Bahan Lapsus Brain Tumor

of 32
-
Upload
nyoman-d-airbud -
Category
Documents
-
view
220 -
download
0
Transcript of Bahan Lapsus Brain Tumor
-
8/12/2019 Bahan Lapsus Brain Tumor
1/32
-
8/12/2019 Bahan Lapsus Brain Tumor
2/32
ymptoms of solid neoplasms of the brain (primary brain tumors and secondary tumors
alike) can be divided in main categories*
/onse0uences of intracranial hypertension* The symptoms that often occur first
are those that are the conse0uences of increased intracranial pressure* 1argetumors or tumors with e&tensive perifocal swelling (edema) inevitably lead to
elevated intracranial pressure(intracranial hypertension), which translates clinically
into headaches, vomiting(sometimes without nausea), altered state
of consciousness(somnolence, coma), dilation of the pupil on the side of the lesion
(anisocoria),papilledema(prominent optic discat the funduscopic eye e&amination).
!owever, even small tumors obstructing the passage of cerebrospinal fluid(/2)
may cause early signs of increased intracranial pressure. #ncreased intracranial
pressure may result in herniation(i.e. displacement) of certain parts of the brain,
such as the cerebellar tonsilsor the temporal uncus, resulting in
lethal brainstemcompression. #n very young children, elevated intracranial pressure
may cause an increase in the diameter of the skulland bulging of the fontanelles.
3ysfunction* depending on the tumor location and the damage it may have
caused to surrounding brainstructures, either through compression or infiltration,
any type of focal neurologic symptomsmay occur, such
as cognitiveand behavioralimpairment (including impaired 4udgment, memory loss,
lack of recognition, spatial orientation disorders), personalityor emotional
changes,hemiparesis, hypoesthesia, aphasia, ata&ia, visual fieldimpairment,impaired sense of smell, impaired hearing, facial paralysis,double vision, di$$iness,
but more severe symptoms might occur too such as* paralysis on one side of the
bodyhemiplegiaor impairment to swallow . These symptoms are not specific for
brain tumors + they may be caused by a large variety of neurologic conditions
(e.g.stroke, traumatic brain in4ury). What counts, however, is the location of the
lesion and the functional systems (e.g.motor, sensory, visual, etc.) it affects. A
bilateral temporal visual fielddefect (bitemporal hemianopia5due to compression of
theoptic chiasm), often associated with endocrine dysfunction5
eitherhypopituitarismor hyperproduction of
pituitaryhormonesandhyperprolactinemiais suggestive of a pituitary tumor.
#rritation* abnormal fatigue, weariness, absences and tremors, but also epileptic
sei$ures.
http://en.wikipedia.org/wiki/Intracranial_hypertensionhttp://en.wikipedia.org/wiki/Edemahttp://en.wikipedia.org/wiki/Intracranial_pressurehttp://en.wikipedia.org/wiki/Headacheshttp://en.wikipedia.org/wiki/Vomitinghttp://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Consciousnesshttp://en.wikipedia.org/wiki/Somnolencehttp://en.wikipedia.org/wiki/Comahttp://en.wikipedia.org/wiki/Anisocoriahttp://en.wikipedia.org/wiki/Papilledemahttp://en.wikipedia.org/wiki/Papilledemahttp://en.wikipedia.org/wiki/Optic_dischttp://en.wikipedia.org/wiki/Cerebrospinal_fluidhttp://en.wikipedia.org/wiki/Herniationhttp://en.wikipedia.org/wiki/Cerebellar_tonsilshttp://en.wikipedia.org/wiki/Uncushttp://en.wikipedia.org/wiki/Brainstemhttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/wiki/Fontanellehttp://en.wikipedia.org/wiki/Human_brainhttp://en.wikipedia.org/wiki/Focal_neurologic_symptomhttp://en.wikipedia.org/wiki/Cognitivehttp://en.wikipedia.org/wiki/Behavioralhttp://en.wiktionary.org/wiki/personalityhttp://en.wikipedia.org/wiki/Hemiparesishttp://en.wikipedia.org/wiki/Hypoesthesiahttp://en.wikipedia.org/wiki/Aphasiahttp://en.wikipedia.org/wiki/Ataxiahttp://en.wikipedia.org/wiki/Visual_fieldhttp://en.wikipedia.org/wiki/Facial_paralysishttp://en.wikipedia.org/wiki/Diplopiahttp://en.wikipedia.org/wiki/Dizzinesshttp://en.wikipedia.org/wiki/Dizzinesshttp://en.wikipedia.org/wiki/Hemiplegiahttp://en.wikipedia.org/wiki/Hemiplegiahttp://en.wikipedia.org/wiki/Strokehttp://en.wikipedia.org/wiki/Traumatic_brain_injuryhttp://en.wikipedia.org/wiki/Visual_fieldhttp://en.wikipedia.org/wiki/Bitemporal_hemianopiahttp://en.wikipedia.org/wiki/Optic_chiasmhttp://en.wikipedia.org/wiki/Hypopituitarismhttp://en.wikipedia.org/wiki/Hypopituitarismhttp://en.wikipedia.org/wiki/Hormoneshttp://en.wikipedia.org/wiki/Hormoneshttp://en.wikipedia.org/wiki/Hyperprolactinemiahttp://en.wikipedia.org/wiki/Tremorhttp://en.wikipedia.org/wiki/Epilepsyhttp://en.wikipedia.org/wiki/Epilepsyhttp://en.wikipedia.org/wiki/Intracranial_hypertensionhttp://en.wikipedia.org/wiki/Edemahttp://en.wikipedia.org/wiki/Intracranial_pressurehttp://en.wikipedia.org/wiki/Headacheshttp://en.wikipedia.org/wiki/Vomitinghttp://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Consciousnesshttp://en.wikipedia.org/wiki/Somnolencehttp://en.wikipedia.org/wiki/Comahttp://en.wikipedia.org/wiki/Anisocoriahttp://en.wikipedia.org/wiki/Papilledemahttp://en.wikipedia.org/wiki/Optic_dischttp://en.wikipedia.org/wiki/Cerebrospinal_fluidhttp://en.wikipedia.org/wiki/Herniationhttp://en.wikipedia.org/wiki/Cerebellar_tonsilshttp://en.wikipedia.org/wiki/Uncushttp://en.wikipedia.org/wiki/Brainstemhttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/wiki/Fontanellehttp://en.wikipedia.org/wiki/Human_brainhttp://en.wikipedia.org/wiki/Focal_neurologic_symptomhttp://en.wikipedia.org/wiki/Cognitivehttp://en.wikipedia.org/wiki/Behavioralhttp://en.wiktionary.org/wiki/personalityhttp://en.wikipedia.org/wiki/Hemiparesishttp://en.wikipedia.org/wiki/Hypoesthesiahttp://en.wikipedia.org/wiki/Aphasiahttp://en.wikipedia.org/wiki/Ataxiahttp://en.wikipedia.org/wiki/Visual_fieldhttp://en.wikipedia.org/wiki/Facial_paralysishttp://en.wikipedia.org/wiki/Diplopiahttp://en.wikipedia.org/wiki/Dizzinesshttp://en.wikipedia.org/wiki/Hemiplegiahttp://en.wikipedia.org/wiki/Strokehttp://en.wikipedia.org/wiki/Traumatic_brain_injuryhttp://en.wikipedia.org/wiki/Visual_fieldhttp://en.wikipedia.org/wiki/Bitemporal_hemianopiahttp://en.wikipedia.org/wiki/Optic_chiasmhttp://en.wikipedia.org/wiki/Hypopituitarismhttp://en.wikipedia.org/wiki/Hormoneshttp://en.wikipedia.org/wiki/Hyperprolactinemiahttp://en.wikipedia.org/wiki/Tremorhttp://en.wikipedia.org/wiki/Epilepsyhttp://en.wikipedia.org/wiki/Epilepsy -
8/12/2019 Bahan Lapsus Brain Tumor
3/32
The above symptoms are true for A11 types of neoplasm of the brain (including
secondary tumors). #t is common that a person carriesa primary benign neoplasm for
several years and have no visible symptoms at all. 6any present some uncertain and
intermittent symptoms like headaches and occasional vomiting or weariness, which can
be easily mistaken for gastritisor gastroenteritis. #t might seem strange that despite
having a mass in his skull e&ercising pressure on the brain the patient feels no pain, but
as anyone who has suffered a concussion can attest, pain is felt on the outside of
the skulland not in the brain itself. The brain has no nerve sensors in the meninges
(outer surface) with which to feel or transmit pain to the brain7s pain center" it cannot
signal pain without a sensory input. That is why secondary symptoms like those
described above should alert doctors to the possible diagnosis of a neoplasm of the
brain.
#n a recent study by the 3utch 8' Association, a list of causes of headaches 9:;waspublished, that should alert 8'7s to take their diagnosis further than to choose for
symptomatic treatment of headaches with simple pain medication (note the occurrence
of brain tumors as possible cause)*
Alarm signals Possible cause
First headache complaint from person
over 50 years old
brain tumor, arteritis temporalis
First migraine attack in person over 40years old
brain tumor
Headache in person under 6 years old brain tumor, hydrocephalus
Person over 50 years old ith pain at
temples!iant"cell arteritis
Pregnancy ith unknon headache pre"eclampsia
#ncreased headaches after trauma sub$epidural hematoma
http://en.wikipedia.org/wiki/Gastritishttp://en.wikipedia.org/wiki/Gastroenteritishttp://en.wikipedia.org/wiki/Skullhttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-1http://en.wikipedia.org/wiki/Giant-cell_arteritishttp://en.wikipedia.org/wiki/Hydrocephalushttp://en.wikipedia.org/wiki/Giant-cell_arteritishttp://en.wikipedia.org/wiki/Headachehttp://en.wikipedia.org/wiki/Pre-eclampsiahttp://en.wikipedia.org/wiki/Hematomahttp://en.wikipedia.org/wiki/Gastritishttp://en.wikipedia.org/wiki/Gastroenteritishttp://en.wikipedia.org/wiki/Skullhttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-1http://en.wikipedia.org/wiki/Giant-cell_arteritishttp://en.wikipedia.org/wiki/Hydrocephalushttp://en.wikipedia.org/wiki/Giant-cell_arteritishttp://en.wikipedia.org/wiki/Headachehttp://en.wikipedia.org/wiki/Pre-eclampsiahttp://en.wikipedia.org/wiki/Hematoma -
8/12/2019 Bahan Lapsus Brain Tumor
4/32
%evere headaches and very high bloodpressure
malignant hypertension
&cute severe headache meningitis,'(&)'erebrovascular accident orstroke*, subarachnoidal hemorrhage
Headache and fever )ith reducedconsciousness*
meningitis
%tiffness of the neck$neurologicaldysfunction
meningitis, brain tumor
Headache ith signs ofelevatedintracranial pressure
brain tumor
Focal neurological dysfunction brain tumor
+arly morning vomiting or vomiting
unrelated to headache or other illnessbrain tumor
ehavioral changes or rapid decline in
school resultsbrain tumor
/ause
Aside from e&posure to vinyl chlorideor ioni$ing radiation, there are no known
environmental factors associated with brain tumors. 6utations and deletions of so
called tumor suppressor genesare thought to be the cause of some forms of brain
tumors. 'eople with various inherited diseases, such as on !ippel1indau
syndrome, multiple endocrine neoplasia, neurofibromatosistype < are at high risk of
developing brain tumors.
Although studies have not shown any link between cell phone radiationand brain
tumors,9/scale into 8roup
-
8/12/2019 Bahan Lapsus Brain Tumor
5/32
some risk of carcinogenicity, so additional research into the longterm, heavy use of
mobile phones needs to be conducted. 9;
9edit;Types
Tumors can be benignor malignant, can occur in different parts of the brain, and may or
may not be primary tumors. A primary tumor is one that has started in the brain, as
opposed to a metastatictumor, which is something that has spread to the brain from
another part of the body.9?;Tumors may or may not be symptomatic* some tumors are
discovered because the patient has symptoms, others show up incidentally on an
imaging scan, or at an autopsy.
The most common primary brain tumors are*9@;
8liomas (@.?) 6eningiomas (
-
8/12/2019 Bahan Lapsus Brain Tumor
6/32
[edit]Anatomy
2rom the brainWikipedia article and for the purpose of understanding this article some
summary notes about the brain and its different types of organic tissues will be
provided.
When reading the human brain in the picture on the right, only a few of the areas are
really of interest to us. The first type of tissue encountered beneath the skullbone in the
intracranial cavity is actually not shown on this picture* the meninges. This is what is
inflamed in meningitis.
[edit]Meninges
!uman brains are surrounded by a system of connective tissuemembranes
called meningesthat separate the skullfrom the brain. This threelayered covering is
composed of (from the outside in) the dura mater(hard mother), arachnoidmater(spidery mother), and pia mater(soft mother). The arachnoid and pia are
physically connected and thus often considered as a single layer, the piaarachnoid.
Below the arachnoid is the subarachnoid spacewhich contains cerebrospinal fluid,
which circulates in the narrow spaces between cells and through cavities
called ventricles, and serves to nourish, support, and protect the brain tissue. Blood
vesselsenter the central nervous systemthrough the perivascular space above the pia
mater. The cells in the blood vessel walls are 4oined tightly, forming the blood+brain
barrier which protects the brain from to&insthat might enter through the blood. Tumors
of the meninges are meningiomaand are often benign neoplasms.
[edit]Brain matter
The brains of vertebrates(including humans) are made of very soft tissue, with a te&ture
that has been compared to gelatin. 1iving brain tissue is pinkish on the outside and
mostly white on the inside, with subtle variations in color. Three separate brain areas
make up the ma4ority of brain volume*
telencephalon (cerebral hemispheres or cerebrum)
mesencephalon (midbrain)
cerebellum
These areas are composed of two broad classes of cells* neuronsand glia. These two
types are e0ually numerous in the brain as a whole, although glial
http://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=5http://en.wikipedia.org/wiki/Human_brainhttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=6http://en.wikipedia.org/wiki/Connective_tissuehttp://en.wikipedia.org/wiki/Meningeshttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/wiki/Human_brainhttp://en.wikipedia.org/wiki/Dura_materhttp://en.wikipedia.org/wiki/Dura_materhttp://en.wikipedia.org/wiki/Arachnoid_materhttp://en.wikipedia.org/wiki/Arachnoid_materhttp://en.wikipedia.org/wiki/Pia_materhttp://en.wikipedia.org/wiki/Subarachnoid_spacehttp://en.wikipedia.org/wiki/Cerebrospinal_fluidhttp://en.wikipedia.org/wiki/Ventricular_systemhttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Central_nervous_systemhttp://en.wikipedia.org/wiki/Toxinshttp://en.wikipedia.org/wiki/Meningiomahttp://en.wikipedia.org/wiki/Benign_neoplasmshttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=7http://en.wikipedia.org/wiki/Vertebrateshttp://en.wikipedia.org/wiki/Telencephalonhttp://en.wikipedia.org/wiki/Cerebrumhttp://en.wikipedia.org/wiki/Mesencephalonhttp://en.wikipedia.org/wiki/Cerebellumhttp://en.wikipedia.org/wiki/Neuronshttp://en.wikipedia.org/wiki/Gliahttp://en.wikipedia.org/wiki/Glial_cellshttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=5http://en.wikipedia.org/wiki/Human_brainhttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=6http://en.wikipedia.org/wiki/Connective_tissuehttp://en.wikipedia.org/wiki/Meningeshttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/wiki/Human_brainhttp://en.wikipedia.org/wiki/Dura_materhttp://en.wikipedia.org/wiki/Arachnoid_materhttp://en.wikipedia.org/wiki/Arachnoid_materhttp://en.wikipedia.org/wiki/Pia_materhttp://en.wikipedia.org/wiki/Subarachnoid_spacehttp://en.wikipedia.org/wiki/Cerebrospinal_fluidhttp://en.wikipedia.org/wiki/Ventricular_systemhttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Central_nervous_systemhttp://en.wikipedia.org/wiki/Toxinshttp://en.wikipedia.org/wiki/Meningiomahttp://en.wikipedia.org/wiki/Benign_neoplasmshttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=7http://en.wikipedia.org/wiki/Vertebrateshttp://en.wikipedia.org/wiki/Telencephalonhttp://en.wikipedia.org/wiki/Cerebrumhttp://en.wikipedia.org/wiki/Mesencephalonhttp://en.wikipedia.org/wiki/Cerebellumhttp://en.wikipedia.org/wiki/Neuronshttp://en.wikipedia.org/wiki/Gliahttp://en.wikipedia.org/wiki/Glial_cells -
8/12/2019 Bahan Lapsus Brain Tumor
7/32
-
8/12/2019 Bahan Lapsus Brain Tumor
8/32
-
8/12/2019 Bahan Lapsus Brain Tumor
9/32
highresolution techni0ues, such as computed tomography(/T)scans and
especially magnetic resonance imaging(6>#). Deoplasms will often show as differently
colored masses (also referred to as processes) in /T or 6># results.
Benign brain tumors often show up as hypodense (darker than brain tissue) masslesions on cranial /Tscans. =n 6>#, they appear either hypo (darker than brain tissue) or
isointense (same intensity as brain tissue) on T:weighted scans, or hyperintense (brighter
than brain tissue) on T#, although the appearance is variable.
/ontrast agent uptake, sometimes in characteristic patterns, can be demonstrated on
either /T or 6>#scans in most malignant primary and metastatic brain tumors.
'erifocal edema, or pressureareas, or where the brain tissue has been compressed by
an invasive process also appears hyperintense on T#, they might indicate the
presence a diffuse neoplasm (unclear outline)
This is because these tumors disrupt the normal functioning of theblood+brain
barrierand lead to an increase in its permeability. !owever it is not possible to diagnose
high versus low grade gliomas based on enhancement pattern alone.
8lioblastoma multiformeand anaplastic astrocytomahave been associated9by whom?;with
the genetic acute hepatic porphyrias('/T,A#',!/'and '), including positive testing
associated with drug refractory sei$ures. 9citation needed;%ne&plained complications
associated with drug treatments with these tumors should alert physicians to anundiagnosed neurological porphyria.
The definitive diagnosisof brain tumor can only be confirmed by histological
e&aminationof tumortissuesamples obtained either by means of brain biopsyor
open surgery. The histological e&amination is essential for determining the appropriate
treatment and the correct prognosis. This e&amination, performed by a pathologist,
typically has three stages* interoperative e&amination of fresh tissue, preliminary
microscopic e&amination of prepared tissues, and followup e&amination of prepared
tissues after immunohistochemical staining or genetic analysis.
http://en.wikipedia.org/wiki/Computed_tomographyhttp://en.wikipedia.org/wiki/Magnetic_resonance_imaginghttp://en.wikipedia.org/wiki/Contrast_agenthttp://en.wikipedia.org/wiki/Contrast_agenthttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrierhttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrierhttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrierhttp://en.wikipedia.org/wiki/Glioblastoma_multiformehttp://en.wikipedia.org/wiki/Astrocytomahttp://en.wikipedia.org/wiki/Wikipedia:Avoid_weasel_wordshttp://en.wikipedia.org/wiki/Wikipedia:Avoid_weasel_wordshttp://en.wikipedia.org/wiki/Wikipedia:Avoid_weasel_wordshttp://en.wikipedia.org/wiki/Porphyriahttp://en.wikipedia.org/wiki/Porphyria_cutanea_tardahttp://en.wikipedia.org/wiki/Porphyria_cutanea_tardahttp://en.wikipedia.org/wiki/Acute_intermittent_porphyriahttp://en.wikipedia.org/wiki/Hereditary_coproporphyriahttp://en.wikipedia.org/wiki/Hereditary_coproporphyriahttp://en.wikipedia.org/wiki/Variegate_porphyriahttp://en.wikipedia.org/wiki/Wikipedia:Citation_neededhttp://en.wikipedia.org/wiki/Wikipedia:Citation_neededhttp://en.wikipedia.org/wiki/Medical_diagnosishttp://en.wikipedia.org/wiki/Histologyhttp://en.wikipedia.org/wiki/Histologyhttp://en.wikipedia.org/wiki/Tumorhttp://en.wikipedia.org/wiki/Tumorhttp://en.wikipedia.org/wiki/Biological_tissuehttp://en.wikipedia.org/wiki/Biopsyhttp://en.wikipedia.org/wiki/Surgeryhttp://en.wikipedia.org/wiki/Prognosishttp://en.wikipedia.org/wiki/Pathologisthttp://en.wikipedia.org/wiki/Computed_tomographyhttp://en.wikipedia.org/wiki/Magnetic_resonance_imaginghttp://en.wikipedia.org/wiki/Contrast_agenthttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrierhttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrierhttp://en.wikipedia.org/wiki/Glioblastoma_multiformehttp://en.wikipedia.org/wiki/Astrocytomahttp://en.wikipedia.org/wiki/Wikipedia:Avoid_weasel_wordshttp://en.wikipedia.org/wiki/Porphyriahttp://en.wikipedia.org/wiki/Porphyria_cutanea_tardahttp://en.wikipedia.org/wiki/Acute_intermittent_porphyriahttp://en.wikipedia.org/wiki/Hereditary_coproporphyriahttp://en.wikipedia.org/wiki/Variegate_porphyriahttp://en.wikipedia.org/wiki/Wikipedia:Citation_neededhttp://en.wikipedia.org/wiki/Medical_diagnosishttp://en.wikipedia.org/wiki/Histologyhttp://en.wikipedia.org/wiki/Histologyhttp://en.wikipedia.org/wiki/Tumorhttp://en.wikipedia.org/wiki/Biological_tissuehttp://en.wikipedia.org/wiki/Biopsyhttp://en.wikipedia.org/wiki/Surgeryhttp://en.wikipedia.org/wiki/Prognosishttp://en.wikipedia.org/wiki/Pathologist -
8/12/2019 Bahan Lapsus Brain Tumor
10/32
[edit]Pathology
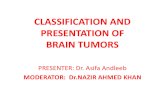
6icrographof an oligodendroglioma, a type of brain cancer. Brain biopsy. !GF stain.
Tumors have characteristics that allow determination of its malignacy, how it will evolve
and it will allow the medical team to determine the management plan.
Anaplasia* or dedifferentiation" loss of differentiation of cells and of their orientation to
one another and blood vessels, a characteristic of anaplastic tumor tissue. Anaplastic
cells have lost total control of their normal functions and many have deteriorated cell
structures. Anaplastic cells often have abnormally high nucleartocytoplasmic ratios,
and many are multinucleated. Additionally, the nuclei of anaplastic cells are usually
unnaturally shaped or oversi$ed nuclei. /ells can become anaplastic in two ways*
neoplastic tumor cells can dedifferentiate to become anaplasias (the dedifferentiation
causes the cells to lose all of their normal structure-function), or cancer stem cells can
increase in their capacity to multiply (i.e., uncontrollable growth due to failure of
differentiation).
Atypia* is an indication of abnormality of a cell (which may be indicative for malignancy).
ignificance of the abnormality is highly dependent on conte&t.
Deoplasia* is the (uncontrolled) division of cells" as such neoplasia is not problematic
but its conse0uences are* the uncontrolled division of cells means that the mass of a
neoplasm increases in si$e, and in a confined space such as the intracranial cavity this
0uickly becomes problematic because the mass invades the space of the brain pushing
it aside, leading to compression of the brain tissue and increased intracranial pressure
and destruction of brain parenchyma. #ncreased #ntracranial pressure (#/') may be
attributable to the direct mass effect of the tumor, increased blood volume, or increased
cerebrospinal fluid (/2) volume may in turn have secondary symptoms
http://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=11http://en.wikipedia.org/wiki/Micrographhttp://en.wikipedia.org/wiki/Oligodendrogliomahttp://en.wikipedia.org/wiki/Biopsyhttp://en.wikipedia.org/wiki/H%26E_stainhttp://en.wikipedia.org/wiki/Anaplasiahttp://en.wikipedia.org/wiki/Atypiahttp://en.wikipedia.org/wiki/Neoplasiahttp://en.wikipedia.org/wiki/Parenchymahttp://en.wikipedia.org/wiki/File:Oligodendroglioma1_high_mag.jpghttp://en.wikipedia.org/wiki/File:Oligodendroglioma1_high_mag.jpghttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=11http://en.wikipedia.org/wiki/Micrographhttp://en.wikipedia.org/wiki/Oligodendrogliomahttp://en.wikipedia.org/wiki/Biopsyhttp://en.wikipedia.org/wiki/H%26E_stainhttp://en.wikipedia.org/wiki/Anaplasiahttp://en.wikipedia.org/wiki/Atypiahttp://en.wikipedia.org/wiki/Neoplasiahttp://en.wikipedia.org/wiki/Parenchyma -
8/12/2019 Bahan Lapsus Brain Tumor
11/32
Decrosis* is the (premature) death of cells, caused by e&ternal factors such as infection,
to&in or trauma. Decrotic cells send the wrong chemical signals which
prevents phagocytesfrom disposing of the dead cells, leading to a build up of dead
tissue, cell debris and to&ins at or near the site of the necrotic cells 9H;
Arterial and venous hypo&ia, or the deprivation of ade0uate o&ygen supply to certain
areas of the brain, occurs when a tumor makes use of nearby blood vessels for its
supply of blood and the neoplasm enters into competition for nutrients with the
surrounding brain tissue.
6ore generally a neoplasm may cause release of metabolic end products (e.g., free
radicals, altered electrolytes, neurotransmitters), and release and recruitment of cellular
mediators (e.g., cytokines) that disrupt normal parenchymal function.
[edit]
Classification[edit]Secondary brain tumors
econdary tumors of the brain are metastatic tumorsthat invaded the intracranial
sphere from cancersoriginating in other organs. This means that a cancerous neoplasm
has developed in another organ elsewhere in the body and that cancer cells have
leaked from that primary tumor and then entered the lymphatic systemand blood
vessels. These are most common among brain tumors. #n the %nited tates there are
about :H, new cases every year.9C;They then circulate through the bloodstream,
and are deposited in the brain. There, these cells continue growing and dividing,becoming another invasive neoplasm of the primary cancer7s tissue. econdary tumors
of the brain are very common in the terminal phases of patients with an incurable
metastasi$ed cancer" the most common types of cancers that bring about secondary
tumors of the brain are lung cancer, breast cancer, malignantmelanoma, kidney
cancerand colon cancer(in decreasing order of fre0uency).
econdary brain tumors are the most common cause of tumors in the intracranial cavity.
The skullbone structure can also be sub4ect to a neoplasm that by its very nature
reduces the volume of the intracranial cavity, and can damage the brain.
[edit]By behavior
Brain tumors or intracranial neoplasms can be cancerous(malignant) or noncancerous
(benign). !owever, the definitions of malignant or benign neoplasms differs from those
commonly used in other types of cancerous or noncancerous neoplasms in the body.
#n cancers elsewhere in the body, three malignant properties differentiate benign tumors
http://en.wikipedia.org/wiki/Necrosishttp://en.wikipedia.org/wiki/Phagocyteshttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-necrs-7http://en.wikipedia.org/wiki/Hypoxia_(medical)http://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=12http://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=13http://en.wikipedia.org/wiki/Metastasishttp://en.wikipedia.org/wiki/Cancerhttp://en.wikipedia.org/wiki/Lymphatic_systemhttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-8http://en.wikipedia.org/wiki/Lung_cancerhttp://en.wikipedia.org/wiki/Breast_cancerhttp://en.wikipedia.org/wiki/Melanomahttp://en.wikipedia.org/wiki/Melanomahttp://en.wikipedia.org/wiki/Kidney_cancerhttp://en.wikipedia.org/wiki/Kidney_cancerhttp://en.wikipedia.org/wiki/Colon_cancerhttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=14http://en.wikipedia.org/wiki/Canceroushttp://en.wikipedia.org/wiki/Necrosishttp://en.wikipedia.org/wiki/Phagocyteshttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-necrs-7http://en.wikipedia.org/wiki/Hypoxia_(medical)http://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=12http://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=13http://en.wikipedia.org/wiki/Metastasishttp://en.wikipedia.org/wiki/Cancerhttp://en.wikipedia.org/wiki/Lymphatic_systemhttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Blood_vesselshttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-8http://en.wikipedia.org/wiki/Lung_cancerhttp://en.wikipedia.org/wiki/Breast_cancerhttp://en.wikipedia.org/wiki/Melanomahttp://en.wikipedia.org/wiki/Kidney_cancerhttp://en.wikipedia.org/wiki/Kidney_cancerhttp://en.wikipedia.org/wiki/Colon_cancerhttp://en.wikipedia.org/wiki/Human_skullhttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=14http://en.wikipedia.org/wiki/Cancerous -
8/12/2019 Bahan Lapsus Brain Tumor
12/32
from malignant forms of cancer* benign tumors are selflimited and do not invade or
metastasi$e. /haracteristics of malignant tumors include*
uncontrolled mitosis (growth by division beyond the normal limits)
anaplasia* the cells in the neoplasm have an obviously different form (in si$e and
shape). Anaplastic cells display markedpleomorphism. The cell nucleiare characteristically
e&tremely hyperchromatic (darkly stained) and enlarged" the nucleus might have the same
si$e as the cytoplasmof the cell (nuclearcytoplasmic ratio may approach :*:, instead of the
normal :*? or :*E ratio).8iant cells+ considerably larger than their neighbors + may form
and possess either one enormous nucleus or several nuclei (syncytia). Anaplastic nuclei are
variable and bi$arre in si$e and shape.
invasion or infiltration (medical literature uses these terms as synonymous e0uivalents.
!owever, for clarity, the articles that follow adhere to a convention that they mean slightly
different things" this convention is not followed outside these articles)*
#nvasion or invasiveness is the spatial e&pansion of the tumor through
uncontrolled mitosis, in the sense that the neoplasm invades the space occupied by
ad4acent tissue, thereby pushing the other tissue aside and eventually compressing the
tissue. =ften these tumors are associated with clearly outlined tumors in imaging.
#nfiltration is the behavior of the tumor either to grow (microscopic) tentacles that
push into the surrounding tissue (often making the outline of the tumor undefined ordiffuse) or to have tumor cells seeded into the tissue beyond the circumference of the
tumorous mass" this does not mean that an infiltrative tumor does not take up space or
does not compress the surrounding tissue as it grows, but an infiltrating neoplasm
makes it difficult to say where the tumor ends and the healthy tissue starts.
metastasis (spread to other locations in the body via lymph or blood).
=f the above malignant characteristics, some elements do not apply to primary
neoplasms of the brain*
'rimary brain tumors rarely metastasi$e to other organs" some forms of primary brain
tumors can metastasi$e but will not spread outside the intracranial cavity or the central
spinal canal. 3ue to the blood+brain barriercancerous cells of a primary neoplasm cannot
enter the bloodstream and get carried to another location in the body. (=ccasional isolated
http://en.wikipedia.org/wiki/Anaplasiahttp://en.wikipedia.org/wiki/Pleomorphism_(cytology)http://en.wikipedia.org/wiki/Cell_nucleihttp://en.wikipedia.org/wiki/Cell_nucleihttp://en.wikipedia.org/wiki/Cytoplasmhttp://en.wikipedia.org/wiki/Giant_cellshttp://en.wikipedia.org/wiki/Giant_cellshttp://en.wikipedia.org/wiki/Syncytiumhttp://en.wikipedia.org/wiki/Metastasishttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrierhttp://en.wikipedia.org/wiki/Anaplasiahttp://en.wikipedia.org/wiki/Pleomorphism_(cytology)http://en.wikipedia.org/wiki/Cell_nucleihttp://en.wikipedia.org/wiki/Cytoplasmhttp://en.wikipedia.org/wiki/Giant_cellshttp://en.wikipedia.org/wiki/Syncytiumhttp://en.wikipedia.org/wiki/Metastasishttp://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrier -
8/12/2019 Bahan Lapsus Brain Tumor
13/32
case reports suggest spread of certain brain tumors outside the central nervous system,
e.g. bone metastasis of glioblastoma multiforme.9I;)
'rimary brain tumors generally are invasive (i.e. they will e&pand spatially and intrude
into the space occupied by other brain tissue and compress those brain tissues), however
some of the more malignant primary brain tumors will infiltrate the surrounding tissue.
=f numerous grading systemsin use for the classification of tumor of the central
nervous system, the World !ealth =rgani$ation(W!=) grading systemis commonly
used for astrocytoma. Fstablished in :II in an effort to eliminate confusion regarding
diagnoses, the W!= system established a fourtiered histologic grading guideline for
astrocytomas that assigns a grade from : to ?, with : being the least aggressive and ?
being the most aggressive.
[edit]TreatmentWhen a brain tumor is diagnosed, a medical team will be formed to assess the
treatment options presented by the leading surgeon to the patient and his-her family.
8iven the location of primary solid neoplasms of the brain in most cases a donothing
option is usually not presented. Deurosurgeons take the time to observe the evolution of
the neoplasm before proposing a management plan to the patient and his-her relatives.
These various types of treatment are available depending on neoplasm type and
location and may be combined to give the best chances of survival*
surgery* complete or partial resection of the tumor with the ob4ective of removing as
many tumor cells as possible
radiotherapy* the most commonly used treatment for brain tumors" the tumor is irradiated
with beta, & rays or gamma rays.
chemotherapy* is a treatment option for cancer, however it is seldom used to treat brain
tumors as the blood and brain barrier prevents the drugs from reaching the cancerous cells.
/hemotherapy can be thought of as a poison that prevents the growth and division of all
cells in the body including cancerous cells. Thus the significant side effects associated and
e&perienced by patients undergoing chemotherapy.
A variety of e&perimental therapies are available through clinical trials9:;
http://en.wikipedia.org/wiki/Glioblastoma_multiformehttp://en.wikipedia.org/wiki/Glioblastoma_multiformehttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-9http://en.wikipedia.org/wiki/Grading_of_the_tumors_of_the_central_nervous_systemhttp://en.wikipedia.org/wiki/Grading_of_the_tumors_of_the_central_nervous_systemhttp://en.wikipedia.org/wiki/World_Health_Organizationhttp://en.wikipedia.org/wiki/Grading_of_the_tumors_of_the_central_nervous_system#WHO_gradinghttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=15http://en.wikipedia.org/wiki/Brain_tumor#cite_note-10http://en.wikipedia.org/wiki/Glioblastoma_multiformehttp://en.wikipedia.org/wiki/Brain_tumor#cite_note-9http://en.wikipedia.org/wiki/Grading_of_the_tumors_of_the_central_nervous_systemhttp://en.wikipedia.org/wiki/World_Health_Organizationhttp://en.wikipedia.org/wiki/Grading_of_the_tumors_of_the_central_nervous_system#WHO_gradinghttp://en.wikipedia.org/w/index.php?title=Brain_tumor&action=edit§ion=15http://en.wikipedia.org/wiki/Brain_tumor#cite_note-10 -
8/12/2019 Bahan Lapsus Brain Tumor
14/32
urvival rates in primary brain tumors depend on the type of tumor, age, functional
status of the patient, the e&tent of surgical tumor removal and other factors specific to
each case.9::;
[edit]Surgery
The primary and most desired course of action described in medical literature is surgical
removal (resection) via craniotomy. 6inimally invasive techni0ues are being studied but
are far from being common practice. The prime remediating ob4ective of surgery is to
remove as many tumor cells as possible, with complete removal being the best outcome
and cytoreduction(debulking) of the tumor otherwise. #n some cases access to the
tumor is impossible and impedes or prohibits surgery.
6any meningiomas, with the e&ception of some tumors located at the skull base, can be
successfully removed surgically. 6ostpituitary adenomascan be removed surgically,
often using a minimally invasive approach through thenasal cavityand skull base
(transnasal, transsphenoidal approach). 1arge pituitary adenomasre0uire
a craniotomy(opening of the skull) for their removal. >adiotherapy,
including stereotacticapproaches, is reserved for inoperable cases.
everal current research studies aim to improve the surgical removal of brain tumors by
labeling tumor cells with @aminolevulinic acidthat causes them to fluoresce.9:
-
8/12/2019 Bahan Lapsus Brain Tumor
15/32
for a total of : to treatments, depending on the type of tumor. This additional
treatment provides some patients with improved outcomes and longer survival rates.
>adiosurgery is a treatment method that uses computeri$ed calculations to focus
radiation at the site of the tumor while minimi$ing the radiation dose to the surrounding
brain. >adiosurgery may be an ad4unct to other treatments, or it may represent the
primary treatment techni0ue for some tumors.
>adiotherapy may be used following, or in some cases in place of, resection of the
tumor. 2orms of radiotherapy used for brain cancer includee&ternal beam radiation
therapy, brachytherapy, and in more difficult cases, stereotacticradiosurgery, such
as 8amma knife,/yberknifeor Dovalis T&radiosurgery.9:;
>adiotherapy is the most common treatment for secondary brain tumors. The amount of
radiotherapy depends on the si$e of the area of the brain affected by cancer./onventional e&ternal beam 7whole brain radiotherapy treatment7 (WB>T) or 7whole
brain irradiation7 may be suggested if there is a risk that other secondary tumors will
develop in the future.9:?;tereotactic radiotherapy is usually recommended in cases
involving fewer than three small secondary brain tumors.
#n ) and whole
brain radiation therapy (WB>T) for the treatment of metastatic brain tumors have more
than twice the risk of developing learning and memory problems than those treated with
> alone.9:@;9:E;
[edit]Chemotherapy
'atients undergoing chemotherapy are administered drugs designed to kill tumor cells.
Although chemotherapy may improve overall survival in patients with the most
malignant primary brain tumors, it does so in only about
-
8/12/2019 Bahan Lapsus Brain Tumor
16/32
how brain tumor patients are performing on current therapies. They also show a listing
of chemotherapy agents used to treat high grade glioma tumors.9:H;
[edit]!ther
A shuntis used not as a cure but to relieve symptoms by reducing hydrocephaluscaused by blockage of cerebrospinal fluid.9:C;
>esearchers are presently investigating a number of promising new treatments
including gene therapy, highly focused radiation therapy, immunotherapy and novel
chemotherapies. A variety of new treatments are being made available on an
investigational basis at centers speciali$ing in brain tumor therapies.
[edit]Prognosis
The prognosis of brain cancer varies based on the type of cancer. 6edulloblastoma hasa good prognosis with chemotherapy, radiotherapy, and surgical resectionwhile
glioblastoma multiforme has a median survival of only :< months even with
aggressivechemoradiotherapyand surgery. Brainstem gliomas have the poorest
prognosis of any form of brain cancer, with most patients dying within one year, even
with therapy that typically consists of radiation to the tumor along with corticosteroids.
!owever, one type of brainstem glioma, a focal 9:I;seems open to e&ceptional prognosis
and longterm survival has fre0uently been reported.
[edit]"lioblastoma multiforme
Main article:Glioblastoma multiforme
8lioblastoma multiforme is the deadliest and most common form of malignant brain
tumor. Fven when aggressive multimodality therapy consisting of radiotherapy,
chemotherapy, and surgical e&cision is used, median survival is only :
-
8/12/2019 Bahan Lapsus Brain Tumor
17/32
=ligodendroglioma is an incurable but slowly progressive malignant brain tumor. They
can be treated with surgical resection,chemotherapy, and-orradiotherapy. 2or
suspected lowgrade oligodendrogliomas in select patients, some neurooncologists opt
for a course of watchful waiting, with only symptomatic therapy. Tumors with the :p-:I0
codeletion have been found to be especially chemosensitive, and one source reports
oligodendrogliomas to be among the most chemosensitive of human solid
malignancies.9
-
8/12/2019 Bahan Lapsus Brain Tumor
18/32
Measur
es
Se
x
DA
SR
All
age
s
Und
er 1
1
4
5
9
10
14
15
19
20
24
25
29
30
34
35
39
40
44
45
49
50
54
55
59
60
64
65
69
70
74
75
79
80
8485+
Absolut
e
figures
M 2,13
1 7 34 40 31 37 33 48 61 87
10
0
116.
1
14
2 24226425823719312873
F 1,59
8 7 42 39 37 28 25 37 50 42 73 87 99 140 191 166 169 158 111 97
Rates
per
100,00
0
inabita
nts
M 7.7 8.5 2.1 2.
8
2.
7 2.0 2.1 1.9 2.8 3.7 4.6 5.1 6.6 9.3
15.
7
18.
6
24.
0
25.
8
26.
7
26.
6
21.
2
F 5.3 6.2 2.2 3.
6
2.
8 2.5 1.7 1.5 2.2 3.0 2.2 3.7 4.9 6.3 8.8
12.
9
14.
3
16.
2
17.
1
15.
1
12.
8
[edit]$nited States
#n the %nited tates in the year egistry of the %nited tates, 'rimary Brain
Tumors in the %nited tates, tatistical >eport,
-
8/12/2019 Bahan Lapsus Brain Tumor
19/32
[edit]'esicular stomatitis &irus
#n
-
8/12/2019 Bahan Lapsus Brain Tumor
20/32
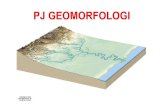
A brainstemgliomain fouryear old. 6>#sagittal,without contrast
#n the %, about
-
8/12/2019 Bahan Lapsus Brain Tumor
21/32
Brain tumors may originate from neural elements within the brain, or they may representspread of distant cancers. 'rimary brain tumors arise from /D tissue and account forroughly half of all cases of intracranial neoplasms. The remainder of brain neoplasmsare caused by metastatic lesions. #n adults, two thirds of primary brain tumors arise fromstructures above the tentorium (supratentorial), whereas in children, two thirds of brain
tumors arise from structures below the tentorium (infratentorial). 8liomas,metastases, meningiomas, pituitary adenomas, andacoustic neuromasaccount forI@ of all brain tumors. /lassification by tumor cell type is irrelevant to the emergencyphysician because emergent treatment is the same regardless of the tumor type.
Deoplasms, brain. /T images of several tumor types. lide courtesyof %6A /ontinuing Fducation =ffice.
6any review articles have been written on brain tumors, and this discussion at timesdraws from the consensus of these reviews. 9:,
-
8/12/2019 Bahan Lapsus Brain Tumor
22/32
Deoplasms, brain. /olloid cyst of the third ventricle with obstructive
hydrocephalus. #mage courtesy of 'eter 2errera, 63.
The cumulative effects of tumor invasion, edema, and hydrocephalus may elevate theintracranial pressure (#/') and impair cerebral perfusion. #ntracranial compartmentalrise in #/' may provoke shifting or herniation of tissue under the fal& cerebri, throughthe tentorium cerebelli, or through the foramen magnum.
lowgrowing tumors, particularly tumors e&panding in the socalled silent areas of thebrain, such as the frontal lobe, may be associated with a more insidious clinical course.These tumors tend to be larger at detection.
6ost primary brain tumors do not metastasi$e, but if they do metastasi$e, intracranialspread generally precedes distant dissemination.
6etastatic brain tumors from non/D primary tumors may be the first sign ofmalignancy, or they may herald a relapse. Donetheless, the signs and symptoms ofbrain metastases simulate those of primary brain tumors.
1eptomeningeal infiltration may present with dysfunction of multiple cranial nerves.
#pidemiology
)re*uency
United States
Fstimates of the annual incidence rate of primary brain tumors range from H:I.: casesper :, population. 6etastatic tumors to the brain are more common with morethan
-
8/12/2019 Bahan Lapsus Brain Tumor
23/32
Mortality+Morbidity
#n the %nited tates in :III, primary cancers of the central nervous system were the
cause of death in appro&imately :,: people. Brain tumors are the second most common cancer in children, comprising :@
-
8/12/2019 Bahan Lapsus Brain Tumor
24/32
interval. !eadache was the number one symptom e&perienced in more than half ofpatients.9:;
Although headache is the symptom customarily associated with an intracranial
neoplasm, it often is a late complaint. %sually, headache is not an isolated finding.o !eadache is the worst symptom in only one half of patients.
o 6ost headaches in patients with brain tumors are nonspecific and
resemble tensiontype headaches.9C, ::, :
-
8/12/2019 Bahan Lapsus Brain Tumor
25/32
o Any middleaged or elderly patients presenting with a first sei$ure should
have /D tumor high in the differential diagnosis.o 'atients with a brain tumor may present with acute neurologic changes
mimicking those associated with stroke.
Physical
Do physical finding or pattern of findings unmistakably identifies a patient with a /Dneoplasm.
Based on their location, intracranial tumors may produce a focal or generali$ed
deficit, but signs may be lacking (especially if the tumor is confined to the frontal lobe)or even falsely locali$ing.
'apilledema, which is more prevalent with pediatric brain tumors, reflects an
increase in #/' of several days or longer. 'apilledema usually does not cause visualloss. Dot all patients with /D tumors develop papilledema.
3iplopia may result from displacement or compression of the si&th cranial nerve
at the base of the brain. #mpaired upward ga$e, called 'arinaud syndrome, may occur with pineal tumors. Tumors of the occipital lobe specifically may produce homonymous hemianopia
or partial visual field deficits. Deoplasms, brain. =ccipital lobeglioblastoma with surrounding edema.
Anosmia may occur with frontal lobe tumors.
Brainstem and cerebellar tumors induce cranial nerve palsies, ata&ia,
incoordination, nystagmus, pyramidal signs, and sensory deficits on one or both sidesof the body.
o Three cranial nerves run through the cerebellopontine angle* facial,
cochlear, and vestibular. 6asses in these regions may impair the functions of thesenerves.
o Acoustic neuromas most commonly originate from the vestibular nerve
(part of cranial nerve ###).Causes
Although few factors are une0uivocally associated with an increased risk of braincancer, some are conse0uential.
6ost /D neoplasms are thought to arise from individual cell mutations.
http://refimgshow%283%29/ -
8/12/2019 Bahan Lapsus Brain Tumor
26/32
A prior history of irradiation to the head for reasons other than treatment of the
present tumor may increase the chance of primary brain tumor. A few inherited diseases, such as neurofibromatosis, tuberous sclerosis, multiple
endocrine neoplasia (type :), and retinoblastoma, increase the predilection to develop/D tumors.
The most common tumors originating from the cerebellopontine angle areacoustic neuroma and meningioma.
'rimary /D lymphoma is a relatively fre0uent occurrence in !# patients.
6etastatic tumors reach the brain via hematogenous dissemination through the
arterial system.o 1ung cancer is by far the most common solid tumor disseminating to the
brain, followed by breast, melanoma, and colon cancer.o 1ess common sources of metastasis are malignant melanoma,testicular
cancer, and renal cell cancer.o 'rostate, uterine, and ovarian cancersare unlikely sources of brain
metastasis.
Differential Diagnoses Fncephalitis
Fpidural !ematoma
troke, !emorrhagic
troke, #schemic
ubdural !ematoma
.aboratory Studies
'atients with cancer are predisposed to medical complications, including
bleeding disturbances (hyperviscosity), metabolic disorders (hypercalcemia), andproduction of e&cessive hormones (syndrome of inappropriate antidiuretic hormone
secretion). With clinical suspicion of cancer, obtain routine laboratory studies on admission,
including a /B/, coagulation studies, and analysis of electrolytes and comprehensivemetabolic panel.
Imaging Studies
=btain neuroimaging studies in patients with symptoms suggestive of anintracranial neoplasm (eg, acute mental status changes" newonset sei$ures" focal,motor, or sensory deficits, including gait disturbance" suspicious headache" signs ofelevated #/', such as papilledema).
Although some tumors e&hibit a characteristic appearance, do not make an
une0uivocal diagnosis based solely on radiologic findings. 8enerally, /T is the imaging modality of choice for the F3 physician.
#ntravenous contrast material assists in tumor identification. 6ost tumorsdemonstrate enhancement with contrast material administration.
Tumors may appear hypodense, isodense, or hyperdense, or they may
have mi&ed density. 6etastases to the brain tend to be multiple, but certain tumors, such as
renal cell carcinomas, tend to be solitary metastatic brain lesions.
http://emedicine.medscape.com/article/1947145-overviewhttp://emedicine.medscape.com/article/277496-overviewhttp://emedicine.medscape.com/article/279007-overviewhttp://emedicine.medscape.com/article/279007-overviewhttp://emedicine.medscape.com/article/281340-overviewhttp://emedicine.medscape.com/article/281340-overviewhttp://emedicine.medscape.com/article/458011-overviewhttp://emedicine.medscape.com/article/258148-overviewhttp://emedicine.medscape.com/article/255771-overviewhttp://emedicine.medscape.com/article/791896-overviewhttp://emedicine.medscape.com/article/824029-overviewhttp://emedicine.medscape.com/article/828005-overviewhttp://emedicine.medscape.com/article/780258-overviewhttp://emedicine.medscape.com/article/766373-overviewhttp://emedicine.medscape.com/article/246650-overviewhttp://emedicine.medscape.com/article/246650-overviewhttp://emedicine.medscape.com/article/1947145-overviewhttp://emedicine.medscape.com/article/277496-overviewhttp://emedicine.medscape.com/article/279007-overviewhttp://emedicine.medscape.com/article/279007-overviewhttp://emedicine.medscape.com/article/281340-overviewhttp://emedicine.medscape.com/article/458011-overviewhttp://emedicine.medscape.com/article/258148-overviewhttp://emedicine.medscape.com/article/255771-overviewhttp://emedicine.medscape.com/article/791896-overviewhttp://emedicine.medscape.com/article/824029-overviewhttp://emedicine.medscape.com/article/828005-overviewhttp://emedicine.medscape.com/article/780258-overviewhttp://emedicine.medscape.com/article/766373-overviewhttp://emedicine.medscape.com/article/246650-overviewhttp://emedicine.medscape.com/article/246650-overview -
8/12/2019 Bahan Lapsus Brain Tumor
27/32
With increasing availability, 6>#s may supplant /Ts as the imaging procedures
of choice. An 6># is most helpful for identifying tumors in the posterior fossa
(including acoustic neuromas), hemorrhagic lesions. #t is useful in patients with anallergy to iodinated contrast material or renal insufficiency.
3rawbacks to 6># include incompatibility with certain medical e0uipment,longer imaging times (increased risk of motion artifact), and poor visuali$ation of thesubarachnoid space.
Deither /T nor 6># can be used to differentiate tumor recurrence from
radionecrosis. =n plain skull radiographs, large pituitary adenomas are associated with a large
sella turcica.
Procedures
1umbar puncture is not indicated in the F3 in the patient with suspected /Dneoplasms.
Prehospital Care'rehospital care is supportive and directed to the presenting symptom comple&. 2ore&le, treat sei$ures in the usual manner. Airway disturbance, breathing difficulty,signs of pronounced elevation in #/', and notable impairment of consciousness maynecessitate definitive airway control with endotracheal intubation and, possibly,hyperventilation.
#mergency Department Care
F3 treatment of the patient with an intracerebral neoplasm depends on both the natureof the tumor and the general condition of the patient. 3ecisions regarding surgicalresection, initiation of radiation treatment, and chemotherapy are beyond the scope ofpractice of the F3 physician.
/orticosteroids may dramatically reduce signs and symptoms related to cerebral
edema. Affected patients may e&perience relief within the first few hours of steroidtherapy.
o 3e&amethasone is the agent of choice because of its minimal salt
retaining properties. >ecommended doses generally range from ?
-
8/12/2019 Bahan Lapsus Brain Tumor
28/32
3iscuss the use of mannitol with the appropriate consultant. Although mannitol
may reduce transiently lower #/', concern about rebound increases in #/' makes itsuse problematic.
Consultations
1ocal practice patterns govern re0uests for consultations.
8enerally, care of patients with a brain tumor is multidisciplinary, re0uiring
assistance from a neurosurgeon, an oncologist, a radiologist, and an e&pert inradiation therapy.
6anagement varies greatly depending on tumor location, tissue type, and
comorbid conditions. urgical treatment options may include tumor removal or debulking, installation
of a ventricular shunt, and placement of radioactive implants.
Medication Summary
'ractice parameters from the American Academy of Deurology discourage prophylactic
use of anticonvulsants for sei$ures in patients with newly diagnosed brain tumors andsuggest that it is appropriate to taper and discontinue anticonvulsant usepostoperatively in patients without sei$ures.9:;Anticonvulsant use may be reserved forpatients with clinical sei$ures, but some physicians prescribe prophylacticanticonvulsants in patients with cortical tumors.
Corticosteroids
Class Summary
teroids are thought to stabili$e cell membranes and diminish the vasogenic edemaassociated with tumors.
iew full drug information
De,amethasone /Decadron0
%sed in treatment of vasogenic cerebral edema" improves endothelial integrity.
-yperosmolar agents
Class Summary
These agents may reduce #/' and cerebral edema by creating an osmotic gradientacross an intact bloodbrain barrier. As water diffuses from the brain into theintravascular compartment, #/' decreases.
iew full drug information
Mannitol /!smitrol0
http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741http://reference.medscape.com/drug/osmitrol-mannitol-343061http://reference.medscape.com/drug/osmitrol-mannitol-343061http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741http://reference.medscape.com/drug/osmitrol-mannitol-343061http://reference.medscape.com/drug/osmitrol-mannitol-343061 -
8/12/2019 Bahan Lapsus Brain Tumor
29/32
6ay reduce subarachnoid space pressure by creating osmotic gradient betweencerebrospinal fluid in arachnoid space and plasma. Dot for longterm use.
)urther Inpatient Care
2urther inpatient care is comple& and may involve multiple consultants,
depending on the tumor type and overall prognosis. 3efinitive diagnosis re0uires tissue biopsy performed by a 0ualified
neurosurgeon. Additional neurosurgical options include resection or debulking and placement of
a ventricular shunt with obstructive hydrocephalus. The admitting physician should coordinate oncologic or radiation oncology
consultations.
)urther !utpatient Care
The patient7s primary physician best manages coordination of consultants, butthe responsible neurosurgeon should direct the treatment of specific postoperative
complications or care. A common problem confronting the F3 physician is a patient with a known brain
neoplasm complaining of a headache or worsening other symptoms. This scenarioalways raises the possibility of tumor recurrence or worsening cerebral edema. =btain a/T scan or 6># to rule out lifethreatening events, such as hemorrhage or herniation.
>adiation therapy for gliomas usually is performed on an outpatient basis.
Inpatient 1 !utpatient Medications
teroids or anticonvulsants may be used.
'rovide medications for patient comfort and pain control.
Transfer
Dew occurrence of /D tumor may re0uire transfer to a facility with appropriateneurosurgical staff.
peak directly to the consultant prior to transfer to address initiation of steroid or
anticonvulsant treatment.
Complications
Acute symptoms in a patient with a brain tumor, particularly when signs andsymptoms simulate the presentation of a cerebrovascular accident, suggest thepossibility of acute hemorrhage into a tumor. Brain neoplasms predisposed tohemorrhage include lung cancer, melanoma, and choriocarcinoma.
1esions near the third ventricle can cause paro&ysmal symptoms of headache,
syncope, or mental status change. Additionally, vomiting, ata&ia, memory changes,visual disturbances, or personality changes may occur.
Fpisodic increases in #/' secondary to pressure arising from blockage of
cerebrospinal fluid outflow cause transient symptoms. udden death is a reported complication from obstruction of outflow
drainage from the third ventricle.
-
8/12/2019 Bahan Lapsus Brain Tumor
30/32
udden increases in #/' may lead to lifethreatening brain herniation, which
shifts the brain parenchyma in the direction of least resistance* caudally through theforamen magnum (posterior fossa tumors) or transtentorial apertures.
ome pituitary tumors are hormonally active and capable of producing
acromegaly or galactorrhea. 'ituitary apople&y, an unusual complication arising from
pituitary adenomas, describes hemorrhage into the tumor, leading to headache,deterioration of vision, oculomotor palsies, and shock secondary to acute adrenalinsufficiency.
Although radiation therapy rarely causes acute to&icity with modern dosing
schedules and concomitant use of steroids, subacute or chronic effects may occur. ubacute encephalopathy occurs E:E weeks after radiation therapy and
is characteri$ed by somnolence and headaches. /hronic effects of prolonged radiation treatment tend to be more serious
and range from impairment of intellectual capacity to complete incapacity.
Prognosis
Tumor resectability, tumor location, age of the patient, and tumor histology are
the primary determinants of survival. Without radiation therapy, the mean life e&pectancy of a patient with brain
metastases is : month. >adiation therapy may e&tend survival to ?E months. 'atients with sei$ures secondary to a brain tumor generally e&perience obvious
neurologic deterioration over a Emonth course. 6ost patients with brain metastases die from progression of their primary
malignancy rather than from brain damage.
Patient #ducation
2or e&cellent patient education resources, visit e6edicine!ealth7s /ancer
/enter. Also, see e6edicine!ealth7s patient education article Brain /ancer.
Brain Cancer Staging Author* Keffrey D Bruce, 63" /hief Fditor* Kules F !arris, 63
ttp!""e(e%i*ine.(e%s*ape.*o("arti*le"2006770"p$.17!33"14 )anuari 2013
Staging of Brain Cancers
The histologic classification employed by the World !ealth =rgani$ation (W!=) forcentral nervous system (/D) tumors, shown below, makes use of ? grades. 9:,
-
8/12/2019 Bahan Lapsus Brain Tumor
31/32
1esions that are generally infiltrating and low in mitotic activity but recur" some tumor
types tend to progress to higher grades of malignancy 3iffuse astrocytoma, oligodendroglioma, oligoastrocytoma
Grade III:
1esions with histologic evidence of malignancy, generally in the form of mitotic activity,
clearly e&pressed infiltrative capabilities, and anaplasia Anaplastic astrocytoma, anaplastic oligoastrocytoma, anaplastic oligoastrocytoma
Grade IV:
1esions that are mitotically active, necrosisprone, and generally associated with a rapid
preoperative and postoperative evolution of disease 8lioblastoma
Brain Cancer Treatment Protocols Author* Keffrey D Bruce, 63" /hief Fditor* Kules F !arris, 63
ttp!""e(e%i*ine.(e%s*ape.*o("arti*le"2005182"p$.17!36"14anuari2013Treatment Protocols
urgical resection is the primary treatment for all tumor grades. The surgical goal isgross total resection, though less aggressive resection is employed for tumor involvingelo0uent brain.
There is significant divergence of opinion, particularly for grade ## lesions, especially forgrade ## astrocytoma. >adiation and chemotherapy dosages vary considerably amonginstitutions. Those below represent successful regimens from recent clinical trials.3e&amethasone and sei$ure treatment or prophyla&is is commonly appropriate. 9:,
-
8/12/2019 Bahan Lapsus Brain Tumor
32/32
'ostoperative radiation therapy is often employed for unresectable, residual, or recurrent
tumor /hemotherapy is often used for lowgrade oligodendrogliomas, particularly with :p:I0
deletion, which is a marker for tumor susceptibility to chemotherapy9:,