Prof dr M Claeys UZ Antwerpen Universiteit Antwerpen · Prof dr M Claeys UZ Antwerpen Universiteit...
60
Acute coronaire syndromen Prof dr M Claeys UZ Antwerpen Universiteit Antwerpen Aanvullingen van Paul Calle op basis van ESC guidelines 2015 (ivm non-STEMI) en ERC guidelines 2015 (ivm ACS)
Transcript of Prof dr M Claeys UZ Antwerpen Universiteit Antwerpen · Prof dr M Claeys UZ Antwerpen Universiteit...
Acute coronaire syndromenProf dr M Claeys
UZ AntwerpenUniversiteit Antwerpen
Aanvullingen van Paul Calleop basis van ESC guidelines 2015
(ivm non-STEMI) en ERC guidelines 2015 (ivm ACS)



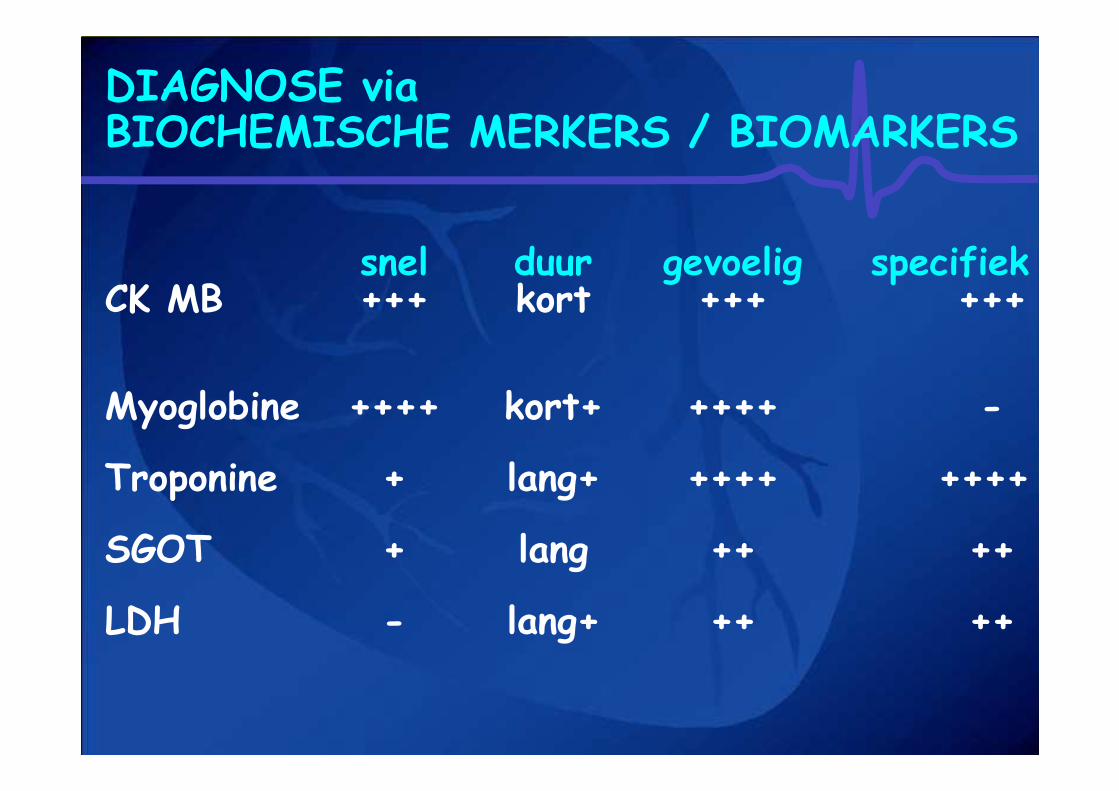
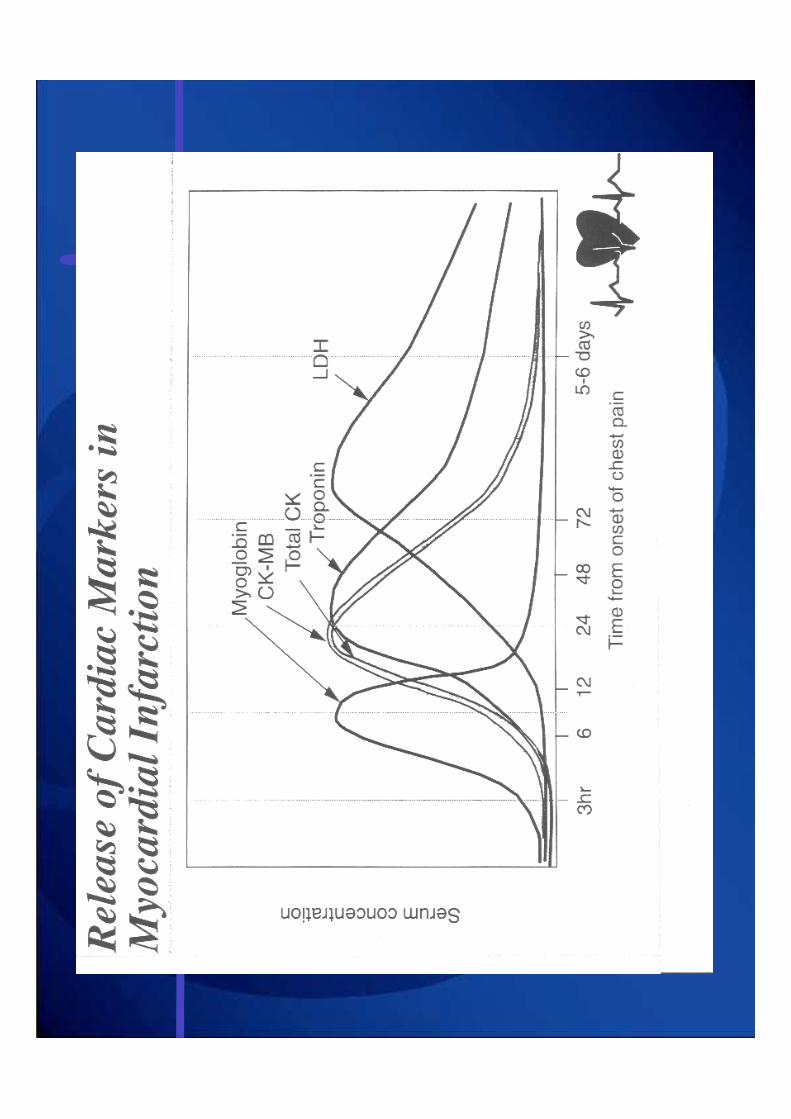
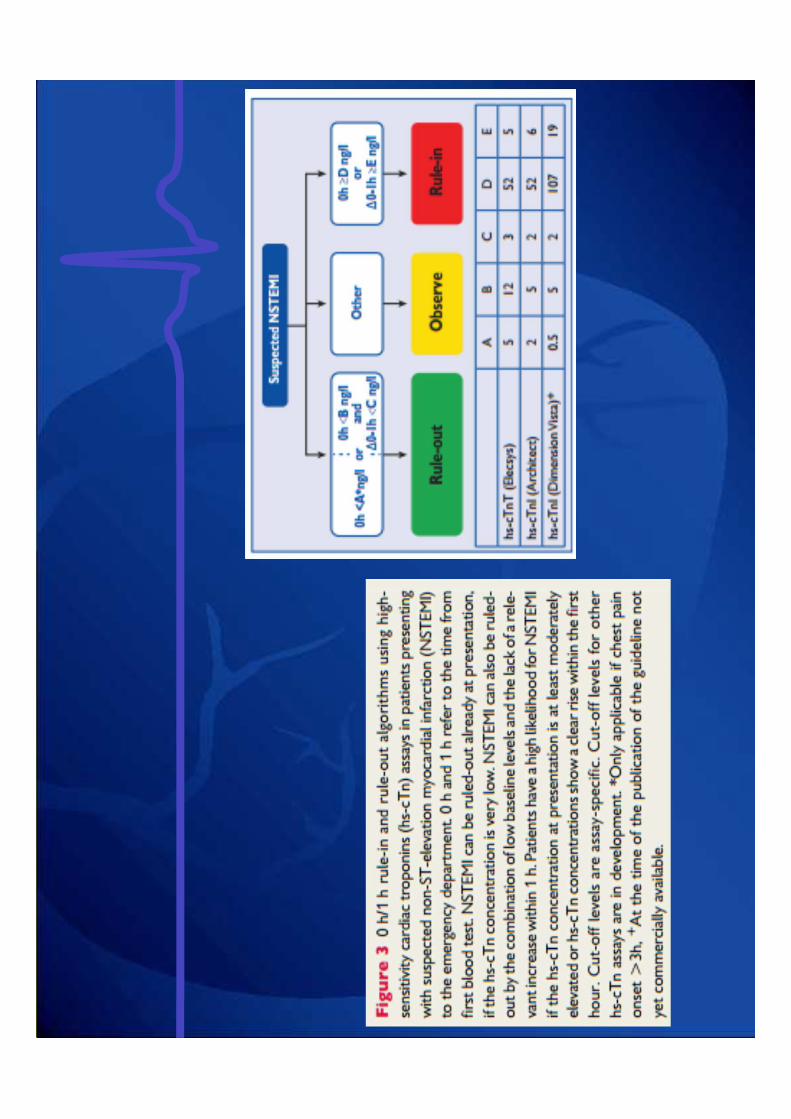
DIAGNOSE viaBIOCHEMISCHE MERKERS / BIOMARKERS
snel duur gevoelig specifiekCK MB +++ kort +++ +++
Myoglobine ++++ kort+ ++++ -
Troponine + lang+ ++++ ++++
SGOT + lang ++ ++
LDH - lang+ ++ ++

TRIADE VAN ACS
AnamneseCardiac enzymes
Surface ECG
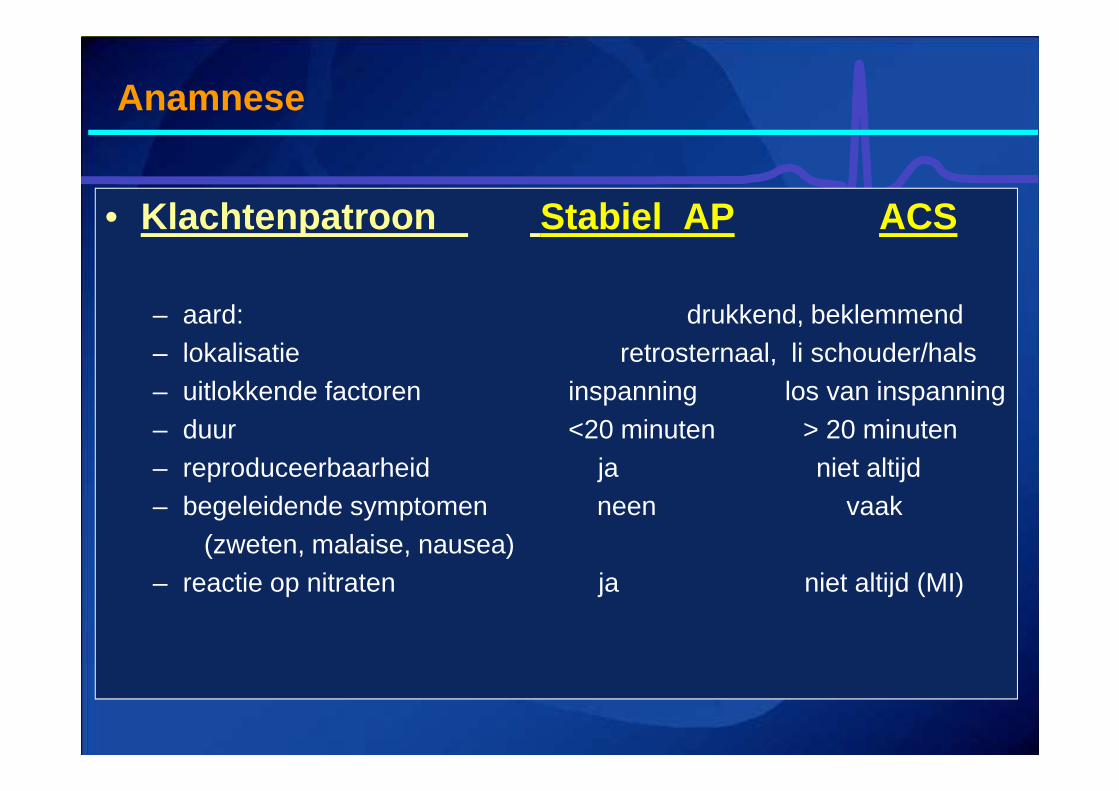
Anamnese
• Klachtenpatroon Stabiel AP ACS
– aard: drukkend, beklemmend– lokalisatie retrosternaal, li schouder/hals– uitlokkende factoren inspanning los van inspanning – duur <20 minuten > 20 minuten– reproduceerbaarheid ja niet altijd– begeleidende symptomen neen vaak
(zweten, malaise, nausea)– reactie op nitraten ja niet altijd (MI)
Early diagnosis (preferentially prehospital)
• Rhythm monitoring
• 12 lead ECG
+ wireless data transfer!
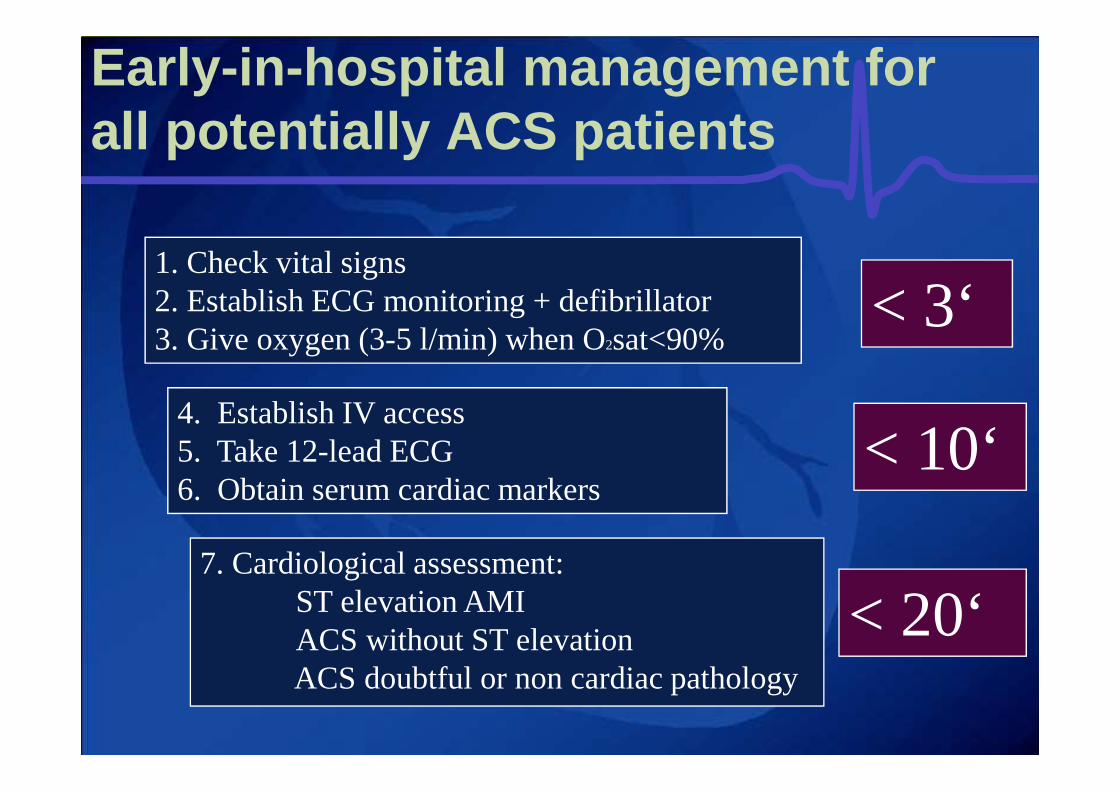
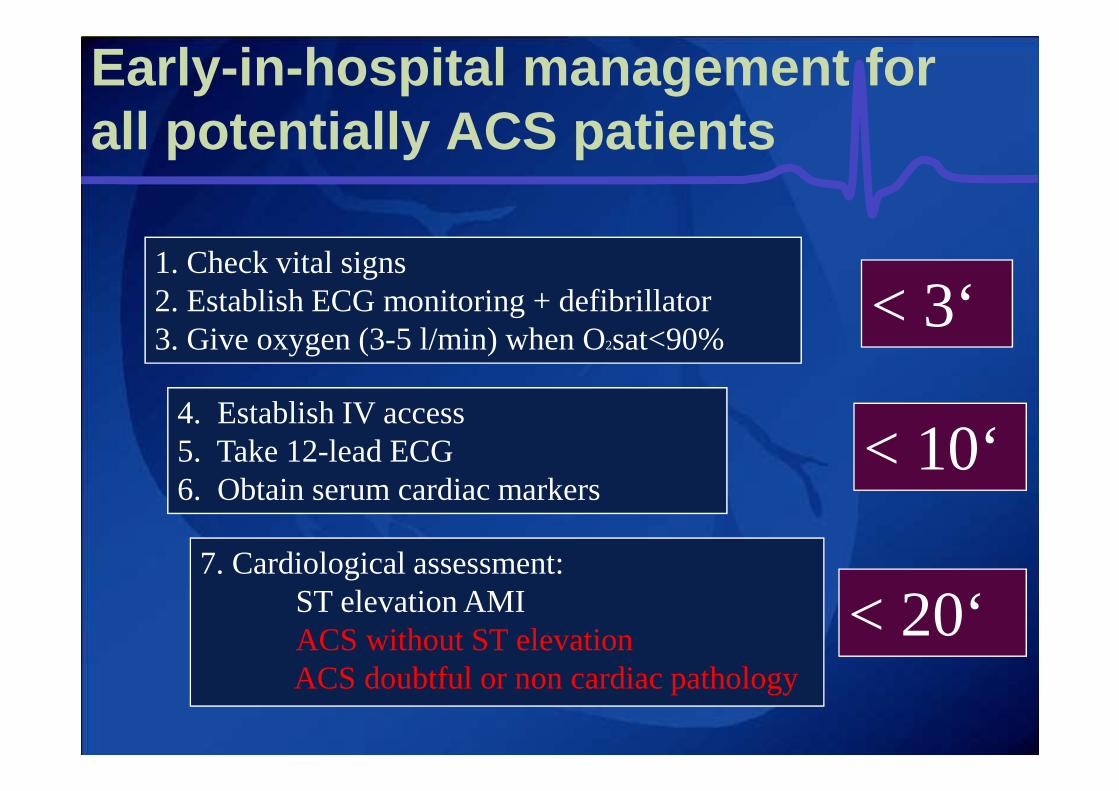
Early -in-hospital management forall potentially ACS patients
1. Check vital signs2. Establish ECG monitoring + defibrillator 3. Give oxygen (3-5 l/min) when O2sat<90%
4. Establish IV access5. Take 12-lead ECG6. Obtain serum cardiac markers
7. Cardiological assessment:ST elevation AMI ACS without ST elevationACS doubtful or non cardiac pathology
< 3‘
< 10‘
< 20‘
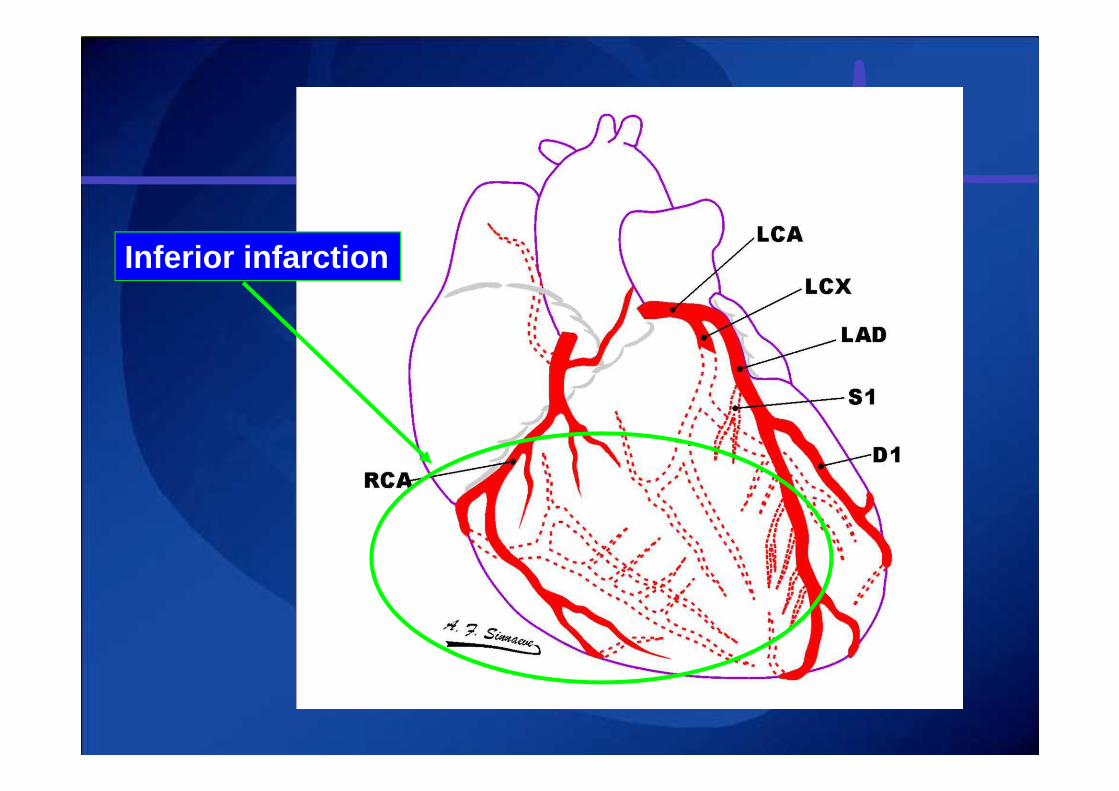
Inferior infarction
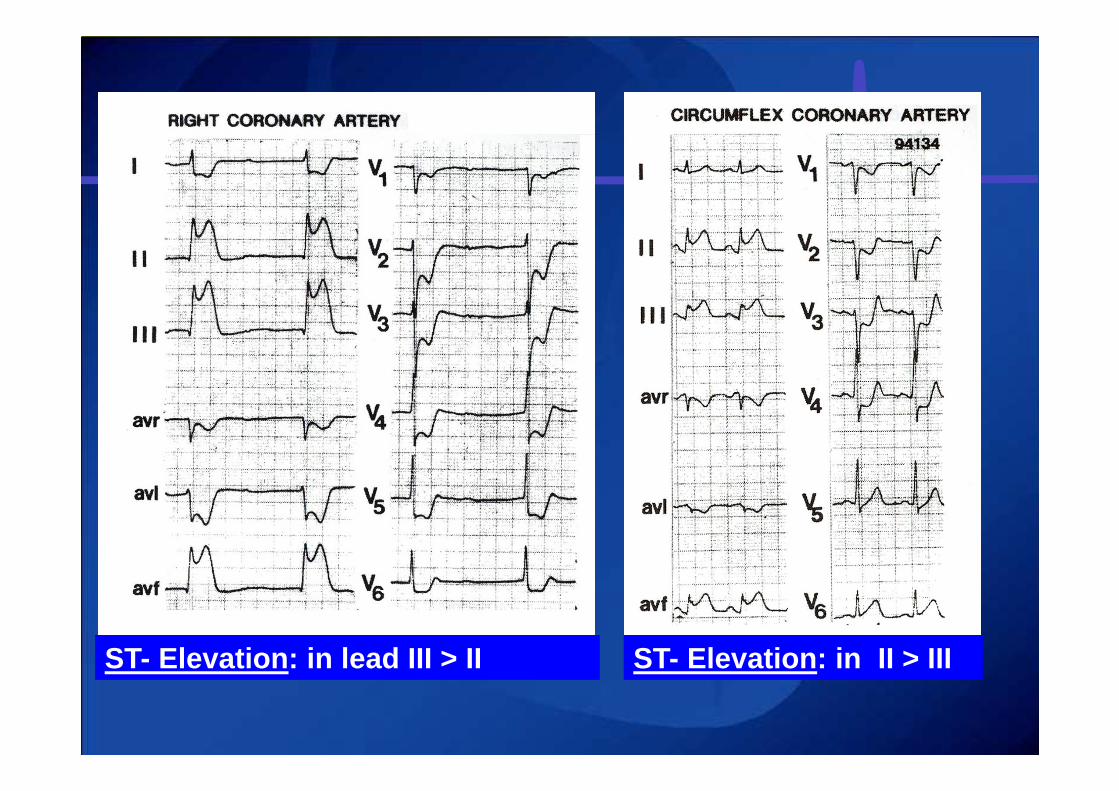
ST- Elevation: in lead III > II ST- Elevation: in II > III
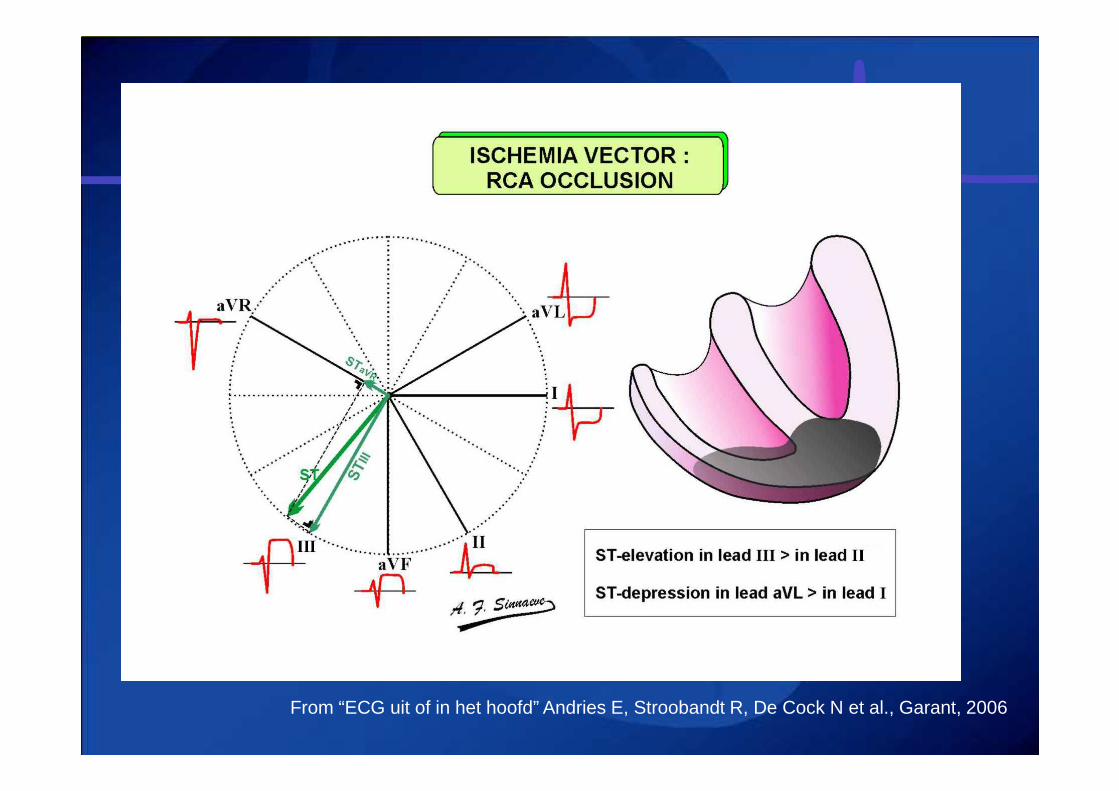
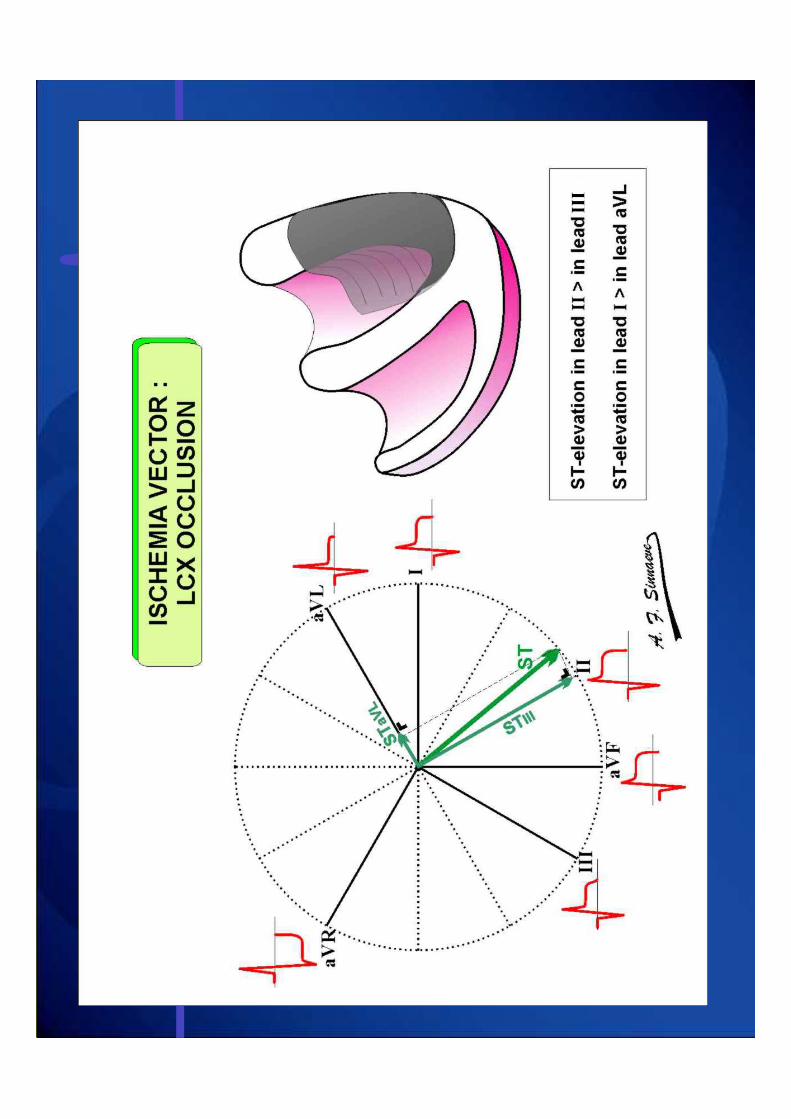
From “ECG uit of in het hoofd” Andries E, Stroobandt R, De Cock N et al., Garant, 2006
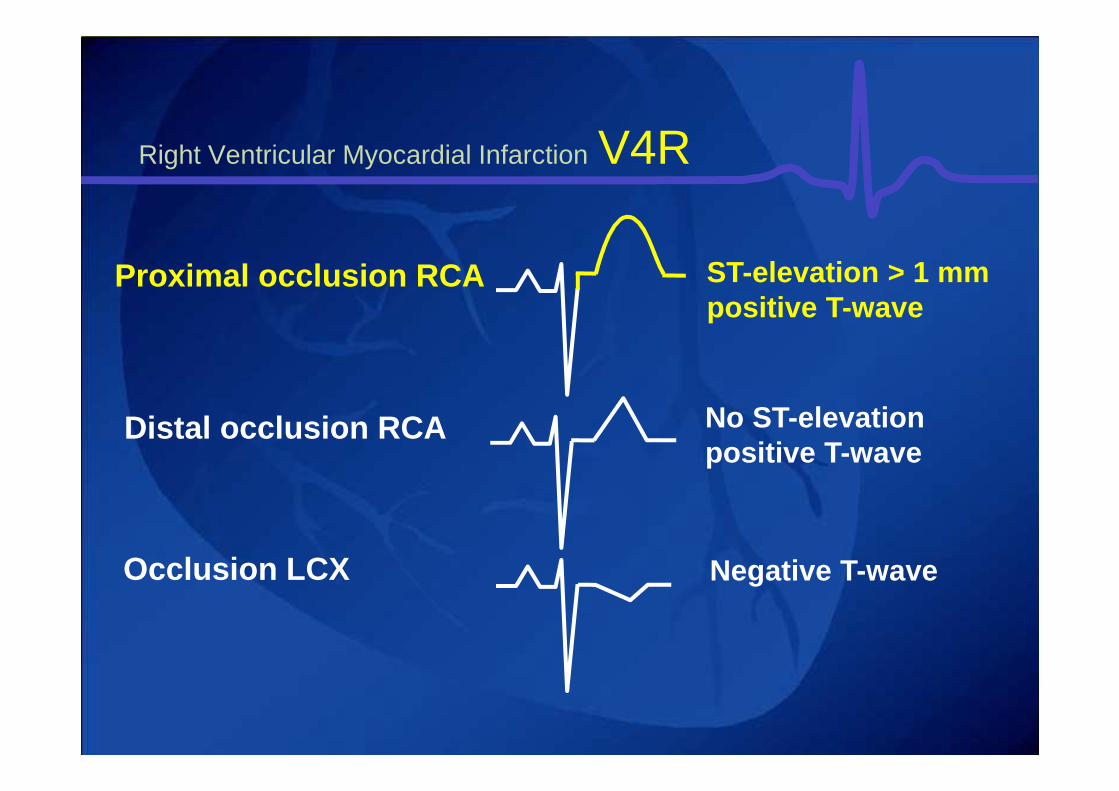
Proximal occlusion RCA ST-elevation > 1 mmpositive T-wave
Distal occlusion RCA No ST-elevationpositive T-wave
Occlusion LCX Negative T-wave
Right Ventricular Myocardial Infarction V4R
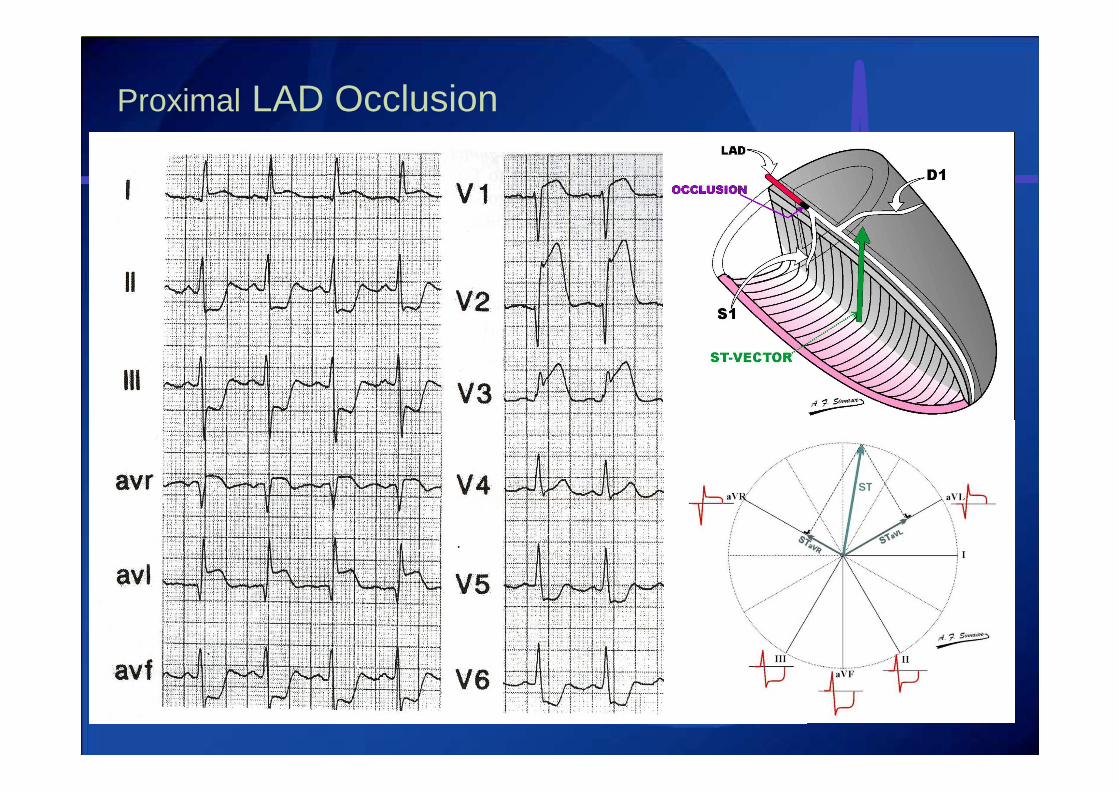
Proximal LAD Occlusion
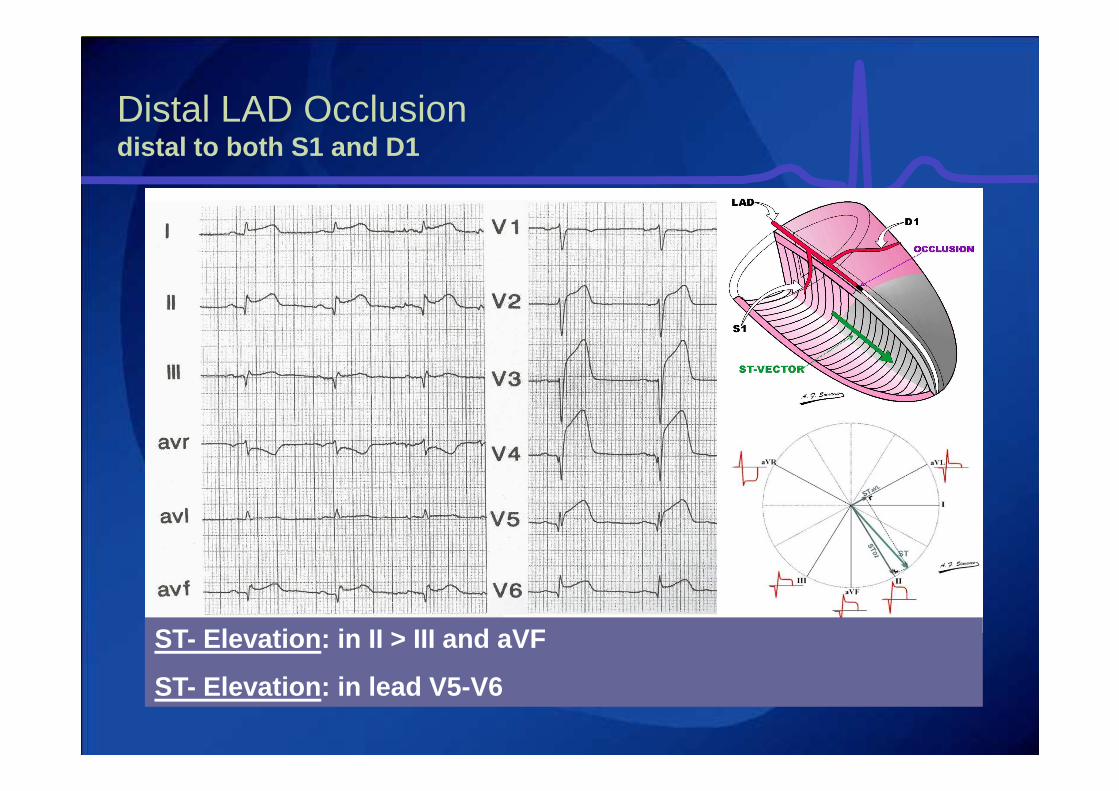
Distal LAD Occlusiondistal to both S1 and D1
ST- Elevation: in II > III and aVF
ST- Elevation: in lead V5-V6
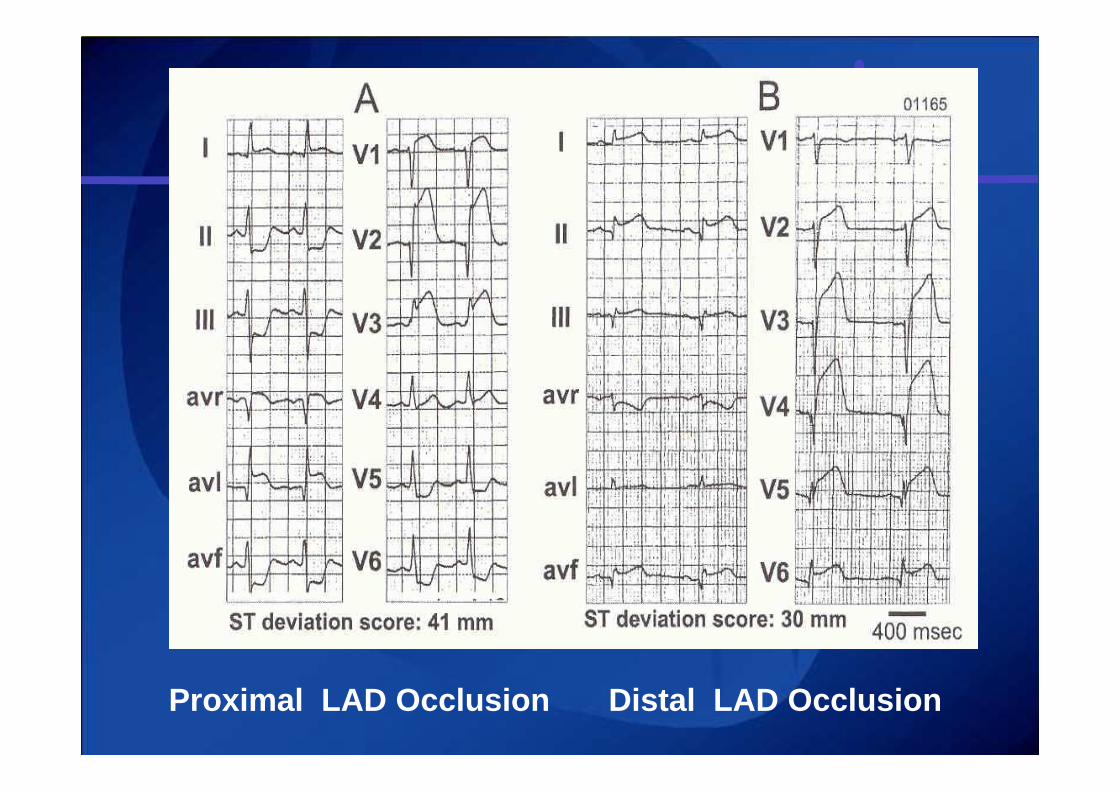
Proximal LAD Occlusion Distal LAD Occlusion
KEY POINT: Anterior infarction
DIAGNOSIS of anterior wall infarction
ST-elevation in the precordial leads V1 to V4
SITE of OCCLUSION in the LAD and AREA at RISKcan be recognized in the frontal leads
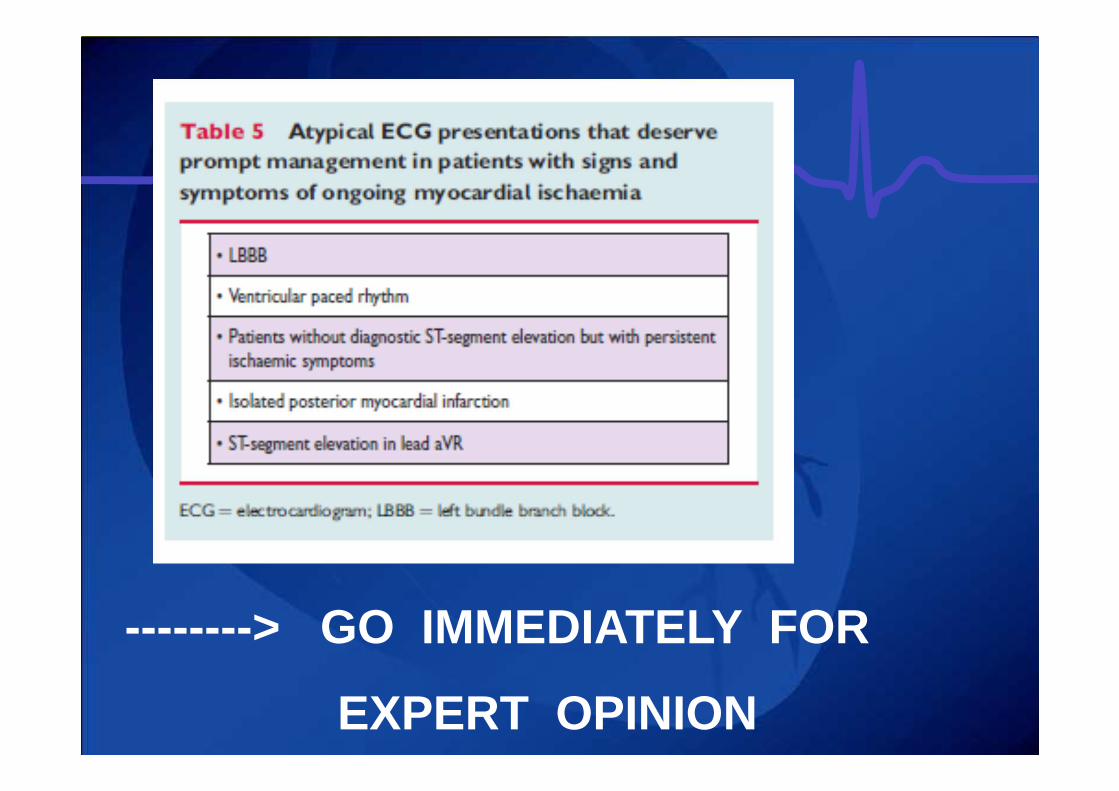
--------> GO IMMEDIATELY FOR
EXPERT OPINION
Case: 81 y old female
• Medical history:– no severe diseases– No cardiac risk factors– No medications
• Actual medical problem– Prolonged chest pain(>36h)– Last hours more dyspnea on exercise
(NYHA class ¾)– General malaise- dizziness- diaphoresis
Case: 81 y old female
• Clinical examination:– RR: 90/65 , heart rate 90 bpm,– Systolic murmur, – Normal CVP, bilateral lung crackles
(Killip 2)
• Labo:– Trop 10 ng/ml, creat 1.5mg%– NT-proBNP: >8000 pg/ml
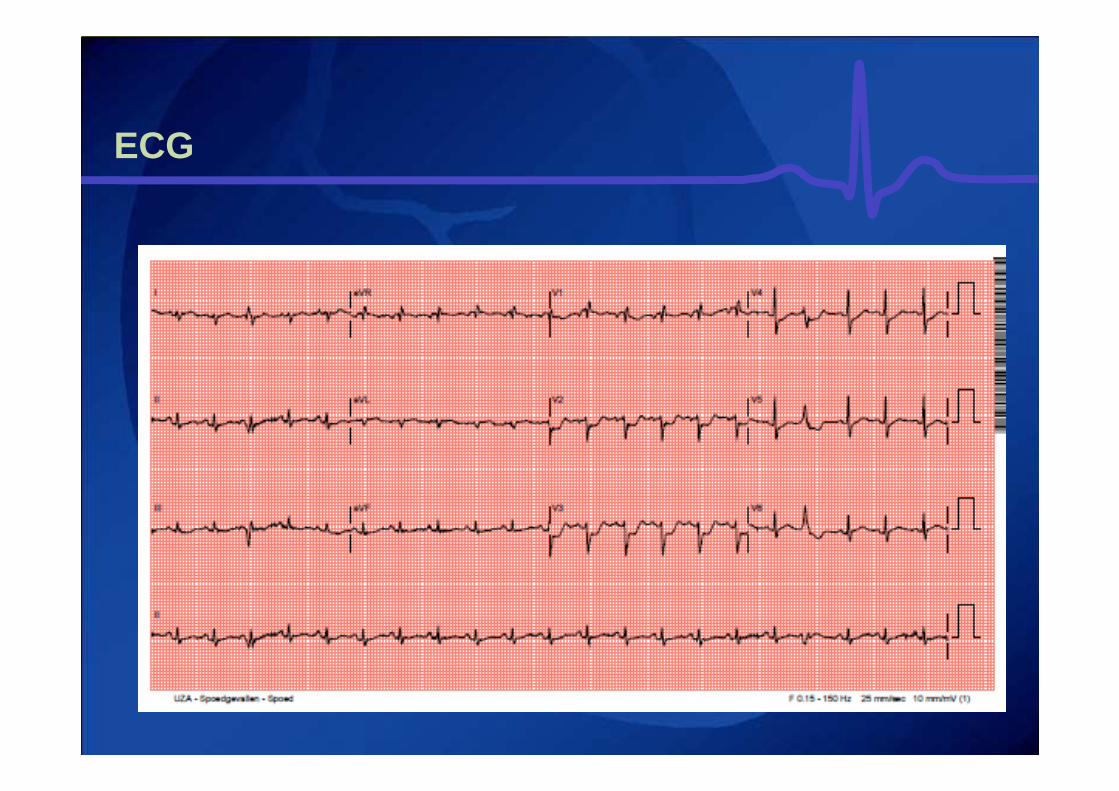
ECG
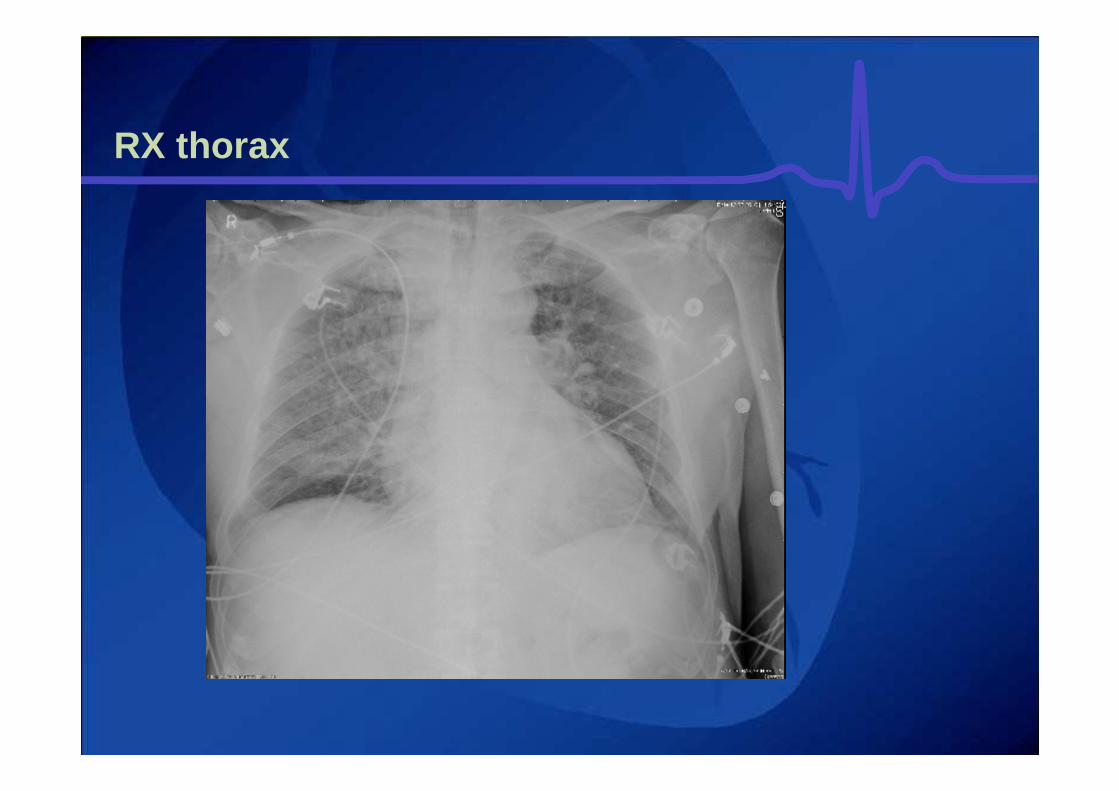
RX thorax
Case: 81 y old female
• Diagnostic evaluation:– Subacute posterior infarction– Signs of left cardiac failure – (evolution to cardiogenic shock)– Discrepancy between severity/extent of
ischemia and hemodynamic status
• Management– Echocardiography or cardiac
catheterisation– Medical treatment: ASA - UFH
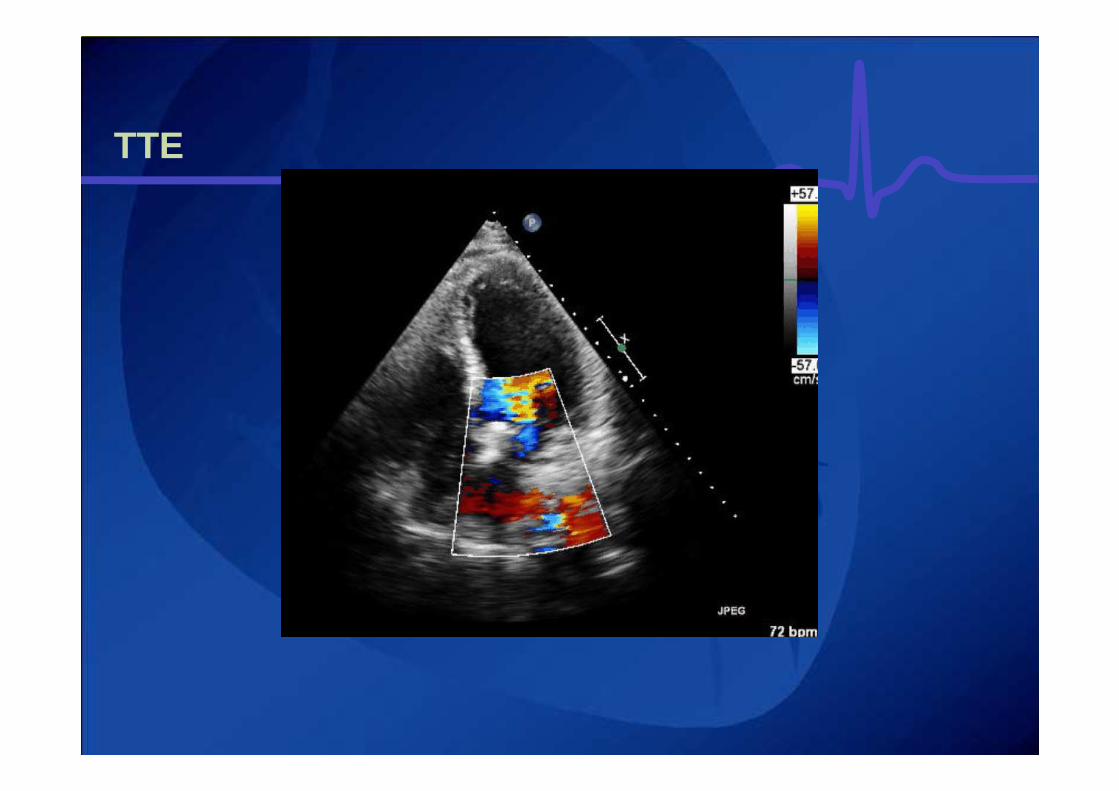
TTE
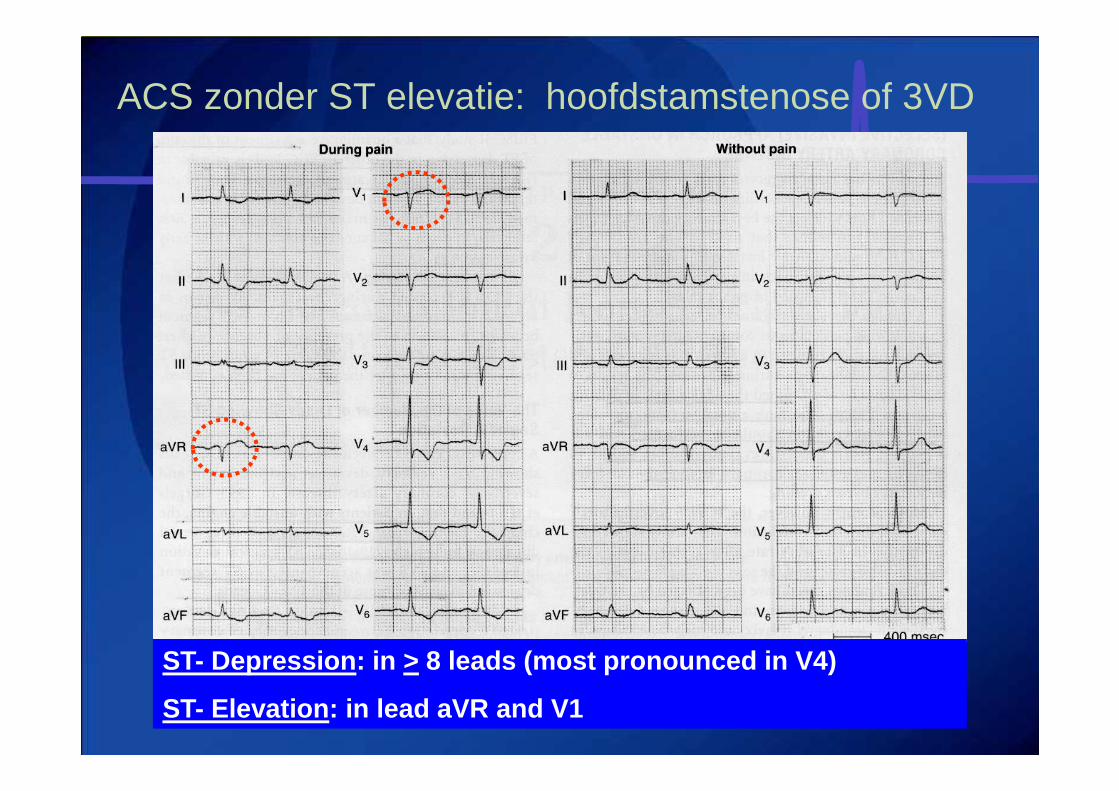
ACS zonder ST elevatie: hoofdstamstenose of 3VD
ST- Depression: in > 8 leads (most pronounced in V4)
ST- Elevation: in lead aVR and V1
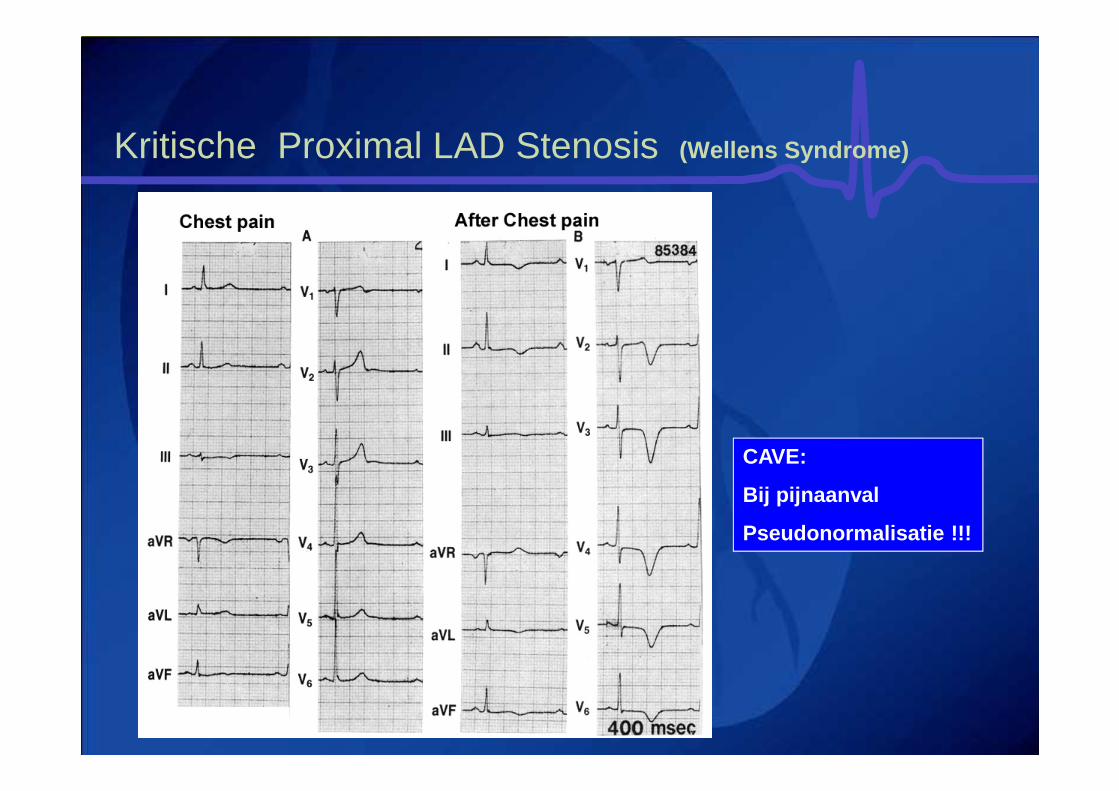
Kritische Proximal LAD Stenosis (Wellens Syndrome)
CAVE:
Bij pijnaanval
Pseudonormalisatie !!!
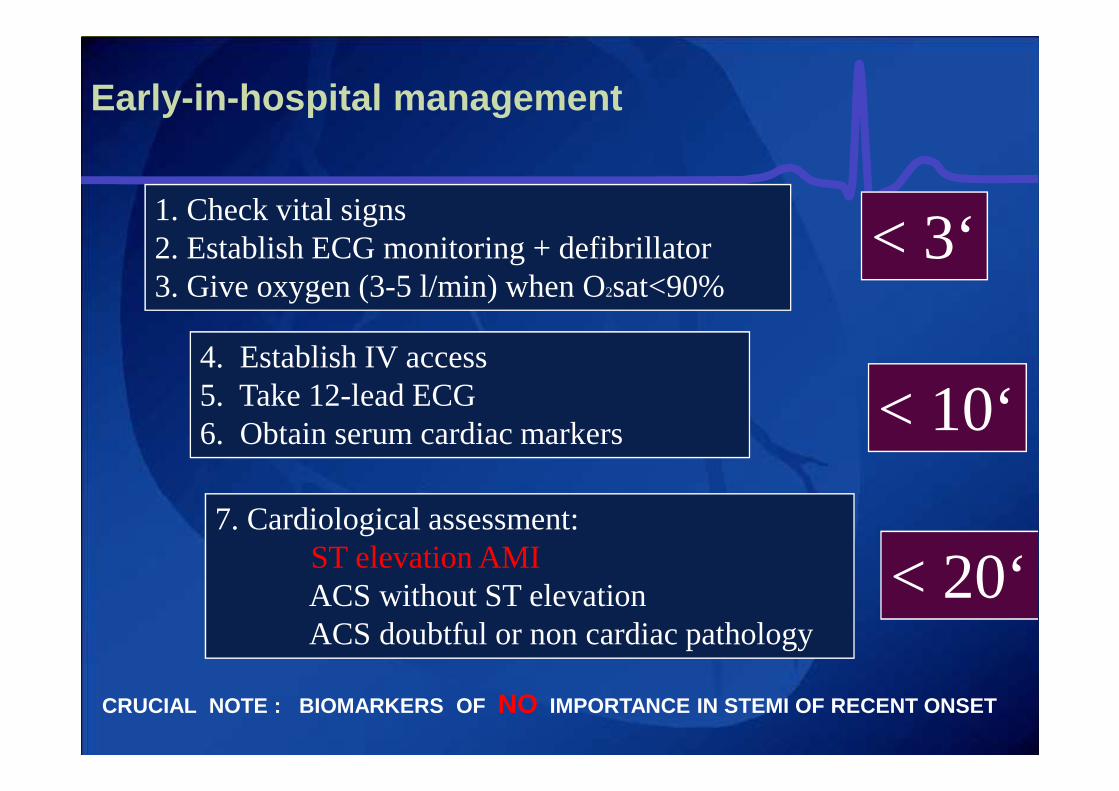
Early-in -hospital management
1. Check vital signs2. Establish ECG monitoring + defibrillator 3. Give oxygen (3-5 l/min) when O2sat<90%
4. Establish IV access5. Take 12-lead ECG6. Obtain serum cardiac markers
7. Cardiological assessment:ST elevation AMIACS without ST elevationACS doubtful or non cardiac pathology
< 3‘
< 10‘
< 20‘
CRUCIAL NOTE : BIOMARKERS OF NO IMPORTANCE IN STEMI OF RECENT ONSET
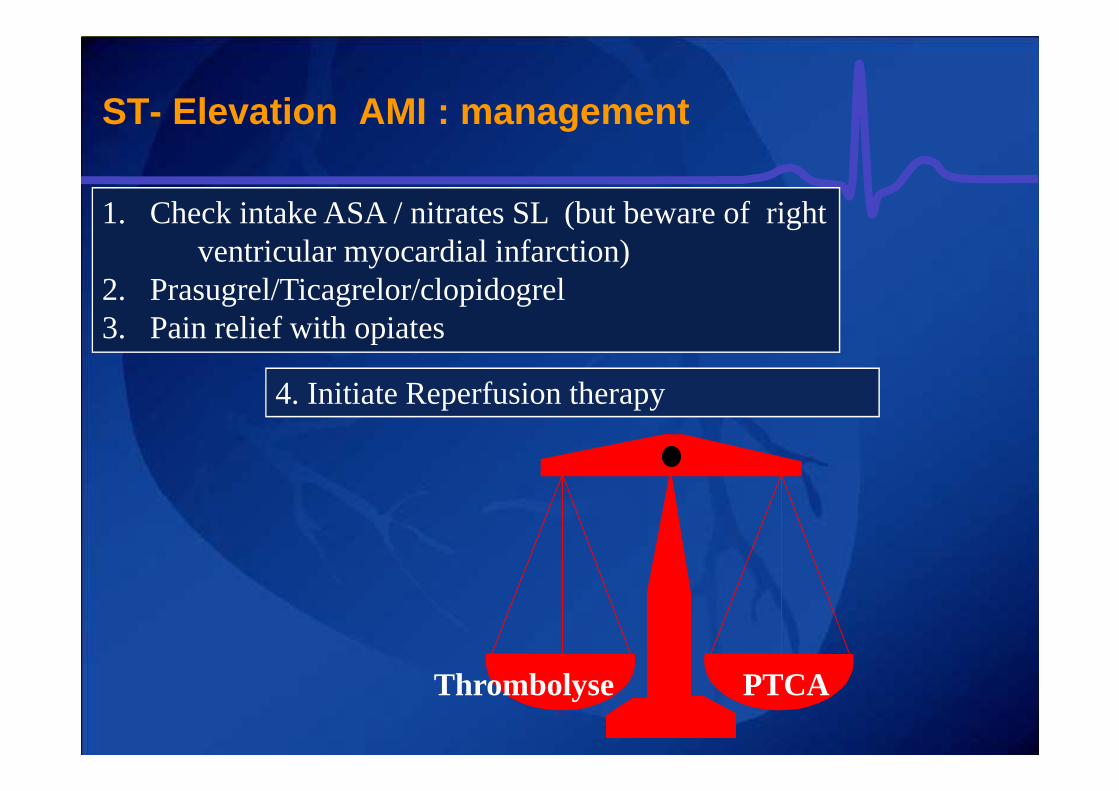
ST- Elevation AMI : management
1. Check intake ASA / nitrates SL (but beware of right ventricular myocardial infarction)
2. Prasugrel/Ticagrelor/clopidogrel3. Pain relief with opiates
4. Initiate Reperfusion therapy
Thrombolyse PTCA
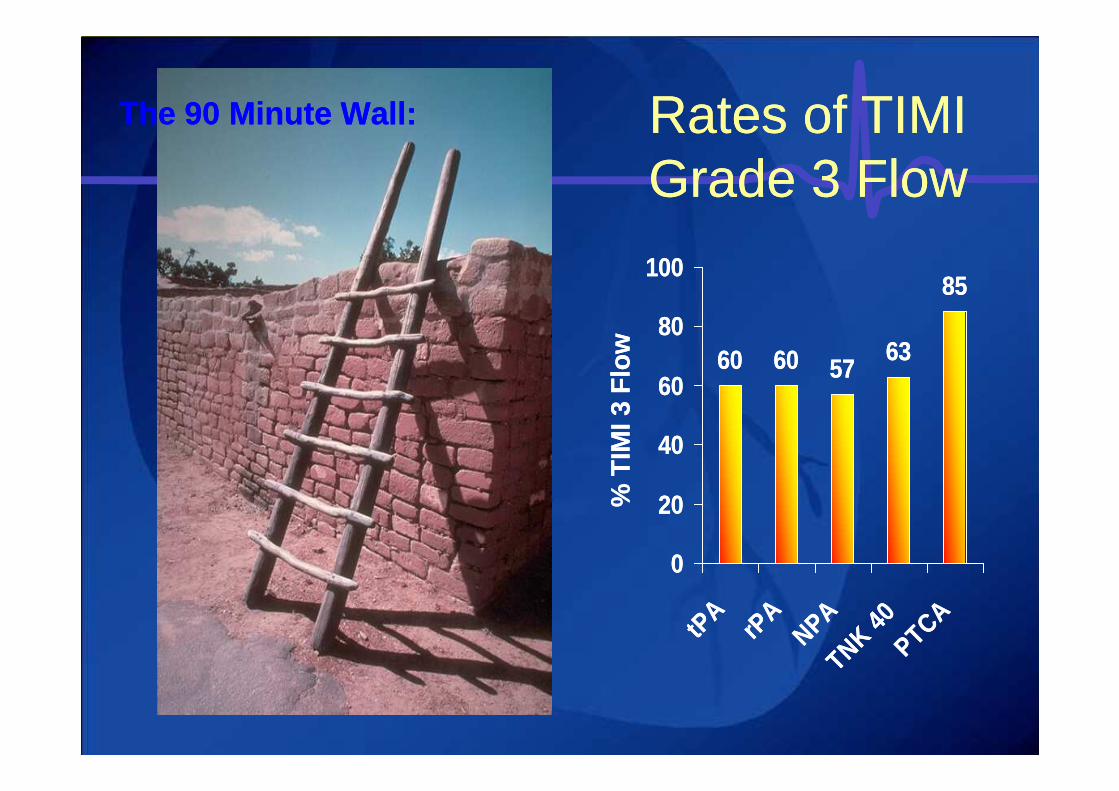
60 60 5763
85
0
20
40
60
80
100
tPA
rPA
NPATNK 40
PTCA
60 60 5763
85
0
20
40
60
80
100
tPA
rPA
NPATNK 40
PTCA
The 90 Minute Wall:The 90 Minute Wall: Rates of TIMI Grade 3 FlowRates of TIMI Grade 3 Flow
% T
IMI 3
Flo
w%
TIM
I 3 F
low
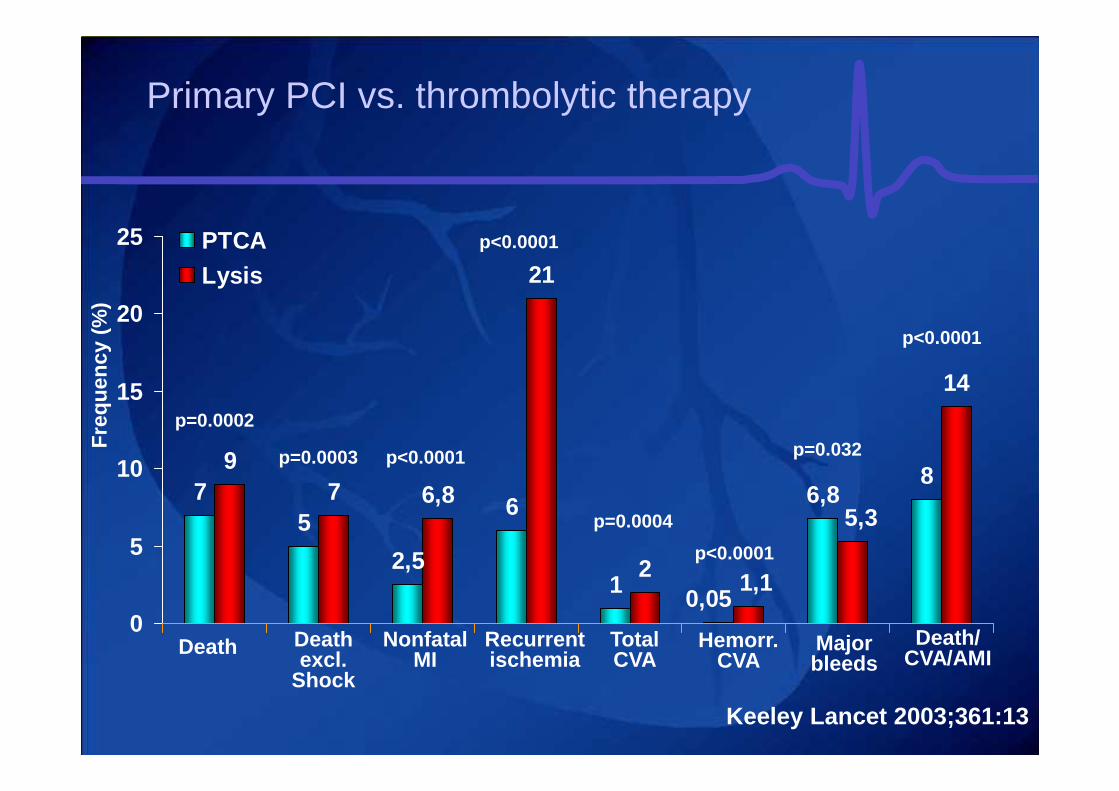
Primary PCI vs. thrombolytic therapy
Keeley Lancet 2003;361:13
75
2,5
6
1
6,88
97 6,8
21
2
14
0,05
5,3
1,1
0
5
10
15
20
25 PTCALysis
Death Death excl.
Shock
Nonfatal MI
Recurrent ischemia
Total CVA
Hemorr. CVA
Major bleeds
Death/ CVA/AMI
p=0.0002
p=0.0003 p<0.0001
p<0.0001
p=0.0004
p<0.0001
p=0.032
p<0.0001
Fre
quen
cy (
%)
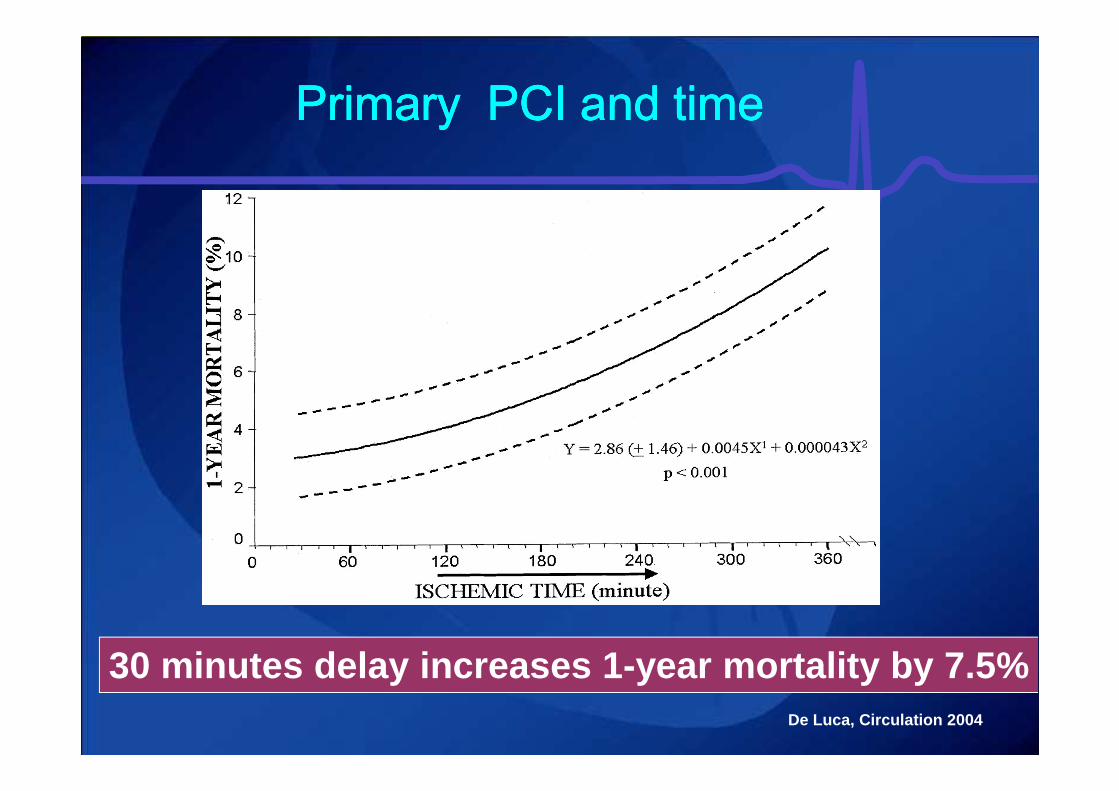
De Luca, Circulation 2004
Primary PCI and timePrimary PCI and timePrimary PCI and timePrimary PCI and time
30 minutes delay increases 1-year mortality by 7.5%
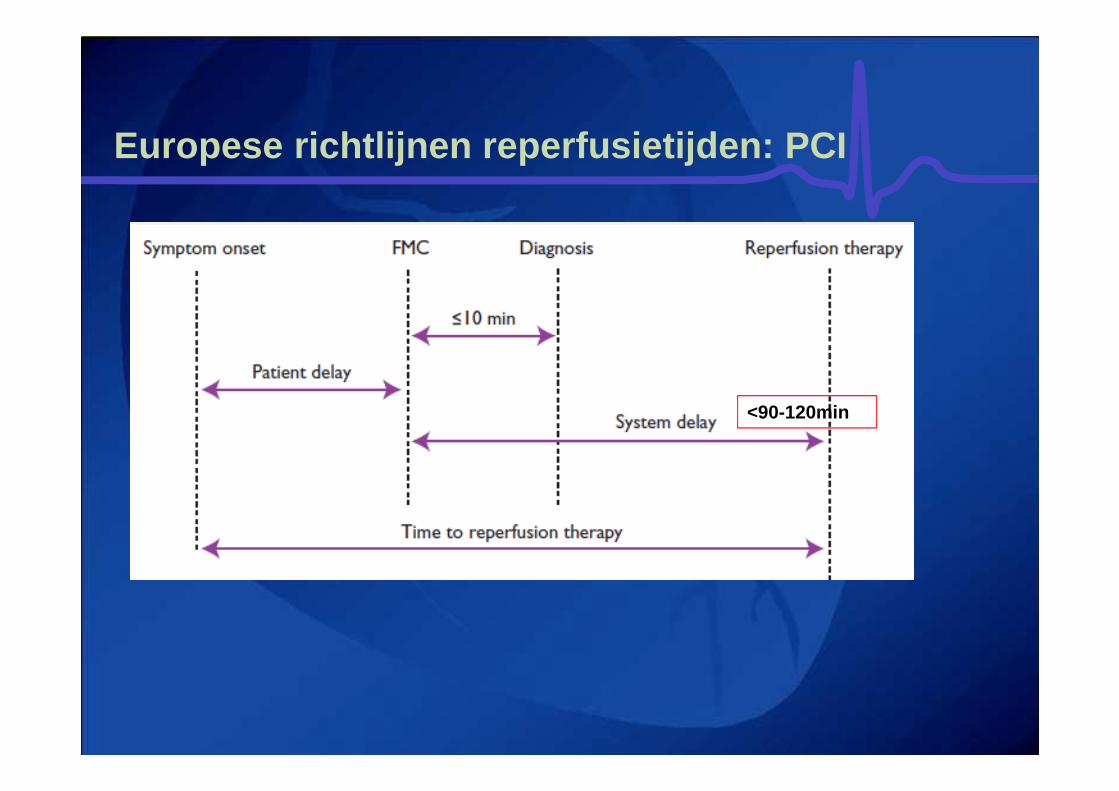
Europese richtlijnen reperfusietijden : PCI
<90-120min
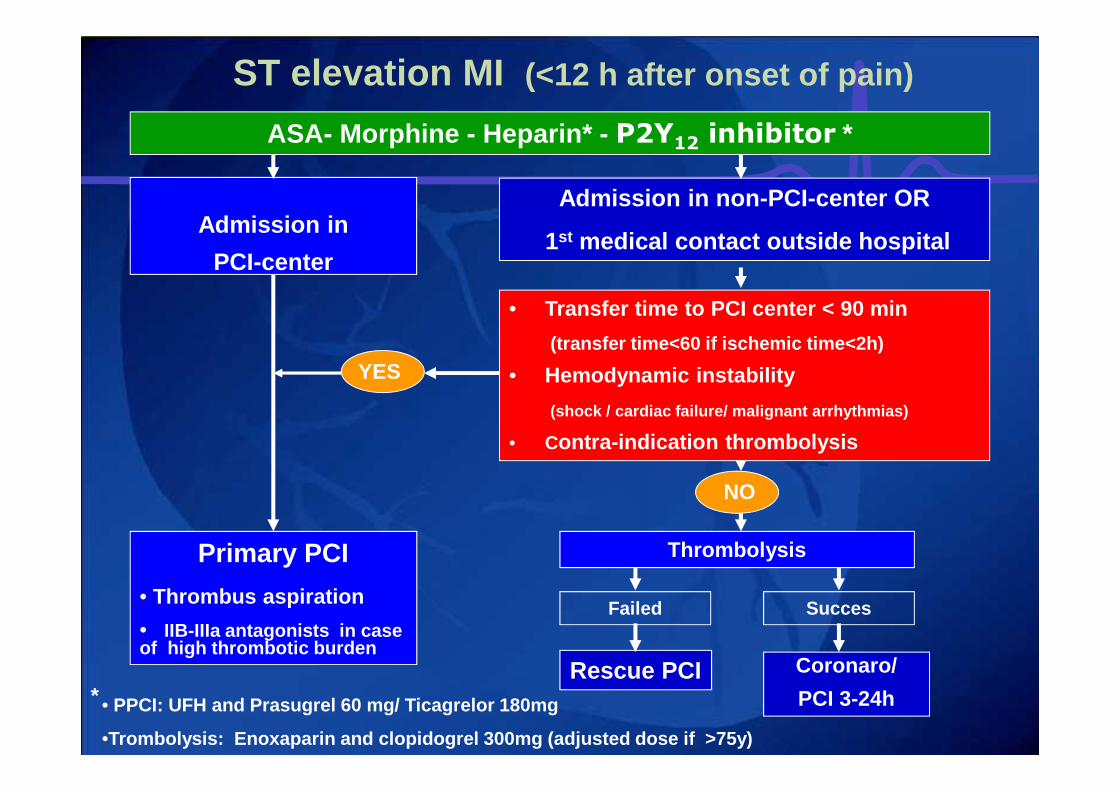
ST elevation MI (<12 h after onset of pain)
Admission in
PCI-center
Primary PCI
• Thrombus aspiration
• IIB-IIIa antagonists in case of high thrombotic burden
Admission in non-PCI-center OR
1st medical contact outside hospital
• Transfer time to PCI center < 90 min
(transfer time<60 if ischemic time<2h)
• Hemodynamic instability
(shock / cardiac failure/ malignant arrhythmias)
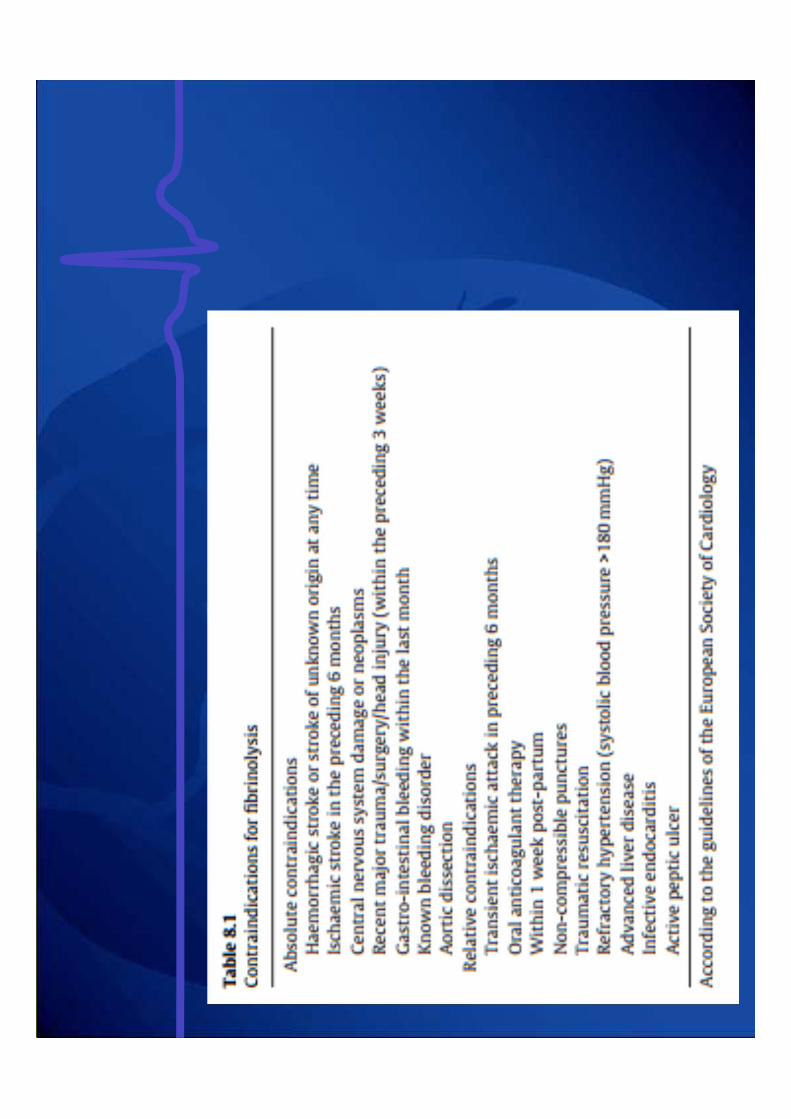
• Contra-indication thrombolysis
Thrombolysis
YES
NO
• PPCI: UFH and Prasugrel 60 mg/ Ticagrelor 180mg
•Trombolysis: Enoxaparin and clopidogrel 300mg (adjus ted dose if >75y)
ASA- Morphine - Heparin* - P2Y12 inhibitor *
Failed
Rescue PCI
Succes
Coronaro/
PCI 3-24h*

STEMI: prehospital pretreatment
• ATLANTIC TRIAL (30 min difference in Tica)
PrehospTica
InhospTica
Death 30d 3.3% 2.0%
Stent tromb 0.2% 1.2%*
NEJM 2014:371:1061
---------> MARGINAL, IF ANY, BENEFIT
Early -in-hospital management forall potentially ACS patients
1. Check vital signs2. Establish ECG monitoring + defibrillator 3. Give oxygen (3-5 l/min) when O2sat<90%
4. Establish IV access5. Take 12-lead ECG6. Obtain serum cardiac markers
7. Cardiological assessment:ST elevation AMI ACS without ST elevationACS doubtful or non cardiac pathology
< 3‘
< 10‘
< 20‘

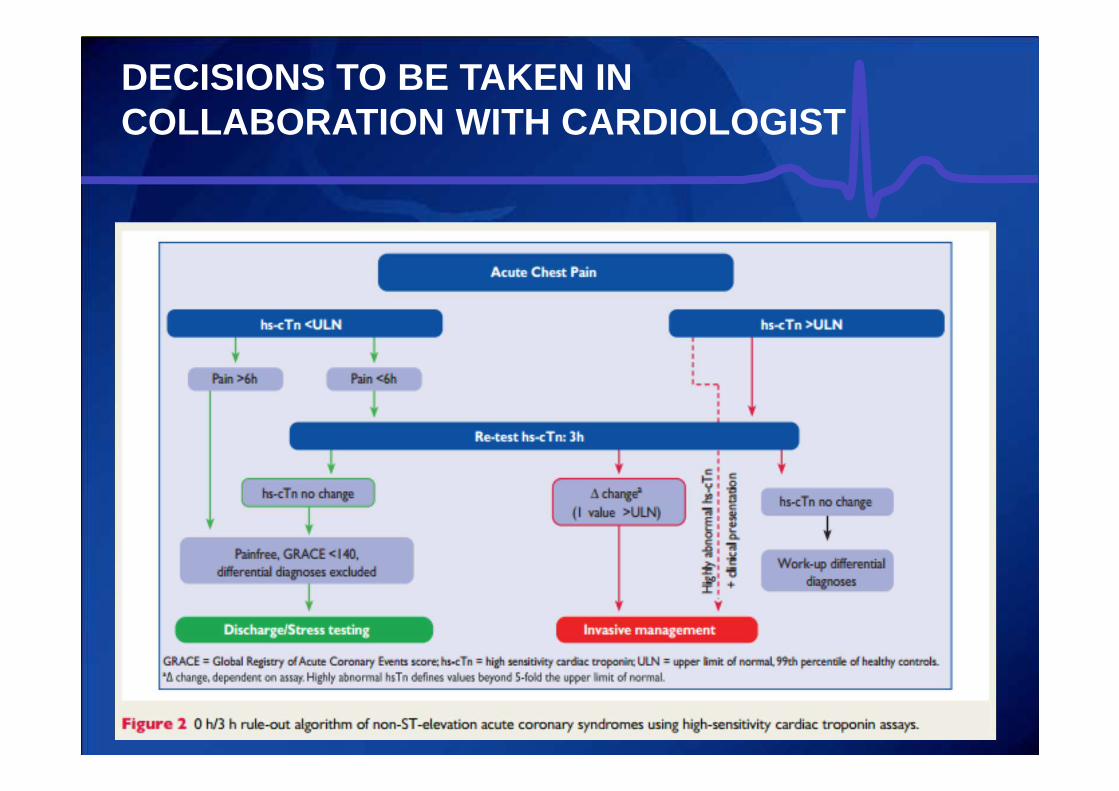
DECISIONS TO BE TAKEN IN COLLABORATION WITH CARDIOLOGIST
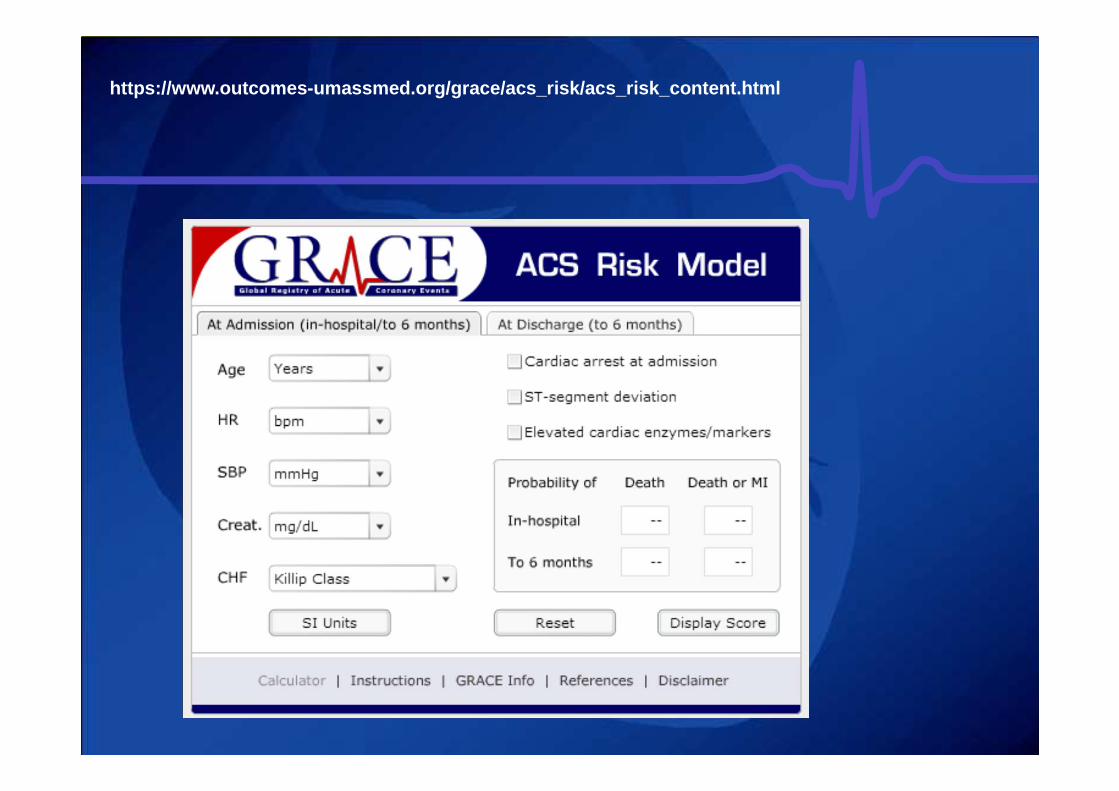
https://www.outcomes-umassmed.org/grace/acs_risk/ac s_risk_content.html
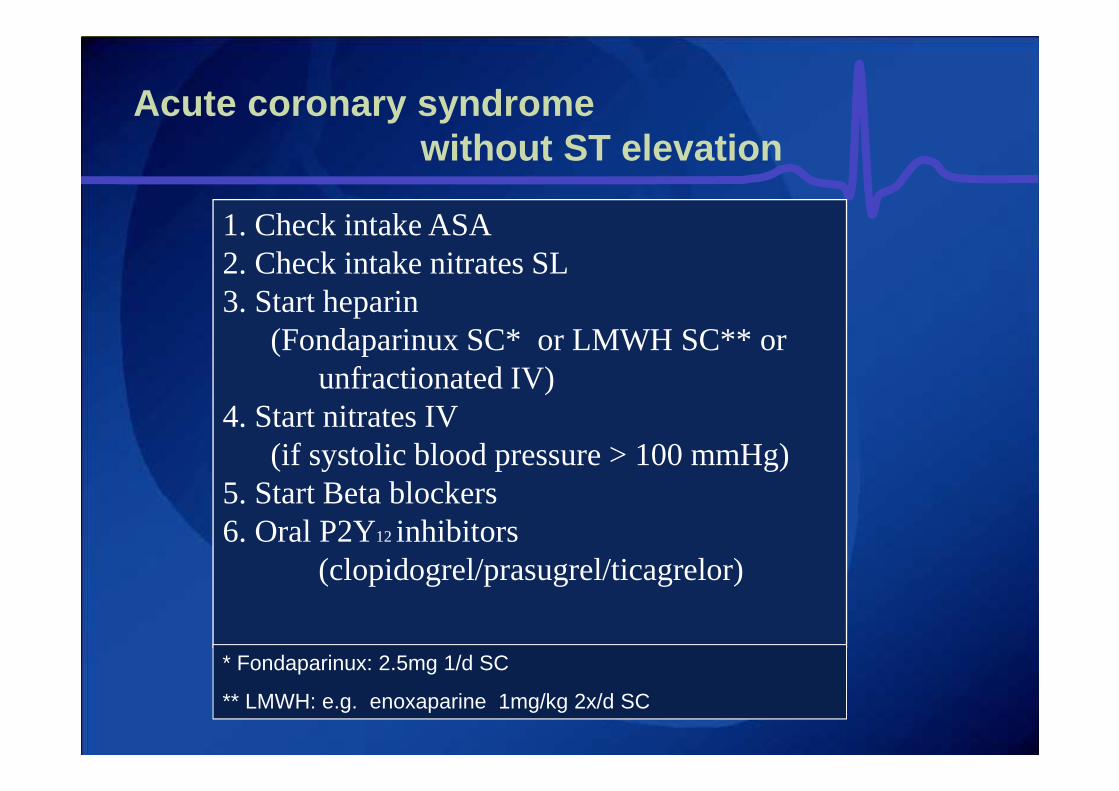
Acute coronary syndrome without ST elevation
1. Check intake ASA 2. Check intake nitrates SL3. Start heparin
(Fondaparinux SC* or LMWH SC** or unfractionated IV)
4. Start nitrates IV (if systolic blood pressure > 100 mmHg)
5. Start Beta blockers6. Oral P2Y12 inhibitors
(clopidogrel/prasugrel/ticagrelor)
* Fondaparinux: 2.5mg 1/d SC
** LMWH: e.g. enoxaparine 1mg/kg 2x/d SC
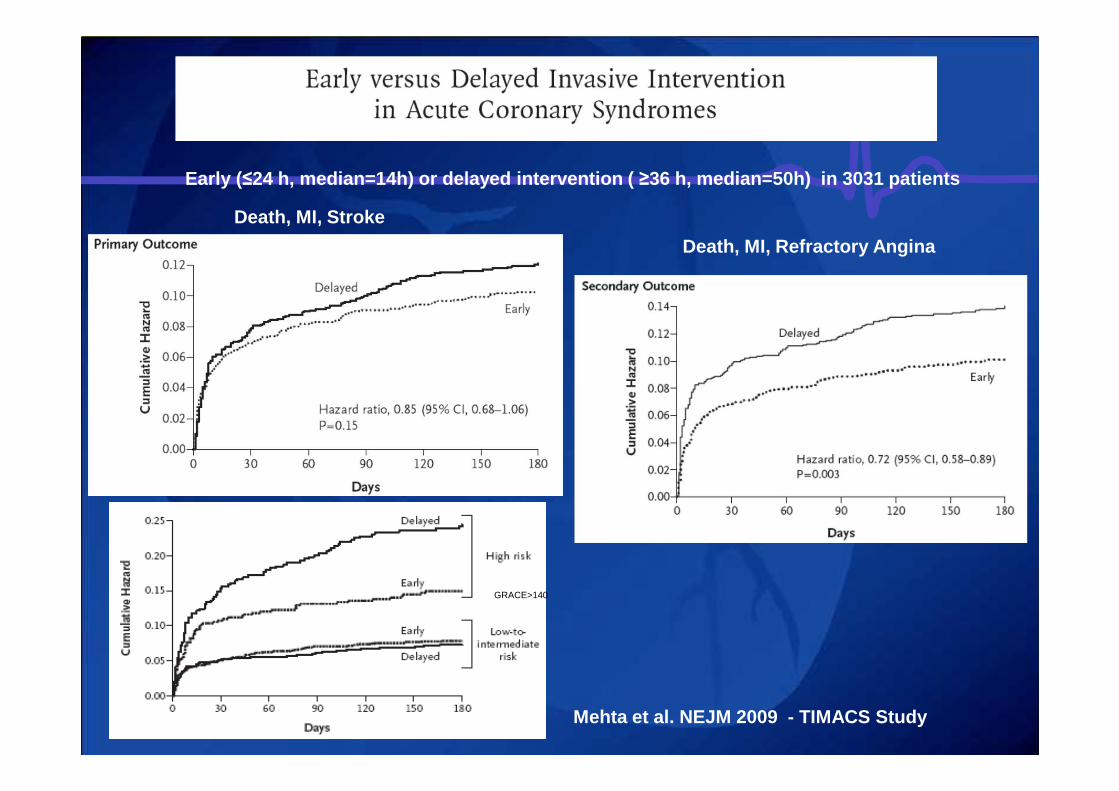
Mehta et al. NEJM 2009 - TIMACS Study
Early ( ≤24 h, median=14h) or delayed intervention ( ≥36 h, median=50h) in 3031 patients
Death, MI, Refractory Angina
Death, MI, Stroke
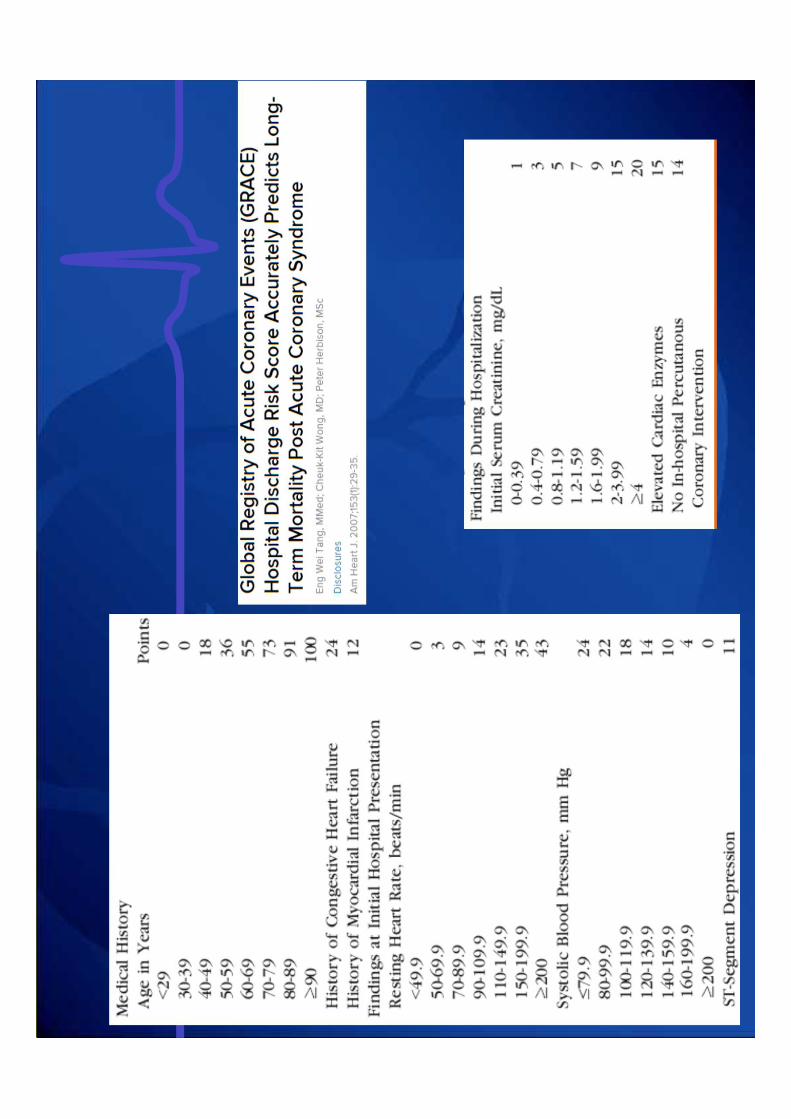
GRACE>140
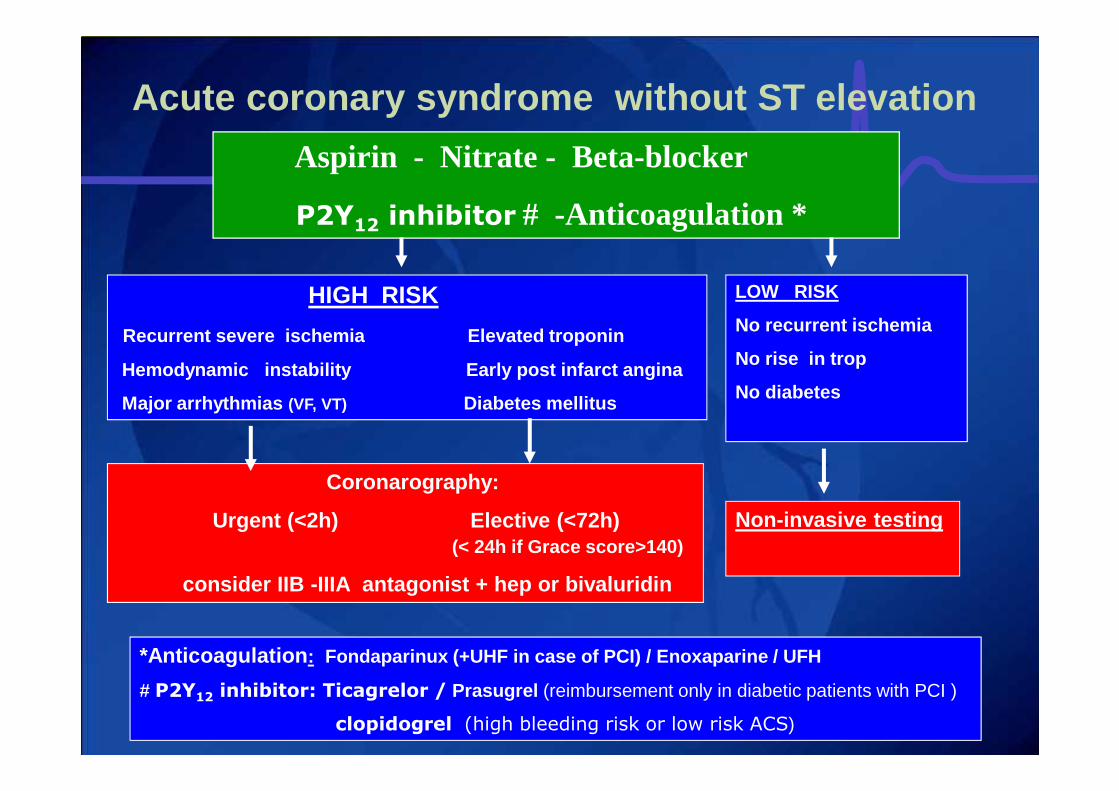
Acute coronary syndrome without ST elevation
Aspirin - Nitrate - Beta-blocker
P2Y12 inhibitor # -Anticoagulation *
*Anticoagulation : Fondaparinux (+UHF in case of PCI) / Enoxaparine / U FH
# P2Y12 inhibitor: Ticagrelor / Prasugrel (reimbursement only in diabetic patients with PCI )
clopidogrel (high bleeding risk or low risk ACS)
HIGH RISK
Recurrent severe ischemia Elevated troponin
Hemodynamic instability Early post infarct angina
Major arrhythmias (VF, VT) Diabetes mellitus
Coronarography:
Urgent (<2h) Elective (<72h)(< 24h if Grace score>140)
consider IIB -IIIA antagonist + hep or bivaluridin
LOW RISK
No recurrent ischemia
No rise in trop
No diabetes
Non-invasive testing
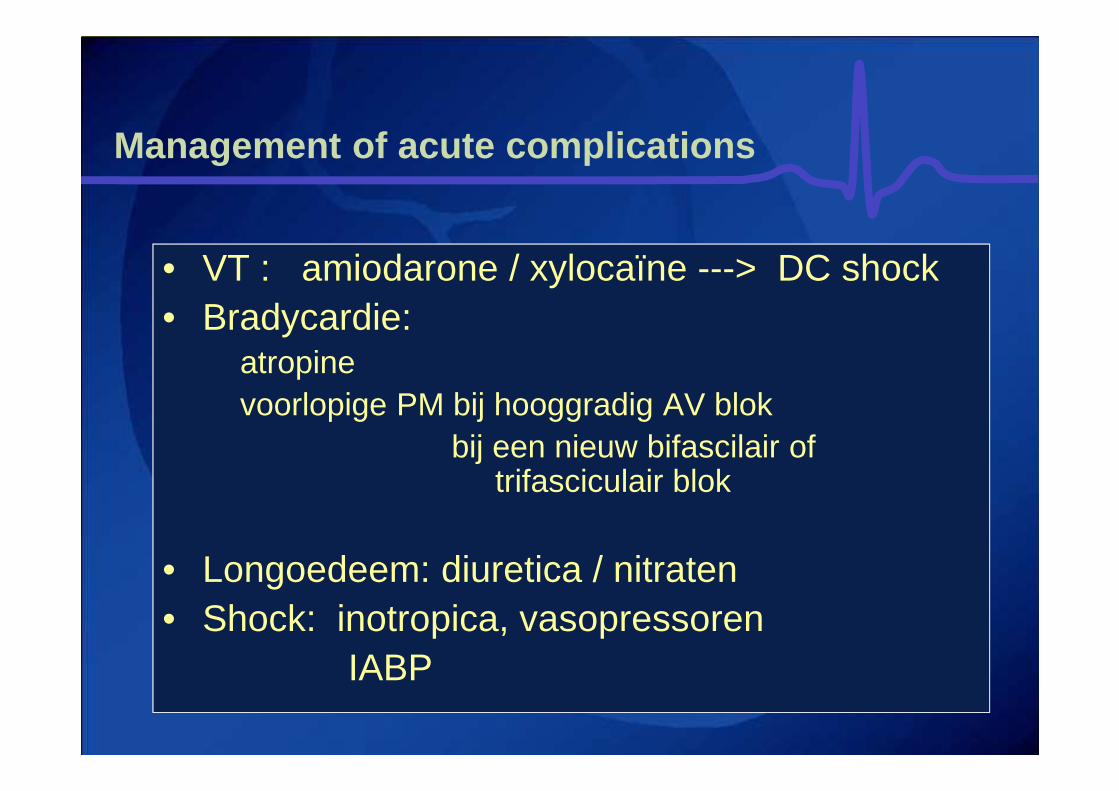
Management of acute complications
• VT : amiodarone / xylocaïne ---> DC shock• Bradycardie:
atropinevoorlopige PM bij hooggradig AV blok
bij een nieuw bifascilair of trifasciculair blok
• Longoedeem: diuretica / nitraten• Shock: inotropica, vasopressoren
IABP
57
Bradycardie
Definitie < 60/min• Sinusbradycardie
Acuut inferior infarct, medicamenteus, fysiologisch
• Sick sinussyndroomSinusbradycardieSinusarrest
• AV-blokTweede graadsDerde graads
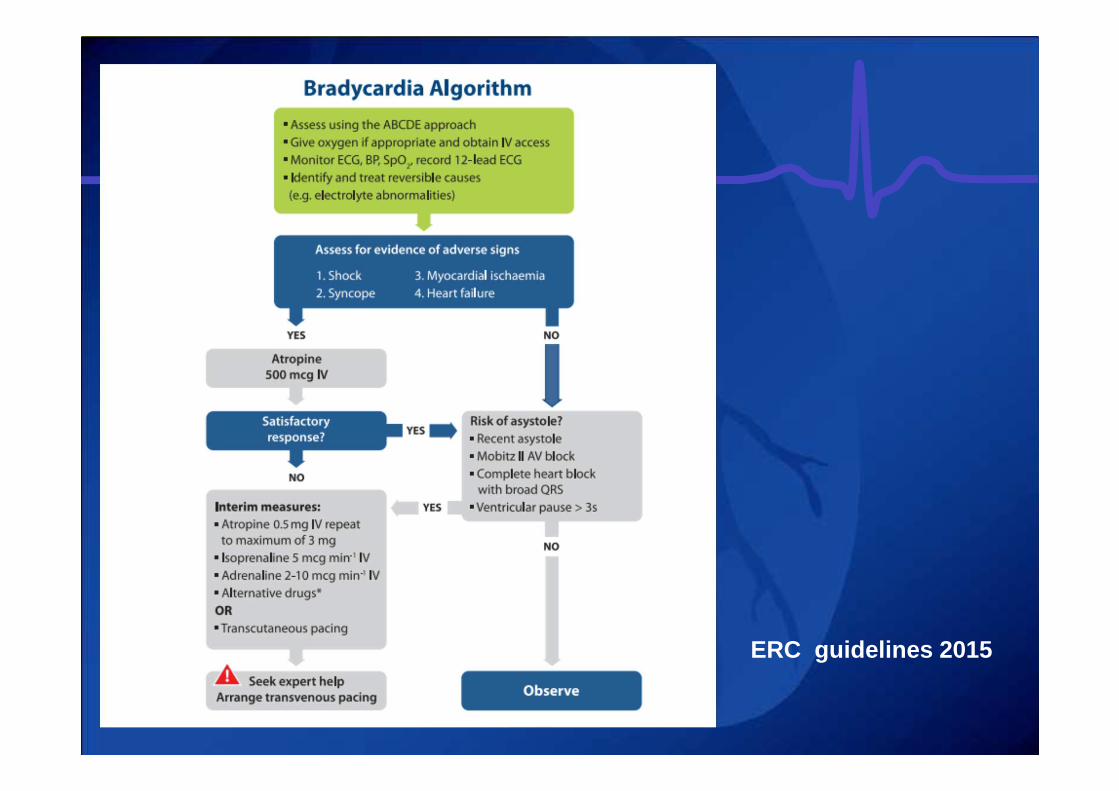
ERC guidelines 2015
- Aminophylline (100 – 200 mg slow IV injection) shouldbe considered if bradycardia is caused by inferior MI, cardiac transplant or spinal cord injury
- Glucagon dose: 0,05 mg/kg IV loading dose, followed b y1 to 15 mg/hour
- Do not give atropine to patients with cardiac transplant as it can cause high-degree AV block and sinus arrest