IMPLEMENTATIE ESC GUIDELINES 2013 LIPIDEN IN...
54
• Dr. Celen Hendrik • Cardiologie • Heilig Hart Ziekenhuis Leuven • 6/3/2013 IMPLEMENTATIE ESC GUIDELINES 2013 LIPIDEN IN PRAKTIJK Casuistiek
Transcript of IMPLEMENTATIE ESC GUIDELINES 2013 LIPIDEN IN...
• Dr. Celen Hendrik
• Cardiologie
• Heilig Hart Ziekenhuis Leuven
• 6/3/2013
IMPLEMENTATIE ESC GUIDELINES 2013 LIPIDEN IN PRAKTIJK
Casuistiek
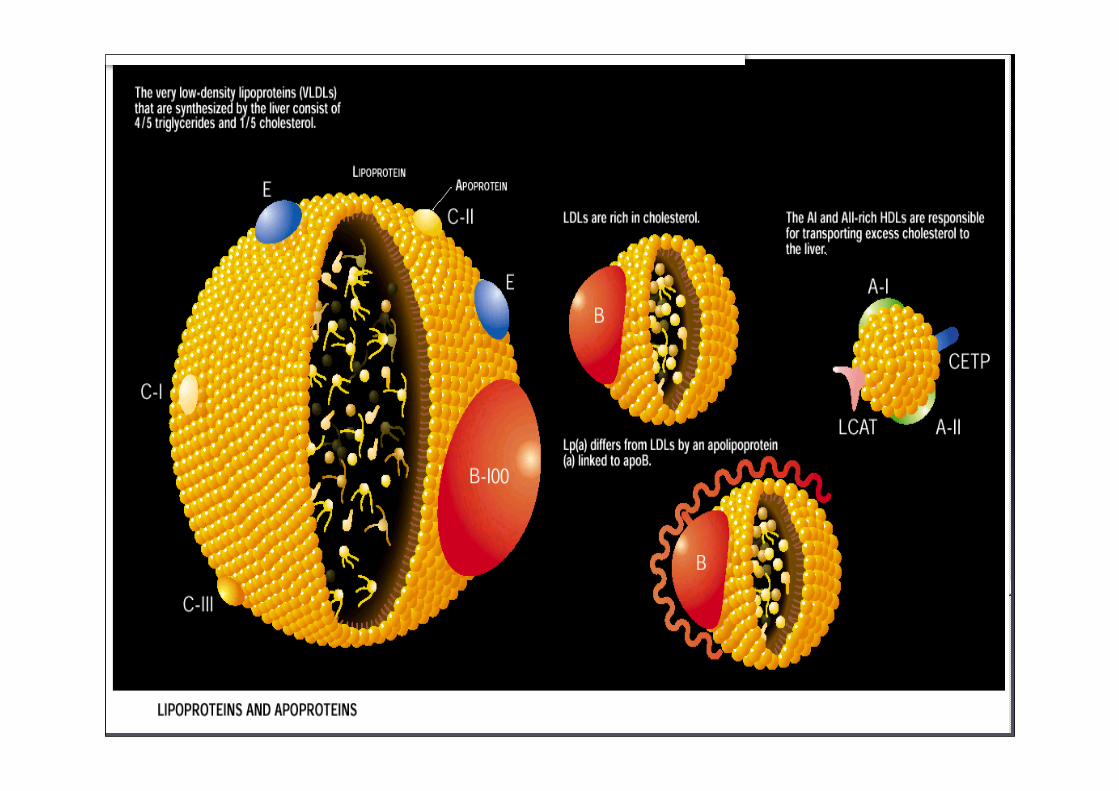
• Risicofactoren, Lipoproteïnes en Atherogenese
• Werkingsmechanisme van hyolipimiërende farmaca
• Richtlijnen
• Casuistiek
IMPLEMENTATIE ESC GUIDELINES LIPIDEN
2010 IN PRAKTIJK
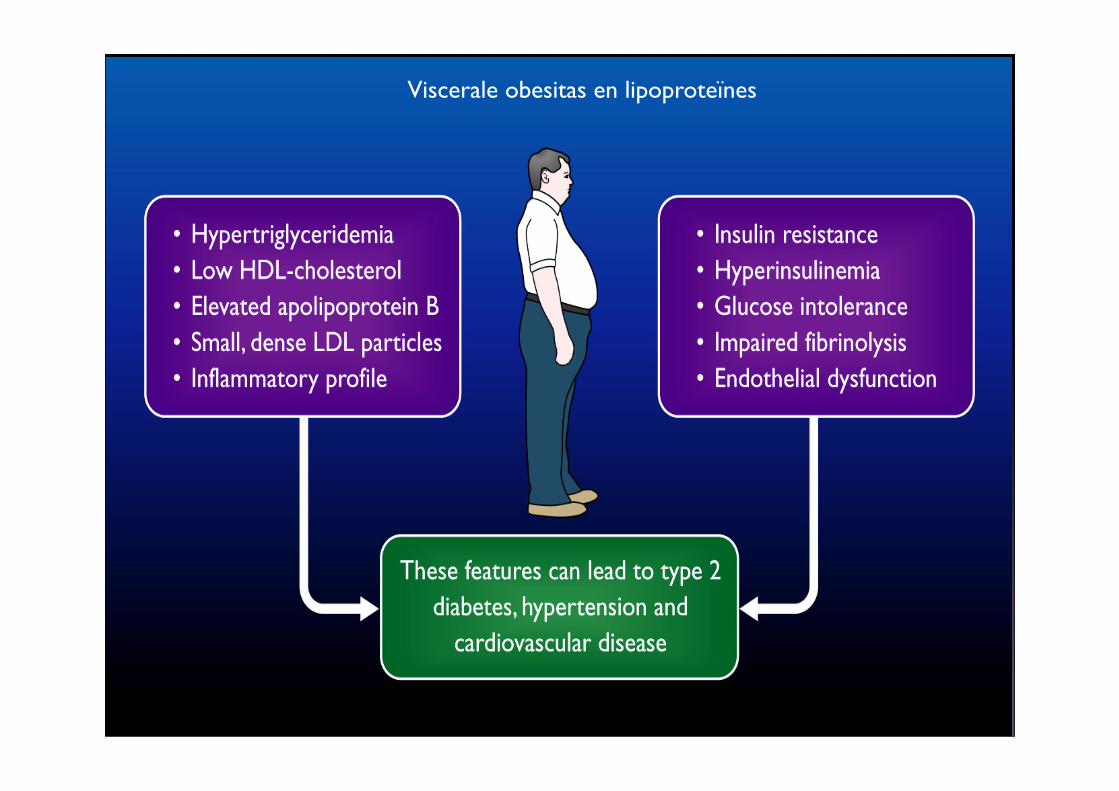
Viscerale obesitas en lipoproteïnes
0
25
50
75
100
125
150
≤ 204 205-234
235-264
265-294
≥ 295
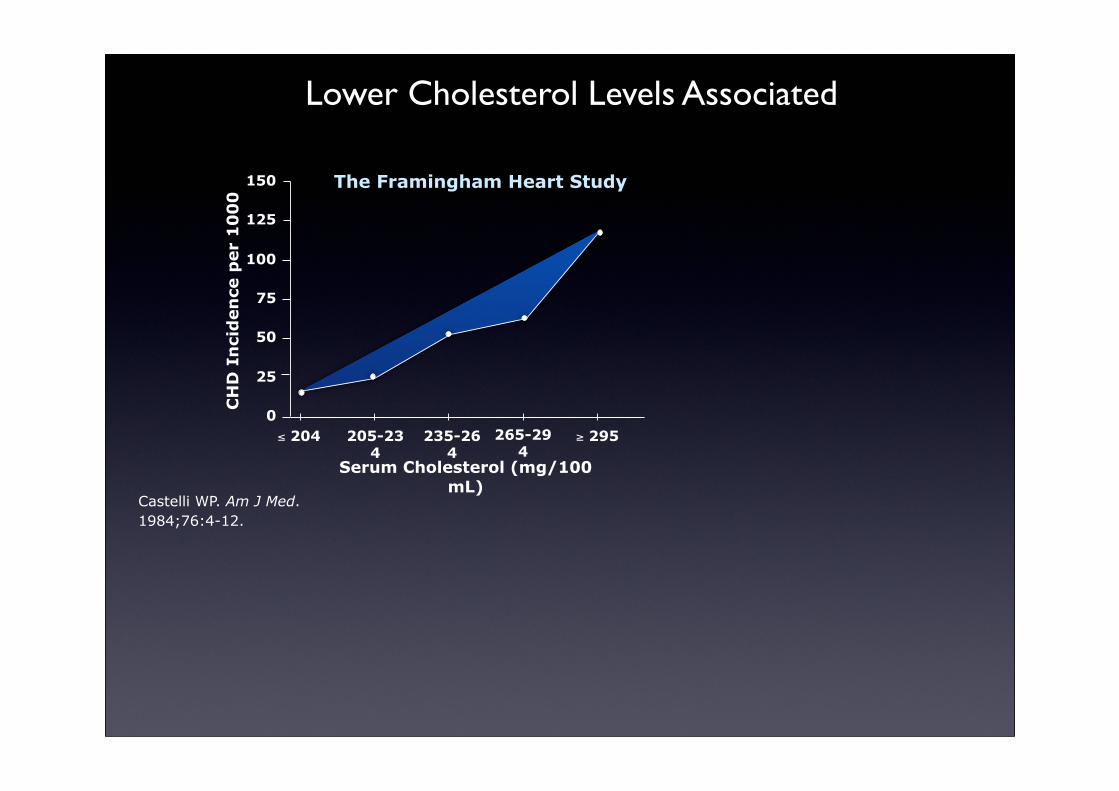
Castelli WP. Am J Med. 1984;76:4-12.
CH
D I
nci
den
ce p
er
10
00
Serum Cholesterol (mg/100 mL)
The Framingham Heart Study
Lower Cholesterol Levels Associated
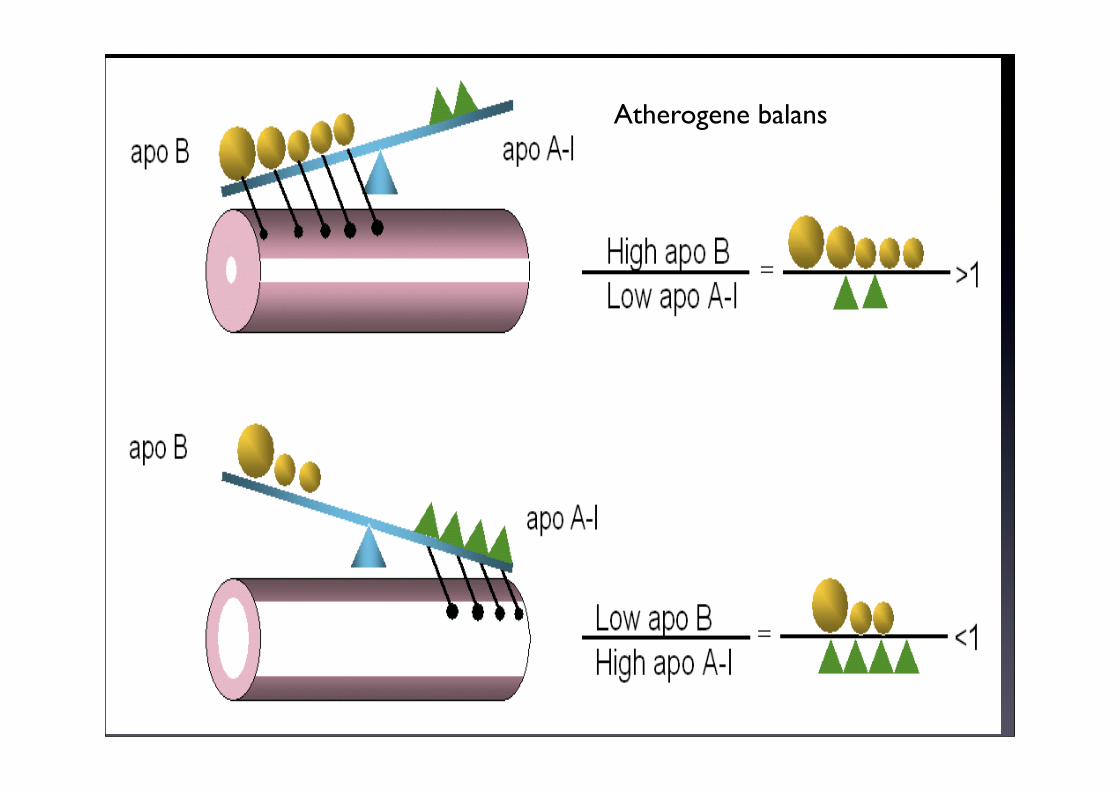
Atherogene balans
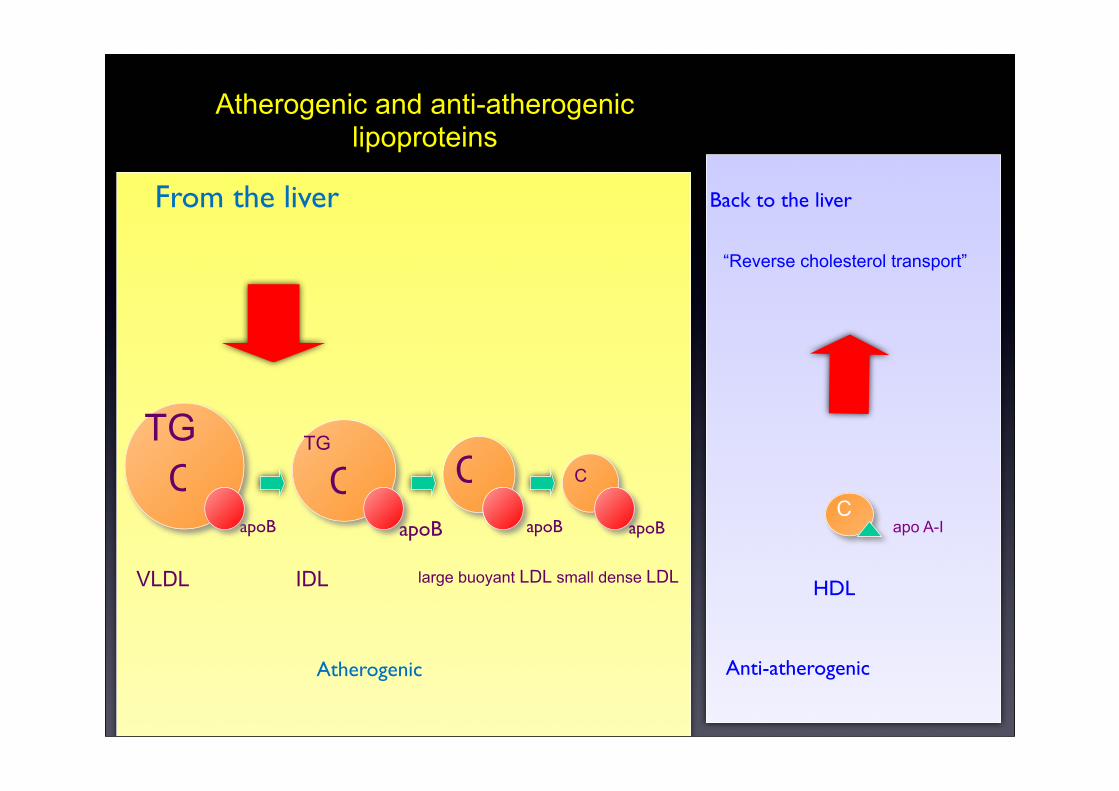
From the liver
Capo A-I
HDL
Back to the liver
“Reverse cholesterol transport”
Atherogenic Anti-atherogenic
apoB
VLDL IDL large buoyant LDL
apoB apoB
TG
C C
small dense LDL
apoB
C
TGC
Atherogenic and anti-atherogenic lipoproteins
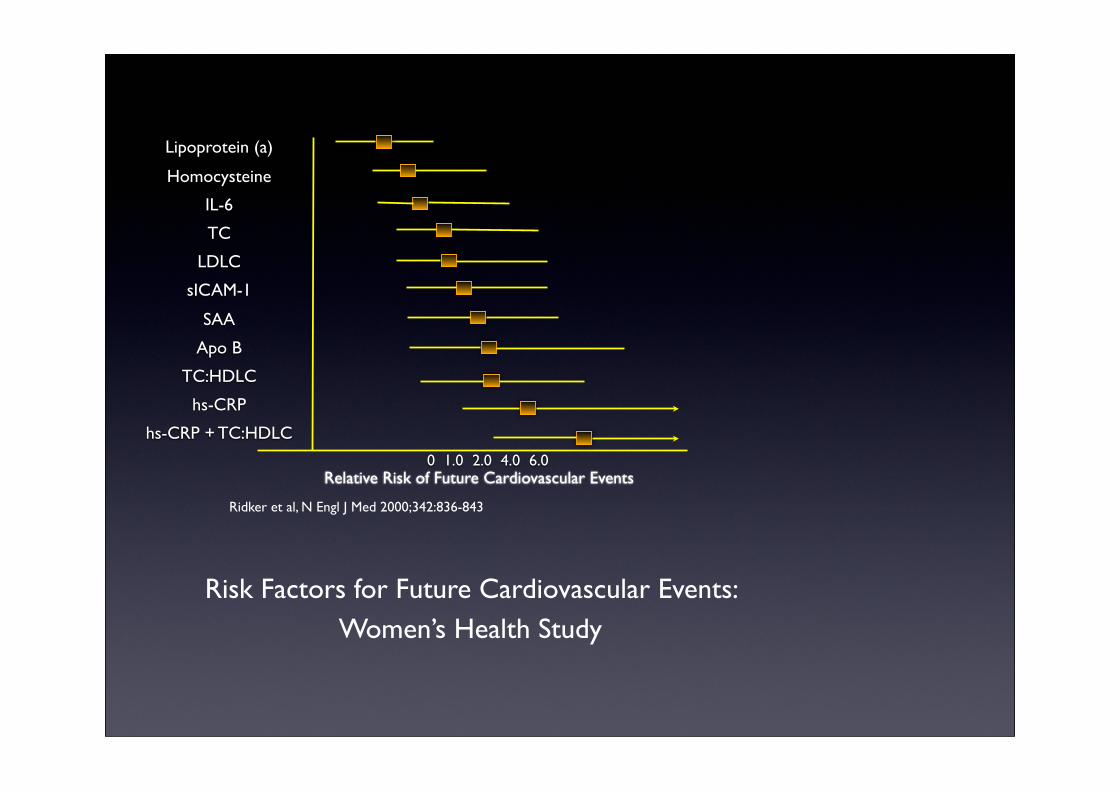
0 1.0 2.0 4.0 6.0
Lipoprotein (a)
Homocysteine
IL-6
TC
LDLC
sICAM-1
SAA
Apo B
TC:HDLC
hs-CRP
hs-CRP + TC:HDLC
Relative Risk of Future Cardiovascular Events
Ridker et al, N Engl J Med 2000;342:836-843
Risk Factors for Future Cardiovascular Events: Women’s Health Study
• Hoeksteen van de lipidentherapie
• Associatie met pathogenese atherosclerose en cardiale eindpunten
• 10% stijging resulteert in 20% stijging in CVrisico1
• bevat vooral cholesterolester en veel lipoproteine B
• opname door hepatocyten en non hepatisch weefsel
• dense smalle LDL cholesterolpartikels
1. Wood D et al. Atherosclerosis. 1998;140:199-270.2. National Centre for Health Statistics. National Health and Nutrition Examination Survey (III), 1994. 3. Jacobson TA, et al. Arch Intern Med. 2000;160:1361-1369.
LDL Cholesterol
50
Secondary Prevention
Primary Prevention
CARE-Rx
4S-Rx
LIPID-Rx
CARE-PL
LIPID-PL
4S-PL
AFCAPS-RxAFCAPS-PL
WOSCOPS-RxWOSCOPS-PL
70 90 110 130 150 170 190 210
0
5
10
15
20
25
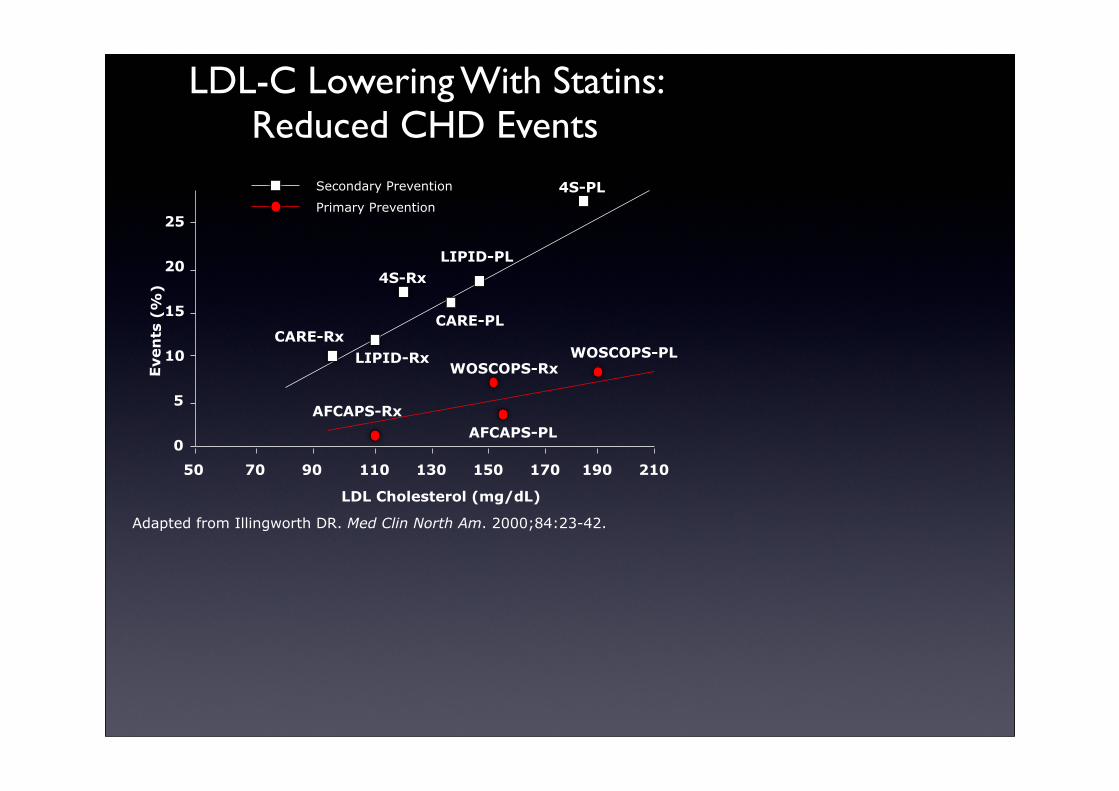
Adapted from Illingworth DR. Med Clin North Am. 2000;84:23-42.
LDL Cholesterol (mg/dL)
Eve
nts
(%
)
LDL-C Lowering With Statins: Reduced CHD Events
• Laag HDL cholesterol onafhankelijke predictor voor CHD1
• Hoe lager het HDL-cholesterol, hoe hoger risico CHD2
• Laag HDL is gedefinieerd als < 40 mg/dL1
• HDL cholesterol is laag als triglyceridengehalte hoog is
1. NCEP, Adult Treatment Panel III. JAMA. 2001;285:2486-2497. 2. Wood D, et al. Atherosclerosis. 1998;140:199-270.
HDL Cholesterol
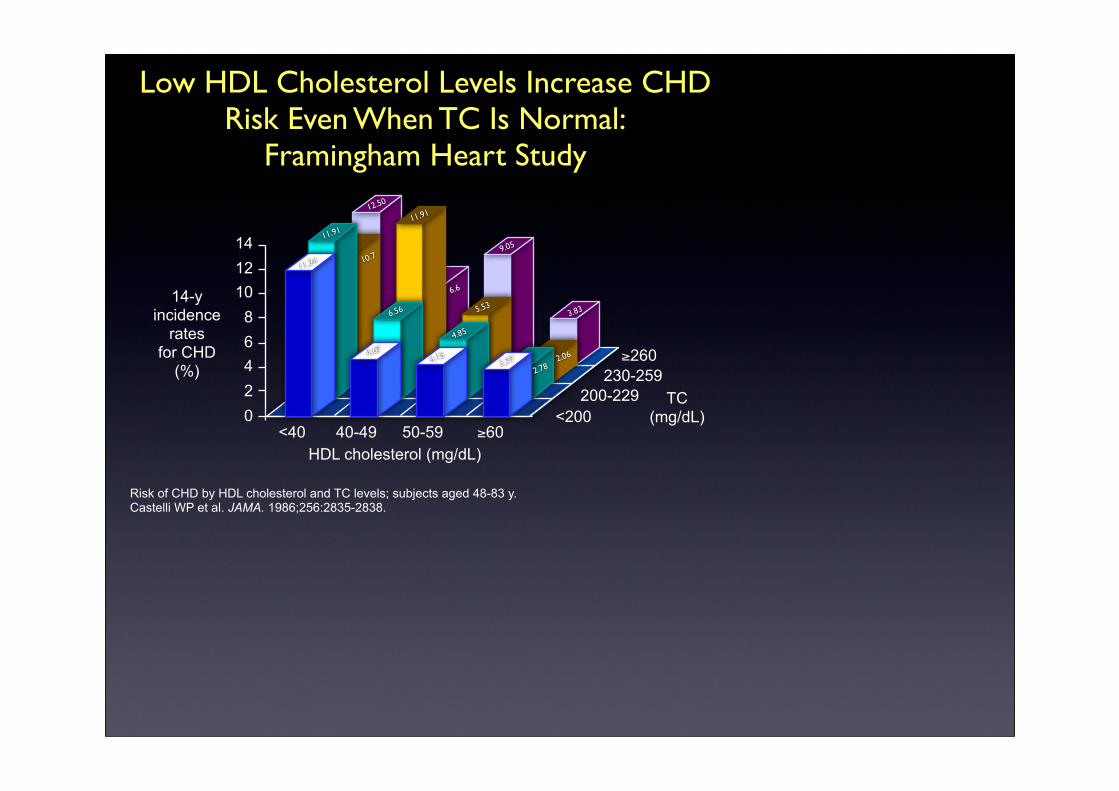
Low HDL Cholesterol Levels Increase CHD Risk Even When TC Is Normal:
Framingham Heart Study
Risk of CHD by HDL cholesterol and TC levels; subjects aged 48-83 y.Castelli WP et al. JAMA. 1986;256:2835-2838.
02468
101214
<40 40-49 50-59 ≥60<200
230-259200-229
≥260
HDL cholesterol (mg/dL)
TC(mg/dL)
14-y incidence
ratesfor CHD
(%)
11.24
11.91
12.50
11.91
6.56
4.67
9.05
5.53
4.85
4.153.77
2.782.06
3.83
10.7
6.6
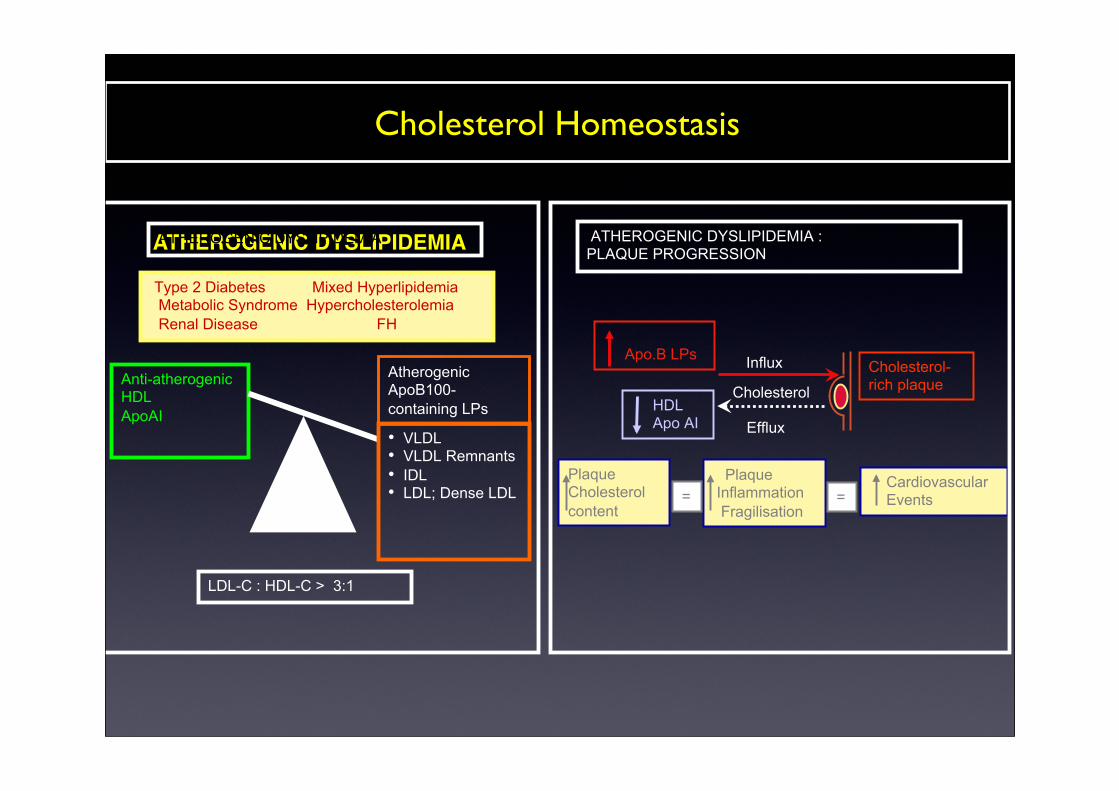
Cholesterol Homeostasis
ATHEROGENIC DYSLIPIDEMIA
Anti-atherogenic HDL ApoAI
ATHEROGENIC DYSLIPIDEMIA
Atherogenic ApoB100-containing LPs
Type 2 Diabetes Mixed Hyperlipidemia Metabolic Syndrome Hypercholesterolemia Renal Disease FH
• VLDL • VLDL Remnants • IDL • LDL; Dense LDL
LDL-C : HDL-C > 3:1
Efflux
Influx Cholesterol-rich plaque
Plaque Cholesterol content
Plaque Inflammation Fragilisation
= = Cardiovascular Events
Apo.B LPs
HDL Apo AI
ATHEROGENIC DYSLIPIDEMIA : PLAQUE PROGRESSION
Cholesterol
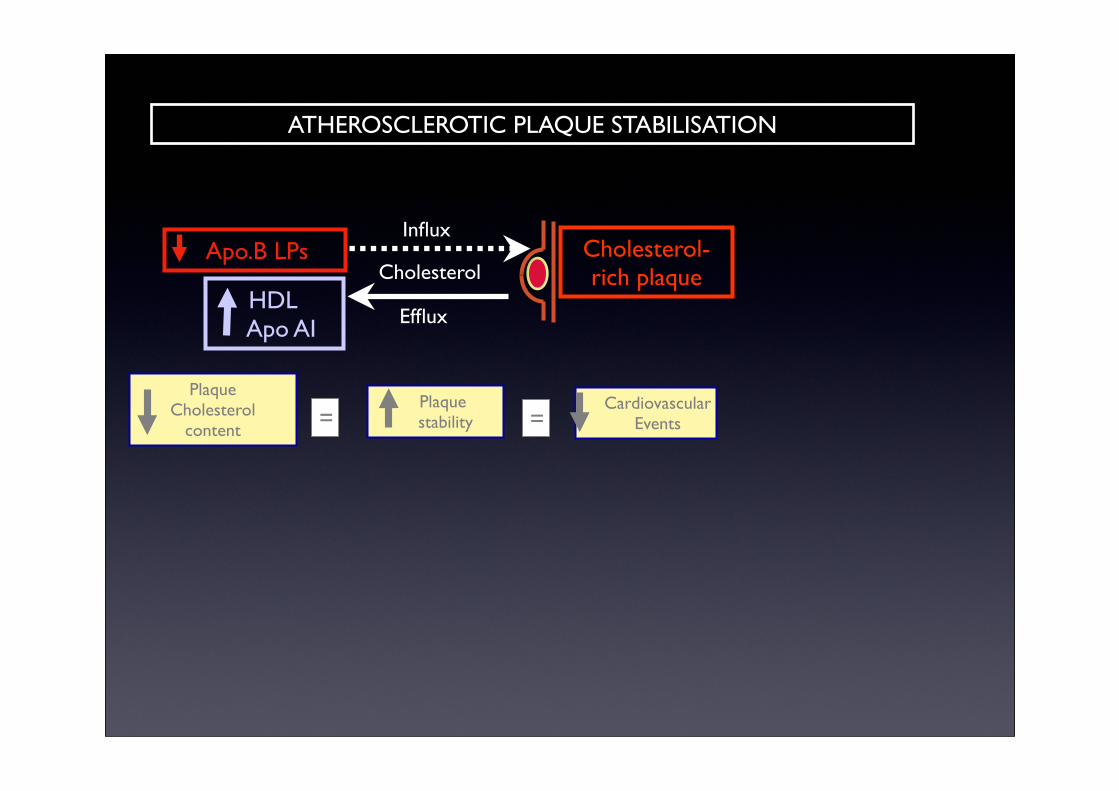
Efflux
Influx Cholesterol-rich plaque
Plaque Cholesterol
content
Plaque stability = =
Cardiovascular Events
Apo.B LPs
HDL Apo AI
ATHEROSCLEROTIC PLAQUE STABILISATION
Cholesterol
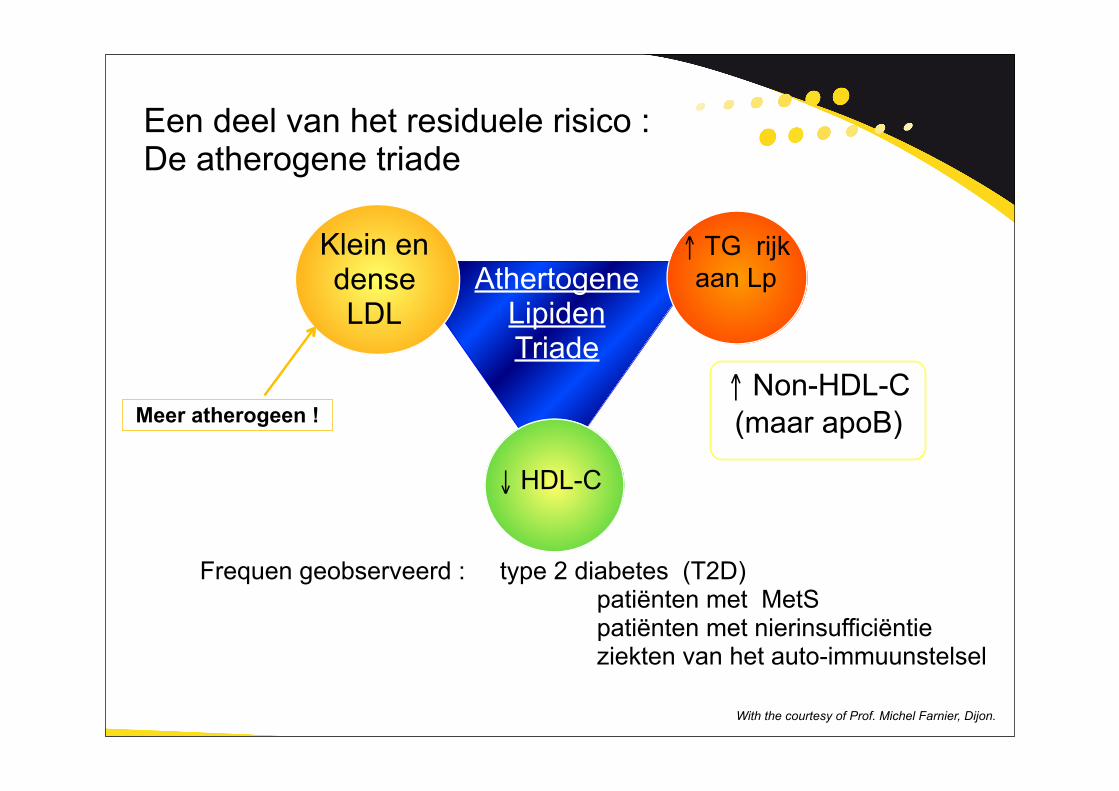
Een deel van het residuele risico :De atherogene triade
↓ HDL-C
↑ Non-HDL-C (maar apoB)
Klein en denseLDL
Athertogene Lipiden Triade
Frequen geobserveerd : type 2 diabetes (T2D) patiënten met MetS patiënten met nierinsufficiëntie ziekten van het auto-immuunstelsel
↑ TG rijk aan Lp
Meer atherogeen !
With the courtesy of Prof. Michel Farnier, Dijon.
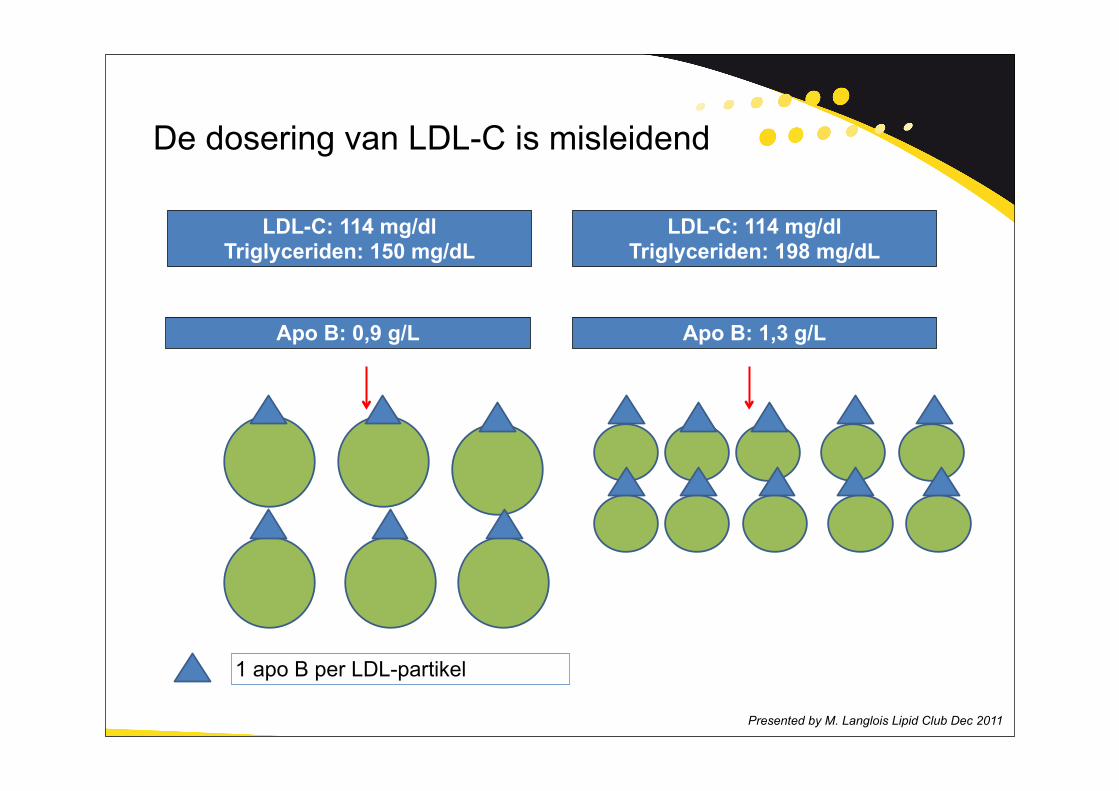
De dosering van LDL-C is misleidend
Presented by M. Langlois Lipid Club Dec 2011
LDL-C: 114 mg/dlTriglyceriden: 150 mg/dL
LDL-C: 114 mg/dlTriglyceriden: 198 mg/dL
Apo B: 0,9 g/L Apo B: 1,3 g/L
1 apo B per LDL-partikel
Non-HDL-C
Het bepalen van non-HDL-C (TC - HDL-C) bevat alle atherogene lipoproteïnes :
VLDL, IDL, LDL
•hypercholesterolaemie : LDL receptorgenmutatie ?
•hypercholesterolaemie met laag HDL
•Gemengde dyslipidaemie :apo B overproductie?
•hypertriglyceridaemie : LPL deficientie
•metabool syndroom
•geïsoleerd laag HDLfamiliaal hypoalfalipoporteïnaemie
•normaal lipidenprofiel en CVD ?
Dyslipidaemie
• Risicofactoren, Lipoproteïnes en Atherogenese
• Werkingsmechanisme van hyolipimiërende farmaca
• Richtlijnen
• Casuistiek
IMPLEMENTATIE ESC GUIDELINES LIPIDEN
Casuistiek
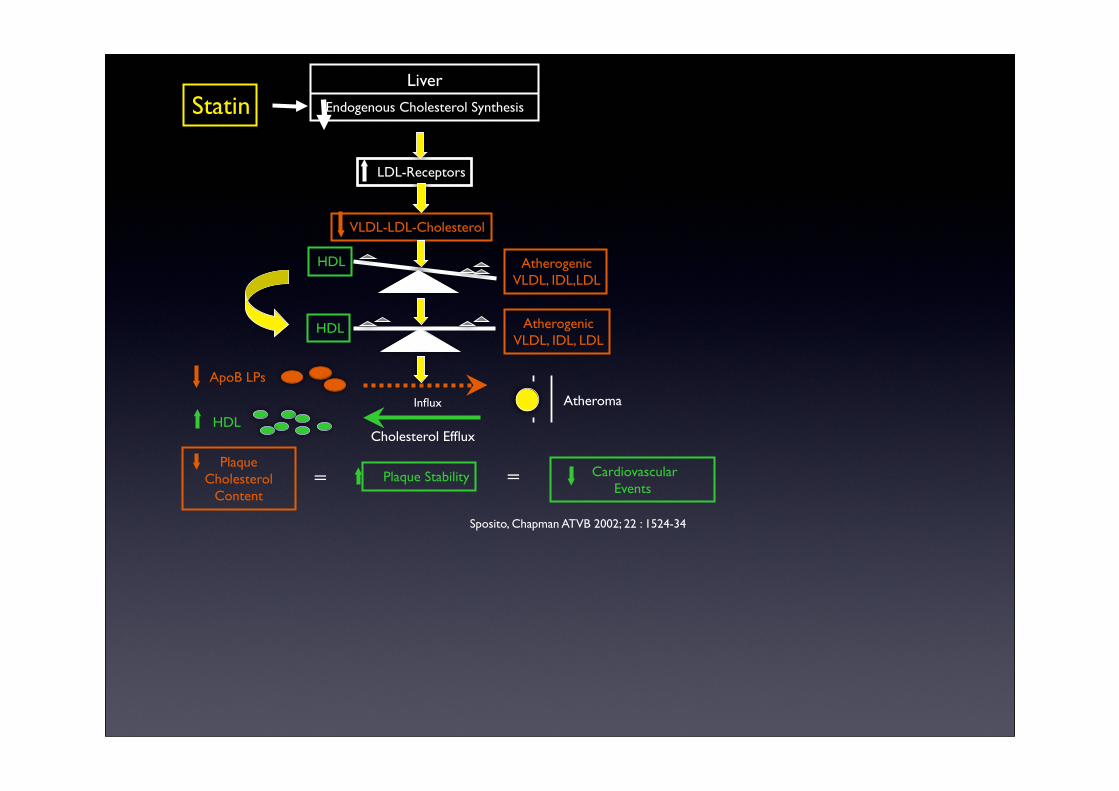
HDL AtherogenicVLDL, IDL,LDL
LDL-Receptors
VLDL-LDL-Cholesterol
HDL AtherogenicVLDL, IDL, LDL
Cholesterol Efflux
Influx
ApoB LPs
HDL
PlaqueCholesterol
Content Plaque Stability Cardiovascular
Events
Liver
Endogenous Cholesterol Synthesis
==
Statin
Atheroma
Sposito, Chapman ATVB 2002; 22 : 1524-34
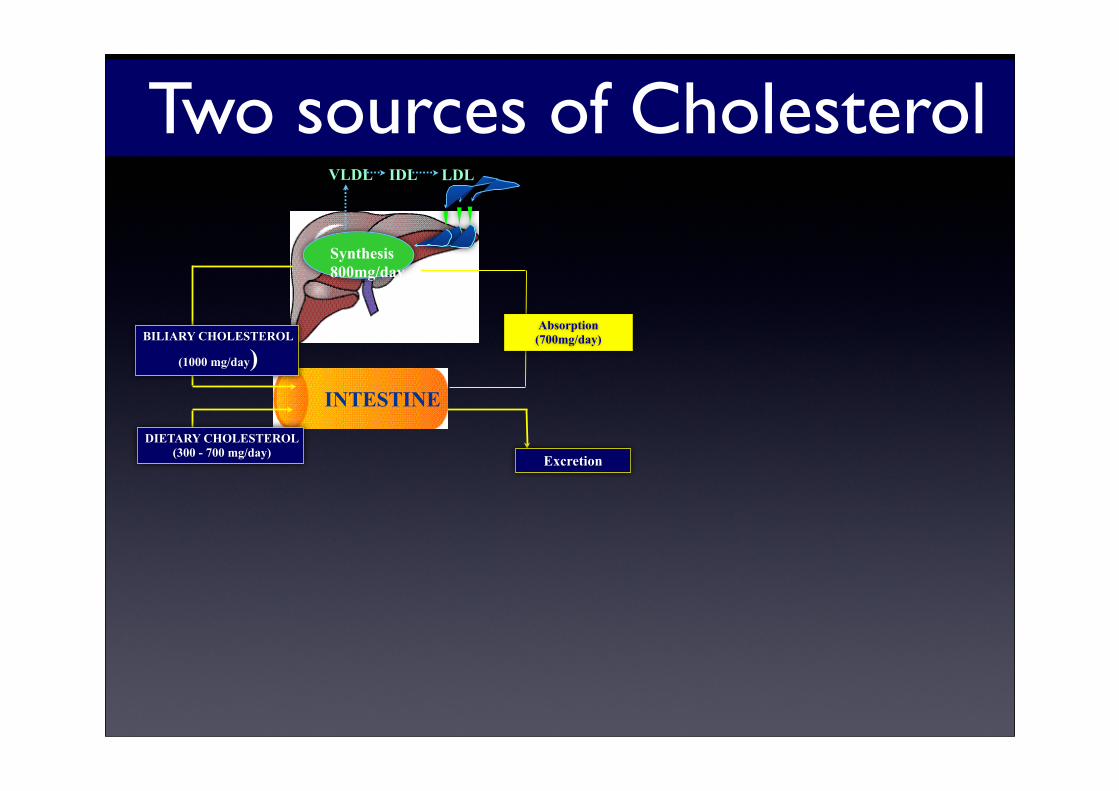
BILIARY CHOLESTEROL
(1000 mg/day)INTESTINE
Excretion
VLDL LDL
Absorption(700mg/day)
Synthesis800mg/day
IDL
DIETARY CHOLESTEROL(300 - 700 mg/day)
Two sources of Cholesterol
• Risicofactoren, Lipoproteïnes en Atherogenese
• Werkingsmechanisme van hyolipimiërende farmaca
• Richtlijnen
• Casuistiek
IMPLEMENTATIE ESC GUIDELINES LIPIDEN
Casuistiek
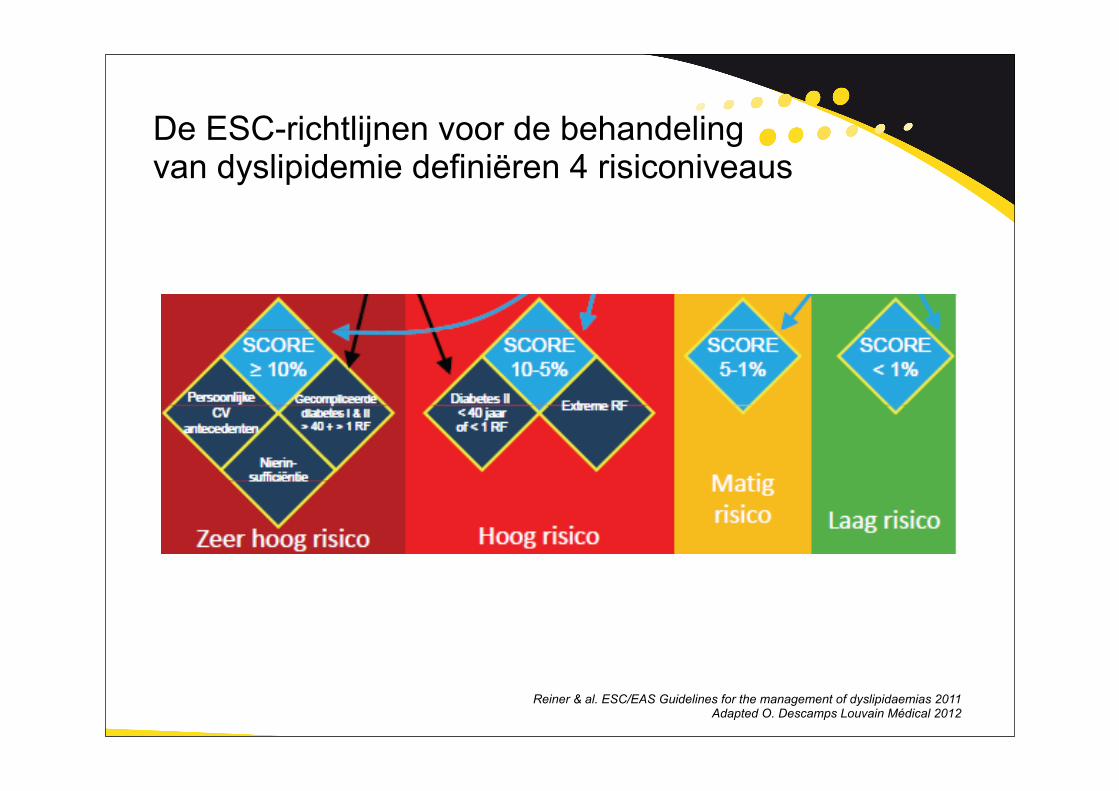
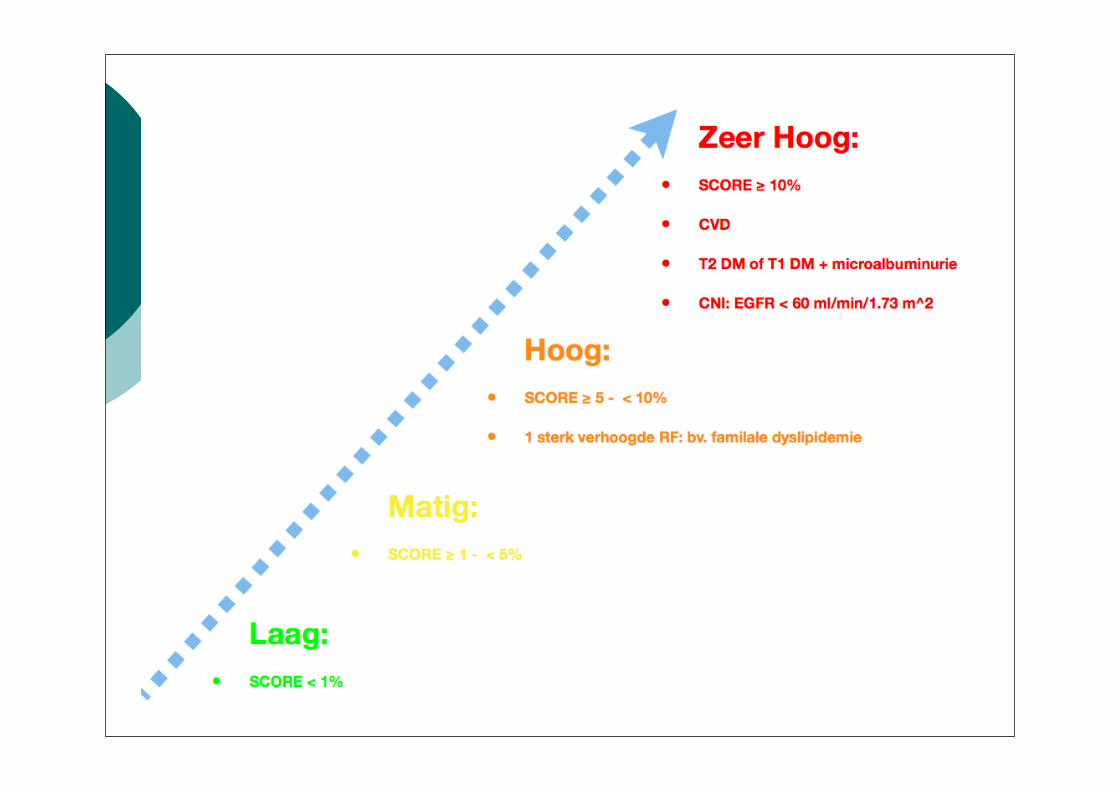
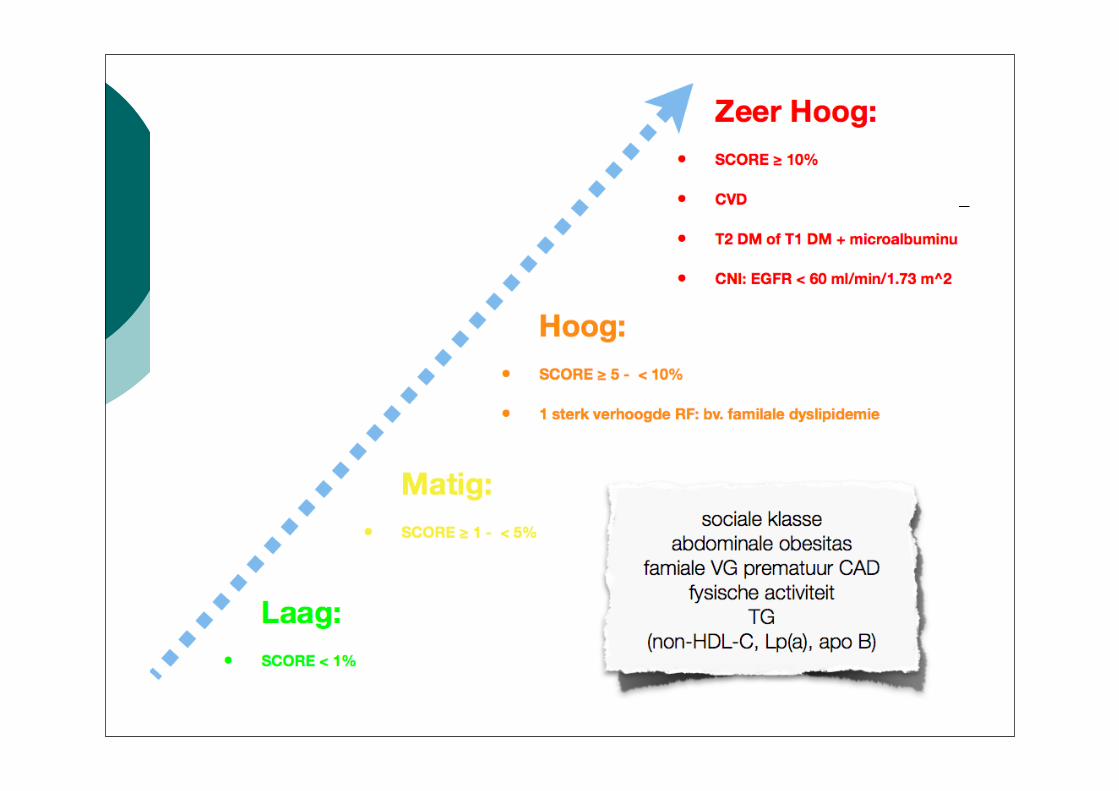
De ESC-richtlijnen voor de behandeling van dyslipidemie definiëren 4 risiconiveaus
Reiner & al. ESC/EAS Guidelines for the management of dyslipidaemias 2011Adapted O. Descamps Louvain Médical 2012
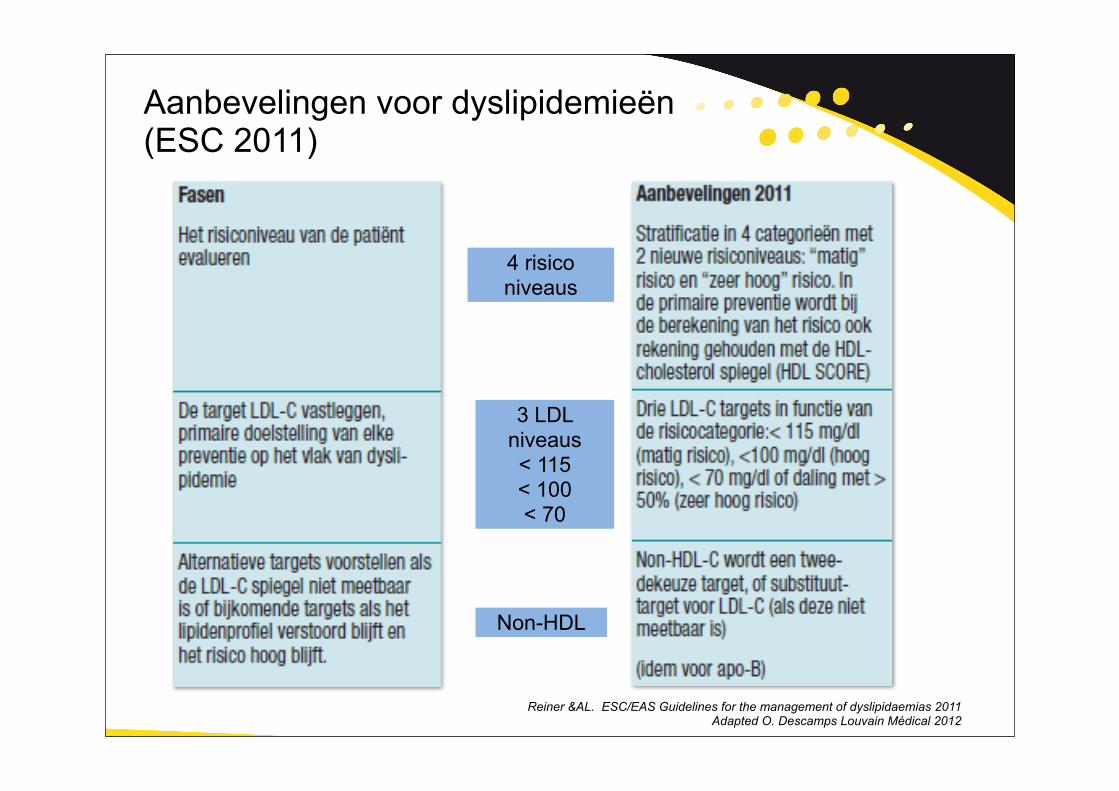
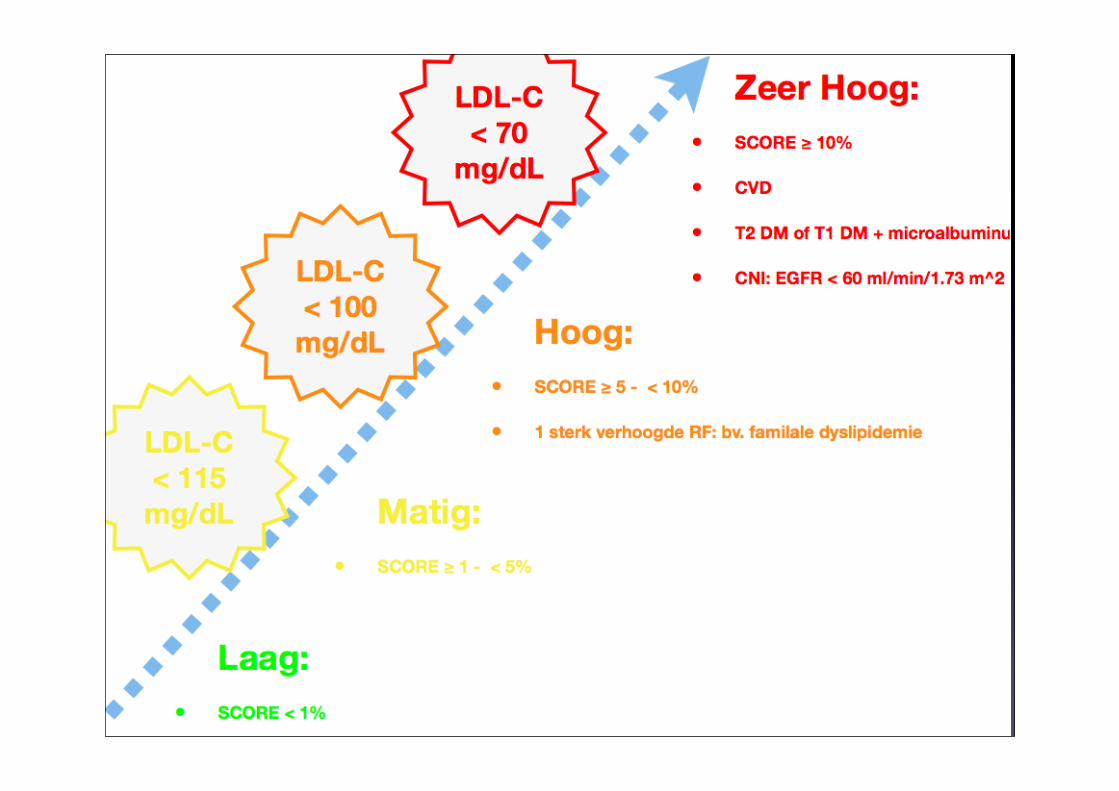
4 risico niveaus
3 LDL niveaus< 115< 100< 70
Non-HDL
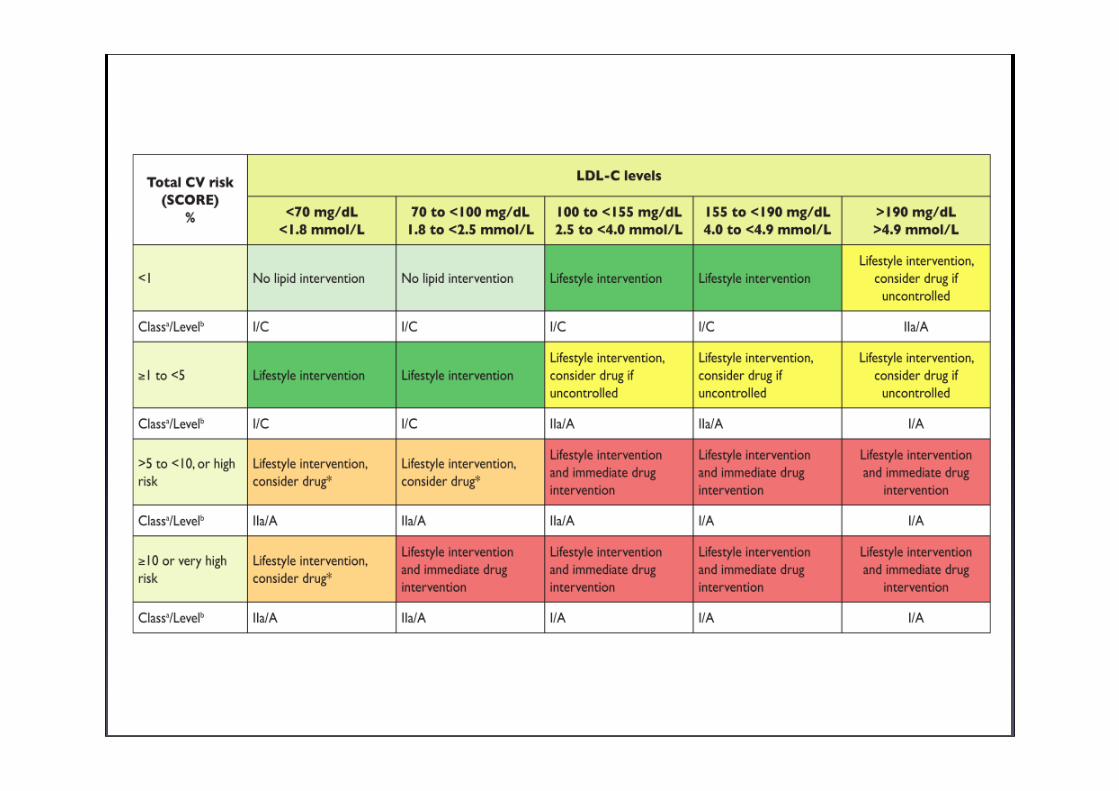
Aanbevelingen voor dyslipidemieën (ESC 2011)
Reiner &AL. ESC/EAS Guidelines for the management of dyslipidaemias 2011Adapted O. Descamps Louvain Médical 2012
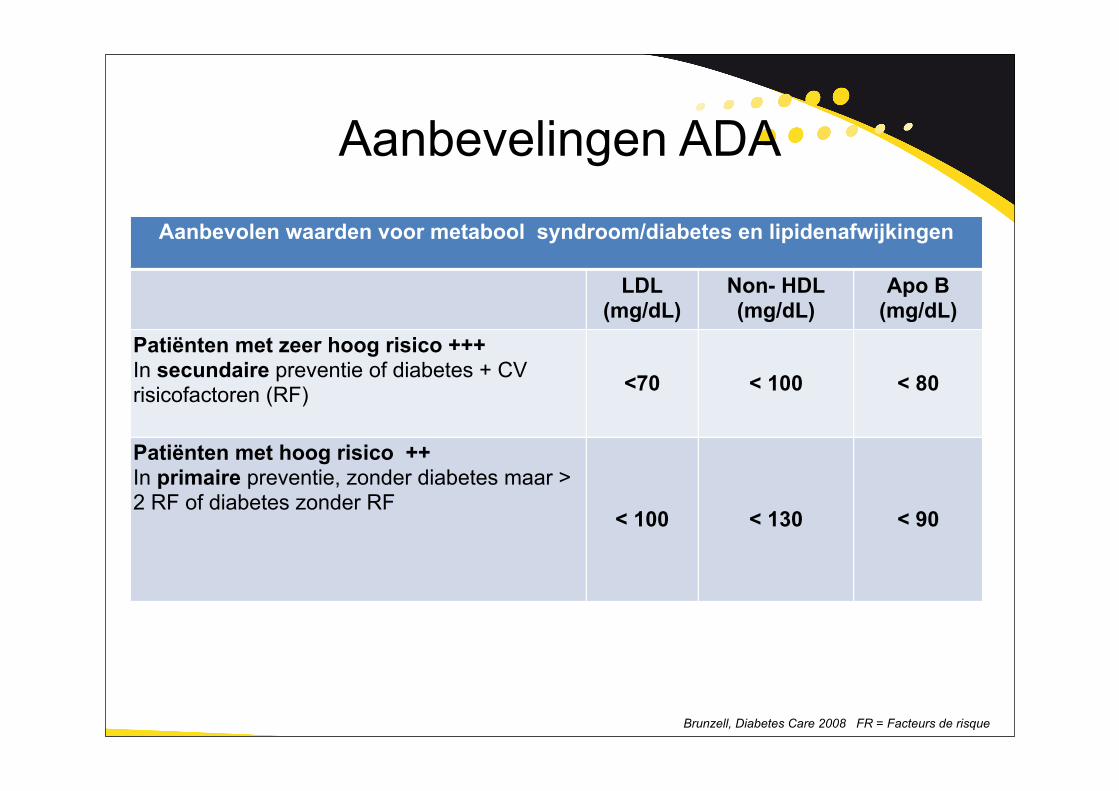
Aanbevelingen ADA
Brunzell, Diabetes Care 2008 FR = Facteurs de risque
Aanbevolen waarden voor metabool syndroom/diabetes en lipidenafwijkingenAanbevolen waarden voor metabool syndroom/diabetes en lipidenafwijkingenAanbevolen waarden voor metabool syndroom/diabetes en lipidenafwijkingenAanbevolen waarden voor metabool syndroom/diabetes en lipidenafwijkingen
LDL(mg/dL)
Non- HDL(mg/dL)
Apo B(mg/dL)
Patiënten met zeer hoog risico +++In secundaire preventie of diabetes + CVrisicofactoren (RF) <70 < 100 < 80
Patiënten met hoog risico ++In primaire preventie, zonder diabetes maar > 2 RF of diabetes zonder RF
< 100 < 130 < 90
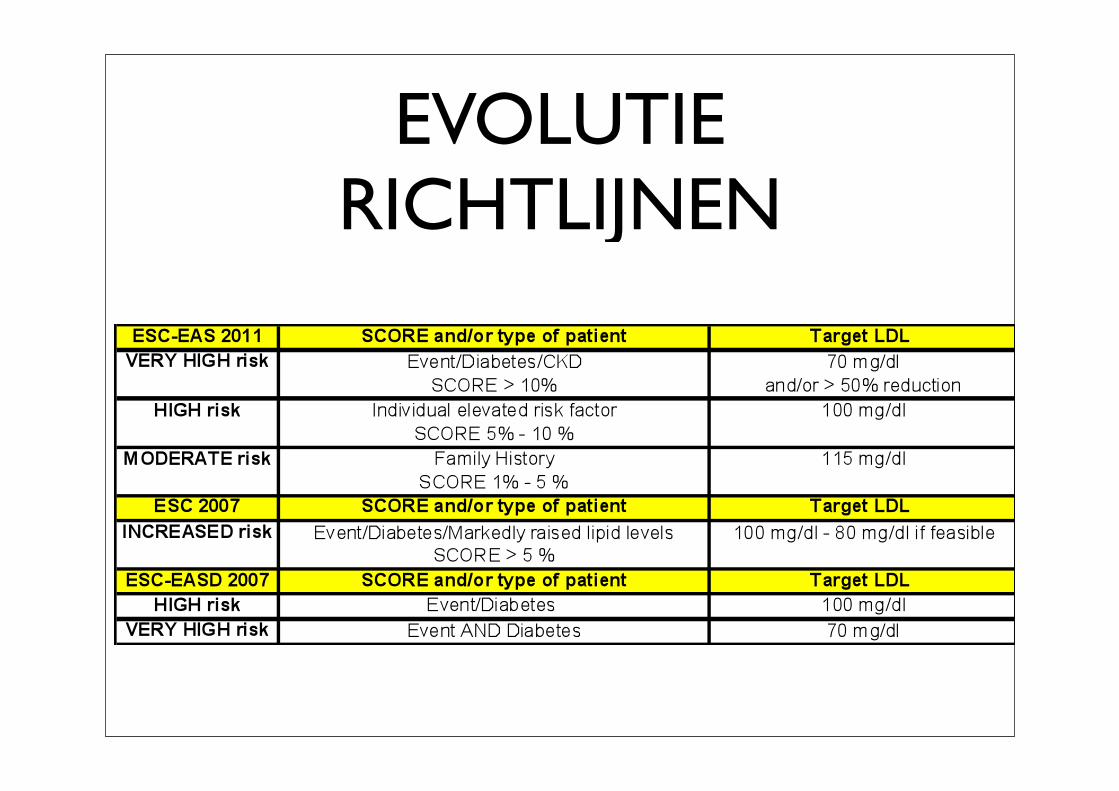
EVOLUTIE RICHTLIJNEN
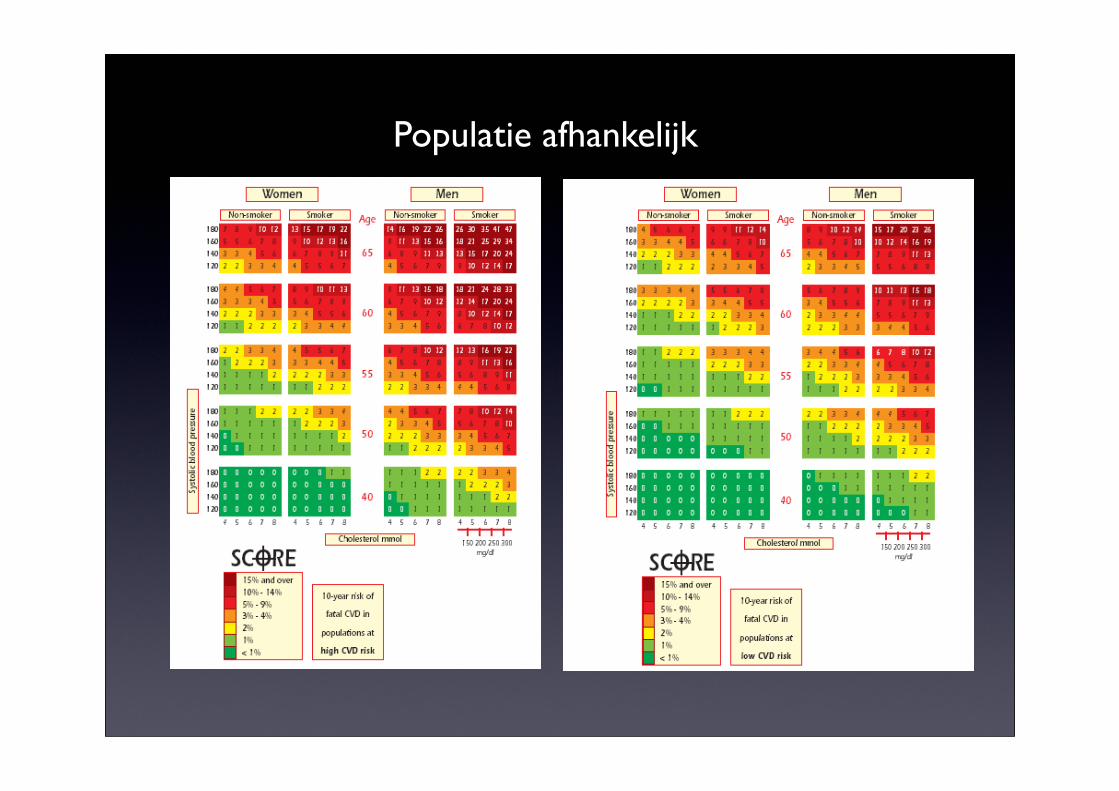
Populatie afhankelijk
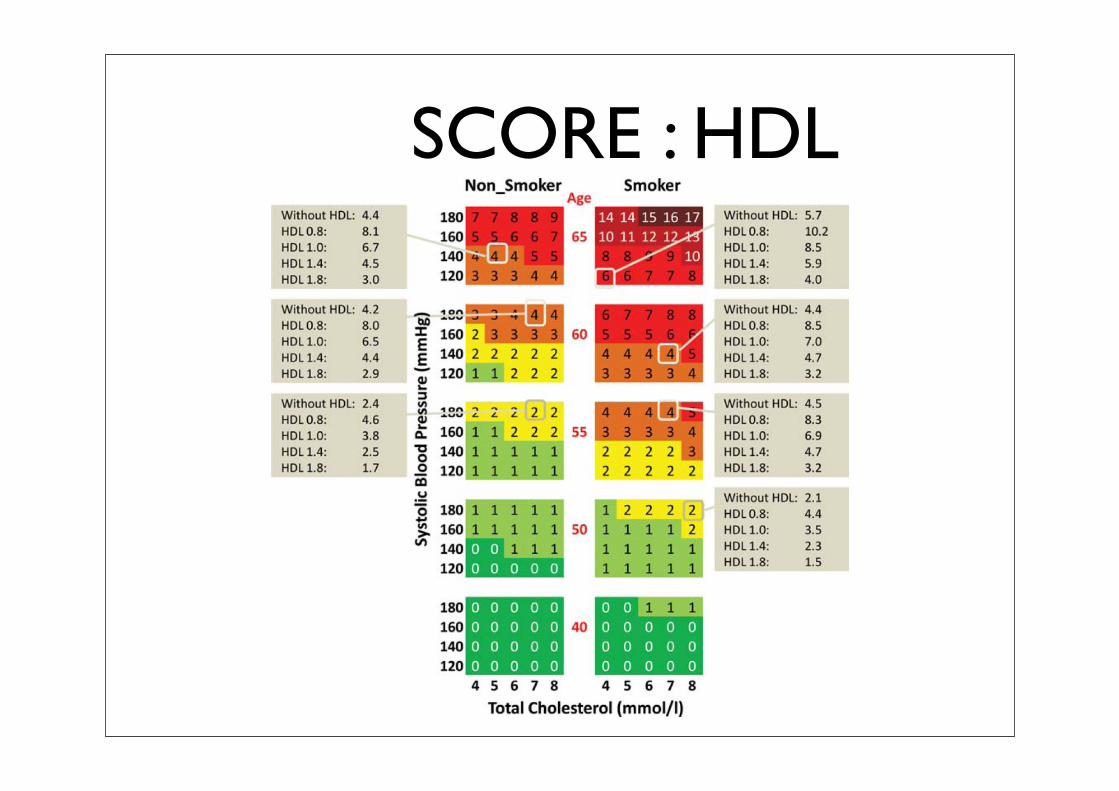
SCORE : HDL
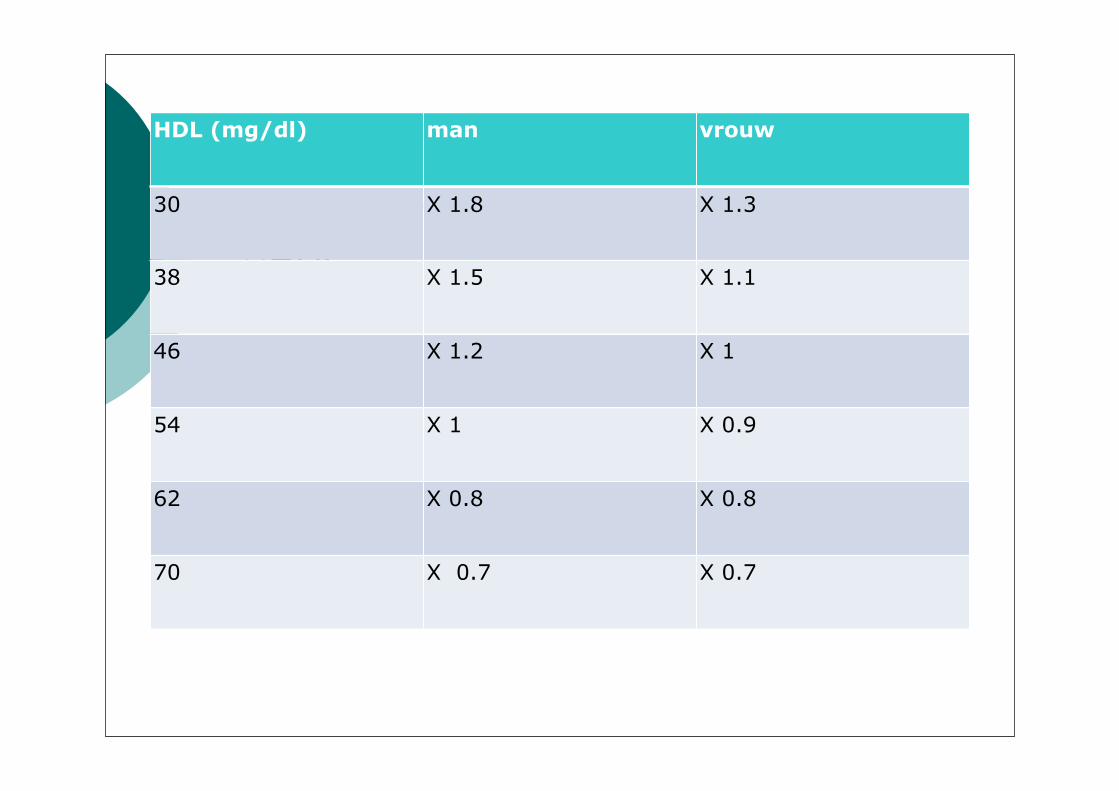
HDL
HDL (mg/dl) man vrouw
30 X 1.8 X 1.3
38 X 1.5 X 1.1
46 X 1.2 X 1
54 X 1 X 0.9
62 X 0.8 X 0.8
70 X 0.7 X 0.7
Factoren die het risico verhogen
• Familiaal vroegtijdig CV ziekten(man < 55j, vrouw < 60j)Risico x 1.7 vrouw x 2.0 man
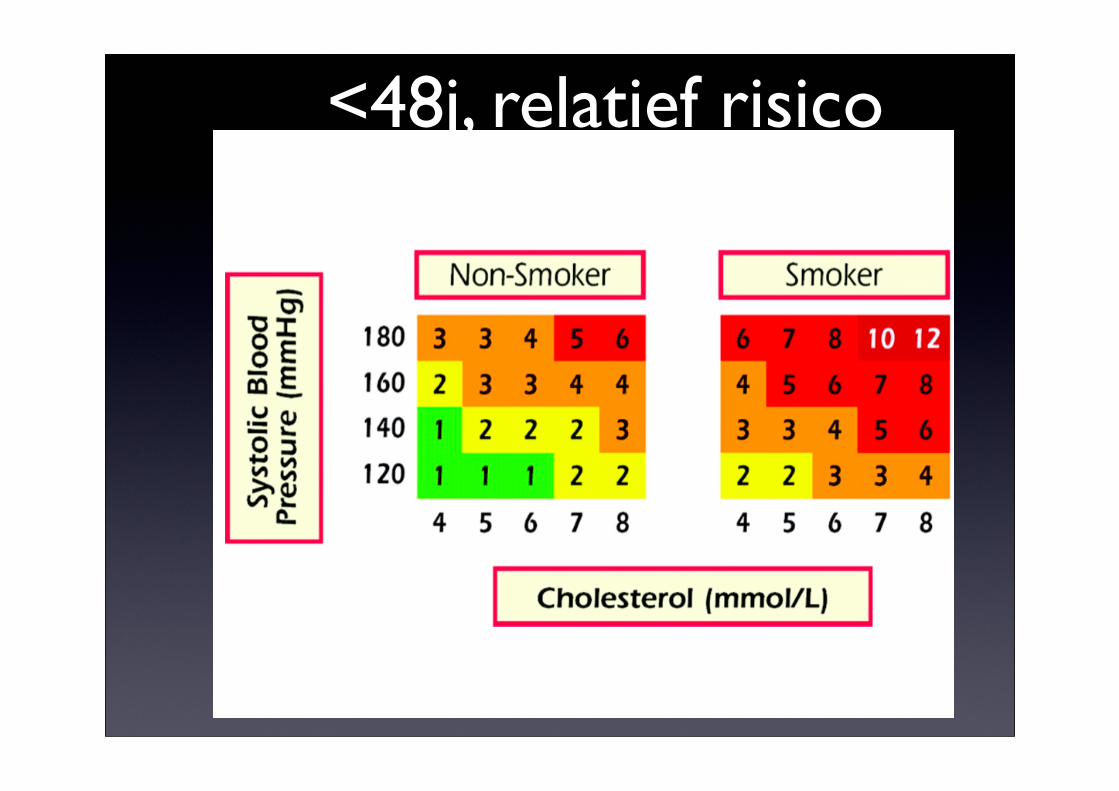
<48j, relatief risico
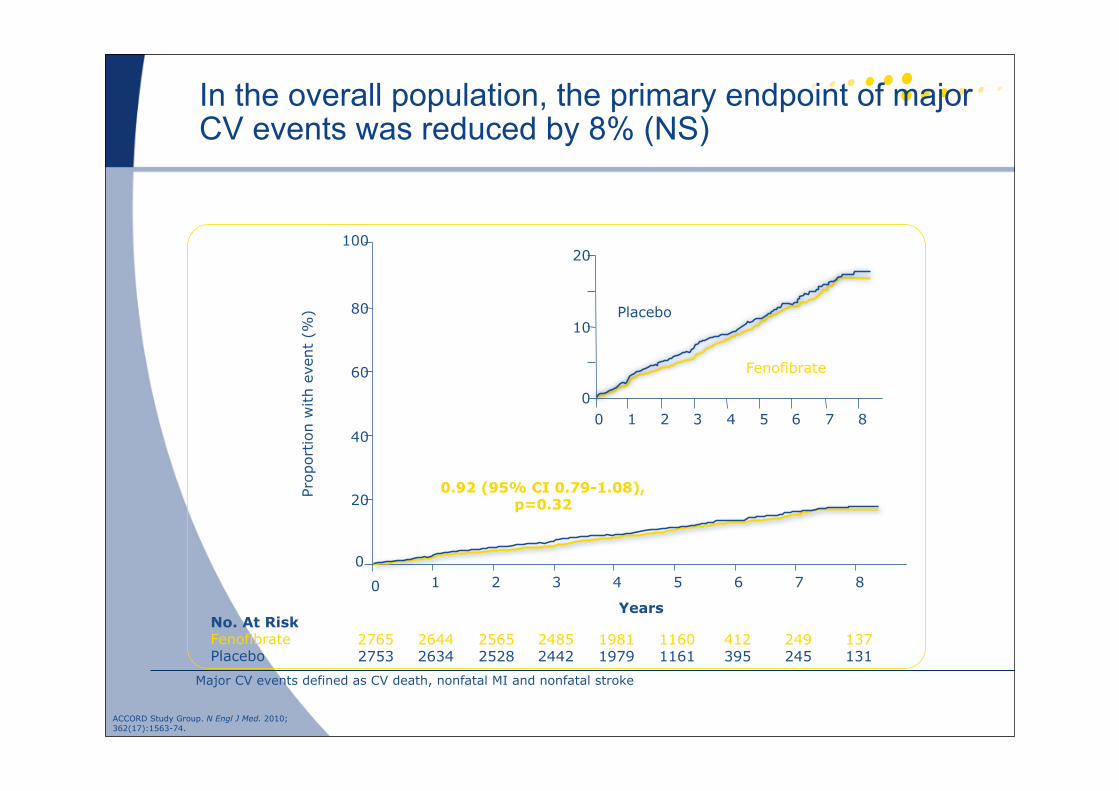
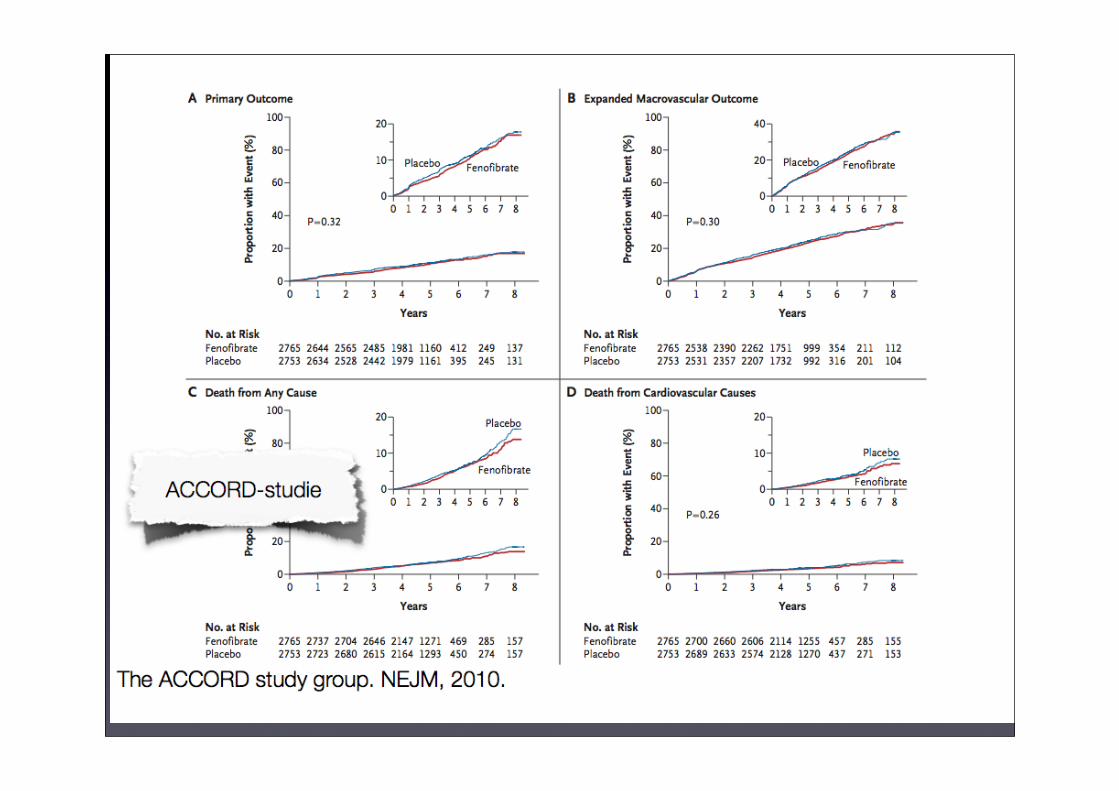
In the overall population, the primary endpoint of major CV events was reduced by 8% (NS)
0
20
40
60
80
100
Prop
ortion
with
even
t (%
)
0 1 2 3 4 5 6 7 8
27652753
26442634
25652528
24852442
19811979
11601161
412395
249245
137131
No. At RiskFenofibratePlacebo
Years
0.92 (95% CI 0.79-1.08),p=0.32
0
10
20
0 1 2 3 4 5 6 7 8
Placebo
Fenofibrate
Major CV events defined as CV death, nonfatal MI and nonfatal stroke
ACCORD Study Group. N Engl J Med. 2010;362(17):1563-74.
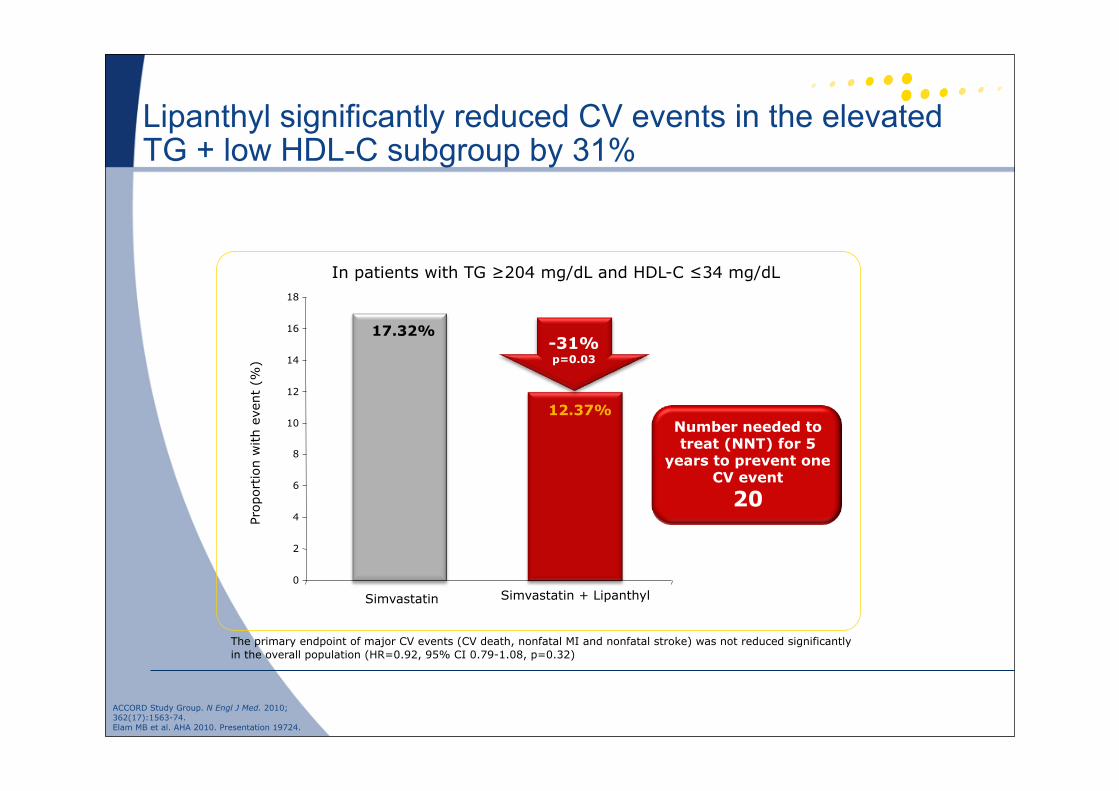
Lipanthyl significantly reduced CV events in the elevated TG + low HDL-C subgroup by 31%
The primary endpoint of major CV events (CV death, nonfatal MI and nonfatal stroke) was not reduced significantly in the overall population (HR=0.92, 95% CI 0.79-1.08, p=0.32)
ACCORD Study Group. N Engl J Med. 2010;362(17):1563-74.Elam MB et al. AHA 2010. Presentation 19724.
17.32%
12.37%
0
2
4
6
8
10
12
14
16
18
Prop
ortion
with
even
t (%
)
Simvastatin Simvastatin + Lipanthyl
-31% p=0.03
Number needed to treat (NNT) for 5
years to prevent one CV event
20
In patients with TG ≥204 mg/dL and HDL-C ≤34 mg/dL
SCORE enDIABETES?
• 5X VROUWEN
• 3X MANNEN
• UKPDS RISC ENGINE
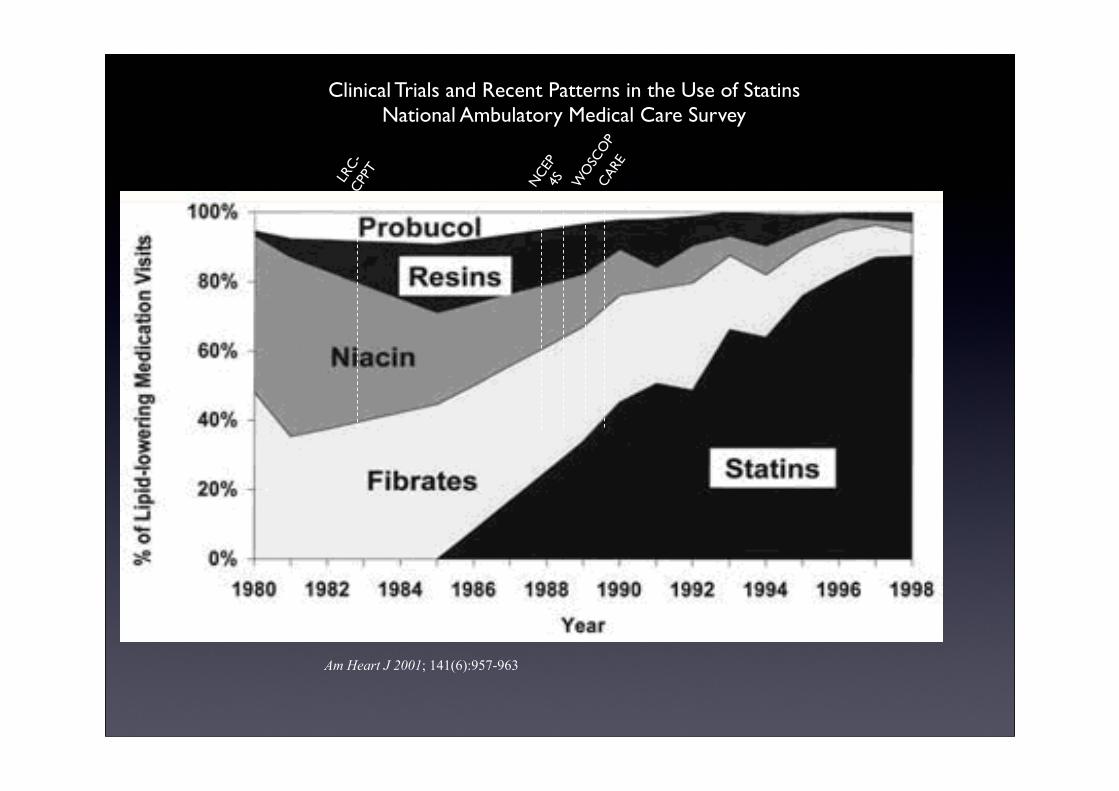
Am Heart J 2001; 141(6):957-963
LRC-
CPPT
NCE
P4S W
OSC
OP
CAR
E
Clinical Trials and Recent Patterns in the Use of StatinsNational Ambulatory Medical Care Survey
• Chapter 1 : Generic + ZOCOR
• Prescribed freely without any control ( ~ cheap products ) • IndicaAon : PaAents with Hypercholesterolemia • Products : Zocor, Simva Generic, Prava Generic, Pravasine, atorva Generic, Totalip
Chapter 2 : Original StaAns• Prescribed in B with a posteriori control• Reimbursement: PaAents not at goal aKer 3 months on cheap staAns• Products : AtorvastaAn 10,20,40,80 mg and RosuvastaAn 10,20,40 mg
Chapter 4 : EZETROL & INEGY• Prescribed in Bf with a priori control through the medical advisor• General PracAAoner needs a posiAve advice of the Specialist• IndicaAon : PaAents at goal aKer 3 months aKer staAn therapy• Products : Ezetrol and Inegy 10/20, 10/40, 10/80 mg