Metabole Alkalose tijdens Citraat Based CRRT · Metabole Alkalose Definitie: een te hoge pH van het...
94
Metabole Alkalose tijdens Citraat Based CRRT Hilde de Geus Renal Practitioners Symposium Zwolle November 2018
Transcript of Metabole Alkalose tijdens Citraat Based CRRT · Metabole Alkalose Definitie: een te hoge pH van het...

Metabole Alkalose tijdens Citraat Based
CRRT
Hilde de Geus
Renal Practitioners Symposium Zwolle
November 2018
Wat is een Metabole Alkalose?
Metabole Alkalose
Definitie: een te hoge pH van het bloed > 7.4 dat wordt
veroorzaakt door een te kort aan zure of een overschot aan
basische stoffen
Metabole Alkalose
Chemische buffering: Bicarbonaat-Koolstofdioxide buffer
H+ + HCO3- H2CO3 CO2 + H2O
Metabole Alkalose
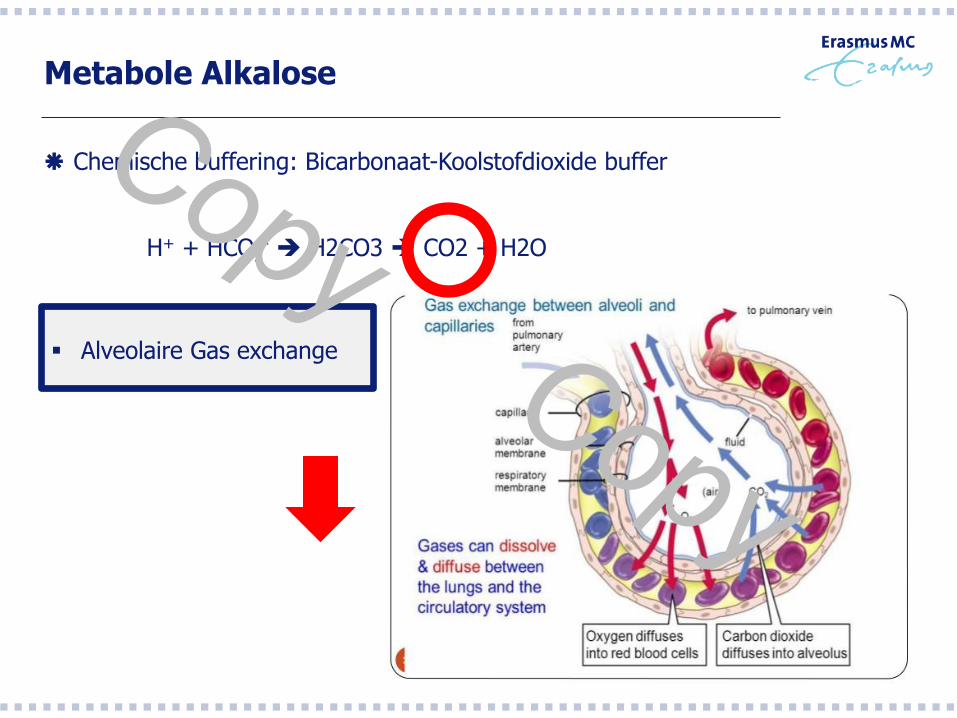
Chemische buffering: Bicarbonaat-Koolstofdioxide buffer
H+ + HCO3- H2CO3 CO2 + H2O
Alveolaire Gas exchange
Metabole Alkalose
Chemische buffering: Bicarbonaat-Koolstofdioxide buffer
H+ + HCO3- H2CO3 CO2 + H2O
Resorptie van HCO3 (80-90% in proximale tubulus)
Excretie van H+ (Actieve excretie in proximale en distale tubulus, Fosfaat buffer
Ammonia buffer)
Bij ernstige acidose raken de BIC en Fosfaat buffers uitgeput, de ammoniabuffer
wordt belangrijker omdat tubulus cellen ammonia kunnen produceren
Metabole Alkalose
Verlies van zuren via nieren: hyperaldosteronisme
via nieren: renale tubulaire acidose
via maag-darm: braken, maagsonde
via maag-darm: diarree
Inname van basische stoffen Rennies (Calciumcarbonaat)
Citraat
Laxantia misbruik
Diuretica gebruik
Hypercorticisme (gebruik van glucocorticoiden: hypokaliemische alkalose)
Wat is Citraat?
Citraat
C6H5O7 : koolwaterstofverbinding
Wordt omgezet in H20 en BIC
Trinatrium Citraat = anticoagulant
Sterke bindingscapaciteit voor geioniseerd Calcium en Magnesium
Calcium = belangrijke co-factor voor de stollingscascade
Citraat is co-factor in de ademhalingsketen (citroen zuur cyclus)
Wat is Citraat? - Antistollingsmiddel -

Het hemofilter
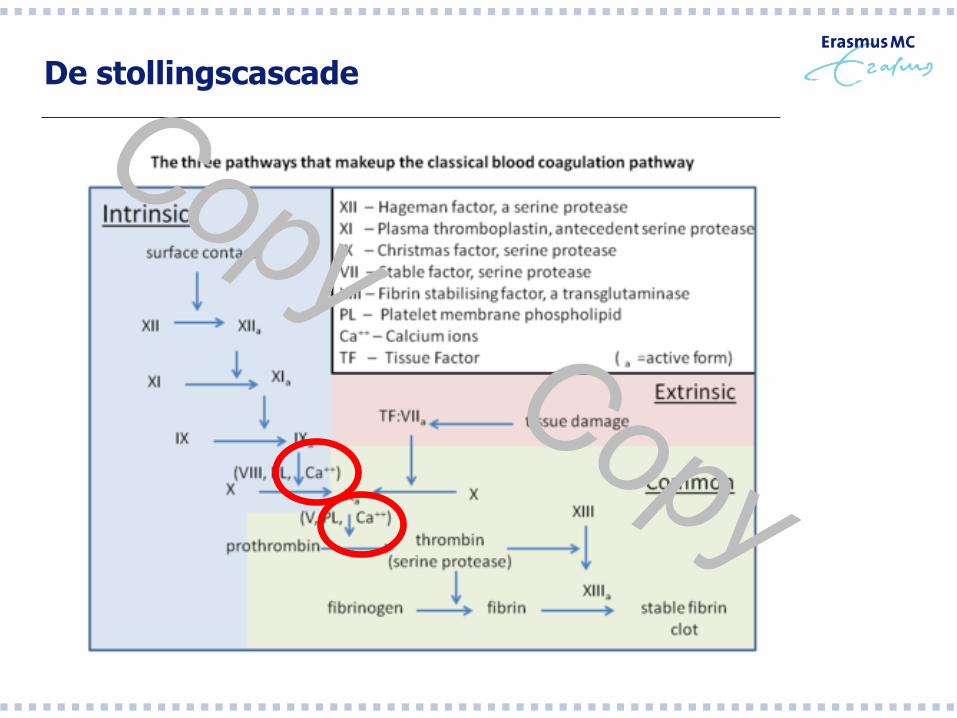
De stollingscascade
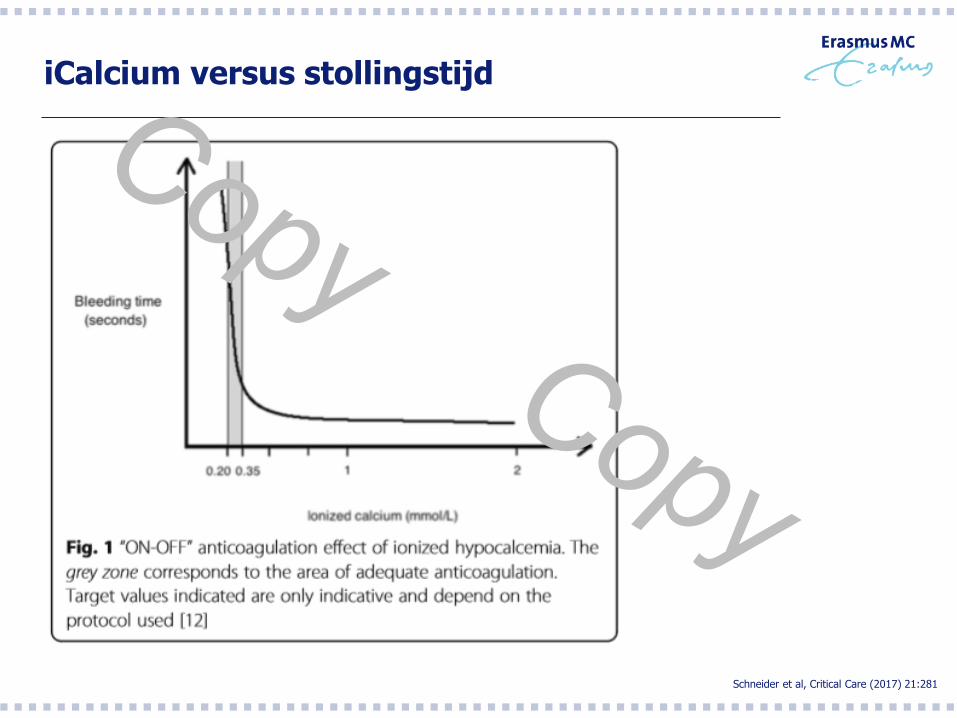
iCalcium versus stollingstijd
Schneider et al, Critical Care (2017) 21:281
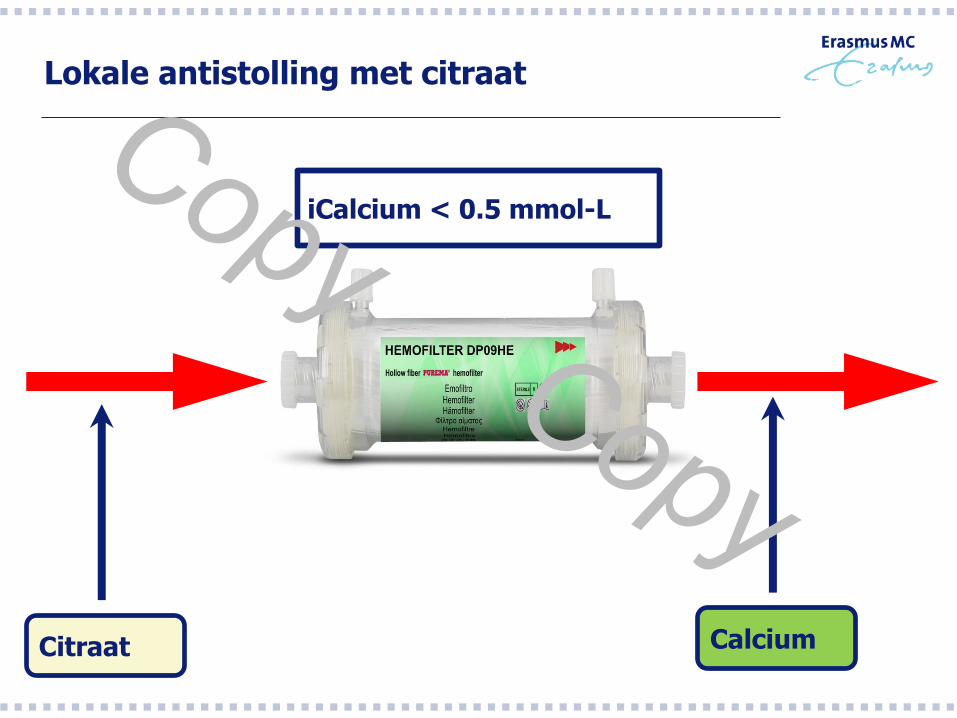
Lokale antistolling met citraat
Citraat Calcium
iCalcium < 0.5 mmol-L
Wat is Citraat? - Bicarbonaat donor -
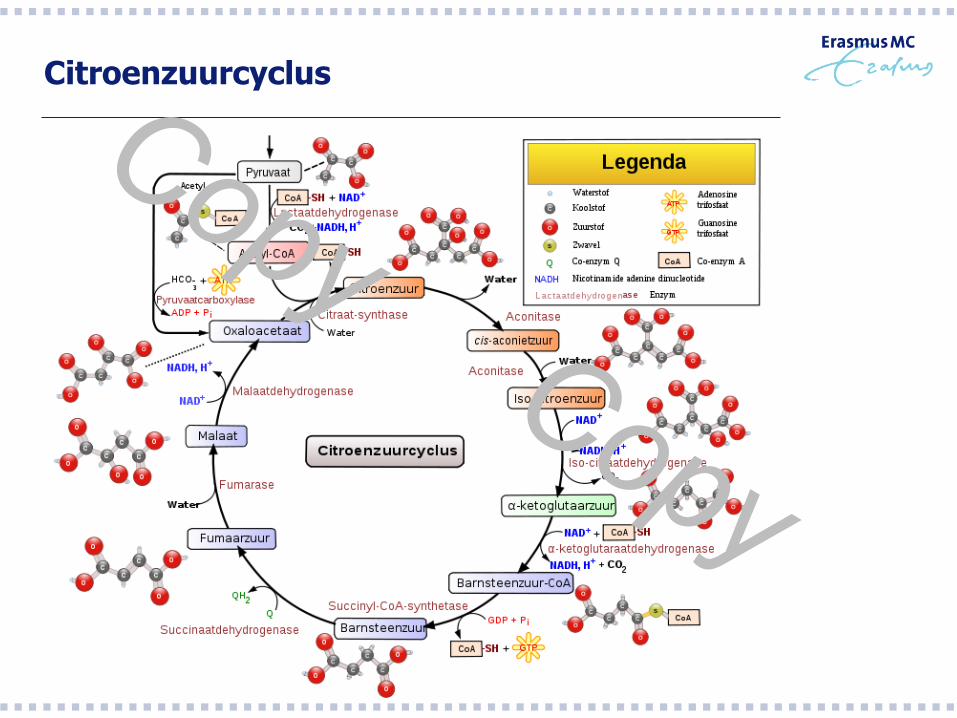
Citroenzuurcyclus
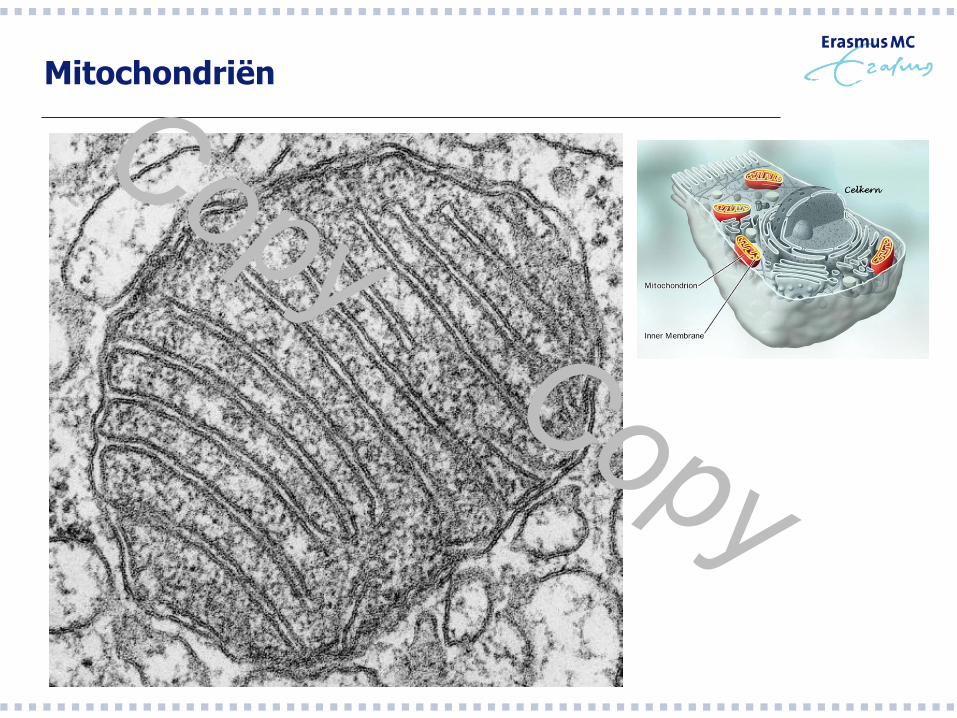
Mitochondriën
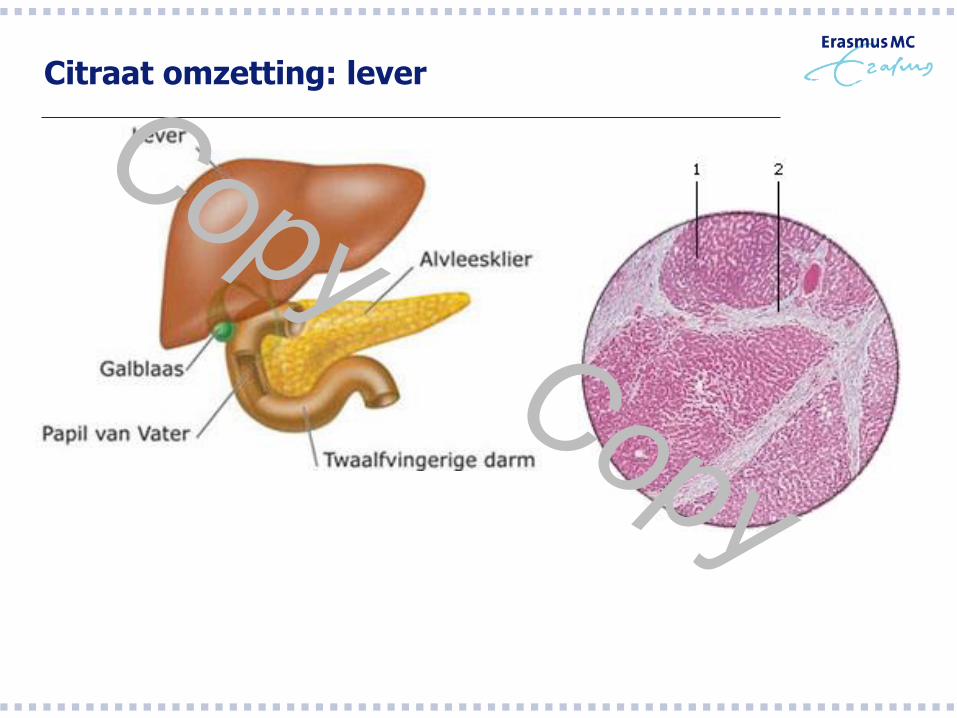
Citraat omzetting: lever

Citraat omzetting: dwarsgestreepte spieren
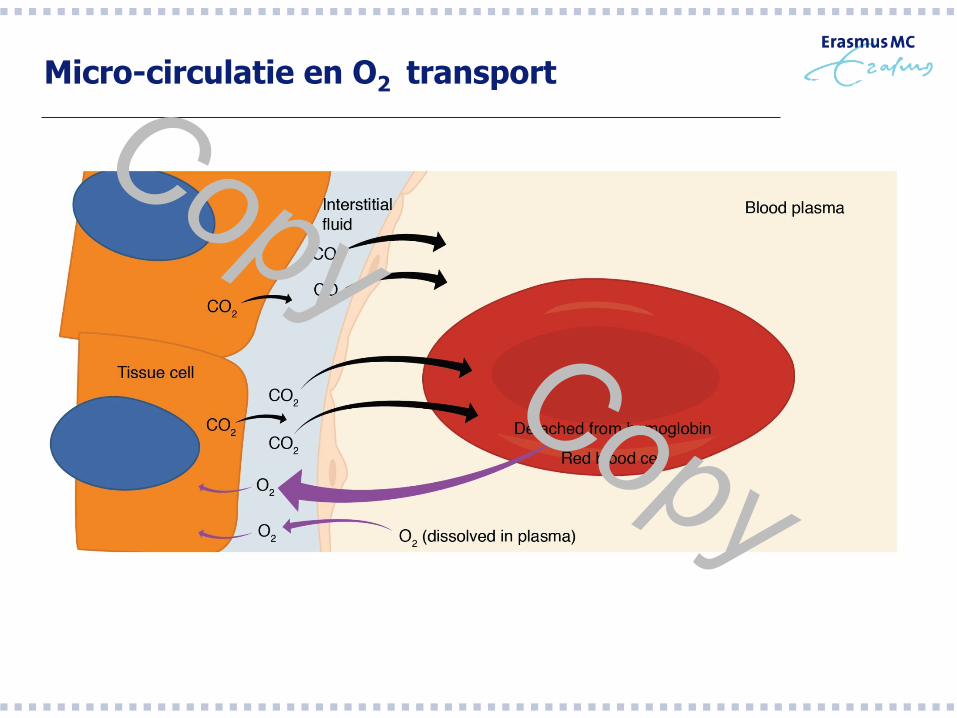
Micro-circulatie en O2 transport
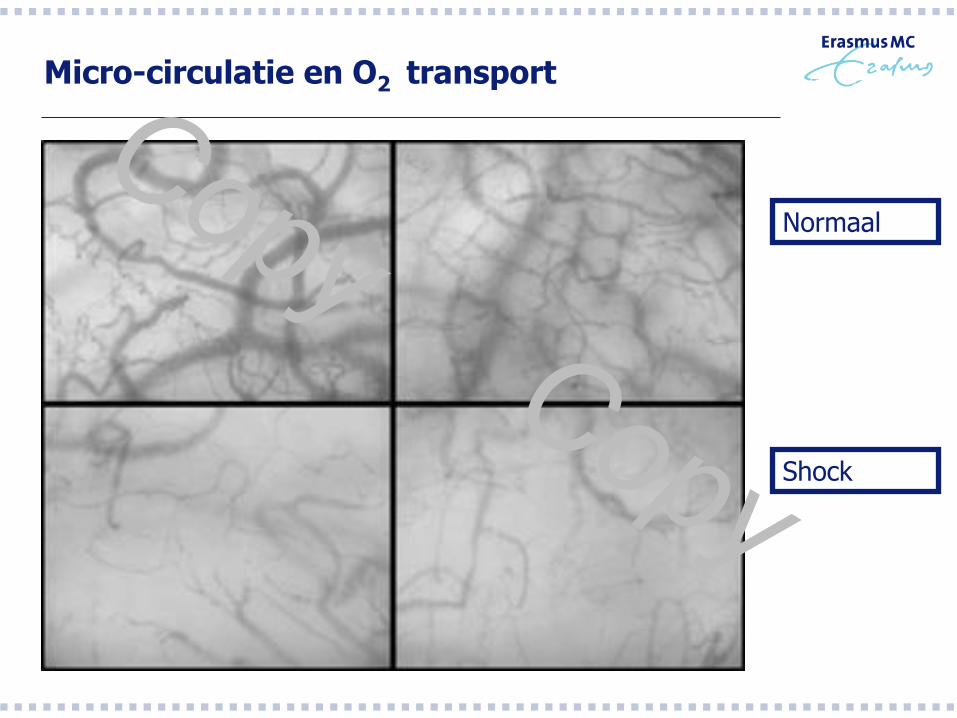
Micro-circulatie en O2 transport
Normaal
Shock
Citraat toepassing tijdens CRRT - Welke verschillen zijn er tussen de beschikbare Citraat protocollen? -

Wat is er te koop in NL ?
Wat is er te koop in NL ?
Doel:
-1. Citraat concentratie 3-4 mmol-l in het hemofilter
-2. iCalcium < 0.35 mmol-l in het extracorporele systeem
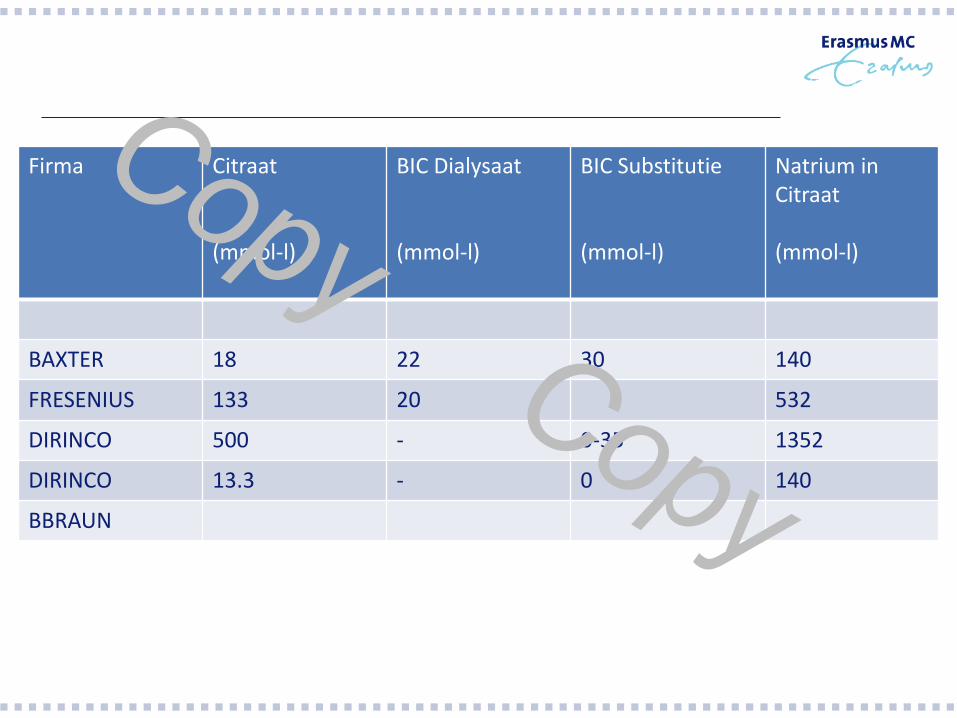
Firma Citraat (mmol-l)
BIC Dialysaat (mmol-l)
BIC Substitutie (mmol-l)
Natrium in Citraat (mmol-l)
BAXTER 18 22 30 140
FRESENIUS 133 20 532
DIRINCO 500 - 0-35 1352
DIRINCO 13.3 - 0 140
BBRAUN
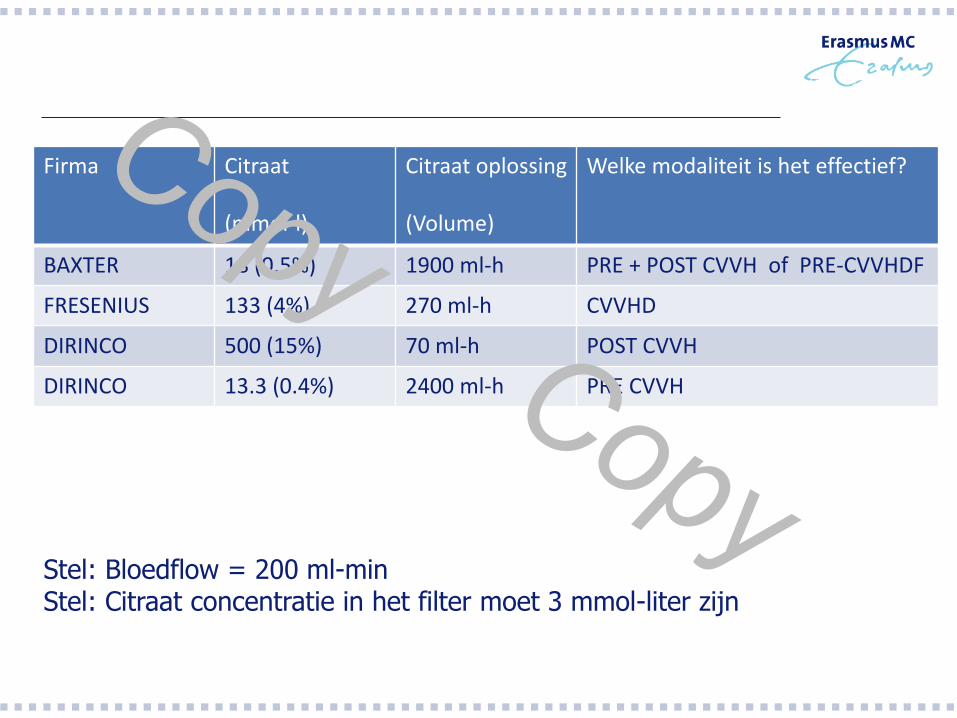
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
Welke modaliteit is het effectief?
BAXTER 18 (0.5%) 1900 ml-h PRE + POST CVVH of PRE-CVVHDF
FRESENIUS 133 (4%) 270 ml-h CVVHD
DIRINCO 500 (15%) 70 ml-h POST CVVH
DIRINCO 13.3 (0.4%) 2400 ml-h PRE CVVH
Stel: Bloedflow = 200 ml-min Stel: Citraat concentratie in het filter moet 3 mmol-liter zijn
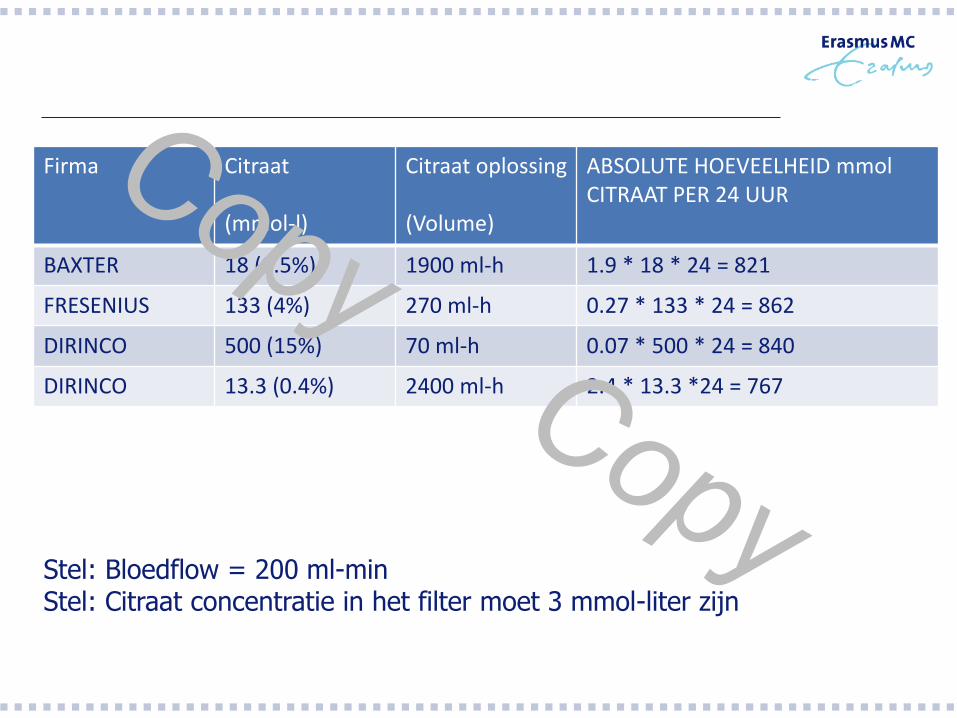
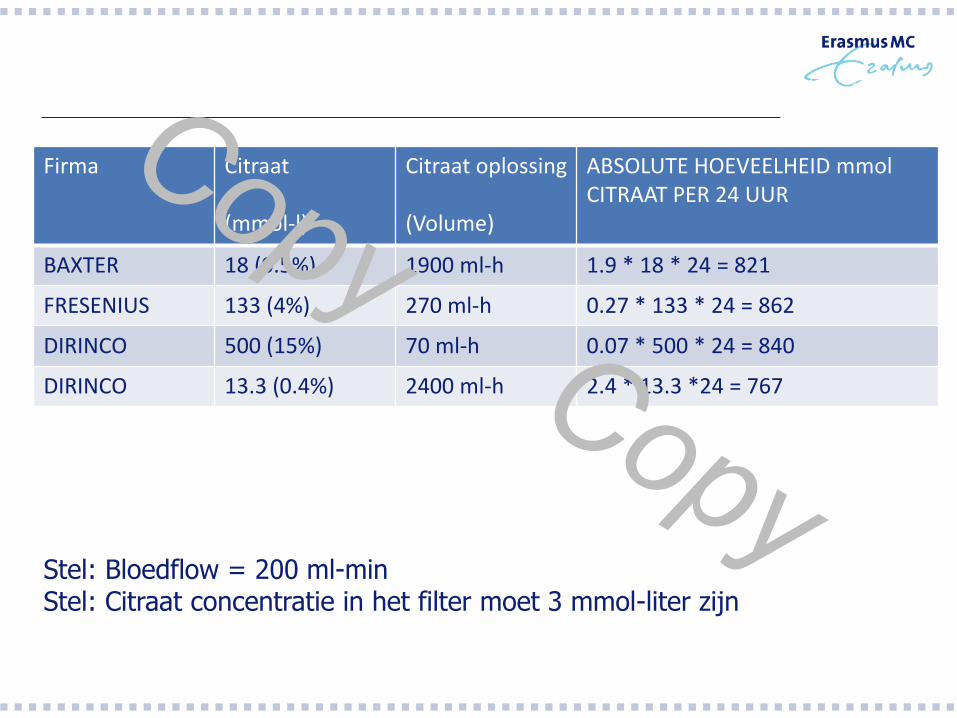
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
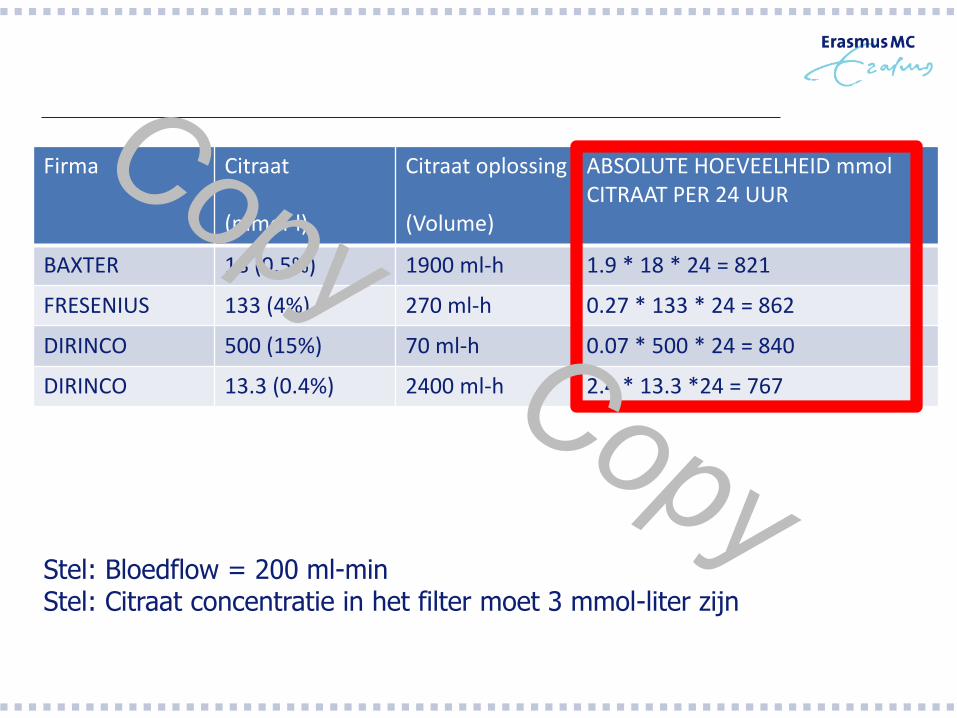
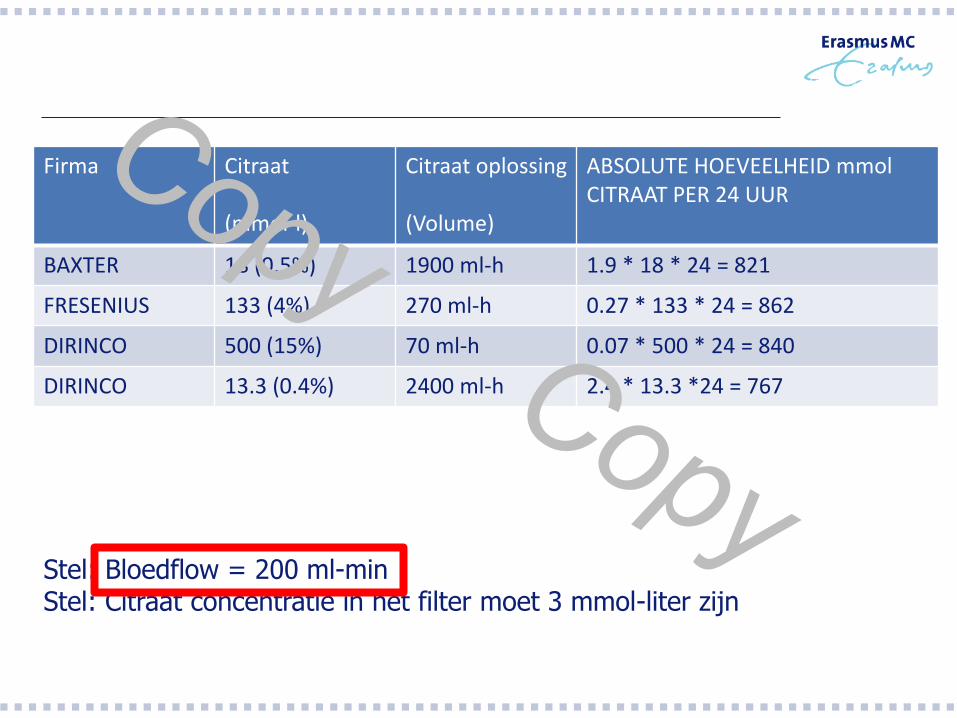
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 1900 ml-h 1.9 * 18 * 24 = 821
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 70 ml-h 0.07 * 500 * 24 = 840
DIRINCO 13.3 (0.4%) 2400 ml-h 2.4 * 13.3 *24 = 767
Stel: Bloedflow = 200 ml-min Stel: Citraat concentratie in het filter moet 3 mmol-liter zijn
Dus welke factoren bepalen Alkalose? - Machineinstellingen -
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 1900 ml-h 1.9 * 18 * 24 = 821
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 70 ml-h 0.07 * 500 * 24 = 840
DIRINCO 13.3 (0.4%) 2400 ml-h 2.4 * 13.3 *24 = 767
Stel: Bloedflow = 200 ml-min Stel: Citraat concentratie in het filter moet 3 mmol-liter zijn
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 1900 ml-h 1.9 * 18 * 24 = 821
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 70 ml-h 0.07 * 500 * 24 = 840
DIRINCO 13.3 (0.4%) 2400 ml-h 2.4 * 13.3 *24 = 767
Stel: Bloedflow = 200 ml-min Stel: Citraat concentratie in het filter moet 3 mmol-liter zijn
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 1900 ml-h 1.9 * 18 * 24 = 821
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 70 ml-h 0.07 * 500 * 24 = 840
DIRINCO 13.3 (0.4%) 2400 ml-h 2.4 * 13.3 *24 = 767
Stel: Bloedflow = 200 ml-min Stel: Citraat concentratie in het filter moet 3 mmol-liter zijn
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 2000 ml-h 2.0 * 18 * 24 = 864
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 72 ml-h 0.072 * 500 * 24 = 864
DIRINCO 13.3 (0.4%) 2700 ml-h 2.7 * 13.3 * 24 = 862
BLOEDFLOW = 100 ML-MIN
BAXTER 18 (0.5%) 1000 ml-h 1.0 * 18 * 24 = 432
FRESENIUS 133 (4%) 135 ml-h 0.14 * 133 * 24 = 447
DIRINCO 500 (15%) 36 ml-h 0.036 * 500 * 24 = 432
DIRINCO 13.3 (0.4%) 1350 ml-h 1.35 * 13.3 * 24 = 431
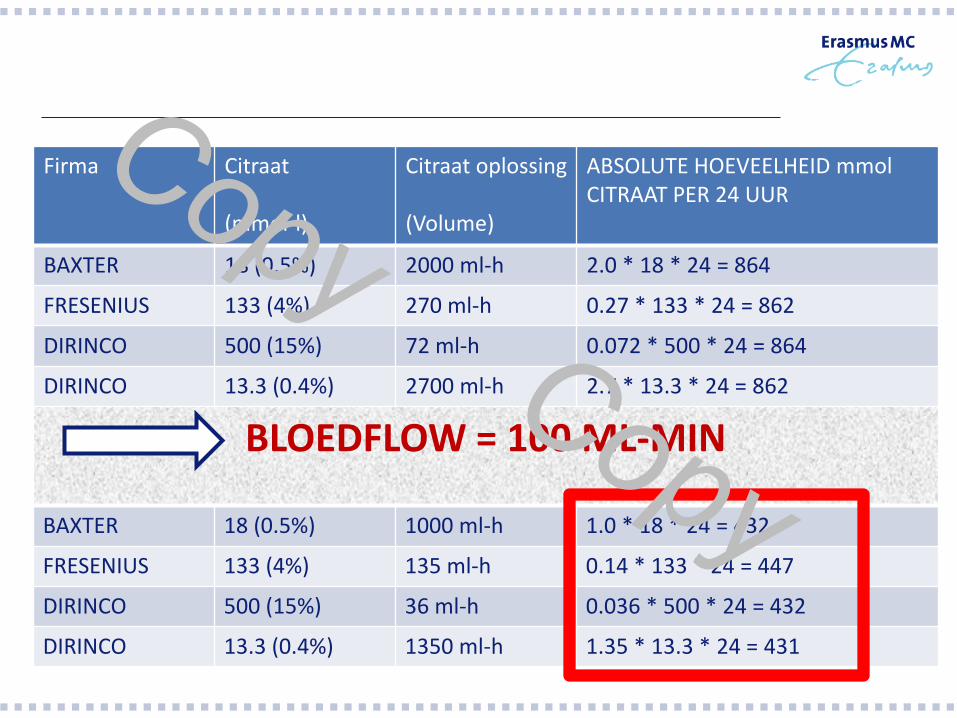
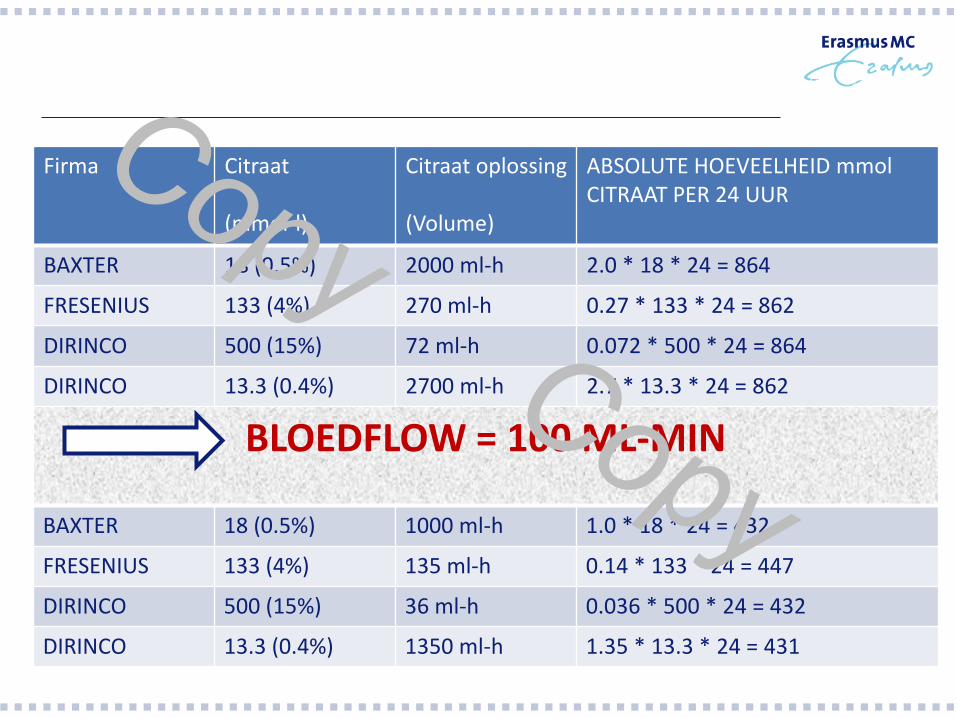
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 2000 ml-h 2.0 * 18 * 24 = 864
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 72 ml-h 0.072 * 500 * 24 = 864
DIRINCO 13.3 (0.4%) 2700 ml-h 2.7 * 13.3 * 24 = 862
BLOEDFLOW = 100 ML-MIN
BAXTER 18 (0.5%) 1000 ml-h 1.0 * 18 * 24 = 432
FRESENIUS 133 (4%) 135 ml-h 0.14 * 133 * 24 = 447
DIRINCO 500 (15%) 36 ml-h 0.036 * 500 * 24 = 432
DIRINCO 13.3 (0.4%) 1350 ml-h 1.35 * 13.3 * 24 = 431
Dus welke factoren bepalen Alkalose? - Machine instellingen Dialysaat en of Substitutie vloeistofsamenstelling -
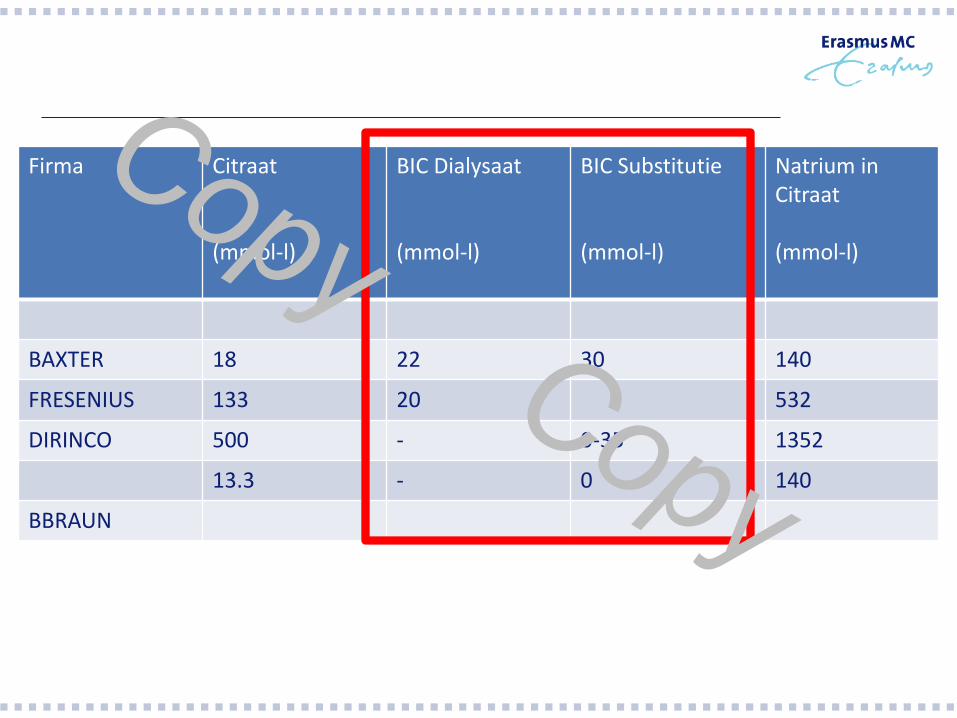
Firma Citraat (mmol-l)
BIC Dialysaat (mmol-l)
BIC Substitutie (mmol-l)
Natrium in Citraat (mmol-l)
BAXTER 18 22 30 140
FRESENIUS 133 20 532
DIRINCO 500 - 0-35 1352
13.3 - 0 140
BBRAUN
Dus welke factoren bepalen Alkalose? - Streefwaarden (Protocol related) -
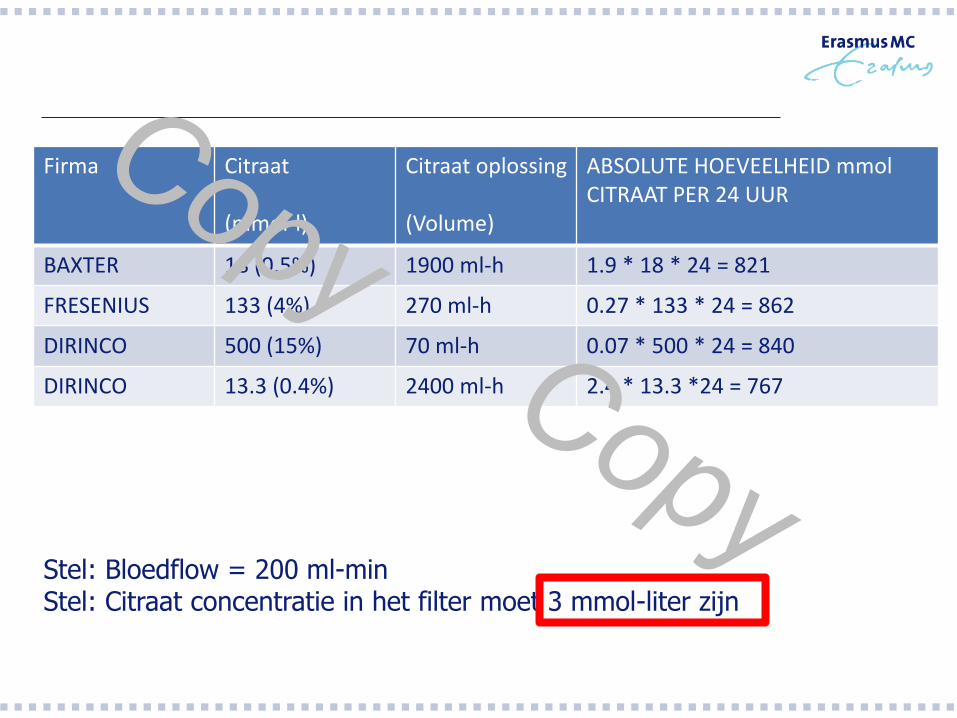
Firma Citraat (mmol-l)
Citraat oplossing (Volume)
ABSOLUTE HOEVEELHEID mmol CITRAAT PER 24 UUR
BAXTER 18 (0.5%) 1900 ml-h 1.9 * 18 * 24 = 821
FRESENIUS 133 (4%) 270 ml-h 0.27 * 133 * 24 = 862
DIRINCO 500 (15%) 70 ml-h 0.07 * 500 * 24 = 840
DIRINCO 13.3 (0.4%) 2400 ml-h 2.4 * 13.3 *24 = 767
Stel: Bloedflow = 200 ml-min Stel: Citraat concentratie in het filter moet 3 mmol-liter zijn
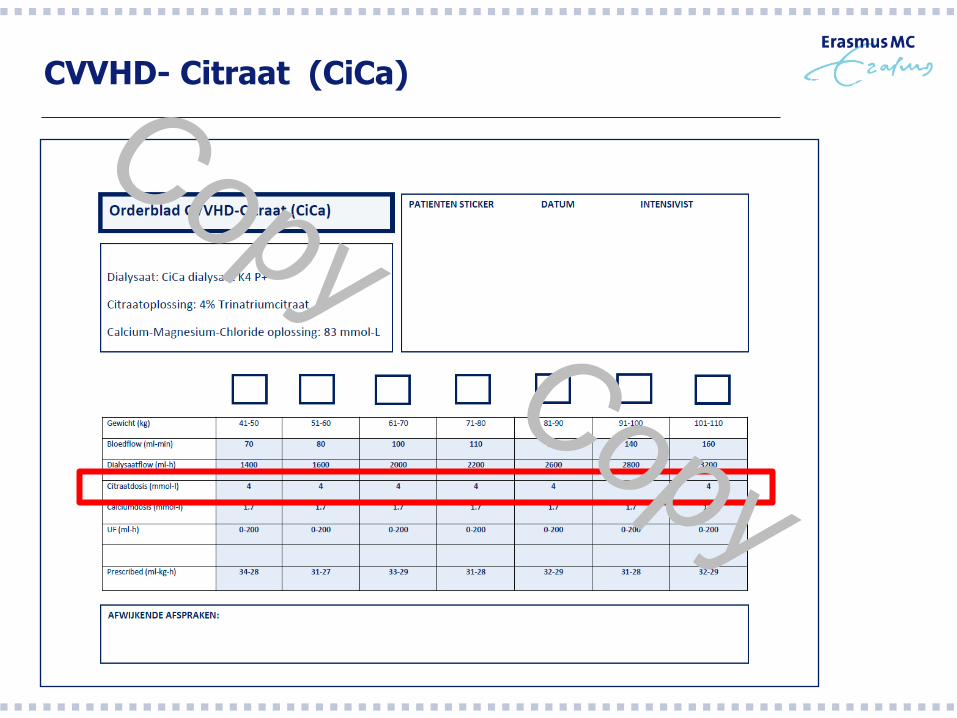
CVVHD- Citraat (CiCa)
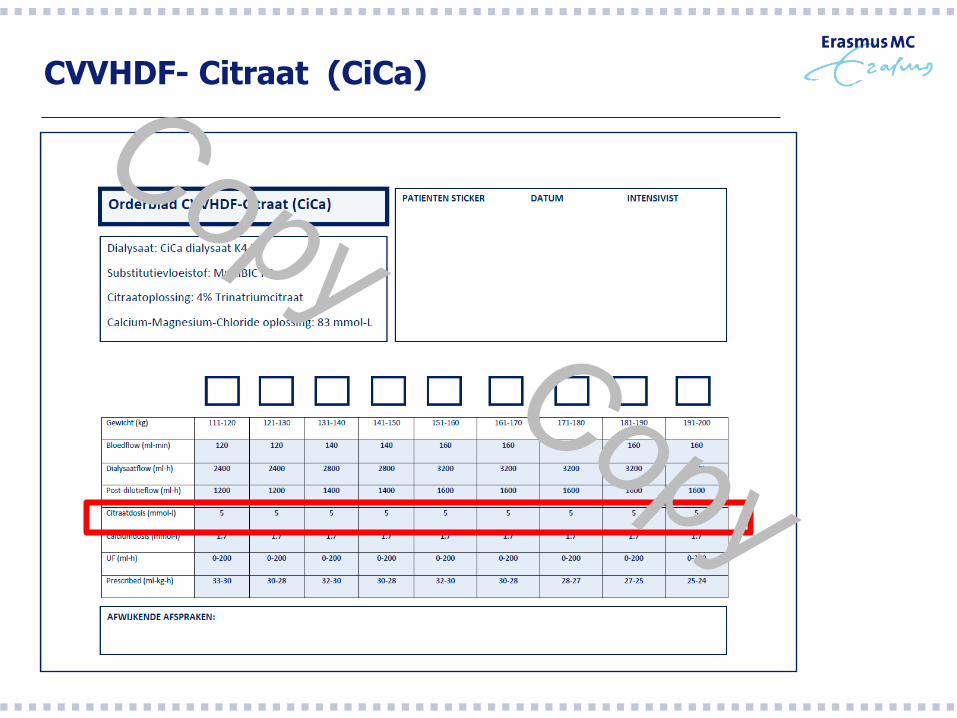
CVVHDF- Citraat (CiCa)
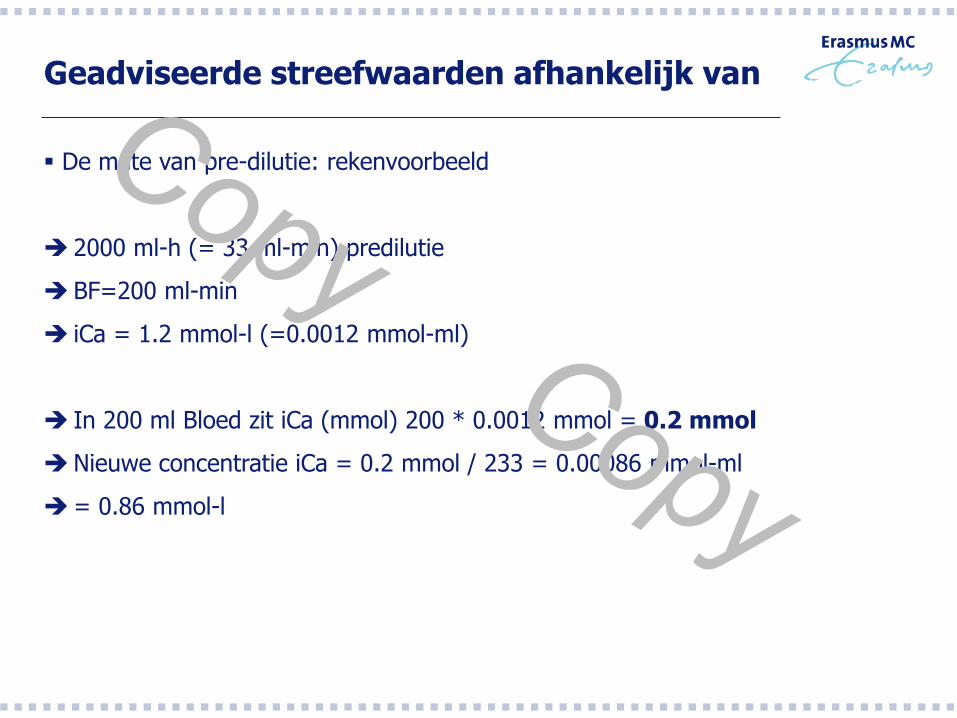
Geadviseerde streefwaarden afhankelijk van
De mate van pre-dilutie: rekenvoorbeeld
2000 ml-h (= 33 ml-min) predilutie
BF=200 ml-min
iCa = 1.2 mmol-l (=0.0012 mmol-ml)
In 200 ml Bloed zit iCa (mmol) 200 * 0.0012 mmol = 0.2 mmol
Nieuwe concentratie iCa = 0.2 mmol / 233 = 0.00086 mmol-ml
= 0.86 mmol-l
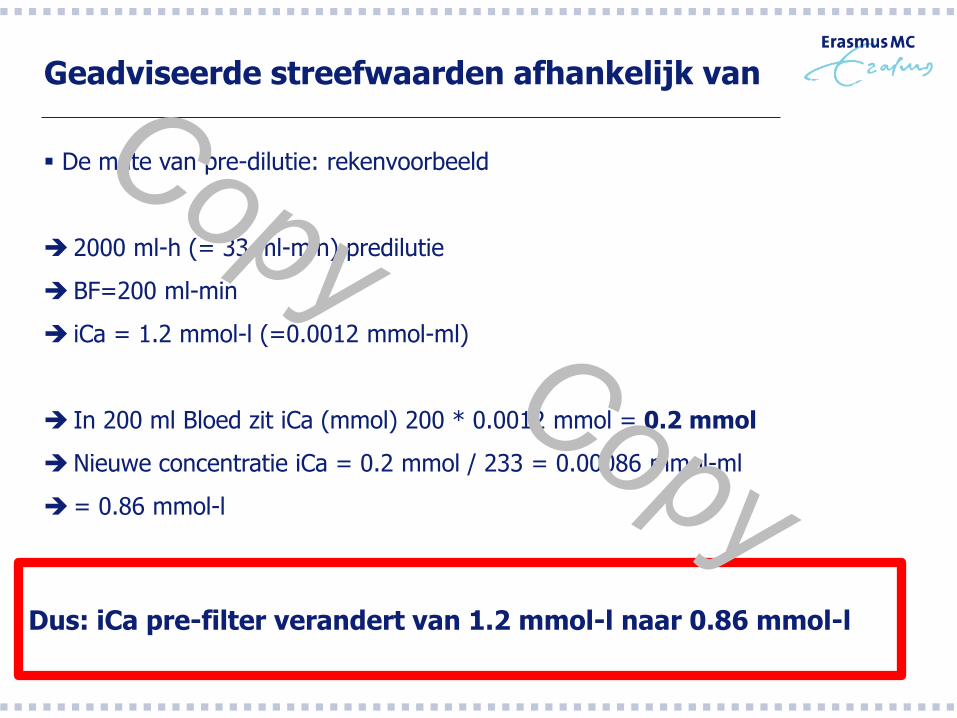
Geadviseerde streefwaarden afhankelijk van
De mate van pre-dilutie: rekenvoorbeeld
2000 ml-h (= 33 ml-min) predilutie
BF=200 ml-min
iCa = 1.2 mmol-l (=0.0012 mmol-ml)
In 200 ml Bloed zit iCa (mmol) 200 * 0.0012 mmol = 0.2 mmol
Nieuwe concentratie iCa = 0.2 mmol / 233 = 0.00086 mmol-ml
= 0.86 mmol-l
Dus: iCa pre-filter verandert van 1.2 mmol-l naar 0.86 mmol-l
Geadviseerde streefwaarden afhankelijk van
De mate van indikking over het filter heen (Hoe groot is de UF en
de Hemofiltratie component)
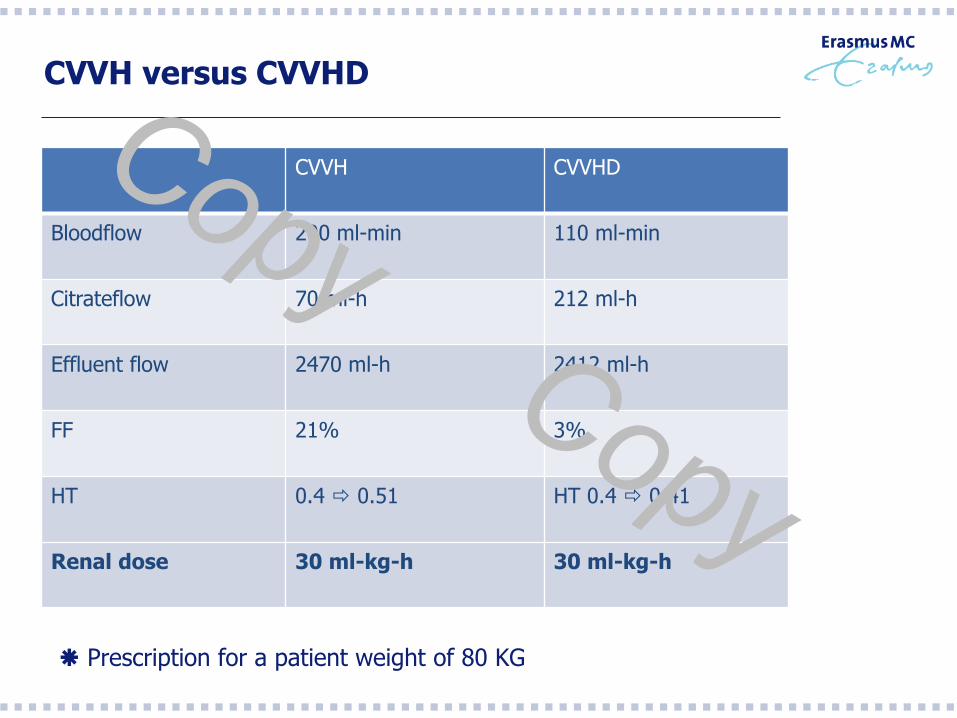
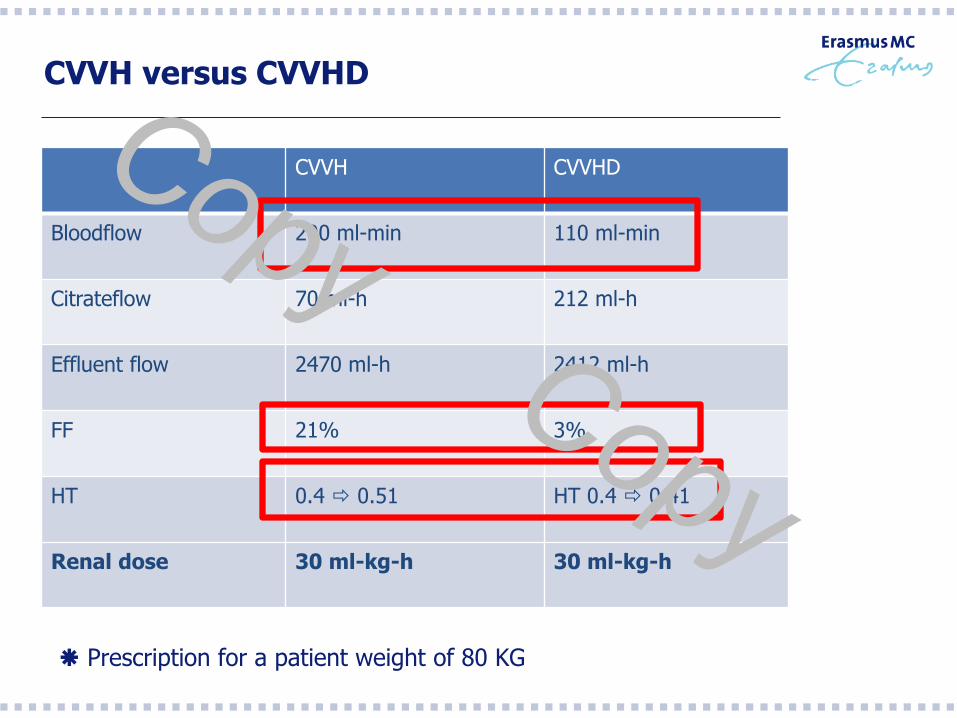
CVVH versus CVVHD
CVVH CVVHD
Bloodflow 200 ml-min 110 ml-min
Citrateflow 70 ml-h 212 ml-h
Effluent flow 2470 ml-h 2412 ml-h
FF 21% 3%
HT 0.4 0.51 HT 0.4 0.41
Renal dose 30 ml-kg-h 30 ml-kg-h
Prescription for a patient weight of 80 KG
CVVH versus CVVHD
CVVH CVVHD
Bloodflow 200 ml-min 110 ml-min
Citrateflow 70 ml-h 212 ml-h
Effluent flow 2470 ml-h 2412 ml-h
FF 21% 3%
HT 0.4 0.51 HT 0.4 0.41
Renal dose 30 ml-kg-h 30 ml-kg-h
Prescription for a patient weight of 80 KG
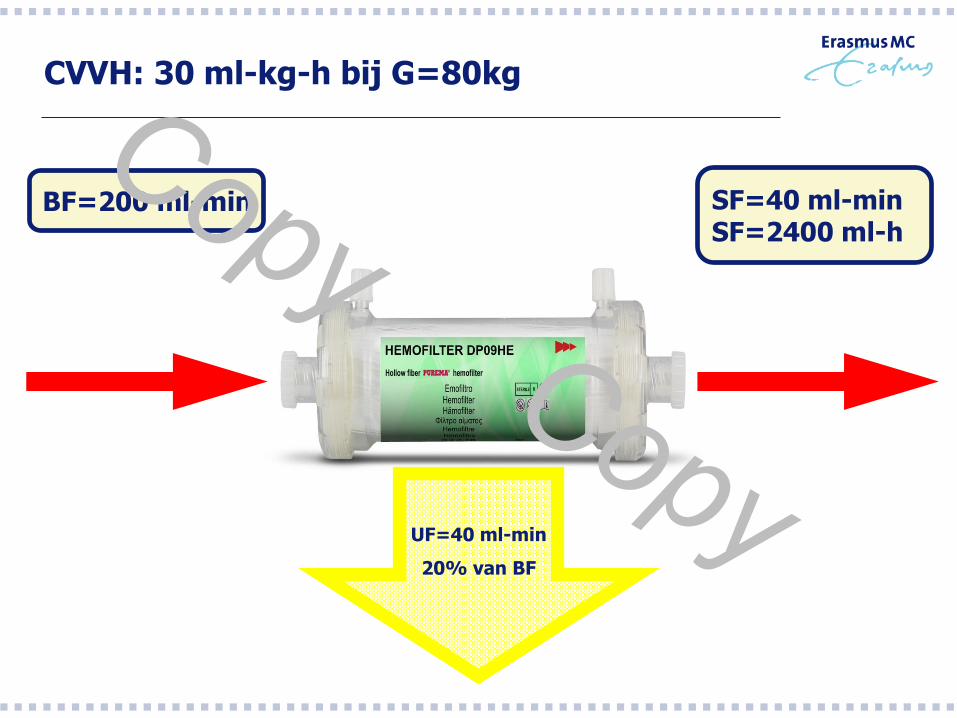
CVVH: 30 ml-kg-h bij G=80kg
BF=200 ml-min SF=40 ml-min SF=2400 ml-h
UF=40 ml-min
20% van BF
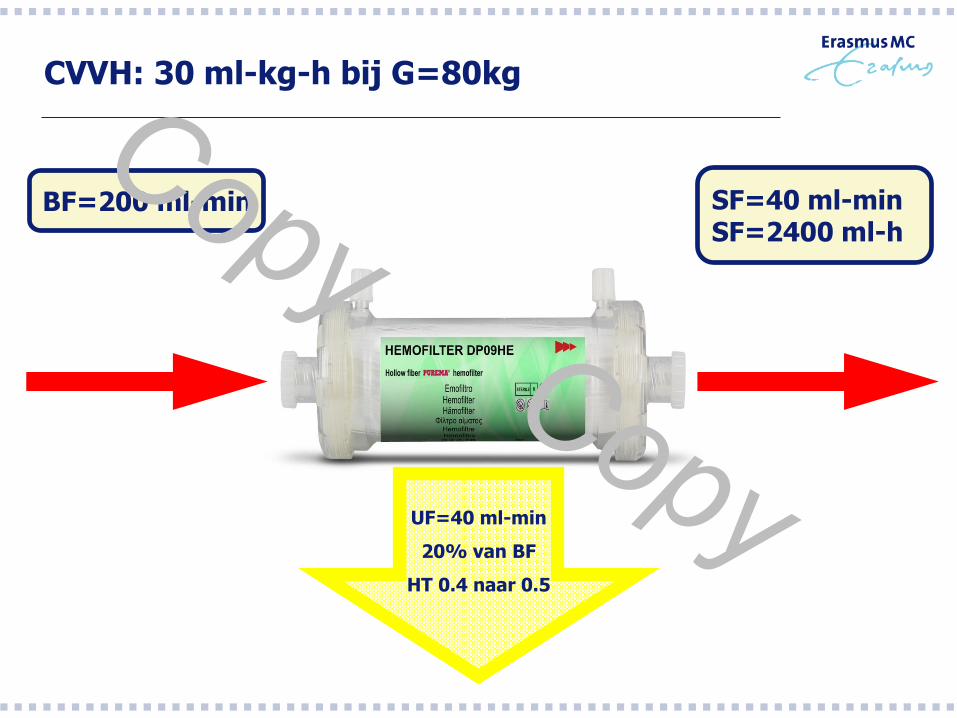
CVVH: 30 ml-kg-h bij G=80kg
BF=200 ml-min SF=40 ml-min SF=2400 ml-h
UF=40 ml-min
20% van BF
HT 0.4 naar 0.5
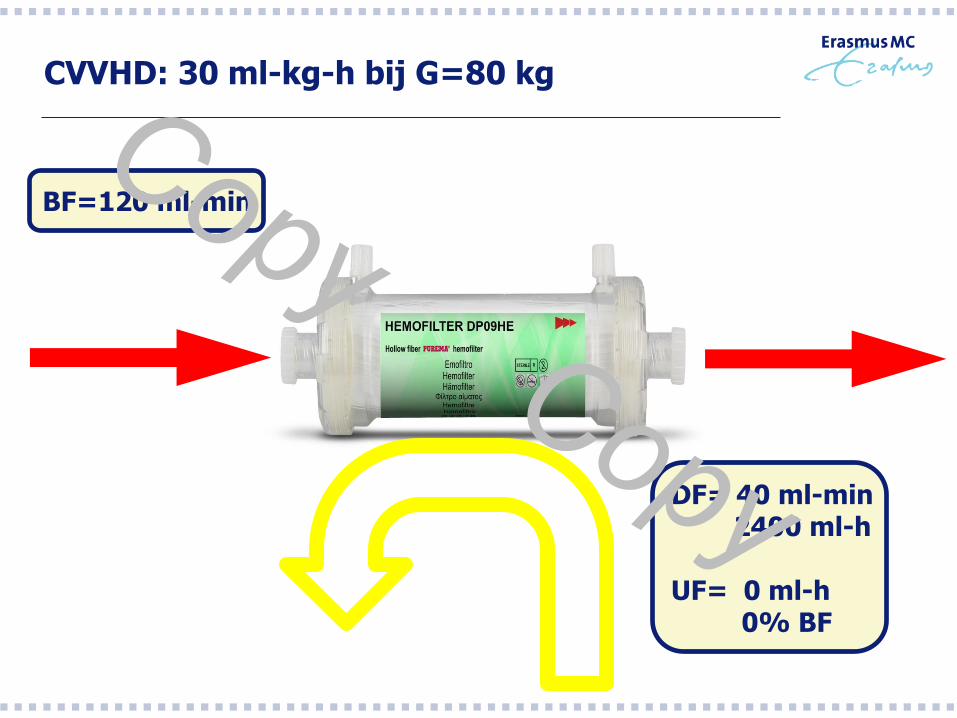
CVVHD: 30 ml-kg-h bij G=80 kg
BF=120 ml-min
DF= 40 ml-min 2400 ml-h UF= 0 ml-h 0% BF
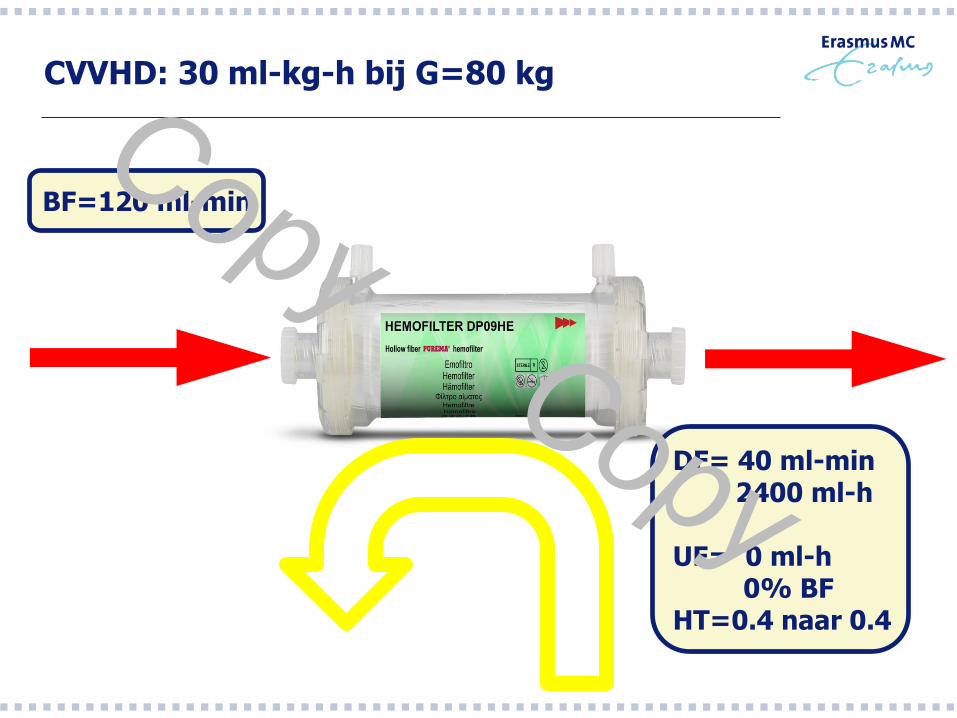
CVVHD: 30 ml-kg-h bij G=80 kg
BF=120 ml-min
DF= 40 ml-min 2400 ml-h UF= 0 ml-h 0% BF HT=0.4 naar 0.4
Dus welke factoren bepalen Alkalose? - “Calcium huishouding van de patient” -
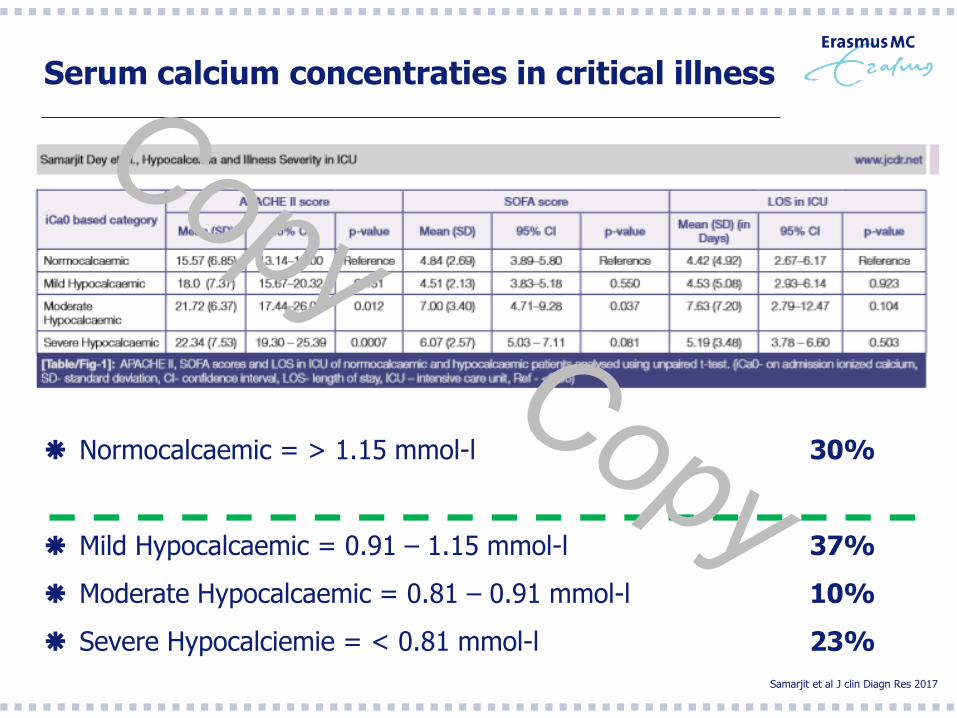
Serum calcium concentraties in critical illness
Normocalcaemic = > 1.15 mmol-l 30%
Mild Hypocalcaemic = 0.91 – 1.15 mmol-l 37%
Moderate Hypocalcaemic = 0.81 – 0.91 mmol-l 10%
Severe Hypocalciemie = < 0.81 mmol-l 23%
Samarjit et al J clin Diagn Res 2017
Serum Calcium afwijkingen bij ziektebeelden
Pancreatitis
Maligniteiten (Bot metastasen, Multipel Myeloom, ..)
Hyperparathyreoidie
Hypoparathyreoidie
Medicamenteus (Vitamine D)
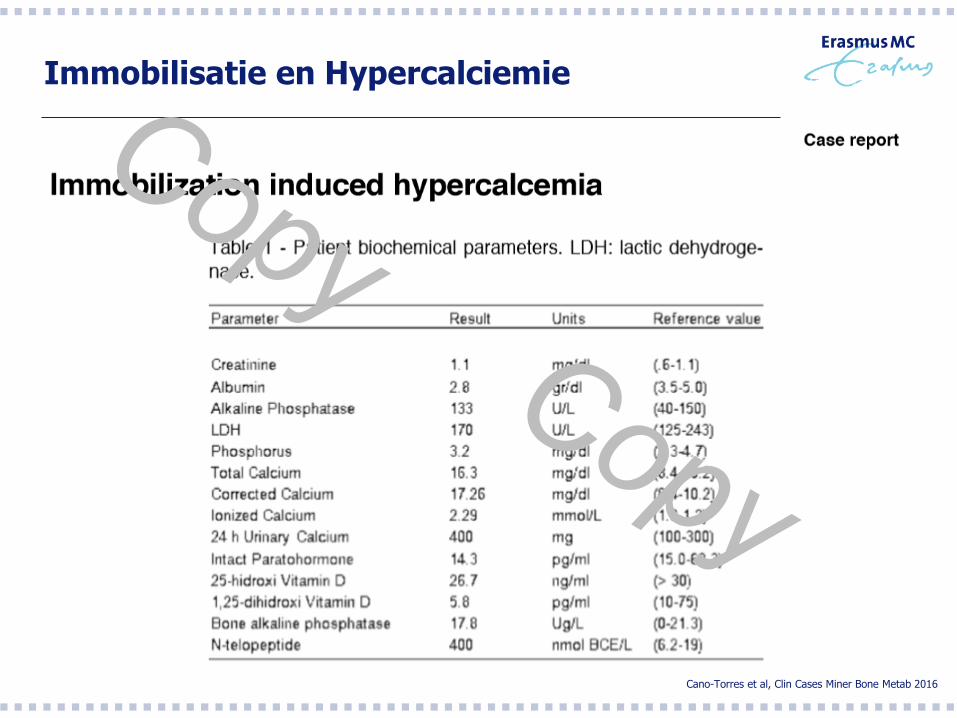
Immobilisatie en Hypercalciemie
Cano-Torres et al, Clin Cases Miner Bone Metab 2016
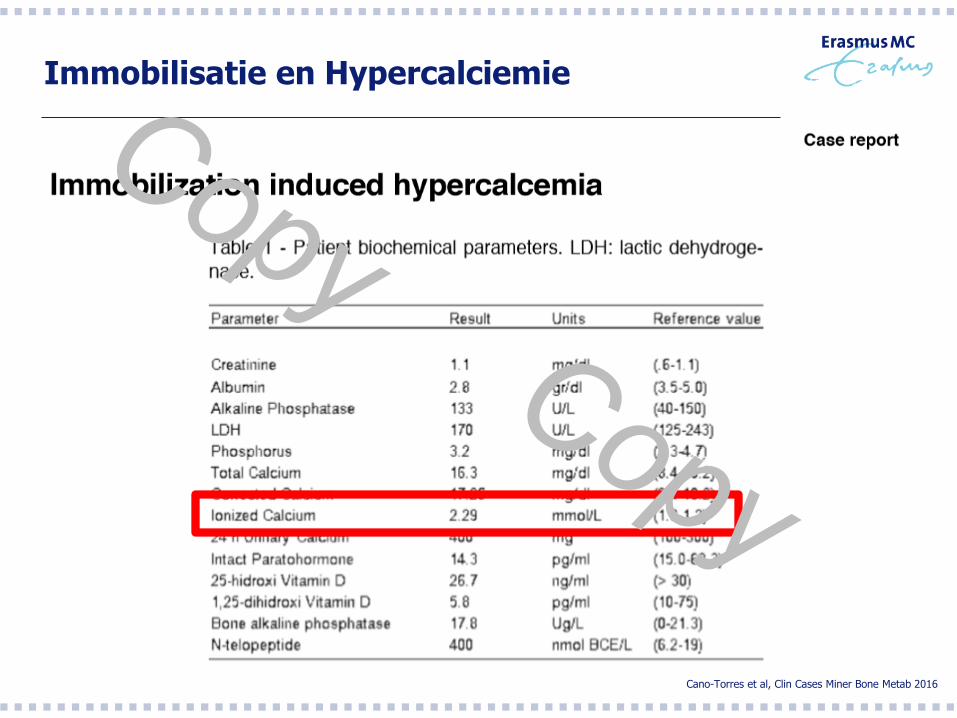
Immobilisatie en Hypercalciemie
Cano-Torres et al, Clin Cases Miner Bone Metab 2016
Dus welke factoren bepalen Alkalose? - Filter karakteristieken -
Het Hemofilter
1/3 van de Citraat oplossing verdwijnt direct in het dialysaat dan
wel ultrafiltraat
Adsorptie eigenschappen van het hemofilter
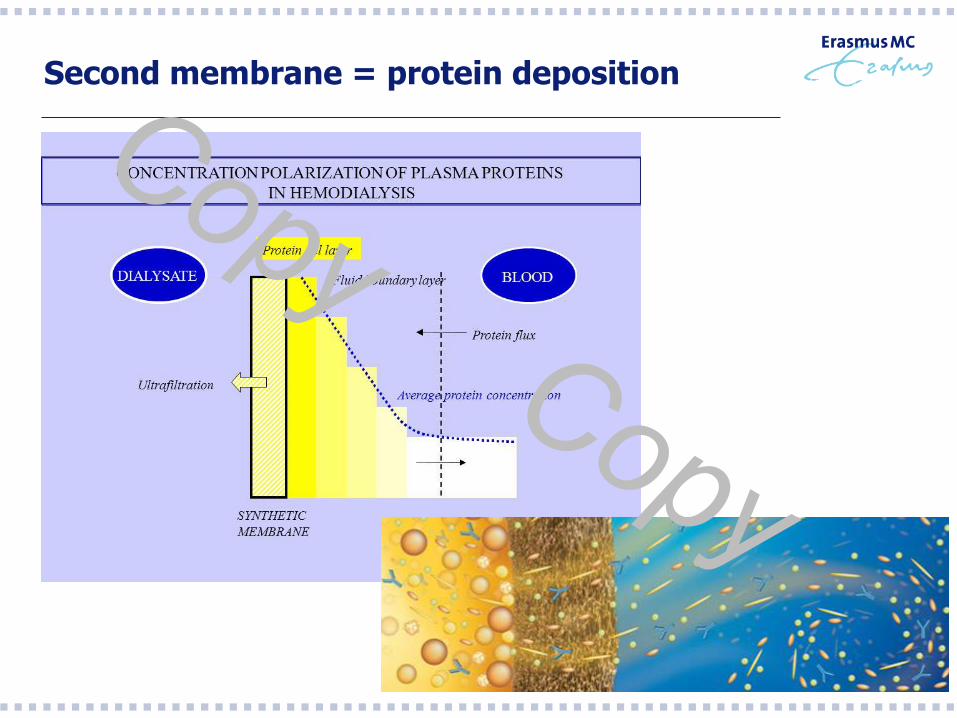
Second membrane = protein deposition
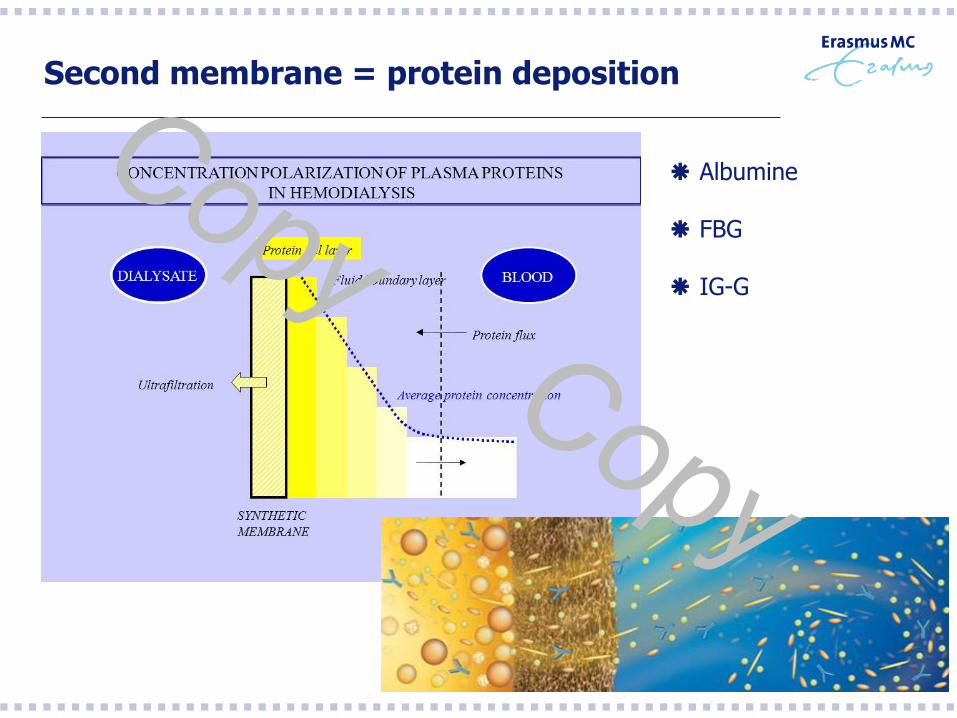
Second membrane = protein deposition
Albumine
FBG
IG-G
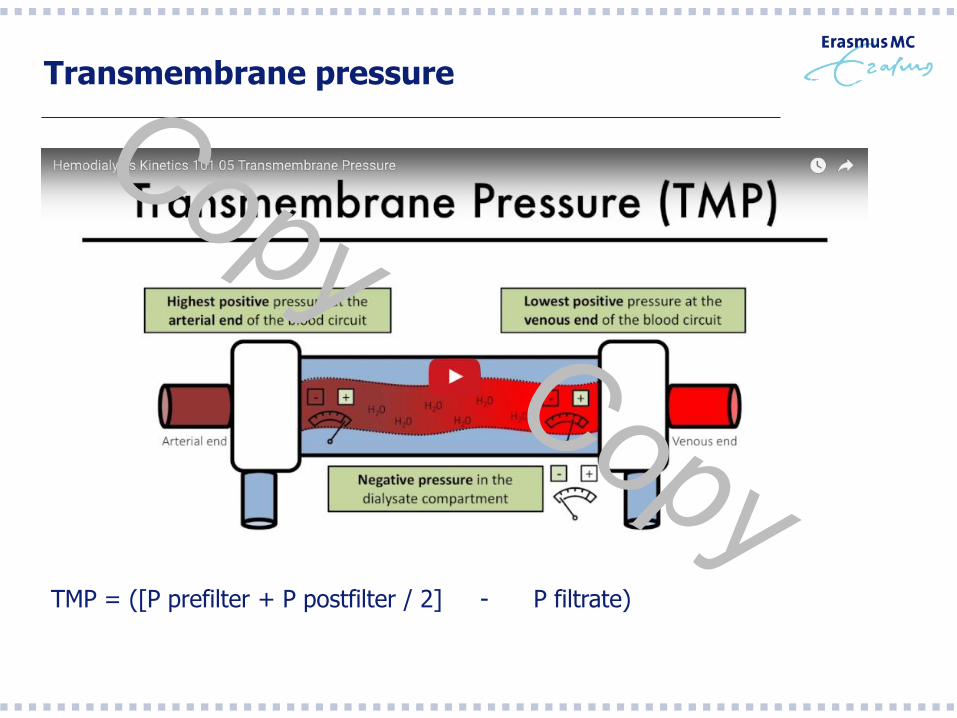
Transmembrane pressure
TMP = ([P prefilter + P postfilter / 2] - P filtrate)
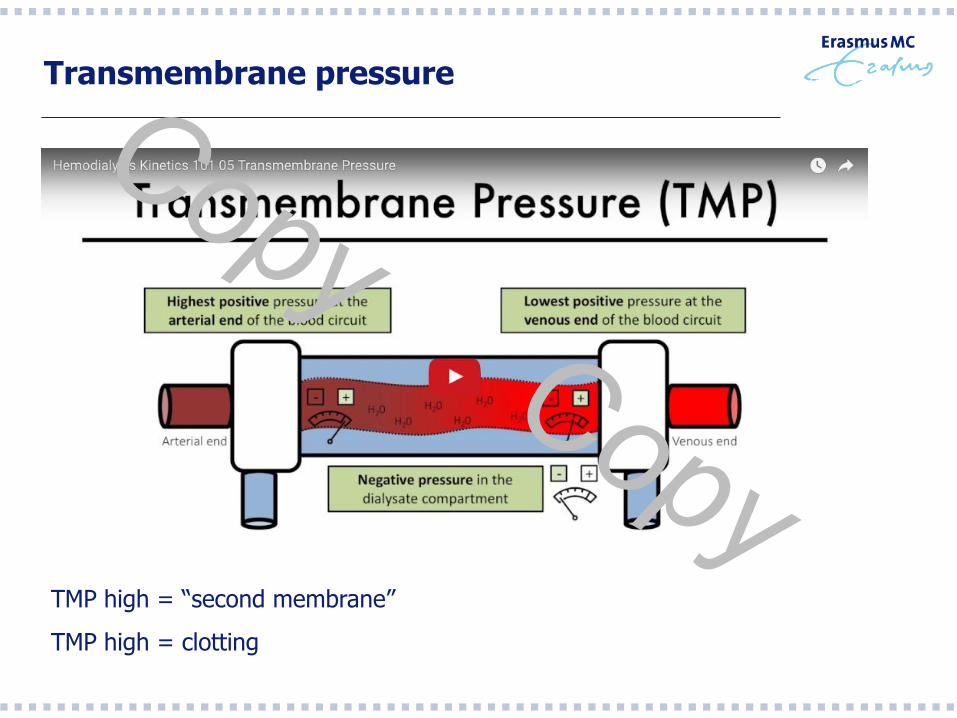
Transmembrane pressure
TMP high = “second membrane”
TMP high = clotting
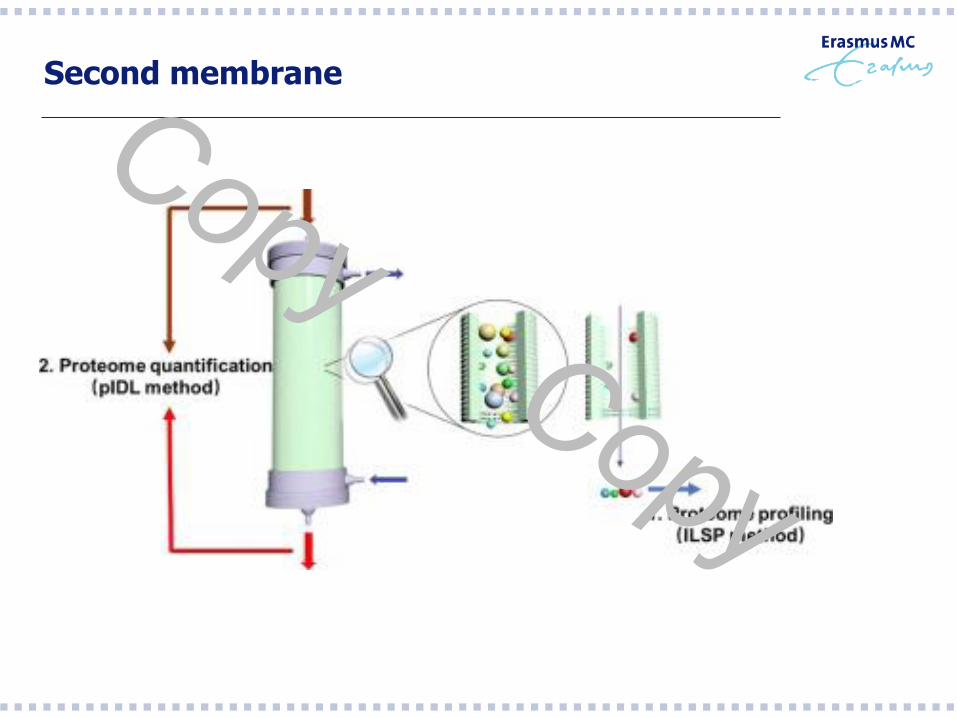
Second membrane
Citraat overload: serieus bussiness? - Metabole Complicaties van Citrate based CRRT -
Alkalose tijdens CiCa CRRT
Klingele et al, Critical Care 2017: 294
Alkalose tijdens CiCa CRRT
Retrospectieve study
2009-2012
Patienten met leverinsufficientie
CiCa CVVHD Fresenius Multifiltrate 4% Citraat oplossing
N=69 patienten
Klingele et al, Critical Care 2017: 294
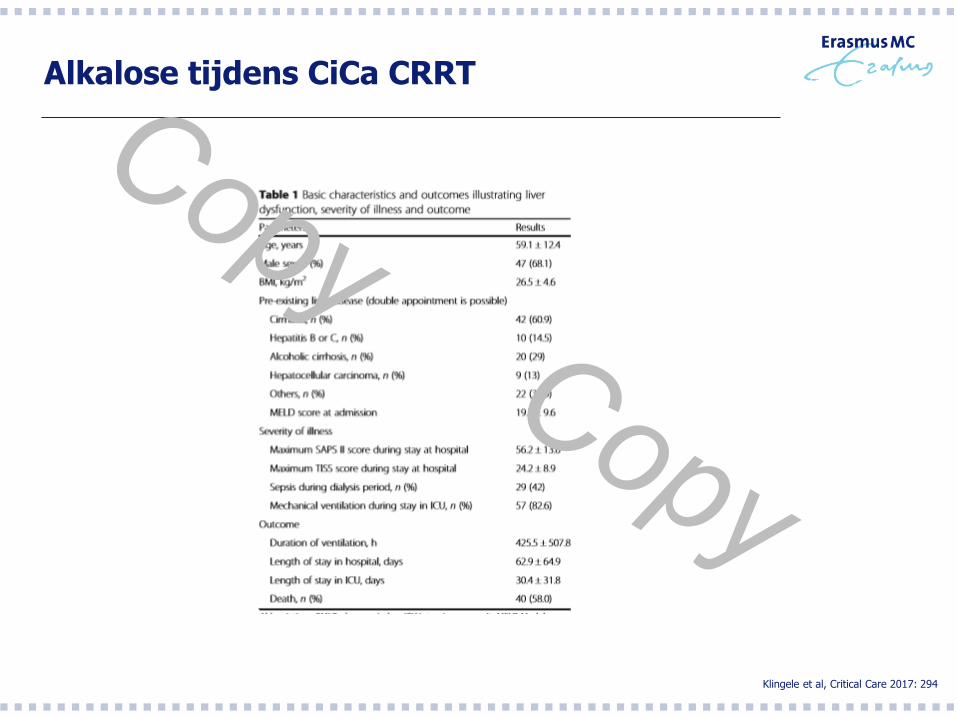
Alkalose tijdens CiCa CRRT
Klingele et al, Critical Care 2017: 294
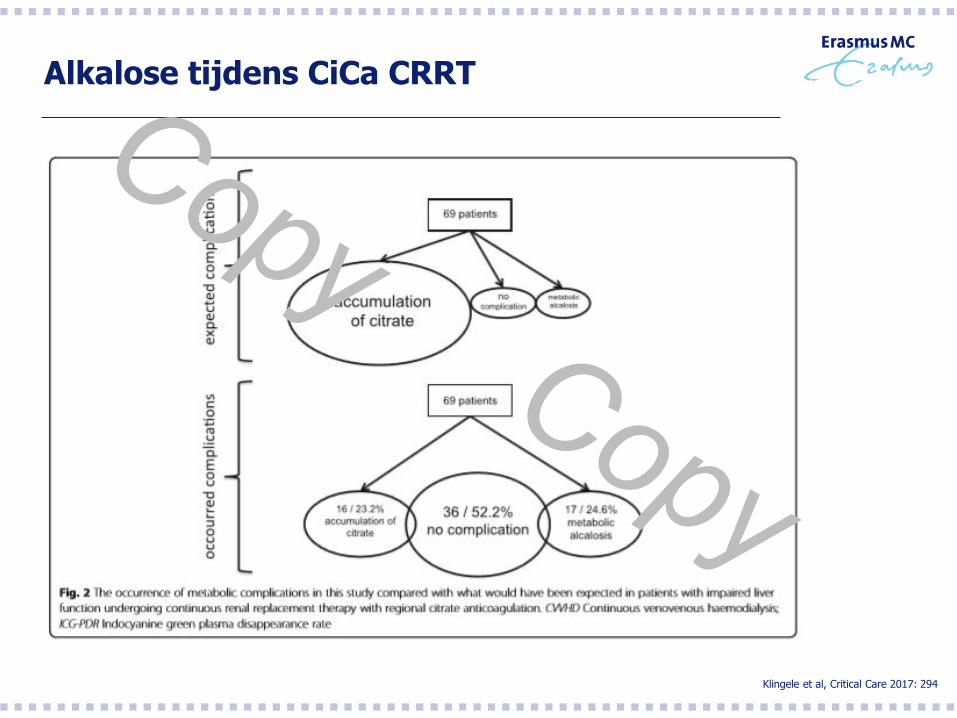
Alkalose tijdens CiCa CRRT
Klingele et al, Critical Care 2017: 294
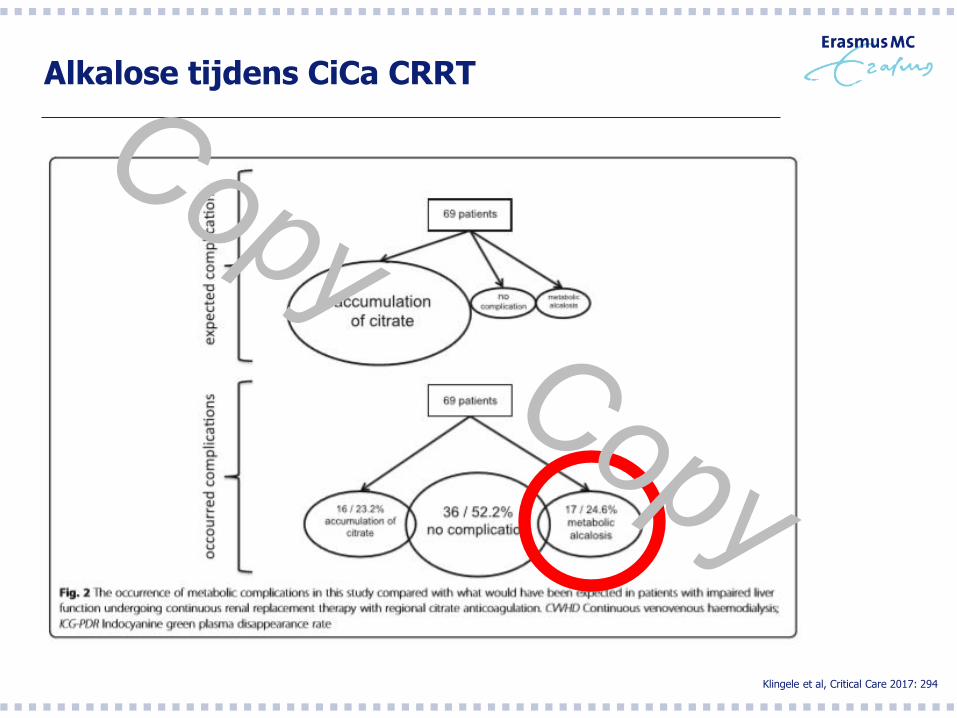
Alkalose tijdens CiCa CRRT
Klingele et al, Critical Care 2017: 294
Citraat overload: serieus bussiness? - Casuïstiek EMC -
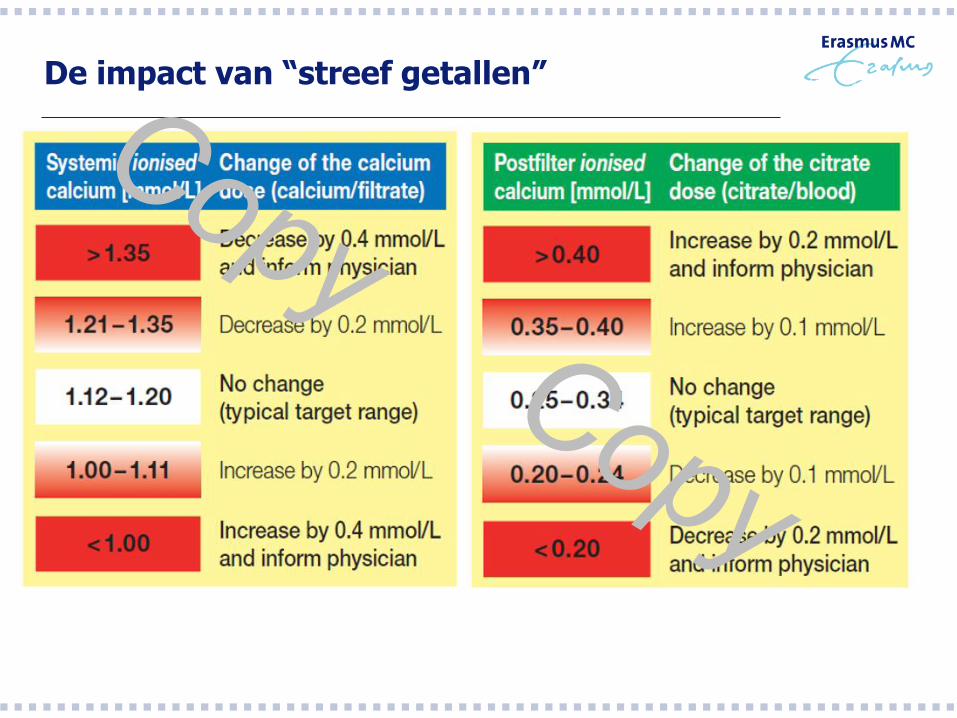
De impact van “streef getallen”
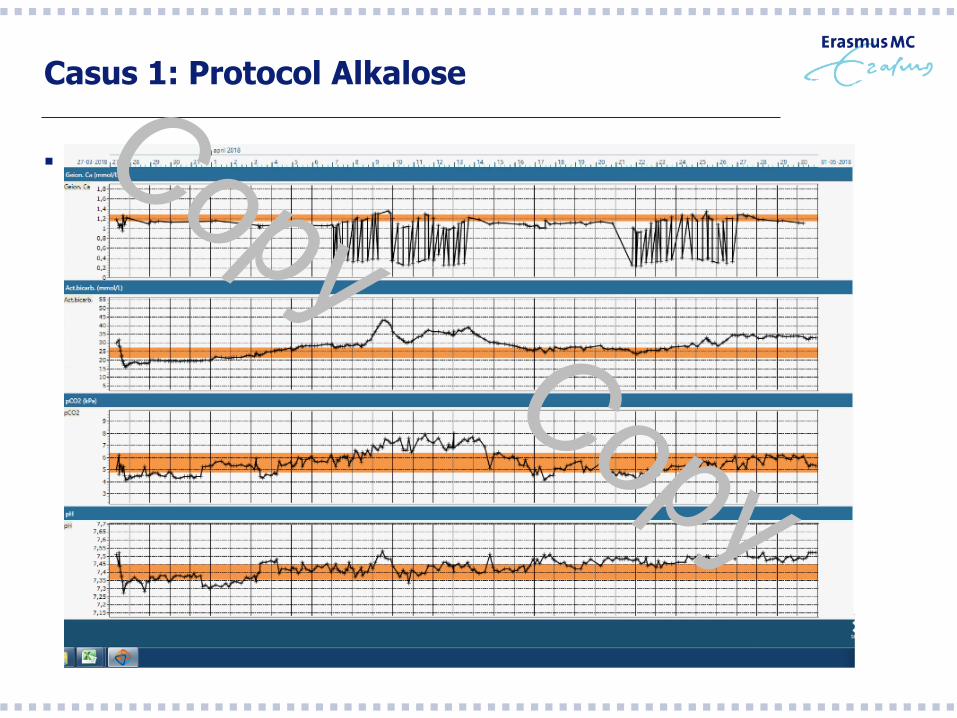
Casus 1: Protocol Alkalose
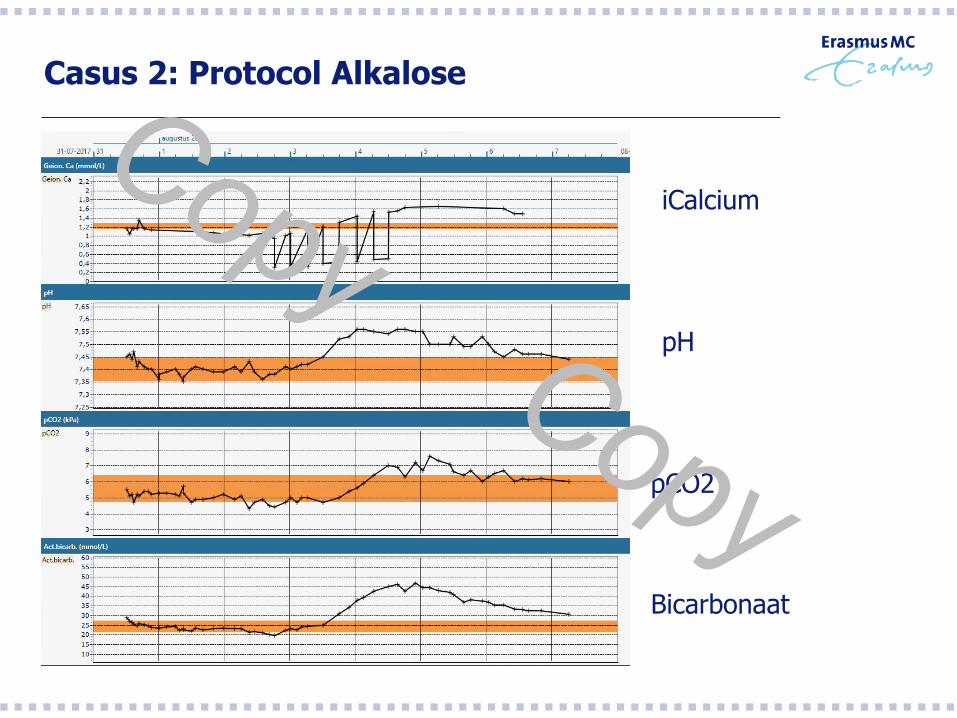
Casus 2: Protocol Alkalose
iCalcium
pH
pCO2
Bicarbonaat
Casus 3: Second Membrane?
Man 73 jaar
Verwezen voor hart ruisje bij screening voor prostaat ok
Electieve TAVI
Gecompliceerd door AKI met anurie, Longembolieën en een shunt tussen LVOT
en RA-RV
ASD werd gesloten met ASD closure device gecompliceerd door
Massale hemolyse, cardiogene shock waarvoor openhart chirurgie
Groot defect in annulus gedicht met een patch, TAVI verwijderd
Gecompliceerd perop door longbloeding en tweede pomp run bij AOI
Re-sternotomie ivm tamponade
Intermitterend 3e graads AV blok
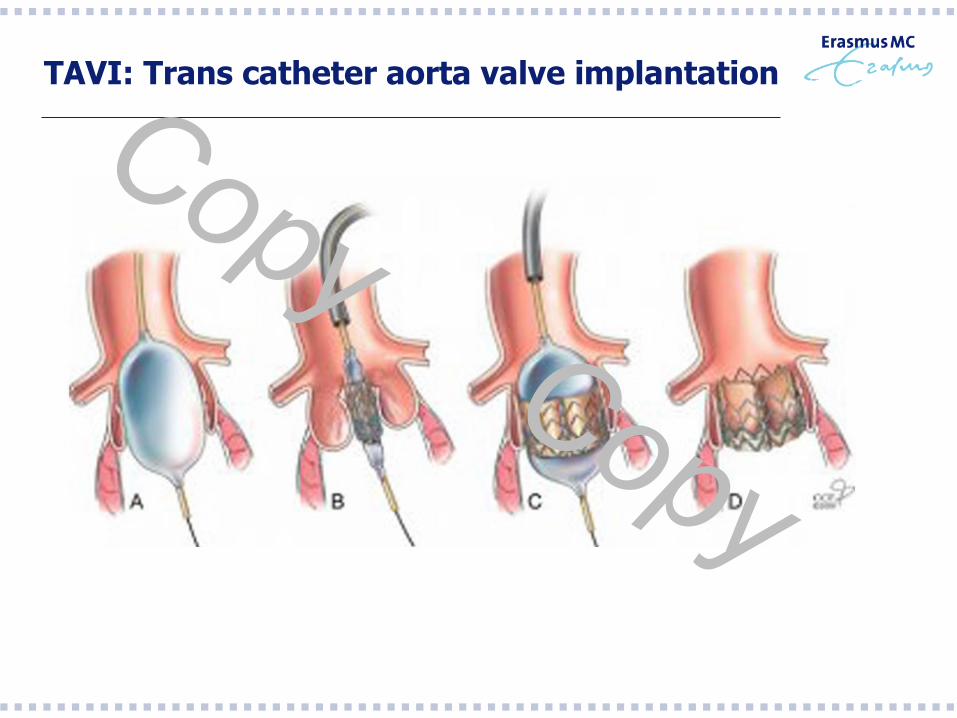
TAVI: Trans catheter aorta valve implantation
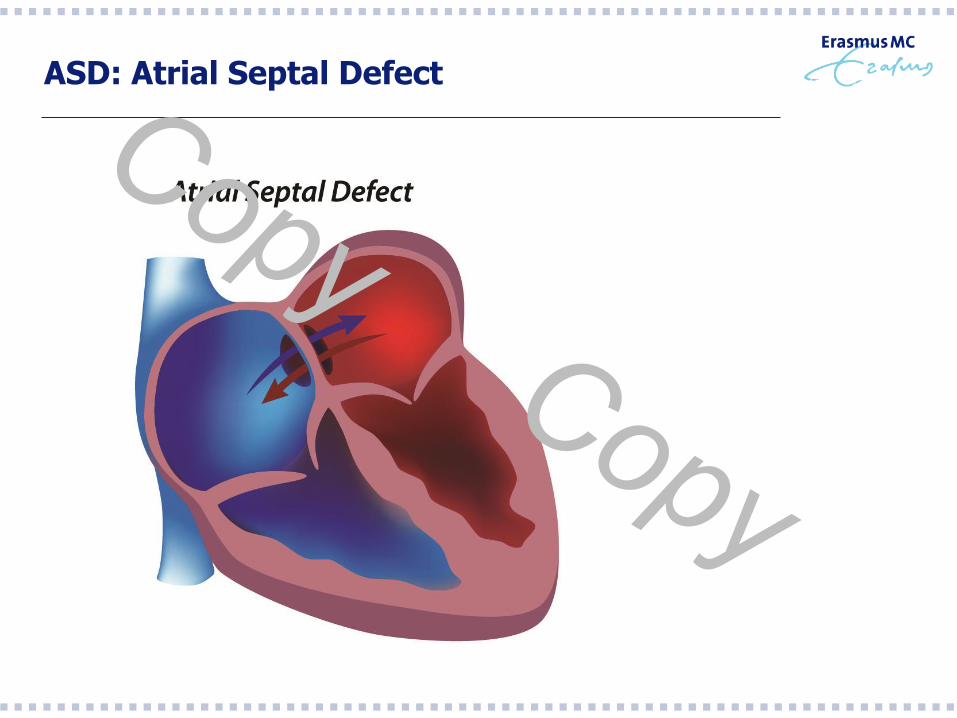
ASD: Atrial Septal Defect
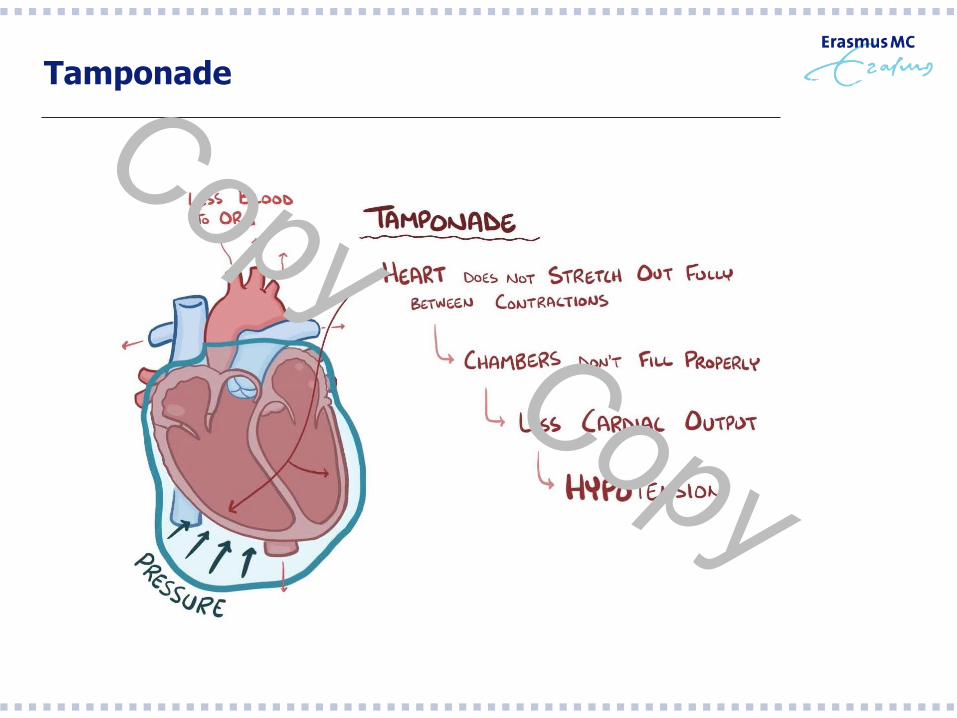
Tamponade
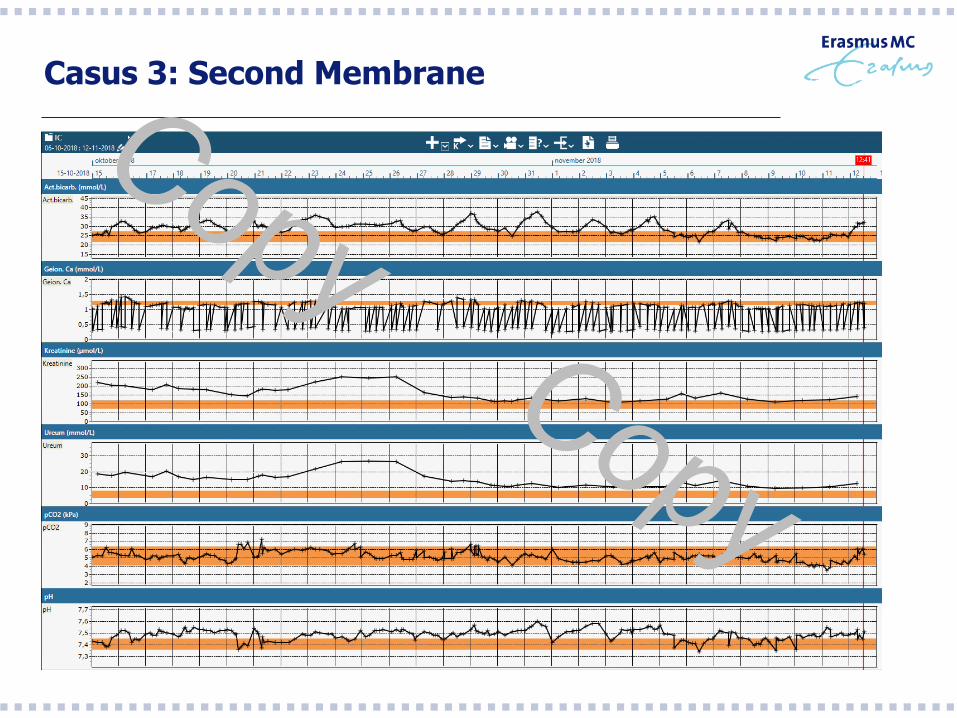
Casus 3: Second Membrane
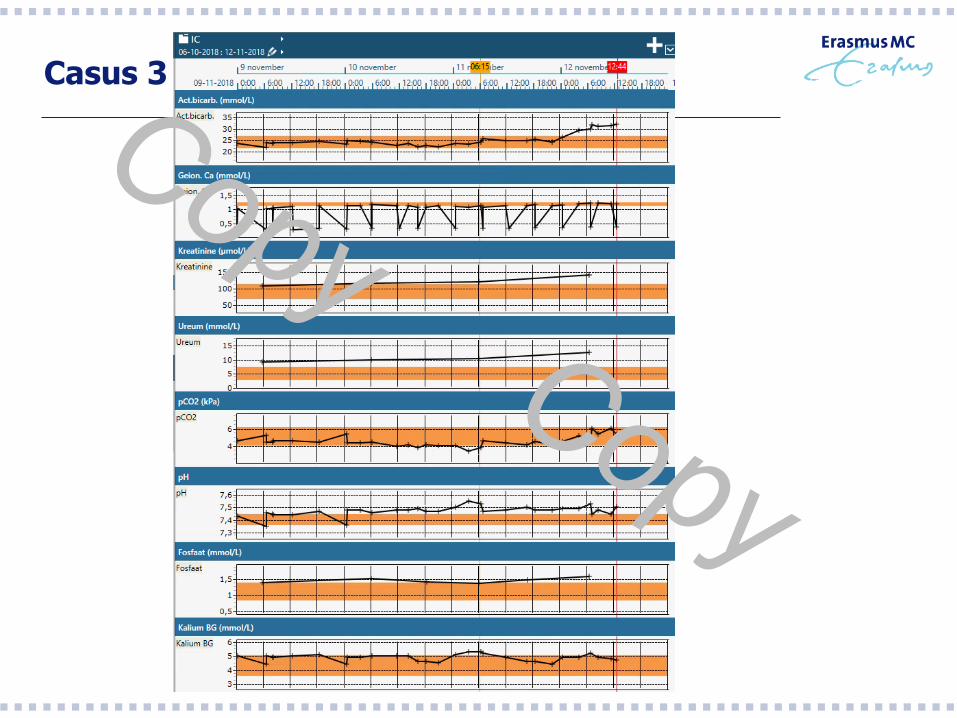
Casus 3
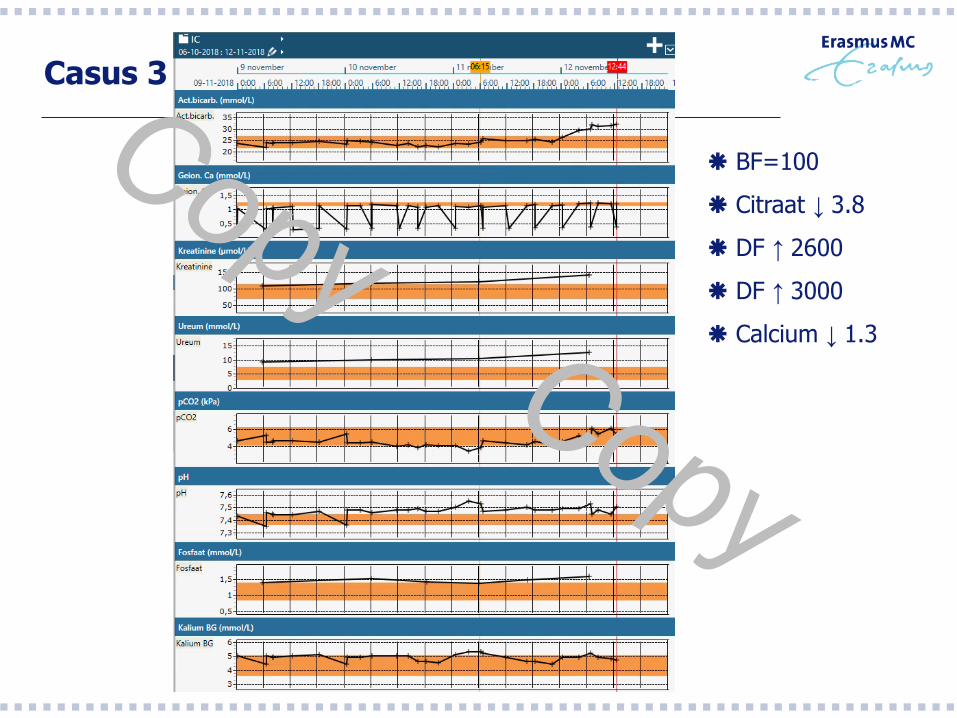
Casus 3
BF=100
Citraat ↓ 3.8
DF ↑ 2600
DF ↑ 3000
Calcium ↓ 1.3
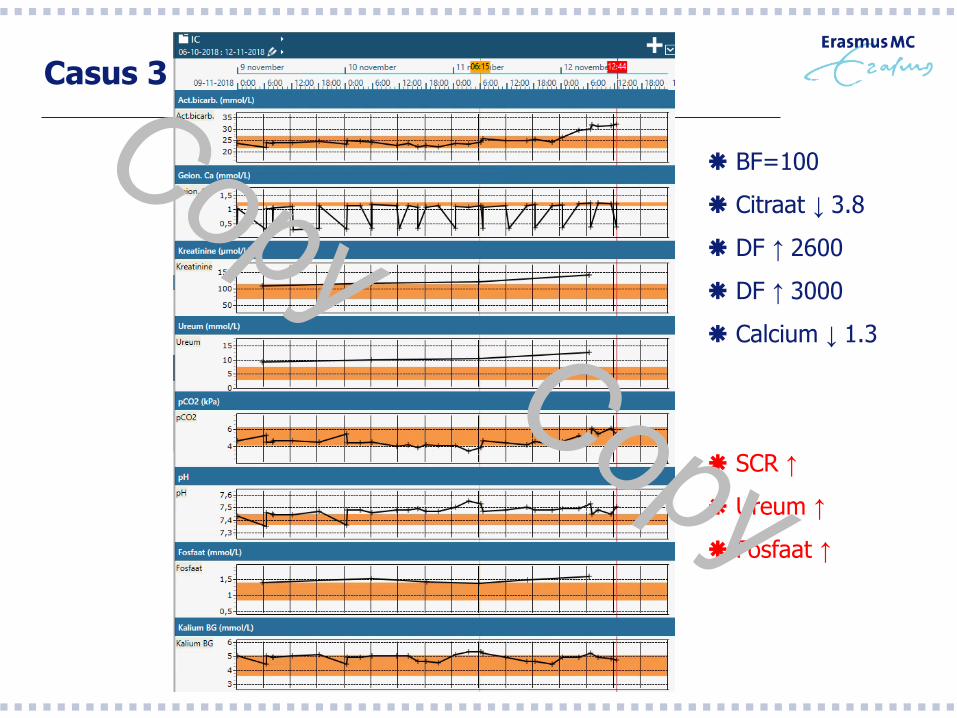
Casus 3
BF=100
Citraat ↓ 3.8
DF ↑ 2600
DF ↑ 3000
Calcium ↓ 1.3
SCR ↑
Ureum ↑
Fosfaat ↑
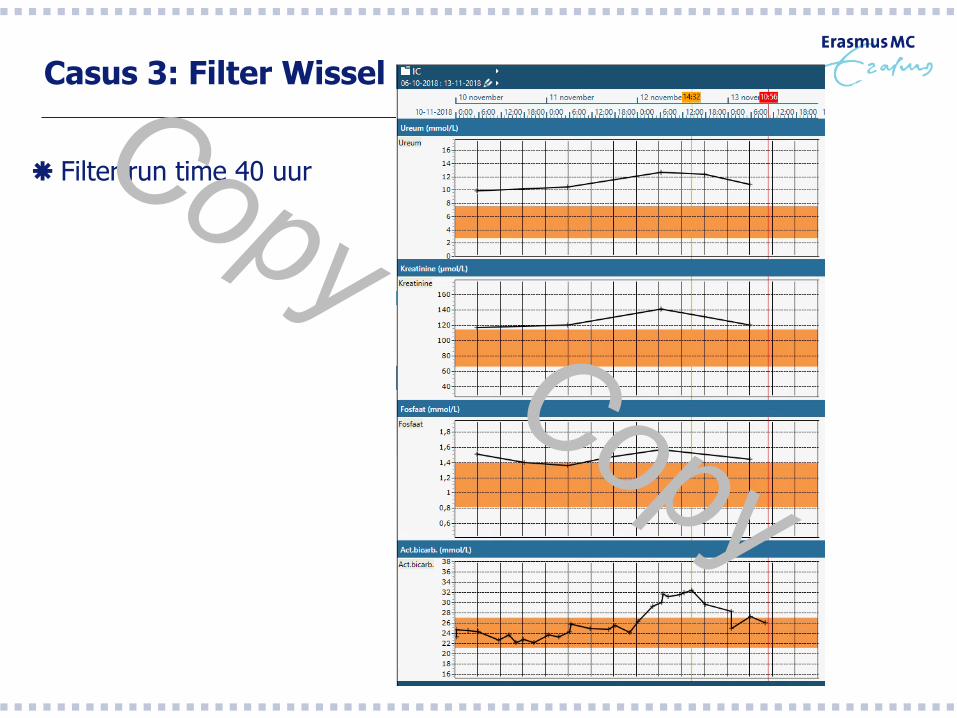
Casus 3: Filter Wissel
Filter run time 40 uur
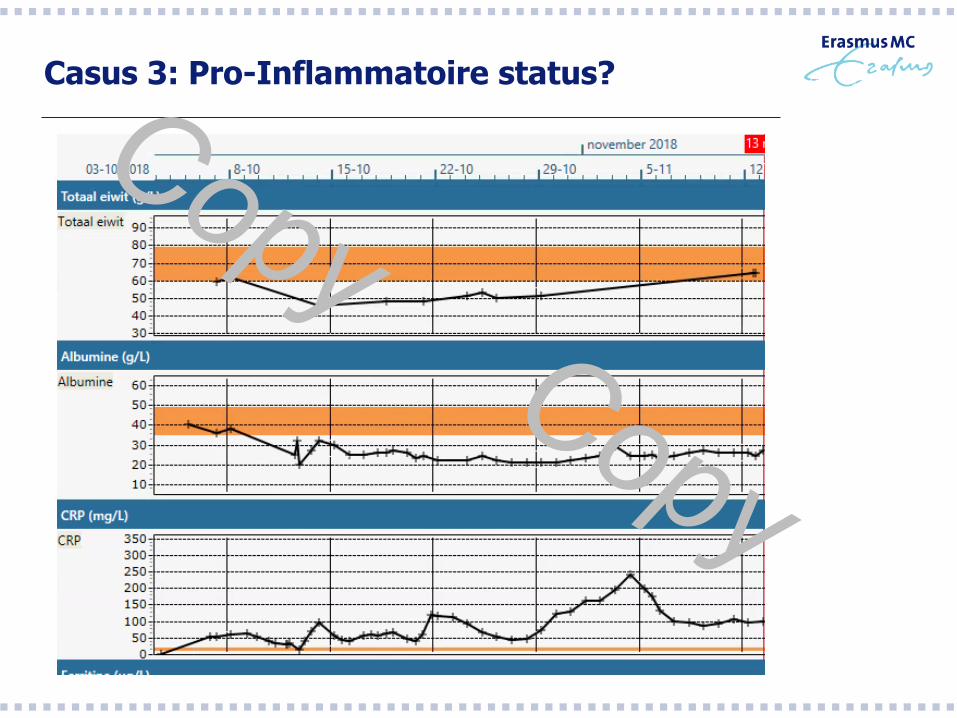
Casus 3: Pro-Inflammatoire status?
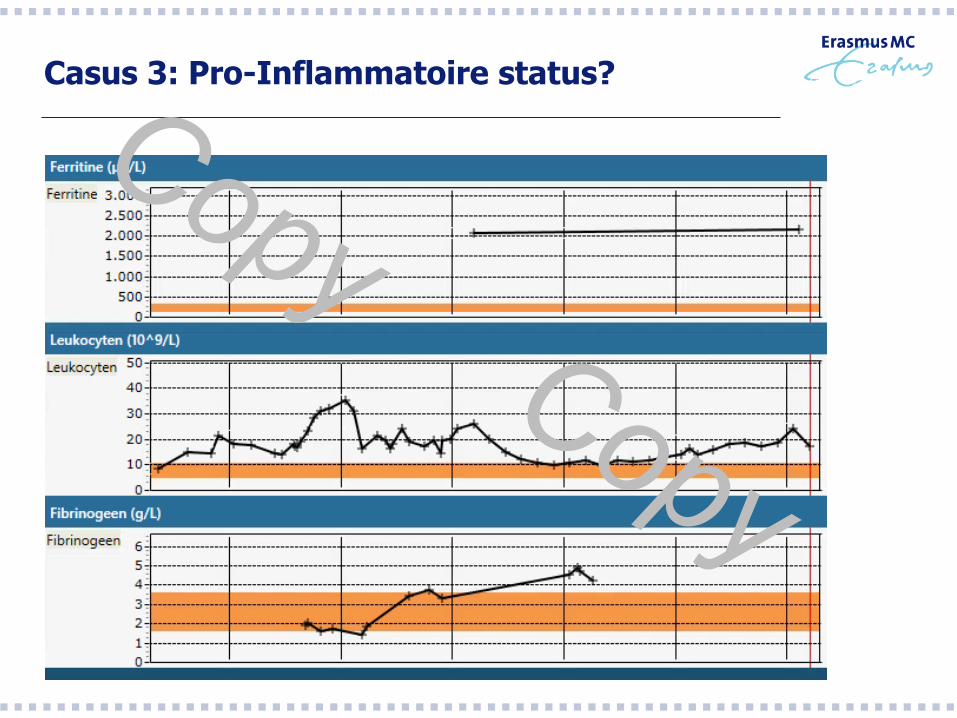
Casus 3: Pro-Inflammatoire status?
Dus welke factoren bepalen Alkalose? - Samenvattend -
Alkalose bij Citraat based CRRT
Machine instellingen Bloedflow bij koppeling citraat pomp
BIC content dialysaat-substitutievloeistof
Streefwaarden Mate van pre-dilutie
Mate van UF (vooral bij hemofiltratie)
Patiënt karakteristieken Calcium metabolisme tijdens ziekte
Cytokine storm eiwitcontent bloed
Filtereigenschappen “Second membrane” vorming
Hoe beïnvloed je Alkalose tijdens CRRT? - Samenvattend -
Alkalose bij Citraat based CRRT
Machine instellingen Bloedflow bij koppeling citraat pomp
BIC content dialysaat-substitutievloeistof
Streefwaarden Mate van pre-dilutie
Mate van UF (vooral bij hemofiltratie)
Patiënt karakteristieken Calcium metabolisme tijdens ziekte
Cytokine storm eiwitcontent bloed
Filtereigenschappen “Second membrane” vorming
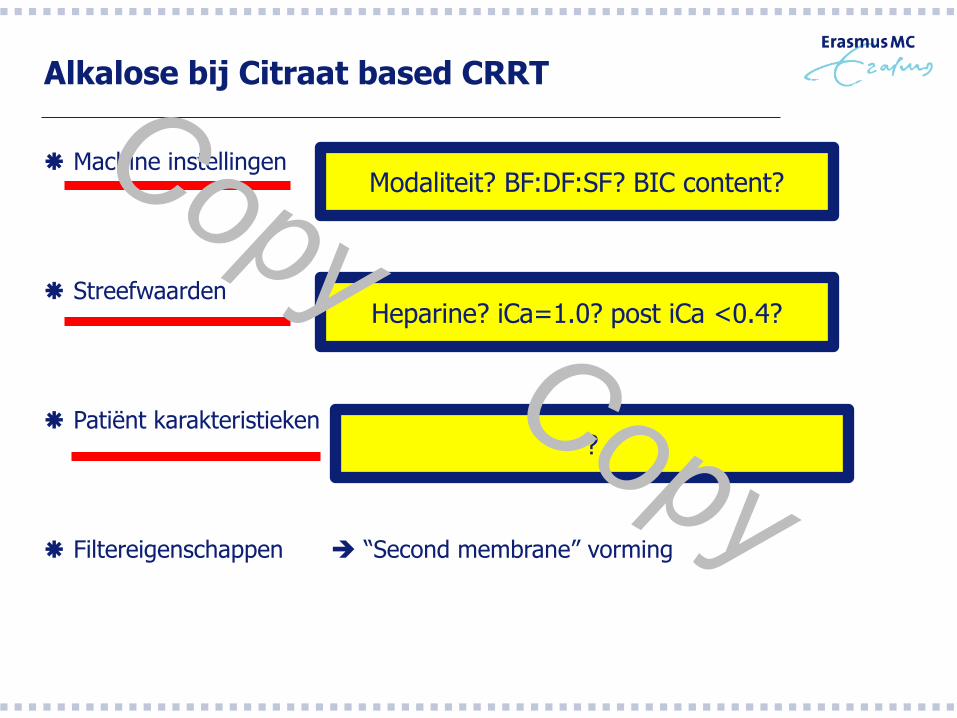
Alkalose bij Citraat based CRRT
Machine instellingen Bloedflow bij koppeling citraat pomp
BIC content dialysaat-substitutievloeistof
Streefwaarden Mate van pre-dilutie
Mate van UF (vooral bij hemofiltratie)
Patiënt karakteristieken Calcium metabolisme tijdens ziekte
Cytokine storm eiwitcontent bloed
Filtereigenschappen “Second membrane” vorming
Modaliteit? BF:DF:SF? BIC content?
Heparine? iCa=1.0? post iCa <0.4?
Alkalose bij Citraat based CRRT
Machine instellingen Bloedflow bij koppeling citraat pomp
BIC content dialysaat-substitutievloeistof
Streefwaarden Mate van pre-dilutie
Mate van UF (vooral bij hemofiltratie)
Patiënt karakteristieken Calcium metabolisme tijdens ziekte
Cytokine storm eiwitcontent bloed
Filtereigenschappen “Second membrane” vorming
Modaliteit? BF:DF:SF? BIC content?
Heparine? iCa=1.0? post iCa <0.4?
?
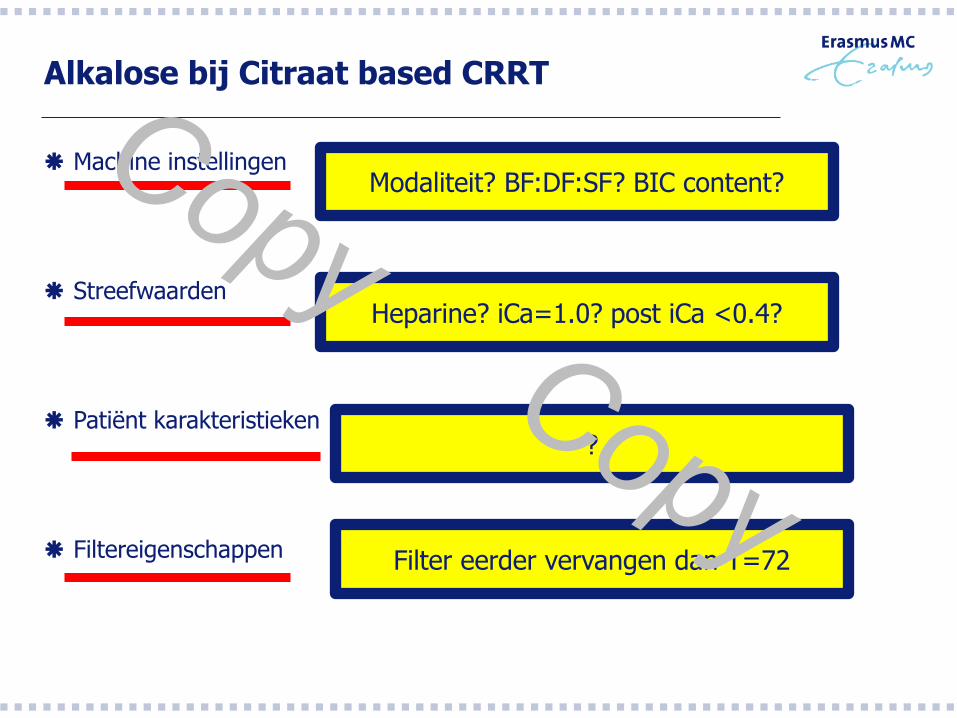
Alkalose bij Citraat based CRRT
Machine instellingen Bloedflow bij koppeling citraat pomp
BIC content dialysaat-substitutievloeistof
Streefwaarden Mate van pre-dilutie
Mate van UF (vooral bij hemofiltratie)
Patiënt karakteristieken Calcium metabolisme tijdens ziekte
Cytokine storm eiwitcontent bloed
Filtereigenschappen “Second membrane” vorming
Modaliteit? BF:DF:SF? BIC content?
Heparine? iCa=1.0? post iCa <0.4?
?
Filter eerder vervangen dan T=72
Alkalose tijdens CRRT EMC protocol
- Protocol behandelalgoritme -
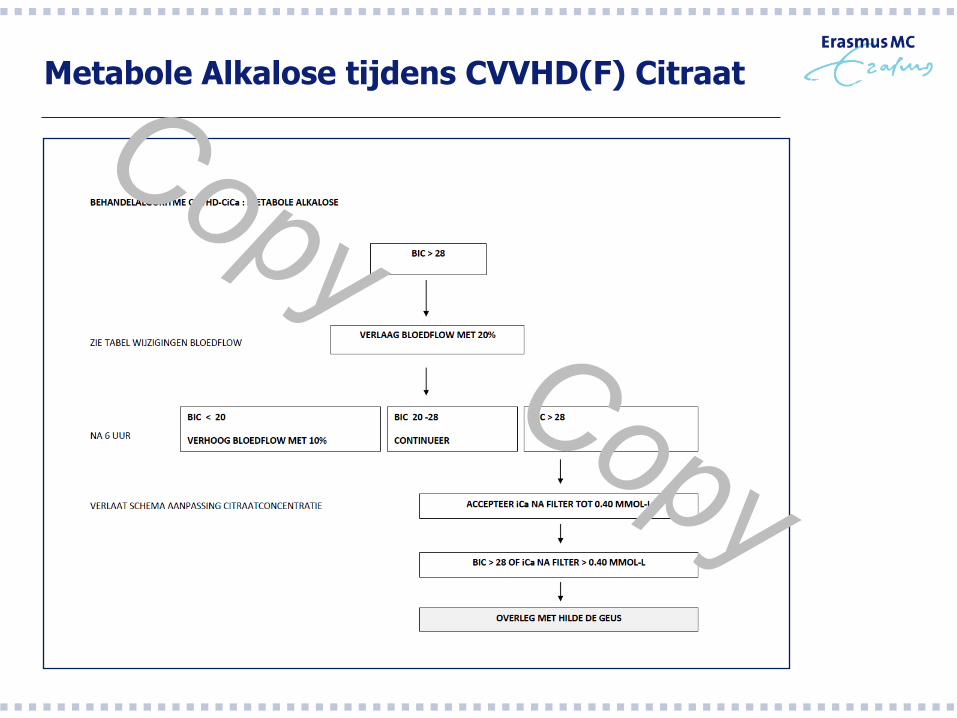
Metabole Alkalose tijdens CVVHD(F) Citraat
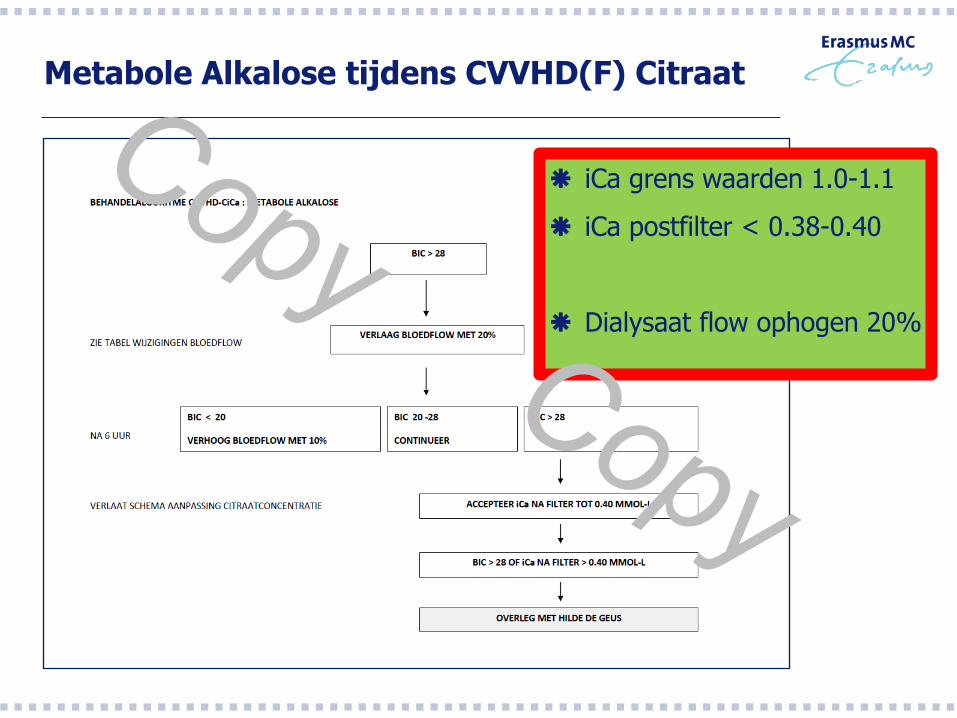
Metabole Alkalose tijdens CVVHD(F) Citraat
iCa grens waarden 1.0-1.1
iCa postfilter < 0.38-0.40
Dialysaat flow ophogen 20%
Is er een oplossing voor Casus 3?

Vragen… ?
Hilde de Geus, MD, PhD
Internist-Intensivist Erasmus MC Rotterdam
Aandachtsgebied: Nefrologie