
Oncologie in Perspectief Neoadjuvante CT · ER neg HER2 pos Triple neg . Waarom neoadjuvante CT ......
94
Oncologie in Perspectief Maatwerk in 2016 Neoadjuvante CT Marie-Jeanne Vrancken Peeters Oncologisch Chirurg Antoni van Leeuwenhoek NKI
Transcript of Oncologie in Perspectief Neoadjuvante CT · ER neg HER2 pos Triple neg . Waarom neoadjuvante CT ......

Oncologie in Perspectief Maatwerk in 2016 Neoadjuvante CT
Marie-Jeanne Vrancken Peeters Oncologisch Chirurg Antoni van Leeuwenhoek NKI
Maatwerk bij NAC voor BK
Introductie
Waarom neoadjuvante chemotherapie
Locale behandeling op maat na NAC
Praktische “take home messages”
QUIZ: borstkankerboek
1. Hoeveel mannen en vrouwen in NL
kregen in 2015 borstkanker?
QUIZ: borstkankerboek
2. a. Hoeveel % van de BK patienten in NL
wordt met NAC behandeld?
b. Hoeveel % van de BK patienten in NL
wordt krijgt adjuvante CT?
Dedicated Breast Cancer Team
Gabe Sonke
Emiel Rutgers
Marie Jeanne Vrancken Peeters
Paula Elkhuizen
Sabine Linn
Hester Oldenburg
Carolien Smorenburg
Claudette Loo
Jacqueline Stouthard
Nicola Russell EORTC
BOOG
NABON
Leonie Woerdeman NBCA
LPRM
BOOG
Bestuur Pathologie
NVCO/ NBCA
Pink Ribbon Richtlijn
reconstructies
Bevolkings-onderzoek
Frederieke van Duijnhoven
Jos vd Hage
Gonneke Winter
Introductie
Jelle Wesseling
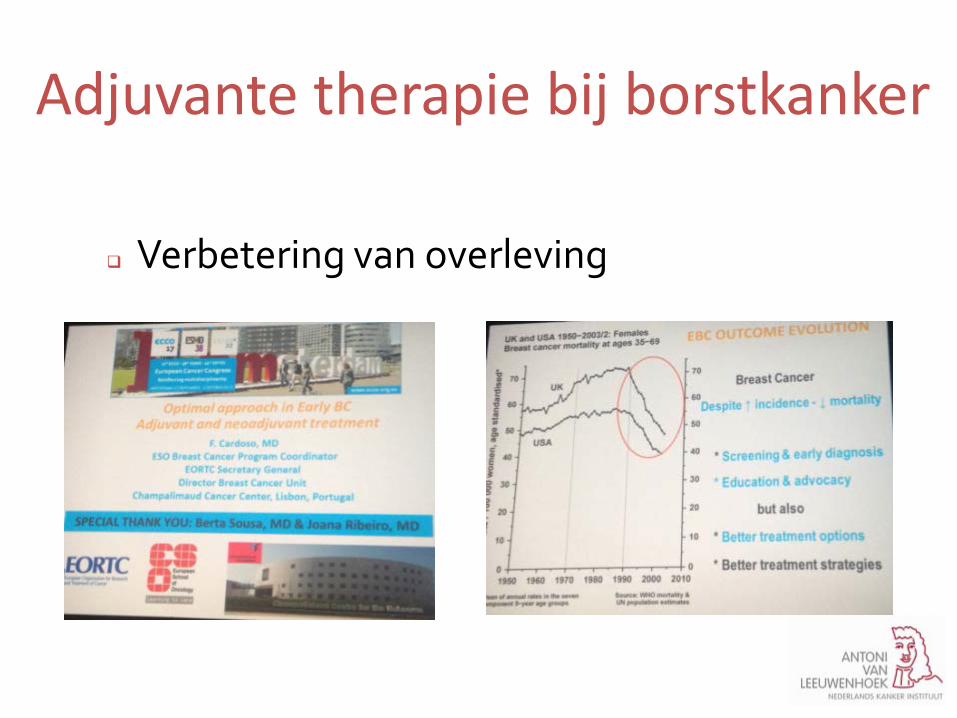
Verbetering van overleving
Adjuvante therapie bij borstkanker
Neoadjuvante therapie bij BK
Verbetering van overleving
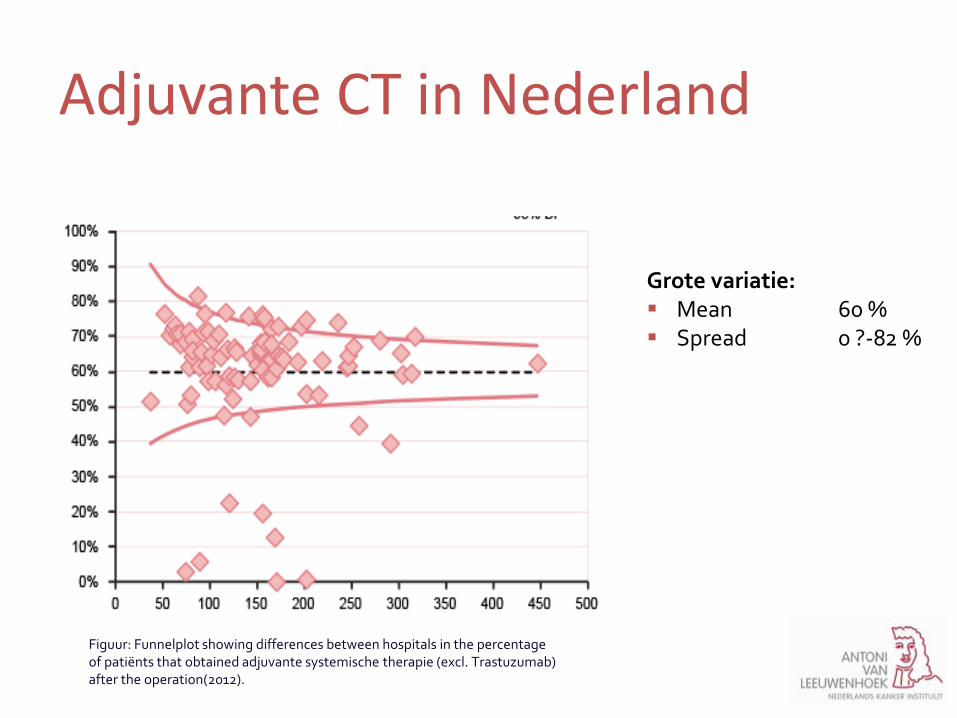
Adjuvante CT in Nederland
Figuur: Funnelplot showing differences between hospitals in the percentage of patiënts that obtained adjuvante systemische therapie (excl. Trastuzumab) after the operation(2012).
Grote variatie: Mean 60 % Spread 0 ?-82 %
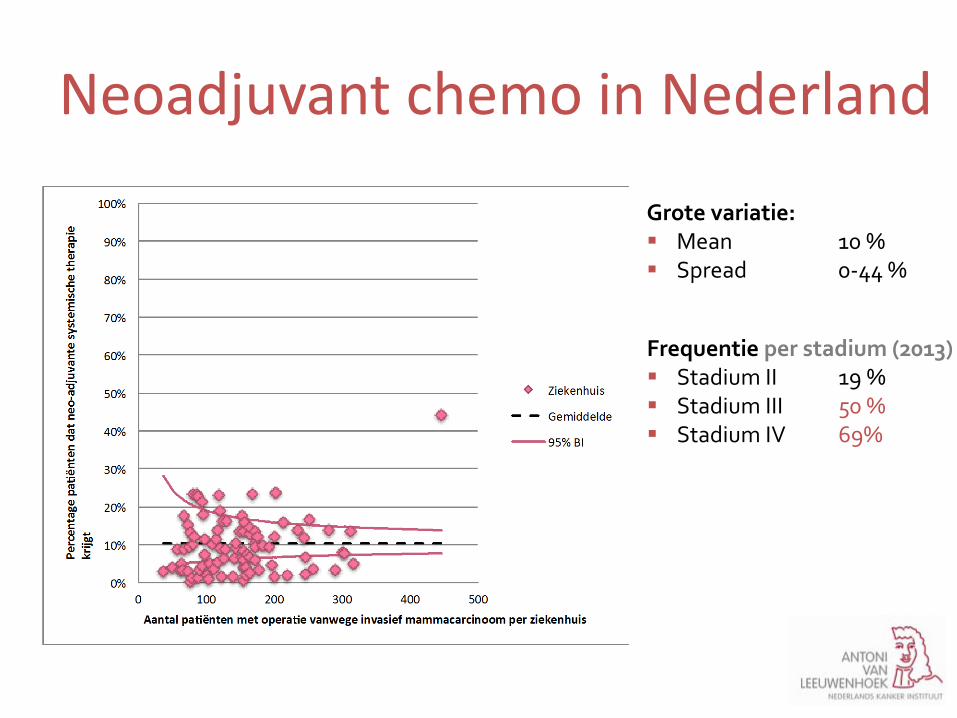
Neoadjuvant chemo in Nederland
– NBCA = NABON Breast Cancer Audit
Frequentie per stadium (2013) Stadium II 19 % Stadium III 50 % Stadium IV 69%
Grote variatie: Mean 10 % Spread 0-44 %
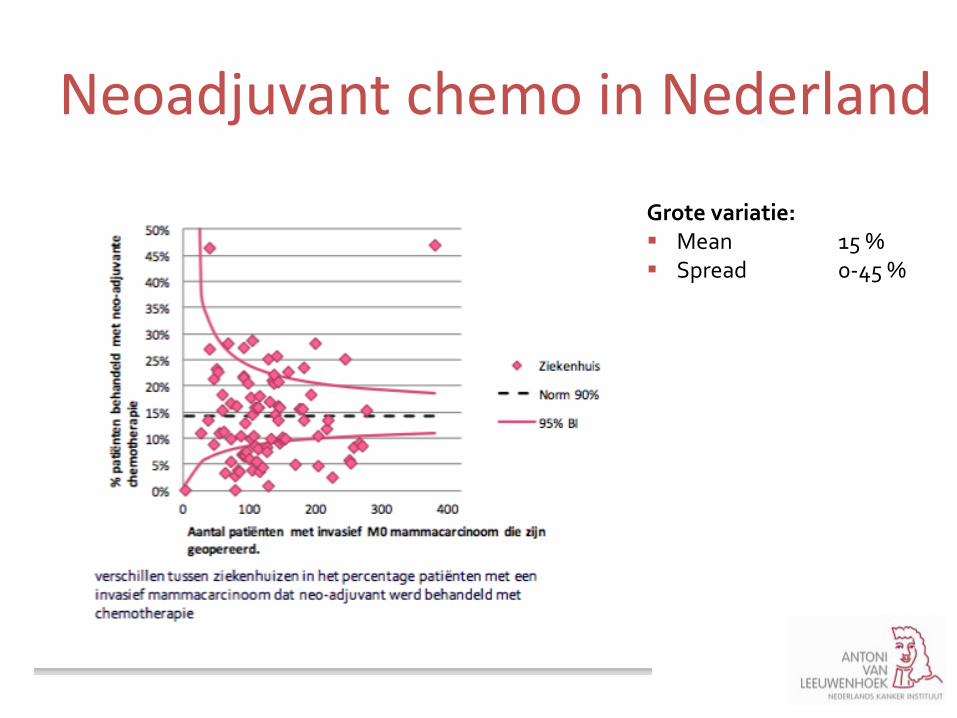
Neoadjuvant chemo in Nederland – NBCA = NABON Breast Cancer Audit
Grote variatie: Mean 15 % Spread 0-45 %
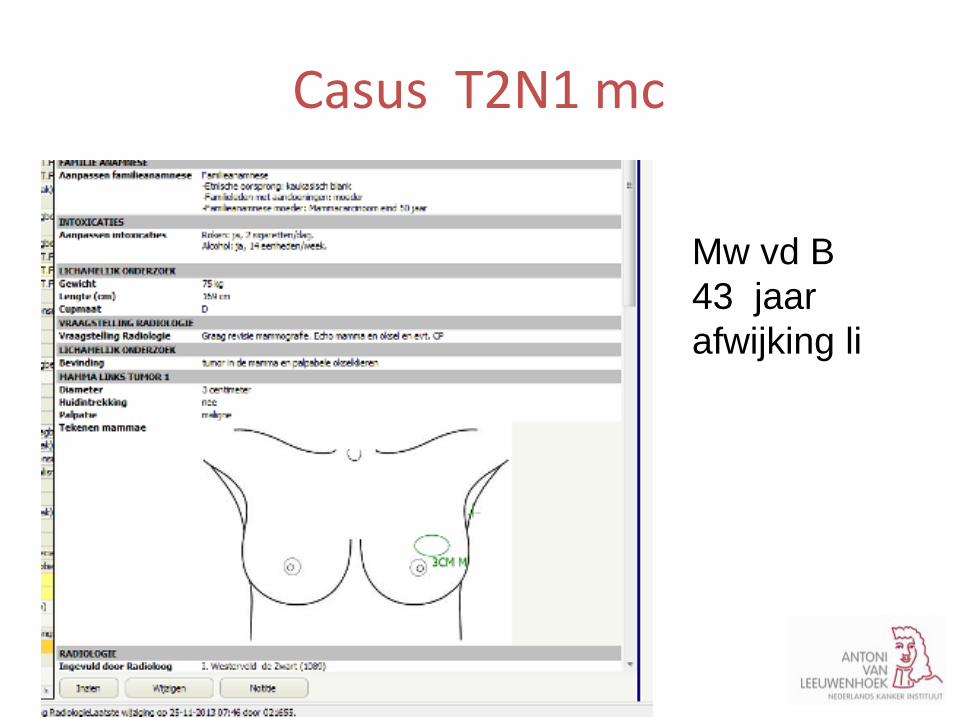
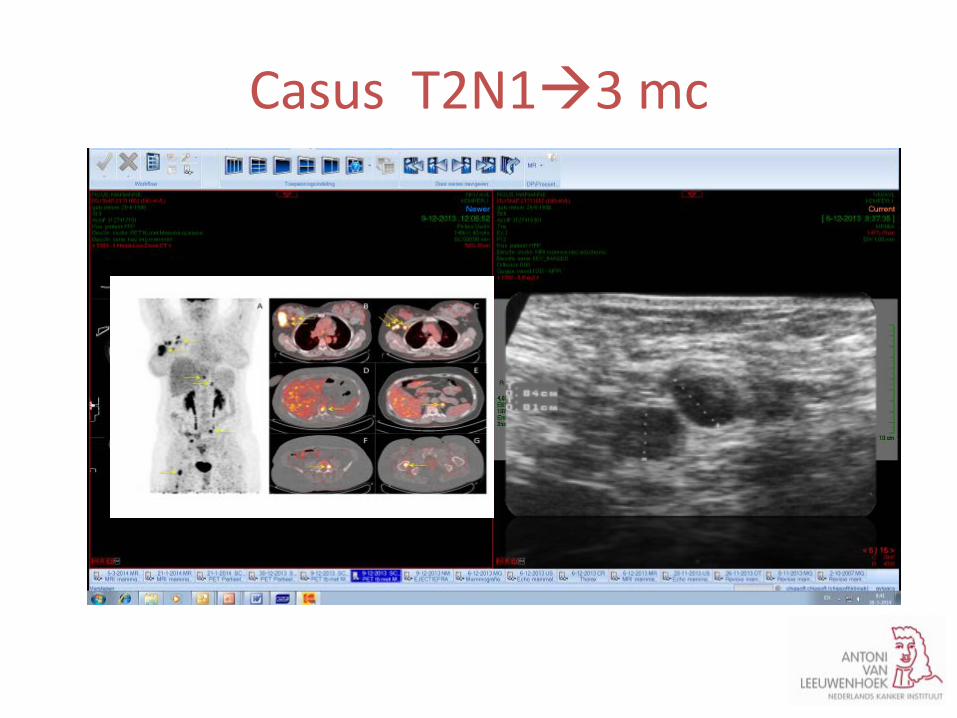
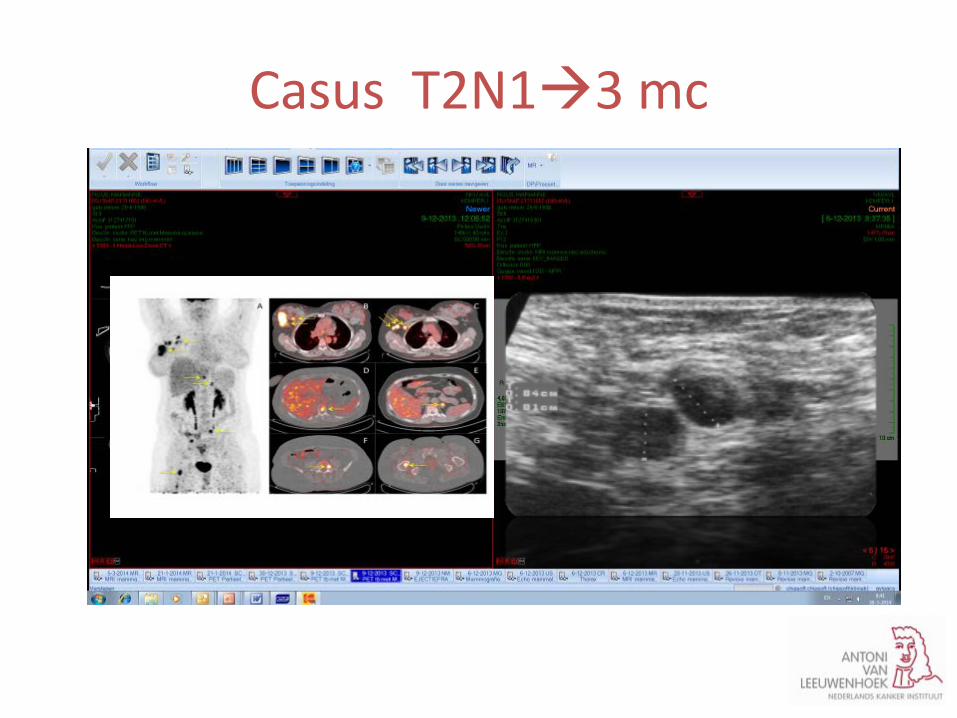
Casus T2N1 mc
Mw vd B 43 jaar afwijking li
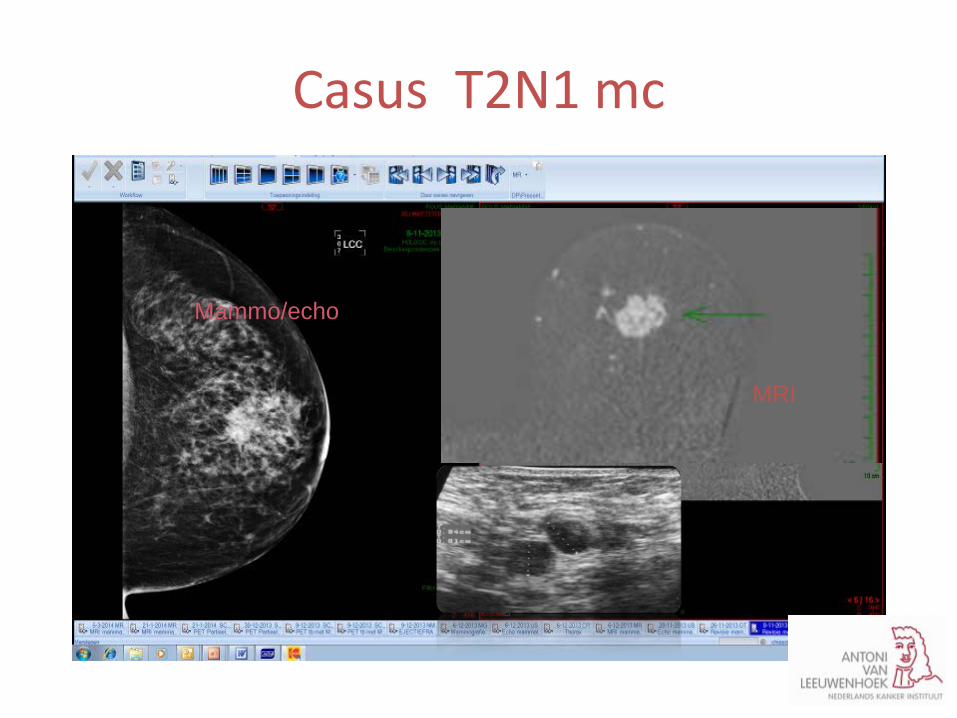
Casus T2N1 mc
Mammo/echo
MRI
Casus T2N1 mc
Meerdere mogelijkheden voor behandeling Borstsparende operatie plus OKD SSA plus OKD plus reconstructie GRM of eerst voorbehandelen met chemo?
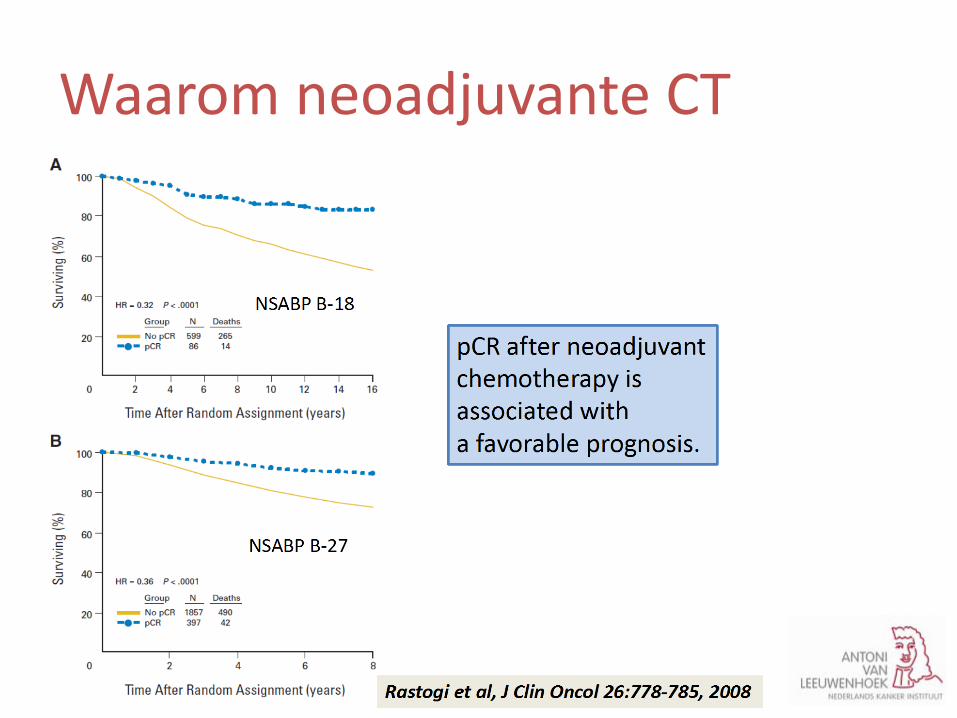
Waarom neoadjuvante CT
Waarom neoadjuvante CT
n±6,000 pts
n±6,000 pts Von Minckwitz et al. JCO 2012
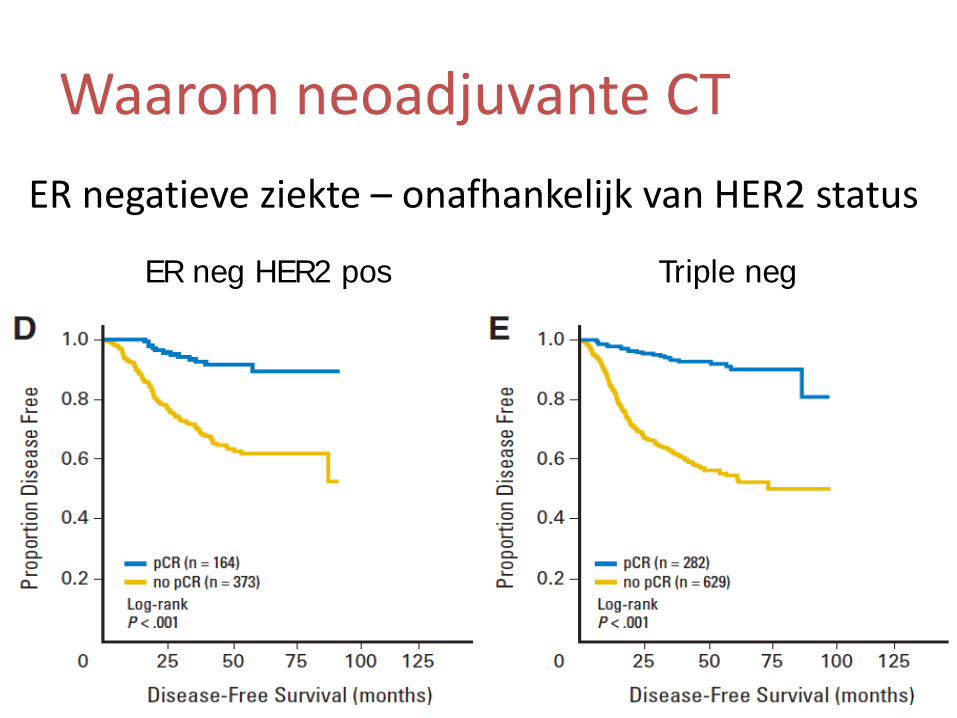
ER negatieve ziekte – onafhankelijk van HER2 status
ER neg HER2 pos Triple neg
Waarom neoadjuvante CT
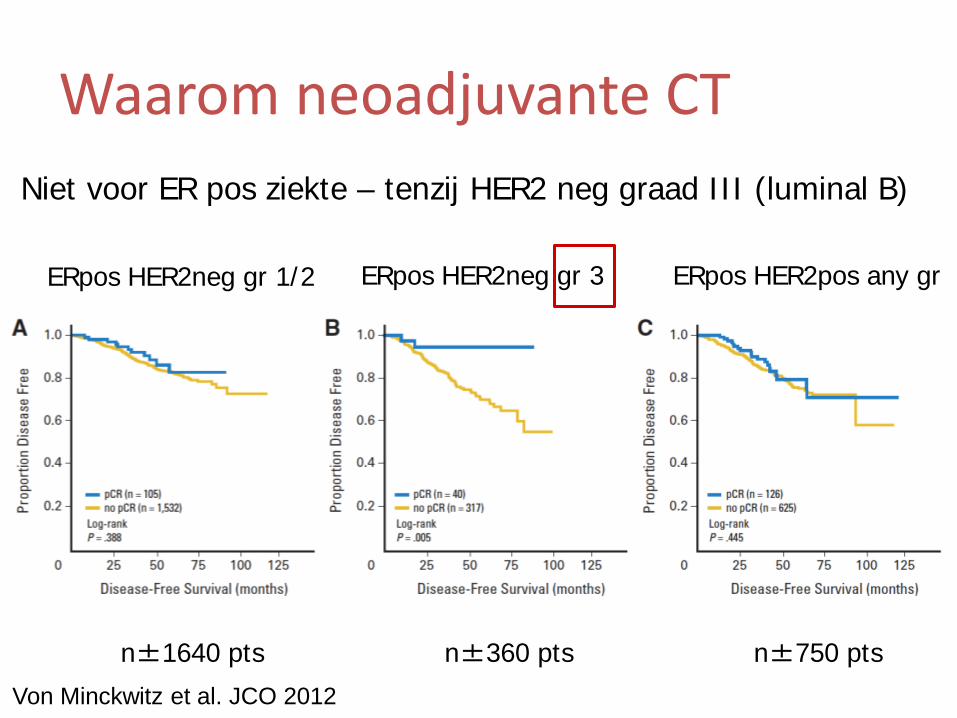
Von Minckwitz et al. JCO 2012
ERpos HER2neg gr 1/2 ERpos HER2neg gr 3 ERpos HER2pos any gr
n±1640 pts n±360 pts n±750 pts
Niet voor ER pos ziekte – tenzij HER2 neg graad III (luminal B)
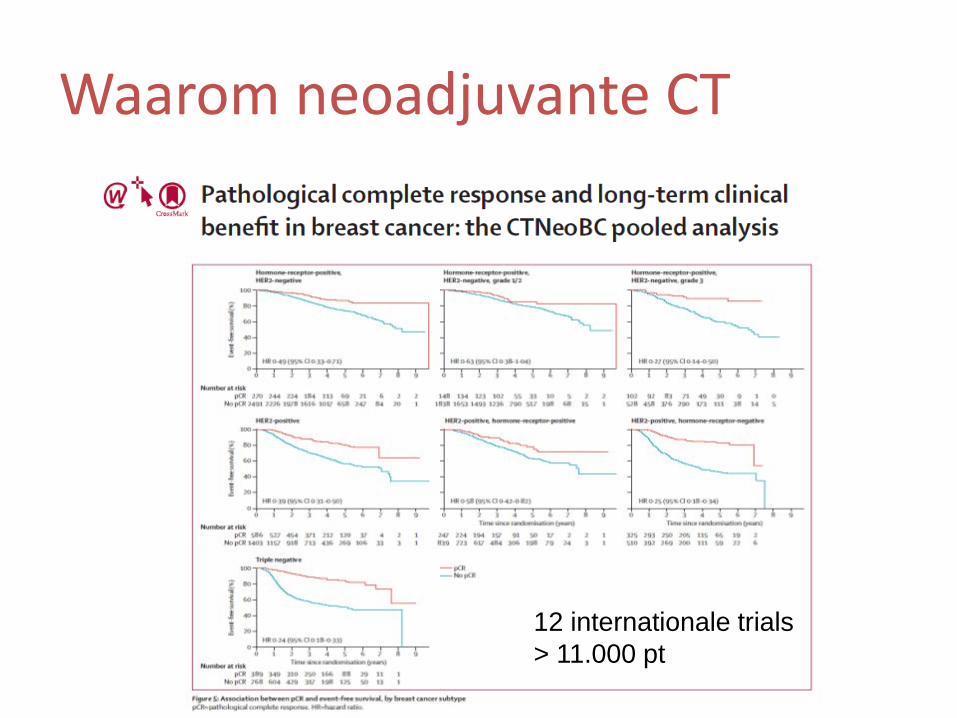
Waarom neoadjuvante CT
12 internationale trials > 11.000 pt
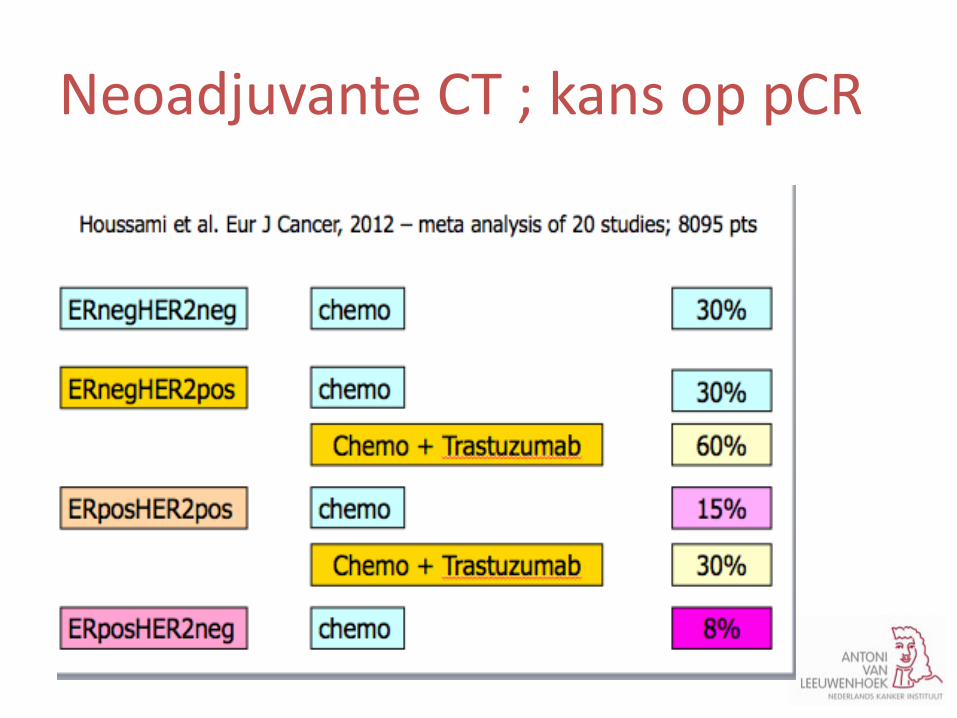
Neoadjuvante CT ; kans op pCR
Casus T2N1 mc
Meerdere mogelijkheden voor behandeling afhankelijk van tumortype mammaprint
Casus T2N1 mc
Meerdere mogelijkheden voor behandeling afhankelijk van tumortype mammaprint Biopt: ER neg, PR neg, Neu pos
indien ER pos PR pos Neu neg mammaprint
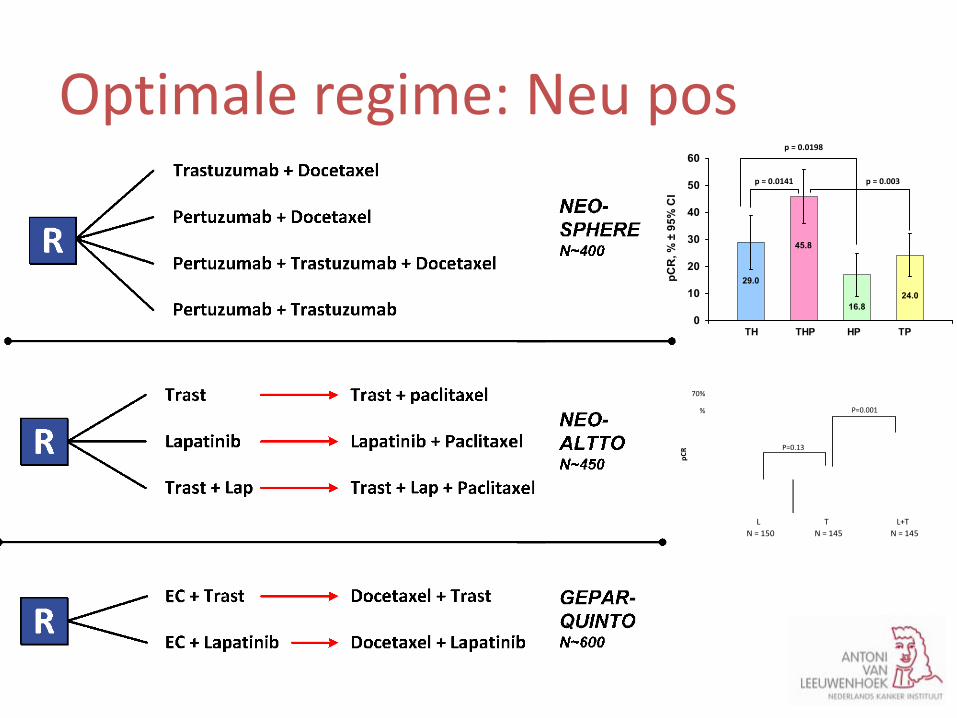
Optimale regime: Neu pos
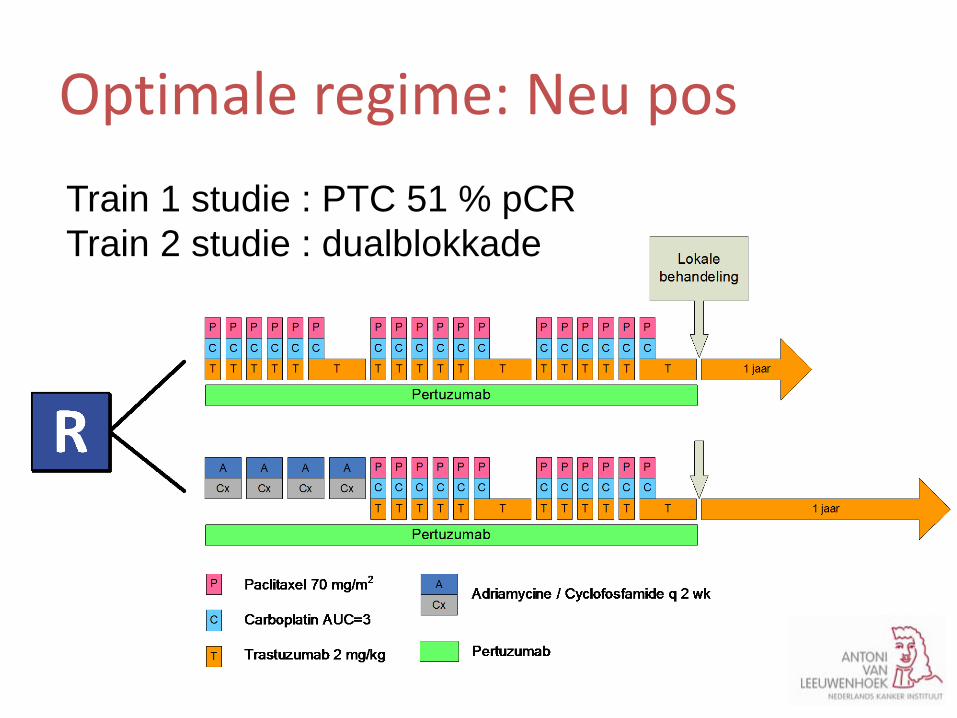
Optimale regime: Neu pos Train 1 studie : PTC 51 % pCR Train 2 studie : dualblokkade
Maatwerk bij NAC voor BK
Introductie
Waarom neoadjuvante chemotherapie
Locale behandeling op maat na NAC
Praktische “take home messages”
QUIZ: borstkankerboek
4. a. Welke subtypen BK ken je?
b. Incidentie per subtype?
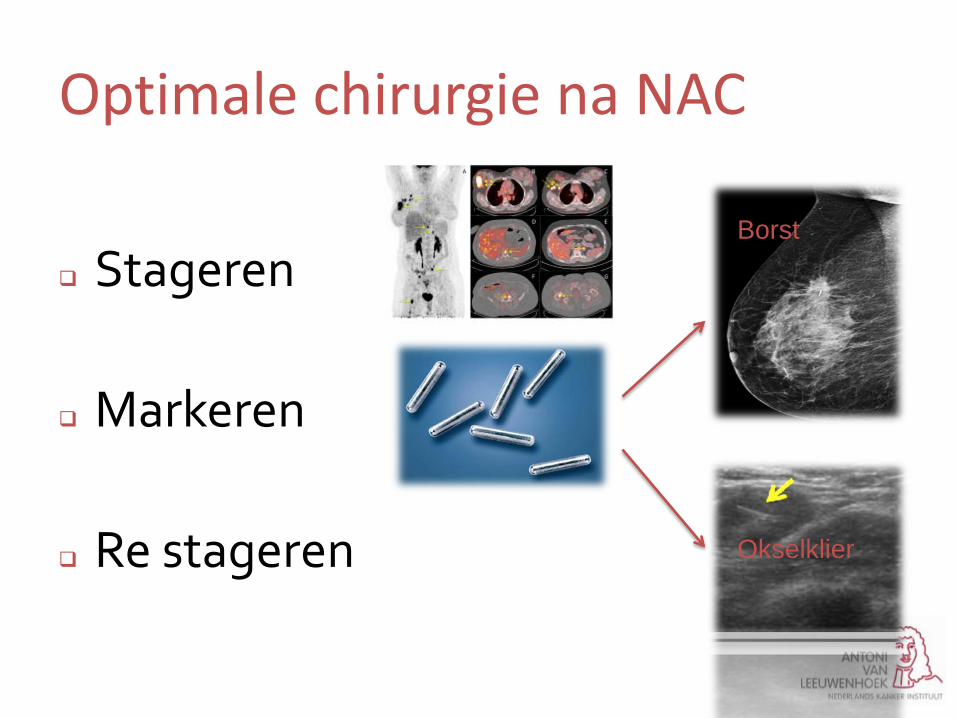
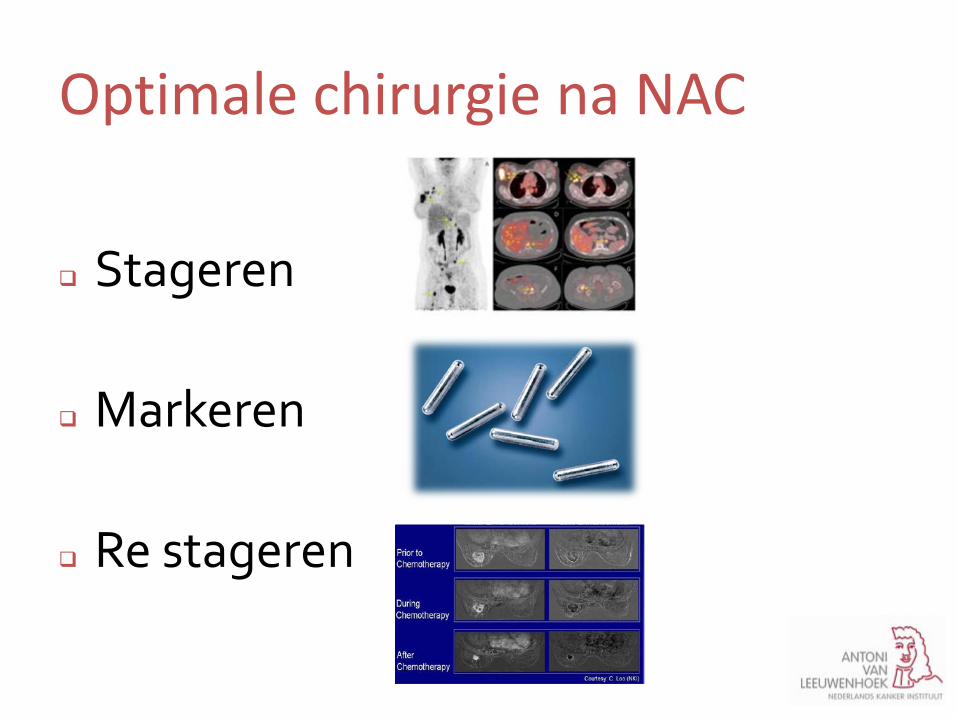
Optimale chirurgie na NAC
Stageren
Markeren
Re stageren
Optimale chirurgie na NAC
Stageren
FDG-avide klieren zijn erg voorspellend (98 %) voor N+ Detectie occulte N3-klieren 18% patiënten Accurate methode voor detectie afstandsmetastasen
2013 Koolen et al. Breast Cancer research and treatment
Casus T2N13 mc
Optimale chirurgie na NAC
Stageren
Markeren
Re stageren
Borst Okselklier
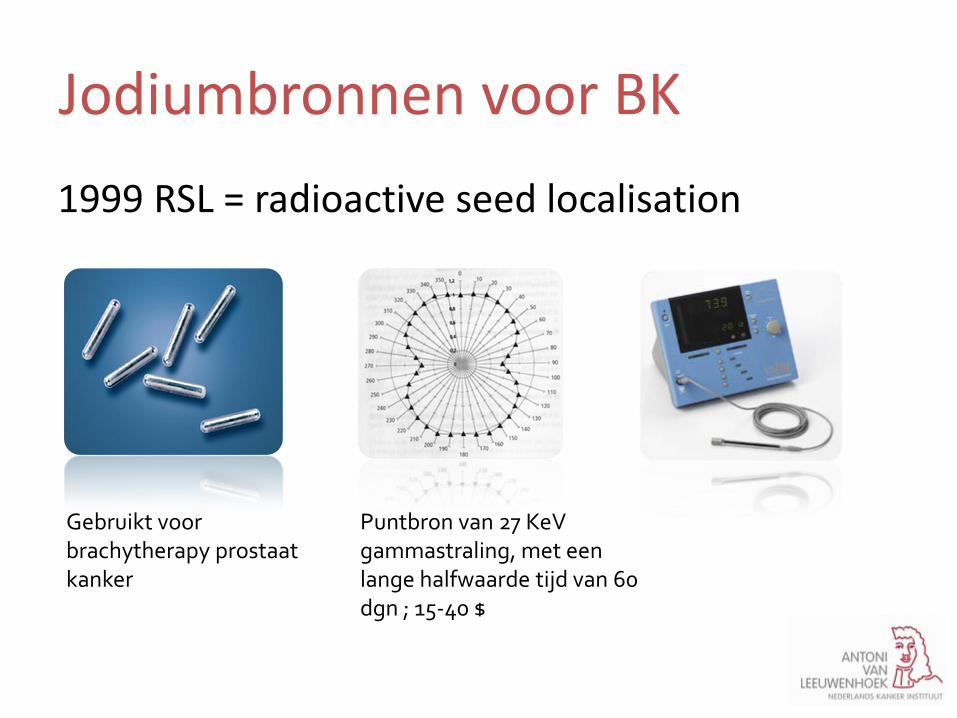
1999 RSL = radioactive seed localisation
Gebruikt voor brachytherapy prostaat kanker
Puntbron van 27 KeV gammastraling, met een lange halfwaarde tijd van 60 dgn ; 15-40 $
Jodiumbronnen voor BK

Jodiumbronnen voor BK
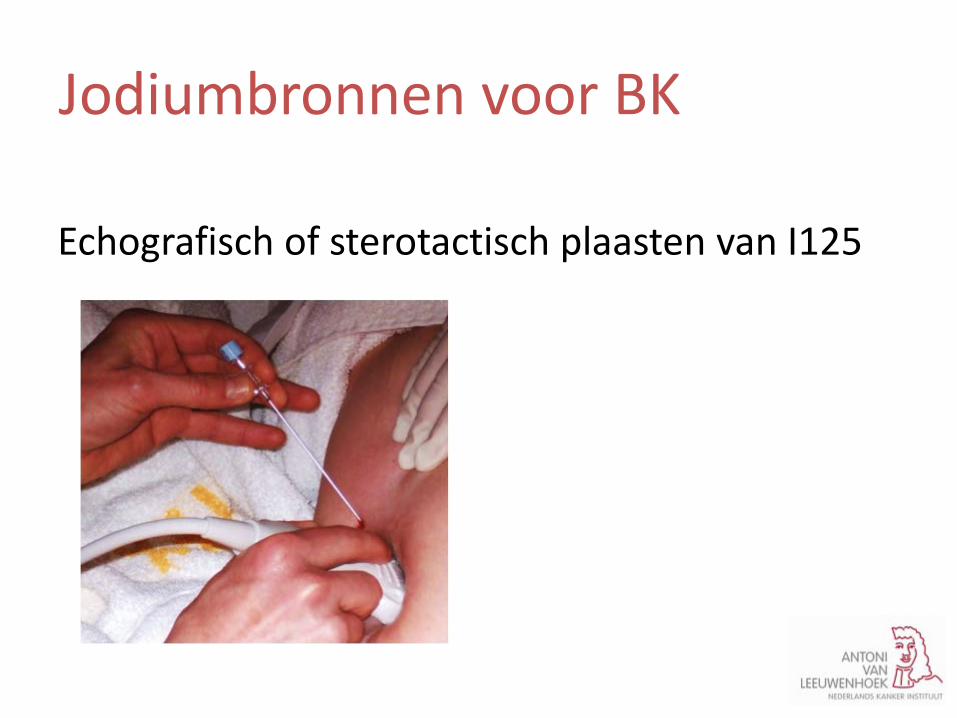
Echografisch of sterotactisch plaasten van I125
Jodiumbronnen voor BK

Mammografie: exacte positie van de I125 bron
Jodiumbronnen voor BK

WLE I125: bron gedetecteerd mbt gammaprobe
specimen picture on OR
Jodiumbronnen voor BK
• video
Jodiumbronnen voor BK
2000 in US: Prof Richard Gray, Chirurg
Jodiumbronnen voor BK

2000 in US: Prof Richard Gray, Chirurg 2003 in Nederland: Dr Jansen, radioloog in Catharina ZH Eindhoven 2009 Brainport Award
Jodiumbronnen voor BK

1979 Draadgeleide localisatie
Andere localisatie technieken

IUL = intraoperatieve ultrasound/echografie
Andere localisatie technieken
Voordelen Jodiumbron
Puntbron
Preoperatief locatie tov de tumor te zien
Lange halfwaarde tijd NAC
Meerdere bronnen plaatsen indien nodig
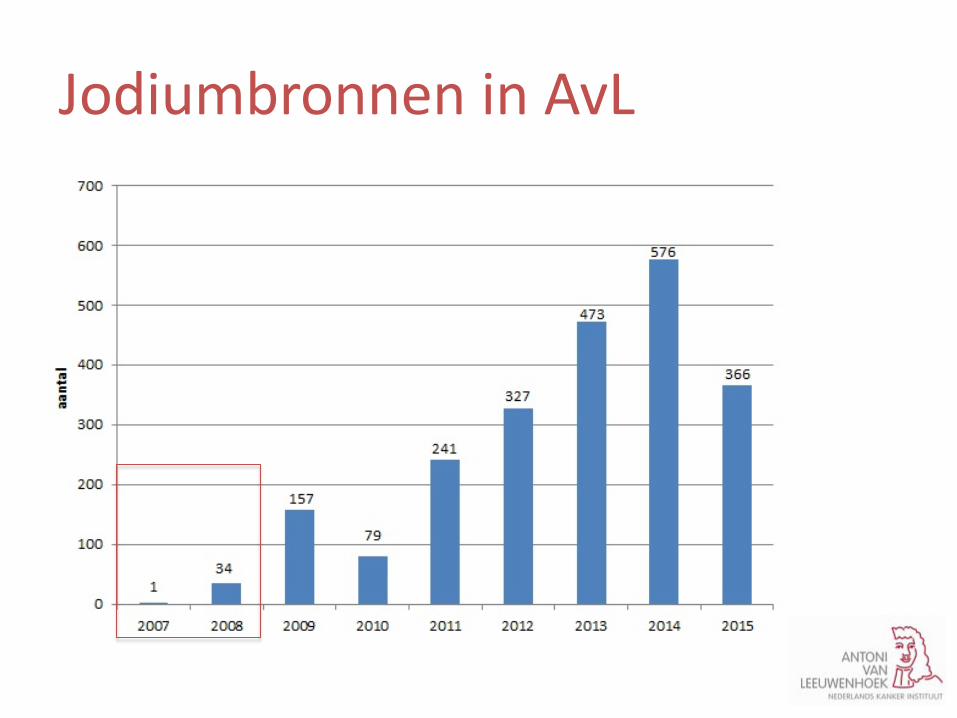
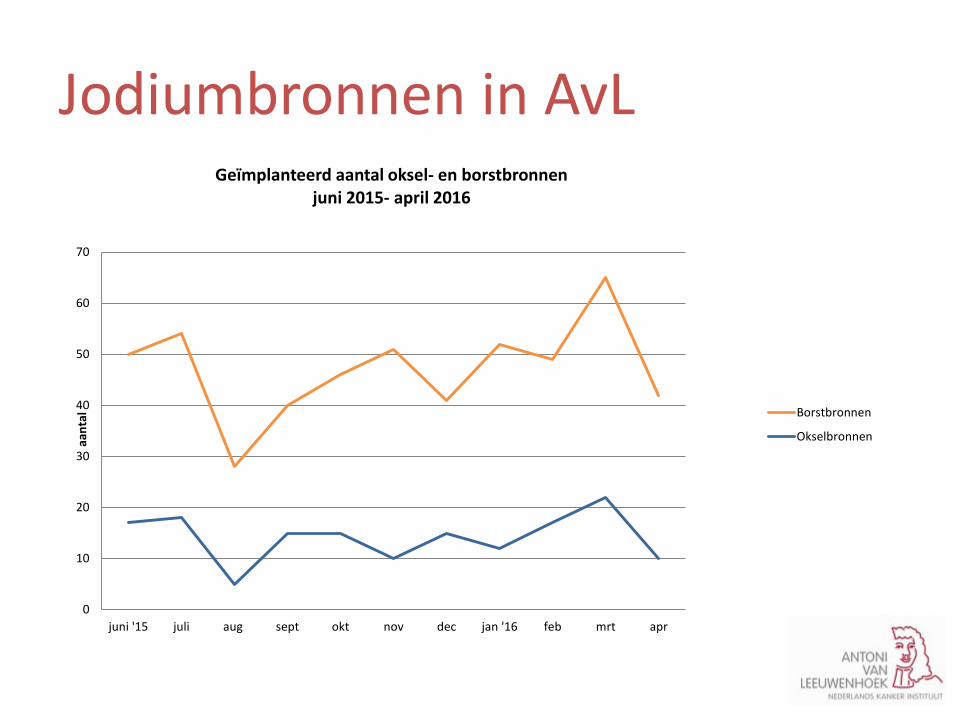
Jodiumbronnen in AvL
0
10
20
30
40
50
60
70
juni '15 juli aug sept okt nov dec jan '16 feb mrt apr
aan
tal
Geïmplanteerd aantal oksel- en borstbronnen juni 2015- april 2016
Borstbronnen
Okselbronnen
Jodiumbronnen in AvL
Nadelen Jodiumbron
Stralen hygiene protocollen
Met name bij het opstarten
• video
Jodiumbronnen voor BK
Optimale chirurgie na NAC
Stageren
Markeren
Re stageren
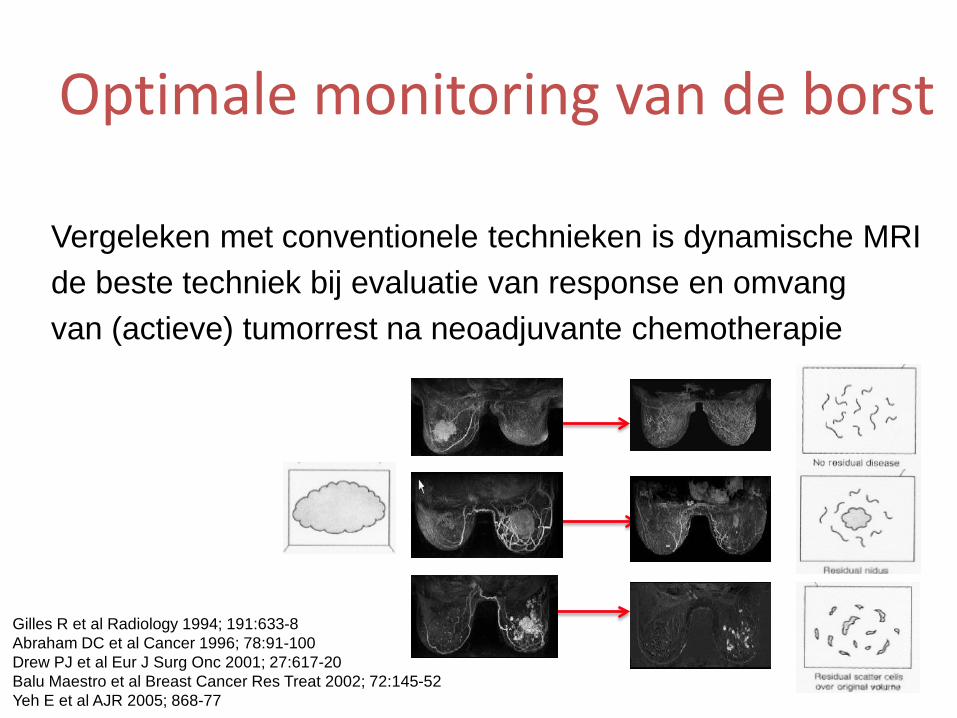
Gilles R et al Radiology 1994; 191:633-8 Abraham DC et al Cancer 1996; 78:91-100 Drew PJ et al Eur J Surg Onc 2001; 27:617-20 Balu Maestro et al Breast Cancer Res Treat 2002; 72:145-52 Yeh E et al AJR 2005; 868-77
Optimale monitoring van de borst
Vergeleken met conventionele technieken is dynamische MRI de beste techniek bij evaluatie van response en omvang van (actieve) tumorrest na neoadjuvante chemotherapie
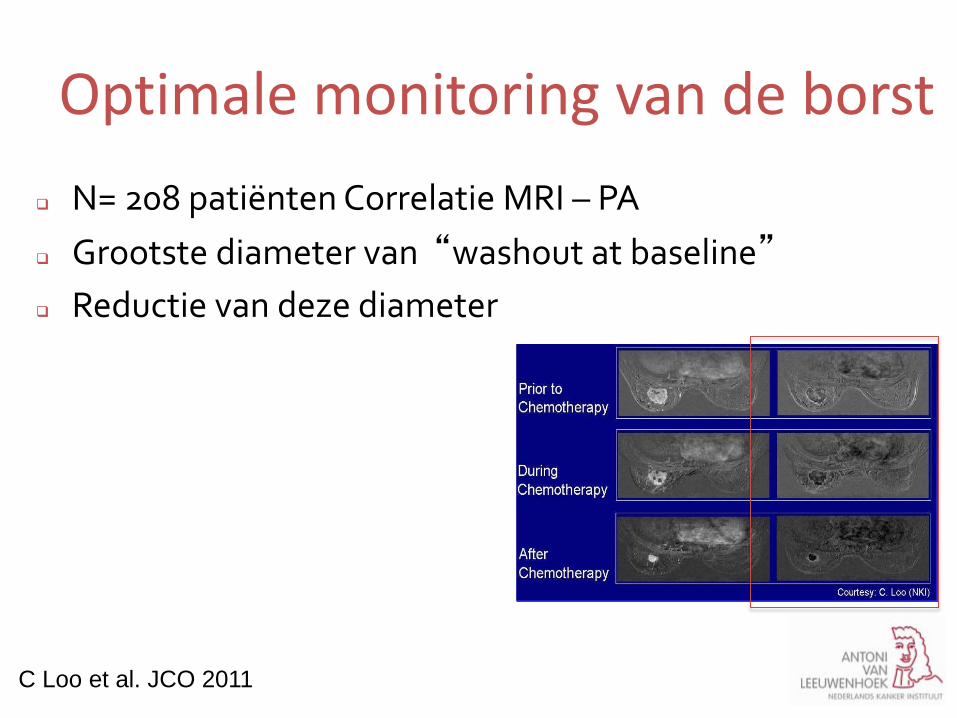
Optimale monitoring van de borst N= 208 patiënten Correlatie MRI – PA Grootste diameter van “washout at baseline” Reductie van deze diameter
C Loo et al. JCO 2011
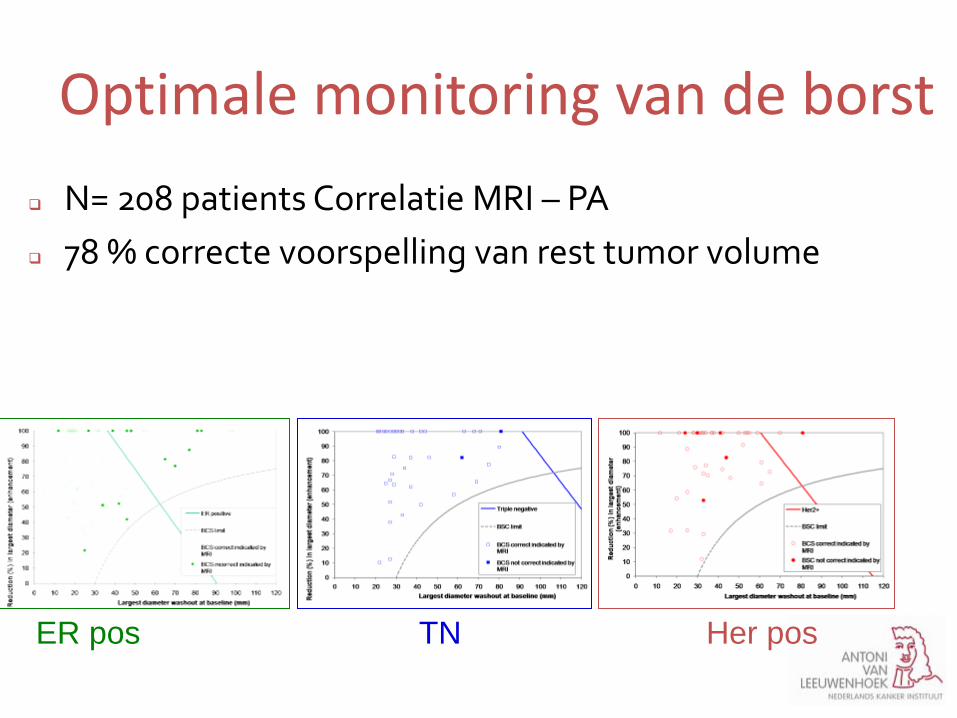
N= 208 patients Correlatie MRI – PA 78 % correcte voorspelling van rest tumor volume
ER pos TN Her pos
Optimale monitoring van de borst
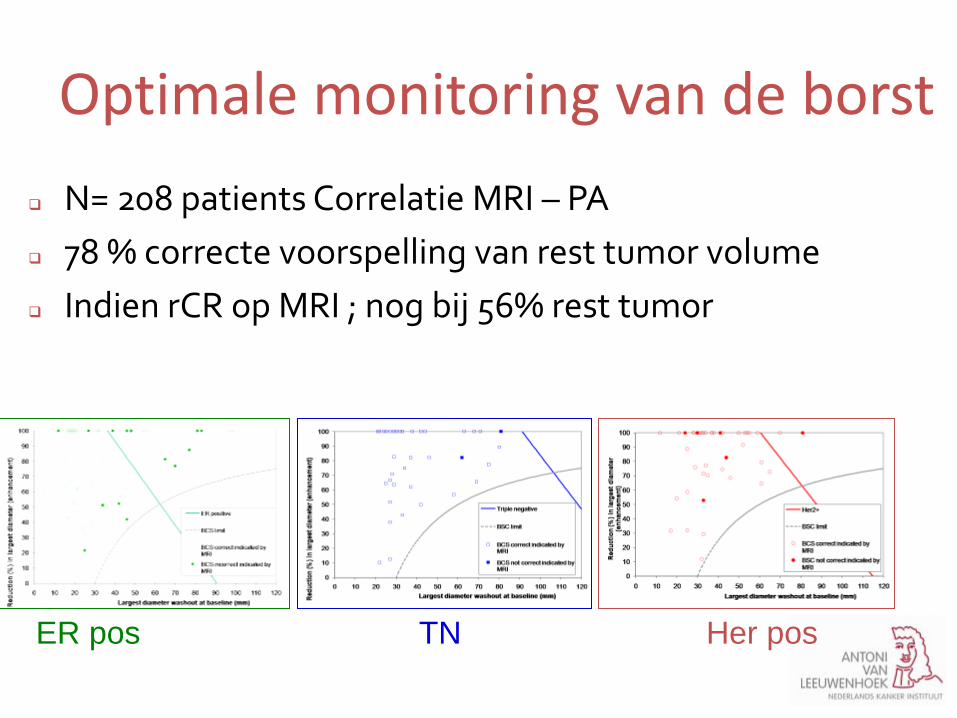
N= 208 patients Correlatie MRI – PA 78 % correcte voorspelling van rest tumor volume Indien rCR op MRI ; nog bij 56% rest tumor
Optimale monitoring van de borst
ER pos TN Her pos
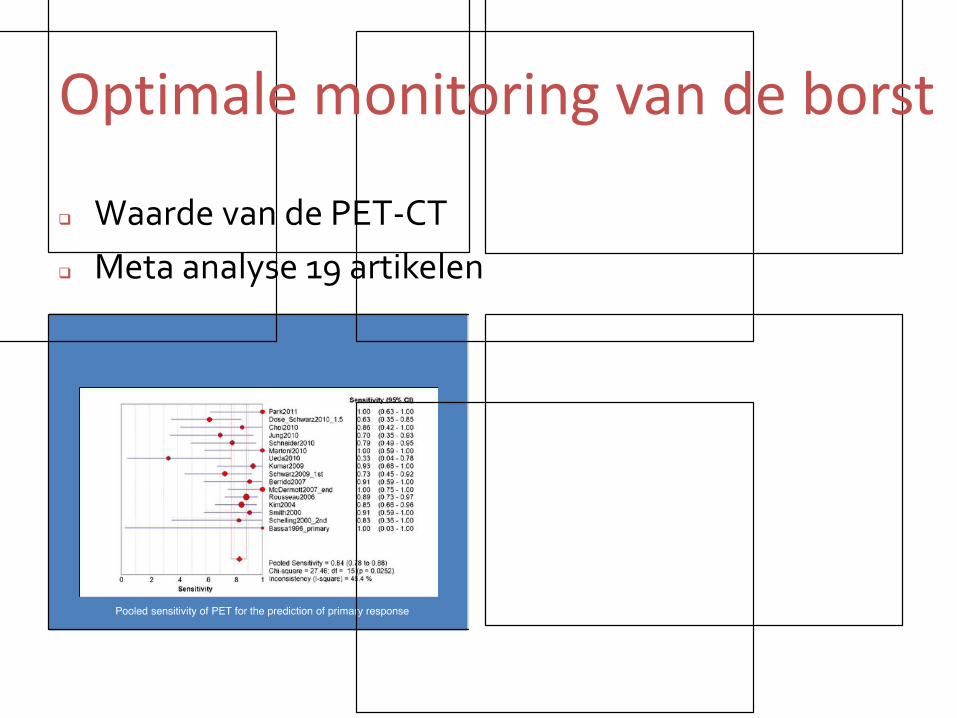
Waarde van de PET-CT Meta analyse 19 artikelen
Optimale monitoring van de borst
Optimale monitoring van de borst
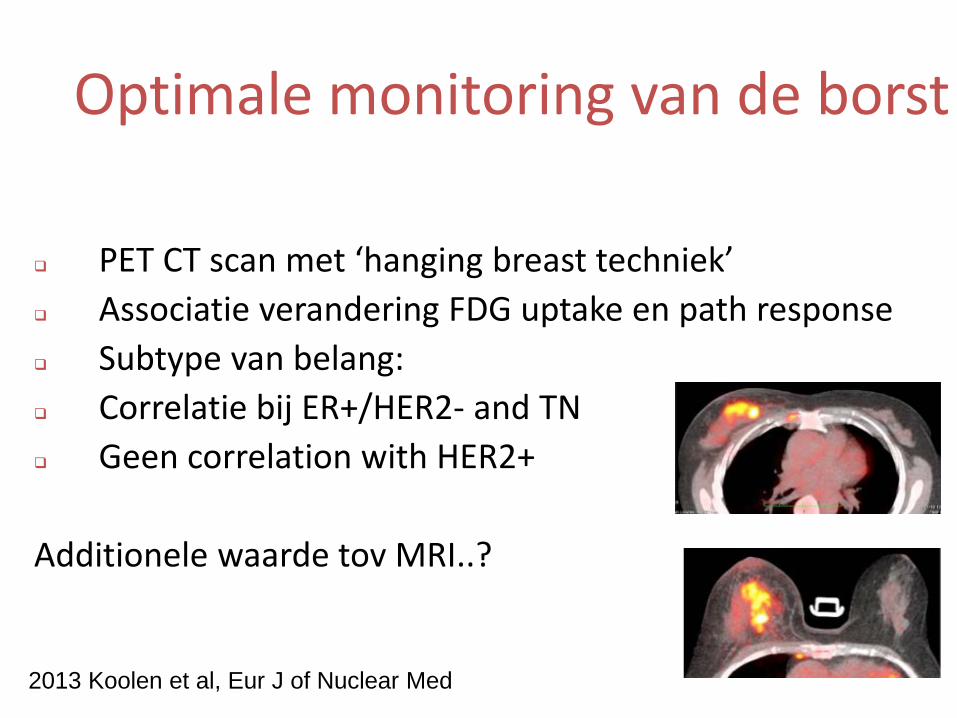
PET CT scan met ‘hanging breast techniek’ Associatie verandering FDG uptake en path response Subtype van belang: Correlatie bij ER+/HER2- and TN Geen correlation with HER2+
Additionele waarde tov MRI..?
2013 Koolen et al, Eur J of Nuclear Med
QUIZ: borstkankerboek
4. Hoe groot/klein is een jodiumbron ?
QUIZ: borstkankerboek
5. Hoe heet dit schilderij? En wie heeft het
geschilderd?
Casus T2N3 mc
2015 after first cycles of PTC
2015 Final MRI
Factoren die meegenomen worden in MDO: tumorgrootte borst / oksel op MRI / PET aanwezige microcalcificaties: DCIS multifocaliteit oncoplastische mogelijkheden voorkeur van de patiënt genetische factoren
Optimale chirurgie: borst
Factoren die meegenomen worden in MDO: tumorgrootte borst / oksel op MRI / PET aanwezige microcalcificaties: DCIS multifocaliteit oncoplastische mogelijkheden voorkeur van de patiënt genetische factoren
Optimale chirurgie: borst
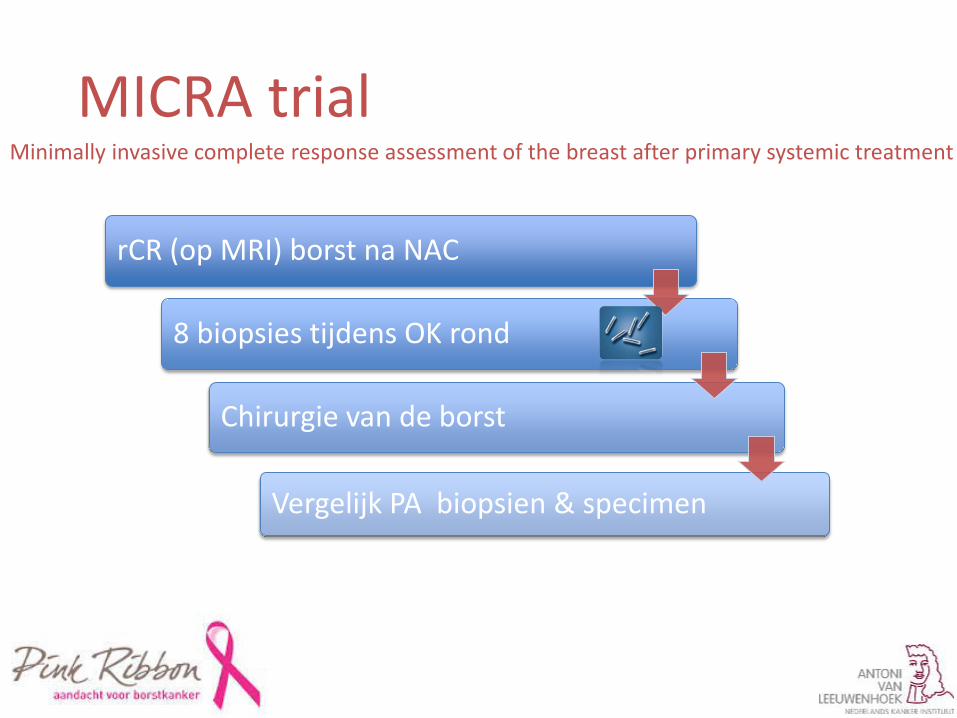
rCR (op MRI) borst na NAC
8 biopsies tijdens OK rond
Chirurgie van de borst
Vergelijk PA biopsien & specimen
MICRA trial Minimally invasive complete response assessment of the breast after primary systemic treatment
Optimale chirurgie : oksel
pCR oksel in > 30 % van de patienten
Straver 2010; Tweigeri Cancer Chemother Pharmacol 2016; Diego Ann Surg Oncol 2015; Boughey J Clin Oncol.
Optimale chirurgie : oksel
pCR oksel in > 30 % van de patienten
Toch vaak OKD na NAC indien N1-2 of 3 voorafgaand aan chemo
Straver 2010; Tweigeri Cancer Chemother Pharmacol 2016; Diego Ann Surg Oncol 2015; Boughey J Clin Oncol.
Optimale chirurgie : oksel
pCR oksel in > 30 % van de patienten Re- stagering met echo, MRI, PET Re-stagering met SN postchemo
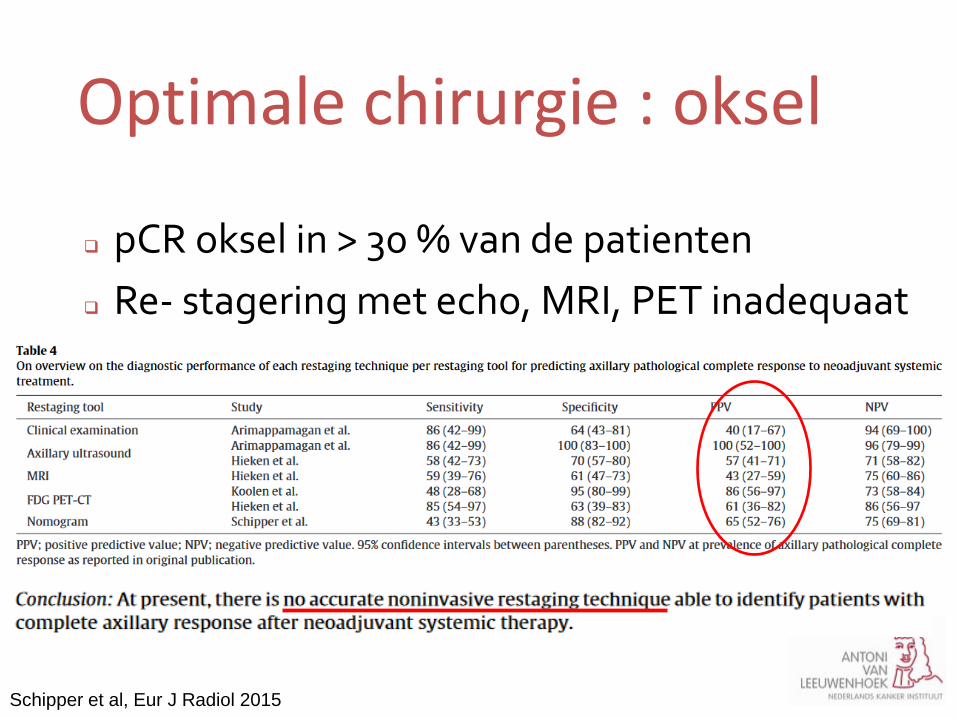
Optimale chirurgie : oksel
pCR oksel in > 30 % van de patienten Re- stagering met echo, MRI, PET inadequaat SN postchemo :
Schipper et al, Eur J Radiol 2015
Optimale chirurgie : oksel
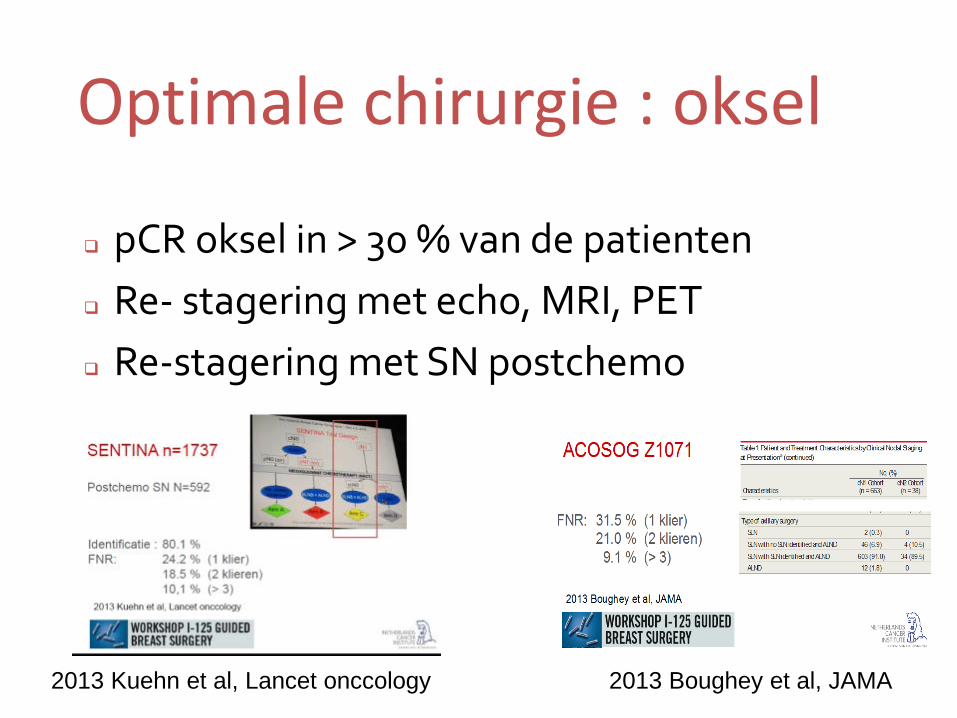
pCR oksel in > 30 % van de patienten Re- stagering met echo, MRI, PET Re-stagering met SN postchemo
2013 Kuehn et al, Lancet onccology 2013 Boughey et al, JAMA
Optimale chirurgie : oksel
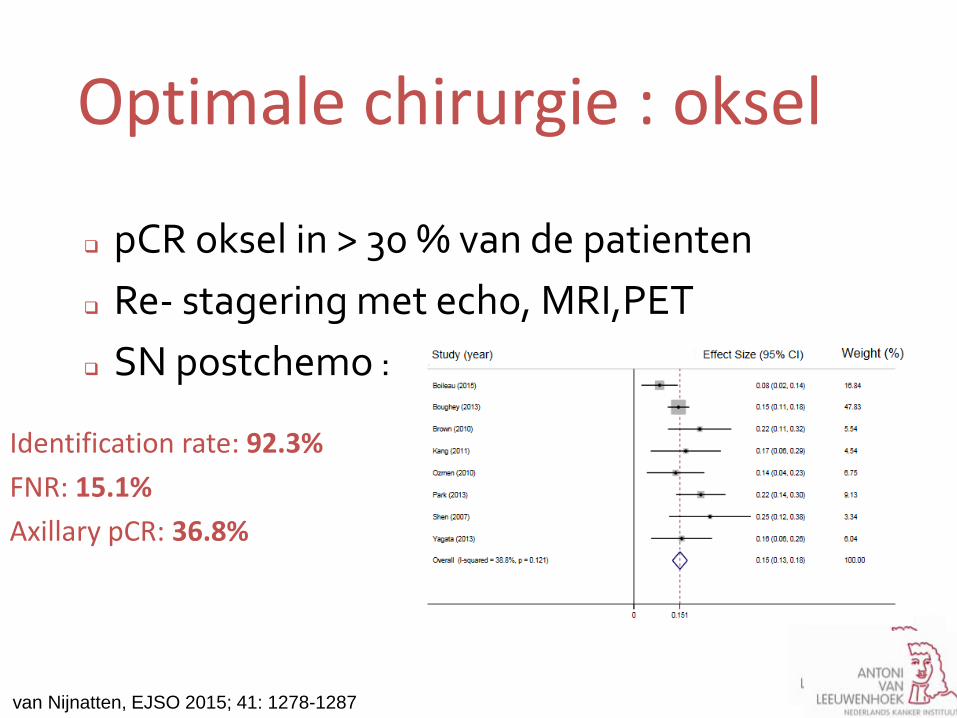
pCR oksel in > 30 % van de patienten Re- stagering met echo, MRI,PET SN postchemo :
van Nijnatten, EJSO 2015; 41: 1278-1287
Identification rate: 92.3% FNR: 15.1% Axillary pCR: 36.8%
Optimale chirurgie : oksel

Optimale chirurgie : oksel
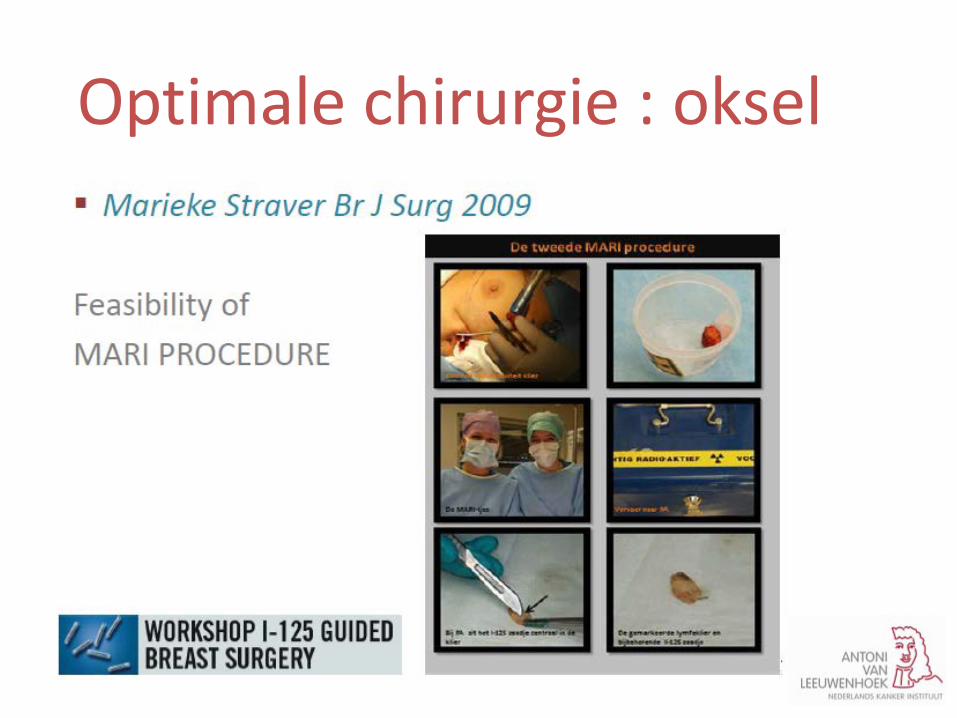
MARI procedure
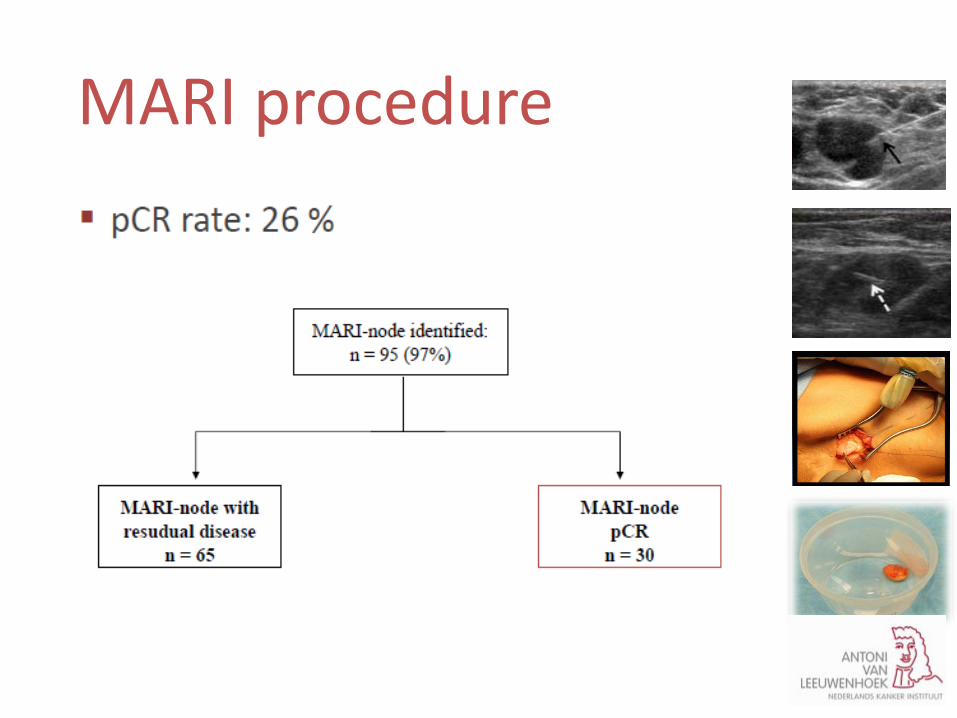
MARI procedure
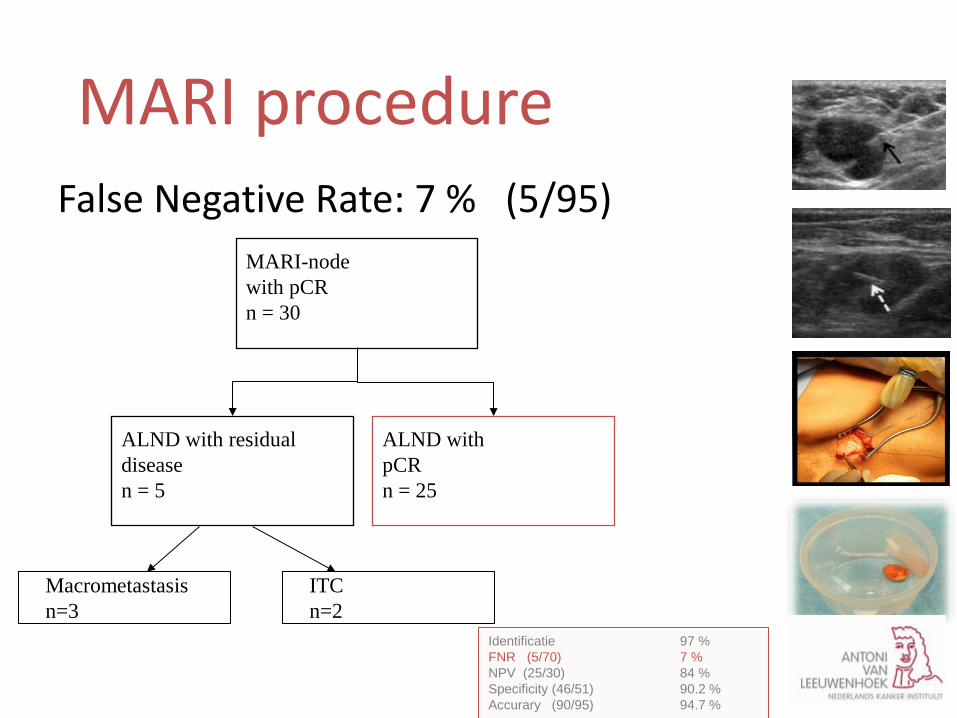
False Negative Rate: 7 % (5/95) MARI-node with pCR n = 30
ALND with residual disease n = 5
ALND with pCR n = 25
Macrometastasis n=3
ITC n=2
Identificatie 97 % FNR (5/70) 7 % NPV (25/30) 84 % Specificity (46/51) 90.2 % Accurary (90/95) 94.7 %
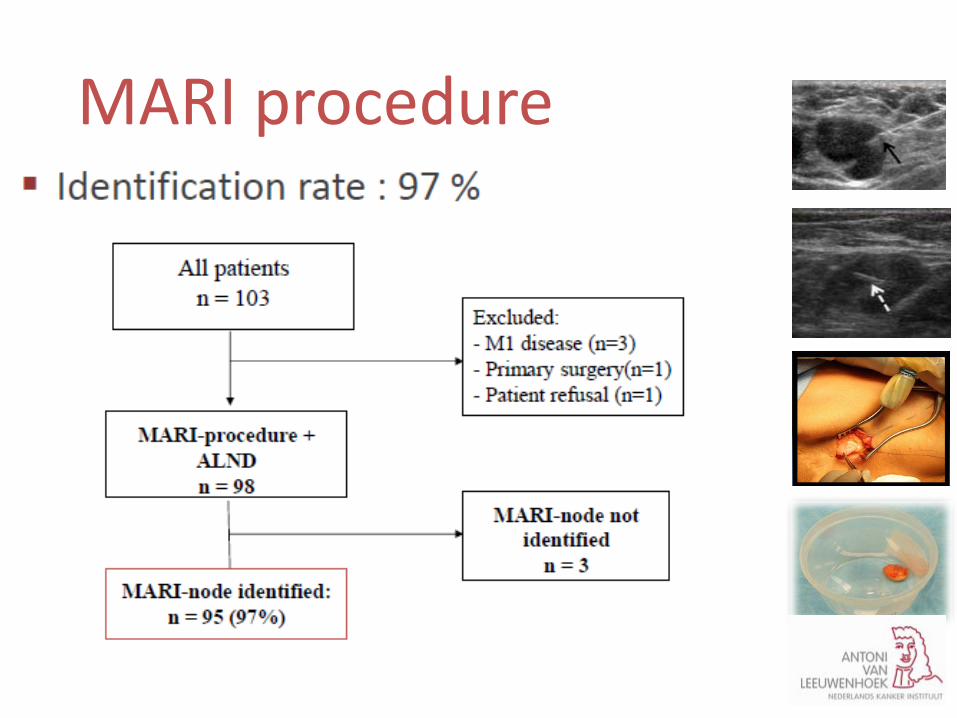
MARI procedure
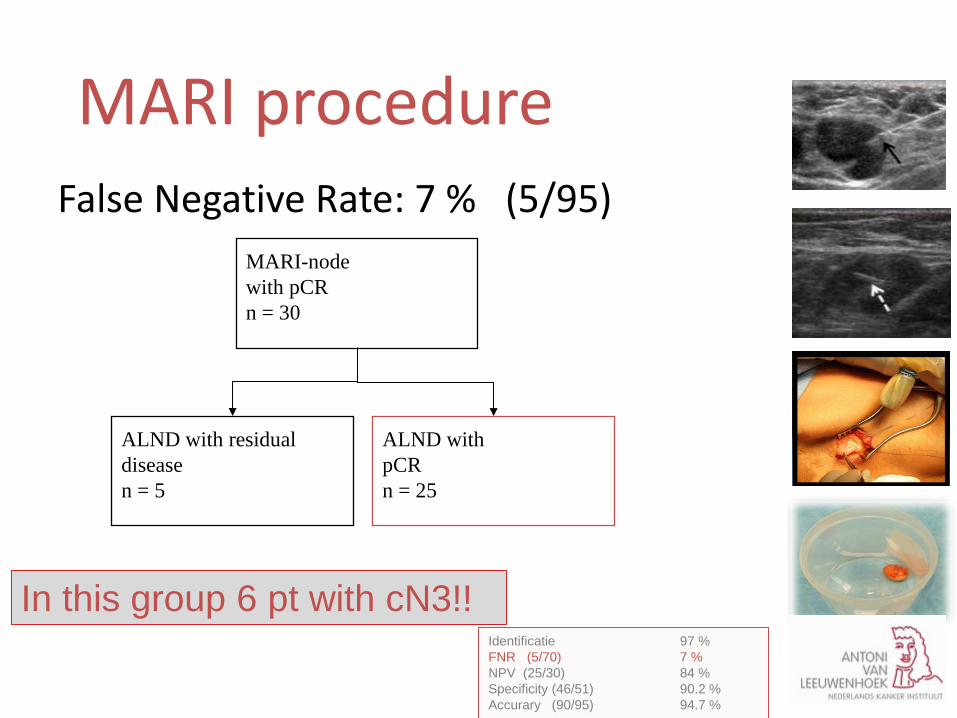
False Negative Rate: 7 % (5/95) MARI-node with pCR n = 30
ALND with residual disease n = 5
ALND with pCR n = 25
Macrometastasis n=3
ITC n=2
Identificatie 97 % FNR (5/70) 7 % NPV (25/30) 84 % Specificity (46/51) 90.2 % Accurary (90/95) 94.7 %
MARI procedure
In this group 6 pt with cN3!!
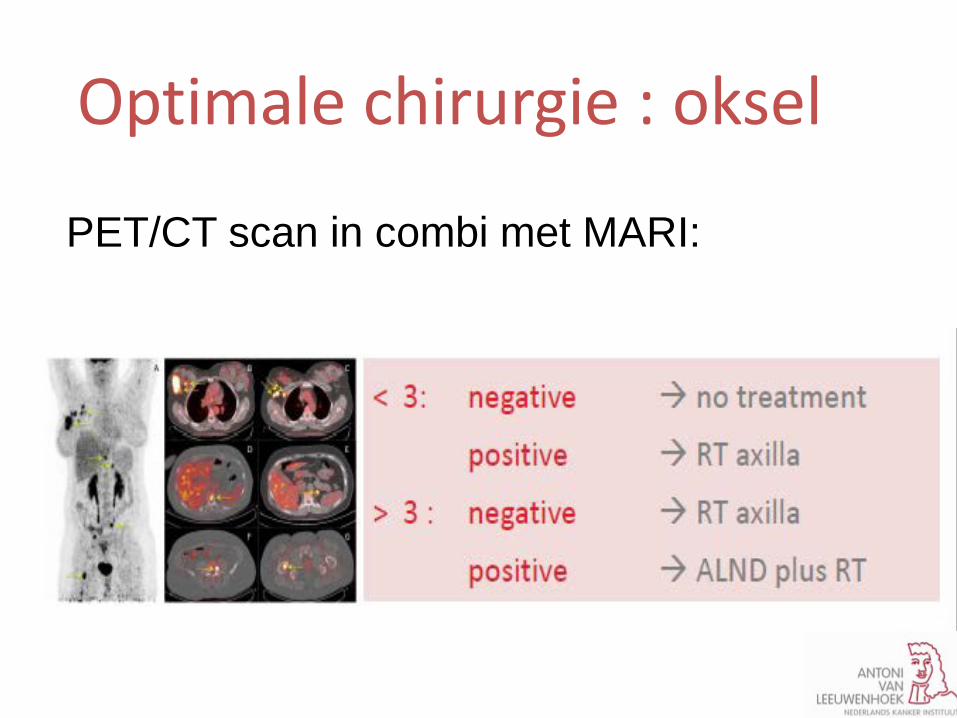
Optimale chirurgie : oksel
PET/CT scan in combi met MARI:
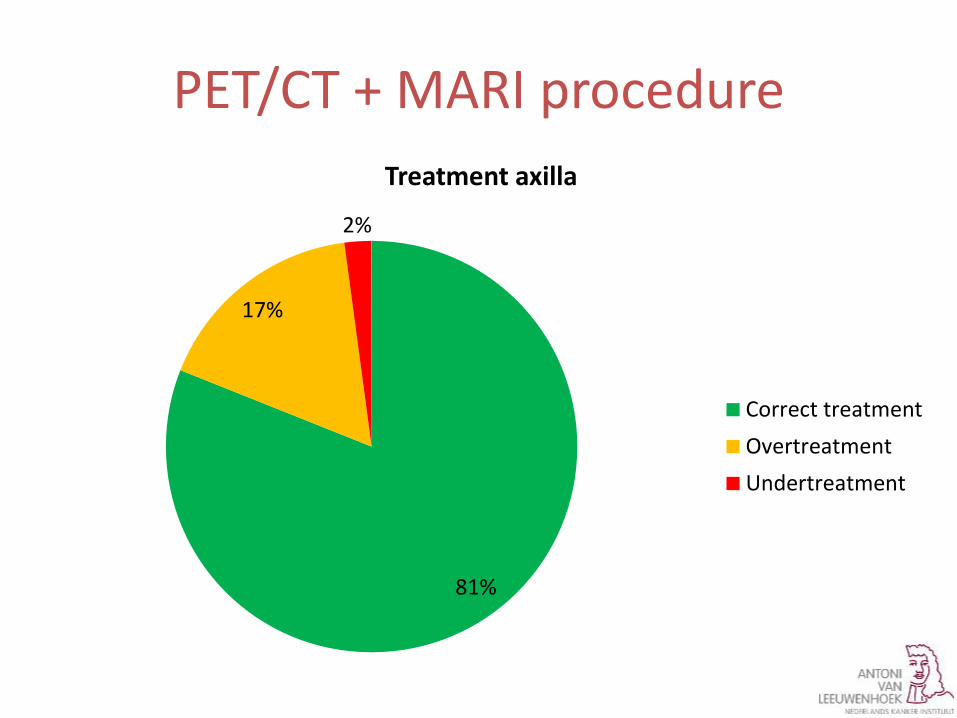
PET/CT + MARI procedure
81%
17%
2%
Treatment axilla
Correct treatmentOvertreatmentUndertreatment
Casus T2N13 mc
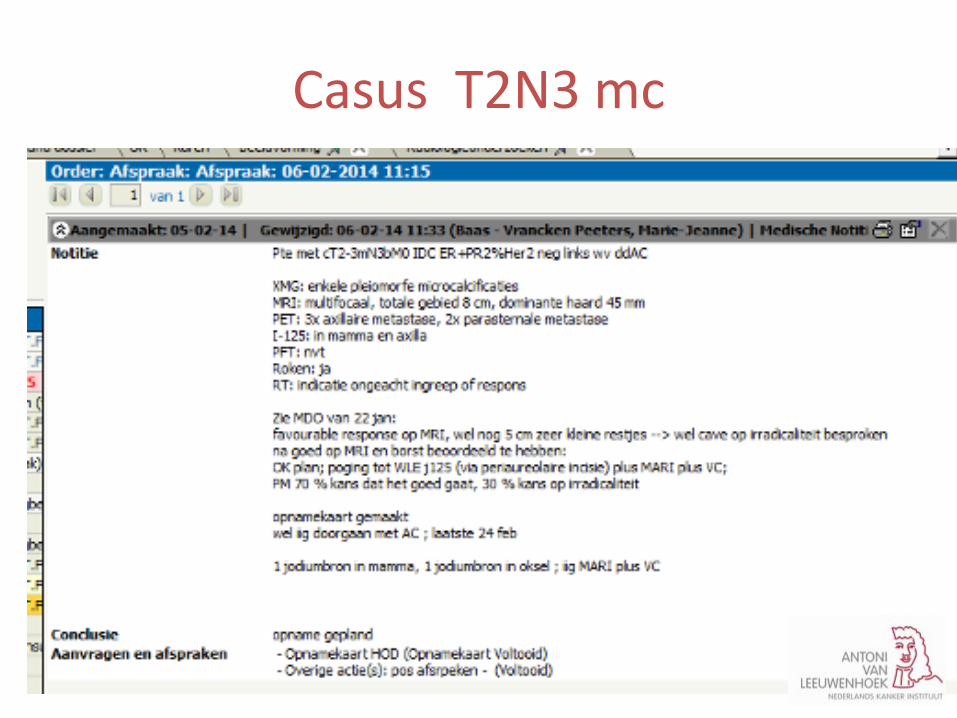
Casus T2N3 mc
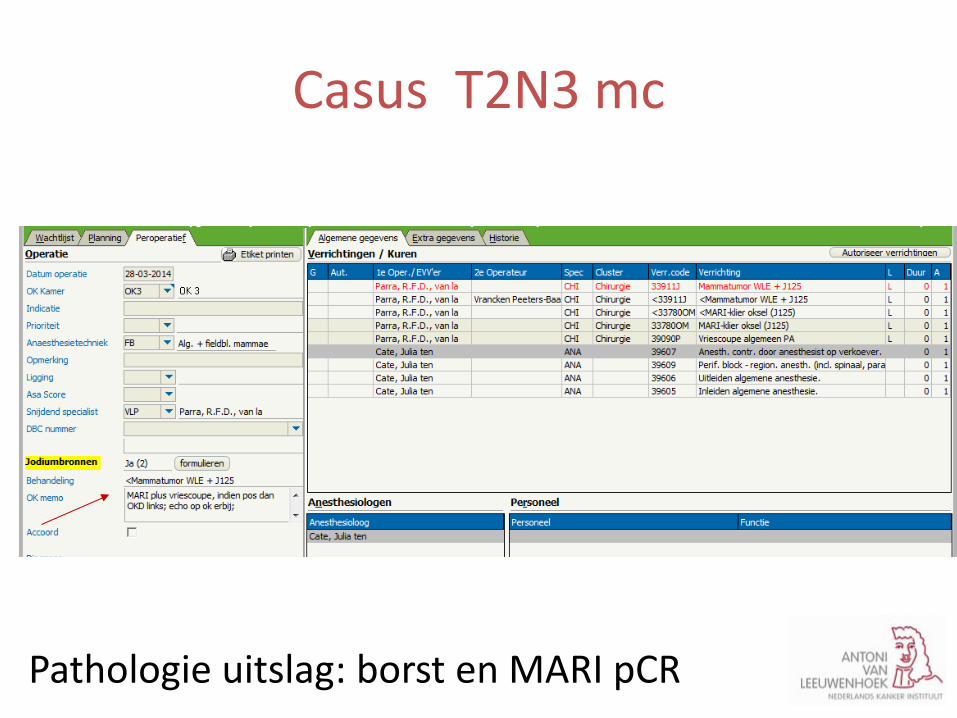
• WLE I 125 plus MARI procedure
Pathologie uitslag: borst en MARI pCR
Casus T2N3 mc
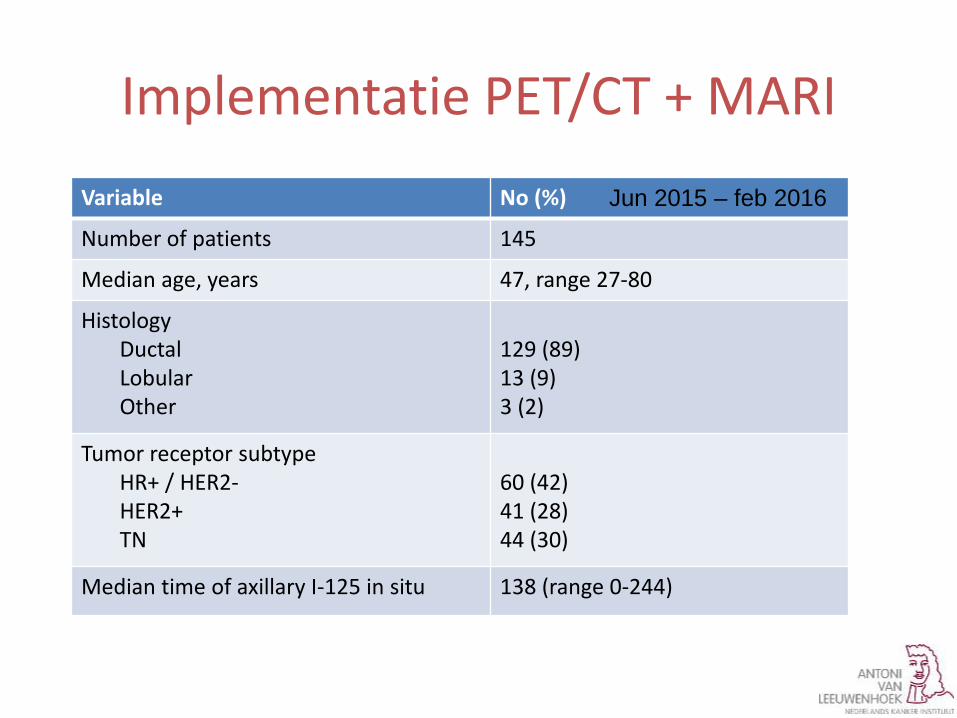
Variable No (%)
Number of patients 145
Median age, years 47, range 27-80
Histology Ductal Lobular Other
129 (89) 13 (9) 3 (2)
Tumor receptor subtype HR+ / HER2- HER2+ TN
60 (42) 41 (28) 44 (30)
Median time of axillary I-125 in situ 138 (range 0-244)
Implementatie PET/CT + MARI Jun 2015 – feb 2016
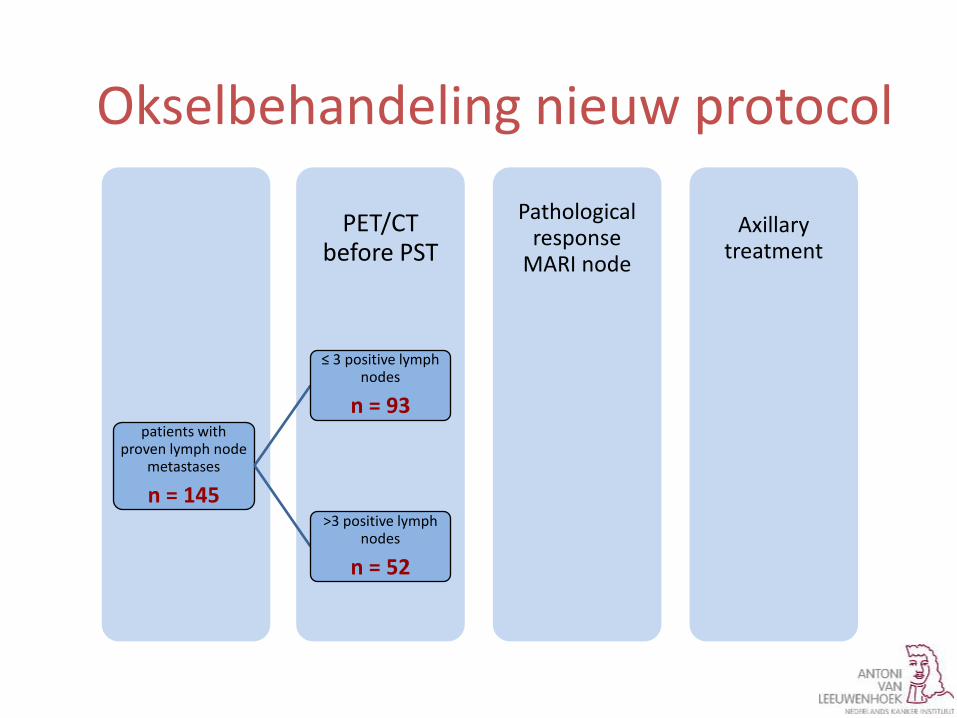
Axillary treatment
Pathological response
MARI node
PET/CT before PST
patients with proven lymph node
metastases
n = 145
≤ 3 positive lymph nodes
n = 93
pCR no further axillary treatment
residual disease axillary radiotherapy
>3 positive lymph nodes
n = 52
pCR axillary radiotherapy
residual disease ALND + axillary radiotherapy
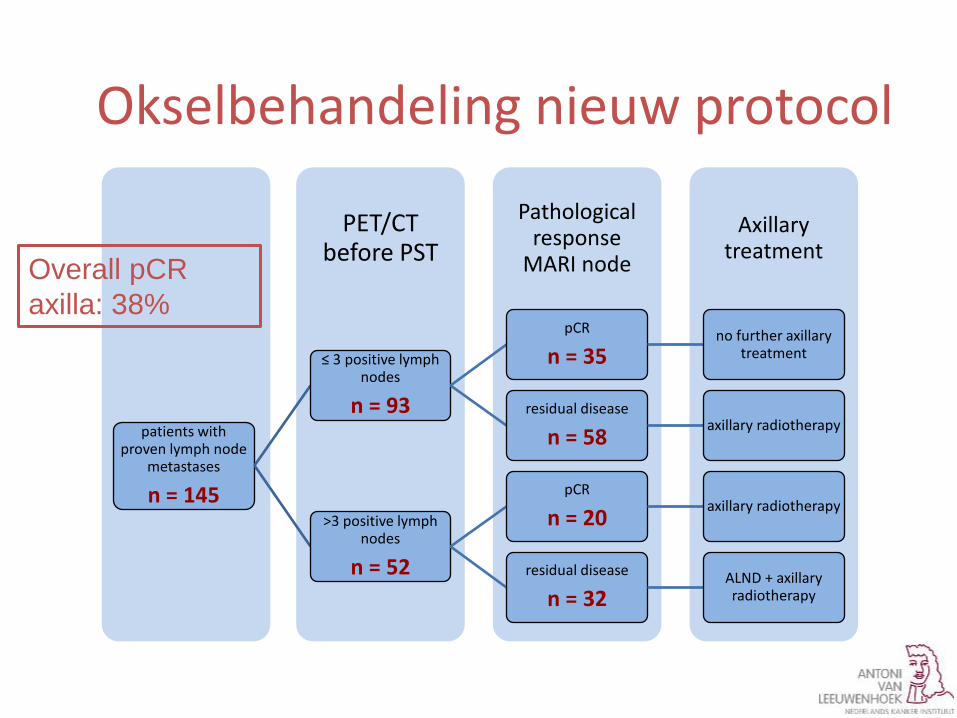
Okselbehandeling nieuw protocol
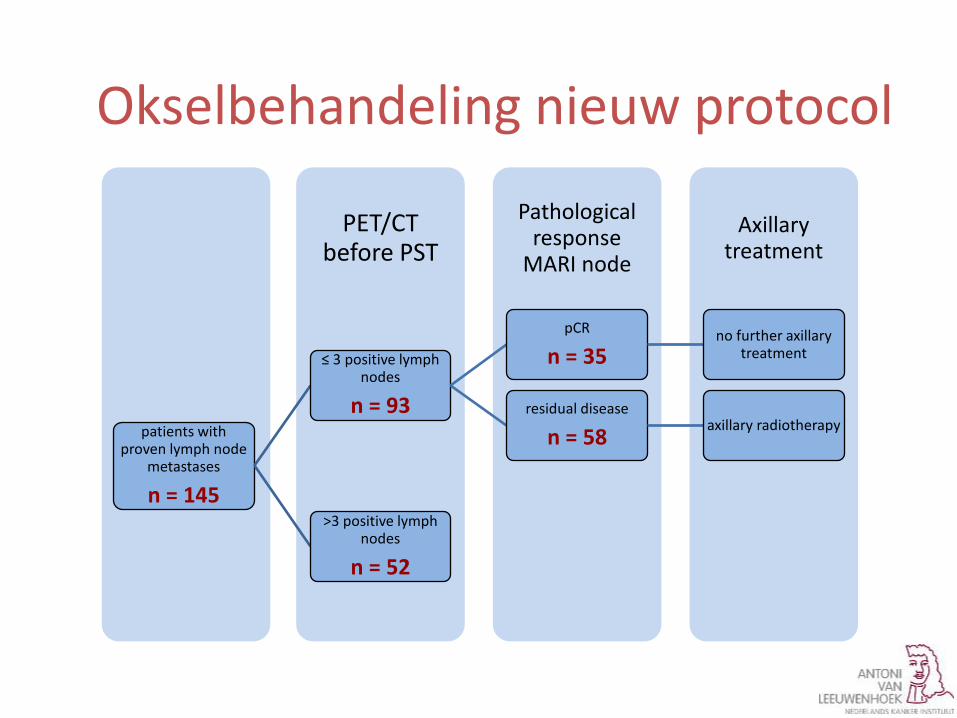
Axillary treatment
Pathological response
MARI node
PET/CT before PST
patients with proven lymph node
metastases
n = 145
≤ 3 positive lymph nodes
n = 93
pCR
n = 35 no further axillary
treatment
residual disease
n = 58 axillary radiotherapy
>3 positive lymph nodes
n = 52
pCR axillary radiotherapy
residual disease ALND + axillary radiotherapy
Okselbehandeling nieuw protocol
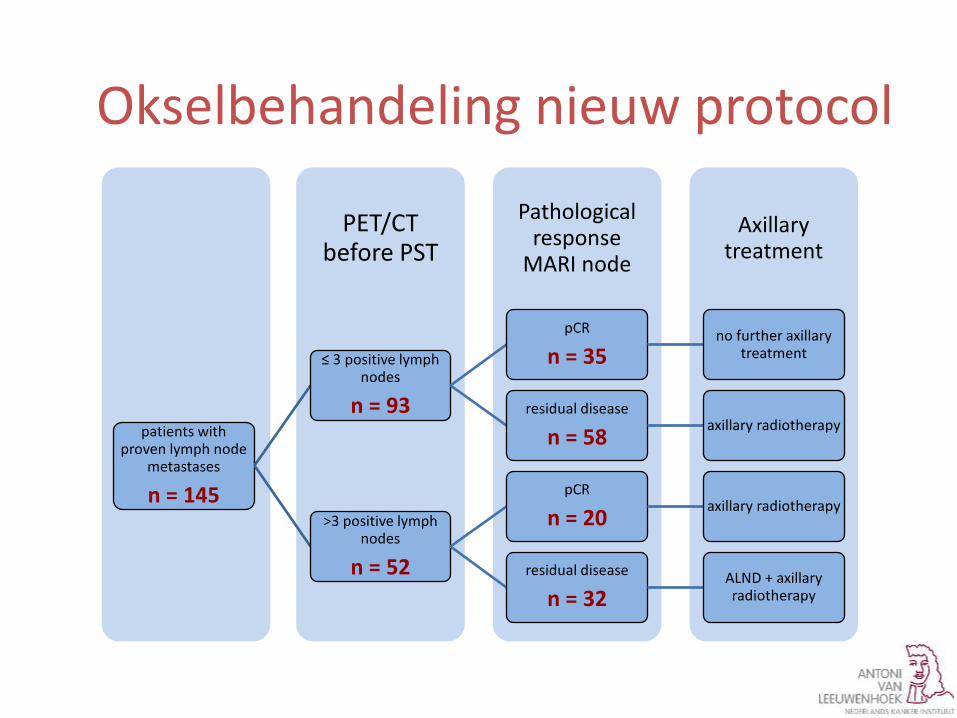
Axillary treatment
Pathological response
MARI node
PET/CT before PST
patients with proven lymph node
metastases
n = 145
≤ 3 positive lymph nodes
n = 93
pCR
n = 35 no further axillary
treatment
residual disease
n = 58 axillary radiotherapy
>3 positive lymph nodes
n = 52
pCR
n = 20 axillary radiotherapy
residual disease
n = 32 ALND + axillary radiotherapy
Okselbehandeling nieuw protocol
Axillary treatment
Pathological response
MARI node
PET/CT before PST
patients with proven lymph node
metastases
n = 145
≤ 3 positive lymph nodes
n = 93
pCR
n = 35 no further axillary
treatment
residual disease
n = 58 axillary radiotherapy
>3 positive lymph nodes
n = 52
pCR
n = 20 axillary radiotherapy
residual disease
n = 32 ALND + axillary radiotherapy
Overall pCR axilla: 38%
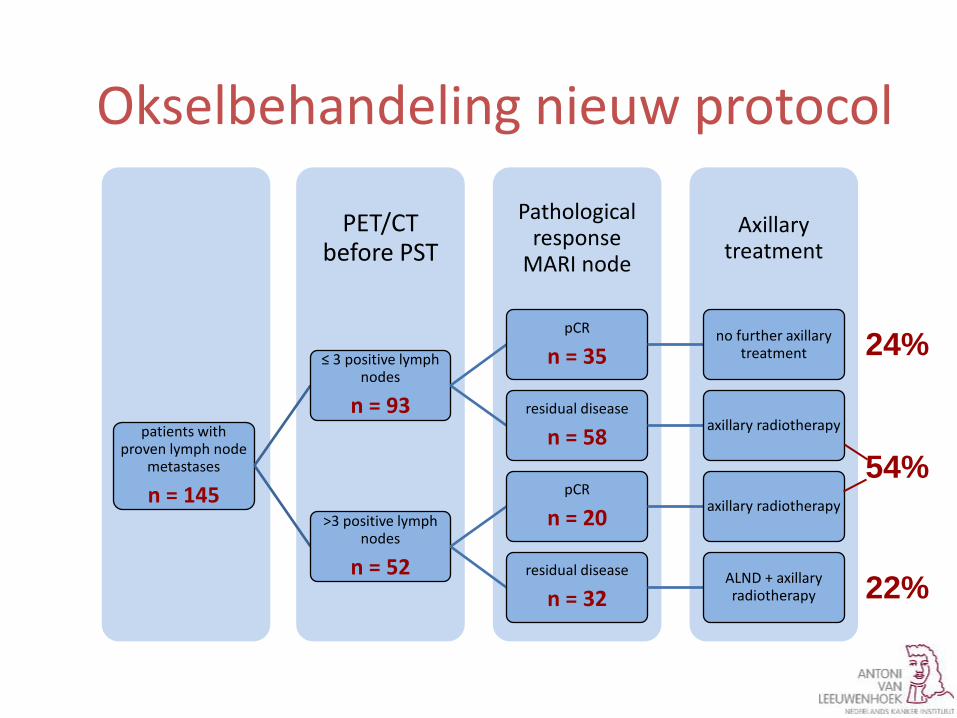
Okselbehandeling nieuw protocol
Axillary treatment
Pathological response
MARI node
PET/CT before PST
patients with proven lymph node
metastases
n = 145
≤ 3 positive lymph nodes
n = 93
pCR
n = 35 no further axillary
treatment
residual disease
n = 58 axillary radiotherapy
>3 positive lymph nodes
n = 52
pCR
n = 20 axillary radiotherapy
residual disease
n = 32 ALND + axillary radiotherapy
24%
54%
22%
Okselbehandeling nieuw protocol
Conclusie
• Combinatie van pre-NAC PET/CT en post-NAC MARI-procedure reduceert OKDs met 78%
• Median follow-up 6 mnd: geen locaal recidief • Langere follow-up nodig
Adjuvante CT doe het neo Stagering met PET Markering met I 125 bronnen Monitoring met MRI Streven naar pCR Chirurgisch plan aanpassen op response
Take home messages
Vragen?
• Dank voor uw aandacht!
• Workshop I-125 seeds: [email protected] • MICRA trial: [email protected]


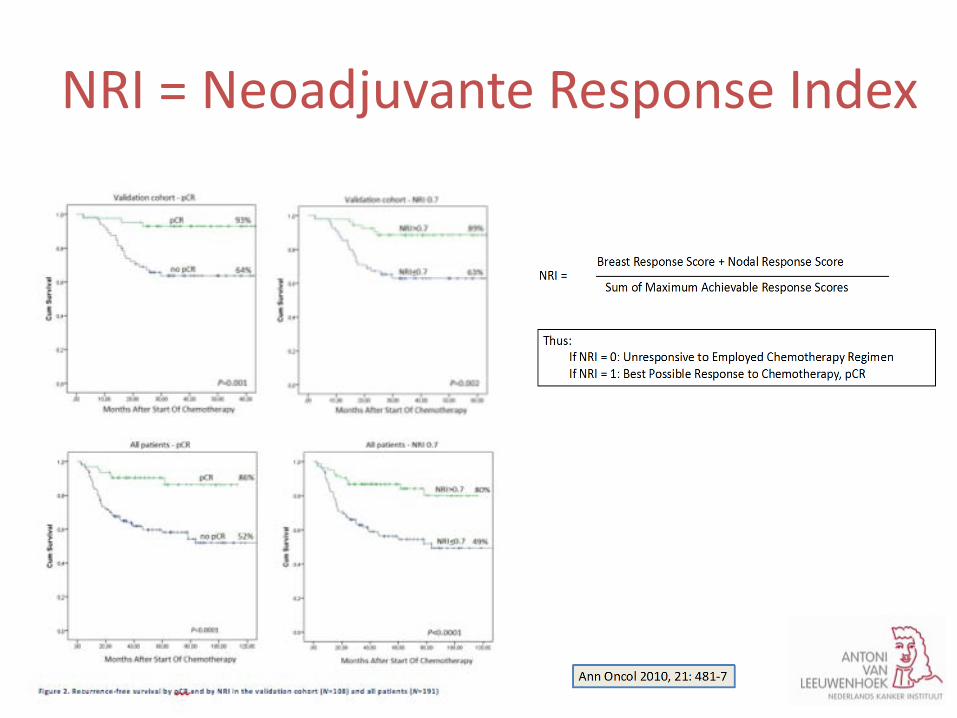
NRI = Neoadjuvante Response Index
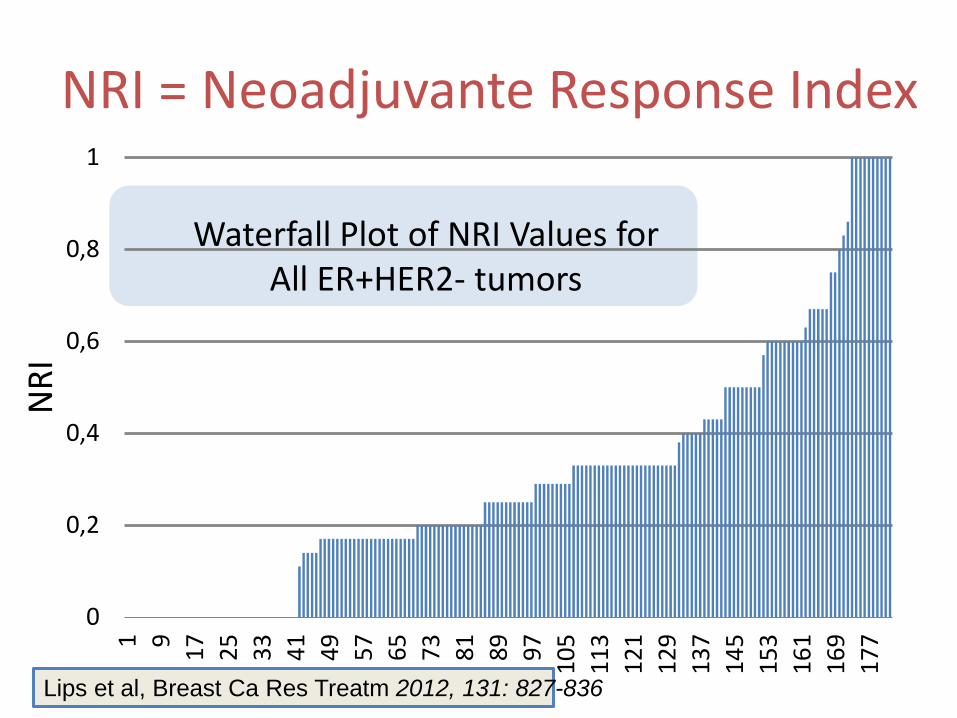
Waterfall Plot of NRI Values for All ER+HER2- tumors
0
0,2
0,4
0,6
0,8
11 9 17 25 33 41 49 57 65 73 81 89 97 105
113
121
129
137
145
153
161
169
177
NRI
Lips et al, Breast Ca Res Treatm 2012, 131: 827-836
NRI = Neoadjuvante Response Index
Verdere verbeteringen bij NAC
Nieuwe medicamenten Effectiever gebruik van bestaande
medicamenten Medicatie aanpassen aan response
- methoden response monitoring
- welke mate van response is nodig - bestaat non-cross resistente chemotherapie
Waarom neoadjuvante CT
Verbetering van de overleving
Mogelijkheid tot response monitoring
Kennis tot verbetering van de behandelingen
Tailored treatment: systemisch als locoregionaal
Vraagstukken: 1. optimale regime / switch per subtype 2. optimale monitoring per subtype 3. optimale chirurgie na NAC
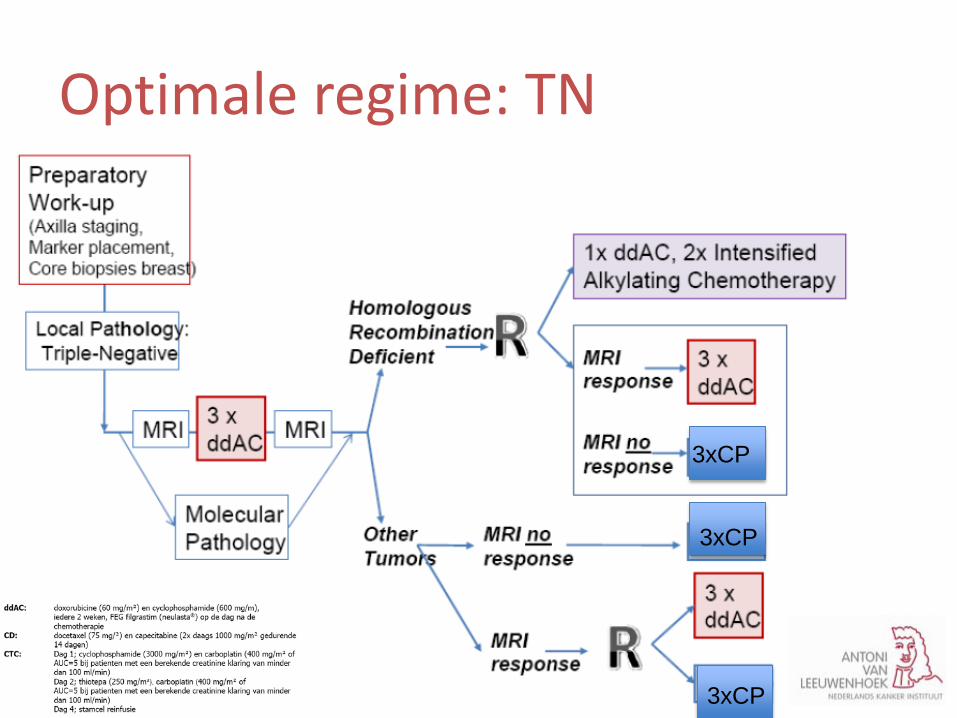
TNM-studie Bij ongeveer 50 % vd TN borstkankertumoren is er sprake van een homologe recombinatiedeficiëntie, DNA- reparatiemechanisme niet functioneert Geen herstel dubbelstrengs DNA- breuken Alkylererende middelen in hoge dosis (CTC) zorgt juist voor dubbelstrengs DNA schade
Optimale regime: TN
Optimale regime/switch
Optimale regime: TN
3xCP
3xCP
3xCP
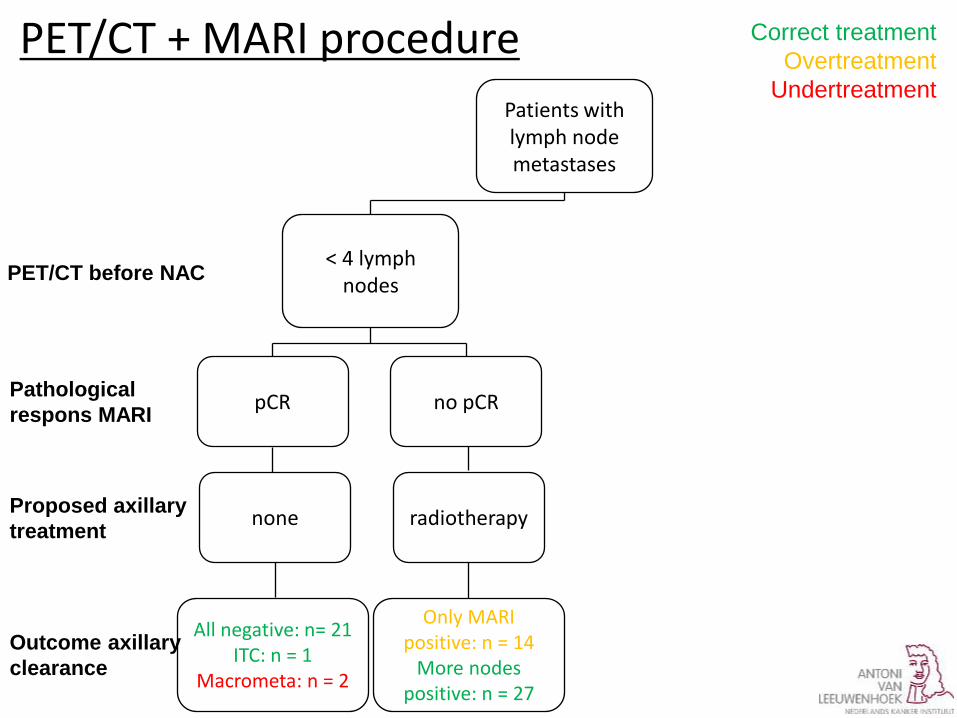
All negative: n= 21 ITC: n = 1
Macrometa: n = 2
none
pCR
< 4 lymph nodes
Patients with lymph node metastases
no pCR
radiotherapy
Only MARI positive: n = 14
More nodes positive: n = 27
radiotherapy
PET/CT + MARI procedure
PET/CT before NAC
Pathological respons MARI
Proposed axillary treatment
Outcome axillary clearance
Correct treatment Overtreatment
Undertreatment
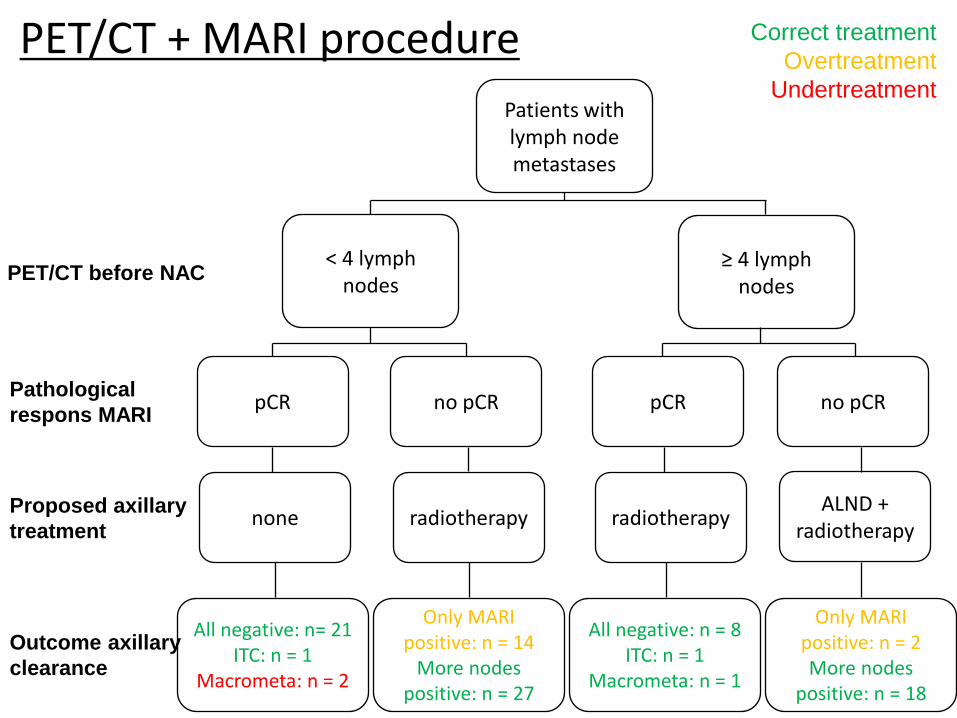
All negative: n= 21 ITC: n = 1
Macrometa: n = 2
none
pCR
< 4 lymph nodes
Patients with lymph node metastases
≥ 4 lymph nodes
no pCR
radiotherapy
Only MARI positive: n = 14
More nodes positive: n = 27
All negative: n = 8 ITC: n = 1
Macrometa: n = 1
radiotherapy
pCR no pCR
ALND + radiotherapy
Only MARI positive: n = 2 More nodes
positive: n = 18
PET/CT + MARI procedure
PET/CT before NAC
Pathological respons MARI
Proposed axillary treatment
Outcome axillary clearance
Correct treatment Overtreatment
Undertreatment