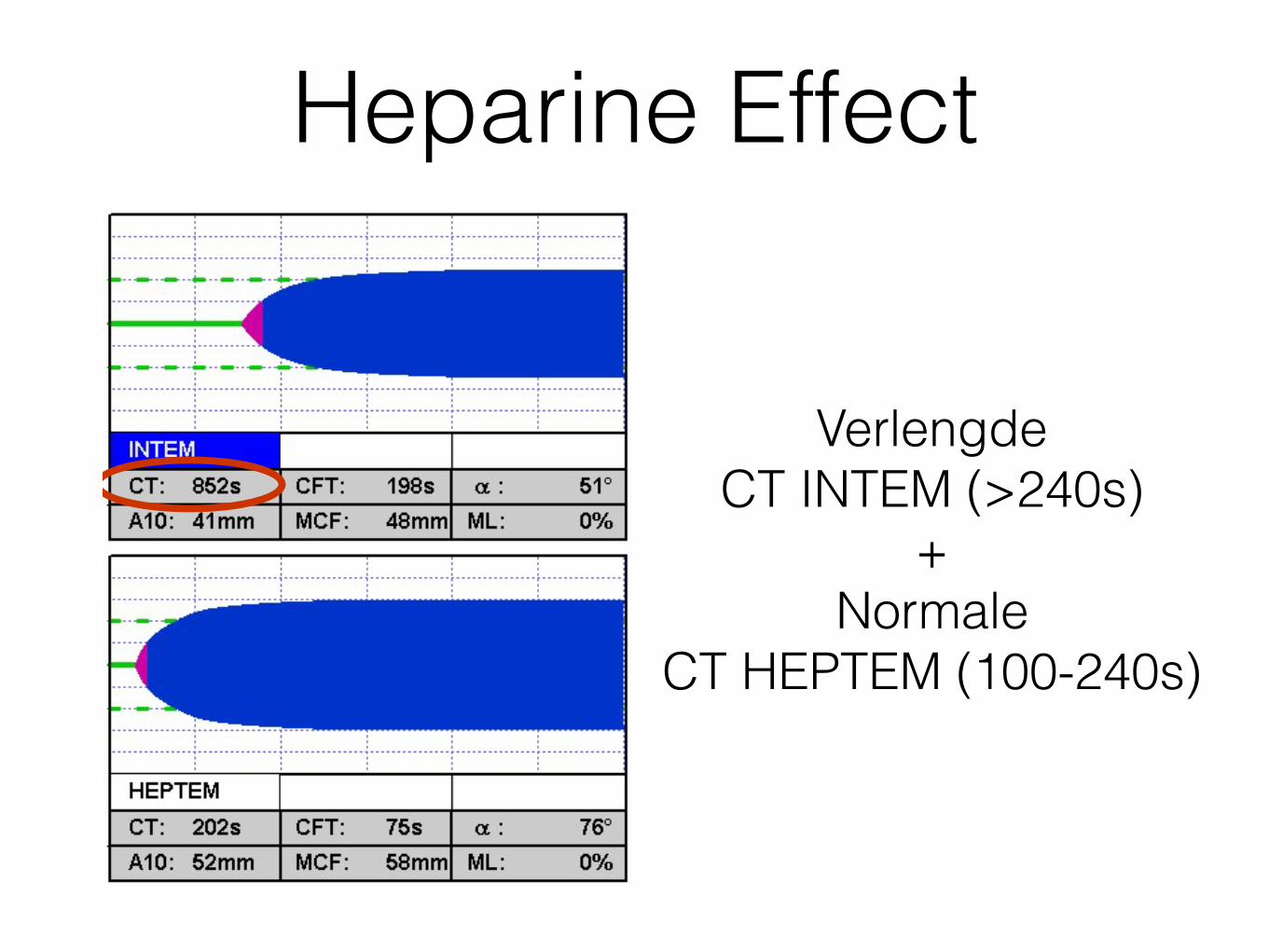
Heparine EffectEXTEM: normal, insensitive to heparin,ruling out fibrinogen or platelet influenceon amplitude
INTEM: •Long CT => due to heparin influence or factor deficiency => Check HEPTEM•Slightly low amplitude => due to heparin influence or platelet or fibrinogen deficiency=> check FIBTEM & HEPTEM
FIBTEM:Normal => sufficient fibrinogen available
HEPTEM: (with heparinase)•CT and CFT back to normal=> long CT in INTEM due to heparin
•Amplitude back to normal=> low amplitude in INTEM due to heparin
Note: in case a long INTEM CT is not corrected by HEPTEM , then the prolonged CT is generallydue to factor deficiency (keep in mind that factor deficiency is only detected when approx. <30% factors are left). Also consider a protamin overdose in such cases.
Heparin influence
Verlengde CT INTEM (>240s)
+ Normale
CT HEPTEM (100-240s)
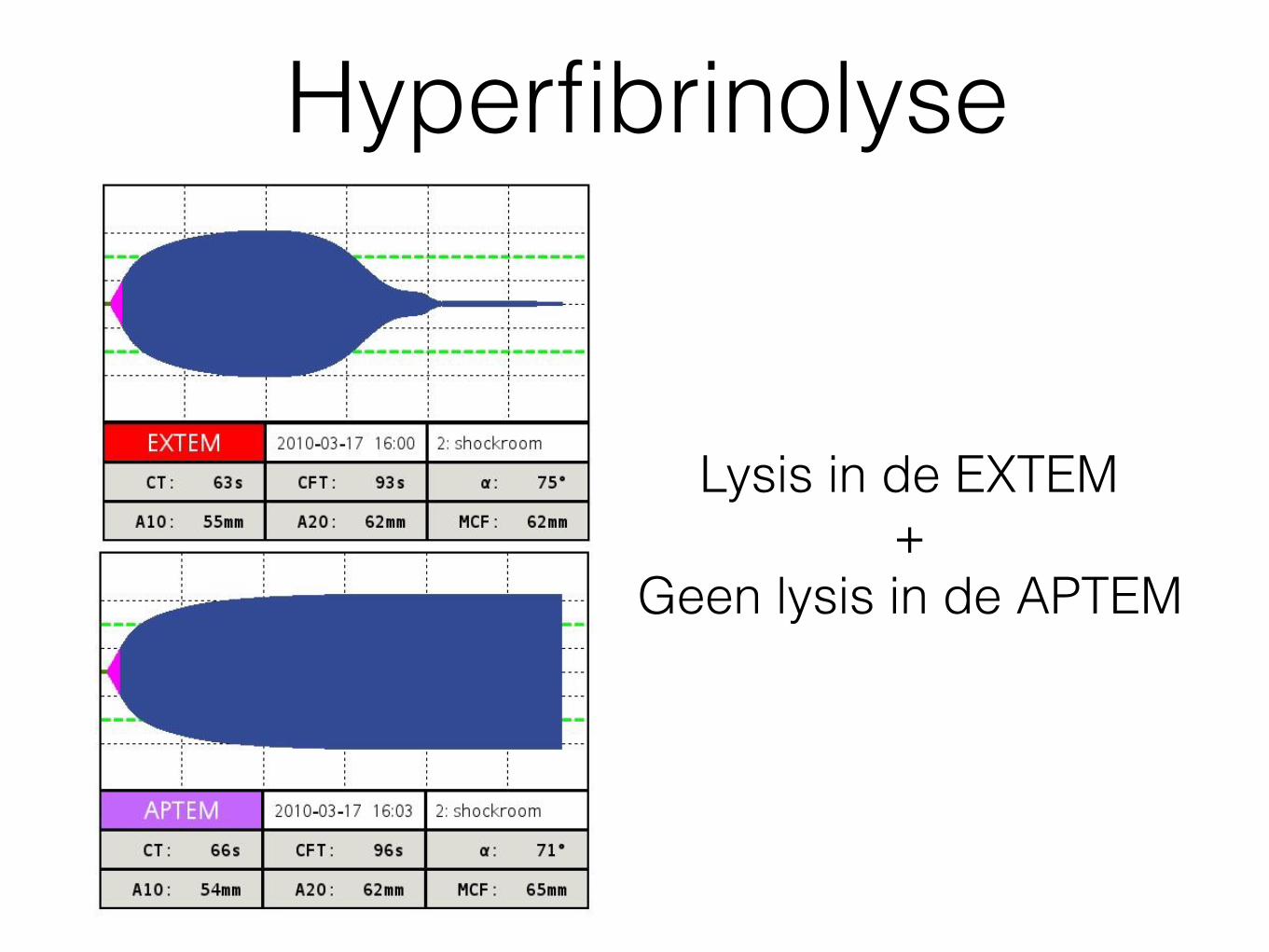
Hyperfibrinolyse
Lysis in de EXTEM+
Geen lysis in de APTEM
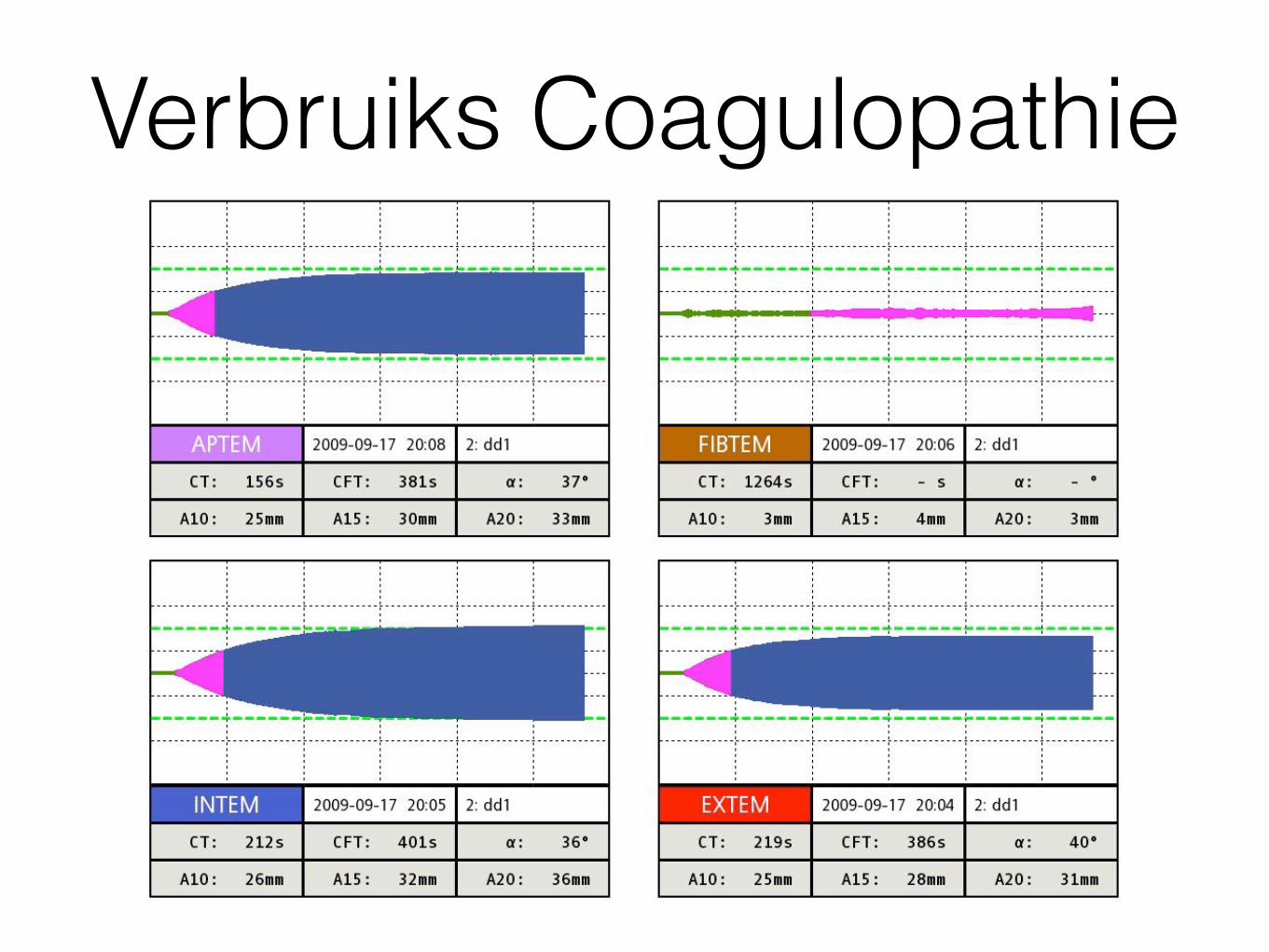
Verbruiks Coagulopathie
ROTEM Casuïstiek
Casus
• Vrouw 70 jaar, blanco VG, geen med. • Thuis onwel • Type A dissectie
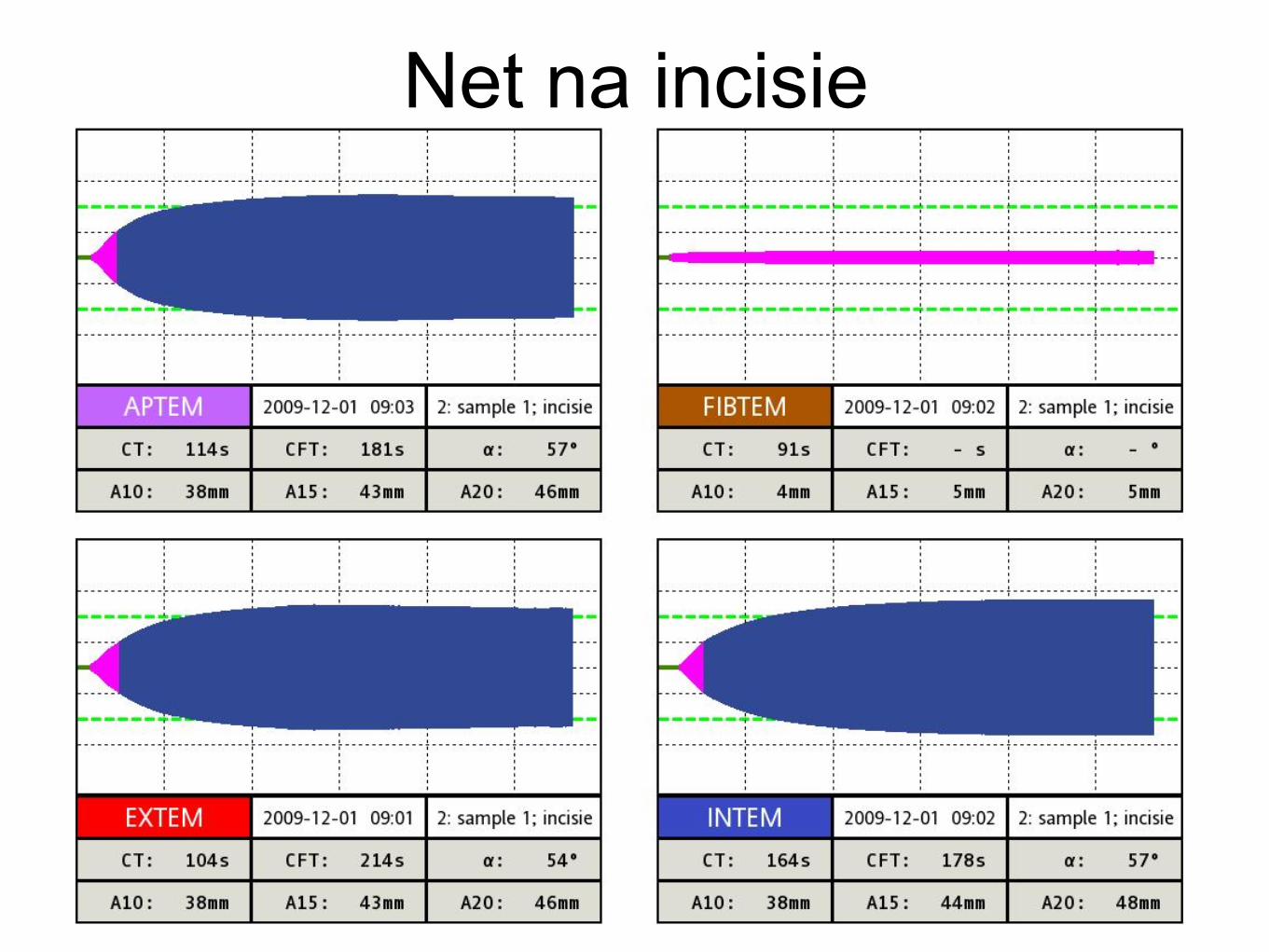
Net na incisie
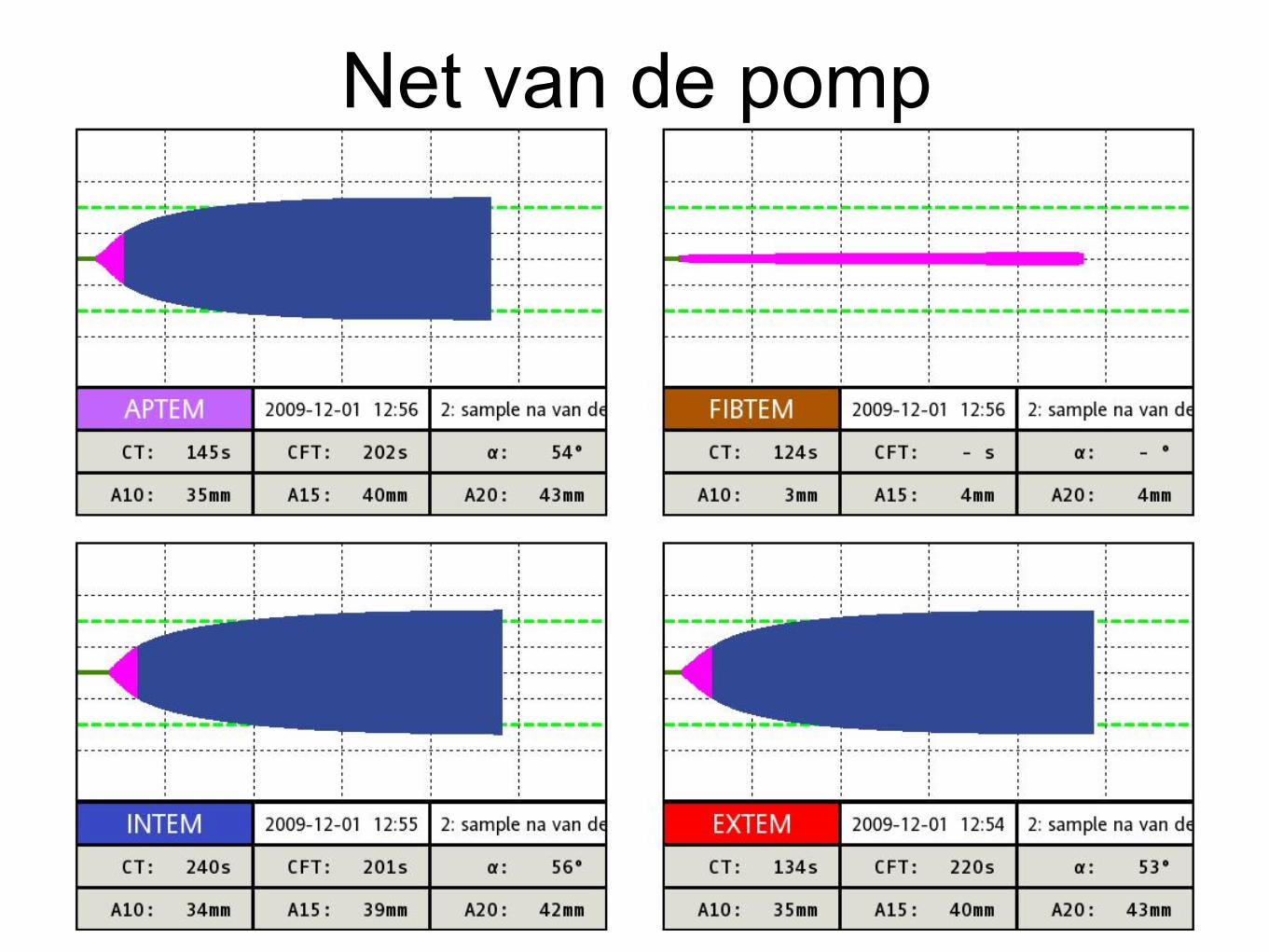
Net van de pomp
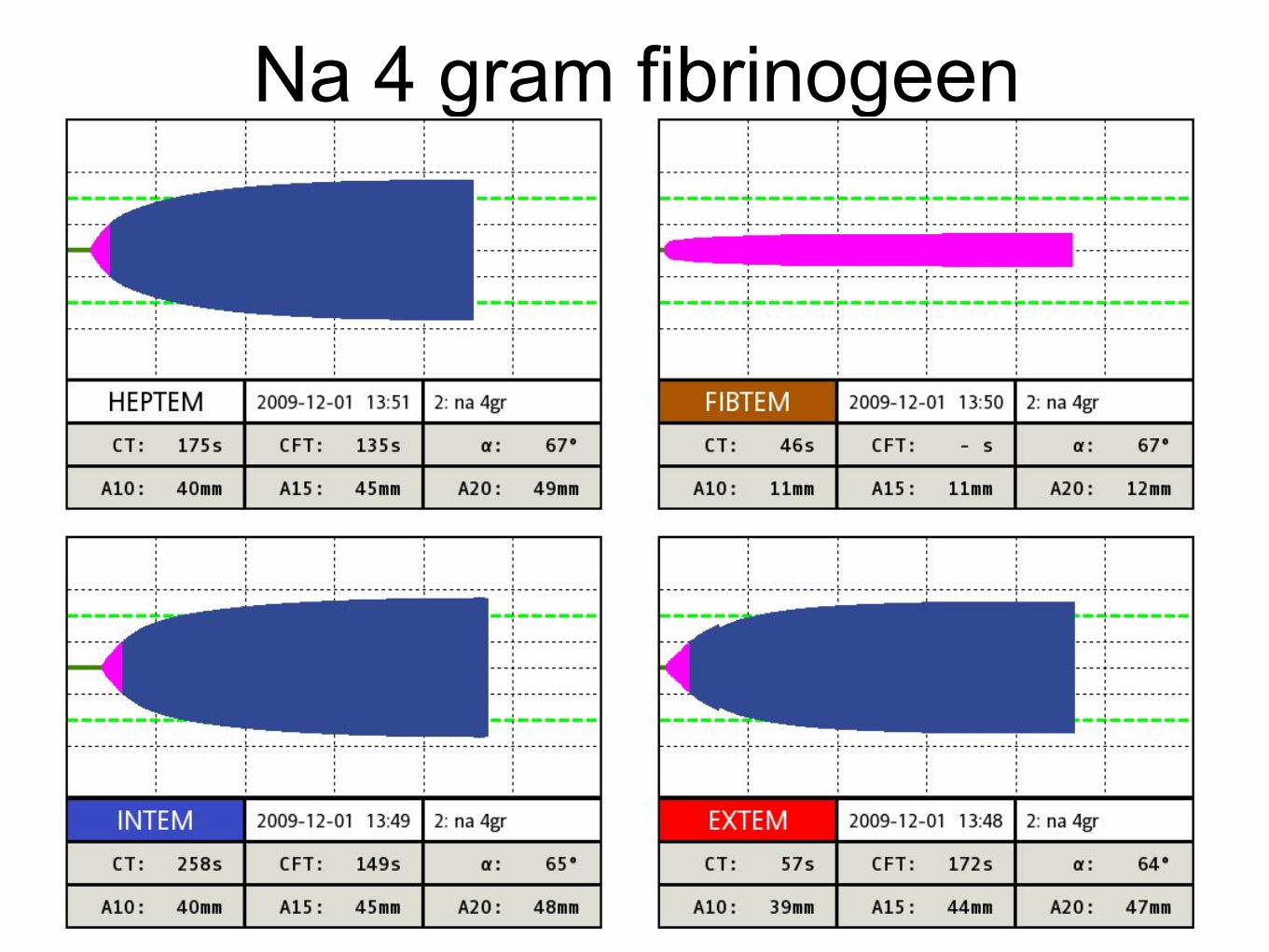
Na 4 gram fibrinogeen
Trauma patient
• Car vs scooter • Thrown from his scooter and into a steel
fence with his head (no helmet) • GCS 3, SpO2 70%, gasping, pin-point
pupils left and right, • Severe traumatic brain injury and open tib-
fib fracture

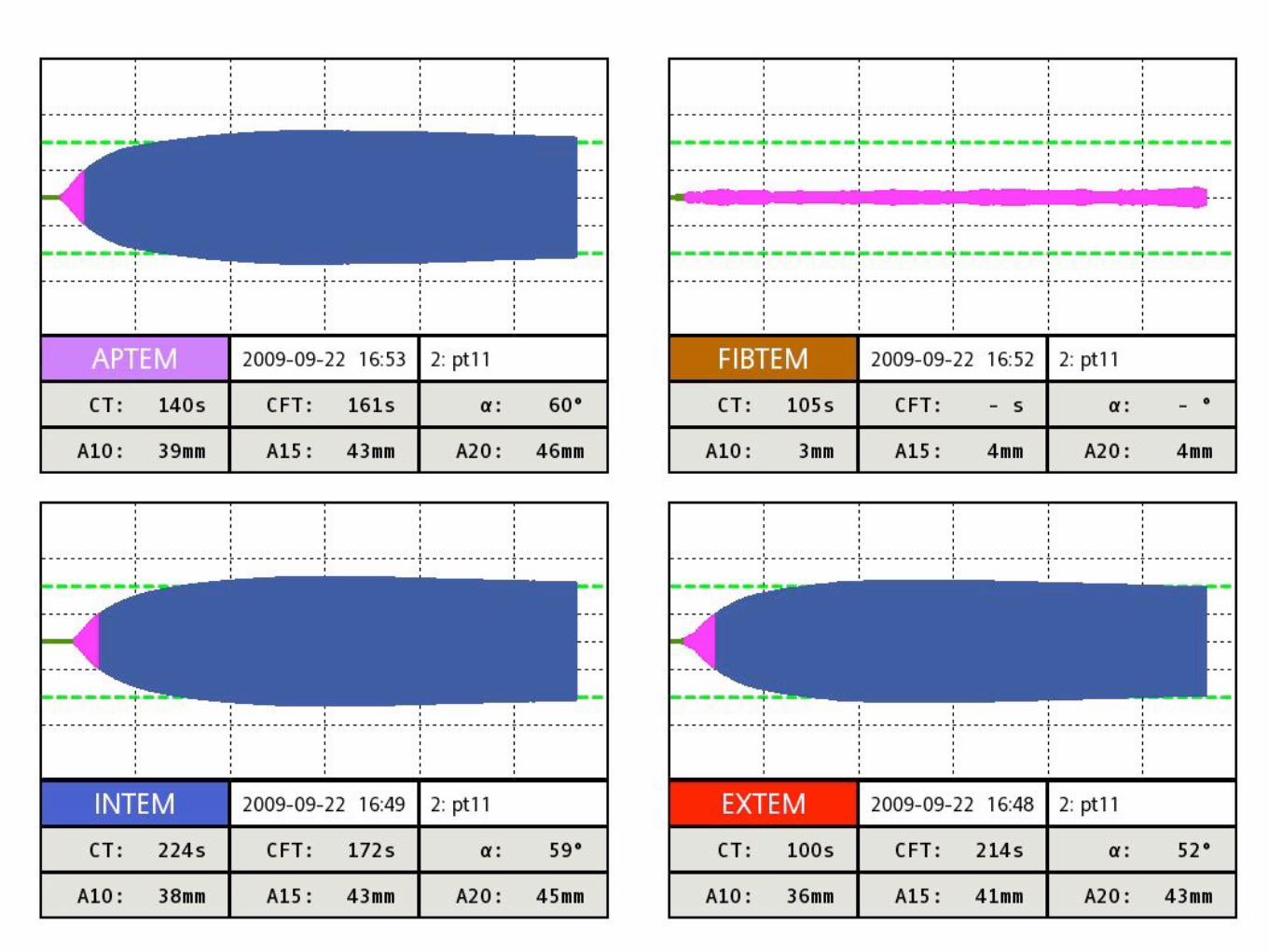
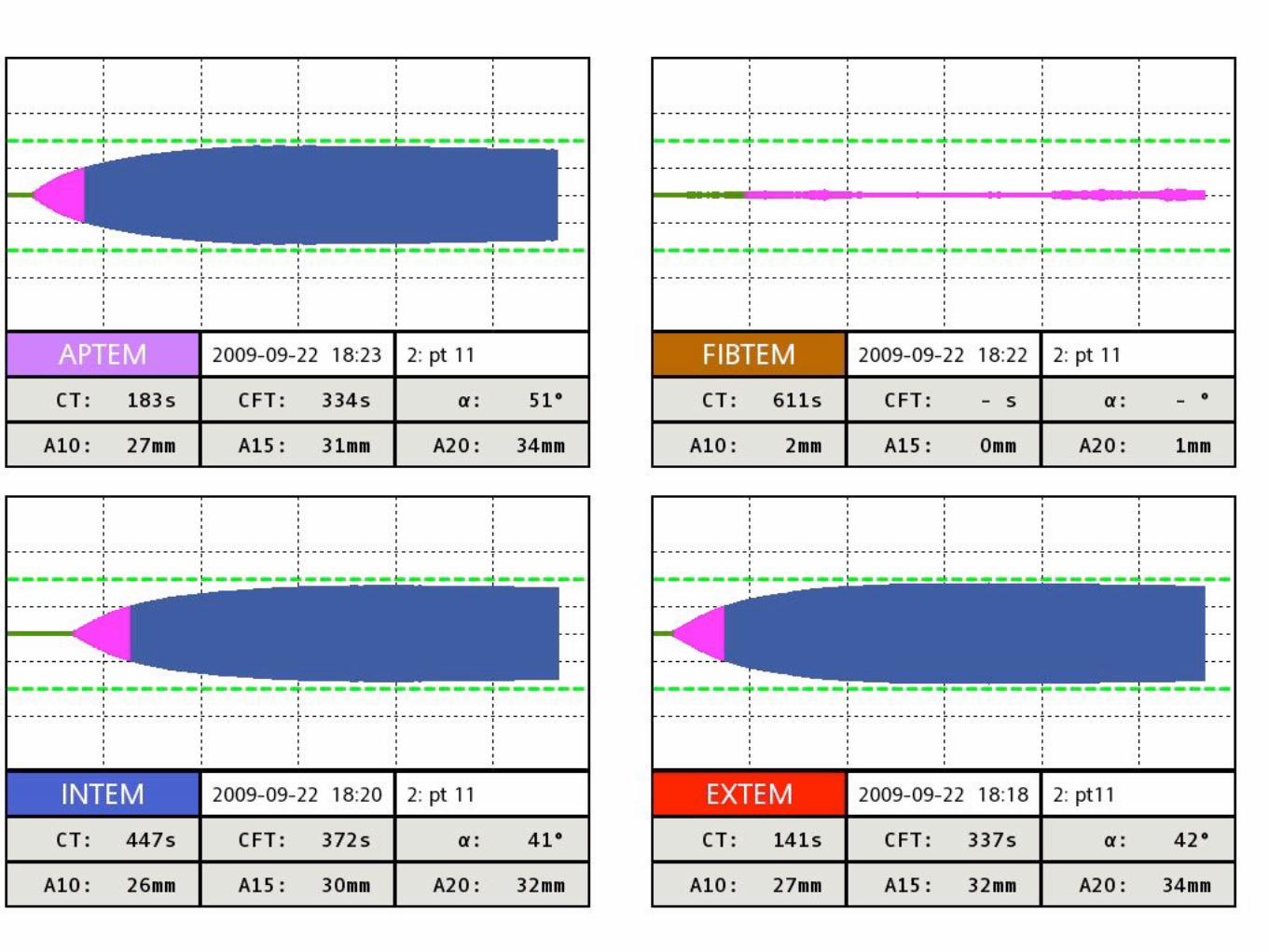
Multi-trauma patient
• Pedestrian hit by a bus on highway A22 • Intubated at the scene • Epidural and subdural hematoma • Traumatic aortic disection • Tension pneumothorax left and right • Femur # and tib-fib # • Liver lacerations
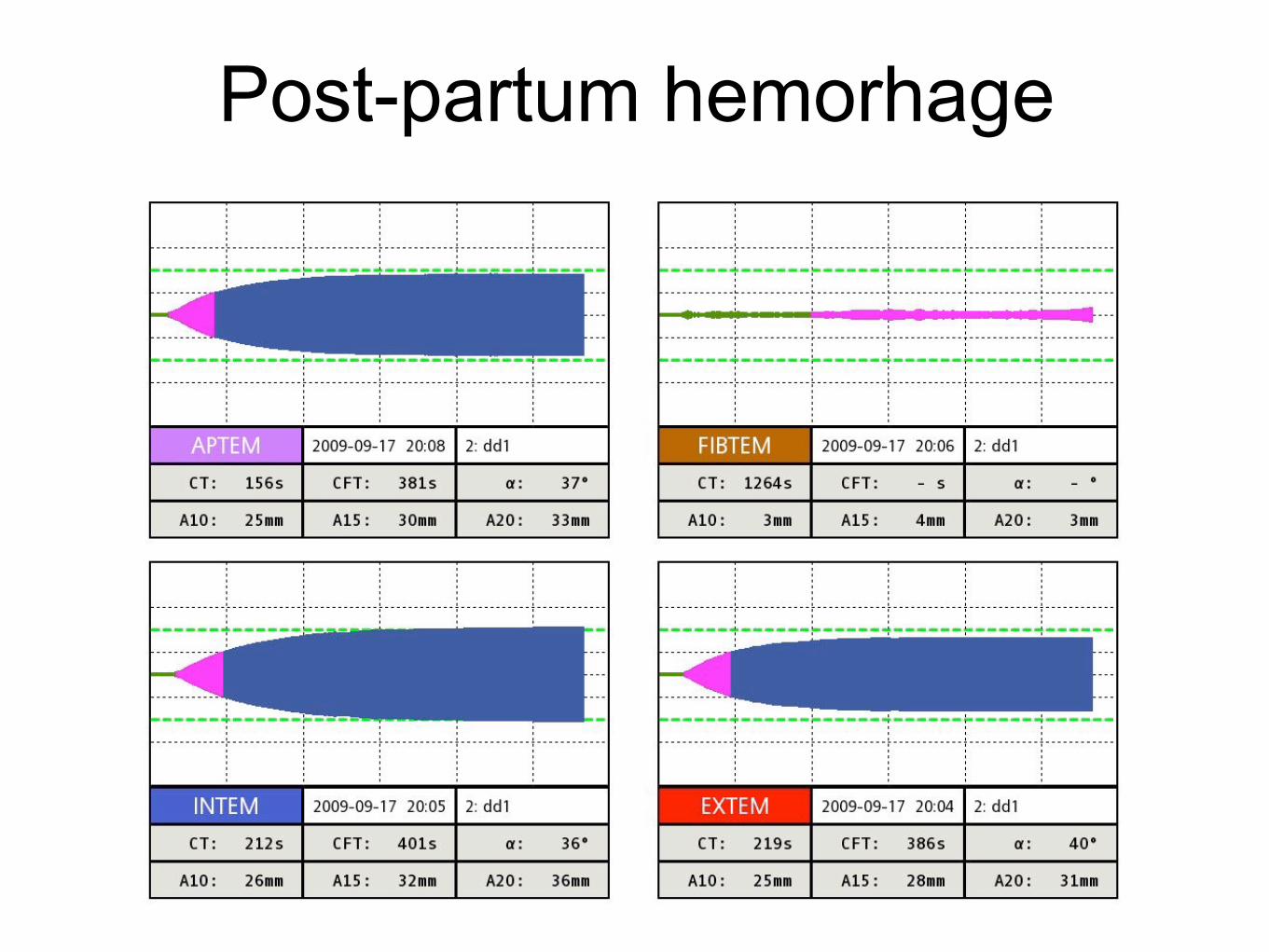
Post-partum hemorhage
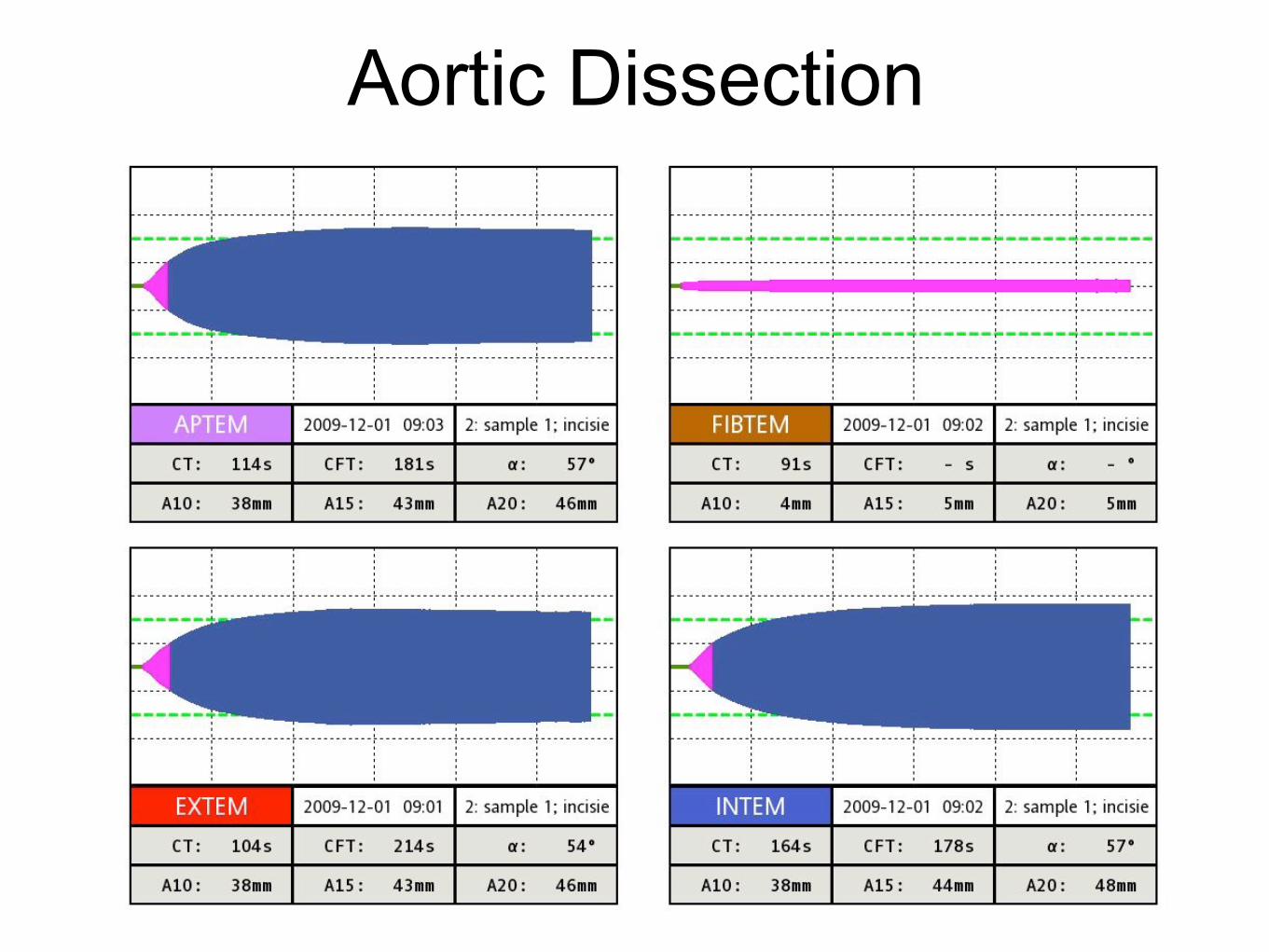
Aortic Dissection
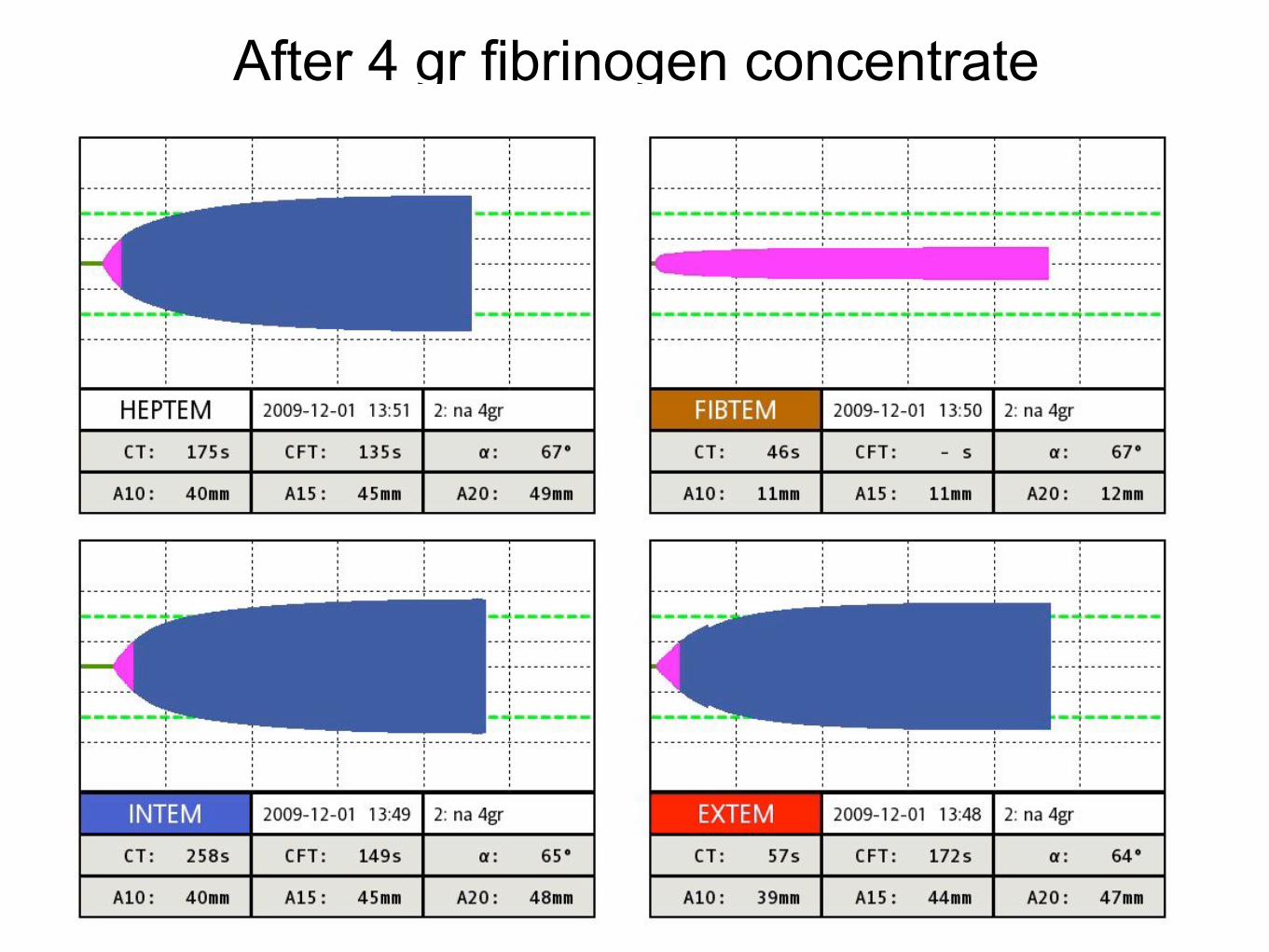
After 4 gr fibrinogen concentrate
Out-of-hospital cardiac arrest
• Male, 82 yrs, witnessed arrest, immediate start of BLS,
• First rhythm VF, 3x ECV, then PEA, • no ROSC, died in the ER
ROTEMversus
INR/aPTT/Fibr
Usefulness of standard plasma coagulation testsin the management of perioperative coagulopathicbleeding: is there any evidence?T. Haas1*, D. Fries2, K. A. Tanaka3, L. Asmis4, N. S. Curry5 and H. Schochl6,7
1 Department of Anaesthesia, University Children’s Hospital Zurich, Steinwiesstrasse 75, 8032 Zurich, Switzerland2 Department of General and Surgical Critical Care Medicine, Innsbruck Medical University, Anichstrasse 35, 6020 Innsbruck, Austria3 Department of Anesthesiology, University of Pittsburgh Medical Center, 200 Lothrop Street, PUH C-215, Pittsburgh, PA, USA4 Unilabs, Coagulation Lab and Centre for Perioperative Thrombosis and Hemostasis, Hufgasse 17, 8008 Zurich, Switzerland5 Oxford Haemophilia and Thrombosis Centre, Oxford University Hospitals NHS Trust, Oxford, UK6 Department of Anaesthesiology and Intensive Care Medicine, AUVA Trauma Centre, Salzburg Academic Teaching Hospital of the ParacelsusMedical University, Salzburg, Austria7 Ludwig Boltzmann Institute for Experimental and Clinical Traumatology, Vienna, Austria
* Corresponding author. E-mail: [email protected]
Editor’s key points
† The authors review theevidence for thecontinued use of standardlaboratory tests ofcoagulation.
† They conclude that thereis minimal evidence forthe use of standardlaboratory tests in guidingthe management ofperioperative bleeding.
Summary. Standard laboratory coagulation tests (SLTs) such as prothrombin time/international normalized ratio or partial thromboplastin time are frequently used to assesscoagulopathy and to guide haemostatic interventions. However, this has been challengedby numerous reports, including the current European guidelines for perioperative bleedingmanagement, which question the utility and reliability of SLTs in this setting. Furthermore,the arbitrary definition of coagulopathy (i.e. SLTs are prolonged by more than 1.5-fold) hasbeen questioned. The present study aims to review the evidence for the usefulness of SLTsto assess coagulopathy and to guide bleeding management in the perioperative andmassive bleeding setting. Medline was searched for investigations using results of SLTs as ameans to determine coagulopathy or to guide bleeding management, and the outcomes(i.e. blood loss, transfusion requirements, mortality) were reported. A total of 11 guidelinesfor management of massive bleeding or perioperative bleeding and 64 studies investigatingthe usefulness of SLTs in this setting were identified and were included for final datasynthesis. Referenced evidence for the usefulness of SLTs was found in only threeprospective trials, investigating a total of 108 patients (whereby microvascular bleeding wasa rare finding). Furthermore, no data from randomized controlled trials support the use ofSLTs. In contrast, numerous investigations have challenged the reliability of SLTs to assesscoagulopathy or guide bleeding management. There is actually no sound evidence fromwell-designed studies that confirm the usefulness of SLTs for diagnosis of coagulopathy orto guide haemostatic therapy.
Keywords: bleeding; blood; coagulation; coagulopathy; transfusion
Perioperative management of coagulopathic bleedingrequires timely haemostatic intervention using allogeneic bloodproducts, administration of coagulation factor concentrates,or both. To guide these interventions, fast laboratory workupis essential. If it comes to the question which laboratory testshould be performed to assess haemostasis, current guidelinesusually refer to standard plasma coagulation tests (SLTs),that is, prothrombin time (PT)/international normalized ratio(INR) and activated partial thromboplastin time,1 – 7 whileviscoelastic tests (i.e. thrombelastography) are less commonlyadvocated.7 Although the complete panel of standard co-agulation testing almost always covers additional measure-ments of fibrinogen and platelet count, interpretation of SLTsis most frequently used to assess coagulopathy. Generally
speaking, coagulopathy is presumed when SLTs are prolongedby more than 1.5-fold, although the evidence to supportthis degree of prolongation as diagnostic of coagulopathy islimited.
However, there are major limitations to these SLTs. Thesetests are time-consuming (with turnaround times sometimeslonger than 60 min)8 and, as a consequence, they are oftenomitted in situations of severe bleeding, where prompt treat-ment must be ensured. In addition, if the results of PT/aPTTare more than 1.5 times prolonged, the treatment optionsrange from transfusion of fresh-frozen plasma (FFP) to admin-istration of coagulation factor concentrates such as prothrom-bin complex concentrates (PCC) or activated recombinantfactor VII. Notably, all these treatment options may be linked
& The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
British Journal of Anaesthesia 114 (2): 217–24 (2015)Advance Access publication 8 September 2014 . doi:10.1093/bja/aeu303
at Vrije U
niversiteit Am
sterdam on January 23, 2015
http://bja.oxfordjournals.org/D
ownloaded from
Usefulness of standard plasma coagulation testsin the management of perioperative coagulopathicbleeding: is there any evidence?T. Haas1*, D. Fries2, K. A. Tanaka3, L. Asmis4, N. S. Curry5 and H. Schochl6,7
1 Department of Anaesthesia, University Children’s Hospital Zurich, Steinwiesstrasse 75, 8032 Zurich, Switzerland2 Department of General and Surgical Critical Care Medicine, Innsbruck Medical University, Anichstrasse 35, 6020 Innsbruck, Austria3 Department of Anesthesiology, University of Pittsburgh Medical Center, 200 Lothrop Street, PUH C-215, Pittsburgh, PA, USA4 Unilabs, Coagulation Lab and Centre for Perioperative Thrombosis and Hemostasis, Hufgasse 17, 8008 Zurich, Switzerland5 Oxford Haemophilia and Thrombosis Centre, Oxford University Hospitals NHS Trust, Oxford, UK6 Department of Anaesthesiology and Intensive Care Medicine, AUVA Trauma Centre, Salzburg Academic Teaching Hospital of the ParacelsusMedical University, Salzburg, Austria7 Ludwig Boltzmann Institute for Experimental and Clinical Traumatology, Vienna, Austria
* Corresponding author. E-mail: [email protected]
Editor’s key points
† The authors review theevidence for thecontinued use of standardlaboratory tests ofcoagulation.
† They conclude that thereis minimal evidence forthe use of standardlaboratory tests in guidingthe management ofperioperative bleeding.
Summary. Standard laboratory coagulation tests (SLTs) such as prothrombin time/international normalized ratio or partial thromboplastin time are frequently used to assesscoagulopathy and to guide haemostatic interventions. However, this has been challengedby numerous reports, including the current European guidelines for perioperative bleedingmanagement, which question the utility and reliability of SLTs in this setting. Furthermore,the arbitrary definition of coagulopathy (i.e. SLTs are prolonged by more than 1.5-fold) hasbeen questioned. The present study aims to review the evidence for the usefulness of SLTsto assess coagulopathy and to guide bleeding management in the perioperative andmassive bleeding setting. Medline was searched for investigations using results of SLTs as ameans to determine coagulopathy or to guide bleeding management, and the outcomes(i.e. blood loss, transfusion requirements, mortality) were reported. A total of 11 guidelinesfor management of massive bleeding or perioperative bleeding and 64 studies investigatingthe usefulness of SLTs in this setting were identified and were included for final datasynthesis. Referenced evidence for the usefulness of SLTs was found in only threeprospective trials, investigating a total of 108 patients (whereby microvascular bleeding wasa rare finding). Furthermore, no data from randomized controlled trials support the use ofSLTs. In contrast, numerous investigations have challenged the reliability of SLTs to assesscoagulopathy or guide bleeding management. There is actually no sound evidence fromwell-designed studies that confirm the usefulness of SLTs for diagnosis of coagulopathy orto guide haemostatic therapy.
Keywords: bleeding; blood; coagulation; coagulopathy; transfusion
Perioperative management of coagulopathic bleedingrequires timely haemostatic intervention using allogeneic bloodproducts, administration of coagulation factor concentrates,or both. To guide these interventions, fast laboratory workupis essential. If it comes to the question which laboratory testshould be performed to assess haemostasis, current guidelinesusually refer to standard plasma coagulation tests (SLTs),that is, prothrombin time (PT)/international normalized ratio(INR) and activated partial thromboplastin time,1 – 7 whileviscoelastic tests (i.e. thrombelastography) are less commonlyadvocated.7 Although the complete panel of standard co-agulation testing almost always covers additional measure-ments of fibrinogen and platelet count, interpretation of SLTsis most frequently used to assess coagulopathy. Generally
speaking, coagulopathy is presumed when SLTs are prolongedby more than 1.5-fold, although the evidence to supportthis degree of prolongation as diagnostic of coagulopathy islimited.
However, there are major limitations to these SLTs. Thesetests are time-consuming (with turnaround times sometimeslonger than 60 min)8 and, as a consequence, they are oftenomitted in situations of severe bleeding, where prompt treat-ment must be ensured. In addition, if the results of PT/aPTTare more than 1.5 times prolonged, the treatment optionsrange from transfusion of fresh-frozen plasma (FFP) to admin-istration of coagulation factor concentrates such as prothrom-bin complex concentrates (PCC) or activated recombinantfactor VII. Notably, all these treatment options may be linked
& The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
British Journal of Anaesthesia 114 (2): 217–24 (2015)Advance Access publication 8 September 2014 . doi:10.1093/bja/aeu303
at Vrije U
niversiteit Am
sterdam on January 23, 2015
http://bja.oxfordjournals.org/D
ownloaded from
RESEARCH Open Access
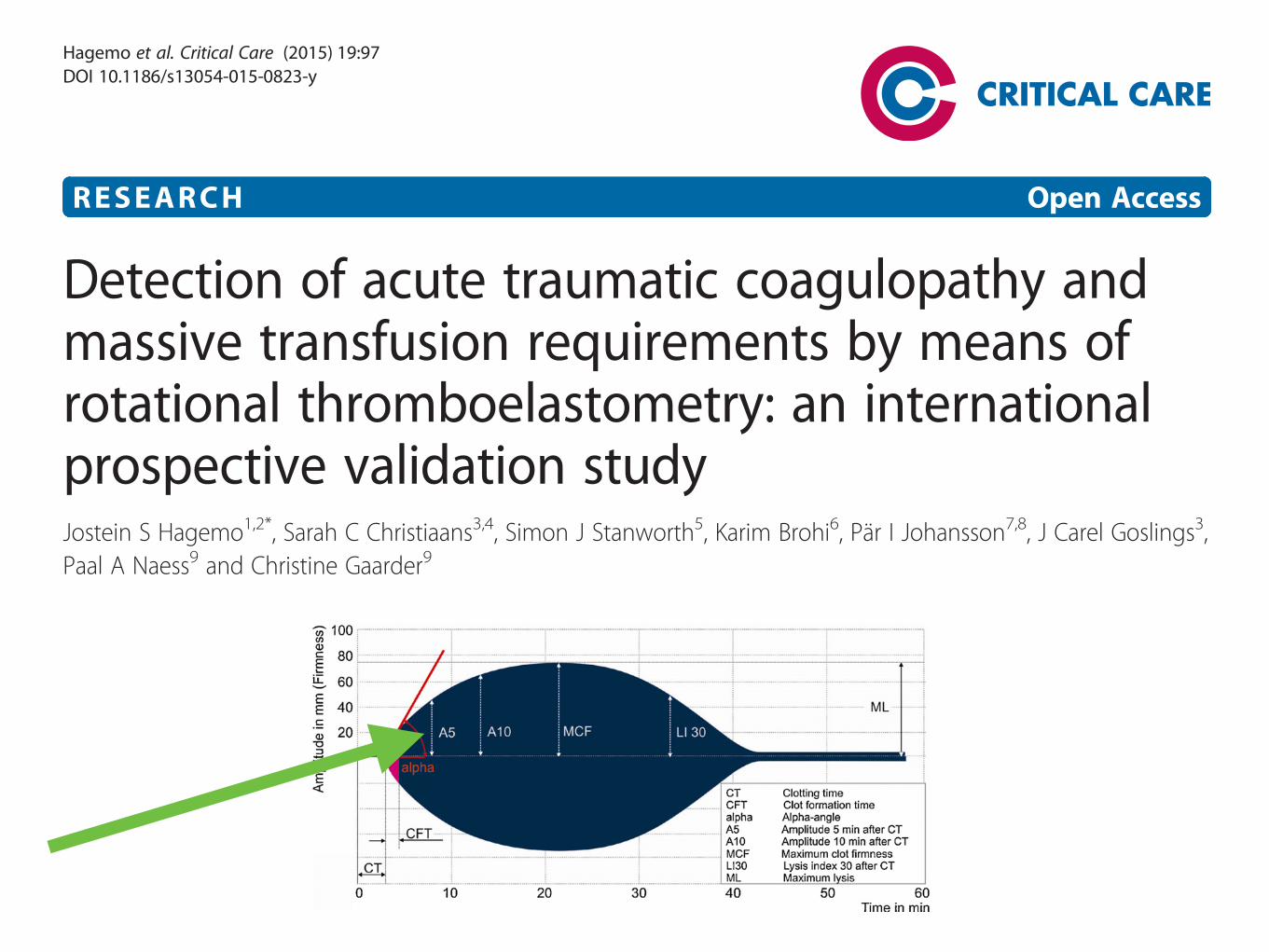
Detection of acute traumatic coagulopathy andmassive transfusion requirements by means ofrotational thromboelastometry: an internationalprospective validation studyJostein S Hagemo1,2*, Sarah C Christiaans3,4, Simon J Stanworth5, Karim Brohi6, Pär I Johansson7,8, J Carel Goslings3,Paal A Naess9 and Christine Gaarder9
Abstract
Introduction: The purpose of this study was to re-evaluate the findings of a smaller cohort study on the functionaldefinition and characteristics of acute traumatic coagulopathy (ATC). We also aimed to identify the threshold values forthe most accurate identification of ATC and prediction of massive transfusion (MT) using rotational thromboelastometry(ROTEM) assays.
Methods: In this prospective international multicentre cohort study, adult trauma patients who met the local criteriafor full trauma team activation from four major trauma centres were included. Blood was collected on arrival to theemergency department and analyzed with laboratory international normalized ratio (INR), fibrinogen concentration andtwo ROTEM assays (EXTEM and FIBTEM). ATC was defined as laboratory INR >1.2. Transfusion requirements of ≥10 unitsof packed red blood cells within 24 hours were defined as MT. Performance of the tests were evaluated by receiveroperating characteristic curves, and calculation of area under the curve (AUC). Optimal cutoff points were estimatedbased on Youden index.
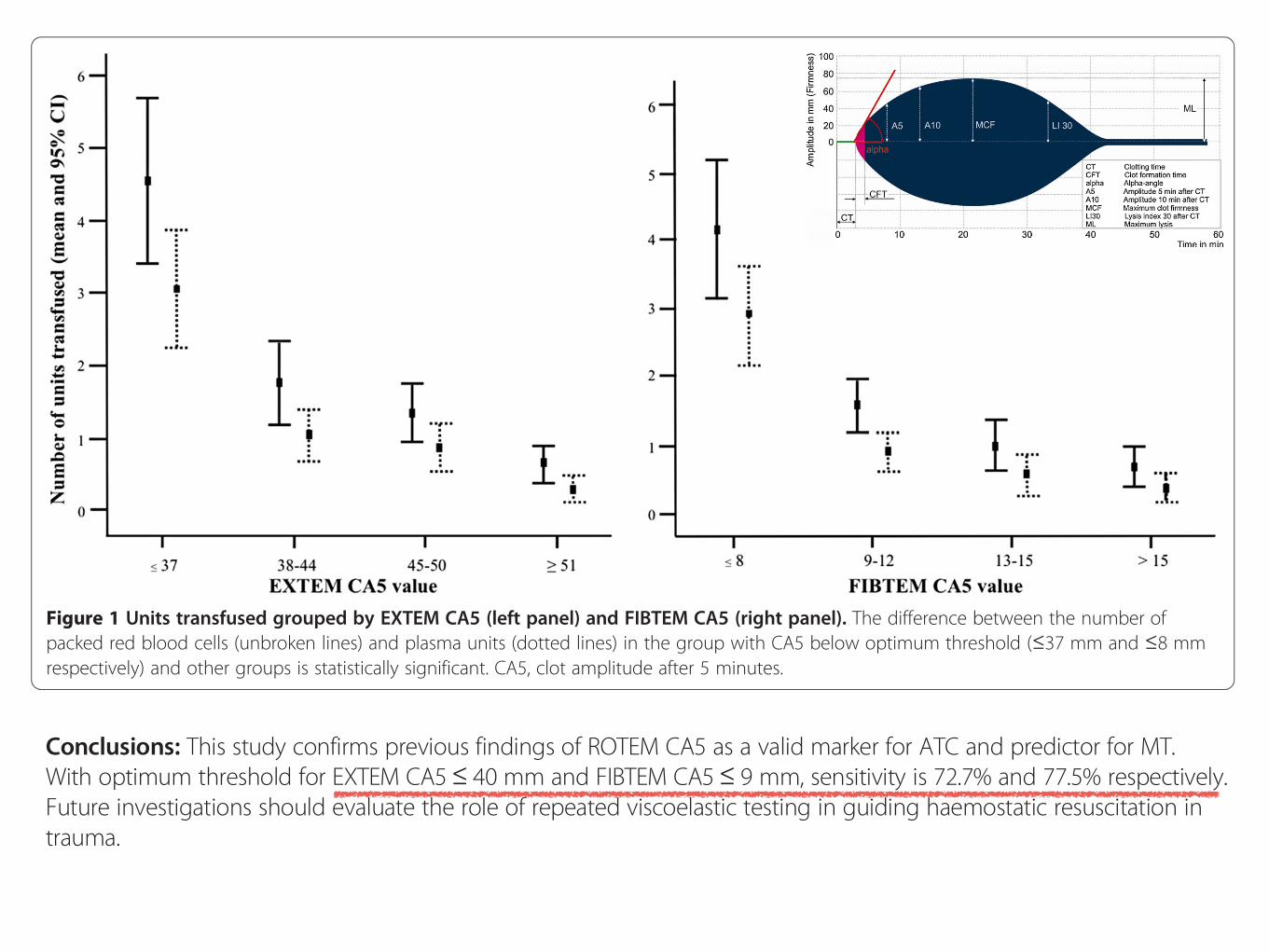
Results: In total, 808 patients were included in the study. Among the ROTEM parameters, the largest AUCs were foundfor the clot amplitude (CA) 5 value in both the EXTEM and FIBTEM assays. EXTEM CA5 threshold value of ≤37 mm hada detection rate of 66.3% for ATC. An EXTEM CA5 threshold value of ≤40 mm predicted MT in 72.7%. FIBTEM CA5threshold value of ≤8 mm detected ATC in 67.5%, and a FIBTEM CA5 threshold value ≤9 mm predicted MT in 77.5%.Fibrinogen concentration ≤1.6 g/L detected ATC in 73.6% and a fibrinogen concentration ≤1.90 g/L predicted MT in77.8%. Patients with either an EXTEM or FIBTEM CA5 below the optimum detection threshold for ATC receivedsignificantly more packed red blood cells and plasma.
Conclusions: This study confirms previous findings of ROTEM CA5 as a valid marker for ATC and predictor for MT.With optimum threshold for EXTEM CA5≤ 40 mm and FIBTEM CA5≤ 9 mm, sensitivity is 72.7% and 77.5% respectively.Future investigations should evaluate the role of repeated viscoelastic testing in guiding haemostatic resuscitation intrauma.
* Correspondence: [email protected] of Research, Norwegian Air Ambulance Foundation, Postboks39 1441, Drøbak, Norway2Department of Anaesthesiology, Oslo University Hospital, Rikshospitalet,Postboks 4950, Nydalen, 0424 Oslo, NorwayFull list of author information is available at the end of the article
© 2015 Hagemo et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Hagemo et al. Critical Care (2015) 19:97 DOI 10.1186/s13054-015-0823-y
study was to evaluate the utility of these interim values inpredicting whether the ROTEM1 test would indicate coagulopathywhen run to completion.
The aim of this study is to determine whether measures of clotstrength reported at 5 and 10 min after initiation of clotting(defined by ROTEM1 as A5 and A10) provide a reliable indication ofcoagulopathy when the ROTEM1 EXTEM test is run to completionon blood derived from severely injured battlefield casualties.
Methods
In accordance with standard laboratory practise,14 normalrange data was derived from venous samples collected, withinformed consent, from a population of 50 healthy volunteersundergoing routine assessment as part of the Emergency DonorPanel (EDP) at the UK DMS deployed Role 3 Field Hospital at CampBastion (R3 Bastion), Afghanistan. The patient population com-prised 48 casualties presenting to R3 Bastion during the studyperiod (21 May 09–3 July 09). All of these casualties were classifiedas seriously injured and had been triaged as T1 or T2. T1 and T2casualties are those that have immediate or urgent clinicalproblems requiring full trauma team activation. Venous bloodsamples were collected prospectively from these patients, as partof their routine clinical evaluation ROTEM1 values from theinjured patients were compared to the reference range derivedfrom the uninjured service personnel at Bastion.
Blood samples were collected by assigned nurses or doctors aspart of their defined role in the trauma team. Samples werecollected from either 16 G peripheral cannulae or 8.5 Fr centralvenous line (depending on the first vascular access gained).Samples for ROTEM1 were analysed within 5 min by designatedoperating room staff. Blood samples sent to the laboratory wereimmediately placed on a standard laboratory tube roller untilanalysis was performed.
ROTEM1 analysis was performed according to the manufac-turers instructions for EXTEM and FIBTEM. Briefly, 4.5 ml bloodsamples were taken into citrated vacutainers (BD Vacutainer1,Model 367691). ROTEM1 testing involved adding calcium(STARTEM1), tissue factor (EXTEM1) and, in the case of FIBTEMtesting, a platelet inhibitor, cytochalasin D, (FIBTEM1) to theROTEM1 cup. 300 ml of citrated blood was then added to the cupand mixed with the reagents using the standard automaticpipetting sequence of ROTEM1, and the test started within 30 s.
A typical ROTEM1 trace (TEMogram) from a normal volunteeris shown in Fig. 1.
The following parameters are routinely reported:
Clotting time (CT) representing clot initiation.Clot formation time (CFT) and angle representing clot dynamics.Maximum clot firmness (MCF) representing ultimate clotstrength.
Amplitude at 5 min (A5) and 10 min (A10) are interim values ofclot strength and relate to the amplitude at 5 and 10 min afterclotting time.
Definition of coagulopathy as determined by ROTEM1
There are no formal definitions of coagulopathy as determinedby viscoelastic methods, including ROTEM1, and no publishedpeer reviewed papers defining actual parameters to establish thepresence or absence of coagulopathy. In 200815 the ROTEM1
Expert Working Group Meeting recommended that an EXTEM MCFof 30–45 mm may require treatment depending on the clinicalcondition of the patient. Experimental dilution of blood to modelcoagulapathies (60% dilution,16 and PT of 1.7 times normal17) havecorresponding EXTEM MCF of 40 mm and 39 mm. We have used afigure of EXTEM MCF < 40 mm as one definition of hypocoagula-tion as this represents a risk of bleeding and may require treatmentto prevent further deterioration to a clinical coagulopathy.
Using a single parameter such as MCF to diagnose coagulopathyis potentially too simplistic a tool and of no real value unless it isgrossly abnormal. It is unlikely that a result 1 or 2 mm outsidenormal is a clinical problem, unless that subtle abnormality ispresent in more than one clotting domain. In this case the patientmay be at increased risk of a clinical bleeding problem and as suchcould be assumed to be at increased risk of coagulopathy. As such asubtle abnormality in 2 out of 3 domains should alert the clinicianto the possibility that there is a clinical problem, and in the contextof the specific circumstances of the patient may representcoagulopathy. We have therefore compared an alternative putativedefinition of coagulopathy; the presence of abnormal values in twoof the three domains (initiation, dynamics and strength) termedthe ‘‘2/3 rule’’.
Therefore, in this study two alternative definitions of coagulo-pathy were used, the first based on an MCF of <40 mm and thesecond on the putative ‘‘2/3 rule’’ (using the locally derived normalvalues, Table 1). This putative ‘‘2/3 rule’’ is only intended as apotentially interesting alternative since it has not yet been
Fig. 1. Illustration of a TEMogram showing three domains of clotting, clot initiation (clotting time), clot dynamics (a angle, clot formation time) and clot firmness (max clotfirmness) Interim value of A5, A10, and lysis index are also shown.Figure taken from TEM1 training material.
T. Woolley et al. / Injury, Int. J. Care Injured 44 (2013) 593–599594
ConclusionsIn conclusion, this study confirms the previous findingthat the ROTEM CA5 value measured on arrival is avalid marker for ATC and predicts MT requirements.An EXTEM CA5 threshold value of ≤40 mm has adetection rate of 72.7%, whereas a FIBTEM CA5threshold value of ≤9 mm detects MT requirementsin 77.5% of cases. Fibrinogen concentration was sig-nificantly better than ROTEM assays in predictingATC, and a fibrinogen concentration ≤1.90 g/L had adetection rate of 77.8% for MT requirement. Future
studies should be directed at identifying the role ofrepeated VHA measurements in guiding haemostaticresuscitation in trauma.
Key messages
! The ROTEM assay is a valid predictor ofcoagulopathy and MT.
! Optimal cutoff value for CA5 was found at≤40 mm for the EXTEM assay and ≤9 mm forthe FIBTEM assay.
Table 4 Optimum thresholds and respective test accuracy parameters for predicting (a) acute traumatic coagulopathy(ATC) defined as INR >1.2 and (b) massive transfusion (MT) (defined as ≥10 units of PRBC)Test parameter Optimum threshold Detection rate False positive rate PPV NPV
(a)
EXTEM CA5 ≤37 (34-39) 66.3 (55.1-76.3) 18.8 (15.9-21.9) 29.9 (23.4-37.1) 95.2 (93.2-96.8)
FIBTEM CA5 ≤8 (5-8) 67.5 (55.9-77.8) 20.7 (17.7-23.9) 26.9 (20.8-33.8) 95.6 (93.5-97.1)
Fibrinogen ≤1.61 (1.36-1.9) 73.6 (63.0-82.4) 11.5 (9.2-14.1) 45.1 (36.7-53.6) 96.3 (94.5-97.7)
Platelet count ≤199 (128-199) 61.7 (46.4-75.5) 29.9 (26.6-33.4) 11.9 (8.1-16.7) 96.5 (94.6-97.9)
(b)
EXTEM CA5 ≤40 (32-40) 72.7 (57.2-85.0) 31.3 (28.0-34.8) 12.2 (8.5-16.8) 97.7 (96.0-98.8)
FIBTEM CA5 ≤9 (6-9) 77.5 (61.5-89.2) 32.8 (29.4-36.4) 11.4 (7.9-15.8) 98.2 (96.6-99.2)
Fibrinogen ≤1.90 (1.39-2.18) 77.8 (62.9-88.8) 29.7 (26.4-30.1) 14.0 (9.9-18.9) 98.1 (96.5-99.1)
INR ≥1.13 (1.0-1.16) 70.2 (55.1-82.7) 19.0 (16.2-22.1) 19.2 (13.6-25.9) 97.7 (96.2-98.7)
Platelet count ≤174 (159-182) 52.8 (41.9-63.5) 14.8 (12.2-17.7) 32.2 (24.7-40.4) 93.1 (90.8-95.0)
INR, international normalized ratio; PRBC, packed red blood cells; PPV, positive predictive value; NPV, negative predictive value; CA5, clot amplitude after5 minutes.
Figure 1 Units transfused grouped by EXTEM CA5 (left panel) and FIBTEM CA5 (right panel). The difference between the number ofpacked red blood cells (unbroken lines) and plasma units (dotted lines) in the group with CA5 below optimum threshold (≤37 mm and ≤8 mmrespectively) and other groups is statistically significant. CA5, clot amplitude after 5 minutes.
Hagemo et al. Critical Care (2015) 19:97 Page 5 of 7
RESEARCH Open Access
Detection of acute traumatic coagulopathy andmassive transfusion requirements by means ofrotational thromboelastometry: an internationalprospective validation studyJostein S Hagemo1,2*, Sarah C Christiaans3,4, Simon J Stanworth5, Karim Brohi6, Pär I Johansson7,8, J Carel Goslings3,Paal A Naess9 and Christine Gaarder9
Abstract
Introduction: The purpose of this study was to re-evaluate the findings of a smaller cohort study on the functionaldefinition and characteristics of acute traumatic coagulopathy (ATC). We also aimed to identify the threshold values forthe most accurate identification of ATC and prediction of massive transfusion (MT) using rotational thromboelastometry(ROTEM) assays.
Methods: In this prospective international multicentre cohort study, adult trauma patients who met the local criteriafor full trauma team activation from four major trauma centres were included. Blood was collected on arrival to theemergency department and analyzed with laboratory international normalized ratio (INR), fibrinogen concentration andtwo ROTEM assays (EXTEM and FIBTEM). ATC was defined as laboratory INR >1.2. Transfusion requirements of ≥10 unitsof packed red blood cells within 24 hours were defined as MT. Performance of the tests were evaluated by receiveroperating characteristic curves, and calculation of area under the curve (AUC). Optimal cutoff points were estimatedbased on Youden index.
Results: In total, 808 patients were included in the study. Among the ROTEM parameters, the largest AUCs were foundfor the clot amplitude (CA) 5 value in both the EXTEM and FIBTEM assays. EXTEM CA5 threshold value of ≤37 mm hada detection rate of 66.3% for ATC. An EXTEM CA5 threshold value of ≤40 mm predicted MT in 72.7%. FIBTEM CA5threshold value of ≤8 mm detected ATC in 67.5%, and a FIBTEM CA5 threshold value ≤9 mm predicted MT in 77.5%.Fibrinogen concentration ≤1.6 g/L detected ATC in 73.6% and a fibrinogen concentration ≤1.90 g/L predicted MT in77.8%. Patients with either an EXTEM or FIBTEM CA5 below the optimum detection threshold for ATC receivedsignificantly more packed red blood cells and plasma.
Conclusions: This study confirms previous findings of ROTEM CA5 as a valid marker for ATC and predictor for MT.With optimum threshold for EXTEM CA5≤ 40 mm and FIBTEM CA5≤ 9 mm, sensitivity is 72.7% and 77.5% respectively.Future investigations should evaluate the role of repeated viscoelastic testing in guiding haemostatic resuscitation intrauma.
* Correspondence: [email protected] of Research, Norwegian Air Ambulance Foundation, Postboks39 1441, Drøbak, Norway2Department of Anaesthesiology, Oslo University Hospital, Rikshospitalet,Postboks 4950, Nydalen, 0424 Oslo, NorwayFull list of author information is available at the end of the article
© 2015 Hagemo et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Hagemo et al. Critical Care (2015) 19:97 DOI 10.1186/s13054-015-0823-y
study was to evaluate the utility of these interim values inpredicting whether the ROTEM1 test would indicate coagulopathywhen run to completion.
The aim of this study is to determine whether measures of clotstrength reported at 5 and 10 min after initiation of clotting(defined by ROTEM1 as A5 and A10) provide a reliable indication ofcoagulopathy when the ROTEM1 EXTEM test is run to completionon blood derived from severely injured battlefield casualties.
Methods
In accordance with standard laboratory practise,14 normalrange data was derived from venous samples collected, withinformed consent, from a population of 50 healthy volunteersundergoing routine assessment as part of the Emergency DonorPanel (EDP) at the UK DMS deployed Role 3 Field Hospital at CampBastion (R3 Bastion), Afghanistan. The patient population com-prised 48 casualties presenting to R3 Bastion during the studyperiod (21 May 09–3 July 09). All of these casualties were classifiedas seriously injured and had been triaged as T1 or T2. T1 and T2casualties are those that have immediate or urgent clinicalproblems requiring full trauma team activation. Venous bloodsamples were collected prospectively from these patients, as partof their routine clinical evaluation ROTEM1 values from theinjured patients were compared to the reference range derivedfrom the uninjured service personnel at Bastion.
Blood samples were collected by assigned nurses or doctors aspart of their defined role in the trauma team. Samples werecollected from either 16 G peripheral cannulae or 8.5 Fr centralvenous line (depending on the first vascular access gained).Samples for ROTEM1 were analysed within 5 min by designatedoperating room staff. Blood samples sent to the laboratory wereimmediately placed on a standard laboratory tube roller untilanalysis was performed.
ROTEM1 analysis was performed according to the manufac-turers instructions for EXTEM and FIBTEM. Briefly, 4.5 ml bloodsamples were taken into citrated vacutainers (BD Vacutainer1,Model 367691). ROTEM1 testing involved adding calcium(STARTEM1), tissue factor (EXTEM1) and, in the case of FIBTEMtesting, a platelet inhibitor, cytochalasin D, (FIBTEM1) to theROTEM1 cup. 300 ml of citrated blood was then added to the cupand mixed with the reagents using the standard automaticpipetting sequence of ROTEM1, and the test started within 30 s.
A typical ROTEM1 trace (TEMogram) from a normal volunteeris shown in Fig. 1.
The following parameters are routinely reported:
Clotting time (CT) representing clot initiation.Clot formation time (CFT) and angle representing clot dynamics.Maximum clot firmness (MCF) representing ultimate clotstrength.
Amplitude at 5 min (A5) and 10 min (A10) are interim values ofclot strength and relate to the amplitude at 5 and 10 min afterclotting time.
Definition of coagulopathy as determined by ROTEM1
There are no formal definitions of coagulopathy as determinedby viscoelastic methods, including ROTEM1, and no publishedpeer reviewed papers defining actual parameters to establish thepresence or absence of coagulopathy. In 200815 the ROTEM1
Expert Working Group Meeting recommended that an EXTEM MCFof 30–45 mm may require treatment depending on the clinicalcondition of the patient. Experimental dilution of blood to modelcoagulapathies (60% dilution,16 and PT of 1.7 times normal17) havecorresponding EXTEM MCF of 40 mm and 39 mm. We have used afigure of EXTEM MCF < 40 mm as one definition of hypocoagula-tion as this represents a risk of bleeding and may require treatmentto prevent further deterioration to a clinical coagulopathy.
Using a single parameter such as MCF to diagnose coagulopathyis potentially too simplistic a tool and of no real value unless it isgrossly abnormal. It is unlikely that a result 1 or 2 mm outsidenormal is a clinical problem, unless that subtle abnormality ispresent in more than one clotting domain. In this case the patientmay be at increased risk of a clinical bleeding problem and as suchcould be assumed to be at increased risk of coagulopathy. As such asubtle abnormality in 2 out of 3 domains should alert the clinicianto the possibility that there is a clinical problem, and in the contextof the specific circumstances of the patient may representcoagulopathy. We have therefore compared an alternative putativedefinition of coagulopathy; the presence of abnormal values in twoof the three domains (initiation, dynamics and strength) termedthe ‘‘2/3 rule’’.
Therefore, in this study two alternative definitions of coagulo-pathy were used, the first based on an MCF of <40 mm and thesecond on the putative ‘‘2/3 rule’’ (using the locally derived normalvalues, Table 1). This putative ‘‘2/3 rule’’ is only intended as apotentially interesting alternative since it has not yet been
Fig. 1. Illustration of a TEMogram showing three domains of clotting, clot initiation (clotting time), clot dynamics (a angle, clot formation time) and clot firmness (max clotfirmness) Interim value of A5, A10, and lysis index are also shown.Figure taken from TEM1 training material.
T. Woolley et al. / Injury, Int. J. Care Injured 44 (2013) 593–599594
De Toekomst
REVIEW Open Access
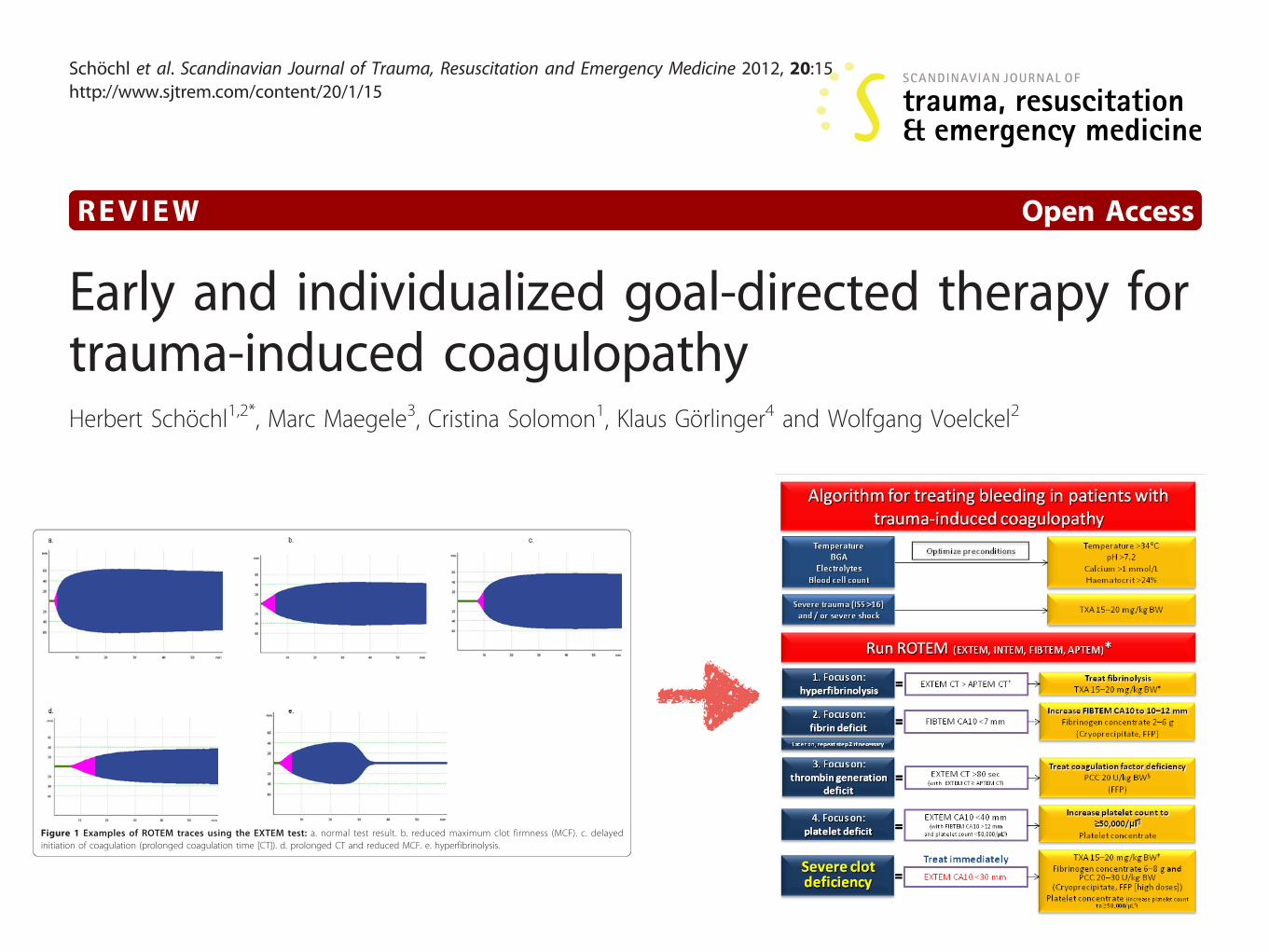
Early and individualized goal-directed therapy fortrauma-induced coagulopathyHerbert Schöchl1,2*, Marc Maegele3, Cristina Solomon1, Klaus Görlinger4 and Wolfgang Voelckel2
AbstractSevere trauma-related bleeding is associated with high mortality. Standard coagulation tests provide limitedinformation on the underlying coagulation disorder. Whole-blood viscoelastic tests such as rotationalthromboelastometry or thrombelastography offer a more comprehensive insight into the coagulation process intrauma. The results are available within minutes and they provide information about the initiation of coagulation,the speed of clot formation, and the quality and stability of the clot. Viscoelastic tests have the potential to guidecoagulation therapy according to the actual needs of each patient, reducing the risks of over- or under-transfusion.The concept of early, individualized and goal-directed therapy is explored in this review and the AUVA TraumaHospital algorithm for managing trauma-induced coagulopathy is presented.
Keywords: ROTEM, TEG, trauma, goal-directed coagulation therapy
IntroductionMajor brain injury and uncontrolled blood loss remainthe primary causes of early trauma-related mortality[1-3]. One-quarter to one-third of trauma patients exhi-bit trauma-induced coagulopathy (TIC) [4,5], which isassociated with increased rates of massive transfusion(MT) and multiple organ failure (MOF), prolongedintensive care unit and hospital stays, and a four-foldincrease in mortality [4]. Most patients with coagulopa-thy also have uncontrolled bleeding, and early diagnosisof the underlying coagulation disorder is paramount foreffective treatment.One major challenge in treating severely bleeding
trauma patients is to determine whether the blood lossis attributable to surgical causes or coagulopathy. If thepatient is coagulopathic, it is paramount to characterizethe cause of the coagulopathy and whether thrombingeneration is impaired or clot quality or stability isdiminished. Recent data suggest that whole-blood vis-coelastic tests, such as thromboelastometry (ROTEM®,Tem International GmbH, Munich, Germany) or throm-belastography (TEG®, Haemonetics Corp., Braintree,MA, USA) portray trauma induced coagulopathy (TIC)
more accurately and substantially faster than standardcoagulation tests [6-8]. There is increasing evidence thatthese coagulation monitoring devices are helpful inguiding coagulation therapy for heavily bleeding traumapatients according to their actual needs [9].The intention of this review is to examine the concept
of individualized, early, goal-directed therapy for TIC,using viscoelastic tests and targeted coagulation therapy.In addition, the AUVA Trauma Hospital algorithm formanaging TIC is presented.
Value of standard coagulation testsFast, reliable diagnosis and characterization of TIC isimportant. Standard coagulation tests (e.g. prothrombintime [PT], international normalized ratio [INR], pro-thrombin time index [PTI] and activated partial throm-boplastin time [aPTT]) fail to accurately describe thecomplex nature of TIC for several reasons [4,5]. In vivocoagulation occurs primarily on the surface of plateletsand tissue factor-bearing cells [10], and red blood cells(RBCs) also play a significant role in haemostasis [11].Standard coagulation tests are performed using plasmain the absence of blood cells (these are removed by cen-trifugation). Also, these tests are stopped upon forma-tion of the first fibrin strands, when only ~5% of thetotal thrombin has been generated [12]. Moreover, thesetests do not assess the quality/the strength of the clot.
* Correspondence: [email protected] Boltzmann Institute of Experimental and Clinical Traumatology,Vienna, AustriaFull list of author information is available at the end of the article
Schöchl et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012, 20:15http://www.sjtrem.com/content/20/1/15
© 2012 Schöchl et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative CommonsAttribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction inany medium, provided the original work is properly cited.
Figure 2 ROTEM-guided treatment algorithm: managing trauma-induced coagulopathy and diffuse microvascular bleeding (AUVATrauma Hospital, Salzburg, Austria). The algorithm represents standard operating procedure for ROTEM-guided haemostatic therapy uponadmission of trauma patients to the emergency room. In parentheses: haemostatic agents suggested for use in clinics where coagulation factorconcentrates are not available. * For patients who are unconscious or known to be taking platelet inhibitor medication, Multiplate tests(adenosine diphosphate [ADP] test, arachidonic acid [ASPI] test, and thrombin receptor activating peptide-6 [TRAP] test) are also performed. § Ifdecreased ATIII is suspected or known, consider co-administration of ATIII. † Any major improvement in APTEM parameters compared tocorresponding EXTEM parameters may be interpreted as a sign of hyperfibrinolysis. ‡ Only for patients not receiving TXA at an earlier stage ofthe algorithm. Traumatic brain injury: platelet count 80,000-100,000/μl. Normal values: EXTEM/APTEM coagulation time (CT): 38-79 seconds;EXTEM/APTEM clot amplitude at 10 minutes (CA10): 43-65 mm; EXTEM/APTEM maximum lysis (ML) < 15%; FIBTEM CA10: 7-23 mm; INTEM CT:100-240 seconds. CA10, clot amplitude at 10 minutes; BGA, blood gas analysis; BW, body weight; Ca, calcium; CT, clotting time; FFP, fresh frozenplasma; ISS, injury severity score; MCF, maximum clot firmness; ML, maximum lysis; PCC, prothrombin complex concentrate; TXA, tranexamic acid.
Schöchl et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012, 20:15http://www.sjtrem.com/content/20/1/15
Page 5 of 11
Hyperfibrinolysis is recognized as a potential contributorto mortality in trauma [13-15], and this aspect is notassessed by standard coagulation tests [16].Coagulation factors do not decrease homogeneously in
severe bleeding. Although there may be a tendencytowards excessive thrombin generation, coagulation fac-tor levels are decreased and fibrinogen appears to reachcritical levels at an early stage [17-19]. Therefore, mea-surement of fibrinogen concentration is strongly recom-mended in trauma patients [14,19]. However, whenusing artificial colloids, falsely high fibrinogen levels arerecorded by some coagulation analysers that employ theClauss method [20,21]. Artificial colloids also impairfibrin polymerization, and standard laboratory measure-ment does not represent fibrinogen functionality [22].Another shortcoming of standard coagulation tests,
including fibrinogen concentration measurement, is thatthe results are available only after a substantial timedelay. Median turnaround times of 78-88 minutes havebeen reported [23,24].In summary, standard coagulation tests are unable to
characterize the complex nature of TIC. They are time-consuming and offer little prognostic value regardingtransfusion requirements [25].
Role of thromboelastometry/thrombelastographyTrauma care providers are increasingly aware that vis-coelastic coagulation monitors such as thromboelasto-metry (ROTEM) and thrombelastography (TEG) arevaluable alternatives to standard coagulation testing,
providing a more comprehensive overview of the coagu-lation process [6,8,23,26-29]. In contrast to most stan-dard coagulation measurements, ROTEM and TEG canbe used as point-of-care methods. Viscoelastic tests areperformed in whole blood as opposed to plasma, whichprovides a better reflection of the in vivo situation,avoids the need for centrifugation and allows initialresults to be available within minutes [23,30].ROTEM and TEG tests provide dynamic information
on the speed of coagulation initiation, kinetics of clotgrowth, clot strength, and breakdown of the clot [16,31].The ROTEM device uses a plastic pin immersed verti-cally into a cup containing the blood sample; the pin isrotated slowly, backwards and forwards, through anangle of 4.75°. The device has four channels, allowingfour tests to be performed simultaneously. Two basicROTEM tests that use intrinsic activation (INTEM) andextrinsic activation (EXTEM) provide information onthe general coagulation status (impaired, normal, andhypercoagulable). Figure 1 shows examples of EXTEMplots with normal and impaired coagulation. A set ofstandard reagents can additionally be used to character-ize coagulopathy. For example, the FIBTEM test, whichcomprises the EXTEM assay with added cytochalasin Dto inhibit platelets, provides information on the fibrincomponent of the clot.The TEG device uses a stationary torsion wire and the
cup is rotated. TEG is a two channel system that useseither kaolin as an activator or a combination of kaolinand tissue factor (’rapid TEG’ or ‘r-TEG’ assay). The
Figure 1 Examples of ROTEM traces using the EXTEM test: a. normal test result. b. reduced maximum clot firmness (MCF). c. delayedinitiation of coagulation (prolonged coagulation time [CT]). d. prolonged CT and reduced MCF. e. hyperfibrinolysis.
Schöchl et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012, 20:15http://www.sjtrem.com/content/20/1/15
Page 2 of 11
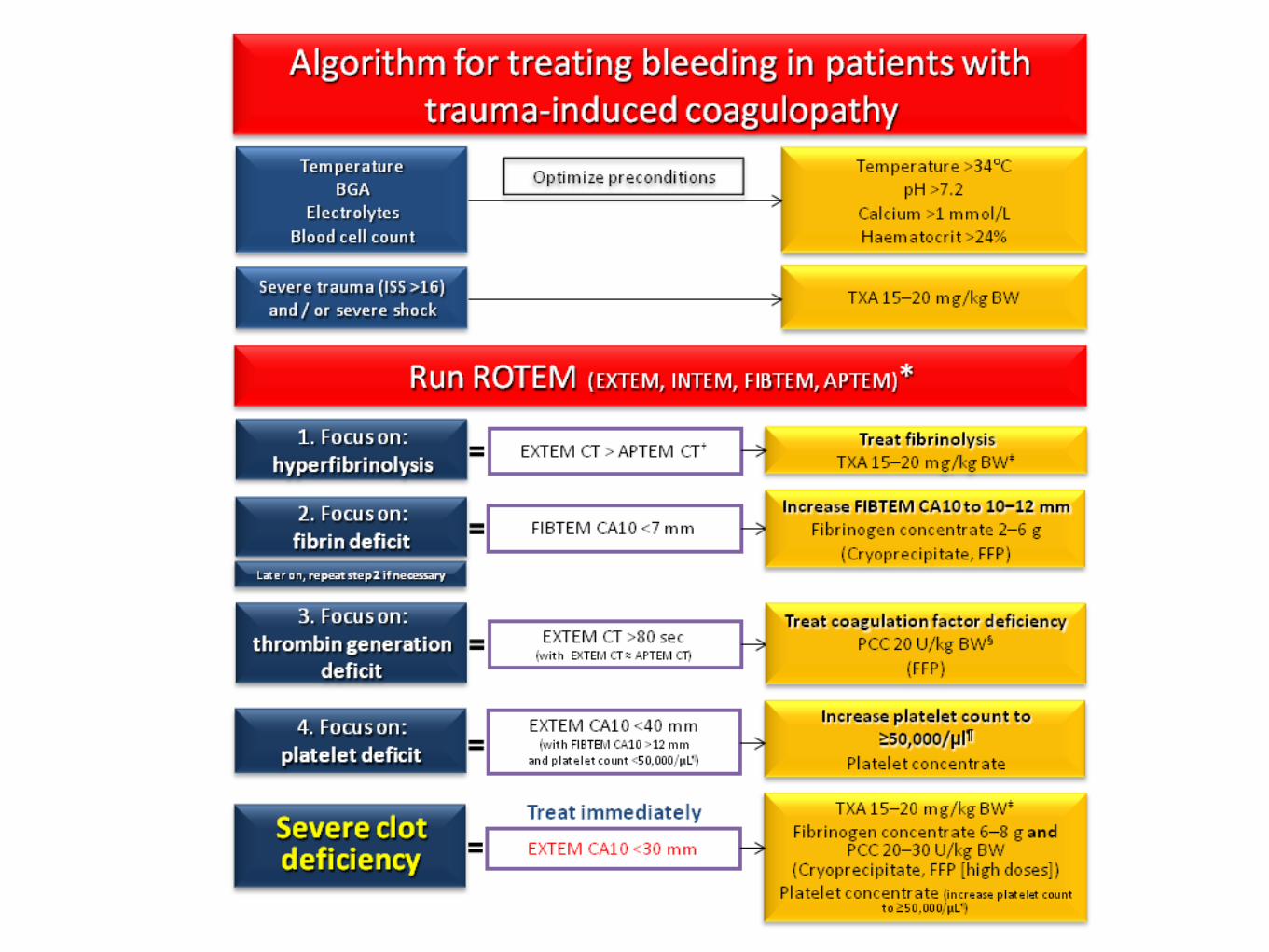
Figure 2 ROTEM-guided treatment algorithm: managing trauma-induced coagulopathy and diffuse microvascular bleeding (AUVATrauma Hospital, Salzburg, Austria). The algorithm represents standard operating procedure for ROTEM-guided haemostatic therapy uponadmission of trauma patients to the emergency room. In parentheses: haemostatic agents suggested for use in clinics where coagulation factorconcentrates are not available. * For patients who are unconscious or known to be taking platelet inhibitor medication, Multiplate tests(adenosine diphosphate [ADP] test, arachidonic acid [ASPI] test, and thrombin receptor activating peptide-6 [TRAP] test) are also performed. § Ifdecreased ATIII is suspected or known, consider co-administration of ATIII. † Any major improvement in APTEM parameters compared tocorresponding EXTEM parameters may be interpreted as a sign of hyperfibrinolysis. ‡ Only for patients not receiving TXA at an earlier stage ofthe algorithm. Traumatic brain injury: platelet count 80,000-100,000/μl. Normal values: EXTEM/APTEM coagulation time (CT): 38-79 seconds;EXTEM/APTEM clot amplitude at 10 minutes (CA10): 43-65 mm; EXTEM/APTEM maximum lysis (ML) < 15%; FIBTEM CA10: 7-23 mm; INTEM CT:100-240 seconds. CA10, clot amplitude at 10 minutes; BGA, blood gas analysis; BW, body weight; Ca, calcium; CT, clotting time; FFP, fresh frozenplasma; ISS, injury severity score; MCF, maximum clot firmness; ML, maximum lysis; PCC, prothrombin complex concentrate; TXA, tranexamic acid.
Schöchl et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012, 20:15http://www.sjtrem.com/content/20/1/15
Page 5 of 11
15


Vragen ?