Het is er! - Antoni van Leeuwenhoek 1... · Nivolumab (BMS-936558) ... TNBC, triple negative breast...
35
Transcript of Het is er! - Antoni van Leeuwenhoek 1... · Nivolumab (BMS-936558) ... TNBC, triple negative breast...
Immunotherapie voor de oncologische praktijk
Het is er!
Disclosures
• Advisory role: BMS, MSD, Novartis, Pfizer, Roche/Genentech
• Honoraria: BMS, MSD, Novartis
• Funding: Merck-Serono, BMS, Novartis, Pfizer, Roche/ Genentech
Inhoud
• Werkingsmechanismen • Bijwerkingen • Selectie patienten • Casuistiek

WERKINGSMECHANISMEN
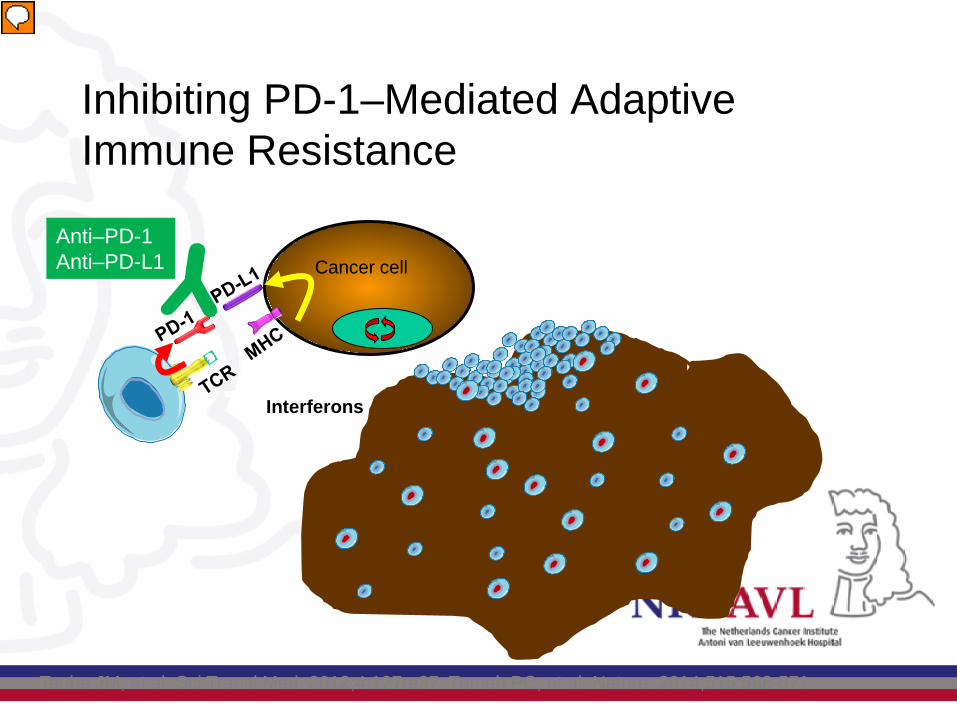
Inhibiting PD-1–Mediated Adaptive Immune Resistance
Taube JM, et al. Sci Transl Med. 2012;4:127ra37. Tumeh PC, et al. Nature. 2014;515:568-571.
Cancer cell
Interferons
Anti–PD-1 Anti–PD-L1
Presentator
Presentatienotities
PD-1, programmed death 1; PD-L1, programmed death ligand 1; TCR, T-cell receptor; MCH, major histocompatibility complex.
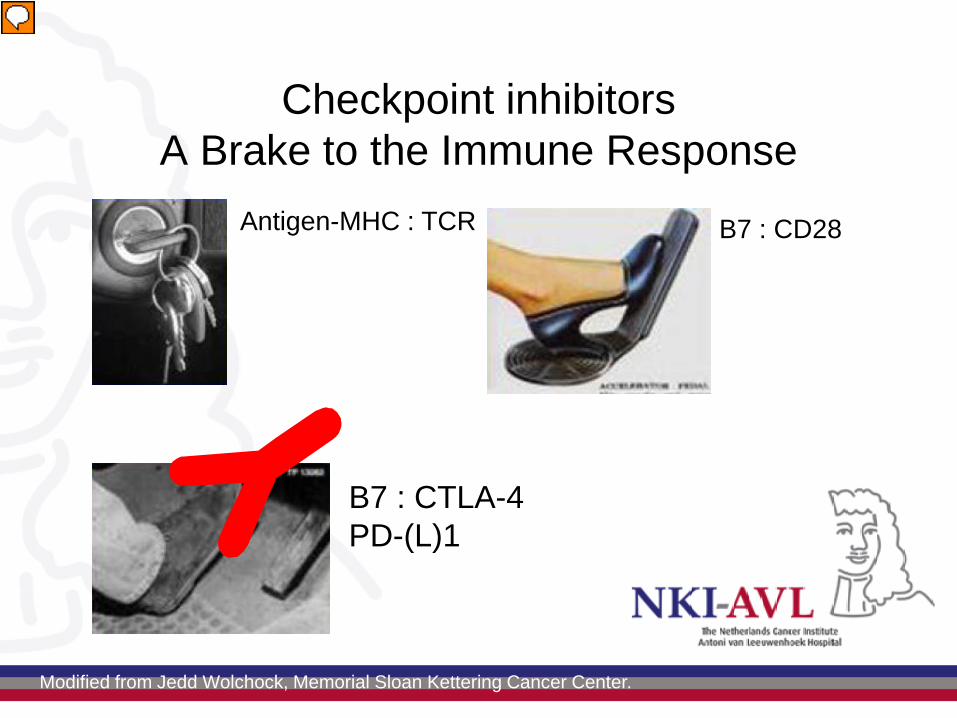
Checkpoint inhibitors A Brake to the Immune Response
Antigen-MHC : TCR B7 : CD28
B7 : CTLA-4 PD-(L)1
Modified from Jedd Wolchock, Memorial Sloan Kettering Cancer Center.
Presentator
Presentatienotities
CTLA-4, cytotoxic T-lymphocyte-associated protein 4; MHC, major histocompatibility complex; TCR, T-cell receptor.
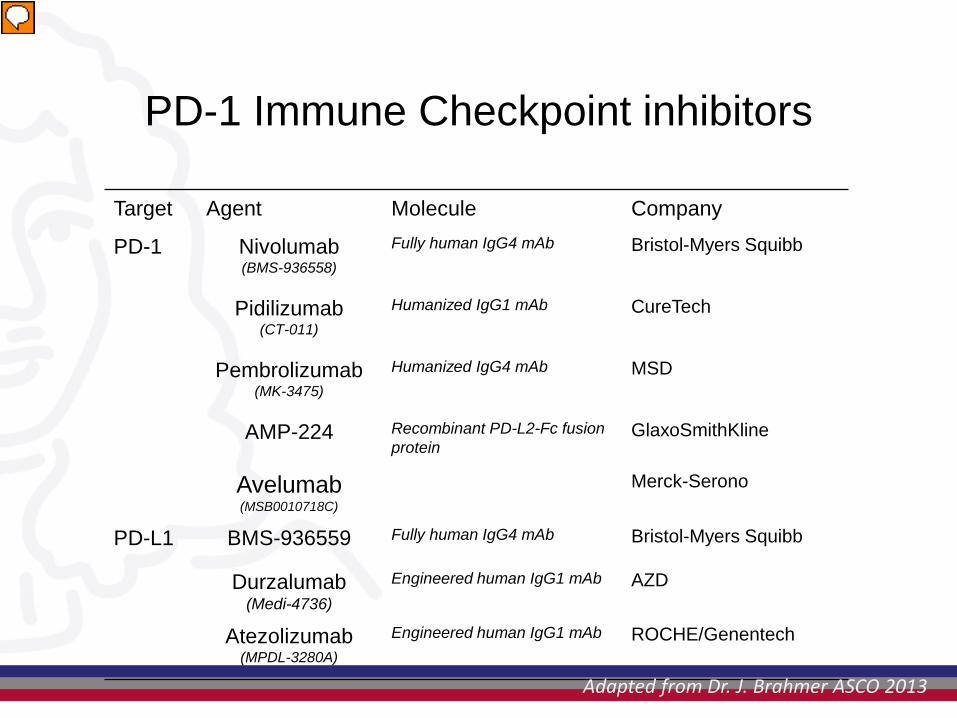
PD-1 Immune Checkpoint inhibitors
Target Agent Molecule Company
PD-1 Nivolumab (BMS-936558)
Fully human IgG4 mAb Bristol-Myers Squibb
Pidilizumab (CT-011)
Humanized IgG1 mAb CureTech
Pembrolizumab (MK-3475)
Humanized IgG4 mAb MSD
AMP-224 Recombinant PD-L2-Fc fusion protein
GlaxoSmithKline
Avelumab (MSB0010718C)
Merck-Serono
PD-L1 BMS-936559 Fully human IgG4 mAb Bristol-Myers Squibb
Durzalumab (Medi-4736)
Engineered human IgG1 mAb AZD
Atezolizumab (MPDL-3280A)
Engineered human IgG1 mAb ROCHE/Genentech
Adapted from Dr. J. Brahmer ASCO 2013
Presentator
Presentatienotities
Nivo ph2 incl combinations; prolonged responses
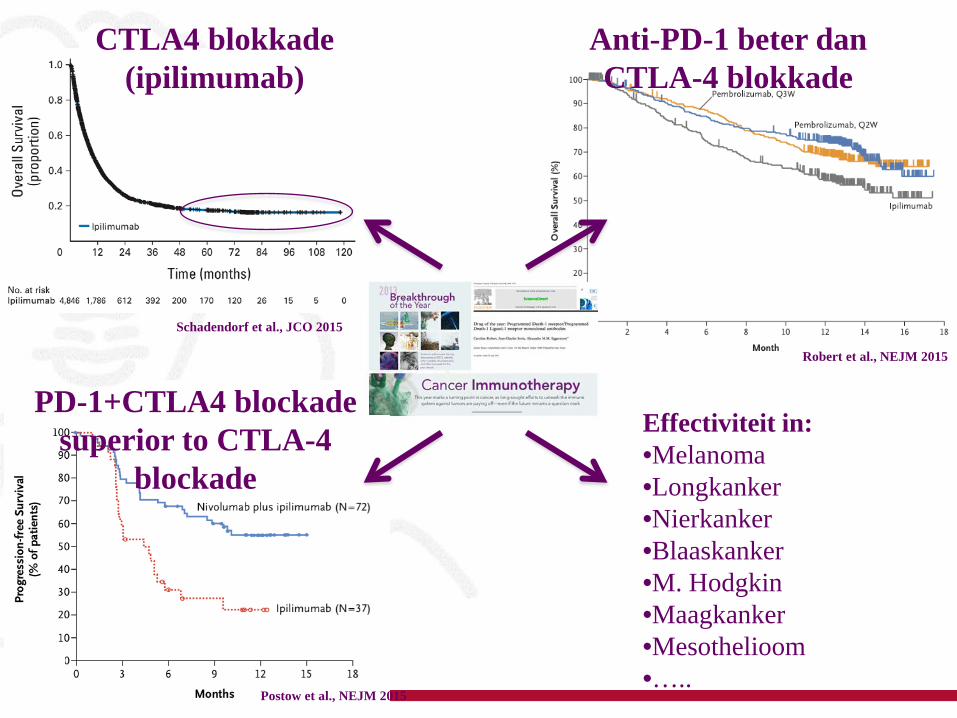
Schadendorf et al., JCO 2015
CTLA4 blokkade (ipilimumab)
Anti-PD-1 beter dan CTLA-4 blokkade
Robert et al., NEJM 2015
Postow et al., NEJM 2015
Effectiviteit in: •Melanoma •Longkanker •Nierkanker •Blaaskanker •M. Hodgkin •Maagkanker •Mesothelioom •…..
PD-1+CTLA4 blockade superior to CTLA-4
blockade
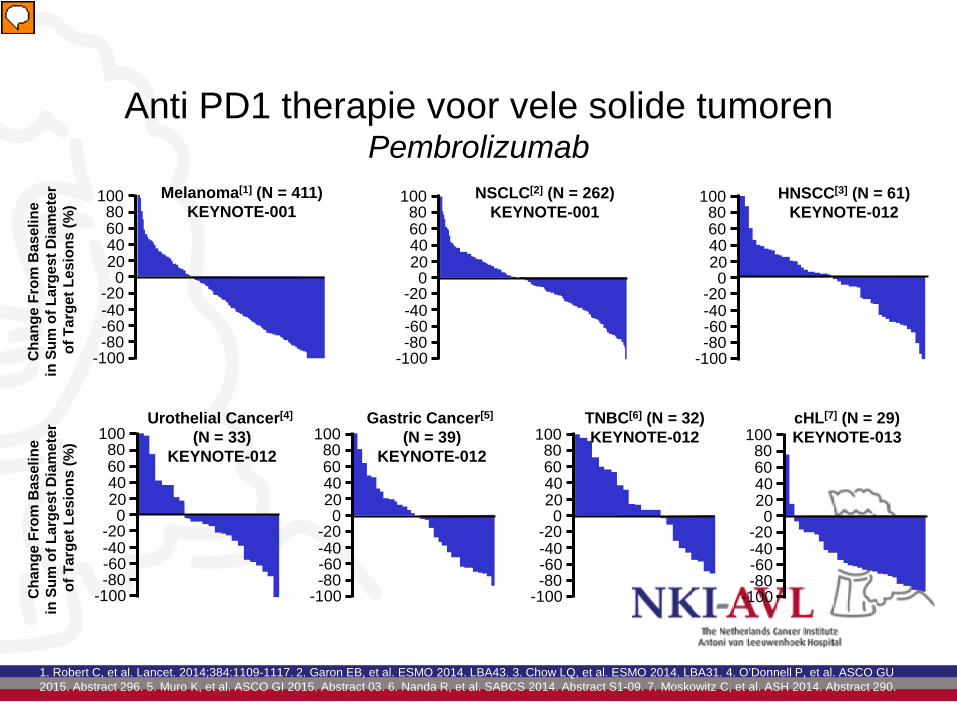
Anti PD1 therapie voor vele solide tumoren Pembrolizumab
1. Robert C, et al. Lancet. 2014;384:1109-1117. 2. Garon EB, et al. ESMO 2014. LBA43. 3. Chow LQ, et al. ESMO 2014. LBA31. 4. O’Donnell P, et al. ASCO GU 2015. Abstract 296. 5. Muro K, et al. ASCO GI 2015. Abstract 03. 6. Nanda R, et al. SABCS 2014. Abstract S1-09. 7. Moskowitz C, et al. ASH 2014. Abstract 290.
100 80 60 40 20 0
-20 -40 -60 -80
-100 Cha
nge
From
Bas
elin
e
in S
um o
f Lar
gest
Dia
met
er
of T
arge
t Les
ions
(%)
Melanoma[1] (N = 411) KEYNOTE-001
100 80 60 40 20 0
-20 -40 -60 -80
-100
NSCLC[2] (N = 262) KEYNOTE-001
100 80 60 40 20 0
-20 -40 -60 -80
-100
HNSCC[3] (N = 61) KEYNOTE-012
100 80 60 40 20 0
-20 -40 -60 -80
-100 Cha
nge
From
Bas
elin
e
in S
um o
f Lar
gest
Dia
met
er
of T
arge
t Les
ions
(%)
Urothelial Cancer[4] (N = 33)
KEYNOTE-012 100 80 60 40 20 0
-20 -40 -60 -80
-100
Gastric Cancer[5] (N = 39)
KEYNOTE-012 100 80 60 40 20 0
-20 -40 -60 -80
-100
TNBC[6] (N = 32) KEYNOTE-012 100
80 60 40 20 0
-20 -40 -60 -80
-100
cHL[7] (N = 29) KEYNOTE-013
Presentator
Presentatienotities
NSCLC, non-small cell lung cancer; HNSCC, head and neck squamous cell carcinoma; EGFR, epidermal growth factor receptor; ALK, anaplastic lymphoma kinase; TNBC, triple negative breast cancer; cHL, classical Hodgkin’s lymphoma.
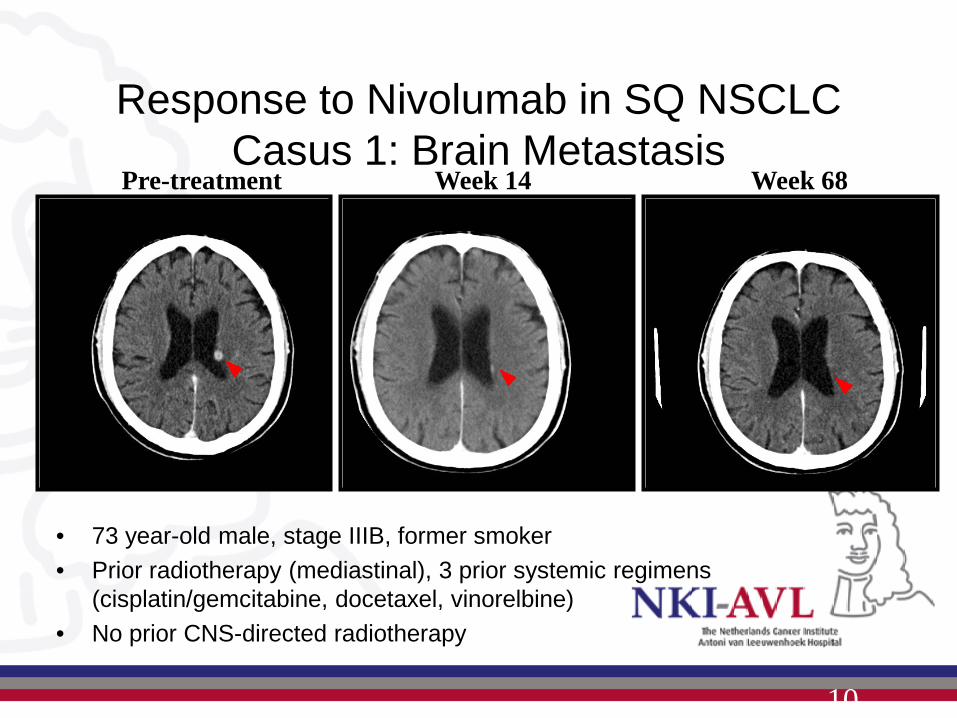
Response to Nivolumab in SQ NSCLC Casus 1: Brain Metastasis
• 73 year-old male, stage IIIB, former smoker • Prior radiotherapy (mediastinal), 3 prior systemic regimens
(cisplatin/gemcitabine, docetaxel, vinorelbine) • No prior CNS-directed radiotherapy
Pre-treatment Week 14 Week 68
10
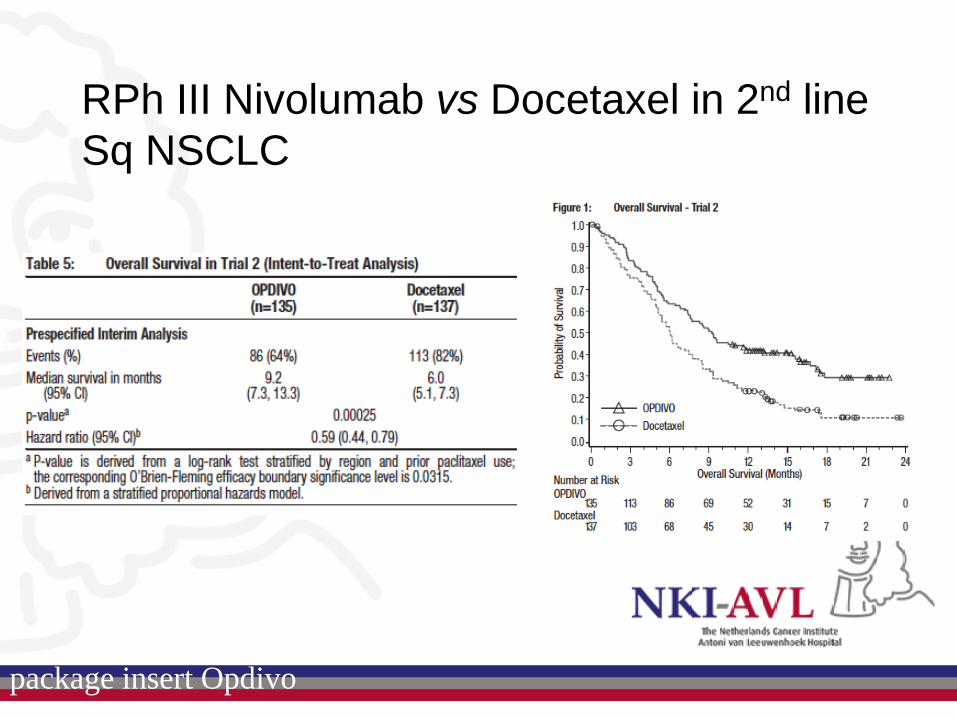
RPh III Nivolumab vs Docetaxel in 2nd line Sq NSCLC
package insert Opdivo

BIJWERKINGEN
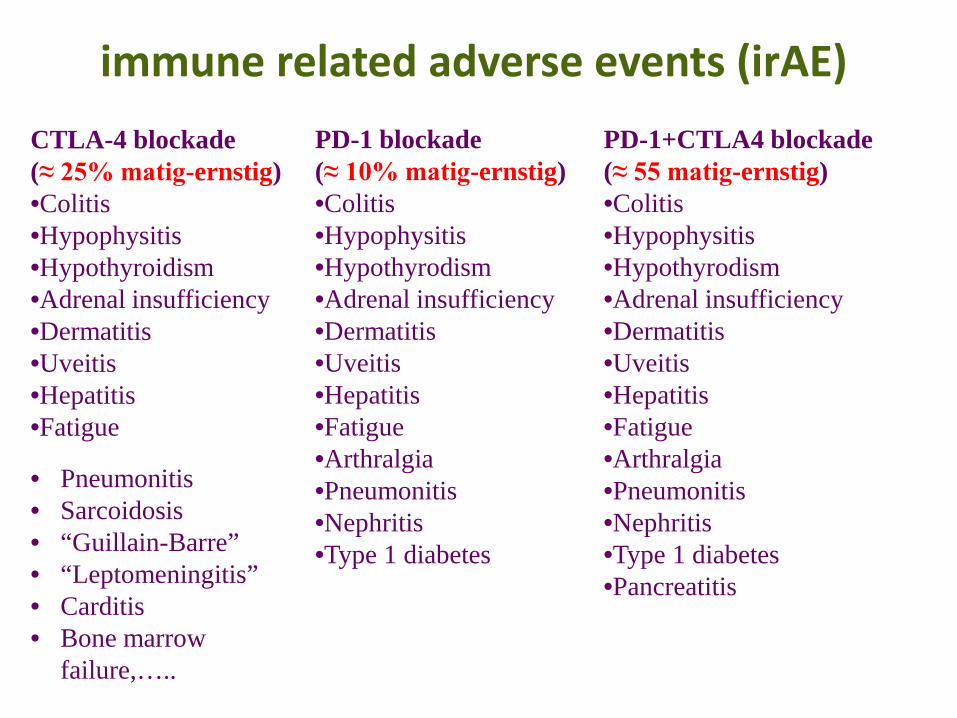
immune related adverse events (irAE) CTLA-4 blockade (≈ 25% matig-ernstig) •Colitis •Hypophysitis •Hypothyroidism •Adrenal insufficiency •Dermatitis •Uveitis •Hepatitis •Fatigue
PD-1 blockade (≈ 10% matig-ernstig) •Colitis •Hypophysitis •Hypothyrodism •Adrenal insufficiency •Dermatitis •Uveitis •Hepatitis •Fatigue •Arthralgia •Pneumonitis •Nephritis •Type 1 diabetes
PD-1+CTLA4 blockade (≈ 55 matig-ernstig) •Colitis •Hypophysitis •Hypothyrodism •Adrenal insufficiency •Dermatitis •Uveitis •Hepatitis •Fatigue •Arthralgia •Pneumonitis •Nephritis •Type 1 diabetes •Pancreatitis
• Pneumonitis • Sarcoidosis • “Guillain-Barre” • “Leptomeningitis” • Carditis • Bone marrow
failure,…..
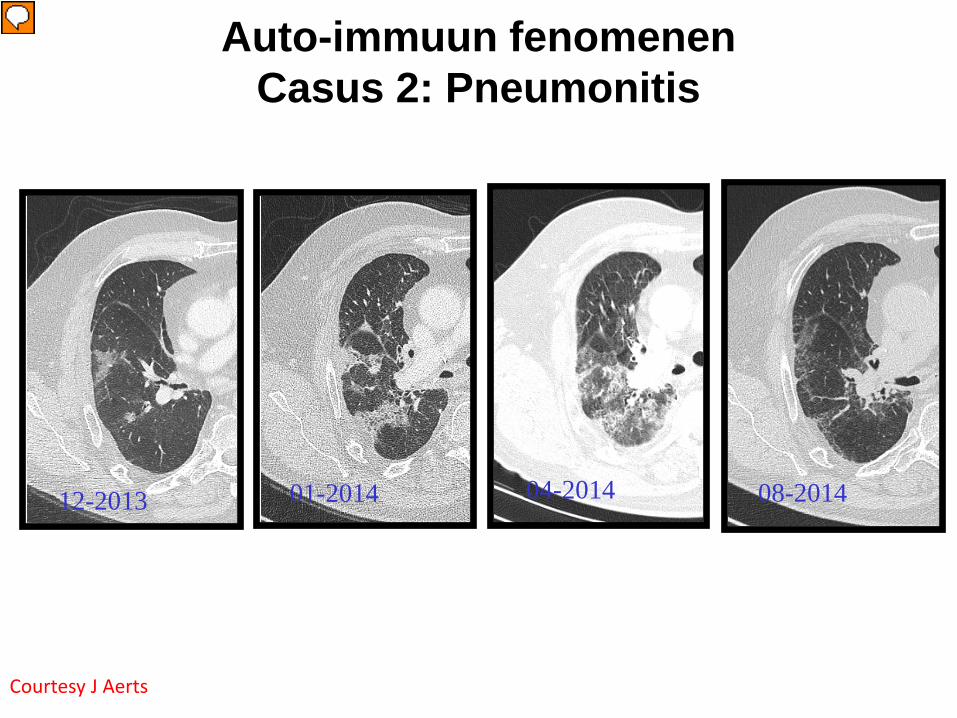
Auto-immuun fenomenen Casus 2: Pneumonitis
Courtesy J Aerts
12-2013 01-2014 04-2014 08-2014
Presentator
Presentatienotities
Jan 2014 Start prednison 60mg, Stop anti pd-1 Na 1 week afname afwijkingen start afbouw prednison Feb 2014 pred 10mg herstart pd-1 Apr 2014 Opnieuw interstitiele afwijkingen. Herstart prednison 30-20 Afbouwen lukt nu niet Dus persisterende respons Dus 2* pneumonitis en hypothyreoidie, Permanent discontinueren anti-PD1 Continueren prednison op 10mg
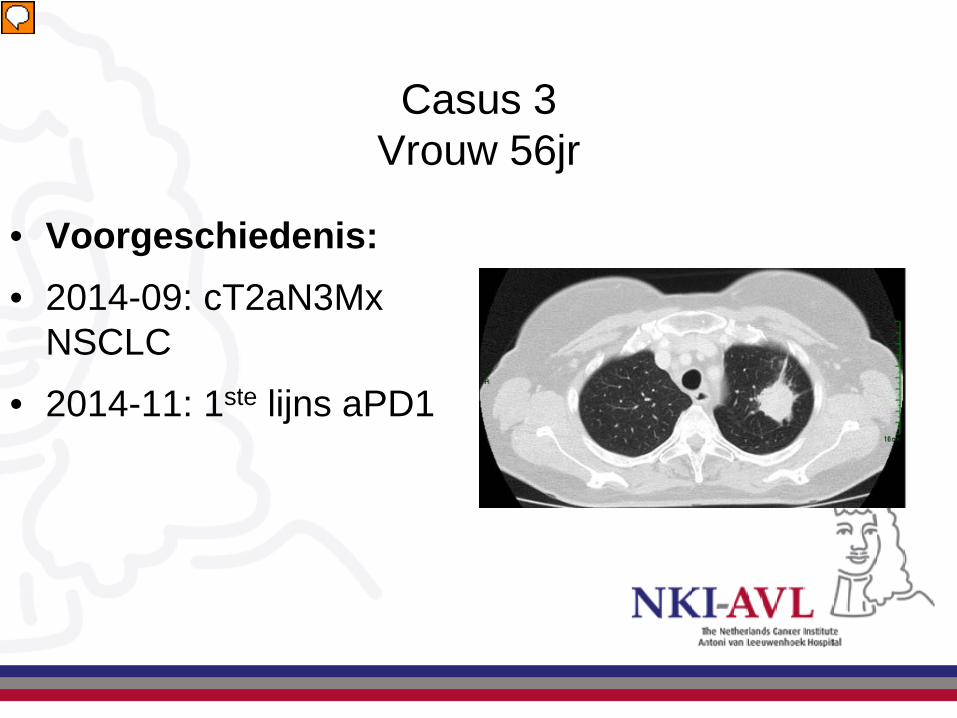
Casus 3 Vrouw 56jr
• Voorgeschiedenis: • 2014-09: cT2aN3Mx
NSCLC • 2014-11: 1ste lijns aPD1
Presentator
Presentatienotities
2013: Haardvorming LBK (matig PET-avide): Diagnose COP na transthoracale punctie) 2014-09: cT2aN3Mx NSCLC (KRAS/EGFR/ALK negatief), asymptomatische hersenmets 2014-10: WBRT 5x 4 Gy 2014-10: Trombose vena sucblavia/vena jugularis 2014-11: Inclusie in trial met eerste lijns aPD1
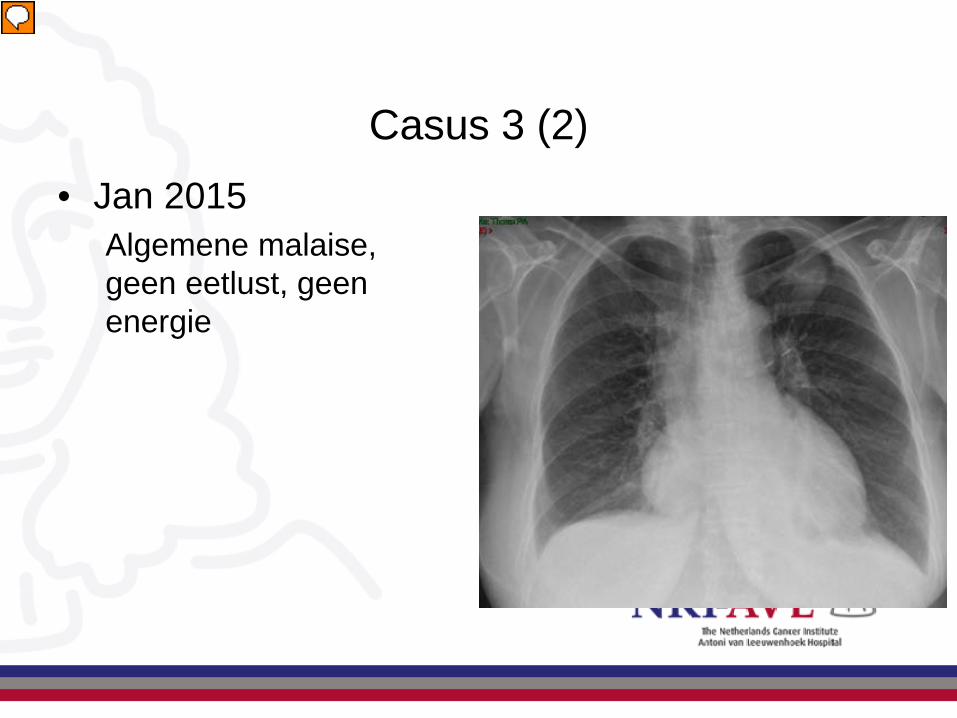
Casus 3 (2) • Jan 2015
Algemene malaise, geen eetlust, geen energie
Presentator
Presentatienotities
Jan 2015 Algemene malaise, geen eetlust, geen energie, Lab gb, TSH normaal Controles gb., stabiel gewicht, dd bijwerking IT, maar welke. B/ NH, en controle 1wk. FU +3dgn gaat slechter. Opname voor analyse. Lab: milde leverfunctie stoornis FU +4 dgn: Ernstige lever en nier-functiestoornis. ECG: microvoltages Consult cardio: gb, echo dag erop. X-thorax 19.00:
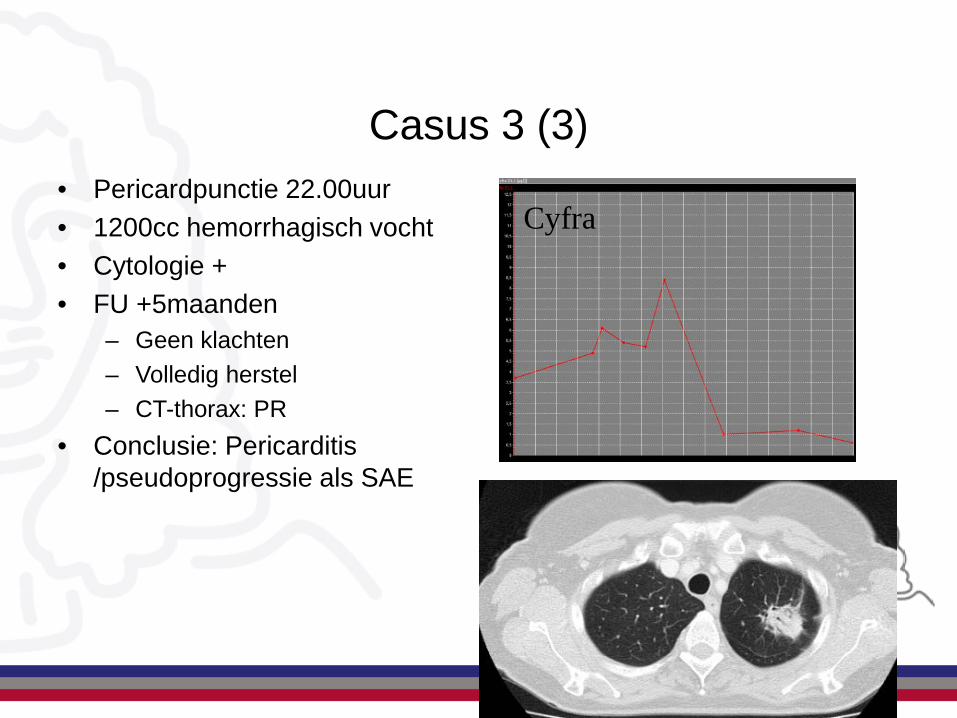
Casus 3 (3)
Cyfra • Pericardpunctie 22.00uur • 1200cc hemorrhagisch vocht • Cytologie + • FU +5maanden
– Geen klachten – Volledig herstel – CT-thorax: PR
• Conclusie: Pericarditis /pseudoprogressie als SAE
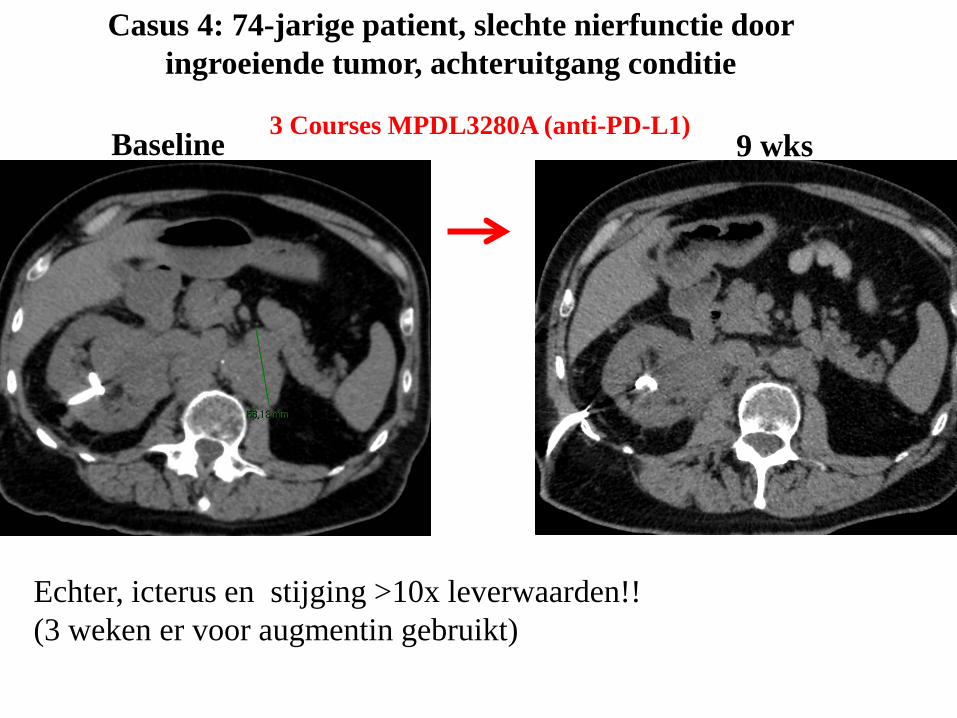
Echter, icterus en stijging >10x leverwaarden!! (3 weken er voor augmentin gebruikt)
Baseline 3 Courses MPDL3280A (anti-PD-L1) 9 wks
Casus 4: 74-jarige patient, slechte nierfunctie door ingroeiende tumor, achteruitgang conditie
Hoe om te gaan met irAEs
• Bijna altijd omkeerbaar
• Snel ontdekken – snel behandelen -> aanwezigheid internist-oncoloog met immuun-expertise
• Vroeg starten met immuun suppressie – Hit Fast
• Niet twijfelen om immuunsuppressie te escaleren
• Tijdig afbouwen – Hit Short
• De ernst van de bijwerkingen wordt bepaald door de reactie van de patient en de dokter
BEOORDELING RESPONS
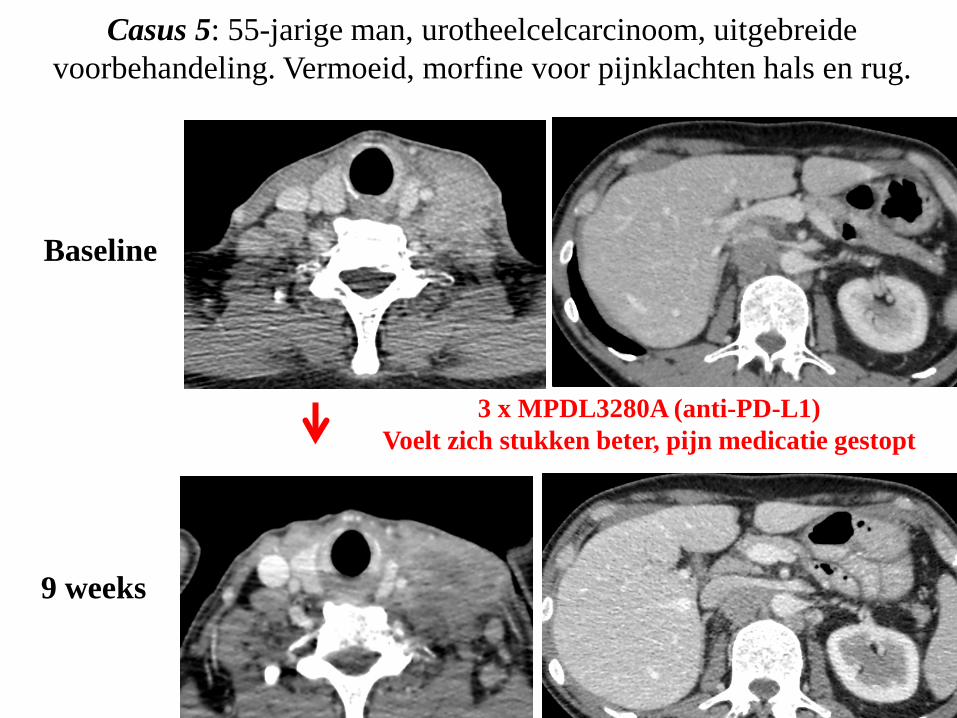
Baseline
9 weeks
3 x MPDL3280A (anti-PD-L1) Voelt zich stukken beter, pijn medicatie gestopt
Casus 5: 55-jarige man, urotheelcelcarcinoom, uitgebreide voorbehandeling. Vermoeid, morfine voor pijnklachten hals en rug.
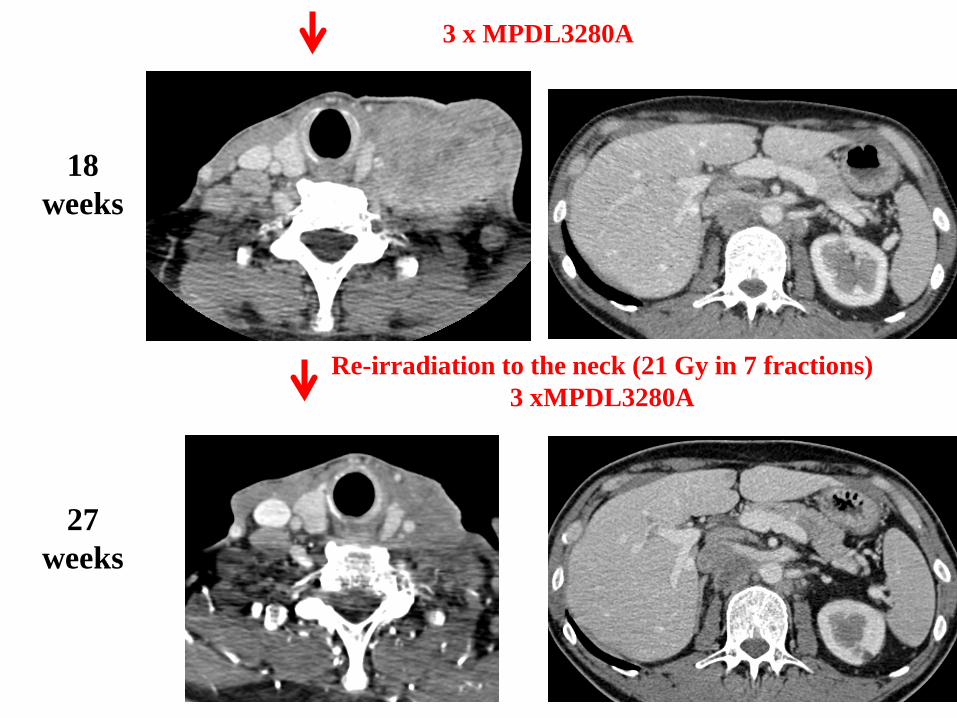
18 weeks
3 x MPDL3280A
27 weeks
Re-irradiation to the neck (21 Gy in 7 fractions) 3 xMPDL3280A
Casus 6 (1) Pseudoprogressie
• Man 64 jr, NSCLC IV, bijnier en hersen mets • 10/2013 WBRT en start Cisplatin en pemetrexed. Maximale
respons progressie • 1/2014: Start anti PD1 therapie, maximale respons: partiele
respons • 11/2014: Groei intra- abdominale meta’s (oa pancreas kop). • 12/2014: Continueren groei en PA bewijs meta
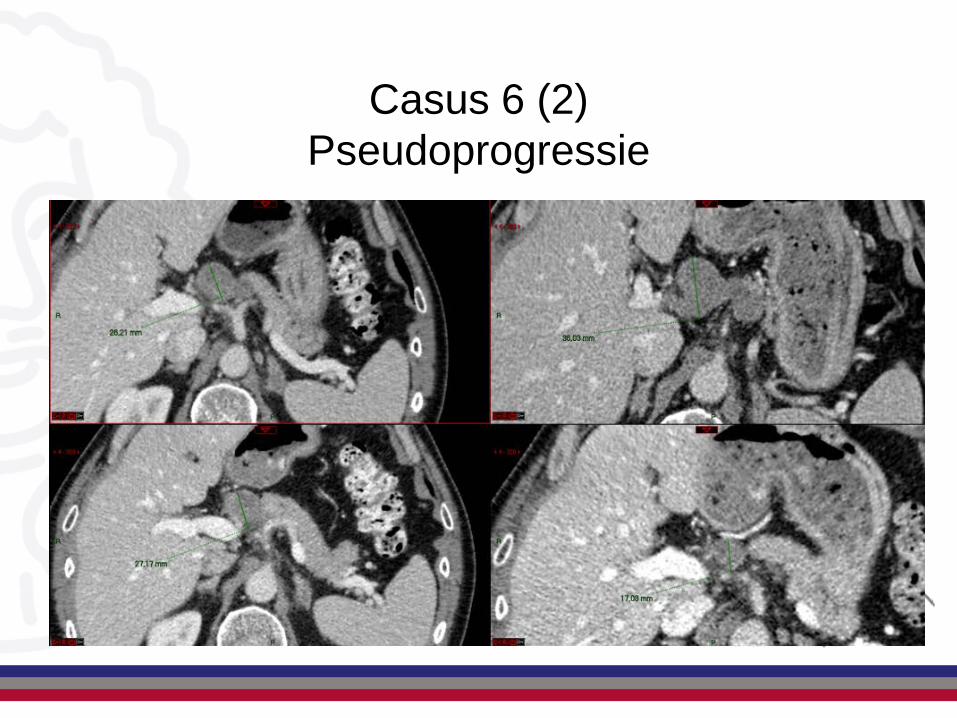
Casus 6 (2) Pseudoprogressie
SELECTIE PATIENTEN
Wat hebben we in onze handen om de patienten te selecteren
• PD-L1 expressie • Mutational load
– Roken – UV licht – DNA mismatch repair defect
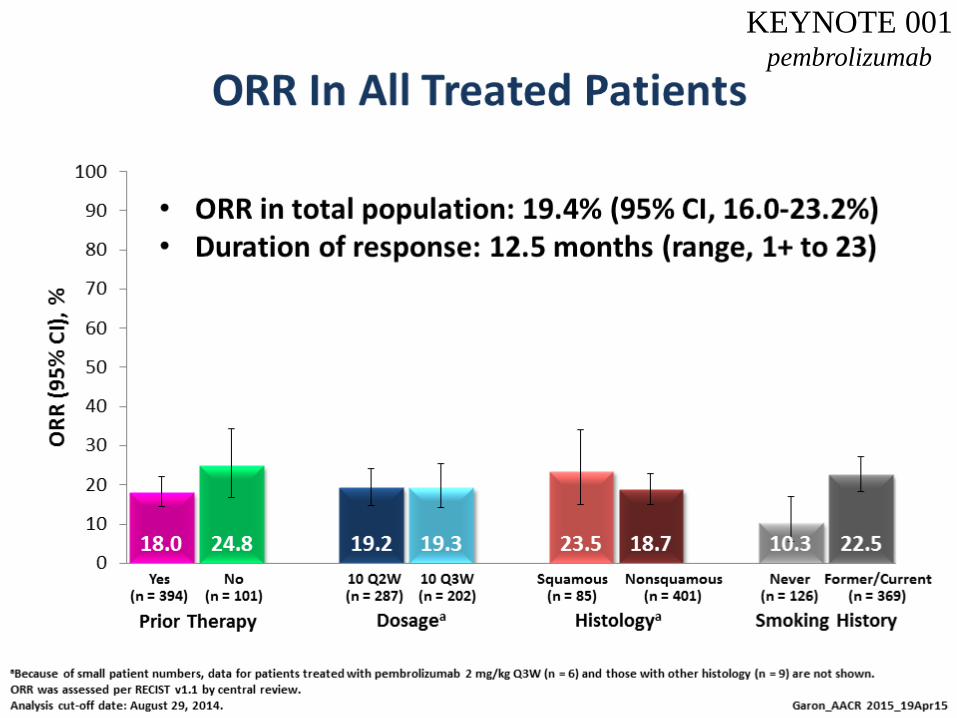
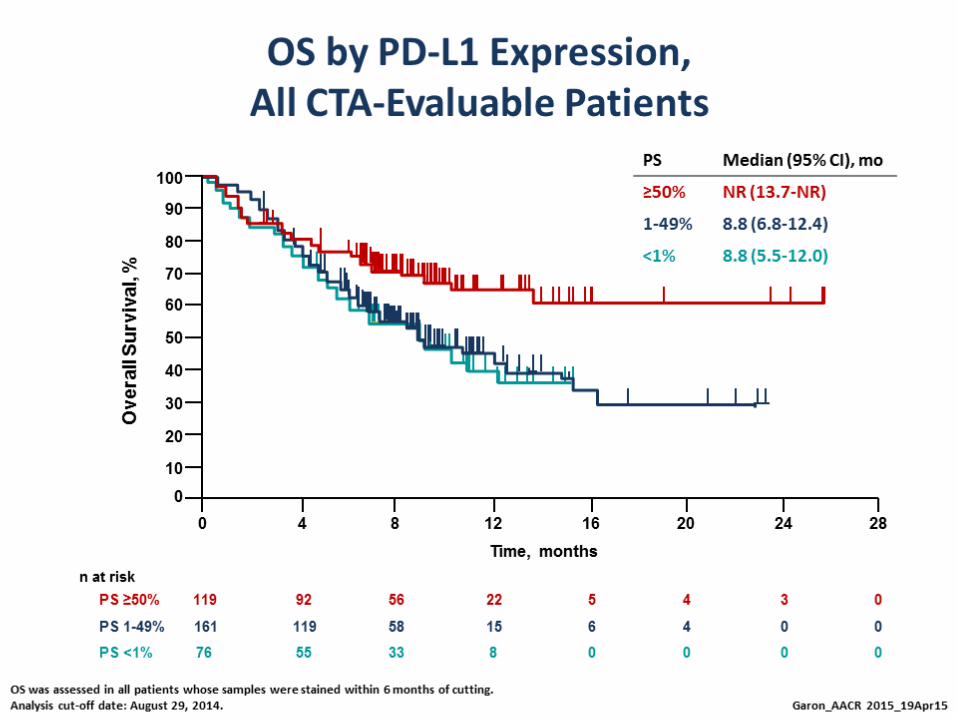
KEYNOTE 001 pembrolizumab
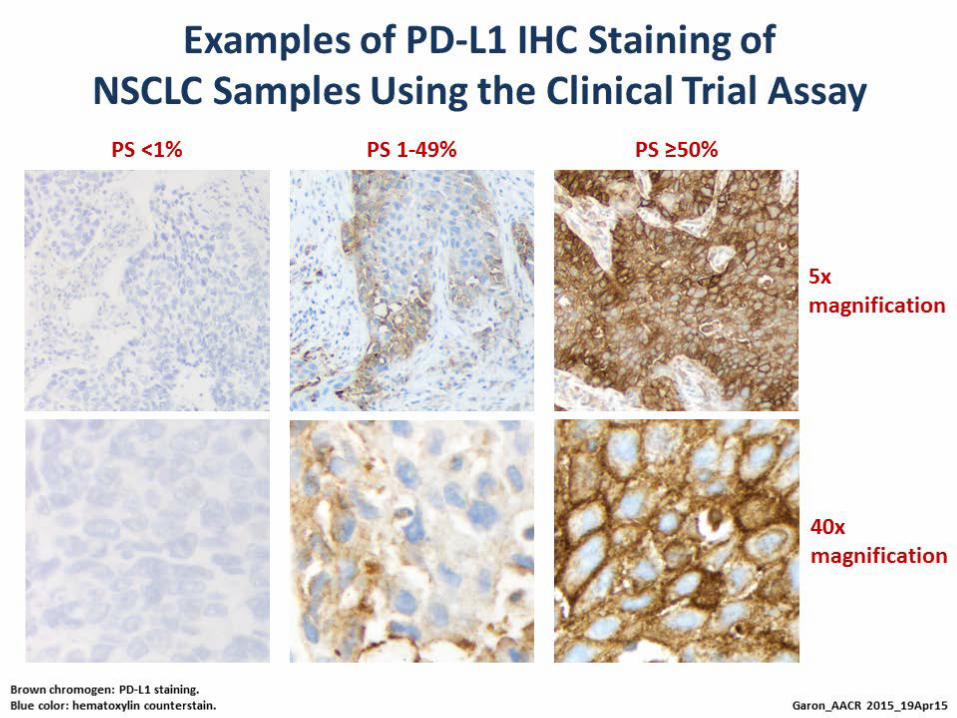
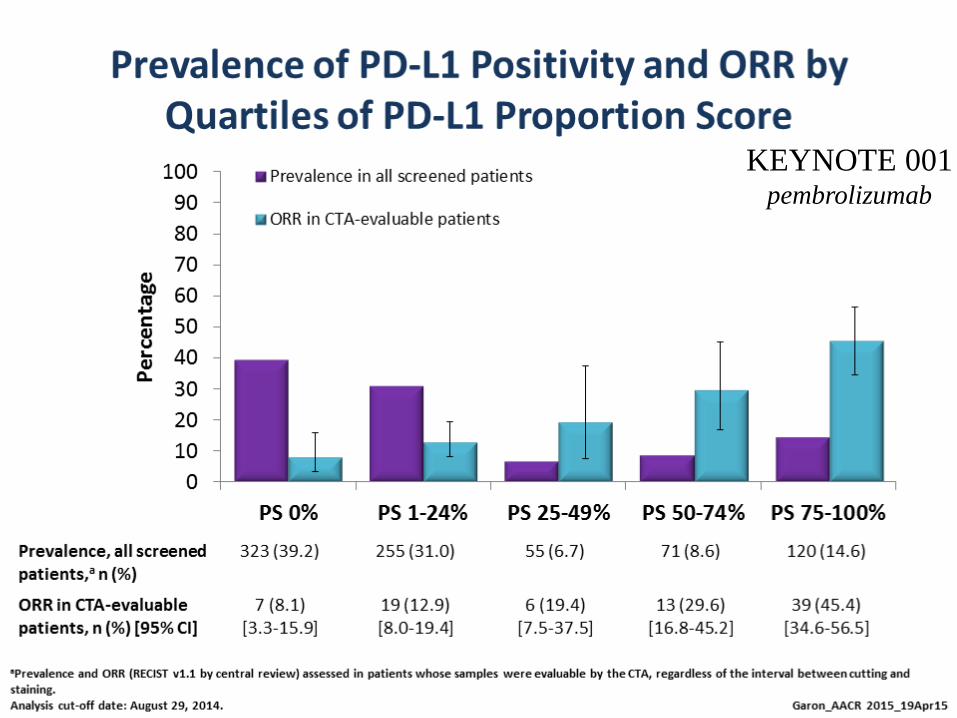
KEYNOTE 001 pembrolizumab
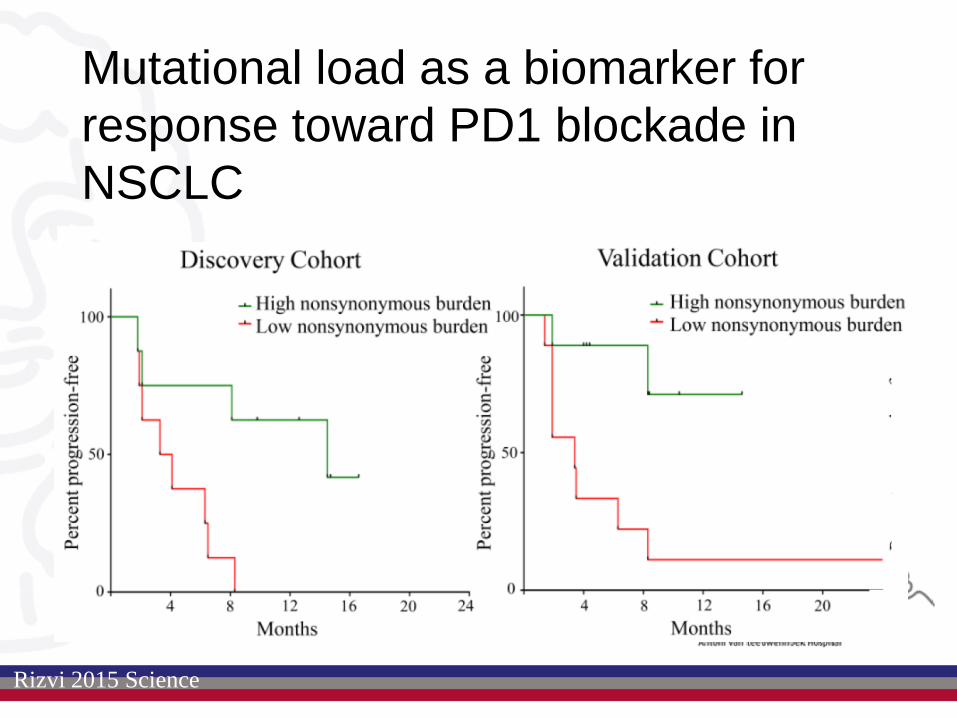
Mutational load as a biomarker for response toward PD1 blockade in NSCLC
Rizvi 2015 Science
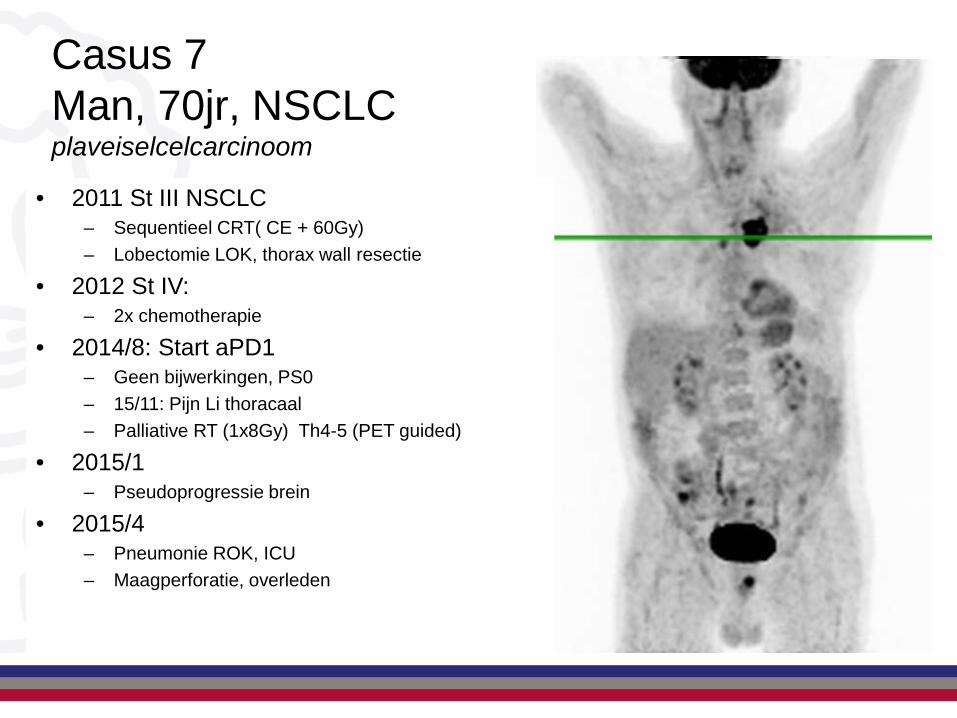
Casus 7 Man, 70jr, NSCLC plaveiselcelcarcinoom
• 2011 St III NSCLC – Sequentieel CRT( CE + 60Gy) – Lobectomie LOK, thorax wall resectie
• 2012 St IV: – 2x chemotherapie
• 2014/5: PD – Beenmergfalen
• 2014/8: Start aPD1 – Geen bijwerkingen, PS0 – 15/11: Pijn Li thoracaal – Palliative RT (1x8Gy) Th4-5 (PET guided)
• 2011 St III NSCLC – Sequentieel CRT( CE + 60Gy) – Lobectomie LOK, thorax wall resectie
• 2012 St IV: – 2x chemotherapie
• 2014/8: Start aPD1 – Geen bijwerkingen, PS0 – 15/11: Pijn Li thoracaal – Palliative RT (1x8Gy) Th4-5 (PET guided)
• 2015/1 – Pseudoprogressie brein
• 2015/4 – Pneumonie ROK, ICU – Maagperforatie, overleden
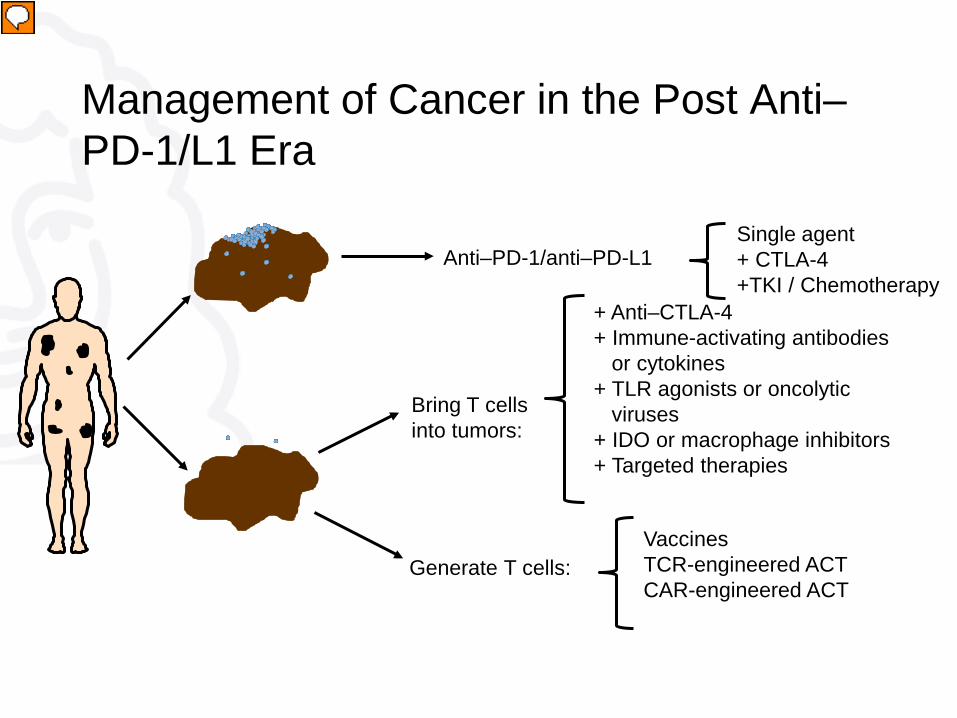
Anti–PD-1/anti–PD-L1
Generate T cells:
+ Anti–CTLA-4 + Immune-activating antibodies or cytokines + TLR agonists or oncolytic viruses + IDO or macrophage inhibitors + Targeted therapies
Bring T cells into tumors:
Vaccines TCR-engineered ACT CAR-engineered ACT
Management of Cancer in the Post Anti–PD-1/L1 Era
Single agent + CTLA-4 +TKI / Chemotherapy
Presentator
Presentatienotities
PD-1, programmed death 1; PD-L1, programmed death ligand 1; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; TLR, toll-like receptor; IDO, indoleamine-pyrrole 2,3-dioxygenase; CAR, chimeric antigen receptor; ACT, adoptive cell transfer.

Slide 30
Presented By Scott Gettinger at 2014 ASCO Annual Meeting