Anesthesie voor Abdominale Heelkunde - UZ Leuven · 2016-09-15 · Anesthesie voor Abdominale...
89
Anesthesie voor Abdominale Heelkunde M. Verhaegen Co-assistenten 08 - 09 - 2016
Transcript of Anesthesie voor Abdominale Heelkunde - UZ Leuven · 2016-09-15 · Anesthesie voor Abdominale...
Anesthesie voor Abdominale Heelkunde
M. Verhaegen
Co-assistenten 08 - 09 - 2016
Anesthesie voor Abdominale Heelkunde
1. Algemene aandachtspunten
– Beknopt overzicht aandachtspunten pre-, per- en postoperatief
2. Rapid sequence inductie and intubatie
3. Laparoscopie met een CO2-pneumoperitoneum
– Insufflatie gas
– Pathofysiologische effecten
– Verwikkelingen
– Contra-indicaties
– Anesthesie-specifieke aandachtspunten
1. ALGEMENE AANDACHTSPUNTEN
Anesthesie voor Abdominale Heelkunde
Abdominal Surgery: Preoperative Attention Points
• Routine preoperative evaluation:
• “Pre-operatieve screening en medicatie” (les E. Vandermeulen)
• Specific attention points in patients planned for abdominal surgery
– Weight loss, malnutrition, anemia
• E.g. Hypoalbuminemia
– Hepatobiliary pathology: (severe) hepatic dysfunction is possible
– Assessment of intravascular volume status
• “Vochtbeleid: krystalloïden – colloïden” (les M. Verhaegen)
– Diagnosis of electrolyte or acid-base disturbances
• “Zuur-base stoornissen” (les M. Verhaegen)
– Assess risk of pulmonary aspiration of gastric contents
• Discuss anesthetic technique: general anesthesia +/- epidural anesthesia/analgesia
– Surgical procedure
– Contraindication for a specific technique
– Patient preference / objection
Abdominal Surgery: Intraoperative Attention Points
• Monitoring
– Routine monitoring
– Invasive monitoring depends on
• Surgical procedure
• Co-morbidity
• Temperature: take measures to prevent hypothermia as soon as the patient enters the operating room
– Warm room at induction
– Intravenous fluid warmer (install before induction of anesthesia!)
– Hot air warming device or warming mattress
– Cover the patient as much as possible
• Antibiotic prophylaxis
– Before incision
– Repeat dose
– UZ Leuven guidelines (“Antibioticagids”)
Abdominal Surgery: Intraoperative Attention Points
• Muscle relaxation and neuromuscular monitoring
– Intraoperatively
– Quantitative neuromuscular monitoring is absolutely necessary before emergence from anesthesia
and extubation
• TOF ≥ 2 before reversal with neostigmine should be attempted
• TOF ratio > 0.9 at adductor pollicis muscle::
• Fluid management
• “Vochtbeleid: krystalloïden – colloïden” (les M. Verhaegen)
• Prevention of postoperative nausea and vomiting
• Analgesia resulting in painfree arrival in the PACU
Abdominal Surgery: Postoperative Attention Points
• Postoperative fluid management
• Postoperative analgesia
• Thrombosis prophylaxis
• Prevention of stress ulcers
• Postoperative nausea and vomiting
• Postoperative continuation of preoperative medication
2. RAPID SEQUENCE INDUCTIE EN INTUBATIE
Anesthesie voor Abdominale Heelkunde
Risk Factors for Pulmonary Aspiration of Gastric Contents
• Emergent surgery
– Nil per os (npo) < 6 hrs
• Clear liquids < 2 hrs
• Breast milk < 4 hrs
– Acute trauma immediately after eating (delayed gastric emptying), even if surgery is scheduled after 6 hrs npo
• Patients at risk for significant gastric contents or increased intragastric pressure
– Gastric outlet obstruction
– Slow / delayed gastric emptying (e.g. diabetes mellitus, medication)
– Bowel obstruction
– Paralytic ileus
– Pregnancy
– Morbid obesity
– Excessive ascites
• Severe gastro-esophageal reflux disease
Determine if a rapid sequence intubation (RSI) is indicated
“Seven P’s” of RSI in Adults
1. Preparation
2. Preoxygenation
3. Pretreatment
4. Paralysis following induction
5. Protection and positioning
6. Placement with proof
7. Postintubation management
1. Preparation (1)
• Exclude contra-indications to RSI Consider awake fiberoptic intubation
– Anticipated difficult intubation
– Allergy to rapid onset muscle relaxants
• Check and prepare equipment
– Endotracheal tube
• Appropriate size
• Cuff free of leaks (tested)
– Stylet (+/- placed in the tube)
– Laryngoscope
• Tested
• Different blades should be readily available
– Suction device, checked and ready
– Oral airway
• If mask ventilation is unexpectedly needed
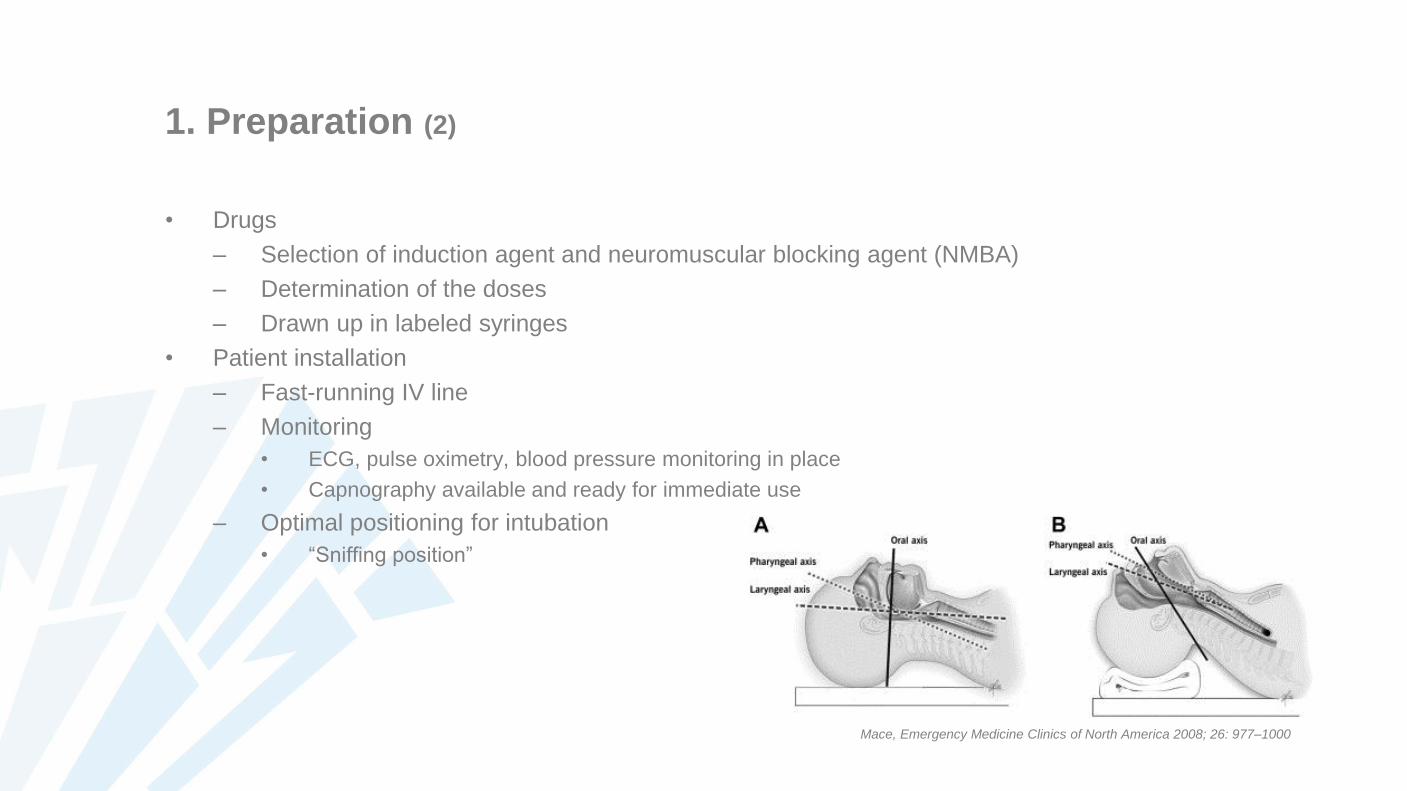
1. Preparation (2)
• Drugs
– Selection of induction agent and neuromuscular blocking agent (NMBA)
– Determination of the doses
– Drawn up in labeled syringes
• Patient installation
– Fast-running IV line
– Monitoring
• ECG, pulse oximetry, blood pressure monitoring in place
• Capnography available and ready for immediate use
– Optimal positioning for intubation
• “Sniffing position”
Mace, Emergency Medicine Clinics of North America 2008; 26: 977–1000
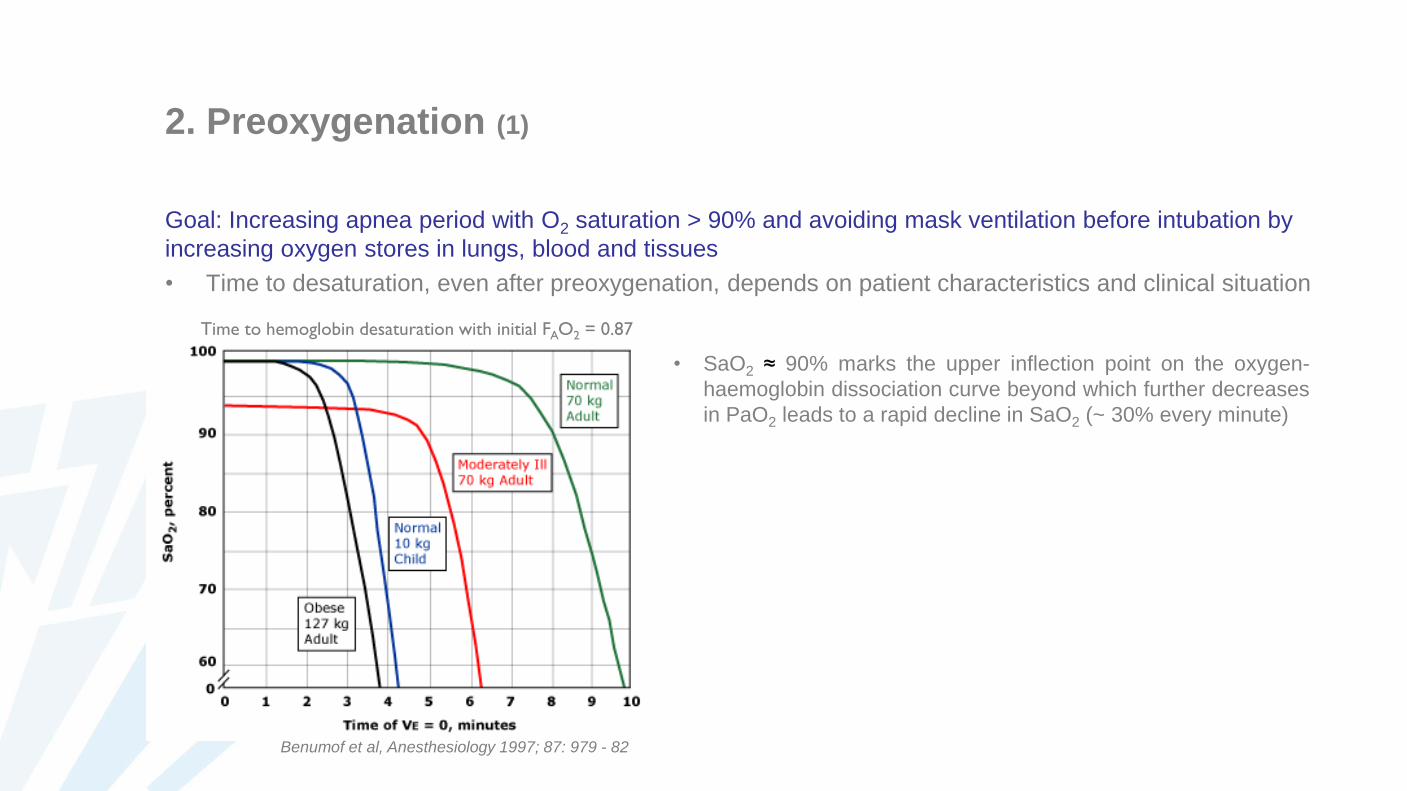
2. Preoxygenation (1)
Goal: Increasing apnea period with O2 saturation > 90% and avoiding mask ventilation before intubation by
increasing oxygen stores in lungs, blood and tissues
• Time to desaturation, even after preoxygenation, depends on patient characteristics and clinical situation
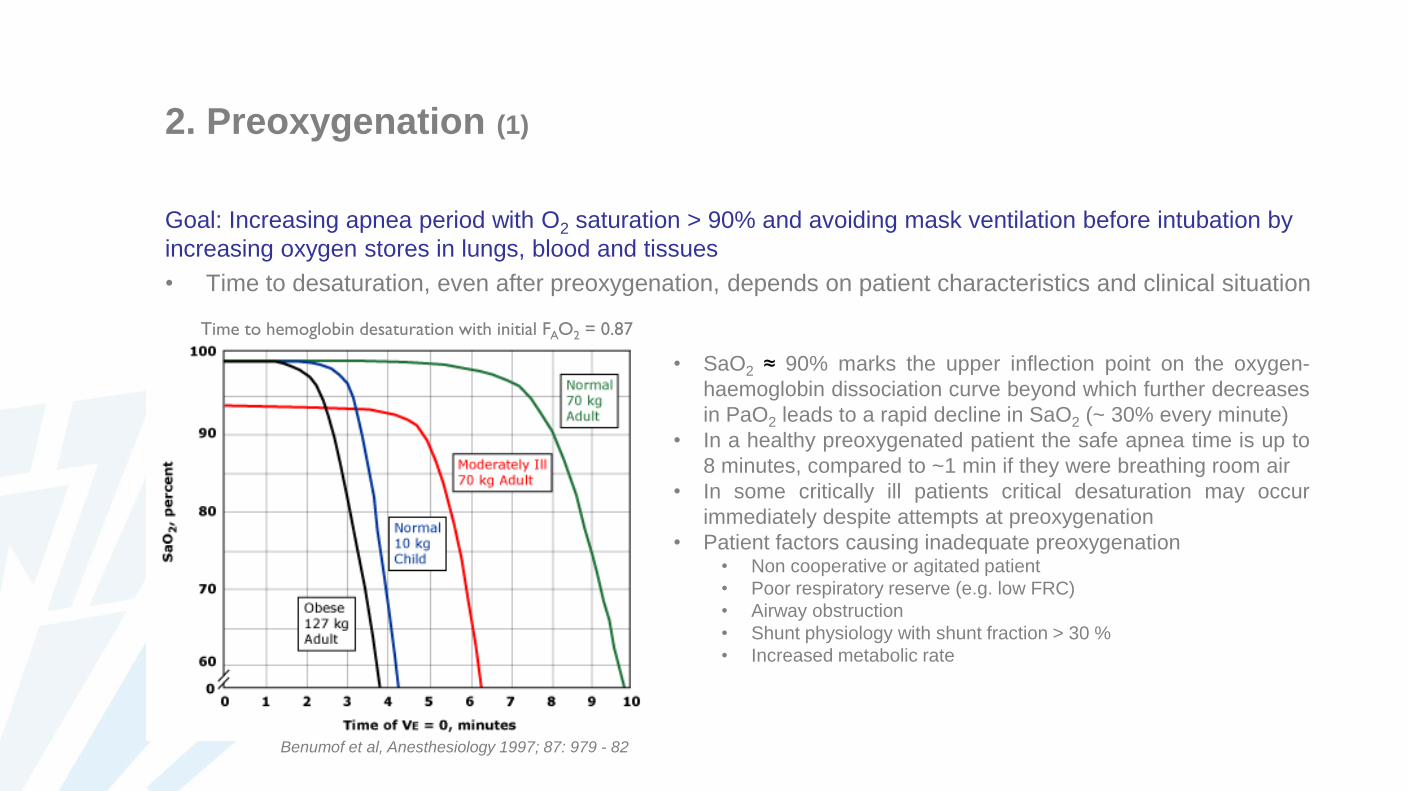
Benumof et al, Anesthesiology 1997; 87: 979 - 82
Time to hemoglobin desaturation with initial FAO2 = 0.87
• SaO2 ≈ 90% marks the upper inflection point on the oxygen-
haemoglobin dissociation curve beyond which further decreases
in PaO2 leads to a rapid decline in SaO2 (~ 30% every minute)
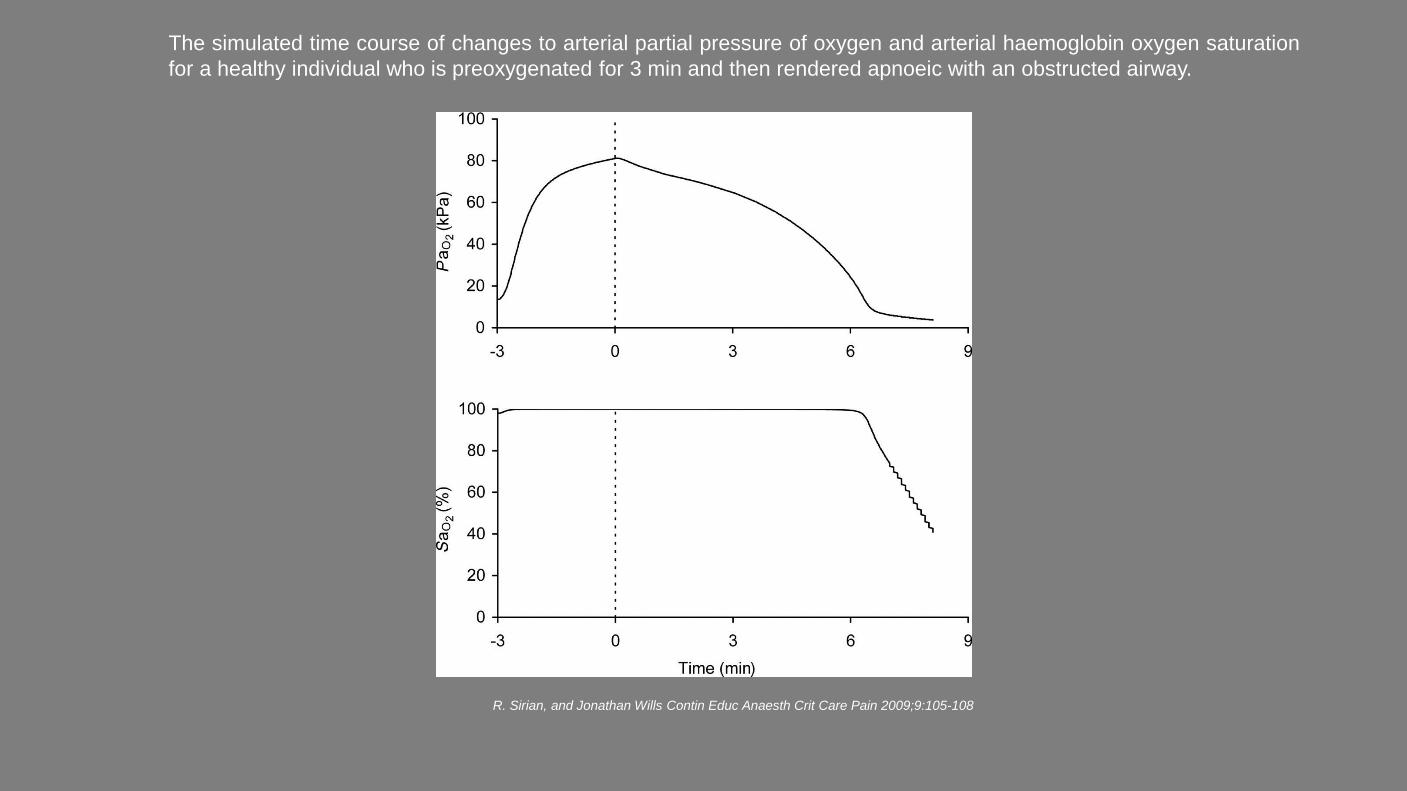
The simulated time course of changes to arterial partial pressure of oxygen and arterial haemoglobin oxygen saturation
for a healthy individual who is preoxygenated for 3 min and then rendered apnoeic with an obstructed airway.
R. Sirian, and Jonathan Wills Contin Educ Anaesth Crit Care Pain 2009;9:105-108
2. Preoxygenation (1)
Goal: Increasing apnea period with O2 saturation > 90% and avoiding mask ventilation before intubation by
increasing oxygen stores in lungs, blood and tissues
• Time to desaturation, even after preoxygenation, depends on patient characteristics and clinical situation
Benumof et al, Anesthesiology 1997; 87: 979 - 82
Time to hemoglobin desaturation with initial FAO2 = 0.87
• SaO2 ≈ 90% marks the upper inflection point on the oxygen-
haemoglobin dissociation curve beyond which further decreases
in PaO2 leads to a rapid decline in SaO2 (~ 30% every minute)
• In a healthy preoxygenated patient the safe apnea time is up to
8 minutes, compared to ~1 min if they were breathing room air
• In some critically ill patients critical desaturation may occur
immediately despite attempts at preoxygenation
• Patient factors causing inadequate preoxygenation• Non cooperative or agitated patient
• Poor respiratory reserve (e.g. low FRC)
• Airway obstruction
• Shunt physiology with shunt fraction > 30 %
• Increased metabolic rate
2. Preoxygenation (2)
Goal: Increasing apnea period with O2 saturation > 90% and avoiding mask ventilation before intubation by
increasing oxygen stores in lungs, blood and tissues
• Technique of choice: 100 % oxygen by tight-fitting face mask during 3 - 5 minutes
• Alternative technique: 8 vital capacity breaths (maximal breaths) during 100 % oxygen administration
Denitrogenation: replacing nitrogen with oxygen in the lungs (in the FRC)
– The lungs serve as a large O2 reservoir during apnea
– When breathing room air (79% nitrogen) ~450 mL of O2 is present in the lungs of an average healthy adult
– When a patient breathes 100% O2, this washes out the nitrogen, increasing the O2 in the lungs to ~3,000 mL
Increasing oxyhemoglobin saturation
(Oxygenation of plasma is not relevant: low solubility of O2 in blood)
3. Pretreatment
Goal: prevention of potentially adverse consequences of the physiologic responses to RSI
Drugs used for pretreatment vary with clinical circumstances
• Opioid
– Fentanyl, sufentanil
– To blunt increases in heart rate and blood pressure during laryngoscopy and intubation
• Lidocaine
– 1.5 mg/kg iv 2 - 3 min before intubation
– Suppression of cough reflex and attenuation of increased airway resistance following intubation?
– Attenuation of ICP rise upon intubation in patients at risk of adverse effects of an increase in ICP?
4. Paralysis following Induction (1)
Goal: almost simultaneous, rapid induction and paralysis
• Selection of appropriate agents
– Precalculated dosage, adequate to provide prompt loss of consciousness and muscle relaxation
– Problem: hemodynamically unstable patients
• Intubation 45 - 60 sec after the administration of the NMBA
1. Induction: Rapidly acting intravenous induction agent
– Propofol (1.5 – 2.5 mg/kg)
• Advantage: bronchodilation
• Disadvantage: hypotension (reduction of cerebral perfusion pressure)
– Etomidate (0.3 mg/kg)
• Advantage: hemodynamic stability
• Disadvantage: suppression of adrenal cortisol production
4. Paralysis following Induction (2)
2. Paralysis: Rapidly acting NMBA immediately following induction agent
– Succinylcholine
• Depolarizing NMBA
• Dosage: 1 – 1.5 mg/kg
– Rapid onset (45 - 60 sec), short half-life (6 - 10 min)
• Contraindications
– Significant (acute) hyperkalemia (ECG changes)
– Risk of malignant hyperthermia
» Personal or family history
» Specific diseases
– Rhabdomyolysis
– Acetylcholine receptor upregulation
» Denervating diseases
» Myopathies
» Prolonged total body immobilization
» Extensive burn injuries ≥ 72 hrs old
» Crush injuries ≥ 72 hrs old
4. Paralysis following Induction (3)
2. Paralysis: Rapidly acting NMBA immediately following induction agent
– Rocuronium
• Non-depolarizing NMBA
• RSI dosage: 0.9 – 1.3 mg/kg
– Rapid onset (45 - 60 sec)
• Longer duration of action than succinylcholine
– Duration of action of approximately 60 min after 1 mg/kg (may be much longer in older patients)
– Reversal is possible
» Neostigmine
• Only after sufficient spontaneous reversal (at least 2 and preferably 3 responses with TOF monitoring)
• No use in acute situations
» Suggamadex
» 16 mg/kg immediately after administration of RSI dose of rocuronium (unexpected cannot intubate,
cannot ventilate situation)
» Ac
5. Protection and Positioning
Goal: Protection of the airway against aspiration of gastric contents prior to intubation
• Avoid mask ventilation
– Maximal preoxygenation
– O2-saturation < 90 % gentle mask ventilation (with cricoid pressure?)
• Cricoid pressure (Sellick’s maneuver) during induction?
– Goal: Prevention of passive regurgitation by occlusion of the esophagus
– Discussion about effectiveness and safety
Sellick’s Maneuver (Cricoid Pressure) (1)
• Effectiveness has been questioned
– Lateral displacement of esophagus, instead of occlusion (MRI)
• But: occlusion of hypopharynx is relevant
– Decreased lower esophageal sphincter tone? (clinical study)
• Potentially increased risk of regurgitation
• Risks
– May worsen visualization
– Laryngeal obstruction with difficulty to pass the endotracheal tube
– Trauma
• Laryngeal trauma
• Esophageal rupture
– Displacement of unstable cervical spine
Currently there is insufficient evidence to support or to abandon the use of cricoid pressure during RSI
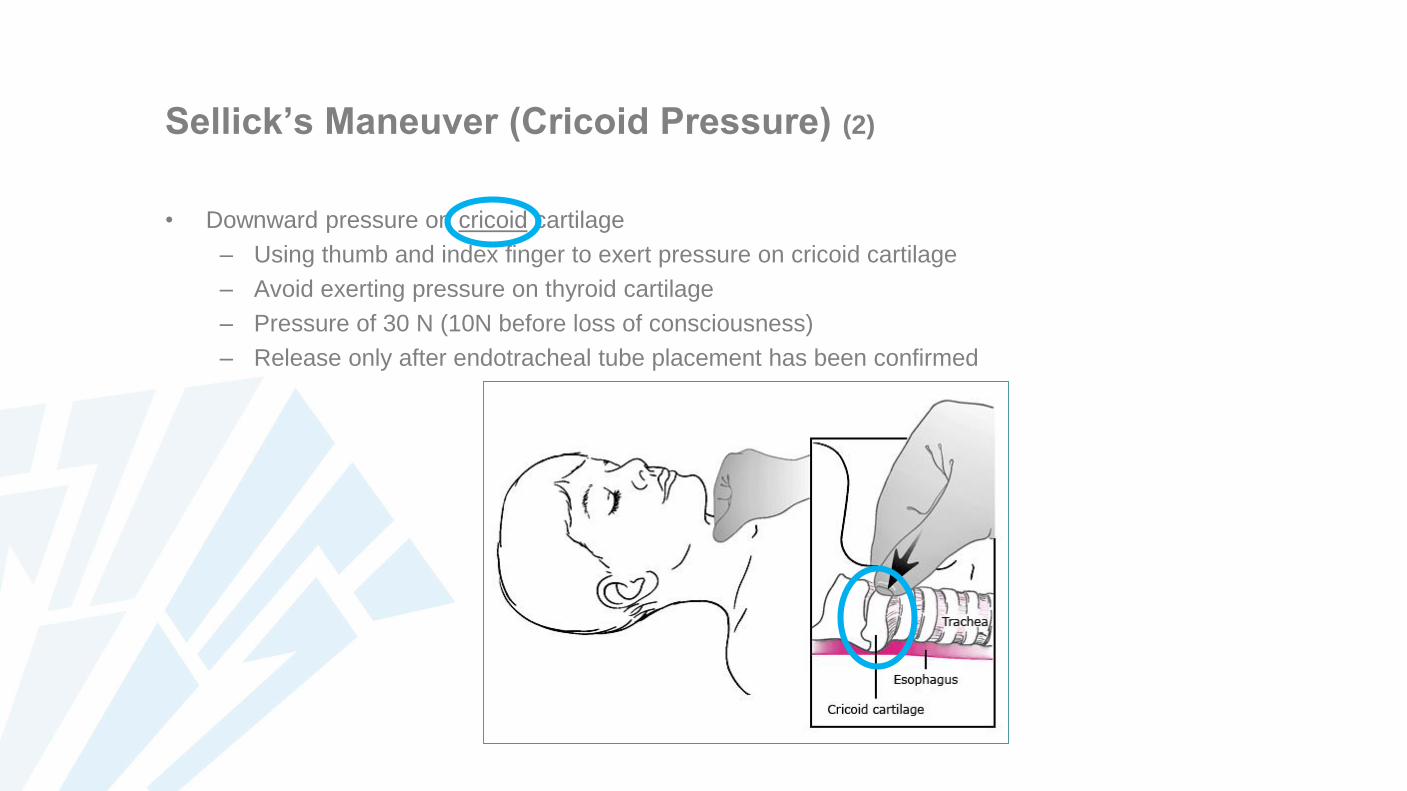
Sellick’s Maneuver (Cricoid Pressure) (2)
• Downward pressure on cricoid cartilage
– Using thumb and index finger to exert pressure on cricoid cartilage
– Avoid exerting pressure on thyroid cartilage
– Pressure of 30 N (10N before loss of consciousness)
– Release only after endotracheal tube placement has been confirmed
6. Placement with Proof
• Laryngoscopy after sufficient muscle relaxation has been achieved (45 – 60 s after NMBA administration)
• Placement of endotracheal tube (+/- stylet)
• Confirmation of endotracheal tube placement
– End-tidal CO2-measurement
– Auscultation over both sides of the chest and the stomach
– (Visualization of the endotracheal tube between the vocal cords)
– (Misting of the tube with ventilation)
• Check the depth of the tube
– Auscultation is equal over both lungs
7. Postintubation Management
• Secure the properly placed endotracheal tube
• Start mechanical ventilation
3. LAPAROSCOPIE MET CO2-PNEUMOPERITONEUM
Anesthesie voor Abdominale Heelkunde
Laparoscopic Surgery with CO2-Pneumoperitoneum: Topics
• Insufflation gas
• Pathophysiology
• Complications
• Contraindications
• Anesthesia
Laparoscopic Procedures for Gastrointesinal Surgery
• Diagnostic surgery
• Cholecystectomy
• Nissen fundiplication
• Bowel surgery
• Gastrectomy
• Bariatric surgery
• Pyloromyotomy
• Pancreatic surgery (Whipple)
• Partial hepatectomy
• Splenectomy
• Lymphadenectomy
• Inguinal hernia
• Appendectomy
• …
Laparoscopic Surgery: Potential Benefits
• Less tissue trauma
• Reduced surgical stress response
• Pulmonary function less impaired postoperatively
• Less postoperative ileus
• Reduced postoperative pain
• Faster postoperative recovery and ambulation
• Shorter hospital stay
• Better cosmetic results
• High patient satisfaction
• Cost savings
Mainly postoperative advantages
Every benefit has not been demonstrated for every procedure
Laparoscopic Surgery: Technical Aspects
• Creation of working space
– Pneumoperitoneum
– Gasless lifting system
– Combination of both techniques
• Gravity as a retractor extreme positioning
– Upper abdominal: reverse Trendelenburg positioning
– Lower abdominal: Trendelenburg positioning
• Robot-assisted laparoscopic surgery
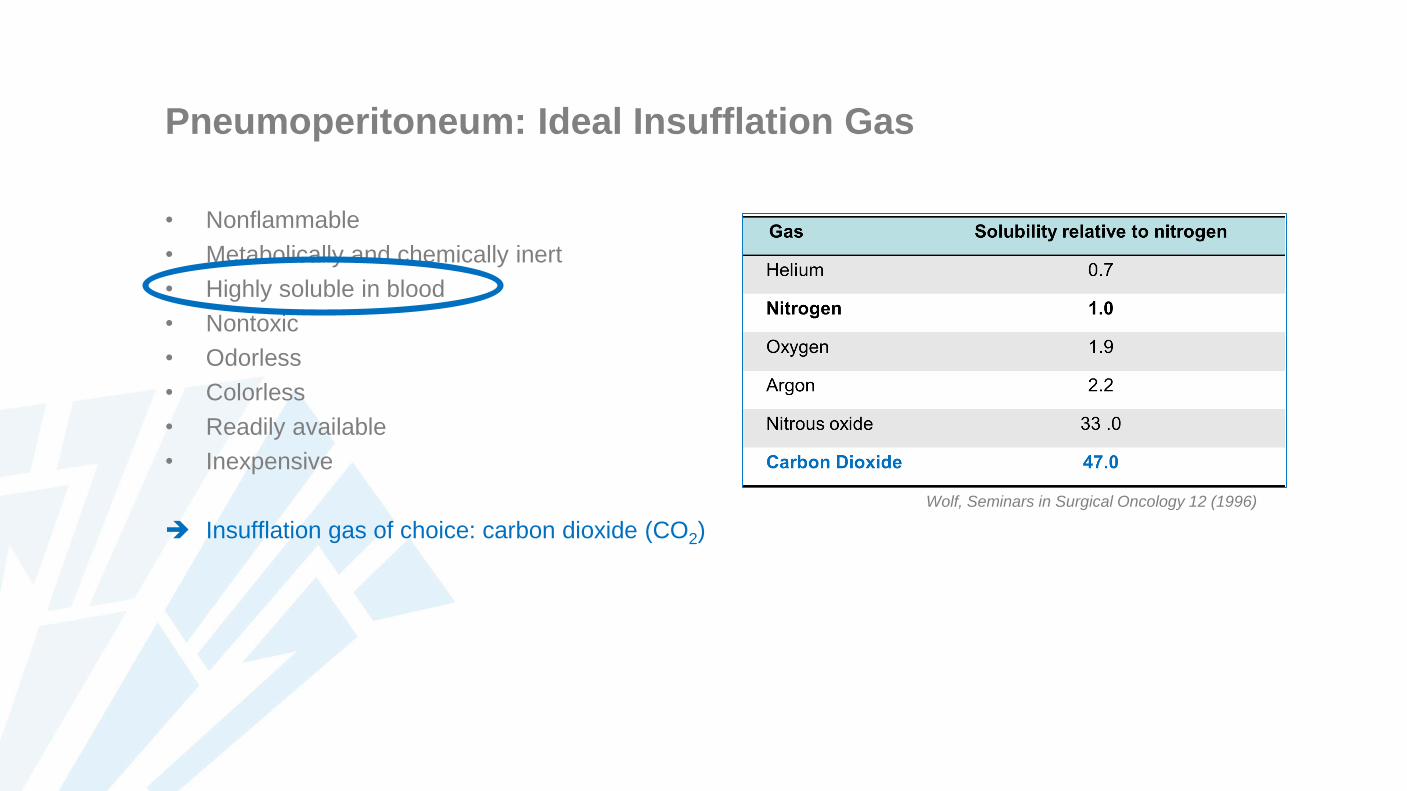
Pneumoperitoneum: Ideal Insufflation Gas
• Nonflammable
• Metabolically and chemically inert
• Highly soluble in blood
• Nontoxic
• Odorless
• Colorless
• Readily available
• Inexpensive
Insufflation gas of choice: carbon dioxide (CO2)
Wolf, Seminars in Surgical Oncology 12 (1996)
Pneumoperitoneum: Insufflation Gas
• Carbon dioxide
Highly soluble in blood
Non-flammable
Hypercapnia
Irritation of diaphragma and peritoneum ( shoulder pain)
Used for the vast majority of laparoscopic cases
• Nitrous oxide
Highly soluble in blood (but less soluble than CO2)
No irritation of diaphragm or peritoneum
• Surgery under local anesthesia
Supports combustion
• No major surgery possible
Used occasionally
CO2 – PP: Pathophysiologic Changes
• Absorption of insufflated CO2
– Extraperitoneal > intraperitoneal insufflation
• Increased intra-abdominal pressure (IAP)
– Intraperitoneal > extraperitoneal insufflation
Cardiovascular effects
Pulmonary effects
CO2 - PP: Absorption of Insufflated CO2 (1)
Parameters affecting absorption of CO2
• Approach: extraperitoneal vs intraperitoneal insufflation
• Site of surgery: pelvic vs upper abdominal surgery
• Intra-abdominal pressure
• Duration of pneumoperitoneum
• Subcutaneous emphysema
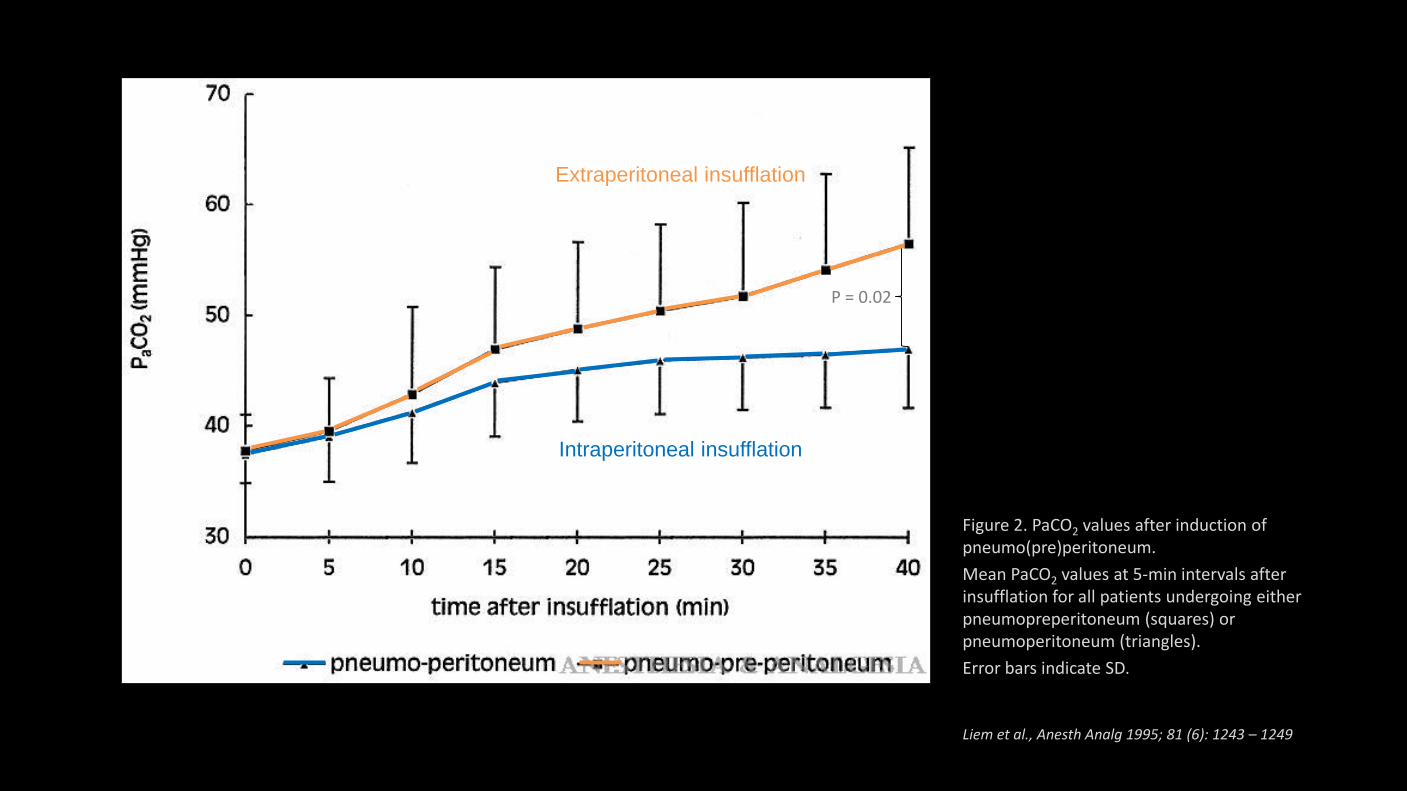
Figure 2. PaCO2 values after induction of pneumo(pre)peritoneum.
Mean PaCO2 values at 5-min intervals after insufflation for all patients undergoing either pneumopreperitoneum (squares) or pneumoperitoneum (triangles).
Error bars indicate SD.
Liem et al., Anesth Analg 1995; 81 (6): 1243 – 1249
P = 0.02
Extraperitoneal insufflation
Intraperitoneal insufflation
CO2 - PP: Absorption of Insufflated CO2 (2)
Extraperitoneal vs intraperitoneal insufflation
• Intraperitoneal insufflation of CO2
– CO2-filled space lined by a membrane
– Limited expansion (→ absorption is self-limiting)
• PaCO2 increase reaches plateau after 15 – 30 min
– Subcutaneous emphysema < 2 %
• Extraperitoneal insufflation of CO2
– CO2 migrates into tissues not confined by a membrane
– CO2 progressively dissects tissues (absorption ≈ unlimited)
• PaCO2 increase continues for much longer than 30 min
– High incidence of subcutaneous CO2 emphysema
CO2-PP: Absorption of Insufflated CO2 (3)
Upper vs lower abdominal surgery
• Upper abdominal surgery: intraperitoneal insufflation
• PaCO2 increase during 15 – 30 min
• PaCO2 increase of 20 – 30 % from baseline
• Lower abdominal surgery
– Intraperitoneal insufflation
• PaCO2 increase during 15 – 30 min
• PaCO2 increase of 10 – 15 % from baseline
– Extraperitoneal insufflation
• PaCO2 increase continues (> 30 min)
• PaCO2 increase is generally > 30 % from baseline
CO2 - PP: Absorption of Insufflated CO2 (4)
• Approach: extraperitoneal vs intraperitoneal insufflation
• Site of surgery: pelvic vs upper abdominal surgery
• Intra-abdominal pressure
– Limited effect at low IAP during intraperitoneal insufflation
– More important during extraperitoneal insufflation
• Increasing contact surface
• Duration of pneumoperitoneum
– Important during extraperitoneal insufflation
• Subcutaneous emphysema
– Complication
– May result in severe hypercarbia
– Incidence: extraperitoneal >>> intraperitoneal insufflation
CO2 – PP: Cardiovascular Effects
• Cardiac arrhythmias
• Systemic hemodynamic effects
• Regional hemodynamic effects
– Renal effects
– Splanchnic perfusion
– Venous stasis
CO2 – PP: Cardiac Arrhythmias (1)
• Reflex increase of vagal tonus
– Bradycardia, asystole
– Eliciting factors
• Stretching of the peritoneum during insufflation
• Electrocoagulation of the fallopian tubes
– Accentuated in case of
• Superficial level of anesthesia
• Patients on b – blocking drugs
– Treatment
• Immediately interrupt insufflation
• Atropine
• Deepening of anesthesia after recovery of heart rate
CO2 – PP: Cardiac Arrhythmias (2)
• Arrhythmias due to acute pathophysiologic hemodynamic changes during insufflation
– Early during insufflation
– Patients with cardiac disease may be at higher risk
• Gas embolism may cause cardiac arrhythmias
• Increased PaCO2?
– Arrhythmias also occur without a high PaCO2
– Arrhythmias do not correlate with magnitude of PaCO2
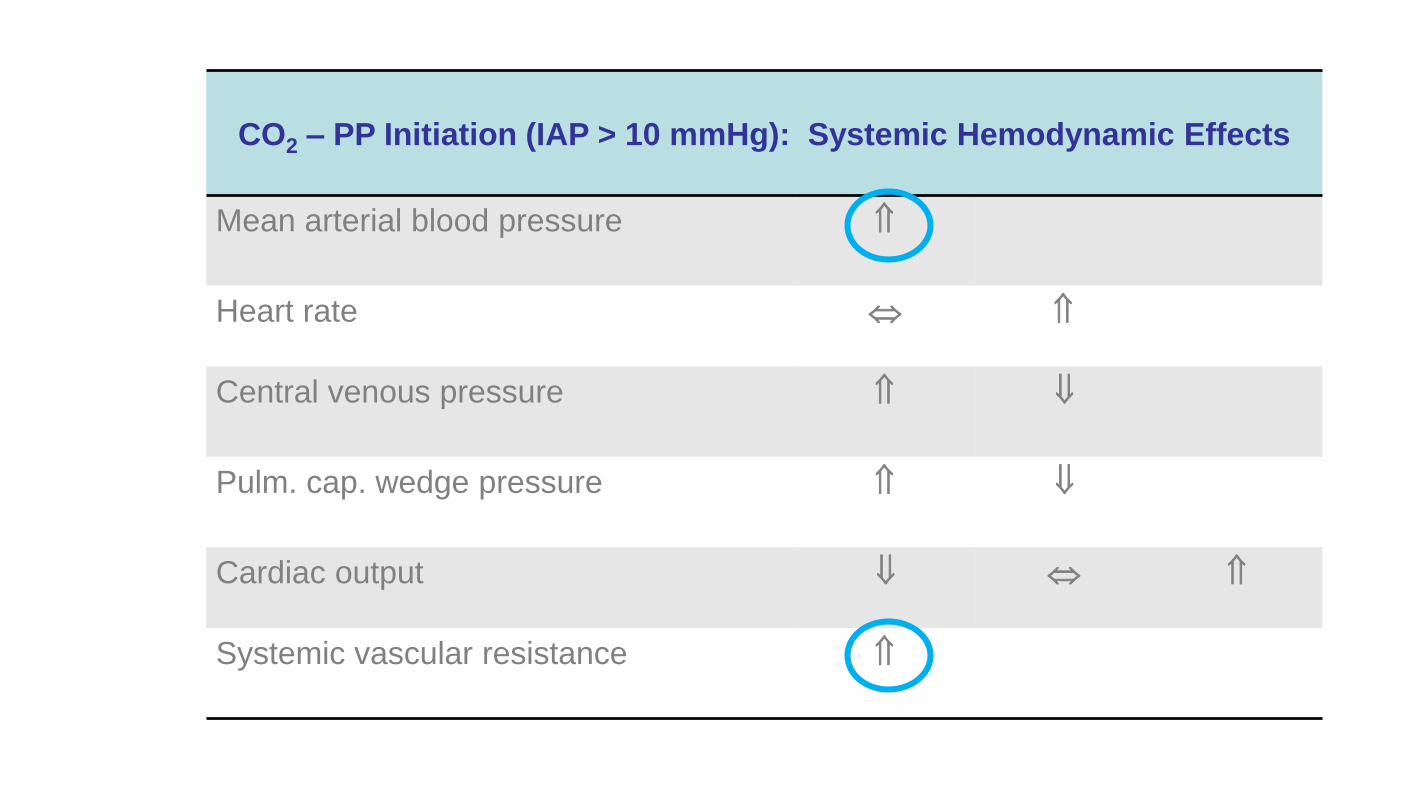
CO2 – PP Initiation (IAP > 10 mmHg): Systemic Hemodynamic Effects
Mean arterial blood pressure
Heart rate
Central venous pressure
Pulm. cap. wedge pressure
Cardiac output
Systemic vascular resistance
CO2 – PP: Systemic Hemodynamic Effects (1)
Pathophysiologic mechanism: Multifactorial
• Autotransfusion effect
– Compression of splanchnic blood vessels
• Reduced venous return
– Compression of vena cava inferior
– Increased intrathoracic pressure
– Pooling of blood in the legs
• Increased systemic vascular resistance
– Mechanical mechanism
– Release of neurohumoral factors
• Vasopressin
CO2 – PP: Systemic Hemodynamic Effects (2)
Parameters affecting balance between mechanisms
• Intra-abdominal pressure
• Intravascular volume status
• Patient positioning
• PaCO2
• Associated cardiac disease
• Anesthesia
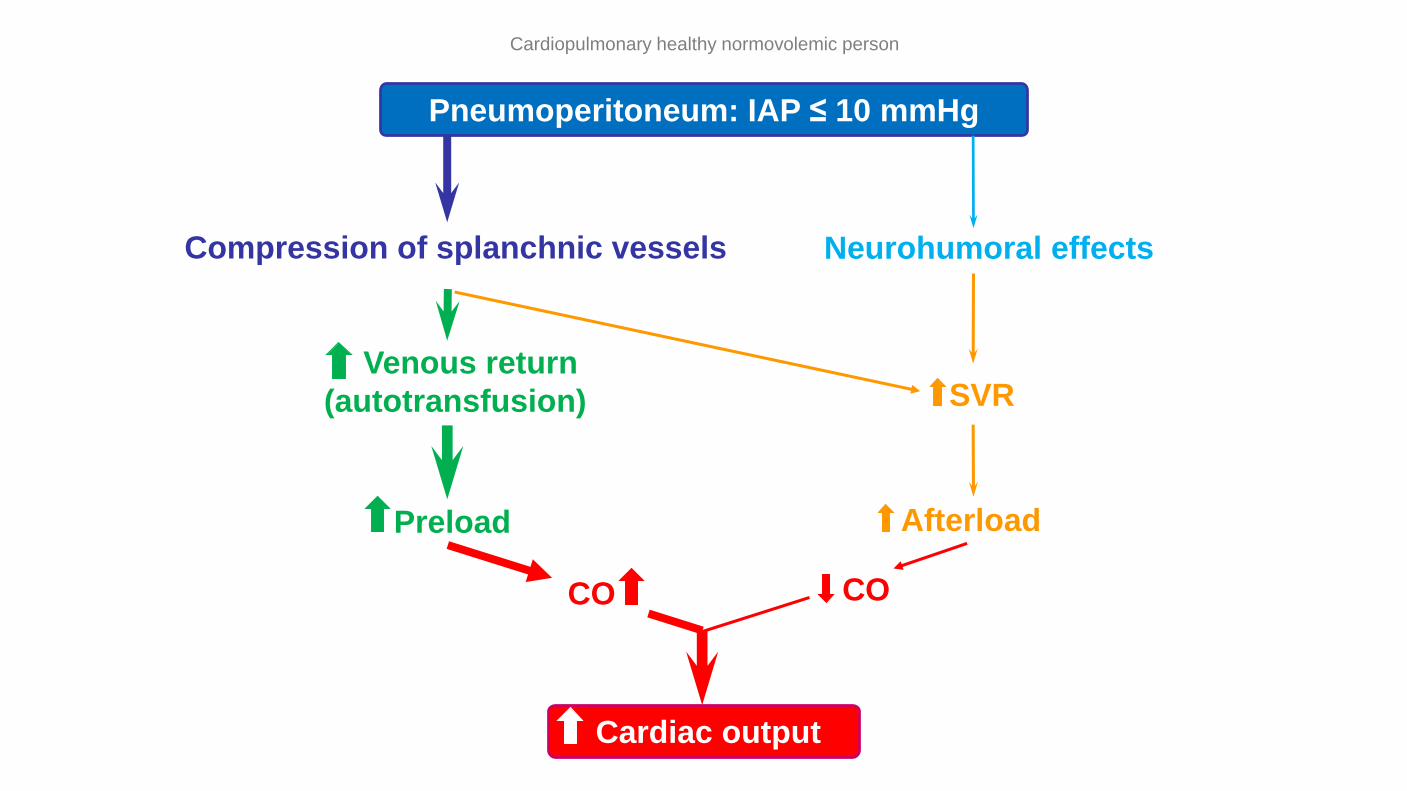
Pneumoperitoneum: IAP ≤ 10 mmHg
Cardiopulmonary healthy normovolemic person
Compression of splanchnic vessels
Venous return
(autotransfusion)
Preload
CO
Cardiac output
Neurohumoral effects
Afterload
CO
SVR
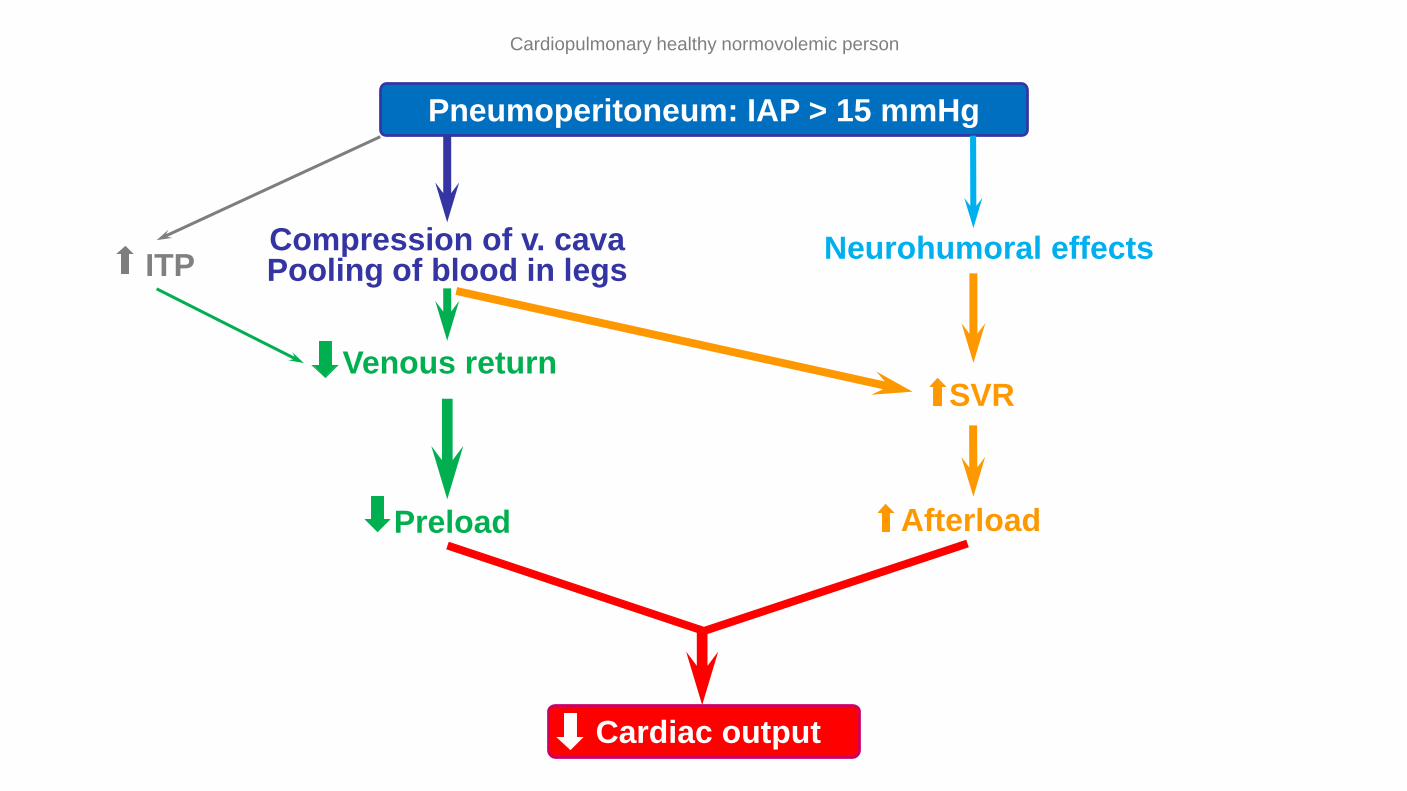
Pneumoperitoneum: IAP > 15 mmHg
Compression of v. cavaPooling of blood in legs
Cardiac output
Venous return
Preload
ITPNeurohumoral effects
SVR
Afterload
Cardiopulmonary healthy normovolemic person
CO2 – PP: Systemic Hemodynamic Effects (3)
• Intravascular volume status
– Hypovolemia increases the negative hemodynamic effects of an increased IAP
• No splanchnic recruitment possible
• Aggravates SVR increase
• Patient positioning
– Trendelenburg positioning
• Attenuates SVR increase
– Reverse Trendelenburg positioning
• Pooling of blood in the lower limbs
• Aggravates increase of SVR
• Avoid insufflation with the patient in reverse Trendelenburg position
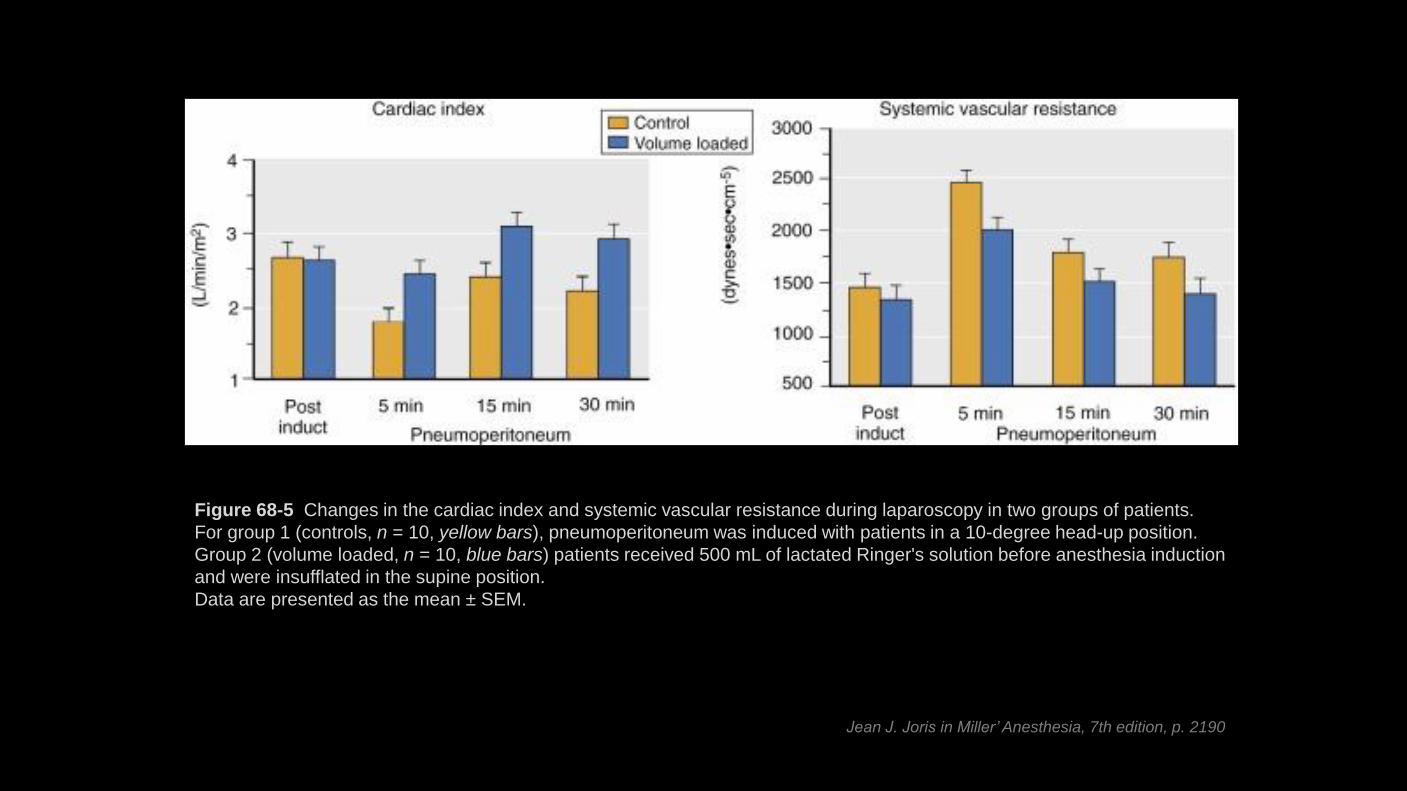
Figure 68-5 Changes in the cardiac index and systemic vascular resistance during laparoscopy in two groups of patients.
For group 1 (controls, n = 10, yellow bars), pneumoperitoneum was induced with patients in a 10-degree head-up position.
Group 2 (volume loaded, n = 10, blue bars) patients received 500 mL of lactated Ringer's solution before anesthesia induction
and were insufflated in the supine position.
Data are presented as the mean ± SEM.
Jean J. Joris in Miller’ Anesthesia, 7th edition, p. 2190
CO2 – PP: Systemic Hemodynamic Effects (4)
• PaCO2
– Moderate hypercarbia
• Slight myocardial stimulation
• Decreased systemic vascular resistance
– Severe hypercarbia
• Decreased myocardial contractility
• Decreased arrhythmia threshold
• Associated cardiac disease
– More severe hemodynamic changes?
• Anesthesia
– Vasodilatation reduces SVR increase
– Negative inotropic effects of anesthetics
CO2 – PP: Renal Effects
• Decreased diuresis, glomerular filtration rate, renal blood flow
– < 50 % of baseline values
– Normalization after deflation
• Mechanisms
– Direct renal parenchymal compression
– Venous congestion (reduced flow in v. cava inferior)
• Clinical consequences?
– Recuperation after release of pneumoperitoneum
– Postoperative renal dysfunction in specific patient populations?
• Pre-existing renal dysfunction?
CO2 – PP: Effects on Splanchnic Perfusion (1)
Mechanisms with opposing effects variable effect on splanchnic perfusion
• Mechanical compression: splanchnic blood flow decrease
– Abdominal organ microcirculation
– Abdominal blood vessels
• Direct effect of CO2 from the PP: splanchnic vasodilation
CO2 – PP: Effects on Splanchnic Perfusion (2)
• Hepatoportal circulation
– Decreased blood flow
– Postoperative liver dysfunction?
• Patients with pre-existing liver disease?
• Gastrointestinal circulation
– Effects on blood flow depend on IAP
• IAP < 12 mmHg: moderate splanchnic hyperemia
• IAP > 15 mmHg: pressure-induced blood flow decrease
– Risk of splanchnic ischemia and bacterial translocation?
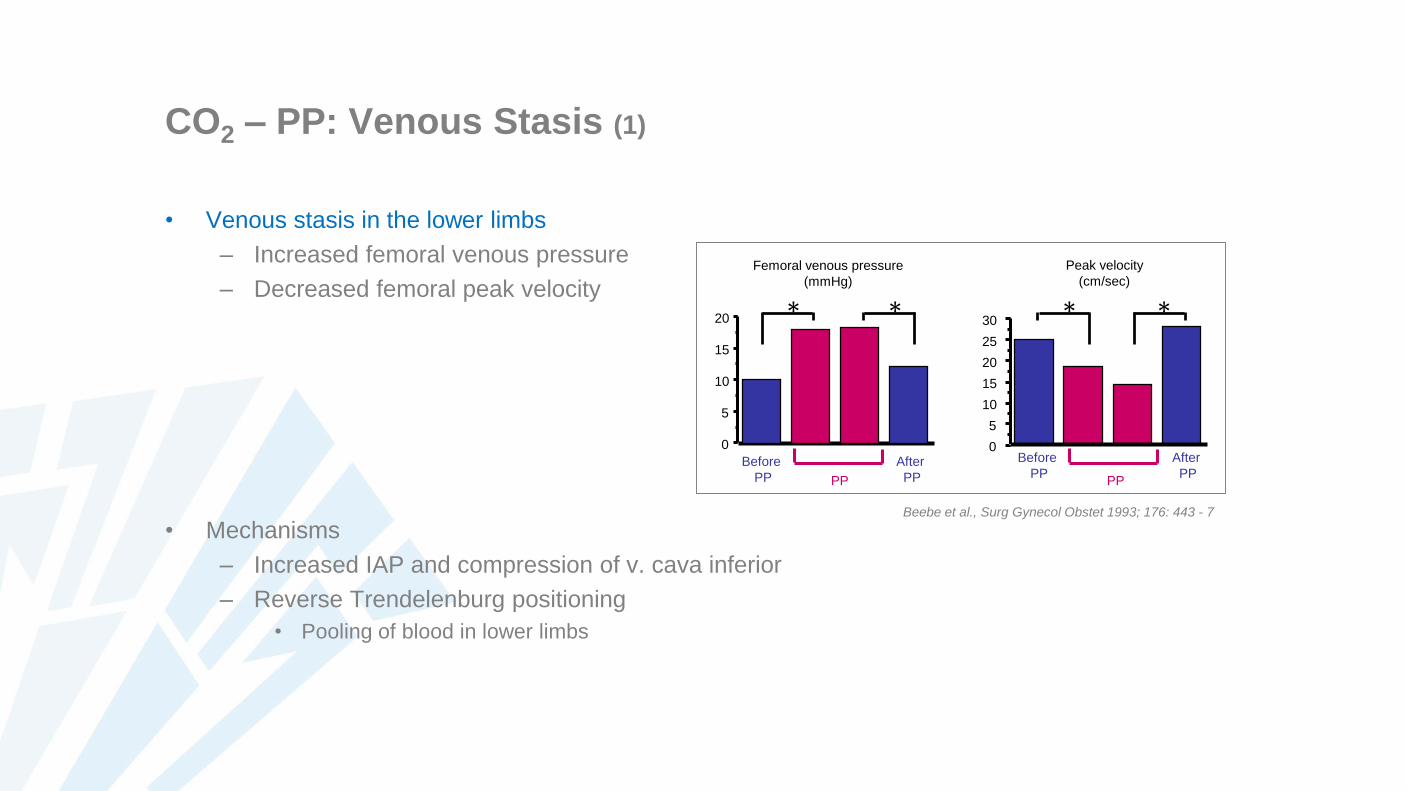
CO2 – PP: Venous Stasis (1)
• Venous stasis in the lower limbs
– Increased femoral venous pressure
– Decreased femoral peak velocity
• Mechanisms
– Increased IAP and compression of v. cava inferior
– Reverse Trendelenburg positioning
• Pooling of blood in lower limbs
0
5
10
15
20
0
5
10
15
20
25
30
PP PP
Before
PP
After
PP
Before
PP
After
PP
* * * *
Femoral venous pressure
(mmHg)
Peak velocity
(cm/sec)
Beebe et al., Surg Gynecol Obstet 1993; 176: 443 - 7

CO2 – PP: Venous Stasis (2)
Increased risk of venous thrombosis?
• Factors increasing risk vs open procedures
– Venous stasis in the legs
– Longer lasting procedures
• Factors reducing risk vs open procedures
– Earlier ambulation
– Less surgery-induced hypercoagulability
• Less tissue trauma
With thrombosis prevention: no increased risk
– Low molecular weight heparins
– Compressive stockings
CO2-PP: Pulmonary Effects
CO2 – PP has significant pulmonary effects due to
• Increased intra-abdominal pressure
• CO2 – absorption
CO2-PP: Intra-Operative Pulmonary Effects (1)
Increased intra-abdominal pressure
• Cranial displacement of diaphragm
• Increased airway pressure
• V/Q mismatches
Functional residual capacity: decrease
Thoracopulmonary compliance: decrease
– 30 – 50 % decrease in healthy persons
(Micro)Atelectasis
Impaired oxygenation and hypoxemia
– Generally no problem in healthy persons
– Obese patients, patients with pre-existing pulmonary disease
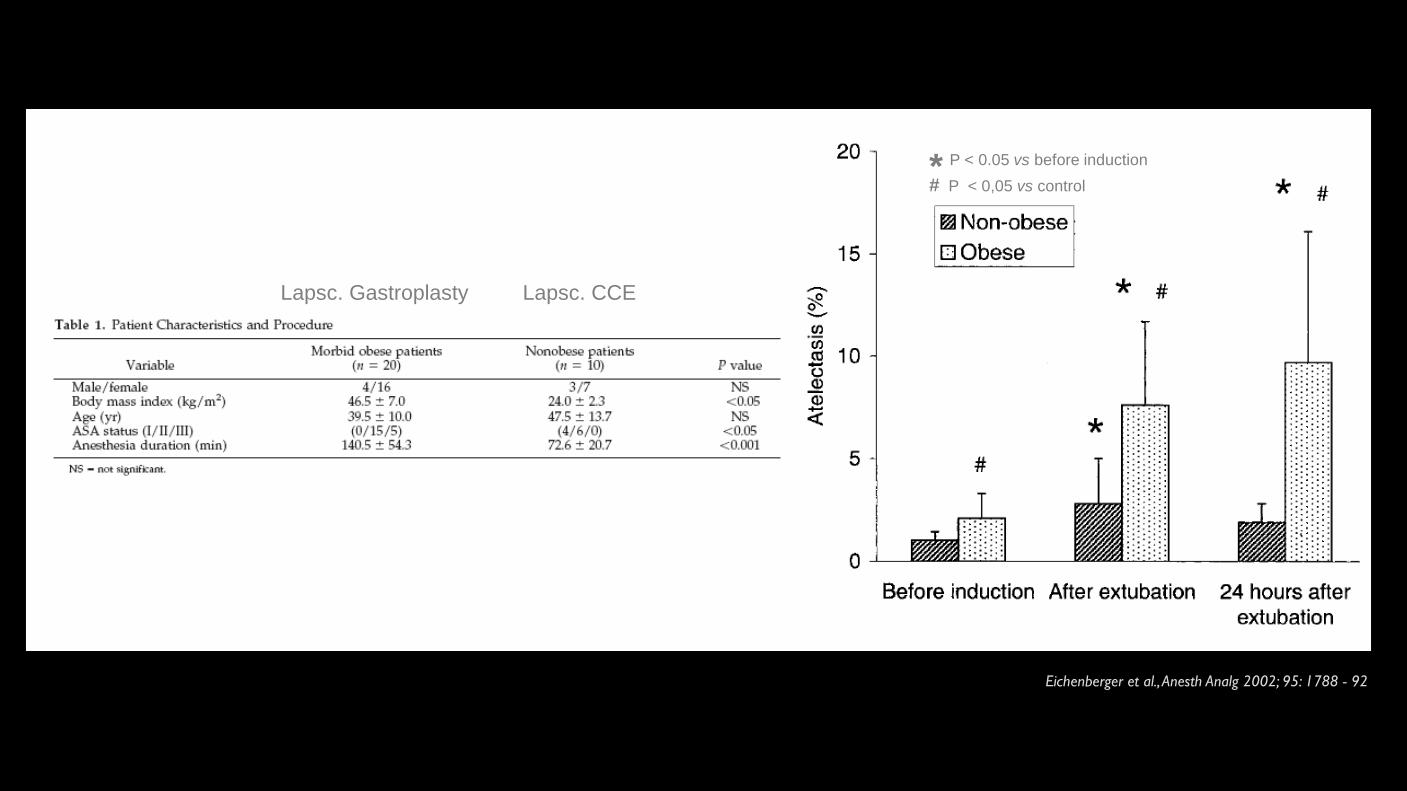
Eichenberger et al., Anesth Analg 2002; 95: 1788 - 92
* P < 0.05 vs before induction
# P < 0,05 vs control
Lapsc. Gastroplasty Lapsc. CCE
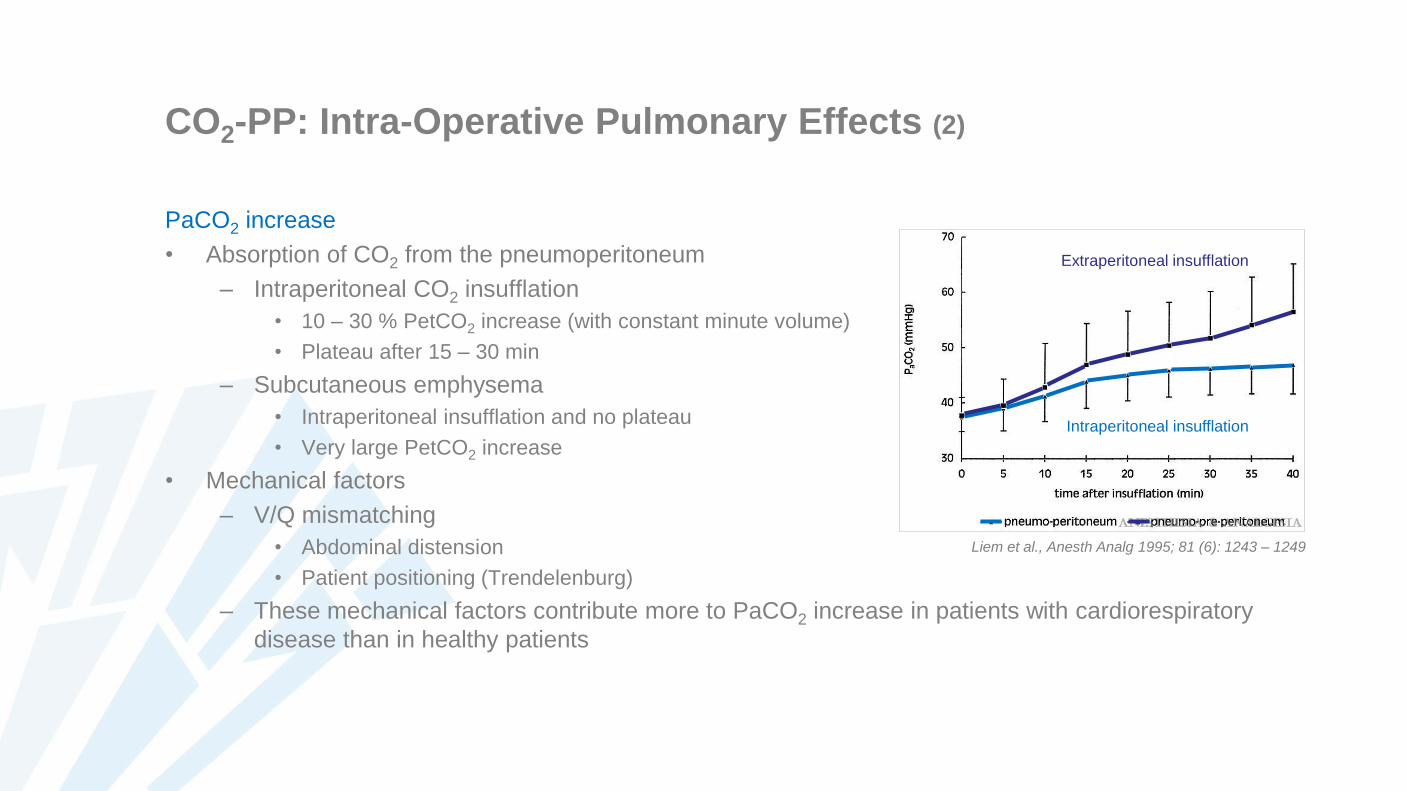
CO2-PP: Intra-Operative Pulmonary Effects (2)
PaCO2 increase
• Absorption of CO2 from the pneumoperitoneum
– Intraperitoneal CO2 insufflation
• 10 – 30 % PetCO2 increase (with constant minute volume)
• Plateau after 15 – 30 min
– Subcutaneous emphysema
• Intraperitoneal insufflation and no plateau
• Very large PetCO2 increase
• Mechanical factors
– V/Q mismatching
• Abdominal distension
• Patient positioning (Trendelenburg)
– These mechanical factors contribute more to PaCO2 increase in patients with cardiorespiratory
disease than in healthy patients
Extraperitoneal insufflation
Intraperitoneal insufflation
Liem et al., Anesth Analg 1995; 81 (6): 1243 – 1249
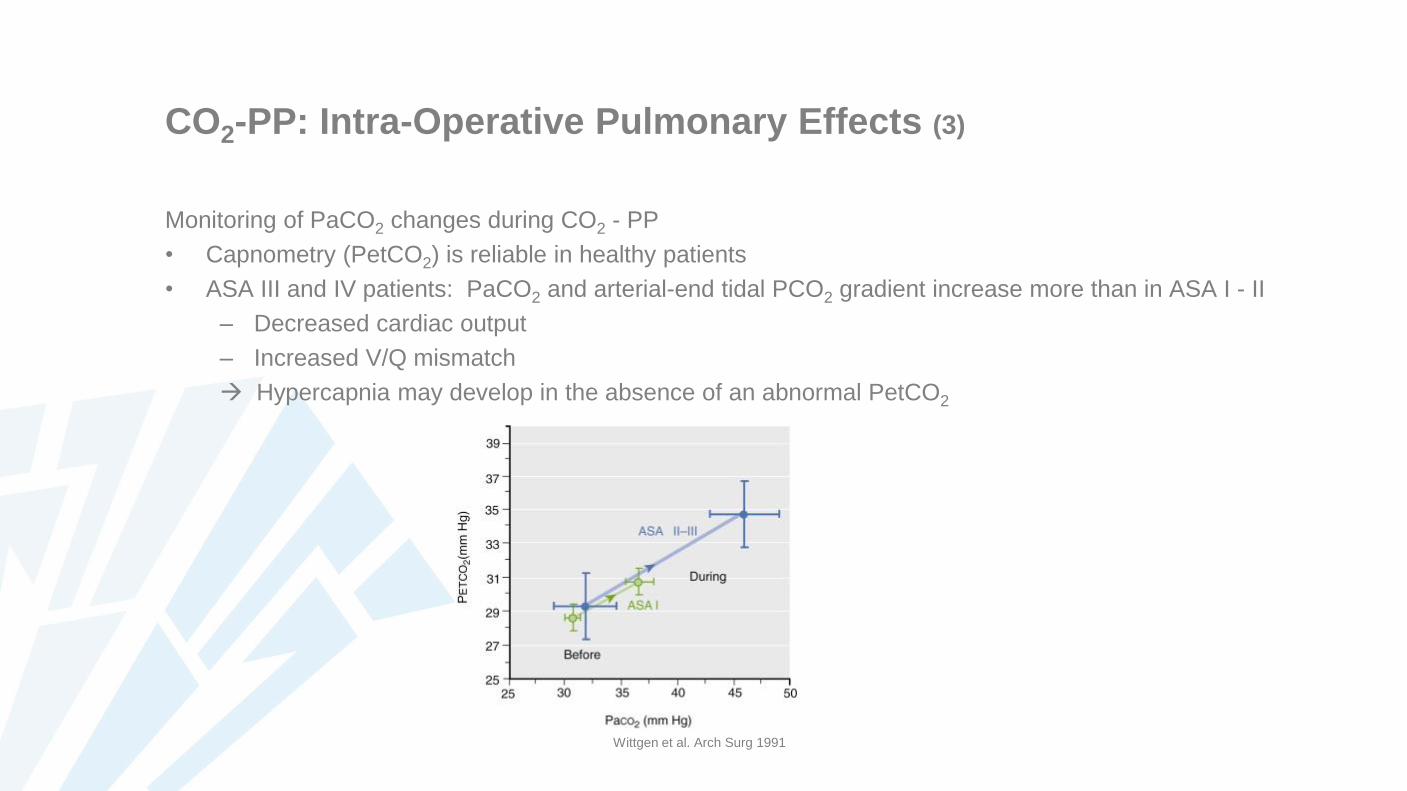
CO2-PP: Intra-Operative Pulmonary Effects (3)
Monitoring of PaCO2 changes during CO2 - PP
• Capnometry (PetCO2) is reliable in healthy patients
• ASA III and IV patients: PaCO2 and arterial-end tidal PCO2 gradient increase more than in ASA I - II
– Decreased cardiac output
– Increased V/Q mismatch
Hypercapnia may develop in the absence of an abnormal PetCO2
Wittgen et al. Arch Surg 1991
CO2-PP: Postoperative Respiratory Effects (1)
• Increased minute ventilation to eliminate absorbed CO2
– Increased respiratory rate
– Increased PetCO2
– Up to 2 hours postoperatively
– Increased work of breathing may be a problem in patients with serious cardiopulmonary disease
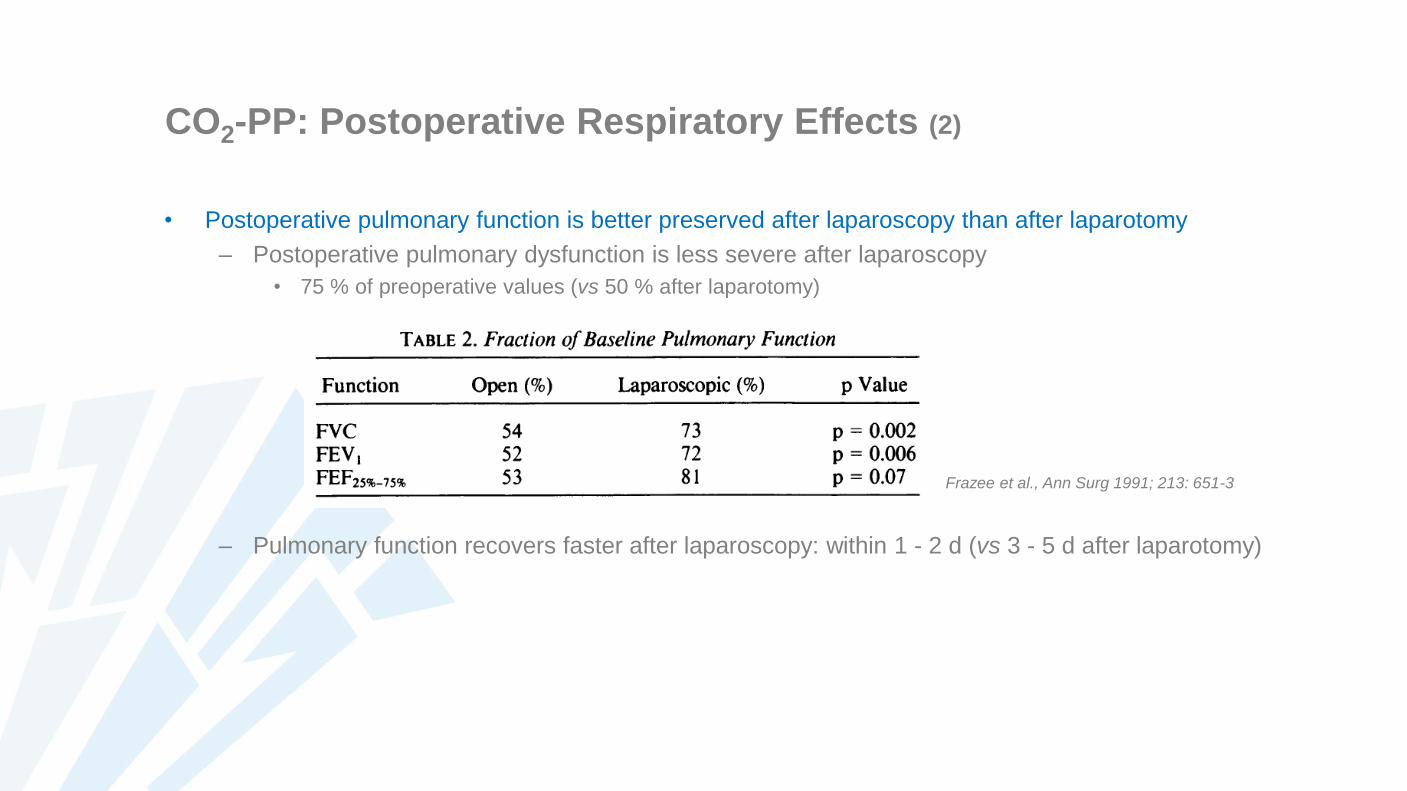
CO2-PP: Postoperative Respiratory Effects (2)
• Postoperative pulmonary function is better preserved after laparoscopy than after laparotomy
– Postoperative pulmonary dysfunction is less severe after laparoscopy
• 75 % of preoperative values (vs 50 % after laparotomy)
– Pulmonary function recovers faster after laparoscopy: within 1 - 2 d (vs 3 - 5 d after laparotomy)
Frazee et al., Ann Surg 1991; 213: 651-3
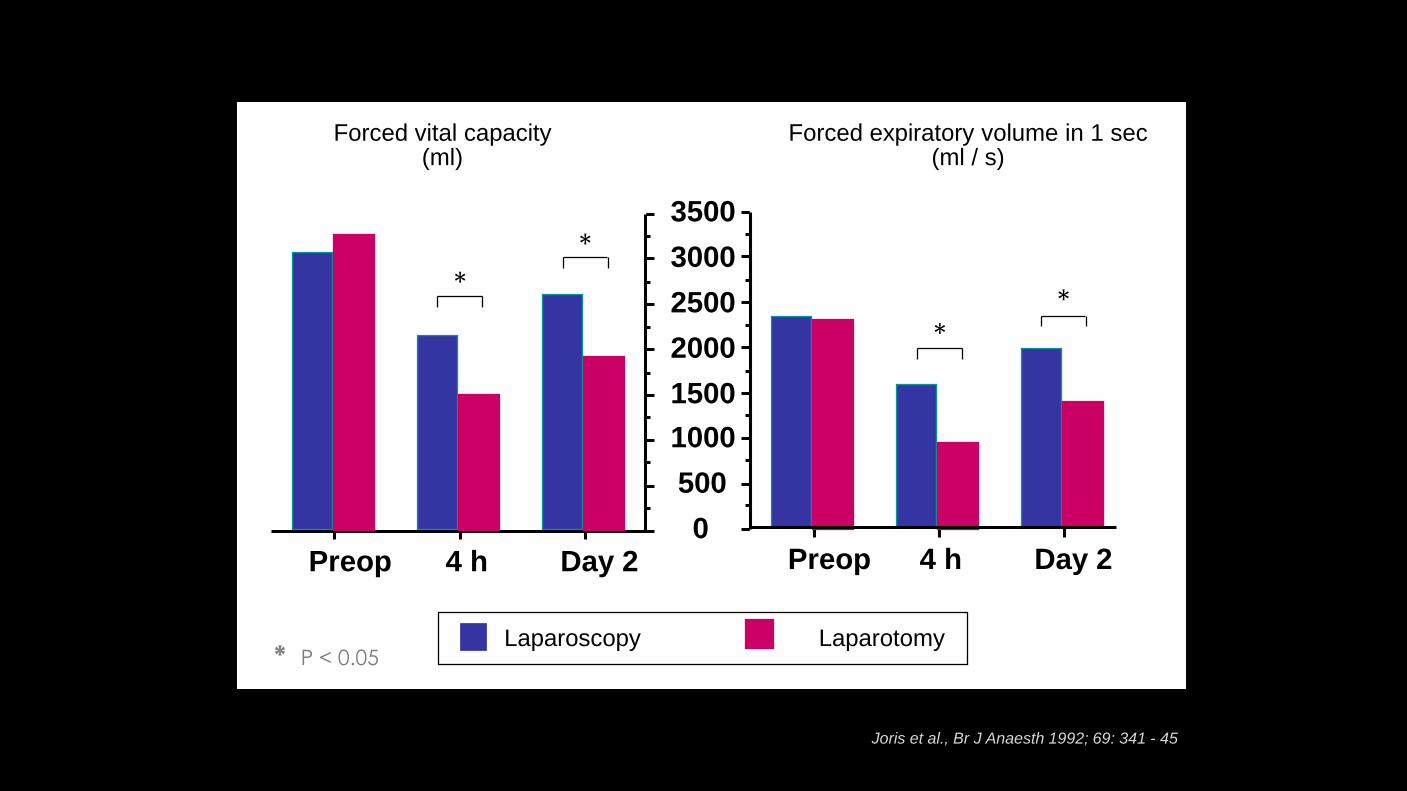
Joris et al., Br J Anaesth 1992; 69: 341 - 45
Preop 4 h Day 2 Preop 4 h Day 20
500
1000
1500
2000
2500
3000
3500
Forced vital capacity(ml)
Forced expiratory volume in 1 sec(ml / s)
*
* P < 0.05
*
**
Laparoscopy Laparotomy

CO2-PP: Postoperative Respiratory Effects (3)
• Postoperative pulmonary function is better preserved after laparoscopy than after laparotomy
– Postoperative pulmonary dysfunction is less severe after laparoscopy
• 75 % of preoperative values (vs 50 % after laparotomy)
– Pulmonary function recovers faster after laparoscopy: within 1 - 2 d (vs 3 - 5 d after laparotomy)
– Pulmonary dysfunction is less severe after gynecologic than after upper abdominal laparoscopy
Joris et al., Br J Anaesth 1997; 79: 422 - 26
CO2-PP: Postoperative Respiratory Effects (3)
• Postoperative pulmonary function is better preserved after laparoscopy than after laparotomy
– Postoperative pulmonary dysfunction is less severe after laparoscopy
• 75 % of preoperative values (vs 50 % after laparotomy)
– Pulmonary function recovers faster after laparoscopy: within 1 - 2 d (vs 3 - 5 d after laparotomy)
– Pulmonary dysfunction is less severe after gynecologic than after upper abdominal laparoscopy
– Pulmonary dysfunction after laparoscopy is more severe and recovers slower in older patients, obese
patients, smokers and COPD patients
• But also in these patients pulmonary function is better preserved after laparoscopy than after laparotomy
• Diaphragm dysfunction following upper abdominal laparoscopic surgery
– Inhibition of phrenic discharge by visceral afferents from the gallbladder area or somatic afferents
from the abdominal wall
Laparoscopy with CO2-PP: Complications (1)
• Veress needle / trocar trauma
• Subcutaneous emphysema
• Pneumothorax
Pneumomediastinum
Pneumopericardium
• Gas embolism
• Endobronchial intubation
• Peripheral nerve damage
Incidence: no precise data
Consequences may be severe
Laparoscopy with CO2-PP: Complications (2)
• Anesthesiologist may be the first to notice signs of a complication, even if the event is surgery related
• Diagnosis may be difficult and delayed
– E.g. Significant retroperitoneal hematoma may develop insidiously
– Differential diagnosis of complications with pulmonary effects
• Endobronchial intubation
• Subcutaneous emphysema
• Capnothorax
• Pneumothorax
• Massive CO2 embolism
Veress Needle / Trocar Trauma
• Injury to large blood vessels
– Aorta, inferior v. cava, iliac vessels
• Injury to abdominal wall vasculature
• Retroperitoneal hematoma
– Concealed bleeding difficult diagnosis
• Abdominal organ perforation
– Small / large bowel, liver, spleen
– Avoid gastric distension (mask ventilation)
• Diafragm, pleura, pericard perforation
CO2 – PP: Subcutaneous Emphysema (1)
• Severe hypercapnia
– Persisting in spite of increasing minute ventilation
• Mechanism
– Accidental extraperitoneal CO2 insufflation
– Side-effect of intentional extraperitoneal CO2 - PP
• Diagnosis
– Sudden large increase in PETCO2 after PetCO2 had reached a plateau
• PETCO2 increase larger than 30 % from baseline
• PETCO2 increase later than 30 min after beginning of insufflation
– Crepitus: abdominal wall, chest wall
• Sometimes there is ocular and/or pharyngeal emphysema
CO2 – PP: Subcutaneous Emphysema (2)
• Intraoperative management
– Increase minute ventilation
• Sometimes it is impossible to sufficiently increase MV and maintain normoventilation
– Reduce insufflation pressure
– Muscle relaxation
• May facilitate mechanical ventilation (?)
– If PCO2 remains too high
• Determine if hypercapnia is acceptable
• Limit duration of surgery
• Desufflate intermittently
• Abolish laparoscopic procedure
– Determined by PCO2 and cardiopulmonary status
CO2 – PP: Subcutaneous Emphysema (3)
• Postoperative attention points
– Subcutaneous CO2 readily resolves after desufflation
– Keep patient mechanically ventilated until hypercapnia is sufficiently corrected
• This avoids excessive work of breathing
– Be aware of risk of pharyngeal emphysema
• Generally, patients can be extubated, but if in doubt check presence of air leak with deflated cuff
Anesthesia and Analgesia 1995; 80: 201 - 203
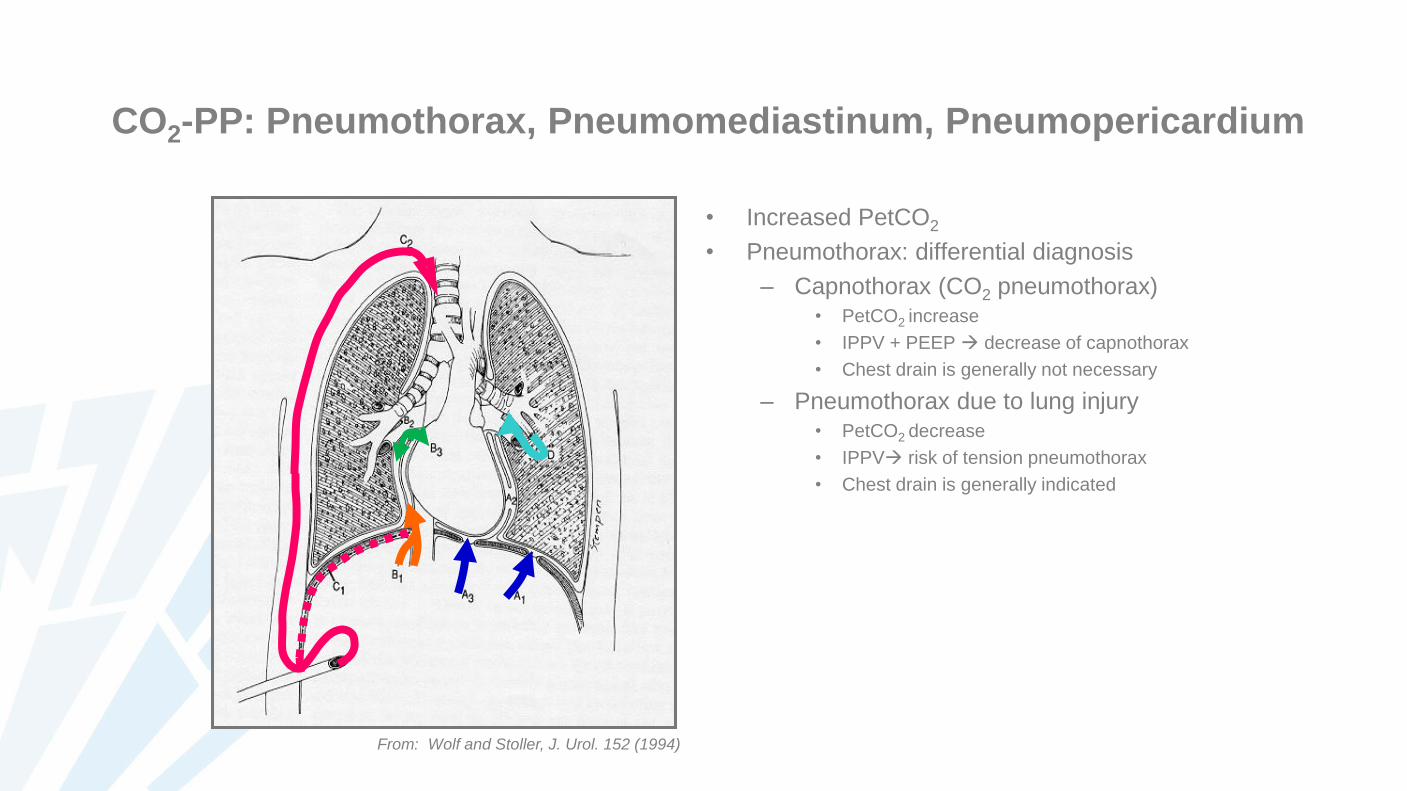
CO2-PP: Pneumothorax, Pneumomediastinum, Pneumopericardium
• Increased PetCO2
• Pneumothorax: differential diagnosis
– Capnothorax (CO2 pneumothorax)• PetCO2 increase
• IPPV + PEEP decrease of capnothorax
• Chest drain is generally not necessary
– Pneumothorax due to lung injury• PetCO2 decrease
• IPPV risk of tension pneumothorax
• Chest drain is generally indicated
From: Wolf and Stoller, J. Urol. 152 (1994)
CO2 - PP: Gas Embolism (1)
• Venous CO2 embolism
– During insufflation, early after Veress needle insertion: massive CO2 embolism
• Direct intravenous insufflation
• Insufflation in abdominal organs
Gas lock in v. cava and right atrium fall in cardiac output, possibly circulatory arrest
– During laparoscopic surgery
• Passage of CO2 into abdominal wall and peritoneal vessels
• Open vessels on liver surface during gallbladder dissection
Generally, signs and symptoms of gas embolism develop slower
• Paradoxal embolism through patent foramen ovale or ASD
– Acute right ventricular hypertension
– Cerebral CO2 embolism
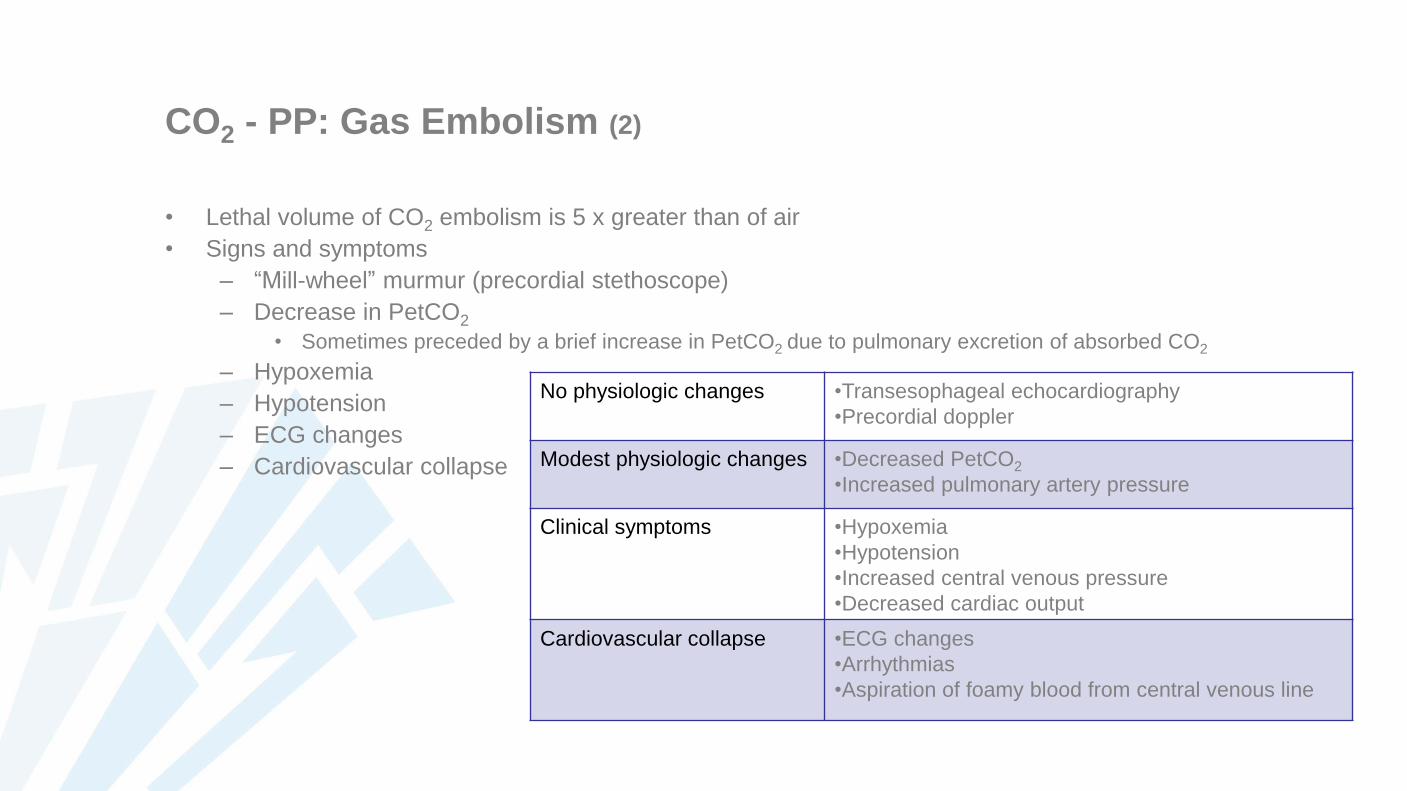
CO2 - PP: Gas Embolism (2)
• Lethal volume of CO2 embolism is 5 x greater than of air
• Signs and symptoms
– “Mill-wheel” murmur (precordial stethoscope)
– Decrease in PetCO2
• Sometimes preceded by a brief increase in PetCO2 due to pulmonary excretion of absorbed CO2
– Hypoxemia
– Hypotension
– ECG changes
– Cardiovascular collapse
No physiologic changes •Transesophageal echocardiography
•Precordial doppler
Modest physiologic changes •Decreased PetCO2
•Increased pulmonary artery pressure
Clinical symptoms •Hypoxemia
•Hypotension
•Increased central venous pressure
•Decreased cardiac output
Cardiovascular collapse •ECG changes
•Arrhythmias
•Aspiration of foamy blood from central venous line
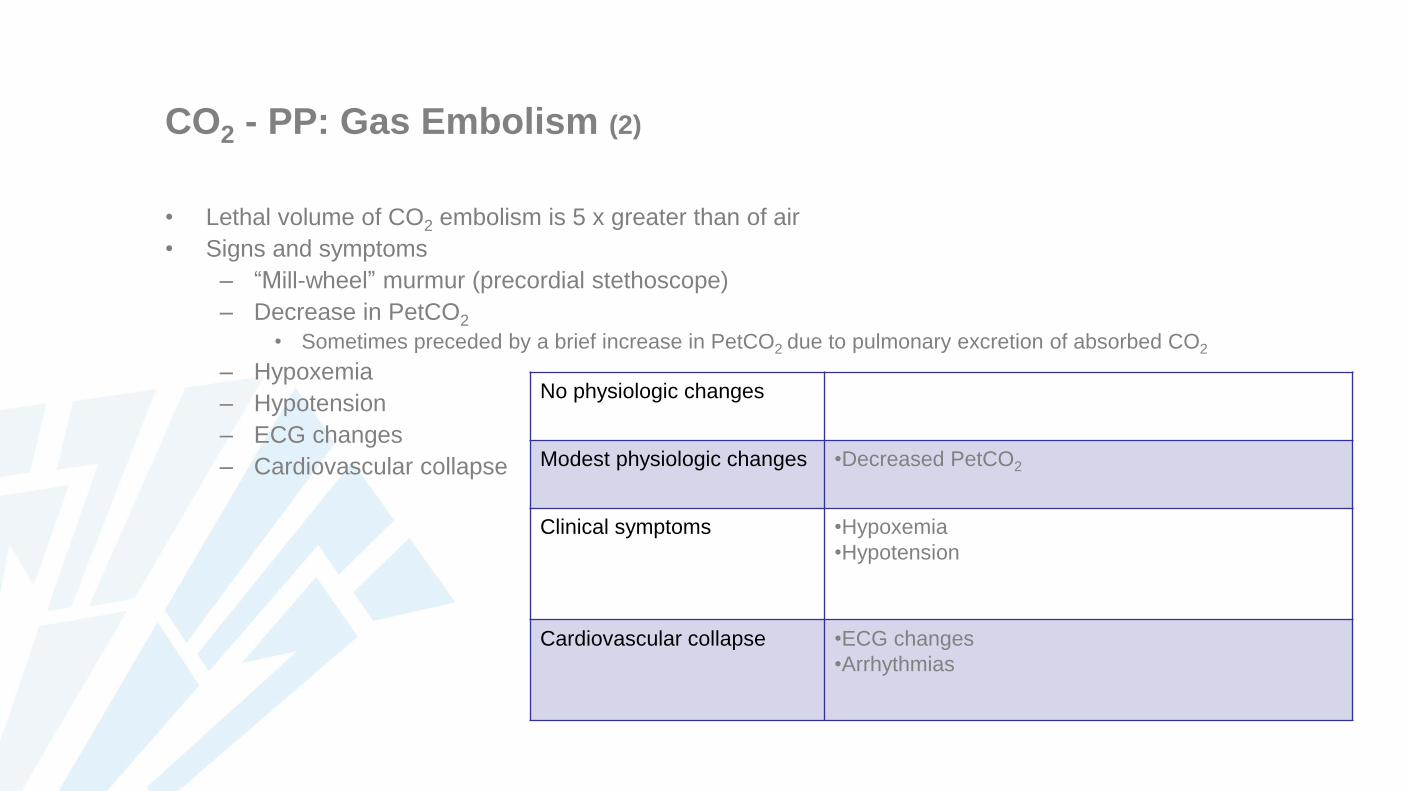
CO2 - PP: Gas Embolism (2)
• Lethal volume of CO2 embolism is 5 x greater than of air
• Signs and symptoms
– “Mill-wheel” murmur (precordial stethoscope)
– Decrease in PetCO2
• Sometimes preceded by a brief increase in PetCO2 due to pulmonary excretion of absorbed CO2
– Hypoxemia
– Hypotension
– ECG changes
– Cardiovascular collapse
No physiologic changes
Modest physiologic changes •Decreased PetCO2
Clinical symptoms •Hypoxemia
•Hypotension
Cardiovascular collapse •ECG changes
•Arrhythmias
CO2 - PP: Gas Embolism (3)
• Treatment
– Immediately stop insufflation and release pneumoperitoneum
– Ventilation with 100 % oxygen
– Durant’s position to clear right ventricular outflow
• Left lateral decubitus
• Steep Trendelenburg
– Aspiration of gas (if central venous catheter in situ)
– Cardiopulmonary resuscitation
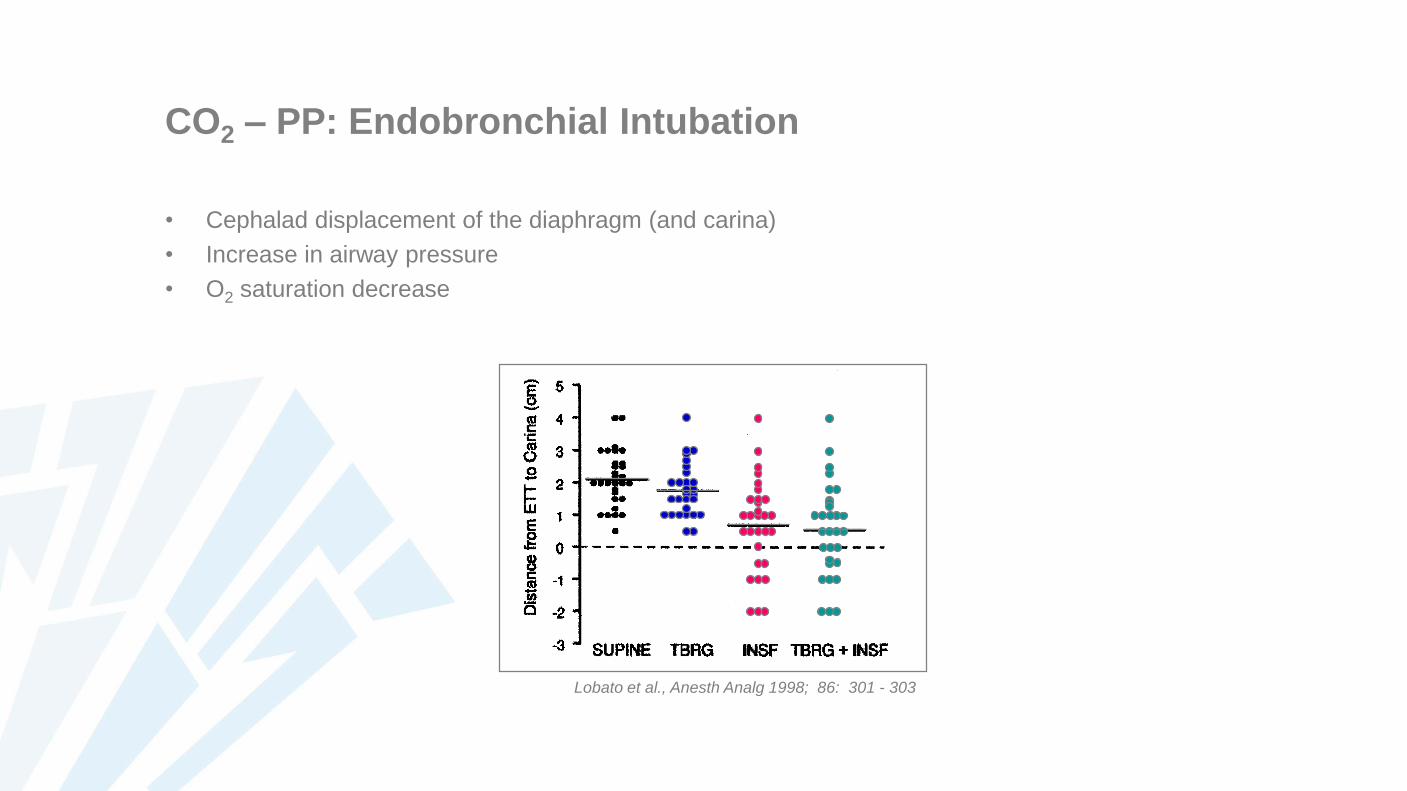
CO2 – PP: Endobronchial Intubation
• Cephalad displacement of the diaphragm (and carina)
• Increase in airway pressure
• O2 saturation decrease
Lobato et al., Anesth Analg 1998; 86: 301 - 303
Peripheral Nerve Damage
Careful positioning
• Head-down position
– Avoid shoulder braces (risk of brachial plexus lesion)
– Vacuum / anti-slip mattress
• Lithotomy position
– Common peroneal nerve lesion
– Long-lasting procedures: compartment syndrome
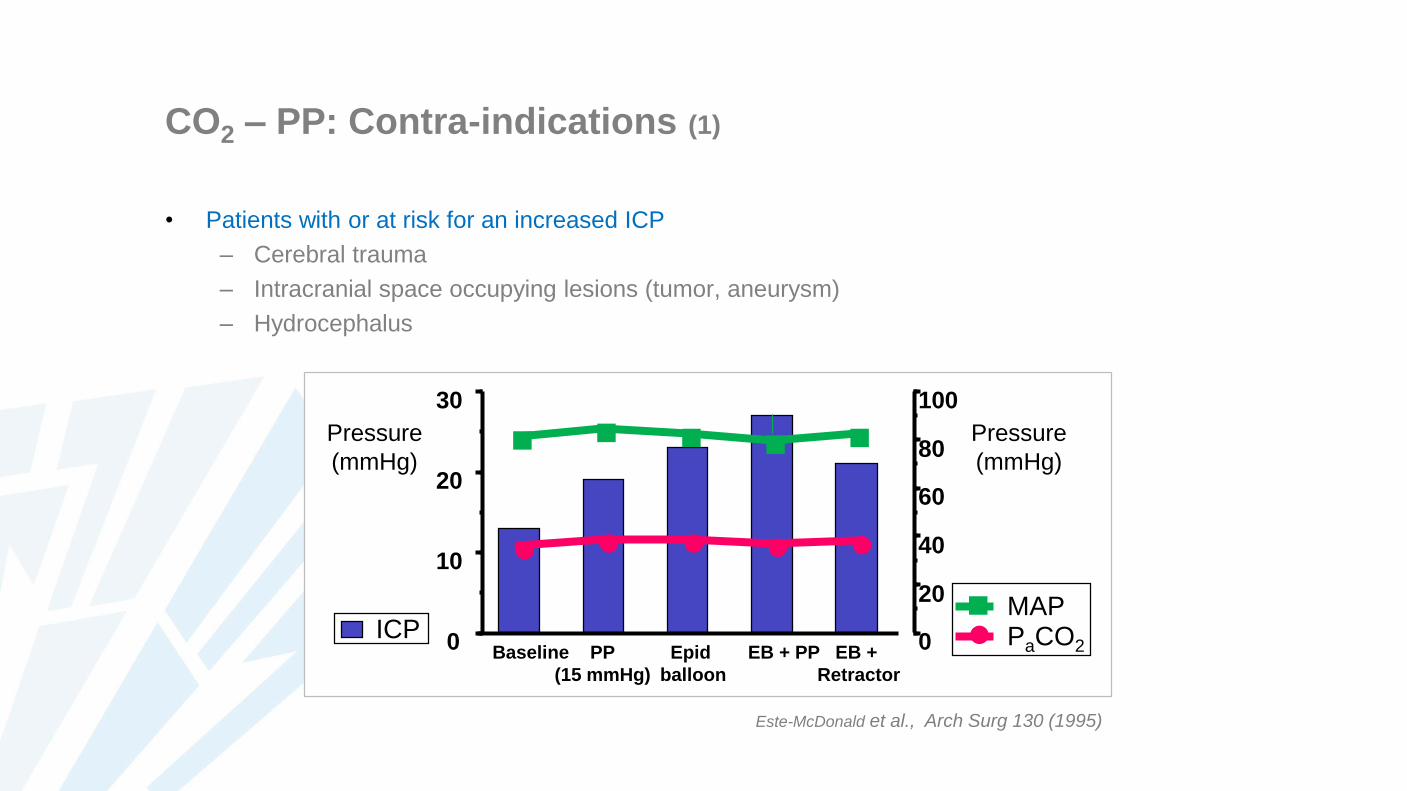
CO2 – PP: Contra-indications (1)
• Patients with or at risk for an increased ICP
– Cerebral trauma
– Intracranial space occupying lesions (tumor, aneurysm)
– Hydrocephalus
ICPBaseline PP
(15 mmHg)
Epid
balloon
EB + PP EB +
Retractor
Pressure
(mmHg)n n n n n
l l l l l
0
10
20
30
0
20
40
60
80
100
Pressure
(mmHg)
n MAP
l PaCO2
Este-McDonald et al., Arch Surg 130 (1995)
CO2 – PP: Contra-indications (2)
• Significant hypovolemia, shock
More pronounced hemodynamic effects of increased IAP
• Low cardiac output
• Renal and splanchnic hypoperfusion
• Selected cardiopulmonary problems
– Very low cardiac output
– Severe heart failure
– Cardiac right-left shunt
– Severe aortic valve insufficiency
– Severe pulmonary hypertension
– Some complex congenital cardiopathies
• Closed angle glaucoma
CO2 – PP: Relative Contra-indications
• Heart failure
• Patent foramen ovale
• Severe pulmonary disease
– Intra-operative ventilation problems
– However: less severe postoperative pulmonary dysfunction compared to laparotomy
• Significantly impaired renal function?
– Avoid prolonged laparoscopic surgery with high IAP?
– Hemodynamic optimalization to better tolerate increased IAP?
• Patients at risk for splanchnic ischemia?
– Avoid prolonged laparoscopic surgery with high IAP?
• Patient in whom an increased intraocular pressure (IOP) should be avoided
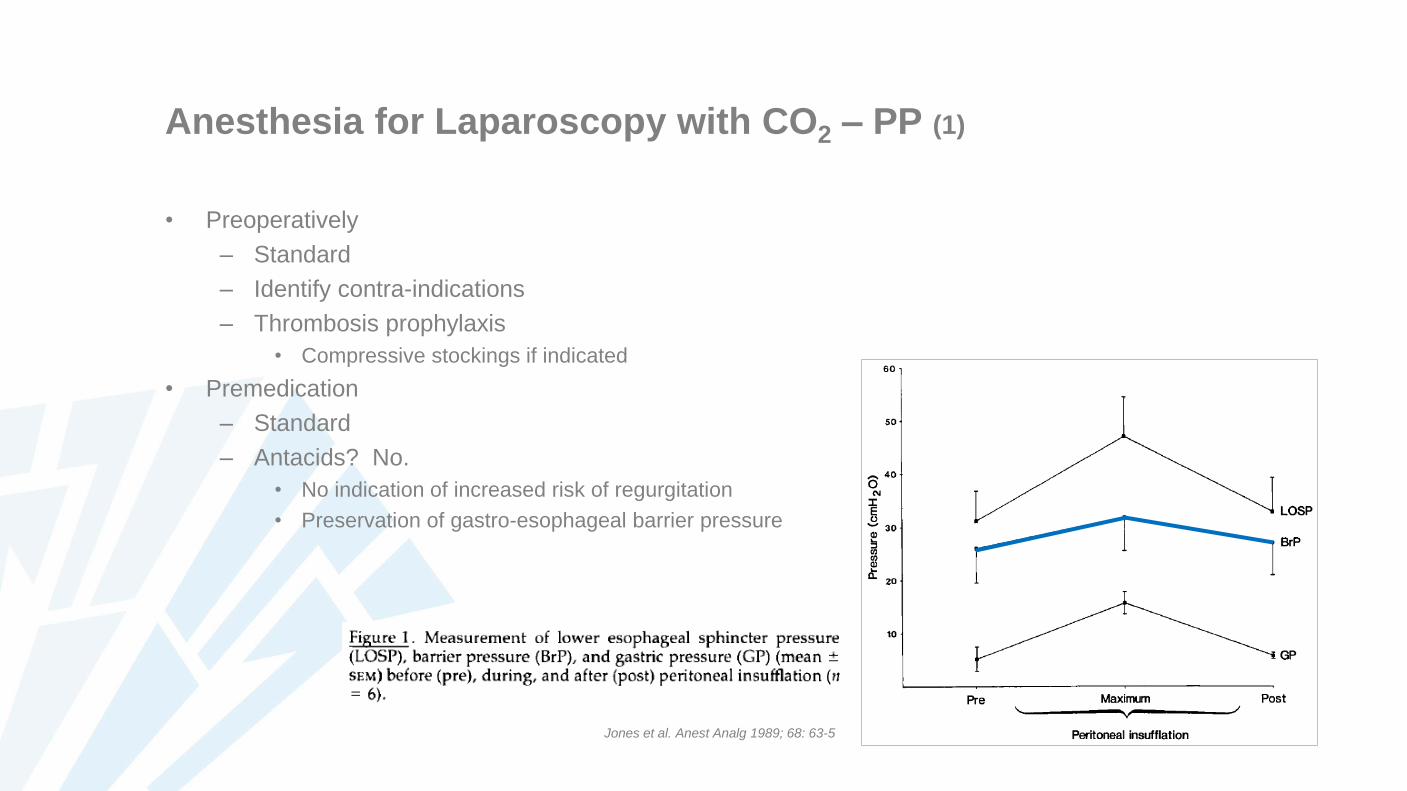
Anesthesia for Laparoscopy with CO2 – PP (1)
• Preoperatively
– Standard
– Identify contra-indications
– Thrombosis prophylaxis
• Compressive stockings if indicated
• Premedication
– Standard
– Antacids? No.
• No indication of increased risk of regurgitation
• Preservation of gastro-esophageal barrier pressure
Jones et al. Anest Analg 1989; 68: 63-5
Anesthesia for Laparoscopy with CO2 – PP (2)
• Monitoring
– Standard intraoperative monitoring
• Non-invasive blood pressure, ECG, capnography, pulse oxymetry
Only indirect evidence of PP-induced hemodynamic changes
– Arterial line
• Severe pre-existing cardiac and pulmonary disease
– Hemodynamic response to PP + positioning
– Arterial – end tidal PCO2 difference
• Surgical procedure
– Transesophageal echocardiography
• Severe cardiac co-morbidity, but indication for laparoscopy?
Anesthesia for Laparoscopy with CO2 – PP (3)
• Neuraxial anesthesia (epidural, CSE, spinal)
– Extensive block is necessary (T4 - L5) for surgical laparoscopy
– Short procedures, lower abdomen
• E.g. tubal ligation
– Reduced insufflation pressure
– No extreme head-down positioning
– Hemodynamic effects of PP under epidural anesthesia: no data
– Insufflation gas
• Nitrous oxide?
– Less irritation of peritoneum and diaphragm
– No electrocautery possible
• CO2
– Increased minute ventilation (increased work of breathing) to maintain PaCO2
For selected, brief procedures without electrocautery only
Anesthesia for Laparoscopy with CO2 – PP (4)
• General anesthesia: technique of choice for laparoscopy
– Intubation and mechanical ventilation
• Technique of choice
• Adjust minute volume to maintain PetCO2 between 35 - 40 mmHg
• Check position of endotracheal tube after induction of PP
– Risk of endobronchial intubation
– Check again with Trendelenburg positioning
• Laryngeal mask?
– Possible, but disadvantages
– Does not protect airway against aspiration of gastric contents
– Ventilation problems
» ↓ thoracopulmonary compliance and airway pressure > 20 cmH2O
» ProSeal laryngeal mask?
Anesthesia for Laparoscopy with CO2 – PP (5)
• General anesthesia: technique of choice for laparoscopy
– Antiemetic
• Laparoscopy: increased risk of PONV (40 – 75% of patients)
– Nitrous oxide ? Controversial
• Bowel distension?
– Not convincingly demonstrated
• Worsens cardiovascular effects of CO2 emboli
• Explosion hazard?
– Bowel perforation and combustion of bowel gases
– Unlikely in routine clinical practice
• Increased incidence of PONV?
No conclusive evidence against the use of N2O
Anesthesia for Laparoscopy with CO2 – PP (6)
• Recovery and postoperative care
– Postoperative elimination of absorbed CO2
• Absorption in blood of residual CO2
• CO2 release from body stores
Increased work of breathing
Caution in patients with severe cardiopulmonary disease
– Nausea and vomiting
• Prevention indicated
Anesthesia for Laparoscopy with CO2 – PP (7)
• Postoperative analgesia
– Incisional pain, intra-abdominal (visceral) pain, shoulder pain
– After laparoscopy pain is generally less intense and of shorter duration than after laparotomy, but
• Pain is variable in duration, severity and character
• Patients may experience severe pain after laparoscopic surgery
Anesthesia for Laparoscopy with CO2 – PP (8)
• Postoperative analgesia: multimodal approach
– Intraperitoneal local anesthetic
• Conflicting results
• More successful after pelvic laparoscopy?
• Generally not effective for visceral pain
– Infiltration of skin with local anesthetic
– Evacuation of insufflation gas
• Residual CO2 causes shoulder pain
• Gas drain
– NSAIDs
• Reduced need for opioid analgesia
– Opioids may be necessary!