Medicine - CCMS Homepage€¦ · Mahmoud K. Effat, MD Heidar K. Jahromi, MD John P. Maher, MD...
32
YOUR COMMUNITY RESOURCE FOR WHAT’S HAPPENING IN HEALTH CARE CHESTER COUNTY Medicine Published by Pennsylvania’s First Medical Society SUMMER 2016 SPRINTING TOWARDS IMPROVED HEALTH... ...THROUGH INTENSIVE BLOOD PRESSURE CONTROL Chester County The Art of
Transcript of Medicine - CCMS Homepage€¦ · Mahmoud K. Effat, MD Heidar K. Jahromi, MD John P. Maher, MD...

Y O U R C O M M U N I T Y R E S O U R C E F O R W H A T ’ S H A P P E N I N G I N H E A L T H C A R E
CHESTER COUNTYMedicineP u b l i s h e d b y P e n n s y l v a n i a ’ s F i r s t M e d i c a l S o c i e t y
SUMMER 2016
SPRINTING TOWARDSIMPROVED HEALTH......THROUGH INTENSIVE BLOOD PRESSURE CONTROL
Chester CountyThe Art of
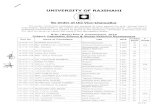
What is a Quality Colonoscopy? Not all colonoscopies are alike! Studies show a marked difference in colorectal cancer (CRC)
risk reduction between facilities and physicians
What are the most important factors for a high quality colonoscopy? *ASGE guidelines
Cecal intubation rate with photo documentation, i.e. How often do we make it to the end?
o Benchmark: >90%
o West Chester Gastrointestinal Group (WCGG): 99%
Proper use of recommended intervals between colonoscopies performed for average-‐risk patients and
for colon polyp surveillance.
o WCGG has a robust, blinded, quarterly evaluation of representative pathology for each physician to ensure proper surveillance. Our CMS QualityNet Data shows compliance in excess of 98%.
Adenoma Detection Rate or ADR, the most important measure of a quality colonoscopy (i.e. how
often do we detect a pre-‐cancerous polyp in the colon and remove it?)
o Benchmark by ASGE/AGA: ADR target of 30% is recommended for men and 20% for women.
WEST CHESTER ● EXTON ● KENNETT SQUARE ● WEST GROVE www.westchestergi.com (610) 431-‐3122
For every 1% increase in ADR, there was a 3% reduction in CRC incidence and 5% reduction in cancer mortality. Higher ADRs were associated with lower risk of cancer in both men and women.
Corley, D et al, Adenoma Detection Rate and Risk of Colorectal Cancer and Death, NEJM, 2014; 370:1298-‐306.
Source: GIQuIC, a CMS approved Qualified Clinical Data Registry (QCDR)

BRIGHTER DAYSARE HERE
EYE CAREC H E S T E R C O U N T Y
(610) 696-1230 | CHESTERCOUNTYEYECARE.COM | WEST CHESTER | EXTON | WEST GROVE
Cataracts cloud your vision causing everything in sight to appear dull and faded. Brighten up your life again with advanced cataract surgery performedby our trusted surgeons.
SCHEDULE YOUR CATARACT EVALUATION TODAY!

12
SPRINTING TOWARDSIMPROVED HEALTH......THROUGH INTENSIVE BLOOD PRESSURE CONTROL
Chester County Medicine is a publication of the Chester County Medical Society (CCMS). The Chester County Medical Society’s mission has evolved to represent and serve all physicians of Chester County and their patients in order to preserve the doctor-patient relationship, maintain safe and quality care, advance the practice of medicine and enhance the role of
medicine and health care within the community, Chester County and Pennsylvania.
The opinions expressed in these pages are those of the individual authors and not necessarily those of the Chester County
Medical Society. The ad material is for the information and consideration of the reader. It
does not necessarily represent an endorsement or recommendation by the Chester County
Medical Society.
Chester County Medicine ispublished by
Hoffmann Publishing Group, Inc.,Reading PA 19608
HoffmannPublishing.com For advertising information,
contact Karen Zach610.685.0914
2013-2016CCMS OFFICERS
PresidentWinslow W. Murdoch, MD
President-ElectMian A. Jan, MD, FACC
Vice PresidentBruce A. Colley, DO
SecretaryDavid E. Bobman, MD
TreasurerLiza P. Jodry, MD
Board MembersMahmoud K. Effat, MD
Heidar K. Jahromi, MD
John P. Maher, MD
Charles P. McClure, MD
David A. McKeighan
Executive Director Rosemary McNeal
Administrative Assistant CCMS Headquarters
(610) 827-1543
Chester County Medicine is published by Hoffmann Publishing Group, Inc. Reading, PA I HoffmannPublishing.com I 610.685.0914 I for advertising information: [email protected]
Contents
Letters to the Editor: If you would like to respond to an item you read in Chester County Medicine, or suggest additional content, please submit a message to [email protected] with “Letter to the Editor” as the subject. Your message will be read and considered by the editor, and may appear in a future issue of the magazine.
Cover: “A Tuscan Village” by Judy Antonelli Klanderman
S U M M E R 2 0 1 6
8
In Every Issue6 President’s Message16 The Art of Chester County
Features15 Confronting A Crisis: An open letter to America’s Physicians on the Opioid Epidemic20 Pennsylvania Delegation Advocates to End Mandatory, Secured Recertifying MOC Exams22 William Darlington23 Chester County Medical Society Annual Legislative Clam Bake24 Opioids For Pain: Be Smart. Be Safe. Be Sure.26 Are You Ordering, Prescribing, or Referring for MA Beneficiaries?27 Save the Date: Oct. 21: Paoli Hospital Auxiliary’s Fall Fine Art Show and Cocktail Party28 ZIKA Virus Disease: Are We Prepared?30 NIH Launches Moms’ Mental Health Matters30 Consider Membership in The Chester County Medical Society
Cardio-Renal Syndrome A Complex, Difficult to
Manage Condition
16Judy Antonelli KlandermanA Chester County Gem
8
Disruptive Innovation
Disruptive Innovation – an innovation that creates a new market and value network and eventually disrupts an existing market and value network, displacing
established market leaders and alliances. (Clay Christensen, 1995) As anyone reading this article knows, the healthcare system is ready for disruption. As a primary care physician’s wife, I have been watching attempts at riding the healthcare disruption wave since my husband, Winslow started practice in the late 1980s. DRGs, HMOs, and all of the 3 letter acronyms that followed promised positive change but put fear in the hearts of participants in the system on the verge of disruption. There are unique characteristics of many physicians I have known over the years, as I’ve been tangentially in the business since my husband was in medical school. Their hearts are good. First and foremost they want the best for their patients and healthy outcomes are more important than incomes. They are also implicitly risk adverse – which carries through to business decisions. They often like the idea of change, but not change itself. But now there will be no choice, and it is realized. Fear is thick, though in many cases physicians are just too busy to do
6 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
President’s Message
anything about it. The patient comes first, and there are so many of them. Reimbursements low, patient volume increasing, our population aging and more needy – when can they find time to investigate options for positive change, or research what may be happening around them in the realm of disruptive innovation? Let’s understand disruptive change. Industries change for different reasons. Sometimes the cause is crises (i.e. the financial markets). Sometimes competitive dynamics produce big changes in the landscape over time – think about how the Japanese auto industry gained market share in the U.S. Sometimes there is a distinct catalyst – digitation of content and the iPod, for example. Digital files of music changed the music industry and the iPhone and its applications changed handsets, demonstrating the power of creative destruction. Film was disrupted with digital cameras, legacy software was displaced with software in the cloud – the list goes on. Think about it. Kodak. Pontiac. The healthcare industry’s disruption is taking place at a time when the overall pace of change in the economy continues to increase. The odds that an industry leader will lose its position within 5 years has tripled in the past 25 years. So, though as physicians and people in the healthcare industry tend to feel singled out, there are few industries that have not been disrupted. There are few industries without layers of regulatory hoops to jump through. Rather than be fearful, we all need to embrace ambiguity. Much more easily said than done, but with ambiguity comes opportunity. What will that opportunity be? We don’t know. Most likely it will be an entire new ecosystem of healthcare, with opportunities for all of us. What can we say about people who seem to be “lucky”? Personally I believe we need to be tuned in to be able to seize an opportunity when it comes along. You need to see the good fortune when it is presented. Pushing back and trying to make the same square peg fit in a round hole leads to frustration, and I’ve seen so much of it. How can we do exactly what we are doing by tweaking our existing model? It won’t work. Disruptive change is not a tweak. It is an LP recording to a digital music file, it is a film to digital photos, landlines to personal cell phones. That is what is
BY DR. DONNA MURDOCH

going on – and as physicians (and those who love them), we need to keep our eyes and hearts open during this time of ambiguity. Opportunity will come your way if you let it. People will always want relationships. People will always value the verbal (or video) assurance of a trusted physician. It is doubtful that part will change for a long time, especially as our population continues to age. But – and this is not easy – try to be open to true innovation. You will see it. Someone will approach you with it. Your automatic reflex might be to say no, it won’t work. In your day to day life you are probably right, it wouldn’t within your present context. But perhaps a new way of working will be better. There are no promises, and no assurances. The only thing we can know for sure is that continuing to try to push the square peg in the round hole will be increasingly painful – so let’s (self included) keep our eyes on the horizon. As I conclude this letter, Winslow (current President of the Chester County Medical Society) is telling me that this is his parting President’s letter. I am honored he offered this space to me. He has been through many trials, tribulations, and changes throughout his 27 years in practice but one thing has remained
the same. His patients have always come first. I am always in awe, but not surprised. At times when he has considered giving up on medicine, I’ve reminded him – you ARE Dr. Murdoch. What else would you do? To be born with a distinct calling, with a gift to help and heal – that is special. I am in awe of all of you who were given that same gift. So please be a part of something new and innovative rather than fight it. It may be just what you need to continue to do what you do best.
Warmest Regards to All,
Donna Murdoch, EdD Adjunct ProfessorUniversity of Pennsylvania Graduate School of EducationColumbia University Teachers College
S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 7
w w w . C H E S T E R C M S . o r g
Winslow W. Murdoch, MD, practices family medicine in West Chester. He is president of the Chester County Medical Society. Contact Dr. Murdoch at [email protected].
Now is the timeto jumpstart your health & wellness.
Live your best. I acac.com
expert support intro to group exercisefull access to fitness center
Award-winning p.r.e.p.® is a great way to try acac Fitness & Wellness.
Don’t stall - visit or contact us today to get started.
acac West Chester1130 McDermott DriveWest Chester, PA 19380610.431.7000
acac Eagleview699 Rice Blvd, Suite 100Exton, PA 19341610.425.3188
BY DR. DONNA MURDOCH

Cardio-Renal SyndromeA Complex, Difficult to Manage Condition
BY MIAN A. JAN, M.D.AMBEREEN M. JAN, M.D.
8 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
The pyramid in figure 9 is an excellent
representation of how CRS progresses
and how in each step we can modify the risks and
institute treatment. At the bottom of the pyramid are patients
who do not have CRS but are at high risk and this is similar for
both the kidney and heart. Diabetes, hypertension, smoking,
and high cholesterol are primary targets. Proteinurea in kidneys
and LVH and beginning of atherosclerosis in the heart are the
initiating phases and should be managed aggressively with life
style modifications and drug therapy to prevent patients from
progressing to the end stage where prognosis becomes grave
and therapeutic options limited.
Part 2
REDUCING RISKS OF CRS
Figure 9
End- stage
Progression
Stages of
Chronic KidneyDisease
Kidney Failure (ESRD)
Decreased GFR
Age, DM, HBP, Family
History
Age, DM, HBP, Family
History
CardiovascularDisease
Heart Failure
CVD Events
CAD, LVHDamage(Proteinuria) Imitation
At increased risk
S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 9
w w w . C H E S T E R C M S . o r g
Continued on page 10
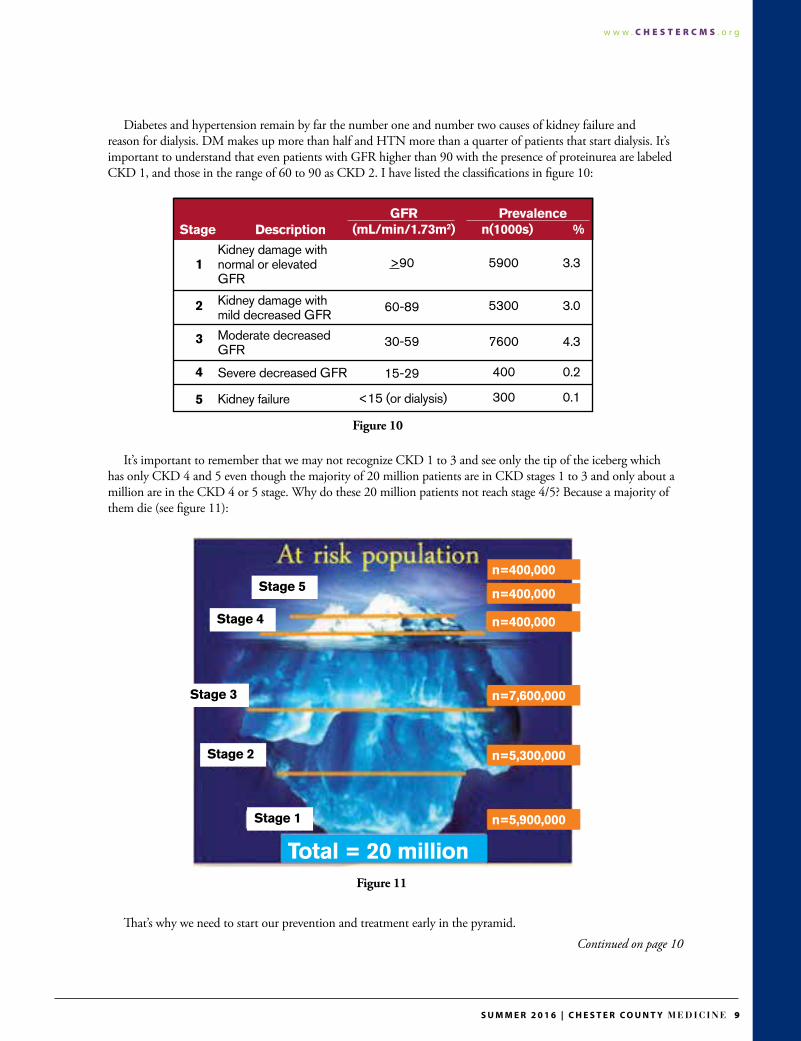
Diabetes and hypertension remain by far the number one and number two causes of kidney failure and reason for dialysis. DM makes up more than half and HTN more than a quarter of patients that start dialysis. It’s important to understand that even patients with GFR higher than 90 with the presence of proteinurea are labeled CKD 1, and those in the range of 60 to 90 as CKD 2. I have listed the classifications in figure 10:
It’s important to remember that we may not recognize CKD 1 to 3 and see only the tip of the iceberg which has only CKD 4 and 5 even though the majority of 20 million patients are in CKD stages 1 to 3 and only about a million are in the CKD 4 or 5 stage. Why do these 20 million patients not reach stage 4/5? Because a majority of them die (see figure 11):
That’s why we need to start our prevention and treatment early in the pyramid.
Figure 10
Figure 11
Stage
1Kidney damage withnormal or elevatedGFR
>90 5900 3.3
5300 3.0
7600 4.3
400 0.2
300 0.1
60-89
30-59
15-29
<15 (or dialysis)
Kidney damage with mild decreased GFR
Moderate decreased GFR
Severe decreased GFR
Kidney failure
2
3
4
5
DescriptionGFR
(mL/min/1.73m2)Prevalence
n(1000s) %
Stage 5n=400,000
n=400,000
n=7,600,000
n=5,300,000
n=5,900,000
Total = 20 million
n=400,000Stage 4
Stage 3
Stage 2
Stage 1

10 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
MARKERS FOR CRS
*B-Type Natriuretic peptide Meta-analysis of BNP guided therapy showed reduction in all-cause mortality (see figure 12). Most physicians feel that since BNP is elevated in renal failure it is not a good marker but as you can see in figure 13, rarely is BNP higher than 300 in pure renal failure; only when accompanied by CHF does that number climb up and is a good guide for management.
*Copeptin
Copeptin is C-terminal pro-vasopressin and is very stable in serum thus easily measured. Data shows it’s a better predictor of mortality and morbidity in patients with CHF post MI. Can levels guide therapy? The data is still murky and needs further testing.
*Cystatin C Cystatin is a Cystein protease inhibitor and measures renal function better than Creatinin, correllates well with BNP and can give complimentary information. Data reveals that even a rise of .3mg/l increases mortality and morbidity and decreases survival. When Creatinin rises .2mg/dl and Cystatin .3mg/l 90-day mortality increases to 44.8%.
MANAGEMENT
*Risk Modification We have already talked about risk factor modification, I have listed these in figure 14. To slow the progression of kidney disease, keep BP under 130 systolic (although the recent SPRINT trial has shown BP under 120 systolic reduces future events), keep HgAiC under 7, preferably under 6.5, and keep hemoglobin in good range. Avoid nephrotoxins such as contrast agents, aminoglycosides and NSAIDs.
*Diuretics
Diuretics are major weapons in management of CRS. Although diuretic resistance is a real entity, a majority of the time overaggressive diureses causes a prerenal state resulting in rising GFR. Maintaining fluid balance is the most important part of treatment of CRS, since patients often oscillate between
Figure 13
Figure 14
Figure 12

10 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6 S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 11
w w w . C H E S T E R C M S . o r g
Mian A. Jan is an interventional cardiologist practicing in Chester County.Ambereen M. Jan is a nephrologist practicing in Chester County.
CHF and azotemia. Swan Ganz and CVP catheters may help. With liver and GI congestion oral diuretics are not effective and thus IV loop diuretics are used instead. There is now significant data available that shows IV infusion may be better and not only reduce hospital stay but also the event rate and should be considered early.
*Ultrafiltration
The UNLOAD Trial compared diuretics with Ultrafiltration and showed more weight loss at 48 hours and at 90 days there was 44% less readmission. Currently ACC/AHA gives an Ultrafiltration Class 2A recommendation for refractory heart failure. Unfortunately, the cost is $10,000 and each filter costs an additional $900.
*Vasodilators Vasodilators like Nesiritide in a meta-analysis of 6 trials made kidney function worse (see figure 15).
Although the ASCEND-HF Trial of 7000 patients from 300 centers did not show any decline in renal function there was also no significant difference in 30-day readmission rate or death. While the trial confirmed the safety of the drug it did not show significant benefits.
*Vasopressin Antagonists
Vasopressin Antagonists should be effective since: -V1 receptors mediate vasoconstriction -V2 receptors mediate water resorption
Blocking V1 and V2 receptors should improve CRS. The EVEREST Trial of 4000 patients showed benefits in dyspnea on day 1 and weight loss on day 7 but no mortality benefit and the cost is $6000. Tolvaptan is currently approved for Hyponatremia and is very effective for that purpose.
*ACE and ARBs in Cardio-Renal Syndrome
ACE and ARBs should be used since they have a protective effect on both the kidney and heart. They are often stopped because of rising Creatinin which is more likely to be from aggressive diuresis and a prerenal state. Allow for a 30% rise before discontinuing.
*Beta Blockers
Since CRS has an overactive sympathetic nervous system with: -Beta 1 causing vasoconstriction and increased Renin -Beta 2 causing RV vasodilation -Alpha 1 causing Systemic and RV Vasodilation
Carvedilol is especially effective because it has Alpha blockade capability and is non selective.
*Furosemide and Hypertonic Saline Although counterintuitive, data shows that this combination can be effective. Patema, et. al., showed: -increased diuresis and natriuresis -better survival at 48 months -rapid attainment of dry weight -improved renal function -lower readmission rates
Larger trials are in progress which could lend clarity.
*Adenosin Receptor Antagonists
On paper they should be very effective but data so far has not been very supportive so the jury is still out.
SUMMARY CRS is a very common, complex and difficult to manage condition; I believe aggressive early prevention is the key. Once Cardio-Renal Syndrome is established, the team approach between intensivist, cardiologist and nephrologist with close hemodynamic monitoring and expert nursing care can result in favorable outcomes.
Figure 15
NesiritideBetter
0 0.5 1 1.5 2 2.5
A
B
C
D
E
F
NesiritideWorse

SPRINTINGTOWARDS IMPROVED HEALTH...
BY MICHAEL LATTANZIO, MD
12 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
12 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6 S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 13
w w w . C H E S T E R C M S . o r g
Continued on page 14
The intensity of blood pressure that is required to maximally reduce cardiovascular disease events is debatable. Observational studies have consistently demonstrated that lower blood pressure correlates with reduced cardiovascular disease events. Conversely, prospective
studies have failed to consistently demonstrate CV disease reduction with achieved BP targets less than 140/90. For instance, in the Action to Control Cardiovascular Risk in Diabetes Blood Pressure (ACCORD-BP) Trial, there was a non-significant reduction in CV endpoints among diabetic patients with hypertension treated to a SBP target less than 120mmHg (1). The Systolic Blood Pressure Intervention Trial (SPRINT) was designed to determine whether intensive blood pressure treatment confers greater cardiovascular benefit than standard blood pressure control in a population at high risk of CV disease events (2). The study was a multi-centered, randomized control trial that enrolled over 9000 individuals. Intensive blood pressure reduction was defined as a SBP less than 120mmHg. Standard blood pressure reduction was defined as a SBP less than 140mmHg. The study did not enroll individuals with diabetes or prior CVA, but did enroll some patients with advanced age and mild chronic kidney disease. The primary endpoint was myocardial infarction, CVA, CHF, or death from CV events. After a median follow-up of 3.26 years, the study was halted prematurely owing to a significantly lower rate of the primary composite outcome in the intensive-treatment group than in the standard-treatment group (1.65% per year vs. 2.19% per year; hazard ratio with intensive treatment, 0.75; 95% confidence interval [CI], 0.64 to 0.89; P<0.001) (2). All-cause mortality was also significantly lower in the intensive-treatment group (hazard ratio, 0.73; 95% CI, 0.60 to 0.90; P=0.003) (2). Rates of serious adverse events of hypotension, syncope, electrolyte abnormalities, and acute kidney injury were higher in the intensive therapy group.
...THROUGH INTENSIVE BLOOD PRESSURE CONTROL

CONFRONTING A CRISIS: An open letter to America’s Physicians
on the Opioid Epidemic
The SPRINT trial provides strong evidence that targeting a SBP less than 120mmHg in high-risk patients without diabetes can provide further CV risk reduction. However, the following considerations need to be highlighted prior to a broad application of the SPRINT results. The first issue is how the BP was actually measured. In the SPRINT trial, patients were placed in a silent room for 5 minutes and then the BP was measured with an automated machine. In real-life practice, this method of BP measurement is rarely performed. In fact, studies suggest that office BP measurements can be ~10mmHg higher than the measured BP readings from clinical trials. Therefore, the achieved, intensive BP target seen in SPRINT of 120mmHg may actually be an office reading of 130mmHg in real-life practice. Secondly, it cannot be understated that the patients in the intensive group did have higher risks of complications related to achieving a reduced BP target. This adverse risk came despite the fact that SPRINT trial participants are followed rigorously and that the enrolled participants would generally be considered less “frail” than individuals encountered in real-life practice. In summary, the SPRINT trial provides solid evidence that achieving a more intensive BP in high-risk individuals can reduce CV events. The results of SPRINT cannot be applied to diabetic patients or individuals with prior CVA history, since these patients were excluded from the study. Individuals treated to a more intensive BP target did have a higher risk of adverse events, including renal failure. The ultimate question is whether the measured BP in the SPRINT trial of 120mmHg parallels a BP measurement of 120mmHg BP in clinical practice. It is my opinion, that achieving an office SBP of 130mmHg is equivalent to the 120mmHg measurement in SPRINT and will afford the same CV protection. Blood pressure reduction strategies, particularly when attempting to achieve a more intensive BP target, need to be individualized with close monitoring of clinical efficacy and patient safety.
Michael R. Lattanzio, DO, is a clinical nephrologist and hypertension specialist with Clinical Renal Associates of Chester County.
References(1) Effects of Intensive Blood-Pressure Control in Type 2 Diabetes Mellitus. N Engl J Med 2010; 362:1575-1585. April 29, 2010
(2) A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med 2015; 373:2103-2116. November 26, 2015 after polypectomy. Ann Intern Med 2008;141:264–71.
SPRINTING TOWARDSIMPROVED HEALTH......THROUGH INTENSIVE BLOOD PRESSURE CONTROLContinued from page 13
w w w . C H E S T E R C M S . o r g
14 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
The medical profession must play a lead role in reversing the opioid
epidemic that, far too often, has started from a prescription pad. For the past 20 years, public policies—well-intended but now known to be flawed—compelled doctors to treat pain more aggressively for the comfort of our patients. But today’s crisis plainly tells us we must be much
more cautious with how we prescribe opioids. At present, nearly 2 million Americans—people across the economic spectrum, in small towns and big cities—suffer from an opioid use disorder. As a result, tens of thousands of Americans are dying every year and more still will die because of a tragic resurgence in the use of heroin. As a profession that places patient well-being as our highest priority, we must accept responsibility to re-examine prescribing practices. We must begin by preventing our patients from becoming addicted to opioids in the first place. We must work with federal and private health insurers to enable access to multi-disciplinary treatment programs for patients with pain and expand access for medication-assisted treatment for those with opioid use disorders. We must do these things with compassion and attention to the needs of our patients despite conflicting public policies that continue to assert unreasonable expectations for pain control.
As a practicing emergency physician and AMA president, I call on all physicians to take the following steps—immediately—to reverse the nation’s opioid overdose and death epidemic:
• Avoid initiating opioids for new patients with chronic non-cancer pain unless the expected benefits are anticipated to outweigh the risks. Non-pharmacologic therapy and non-opioid pharmacologic therapy are preferred.
• Limit the amount of opioids prescribed for post-operative care and acutely-injured patients. Physicians should prescribe the lowest effective dose for the shortest possible duration for pain severe enough to require opioids, being careful not to prescribe merely for the possible convenience of prescriber or patient. Physician professional judgment and discretion is important in this determination.
• Register for and use your state prescription drug monitoring program (PDMP) to assist in the care of patients when considering the use of any controlled substances.
• Reduce stigma to enable effective and compassionate care.
• Work compassionately to reduce opioid exposure in patients who are already on chronic opioid therapy when risks exceed benefits.
• Identify and assist patients with opioid use disorder in obtaining evidence-based treatment.
• Co-prescribe naloxone to patients who are at risk for overdose.
BY STEVEN J. STACK, MD, EMERGENCY PHYSICIAN AND THE 170TH PRESIDENT
OF THE AMERICAN MEDICAL ASSOCIATION
Together we can make a difference.
CONFRONTING A CRISIS: An open letter to America’s Physicians
on the Opioid Epidemic
As physicians, we are on the front lines of an opioid epidemic that is crippling communities across the country. We must accept and embrace our professional responsibility to treat our
patients’ pain without worsening the current crisis. These are actions we must take as physicians individually and collectively to do our part to end this epidemic.
w w w . C H E S T E R C M S . o r g
14 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6 S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 15

16 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g

BY MIAN A. JAN, MD
The year was 1998, when this youthful sophisticated lady, Judy Klanderman, came to see me for chest pain. I had never heard of her which in itself is sad, because as I discovered later she is an exceptional artist, which I found out
after a successful procedure I had performed on her, and she gifted me with a stunning West Chester watercolor. The fact is that despite great interest in art I had never heard of her. It’s a sad affair when we do not recognize our artists, for Chester County has a tradition of great artists, from the Wyeths, to Pippin to Pyle to Rubincam, and more recently Sculthorpe, Bollinger, Martinez, Scarborough, and of course Judy. However, I am not talking about these masters I am speaking of the lesser known artists, though not in skill, that are left in obscurity and have difficulties even making ends meet. There is considerable data to show that cultures that respect art and artists do well in all aspects of life. Judy, as often happens with me and my patients, became my long term patient and also a trusted friend. Over the years I was honored to acquire many of her wonderful works some of which are exhibited in this article. If I could I would have acquired a lot more. Judy paints from the heart and her paintings are vibrant, colorful and full of life. While she paints she develops rapport with her inner personal feelings and excitement blends with objective realism, giving a unique flavor to the subject. I have included a summer and winter scene she did of my family and me at our house and although a photograph does not do justice to the painting one can see the mastery of the medium. A watercolor teacher for thirty years and pastel for ten, Judy currently paints in all three mediums, oil, acrylic, and watercolor; she has had thirty-six solo shows. Additionally, Judy is the author of an award winning book, A Tribute to Cape May. Judy and her husband Mr. Klanderman are keen travelers and many of her works are done in European landscapes. The majority of her work is the plein air of the beautiful and stunning landscape that we are fortunate to have around us in Chester County.
Judy Antonelli KlandermanA Chester County Gem
S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 17
w w w . C H E S T E R C M S . o r g
Continued on page 18
“A Tuscan Farm” Watercolor
Note: Each painting shown is from the collection of Mian and Ambereen Jan
Chester CountyThe Art of

“A Tuscan Village” Oil on Canvas
“Winter Sundown” Pastel
“Winter Sunrise” Pastel
w w w . C H E S T E R C M S . o r g
18 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6

Judy has been featured in the American Artists Magazine and international fine art card companies Marcell Schurman of San Francisco and Caspari of New York have used her work often. Major corporations such as Wilmington Trust Bank, MBNA Bank, McGraw Hill New York, Bell Atlantic, and many private collectors have her works in their collections. She is also the winner of many awards for her work. Judy attended Drexel University and the Barnes Stone Studio, and has studied with many outstanding international artists. Her professional memberships include the Pennsylvania watercolor society, Chester County Art Association, Pastel Society of America and Philadelphia Watercolor Society where she was a board member and vice president.
I end this with the hope for many more great creations from Judy Klanderman and as she moves into her golden years more recognition from the citizens of Chester County.
Dr. Mian Jan is a cardiologist practicing in Chester County and is President-Elect of the Chester County Medical Society. He and his wife Ambereen Jan are avid collectors of Chester County Art.
w w w . C H E S T E R C M S . o r g
18 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6 S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 19
20 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
Pennsylvania Delegation Advocates to End Mandatory, Secured Recertifying MOC Exams
Though physicians are certainly committed to lifelong learning, we’ve heard from many Pennsylvania Medical Society (PAMED) members that Maintenance of Certification (MOC) is a time-consuming, burdensome disaster that is out of touch with their current practice of medicine. PAMED and its physician leaders, as well as several other state medical societies, continued their advocacy efforts on behalf of physicians at the recent annual meeting of the American Medical Association (AMA) House of Delegates in Chicago. At this meeting, PAMED and the Pennsylvania Delegation to the AMA extended their leadership roles in our initiative to further educate their physician colleagues on matters related to the fiscal affairs of the American Board of Internal Medicine (ABIM) and the questionable value of MOC as we support AMA, state, and specialty efforts to create a continuous professional development process that works for all physicians. “The Pennsylvania Delegation took the position we’ve been hearing from members for quite some time in opposition to MOC to the annual AMA meeting,” said PAMED President Scott Shapiro, MD. “During this meeting, PAMED continued its leadership on this issue, convening a national discussion panel to present their research findings, insights, and recommendations regarding the failures of the ABIM and the MOC process. The discussion regarding the actions, finances, and possible historical motivations for the ABIM’s actions was eye-opening and alarming.”
The AMA House of Delegates ultimately approved resolution 309 as amended, which includes language that:
Calls for the immediate end of any mandatory, secured recertifying examination by the American Board of Medical Specialties (ABMS) or other certifying organizations as part of the recertification process for all those specialties that still require a secure, high-stakes recertification examination.
Directs the AMA to continue to work with the ABMS to encourage the development by and the sharing between specialty boards of alternative ways to assess medical knowledge other than by a secure exam.
Directs the AMA to continue to support the requirement of CME and ongoing, quality assessments of physicians, where such CME is proven to be cost-effective and shown by evidence to improve quality of care for patients.
Directs the AMA to support a recertification process based on high quality, appropriate CME material.
20 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6 S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 21
w w w . C H E S T E R C M S . o r g
This process will be directed by AMA-recognized specialty societies covering the physician’s practice area, in cooperation with other willing stakeholders that would be completed on a regular basis as determined by the individual medical specialty, to ensure lifelong learning. The adoption of this resolution was viewed as a strong message from physicians across the country to have the AMA take a stronger position on the matters related to the ABIM and MOC. Resolution 309 was cosponsored by
Pennsylvania, Florida, California, Georgia, Washington, New York, and Virginia. Prior to the resolution being adopted, the stage was set by the panel discussion sponsored by PAMED and the Pennsylvania delegation featuring Charles Kroll, CPA, Bonnie Weiner, MD, Wes Fisher, MD, and PAMED President Scott Shapiro, MD, and the announcement that PAMED issued a statement of no confidence in the ABIM. One physician said that the “Pennsylvania Medical Society melted the meeting down with a blistering two-hour exposé on the abuses of the ABIM and the boards in general. With a much needed boost in morale and the data to support strong action, the full house convened on Wednesday and the delegates soundly rejected the Committee’s butchering of the resolution, extracted it to a full vote on the house floor, and restored the strong language of the first resolved.” Dr. Shapiro added: “This was a continuation of efforts that have been ongoing for years led by physician leaders in Pennsylvania. The Pennsylvania delegation is very proud to announce that the culmination of years of our hard work resulted in the AMA passing a resolution that was co-authored by our Pennsylvania delegation that ultimately creates AMA policy calling for the immediate end of all high-risk security risk certification examinations by the ABIM, and all our specialties that still require a needless similar exam.”
Check Out www.chestercms.org – we’ve revised our webpage!CCMS members – send us a
link to your practice website.
We are developing a directory
for patients to use in finding
physicians – it will be a
Practice Directory Guide and
feature only websites with
CCMS members. Send
your website address
to chescomedsoc@
comcast.net.
Staying up to date on the latest news and advocacy issues impacting Pennsylvania physicians just became easier with the launch of the Pennsylvania Medical Society’s new mobile app.
Download this app to your iPhone
or Android device to receive daily news updates and act
on important advocacy issues. Be the first to know about
important physician-related issues being discussed at
the state capitol. The app offers a quick and easy tool to
communicate with your state and federal legislators. Save
time, save money and stay compliant with updates from
PAMED’s practice support experts. Learn about upcoming
state and county educational events. Read PAMED’s
quarterly magazine and view our member directory.
TECHNOLOGY UPDATE
22 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
William Darlington was an American physician, botanist, and member of the U.S. House of Representatives from Pennsylvania. His ancestors followed William
Penn to Pennsylvania. He was born April 28, 1782 in Birmingham, Chester County, Pennsylvania. He was raised as a Quaker and attended the Friends School at Birmingham, spending much of his time during his youth on a farm. He later became an Episcopalian, and a botanist, studied medicine, and graduated from the medical department of the University of Pennsylvania in Philadelphia in 1804. He was the first native of Chester County to receive a medical degree. William went to the East Indies as ship’s surgeon in 1806. He returned to West Chester, near Birmingham, in 1807 and was a practicing physician there for a number of years. He raised a company of volunteers at the beginning of the War of 1812 and was major of a volunteer regiment. Dr. Darlington was elected as a Democratic-Republican to the Fourteenth U.S. Congress (1815 – 1817). He was again elected to the Sixteenth (1819 – 1821) and Seventeenth (1821 – 1823) Congresses. Darlington was appointed canal commissioner in 1825, and served as president of the West Chester Railroad. He established a natural history society in West Chester in 1826 and published several works on botany and natural history. Dr. Darlington was one of the founding physician members of the Chester County Medical Society (the state’s first county medical society) in 1828. The degree of L.L.D. was conferred on him by Yale University in 1848, and he was awarded a Doctor of Physical Science in 1855 by Dickinson College. He served as director and president of the National Bank of Chester County from 1830 to 1863. He died in West Chester in 1863, and was interred in Oakland Cemetery.
William Darlington (April 28, 1782 – April 23, 1863)
JOIN US SEPTEMBER 16TH AT THE CCMS CLAMBAKE AS WE AWARD THE 2016 DR. WILLIAM DARLINGTON MEMORIAL SCHOLARSHIP
TO A WEST CHESTER UNIVERSITY STUDENT.
22 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6 S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 23
w w w . C H E S T E R C M S . o r g
Join Us!CHESTER COUNTY MEDICAL SOCIETY
ANNUAL LEGISLATIVE CLAM BAKE FRIDAY SEPTEMBER 16, 2016RADLEY RUN COUNTRY CLUB
6:00 PM RECEPTION7:00 PM DINNER
Join Us For An Outstanding Evening With Our Local Elected Officials
Including The Installation Of Mian Jan, As President Of The Chester County Medical Society
Fifty Years In Medicine Awards
Presentation Of The Dr. William Darlington Memorial Scholarship To A West Chester University Student
Only $29 For CCMS Members And Their Guest(s)
Sign Up And Send In With Payment - $29/PersonChecks Payable To
Chester County Medical Society600 N. Jackson St. Suite 201A
Media, PA 19063-2561
Questions? - Call Our Staff (610) 827-1543

OPIOIDS FOR PAIN: Be Smart. Be Safe.
Be Sure.
Prescription opioid medications serve an effective role in pain management, but growing abuse of these drugs has reached epidemic proportions in Pennsylvania. To fight back, the Pennsylvania Medical Society has created a public advocacy program called: Opioids for Pain: Be smart. Be safe. Be sure.
This program has several simple goals:
• Reduce opioid abuse and overdoses• Educate patients about the safe use of opioids and the warning signs of addiction• Help physicians prescribe opioid drugs with more precision and less potential for abuse
The key points of the Opioids for Pain program:
1. Be smart — Patients should know the risks of opioid use when they receive a prescription. No one plans on becoming an addict, but many do by ignoring dosage limits and frequency.2. Be safe — Patients should be instructed on how to use opioids for moderate to severe pain, and warned not to save extras or give them to friends or relatives. Physicians are encouraged to write smaller prescriptions with fewer refills. The PAMED website has a link to find where to safely dispose of leftover medications.3. Be sure — Patients should be told of the early signs of addiction or abuse and how to protect themselves from addiction, including how to avoid it and where to turn if they feel they may have developed a problem.
24 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g

S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 25
w w w . C H E S T E R C M S . o r g
Learn more. Call (610) 374-1936 or visit www.stratixsystems.com.
IT Support & Network Services
Managed & Cloud IT Services
Document Management
Printing & Imaging Systems
Berks County Medical Society members trust Stratix Systems to take
care of their technology pains.
No one knows technology solutions like Stratix.
Technology Solutions to Help Your Healthcare Organization Deliver Better Care
Chester County Medical Society members trust Stratix Systems to take
care of their technology pains.
FOR LAWMAKERSEducate citizens in your district through these resources. PAMED has created posters for you to distribute at events and ready-made stories and images to add to your newsletter, website and social media pages.Go to PAMED website – www.pamedsoc.org to Download Lawmaker Resources
FOR PHYSICIANSLearn five ways you can take the lead in addressing opioid abuse and misuse with your patients. PAMED has also created printable tear-off sheets and waiting room posters for physicians to use.Go to PAMED website – www.pamedsoc.org to Download Physician Resources
FOR PATIENTSPatients need to work with their physicians to be smart, safe and sure about opioid use. PAMED resources include seven questions patients should ask their physician as well as a list of where they can drop off unused medications.Go to PAMED website – www.pamedsoc.org to Download Patient Resources

26 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
Are You Ordering, Prescribing, or Referring for MA Beneficiaries?Don’t Forget to Revalidate in Medicaid!
The PA Department of Human Services (DHS) made a change to its PROMISe internet portal designed to let physicians and other providers know if they are not enrolled or revalidated in Medicaid, known as Medical Assistance (MA) in Pennsylvania. Per a DHS Medical Assistance Bulletin issued on April 1, 2016, claims submitted to the PROMISe system with an NPI number in the field for an ordering or referring provider, who is not enrolled or revalidated in the MA program, will automatically generate a message on the claim remittance advice to alert the billing provider that the ordering, referring or prescribing provider is “not on file” and must enroll or revalidate in the MA Program. When processing claims that include a field for an ordering or referring provider, DHS uses the National Provider Identification (NPI) number on the claim to validate the provider’s enrollment in the MA Program. The Affordable Care Act requires that all practitioners, including those who order, refer, or prescribe items or services for MA beneficiaries, must enroll in the MA Program. This requirement applies even if those providers do not submit claims to the state Medicaid program for Medicaid-covered services rendered to Medicaid beneficiaries.
Beginning September 25, 2016, claims will be denied if the ordering, referring or
prescribing provider appearing on the claim is not enrolled in the MA Program.
In cases where a provider who is not enrolled in the MA fee-for-service program orders, refers, or prescribes a service for a MA fee-for-service beneficiary, the claim submitted by the rendering or billing provider will not be paid, even though the rendering or billing provider is enrolled in the MA program. DHS says that examples of services that require a prescription, an order, or a referral are:
• All medications
• Medical supplies, medical equipment, orthotics, and prosthetics
• Lab tests
• Home health services
• Radiologic imaging services
• Hospital admissions
• Procedures done in a hospital short procedure unit (SPU), an ambulatory surgical center, or a treatment room
Questions? Contact the DHS Program Office at 1-800-537-8862 with any questions or concerns. PAMED members also can contact PAMED’s Knowledge Center at 855-PAMED4U (855-726-3348). Physicians and practices can find more PAMED resources on revalidation and the application process, including information on how to verify whether you are enrolled in the MA program.
w w w . C H E S T E R C M S . o r g
K a t h e r i n e A c e t o n eA n n e t t e A l e s s i
N a n c y B a r c hA l B a r k e r
J a ca l y n B e a mG r e g o r y B l u e
H a r r y B o a r d m a nR i c h a r d B o l l i n g e r
Pa t r i c i a B ra n d tJ o a n n e Le g n i n i C a r o t h e r s
B e t h C l a r kS u e C i c c o n eM a r k D a n c e
C h r i s t i a n e D a v i dB ra d E a r lC h i E b e r t
Lo r e E va n sL i z Fi n l e y
J o e G r u b bM a g g i e H a g s t r o m
M a r y Wo l f i n g t o n J o n e sM a d e l e i n e K e l l y
L i d i a K o h u t i a kD i a n e L a v e l l e
G e o rg a n n a Le n s s e nB ra d l e y M a t t e s
V i c t o r M o r d a s o vLe e M u s l i nA b b y O b e r
D a v i d O l e s k iJ a c k Pa o l i n i
J o h n Po m p e oPe t e r M c D a n i e l
D e n i s e S e d o rS a n d ra S e v e r s o n
G e n e v i e v e S n y d e rR o b S t e i n
J a s S z yg i e lN a n c y Fr e e m a n Ta b a s
L i n We b b e rS u s a n B a n k e r t
T h o m a s B e n f i e l dD a n B u r s t e i n
To b y C h a d s e yK a t h l e e n Fr i e d b e rg
G r e g o r y M e y e r sJ a c k H a y e s
N e l l H a z i n s k iB r i a n M a r s h a l l
S u z a n n e O s wa l dG e o rg e Wa t s o n
S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 27
K a t h e r i n e A c e t o n eA n n e t t e A l e s s i
N a n c y B a r c hA l B a r k e r
J a ca l y n B e a mG r e g o r y B l u e
H a r r y B o a r d m a nR i c h a r d B o l l i n g e r
Pa t r i c i a B ra n d tJ o a n n e Le g n i n i C a r o t h e r s
B e t h C l a r kS u e C i c c o n eM a r k D a n c e
C h r i s t i a n e D a v i dB ra d E a r lC h i E b e r t
Lo r e E va n sL i z Fi n l e y
J o e G r u b bM a g g i e H a g s t r o m
M a r y Wo l f i n g t o n J o n e sM a d e l e i n e K e l l y
L i d i a K o h u t i a kD i a n e L a v e l l e
G e o rg a n n a Le n s s e nB ra d l e y M a t t e s
V i c t o r M o r d a s o vLe e M u s l i nA b b y O b e r
D a v i d O l e s k iJ a c k Pa o l i n i
J o h n Po m p e oPe t e r M c D a n i e l
D e n i s e S e d o rS a n d ra S e v e r s o n
G e n e v i e v e S n y d e rR o b S t e i n
J a s S z yg i e lN a n c y Fr e e m a n Ta b a s
L i n We b b e rS u s a n B a n k e r t
T h o m a s B e n f i e l dD a n B u r s t e i n
To b y C h a d s e yK a t h l e e n Fr i e d b e rg
G r e g o r y M e y e r sJ a c k H a y e s
N e l l H a z i n s k iB r i a n M a r s h a l l
S u z a n n e O s wa l dG e o rg e Wa t s o n
Save the DateOctober 21,
20166 -10 PM
The community is already buzzing about Paoli Hospital Auxiliary’s First Ever Fall Fine Art Show and Cocktail Party. This reception will be held at Hillhouse, a private historical Berwyn estate, and all proceeds from art sales will benefit both the artist and the Auxiliary’s annual pledge to Paoli Hospital.
Richard Bollinger, a nationally known Chester County artist, will be the featured artist at the event. In addition to displaying several original paintings for sale at the show, he will also be creating an original work of art to be raffled off. Mr. Bollinger’s work is representedin 125 galleries across America. He has received numerous awards, and was commissioned to produce the official commerative painting for the centennial celebration of Valley Forge National Historic Park. Many of us are familiar with his beautiful art.
The Paoli Hospital Fall Fine Art Show will also include 50 other locally and regionally known artists. Their showings will representvarious types of painting such as oils, water colors, mixed media, acrylics, etc., as well as sculpture, pottery, 3D art and much more. A list of the participating artists is left of this article.
Invitations for the event will be mailed in early September. Admission is $50 and includes wine and hors d’oeuvres. Raffle tickets for Richard Bollinger’s painting can be purchased now at a cost of $15 each or 3 for $30. Information about the event or purchasing raffles can be obtained by calling 484-565-1380.
Attendance will be limited to the first 300 participants
w w w . C H E S T E R C M S . o r g

BY JOHN P. MAHER, MD, MPH
ZIKA VIRUS DISEASEARE WE PREPARED?
28 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
As of June 29, 2016, the United States had reported 935 cases of Zika virus infections. Fortunately, and at least so far, none of these cases had been acquired locally by
mosquito-borne transmission. In fact, 934 of them were travel-associated cases, including 13 sexually transmitted, and 4 Guillain-Barré cases. The good news, if one can call it that, is that thus far no vector-borne transmission had occurred in the United States. On the bad news side, there are these worrisome facts: of these 935 cases, 4 developed Guillain-Barré syndrome; the 935 laboratory-confirmed cases reported to the CDC’s ArboNET program involved 45 of the 50 US states, plus the District of Columbia. There is also the fact that here in the US we have dozens of Aedes species, including at least two of the major potential mosquito vectors for the Zika virus, namely: Aedes aegypti (known by many as the Yellow Fever mosquito), and Aedes albopictus (a.k.a. the Asian Tiger mosquito). These two vectors prefer hot humid climates, and are found in the US especially across the southern tier states from southern California, across Arizona, New Mexico, Texas and the Gulf states, through Florida, and up the East Coast, especially from North Carolina, Virginia, into Maryland, New Jersey and the southeastern PA area, as well as extending to NYC, Connecticut and even Massachusetts. Zika is not really a new disease but its recent explosive spread has created fear and near panic in some areas. First discovered in Africa in 1947, it is named for the Zika Forest area of Uganda, Africa. Several years later, in 1952, the first human cases of Zika were detected, and since then outbreaks of Zika have been reported in tropical Africa, southeast Asia, and certain Pacific Islands. Such outbreaks had probably occurred in many locations, but went unrecognized and unreported. Before 2007, at least 14 Zika cases had been documented. Because the symptoms of Zika are similar to those of many other mosquito-borne diseases, many cases may not have been recognized especially in those regions where such diseases are common (malaria, dengue, chikungunya, viral encephalitides such as
Japanese B encephalitis), with overlapping areas of distribution. Brazil alone reports 2 million cases of dengue a year. However, for whatever environmental, genetic or socioeconomic reasons, the incidence of Zika infections in South America, particularly Brazil, began to soar, along with a growing number of cases of neonatal/congenital microcephaly, generating a clear “tip of the iceberg” alarm signal not only among healthcare professionals there but across the global public health community. Thus, in May 2015, the Pan American Health Organization (PAHO) issued an alert regarding the first confirmed Zika infection in Brazil. According to Chen, et al. (Ann. Int. Med. (9), 2016) the virus was initially detected in northeast Brazil, then in other states there, and subsequently was found in several other South American countries (Columbia, Ecuador, Suriname, Venezuela, French Guyana, and Paraguay). Transmission has since been documented in Central America (Panama, El Salvador, Honduras, Guatemala), the Caribbean (Martinique, Dominican Republic, especially Puerto Rico), and Mexico. By late January 2016, a total of 20 countries and territories in the Americas had Zika virus circulating. On February 1, 2016, the World Health Organization (WHO), recognizing that local transmission has been reported in many countries and territories, and that the virus will likely continue to spread to new areas, officially declared Zika virus a “Public Health Emergency of International Concern (PHEIC)” indicating a public health crisis of potentially global impact. Only 3 such declarations have been previously issued by WHO (Swine Flu, 2009; Polio, May 2014; and Ebola, August 2014).
So, what is Zika? Zika virus disease is caused by the Zika virus, which is (most often) spread to people by mosquito bites. An estimated 80% who get Zika have no symptoms. When symptoms do occur they are usually mild, lasting a few days to a week, and resolve on their own. Most commonly, symptoms include fever, rash, arthralgias and red eyes.

S U M M E R 2 0 1 6 | C H E S T E R C O U N T Y M E D I C I N E 29
w w w . C H E S T E R C M S . o r g
Transmission: Most Zika infections are spread through the bite of mosquitoes of the Genus Aedes, but there is some evidence of possible tick-borne transmission as well. It can also be passed from a pregnant mother to the child in utero, or during the birth process itself. Recently, there is evidence it can also be spread sexually, as well as by blood transfusions if the donor was infected. During one outbreak in French Polynesia, nearly 3% of blood donors tested positive for Zika. In addition, there have now been 5 reports of laboratory acquired Zika infections (only one in a US lab) but the actual route of that transmission has not been clearly established. By late June, WHO reported ongoing transmission in 61 countries worldwide. Because Aedes mosquitoes are found throughout the tropics, outbreaks will likely continue in those regions. Thus, it is essential that pregnant women be aware that no one knows whether there is a “safe period” during pregnancy to travel in such areas.
Treatment: There is no known treatment available at this time. Research on a preventive vaccine is being pushed, and at least one organization has been producing genetically engineered mosquitoes which could mate with wild mosquitoes and pass a lethal gene which kills their offspring before they attain adulthood. Meanwhile, the old stand-by measures (use of repellants, protective clothing, eliminating wet breeding sites, and avoiding mosquito bites) still provide some protection against these aggressive daytime feeders. Some are suggesting the need to bring back the use of the long-banned insecticide, DDT, for this purpose. Meanwhile, on May 26th, the AMA sent a formal letter to the leadership of both Houses of Congress urging them to take immediate action to provide the necessary resources to combat the spread of the Zika virus here.
Zika Virus and Birth Defects: Zika virus is a flavivirus, a genus of single strand RNA viruses which includes Dengue, Chikungunya, West Nile Virus, and Japanese B encephalitis virus, meaning that some, if not all of them can be neurotropic and cause CNS damage.(Jin, J: JAMA, June 14, 2016). There is growing evidence and concern that Zika can cause the Guillain-Barré syndrome in some victims, but the major health concern at this time is the link between Zika and pregnancy loss and birth defects. In particular, Zika infections have been linked to congenital microcephaly in infants. Symptoms of various neurological abnormalities have been seen in infants, both with and without microcephaly, born after maternal Zika infection. In a six month period (October 2015- April 2016) Brazil reported just over 6900 such cases.
Diagnostic Testing: Diagnostic testing for Zika virus can be done using both molecular and serologic methods. An ELISA test can be used to detect anti-Zika virus IgM antibodies. However, to resolve issues of false positives due to cross-reactivity, the plaque reduction neutralization test (PRNT) should also be performed. The Food and Drug Administration has issued an Emergency Use Authorization (EUA) for two diagnostic tools for Zika virus: the Zika MAC-ELISA, and Trioplex Real-Time RT-PCR Assay, which is being distributed to qualified laboratories which are certified to perform high-complexity tests in the US.
Clinicians should contact their state or local health department to facilitate testing, and obtain instructions about specimen collection and submission. Remember, also, that Zika infections are mandatorily reportable diseases. Keep in mind that there can be cross-reactivity between flaviviruses, including between Zika and Dengue. If serologic testing indicates recent flavivirus infection which could be either Zika or Dengue, patients should be clinically managed for both, to reduce the risk of hemorrhage and shock.
For recent revised guidelines on progression and interpretation of serum antibody testing, see MMWR, 65 (21); June 3, 2016.
Information Resources: The CDC periodically updates its Interim Guidance directions for health care providers caring for infants, children and/or women of reproductive age. For their latest, up-to-date guidance concerning prevention, diagnostic testing, and reporting, as well as for downloadable fact sheets for their patients, clinicians should visit http://www.cdc.gov/Zika. The WHO website also provides a variety of resource materials in many different languages.
[ N.B.: The author gladly acknowledges the liberal use of CDC and WHO sources, as well as articles from the JAMA, the Annals of Internal Medicine, and a variety of news media stories, in doing the background research for this article.]

30 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
w w w . C H E S T E R C M S . o r g
NIH Launches Moms’ Mental Health Matters
The National Institutes of Health (NIH) has launched Moms’ Mental Health Matters, a new initiative to raise awareness among pregnant and postpartum mothers, their families, and health care providers about depression and anxiety during pregnancy and after the baby is born.
The NIH has developed free health education materials in English and Spanish, including posters that describe the signs of perinatal depression and anxiety, counter the idea that all moms are happy during this time, and encourage pregnant women to know the signs of depression and anxiety before their baby’s arrival.
The program has also developed an action plan to help moms identify when to seek help. In addition, the conversation starter postcard, specifically designed for the mom’s support system, offers suggestions for communicating with a loved one about this issue.
Learn more and order free materials at www.nichd.nih.gov/MaternalMentalHealth
CONSIDER MEMBERSHIPin The Chester County Medical Society
Member BenefitsJoin Us!
To learn more, join or renew, visit https://www.pamedsoc.org/about-pamed/Membership
Established in 1828, the Chester County Medical Society, founded by Dr. William Darlington, M.D., is thought to be the oldest county medical society in the State. The Medical Society is involved in all aspects of healthcare policy, practice, and education and serves to advance the health of the community and to protect and expand the healthcare resources available to its citizens.
The Chester County Medical Society works collaboratively with the Pennsylvania Medical Society, but our focus is on our local community. The Society’s role in Chester County is to support, protect, and advocate for our physicians and our patients. We look forward to growing an important healthcare service for our community that will benefit us all, and we look forward to hearing from you.
Help Patients Find You! CCMS Members are listed in the Pennsylvania Medical Society’s “Find a Physician” program.
Legislative Support Representation with local legislatorsContact your local legislator by getting their contact information provided on our Legislator page.
General Membership Meeting General Membership Meeting — an annual meeting which provides members the opportunity to impact their Society’s activities and goals.
Legislative Dinner Legislative Dinner — a.k.a. “The Clam Bake” — an annual meeting for members to meet with local legislators in an informal setting for cocktails and dinner to discuss healthcare issues.
Chester County Medicine Chester County Medicine has been the CCMS’s official publication for several decades. CCMS members will receive a complimentary subscription to Chester County Medicine magazine, the Society’s new twist on its longtime quarterly publication.
DocBookMD — an exclusive HIPAA-secure messaging application for smart phone and tablet devices.

30 C H E S T E R C O U N T Y M e d i c i n e | S U M M E R 2 0 1 6
Cost per person (covers educational materials, CME and CPE credits, and food at live programs):
• PAMED member physician—$2,500 Physicians who enroll at the member rate agree to maintain PAMED membership for the program’s duration. There are scholarship opportunities available for PAMED members. Learn more at www.pamedsoc.org/YRA.
• Physician non-member of PAMED—$3,500 To qualify for the member rate, call 855-PAMED4U or join online at www.pamedsoc.org/join.
Designed for physicians in practices, groups, hospitals, and health systems, this program provides broad, practical leadership training, networking and mentoring, and strategies to address challenges.
The 10-month program runs September 2016 through June 2017 and includes eight online courses and three day-long live sessions offering 60.5 CME and CPE credits. Facilitators are AAPL faculty and, for some online discussions, PAMED staff.
Scheduled courses include:
• Physician in Management: Communication
• Productive Behavior, Restoring Productivity Live Session—Oct. 14, 2016
• Meta-Leadership: Removing Barriers and Building Bridges
• Physician in Management: Effective Physician Leadership
• Physician in Management: Finance
• Physician in Management: Quality
• Physician in Management: Negotiation Live Session—April 7, 2017
• Strategic Decision-Making
• Strategic Planning
• Strategic Thinking
• Building and Leading Effective Teams Live Session—June 23, 2017
CME and CPECourses are accredited for CME. The courses in this program qualify for credit toward the CPE designation and for AAPL’s master’s degree programs with Carnegie Mellon University, Thomas Jefferson University, University of Massachusetts Amherst, and University of Southern California. For more information about the graduate programs, visit www.physicianleaders.org/education/programs/masters.
2016-2017 Year-Round Leadership Academy
“I’m fortunate to have received a scholarship to participate in PAMED’s Year-Round Leadership Academy. Throughout the years of medical school, residency, and fellowship, the focus is becoming a good clinician. Our teachers guide us through complexities of assessing, diagnosing, and treating patients for many different conditions. Then, we enter into “practice” and realize how critical leadership skills are to providing the standard of care we seek to achieve. This leadership series builds the foundation necessary to navigate conversations we encounter as a routine part of practice. It provides the resources that have made me more confident to pursue leadership roles.”
Chad Walker, DO Rheumatology Professional Orthopaedic Associates Scranton, PA
Register now at www.pamedsoc.org/YRA or by completing the form on the reverse side.
Cost per person (covers educational materials, CME and CPE credits, and food at live programs):
• PAMED member physician—$2,500 Physicians who enroll at the member rate agree to maintain PAMED membership for the program’s duration. There are scholarship opportunities available for PAMED members. Learn more at www.pamedsoc.org/YRA.
• Physician non-member of PAMED—$3,500 To qualify for the member rate, call 855-PAMED4U or join online at www.pamedsoc.org/join.
Designed for physicians in practices, groups, hospitals, and health systems, this program provides broad, practical leadership training, networking and mentoring, and strategies to address challenges.
The 10-month program runs September 2016 through June 2017 and includes eight online courses and three day-long live sessions offering 60.5 CME and CPE credits. Facilitators are AAPL faculty and, for some online discussions, PAMED staff.
Scheduled courses include:
• Physician in Management: Communication
• Productive Behavior, Restoring Productivity Live Session—Oct. 14, 2016
• Meta-Leadership: Removing Barriers and Building Bridges
• Physician in Management: Effective Physician Leadership
• Physician in Management: Finance
• Physician in Management: Quality
• Physician in Management: Negotiation Live Session—April 7, 2017
• Strategic Decision-Making
• Strategic Planning
• Strategic Thinking
• Building and Leading Effective Teams Live Session—June 23, 2017
CME and CPECourses are accredited for CME. The courses in this program qualify for credit toward the CPE designation and for AAPL’s master’s degree programs with Carnegie Mellon University, Thomas Jefferson University, University of Massachusetts Amherst, and University of Southern California. For more information about the graduate programs, visit www.physicianleaders.org/education/programs/masters.
2016-2017 Year-Round Leadership Academy
“I’m fortunate to have received a scholarship to participate in PAMED’s Year-Round Leadership Academy. Throughout the years of medical school, residency, and fellowship, the focus is becoming a good clinician. Our teachers guide us through complexities of assessing, diagnosing, and treating patients for many different conditions. Then, we enter into “practice” and realize how critical leadership skills are to providing the standard of care we seek to achieve. This leadership series builds the foundation necessary to navigate conversations we encounter as a routine part of practice. It provides the resources that have made me more confident to pursue leadership roles.”
Chad Walker, DO Rheumatology Professional Orthopaedic Associates Scranton, PA
Register now at www.pamedsoc.org/YRA or by completing the form on the reverse side.
Cost per person (covers educational materials, CME and CPE credits, and food at live programs):
• PAMED member physician—$2,500 Physicians who enroll at the member rate agree to maintain PAMED membership for the program’s duration. There are scholarship opportunities available for PAMED members. Learn more at www.pamedsoc.org/YRA.
• Physician non-member of PAMED—$3,500 To qualify for the member rate, call 855-PAMED4U or join online at www.pamedsoc.org/join.
Designed for physicians in practices, groups, hospitals, and health systems, this program provides broad, practical leadership training, networking and mentoring, and strategies to address challenges.
The 10-month program runs September 2016 through June 2017 and includes eight online courses and three day-long live sessions offering 60.5 CME and CPE credits. Facilitators are AAPL faculty and, for some online discussions, PAMED staff.
Scheduled courses include:
• Physician in Management: Communication
• Productive Behavior, Restoring Productivity Live Session—Oct. 14, 2016
• Meta-Leadership: Removing Barriers and Building Bridges
• Physician in Management: Effective Physician Leadership
• Physician in Management: Finance
• Physician in Management: Quality
• Physician in Management: Negotiation Live Session—April 7, 2017
• Strategic Decision-Making
• Strategic Planning
• Strategic Thinking
• Building and Leading Effective Teams Live Session—June 23, 2017
CME and CPECourses are accredited for CME. The courses in this program qualify for credit toward the CPE designation and for AAPL’s master’s degree programs with Carnegie Mellon University, Thomas Jefferson University, University of Massachusetts Amherst, and University of Southern California. For more information about the graduate programs, visit www.physicianleaders.org/education/programs/masters.
2016-2017 Year-Round Leadership Academy
“I’m fortunate to have received a scholarship to participate in PAMED’s Year-Round Leadership Academy. Throughout the years of medical school, residency, and fellowship, the focus is becoming a good clinician. Our teachers guide us through complexities of assessing, diagnosing, and treating patients for many different conditions. Then, we enter into “practice” and realize how critical leadership skills are to providing the standard of care we seek to achieve. This leadership series builds the foundation necessary to navigate conversations we encounter as a routine part of practice. It provides the resources that have made me more confident to pursue leadership roles.”
Chad Walker, DO Rheumatology Professional Orthopaedic Associates Scranton, PA
Register now at www.pamedsoc.org/YRA or by completing the form on the reverse side.
DELAWARE COUNTY’S ‘TOP DOCS’ ARE WITH
CROZER-KEYSTONE
CONGRATULATIONS TO THE FOLLOWING PHYSICIANS:
Thirty-five Crozer-Keystone Health System physicians were included in Philadelphia magazine’s 2016 “Top Doctors” issue published in April. The doctors were nominated
in surveys of their peers conducted by Castle Connolly Medical Ltd.
Taro Arai, M.D. Colorectal Surgery
Thomas Bader, M.D. Obstetrics and Gynecology
Kenneth Briskin, M.D. Otolaryngology
Kenneth Boyd, M.D. Colorectal Surgery
David Broyles, D.O. Family Medicine
Robert Cabry Jr., M.D. Sports Medicine
Catherine DiGregorio, M.D. Pain Medicine
Nicholas DiNubile, M.D. Orthopedic Surgery
Igor Dorokhine, M.D. Geriatric Medicine
Christine Egan, M.D. Dermatology
Albert El-Roeiy, M.D. Reproductive Endocrinology
John Feehery, M.D. Otolaryngology
Karl Grunewald, M.D. Thoracic and Cardiac Surgery
Linwood Haith Jr., M.D. Surgery
John Hiehle Jr., M.D. Diagnostic Radiology
Rima Himelstein, M.D. Adolescent Medicine
Jackeline Iacovella, M.D. Infectious Disease
Deborah Kahn, M.D. Geriatric Medicine
Thomas Klein, M.D. Allergy and Immunology
Pei Ann Kong, M.D. Internal Medicine
Mark Lisberger, M.D. Cardiovascular Disease
James McGlynn, M.D. Orthopedic Surgery
Stephen Nelson, M.D. Infectious Disease
Joel Noumoff, M.D. Gynecologic Oncology
Nathan Okechukwu, M.D. Nephrology
Hemchand Ramberan, M.D. Gastroenterology
Anthony Rooklin, M.D. Allergy and Immunology
John Sprandio, M.D. Medical Oncology
Marc Surkin, M.D. Otolaryngology
Dean Trevlyn, M.D. Orthopedic Surgery
Stephen Walker, M.D. Urology
Christopher Williams, M.D. Ophthalmology
Sean Wright, M.D. Plastic Surgery
Lubna Zuberi, M.D. Endocrinology
Alan Zweben, M.D. Internal Medicine
crozerkeystone.org
TopDocsDelcoAd16.indd 1 7/7/16 8:24 AM