
Brain Tumors (Subramaniam)
31
Brain Tumors Brain Tumors Deepa Subramaniam, M.D. Deepa Subramaniam, M.D. Director, Brain Tumor Center Director, Brain Tumor Center Lombardi Comprehensive Cancer Center Lombardi Comprehensive Cancer Center Georgetown University Hospital Georgetown University Hospital Apr 20, 2009 Apr 20, 2009
description
Transcript of Brain Tumors (Subramaniam)

Brain TumorsBrain Tumors
Deepa Subramaniam, M.D.Deepa Subramaniam, M.D.
Director, Brain Tumor CenterDirector, Brain Tumor Center
Lombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Georgetown University HospitalGeorgetown University Hospital
Apr 20, 2009Apr 20, 2009

Classification: 1Classification: 1oo CNS CNS TumorsTumorsGlial tumorsGlial tumors
Astrocytic:Astrocytic:I: pilocytic I: pilocytic II: fibrillary, gemistocyticII: fibrillary, gemistocyticIII: anaplasticIII: anaplasticIV: glioblastoma (var. gliosarcoma, GC GBM)IV: glioblastoma (var. gliosarcoma, GC GBM)
Oligodendroglial:Oligodendroglial:II: oligodendroglioma, III: anaplasticII: oligodendroglioma, III: anaplastic
Ependymal:Ependymal:I: subependymoma, II: ependymoma, III: I: subependymoma, II: ependymoma, III: anaplasticanaplastic

Classification of CNS Classification of CNS tumorstumors
Neuronal tumors:Neuronal tumors:Gangliocytoma, ganglioglioma, esthesioneuroblastomaGangliocytoma, ganglioglioma, esthesioneuroblastoma
Neuroblastic/glioblastic origin:Neuroblastic/glioblastic origin:Neuroblastoma, medulloblastoma (PNET), RBNeuroblastoma, medulloblastoma (PNET), RB
Pineal parenchymal origin:Pineal parenchymal origin:Pineocytoma, pineoblastomaPineocytoma, pineoblastoma
Meningeal origin:Meningeal origin:Meningioma, atypical meningioma, malignant Meningioma, atypical meningioma, malignant meningiomameningioma
Germ cell origin:Germ cell origin:Pure germinoma, dysgerminomaPure germinoma, dysgerminoma
MPNSTMPNSTChordomaChordoma

High cellularity/Nuclear atypiaHigh cellularity/Nuclear atypia
Geographic necrosis/ Geographic necrosis/ PseudopalisadingPseudopalisading
Vascular proliferationVascular proliferation
WHO Grading SystemWHO Grading System

WHO Grading SystemWHO Grading System
# of # of morphologic morphologic
criteriacriteria
Median Median survival survival
(yrs)(yrs)
WHO Gr IWHO Gr I 00 >10>10
WHO Gr IIWHO Gr II 11 77
WHO Gr IIIWHO Gr III 22 33
WHO Gr IVWHO Gr IV 3-43-4 1-21-2

Molecular ProgressionMolecular Progression

Predisposing FactorsPredisposing Factors
Cranial irradiationCranial irradiation NCI Case-control Study:NCI Case-control Study:
GST polymorphismsGST polymorphisms Cyt P450 isoenzymesCyt P450 isoenzymes Inverse relationship to allergic and AI Inverse relationship to allergic and AI
dzdz No relationship to cell phones or No relationship to cell phones or
transmission lines*transmission lines*

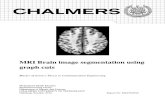
Diagnosis: MRI in HGGDiagnosis: MRI in HGG
T1 weighted post-gadolinium T2 weighted image

High grade gliomas: SurgeryHigh grade gliomas: SurgeryMaximal surgical resection (GTR vs NTR)Maximal surgical resection (GTR vs NTR)
• rapid symptom resolution, decreased mass rapid symptom resolution, decreased mass effecteffect
• adequate tissue for accurate histologic adequate tissue for accurate histologic grading,grading,
• reduces tumor burden prior to chemoradiationreduces tumor burden prior to chemoradiation
Reoperation for recurrent disease Reoperation for recurrent disease • MS with reoperation for recurrent GBM: 14-36 MS with reoperation for recurrent GBM: 14-36
weeksweeks• MS with reoperation for recurrent AA: 56-88 MS with reoperation for recurrent AA: 56-88
weeksweeksHarsh GR et al. Neurosurgery 1987Harsh GR et al. Neurosurgery 1987

HGG: RadiationHGG: Radiation
Brain Tumor Study Group: Brain Tumor Study Group: Addition of adjuvant WBRT Addition of adjuvant WBRT increased MS from 14 to 36 increased MS from 14 to 36 weeks*weeks*
Shift from WBRT to Shift from WBRT to focal EBRTfocal EBRT**** Dose-response relationship***Dose-response relationship***
*Walker MD et al. J Neurosurg 1978*Walker MD et al. J Neurosurg 1978**Liang BC, et al. J Neurosurg 1991**Liang BC, et al. J Neurosurg 1991***Walker MD, Int J Radiat Oncol Biol Phys 1979***Walker MD, Int J Radiat Oncol Biol Phys 1979

HGG: RadiationHGG: Radiation
Phase II studies of high-dose boost Phase II studies of high-dose boost added to standard XRT: OS benefitadded to standard XRT: OS benefit
Randomized Phase III trial of SRS Randomized Phase III trial of SRS boost: No added benefitboost: No added benefit

HGG: Single Agent ChemoHGG: Single Agent Chemo1978:1978: BTSG (Protocol 69-01): BTSG (Protocol 69-01): Walker, MD. J Neurosurg 1978Walker, MD. J Neurosurg 1978
18-month survival:18-month survival: WBRT + carmustine (19%) > WBRT (4%)WBRT + carmustine (19%) > WBRT (4%)
1983: BTSG (Protocol 75-01): 1983: BTSG (Protocol 75-01): Green, SB. Cancer Treat Rep 1983Green, SB. Cancer Treat Rep 1983
WBRT + procarbazine = WBRT + carmustineWBRT + procarbazine = WBRT + carmustine

HGG: Combination chemoHGG: Combination chemoNorthern California Oncology Group protocol 6G61Northern California Oncology Group protocol 6G61
Randomized trial comparing PCV to BCNU after adjuvant radiotherapyRandomized trial comparing PCV to BCNU after adjuvant radiotherapy
PCV improves TTP and OS in Anaplastic AstrocytomaPCV improves TTP and OS in Anaplastic Astrocytoma
Levin VA, Int J Radiation Oncology Biol. Phys. 1990 Levin VA, Int J Radiation Oncology Biol. Phys. 1990
TreatmentTreatment AA (50AA (50thth)) GBM (50GBM (50thth))
TTP: BCNUTTP: BCNU 62.7 weeks62.7 weeks 34.4 weeks34.4 weeks
TTP: PCVTTP: PCV 125.6 weeks125.6 weeks 37.4 weeks37.4 weeks
Survival: BCNUSurvival: BCNU 82.1 weeks82.1 weeks 57.4 weeks57.4 weeks
Survival: PCVSurvival: PCV 157.1 weeks157.1 weeks 50.4 weeks50.4 weeks

Adjuvant Chemo: Adjuvant Chemo: CombinationCombinationFine et al. Cancer, 1993:Fine et al. Cancer, 1993: Meta-analysis of 16 randomized trials, 17-year period, 3000 Meta-analysis of 16 randomized trials, 17-year period, 3000
patients (GBM and AA), assigned to WBRT patients (GBM and AA), assigned to WBRT ++ nitrosoureas nitrosoureas• Absolute increase in survival with addition of chemo was Absolute increase in survival with addition of chemo was
10.1% at 1 year, 8.6% at 2 years10.1% at 1 year, 8.6% at 2 years• Median survival increased from 9.4 to 12 monthsMedian survival increased from 9.4 to 12 months
Medical Research CouncilMedical Research Council. . JCO, 2001:JCO, 2001: Randomized study where 674 patients (GBM and AA) were Randomized study where 674 patients (GBM and AA) were
treated with surgery + RT treated with surgery + RT ++ PCV PCV• MS of GBM: 9.5 months MS of GBM: 9.5 months vv 10 months; MS of AA: 13 months 10 months; MS of AA: 13 months
Stewart, LA. Lancet, 2002:Stewart, LA. Lancet, 2002: Meta-analysis of 12 RCTs, 3004 patients, compared RT alone Meta-analysis of 12 RCTs, 3004 patients, compared RT alone
to RT + chemoto RT + chemo• Absolute increase in survival with addition of chemo was 6% at Absolute increase in survival with addition of chemo was 6% at
1 year1 year• Median survival increased by 2 monthsMedian survival increased by 2 months

Newer agentsNewer agents
Temozolomide:Temozolomide: Novel alklyating agentNovel alklyating agent Orally active, 100% Orally active, 100%
bioavailablebioavailable Pro drug with good Pro drug with good
CSF penetration – CSF penetration – converted to an active converted to an active metabolite (MTIC) in metabolite (MTIC) in CNSCNS
Well tolerated/immune Well tolerated/immune suppressionsuppression
MGMT silencing – MGMT silencing – molecular markermolecular marker
N
H
N
O
N
NH
H2N

HRQOL: TMZ vs PCB for recurrent HRQOL: TMZ vs PCB for recurrent GBM: GBM:
Osoba et al. JCO 2000Osoba et al. JCO 2000

TMZ in Newly Diagnosed GBM: TMZ in Newly Diagnosed GBM:
Stupp NEJM 2005Stupp NEJM 2005

Stupp NEJM 2005Stupp NEJM 2005
PFS Benefit
OS Benefit

MGMT gene methylationMGMT gene methylation
Hegi ME et al. NEJM 2005Hegi ME et al. NEJM 2005

Glioblastoma ResearchGlioblastoma Research

Overcoming ResistanceOvercoming Resistance

Individualized therapyIndividualized therapy

Targeting angiogenesisTargeting angiogenesis
BevacizumabBevacizumab AZD2171AZD2171 Vatalanib (PTK 787)Vatalanib (PTK 787) Vandetanib (ZD6474)Vandetanib (ZD6474)

Bevacizumab/IrinotecanBevacizumab/Irinotecan
Phase II study (Phase II study (Vredenburgh et al, JCO 2007Vredenburgh et al, JCO 2007):): 63% radiographic response rates in 63% radiographic response rates in
AA+GBM study (CCR, Feb 2007)AA+GBM study (CCR, Feb 2007) 6-month PFS 46%, 6-month OS 77% in 6-month PFS 46%, 6-month OS 77% in
GBM GBM (n=35; 1 CNS bleed, 4 DVT/PE; (n=35; 1 CNS bleed, 4 DVT/PE; JCO, Oct 2007JCO, Oct 2007))

AZD2171 (Cediranib)AZD2171 (Cediranib)
Phase II multicenter trialPhase II multicenter trial 56% radiographic partial responses56% radiographic partial responses 25% APFS25% APFS PFS 117 daysPFS 117 days OS 221 daysOS 221 days
Phase III RCT lomustine, vs Phase III RCT lomustine, vs AZD2171 vs combinationAZD2171 vs combination

Novel agentsNovel agents
EGFR inhibitors (erlotinib)EGFR inhibitors (erlotinib) PKC inhibitors (enzastaurin)PKC inhibitors (enzastaurin) Integrin inhibitors (cilengitide)Integrin inhibitors (cilengitide) mTOR inhibitors (everolimus, mTOR inhibitors (everolimus,
temsirolimus)temsirolimus)

Metastatic Brain DiseaseMetastatic Brain Disease
150,000 annual cases in the US150,000 annual cases in the US 10-20% of all cancers will 10-20% of all cancers will
metastasizemetastasize Most common to brain:Most common to brain:
Lung cancerLung cancer BreastBreast MelanomaMelanoma KidneyKidney

Metastatic Brain DiseaseMetastatic Brain Disease
Standard therapy:Standard therapy: Whole brain radiationWhole brain radiation Stereotactic radiosurgeryStereotactic radiosurgery Surgical resectionSurgical resection Combination of the aboveCombination of the above
NO SYSTEMIC THERAPIESNO SYSTEMIC THERAPIESThe Basic premise: BBB is intactThe Basic premise: BBB is intact

The Blood-Brain BarrierThe Blood-Brain Barrier

BBB: Drug transportersBBB: Drug transporters

CNS Metastases: Novel CNS Metastases: Novel ApproachesApproaches
NanoparticlesNanoparticles ImmunoliposomesImmunoliposomes Peptide vectorsPeptide vectors Endogenous-carrier mediated Endogenous-carrier mediated
transporttransport Small molecule TKIsSmall molecule TKIs











![Presentatie Brain@Work (Model)[1]](https://static.fdocuments.nl/doc/165x107/559dc3c61a28ab843e8b4750/presentatie-brainwork-model1.jpg)
