Low thoracic versus lumbar epidural anesthesia during the...
35
By Jon Gutteling Low thoracic versus lumbar epidural anesthesia during the first phase of labor J. Gutteling, RUG ID: 1924214 Mentor: J.M.G. Cobben, Anesthesiologist 15 October 2012 – 15 march 2013 Anesthesiology Department, Deventer Hospital
Transcript of Low thoracic versus lumbar epidural anesthesia during the...

By
Jon Gutteling
Low thoracic versus lumbar epidural anesthesia during the first phase of labor
J. Gutteling, RUG ID: 1924214
Mentor: J.M.G. Cobben, Anesthesiologist
15 October 2012 – 15 march 2013
Anesthesiology Department, Deventer Hospital

Abstract (Dutch) 1
Samenvatting
Introductie
Er zijn aanwijzingen dat de pijn die vrouwen ervaren tijdens de baring intenser is dan
vrijwel alle pijn van andere oorsprong. Epidurale analgesie (“een epiduraal”) is
wereldwijd een veel toegepaste anesthesietechniek die zeer geschikt is voor perinatale
anesthesie. De meest gebruikte hoogte om een epiduraal te prikken is de (laag)
lumbale regio. Gezien het feit dat de meeste pijn tijdens de ontsluitingsfase wordt
gevoeld via zenuwwortels ter hoogte van T10-L1, is onze hypothese dat thoracale
epidurale anesthesie resulteert in betere analgesie en minder kunstverlossingen en
sectio’s dan lumbale epidurale anesthesie tijdens de ontsluitingsfase van de partus.
Methoden
Om deze hypothese te toetsen werden twee studies opgezet. Ten eerste een
retrospectieve dossierstudie naar alle bevallingen met epidurale analgesie de
afgelopen vier jaar, om te kijken naar de primaire uitkomst van de bevalling.
Daarnaast een prospectieve observationele studie, waarin alle vrouwen met een
thoracale (T10-L1) of lumbale (L1-L5) epidurale katheter werden geïncludeerd. De
pijn die ze beleefden werd elk uur met de visueel analoge schaal (VAS) vastgelegd,
daarnaast werd bijgehouden hoe snel en hoe vaak er door de barende om extra
pijnstilling werd gevraagd.
Resultaten
De retrospectieve database bevatte bruikbare gegevens van 1172 patiënten. Hiervan
had 96 een thoracale en 1096 een lumbale epiduraal. We vonden geen statistisch
significante resultaten betreffende de incidentie van spontane bevallingen, sectio’s en
kunstverlossingen. Ook de APGAR score van de pasgeborene en de tijd vanaf het
plaatsen van de epidurale katheter tot de bevalling klaar was lieten geen verschil zien.
In de prospectieve studie zijn 44 patiënten geïncludeerd. Hiervan kregen 13 een
thoracale epidurale katheter en 31 patiënten een lumbale. Grafische weergave liet
mogelijke verschillen in VAS scores zien, er waren echter geen significante
verschillen in VAS scores of vraag naar extra pijnstilling. Wel was er een trend van
kortere ontsluitingsduur na het plaatsen van de epiduraal te zien bij de thoracale
groep.
Conclusie
We vonden geen significant verschil in door de patiënten gerapporteerde pijnscores in
de twee groepen. Ondanks dat er aanwijzingen zijn dat er verschillen zijn tussen
epidurale katheters op thoracale en lumbale segmenten, zoals een kortere totale
ontsluitingstijd en minder vraag naar extra pijnstilling in de thoracale groep, zijn onze
resultaten niet conclusief. Er is meer onderzoek nodig naar het verschil in
pijnbestrijding en bevallingsuitkomst tussen epidurale analgesie op deze twee
hoogtes.

Abstract 2
Abstract
Introduction
There are indications that the pain parturients experience during labor is one of the
most intense pain experiences known. Epidural analgesia (“an epidural”) is a widely
used central neuraxial block very suitable for perinatal analgesia. The most common
used puncture site for epidural analgesia is in the lumbar region. Given the fact that
most pain experienced during the first phase of labor originates from the low thoracic
(T10- L1) spinal segments, we hypothesized that a epidural catheter placed in the
lower thoracic epidural space would result in better analgesia and less instrumental
assisted vaginal deliveries and caesarian sections than a catheter placed in the lumbar
epidural space.
Methods
To test this hypothesis, two studies were set up. Firstly a retrospective assessment of
all epidurals during labor performed in the Deventer Hospital the past four years, to
assess possible effects on primary labor outcome. Secondly a prospective
observational study in which we included all parturients who received lumbar (L1-L5)
or thoracic (T10-L1) epidural analgesia. We recorded pain using the visual analog
scale (VAS) and the frequency of escape bolus requests during the first phase of
labor.
Results
The retrospective study had usable data from 1172 patients. Ninety-six received an
epidural catheter in the thoracic region and 1096 a lumbar one. We found no
significant differences in incidence of caesarian sections, spontaneous deliveries and
instrumental deliveries. APGAR scores and total labor time were not significantly
different. In the prospective study we included 44 patients. Thirteen had a thoracic
and 31 a lumbar epidural catheter. While graphical representation did look promising,
there were no significant differences in VAS scores, amount of escape bolus requests
and time until escape bolus requests. A trend showing patients in the thoracic epidural
group requiring less time between the puncture and transition to the delivery phase
was seen.
Conclusion
We found no significant difference in VAS pain scores reported by parturients with
epidural catheters on lumbar or thoracic levels. Though there are indications that there
are differences in the degree of analgesia and other labor parameters between the two
epidural level modalities, such as a shorter total labor time and fewer escape bolus
requests in the thoracic group, our results remain inconclusive. More research is
needed to further objectify the difference in pain relief and labor outcome by thoracic
and lumbar epidurals.

Table of Contents 3
Table of Contents 1. Introduction ...................................................................................................................... 4
1.1 Physiology of labor pain .............................................................................................................. 4
1.1.1 Stages of labor ................................................................................................................................................... 4 1.1.2 Pain during labor ............................................................................................................................................. 4
1.2 Epidural anesthesia ..................................................................................................................... 5
1.2.1 Introduction to epidural anesthesia ........................................................................................................... 5 1.2.2 Brief history ........................................................................................................................................................ 5 1.2.3 Anatomy ............................................................................................................................................................... 5 1.2.4 Technique ............................................................................................................................................................ 6 1.2.5 Medication .......................................................................................................................................................... 7 1.2.6 Epidural analgesia during labor ................................................................................................................. 7 1.2.7 Complications .................................................................................................................................................... 7
1.3 Research question ........................................................................................................................ 8
2. Methods ............................................................................................................................ 9 2.1 Retrospective analysis.................................................................................................................. 9
2.1.1 Data collection .................................................................................................................................................. 9 2.1.2 Population and collected data ..................................................................................................................... 9 2.1.3. Statistical Analysis .......................................................................................................................................... 9
2.2 Prospective analysis ................................................................................................................... 10
2.2.1 Design ................................................................................................................................................................ 10 2.2.2 Measurements ................................................................................................................................................. 10 2.2.3 Study population ............................................................................................................................................ 10 2.2.4 Statistical analysis ......................................................................................................................................... 11
3. Results ............................................................................................................................. 12 3.1 Retrospective study results ....................................................................................................... 12
3.1.1 Labor outcome ................................................................................................................................................ 12 3.1.2 Height of the epidural and labor time .................................................................................................... 13 3.1.3 APGAR score after 5 minutes .................................................................................................................... 13
3.2 Results of prospective study ...................................................................................................... 14
3.2.1 Graphic representation ............................................................................................................................... 14 3.2.2.VAS score analysis ........................................................................................................................................ 14 3.2.3 ANOVA for repeated measures ................................................................................................................. 15 3.2.3.Inter-patient variables ................................................................................................................................. 16 3.2.4 Escape boluses................................................................................................................................................ 17
4. Discussion ....................................................................................................................... 18 4.1 Main results ................................................................................................................................ 18
4.2 Results in relation to other studies ........................................................................................... 19
4.3 Thoughts on the study ............................................................................................................... 20
4.3.1 Design of the prospective study ................................................................................................................ 20 4.3.2 Patient enrollment ......................................................................................................................................... 20 4.3.3 Measuring pain .............................................................................................................................................. 20 4.3.4 Parity ................................................................................................................................................................. 21 4.3.5 Sacral roots, sacral sparing ....................................................................................................................... 21 4.3.6 Epidural catheter location and epidural space fluid dynamics ..................................................... 21 4.3.7 Complications ................................................................................................................................................. 22
4.4 Clinical implications .................................................................................................................. 22
5. Conclusion ...................................................................................................................... 23
6. References ....................................................................................................................... 24
7. Acknowledgements ........................................................................................................ 26

Introduction 4
1. Introduction
1.1 Physiology of labor pain
1.1.1 Stages of labor
Labor is divided into three separate stages. (1) The first stage starts with regular
uterine contractions until full cervical dilation is reached. The first stage is further
divided in the “latent” and “active” phase following the increasing speed of cervical
dilation. The second stage starts at full cervical dilation and lasts until the fetus is
born. Finally, the third stage is the delivery of the placenta and placental membranes.
1.1.2 Pain during labor
There are indications that the pain parturients experience during labor is one of the
most intense pain experiences known. According to Melzack this feeling of pain is
only surpassed by the traumatic amputation of a digit or by the complex regional pain
syndrome. (2) During labor, pain increases as contractions increase in strength,
frequency and with advance of cervical dilation. For most patients, the zenith of pain
is reached right before full dilation. (3–5)
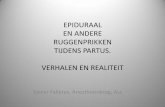
The pain originates from five separate
locations: the uterus, the lower segment of the
uterus, the cervix, the vagina and the
perineum. The thoracic segments T10-T12
and lumbar segment L1 innervate the uterus,
the distal uterus segment and cervical area.
Proximal vaginal innervation is mostly
identical to the innervation of the uterus and
cervical area, the distal part of the vagina and
perineum are innervated through the nervus
pudendus, originating from the sacral spine
segments S2-S4 (See figure 1).
The etiology of pain during labor is
multifactorial. There are parameters of the
delivery itself such as the stage and duration.
But also physical properties of the mother and
child, parity, weight, social-demographic
characteristics, ethnical background, attitude
towards labor and delivery, relatives,
surroundings and support from hospital staff
play a role. (6)
Pharmacological treatment available for labor pain roughly consists of three groups.
These are systemic opioids such as (remi)fentanyl and Meperidine (Demerol), inhaled
anesthetics such as nitrous oxide with oxygen (Entonox) and neuraxial blockades such
Figure 1: Schematic view of pain
pathways during labor. The T10-L1
segments innervate the uterus, distal
uterus segment and cervical area, where
pain is mostly felt during labor. The
nervus pudendus arises from the sacral
segments, innervating most of the vagina
and perineum where pain is mostly felt
during the delivery phase. RD Miller.
Basics of anesthesia, 6th edition.

Introduction 5
as epidural analgesia. Systemic opioids and epidural analgesia are both widely used
(7). Reviews have shown that epidural analgesia during labor is superior to systemic
opiate usage for analgesia and safety, for both mother and child. Inhaled anesthetics
such as nitrous oxide do have some analgesic properties, but are inferior to systemic
opioids and epidural anesthesia. (7,8)
1.2 Epidural anesthesia
1.2.1 Introduction to epidural anesthesia
Epidural analgesia (“an epidural”) is a central neuraxial block very suitable for
perinatal, intraoperative and postoperative analgesia. It can be applied at all levels of
the spinal cord with a single injection or with a catheter in the epidural space with
local anesthetic or in combination with, for example, an opioid.
1.2.2 Brief history
The first practitioners of epidural anesthesia were
Sicard (1872-1929) and Cathelin (1873- 1945)
who, in 1901, injected cocaine in the sacral hiatus
of their patients. Both doctors were unable to
provide epidural anesthesia at higher levels. In
1921 Pagés (1886-1923), a Spanish military
physician, was the first to use a blunt needle and
both acoustic and tactile feedback for puncturing
the ligamentum flavum. He died shortly after
publishing in a Spanish journal. His findings were
never translated or taught to an apprentice and
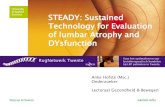
were forgotten. (9) In 1939 Dogliotti (1897-1966)
used local anesthetics for epidural anesthesia and
studied the spread of solutions in the epidural
space (See figure 2). He was the first to use the
“loss of resistance” technique to identify the
epidural space. His textbook describes using
continuous pressure on a syringe filled with saline
as the needle punctures through the ligamentum
flavum into the epidural space. (10) His method to
identify the epidural space is still being used
today.
1.2.3 Anatomy
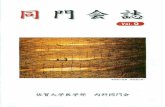
The epidural space is an anatomical space surrounding the dura mater laterally,
anteriorly and posteriorly (See figure 3). Rostrally it is confined by the foramen
magnum and caudally by the ligamentum sacrococcygeum. Anteriorly it is limited by
the ligamentum longitudinale and posteriorly by the laminae vertebrae as well as the
ligamentum flavum connecting these laminae. It contains fatty and connective tissue,
lymphatic vessels, nerve roots, arteries and the epidural venous plexus. Every
vertebral level has its own sub-compartment, though liquids are usually able to
communicate freely through the entire epidural space. (9,11)
Figure 2: Drawing by Doglotti (10)
showing the “Periduralraum”, the
epidural space. Both the median (A)
and paramedian (B) approach are
shown. S.G: Spinal ganglion. Doglotti,
1939: Eine neue Methode der
regionären Anästhesie: Die peridurale
segmentäre anästhesie".

Introduction 6
The spread of any solution in the epidural space is not uniform and this might account
for occasional unpredictable results. (12) Contrary to popular belief, the nerve roots
found in the epidural space vary greatly in size across different individuals. This
might account for the large variation in block quality amongst different patients. (13)
While the sensory dorsal spinal roots are larger then the anterior motor roots, anterior
roots are easier to block. An explanation for this seemingly contradiction is the fact
that the sensory root is composed of a bundle of fibers, resulting in a far larger surface
area on which the local anesthetic works. (14)
1.2.4 Technique
For placement of an epidural catheter, a
needle with a lateral opening such as the
Tuohy needle is used. The patient is
placed in either the lateral decubitus or
sitting position. After identification of the
puncture spot for either median or
paramedian positioning, the needle with
mandarin (to prevent skin plugs being
lodged into the epidural space causing
epidermoid tumors) is inserted and placed
in the ligamentum flavum. In the lumbar
region this ligament is usually found 3.5–6
cm below the skin surface and is 4-6 mm
thick. On thoracic levels it is 3-5 mm
thick. Because the spinal cord ends around
the L1–L2 lumbar segment, there is a
theoretical risk for neurological damage
should there be an accidental dural puncture at thoracic height. In a retrospective
study of 4185 epidurals Giebler et al. found that thoracic epidural punctures are not
associated with an increase in neurological injury. (15) The increased angle of needle
insertion required for thoracic punctures is assumed to add an element of safety to
prevent dural punctures in thoracic epidurals. (9)
There are several ways to identify the epidural space (9). The loss of resistance
method features the use of constant pressure on a special air or saline-filled low-
friction syringe. When the needle enters the epidural space the fluid or air bubble
suddenly flows into the space without resistance. The hanging drop method can be
used because there is a sub atmospheric pressure in the epidural space. A drop of fluid
is placed in the hub of the needle and as the needle progresses through the
ligamentum flavum and thus enters the epidural space, the sub atmospheric pressure
sucks the hanging drop into the needle.
Technological innovations for the identification of the epidural space are also
available. One example is the acoustic puncture assist device, which uses a
continuous infusion to measure the pressure at needlepoint and emits a tone with its
frequency depending on the measurement. (16)
Figure 3: The epidural space and contents of
the dural sac shown at the level of the 4th
lumbar segment. The ligamentum flavum is
also shown posterior to the epidural space.
Millers Anesthesia, RD Miller, 7th edition.

Introduction 7
After the epidural space is identified a special catheter is inserted into the epidural
space as to be able to continuously administer local anesthetics with adjuvants. For
obstetric use the catheter should be inserted only 4-6 cm into the epidural space. (17)
1.2.5 Medication
After insertion of the catheter a small test dose is administered to assess a possible
intrathecal or intravenous catheter placement. Usually this is a small dose of lidocaine
with adrenaline. After administration the patient is monitored for signs of intrathecal
or intravenous injection. (18) Drugs used in epidural analgesia are local anesthetics of
which bupivacaine is the most commonly used. There are additives that can be
combined with local anesthetics to create a better or longer lasting effect or even a
quicker block onset. Commonly used additives are opioids, bicarbonate and alfa-2-
receptorantagonists. (6,19)
1.2.6 Epidural analgesia during labor
For obstetric use 0.0625%, 0.125% and 0.25% concentrations of bupivacaine are
used. A systematic review comparing epidural to systemic or no analgesia shows that
when opioids are used simultaneously a smaller dosage of local anesthetics is
required. (7) The chance of motor block is also reduced using lower concentrations of
the local anesthetic. A possible explanation for the lower required volumes for
obstetric use is the increased abdominal pressure and prominent epidural venous
plexus in parturients. The Dutch guideline for medical pain management during labor
suggests using bupivacaine 0.125% with 8-12 mL per hour continuous epidural
infusion. (6) Obesity, multiparity and more than 7 cm cervical dilation are associated
with a smaller chance of successful analgesia using an epidural. (20)
1.2.7 Complications
Epidural anesthesia during labor is possibly associated with a longer delivery phase,
greater chance of instrumental delivery, hypotension, urinary retention and motor
blockade. (6) Possible complications of an epidural puncture are accidental dural
perforation, intravasal or spinal catheter placement, systemic toxicity and in rare cases
epidural hematoma. Dural perforation resulting in a spinal positioning of the epidural
needle has an overall incidence of 0.5%. Should the epidural dosage of local
anesthetic be injected spinally this can result in a total spinal anesthesia. This is a
severe complication where the patient loses consciousness and ventilatory drive and
will be extremely hypotensive. With adequate support such as mechanical ventilation
and inotropics a complete recovery is likely. (19) Fortunately this complication is
extremely rare.

Introduction 8
1.3 Research question
The guideline for epidural anesthesia during labor in the Netherlands does not specify
at which spinal segment the catheter should be placed. (6) Textbooks usually specify
the L1-L5 segments. (9,11,19) Anesthesiologists are very reluctant to use a thoracic
segment to place an epidural catheter. This is mainly because the dura is thinner in the
thoracic region and the chance of a dural puncture might be greater. However, when
the physiology of pain during the first stage of labor is taken into account, choosing a
lumbar segment for epidural puncture seems illogical. The pain is described as
originating in the T10-L1 segments. In theory placing the catheter in this segment
should result in a better analgesia during this stage. In practice this remains unclear:
we found previous studies that differentiate in epidural puncture height and analgesic
qualities during labor.
In the Deventer Hospital both low-thoracic and lumbar epidurals are used for
analgesia during labor. Because only local anesthetics are used it can be expected that
after the initial bolus the area of analgesia would be the dermatomes according the
level of insertion, which are usually L1-L4. On this level, regular escape boluses are
needed. This is why some anesthesiologists insert the epidural catheter at a low
thoracic level. There has however, to our knowledge, never been a study that analyzes
if any difference between the level of analgesia between low thoracic and lumbar
epidurals for obstetric analgesia exists. This leads to our main research question,
which is formulated as follows: Does the height of the epidural catheter have an
effect on the quality of analgesia?
Hypothesis: “Taking the physiology of labor pain into account we hypothesized that
an epidural placed at a low thoracic segment should result in more stable analgesia
and thus needing less boluses during the first stage of labor. We also hypothesized
that a thoracic placed epidural catheter should result in less caesarian sections and
instrumental deliveries.”
The aim of this study is to assess whether there is a difference in quality of analgesia
between lumbar and low thoracic epidurals. Firstly a retrospective assessment of
epidural block height and primary labor outcome to determine whether the different
modalities show different incidence of caesarian sections or instrumental deliveries.
Secondly, to answer our main research question, the study tries to evaluate levels of
pain with both types of epidural, taking into account the number of rescue boluses.
Evaluating the pain proved impossible with the available retrospective data, so in
order to assess differences in levels of analgesia during the first stage of labor, a
prospective observational trial was set up.

Methods 9
2. Methods
2.1 Retrospective analysis
The retrospective assessment of epidural block height and primary labor outcome was
done to determine whether the different modalities show different incidences of
caesarian sections or instrumental deliveries. Unfortunately we could not gather
reliable information about the quality of the analgesia of these patients.
2.1.1 Data collection
A database of all epidurals performed and
registered by the anesthesiology department
of the Deventer Hospital between 1 January
2009 and 1 October 2012 was used. Data included
were the obstetric epidural itself and known epidural
puncture level. Also, a separate dataset from the
obstetrics department with information of all the
patients was acquired, containing labor start and
outcome, age of parturient, newborn weight, APGAR
score after 5 minutes, puncture time and delivery
time. To avoid human errors in database processing
an SQL script was written to combine the two
separate sets of data into a single database, using the
patient ID and procedure date as identifiers to match
cases. After combining these two datasets the data
were rendered anonymous by removing the patient
name and patient ID number. Excluded were
mismatches (punctures without accompanying labor, deliveries without epidural
puncture data), epidurals for abortions or miscarriages and double punctures.
2.1.2 Population and collected data
The datasets of the anesthesiology and obstetric departments contained 1245 and 1278
entries respectively. After exclusion the resulting dataset contained 1172 patient
entries usable for statistical analysis. (See figure 4) Of the 1172 patients total 96
received a low thoracic epidural and 1096 a lumbar puncture. The average age of the
patients was 29.8 years (17-46). All patients were female. See addendum A for the
table showing variables used in the dataset, data types and outcome possibilities.
2.1.3. Statistical Analysis
Statistical analysis was performed using SPSS 20 for Mac (IBM, 2011, RUG license).
The Pearson Chi-square test was used for nominal variables. For ordinal variables the
Mann-Whitney test was used and continuous variables were analyzed with the
Student T-test. The threshold used for statistical significance was a p-value of <0.05,
p-values between 0.05 and 0.1 were considered as trends.
Obstetric data n=1245
Anesthesiology data n=1278
Figure 4: Flowchart showing the
acquisition of the retrospective
database.
Matched by patient ID and procedure date. Excluded: - Entries with missing data
- Procedure mismatch - Multiple punctures
-Abortions/miscarriages
Final dataset, n=1172
Lumbar: n=1076 Thoracic: n=96

Methods 10
2.2 Prospective analysis
To assess differences in levels of analgesia between the two modalities during first
stage of labor the prospective study was set up.
2.2.1 Design
The aim of the prospective observational part of the
study was to assess levels of analgesia by different
epidural puncture levels. Being observational, this
study did not have any effect on the treatment the
women in labor received. After consulting the
medical ethics committee at the Isala Klinieken in
Zwolle and receiving a waiver showing no
objection, the observational trial started (See
addendum B through D for these documents).
Women receiving epidural analgesia during labor
were asked to participate in the study a short while
after placing the epidural. Upon verbal agreement,
written informed consent was acquired and patients
were included in the study.
Exclusion criteria were patient refusal to enter the
study, inability to give informed consent, epidural
analgesia in case of stillbirth or (medically
indicated) abortion, incomplete or unusable forms,
complications of the puncture or simultaneous use
of systemic opiate analgesia. Epidural puncture
level was solely dependent on the anesthesiologist performing the procedure. Both
delivery room staff and the patient were unaware of the level of the epidural catheter
making it a single-blinded non-randomized observational trial.
2.2.2 Measurements
After patients were included, the puncture level and patient ID were registered.
Lumbar epidural catheter placement was defined as the catheter being in the L1-5
segments, thoracic placement as T10-L1 segments. Back at the delivery room pain
scores were measured hourly by the delivery room staff using the Visual Analog
Scale (VAS). This is a validated, quick and easy to use rating scale suitable to
measure pain. (21,22) After delivery the patient’s file was studied for additional labor
and birth variables: APGAR, total labor time after the puncture, use of rescue boluses,
labor start and outcome.
2.2.3 Study population
During the study, a total of 57 women in labor received epidural analgesia (See figure
5). Three patients were not included because they had an epidural for medically
indicated abortion. Ten patients were unable or unwilling to provide consent. Of the
remaining 44 patients, 40 had usable escape-bolus data and 39 had VAS
measurements usable for analysis.
All epidurals performed during trial period: n=57
Usable for VAS analysis: n=39 Of which: Thoracic: n=11 Lumbar: n=28
Lumbar:
Failure to receive consent: n=10 Miscarriage/abortion: n=3
Unusable data: n=5 (VAS) n=4 (other parameters)
Figure 5: flowchart depicting the
algorithm used for inclusions in the
prospective study.
Total inclusions: n=44

Methods 11
2.2.4 Statistical analysis
Graphic representations include all measurements over time and averages per group
per hour. To compare VAS scores per hour between groups One-Way Analysis of
Variance (ANOVA) tables and T-tests were used, both are suitable to analyze VAS
scores. (23) All measurements between groups over time were analyzed with
Repeated Measures ANOVA.
Other mathematical operations performed to analyze the reported VAS scores were
slope calculation and comparing the maximum and minimal score measured per
patient. Thus reducing the series of measurements per patient to a single number and
enabling easier statistical analysis using the Student T-test.

Results 12
3. Results
3.1 Retrospective study results
Firstly the hypothesis that a difference in epidural segment puncture level could affect
the primary labor outcome was tested, see table 1.
3.1.1 Labor outcome
Of the 634 total spontaneous deliveries, 584 women received lumbar and 50 received
thoracic epidurals. No significant difference has been found in epidural catheter level
and the chance of spontaneous delivery (p=0.680).
Of the 271 caesarean sections, in 246 cases a lumbar epidural catheter was placed and
in 25 cases a thoracic epidural catheter. No significant difference in incidence of
caesarian section for the different epidural modalities was detected (p=0.479).
Because of the low incidence of instrumental deliveries all the instrumental deliveries
were first placed in one group. Resulting in a total of 267 entries, total, 246 of which
were lumbar and 21 of which were thoracic. No statistical significance was found for
the grouped instrumental deliveries (p=0.825).
Of all the instrumental deliveries 182 deliveries were vacuum extractions using a hard
cup, of those 182, 168 had a lumbar epidural and 14 were thoracic. No statistical
significance was found between the groups (p=0.789).
For both the 24 soft cup vacuum extractions and the 39 deliveries using obstetric
forceps, no significant differences were found. Complex deliveries requiring
professional help with the delivery of the head, shoulder or fundal expression had
such a small incidence that no reliable statistical analysis could be performed on the
acquired data.
Labor Outcome
Lumbar
(n= 1076)
Thoracic
(n=96)
Total
(n=1172) p-value
Spontaneous 584 50 634 0.680
C. Section 246 25 271 0.479
Instrumental 246 21 267 0.825
Vacuum (Hard cup) 168 14 182 0.789
Vacuum (Soft cup) 24 3 27 0.576
Forceps 39 2 41 0.431
Help w. head 3 0 3 0.604
Help w. shoulder 8 1 9 0.748
Fundus expression 4 1 5 0.335
Table 1: Labor outcome for all epidural catheters placed on lumbar and thoracic level. Instrumental
deliveries are first calculated as a single group and then divided into their subsequent types. None of the
results were significant (p<0.05).

Results 13
3.1.2 Height of the epidural and labor time
The labor after puncture time is the time in minutes
calculated from the epidural puncture itself until the
delivery. Whilst the mean time for thoracic
epidurals appeared slightly shorter, an independent
samples t-test was performed and revealed that
there was no significant difference in labor time
between thoracic (M=322.2 SD=189) and lumbar
(M=325.7 SD=195) placed epidurals (p=0.869).
3.1.3 APGAR score after 5 minutes
To analyze whether the APGAR score after 5
minutes differs amongst the lumbar and thoracic
epidural groups the Mann-Whitney test for ordinal
variables was used showing no significance
(p=0.710). See table 2 for the distribution of
APGAR scores per group.
APGA
R
Lumbar
(n=1076
)
Thoraci
c (n=96)
10 740 70
9 216 9
8 64 10
7 19 3
6 9 2
5 3 2
4 2 0
3 2 0
2 1 0
1 2 0
0 18 0
Table 2: APGAR score for all
epidural catheters placed on
lumbar and thoracic levels. No
APGAR scores <5 were recorded
for patients with thoracic placed
epidural catheters.

Results 14
3.2 Results of prospective study
Secondly the hypothesis that a difference
in epidural segment puncture level could
result into better pain relief during labor
was investigated.
3.2.1 Graphic representation
A parallel plot of all the VAS
measurements grouped by epidural
catheter level (“Spaghettigram”) revealed
no noticeable differences in VAS scores
(See addendum E).
Figure 6 shows the averaged VAS values
per group for the first five hourly
measurements. Looking at the first three
hours, both groups show increasing VAS
scores. The thoracic group appears to have
higher averaged VAS scores. After 3 hours less patients of the thoracic group are still
in labor (See section 3.2.2).
3.2.2. VAS score analysis
As the average remaining labor time after placing the epidural catheter in this study
was approximately 4.5 hours, pain scores per group were compared at every hour for
the first five hourly measurements, table 3. Whilst the graphical representation of the
average pain for both groups suggests that epidural catheter height does affect the
quality of analgesia, statistical analysis does not support this observation. Analysis
was performed using One-Way ANOVA.
Time
(hours)
Lumbar
(mean, SD, n)
Thoracic
(mean, SD, n)
p-value
1 M: 9.9, SD: 15.5, n=28 M: 9.5, SD: 18.2, n=11 0.945
2 M: 22.2, SD: 23.7, n=27 M: 23.5: SD: 21.9, n=11 0.879
3 M: 36.0, SD: 31.6, n=19 M: 39.3, SD: 31.9, n=10 0.788
4 M: 33.8, SD: 23.3, n=14 M: 39.3, SD: 14.5, n=4 0.686
5 M: 43.5, SD: 34.1, n=14 M: 54.5, SD: 14.9, n=2 0.667
Table 3: Mean and standard deviation (SD) of VAS pains scores per hour grouped
by lumbar, middle and thoracic epidural catheter placement. Measurements were
compared per time unit. Note the decrease in entries after t=3 for thoracic
epidurals. No significant results were found (p<0.05).
(p<0.05).
Figure 6: Plot of the averaged (per hour) reported
VAS scores during the first 5 hourly measurements.

Results 15
3.2.3 ANOVA for repeated measures
A better way to perform statistical analysis
for our model is the ANOVA test for
repeated measures. The VAS score, time
and the different groups are integrated
using this test. As there was a substantial
lower amount of measurements for the
thoracic group after 4 hours the repeated
measurements ANOVA were performed
using three different time windows. All
analyses started at t=1, the end points were
after 3, 4 and 5 hours respectively. The
post-hoc plot of the estimated marginal
means for VAS scores in the first three
hours for both groups for is shown in
figure 7. This plot takes into consideration
each mean in proportion to the unequal
sample size.
Analysis did show significant values for
within-subject tests showing that for both
groups, the VAS scores are affected by a
significant time effect. Between-groups tests checking for possible differences
between the separate groups were not statistically significant, as shown in table 4.
Time
window
Within-subjects
p-value
Between groups
p-value 1-3 < 0.001* 0.455
1-4 0.004* 0.898
1-5 0.08** 0.714
Figure 7: Plot showing the estimated marginal means
of the VAS score for the first three hours for thoracic
and lumbar epidural catheters. Both groups show an
increase of reported pain in time. No significant
differences between the groups were found.
Table 4: Results of Repeated Measures ANOVA to analyze the
different VAS scores amongst the two groups. Analysis performed
using three time windows (in hours). The within-subjects values
show that for the first two time windows the changes in VAS over
time are significant (*). In the third window a trend is visible (**).
Between groups no significant results were found (p<0.05).

Results 16
3.2.3. Inter-patient variables
One of the ways to check the difference in
analgesia between the two modalities is to look at
the highest, lowest and average VAS score for
every patient measurement series. The total
duration after receiving the epidural was also
calculated. Another variable worth interpreting
was the slope of the VAS measurements in
individual patients. The slope was calculated by
calculating the difference between the last and
first measurement divided by the total amount of
measurements, under the assumption that most
pain scores were increasing over time (See table
5).
No significant differences were found between groups for minimum, maximum,
average pain or slope. For the duration of labor after the epidural catheter placement a
trend was found towards thoracic epidurals being associated with shorter total dilation
time after the epidural procedure, see figure 8.
Measure p-value
Average VAS 0.564
Minimum VAS 0.771
Maximum VAS 0.680
Duration 0.076**
VAS Slope 0.219
Figure 8: The average VAS, duration and the VAS increase per hour. Figure 8a shows the thoracic group
having a lower average VAS than the lumbar group, though not statistically significant (p=0.564). In figure
8b we see that the duration of labor after the epidural procedure shows a trend towards being lower in the
thoracic group (p=0.076). The slope of the VAS score over time as seen in figure 8c is greater in the thoracic
group, but not significant (p=0.219).
Table 5: Statistical analysis of the
calculated measures between groups.
None of the results were significant
(p<0.05). However, there was a trend
showing the total labor time after
epidural catheter placement being lower
in the thoracic group (p=0.076).
a b c

Results 17
3.2.4 Escape boluses
Another method to measure the amount of pain in patients is to look at the amount of
requests for additional boluses of local anesthetic through the epidural catheter. In our
study a total of 20 patients (50%) asked for additional analgesia. As shown in table 6,
52% of the patients in the lumbar epidural catheter group requested more additional
analgesia, versus 45% in the thoracic group. This difference is not significant
(p=0.907).
3.2.5 Time until escape bolus requests
The period of time before patients requested
additional analgesia. Plotting the mean time until
requests for analgesia, patients in the thoracic group
appear to request more analgesia sooner than patients
from the other groups, figure 9). The lumbar group
requested after a mean time of 180 minutes, the
thoracic group after a mean of 162 minutes. However,
we found no statistical significance difference was
found (p=0.537).
Escape bolus None Once Twice Total
Lumbar 14 (48%) 10 (35%) 5 (18%) 29
Thoracic 6 (55%) 3 (27%) 2 (18%) 11
Total 20 13 7 40
Figure 9: The average time before
the patient requested additional
analgesia for both groups. The
differences are not significant.
Table 6: Cross tabulation showing escape bolus requests for both
epidural catheter levels. Of the 40 usable entries 20 patients
requested additional pain relief with the epidural catheter in situ.
The maximum amount of requests per patient in both groups was
two.

Discussion 18
4. Discussion
4.1 Main results
The aim of our study was to assess whether a difference in epidural puncture height
during labor would result in better analgesia and less instrumental assisted vaginal
births. Both our hypotheses that a thoracic placed epidural catheter would give better
pain relief during labor as well as less instrumental deliveries were not statistically
proven. While some trends were seen, no statistically significant results were found.
4.1.1 VAS Scores
We did not find any statistically significant differences in VAS scores in between
groups. Based on the visual representations of the measurements one could argue that
the lumbar group offers the best pain relief (see figure 6,7). Our study shows that the
average VAS for both groups appears higher than expected based on available
literature. (2,7,8,24) Besides the variation in epidural catheter segment level we
identified another deviation from regular practice in both groups that could cause this.
By request of the obstetricians the epidural infusion solution does not contain opioids,
despite the national guidelines for epidural analgesia during labor that recommend
doing so. (6)
4.1.2 Escape boluses
The use of escape bolus requests as a measure of pain is logical. If the parturient still
has pain despite the in situ epidural catheter, she asks for more analgesia. Therefore
we see these requests as a measure of acute pain. In our study, the amount of escape
bolus requests in the thoracic group (45%) is lower than in the lumbar group (52%).
This suggests thoracic placed epidurals offer better analgesia. However, taking into
account the time until the request for additional analgesia, the patients in the thoracic
group request escape boluses sooner. This is surprising, because one would expect the
group with the most requests for additional analgesia to have a shorter time until the
first request as well. An explanation can perhaps be found in the average VAS scores
as the thoracic group shows a greater increase in VAS over time while having shorter
total time. This does lead to the question if patients in the thoracic group would have
requested more escape boluses if their labor would have taken longer.
4.1.3 Other measures
After reducing all measurements for every patient down to one single value for easier
statistical analysis something interesting happened. Although not significant, the
average VAS score in the thoracic group was lower. This contradicts the hourly
averaged VAS graph we see in section 3.1.1 where the VAS scores in the thoracic
group are consistently higher. An explanation for this is found in the total time
measured. Some patients with a lumbar epidural had a longer total labor time in which
they also reached prolonged high VAS scores. Because they had high VAS scores for
a longer period the resulting average VAS per patient is greater. In our other analyses
this is not taken into account because we used small time windows such as the first

Discussion 19
three or four hours to ensure enough measurements in both groups for statistical
testing.
The difference in duration of labor remaining after puncture is interesting. In our
retrospective study we found no difference between the groups. In our prospective
study however, there is a visible trend towards thoracic placed deliveries being faster.
This could addressed to the small amount of patients we included with a thoracic
placed epidural catheter or because we did not adjust for other factors that could
speed up the dilation such as oxytocin use.
4.1.4 Caesarian sections and instrumental deliveries
It is known that the chance of an instrumental assisted vaginal birth (instrument
delivery) for parturients with an epidural is increased. (7) Our hypothesis that a higher
placed epidural catheter would result in better remaining motor function during the
expulsion phase and thus in less instrumental deliveries, was not proven. This might
be explained by the relatively small amount of patients with a thoracic epidural
puncture that required instrumental assistance, resulting in an underpowered statistical
analysis.
The incidence of spontaneous delivery and caesarian sections were also compared.
We did not find any significant differences. Were we to find a significant increase in
incidence of caesarian sections or decrease in spontaneous deliveries in the
retrospective study, continuing performing thoracic placed epidurals would be
questionable. Another finding by Anim-Somuah was that the APGAR score is equal
for both the groups with and without epidural analgesia. (7) Our results augment this
by showing that between the two epidural height modalities there is no difference in
APGAR score.
4.2 Results in relation to other studies
The fact that there are no other published studies about differences in epidural
segment level during labor could mean two things. Either there have never been
results interesting enough to publish or the difference has never been studied. In the
United States, for example, where more than 60% of all deliveries are with epidural or
spinal analgesia (25), it is hard to believe that variation of this basic parameter has not
been studied.
Whilst we could not find other studies about pain relief during labor via epidural
analgesia on thoracic and lumbar levels, there are studies that analyze transcutaneous
electrical stimulation (TENS) on thoracic and sacral levels for pain relief during labor.
These locations used in these trials are usually on the T10 and S2 segment, based on
the known pain physiology during labor. (26) A review by Francis (27) on TENS
during labor shows that, for it to be effective, the intensity has to be adjusted
according to the current pain. However, a recent review by Mello et al. shows there is
no evidence that it reduces the use of additional analgesics. (28)The Cochrane review
by Dowswell et al. also shows there is little evidence TENS provides adequate
analgesia. (26)

Discussion 20
4.3 Thoughts on the study
4.3.1 Design of the prospective study
The golden standard for medical research is a randomized controlled trial (RCT). For
the prospective part of our study this would have been our preferred study type.
However because of time restraints it was impossible to set up an RCT with full
medical ethics board approval in the relatively short time period available.
We avoided this by designing a prospective observational study in which we
successfully managed to measure patient pain as well as other variables such as
requests for additional analgesia in both lumbar and thoracic epidural catheter groups.
Because the study was not a double-blinded RCT, our design also introduced a degree
of bias: the administered treatment was not blinded nor randomized. The
anesthesiologist performing the procedure chose the level based purely on personal
preference.
4.3.2 Patient enrollment
The amount of patients that we managed to include for the observational trial was
smaller than expected. We identified multiple causes. Our estimation of the average
amount of epidurals per day could be erroneous. It was based on the patient numbers
in the retrospective study in which we found 1172 epidurals during 1369 days
resulting in ~0.86 per day. In our study we included 44 patients during the 70 days of
inclusion resulting in an average of ~0.63 per day. Based on our calculations we
expected to include around 60 patients. Unfortunately not every patient was able to
provide informed consent. This was mainly due to failure of the attending
anesthesiologist to get the patient to enroll in the study (n=10). Another possible
factor that was not taken into account is the seasonal nature of human birth that
traditionally shows fewer births during winter season. (29)
4.3.3 Measuring pain
How to measure something as subjective and elusive as pain has long been subject to
discussion. Today there are numerous variants of scores that can be used for this
purpose but there is still no consensus for a “standard” measure (30)if one would exist
at all. The visual analog scale (VAS) has been widely used in a diverse adult
populations to evaluate different kinds of pain.(22),
Research evaluating the VAS originates mostly from social sciences. Because of its
historic use, we “automatically” assumed it would be the best score suitable for our
study. However, recent literature shows that both the numeric rating scale (NRS) and
VAS are evenly matched for acute pain. (14,31,32) In our study however, we used the
VAS and dedicated VAS rulers to measure it.
To assess the quality of an epidural block not only the amount of analgesia is
important but the height or spread of the block as well. It is regrettable (but
comprehensible) assessing dermatome height is an accurate and time-consuming
activity that requires patience and accuracy, for which there is no place in the delivery
room. The interval of measuring the VAS score is subject to discussion as well. We
chose to measure pain using the VAS by the hour. Smaller time intervals between

Discussion 21
measurements were preferable, but because of logistic reasons we chose to add the
VAS measurement to the nurses’ series of vital sign measurements. Our VAS
measurement started 1 hour after placing the epidural catheter. If we were to re-design
our study we would have added a VAS check before leaving the anesthesiology
department to establish a baseline for future measurements. Another important factor
we did not measure was the patient satisfaction about pain relief during labor. This
could have given a good indication about whether the analgesia was adequate during
the entire labor process.
4.3.4 Parity
One aspect we did not take into account was the parity of the parturients receiving an
epidural. It is known that women who have their first delivery (nulliparae), experience
the most pain during the first phase of the delivery. (2,4)In the Deventer Hospital the
obstetricians have a policy of mostly proposing epidural analgesia as pain relief to
nulliparae. This might also explain why parturients in both our study groups appear to
show more pain than expected based on available literature. In our study we did not
look at possible differences between multi and nulliparae because it would make the
groups available for statistical analysis even smaller whilst also introducing bias in
patient selection.
4.3.5 Sacral roots, sacral sparing
Taking into account the physiology of labor pain, it seems logical that placing a
thoracic epidural results in better analgesia during the first phase of labor. However,
during the second phase most pain is caused by pressure on the vaginal wall and
perineum, both of which are innervated by the nervus pudendus originating from
sacral nerve roots. (2) In lumbar epidurals sometimes a phenomenon called sacral
sparing occurs: a reduced effect of the local anesthetics in the sacral region. (33) It
remains unclear if a thoracic placed epidural catheter results in a difference in
analgesia during this the second phase, as we did not measure analgesia during the
delivery itself.
4.3.6 Epidural catheter location and epidural space fluid dynamics
As mentioned in our introduction, the location where the epidural catheter eventually
ends up is subject of discussion. In a radiological analysis Beck has shown that even
though the epidural catheter is expected to assume a cranial position only 48% of
catheter tips did end up in a cranial position, 9% caudal and 43% was still near the
insertion site. (34) This makes the assumed location of the epidural catheter somewhat
questionable. However, with current techniques and materials this is the best result
achievable.
It is known that the distribution of the local anesthetic in the epidural space is non-
uniform and difficult to predict. (9,12,13) Additionally, for pregnant women the
distribution is also affected by engorgement of the epidural venous plexus resulting in
increased pressure in the epidural space. (9) Compared to normal physiology a
smaller volume of solution might result in equivalent spread.
Another point of discussion is whether there is an actual difference between the
maximum heights reached by the injected solution between the two epidural groups. It

Discussion 22
is known that epidural infusions tend to migrate to higher thoracic segment levels.
(9,19) Taking this into account, perhaps it would have been wise to have used smaller
solution volumes for the thoracic epidurals. This would be to avoid injecting so much
volume in the epidural space that any difference made by diversifying the puncture
location is nullified by the wash of solution injected. We acknowledge that future
research towards better understanding of the behavior of solutions in the epidural
space in both parturients and normal patients is invaluable.
4.3.7 Complications
As Sprigge and Harper show in a survey of 18333 epidural punctures, the chance of
an accidental dural perforation is 0.91%. (35) In our prospective study no dural
punctures were recorded in either group. In the Deventer Hospital delivery rooms it is
custom to disable the continuous epidural infusion once the expulsion phase begins
and the parturient has to push. In the past, motor function was often completely
blocked rendering the women unable to do so. This was most likely due to high
concentrations of local anesthetic. In our study only one block was described as too
high, remarkably in the group with lumbar punctures. An explanation might be found
within the individual patient characteristics such as the body mass index. No complete
motor blocks during the delivery phase were registered. There were no other
anesthesia-associated complications in the study.
4.4 Clinical implications
Our results show a few trends in favor of thoracically placed epidurals and some in
favor of standard lumbar epidurals. But they are inconclusive overall. While the local
anesthesiologists acknowledge that there appear to be certain advantages in using a
thoracically placed epidural, the current standard treatment will probably not change
until more proof is found that epidural catheters on a thoracic level provide better pain
relief during labor.
A possible way for this is continuing the current prospective study. But as mentioned
above, there are downsides to not having a full-fledged RCT. We advise starting a
continuation of this study where patients are randomized between T10-L1 and L1-L5
segment punctures. Because of the relatively small amount of requests for epidural
anesthesia during labor in the Deventer Hospital, it might be wise to involve multiple
other hospitals to reach acceptable inclusion numbers.

Conclusion 23
5. Conclusion
Epidural analgesia is a safe, effective and reliable method of pain relief during clinical
deliveries.
We were unable to verify our hypothesis that thoracic epidural anesthesia during the
first phase of labor results in better pain relief and less instrumental deliveries. We
found no significant difference in analgesia using VAS scores reported by parturients
with epidural catheters on lumbar or thoracic levels. The number of escape boluses
was higher in the group with lumbar placed epidural catheter, though not statistically
significant. The thoracic group requested escape boluses considerably sooner than the
lumbar group.
In our study, the difference in puncture height of the epidural catheter did not affect
the incidence of spontaneous delivery, caesarian sections or instrumental deliveries.
APGAR scores of the newborn were not significantly different. The labor time after
the epidural puncture was shorter for patients in the thoracic group during the
prospective study, though we did not see this difference in the retrospective study.
More research is needed to further objectify the difference in pain relief by thoracic
and lumbar epidurals and the properties of fluids injected the epidural space before
clinical practice will change.

References 24
6. References
1. Friedman E. The graphic analysis of labor. American Journal of Obstetrics and Gynecology.
1954;(68(6):):1568.
2. Melzack R, Kinch R, Dobkin P. Severity of labour pain influence of physical as well as
psychologic variables. Canadian Medical Association Journal. 1984;130(5):579–84.
3. Corli O, Grossi E, Roma G, Battagliarin G. Correlation between subjective labour pain and
uterine contractions: a clinical study. Pain. 1986 Jul;26(1):53–60.
4. Lowe N. The nature of labor pain. American Journal of Obstetrics and Gynecology. 2002
May;186(5):S16–S24.
5. Brown ST, Campbell D, Kurtz a. Characteristics of labor pain at two stages of cervical dilation.
Pain. 1989 Sep;38(3):289–95.
6. Nederlandse Vereniging voor Anesthesiologie en Nederlandse Vereniging voor Obstetrie en
Gynaecologie. Richtlijn medicamenteuze pijnbehandeling tijdens de bevalling. 2008.
7. Anim-Somuah M. Epidural versus non-epidural or no analgesia in labour. The Cochrane
Collaboration. 2011;(12).
8. Leighton B. The effects of epidural analgesia on labor, maternal, and neonatal outcomes: A
systematic review*1. American Journal of Obstetrics and Gynecology. 2002 May;186(5):S69–
S77.
9. Miller R. Miller’s Anesthesia 7th edition. 7th ed. Churchill Livingstone; 2009.
10. Dogliotti A. Eine neue Methode der regionären Anästhesie: Die peridurale segmentäre
anästhesie". Zentralblatt fuer Chirurgie. 1931;58:3141–5.
11. Miller R, Pardo M. Basics of Anesthesia. 6th ed. Elsevier Saunders; 2011.
12. Hogan Q. Distribution of solution in the epidural space: Examination by cryomicrotome
section. Regional Anesthesia and Pain Medicine. 2002 Mar;27(2):150–6.
13. Hogan Q, Toth J. Anatomy of soft tissues of the spinal canal. Regional anesthesia and pain
medicine. 1999;
14. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales.
Pain. International Association for the Study of Pain; 2011 Oct;152(10):2399–404.
15. Giebler R, Scherer R, Peters J. Incidence of Neurologic Complications Related to Thoracic
Epidural Catheterization. Anesthesiology. 1997;
16. Lechner TJM, Van Wijk MGF, Maas a JJ. Clinical results with a new acoustic device to
identify the epidural space. Anaesthesia. 2002 Aug;57(8):768–72.
17. Beilin Y, Bernstein HH, Zucker-Pinchoff B. The optimal distance that a multiorifice epidural
catheter should be threaded into the epidural space. Anesthesia and analgesia. 1995
Aug;81(2):301–4.
18. Mhyre JM, Greenfield MLVH, Tsen LC, Polley LS. A systematic review of randomized
controlled trials that evaluate strategies to avoid epidural vein cannulation during obstetric
epidural catheter placement. Anesthesia and analgesia. 2009 Apr;108(4):1232–42.
19. Noordzij P, Klimek M, Stamer A. Klinische Anesthesiologie. 2nd ed. De Tijdstroom; 2012.
20. Agaram R, Douglas MJ, McTaggart R a, Gunka V. Inadequate pain relief with labor epidurals:
a multivariate analysis of associated factors. International journal of obstetric anesthesia.
Elsevier Ltd; 2009 Jan;18(1):10–4.

References 25
21. Bijur P, Silver W, Gallagher E. Reliability of the Visual Analog Scale for Measurement of
Acute Pain. Academic emergency …. 2008;8(12):1153–7.
22. Hawker G a, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale
for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire
(MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS),
Short Form-36 Bodily Pain Scale (SF. Arthritis care & research. 2011 Nov;63 Suppl
1(November):S240–52.
23. Dexter F, Chestnut D. Analysis of Statistical Tests to Compare Visual Analog Scale
Measurements among Groups. Anesthesiology. 1995;
24. Melzack R. The myth of painless childbirth (the John J. Bonica lecture). Pain. 1984
Aug;19(4):321–37.
25. Osterman MJK. National Vital Statistics Reports Epidural and Spinal Anesthesia Use During
Labor : 27-state Reporting Area , 2008. U.S. DEPARTMENT OF HEALTH AND HUMAN
SERVICES. 2011;59(5):1–14.
26. Dowswell T, Bedwell C. Transcutaneous electrical nerve stimulation (TENS) for pain
management in labour. The Cochrane Collaboration. 2009;(9).
27. Francis R. TENS (Transcutaneous electrical nerve stimulation) for labour pain. The practising
midwife. 2012;15(5):20–4.
28. Mello LFD, Nóbrega LF, Lemos A. Transcutaneous electrical stimulation for pain relief during
labor: a systematic review and meta-analysis. Revista brasileira de fisioterapia (São Carlos
(São Paulo, Brazil)). 2011;15(3):175–84.
29. Bobak M, Gjonca a. The seasonality of live birth is strongly influenced by socio-demographic
factors. Human reproduction (Oxford, England). 2001 Jul;16(7):1512–7.
30. Powell RA, Downing J, Ddungu H, Mwangi-powell FN. Chapter 10 Pain History and Pain
Assessment Are there key elements to the pain assessment process. 2010;
31. Breivik H, Borchgrevink PC, Allen SM, Rosseland L a, Romundstad L, Hals EKB, et al.
Assessment of pain. British journal of anaesthesia. 2008 Jul;101(1):17–24.
32. Hjermstad MJ, Fayers PM, Haugen DF, Caraceni A, Hanks GW, Loge JH, et al. Studies
comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for
assessment of pain intensity in adults: a systematic literature review. Journal of pain and
symptom management. Elsevier Inc; 2011 Jun;41(6):1073–93.
33. Arendt K, Segal S. Why Epidurals Do Not Always Work. Reviews in Obstetrics and
Gynecology. 2008;1(2):49–55.
34. Beck H. The effect of the Tuohy cannula on the positioning of an epidural catheter. A
radiologic analysis of the location of 175 peridural catheters. Reg Anaesth. 1990 Jan
1;39(4):418–20.
35. Sprigge JS, Harper SJ. Accidental dural puncture and post dural puncture headache in obstetric
anaesthesia: presentation and management: a 23-year survey in a district general hospital.
Anaesthesia. 2008 Jan;63(1):36–43.

Acknowledgements 26
7. Acknowledgements I would like to thank my mentor, Jan-Hein Cobben for his help in devising the study
subject as well as his help during the process of designing, collecting data and writing
the report. Secondly I would like to acknowledge the assistance of all the
anesthesiologists in the Deventer Hospital for their work to include patients.
My gratitude for the gynecologists for their help setting up the study and most
important of all, I would like to thank the delivery room staff for their valuable help
with the measurements, without them the study would not have been possible.
Finally I would like to thank my colleagues for all their support, help with
proofreading, valuable insights and all the coffee breaks.
Jon Gutteling
Deventer,
March 28, 2013

Addendum 27
ADDENDUM
Table of Contents
A. Database parameters ........................................................................................................ 28
B. Ethics board waiver .......................................................................................................... 29
B: Patient information letter ................................................................................................ 30
B: Consent form ..................................................................................................................... 33
C. “Spaghettigram”/ Parallel VAS plot ............................................................................... 34
Low thoracic versus lumbar epidural anesthesia during the first phase of labor

Addendum 28
A. Database parameters
Name Type Possibilities
IP Code/String Age Continuous In years
Date Unix time stamp Level Dichotomous 0 = Lumbar, 1 = Thoracic
VAS* Ordinal 0-100, per hour
Escape bolus* Scale Amount of requests
Escape bolus- time* Continuous In minutes
Start of labor Categorical 1 = Spontaneous contractions
2 = Spontaneous rupture membranes
3 = Spontaneous contractions + rupture of membranes
4 = Stimulation after spontaneous rupture of membranes
5 = Amniotomy
6 = Chemical
7 = Amniotomy + chemical
End point Categorical 1 = Spontaneous partus
2 = Caesarian section
3 = Vacuum extraction (hard cup)
4 = Vacuum extraction (soft cup)
5 = Forcipal extraction
6 = Other
Time Continuous In minutes
APGAR 5 Ordinal 0-10
Gemelli Dichotomous 0,1

Addendum 29
B. Ethics board waiver

Addendum 30
C: Patient information letter
(According to CCMO model letter)
Onderzoek naar verschil in effect van hoge en lage ruggenprik
tijdens de bevalling
Deventer, 25-09-2012
Geachte mevrouw,
In het Deventer ziekenhuis doen wij medisch-wetenschappelijk onderzoek naar welke
methode van ruggenprik de beste pijnbestrijding geeft tijdens de ontsluitingsfase van de
bevalling. Wij vragen u vriendelijk en vrijblijvend om mee te doen aan dit onderzoek.
Om een weloverwogen beslissing te kunnen maken vragen wij u om deze informatiebrief
en de algemene brochure rustig door te lezen en te bespreken met uw naasten.
Als u na het lezen van deze informatie nog vragen heeft kunt u contact opnemen met de
onderzoeker of met een onafhankelijke arts. Op bladzijde 3 vindt u de contactgegevens.
Misschien dat u het gevoel heeft dat u op dit moment niet in staat bent een
bewuste/weldoordachte keuze te maken. In dat geval kunt u altijd achteraf (na uw
bevalling) aangeven dat uw gegevens uit het onderzoek verwijderd moeten worden.
Wat is het doel van het onderzoek? Door dit onderzoek krijgen artsen een beeld van welke soort ruggenprik de beste
pijnbestrijding geeft tijdens de ontsluitingsfase van de bevalling. Dit heeft mogelijk
gevolgen voor de manier waarop toekomstige patiënten behandeld worden. Wij zijn
vooral geïnteresseerd in mate van pijnstilling na de ruggenprik.
Welke behandeling wordt onderzocht? Wij onderzoeken of de hoogte van de ruggenprik invloed heeft op de mate van pijn die u
ervaart. In het Deventer Ziekenhuis worden twee verschillende hoogtes (onderrug of
hoger) met goed resultaat gegeven. Deze hoogte hangt af van de voorkeur en ervaring
van diegene die prikt.
Hoe wordt het onderzoek uitgevoerd? Alle vrouwen die tussen 1 december 2012 en 1 maart 2013 tijdens de ontsluitingsfase van
de bevalling een ruggenprik krijgen, zullen worden gevraagd om mee te doen aan dit
onderzoek. De onderzoeker of verpleegkundige zal bij iedereen die een ruggenprik heeft
gekregen elk uur een pijnscore afnemen.
Wat wordt er van u verwacht? Meedoen met dit onderzoek zal voor u betekenen dat er na het krijgen van de ruggenprik

Addendum 31
elk uur iemand langskomt op de verloskamer. Dit kan de hoofdonderzoeker zijn of een
verpleegkundige. Deze persoon zal u vragen hoeveel pijn u op dat moment ervaart. Dit
zal gebeuren met een speciale pijnlineaal, waarop u aanwijst hoeveel pijn u heeft. Dit
kost ongeveer één minuut per keer.
Wat is er meer of anders dan de normale behandeling? U krijgt de normale behandeling: een ruggenprik in de onderrug of hoger. Deze hoogte
hangt af van de voorkeur en ervaring van diegene die prikt. Het onderzoek heeft geen
invloed op de soort behandeling die u krijgt. Het onderzoek betekent voor u dat er na het
krijgen van de ruggenprik een onderzoeker langskomt om te vragen hoeveel pijn u heeft.
Wat zijn de mogelijke voor- en nadelen van deelname aan dit onderzoek? U heeft zelf geen voordeel van deelname aan dit onderzoek. Voor de toekomst kan het
onderzoek wel nuttige gegevens opleveren.Het nadeel is dat er tijdens de bevalling een
aantal keer iemand komt vragen hoeveel pijn u heeft.
Wat gebeurt er als u niet wenst deel te nemen aan dit onderzoek? U beslist zelf of u meedoet aan het onderzoek. Deelname is vrijwillig. Als u besluit niet
mee te doen, hoeft u verder niets te doen. U hoeft niets te tekenen. U hoeft ook niet te
zeggen waarom u niet wilt meedoen. U krijgt de behandeling die u anders ook zou
krijgen. Als u wel meedoet, kunt u zich altijd bedenken en toch stoppen. Ook tijdens het
onderzoek.
Wat gebeurt er als het onderzoek is afgelopen? Deelname aan het onderzoek eindigt na uw bezoek aan het Deventer Ziekenhuis.
Deelname aan het onderzoek wordt voortijdig beëindigd indien u dit zelf besluit of de
onderzoeker het noodzakelijk acht omdat uw veiligheid of gezondheid in gevaar is. Er
zijn geen risico’s aan tussentijdse beëindiging van het onderzoek voor uw gezondheid.
Uw gezondheid loopt geen gevaar als het onderzoek tussentijds beëindigd wordt.
Bent u verzekerd wanneer u aan het onderzoek meedoet? Omdat de behandeling bij dit onderzoek niet afwijkt van de normale behandeling is er
géén aparte verzekering afgesloten. U valt onder de normale verzekering die u en het
ziekenhuis hebben afgesloten.
Wat gebeurt er met uw gegevens? Uw gegevens zijn vertrouwelijk en zullen anoniem worden verwerkt. Alleen de
informatie die van belang is voor het onderzoek zal worden bekeken. Uw privacy en
medische gegevens zullen volgens de geldende regels worden behandeld en bewaakt. De
resultaten van de vragenlijsten worden in een computerbestand opgeslagen. Gegevens
zoals uw naam en geboortedatum worden vervangen door een codenummer. Alleen dat
codenummer zal worden gebruikt in documentatie of rapporten over dit onderzoek.
Alleen de hoofdonderzoekers weten welke code u heeft. Alle formulieren waar uw
persoonsgegevens op staan worden na afloop van het onderzoek vernietigd. De
hoofdonderzoeker kan bij een vervolgonderzoek uw gegevens terughalen via een
bepaalde “sleutel”.

Addendum 32
Zijn er extra kosten wanneer u besluit aan dit onderzoek mee te doen? Er zijn geen extra kosten verbonden aan deelname aan dit onderzoek.
Welke medisch-ethische toetsingscommissie heeft dit onderzoek
goedgekeurd? In overleg met toetsingscommissie Isala Klinieken Zwolle is besloten dat het onderzoek
niet medisch ethisch getoetst hoefde te worden. Wel zijn deze informatiebrief en het
toestemmingsformulier geaccordeerd door de METC.
Wilt u verder nog iets weten? Voor vragen kunt u altijd contact opnemen met hoofdonderzoeker: Dhr. J. Gutteling via
e-mail ([email protected]) of telefonisch (0570-53 53 53 doorverbinden met nummer
2869). De onafhankelijk arts is P.J.Q. van der Linden, gynaecoloog. Bereikbaar via
email: [email protected].
Bij klachten voor, tijdens of na het onderzoek, kunt u contact opnemen met de
klachtencommissie van het Deventer Ziekenhuis via tel: 0570 – 53 61 44.
Bijlagen:
Algemene brochure medisch-wetenschappelijk onderzoek met mensen
Toestemmingsverklaring
Met vriendelijke groet,
Dhr. J. Gutteling
Hoofdonderzoeker:
J. Gutteling BSc, Afdeling Anesthesiologie
Deventer Ziekenhuis
Nico Bolkesteinlaan 75
7416 SE Deventer
Tel: 0570-53 53 53 intern 2869
e-mail: [email protected]
Begeleider:
Dr. J.M.G. Cobben, Anesthesioloog
Deventer Ziekenhuis
Nico Bolkesteinlaan 75
7416 SE Deventer

Addendum 33
D: Consent form
(According to CCMO model consent form)

Addendum 34
E. Parallel plot of VAS (“Spaghettigram”)