Clinical - AACB
40
Clinical NEWSLETTER NUMBER 65, JUNE 1982 PUBLISHED FOR THE AUSTRALIAN ASSOCIATION OF CLINICAL BIOCHEMISTS
Transcript of Clinical - AACB

Clinical N E W S L E T T E R
NUMBER 65, JUNE 1982
P U B L I S H E D F O R T H E A U S T R A L I A N A S S O C I A T I O N O F C L I N I C A L B I O C H E M I S T S

A U S T R A L I A N A S S O C I A T I O N OF C L I N I C A L B I O C H E M I S T S
Incorporated under the Associations Incorporation Act (SA)
Council, 1981-1982 Pres iden t : Maur ice L . W e l l b y , F R C P A , F A A C B .
r
M D , M S c , F R A C P ,
Vice-President: Peter M. D e n n i s , M B , F R A C P , F R C P A , F A A C B .
C h B , F R C P a t h ,
H o n o r a r y S e c r e t a r y : Rona ld C . B o w y e r , B S c , P h D , F A A C B , B i o chemis t r y Dep t . , R o y a l Per th H o s p i t a l , P e r t h , W A , 6 0 0 0 .
Hono ra r y T r e a s u r e r : Jan P i c k e r i n g , B S c , M S c , M A A C B , Division o f C l i n i c a l C h e m i s t r y , P r ince Hen ry Hosp i t a l , L i t t l e B a y , N S W .
C h a i r m a n o f the B o a r d o f E x a m i n e r s : Wi l l iam J . R i l e y , B S c , P h D , F A A C B .
Nat iona l Rep resen ta t i ve to t he I F C C : J o h n F . C o n n e l l y , M D , M A A C B .
B r a n c h Rep resen ta t i ves : Peter G r e e n a c r e , B S c , F A I M L S , M A A C B (New S o u t h W a l e s ) ; A n n e E . B a r r , B S c ( H o n s ) , M S c ( Q u e e n s l a n d ) ; R i c h a r d J . Maer-sche l , M S c ( S o u t h A u s t r a l i a ) ; C M . S h o w e l l , F A I M L S , M A A C B ( T a s m a n i a ) ; A l a n T o n g , B S c , M A A C B ( V i c t o r i a ) ; G a r t h W i l s o n , M S c , M A A C B (Weste rn A u s t r a l i a ) .
C H A I R M E N O F C O M M I T T E E S
E d u c a t i o n : Jean E . R o b i n s o n , B S c , M S c , F A A C B .
Pub l i ca t i ons : G r a h a m H . Wh i t e , B S c , P h D , M A A C B .
Scientif ic & T e c h n i c a l : T . Des G e a r y , B S c , M A A C B .
T H E
C l i n i c a l i o c h e m i s t
N E W S l [ I T E R
T h e Clinical Biochemist is pub l i shed f ou r t imes a year by the A u s t r a l i a n A s s o c i a t i o n of C l i n i ca l B i o c h e m i s t s , in M a r c h , J u n e , Sep tember and D e c e m b e r . Su i t ab l e c o n t r i bu t ions w o u l d be w e l c o m e d by the E d i t o r ,
N a n c y E . Da le , M S c , F A A C B , B i o c h e m i s t r y D e p a r t m e n t , R o y a l P r i nce A l f r e d H o s p i t a l , C a m p e r d o w n , N S W , 2 0 5 0 . T e l . N o : ( 0 2 ) 5 1 6 8 8 3 2 or 5 1 6 8 8 1 6 .
and mus t be rece ived b y 2 4 J a n u a r y , A p r i l , J u l y or O c t o b e r .
Other AACB Publications
include:
T h e Clinical Biochemist Reviews, c o n s is t ing o f E d u c a t i o n a l R e v i e w s and T e c h nical R e p o r t s f r o m the E d u c a t i o n and S c i e n t i f i c & T e c h n i c a l C o m m i t t e e s o f the A A C B .
T h e Clinical Biochemist - Proceedings, c o n ta in ing abs t rac ts o f papers presented at the A n n u a l C o n f e r e n c e o f the A u s t r a l i a n A s s o c i a t ion o f C l i n i c a l B i o c h e m i s t s .
S ta temen ts o f o p i n i o n are those o f the con t r i bu to rs and do not necessar i l y represent o f f i c ia l po l i c ies o f the A s s o c i a t i o n .
Printed by: Pub l i c i t y Press ( N S W ) , 6 6 O ' R i o r d a n S t r e e t , A l e x a n d r i a , N S W , 2 0 1 5 .
Published for the AACB by Associated Business Publications, 104/3 Smail Street, Ultimo NSW, 2007. Postal address PO Box 440, Broadway, 2007.
All advertising enquiries to Mr. Ian Col/ins, 212-2780, 212-3780.
Copyright © 1982 . T h e Austral ian Associat ion of Cl inical Biochemists I n c .
Registered by Austra l ia Post Publ icat ion No. N B P 2747
D E A D L I N E F O R S E P T E M B E R I S S U E IS 24 J U L Y , 1982
The Clinical Biochemist, Newsletter, June 1982

9
W e ' v e d o n e i t w i t h t h e V P S e r i e s I I F .
r Technology* of the future intro
duced by A B B O T T today. T h e V P " Series I I -F gives you 55 chemistr ies today and increased test ing capabil i t ies as addit ional I IA, E I A and FIA assays become available (single and . f multiple reagent addit ion).
Minimize your risks of obso lescence by choosing an instrument wi th mul t i - technology analysis modes. T h e V P Series I I -F.
FLUORESCENCE Amikacin Gentamicin Phenobarbital Phenytoin Primidone Theophylline Tobramycin
ABSORBANCE Albumin* Alkaline Phosphatase* AT-I I I * BUN* Calcium* Cholesterol* CK-MB* CK-NAC* GGTP* Glucose* Glycospec (MBA l t ,* HBDH* HDL* LDH* S G P T ( A L T ) * S G O T ( A S T ) * Tetrazyme (T4 )* Thyrozyme ( T 3 T B G )* Total Bilirubin* Total Protein* Triglycerides* Uric Acid* Acid Phosphatase Alcohol Aldolase Amylase Carbamazepine Chloride Cholinesterase c o 2
Creatinine Ethosuximide Lactic Acid IAP Magnesium Phenobarbital Phenytoin Phosphorous Primidone Theophylline
LIGHT SCATTERING Amphetamines Barbiturates Benzodiazepine Metabolite Cocaine Metabolite IgA* IgG* IgM* Methadone Opiates Propoxyphene
•Abbott A G E N T 1 " Chemistries
Abbott Diagnostics Division S y d n e y (02) 6 6 8 9 6 1 0 Melbourne (03) 8 1 3 1211 B r i s b a n e (07) 2 7 7 6 0 2 2 Per th (09) 3 6 2 1 9 4 4 Wel l ington N.Z. 2 8 5 0 7 0
The Clinical Biochemist, Newsletter, June 1982 3

FOR THERAPEUTIC DRUG CONTROL...
The ICL Sentiy" Provides Confidence, Assures Quality, Protection, and Vigilence!
"We Have Confidence In The Serum Drug Levels We Report Because Of The ICL Sentry Program."
It's a total program • controls for 14* therapeutic drugs • a variety of methodologies • three diagnostically critical levels; TDCI high (toxic), TDC II mid-range (therapeutic), and TDC III low.
Plus, The ICL Sentry, a 10ml vial of unassayed TDC which permits the lab to assay any of the 14 constituents for comparison of results obtained by leading regional reference laboratories.
And Sentry is available with each TDC kit...FREE! CHECK THESE ADVANTAGES! • Sentry— Intralaboratory proficiency program • 14 constituent assays in each 10ml vial • Stable for 30 days after reconstitution • Four Convenient Packages:
• TDC 1,12 x 10ml vials, plus 1 vial Sentry • TDC II. 12 x 10ml vials, plus 1 vial Sentry • TDC III, 12 x 10ml vials, plus 1 vial Sentry • Tri-Level Multi-Pack. 4 x 10ml vials each of
TDC I. II, and III. plus 1 vial Sentry. • No special diluents required • Human Serum Base • Two years dating, unreconstituted.
The ICL Sentry TDC Program... assures confidence in your drug level reports... maintains vigilence in your lab... insures patient care! Get the Sentry! Check with your ICL representative or call us direct.
"Carbamezepine. Ethosuximide. Pheno-barbital. Phenytoin. Primidone. Diso-pyramide. Lidocaine. Procainamide. N-Acetylprocainamide. Quinidine. Amikacin. Gentamicin. Tobramycin. Theophylline.
ICL SCIENTIFIC I (A part of the [ Boehringer Mannheim
Group)
B O E H R I N G E R MANNHEIM AUSTRALIA , P.O. BOX 316, NORTH R Y D E , N.S.W. 2113.
4 The Clinical Biochemist, Newsletter, June 1982

T H E
Clinical iochemist
N E W S L E T T E R NUMBER 65, JUNE 1982 Published for the A ustralian Association of Clinical Biochemists
Contents E D I T O R I A L 7 "What does the Future hold for Clinical Biochemists in Austral ia?"
P.M. Dennis
N O T I C E B O A R D 11 Ballot — Constitution Changes Election of Officers of the Association 1982-1983 Association of Clinical Biochemists' Jubilee Meeting Roche Diagnostics Travel Award Awards to Members (Roche Award and Ortho Travelling Fellowship) Position Wanted
13 Instructions re Abstracts of Papers and Posters — A A C B Conference — Adelaide 1982
R E P O R T S
A R T I C L E
14 Chemical Pathology Course 1982
23 "Monoclonal Antibodies" Margaret Stuart
NEWS O F M E M B E R S
R E G U L A R F E A T U R E S
19 From NSW — New Associate Members
15 Publications by A A C B Members 18 Book Review 19 Enzyme Column "Problems with Amylase Assays' 24 From the Education Committee 27 From the Scientific and Technical Committee 31 Forthcoming Meetings 35 Letters to the Editor 35 New Products and Developments 38 Chemical Crossword 1
B R A N C H NEWS 28 Tasmania and Western Australia
Front Cover "Colonel Light's Vision" by sculptor Birnie Rhind is erected on Montefiore Hill, North Adelaide and is a familiar landmark. The photograph is by Mark Fitzgerald and was provided by Dr. Tom Hartley of the 1982 Conference Committee. See page 9 for further information.
The Clinical Biochemist, Newsletter, June 1982 5

More than 2,900 clinical
laboratories worldwide hove already
cut health care costs with the
Du Pont aca.
Here's why: T h e unique Du Pont aca (Automatic Cl inical Analyzer) quickly and accurately analyzes blood and other body fluids for any of 4 2 different substances. It does only those tests requested by the physician. And it's ready for act ion 2 4 hours a day, every day of the year.
D u Pont research has t ransformed laborious chemistry procedures into compact test packs that no longer take up trained personnel 's valuable t ime. T h e blood sample and test pack are p laced into the aca , a button is pushed and the instrument does the analysis and prints out the result. T h e whole procedure is as s imple as that.
First results are available in
approximately 7 « minutes and succeed ing test results follow at the rate of about 100 per
hour. S T A T tests can be introduced at any t ime. Laborator ies using the a c a have reported increases in chemist ry vo lumes of up to 100% with no increase in staff numbers . In fact, the aca frees laboratory members for less mundane tasks, enabl ing an expansion of laboratory serv ices in other areas.
Let us give you a convinc ing demonstration of how you can cut your laboratory costs. Call us on ( 02 ) 8 8 7 1 3 3 3 , or write to Du Pont (Austral ia) Ltd., R o o m 4 4 2 . 168 Walker Street, North Sydney, N S W 2 0 6 0 .
Clinical Systems designed to advance with medic ine DP355
6 The Clinical Biochemist, Newsletter, June 1982

Guest Editorial m—
What Does the Future Hold for Clinical Biochemists in Australia? P.M. Dennis
Dr. P.M. Dennis
Recent editorials in our Newsletter have commented on various aspects of the Association as they were in its early days and as they are now. It is not unreasonable to ask what the future holds for clinical biochemistry in this country, a question which is of vital concern to all of us especially our younger colleagues.
We are now at a stage where clinical biochemistry in this country has come of age and our Association is a body to be reckoned with. The success of the A A C B today is proof of the energy and foresight of our founder members, whose work in the early days has been reviewed recently by the editor of the Newsletter. We can now boast a membership of almost 850, active branch and federal standing committees, a viable financial situation and a council which is very much concerned about the interests of all members and the future of clinical biochemistry in Australia. The A A C B is increasingly respected by professionals in the health field in this country and highly regarded by our colleagues internationally.
Our publications, although responsible for a major proportion of our annual expenditure and our treasurer's anxieties, have been very well received in Australia and are both widely and genuinely acclaimed overseas. The Clinical Biochemist is in my view one of the most tangible pieces of evidence for this "coming of age" of the A A C B .
The Technological Revolution
There is no doubt that clinical biochemistry has entered a technological revolution, the electronic age. Lasers, new electrode technology, microchips and integrated circuits have long since transformed our compliant and faithful old spectrophotometers, from the status of old friend to that of an impregnable automaton. There is every sign that these rapid and perhaps alarming changes are continuing in a way comparable to the renaissance or the industrial revolution. A major role of the clinical biochemist is to interpret the advantages of the technological revolution to both doctors and health administrators.
The clinical biochemist's ability to measure common analytes as well as hormones, drugs, neurotransmitters, receptor sites etc. has increased our repertoire at least three fold in the last 10 years and has provided a mass of information which creates intellectual indigestion in clin-
Dr. Peter Dennis is Director of Chemical Pathology and Chairman of Pathology Services at Prince Henry's Hospital, Melbourne and at present, Vice-President of the AACB. He has previously been a Chairman of the Victorian Branch, Chairman of the Education Committee (1979-81) and was national representative to the I FCC 1974 to 1980. He is an associate editor of Pathology and an editor of I F C C News.
He graduated in medicine from Otago University, New Zealand and trained initially in internal medicine and later in chemical pathology in New Zealand and at the Royal Postgraduate Medical School. At the latter institution he was engaged in research on the metabolism of adrenal corticosteroids with Dr. C.L. Cope.
His major continuing interests in clinical biochemistry are in the fields of endocrine chemistry, protein abnormalities and the application of computers in clinical laboratories. He is also concerned with promoting the best conditions for postgraduate training for clinical biochemists.
icians. New instrumentation based on rapid developments in analytical chemistry and physics have placed at the disposal of the clinical biochemists means of analysing minute samples quickly, accurately and precisely. What used to be termed micromethods 20 years ago may now be regarded as "macro or mega-methods".
Regrettably with the exception of atomic absorption spectroscopy there have been few major technological advances developed in Australia which have aided the clinical biochemist. Australia is small in terms of population, although almost twice the size of Sweden and three times that of Denmark, two countries which have made major scientific and technical contributions to clinical chemistry. There must be a lesson for us here. The future for clinical biochemists will be brighter if we can encourage our local industries to collaborate with us in methodological and technological developments as has occurred widely in Europe and North America. We will have to convince funding bodies and our governments of the necessity to support such ventures.
The Clinical Biochemist, Newsletter, June 1982 7

Automated Protein and Drug Analysis. Introducing the only totally
automated protein and drug analyser available.
This new system takes the field-proven ICS™ with its exclusive rate methodology and adds another dimension—that of walk-away capability. So you save technologist time, which saves you money.
And when you choose an Auto ICS , you also choose versatility. Because with the newly available drug kits, you can now
have a fast, accurate method for therapeutic drug monitoring. NO O T H E R S I N G L E S Y S T E M PROV I D E S T O T A L L Y A U T O M A T E D D R U G A N D PROTEIN T E S T I N G .
A sophisticated data processor makes the most of the 60-second assay to provide true panel testing. The selected protein or drug assays are performed and results printed before the instrument proceeds to the next patient sample. And the data processor also makes diagnostics and troubleshooting easy.
A manual version is
also available which can be updated to an automated system at any time.
So when you want total capability for your drug and protein assays, choose the Beckman ICS Immunochemistry System.
For more information contact Beckman Instruments (Australia) Pty. Ltd., Analytical Instruments Sales & Service Operation, 24 College St., Gladesville, N.S.W., or telephone Sydney (02) 896-2288, Melbourne (03) 544-3144, Adelaide (08) 268-4828, Brisbane (07) 369-9896.
• i 1
~ 1
E C K M AIM 8 The Clinical Biochemist, Newsletter, June 1982

Career Opportunities for Clinical Biochemists
We have clearly been through the "logarithmic" phase of growth in the number of positions for clinical biochemists in this country and are now approaching a plateau. A decline in the number of positions would be unthinkable. There have already been some ominous signs that reductions could occur due to a process euphemistically called rationalisation, which appears to apply to many sections of our community but not necessarily to the numbers of our representatives in parliament.
The quality of young graduates entering the field these days tends to be higher than it was ten years ago, undoubtedly reflecting the deteriorating ratio between the production rates of institutes of tertiary education and available posts for clinical biochemists. There is not much immediate hope for improvement here, a fact which university departments for obvious reasons, sometimes omit to tell their undergraduate students.
Another black cloud on the horizon is the temptation for employing authorities, facing a financial squeeze, to use cheaper (non-graduate) staff. Obviously there must be an ideal balance of clinical biochemists, technologists and technicians in any laboratory, but it is one's observation that a more effective diagnostic service wil l generally be provided by laboratories with higher proportions of graduate staff. This is due to better liaison with clinicians and a better appreciation of the requirements of clinicians.
Post Graduate Training and Qualifications for Clinical Biochemists
The Association has recognised the importance of these aspects for many years, and some impetus was given to clinical biochemists to pursue post graduate study by the creation of Membership and Fellowship examinations. The Education Committee which was restructured in 1979 has been vigorous in many activities, not the least being publications of 77ie Clinical Biochemist — Reviews and Bibliographies, The Technical Bulletins prepared by the Scientific and Technical Committee represent another important source of educational material. However in this writer's view post graduate education is a very personal activity and no amount of courses, tutorials or seminars will force the unmotivated to succeed.
There has been some debate about the value of acquiring post graduate qualifications both professional and academic in clinical biochemistry. There is no doubt in my mind that the growing number of personnel holding such qualifications in our ranks has strengthened the health services in this country and improved the scientific statute of our discipline. Thus one should encourage clinical biochemists at all levels to be continually and actively involved in post graduate education and promote the value of our Association's qualifications.
It is hoped that young clinical biochemists do not regard the acquisition of a post graduate degree or diploma as merely an automatic ticket to promotion (although this is a perfectly understandable view), but rather as evidence of professional and academic excellence. Fortunately governments and most employers now recognise the Association's qualifications as a reliable indicator of a clinical biochemist's competence.
The Role of the Clinical Biochemist
The major contributions which clinical biochemists make to patient care is well recognised by most clinicians.
The Clinical Biochemist, Newsletter, June 1982
It is the nature of this involvement which clinical biochemists should be considering.
Regrettably many doctors still regard the role of laboratory scientists merely to provide a reliable and quick service; unfortunately, the latter attribute impresses some of our medical colleagues most. An encouraging change which has come with the appreciation of the qualities of clinical biochemists is the readiness of clinicians to involve us in consultations and case discussions. Some clinical biochemists may see this as a waste of time and their energies better spent in the pursuit of excellence within their laboratories.
It has been pointed out by many distinguished clinicial biochemists that it is the unanswered questions in medicine which present the greatest challenges to our field. As Professor Laurell reminded us, the gold for clinical chemistry is to be found in the stream of medicine. The high standards of clinical biochemistry laboratories in this country is well recognised and must be maintained while at the same time the clinical role of the biochemist is to be encouraged.
9
M E S S A G E F R O M T H E E D I T O R
I apologise for the lateness of this Newsletter but I am most grateful for the assistance of John Whitfield and his help in collating the material when a room in Gloucester House ( R P A H ) became the temporary editorial office of the Newsletter. I think that only those members who have had dealings with our Publisher, Keith Collins, realise the extent of his ready help and co-operation so no-one will be surprised to hear that Keith virtually put this issue together, even to the extent of chasing up tardy contributors. (Usually an editorial responsibility.) Once again I thank him on my own behalf and on behalf of the whole association for all that he does towards making our publications successful.
2 1 S T A N N I V E R S A R Y A N N U A L A A C B C O N F E R E N C E
A D E L A I D E , 1982
As in previous years, the front cover of the June issue of the Newsletter carries a picture of the city which is hosting the Annual Conference. Colonel Light's comments are reproduced here:
'The reasons that led me to fix Adelaide where it is I do not expect to be generally understood or calmly judged at present. My enemies, however, by disputing their validity in every particular, have done me the good service of fixing the whole of the responsibility upon me. I am perfectly willing to bear it; and I leave it to posterity, and not to them, to decide whether I am entitled to praise or blame'. William Light in the Preface of his Brief Journal 1836-1837.
Full details of the meeting were printed in the December issue of the Newsletter ( 1981 , 63, 11) and information concerning abstracts appears on page 13 of this issue. A registration form is also enclosed. The South Australian committee is hoping for a large attendance at the meeting to celebrate our 21st Birthday.

10
COLORI METRIC T R I G L Y C E R I D E S SVR
5-minute end-point — reaction — 5-day reconstituted — stability
Human Serum base — calibrator —
Linearity to 700 mg/dl —
No reagent blanking — required —
No caustic reagents —
Single Vial —
Rapid throughput Saves time Reduced reagent wastage Saves money More reliable results Reacts in same way as patient specimens Reduces expense of repeats Saves time Reduces cost Safe for personnel and equipment Fewer pipetting steps Saves time Reduces error
T R I G L Y C E R I D E S AUTOMATED R E A G E N T
CALIBRATOR • Human Serum Based —
5-day Reconstituted Stability Pack Size
Reacts in similar manner to patient sera More accurate and reliable results Reduces wastage Saves money 10 x 2.0 ml
C CALBIOCHEM-BEHRING AUSTRALIA PTY LIMITED
P.O. Box 200 Kingsgrove NSW 2208 Telex AA20484 Telephone: Sydney (02) 502 3755 • Melbourne (03) 51 0668 • Brisbane (07) 44 3661
• Adelaide (08) 352 2655 • Perth (09) 386 6311
The Clinical Biochemist, Newsletter, June 1982

AACB NOTICE BOARD NSTtCtlOMO
B A L L O T - C O N S T I T U T I O N C H A N G E S
Because of delays in mailing ballot papers to some NSW members, the returning officers decided to accept all votes received by the Federal Secretary up to and including 20 April 1982.
The results of the Ballot are as follows: 236 votes were received, of which 233 were valid votes
(98.7%). Al l motions were passed with a comfortable majority,
which was in each case between 94 and 97% of the valid votes.
E L E C T I O N O F O F F I C E R S O F T H E A S S O C I A T I O N F O R 1 9 8 2 - 1 9 8 3
The Secretary reports that as only one nomination was received for each of the four positions, the following have been elected.
President: Dr. M.L. Wellby. Vice-President: Dr. P.M. Dennis. Treasurer: Miss J . Pickering. Secretary: Dr. R.C. Bowyer. Neither Dr. Wellby nor Dr. Dennis will be eligible for a
further term in the same office.
A S S O C I A T I O N O F C L I N I C A L B I O C H E M I S T S
W E S T M I D L A N D S R E G I O N
A J U B I L E E M E E T I N G
will be held in Birmingham on 19-20 J U L Y 1983
to celebrate the
30TH A N N I V E R S A R Y O F T H E F O R M A T I O N O F T H E R E G I O N
and the
6 0 T H B I R T H D A Y O F P R O F E S S O R T O M W H I T E H E A D
The scientific programme will include symposia on:
New analytical techniques Quality Assurance Clinical Chemistry and the Community The meeting wil l have a wide appeal with disting
uished national and international speakers. There wil l be a trade exhibit ion, poster sessions
and a Gala Dinner. Ful l details and registration forms will be available
early in 1983. Al l enquiries should be addressed to: Dr. D.J . Worthington, Clinical Chemistry Department, Queen Elizabeth Hospital, Edgbaston, Birmingham B15 2TH
R O C H E D I A G N O S T I C S T R A V E L A W A R D
During 1982 Roche Diagnostics will sponsor a Travel Award in connection with the Annual Scientific Meeting of the Association being held in Adelaide. The award will apply to travel, accommodation and registration costs for one person.
The award is open to any financial member of the A A C B who is currently employed in the clinical biochemistry field in Australia. It will be administered by the A A C B Council or their nominees, who will select an applicant on the basis of a submitted paper to be delivered at the Adelaide meeting.
There are no stipulations as to content or nature of the submitted work other than it be relevant to the practice and advancement of clinical biochemistry in the Asian Pacific region. An application form is included in this issue and is also obtainable from the Honorary Secretary of the A A C B , to whom interested persons should forward their application by 31 August 1982. The completed work must be submitted by 1 October and should conform to the normal regulations governing congress papers.
The Association greatly appreciates the contributions made by Roche Products Diagnostic Division, both in providing the two Travel Awards to Adelaide and Singapore and in many ways in the past
A W A R D S T O M E M B E R S
Congratulations to the two members who were successful - to all the others try again!
Roche Award for Singapore - Mr. Timothy J . Wilke from the Commonwealth Department of Health, Too-woomba, Queensland, for a paper concerning anomalous F T I values in patients with altered TBG-capacity.
Ortho Travelling Fellowship Award - Mr. David M. Rutherford from the Biochemistry Department of the Alfred Hospital, Melbourne. His program is still subject to revision but his general aim is to improve his knowledge of quality control programmes for urine toxicology by visiting eminent toxicologists in the USA.
P O S I T I O N W A N T E D
The Editor has received a letter from one of our overseas members, Mui Soot-Fong who is shortly leaving Malaysia to reside in Sydney.
Her husband is studying at the University of NSW and she would like a position somewhere near that University. A t present she is employed as a hospital biochemist at the Kuala Lumpur General Hospital in a laboratory which performs a wide variety of investigations.
Mui Soot-Fong has provided a detailed account of her experience which is available from the Editor.
The Clinical Biochemist, Newsletter, June 1982 11

M a l l i n c k r o d t • ®
DIAGNOSTICS Dai-lchi — Nummer een — Nummer ein — Numero uno — Numero urn
NO MATTER HOW YOU SAY IT
I T S T I L L M E A N S N o . 1 whether it be Generators, Cold kits, Isotopes or the
Mallinckrodt, Frosst and Immuno Nuclear Corp. ranges of RIA Kits.
Quality assurance and service are No. 1 at Mallinckrodt Australia and its world wide affiliates. Our staff, both in Australia and Overseas work day and night to ensure that the product reaches you on schedule and as close to peak performance as is humanly possible. We never give up — even during difficult times (for all of us) when severe dislocation of transport is experienced.
For further information or technical service please call
Mallinckrodt m a k e s t h e c r i t i c a l d i f f e r e n c e
Mallinckrodt Australia Pty. Ltd. P.O. Box 194. Clayton, Victoria. 3168 Melbourne (03) 579 2211. Sydney (02) 713 6575
Mallinckrodt also offer re-usable plastic laboratory ware and the Johns disposable range • Barosperse (Barium Sulphate) and the N.C.C. Line of Catheters.
12 The Clinical Biochemist, Newsletter, June 1982

I N S T R U C T I O N S R E A B S T R A C T S O F P A P E R S A N D P O S T E R S T O B E P R E S E N T E D A T T H E 2 1 S T A N N I V E R S A R Y A A C B C O N F E R E N C E
IN A D E L A I D E , 2-5 N O V E M B E R , 1 9 8 2
A . T h e dead l i ne fo r rece iv ing abs t rac ts is 26 July 1982.
B . A b s t r a c t s are to be sen t t o : D r . R . A . J . C o n y e r s , I ns t i t u te o f Med ica l and V e t e r i n a r y S c i e n c e , P O B o x 1 4 , R u n d l e S t r e e t , A d e l a i d e , S A , 5 0 0 0 .
C . I n d i c a t e w h e t h e r y o u w o u l d p re fe r to present y o u r w o r k as a poster o r an o ra l p resen ta t i on .
D. P r e p a r e y o u r abs t rac t to c o n f o r m w i t h the f o l l o w i n g :
1 . Use A 4 size paper and t ype t e x t Vh s p a c e d .
2 . A m a x i m u m o f 3 0 0 w o r d s is ava i lab le f o r the a b s t r a c t t e x t .
3 . Marg ins o f 2.5 c m shou ld be le f t on each s ide , w i t h a 2 .5 c m space a t the top and b o t t o m o f each page.
4 . T y p e the t i t le o f the paper in U P P E R C A S E le t te rs 2 .5 c m f r o m the t o p edge o f the page.
5 . T y p e the n a m e ( s ) o f the a u t h o r ( s ) t w o spaces b e l o w the t i t le . Under l ine the name o f the a u t h o r p resent ing the paper .
6 . T y p e the pro fess iona l address(es) o f the a u t h o r ( s ) t w o spaces be low the au tho r ( s ) n a m e ( s ) . Unde r l i ne addresses.
7 . L e a v e a doub le space and p roceed w i t h the abs t rac t us ing 1/2 spac ing .
8 . Pho tog raphs o r d iagrams shou ld N O T be used . A sma l l tab le a n d / o r re fe rences m a y be inc luded i f requ i red bu t the t e x t shou ld be shor t ened acco rd ing l y .
9 . R e f e r e n c e s shou ld f o l l o w the s t y le o f The Clinical Biochemist -Reviews, V o l . 2 , N o . 3 . , e.g. , G O R S K Y , J . E . , and D I E T Z , A . A . , Clin. Chem. 2 4 , 1 4 8 5 ( 1 9 7 8 ) .
1 0 . O n l y s tandard or c o m m o n l y accep ted abb rev ia t i ons s h o u l d be used .
1 1 . S . I. un i ts and the i r s tandard abb rev ia t i ons shou ld be u s e d .
1 2 . I n genera l , the l a y o u t g iven in The Clinical Biochemist — Reviews,
V o l u m e 2 , N o . 3 , Oc tobe r 1 9 8 1 , shou ld be f o l l o w e d .
E . A u t h o r s m a k i n g ora l p resen ta t ions shou ld ind ica te w h e t h e r t h e y w i s h the i r papers t o be cons idered fo r the pr ize .
. / The Clinical Biochemist, Newsletter, June 1982 13

Chemical Pathology Course — 1982
A new venture was undertaken in the chemical pathology course for this year, as a residential venue was chosen and it was hoped that most registrants would live in full-time. The course was held from Sunday, 28 February to Friday, 5 March, 1982, at the Institute of Administration of the University of New South Wales, which is situated in the grounds of Prince Henry Hospital at Little Bay. Initial planning for the course commenced in February, 1981, and the final composition of the organising committee was:
David Rothfield (Chairman) Matthew Meerkin Daya Naidoo Jean Robinson Margaret Stuart Lindsay Wyndham The Institute of Administration is situated near the edge
of the cl i f fs overlooking Litt le Bay and is surrounded by a golf course. The residential accommodation, for a maximum of 7 0 registrants, consists of single rooms with private facilities. There are two main seminar rooms, the larger of which can hold 100 people, and ten small syndicate rooms. The seminar rooms are well equipped with all audio-visual aids and the syndicate rooms have large tables and comfortable chairs for round-table discussion, together with blackboards and stands with large sheets of white paper for preparing reports. Overhead transparencies for syndicate reporting were provided by the course committee.
All meals, from dinner on Sunday evening until afternoon tea on Friday afternoon, were included in the full registration, with the exception of the special course dinner, which was held on Monday evening and for which an extra charge was made. Day registrants were entitled to all meals except breakfast. There was a common room with a bar which opened before dinner and after the evening sessions, when coffee was also provided. The staff of the Institute was helpful in all areas and from comments received the venue was considered a great success. Some people who had registered as day registrants took the opportunity to live in after they had seen the facilities — and others wished they had done so! Certainly a far greater interchange among participants resulted from being in residence.
There was a total of 86 registrants, 21 of whom were medically qualified. Registrants in full-time residence numbered 49 and 19 attended each day as full-time non-resident registrants. The remaining 18 were able to attend on some days only, a total of 34 day registrations being received from them, and two of these lived in part-time. Two speakers were also in residence for part of the time. All members of the committee except Lindsay Wyndham also lived in — Lindsay delivered a daughter on the Wednesday preceding the course and had to be excused! She had contributed a great deal to the preparations for the course, particularly in relation to the sessions on renal function.
There were 20 full-time registrants from Victor ia, nine from Queensland, three from Western Australia, two each from Northern Territory and South Australia, one each from the Australian Capital Territory and Tasmania and 30 from New South Wales. There was one part-time registrant from A C T and there were 17 from NSW. Sixty-one people
returned the questionnaire given to each registrant and 39 of these gave continuing self-education as their purpose for attending the course. Eight were preparing for the F R C P A examinations, 13 for the M A A C B , one for the F A A C B , two for the F A I M L S and one for an MSc in Clinical Biochemistry. Four people were attempting to obtain more than one further qualification.
It was decided that the course should have two major themes and one minor theme and the planning followed this aim. The first major theme was renal function and this occupied the first two days of the course, with four didactic sessions on all aspects of renal function, one session partly didactic and partly discussion on development of a method related to renal function and two sessions of a tutorial nature. The first of these "syndicate" sessions was devoted to five different topics, each of which was covered by two different groups to which a syndicate adviser had been appointed and the second session involved members of the groups reporting their findings to a combined audience. The topics covered both clinical and technical aspects and registrants were allotted to groups prior to the course. No choice was allowed; groups were composed of a mix based on discipline, sex and state so that each group had a similar composition. A brief to the syndicate and a pre-course reading list for the topic was sent out before the course.
The sessions on renal function flowed together very smoothly and it was obvious that the speakers had communicated with one another before the course. We were very fortunate that Dr. L . J . Barratt, our special guest speaker from South Australia, was able to remain with us until the end of the syndicate reporting session and to coordinate the reporting at that session, as he gave a definite continuity to the whole topic. The presence of such a speaker who is not liable to be called away was a great advantage.
The second major theme was diabetes, and this also occupied the larger part of two days. There were six main speakers, mostly drawn from experts from the local scene, but Prof. G. Kellerman came down from Newcastle to share his expertise. There were seven syndicate groups for the session on diabetes and for all but two of them pre-course briefs were sent out. Once again a mix of registrants was arbitrarily placed into each syndicate, each with its syndicate adviser. Three groups only were duplicated for this session — coma and ketoacidosis, diabetes mellitus in pregnancy and hypoglycaemia. The syndicate advisers for the last topic elected to combine into one larger group. We were indebted to Dr. W. Kidson, one of the main speakers on the Wednesday, who returned on Thursday morning to coordinate the syndicate reporting.
The rest of Thursday was made up of two smaller sessions, one of "the abc of Beer's L a w " and the other on pH and blood gas measurement, which fitted in with both the major themes.
On Tuesday and Thursday evenings, the after-dinner sessions were spent in "test-and-teach" exercises based on the themes which had preceded them.
The minor theme, which occupied the whole of Friday morning, was alcohol. Once again local experts gave their time to address the course from several points of view of
14 The Clinical Biochemist, Newsletter, June 1982

this, the cause of so many of the problems seen daily in our hospitals.
The final session on Friday afternoon was on algorithms of various parameters which had been covered throughout the week. Once again we broke into groups for the first part of the session then returned to report the findings in the second part. Fortunately by this time a degree of levity was apparent, as saturation point (of learning, one hopes, and not of the substance discussed above) had been reached by at least some of the participants, and while we were assured that algorithms were logical sequences in decision-making, some people were not convinced of their value and one Derson suggested that they were like biochemical Monopoly!
A pre-course reading list was sent to all registrants at the same time as the briefs for the syndicates and included reading for almost all of the sessions of the course.
Course notes on all the major sessions were off-set printed by a commercial firm and were available in a folder generously provided by A H S at the time of registration. Abstracts for the syndicate sessions were also printed and were made available after the reporting sessions were completed, all registrants receiving all abstracts. One of the syndicate sessions on diabetes was the only topic for which no abstract was provided.
Reservation of the Institute of Administration immediately committed us to a minimum outlay of $12,000, as they required a minimum registration of 50 full-time residential participants at $48 per day for five days. We were to a degree concerned when the final day for registration — 15 January — was reached with only 36 registrants, not all of them residential, but as always happens this number more than doubled by starting time. As the $48 a day covered accommodation, all meals except the course dinner and use of all the facilities of the Institute, a full registration of $275 was derived, the extra $7 a day being thought sufficient to cover other expenses. As it was hoped that most people would register as residents, the daily registration for non-residents was pitched a little higher than necessary as a mild deterrent to registering full-time on a nonresidential basis, but this deterrent was unsuccessful. The financial statement is given.
The general consensus seems to be that a very successful
week was held. The educational material was of a high standard, thanks to the experts who gave their time to contribute. The success of the syndicate sessions was due to a combination of active pre-reading by the participants, live-in conditions and effective guidance and preparation by the syndicate advisers. The venue was excellent, the "rest and recreation" periods served a useful purpose in achieving an atmosphere of leisure yet extending the available teaching time into the late afternoons and evenings and the interaction among those in residence was tremendous.
C H E M I C A L P A T H O L O G Y C O U R S E - 1 9 8 2 Statement of Receipts and Payments
R E C E I P T S $
Full registrations 49 13475.00 Day registrations 129 5805.00 Upgrade to o/night stay 5 50.00 Accommodation F r i . night 3 60.00 Course dinner 52 520.00 Course notes 105.00
Total 20015.00
P A Y M E N T S $ $
Printing: Course notes 626.80 Postage and Freight 100.00
Receipts/course notes/folders to Institute/general
Institute of Administration 15495.27 Sundries: Transparencies, etc. 129.60
Total 16351.67
P R E L I M I N A R Y N E T S U R P L U S 3663.33
The gift of a botanical print, costing $75 was made to the Institute of Administration. The above net surplus will therefore be decreased by that amount.
Jean Robinson, Royal Hospital for Women, Paddington NS W
(on behalf of the Committee)
Publications by AACB Members
From the Chemical Pathology Department, Prince Henry's Hospital, Melbourne, Victoria.
"Editorial — The Electrophoresis and Assay of Serum Proteins — A Changing Scene", P.M. Dennis, Pathology, 1981 , 13, 6 5 1 .
"Monitoring Induction of Ovulation by Rapid Radioimmunoassays of Oestrogen and Pregnanediol Glucuron-ides", A . R . MacLean, K . H . Outch, J.M. Russell, J . B . Brown and P.M. Dennis, Annals of Clinical Biochemistry, 1981, 18, 343.
From the Department of Histology and Embryology, University of Sydney, Department of Perinatal Medicine, King George V Hospital, Department of Paediatrics, Prince of Wales' Children's Hospital, Randwick and the Biochemistry Department, Royal Prince Alfred Hospital, Camper-down, NSW.
"Measurement of 'Lamellar Body Phospholipid' in Amniotic Fluid as a Method for Assessing Fetal Lung Maturity", C . G . Duck-Chong, D.J . Henderson-Smart, J.M. Gupta and W.J . Hensley, Clin. Chem., 1981,27 , 1851.
The Clinical Biochemist, Newsletter, June 1982 IS

Introducing the Hitachi 705 The Versatile Analyzer that Gives You the
Assay Results You Want, When You Want Them.
Reagent pipetting systei
Serum pipetting system'
Reaction disk
Sample carousel
Printer
CRT display
Reagent refrigerator
Keyboard
Control unit
boehrinqer w BOEHRINGER MANNHEIM AUSTRALIA PTY. LTD.

H I T A C H I 7 0 5 The new generation of multi-analyzing
systems for clinical chemistry Performs profiles, organ panels, Individual tests, and STATs with equal ease The Hitachi 705 represents a new generation of advanced, discrete, selective, fully automated chemistry analyzers. This self-contained analyzer system utilizes multi-wavelength photometry, a sophisticated microcomputer, and high quality Boehringer Mannheim Diagnostics reagents to give you the assays desired, when you want them, simply and economically.
The Hitachi 705 Offers: Complete test selectivity—you can choose profiles, organ panels, or selected single tests on any sample with pushbutton ease Up to 19 simultaneous assays on a patient specimen, including electrolytes via an optional ISE module Automatic keyboard STAT priority— STATs can be introduced at any time during a routine run; once the STAT is analyzed, the Hitachi 705 automatically returns to the next routine sample Serum indexes— numerical estimates of icterus, turbidity, and hemolysis can be measured and printed out Calculated between-test parameters— up to ten between-test parameters can be calculated and printed out along with the test results
Choice of seven end point (equilibrium*) and kinetic methods of analysis— among these are one and two reagent end point methods and serum and trigger start kinetic methods (variable sensor-signal, regression method according to Pardue*) Quality chemistries—specially packaged Boehringer Mannheim Diagnostics reagents perfectly complement the sophisticated data processing capabilities of the Hitachi 705 to bring you quality assay results. Operating simplicity—the computer-controlled Hitachi 705 is simple to use and ideally suited for dependable 24 hour a day operation
the Hitachi 705 is designed to significantly reduce instrument operating costs through features such as an advanced positive displacement pipetting system, a standby mode that does not consume reagents, infrequent calibration, and reagent volumes as low as 350 /it per test
Hitachi and Boehringer Mannheim Diagnostics ... the only names you need to know when you're ready for a fully automated chemistry analyzer.
'Pardue, H.L., "A comprehensive classification of kinetic methods of analysis used in clinical chemistry," Clin. Chem. 23, 2189 (1977).
This Compact, Selective, and Uniquely Versatile Chemistry Analyzer System Answers Your Laboratory Needs . . . 24 Hours A Day
I/Os BOEHRINGER MANNHEIM AUSTRALIA PTY. LTD. | boahrintjer 6 g BYFIELD STREET, NORTH RYDE 2113 TELEPHONE (02) 888 2122

From the Department of Clinical Biochemistry, The Flinders Medical Centre, Bedford Park, SA.
"Effect of Feedback to Clinical Staff of Information on Clinical Biochemistry Requesting Patterns", A.R. Grivell, H.J. Forgie, C.G. Fraser and M.N. Berry, Clin. Chem. 1981, 27, 1717.
"Analytical Goals for Quantitative Urine Analysis: A Clinical View", M.D.S. Shephard, L.A. Penberthy and C.G. Fraser, Clin. Chem. 1981, 27, 1939 (Letter).
"Commentary: Acceptable Performance Standards for Clinical Laboratory Methods", C.G. Fraser,/. Of Automatic Chemistry, 1982, 4, 1 . ,
"Urinalysis in an Australian Teaching Hospital", M.D.S. Shephard, L.A. Penberthy and C.G. Fraser, Med. j. Aust., 1982, (3 April) 300.
From the Department of Clinical Biochemistry, Queen Elizabeth II Hospital Medical Centre, Nedlands, WA 6009.
"Importance of Fasting Plasma Glucose Concentration and Obesity in the Interpretation of Fasting C-Peptide Values", P. Garcia-Webb, A. Bonser and D. Whiting, Clin. Chim. Acta. 1982, 118, 323.
Book Review
Biochemical Investigations in Endocrinology — Methods and Interpretations, Ade l A. A. Ismai l , 275pp , A c a d e m i c Press 1 9 8 1 , $36 .30 .
There are a vast array of endocrine tests currently employed in clinical endocrinology. In the past many of these tests were only performed under the direct control of an endocrinologist and an endocrine laboratory. However, with the increasing availability of these tests to clinicians, biochemistry departments are being more involved in the performing and sometimes in the interpretation of the various biochemical-endocrine tests. This book is written as a practical guide to the more common biochemical tests in endocrinology.
This book is very clearly and concisely written and takes a very practical approach to the problems. As such it therefore fulfills a real role as many of the larger text books in endocrinology are often difficult to read, do not give precise information about interpretation of the various tests and by their very nature, are frequently out of date. The author has deliberately attempted to bring the information together in the most straightforward and practical manner and to give all the important information in the shortest possible form. All the chapters are set out in a similar manner, giving a brief physiological, biochemical background to the endocrine disease, followed by an outline of the various dynamic tests available. It attempts to give per
spective to the diagnostic potential of each test and give clear guidelines as to the interpretation of the test results. In many of the chapters a simple scheme in the form of flow sheets are provided to take the reader through the stages of endocrine testing for a particular disease. At the end of each chapter a reasonable reference list for further reading is provided. The index is divided into three sections, Section 1 listing under hormone assays, patient preparation and sample collection; Section 2 listing the diseases and Section 3 dealing with listings under drugs affecting hormone assays. This provides excellent accessibility to the information contained in the book.
In the preface the author claims that he has written the book from a clinical and methodological point of view so that biochemists will be able to provide "critical and expert advice on various biochemical tests". In addition, the book is directed at hospital doctors, practitioners and laboratory staff. I do not think the book allows one to become an "expert" on the biochemical tests for endocrinology and I would strongly recommend that the book is not used in this manner. However, as a source of information that is readily accessible to members of an endocrine or biochemical laboratory which provides accurate and reasonably up to date information, the book is invaluable. Certainly for a person entering the field of clinical biochemistry the book would be an excellent starting point. Further, senior biochemistry technicians and laboratory staff would find the book most interesting to read if they are heavily committed to endocrinological biochemistry. However, detailed discussions on the methodology behind the various biochemical tests are not provided.
Although the contents in the main are quite accurate, there are a few areas that I personally would not agree with as regards the emphasis placed on the value of the various tests. For instance, great faith was placed on the value of PTH (parathyroid hormone) estimation in the differential diagnosis of hypercalcaemia, particularly in diagnosing hyperparathyroidism and localisation of the site of tumour. Again, it was stated that the insulin tolerance test was a "powerful test" in the differential diagnosis of Cushing's syndrome. I would doubt that many Australian endocrinologists would agree with this statement! Also some of the criteria used in the diagnosis would have to be tempered by local requirements, for instance the criteria employed for diagnosing growth hormone deficiency, those used in England would have to be balanced against the recommendations of the Australian Pituitary Review Committee. In the section dealing with diagnosis of insulinoma, no mention is made of the use of the C-peptide assay in the differential diagnosis of this condition.
However, overall the book is well written and in line with modern endocrine practice. It discusses well the limitations and uncertainties of radioimmunoassay, it stresses the importance of establishing local normal ranges and the importance of early communication with the laboratory involved prior to undertaking endocrine tests. It is an excellent book for senior technical laboratory staff and for more junior members of the medical staff in an endocrine biochemistry laboratory. The clarity of style will also recommend its use to general physicians interested in endocrinology.
Frank Alford, Director, Endocrine Unit,
St. Vincent's Hospital, Fitzroy, Vic. 3065
18 The Clinical Biochemist, Newsletter, June 1982

Enzyme Column "Problems with Amylase Assays"
A number of factors have been implicated in the large interlaboratory imprecision (CV = 15%) of the local Victorian QC material assayed by the Phadebas kit method. Within our laboratory the CV is about 4%, as it is in most laboratories participating in the QC programme, so the large interlaboratory imprecision is due to differences in accuracy between laboratories. Since normalisation is not currently used in the treatment of results the factors affecting interlaboratory accuracy are (a) Specific technique (e.g., degree of removal of debris from the final supernatant — the kit does not provide satisfactory instructions and different laboratories have used a second supernatant centrifu-gation or a separating disc [Clin. Bioch. Newsletter, 62, p. 23) or the particular spectrophotometer and cuvettes) and (2) Kit Batch (e.g., consistency of tablets).
As far as our local QC goes, we have noted a factor implicating both specific technique and kit batch. The dilution of the final supernatant of highly absorbing specimens (as suggested in the kit method) gives an upward bias of results. For the local QC the final supernatant absorbance is about 2.000 and a 1/3 dilution produces an increase in determined, activity from about 1100 to 1300 U/L. (Our spectrophotometer, PYE-UNICAM SP8 - 100, is linear to absorbance 2.000). A similar bias is shown by dilution of final supernatants of lower absorbances. However, if an ACR standard curve is prepared and used to determine accuracy, rather than the kit provided graph, the bias disappears. This problem was identified on two batches, see table for example.
Absorbance Activity Activity
QC 2.087 QC diluted 1/3 0.729 GibroHi 1.276 Gibro Hi Diluted 1/3 0.438
U/L (Kit Graph) 1140 1320 710 825
U/L (ACR Curve) 1340 1350 830 795
The Phadebas kit method seems technically (though not necessarily clinically) inadequate because the information provided is insufficient to avoid large interlaboratory variation, and the graph provided contributes to this variation — an ACR standard curve seems necessary for best results.
S. Hamber, St. Vincent's Public Hospital, Fitzroy, Melbourne, Victoria
NOTE: ACR has recently been replaced by Humylase Control.
This is available at three levels of activity and is an entirely human based material whereas ACR was supplemented with animal material. It has been known for some time that amylase purified from various species have different relative activities depending on the substrate but with the availability of a human control material this problem should be minimized.
R. Bais, I MVS,
Adelaide
News of Members
The Editor of 77je Clinical Biochemist — Newsletter, Miss Nancy Dale, recently had to spend some time in hospital, carrying on the production of this issue from her sick-bed. I am sure all members will wish her a speedy recovery.
J.W.
Dr. H.L. Webster, formerly at the Royal Alexandria Hospital for Children, Sydney and now working in America sends regards to his former colleagues. His work involves extensive travel and lecturing at scientific meetings on osometry and sweat testing.
Congratulations to Margaret Stuart who has recently been awarded the degree of Doctor of Philosophy from the University of NSW for a thesis on the "Production of Somatomedins". Margaret is currently Vice-Chairman of the NSW Branch and has just completed a very successful tour of the Branches as one of the speakers in the Current Concepts Conference.
NEW ASSOCIATE MEMBERS (Up to March, 1982) New South Wales
Dr. I.D. Caterson, Flying Officer S.R. Connor, Mr. P.J. Compton, Mrs. M.A. Haughton, Mr. P.G. Hassell, Mr. G. Koumanakis, Miss M.J. Roberts, Mr. G.J. Rowe, Mr. C.A. Walters and Miss N.P. Watson.
Queensland Mr. J . Cairns, Mr. M.L. Lewis and Mr. M.T. Lynch.
South Australia Mr. G.D. Bennett, Dr. S.M. Holmes and Dr. H.A. Morris.
Victoria Dr. N.W. Coles, Dr. E.B. Donaldson, Dr. J.C.G. Doery,
Mr. C-T. Lam.
Western Australia Dr. P.E. Hickman, Mr. V. Kathiravelupillai, Mr. A.W.
Prins, Mrs. G. Rowley, Mrs. M.J. Webb.
MISSING MEMBER Mail from this member has been returned to us: Mr. M.
Webb, ICPMR PO Box 60, Wentworthville, NSW 2145.
RESIGNATION Mr. D. Casson, WA Branch.
777e Clinical Biochemist, Newsletter, June 1982 19

Corning reliability... The need for reliable blood gas, electrolytes and control reports may be the only constant in the
environment of critical care.
True sample visibility on both the Corning 178 Blood Gas Analyser and the 902 Sodium/Potassium Analyser allows
you to observe the specimen throughout the analysis and also lets you monitor flushing of the analytical chamber.
Microsampling capability of whole blood as low as 40 pi on the 178 and 65 pi on the 902 permits testing of all
patients on one system .. . including those too young, old or weak to yield a standard syringe sample. The 178
even handles inspired or expired gas analysis.
Simplified test procedure — from the busy specialist to the experienced technologist, the 178/902 system guides the user through the entire test procedure. Both systems
deny sample access unless fully calibrated so you just can't make a mistake.
"Real" endpoint detection reguires both blood gas and electrolyte systems to register results on the basis of true
electrode eguilibrium rather than arbitrary timing.
Easy electrode maintenance — Electrode membranes can be replaced without shutting either system down.
Recalibration is automatic.
Cumulative Quality Control History and Q / C Plotting provide either a tabulated or graphical format of a 31
day history of validation. The HP 85 data reduction system sorts the information from its memory draws the
graph and prints out the chart — in less time than it took to read this paragraph.
t / n ] T o ^ u r i s o n & pdercer 736 2088 20 1301 52 5641 277 1944 451 7911 34 4277
20 The Clinical Biochemist, Newsletter, June 1982

M L
.. .when it s really critical.
The Clinical Biochemist, Newsletter, June 1982 21

Gluc-DH A M E R C K i n n o v a t i o n
G l u c o s e
Glucono lactone
N A D
N A D H .
M E R C K G l u c - D H : a direct enzymatic method for determining glucose levels in biological fluids without the problems associated with unspecific auxiliary reactions used with other systems.
y 1—i
Linearity
0 Versatility
0 Specificity
0 Stability
0 Agreement
linear to 55 mmol/l (1000mg/dl)
for^-D-glucose
12 week shelf life following reconstitution
excellent correlation with values obtained I reference methods
For further information phone:
BOH BDH Chemicals: Melbourne (03) 8591305 Sydney (02)921036 Brisbane (07)2291721
22 The Clinical Biochemist, Newsletter, June 1982

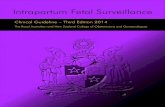
M o n o c l o n a l An t ibod i e s Margaret Stuart,
Garvan Institute of Medical Research, St Vincent's Hospital, Darlinghurst, NSW, 2010
Just as immunoassay has revolutionised the spectrum of clinical chemistry diagnostic assays in the past 15-20 years, so the introduction of monoclonal antibodies has the potential of expanding the range and specificity of these assays, an effect which will be realised in the next decade. Since the hybridomas secreting the antibodies are immortal, a continuing supply of antibodies is ensured. For diagnostic assays, the predefined specificity and endless supply of each antibody will provide the clinical biochemist with a reagent as constant and assured as the supply of inorganic chemicals which he uses in other spheres of his work.
Hybridoma technology was introduced by two Cambridge immunologists, Kohler and Milstein, in 1975. They described how somatic cell fusion of spleen cells from hyper-immunized mice with cultured mouse myeloma cells results in the production of hybridomas secreting antibodies of predefined specificity. A hybridoma produces a single antibody for which specificity is donated by the spleen cell parent and it is immortalised by its genetic inheritance from the myeloma cell. The myeloma cells used are mutants which are defective in the enzyme hypoxan-thine guanine phosphoribosyl transferase (HGPRT), an enzyme required for the "salvage" pathway of purine synthesis. By growing fused spleen-myeloma cell hybrids in a selective medium containing aminopterin which blocks endogenous purine synthesis, hypoxanthine and thymidine (HAT medium), and unfused myeloma cells die. At the end of their short life span any unfused spleen cells also die, and only the newly formed hybridomas will survive. The hybridomas need to be subcloned to ensure monoclonality.
One of the significant advantages in the production of monoclonal antibodies by the hybridoma technique is that an impure antigen may be used for immunisation. Since each responsive spleen cell produces a single immunoglobulin, the selection of the specific antibody required is the task of the laboratory when screening hybridoma medium. Immunisation with an impure antigen merely reduces the percentage of spleen cells which will produce antibodies of the desired specificity. Furthermore, for large molecules or cell types used as immunogens, a family of antibodies directed toward different antigenic determinants (epitopes) of the one antigen may be produced. These are of value to biochemists and immunologists in determining structural properties of molecules and cells.
As chemical reagents monoclonal antibodies have the advantages of their exquisite specificity and large scale production. Hybridomas can be preserved by freezing in liquid nitrogen and, when more reagent is required, they can be regrown in tissue culture to provide potentially limitless quantities of specific antibody. This contrasts with conventional antisera produced in animals which consist of mixtures of antibodies available in limited supply. The ratio of antibodies in serum from each bleed varies and cannot be reproduced exactly. Antisera from sequential bleeds may have different affinities and different cross reactions with structurally related compounds or contaminants in the immunogens.
Monoclonal antibodies will find wide usage as reagents for diagnostic assays, as structural probes, for purification and in immunohistochemistry. Already diagnostic assays using monoclonal antibodies have been described for measurement of human prolactin, CEA, alpha foetoprotein, hepatitis (3 surface antigen, ferritin, hCG, somatomedin and human growth hormone. Both radioimmunoassays and sandwich-type immunoradiometric assays have been described.
It is well known that some hormones are found as a heterogenous mixture in serum. A high correlation between current antiserum assays and monoclonal assays suggests that the monoclonals selected to date are directed toward the major circulating form of the hormone. In the future however, it can be foreseen that antibodies directed toward each of the circulating forms will be isolated and assays could be modified to measure the family of forms, or alternatively, a battery of screening assays could be developed to detect each of the circulating forms.
Monoclonal Antibody Production
Ant igens AtjCA) A ^ C B I AcjCC)
A b c A l ^
A b l C ) - ^ Blood
\ ̂ Fusion
Spleen cells Tumour cells
Tumour cell culture
o o o o o o o o 3 C O O O O O O Q O O O O O O O
O O Q O O Q O
ttubridomas
AbtA) Ab(6) AKC)
© C O c c o
c o o o 0 o 0
° o ° ° o ° o o
The Clinical Biochemist, Newsletter, June 1982 23

C.G. Fraser, Secretary SCIENCE PREPARED BY THE
EDUCATION COMMITTEE
Elucidate the Errors In the following cases, most of the abnormalities seen
are not due to disease processes but to errors. Can you elucidate the source of the errors? (Answers on page 00.)
Case 4 - Miss CH, Age 20
Case 1 — Mr. BB, Age unknown. Sodium Potassium Chloride Bicarbonate Calcium Phosphate
145 mmol/L 7.6 mmol/L 98 mmol/L 25 mmol/L
2.41 mmol/L 5.00 mmol/L
(RR: 132-144) ( R R : 3.1-4.8) (RR: 93-108) (RR: 21-32) (RR: 2.15-2.55) (RR: 0.60-1.25)
Sodium 143 mmol/L (RR 132-144) Potassium 2.7 mmol/L (RR 3.1-4.8) Chloride 129 mmol/L (RR 93-108) Bicarbonate 8 mmol/L (RR 21-32) Urea 1.4 mmol/L (RR 3.0-8.0) Creatinine 0.025 mmol/L (RR 0.06-0.12)
Case 2 - M r s . J F, Age 51
Case 5 - Mrs. I F , Age 27
Date 18/11 27/11 Progesterone 20.0 nmol/L ( R R : depends on
cycle) Sodium 117 mmol/L (RR 132-144) Testosterone 12.0 mmol/L (RR: 0.9-3.6) Potassium 3.2 mmol/L (RR 3.1-4.8) Prolactin 5.0/ig/L (RR:<30 ) Chloride 81 mmol/L (RR 93-108) FSH 1.1 IU/L (RR: <10 mid Bicarbonate 23 mmol/L (RR 21-32)
FSH 1.1 IU/L cycle)
Urea 2.5 mmol/L (RR 3.0-8.0) LH 1.3IU/L (RR :<22 mid Creatinine 0.050 mmol/L (RR 0.06-0.12)
LH 1.3IU/L cycle)
Case 3 - Mrs. 00, Age 63 Date 12/10 Time 16.30 Cortisol (nmol/L) 97
13/10 13/10 13/10 10.00 10.30 11.00
869 966 1007 Synacthen test
Case 6 - M r . DK, Age 77 Date 24/11 26/11 Acid Phos (U/L) 3.8 0.1
31/12 4.9 (RR:0.1-0.6)
Education Committee Report to Council — April 1982
1 STRUCTURE
The Education Committee has had the following membership since the last report to Council: Ms. J .E . Robinson, Chairman; Dr. C.G. Fraser, Secretary; Prof. B.C. Shanley, Mr. G.I.Goodall, Mr. M.J.Staley, Prof. R. Hahnel, Mr. T.D. O'Leary and Dr. L .E. Wyndham, Branch Education Representatives; Mr. I. Farrance, Board of Examiners; Mr. T.D. Geary, Scientific and Technical Committee; Dr. D.W. Thomas, Royal College of Pathologists of Australasia. The Commiteee has continued to work under the Terms of Reference drawn up and agreed to in 1981.
2 MEETINGS A partly funded meeting (accommodation and incidental
expenses) was held in Melbourne on 8 November 1981, before the Annual Scientific Meeting. All members were present except the Western Australian and Royal College of Pathologists of Australasian representatives. Most of the work of the Committee is carried out by postal and telephone communication which is effective in most cases.
3 BUDGET Attempts have been seriously made to keep the expen
diture of the Committee in the 1981/82 financial year to a minimum. The Australian Roman Lecturer, profits from the Scientific Education Seminar, the non-fully funded meeting, and the cost sharing of the deficit of the Current Concepts Conference by the Royal College all helped to trim costs. A budget submission for the 1982/83 financial year has already been circulated to Council; an allocation of $6,000 has been requested. It is hoped that Branches will, as previously requested, charge realistic fees for educational activities in order to make this a realistic estimate of expenditure. It is considered that the current level of activities, whatever the cost, must be maintained.
4 ACTIV IT IES The activities of the State Branches continue to be mon
itored. The 1981 Reports were published in the December issue of the Newsletter.
Omniscience continues to be published as a 2-5 page sec-
24 The Clinical Biochemist, Newsletter, June 1982

tion of the Newsletter as an effective means of communicating news, views, and other material to the entire membership of the Association.
The Clinical Biochemist — Reviews has attracted further subscriptions from Australia and overseas and will be cited in Current Clinical Chemistry following correspondence with Dr. J .G. Lines; negotiations are presently being actively conducted regarding citation in Current Contents. A current real difficulty is the non or late submission of promised material and the consequent very great efforts required of the active members of the Editorial Committee. The role of the members of the Education and Editorial Committees in the preparation of the publications of the Association is under current review; it is hoped that a firm novel proposal will soon be submitted to Council.
The mainly residential Chemical Pathology Course was held in Sydney from 1-5 March 1982. Informal feedback has been excellent. It is hoped that a full report, including a financial statement, will be available in the near future. The Victorian Branch has been formally invited to organise the 1983 course.
The organisation of the 1982 Current Concepts Conference is well in hand and it is highly likely that this eyent, led by Professor L. Lazarus and Dr. M.C. Stuart, will be very successful, in educational terms. It is hoped that definitive recommendations on dynamic investigation of endocrine function will eventuate and be published in the educational February 1983 issue of the Reviews.
The organisation of the visit of the 1982 Roman Lecturer, Professor V. Marks, has proceeded very smoothly. All State Branches have decided on the lecture to be given and the definitive dates of his visit were promulgated very early. Professor Marks has kindly organised his own air tickets and travel arrangements and has promised to provide the texts of his lectures for publication in the February 1983 issue of the Reviews.
In view of the undoubted success of the first Scientific Education Seminar, held in Melbourne after the 1981 Annual Scientific Meeting, which led to promulgation of recommendations in the February 1982 issue of the Reviews, it is highly likely that a second Seminar will be held in Adelaide in November. Planning is in the very early stages but the topic of the Seminar is likely to be in the areas of specimen and data handling. Mr. T.D. Geary is again shouldering much of the work.
Professor B.C. Shanley and Dr. C.G. Fraser have circulated a questionnaire on the teaching of clinical biochemistry to the Dean of every medical school in Australia and to a senior clinical biochemist associated with each school. Interesting replies have been received from more than half the schools and it is hoped that a report and firm recommendations on the undergraduate medical teaching of clinical biochemistry will be prepared before the end of the year.
The Working Party of Council on professional exmina-tions has had input from the Education Committee and the final report has already been submitted to Council.
5 COMMENTARY It is again considered that the Education Committee has
continued to maintain and develop previously existing educational activities and has prepared and/or adopted guidelines for many of these. The Committee has continued to initiate new educational ventures. It is hoped that the Committee will develop further in the future; however, such development will require input from many members of the Association and a high level of activity from those selected or nominated as members of the Committee.
C.G. Fraser, Secretary
Errors Elucidated The procedure by which the clinician obtains a medi
cally useful result is a complex chain of events. Errors can and do arise at every link in the chain. It is very important for the clinical biochemist to be aware of all the possible sources of errors and to be able to easily detect them on inspection of results.
Case 1 illustrates the errors that can arise in transport of the specimen to the laboratory. This sample (from an outpatient) took a day to reach the laboratory. Not surprisingly, the constituents of the erythrocytes present in high concentrations have "leaked" out. The plasma potassium and phosphate are elevated due to this leakage. The data and time that specimens are taken should be noted on the request form and sample tube; the laboratory should refuse to perform analyses if specimens do not reach the laboratory in a timely manner.
Case 2 illustrates the effect of lipaemia. The relative amount of plasma water is reduced by the triglycerides. Plasma electrolytes are mainly in the plasma water. The sample volume (plasma water plus lipid) taken for analysis in the instrumental technique is usually constant and therefore the electrolytes reaching the detector are analysed correctly but appear to be low. Direct potentiometric measurement does give the true values for the plasma electrolytes.
Mrs. 00 (Case 3) presented at Accident and Emergency with clinically obvious Addison's disease. She had at that time an appropriate low plasma Cortisol level. She was
treated with prednisolone which cross reacts in the assay for Cortisol (see Newsletter 57, p. 22) and thus the Synacthen test was invalid and wasted the time of the clinicians, the laboratory and the patient. Treatment with dexamethasone would have been appropriate. It would also help if all drug therapy was noted on clinical biochemistry request forms.
The best clue to the error of Case 4 is the very high plasma chloride. Normal saline has a sodium and chloride concentration of 153 mmol/L and when, as in this case, a patient is being infused with sodium chloride and the sample is taken from the "drip" arm, all plasma analytes except the sodium and chloride are diluted. The sodium may not be abnormal since the plasma sodium concentration is of the same order as the infusate but the plasma chloride is relatively low and therefore becomes elevated.
The results obtained on the sample taken in Case 5 on 18 November are typical of those found in males. Indeed, this sample was taken from the husband of the patient but the request form did not state that fact. Complete unique patient identification must be adequately stated on all request forms.
In Case 6, the result obtained on 26 November is incorrect; the laboratory staff failed to add the appropriate acid preservative to the plasma sample before storing it for subsequent analysis. Acetic acid (20%, 20 £(L) should have been added to a 2 mL aliquot of the plasma sample.
The Clinical Biochemist, Newsletter, June 1982 25

Tota l F l e x i b i l i t y Q U O r T n
F r o m E . N . I .
G E M E N I G E M S T A R F L E X I G E M
Completely complementary systems for clinical analysis. • Cost Efficient • Optimum Chemistry Performance • Minimum Hands-on Operation • Maximum User Serviceability
BRINGING YOU THE WORLD S BEST TECHNOLOGY
Sydney (02) 439 5477 Melbourne (03) 645 2911 Adelaide (08) 212 6510
26 The Clinical Biochemist, Newsletter, June 1982

Scientific and Technical Committee T.D. Geary, Chairman
Report to Federal Council, May 1982 This report was presented to the Federal Council by Mr
L. Penberthy representing the Scientific and Technical Committee.
1. TERMS OF R E F E R E N C E A recommendation was made to Federal Council that
the proposed alterations to the Terms of Reference of the Scientific and Technical Committee be accepted. The new Terms of Reference are available on request from the Chairman of the Scientific and Technical Committee.
2. APPOINTMENTS 2.1 Associate Member of the I FCC Expert Panel on Theory
of Reference Values The Scientific and Technical Committee recommended
the appointment of Mr L.R. Watkinson, Flinders Medical Centre, South Australia.
22 Membership of the Scientific and Technical Committee, Analytical Methods Sub-committee
The Scientific and Technical Committee recommended the appointment of Mr A. Muir, Royal Prince Alfred Hospital, New South Wales. The Members of the Scientific and Technical Committee expressed regret that there was not more competition for positions for which the Scientific and Technical Committee called for nomination. This seemed to indicate either a lack of interest on behalf*of the members of the Association or lack of action by State Branch Committees.
3. REPORT ON THE ACTIV IT IES OF THE S & TC 3.1 Scientific Education Seminar 1981
Quality Control Accept or Reject This seminar has been reported in the Reviews (Febru
ary 1982) and Newsletter (March, 1982). The Organising Committee were particularly happy at
both the recommendations arising from the meeting and the range of laboratories which were represented at the meeting.
3.2 Instrumentation and Diagnostic Products Subcommittee
3.2.1 EVALUA TION REPORTS
Since the last report the ENI Flexigem has been evaluated at the Institute of Medical and Veterinary Science on behalf of the Subcommittee.
This report is available from the Chairman, Mr. T.D. Geary, at the Institute of Medical and Veterinary Science.
3.2.2 WEIGHING SURVEY
Messrs Dawson and Henstridge are preparing a weighing survey which will be part of the General Serum Chemistry
Quality Assurance Programme organised jointly by the Royal College of Pathologists of Australasia and the Association.
3.2.3 TECHNICAL BULLETIN A technical bulletin is being prepared on testing the
quality of laboratory water.
3.3 Analytical Methods Sub-committee The Sub-committee has been responsible for organising
the assignment of target values to the material used in the General Serum Chemistry Programme. A report on the scheme used to assign the enzyme values was published in the second Programme News. It is hoped that in future, where possible, reference methods will be used.
3.4 Quality Control Sub-committee The major activities of the Quality Control Sub-commit
tee have been in implementing a number of national quality control programmes. These activities have been in conjunction with the RCPA Chemical Pathology QAP Group. The members of this Group are Dr D. Thomas (Chairman), Dr R. Bowyer, Mr T.D. Geary and Mr L.A. Penberthy (AACB Representative).
3.4.1 GENERAL URINE CHEMISTRY PROGRAMME
This programme was developed at Flinders Medical Centre by Mr M. Shephard, Dr C. Fraser and Mr L.A. Penberthy.
In the first year (1981) the following analytes were examined:
sodium potassium urea creatinine glucose osmolality calcium phosphate urate protein. This work was carried out as part of an MSc by Mr Shep
hard and the data reduction for the programme was performed on the computer in the Department of Clinical Biochemistry at the Flinders Medical Centre.
Reports on this programme have been published independently and the S & TC will be seeking assistance to investigate recommendations arising from the programme.
The 1982/83 programme has been modified to include: chloride oxalate MHMA 5HIAA Only minor computer programme changes are required
and will be made by Mr Penberthy.
The Clinical Biochemist, Newsletter, June 1982 27

3.4.2 THERAPEUTIC DRUG PROGRAMME
In 1981 this programme was co-ordinated by Mr C. Hann with the assistance of Mr T.D. O'Leary from the Institute of Medical and Veterinary Science. Mr Penberthy developed the computer programmes on the computer system at FMC.
The following drugs were included: Phenytoin Theophylline Valproate Carbarn azepine Paracetamol Quinidine Lithium Digoxin The 1982/83 programme has been modified by replacing
quinidine and digoxin with phenobarbitone and barbiturates. Only minor changes to the computing were necessary. In future the data reduction and organisation will be transferred to the General Serum Chemistry system.
owned by Mr Duncan and the Department of Clinical Biochemistry at Flinders Medical Centre.
A major task of the programme is the massive printing load and to adhere to the timing required for the rapid return of results, it was necessary to purchase a hPgh speed printer for sole use in the programme.
3.4.3.3 Participants in Programme
There are 185 full participants in the programme with another 64 taking either an additional data reduction or sera option. This response is encouraging to the RCPA/ AACB Chemical Pathology QAP Group who in association with the Sub-committees of the S & T C intend to provide educational programmes and newsletters highlighting problem areas revealed as the programme progresses.
3.4.3.4 Programme Information This newsheet is being used to provide information as
well as asking for advice and comment from participants.
3.4.3 THE GENERAL SERUM CHEMISTRY PROGRAMME
The format of The General Serum Chemistry Programme was reviewed in light of the experience gained with the General Urine and Therapeutic Drug Programmes. The format remains essentially the same as that published in the Newsletter (March 1981). The Quality Control Sub-committee continues to ask for comment as the programme belongs to the profession and can only provide for all the requirements if the organisers have adequate feedback.
3.4.3.1 Trials with the Material Provided by Commonwealth Serum Laboratories
(a) S T A B I L I T Y T R I A L S The material supplied by the Commonwealth Serum
Laboratories was subjected to an extensive programme to test for the stability of all analytes measured in the programme. Stability trials are continuing during the running of the cycles at a number of centres.
(b) L I N E A R I T Y TR IALS The material selected was tested to confirm the linear
relationship for all analytes in each specimen.
(c) ANIMAL SUPPLEMENTS The use of human enzymes to supplement some levels of
activity instead of animal had to be deferred until the legality of their use has been clarified. The checking of the material with the animal supplements was carried out at the Flinders Medical Centre and the Institute of Medical and Veterinary Science.
(d) ESTABLISHING T A R G E T VALUES Dr J.B. Edwards co-ordinated the task of establishing
target values for the sera. Specimens were sent to a number of laboratories throughout Australia for the analysis of the twenty-eight analytes.
3.4.3.2 Computing and Printing of Participants Reports After considering the options available, it was decided to
develop programmes and purchase a computer system. Initial development was carried out by Mr B. Duncan with the assistance of Mr L.A. Penberthy on Apple II systems
BRANCH NEWS
TASMANIAN BRANCH NEWS The Current Concepts Conference was held on Saturday,
29 May at Repatriation General Hospital, Hampden Road, Hobart. The theme for the Conference was "Dynamic Endocrine Function Testing" and guest speakers were Professor L. Lazarus and Dr. M.C. Stuart.
WESTERN A U S T R A L I A N BRANCH NEWS Scientific Programme
The programme for the first half of 1982 commenced with the February Scientific Meeting presented by Drs. Steve Wilkinson and Stan Wysocki from the Endocrinology Section at the King Edward Memorial Hospital for Women.
Dr. Wilkinson spoke on "Urinary Steroid Profiles by Gas Chromatography and Mass Spectrometry" and Dr. Wysocki on "Squalene and Foetal Maturity".
The speakers for the March meeting were drawn (and quartered) from Dr. .Garcia-Webb's research group at the Department of Clinical Biochemistry, Queen Elizabeth II Medical Centre. The topic was "Insulin Resistance and Insulin Action: Current Concepts".
Abstract on Insulin Meeting: "Obese subjects with non-insulin-dependent diabetes
have glucose intolerance but are not as a group insulin deficient. Thus it follows that in these subjects insulin must be working less efficiently than normal. At the Queen Elizabeth II Medical Centre we are interested in studying the causes of this type of diabetes. The programme will cover the background to the major lines of research being undertaken at the moment."
The May Scientific Meeting was presented by the Perth Quality Control Group, a subcommittee of the W.A. Branch of the AACB. The title was "Calcium - State of the Art".
28 The Clinical Biochemist, Newsletter, June 1982

NOW YOU CAN AFFORD TO BE SELECTIVE
INTRODUCING
SE33S microlyte ®
© a registered trademark of KONE Corp. Instrument Division
m ' c ' o l y t e
UTILIZING ION SELECTIVE ELECTRODES FOR
K V N q V C q + +
Featuring
E N Q U I R E N O W
• The Best Price on the Market.
• Autocalibration.
• Self-Diagnostic Function.
• A lOOyul (or 5 0 / J I optional) Sample.
.And More
M E D O S C O M P A N Y P T Y . L T D .
medos M E L B O U R N E 62 3581 S Y D N E Y 938 2455 B R I S B A N E 275 1200
A D E L A I D E 464112 P E R T H 361 7099 HOBART 294 9911
OS

MAS REAGENTS CUT TESTING
COSTS MAS liquid stable enzyme reagents provide an opportunity for the laboratory to cut testing costs.
No Reagent Waste No longer must the unused portion of a reagent be discarded. With MAS liquid stable enzyme reagents, only as much working reagent as the test requires is used. Less inventory is needed and waste costs are virtually eliminated.
No Reconstitution MAS reagents eliminate the extra preparation required with lyophilized reagents. A ready to use, stable, product is provided.
Consistency The liquid technology and rigorous quality control of the MAS manufacturing process assures lot to lot consistency. Bottle to bottle homogeneity is maintained and the risks inherent in lyophilization and reconstitution are eliminated.
Superior Shelf Life Waste due to the limited shelf life of reconstituted lyophilized reagents has been eliminated. Previously thought impossible, MAS reagents have a reconstituted shelf life of up to one year.
T H E MAS R E S O U R C E All of the liquid stable enzyme reagents developed and produced by Medical Analysis Systems eliminate the quality control difficulties and waste factors inherent in the use of their lyophilized counterparts. Medical Analysis Systems is currently producing the following enzyme reagents: SGOT/AST CPK C H O L E S T E R O L S G P T / A L T G L U C O S E BUN HBDH A L P GGTP LDH-P LDH-L
Soon to be released: Uric Acid Triglycerides Stable liquid human enzyme control serum
MAS will continue to be a leader in the development and manufacture of liquid stable enzyme reagents as an ever-expanding resource to the diagnostic needs of world-wide public health.
SMI (Aust.) Pty .Ltd., P.O. Box 357,Pennant Hills. 2120. Phone: Sydney (02) 84 3040. Melbourne (03) 6561814.
smi scientific manufacturing
industries pty limited
30 The Clinical Biochemist, Newsletter, June 7982

Abstract: "Three speakers presented different aspects of calcium
measurement. "a) The first speaker reviewed methods currently in use
for total calcium and ionised calcium. He also summarised the findings of a quality assurance survey on calcium carried out by the Perth QC Group amongst eight laboratories in the metropolitan area.
"b) The second speaker related his experience of the reference method for calcium as established at Royal Perth Hospital.
"c) The third speaker provided a personal viewpoint of the use of calcium estimation from a clinical perspective."
/ ; Forthcoming Meetings
V A U S T R A L I A 1982 The Lung Interstitium
9- 13 August, Adelaide, SA. Arranged by the Thoracic Society of Australia. For further information see page 12 of the previous
Newsletter.
Annual General Meeting 11-13 August, University of Sydney, NSW. Endocrine Society of Australia. Contact: Dr. Grant Stone, Department of Veterinary Physiology, University of Sydney, NSW 2006
International Biochemistry Congress. 15-21 August, Perth, W A. Write to: Australian Academy of Science, PO Box 783, Canberra City, ACT, 2601
L A B E X '82 Exhibition of Laboratory Equipment 6-9 September, Hilton International, Sydney, NSW Arranged by IPC Exhibitions who may be contacted at
their Sydney Office: PO Box M204, Sydney Mail Exchange, NSW, 2012 Telephone (02) 699-5651 OR in Melbourne, 196 Wells Street, South Melbourne, Victoria, 3250 Telephone (03) 699-9266
19th Annual Congress of Australian and New Zealand College of Psychiatrists
10- 15 October, Perth, WA. Contact: Michael Margolin, 2nd Floor, 190 Albert Road, South Melbourne 3205
21st Anniversary Scientific Conference and Annual General Meeting of the AACB
2-5 November, Adelaide, SA.
The Clinical Biochemist, Newsletter, June 1982
The June meeting was fully occupied by the WA Branch AGM.
Social Programme After a successful dinner at an Indonesian Restaurant
late last year the Committee planned a luncheon on the upper reaches of the Swan River for April. The response to this was so dismal that it had to be cancelled at the last minute. It is hoped that the new committee will be able to whip up the old enthusiasm for an end-of-year gala event.
B. Rumble, WA Branch Publications Representative
\
J
Full details given in the Newsletter, December 1981, page 11. O V E R S E A S 1982 2nd International Congress on Neonatal Thyroid Screening
16-19 August, Tokyo, Japan. Contact: Dr. John Connelly, Royal Children's Hospital, Parkville, Vic. 3052
Annual Meeting of American Association for Clinical Chemistry (AACC)
8-13 August, Anaheim, California, USA Contact: Dr. Alfred H. Free, PO Box 154, Elkhart, IN 46515, USA.
27th Annual Conference — Royal College of Pathologists of Australasia in Conjunction with NZ Society of Pathologists.
16-19 August, University of Otago Medical School, Dunedin, New Zealand.
Contact: Conference Secretary, Pathology Department, PO Box 913, Dunedin, New Zealand
2nd Asia and Oceania Thyroid Congress. 19-22 August, Tokyo, Japan. Contacts: Dr. Jim Stockigt, Ewen Downie Metabolic Unit, Alfred Hospital, Melbourne, Victoria, 3001.
***7th Asia and Oceania Congress of Endocrinology. 22-26 August, Tokyo, Japan. Contact: The Secretariat, 7th Asia and Oceania Congress of Endocrinology, c/- Japan Convention Services Inc., Nippon PressCenter Bldg, 2-1 Uchisaiwai-cho 2-chome, Chiyoda-ku, Tokyo 100, Japan.
31

A L L T E C H A S S O C I A T E S
AMINO ACID ANALYSIS A M I N O A C I D A N A L Y S I S K I T
Great progress has been made by the introduction of the N-acetyl propyl ester derivatives for the analysis of amino acids by gas and liquid chromatography. These derivatives offer a simple, rapid and quantitative method of analysis at unprecedented speeds. Up to 24 analyses in an eight-hour working day have been achieved. No other method to date has been able to equal this number of amino acids analyses with a single gas chromatograph. Using inexpensive reagents, all 20 common amino acids are derivatized in 30 minutes by a simple test tube procedure. GC analysis is a single column, single injection separation taking 15 minutes. The derivative is extremely stable. Pure standards and derivatives are included in the kit. Until now, analysis of amino acids has been a slow, cumbersome and often imprecise process, normally accompl ished by the ion exchange method in liquid column chromatography. This requires highly trained technicians and critical control. Analysis by ion exchange generally takes 4 to 12 hours per sample, at a substantial cost to the user for reagents and also in time expended for the preparation of samples. Now, all that is changed with the use of the acetyl amino propyl ester kit offered exclusively by Alltech. We are certain that the researchers purchasing our kit and following the procedures supplied with the kit can now approach the analysis of amino acids by gas liquid chromatography with complete confidence.
20 AMINO ACIDS (n-propyl, N-acetyl derivatives)
1. Alanine 2. Valine 3. Glycine 4. Isoleucine 5. Leucine 6. Proline 7. Threonine 8. Serine 9. Aspartic Acid
10. Methionine 11. Cysteine 1 2. Phenylalanine 13. Hydroxyproline 14. Glutamic Acid 15. Histidine 16. Tyrosine 17. Ornithine 18. Lysine 19. Arginine 20. Tryptophane
1 0 1 5
2 ft x 1 / 8 " S S Amino Acid packing 110°C (2 min) to 250°C at 8°C/min until Glutamic then 24°C/min
F lowrate: Helium, 15 ml/min
Co lumn: Pack ing : Temp :
A L L T E C H ASSOCIATES 2 F R E N C H LANE SUMMER HILL NSW 2130
PTY LTD
(02) 799-2022 TLX (AA) 26626
6th International Congress on Hormonal Steroids. 5-10 September, Jerusalem. Contact: Dr. A. Nimrod, Secretary, LOC, PO Box 29784, Tel Aviv. 61297 Israel. Telex 341171 KENS IL.
2nd Asian-Pacific Congress of Clinical Biochemistry. 19-24 September, Singapore. Contact: The Congress Secretary, 2nd Asian-Pacific Congress of Clinical Biochemistry, c/- Singapore Professional Centre, 129B, Block 23, Outram Park, Singapore 0316.
International Diabetes Federation. 10- 17 November, Nairobi. Contact: Dr. P. Zimmet, Royal Southern Memorial Hospital, Caulfield, Vic. 3162
Biotechnology in Clinical Chemistry. 28 September-1 October, Cambridge, UK. Contact: Association of Clinical Biochemists, Cambridge, UK.
O V E R S E A S 1983 XVI Ith European Symposium on Calcified Tissues
11- 14 April, Davos, Switzerland. First circulars available from Dr. D. Cameron.
Clinical Disorders in Bone and Mineral Metabolism. 9-13 May, Detroit, Michigan, USA Contact: Boy Frame MD, Henry Ford Hospital, Division of Bone and Mineral Metabolism, 2799 W. Grant Boulevard, Detroit, Ml. USA 48202
2nd International Symposium on Insulin Receptors. 1-3 September, Rome. Contact: Dr. Len Harrison, University Department of Medicine, Royal Melbourne Hospital, Vic.
***The Editor has further information about these meetings.
EXHIB IT ION G U I D E L I N E S The Scientific Industries Council of Australia has
released a document outlining guidelines and recommendations for Industry and Professional Exhibitions.
This important document is an invaluable guide for those involved in the organisation of an Exhibition. The "Guidelines and Recommendations" are available on request from:
Scientific Industries Council of Australia, C/- Chamber of Commerce in your State.
32 The Clinical Biochemist, Newsletter, June 1982

G e t I n t o El A (And Make it Cost-Effective)
If you are using RIA and want to get away from isotopic assays
If you are sending these tests to another lab because your "volume doesn't warrant doing them in house"
Then Immunotech has good news for you:
•6 month shelf life
• C a n be applied to all spectrophotometers and to most instrument systems
•Only one standard curve for e a c h lot
•Rapid and inexpensive data reduction
Remember— you don't have to use isotopes to provide the best service for your hospital or laboratory.
ENDAB THE REALISTIC ALTERNATIVE
A U S T R A L I A N LABORATORY S E R V I C E S PTY. LTD. 188 PRINCES HWY., A R N C L I F F E
POSTAL A D D R E S S : BOX 193, P.O., R O C K D A L E , N.S.W. 2216
T E L E P H O N E : 599-4098 immunolech
The Clinical Biochemist, Newsletter, June 1982 33

THE ORTHO DIAGNOSTIC SYSTEMS
T R A V E L L I N G FELLOWSHIP
Ortho Diagnostic Systems wish to congratulate David Rutherford of the Alfred Hospital, Melbourne who has been awarded the 1982 Ortho Diagnostic Systems Travelling Fellowship. The award will enable David to visit the United States and further his study of toxicology quality control programs. He will also attend the 34th Annual Meeting of the American Association of Clinical Chemists in Anaheim, California. Please join with us in wishing David a very successful and enlightening program.
Ortho Diagnostic Systems E T H N O R
34 The Clinical Biochemist, Newsletter, June 1982

Letters to the Editor
Dear Editor,
T H E C U R S E O F T H E M I S P R I N T I regret to inform you that the purported message 'Num
ber of Lab Numbers sent=0' is not correct. The message should have read ' N U M B E R O F L A B N U M B E R S S E N T T O KUNU=0 ' .
The explanation of the error is that the Baudot code used in Telex transmission is only a five bit code with 32 possible permutations and use is made of characters known as figure shift and letter shift to change from figures to letters and vice versa. In this case the letter shift character after 19:08 must have been lost during the storm, and the wrong set of characters was printed, e.g. binary 01100 can mean N o r , depending on shift status. No internal checking system is used on the grounds that mistakes are usually obvious. I think it could be said that that is the case here.
Peter Greenacre, Biochemistry Department,
Mater Misericordiae Hospital, PO Box 433, Crows Nest, NSW 2065
New Products and Developments
This following information is provided by the manufacturers or their agen ts.
BECKMAN C E N T R I F U G E HAS MICROPROCESSOR CONTROL, ULTRA-SMOOTH(™ > D R I V E
Beckman Instruments Inc, has introduced a new highspeed refrigerated centrifuge, the Model J2-21M.
New features of the J 2-21M include microprocessor control, which makes centrifugation more automated and more flexible. The system has storage space in its memory for ten programs, so that runs can be repeated exactly time after time; a choice of nine acceleration and ten deceleration rates; and, automatic temperature compensation after keyboard entry of the name of the rotor to be used. Operating parameters and actual conditions are shown on a bright digital display.
The Ultra-Smooth drive, adapted from advanced ultra-centrifuge technology, has no brushes to wear out or replace. A frequency-controlled induction motor provides the high torque and power to accelerate rotors smoothly and fast. Other J 2-21M features include diagnostic signals, automatic partial vacuum, sturdy components and such safeguards as rotor imbalance detection, over-temperature protection and electronic doorlock.
Like the J 2 - 2 1 , the J2-21M accepts eleven rotors, from versatile fixed-angle and swinging-bucket rotors to the unique Elutriator Rotor for harvesting living cells. The J 2-21M reaches a maximum speed of 21,000 rpm and generates forces to 51,500 g.
For more information, contact Beckman Instruments (Australia) Pty L td , Gladesville, NSW.
CORNING & T&M LAUNCH T H E NEW 178 BLOOD GAS SYSTEM
Townson and Mercer Pty Ltd were recently pleased to welcome to Australia Dr Bob Moran for the launch of the new Corning Model 178 automatic blood gas system. Dr Moran of Corning USA is presently Director of the Corning Medical Technical Consultation Centre at Medfield in Massachusetts.
A t a series of seminars held in Queensland, NSW and Victoria, Dr Moran's major topics of discussion were centred about advances in critical care instrumentation. Emphasis was placed on performance determinants and data management in blood gas analysis, including tonometry and control samples.
Response to Dr Moran's seminars by the cross-section of the attending hospital community was excellent. On numerous occasions Dr Moran visited leading hospitals and laboratories and was able to gain an overall perspective of the needs of the Australian hospital environment in relation to the Corning instrumentation range.
ICL S C I E N T I F I C PRODUCTS NOW A V A I L A B L E
I C L Scientific of Fountain Valley, California is part of the Boehringer Mannheim Group and their products are now available from Boehringer Mannheim Australia.
I C L Scientific is a major manufacturer of high quality antisera and immunological products. Also included in the comprehensive I C L range are serology test kits, a three level therapeutic drug control and the patented Kova System for standardised urinalysis.
Further information on the I C L range can be obtained from Boehringer Mannheim Australia, North Ryde, NSW.
SOUTH A U S T R A L I A B U Y S DU PONT ACAs A major order for the Du Pont " a c a " Discrete Clinical
Analyser has been received from South Australia. The Institute of Medical and Veterinary Sciences, which
runs pathology laboratories in the State's public hospitals, has purchased three 30 channel " a c a " analysers with sodium and potassium accessories.
Each machine is capable of performing 30 separate clinical tests.
The equipment is to be placed at the Lyel l McEwen Hospital, El izabeth; the Whyalla District Hospital and the Mount Gambier District Hospital.
Du Pont is currently conducting training courses for South Australian pathology staff on operational techniques at the company's research and test laboratories in Sydney. The equipment will be installed over the next few weeks.
AMINO ACID A N A L Y S E R Waters Associates Pty Ltd announce the release of an
Amino Acid Analyser. The unit comes complete with all requirements for
accurate quantitation of hydrolysate samples at concentrations in the low picomole region. Analysis is performed within eighty minutes and the only pretreatment of samples required is fi ltration. Al l other functions including accurate quantitation, derivitisation etc., are carried out automatically. The unit incorporates an automatic sampler which can handle 48 samples with only twenty microlitres total of sample required.
The inbuilt f lexibil ity of this unit also allows it to be used for protein analysis and purification, peptide mapping and purification as well as free or derivitised amino acid analysis making it a total separation, identification and quantitation system for the protein chemist.
Further details are available from Waters Associates Pty Limited, PO Box 146, Chippendale, NSW.
77?e Clinical Biochemist, Newsletter, June 1982 35

O V E R S E A S V I S I T Stuart Wilson, Service Manager with Boehringer Mann
heim Australia has returned from a visit to the European and North American Headquarters of the Boehringer Mannheim Group.
While in Mannheim he completed a service training course on behalf of the Hitachi 705 Biochemistry Analyser and in the United States he visited both the Indianapolis and Houston facilities of the Boehringer Mannheim Corporation. While there he took the opportunity to attend the installation of two Hitachi 705s and to review the experiences of the American 705 project to date.
The Hitachi 705 will be released in Australia during June, 1981 . The objective of Stuart Wilson's overseas visit was to ensure that Boehringer Mannheim Australia is completely prepared and equipped for this introduction.
BECKMAN APPOINTMENT Beckman Instruments (Australia) Pty Ltd announces
the appointment of Mr Ivan Hart as the National Product Specialist for instruments which are produced by the Spinco Division of Beckman. These include ultracentri-fuges, amino acid analysers, protein sequencers, peptide synthesizers, synthetic peptides and allied instrumentation.
Mr Hart has had 14 years experience on these products and we are certain that this knowledge will be of great benefit to new and old users of Beckman products.
Mr Hart is able to offer a unique service for Beckman rotors. Field Rotor Inspection Program ( F R I P ) is a program which allows Beckman users to have rotors inspected at regular intervals together with a series of lectures on the care of rotors and how to obtain the best use from Beckman products.
LUMINESCENCE - A PHENOMENON BECOMES AN A N A L Y T I C A L TOOL
Luminescence itself, the production of light by living organisms, has been known for centuries but remained an interesting phenomenon without practical applications. More recently, the discovery of a luminescence system specific to the A T P present in all living cells suggested a method of counting all such cells accurately, objectively and rapidly. However, a quarter of a century passed before Lumac pioneered the standardised reagents to release this A T P from the cell ( N R B for bacterial and NRS for somatic cells) and to produce light on contact with it (Lumi t ) . Nowadays, thanks largely to the methods and instruments developed by Lumac, the APT-specif ic luminescence is recognised as an ultra-sensitive measuring technique for routine analysis.
All living cells contain A T P and can be counted with the luminescence system. The practical applications are therefore virtually unlimited. Not only can the number of bacteria in a wide range of samples be determined with unparalleled accuracy, but the same technology allows other cells and the metabolic activity of organisms and seeds to be studied.
The perfecting of methods has gone hand-in-hand with the development of instruments and reagents, giving the analyst a complete measuring system for a wide variety of disciplines including clinical chemistry, biochemistry, haematology, microbiology, environmental research, industrial quality control, agricultural and fermentation processes.
Lumac also leads with the introduction of complete reagent kits for routine analysis in particular fields.
For further information contact Townson and Mercer Pty Ltd in the capital city of your state.
DUAL V A R I A B L E W A V E L E N G T H HPLC D E T E C T O R
Micromeritics have just released their new Universal H P L C Dual Variable Wavelength Detector - Model 788. This detector offers the following unique features:
It simultaneously measures light absorbance at two selectable wavelengths; provides speedy and accurate quantitation of unresolved components; identifies components with identical retention times; has automatic baseline zeroing; high pressure flowcell (3000 psi); two reference sample pairs of UV enhanced silicon photodiodes for maximum stability and minimum noise; a sensitivity monitor with a range 0.005 aufs to 2.56 aufs and is readily adaptable for existing systems.
Technical literature is available from Micromeritics, sole Australian agents, Alltech Associates, 2 French Lane, Summer Hil l , NSW. PYROCERAM BENCH P R O T E C T O R S
The Science Products Division of Crown Corning have released this useful new product which is available in three sizes - 25.4 x 25.4 cm ( 1 0 " x 1 0 " ) , 45.7 x 60 cm ( 1 8 " x 24 " ) and 54.9 x 73.6 cm ( 2 2 " x 2 9 " ) , all of which are 4 mm thick.
Pyroceram is a toughened, white glass/ceramic which has exceptionally high resistance to both thermal and mechanical shock. Under normal working conditions these bench protectors are able to withstand temperatures of around 700°C.
Pyroceram is resistant to strong acids, alkalies, solvents and most other contaminants, and is ideal for use in high-risk damage areas such as near muffle furnaces or in any area where spills of corrosive or staining materials, or burns, are likely to occur.
CK-NAC This latest new product release from Calbiochem-
Behring has been formulated according to the German Society of Clinical Chemistry specifications which parallel the I F C C recommendations.
Reconstitution stability of seven days, sensitivity of 7 U/L and improved precision are some of the features of C K - N A C .
For further information, please contact Calbiochem-Behring Australia Pty L td , PO Box 200, Kingsgrove, 2208.
E L E C T R O N U C L E O N I C S INTERNATIONAL Electronucleonics International (EN I ) makers of the
Gemsael, Gemeni and Flexigem centrifugal analysers, have released a unique small clinical analyser to the international market.
Gemstar, a small benchtop microprocessor controlled discrete chemistry anlayser, brings some remarkable capabilities to the small laboratory and stat-lab.
The system operates in three modes: batch, profile and mix-match, which is a combination of both.
Gemstar has the ability to run up to 12 samples in batch mode, but can perform a profile of up to 12 different tests on one sample.
Gemstar holds up to 30 tests in memory at any one time, including user programmable channels.
Blanks and standards can be stored and recalled. Operation at 25°C, 30°C and 37°C is user selectable. It includes a thermal printer and has the unique chemis
try and instrument user diagnostics which have given the Gemene and Flexigem unique reliability.
Marketed in Australia and New Zealand by Meeco Ltd, Division of Australian Mechanical and Scientific Systems Ltd, the Gemstar is available for outright purchase, lease, or reagent rental at exceptionally reasonable prices.
36 The Clinical Biochemist, Newsletter, June 1982

.new dimensions in product-analyte availability
Ortho* Therapeutic Drug Monitoring (TDM) and Toxicology Controls Comprehensive: controls include most widely prescribed drugs Significant: analytes are assayed at clinically significant levels
Product: fresh human source material for reliable sensitivity
Source material Constituents Methods Levels Ortho Bi-Level Assayed Cardiac Drug Control Set 1, II
Human serum Digoxm Procainamide Propranolol N-Acetylprocamamide Qumidine (Metabolite) Disopyramide Lidocame
EMIT H P L C G L C RIA Fluorome.try
Two clinically significant levels
Ortho Bi-Level Anticonvulsant/ Antiasthmatic Control Set 1, II
Human serum Carbamazepme Phenobarbital Diphenylhydantom Primidone (Phenytom) Theophyll ine Ethosuximide Valproic Ac id
EMIT H P L C G L C RIA
Two clinically significant levels
Ortho Bi-Level Assayed Toxicology Control Set 1, II
Human serum Acetaminophen Diphenylhydantom Amobarbital (Phenytoin) Phenobarbital Propoxyphene Methyprylon Diazepam Meprobamate Salicylate Methaqualone
EMIT H P L C G L C RIA
Two clinically significant levels
Ortho Toxicology Control Urine Proficiency
Pooled normal human urine with speci f ic drugs added
Morphine Amobarbital Morphine Glucuronide Secobarbi tal Codeine Phenobarbital Methadone Amphetamine Methadone Metabolite Methamphetamine Meperidine
Any appropriate method
Formulated at one level
Ortho Diagnostic Systems division pl
E T H N O K rTY LTD hY DN F V
© L 1 T H N O H PTY LIMITED I<ffi>
The Clinical Biochemist, Newsletter, June 1982 37

Chemica l Crossword 1
C O M P I L E D B Y " S P H I N X
Answers to Chemcrypt 5 Compiled by " F A C T '
a mm mm
B O B BOO • K3DB
DOWN
1 Dicarboxylic acid. 2 Old m L 3 Solvents for men only? 4 Noah's source for atomic emission? 5 Pituitary hormone. 6 Group V element. 7 This chronic lung disease of mine? (An unwholesome
exultation!) 8 Almost die from a crack on the head. 9 Charge detector.
18 You and me in America. 19 Measurement. 21 Found in the liver. 25 Substrate for pyrophosphatases. 27 Protein moiety of an enzyme. 2'J Pipe from a broken Thracean without direction. 30 a r ant i t rypsin phenotypes. 31 Measu rement. 33 E.C.2.6.1.2. 34 An eight carbon monocarboxylic acid, initially without
ionic contraction. 40 Releases histamine. Upright member? 41 Extremely small part of her tattoo. 42 Binds C a + + more strongly than calcein. 43 Schi f f base. 48 Currently it's kinky.
A C R O S S
1 Diuretic. 10 Conservative sort of 47 down? 11 The acetate of this element precipitates N a + .
12 Anti upper. Anti downer. 13 The return of 12 gives a flame. 14 Religion of our universal lecturer. 15 Metal, M.P. 824°C. 16 Symbol for a gluteal notch (with apologies). 17 I tramp umpteen times for my darling heart. 20 Singularly alcoholic phenomenon. 21 Group I element. 22 Enzyme Commission. 23 Phonetically, these doctorings should have nothing to
do with medicine. 24 Insurance for a cofactor? 26 Operon. 28 Sleepy score? 29 Initially, this poor note will get the off4<ey on-key
(. . . hopeful ly). 32 When eaten without direction this broken jelly is bad
eating. 33 Place of confession? 34 What has the male heir of a felon to do with alkaline
phenolphthalein? 35 Raised enzyme? 36 Best for zinc. 37 Quantity. 38 Almost the thyroid hormone. 39 Board of supply? 40 Acid isomer of fumaric acid. 44 Blood group. 45 Halogen. 46 Pertaining to a forearm bone. 47 You enzyme! (Can't get the bugs out of this old fash
ioned talk). 49 Implicated in dental caries.
38 The Clinical Biochemist, Newsletter, June 1982

^
count your assets one by one
COBASSET
i r i -
total or discretionary profiles • all stat tests no sample splitting • one patient report cumulative reporting > built-in back-up huge range of tests • optimum methodologies lower capital cost • lower operating cost today s technology • grows with you
DIAGNOSTICS

A N E W M I C R O S A M P L E RANDOM A C C E S S A N A L Y Z E R
The Technicon RA-1000 is a discrete, bench-top, random access analyzer capable of performing up to 12 different analyses per sample at at operational rate of 240 tests/ hour. Sample volumes vary between 3-20 microlitres and reagent volumes are 300 microlitres for the first reagent and, if required, 20-50 microlitres for the second.
Eighteen programmed methods are currently available and users can programme up to 22 additional methods. Thus, a total of 40 methods can be accommodated on the system. Each sample can be analyzed for up to 12 different chemistries and most programmed methods utilize one reagent although a second reagent is required for AST, ALT and LDH. Serum blanks can be accommodatedforall methods,but Technicon recommends blank determinations for only calcium, uric acid and total bilirubin.
Measurement of reactions can be made by end point; zero order kinetics or first order kinetics at one of five different wavelengths — 340; 405 ; 505; 550 and 600 nm. A sixth wavelength, 380 nm, is used for bichromatic blanking of methods using 340 nm and for detection of substrate depletion of enzymatic analyses. Nine measurements of zero order rate reactions are made for each sample and these are made every .1 5 or 30 seconds. The time interval depends upon enzymatic activity of the sample as measured on the first two, 15 second, readings. If activity is low, then thirty second intervals are made and vice versa for samples with high enzymatic activity. Thus, reactions are monitored for a minimum of 135 sec. or 270 sec. which increases precision and ensures linearity of reaction.
The methods currently available are as follows: Zero First End Rate Order Point ALP Creatinine Albumin Amylase Urea Total Bilirubin ALT Calcium AST Cholesterol C P K Glucose GGT Phosphate LDH Total Protein
Triglycerides Uric Acid
SIMPLICITY The Technicon RA-1000 system is designed to be easy to be operated and is ideal as a supportive system orasanon-cal l instrument.The system operates at 30°C or 37°C and is designed to be kept in the stand-by mode for instant access.
The RA-1000 has three different trays (1) Sample tray with capacity for
30 samples. Micro sample cups are used (0.5ml).
(2) Reagent tray with positions for up to 14 reagents. Reagents are placed in special reagent containers each with capacity of 25ml maximum.
(3) Reaction rotor with 100 optical cuvettes. Once used the reaction tray is disposed to waste.
Reagents and samples are aspirated and dispensed into the reaction cuvettes by means of two separate probes connected to positive displacement syringes.
The test/request information for each samples is entered into the system using a simple keyboard. Tests can be entered either individually or in user defined groups.
When specimens and the appropriate reagents are loaded onto their respective rotors the reaction rotor is placed in position and the system is ready to operate. The "operation" button is depressed and the sampl ing of reagents and samples begins.
The results are collated by the microprocessorand printed in sample order with each result being printed for sample 1 before moving on to sample 2 and so on.
INNOVATIVE The RA-1000 uses a totally novel method for overcoming intersample and inter reagent contamination.
It uses an innovative method for reagent/sample aspiration and dispensing.The technique ensuresthat reagent to reagent and sample to
The Technicon RA-1000 system
sample carryover are reduced to insignificant levels (T.8,000) for sample and 1:1,000,000 for reagent). The basis of the technique is the passage of an inert sil icone based hydrophobic liquid immediately following the sampling of reagent or sample.
The appropriate amount of reagent or sample is aspirated through either sample or reagent probe having been determined (based on the method) by the microprocessor. The suction pressure is provided by a separate Hamilton syringe under microprocessor control for both sample and reagents.
When the sample or reagent probe is placed over the reaction cuvette the aspirant is dispensed followed by an air bubble and thence by a small measured volume (10 ul) of the inert liquid which c leans both the inside and outside of the probe. The inert liquid passes into the bottom of the cuvette (below the reading position). In this way the two sample probes are cleaned immediately after reagent or sample dispensing and are ready for the next aspiration.
SUMMARY T H E TECHNICON RA-1000 F E A T U R E S *Random Access *Microsample — 3-20 microlitres *Absolute Calibration *Small Reagent Volume — 300 microlitres.
*Carryover reduced Sample carryover — less than 1 in 8,000 Reagent carryover — less than 1 in 1 0 s
*30°C and 37°C Operation *1 or 2 Reagent Capability *Reaction Time 15 sec to 10 Mins *User Adaptable Chemistries *Digital Output of Collated Data
III TECHNICON Technicon Equipment Pty. Ltd. 80 Talavera Rd. North Ryde, N.S.W. 2113 Telephone (02) 8881133